The need to develop centers for environmental oncology
9
Point of view The need to develop centers for environmental oncology Devra Lee Davis a, * , Maryann Donovan g , Ronald Herberman b , Mitchell Gaynor c , Deborah Axelrod d , Nik van Larebeke e , Annie J. Sasco f a University of Pittsburgh Cancer Institute and Graduate School of Public Health, University of Pittsburgh, Pittsburgh, PA, USA b University of Pittsburgh Cancer Institute, University of Pittsburgh Medical Center, Pittsburgh, PA, USA c Cornell Medical College, Strang Cancer Prevention Center, Cornell, NY, USA d New York University Medical Center, Director Breast Services and Community Outreach, New York, USA e Study Centre for Carcinogenesis and Primary Prevention of Cancer, Ghent University, University Hospital 3K3 f Epidemiology for Cancer Prevention, Inserm, U 593 Universite ´ Victor Segalen Bordeaux 2, Bordeaux, France g University of Pittsburgh Cancer Institute and Department of Pathology, University of Pittsburgh, Pittsburgh, PA, USA Received 22 May 2007; accepted 7 June 2007 Abstract The scale and scope of the cancer problem in the United States today is much greater than four decades ago when the formal war against the disease was first announced. Patterns of the disease are not fully explained by known risk factors. Much progress has been made in understanding the molecular basis of carcinogenesis, particularly the near consensus (realization) that virtually all cancers arise from an accumulation of genetic mutations and the more recent recognition of the role of inflammation and the tissue microenvironment, in particular for hormone- dependant cancers. However, most genetic mutations that contribute to cancer are not inherited, and thus must be attributable to accumulation of somatic mutations and epigenetic changes, from as yet poorly understood environmental factors, that certainly cannot be explained entirely by tobacco, use and arise over the course of a lifetime. Much of the national effort to control cancer has focused on detecting and treating the diseasednot on seeking approaches to prevent cases from arising. Given this reality, we present a cross-disciplinary framework for establishing comprehensive research and policy centers focused on environmental oncology to be based at selected academic cancer centers across the coun- try. The principal goal of such centers is to improve the ability to prevent cancer, by developing effective interventions based on insights obtained from epidemiology, including molecular epidemiology and basic scientific research on genomic, metabolomic, and other biomarkers of expo- sure, susceptibility, and disease. As the needed scientific evidence for environmental factors contributing to cancer is revealed, these academic centers will develop specific interventions and/or policy recommendations regarding ways to lower the burden of cancer, based on existing information about cancer hazards in the personal, occupational, and general environment. Ultimately the centers will improve the ability to iden- tify and control the underlying causes of the occurrence of cancer and its progression. Ó 2007 Elsevier Masson SAS. All rights reserved. Keywords: Cancer; Epidemiology; Toxicology; Environmental; Carcinogenesis; Oncology; Risk 1. Scope of the cancer problem Within the next decade, cancer is likely to replace heart dis- ease as the leading cause of death [1]. One in three Americans will be diagnosed with cancer during their lifetimes, and more than one in four will die of the disease [2]. This growth in im- portance of cancer is not simply a consequence of the expand- ing and aging of the population. For persons aged 45e64, cancer is responsible for more deaths than the next three causes (heart disease, accidents, and stroke) combined. After accidents, cancer is also the leading cause of death in children and young white men and women under the age of 30 [3]. Pub- lic policy efforts to lower the risk of developing cancer by addressing multiple causes that are associated with the ambient environment remain limited. * Corresponding author at: 5150 Centre Ave, Suite 432, Pittsburgh, PA 15232, USA. Tel.: þ1 412 623 1172; fax: þ1 412 623 1382. E-mail address: [email protected] (D. L. Davis). 0753-3322/$ - see front matter Ó 2007 Elsevier Masson SAS. All rights reserved. doi:10.1016/j.biopha.2007.06.006 ARTICLE IN PRESS Please cite this article in press as: Davis D.L. et al., The need to develop centers for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/ j.biopha.2007.06.006 Biomedicine & Pharmacotherapy xx (2007) 1e9 www.elsevier.com/locate/biopha + MODEL
Transcript of The need to develop centers for environmental oncology
ARTICLE IN PRESS
Biomedicine & Pharmacotherapy xx (2007) 1e9www.elsevier.com/locate/biopha
+ MODEL
Point of view
The need to develop centers for environmental oncology
Devra Lee Davis a,*, Maryann Donovan g, Ronald Herberman b, Mitchell Gaynor c,Deborah Axelrod d, Nik van Larebeke e, Annie J. Sasco f
a University of Pittsburgh Cancer Institute and Graduate School of Public Health, University of Pittsburgh, Pittsburgh, PA, USAb University of Pittsburgh Cancer Institute, University of Pittsburgh Medical Center, Pittsburgh, PA, USA
c Cornell Medical College, Strang Cancer Prevention Center, Cornell, NY, USAd New York University Medical Center, Director Breast Services and Community Outreach, New York, USA
e Study Centre for Carcinogenesis and Primary Prevention of Cancer, Ghent University, University Hospital 3K3f Epidemiology for Cancer Prevention, Inserm, U 593 Universite Victor Segalen Bordeaux 2, Bordeaux, France
g University of Pittsburgh Cancer Institute and Department of Pathology, University of Pittsburgh, Pittsburgh, PA, USA
Received 22 May 2007; accepted 7 June 2007
Abstract
The scale and scope of the cancer problem in the United States today is much greater than four decades ago when the formal war against thedisease was first announced. Patterns of the disease are not fully explained by known risk factors. Much progress has been made in understandingthe molecular basis of carcinogenesis, particularly the near consensus (realization) that virtually all cancers arise from an accumulation ofgenetic mutations and the more recent recognition of the role of inflammation and the tissue microenvironment, in particular for hormone-dependant cancers. However, most genetic mutations that contribute to cancer are not inherited, and thus must be attributable to accumulationof somatic mutations and epigenetic changes, from as yet poorly understood environmental factors, that certainly cannot be explained entirely bytobacco, use and arise over the course of a lifetime. Much of the national effort to control cancer has focused on detecting and treating thediseasednot on seeking approaches to prevent cases from arising. Given this reality, we present a cross-disciplinary framework for establishingcomprehensive research and policy centers focused on environmental oncology to be based at selected academic cancer centers across the coun-try. The principal goal of such centers is to improve the ability to prevent cancer, by developing effective interventions based on insights obtainedfrom epidemiology, including molecular epidemiology and basic scientific research on genomic, metabolomic, and other biomarkers of expo-sure, susceptibility, and disease. As the needed scientific evidence for environmental factors contributing to cancer is revealed, these academiccenters will develop specific interventions and/or policy recommendations regarding ways to lower the burden of cancer, based on existinginformation about cancer hazards in the personal, occupational, and general environment. Ultimately the centers will improve the ability to iden-tify and control the underlying causes of the occurrence of cancer and its progression.� 2007 Elsevier Masson SAS. All rights reserved.
