The neuropathology of CAG repeat diseases: review and update of genetic and molecular features
26
Brain Pathology 7: 901-926 (1997) The Neuropathology Review and Features Update of CAG. Repeat of Genetic Yves Robitaillel, lscia Lopes-Cendesl, Mark BecheP, Guy Rouleau', Arthur W. Clark' 1 Departments of Pathology, University of Montreal, and Neurosurgery and Neurology, McGill University, Montreal, Quebec, Canada Department of Pathology (Neuropathology), Johns Hopkins University School of Medicine, Baltimore, Maryland, USA Departments of Pathology and Clinical Neuroscience and the Neuroscience Research Group, University of Calgary, Alberta, Canada Classificationof inherited neurodegenerativedis- eases is increasingly based on their genetic fea- tures, which supplement, clarify, and sometimes replace the older clinical and pathologic schemata. This change has been particularly rapid and impres- sive for the CAG repeat disorders. In Huntington's disease, X-linked spinobulbar muscular atrophy, dentatorubropallidoluysian atrophy, and a series of autosomal dominant cerebellar atrophies, genetic advances have resolved many nosologic issues, and opened new avenues for exploration of pathogene- sis. In this review, we summarize classic and current concepts in neuropathology of these CAG repeat diseases. Introduction: the neuropathology of a genetically defined group of diseases The CAG repeat diseases constitute the majority of so-called "trinucleotide repeat disorders." The first trin- ucleotide repeat diseases were defined as such in 1991. Previous classifications relied on heterogeneous and overlapping clinical and pathologic features. Current classification is based on their genetic determinants, which are inherited expansions of trinucleotide repeat sequences at loci specific to each disorder (110, 174, 225). In most, trinucleotide repeat sizes can increase still further in offspring of an affected subject; and larg- er size of the repeat regions generally is associated with earlier age of onset of the disease (intergenerational anticipation). CAG repeat disorders have now been Corresponding author: Yves Robitaille, Ste-Justine Hospital, Department of Pathology, 3701 CBte Ste-Catherine Road, Montreal, Quebec, Canada H3T 1C5; Tele.: 514/345-4649; Fax: 51413404545; E-mail: yes-robitaille Q algene.com Diseases: and Molecular linked to at least eight loci scattered through the human genome; and al. least four other loci cause non-CAG trinucleotide repeat diseases (La Spada and Clark, this symposium). The CAG repeat sequences encode polyglutamine tracts in the respective genes. Relatively modest increas- es in size of the CAG repeat sequence (and polygluta- mine tracts) is sufficient to produce disease (83, 174). Hence the expansions can be termed "small -scale repeat expansions" (82). By contrast, the non-CAG trinu- cleotide repea': disorders derive from trinucleotide repeat sequences which require much larger expansions to produce disease. These are located in noncoding regions of the respective genes (1 10, 225). The term "large scale repeat expansions" might be used to desig- nate this grou?, which includes fragile X syndrome (frax), myotonic dystrophy (MD), and Friedreichs atax- ia (FA). Other large scale trinucleotide repeat expan- sions have been discovered, but the related disorders are less well studied ( 110, 225). The three "classic't non-CAG trinucleotide repeat disorders are distingusihed by their triplets (CGG for frax, CTG for MD, GAA for FA) and their modes of inheritance (X -linked for frax, autosomal dominant for MD, autosomal recessive for FA). Recent paper s should be consulted (20, 21, 127, 131, 143). The proteins are defined for each of the genes (21, 127, 169, 189). Table I summarizes these features. The reader is referred to reviews and recent publications (13, 22, 26, 35, 42, 48, 49, 53, 67, 93, 97, 102, 110, 111, 153, 218, 220, 225, 230). This symposium focuses on the CAG-repeat disor- ders because of the unifying theme inherent in the type of mutation they all share. They include X-linked spin- obulbar muscular atrophy of Kennedy (SBMA), at least four autosomal dominant cerebellar ataxias, denta- torubro-pallic.oluysian atrophy (DRPLA), and Huntington's disease (HD). The affected proteins are distinct, and the mutated genes widely scattered in the genome. Given this diversity, and the shared feature of CAG repeat expansion, the pathogenetic mechanisms would be expected to include both features in common and features unique to each disorder.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The neuropathology of CAG repeat diseases: review and update of genetic and molecular features

Brain Pathology 7: 901-926 (1997)
The Neuropathology Review and Features
Update of CAG. Repeat of Genetic
Yves Robitaillel, lscia Lopes-Cendesl, Mark BecheP, Guy Rouleau', Arthur W. Clark'
1 Departments of Pathology, University of Montreal, and Neurosurgery and Neurology, McGill University, Montreal, Quebec, Canada Department of Pathology (Neuropathology), Johns Hopkins University School of Medicine, Baltimore, Maryland, USA Departments of Pathology and Clinical Neuroscience and the Neuroscience Research Group, University of Calgary, Alberta, Canada
Classification of inherited neurodegenerative dis- eases is increasingly based on their genetic fea- tures, which supplement, clarify, and sometimes replace the older clinical and pathologic schemata. This change has been particularly rapid and impres- sive for the CAG repeat disorders. In Huntington's disease, X-linked spinobulbar muscular atrophy, dentatorubropallidoluysian atrophy, and a series of autosomal dominant cerebellar atrophies, genetic advances have resolved many nosologic issues, and opened new avenues for exploration of pathogene- sis. In this review, we summarize classic and current concepts in neuropathology of these CAG repeat diseases.
Introduction: the neuropathology of a genetically defined group of diseases
The CAG repeat diseases constitute the majority of so-called "trinucleotide repeat disorders." The first trin- ucleotide repeat diseases were defined as such in 199 1. Previous classifications relied on heterogeneous and overlapping clinical and pathologic features. Current classification is based on their genetic determinants, which are inherited expansions of trinucleotide repeat sequences at loci specific to each disorder (110, 174, 225). In most, trinucleotide repeat sizes can increase still further in offspring of an affected subject; and larg- er size of the repeat regions generally is associated with earlier age of onset of the disease (intergenerational anticipation). CAG repeat disorders have now been
Corresponding author: Yves Robitaille, Ste-Justine Hospital, Department of Pathology, 3701 CBte Ste-Catherine Road, Montreal, Quebec, Canada H3T 1C5; Tele.: 514/345-4649; Fax: 51413404545; E-mail: yes-robitaille Q algene.com
Diseases: and Molecular
linked to at least eight loci scattered through the human genome; and al. least four other loci cause non-CAG trinucleotide repeat diseases (La Spada and Clark, this symposium).
The CAG repeat sequences encode polyglutamine tracts in the respective genes. Relatively modest increas- es in size of the CAG repeat sequence (and polygluta- mine tracts) is sufficient to produce disease (83, 174). Hence the expansions can be termed "small -scale repeat expansions" (82). By contrast, the non-CAG trinu- cleotide repea': disorders derive from trinucleotide repeat sequences which require much larger expansions to produce disease. These are located in noncoding regions of the respective genes (1 10, 225). The term "large scale repeat expansions" might be used to desig- nate this grou?, which includes fragile X syndrome (frax), myotonic dystrophy (MD), and Friedreichs atax- ia (FA). Other large scale trinucleotide repeat expan- sions have been discovered, but the related disorders are less well studied ( 110, 225).
The three "classic't non-CAG trinucleotide repeat disorders are distingusihed by their triplets (CGG for frax, CTG for MD, GAA for FA) and their modes of inheritance (X -linked for frax, autosomal dominant for MD, autosomal recessive for FA). Recent paper s should be consulted (20, 21, 127, 131, 143). The proteins are defined for each of the genes (21, 127, 169, 189). Table I summarizes these features. The reader is referred to reviews and recent publications (13, 22, 26, 35, 42, 48, 49, 53, 67, 93, 97, 102, 110, 111, 153, 218, 220, 225, 230).
This symposium focuses on the CAG-repeat disor- ders because of the unifying theme inherent in the type of mutation they all share. They include X-linked spin- obulbar muscular atrophy of Kennedy (SBMA), at least four autosomal dominant cerebellar ataxias, denta- torubro-pallic.oluysian atrophy (DRPLA), and Huntington's disease (HD). The affected proteins are distinct, and the mutated genes widely scattered in the genome. Given this diversity, and the shared feature of CAG repeat expansion, the pathogenetic mechanisms would be expected to include both features in common and features unique to each disorder.

. . ... . .
! Fragile X Mytonic Dystro,uhy .criQdreiC,* S 4!i?XM' Fragile X (FRAXA) (FRAXE)
_ _ _. __ . ... . . __ . . .- . - I
Hereditary transmission
Gene locus
Triplet repeal
Encoded protein
Principal clinical fealures
Principle types of I e s i o n s
Main neuroanalomic distribution of the lesions
X-IinKed
Xq27 3
C G G
FMR-I (RNA-binding protein)
Mer.lal Retarda!ion Epilepsy Prograthism Enlarged ears Macrogenitalia
Selective hypertrophy of ! cerebral structures
Atrophy posterior fossa on MFI Microcephaly Neuronal heterotopias Dendritic spine abnormalities
Hippocampi, Striatum Cerebellum
' :;ECSSsI:T I Autoscrral Dominant X-:inked
XqPE
G C C
:5q132-13 S ! I C T G
unknown Myotonin Protein Kinase
Mental Retardation ~ Distal Myopathy wit? milder ihan in FFAXA ' Myolonia
I
Mental Fe:arda:ion ' Frontal Baldness i Hypogcnadisn
unknown Myopathic !eatures in skeletal muscle Cerebral a:rophy with overexpression of Tau epitopes. hyperphosphorylate6
unknown I I Distal skeletal rnusc:e , Temporal lobes
C313.q:: '
I GAA
Frataxin-Fhosphatidyl- iosilol Kinase
Ptaxia gait 1 Dysarthna Hyporeflexia Babinski signs
: Lcss of prcpr:ocepl.cr Carciomyccathy
Neuronai loss and glicsis Waillerian degenera!ion 31 long trac!s. spinal Cora Sensory axonopathy
I
Dorsal root ganglia Spinocerebellar tracts Posterior columns Lateral & Clarke's cdumns
. . . - .. .
'Freidreich's A:axia with vitamin E deficiency: locus mapped on ch. B q not associated with triplet repeats. see Belal S et al (1995) Clin Neurosc 3: 39-42
Table 1. Non-CAG Trinucleotide Repeat Disorders
The specific disease-associated proteins include the androgen receptor for SBMA, well characterized before its involvement in SBMA was discovered; and a series of proteins discovered as a result of the genetic investi- gations on the corresponding disease: ataxins 1, 2, and 3 (in SCA1, SCA2, and SCA3, respectively), atrophin (DRPLA), and huntingtin (HD). Recently the CAG expansion of SCA6 was identified in the gene for the human CY 1 A voltage-dependent calcium channel protein. The gene affected in SCA7 has not yet been character- ized.
Increasing size of the CAG repeat expansion does correlate with increasing pathologic severity for several of these disorders. But the genes affected, the anatomic sites targeted, and other clinicopathologic features dif- fer, as summarized in Table 2. Homozygosity has been associated with more severe disease in DRPLA (177) and SCA3MJD (29, 192) but not in HD (133, 226). Although recent genetic advances have clarified many nosologic issues, they have also raised a series of ques- tions about the pathologic correlates which previous pathologic studies either were not designed to answer, or could not have answered because the methods were not available.
Neuropathology in the twenty first century must aim to integrate morphologic and molecular features with
molecular genetics, to advance understanding of basic mechanisms, specific diagnosis, and effective therapy. Geneticists have given us a whole series of questions. What are the functions of the proteins containing the trinucleotide repeat-encoded sequences, and the cellular effects of overexpression or knockout? What are the in vivo morphologic consequences of progressive expan- sion in size of the repeat regions? In which cell popula- tions are the disease-associated proteins located? With what other proteins might they interact? In what subcel- lular compartments can they be found? Other papers in this symposium deal with molecular aspects of the CAG repeat disorders. This review of neuropathology empha- sizes anatomic pathology, with the ultimate aim of facil- itating insight into molecular pathophysiology. An essential reference for developments in neurogenetics is available on the World Wide Web (23 ).
X-linked spinobulbar muscular atrophy (neuronopa-
Spinal and bulbar muscular atrophy, or Kennedy's disease, is an X-linked bulbar and spinal motor neuron disorder. It was mapped to ch Xqll-q12 (56) , and linked to the androgen receptor gene. It was the first of the CAG-repeat disorders to be defined as s uch (109).
Both its pattern of inheritance and its clinicopatho-
thy)
- __ __ ._ _ _ ~- _ _ _ _ _- - - . _..
902 Robitaille et al: Review and Update of Molecular and Genetic Features

logic features distinguish i t from other motor neuron degerative diseases such as infantile spinal amyotrophy (Werdnig-Hoffman disease), juvenile hereditary spinal muscular atrophy (Wohlfart-Kugelbeg-Welander dis- ease), and amyotrophic lateral sclerosis (ALS). It has onset in the third to fifth decade, but a very late onset case from Japan has been reported (39). The disorder is slowly progressive, with a near-normal longevity (77, 101). Occasional cases manifest a more rapid presenta- tion (5). Cramps may precede the onset of weakness, which is usually proximal at first. Fasciculations are widespread, notably including facial muscles. Clinical onset correlates with CAG repeat size; there is dispute over whether this is true of clinical seventy (5, 40, 85, 138).
Because the expansion is located in the gene for the androgen receptor, it is also unique among the CAG repeat disorders in the volume of prior information available on the encoded protein. Gynecomastia (an early sign of the disease), elevated gonadotrophic hor- mones, and testicular atrophy are among the clinical fea- tures indicative of mild feminization (1 80).
The sensory system is not altogether spared. Sensory nerve action potentials in the lower extremities are diminished or absent, and there is vibratory sense loss, less often loss of pain and temperature modalities, in the lower extremities. Hence the term X-linked bulbospinal neuronopathy has been proposed as more appropriate than SBMA(77,228).
Pathologic findings include severe depletion of lower motor nuclei in spinal cord and brainstem (but not affecting the oculomotor nuclei 111, IV, and VI). Upper motor neurons and corticospinal tracts appear unaffect- ed (101, 138, 193). In the sensory system, there is a dis- tal axonopathy affecting both the peripheral and the cen- tral branches of dorsal root ganglion neurons of lum- bosacral segments. Thus the sural nerve shows a marked depletion of large myelinated fibers, and the tractus gra- cilis shows pallor at rostra1 much more than caudal lev- els; whereas the tractus cuneatus is little affected (118, 193, 228). Morphometry revealed atrophy of neuronal perikarya in the dorsal root ganglia (1 18).
The androgen receptor is expressed in lower motor neurons, both in normals and in SBMA subjects (147). However, no changes in expression are reported to account for the disease process. Mosaicism for length of the CAG repeats within the nervous system does not account for the pattern of neurodegeneration (2 12).
Spinocerebellar ataxia type 1 (SCA1) Classification of the hereditary ataxias has bewil-
Figure 1. Olivary nuclei in autosomal dominant spinocerebellar degenerations. A. x 200, KlOver-Banera stain in representative area of SCA l-linked subject. Neuronal loss and gliosis are quite marked in the end-stage. B. x 200, Kliiver-Barrera stain in representative area of SCA 3-linked subject. Neuronat loss and gliosis are less severe compared to SCAl .
dered neurologists for generations (76, 202). Historically, orie group had been designated olivoponto- cerebellar atrophy, OPCA (14), which could be sporadic or inherited. Fifteen years ago, Harding proposed a clas- sification whic:h included those OPCAs which were of adult onset and transmitted in autosomal dominant pat- tern of inheritance. The designations autosomal domi- nant cerebellar atrophy (ADCA) types I, II, I11 and IV were proposed. Type I referred to those with ophthal- moplegia, optic atrophy, dementia, or extrapyramidal signs in addihon to the cerebellar deficits. Type I1 referred to a group with cerebellar ataxia and pigmen- tary retinal degeneratation. Type I11 referred to a pure cerebellar syndrome of late onset (over 60 years). Type IV referred 1.0 a cerebellar ataxia associated with myoclonus and deafness (75). Despite this contribution, classification remained fraught with uncertainties, which impeded pathogenetic understanding.
Recent genetic advances represent an important step toward resolving this confusion (84, 122, 124, 217).
Robitaille et al: Review and Update of Molecular and Genetic Features 903

Within Harding's ADCA I group, SCAl. SCA2, and SCA3, and others have now been distinguished on genetic criteria. With the genetic markers to define subgroups, clinico- pathologic comparisons were more meaning- ful. For example, the olivary nuclei, cerebel- lar cortex, and dentate nuclei were affected in ADCA I; but with genetic markers to distin- guish SCA1, SCA2, and SCA3, it was possi- ble to distinguish histologic patterns of pref- erential damage (Figures 1-3).
SCA 1 corresponds to OPCA 1, or the pro- gressive and dominantly inherited ataxia as described by authors such as Menzel, Schut. Jackson, and others (23, 202). The disease develops in the second decade or later, as a progressive ataxia. This is followed by selec- tive cranial nerve deficits and oculomotor abnormalities. Amyotrophy of all limbs is also characteristic of later stages of the dis- ease. Extrapyramidal signs and retinitis pig- mentosa are not features of SCAl (54, 61).
The disease mapped to the short arm of chromosome 6 (94, 164,235). It was traced to a CAG repeat expansion in a previously unknown gene (9, 151). Age of onset and to some extent disease duration, is inversely pro- portional to CAG repeat amplitudes in 50- 60% of affected subjects (96, 163). The mutated gene codes a protein, ataxin 1, of still unknown physiological significance. There is little or no correlation between sites of expression of ataxin 1 and the sites in rhombencephalon and spinal cord, where most SCAl-vulnerable neurons are localized. Furthermore, mosaicism (regional differences in CAG repeat expansion size) does not account for the pattern of SCAl neuropathol- ogy. We found the CAG repeat expansion size to be essentially the same among 20 different brain regions in each of three subjects with SCAl, with one exception: the cerebellar cor- tex had a slightly smaller CAG repeat expan- sion size (123).
The wild protein and the mutated SCAl variant are both found as intranuclear in all brain regions. In the cerebellar cortex of SCAl subjects, however, its epitopes are also found in the cytoplasm of Purkinje cells (184). Western blot studies of lymphoblastoid cell lines of SCAl subjects revealed that the
. . . .
904 Robitaille et al: Review and Update of Molecular and Genetic Features

length of polyglutamine stretches included within atax- in 1 protein residues also was inversely proportional to age of onset, with pathological threshold estimated to span 37-40 glutamines (217).
The neuropathology of end-stage SCAl is character- istic. We have described in detail the neuropathologic features, and compared them to the findings in SCA?, and SCA3IMJD (171). Gross examination may reveal mild to moderate widening of sulci, chiefly frontotem- poral; mild neuronal cell loss in cerebral cortex, with gliosis, was seen in a few cases. Subcortical white mat- ter of the cerebral hemispheres was unremarkable. Atrophy of the pons and cerebellum, and loss of the bulge of the inferior olive, were obvious in all cases. The spinal cord also showed loss of the cervical and lumbar enlargements and atrophy of ventral roots. Basal ganglia appeared grossly normal, except for one case with mild discoloration of the internal globus pallidus. Sections of b rainstem and cerebellum revealed the sub- stantia nigra and locus coeruleus to be normally pig- mented, whereas the dentate nucleus and cerebellar cor- tex were grossly atrophic.
There is severe loss of Purkinje cells and dentate neu- rons (Figures 2A, 3A), with atrophy of the dentatofugal pathway, a feature SCAl shares with DRPLA. Unlike DFWLA, however, SCAl shows only infrequent and mild to moderate involvement of the globus pallidus. The inferior olive (Figure 1A) and nuclei basis pontis are both severely affected in SCA1. Hence the superior, middle, and inferior cerebellar peduncles (outflow path- ways of the severely affected nuclei) all undergo auo- phy. Purkinje cell loss showed a reproducible regional pattern, with maximal depletion in the verrnis, less severe changes in the lateral hemisphere, and only mild to moderate neuronal loss in the flocculo-nodular lobes.
There was a remarkably severe loss of neurons from the cholinergic system of the basal forebrain, including the diagnonal band of Broca. The striatum may show mild neuronal loss and gliosis; the substantia nigra is normal or shows at most only mild cell loss. Despite sparing of the substantia nigra on histologic evaluation, there was evidence that nigrostriatal pathways were affected. All cases had sub-threshold but significant decreases (range= 45-75%) of dopamine levels in cau- date nucleus and putamen, compared to normal age- matched controls.
Neuronal loss and gliosis of the third, tenth, and twelfth cranial nerves was identified. There was severe loss of spinal anterior horn motor neurons and of neu- rons from the Clarke's columns. Degenerative changes of the posterior columns preferentially involved the
Figure 2. Cerebellzr cortex in autosomal dominant spinocere- bellar ataxias. A. x 200, Klijver-Barrera stain in representative area of laterial cerebellar cortex from an SCA 1-linked subject. Loss of Purkinje cel's is quite extensive. Severity is emphasized by a continuous line of reactive proliferation of Bergmann's glia. 6. x 200, Kl9ver-Barrera stain in representative area of lateral cerebellar cortex ,in SCA 3-linked autosomal dominant ataxia. Depletion of Purkinje cells is much less extensive and marked.
tractus gracilis. Corticospinal tracts underwent distal degeneration. There is immunohistochemical evidence of gliosis in layer 5 of the motor cortex in some Japanese SCAl subjects, but in our cases the upper motor neuron system effect appeared to be a dying-back process. The pattern of lower motor neuron degenera- tion shared with ALS a sparing of Onufs nucleus, but differed in that the neurofilament-filled swellings of proximal motor x o n s seen in rapidly progressive ALS were not a feature of SCA1. The findings are in general accord with prekious reports of SCAl (61, 183, 196) and with a recent comparison of two cases of SCA 1 with two cases of SCA3MJD (44).
In our view, these changes represent a phenotype which is distinguishable from SCA2 and SCA3NJD. For example, the substantia nigra is severely affected in SCA2 and SCA3/MJD, but spared in SCAl . Conversely, the dentatofugal pathways are far more
- .-
Robitaille et al: Review and Update of Molecular and Genetic Features 905

Figure 3. Dentate nucleus in autosomal dominant cerebellar ataxias. A. x 200, KlGver-Barrera stain in representative area of dentate nucleus from an SCA I-linked subject. Loss of neurons is quite extensive. B. x 200, Klliver-Barrera stain in representa- tive area of dentate nucleus in SCA 3-linked autosornal dorni- nant ataxia. Neuronal depletion is mild, as well as reactive glio- sis.
severel y affected in SCAl than in SCA2; SCA3MJD has an intermediate level of involvement, but generally less severe than that in SCAl (Figure 3; see also 44). The mechanism of cell death in SCAl is unknown, but there is evidence to support a role for apoptosis. A recent study using the TUNEL method yielded evidence that some nigral neurons are vulnerable to apoptosis in SCA 1 brains, compared to controls ( 1 14).
The role of anterograde trans-synaptic degeneration and of retrograde degeneration in SCAl should also be considered. In other settings, the inferior olive appears to manifest histologic patterns which distinguish antero- grade trans-synaptic degeneration due to lesions in afferents from the dentato-rubro-olivary pathway, from retrograde degeneration due to lesions of the cerebellar cortex (104). On the other hand, trans-synaptic de, oener- ation of the dentate nucleus has never been observed following selective deafferentation of olivo-cerebellar tracts. Since such trans-synaptic effects can take a long
time to develop, it is plausible that the severe Purkinje cell damage, combined with the long dui-ution of disease in SCAI, is partly responsible for degeneration of the dentate nucleus. An intrinsic vulnerability of dentate neurons, however, probably plays an important, and per- haps the major, role.
Sporadic cases of OPCA are often seen in association with striatonigral degeneration or autonomic dysfunc- tion (Shy-Drager). This "hybrid" degeneration is referred to as multi-system atrophy (MSA). Argyrophilic neuronal and oligodendroglial cytoplasmic inclusions have been identified i n such cases, immunoreactive for ubiquitin (27, 151). We found no such inclusions in our cases of SCAl (OPCA 1). However, there is a recent report of a family with the SCAl mutation, in which autopsy of one member showed lesions typical of MSA, including glial inclu- sions immunoreactive for tau and ubiquitin (62).
Spinocerebellar ataxia type 2 (SCA2) SCA2 is another subset of Harding's (76) ADCA I
group which has been distinguished from other ADCA 1 subsets by linkage analysis (63, 113). I t corresponds to OPCA 2, or spinocerebellar atrophy, Cuban type (23). Patients usually present with cerebellar findings. Slow saccades and sensorimotor neuropathy are particularly common in SCA2 when compared to SCAl and SCA3 (18, 43, 53, 156, Martha Nance this symposium). As with SCAl and SCA3, Parkinsonian features have been all but nonexistent according to most reports. although we have seen mild dystonic posturing and Parkinsonian features in some members of an SCA2 kindred from Austria (Lopes-Cendres per30nal observations). Corticospinal tract signs are less common than in SCA 1 but may occur (43). Dementia is also occasional, not characteristic (43). The mean age of onset is in the sec- ond to fourth decade and the disease duration a little over ten years. Intergenerational anticipation is recog- nized in SCA2 (162).
Large SCA2 kindreds likely due to a founder effect, have been well documented in the Holguin province of Cuba (150). Families have also been recognized in Europe, North America, and Japan (17, 53, 56, 162, 176). The gene maps to chromosome 12q24 (133). After its identification as a CAG-repeat disorder candidate (217), the gene was cloned, and the CAG repeat with expansions in SCA2 patients confirmed. The gene was designated ataxin-2. The protein is cytoplasmic, with an apparent molecular weight of 150kD (92, 161, 176).
The SCA2 mutation may be associated with the most devastating effects on cerebellar afferents. When suh-
- .. . ~ -. ~. . .... . . . . . . .
906 Robitaille et al: Review and Update of Molecular and Genetic Features

Figure 4. DRPLA. The neuropathology of DRPLA is quite variable, but typically is most severe in the dentate nucleus of the cere- bellum (A,B) as in this case of a man who presented with ataxia at age 40, developed chorea, apathy, irritability, and halluci nations, and died at age 59. Low (A) and high (B) magnification of the dentate nucleus show typical neuronal loss and marked disruption of the dentate ribbon. The well-populated caudate nucleus (C) has mild astrocytosis ori GFAP stain (D). Many subthala mic neurons are present (E) among reactive astrocytes. The inferior olivary complex (F,G) has vawolated neurons (arrows) and bizarre reactive astrocytes ("olivary hypertrophy") seen best by GFAP (G). GFAP also reveals mild corona radiata astrocytosis ( H). A-C,E,F = H&E; D.G,H = GFAP; Bars: B,D,G = 25 mm, A,C,E,F = 50 mm, H = 100 mm.
. -~
Robitaille et al: Review and Update of Molecular and Genetic Features 907

jects with SCAl, SCA2, and SCA3 were compared by MRI for sizes of brainstem, middle cerebellar peduncle, and cerebellum, i t was SCA2 which emerged with the most severe reductions (18). Autopsy studies are in accord with the MRI findings. Weights of the brainstem and of the cerebellum are severely reduced. The nuclei basis pontis are devastated, with degeneration of trans- verse pontine fibers, middle and inferior cerebellar peduncles, and subcortical fibers of the cerebellum. The olives undergo severe neuronal loss and gliosis (Figure 1B). Cerebellar Purkinje cells are markedly depleted (Figure 2B), whereas the dentate is much less affected (Figure 3B; see also 43, 150).
The absence of Parkinsonism is remarkable, since the substantia nigra shows rather marked loss of neurons in most reported autopsies. The locus coeruleus remains well populated (43, 150). The cerebral hemispheres can undergo marked atrophy with prominent ventricu- lomegaly in the occasional demented subject (43) and weight of the cerebral hemispheres is somewhat reduced (150). Subtler changes may extend to the pallidurn and the dentatorubral system (43). Our findings in a proband from a large SCA2 French Canadian kindred (120), who died in the end-stage of the disease, are in accord with previous reports of the Holguin cases. There was marked nigral degeneration and relative sparing of the locus coeruleus, as well as absence of structural lesions in cerebral cortex and basal ganglia.
MRI has shown reduction in cervical spinal cord vol- ume in SCA2, as well as in SCAl and SCA3 (18). An axonopathy may affect both descending motor pathways and sensory fibres, but we have not found reports to clearly distinguish between "dying back" and a primary neuronopathy in these systems. The posterior columns show degenerative changes involving tractus gracilis more than tractus cuneatus. Spinocerebellar tracts are also affected, and neurons of the dorsal column of Clarke are reportedly atrophic and reduced in number. Atrophy and depletion of lower motor neurons of the spinal anterior horn and pallor of ventral as well as dor- sal roots are also reported (150). Sural nerve biopsies have shown moderate loss of large myelinated fibers (53).
Spinocerebellar ataxia type 3 (SCA3) and Machado- Joseph disease (MJD)
After loci for SCAl and SCA2 were established, var- ious groups made efforts to determine whether ADCA I families were linked to either locus. This effort yielded evidence for a third locus (63) which was soon con- firmed (199). Simultaneously, studies of Machado-
Joseph disease located the site of the mutation on chro- mosome 14q (210) and implicated a CAG repeat cxpan- sion in a gene at that site (100).
A series of studies then led to demonstration that the "third locus" (SCA3) for ADCA I disorders was in the same gene mutated in MJD at 14q24.3-q31 (182, 198). The size of the responsible CAG-repeat expansions have been shown to influence age of onset, seventy of certain clinical features, and age at death. Severity of some clinical features correlated better with diseasc duration than with CAG repeat expansion size (44). Although MJD was originally described in Portuguese families, it was documented in diverse ethnic groups, probably on the basis of multiple independent mutations at the same genetic site (69, 182, 207, 211).
MJD had been studied for almost 25 years (10, 28) when the allelic identity of SCA3 with MJD was dis- covered. SCA3MJD is perhaps the most heterogeneous and common of the autosomal dominant ataxias (96, 100, 165, 18 1, 203). Progressive cerebellar ataxia asso- ciated with pyramidal tract involvement and oculomotor abnormalities is characteristic; extrapyramidal and peripheral nerve signs may also occur. Onset is typical- ly between 30 and SO years of age, but the disease may begin before 20. In one report of two brothers firs' affected at 8 and 7 years, the authors suggested homozy- gosity for the MJD gene to account for the earlier onset and somewhat greater pathologic severity (29, 192). There is recent evidence that age at death has a stronger inverse correlation with CAG repeat amplitudes than age of onset and disease duration not only in SCA3 kin- dreds, but in SCAl and SCA2 kindreds as well (1 22 and personal observations). As with SCAI, mosaicism in the CNS does not seem to account for selective vulnerabili- ty of neuronal populations (123)
Neuropathologically, SCA3/MJD shows much less effect on the inferior olives (Figure 1C) and the Purkinje cells (Figure 2C) than seen in SCAl and SCA2 (44, 171, 21 1). There are significant degenerative changes in the substantia nigra, dentate nucleus (Figure 3C), nuclei basis pontis, lower motor neurons, and neurons of Clarke's column. The internal globus pallidus is more affected than the external globus pallidus (the inverse of the pattern seen in DRPLA), and the subthalamic nucle- us can be markedly af fected (44, 21 1).
Cranial nerve nuclei which may be affected include 111, IV, VT, VII, VII (vestibular portion), XII, the nucle- us ambiguus, and the dorsal nucleus of the vagus nerve (44, 172, 173, 231). In one of the cases thought to be homozygous, there was also involvement of the nuclei gracilis and cuneatus, the medial lemniscus. the inter-
908 Robitaille et al: Re, 'ew and Update of Molecular and Genetic Features