Keywords: Cancer; Epidemiology; Toxicology; Environmental; Carcinogenesis; Oncology; Risk
1. Scope of the cancer problem
Within the next decade, cancer is likely to replace heart dis-ease as the leading cause of death [1]. One in three Americanswill be diagnosed with cancer during their lifetimes, and more
* Corresponding author at: 5150 Centre Ave, Suite 432, Pittsburgh, PA
15232, USA. Tel.: þ1 412 623 1172; fax: þ1 412 623 1382.
E-mail address: [email protected] (D. L. Davis).
0753-3322/$ - see front matter � 2007 Elsevier Masson SAS. All rights reserve
doi:10.1016/j.biopha.2007.06.006
Please cite this article in press as: Davis D.L. et al., The need to develop cen
j.biopha.2007.06.006
than one in four will die of the disease [2]. This growth in im-portance of cancer is not simply a consequence of the expand-ing and aging of the population. For persons aged 45e64,cancer is responsible for more deaths than the next threecauses (heart disease, accidents, and stroke) combined. Afteraccidents, cancer is also the leading cause of death in childrenand young white men and women under the age of 30 [3]. Pub-lic policy efforts to lower the risk of developing cancer byaddressing multiple causes that are associated with the ambientenvironment remain limited.
d.
ters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/

2 D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
The field of medical oncology has matured impressivelysince its inception some four decades ago amidst military rhet-oric by President Richard M. Nixon. It is now clear, though,that the struggle cannot be won by only attacking the diseaseonce it has arisen. Complex biological processes underlie bothcarcinogenesis and progression of clinically detectable can-cers. As a result, an effective, generally applicable cure forall cancers is unlikely to be in our reach in the foreseeable fu-ture. Renewed efforts are called for to reduce the toll of cancerby redirecting attention to identifying and controlling the un-derlying causes of cancer. Real progress has been made intreating some of the rarer forms of cancer, including childhoodleukemias, testicular, and thyroid cancer, and modest improve-ment has also been noted at least among the white populationfor some common cancers such as breast and colon cancers[4]. Largely because of the unequivocal evidence for the majorcancer risk associated with tobacco use and the resultant de-clines in smoking-related cancers among men, overall cancerdeath rates have dropped in the past decade. In addition,new findings in genomics, proteomics, and metabolomicshave advanced the capacity to tailor treatments for advanceddisease, although wide scale use is far from being the normfor the time being [5]. None of these advances, though, islikely to affect the capacity to prevent cancer from occurring[6]. As the majority of cancers is linked with avoidable envi-ronmental factors that act years before the disease can be de-tected [7], there is renewed appreciation of the need to addressthese through primary and primordial prevention policies [8].
There are nearly ten million cancer survivors in the UnitedStates today, each of whom is concerned with preventing thedisease from developing in their own family and with extend-ing their own survival. The cancer hazards of smoking andalcohol are well established, and the cancer risks of obesityhave recently been confirmed in several studies [9]. Exceptingprograms on smoking control and some workplace hazards, wehave not been able to translate much of what is known aboutcancer causation into effective public policy and programs toavert the disease. A variety of nutritional and other interven-tions are being actively investigated to prevent the recurrenceof cancer or the development of second primary cancers [10].Yet, many interventions that are widely used by cancerpatients and by those seeking to reduce their chance of devel-oping cancer remain outside the purview of clinical trials [11].Little effort has gone into assessing and reducing broad-scalecomplex and non-tobacco-related environmental determinantsof cancer. In addition, no reliable, validated survey instru-ments exist for assessing the positive or negative impact of
1 On April 7, 2005 the following notice appeared on the SEER website: ‘‘Ta-
ble Ie3 was temporarily removed - The Percent Change and APC for
1950-2001 were incorrectly calculated: For incidence data, the yearly rates
for 1950-1972 were age-adjusted using the 1970 standard million population,
and the remaining years (1973-2001) were age-adjusted using the 2000 stan-
dard million population. The mortality trends were based on rates age-adjusted
using the 2000 standard million population.’’ The table has not yet been re--
posted, and no equivalent appears in subsequent SEER reports. See http://
seer.cancer.gov/csr/1975_2001/revisions.html.