Figure 5. DRPLA. Moderate dentate nucleus neuronal loss (A) with severe degeneration of the dentate hilus (B) and marked depop- ulation of the globus pallidus (C,D) are within the spectrum of DRPIA as found in this woman who presented at age 20 with ataxi a followed by a seizure disorder, dementia, and mild chorea until her death at 31 years of age. Globus pallidus neuronal loss and astro- cytosis are less severe in the internal segment (C) than in the external segment (D). The caudate nucleus (E) is intac t although prominent astrocytes are present in the red nucleus (F). There is extensive neuroaxonal dystrophy in the nucleus gracilis (G) , one of the classic findings in the Haw River Syndrome phenotype of DRPIA. Arrows = asrocytes. A,E = H8E; 8-D,F,G = H8E-Luxol Fast Blue; Bars: F = 25 mm, C-E,G = 50 mm, A = 100 mm, B = 1 mm.
~ -~ ~- -. _- Robitaille et al: Review and Update of Molecular and Genetic Features 909

mediolateral columns of the cord, and the dorsal root ganglia (29). A recent clinical and pathologic study ind- cates that SCA3hlJD could be distinguished on clinical criteria from SCA2, but'not from SCAI; whereas the pathologic features of SCA3/MJD and SCAl were dis- tinct (44), in agreement with our studies (171).
Evidence of polyglutamine tract involvement was demonstrated by Western blots and immunocytochemi- cal methods, which revealed a major 68K band, and 2 minor 74K and 87K bands in lymphoblastoid cell extracts of SCA3 subjects. They are integrated within the mutated version of the protein, ataxin 3, encoded by the SCA3MJD gene. The protein has an intracytoplas- mic distribution in normal controls. It was immunocyto- chemically detected as dot-like structures within neu- ronal nuclei of basis pontis, which is severely degener- ated (155). In cultured cells transfected with the SCA3 mutation, apoptosis was triggered only when the mutant gene fragment was translated into polyglutamine residues (90).
SCA sites not yet shown to be associated with CAG repeat mutations (SCA4, SCA5, SCAB)
Three other loci, which are associated with inherited ataxias, but to date have not been shown to be CAG repeat expansion sites, are mentioned here for the sake of clarity regarding the SCA numbering system current- ly in use. Two (SCA4 and SCA5) are from families that fit ADCA I criteria. Intergenerational anticipation sug- gests a trinucleotide repeat expansion for both disorders (121, 166). SCA4 has been mapped to chromosome 16q22.1. Clinically it is a late-onset ataxia associated with a proximal axonal sensory neuropathy. SCAS maps to l l p l l - q l l (57, 135, 166). The neuropathological fea- tures remain to be defined. The recently reported SCA8 locus is associated with an infantile onset, recessively inherited ataxia (107, 145).
Spinocerebellar ataxia type 6 (SCA6) SCA6 has emerged as a separate autosomal dominant
ataxia as the result of using polymorphic CAG repeats to screen DNA from patients with late onset neurode- generative disease. Using this approach, Zhuchenko and colleagues (234) identified a CAG repeat in a gene which proved to encode the human (Y 1 A voltage-depen- dent calcium channel subunit. The gene was indepen- dently mapped to chromosome 1 9 ~ 1 3 (37) and the full- length sequence published (149). Zhuchenko and col- leagues further screened DNA from controls and from I33 patients with progressive cerebellar ataxia for CAG repeat polymorphisrns in this calcium channel gene, and
found eight unrelated patients with a CAG repeat expar.- sion. The a 1 A voltage-dependent calcium channel sub- unit is expressed in cerebellar Purkinje cells. The authors argue that the polyglutamine tract expansion in SCA6 interferes with normal function of this calcium channel.
Neuropathologic studies on two patients from one family with this mutation have revealed severe loss of hrkinje cells as the salient neuropathologic finding. Grossly there was some evidence of cerebellar atrophy and suggestive evidence of brainstem atrophy. Milder neuronal loss of cerebellar granule cells and dentate nucleus neurons, and neurons of the inferior olive, was also described; the nuclei basis pontis and other areas examined, including the spinal cord, showed either nor- mal findings or changes not obviously related to the dis- ease (204). Findings were similar in one French- Canadian kindred in whom the SCA6 mutation had been detected: neuropathology in a single proband revealed a predominantly cerebello-olivary degeneration without involvement of cerebral hemispheres, basal ganglia, basis pontis, dentate nucleus, or motor neurons (person- al observations).
Clinical findings in SCA6, however, include not only mild, slowly progressive cerebellar ataxia, dysarthria and nystagmus, but also vibratory and proprioceptive sensory loss and hypo- or areflexia. Hence involvement of peripheral and sensory pathways sh ould be sought in future neuropathologic studies. The disorder progresses over 20 to 30 years, leading to a wheelchair-bound state. CAG repeat expansion size seemed to correlate inverse- ly with age of onset, but the sample size was small (234).
The mutated gene in SCA6 is of extraordinary inter- est currently, being associated with a function from which a highly plausible pathogenetic mechanism can be conceived. Remarkably, a group who independently cloned the a 1 A voltage-dependent calcium channe I gene found that missense mutations which truncate the protein were associated with familial hemiplegic migraine and episodic ataxia type 2 (149 ). Episodic ataxia type 2 is a distinct cerebellar disorder but has some overlapping features with SCA6 (8, 234). Importantly, the patients with the episodic ataxia type 2 mutations did not have CAG repeat expansions in the same gene (149; see discussion in 234).
Spinocerebellar ataxia type 7 (SCA7) ADCA I1 is associated with retinal degeneration (68,
75). In several families which fit the ADCA II proto- type, linkage studies placed the responsible locus
-~ - _ _ - . -
91 0 Robitaille et al: Review and Update of Molecular and Genetic Features

(SCA7) at chromosome 3p14-21.1 (30, 68, 69, 119). Using a monoclonal antibody which detects polygluta- mine tract expansions, Trottier and colleagues found such expansions in probands of several large European kindreds with ADCA and HD. In ADCA 11, a 130 K glu- tarnine-rich protein was observed on Western blots of lymphoblastoid cell lines, conspicuously in the nuclear fraction, providing evidence for a CAG repeat expan- sion as the responsible mutation in SCA7 (217). To our knowledge, the neuropathological phenotype remains unascertained.
Dentatorubropallidoluysian atrophy (DRPLA) and the Haw River Sydrome (HRS)
DRPLA is an autosomal dominant degenerative dis- ease, mapped to chromosome 12~13.31 (209,219). The identified gene has now been shown to harbor a CAG repeat which is expanded in affected subjects (91, 105, 137). It encodes a protein (atrophin) carrying a polyglu- tarnine tract (130, 136, 179). HRS has clinical and pathologic similarities to DRPLA. Identified in an African-American family with an ancestor from Haw kve r , North Carolina (47), it was traced to a CAG- repeat expansion in the DWLA-associated gene (19) within 5 years of its original description. DWLA and H R S are currently considered variants of the same dis- order.
- The atrophin transcript is expressed in many tissues including brain. In DRPLA subjects, both expanded and normal alleles are transcribed with similar efficiency, and regional mosaicism is detectable in brain, with cerebellar transcripts having slightly smaller CAG repeat regions than transcripts from other brain regions (148). There is evidence for mitotic instability of CAG repeat size in nonneuronal cells of the CNS (208). Both the normal and the expanded versions of atrophin are also detectable in DRPLA brain, about 190 and 205 kDa. respectively. Atrophin has been immunocytochem- ically localized to somatic and somato-dendritic com- partments of cortical cerebral and cerebellar neurons, mainly within Purkinje cells as well as in dentate nucle- us neurons (232).
The clinical phenotype for DRPLA shows extreme heterogeneity both within and between involved kin- dreds (88, 89, 106). In Europe, familial cases with psy- chiatric disturbances and chorea have repeatedly been misdiagnosed as Huntington's disease (222). Adult onset cases often present with ataxia, chorea, and dementia, and childhood to early adult onset cases with progres- sive myoclonus epilepsy and dementia (see review by Martha Nance in this symposium).
Familial DRPI-A may have first been described in a Belgian man (2! 15) and sporadic cases also from Europe and North America (144, 190, 191). Most sporadic and familial reports have since come from Japan, however (66, 139), where DRPLA is much more prevalent than in European populations. Nonetheless, contemporary documentation of DRPLA in the West is increasing (12, 41, 146, 158, 160, 222, 223, 224). Genetic criteria now surpass clinical and pathologic features in diagnostic specificity. "Sporadic" cases of D W L A and undiag- nosed cases a.ith dentatofugal or pallidofugal atrophy should be tested for CAG repeat expansion in the atrophin gene. Cases of DRPLA combined with other neurodegenerative disease (7 1) should become more informative w th application of genetic methods.
In DRPLA, the dentate nuclei are affected, with neu- ronal loss and gliosis in the nucleus and axonal degen- eration in the hilum (Figures 4 and 5). This is variable from case to case, but usually severe. The cerebellar cor- tex is relative,y spared, but an o ccasional case shows marked invohement (206). The paper by Ross and col- leagues (this symposium) compares features of the cere- bellar pathology in DRPLA and juvenile onset Huntington's disease.
The superior cerebellar peduncle, which is the out- flow pathway of the dentate nucleus, is atrophic, as would be expected. The middle cerebellar peduncle is relatively unaffected, again as would be expected from the fact that it!; fibers originate largely in the nuclei basis pontis, which are generally well preserved. The olivary nuclei in the medulla are moderately to severely affect- ed (Figures 4F,G). The red nucleus undergoes variable cell loss and Sliosis (Figure 5F), and myelinated tracts of the brai nstlm tegmentum can be affected. In fact, the tectum and the tegmentum of the brainstem are often atrophic, with involvement including parts of the reticu-
The globu:; pallidus, particularly the outer segment, is characteristically ravaged by the disease (Figure SC,D); and the subthalarnic nucleus may also be involved, perhaps more conspicuously in non-Japanese cases (222, 223, 224; see Figure 4E). Substantia nigra involvement is usually subtle if present (222,223,224). The neostriatiim may be affected (206) and GABA and substance P deficits similar to those of HD have been reported in the globus pallidus externa, apparently reflecting changes in the striatopallidal projections, rather than loss of striatal neurons (99). But the neostn- atal pathology in DRPLA is mild and occasional (Figures 4C, 5E) compared to that of the globus pallidus (Figures 5C,I>). The thalamus may also be affected (12)
. lar formation (88).
Robitaille et al: Review and Update of Molecular and Genetic Features 91 1
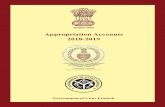
Figure 6. The Caudate Nucleus in Huntington's Disease. The hallmark of HD, degeneration of the striaturn can be classified into dif- ferent grades of severity based on the the Vonsattel (VS) system which uses both gross and microscopic features. Astrocyto sis and medium spiny neuronal loss in the caudate nucleus increase from VS grade 1 (A) which has minimal astrocytosis and an intact neu- ronal population, through VS grades 2 (B) and 3 (C) with increasing reactive astrocytosis and decreasing neuron numbers to VS grade 4 (D) where astrocytes are numerous and neuronal depopulation is severe. Arrows = astrocytes; arrowheads = neurons. A-D = H&E; Bars: A-D, left = 50 mrn, right = 25 mm.
~. . . . . . .. . . . . . .. .. .- . - -. ~ . .. . .. -. ~ ..
912 Robitaille et al: Review and Update of Molecular and Genetic Features

Robitarile et al: Review and Update of Molecular and Genetic Features 91 3

The distribution of lesions in DRPLA has some over- lap with those of Friedreich's ataxia, noticably so in the spinal cord (87, 88). In their review, Iizuka and Hirayama tabulate spinal cord lesions in DRPLA pre- sent in 19 of 23 subjects, including degeneration of pos- terior columns, spinocerebellar tracts, corticospinal tracts, and anterior horn cells (88).
HRS has a pathology broadly similar to that of DWLA. Myelin pallor may be more common or severe in HRS. Involvement of the globus pallidus features mineralization and "mulberry bodies" rather than severe loss of neurons; and neuroaxonal dystrophy of the nucleus gracilis, far in excess of what would be expect- ed for age, has been emphasized in HRS but not in DWLA. Distinction between HRS and D W L A on clin- icopathologic grounds has been debated (46, 188). White matter degeneration, neuroaxonal dystrophy in nucleus gracilis (Figure 5G), and mineralization of the globus pallidus, have also been reported in D W L A (Becher et al. in press). Hence distinctions between HRS and D W L A pathology may recede as the patho- logic heterogeneity of DRPLA is progressively revealed.
Huntington's disease (HD) Huntington's disease (HD) is an entity familiar to
neurologists and geneticists alike (58). The clinical fea- tures include not only the choreic and dementing form of adult onset, but more severe forms of earlier onset, often associated with rigidity (see Martha Nance, this symposium). The gene responsible is linked to a muta- tion on chromosome 4 ~ 1 6 . 3 , a locus which encodes a protein now designated huntingtin. The CAG repeat expansion size of the huntingtin gene correlates inverse- ly with age of onset of th e disease, and directly with the severity of clinical deficits.
Huntingtin harbors polyglutamine tracts and is very widely expressed (116, 117, 126, 185, 201), but with heterogeneity even in the normal neostriatum (51). Discovered as a result of genetic investigations in HD, huntingtin is of unknown function. Both mutated and normal versions of huntingtin are expressed in HD brains (157). The epitopes have been identified in perikarya, in punctate profiles presumed related to synaptic terminals, and in synaptosomes (7, 32, 36, 74, 2 16). Although polyclonal antibodies to huntingtin have immunolabeled components of the nucleus (including neuronal nuclei, 32), the evidence for a nuclear local- ization is in dispute (see Ross et al., this symposium). Huntingtin is ubiquitinated (98) and may interact with proteins of the ubiquitination pathway (see Ross et al,
this symposium). Huntingtin may be essential for normal cerebral
development and homeostasis. In transgenic mice whose huntingtin homologue had undergone targeted disruption, the embryonic homozygotes perished (140). These embryos had an increased rate of apoptosis, suugg esting that huntingtin operates as an apoptosis inhibito- ry factor (45, 233). Heterozygotes with targeted disrup- tion show significant neurologic and neuropathologic changes, though not a precise phenocopy of HD (140). Huntingtin apparently undergoes cleavage during apop- tosis, more avidly with increasing length of its polyglu- tamine tract (65, 141, Wellington et al. this symposium).
Apoptosis studies (159) are one part of the extensive efforts now being made to identify proteins with which huntingtin or polyglutamine tracts may interact, and to establish potential links between the normal or patho- logic effects of normal or mutated huntingtin, with cell processes previously suspected in HD pathogenesis (excitotoxicity, apoptosis, free radical damage, mito- chondrial and other metabolic effects). These topics are developed in the detailed updates provided by Ross and colleagues, and by WelIington and colleagues, in this symposium.
For the classic pathologic changes in the neostriatum, Vonsattel and colleagues (221) have published a useful grading system, ranging from 0 (no changes evident on gross examination and no microscopic abnormalities by routine histologic examination, despite typical clinical course and family history) to 4 (grossly concave head of caudate, with severe neuronal loss and gliosis) (Figure 6). This grading system has been applied in several stud- ies (134), including a recent study correlating seventy of pathology with size of the CAG repeat expansion (59).
A given HD patient may have tissue-specific differ- ences in size of the huntingtin CAG repeat, a phenome- non known as mosaicism. The repeat size is particularly unstable in sperm (213). and meiosis, not mitosis, is probably the event most associated with instability and expansion of the repeats (1 25, 226). Nonetheless, stria- tum and cerebral cortex reportedly harbor larger hunt- ingtin CAG repeat sizes than does cerebellar cortex (214). Despite small regional differences in length of CAG repeats from HD brains (33, 59), mosaicism does not seem to account for much of the selective vulnera- bility in HD or other CAG repeat diseases.
The pathology of Huntington's disease had been extensively studied before the genetic defect was dis- covered. Reviews of pathology and pathogenetic con- cepts are available ( I 1,72,733,75, 178). The remainder of this section gives an overview of some of the perti-
91 4 Robitaille et al: Review and Update of Molecular and Genetic Features

Figure 7. Huntington's Disease. The classic appearance of HD (A, left) compared to control (A, right) emphasizes the marked stri- atal degeneration, but atrophy of the neocortical grey and white matter are also present. Extensive astrocytosis and neuronal loss in the caudate and putarnen (6) contrasts with the lack, in most HD cases, of significant degeneration in the regions affected by other triplet repeat disorders. The neuronal populations of the globus pallidus (C) and subthalamic nucleus (D) are generally intact although varying degrees of astrocytosis are often present in the globus pallidus, as in this case, and thalamus. Arrow=astrocyte; arrowhead=neuron. B-D=H&E; Bars: B-D=25 mm
nent issues that have arisen in HD pathology, indepen- dently of huntingtin and its properties.
The neostriatum is preferentially involved (Figure 7), the earliest detectable change perhaps appearing in the striosomal compartment (79). However, as the matrix becomes involved, changes progress in a dorsal to ven- tral direction. The "small neurons" are selectively vul- nerable, and are currently classified as medium spiny neurons (15). They predominantly express enkephalin and GABA. Certain classes of striatal neurons are remarkably spared (24, 50, 52). The patterns of neuro- transmitter loss in HD brain tissue have been compared in rigid and choreic cases of the disease (200).
A pathophysiologic paradigm has been developed to account for the chorea on the basis of the selective neu- rodegeneration. The major neurotransmitters of the nor- mal caudate inzlude glutamate (corticostriatal afferents), dopamine (nigrostriatal afferents), acetylcholine (intrin- sic interneurons), and GABA (striatal projection neu- rons). Of these, it is the GABAergic population that is most devastated. The physiologic result in the choreic stage of the disease is a loss of striatal inhibitory input to the I ateral globus pallidus. Two important case stud- ies of early or presymptomatic HD yield supportive evi- dence. Enkephalin-containing neurons which project to the external segment of globus pallidus, and substance P
Robitaille et al: Review and Update of Molecular and Genetic Features 91 5

containing neurons which project to substantia nigra, are affected very early in the disease (1, 4), supporting the view that it is preferential loss of striatal projections to lateral pallidum that accounts for the chorea (2, 167, 168).
The pathophysiologic paradigm then proposes that the loss of striatal inhibitory input to the lateral globus pallidus results in an increased output from the lateral globus pallidus to the subthalamic nucleus. Since that pathway (pallidoluysian) is inhibitory, the subthalamic output is suppressed (reminiscent of focal damage to the subthalamic nucleus, which produces hemiballismus). This is summarized and illustrated in (3, 34,73).
Efforts to understand pathogenesis rely on an estab- lished profile of affected and "unaffected" cell popula- tions. Experience teaches that the list of affected popu- lations grows as investigators devote careful attention to various parts of the brain initially overlooked or disput- ed in pathologic descriptions. Involvement of cortex, notably layers V and VI is now well documented (80, 194). Indeed, atrophy of the brain in HD involves cor- tex, subcortical white matter, and thalamus, as well as neostriatum and lenticular nuclei (31, 112, 129; see also Figure 7C). Careful studies reveal cell loss in parts of hippocampus and entorhinal cortex (16,97). Certain cell populations relevant to eye movement abnormalities can be affected in HD (103, 115). The lateral tuberal nucle- us of the hypothalamus is severely affected (108).
Findings in the substantia nigra have been described as essentially normal (128) or showing significant neu- ronal loss and atrophy (152). There is massive loss of striatonigral projection terminals in the pars reticulata (64). Other nuclei which undergo detectable changes include the ventrolateral nucleus (38) and centromedi- an-parafascicular complex (8 1) of the thalamus; the sub- thalamic nucleus (1 12; but see Figure 7D); and the locus coeruleus (237). Evidence for involvement of cerebellar Purkinje cells is convincing (95). The nucleus basalis of Meynert, on the other hand, seems to be spared (6, 25, 205).
Ideally, involvement of a given anatomic site should be characterized as a primary or secondary (trans-synap- tic) effect. A primary effect implies molecular vulnera- bility of that neuronal type, whereas a secondary effect implies a nonspecific degeneration, less informative in working out strategies of therapy and prevention. Studies of the earliest stages of the disease are helpful in making the distinction, as are other approaches, but the distinction is often impossible. Studies of cellular changes in surviving neurons in HD are not extensive. However, altered dendritic morpology (70, 195) and
neuronal atrophy (152) can be detected in certain popu- lations.
In juvenile onset cases the clinical picture differs, and the pathology can be more severe, with extension to the cerebellum. Comparison of DRPLA and juvenile HD reveals some remarkable similarities, as well as differ- ences, as reviewed and illustrated in the manuscript by Ross and colleagues (this symposium).
Analysis of huntingtin CAG repeat polymorphism has become a valuable adjunct in selected autopsies (231). HD does have overlap with other neurodegenera- tive disorders, as well as residual problems of differen- tial diagnosis. Cases in which HD and familial amy- otrophic lateral sclerosis occur in the same subject ( 175) illustrate the heterogeneity on the "fringe" of these established genetic diseases. The neostriatum is involved in various neurodegenerative disorders, but the preferential pattern of involvement seen in HD is rare, Neuroacanthocytosis may approximate it (170), despite a very different pathogenetic point of departure.
For individual cases with pathologic resemblance to HD, where the genetic or nosologic classification is not clear, it will be worthwhile to rule out CAG-repeat expansions in the huntingtin gene. This should be applicable to the rare Huntington-like case with atypical pathologic features (for example, case 1 of Munoz- Garcia and Ludwin (1 32) as well as more common dis- orders such as the dementias lacking distinctive histo- logic features. Recent advances in genetics have helped resolve classification of senile chorea; reported cases did not have CAG repeat expansions in the HD range (186).
Conclusion: CAG repeats and the future of neu- ropathology
This review illustrates a small part of the rich inter- actions between molecular genetics and the neuro- sciences. Genetic advances in understanding the CAG repeat disorders drew upon the existing clinical and pathologic classifications, and refined them. Identification of genetic loci has led to more precise and meaningful comparisons of clinical and pathologic fea- tures in several of the diseases, notably the cerebellar degenerations. The molecular probes made available have enormous implications for clinical and preclinical diagnosis and genetic counseling.
For the neuropatholo,oist, the advances not only facil- itate diagnosis, but also open lines of pathogenetic investigation. It should be emphasized that not all the neuronal degeneration in these disorders is primary; some of the affected neuronal populations probably
-- - - ___ _ - ~. _. - - -
91 6 Robitaille et al: Review and Update of Molecular and Genetic Features

degenerate secondarily, by retrograde or anterograde trans-synaptic mechanisms identical to those which operate after focal lesions of their efferent or afferent projection systems.
That caveat aside, local effects of the mutated pro- teins must account for much of what we see; and the new genetic information has already given some pre- liminary answers to the questions we posed in our intro- duction. Although CAG repeat expansion size seems to influence age of onset and clinical and patholo,' UIC sever- ity in several of these diseases, regional differences in size of the CAG repeat expansions do not correlate well with the neuroanatomic sites (neuronal subsets) most vulnerable to the disease. Nor have regional differences in transcript levels accounted for the selective vulnera- bility in any obvious way. This would suggest that pathogenetic mechanisms depend on something down- stream, somehow involving the encoded protein with the expanded polyglutamine tract. The selective vulner- ability might then depend upon unique features of the affected neuronal populations, such as expression of other proteins with which the mutant protein interacts. Or receptors expressed on a given neuronal population might initiate an intracellular cascade in which the mutant protein constitutes (or strikes) a unique cellular Achilles heel. Hence the efforts, described in other papers of this symposium, to identify other proteins with which the mutated proteins interact; and to identify involvement of the mutant proteins in processes such as apoptosis, excitotoxic or other metabolic effects, which are hypothesized modes of neuronal death.
In general, the mechanisms of the CAG repeat disor- ders are believed to be due to a "gain of function," rather than to a simple loss or impairment of function of the protein. This is discussed elsewhere in this symposium. However, identifying the function of the normal protein seems important to sorting out the pathogenetic effect of the mutation. Of the mutated proteins, just two (the androgen receptor in SBMA and the a l A voltage- dependent calcium channel protein in SCA6) corre- spond to proteins, for which normal functions had been established before the association with mutation and neurologic disease was discovered. For the calcium channel protein, the next pathogenetic breakthrough seems a step away, since the receptor is expressed on Purkinje cells and the mutant protein is now associated with two cerebellar ataxias. Both the established and the newly discovered proteins (ataxins, atrophin, and hunt- instin) and their genes and transcripts permit approach- es to the questions stated in our introduction.
Recent advances in molecular genetics have obvious
implications for the training of neuropatholgists and the practice of neuropathology. Some basic familiarity with molecular genetics and the advances in neurogenetics is essential. The approach to autopsies and biopsies is affected; there i:; a much higher premium now on freez- ing, or otherwise processing, a fragment of fresh tissue for genetic analysis. Enriched by a steady stream of new insights, questions, and methods, modem neuropatholo- gy faces impressive opportunities and challenges.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Albin RL, Reiner A, Anderson KD, Dure LS 4th, Handelin B, Balfour 3, Whetsell WO Jr, Penney JB, Young AB (1 992) Preferential loss of striato-external palllidal projec- tion neurons in presyrnptomatic Huntington's disease. Ann Neurol31:425-30
Albin RL, Rainer A, Anderson KD, Penney JB, Young AB (1990) Striatal and nigral neuron subpopulations in rigid Huntington's disease: implications for the functional anatomy of #chorea and rigid-akinesia. Ann Neuro/27:357- 65 Albin RL. Young AB, Penney JB (1989) The functional anatomy of basal ganglia disorders. Trends Neurosci
Albin RL, Young AB, Penney JB, Handelin B, Balfour R, Anderson KD, Markel DS, Tourtellotte WW, Reiner A (1 990) Abnormalities of striatal projection neurons and N- methyl-D-aspartate receptors in presyrnptomatic Huntington'!; disease. N Eng J Med 322:1293 -8
Amato AA, Prior T, Barohn RJ, Snyder P, Papp A, Mendell JR (1 993) Kennedy's disease: a clinicopathologic correla- tion with riutations in the androgen receptor gene. Neurology 4:791-94 Arendt T, Big1 V, Arendt A, Tennstedt A (1 983) Loss of neu- rons in the nucleus basalis of Meynert in Alzheimer's dis- ease, paralysis agitans and Korsakoffs Disease. Acta Neuropathcl61:101-8 Aronin N. Chase K. Young C, Sapp E, Schwarz C, Matta N, Kornreich R, Landwehrmeyer B, Bird E, Beal MF, Vonsattel J-P, Smith T, Carraway R, Boyce FM, Young AB, Penney JB, DiFiglia M (1995) CAG expansion affects the expression of mutant Huntingtin in th e Huntingtc6i's dis- ease brain. Neuron 15:1193-201 Baloh RW, ' h e Q, Furman JM, Nelson SF (1997) Familial episodic ataxia: Clinical heterogeneity in four families linked to chromosome 19p. Ann Neuro/41:8-16 Banfi S, Seivadio A. Chung M, Kwiatkowski TJ Jr., McCall AE, Duvick, Shen Y, Roth EJ, Orr HT, Zoghbi HY (1994) ldentificatioi and characterization of the gene causing type 1 spinocerebellar ataxia. Nature Genet 7:513-20 Barbeau A. Roy M, Cunha L, de Vincente AN, Rosenberg RN, Nyhan WL, MacLeod PL, Chazot G, Langston LB, Dawson DM, Coutinho P (1984) The natural history of Machado-Joseph disease: an analysis of 138 personally examined cases. Can J Neurol Sci 11 :510-25
Beal MF (1994) Huntington's disease: energy and excito- toxicity. Neurobiol Aging 1 5:275-6
12:366-75
-__ __ - Robitaille et al: Review and Update of Molecular and Genetic Features 91 7