Please cite this article in press as: Davis D.L. et al., The need to develop cen
j.biopha.2007.06.006
integrative or complementary medicine in those who incorpo-rate this modality into their treatment regimens for cancer; noris there a standard protocol for assessing environmental, work-place, and other exogenous factors that can contribute to thedisease evolution.
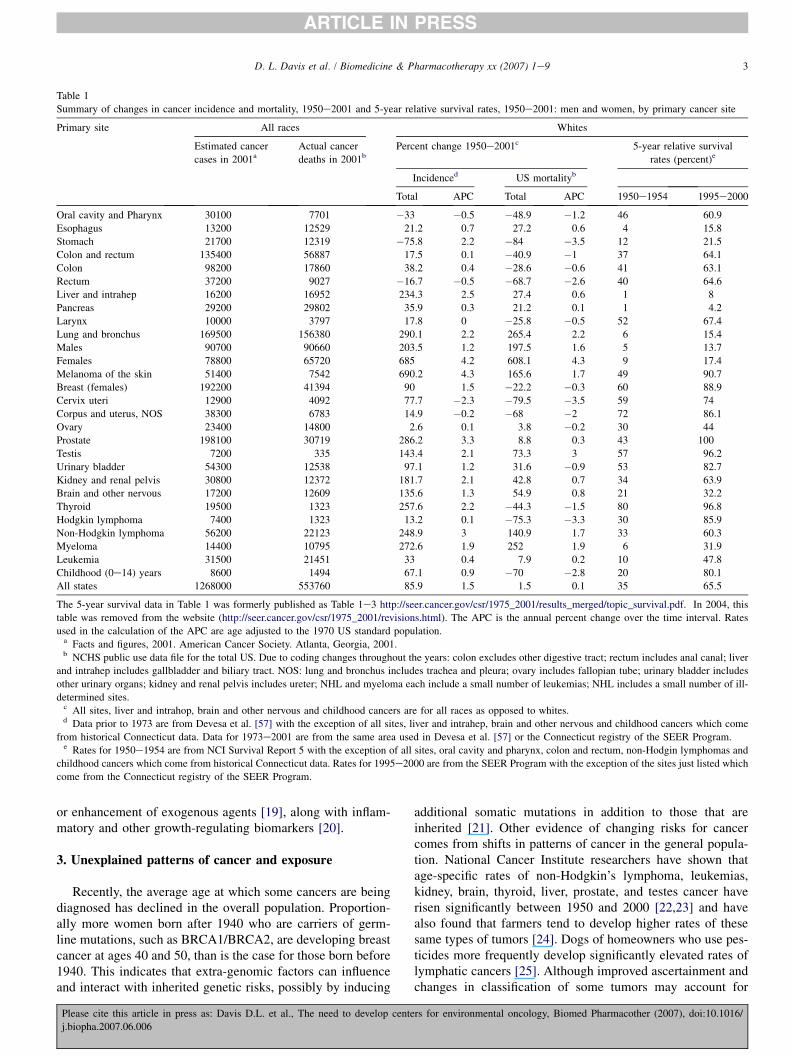
Although United States national cancer incidence hasdeclined for smoking related cancers [12]. Table 1 appearedin the SEER Cancer Statistics Review, 1975e2001.1 As the ta-ble indicates, there were many important increases in inci-dence in this time period. Unfortunately it is not possible tocharacterize these recent patterns in cancer relative to thoseshown in Table 1, because an updated version of that tablehas not appeared since 2004. Questions have been raised aboutthe appropriate population age adjustment that should be usedto make such analyses, and, as a result, these analyses are nolonger being done. It should be noted that if standards re-mained the same, the comparisons will be valid over time, in-dependently of the absolute numerical values of the rates.
2. Importance of acquired factors
Cancer is chiefly a disease of genomic instability, which re-sults when cells lose their ability to perform error-free DNArepair resulting in aberrant growth. Extra-genomic factorsthat alter cell growth also contribute to this process. Thereare reasons to believe that, at the level of cells and tissue,any increase in disorder (entropy), from external factors willbe associated with some increase in the risk of malignanttransformation. Evidence that exogenous exposures in additionto smoking are critical determinants of cancer comes fromstudies of inheritance, and from observations of patterns ofdisease tied with migration, nutrition, and the workplace.With respect to familial studies, fewer than 10% of all cancersarise in persons born with a germ-line mutation. This meansthat most cancer is not inherited, but is acquired over thecourse of a lifetime. Some studies have found that adoptedchildren tend to acquire the cancer risk of their adoptive par-ents as opposed to their biological parents; of 960 familieswith adopted children, the cancer death of an adoptive parentresulted in relative risks of cancer death in the adoptees thatwere 5.16 (1.20e22.2) higher when compared with the riskof cancer in the biologic parent [13]. Analyses of geneticallyidentical twins have found that breast, colon, and prostate can-cer developed in both twins only between 14 and 30% of thetime [14,15]. Studies of migrant populations reveal that secondgeneration immigrants to the United States or Sweden [16]from Asia have a significantly higher incidence of some can-cers, such as breast or cervix cancer, compared to their ances-tors, whereas they lose their risk of traditional cancers such asnasopharyngeal carcinoma [17]. Although they are generallyhealthier in terms of overall mortality than the (overall) totalpopulation, workers with high exposures to specific com-pounds or industrial processes are at increased risk for the de-velopment of many cancers [18]. Serological, immunologicaland gene-expression profiling have identified a number of reg-ulatory genes that affect carcinogenic metabolism such as es-trogen-responsive genes and those involved in detoxification
ters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/
3D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
Table 1
Summary of changes in cancer incidence and mortality, 1950e2001 and 5-year relative survival rates, 1950e2001: men and women, by primary cancer site
Primary site All races Whites
Estimated cancer
cases in 2001aActual cancer
deaths in 2001bPercent change 1950e2001c 5-year relative survival
rates (percent)e
Incidenced US mortalityb
Total APC Total APC 1950e1954 1995e2000
Oral cavity and Pharynx 30100 7701 �33 �0.5 �48.9 �1.2 46 60.9
Esophagus 13200 12529 21.2 0.7 27.2 0.6 4 15.8
Stomach 21700 12319 �75.8 2.2 �84 �3.5 12 21.5
Colon and rectum 135400 56887 17.5 0.1 �40.9 �1 37 64.1
Colon 98200 17860 38.2 0.4 �28.6 �0.6 41 63.1
Rectum 37200 9027 �16.7 �0.5 �68.7 �2.6 40 64.6
Liver and intrahep 16200 16952 234.3 2.5 27.4 0.6 1 8
Pancreas 29200 29802 35.9 0.3 21.2 0.1 1 4.2
Larynx 10000 3797 17.8 0 �25.8 �0.5 52 67.4
Lung and bronchus 169500 156380 290.1 2.2 265.4 2.2 6 15.4
Males 90700 90660 203.5 1.2 197.5 1.6 5 13.7
Females 78800 65720 685 4.2 608.1 4.3 9 17.4
Melanoma of the skin 51400 7542 690.2 4.3 165.6 1.7 49 90.7
Breast (females) 192200 41394 90 1.5 �22.2 �0.3 60 88.9
Cervix uteri 12900 4092 77.7 �2.3 �79.5 �3.5 59 74
Corpus and uterus, NOS 38300 6783 14.9 �0.2 �68 �2 72 86.1
Ovary 23400 14800 2.6 0.1 3.8 �0.2 30 44
Prostate 198100 30719 286.2 3.3 8.8 0.3 43 100
Testis 7200 335 143.4 2.1 73.3 3 57 96.2
Urinary bladder 54300 12538 97.1 1.2 31.6 �0.9 53 82.7
Kidney and renal pelvis 30800 12372 181.7 2.1 42.8 0.7 34 63.9
Brain and other nervous 17200 12609 135.6 1.3 54.9 0.8 21 32.2
Thyroid 19500 1323 257.6 2.2 �44.3 �1.5 80 96.8
Hodgkin lymphoma 7400 1323 13.2 0.1 �75.3 �3.3 30 85.9
Non-Hodgkin lymphoma 56200 22123 248.9 3 140.9 1.7 33 60.3
Myeloma 14400 10795 272.6 1.9 252 1.9 6 31.9
Leukemia 31500 21451 33 0.4 7.9 0.2 10 47.8
Childhood (0e14) years 8600 1494 67.1 0.9 �70 �2.8 20 80.1
All states 1268000 553760 85.9 1.5 1.5 0.1 35 65.5
The 5-year survival data in Table 1 was formerly published as Table 1e3 http://seer.cancer.gov/csr/1975_2001/results_merged/topic_survival.pdf. In 2004, this
table was removed from the website (http://seer.cancer.gov/csr/1975_2001/revisions.html). The APC is the annual percent change over the time interval. Rates
used in the calculation of the APC are age adjusted to the 1970 US standard population.a Facts and figures, 2001. American Cancer Society. Atlanta, Georgia, 2001.b NCHS public use data file for the total US. Due to coding changes throughout the years: colon excludes other digestive tract; rectum includes anal canal; liver
and intrahep includes gallbladder and biliary tract. NOS: lung and bronchus includes trachea and pleura; ovary includes fallopian tube; urinary bladder includes
other urinary organs; kidney and renal pelvis includes ureter; NHL and myeloma each include a small number of leukemias; NHL includes a small number of ill-
determined sites.c All sites, liver and intrahop, brain and other nervous and childhood cancers are for all races as opposed to whites.d Data prior to 1973 are from Devesa et al. [57] with the exception of all sites, liver and intrahep, brain and other nervous and childhood cancers which come
from historical Connecticut data. Data for 1973e2001 are from the same area used in Devesa et al. [57] or the Connecticut registry of the SEER Program.e Rates for 1950e1954 are from NCI Survival Report 5 with the exception of all sites, oral cavity and pharynx, colon and rectum, non-Hodgin lymphomas and
childhood cancers which come from historical Connecticut data. Rates for 1995e2000 are from the SEER Program with the exception of the sites just listed which
come from the Connecticut registry of the SEER Program.
or enhancement of exogenous agents [19], along with inflam-matory and other growth-regulating biomarkers [20].