12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
Becher MW, Rubinsztein DC, Leggo J, Wagster MV, Stine OC, Ranen NG. Franz ML, Abbott MH, Sherr M, MacMillan JC. Barron L, Porteous M, Harper PS. Ross CA. Dentato-rubral and pallido-luysian atrophy (DRPLA): Clinical and neuropathological findings in g enetically con- firmed North American and European pedigrees. Mov Disord (in press) Ben Hamida C, Doerfiinger N, Belal S, Linder C, Reutenauer L, Dib C, Gyapay G, Vignal A, Le Paslier D, Cohen D, Pandolfo M, Mokini V, Novelli G, Hentati F, Ben Hamida M, Mandel J-L, Koenig M (1993) Localization of Friedreich ataxia phenotype with selective vitamin E defi- ciency to chromosome 8q by homozygocity mapping. Nature Genet 5:195-200
Berciano J (1 982) Olivopontocerebellar atrophy: a review of 11 7 cases. J Neurol Sci 53:253-72 Braak H, Braak E (1982) Neuronal types in the striatum of man. Cell Tissue Res 227:319-42 Braak H, Braak E (1992) Allocortical involvement in Huntington's disease. Neuropathol Appl Neurobiol
Brice A, Cancel G, Durr A, Didierjrean 0, lmbert G, Burk K, Saudou F, Yvert G, Abada M, Belal S, Benomar A, Klockgether T, Mandel J-L, Agid Y (1997) SCA 2 (Spinocerebellar ataxia 2): another unstable CAG expan- sion. Molecular and clinical analysis of 101 patients. Neurology 48:A210 Burk K, Abele M, Fetter M, Dichgans J, Skalej M, Laccone F, Didierjean 0, Brice A, Klockgether T (1 996) Autosomal dominant cerebellar ataxia type I . Clinical features and MRI in families with SCAl, SCA2 and SCA3. Brain
Burke JR, Wingfield MS, lewis KE, Roses AD, Lee JE, Hulette C, Pericak-Vance MA, Vance JM (1994) The Haw River syndrome: dentatorubropallidoluysian atrophy (DRPLA) in an African-American family. Nature Genet
Campuzano V, Montermini L, Molto MD, Pianese L, Cosse M, Cavalcanti F,Monros E. Rodius F, Duclos F, Monticelii A, Zara F, Cariizares J, Koutnikova H, Bidichandani SI, Gellera C, Brice A, Trouillas P, De Michele G, Filla A, De Frutos R, Palau F, Patel PI, Di Donato S, Mandel J-L, Cocozza S, Koenig M, Pandolfo M (1 996) Friedreich's ataxia: autosomal recessive disease caused by an intronic GAA repeat expansion. Science
Carvajal JJ, Pook MA, dos Santos M, Doudney K. Hillerman R, Minogue S. Williamson R, Hsuan JJ. Chamberlain S (1996) The Friedreich's ataxia gene encodes a novel phosphatidylinositol-4-phosphate 5- kinase. Nature Genet 14:157-62 Censori B, Provinciali L, Danni M, Chiaramoni L, Maricotti M, Foschi N, Del Pesce M, Salvolini U (1994) Brain involvement in myotonic dystrophy: MRI features and their relationship to clinical and cognitive conditions. Acta Neurol Scand 90:211-7
18:539-47
11911497-1 505
7:521-4
271: 1423-7
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
Center for Medical Gene!ics, Johns Hopkins University (Baltimore, MD) and National Center for Biotechnology Information, National Library of Medicine (Bethesda, MD). 1996. Online Mendelian lnheritance in Man, OMlM (TM). WWW URL http://www3.r.cbi.nlm.nih.govlomim/
CiccheKi F, Gould PV, Parent A (1996) Sparing of striatai neurons coexpressing calretinin and substance P (NKl ) receptor in Huntington's disease. Brain Res 730232-7 Clark AW, Parhad IM, Folstein SE, Whitehouse PJ, Hedreen JC, Price DL, Chase GA (1983) The nucleus basalis in Huntington's disease. Neurology 33:1262-7 CossCe M, Campuzano V, Koutnikova H, Fischbeck K, Mandel J-L, Koenig M, Bidichandani SI, Patel PI, Moite MD, Cariizares J. De Frutos R, Pianese L, Cavalcanti F, Monticelli A, Cocozza S, Montermini L, Massimo P (1 997) Frataxin fracas. Nature Genet 15:3 37-39 Costa C, Duyckaerts C (1993) Oligodendroglial and neu- ronal inclusions in multiple system atrophy. Curr Opin Neurol6:665-71 Coutinho P, Andrade C (1978) Autosomal dominant sys- tem degeneration in Portuguese families of the Azores Islands: a new genetic disorder involving cerebellar, pyra- midal, extrapyramydal and spinal cord motor functions. Neurology 28:703-9 Coutinho P, Guimariies A, Scaravilli F (1 982) The pathol- ogy of Machado-Joseph Disease. Acta Neuropathol
David G, Giunti P, Abbas N, Coullin P, Stevanin G, Horta W, Gemmill R, Weissenbach J . Wood N, Cunha S, Drabkin H, Harding AE, Agid Y, Brice A (1996) The gene for autosomal dominant cerebellar ataxia type II is locat- ed in a 5-cM region in 3p12-pl3: genetic and physical mapping of the SCA7 locus. Am J Hum Genet 59:1328- 36 de la Monte SM, Vonsattel JP, Richardson EP Jr (1988) Morphometric demonstration of atrophic changes in the cerebral cortex, white matter, and neostriaturn in Huntington's disease. J Neuropathol Exp Neurol47:516- 25 De Rooij KE, Dorsman JC, Smoor MA, Den Dunnen JT, Van Ommen GJ (1996) Subcelular focalization of the Huntington's disease gene product in cell lines by immunofluorescence and biochemical subcellular frac- tionation. Hum Mol Genet 5:1093-9 De Rooij KE, De Koning Gans PA, Roos RA, Van Ornmen GJ, Den Dunnen JT (1995) Somatic expansion of the (CAG)n repeat in Huntington disease brains. Hum Genet
DeLong MR (1990) Primate models of movement disor- ders of basal ganglia origin. Trens Neurosci 13:261-5 Dhooge R, Nagels G, Franck F, Bakker CE, Reyniers E, Storm K, Kooy RF, Oostra BA, Willems PJ, Dedeyn PP (1 997)MiidIy impaired water maze performance in male FMRl knockout mice. Neuroscience 76:367-76
DiFiglia M. Sapp E, Chase K. Schwarz C, Meloni A, Young C, Martin E, Vonsattel J-P, Carraway R. Reeves SA, Boyce FM, Aronin N (1995) Huntingtin is a cytoplas- mic protein associated with vesicles in human and rai brain neurons. Neuron 14:1075-81
5 m a - 5 ~
95~270-4
___ -. . . . . . .. _. -. _- - ._ . . - .. -. -. . . . . . -. .-
91 8 Robitaille et al: Review and Update of Molecular and Genetic Features

37. Diriong S, Lory P, Williams ME, Ellis SB, Harpold MM. Taviaux S (1995) Chromosomal localization of the human genes for alpha l A , alpha 16, and alpha 1E voltage- dependent CaP channel subunits. Genomics 3605-9
38. Dom R, Malfroid M, Baro F (1976) Neuropathology of Huntington's chorea. Studies of the ventrobasal complex of the thalamus. Neurology 26:64-8
39. Doyu M, Sobue G, Mitsuma T, Uchida M, lwase T, Takahashi A (1993) Very late onset X-linked recessive bulbospinal neuronopathy: mild clinical features and a mild increase in the size of tandem CAG repeat in andro- gen receptor gene. J Neurol Neurosurg Psychiatr56:832- 3
40. Doyu M, Sobue G, Mukai E, Kachi T, Yasuda T, Mitsuma T, Takahashi A (1992) Severity of X-linked recessive bul- bospinal neuronopathy correlates with size of the tandem CAG peat in androgen receptor gene. Ann Neurol
41. Dubourg 0, Dlirr A, Chneiweiss H, Stevanin G, Cancel G, Penet C, Agid Y, Brice A (1995) [Does the ataxo-choreic form of DRPLA exist in Europe? Search of mutation in 120 families]. [French] Revue Neurologique 151 :657-60
42. Durr A, Cossee M, Agid Y, Campuzano V, Mignard C, Penet C, Mandel J-L. Brice A, Koenig M (1996) Clinical and genetic abnormalities in patients with Friedreich's ataxia. N Eng J Med 3351 169-75
43. DArr A, Smadja 0, Cancel G, Lezin A, Stevanin G, Mikol J, Bellance R, Buisson G-G, Chneiweiss H, Dellanave J, Agid Y, Brice A, Vemant J-C (1995) Autosomal dominant cerebellar ataxia type I in Martinique (French West Indies). Clinical and neuropathological analysis of 53 patients from three unrelated SCA2 families. Brain
44. DArr A, Stevanin G, Cancel G, Duyckaerts C, Abbas N, Didierjean 0, Chneiweiss H, Benomar A. Lyon-Caen 0, Julien J, Serdaru M, Penet C, Agid Y, Brice A (1996) Spinocerebellar ataxia 3 and Machado-Joseph.disease: clinical, molecular, and neuropathological features. Ann Neurol30:490-9
45. Duyao MP, Auerbach AB, Ryan A, Persichetti F, Barnes GT, McNeil SM, Ge P, Vonsattel J-P, Gusella JF, Joyner AL, MacDonald ME (1995) Inactivation of the mouse Huntington's disease gene homolog Hdh. Science
46. Farmer TW, Wingfield MS, Jacobson PL, Katchinoff BL, Lynch SA, Curnes JT (1991) Neuroimaging of a new familial disorder. Ataxia, chorea, seizures, and dementia. J Neuroimaging 1 : 123-8
47. Farmer lW, Wingfield MS, Lynch SA, Vogel FS, Hulette C, Katchinoff B, Jacobson PL (1989) Ataxia, chorea, seizures and dementia. Pathologic features of a newly defined familial disorder. Arch Neurol46:774-9
48. Feng Y, Gutekunst CA. Eberhart DE, Yi H, Warren ST, Hersch SM (1997) Fragile X mental retardation protein- nucleocytoplasmic shuttling and association with somato- dendritic ribosomes. J Neurosci 17:1539-47
49. Feng Y, Zhang F, Lokey LK, Chastain JL. Lakkis L. Eberhart D, Warren ST (1995) Translational suppression by trinucleotide repeat expansion at FMRl . Science
32:707-10
11 8: 1 573-81
2691407-10
268:731-4
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
Ferrante RJ. Beal MF, Kowall NW, Richardson EP Jr, Martin JB (1 987) Sparing of acetylcholinesterase-contain- ing neurons in Huntington's disease. Brain Res 41 1 :162- 6 Ferrante RJ, Gutekunst C-A, Persichetti F, Kowall NW, Gusella JF, Beal F, MacDonald ME, Hersch SM (1997) Heterogeneous expression or huntingtin immilnoreactivi- ty in the normal human neostriatum. Neurology 48:A202
Ferrante RJ, Kowall NW, Beal MF, Martin JB, Bird ED, Richardson EP Jr (1 987) Morphologic and histochemical characteristcs of a spared subset of striatal neurons in Huntington':; disease. J Neuropathol Exp Neurol46:12-27 Filla A, De Michele G, Banfi S, Santoro L, Perretti A, Cavalcanti F, Pianese L, Castaldo I, Barbiere F, Campanella G, Cocozza S (1995) Has spinocerebellar ataxia type 2 a distinct phenotype? Neurology 45793-6 Filla A, De Michele G, Campanella G, Perretti A, Santoro L, Serlenga L, Ragno M, Calabrese 0, Castaldo I, De Joanna G, ICocozza S (1 996) Autosomal dominant cere- bellar ataxia type I. Clinical and molecular study in 36 Italian families including a compa rison between SCAl and SCA2 phenotypes. J Neuro Sci 142:140-7 Filla A, De Michele G, Cavalcanti F, Pianese L, Monticelli A, Campanella G, Cocozza S (1996) The relationship between trinucleotide (GAA) repeat length and clinical features in Friedreich ataxia. Am J Hum Genet 59:554-60 Fischbeck <H, lonasescu V, Ritter AW, lonasescu R, Davies K, Ball S, Bosch P, Burns T. Hausmanowa- Petrusewici: I, Borkowska J, Ringel SP. Stern LZ (1986) Localization of the gene for X-linked spinal muscular atro- phy. Neurolggy 36:1595-8 Flanigan K, Gardiner K, Alderson K, Galster B, Otterud B, Leppert MF, Kaplan C, Ptacek LJ (1996) Autosomal dom- inant spinocerebellar ataxia with sensory axonal neuropa- thy (SCA4): clinical description and genetic localization to chromosome 16q22.1. Am J Hum Genet 59:392-9 Folstein SE Leigh JR, Parhad IM, Folstein MF (1986) The diagnosis 0': Huntington's disease. Neurology 36:1279-83 Furtado S. Suchowersky 0, Rewcastle B, Graham L, Klimek ML, Garber A (1996) Relationship between trinu- cleotide repeats and neuropathological changes in Huntington's disease. Ann Neurol39:132-6 Gaspar C, Lopes-Cendes I, DeStefano AL, Maciel P, Silveira I , ClJutinho P, MacLeod P, Sequeiros J, Farrer LA, Rouleau G.4 (1 996) Linkage disequilibrium analysis in Machado-Joseph disease patients of different ethnic ori- gin. Hum Genet 98:620-4 Genis D, Miltilla T, Volpini V, Rosell J, Djvalos A, Ferrer I, Molins A, Estivill X (1 995) Clinical, neuropathologic, and genetic studies of a large spinocerebellar ataxia type 1 (SCAl ) kindred: (CAG), expansion and early premonitory signs and symptom s. Neurology 45:24-30 Gilman S, Sima AAF, Junck L, Kluin KJ, Koeppe RA, Lohman ME, Little R (1996) Spinocerebellar ataxia type 1 with multiplc2 system degeneration and glial cytoplasmic inclusions. Ann Neurol39: 241-255
Robitaille et al: Review and Update of Molecular and Genetic Features 919