3. Unexplained patterns of cancer and exposure
Recently, the average age at which some cancers are beingdiagnosed has declined in the overall population. Proportion-ally more women born after 1940 who are carriers of germ-line mutations, such as BRCA1/BRCA2, are developing breastcancer at ages 40 and 50, than is the case for those born before1940. This indicates that extra-genomic factors can influenceand interact with inherited genetic risks, possibly by inducing
Please cite this article in press as: Davis D.L. et al., The need to develop cen
j.biopha.2007.06.006
additional somatic mutations in addition to those that areinherited [21]. Other evidence of changing risks for cancercomes from shifts in patterns of cancer in the general popula-tion. National Cancer Institute researchers have shown thatage-specific rates of non-Hodgkin’s lymphoma, leukemias,kidney, brain, thyroid, liver, prostate, and testes cancer haverisen significantly between 1950 and 2000 [22,23] and havealso found that farmers tend to develop higher rates of thesesame types of tumors [24]. Dogs of homeowners who use pes-ticides more frequently develop significantly elevated rates oflymphatic cancers [25]. Although improved ascertainment andchanges in classification of some tumors may account for
ters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/

4 D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
some of these increases, advances in diagnostic technologycannot completely explain these patterns [26e28]. Manysuspected causes of cancer and chronic illness, such as ingre-dients in personal care or household products [29], remainpoorly controlled and these products are often not labeledwhen they contain agents known to cause cancer in animals.Recent studies reported by the Centers for Disease Controland Prevention measured exposures to 116 toxic chemicalsin blood and urine samples taken during 1999 and 2000. Forsome pesticides, such as the widely used, and now restricted,indoor agent chloropyrifos (Dursban), exposures were 3e4times higher than proposed federal reference doses for chil-dren, adolescents and adults [30,31]. While levels of exposureto many other agents in this national survey were below cur-rent standards for any single compound, these standards areset for chemicals individually and not for combined exposures.Based on these findings of extensive exposure to known andsuspected carcinogenic pesticides, the CDC Healthy People2010 Goals include reduced use of pesticides in homes,schools, and gardens, improved public notification about antic-ipated uses of such materials, and better monitoring of bodilyfluids for residues [32]. Canadian provincial efforts are alsomounting to limit the use of such materials [33]. Unfortu-nately, the well-documented and well-funded strategies ofthe tobacco industry to suppress evidence of the harm of theirproduct [34] have also been applied to some widely producedindustrial carcinogenic hazards, such as benzene [35], vinylchloride [36,37], and asbestos [38,39]. It has also proven dif-ficult to document the effects and reduce exposure to the car-cinogenic side-effects of widely used pharmaceutical productssuch as oral contraceptives, hormone replacement therapy, andtamoxifen [40], effectively delaying efforts to control or re-duce exposures to a number of these carcinogens. Funding,rule-making, and enforcement of occupational cancer stan-dards have declined over the past decade, as has the directgovernment initiation of long-term testing of potential carci-nogenic agents that are more broadly distributed [41]. Testingprotocols for drugs and suspect chemicals to evaluate carcino-genicity typically assay relatively high levels of single causesof cancer in homogeneous groups of adult animals; methods toassess the impacts of combined exposures to lower levels inmixtures of suspect materials using heterogeneous and imma-ture populations are not available at this time.
4. Weight of the evidence regarding exogenous factors
When it comes to understanding which agents are likely tocause cancer, scientists rely on the cumulative weight of the ev-idence provided by in vivo and in vitro toxicology, quantitativestructure activity relationships between known and suspectedcarcinogens, and epidemiologic studies often involving highlyexposed workers. For many animal carcinogens to which lowlevels of human exposure can be widespread, their combinedcumulative impacts on humans cannot easily be gauged.Exposures are not well documented, or groups with defined ex-posures may be so small that the power to detect statisticallysignificant effects is limited. Despite these methodological
Please cite this article in press as: Davis D.L. et al., The need to develop cen
j.biopha.2007.06.006
constraints on cancer epidemiology, every compound shownto cause cancer in humans also induces it in animals when ad-equately studied [42]. And similarly, most animal carcinogensturn out to be human carcinogens.
The International Agency for Research on Cancer of theWorld Health Organization and the US National ToxicologyProgram have adopted criteria for identifying and classifyingagents in terms of their capacity to induce cancer in experi-mental animals and humans. More than 900 agents or pro-cesses have been evaluated. Of these, 108 environmental,pharmaceutical or workplace exposures have been identifiedas Class I (confirmed causes of cancer in humans under thisframework); with another 312 considered Class II A or II B(probable human carcinogens, meaning that experimentalevidence shows they cause cancer in animals) [43]. Amongconfirmed human carcinogenic compounds or processes arepainting, shoe manufacturing and repair, hair-dressing, and al-cohol manufacturing [44]. Table 2 in Appendix B describesworkplace, agricultural, pharmaceutical and other chemicalsfor which the US National Toxicology Program finds experi-mental and epidemiological evidence of carcinogenicity,many of which are not directly regulated as carcinogens.
5. The need for environmental oncology
There are many centers of excellence in cancer epidemiol-ogy; however, very few combine such expertise with theability to develop interventions and policies based on the accu-mulating evidence not only from epidemiological studies butalso from many molecular and metabolomic biomarker basicresearch studies. One of the major things that health care insti-tutions can do to reduce the future cancer burden is to movetoward less polluting and less carbon-intensive technology.Consistent with a number of recent policy positions taken byother sectors, such as the banking and business communities,there is renewed interest within the clinical oncology researchcommunity in creating sustainable enterprises in the healthcare sector that are inherently less polluting and more efficientin order to reduce their impact on the local and global environ-ments [45]. New specialties in health care engineering and en-ergy use are promoting more efficient and less polluting use ofnatural resources and other materials within the health care en-vironment, aimed at reducing exposures of hospital employeesto cancer-inducing agents and at lowering environmental risksto the surrounding communities posed by such activities asmedical waste incineration.
In the past few years, a number of health care facilities havebegun to adopt LEED certification [46] and the principles ofsustainable hospitals, as part of an international consortium,Health Care Without Harm [47]. Among the institutions invol-ved in devising environmental preferable purchasing agree-ments thus far are: Kaiser Permanente in California, BethIsrael of New York, the new Children’s Hospital of Pittsburgh,and several other large medical institutions [48]. Health carefacilities that are mounting these efforts are conducting com-prehensive evaluations of hospital-based activities in order toidentify opportunities for cost-effective reductions in the use
ters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/

5D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
of polluting technologies and treatments and curtail the use ofmedical interventions that increase carcinogenic hazards [49].
5.1. Creation of centers for environmental oncology
Given the importance of cancer for the population today, theprojected aging of the population, and the existence of consi-derable information on suspect cancer-causing agents in theambient environment, we propose to create interdisciplinaryand comprehensive centers for environmental oncology to behoused at major academic cancer centers throughout the countryover the next decade. These centers will provide cancer patientsand their families with specific recommendations about envi-ronmental sources of potential cancer-causing hazards thatshould be avoided or reduced and will identify environmentalactivities that can be expected to lessen the chance of recurrenceor developing second primary cancers. As research centers, en-vironmental oncology programs will combine basic scientificinformation on mechanisms of carcinogenesis, including pro-teomic, metabolomic, and genomic studies. This basic researchwill be combined with epidemiological studies of biomarkers ofexposure, of inflammation processes, and susceptibility, and ofearly onset of disease in an effort to better document the connec-tion between exposure and cancer. This will be particularly im-portant in cases of multiple low dose long duration cumulativeexposures and these data will be used to generate clinical toolsto predict and reduce cancer risk and to identify effective inter-ventions. In addition, these centers will develop and validatestrategies for incorporating the on-line use of universal surveyinstruments to generate environmental and occupational histo-ries, and will create risk assessment and outreach programsfor individuals, communities, health care facilities, and the pub-lic and private sectors.
This multi-disciplinary program aims to lower the risk of de-veloping cancer by focusing on identifying ‘‘upstream’’ or con-trollable conditions and strategies for prevention, rather than ontraditional ‘‘downstream’’ consequences. It will identify andpromote concrete steps that can be taken by individuals, hospi-tals, health professionals, the surrounding communities, andprivate and public sector organizations to prevent cancer and re-duce the chance of recurrence or death. Drawing on national andinternational expert resources, these cross disciplinary centerswill gather and carefully assess extensive evidence from the ex-perimental, epidemiological, and clinical literature to identifycarcinogenic hazards for humans and then develop and apply in-terventions based on this evidence. The centers will serve as nat-ural laboratories to incubate and establish practices within thehealth-care environment that reduce the use of toxins overall,promote healthier nutrition and behavior, and enhance effi-ciency in energy, materials, and maintenance. By reviewing,evaluating, and consolidating information on cancer hazardsand on cancer preventive strategies in a single program, weaim to create clear, concise, and effective communication pro-grams to inform patients, their families, and their communitiesabout potential hazards that can be controlled and the things thatthey can do to reduce their chance of recurrence, of developingsecond primary cancers, or of dying from the disease.
Please cite this article in press as: Davis D.L. et al., The need to develop ce
j.biopha.2007.06.006
Through this multifaceted approach, centers for environ-mental oncology will generate information on environmentallinks to cancer, inform the general population, cancer patientsand their families on risks that should be avoided and devisepanels of biomarkers that can be used clinically to indicateenvironmental and nutritional targets of intervention. By com-bining molecular assessments before and after treatment forcancer patients, we will also monitor the extent to which spe-cific nutritional and environmental practices promote recoveryand reduce the chance of recurrence. By pilot testing the use ofautomated questionnaires aimed at identifying novel risk fac-tors and linking these with existing bioinformatics databasesand archived tissue and tumor registries, centers for environ-mental oncology hope to translate advances in molecular on-cology into effective strategies for cancer prevention.
The dissemination of accurate information to patients andthe general population on known and suspected cancer hazardsand on nutritional and other methods believed at this time toreduce the risk of cancer will empower people to make in-formed decisions to protect themselves and their familiesfrom exposure to these preventable risks. Centers for environ-mental oncology will capitalize on the intense interest thatcancer patients have to understand the causes of their disease.The centers will provide a reliable source of accurate informa-tion for patients, their families, and their communities regard-ing activities to be encouraged or discouraged. The programsthat will be developed here will take advantage of the high mo-tivation of many cancer patients and their caregivers to learnmore about their disease and to figure out what they can doto improve their long-term prognosis.
In calling for centers for environmental oncology, thereshould be no delusion that success will be easily measuredin terms of reduced cancer burdens in the near term. Cancerremains a disease with long latencies and multiple causes,many of which are not well understood. Establishing theevidence linking specific chemical exposures to cancer inhumans must be thought of as a work in progress, more akinto an unsolved puzzle characterized by many missing pieces.Despite these uncertainties, there are three major reasonswhy we believe it is prudent to seek to establish academicmedical center-based centers for environmental oncologythat are committed to reducing exposures to synthetic toxicagents and pollutants now and to identifying other potentiallyavoidable causes of cancer with the goal of ultimately lower-ing the cancer burden. First, despite important methodologicalrefinements in research, every compound that has been shownto cause cancer in humans also causes cancer in animals whenadequately tested and, similarly [50], evidence of cancer cau-sation in experimental animals provides at least a high suspi-cion of similar risks for humans. Second, age specific rates ofmany forms of cancer not generally tied with smoking have in-creased. The increase in younger age groups cannot be attrib-uted to underlying inherited traits, as the changes haveoccurred too fast, and therefore point to the role of new andavoidable exposures. Finally, as institutions charged with pro-tecting and preserving the health of individuals, hospitals alsohave a mandate to ensure the safety of their own staff, patients,
nters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/

6 D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
and communities by shifting to safer products wheneverpossible.