63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
Gispert S, Twells R. Orozco G, Brice A, Weber J, Heredero L, Scheufler K. Riley B, Allotey R, Nothers C, Hillermann R, Lunkes A, Khati C, Stevanin G, Hernandez A, Magarifio C, Klockgether T, Durr A, Chneiweiss H, Enczmann J, Farrall M, Beckrnann J, Mu1 Ian M, Wernet P, Agid Y, Freund H-J, Williamson R, Auburger G, Chamberlain S (1993) Chromosomal assignment of the second locus for autosomal dominant cerebellar ataxia (SCA 2) to chromosome 12q23-24.1. Nature Genet
Glass M, Faull RL, Dragunow M (1993) Loss of cannabi- noid receptors in the substantia nigra in Huntington's dis- ease. Neuroscience 56523-7 Goldberg YP, Nicholson DW, Rasper DM, Kalchman MA, Koide HB, Graham RK, Bromm M. Kazemi-Esfarjani P, Thornberry NA, Vaillancourt JP, Hayden MR (1996) Cleavage of huntingtin by apopain. a proapoptotic cys- teine protease, is modulated by the polyglutamine tract. Nature Genet 13:442-9 Goto I, Tobimatsu S, Ohta M, Hosokawa S, Shibasaki H, Kuroiwa Y (1 982) Dentatorubro-pallidoluysian degenera- tion: Clinical, neuro-ophthalmologic, biochemical, and pathologic studies on autosomal dominant dorm. Neurology 32: 1395-9 Gourdon G, Radvanyi F, Lia A-S, Duros C, Blanche M, Abitol M, Junien C, Hofmann-Radvanyi H (1997) Moderate intergenerational and somatic instability of a 55-CTG repeat in transgenic mice. Nat Genet 15:190-2 Gouw LG, Digre KB, Harris CP, Haines JH, Ptacek LJ (1 994) Autosomal dominant cerebellar ataxia with retinal degeneration: clinical, neuropathologic, and genetic analysis of a large kindred. Neurology 44:1441-7 Gouw LG, Kaplan CD, Haines JH, Digre KB, Rutledge SL, Matilla A, Leppert M, Zoghbi HY, Ptacek LJ (1995) Retinal degeneration characterizes a spinocerebellar ataxia map- ping to chromosome 3p. Nature Genet 10:89-93 Graveland GA, Williams RS, Difiglia M (1985) Evidence for degenerative and regenerative changes in neostriatal spiny neurons in Huntington's disease. Science 227:770- 3
Gray F, Eizenbaum JB, Gherardi R, Degos JD, Poirier J (1 985) Luyso-pallido-nigral atrophy and amyotrophic lat- eral sclerosis. Acta Neuropath 66:78-82. Greenamyre JT (1994) Recent developments in the cause and treatment of movement disorders. Curr Opin Neurol7:323-4 Greenamyre JT, Shoulson I (1994) Huntington's Disease. In: Neurodegenerative Diseases. Calne DB (ed) W.B.Saunders Company, pp 685-704 Gutekunst C-A, Levey Al, Heilman CJ, Whaley WL, Yi H, Nash NR, Rees HD, Madden JJ. Hersch SM (1995) Identification and localization of huntingtin in brain and human lymphoblastoid cell lines with anti-fusion protein antibodies. f r oc Natl Acad Sci USA 92:8710-14 Harding AE (1982) The clinical features and classification of the late onset autosomal dominant cerebellar ataxias: A study of 11 families, including descendants of the Drew family of Walworth'. Brain 105:l-28
4:295-99
76.
77.
78.
79.
80.
81.
82.
83.
84.
.85.
86.
87.
88.
89.
Harding AE (1983) Classification of t he hereditary ataxias and paraplegias. Lancet 1:1151-5 Harding AE. Thomas PK, Baraitser M, Bradbury PG, Morgan-Hughes JA, Ponsford JR (1 982) X-linked reces- sive bulbospinal neuronopathy: a report of ten cases. J Neurol Neurosurg Psychiatr 45: 101 2-1 01 9 Hedreen JC, Ross CA. Huntington's Disease. In: The Primary Degenerative Dementias Other Than Alzheimer's Disease, Clark AW, Dickson DW (eds) Carolina Academic Press, Durham (in press) Hedreen JC, Folstein SE (1995) Early loss of neostriatal striosome neurons in Huntington's disease. J Neuropathol Exp Neurol54:105-20 Hedreen JC, Peyser CE, Folstein SE. Ross CA (1991) Neuronal loss in layers V and VI of cerebral cortex in Huntington's disease. Neurosci Lett 133:257-61 Heinsen H, Rub U, Gangnus D, Jungkunz G. Bauer bl, Ulmar G, Bethke B, Schuler M, Bicker F, Eisenrnenger W, Gdtz M, Strik M (1 996) Nerve cell loss in the thalamic cen- tromedian-parafascicular complex in patients with Huntington's disease. Acfa Neuropatho/91:161-8 Hofferbert S, Schanen NC, Chehab F, Francke U (1997) Trinucleotide repeats in the human genome: size distribu- tions for all possible triplets and detection of expanded disease alleles in a group of Huntington disease individu- als by the Repeat Expansion Detection method. Hum Mot Genet 677-83 Housman D (1995) Gain of glutamines, gain of function? Nature Genet 10:3-4 Hurko 0 (1997) Recent advances in heritable ataxias. Ann Neurol 41 14-6 lgarashi S, Tanno Y, Onodera 0. Yamazaki M, Sata S, lshikawa A, Miyatani N, Nagashirna M, lshikawa Y, Sahashi K, Ibi T, Miyatake T, Tsuji S (1 992) Strong corre- lation between the number of CAG repeats in androgen receptor genes and the clinical onset o f features of spinal and bulbar muscular atrophy. Neurology 42:2300-2302 lhara T, Sasaki H, Wakisara A, Takada A, Yoshiki T, Matsuura T, Hamada T, Susuki Y, Tashiro K (1994) Genetic heterogeneity of dominantly inherited olivoponto- cerebellar atrophy (OPCA) in the Japanese: linkage study of two pedigrees and evidence for th e disease locus on chromosome 12q(SCA2). Jpn J Hum Genet 39:305-13 lizuka R, Hirayama K (1 986) Dentato-rubro-pallido- luysian atrophy. In: Handbook of Clinical Neurology; Extrapryamidal Disorders. Vinken PJ, Bruyn GW, Klawans HL (eds). Elsevier Science Publishers, Vol 5, pp 437-43 lizuka R, Hirayama K (1991) Dentato-rubro-pallido- luysian atrophy. In: Handbook of Clinical Neurology, Hereditary Neuropathies and Spinocerebellar Atrophies. de Jong, JMBV (ed). Elsevier Science Publishers, Voi 16,
lizuka R, Hirayama K, Maehara K (1984) Dentatorukro- pallidoluysian atrophy: a clinico-pathological study. J Neurol Neurosurg fsychiatr 47: 1288-98
pp 607-1 8
_ _ -~ _ _ - - _ _ - _ - - __ 920 Robitaille et al: Review and Update of Molecular and Genetic Features

90. lkeda H, Yamaguchi M, Sugai S, Aze Y, Narumiya S, Kakizuka A (1996) Expanded polyglutamine in the Machado-Joseph disease protein induces cell death in vitro and in vivo. Nature Genet 13:196-202
91. lkeuchi T, Koide R, Tanaka H, Onodera 0, lgarashi S, Takahashi H. Kondo R, lshikawa A, Tomoda A, Miike T, Sato K, lhara Y, Hayabara T, Isa F, Tanabe H, Tokiguchi S, Hayashi M, Shimizu N. lkuta F, Naito H, Tsuji S (1995) Dentatorubral-Pallidoluysian A trophy: Clinical features are closely related to unstable expansions of trinucleotide (CAG) repeat. Ann Neurol37:769-75
92. lmbert G, Saudou F, Yvert G, Devys D, Trottier Y, Gamier J-M, Weber C, Mandel J-L, Cancel G, Abbas N, DArr A, Didierjean 0, Stevanin G, Agid Y, Brice A (1996) Cloning of the gene for spinocerebellar ataxia 2 reveals a locus with high sensitivity to expanded CAG/glutamine repeats. Nature Genet 14:285-91
93. lshii S, Nishio T, Sunohora N, Yoshihara T, Takemure K, Hikiji K, Tsujino S, Sakuragawa N (1996) Small increase in triplet repeat length of cerebellum with myotonic dys- trophy. Hum Genet 98:138-40
94. Jackson JF, Currier RD, Teraski PI, Morton NE (1977) Spinocerebellar ataxia and HLA linkage: risk prediction by HLAtyping. N Eng J Med296:1138-41
95. Jeste DV, Barban L, Parisi J (1984) Reduced Purkinje cell density in Huntington's disease. Exp Neurol85:78-86
96. Jodice C, Malaspina P, Persichetti F, Novoletto A, Spadaro M, Giunti P, Morocutti C, Terrenato L, Harding AE, Frontali M (1994) Effect of trinucleotide repeat length and parental sex on phenotypic variationn in spinocere- bellar ataxia 1. Am J Hum Genet 54:959-65
97. Junck L, Gilman S, Gebarski S, Koeppe RA, Kluin KJ, Markel DS (1994) Structural and functional brain imaging in Friedreich's ataxia. Arch Neuro/51:349-55
98. Kalchman MA, Graham RK, Xia G, Koide HB, Hodgson JG, Graham KC, Goldberg YP, Gietz RD, Pickarl CM, Hayden MR (1996) Huntingtin is ubiquitinated and inter- acts with a specific ubiquitin-conjugating enzyme. J Biol Chem 271:19385-94
99. Kanazawa I, Sasaki 11, Muramoto 0, Matsushita M, Mizutani T, lwanbuchi K,'lkeda T, Takahata N (1985) Studies on neurotransmitter markers and striatal neuronal cell density in Huntington's disease and dentatorubropal- lidoluysian atrophy. J Neurol Sci 7 0:151-65
100. Kawaguchi Y, Okamoto T, Taniwaki M, Aizawa M, lnoue M, Katayama S, Kawakami H, Nakamura S, Nishimura M, Akiguchi I , Kimura J, Narumiya S, KakizukaA (1994) CAG expansions in a novel gene for Machado-Joseph disease at chromosome 14q32.1. Nature Genet 8:221-8
101. Kennedy WR, Alter M, Sung JH (1 968) Progressive prox- imal spinal and bulbar muscular atrophy of late onset: a sex-linked recessive trait. Neurology 18:671-80
102.Kluger G, Bohm I, Laub MC, Waldenmeier C (1996) Epilepsy and fragile X mutations. f e d Neurol 15358-60
103. Koeppen AH (1989) The nucleus pontis centralis caudalis in Huntington's disease. J Neurol Sci 91 :129-41
104.Koeppen AH, Barron KD (1984) The neuropathology of olivopontocerebellar atrophy. In:The Olivopontocerabellar Atrophies, Duvoisn RC, Plaitakis A (eds) Raven Press, New York, ~pp. 13-38
105.Koice R, llteuchi T, Onodera 0, Tanaka H, lgarashi S, Endo K. Takahashi H. Kondo R, lshikawea A, Hayashi T, Saito M, h n o d a A. Miike T, Naito H, lkuta F, Tsuji S (1 994) Unstable expansion of CAG repeat in hereditary dentatorubro-pallidoluysian atrophy (DRPLA). Nature Genet 6:9-'13
106.Kornure 0, Sano A, Nishino N, Yamauchi N, Ueno S, Kondoh K, Sano N, Takahashi M. Murayama N, Kodo I, Nagafuchi :S, Yamada M, Kanazawa I (1995) DNA analy- sis in heraditary dentatorubral-pallidoluysian atrophy: Correlation between CAG repeat length and phenotypic variation and the molecular basis of anticipation. Neurology .45: 143-49
107. Koskinen 7; Santavuori P. Saino K, Lappi M, Kallio AK, Rihko H (1994) Infantile onset spinocerebellar ataxia with sensory neuropathy: a new inherited disease. J Neurol Sci121:50.6
108.Kremer HF', Roos RA, Dingjan G. Marani E, Bots GT (1 990) Atrcphy of the hypothalamic lateral tuberal nucle- us in Huntington's disease. J Neuropafhol Exp Neurol
109.La Spada AR, Wilson EM, Lubahn DB, Harding AE, Fischbeck <H (1991) Androgen receptor gene mutations in X-linked spinal and bulbar muscular atrophy. Nature
110.La Spada AR, Paulson HL, Fischbeck KH (1994) Trinucleoticle repeat expansion in neurological disease. Ann Neuro'36:814-22
111. Lamarche JB. Lemieux B, Lieu HB (1984) The neu- ropathology of 7ypical"Friedreich's ataxia in Quebec. Can J Neurol SI: 11 592-600
112.Lange H, Thomer G, Hopf A, Schroder KF (1976) Morphome1:ric studies of the neuropathological changes in choreatic: diseases. J Neurol Sci 28:401-25
113. Lazzarini A, Zimmerman TR Jr, Johnson WG, Duvoisin RC (1992) A 17th-century founder gives rise to a large North American pedigree of autosomal dominant spin- ocerebellar ataxia not linked to the SCAl locus on chro- mosome 6. Neurology 42:2118-24
114. Ledoux S, Desjardins P, Robitaille Y, Kish SJ (1997) Evidence for in situ DNA fragmentation in spinocerebellar ataxia type 1 substantia nigra. Neurology48:A176
115. Leigh RJ, Parhad IM, Clark AW. Buettner-Ennever JA, Folstein SII (1 985) Brainstem findings in Huntington's disease. Fossible mechanisms for slow vertical sac- cades. J Nsurol Sci 71:247-56
116. Li XJ, Li S-H, Sharp AH, Nucifora FC Jr, Schilling G, Lanahan A. Worley P, Snyder SH, Ross CA (1 995) A hunt- ingtin-asso-iated protein enriched in brain with implica- tions for pathology. Nature 378:398-402
117. Li S-H, Sciilling G, Young WS 111, Li X-J, Margolis RL, Stine OC, Wagster MV, Abbott MH, Franz ML, Ranen NG, Folstein SEi, Hedreen JC, Boss CA (1993) Huntington's disease gene (IT-15) is widely expressed in human and rat tissues. Neuron 11 :985-93
491371-82
352177-9
- .
Robitaille et al: Review and Update of Molecular and Genetic Features 92 1