The motto of physicians since Hippocrates has been ‘‘Pri-mum, non nocere.’’ First, do no harm. In devising a compre-hensive system to reduce harm from known and suspectedtoxins within the medical environment and promote healthwithin our communities, centers for environmental oncologywill take this motto to a high level of advancement. Healthcareenvironments provide accessible ‘‘laboratories’’ for workingout feasible and cost-effective interventions aimed at reducingtoxins and promoting efficiency, and providing role models forother corporations or businesses in the region that are seekingto engage in sustainable practices.
A growing and diverse literature is emerging on the topic ofethical responsibilities that arise in the face of uncertainties re-lated to the effects that current patterns of economic develop-ment and industrial activity are having on our health and thatof future generations. Modern complexity has fundamentallyaltered the way we must think about appropriate moral behav-iors in light of the potential harms that may arise from continu-ing our dependence on synthetic materials of unproven safetyand from accepting exposure to complex pollutants [51].Given the health imperitives, ethical behavior must changeto anticipate harm, rather than to wait until harm has been ir-refutably proven to have occurred. Cancer reflects an interplayof factors, many of which are likely to remain well beyond in-dividual human control. Despite that complexity, an argumentcan be made that academic cancer centers should take on theresponsibility of modeling safer, cleaner, and greener prac-tices. These actions will in the short run benefit the immediateenvironment through improvements in efficiency and reduceduse of toxic materials, and may well, in the long run, reducethe burden of the disease.
As one philosopher has recently remarked [52]: ‘‘With cer-tain developments of our powers the nature of human actionhas changed, and, since ethics is concerned with action, itshould follow that the changed nature of human action callsfor a change in ethics as well: this not merely in the sense thatnew objects of action have added to the case material on whichreceived rules of conduct are to be applied, but in the more rad-ical sense that the qualitatively novel nature of certain of our ac-tions has opened up a whole new dimension of ethical relevancefor which there is no precedent in the standards and canons oftraditional ethics.’’ To insist on definitive proof that humanharm has occurred before implementing preventive policies toavoid that harm conflicts with the basic tenets of medicine.
Lack of human evidence for cancer causation by any compoundshould never be interpreted as proof that there is no such associa-tion. A number of legal scholars and public policy developers areadopting a precautionary approach for reducing exposures to sus-pected environmental carcinogens. For example, Carl Cranor hasargued that reviewing courts should consider the potential forharm and the potential for exposure to harmful materials in devel-oping regulatory policies [53]. Recently the outgoing President ofFrance, Jacques Chircac [54] and the Canadian provinces of On-tario, Quebec, and Alberta have advocated for reducing releasesand uses of known and suspect environmental carcinogens, and
Please cite this article in press as: Davis D.L. et al., The need to develop cen
j.biopha.2007.06.006
have devoted substantial financial resources to achieving thesegoals [55]. As an example of such precautionary policies, the statesof Washington and California have begun phasing out flame retar-dants due to their suspected carcinogenicity [56].
A goal of public health is to prevent harm, not simply to treat itonce it has already happened. Proactive measures need to betaken now to prevent or reduce the need for more extreme reac-tive behaviors in the future. Establishing Centers for Environ-mental Oncology at academic medical centers will afford thecreation of multidisciplinary programs that can identify andevaluate avoidable causes of cancer, train health professionalsand communities about opportunities to reduce the use of andexposure to environmental carcinogens, and promote the devel-opment of appropriate local, national, and international policiesto reduce the burden of cancer. It is through these combinedefforts that the Centers for Environmental Oncology will beable to achieve their goal of helping to make prevention thecure for cancer.
Acknowledgments
The authors acknowledge financial support from the HeinzEndowments, the National Cancer Institute, the HighmarkFoundation, and the Flemish government. Matt Zurenski pro-vided research assistance.
Appendix A. proposed programs and design for environ-mental oncology centers
Centers for Environmental Oncology will include four ma-jor divisions that will work collaboratively to leverage re-sources and share results on the most pressing health issuesconcerning the environment.
A.1 Basic research using existing laboratories and tissuesampling and storage program
This component will conduct in vitro and in vivo studies ofcancer-causing and cancer-preventing agents in a hospital-based setting, develop genetic, hormonal and other molecularmarkers of carcinogenic risk including gene-expression profil-ing, inflammatory markers, and other biomarkers of cancer riskand evaluate the role of prenatal, pubertal and other time-periods of enhanced vulnerability, and establish experimentalbases for prevention-based nutritional and other programs.
A.2 Molecular, environmental, and clinical epidemiology
This component will assess nutritional and other cancerpreventive agents in a clinical setting, develop biologicalmarkers of cancer risk, identify novel, clinical markers thatcan be followed to reduce the risk and recurrence of cancer,assess workplace, community and other hazards for cancer, in-cluding the role of equity, social class and ethnicity, pilot testthe use of automated core questionnaires of risk factors, andprovide innovative analyses of geographic and other patternsand trends in cancer in the community.
ters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/

7D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
A.3 Environmental assessment and control
This component will develop cutting edge methods for mea-suring pollutants, devise cost effective modeling systems forcleaning, maintenance, energy and waste reduction, recovery,and recycling within the hospital environment, and create ongo-ing systems for monitoring progress. This method is consistentwith the American Hospitals Association new program, Hospi-tals for a Healthy Environment, and with approaches being pro-duced by the National Institutes of Health. Cross-disciplinaryteams of engineering and scientific experts will be created toprovide service to communities concerned about potential envi-ronmental health conditions that may be affecting their health.