118. Li M, Soubue G, Doyu M, Mukai E. Hashizume Y, Mitsuma T (1995) Primary sensory neurons in x-linked recessive bulbospinal neuronopathy: Histopathology and androgen receptor gene expression. Muscle & Nerve
119. Lindblad K, Savontas ML, Stevanin G, Holrnberg M, Digre K, Zander C, Ehrsson H, David G, et al( l996) An expand- ed CAG repeat sequence in spinocerebellar ataxia type 7. Genome Res 6:965-71
120. Lopes-Cendes I, Andermann E, Attig E, Cendes F, Bosch S, Wagner M, Gerstenbrand F, Anderrnann F, and Rouleau GA (1994) Confirmation of the SCA-2 locus as an alternative locus for dominantly inherited spinocere- bellar ataxia and refinement of the candi date region. Am J Hum Genet 54:774-81
121, Lopes-Cendes I, Andermann E, Rouleau GA (1994) Evidence for the existence of a fourth dominantly inherit- ed spinocerebellar ataxia locus. Genomics 21 270-4
122. Lopes-Cendes I, Destefano AL, Maciel P, Silveira I, Robitaille Y, Shannak K. Koeppen AH et al. The role of CAG trinucleotide repeats in the differential neuropathol- ogy of spinocerebellar ataxias (in press)
123. Lopes-Cendes I, Maciel P, Kish S. Gaspar C, Robitaille Y, Clark HB, Koeppen AH, Name M, Schut L, Silveira I, Coutinho P, Sequeiros J, Rouleau GA (1996) Somatic mosaicisrn in the central nervous system in spinocerebel- lar ataxia type 1 and Machado-Jos eph disease. Ann Neurol40: 199-206
124. Lopes-Cendes I, Silveira I , Maciel P, Gaspar C, Radvany J, Chitayat D, Babul R, Stewart J, Dolliver M, Robitaille Y, Rouleau GA, Sequeiros J (1996) Limits of clinical assess- ment in the accurate diagnosis of Machado-Joseph dis- ease. Arch Neuro/53:116 8-74
125.MacDonald ME, Barnes G, Srinidhi J, Duyao MP, Ambrose CM, Myers RH, Gray J, Conneally PM, Young A, Penney J, Shoulson I, Hollingsworth Z, Koroshetz W, Bird E, Vonsattel JP, Bonilla E, Moscowitz C, Penchaszadeh G, Brzustowicz L, Alvir J, Bickharn Cond e J, Cha J-H, Dure L, Gornez F, Ramos-Arroya M, Sanchez-Rarnos J, Snodgrass S R , de Young M, Wexler NS McFarlane H, Anderson MA, Jenkins B, Gusella JF (1993) Gametic but not somatic instability of CAG repeat length in Huntington's disease. J Med Genet 30:982 -6
126. MacDonald ME, Gusella JF (1996) Huntington's disease: translating a CAG repeat into a pathogenetic mechanism. Curr Opin Neurobiol6:638-43
127. Mahadevan MS, Amerniya C, Jansen G, Sabourin L, Baird S, Neville CE, Wormskarnp N, Segers B, Batzer M. Larnerdin J, de Jong P, Wieringa 8, Korneluk RG (1993) Structure and genornic sequence of the myotonic dystro- phy (DM kinase) gene. Hum Mol Genet 2:299 -304
128. Mann DM (1 989) Subcortical afferent projection systems in Huntington's chorea. Acta Neuropathol78:551-4
129. Mann DM, Oliver R, Snowden JS (1993) The topograph- ic distribution of brain atrophy in Huntington's disease and progressive supranuclear palsy. Acta Neuropathol
130. Margolis RL, Li S-H, Young WS et al (1996) DRPLA gene (atrophin-1) sequence and mRNA expression in human brain. Mol Brain Res 36:219-26
1 a301 -308
851553-9
131. Martorelli L, Martinez JM, Carey N, Johnson K, Baiget PvI (1 995) Comparison of CTG repeat length expansion and clinical progression of rnyotonic dystrophy over a five year period. J Med Genet 32593-6
132. Munoz-Garcia D, Ludwin SK (1986) Adult-onset neuron21 intranuclear hyaline inclusion disease. Neurology 36:785- 90
133. Myers RH. Leavitt J, Farrer LA, Jagadeesh J, McFar1ar.e H, Mastromauro CA, Mark RJ, Gusella JF (1989) Hornozygote for Huntington disease. Am J Hum Genet
134.Myers RH, Vonsattel JP, Stevens TJ. Cupples LA, Richardson EP, Martin JB, Bird ED (1988) Clinical and neuropathologic assessment of severity in Huntington's disease. Neurology 38:341-7
135. Nachmanoff DB, Segal RA, Dawson DM, Brown RB, De Girolarni U (1997) Hereditary ataxia with sensory neu- ronopathy: Biernond's ataxia. Neurology 48273-5
136.Nagafuchi S, Yanagisawa H, Ohsaki E, Shirayama T, Tadokoro K, lnoue T, Yamada M (1994) Structure and expression of the gene responsible for the triplet repeat disorder, dentatorubral and pallidoluysian atrophy (DRPLA). Nature Genet 8:177-82
137.Nagafuchi S. Yanagisawas H, Sato K, Shirayama T, Ohsaki E, Bundo M, Takeda T, Tadokoro K, Kondo I, Murayama N, Tanaka Y, Kikushima H, Umino K, Kurosawa H, Furukawa T, Nihei K, lnoue T, Sano A, Kornure 0, Takahashi M, Yoshizawa T, Kanazawa I, Yarnada M(1994) Dentatorubral and pallidoluysian atro- phy expansion of an unstable CAG trinucleotide on chro- mosome 12p. Nature Genet 6: 14-1 8
138. Nagashima T, Seko K, Hirose K, Mannen T, Yoshimura S, Arirna R, Nagashirna K, Morimatsu Y (1988) Familial bulbo-spinal muscular atrophy associated with testicular atrophy and sensory neuropathy (Kennedy-Alter-Sting syndrome): autopsy case report of two brothers. J Neurol Sci 87:141-152
139. Naito H, Oyanagi S (1982) Familial myoclonus epilepsy and chorcoathetosis: Hereditary dentatorubral-palli- doluysian atrophy. Neurology 2798-807
140. Nasir J, Floresco SB, O'Kusky JR, Diewert VM, Richman JM, Zeisler J, Borowski A, Marth JD, Phillips AG, Hayden MR (1995) Targeted disruption of the Huntington's dis- ease gene results in embryonic lethality and behavioral and morphological changes in heterozygotes. Cell
141. Nasir J, Goldberg YP. Hayden MR (1 996) Huntington dis- ease: new insights into the relationship between CAG expansion and disease. Hum Mol Genet 5 Spec No: 143 1 - 5
142. Nechiporuk A, Lopes-Cendes I, Nechiporuk T, Starkman S, Anderrnann E, Rouleau GA. Weissenbach JS, Kor? E, Pulst S-M, (1 996) Genetic mapping of the spinocerebellar ataxia type 2 gene on human chromosome 12. Neurology
143. Neri C, Cann HM, Dausset J (1 996) Triplet Repeats, neu- rodegenerative and neuropsychiatric diseases. Mechanisms and candidate genes. MS-Medicine Science
45:615-8
81 :811-23
46: 1 73 1 -5
1211361-8
_. .- - - .- - - --
Robitaille et al: Review and Update of Molecular and Genetic Features

144. Neumann MA (1959) Combined degeneration of globus pallidus and dentate nucleus and their projections. Neurology 9:430-8
145. Nikali K, lsosornppi J, Lonnqvist T, May J-I. Suomalainen A, Peltonen L (1997) Toward cloning of a novel ataxia gene: Refined assignment and physical map of the IOSCA locus (SCAB) on 1 Oq24. Genomics 39:185-91
146. Norremolle A, Nielsen JE, Sorensen SA, Hasholt L (1995) Elongated CAG repeats of the 837 gene in a Danish fam- ily with dentato-rubro-pallido-luysian atrophy. Hum Genet
147. Ogata A, Matsuura T, Tashiro K, Morikawa F, Demura T, Koyanagi T, Nagashima K (1994) Expression of androgen receptor in X-linked spinal and bulbar muscular atrophy and amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatr 58:1274-5
148.0nodera 0, Oyake M, Takano H, lkeuchi T, lgarashi S. Tsuji S (1995) Molecular cloning of a full-length cDNA for dentatorubral-pallidoluysian atrophy and regional expres- sion of the expanded alleles in the CNS. Am J Hum Genet
149.Ophoff RA, Terwindt GM, Vergouwe MN, van Eijk R, Oefner PJ, Hoffman SM, Larnerdin JE, Mohrenweiser HW, Bulman DE, Ferrari M, Haan J, Lindhouut D, van Ornmen GJ, Hofker MH, Ferrari MD, Frants RR (1996) Familial herniplegic migraine and episodic ataxia t ype-2 are caused by mutations in the Ca2+ channel gene CACNLl A4. Cell 87:543-52
150. Orozco G, Estrada R, Perry TL, Arana J, Fernandez R, Gonzales-Quevedo A, Galarraga J, Hansen S (1 989) Dominantly inherited olivopontocerebellar atrophy from eastern Cuba. J Neurol Sc 9337-50
151. Orr HT, Chung M-Y. Banfi S, Kwiatkowski TJ Jr, Servadio A, Beaudet AL, McCall AE, Duvick LA, Ranurn LPW, Zoghbi HY (1993) Expansion of an unstable trinucleotide CAG repeat in spinocerebellar ataxia type 1. Nature Genet 4:221-226
152.0yanagi K, Takeda S. Takahashi H, Ohama E, lkuta F (1 989) A quantitative investigation of the substantia nigra in Huntington's disease. Ann Neurol26:13-9
153. Palau F, DeMichele G, Vilchez JJ, Pandolfo M. Monros E. Cocoua S. Smeyers P, Lopez-Arlandis J, Campanella G, DiDonato S, Filla A (1995) Early-onset ataxia with car- diornyopathy and retained tendon reflexes maps to the Friedreich's ataxia locus on chromosome 9q. Ann Neurol
154. Papp MI, Lantos PL (1992) Accumulation of tubular struc- tures in oligodendroglial and neuronal cells as the basic alteration in multiple system atrophy. J Neurol Sci
155. Paulson HL, Subramony SS, Das J, Fratkin 0, McDaniel 0, Pittman RN (1 997) Aberrant nuclear localization of the Machado-Joseph disease gene product in disease brain. Neurology 48:S26.005
156. Perretti A, Santoro L, Lanzillo B, Filla A, De Michele G, Barbieri F, Martino G, Ragno M, Cocozza S, Caruso G (1996) Autosomal dominant cerebellar atazia type I: mul- timodal electrophysiological study and comparison between SCAl and SCA2 patients. J Neurol Sci 142:45- 53
95513-8
5711 050-60
37:359-62
107:172-82
157. Persichetti F, Ambrose CM, Ge P, McNeil SM, Srinidhi J, Anderson IWA, Jenkins B, Barnes GT, Duyao MP, Kanaley L et a1 (1 995) Normal and expanded Huntington's disease gene alleles produce distinguishable proteins due to translation across the CAG repe at. Mol Med 1379-83
158. Pfeiffer RF, McComb RD (1990) Dentatorubro-palli- doluysian atrophy of the myoclonus epilepsy type with posterior column degeneration. Mov Disord 5:l 34-8
159. Porteera-C:ailliau C, Hedreen J, Price DL, Koliastos VE (1 995) Evidence for apoptotic cell death in Huntington dis- ease and excitotoxic animal models. J Neurosci 15:3775- 87
160. Potter NT, Meyer MA, Zirnrnerman AW. Eisenstadt ML.
16
16
Anderson IJ (i995) Molecular and clinical findings in a family wit? dentatorubral-pallidoluysian atrophy. Ann Neurol37::273-7
. Pulst SM, Nechiporuk A, Nechiporuk T, Gispert S, CHen XN, Lopes-Cendes I, Pearlman S, Starkmans, Orozco- Diaz G, Lmkes A, DeJong P, Rouleau GA, Auburger G, Korenberg JR, Figureroa C, Sahba S (1996) Moderate expansion of a normally biallelic trinucleotide repeat in spinoceretellar ataxia type 2. Nature Genet 14:269-276
. Pulst SM, Nechiporu, A, Starkman S (1993) Anticipation in spinoceretellar ataxia type 2. Nature Genet 5:8-10
163.Ranurn LF'W, Chung M, Banfi S, Bryer A, Schut LJ, Ramesar R. Duvick LA, McCall A, Subramony SH, Goldfarb L, Gomez C. Sandkkuijl LA, Orr HT, Zoghbi HY (1 994) Molecular and clinical correlations in spinocerebel- lar ataxia type 1: evidence for familial effects on the age of onset. Am J Hum Genet 53244-51
164. Ranum LPW, Duvick LA, Rich SS, Schut LJ, Litt M, Orr HT (199l)l-ocalization of the autosomal dominant HLA- linked spirocerebellar ataxia (SCA1) locus, in two kin- dreds. witl-in an 8-cM subregion of chromosome 6p. Am J Hum Genet 4931 -41
165.Ranurn LPW, Lundgren JK, Schut LJ, Ahrens MJ, Periman S, Aita J, Bird TD, Gornez C, Orr HT. (1995) Spinocerebellar ataxia type 1 and Machado-Joseph dis- ease: incicence of CAG expansions among adult-onset ataxia patients from 311 families with dominant, reces- sive, or sporadic ataxia. Am J Hum Genet 57:603-8
166. Ranurn LID, Schut LJ, Lundgren JK, Orr HT, Livingston DM (1994) Spinocerebellar ataxia type 5 iin a family descended from the grandparents of President Lincoln maps to cl-rornosome 11. Nature Genet 8:280-4
167. Reiner A. Abin RL, Anderson KD, D'Amato cJ, Penney JB, Young 48 (1988) Differential loss of striatal projection neurons in Huntington disease. Proc Natl Acad Sci USA 855733-7
168. Reiner A, Anderson KD (1990) The patterns of neuro- transmitter and neuropeptide co-occurrence among stri- atal projection neurons: conclusions based on recent find- ings. Brain Res - Brain Res Rev 15251-65
169. Reiss AL. Abrams MT, Greenlaw R, Freund L, Denckla MB (1995) Neurodeveloprnental effects of the FMRl full mutation in humans. Nature Med 1:159-67
170. Rinne JO, Daniel SE, Scaravilli F, Pires M, Harding AE, Marsden C:D (1 994) The neuropathological features of neuroacanl hocytosis. Movement Disorders 9:297-304
Robitaille et al: Review and Update of MolecL!,ar and Genetic Features 923

171. Robitaille Y, Schut LJ, Kish SJ (1995) Structural and immunocytochemical features of olivopontocerebellar atrophy caused by spinocerebellar ataxia type 1 (SCA 1) mutation define a unique phenotype. Acta Neuropathol
172.Romanul FCA, Fowler HL, Radvany J, Feldman RG, Feingold M (1977) Azorean disease of the nervous sys- tem. N Eng J Med296:1505-8
173.Rosenberg RN, Nyhan WL, Bay C, Shore P (1976) Autosomal dominant striatonigral degeneration. A Clinical, pathological and biochemical study of a new genetic disorder. Neurology 26:703-14
174. Ross, CA (1995) When more is less: Pathogenesis of glu- tamine repeat neurodegenerative diseases. Neuron
175. Rubio A, Steinberg K, Figlewicz DA. MacDonald ME, Greenamyre T, Hamill R, Shoulson I, Powers JM (1996) Coexistence of Huntington's disease and familial amy- otrophic lateral sclerosis: case presentation. Acfa Neuropatho/92:421-7
176. Sanpei K, Takano H, lgarashi S, Sato T, Oyake M, Sasaki H. Wakisaka A, Tashiro K, lshida Y, lkeuchi T, Koide R, Saito M, Sato A, Tanaka T, Hanyu S, Takiyama Y, Nishizawa M, Shimizu N, Nomura Y, Segawa M, lwabuchi K, Eguchi I, Tanaka H, Takahashi H, Tsuji S (1996) Identification of the spinocerebellar ataxia type 2 gene using a direct identification of repeat expansion and cloning technique, DIRECT. Nature Genet 14:277-84
177. Sato K, Kashihara K, Okada S, lkeuchi T, Tsuji S, Shomori T, Morimoto K, Hayabara T (1995) Does homozygosity advance the onset of dentatorubral-pallidoluysian atro- phy? Neurology 45:1934-36
178. Schapira AH (1997) Mitochondria1 function in Huntington's disease: clues for pathogenesis and prospects for treat- ment. Ann Neuro141:141-2
179. Schmitt I, Eppleln JT, Reiss 0 (1995) Predominant neu- ronal expression of the gene responsible for denta- torubral-pallidoluysian atrophy (DRPLA) in rat. Hum Mol Genet 4:1619-24
180.Schoenen J, Delwaide PJ, Legors JJ, Franchirnont P (1979) Motoneuropathie hereditaire: la forme proximale de I'adulte liee au sexe (ou maladie de kennedy): obser- vations cliniques et neuroendocrinologiques. J Neural Sci
181. Schols L, Arnoiridis G, Epplen JT, Langkafel M, Przuntek H, Riess 0 (1996) Relations between genotype and phe- notype in German patients with the Machado-Joseph dis- ease mutation. J Neurol Neurosurg Psychiatr 61 :466-70
182. Schols L, Vieira-Saecker AM, Schols S, Przuntek H, Epplen JT, Riess 0 (1995) Trinucleotide expansion within the MJDl gene presents clinically as spinocerebellar ataxia and occurs most frequently in German SCA patients. Hum Mol Genet 4:lOOl-5
183. Schut JW (1 950) Hereditary ataxia: clinical study through six generations. Arch Neurol Psychiatr 63535-68
184. Servadio A, Koshy 8, Armstrong D, Antalffy 8, Orr TH, Zoghbi HY (1995) Expression analysis of the ataxin-1 pro- tein in tissues from normal and spinocerebellar ataxia type 1 individuals. Nafure Genet 10:94-8
901572-81
15:493-6
41:343-57
185.Sharp AH, Loev SJ. Schilling G, Li S-H, Li X-J. Bao J, Wagster MV. Kotzuk JA, Steiner JP, Lo A, Hedreen J. Sisodia S, Snyder SH, Dawson TM, Ryugo D K , Ross CA (1 995) Widespread expression of Huntington's disease gene (IT-15) protein product. Neuron 1 4:1065-74
186. Shinotoh H, Calne DB, Snow 8 , Hayward M. Kremer B, Theilmann J, Hayden MR (1994) Normal CAG repeat length in the Huntington's disease gene in senile chorea. Neurology 44:2183-4
187.Silveira I, Lopes-Cendes I, Kish S, Maciel P, Gaspar C, Coutinho P, Botez MI, Teive H, Arruda W, Steiner CE, Pinto-Junior W, Maciel JA, Jain S. Sack G, Andermann E, Sudarsky L, Rosenberg R, MacLeod P, Chitayat D, Babul R, Sequeiros J, Rouleau GA (19 96) Frequency of spino- cerebellar ataxia type 1, dentatorubropallidoluysian atro- phy, Machado-Joseph disease mutations in a large group of spinocerebellar .ataxic patients. Neurology 46:214-8
188. Singer C (1992) Haw River syndrome or dentato-rubro- pallido-luysian atrophy? Arch Neurol 49:l 3
189. Siomi MC, Zhang Y, Siomi H, Dreyfuss G (1996) Specific sequences in the fragile X syndrome protein FMRl ar,d FXR proteins mediate their binding of 60s ribosomal sub- units and the interactions among them. Mol Cell B i d
190. Smith JK (1975) Dentatorubropallidoluysian atrophy. In: Handbook of Clinical Neurology vol 21; System Disorders and Atrophies, Part I. Vinken PJ, Bruyn GW, eds. Amsterdam: North Holland, pp. 519-34
191. Smith JK, Gonda VE, Malamud N (1958) Unusual form cf cerebellar ataxia. Combined dentato-rubral and pallido- Luysian degeneration. Neurology 8:205-9
192.Sobue G, Doyu M, Nakao N, Shimada N, Mitsuma T, Maruyama H, Kawakami S, Nakarnura S (1996) Homozygosity for Machado-Joseph disease gene enhances phenotypic severity. J Neurol Neurosurg Psychiatr 60:354-6
193. Sobue G, Hashizume Y, Mukai E. Hirayam M, Mitsurna T, Takahashi A (1 989) X-linked recessive bulbospinal neu- ronopathy. Brain 11 2:209-232.
194. Sotrel A, Paskevich PA, Kiely DK. Bird ED, Williams RS, Myers RH (1991) Morphometric analysis of the prefrontal cortex in Huntington's disease. Neurology 41:1117-23
195. Sotrel A, Williams RS, Kaufmann WE, Myers RH (1 993) Evidence for neuronal degeneration and dendritic plastic- ity in cortical pyramidal neurons of Huntington's disease: A quantitative Golgi study. Neurology 43:2088-96
196.Spadaro M, Giunti P, Lulli P, Frontali M, Jodice C, Cappellacci S. Morellini M, Persichetti F, Trabace S , Anastasi R, et al (1992) HLA-linked spinocerebellar atax- ia: a clinical and genetic study of large Italian kindreds. Acta Neurol Scand 84:257-65
197. Spargo E, Everall IP, Lantos PL (1993) Neuronal loss in the hippocampus in Huntington's disease: a comparison with HIV infection. J Neurol Neurosurg Psychiatr 53487- 91
16:3825-32
_ _ .- - . __ .- -- - ~ - - - - _. - -
924 Robitaille et al: Review and Update of Molecular and Genetic Features

198. Stevanin G, Cancel G. DArr A, Chneiweiss H, Dubourg 0, Weissenbach J, Cann HM, Agid Y, Brice A (1995) The gene for spinal cerebellar ataxia 3 (SCA3) is located in a region of approximately 3 cM on chromosome 14q24.3- q32.2. Am J Hum Genet 56:193-201
199. Stevanin G, Le Guern E, Ravis6 N, Chneiweiss H, DArr A, Cancel G, Vignal A, Boch A-L, Ruberg M, Penet C, Pothin Y, Lagroua I, Haguenau M, Rancurel G, Weissenback J. Agid Y, Brice A (1994) A third locus for autosomal domi- nant cerebellar ataxia type I maps to chromosome 14q24.3-qter: evidence for the existence of a fourth locus. Am J Hum Genet 54: 11 -20
200. Storey E, Beal MF (1993) Neurochemical substrates of rigidity and chorea in Huntington's disease. Brain
201. Strong TV, Tagle DA, Valdes JM, Elmer LW, Boehm K, Swaroop M, Kaatz KW, Collins FS, Albin RL (1995) Widespread expression of the human and rat Huntington's disease gene in brain and nonneuronal tis- sues. Nature Genet 5259-65
202. Subramony SH, Currier RD (1991) The classification of familial ataxias In: Handbook of Clinical Neurology vol 16 (60), Hereditary Neuropathies and Spinocerebellar Atrophies, JMBV de Jong, editor, Elsevier, Amsterdam,
203. Subramony SH, Currier RD (1 996) lntrafamilial variability in Machado-Joseph disease. Mov Disord 11 :741-3
204.Subramony SH, Fratkin JD, Manyam BV, Currier RD (1 996) Dominantly inherited cerebello-olivary atrophy is not due to a mutation at the spinocerebellar ataxia-I, Machado-Joseph disease, or dentato-rubro-pallido- luysian atrophy locus. Mov Disord 11 :174-80
205.Tagliavini F, Pilleri G (1983) Basal nucleus of Meynert. A neuropathological study in Alzheimer's disease, simple senile dementia, Picks disease and Huntington's chorea. J Neuro Sci 62243-60
206.Takahashi H, Ohama E, naito H, takeda S, Nakashima S, makifuchi T, lkuta F (1 988) Hereditary dentato-rubral-pal- lidoluysian atrophy: clinical and pathologic variants in a family. Neurology 38: 1065-70
207.Takano H, lkeuchi T, lgarashi S, Oyake M, Koide R, Sasaki R, Sanpei K, Sasaki H, Wakisaka A, Tashiro K, lwabuchi K. Takiyama Y, Nishizawa M, Tanaka H, Tsuji S (1 997) A molecular genetic study on autosomal-dominant ataxias in Japanese. Comparison of the prevalences and CAG repeat expansions among spinocerebellar ataxia (SCA l), spinocerebellar ataxia type 2 (SCAZ), Machado- Joseph disease (MJD), and Dentatorubral-Pallidoluysian atrophy (DRPLA). Neurology 48:A209
208. Takano H, Ondera 0, Takahashi H, lgarashi S, Yamada M, Oyake M, lkeuchi T, Koide R, Tanaka H, lwabuchi K, Tsuji S (1996) Somatic mosaicism of expanded CAG repeats in brains of patients with dentatorubral-palli- doluysian atrophy: cellular population- dependent dynam- ics of mitotic instability. Am J Hum Genet 58:1212-22
209. Takano T, Yamanouchi Y. Nagafuchi S, yamada M (1996) Assignment of the dentatorubral and pallidoluysian atro- phy (DRPLA) gene to 12~13.31 by fluorescence in situ hybridization. Genomics 32:171-2
11 63201 -22
pp. 271-284
210.Takiyama Y, Nishizawa M, Tanaka H, Kawashima S, Sakamoto H, Karube Y, Shimazaki H, Soutome M, Endo K, Ohta S, Kagawa Y, Kanazawa I, Mizuno Y, Yoshida M, Yuasa T, Horikawa Y, Oyanagi K. Nagai H, Kondo T, lnuzuka T, Clnodera 0, Tsuji S (1993) The gene for Machado-Jos,?ph disease maps to human chromosome 14q. Nature Genet 4300-4
211. Takiyama Y, Oyanagi S, Kawashima S, Sakamato H, Saito K, Yoshida M, Tsuji S. Mizuno Y, Nishizawa M (1 994) A clinical and pathologic study of a large Japanese family with Machado-Jospeh disease tightly linked to the DNA markers on chromosome 14q. Neurology 44:1302-8
212.Tanaka F, S,Jbue G, Doyu M, lto Y, Yarnamoto M, Shimada N, Yamamoto K, Riku S, Hshizume Y, Mitsuma T (1996) Differential pattern in tissue-specific somatic mosaicism of expaned CAG trinucleotide repeat in denta- torubral-pallicoluysian atrophy, Machado-Joseph dis- ease, and X-linked recessive spinal and bulbar muscular atrophy. J Neiirol Sci 135:43-50
21 3. Telenius H, Almqvist E, Kremer B, Spence N, Squitieri F, Nichol K, Grandell U, Starr E, Benjamin C, Castaldo, Calabrese 0, Anvret M, Goldberg YP, Hayden MR (1995) Somatic mosaicism in sperm is associated with intergen- erational (CA13)n changes in Huntington disease. Hum Mol Genet 4:189-95
214. Telenius H, Kremer 8, Goldberg YP, Theilmann J, Andrew SE, Zeisler J, Adam S, Greenberg C, lves EJ, Clarke LA, Hayden MR (1 994) Somatic and gonadal mosaicism of the Huntingtoi disease gene CAG repeat in brain and sperm. Nature Genet 6:409-14
21 5. Tteca J, Vari Bogaert L (1 946) Heredo-degenerative hemiballismus: a contribution to the question of primary atrophy of the corpus Luysii. Brain 69:251-63
216.Trottier Y, D e q s D, lmbert G, Saudou F, An I, Lutz Y, Weber C, Agid Y, Hirsch EC, Mandel JL (1995) Cellular localization of the Huntington's disease protein and dis- crimination of :he normal and mutated form. Nature Genet
217. Trottier Y, Luti: Y, Stevanin G, lmbert G, Devys D, Cancel G, Saudou F, Weber C, David G, Tora L, Agid Y, Brice A, Mandel J-L (1 995) Polyglutamine expansion as a patho- logical epitope in Huntington's disease and four dominant cerebellar ataxias. Nature 378:403-6
218.Turpenny P, Clark C, Kelly K (1994) Intelligence quotient profile in myotonic dystrophy, intergenerational deficit, and correlation with CTG amplification. J Med Genet
219. Uyama E, Kondo I, Uchino M, Fukushima T, Murayama N, Kuwano A, lnokuchi N, Ohtani Y, Ando M (1995) Dentatorubral-pallidoluysian atrophy (DRPLA): clinical, genetic, and neuroradiologic studies in a family. J Neurol Sci 130: 146-5:3
220.Vermesh P, Sergeant N, Ruchoux MM, Hofmann- Radvany H, Wattez. Petit H. Dewailly P, Delacourte A (1 996) Specific tau variants in the brains of patients with myotonic dystrophy. Neurology 47:711-7
221.Vonsattel JP, Myers RH, Stevens TJ, Ferrante RJ, Bird ED, Richardscln, EP Jr (1 985) Neuropathological classifi- cation of Huntington's disease. J Neuropath Exp Neurol 44559-77
10:104-10
31 1300-5
.~
Robitaille et al: Review and Update of Molecular and Genetic Features 925

222. Warner m, Lennox GG, Janota I, Harding AE (1994) Autosomal-dominant dentatorubropallidoluysian atrophy in the United Kingdom. Mov Disord 9:289-96
223. Warner l7, Williams L, Harding AE (1994) DRPLA in Europe. Nature Genet 6:225
224. Warner T, Williams LD. Walker RWH, Flinter F, Robb SA, Bundey SE, Honavar M, Harding AE (1995) A clinical and molecular genetic study of dentatorubropallidoluysian atrophy in four European families. Ann Neuro/37:452-9
225. Warren ST (1996) The expanding world of trinucleotide repeats. Science 271 :1374-5
226. Wexler NS, Young AB, Tanzi RE, Travers H (1987) Homozygotes for Huntington's disease. Nature 326:194-7
227. Whittington JE, Keats BJ, Jackson JF, Currier RD, Terasaki PI (1980) Linkage studies on glyoxalase I (GLO), pepsinogen (PG), spinocerebellar ataxia (SCAl), and HLA. Cyfogenet Cell Genet 28:145-50
228. Wilde J, Moss T, Thrush D (1987) X-linked bulbo-spianl neuronopathy: a family study of three patients. J Neurol Neurosurg Psychiatr 50:279-284
229. Willemson R, Smits A, Mohkamsing S, Vanbeerendonk H, Dehaan A, Devries 8, Vandenouweland A, Sistermans E, Galjaard H, Oostra BA (1997) Rapid antibody test for diagnosing Fragile X syndrome. A validation of the tech- nique. Hum Genet 99:308-11
230. Woods BT, Schaumburg HH (1 972) Nigrospinodentatal degeneration with nuclear ophthalmoplegia. An unique and partially treatable clinicopathological entity. J Neuro Sci 17:149-66
231. Xuereb JH, MacMillan JC, Snell R, Davies P, Harper PS (1 996) Neuropathological diagnosis and CAG repeat expansion in Huntington's disease. J Neurol Neurosurg Psychiatr 60:78-81
232.Yazawa I, Nukina N, Hashida H, Goto J, Yarnada M. Kanazawa I (1995) Abnormal gene product identified with hereditary dentatorubral-pallidoluysian atrophy (DRPLA) brain. Nature Genet 10:99-103
233.Zeitlin S, Liu JP, Chapman DL, Papaioannou VE, Efstratiadis A (1 995) Increased apoptosis and early embryonic lethality in mice nullizygous for the Hungtinton's disease gene hornologue. Nature Genet
234. Zhuchenko 0, Bailey J, Bonnen P, Ashizawa T, Stockton DW, Amos C, Dobyns WE, Subramony SH, Zoghbi HY, Lee CC (1997) Autosornal dominant cerebellar ataxia (SCA 6) associated with small polyglutamine expansions in the ~l A-voltage-dependent calcium chan nel. Nature Genet 1552-9
235.Zoghbi HY, Jodice C, Sandkuijl LA, Kwiatkowski TJ Jr., McCall AE, Huntoon SA, Lulli P, Spadaro M, Litt M, Cann HM, Frontali M, Terrenato L (1991) The gene for autoso- ma1 dominant spinocerebellar ataxia (SCA1) maps telom- eric to the HLA complex and is closely linked to the D6S89 locus in three large kindreds. Am J Hum Genet
236.Zuhlke C, Riess 0, Bockel 8, Lange H. Thies U (1993) Mitotic stability and meiotic variability of the (CAG)n repeat in the Huntington disease gene. Hum Mol Genet
237. Zweig RM, Ross CA, Hedreen JC, Peyser C, Cardillo JE, Folstein SE. Price DL (1992) Locus coeruleus involve- ment in Huntington's disease. Arch Neuro/49:152-6
11 11 55-63
49123-30
2:2063-7
- - ._ __ - . - - -_ - - __ - - 926 Robitaille et al: Review and Update of Molecular and Genetic Features