A.4 Outreach and public policy program development
This component will develop scientifically supported andneeds-assessed education programs for target audiences on theenvironment and cancer and will identify and develop policy in-novations, implement novel strategies to pay for and otherwiseencourage prevention and patient navigator programs (provid-ing financial and social support to experts who help cancer pa-tients and their families wend their way through treatment),and create market incentives for businesses to promote preven-tive policies. Education and public policy material will be dis-seminated through state-of-the-art communication media,such as webcasting and video-streaming, hospital-based cabletelevision programming, telemedicine, digitized video, CD-ROMs and printed matter. Interactive multi-media efforts willbe launched as part of continuing medical education trainingprograms in environmental oncology. Public lecture series willbe designed with community input and developed with healthprofessionals, hospitals, patients and various public groups.
Appendix B
Table 2 indicates workplace, agricultural, pharmaceutical andother chemicals for which the US National Toxicology Programfinds experimental and epidemiological evidence of carcinoge-nicity, many of which are not directly regulated as carcinogens.
Table 2
National Toxicology Program’s cancer bioassays [58]
Chemical solvents Benzene
1,1-Dichloroethane
1,2-Dichloropropane
Methylene chloride
Nitromethane (also used
in rocket and engine fuels)
1,2,3-Trichloropropane
Chemicals used or formed in
the manufacturing of dyes
C.I. acid red 114
C.I. basic red 9
2,4-Diaminotoluene
3,30-Dimethlybenzidine dihydrochloride
3,30-Dimethoxybenzidine dihydrochloride
2,4-Dinitrotoluene
Hydrazobenzene
o-Nitrotoluene
o-Toluidine hydrochloride
Please cite this article in press as: Davis D.L. et al., The need to develop ce
j.biopha.2007.06.006
References
[1] Leaf C. The war on cancer, why we’re losing the war on cancer e and
how to win it. Fortune Mag 2004;149(6):77e92.
[2] Deaths/Mortality. National Center for Health Statistics. Accessed May.
Available at, http://www.cdc.gov/nchs/fastats/deaths.htm, 2007;14.
[3] Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, et al. Cancer sta-
tistics. CA Cancer J Clin 2006;2006(56):106e30.
[4] Bailar III JC. Deaths from all cancers: trends in sixteen countries. Ann
NY Acad Sci 1990;609:49e56.
[5] Schmidt C. Metabolmics: what’s happening downstream of DNA. Envi-
ron Health Perspect 2004;112(7):410e5.
[6] Davis D, Hoel D. In: Trends in cancer mortality in industrial countries.
Ann NY Acad Sci, 609; 1990. p. 5e48.
[7] National Cancer Institute. Cancer and the environment. Washington, DC:
National Cancer Institute; 2003.
[8] National Cancer Institute. The majority of cancers are linked to the en-
vironment. benchmarks. National Cancer Institute; 2007. Available atAc-
cessed May 14.
Chemicals used in the
manufacturing of rubber,
vinyl, polyurethane
foams or neoprene
Benzene (rubber manufacturing))
1,3-Butadiene (rubber manufacturing)
Chloroprene (neoprene manufacturing)
2,4-Diaminotoluene (polyethylene
manufacturing)
1,2-Dichloroethane (vinyl chloride
manufacturing)
Glycidol (vinyl manufacturing)
o-Nitrotoluene (rubber manufacturing)
2,4-2,6-Toluene diisocyanate
(polyethylene foam manufacturing)
Chemical intermediates Ethylene oxide (anti-freeze products)
Isoprene (formed during
ethylene production)
Flame retardants 2,2-Bis(bromomethyl)-1,3-propanediol
2,3-Dibromo-1-propanol
Food additive Methyleugenol (flavoring)
Fumigants and pesticides Clonitralid (molluscicide)
1,2-Dibromoethane (also called
ethylene dibromide)
1,2-Dibromo-3-chloropropane(soil fumigant)
1,2-Dichloroethane (soil/grain fumigant)
1,2-Dichloropropane (soil/grain fumigant)
Dichlorvos (insecticide)
Sulfallate (herbicide)
Gasoline additives Benzene
1,2-Dibromoethane (lead scavenger)
1,2-Dichloroethane (lead scavenger)
Microelectronics Indium phosphide (used in semiconductors)
Mycotoxin Ochratoxin A (toxin produced by molds)
Pharmaceutical drugs Acronycine (anti-cancer drug)
Cytembena (cytostatic drug)
Furosemide (diuretic)
Hydrazobenzene (used in making
phenylbutazone, an antiarthritic drug)
Isophosphamide (anti-cancer drug)
Nitrofurazone (anti-bacterial agent)
Phenesterin (anti-cancer drug)
Procarbazine hydrochloride
(anti-cancer drug)
Reserpine (anti-hypertension drug)
Sterilizing agent for medical
instruments
Ethylene oxide
Research chemical 5-Nitroacenaphthenol
Riot control/tear gas 2-Chloroacetophenone
nters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/

8 D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
[9] Calle E, Thun M. Obesity and cancer. Oncogene 2004;23(38):
6365e78.
[10] White JD. Complementary and alternative medicine research: a National
Cancer Institute perspective. Semin Oncol 2002;29(6):546e51.
[11] Patterson RE, Neuhouser ML, Hedderson MM, Schwartz SM,
Standish LJ, Bowen DJ, et al. Types of alternative medicine used by
breast, colon, and prostate cancer patients: predictors, motives and costs.
J Altern Complement Med 2002;8(4):477e85.
[12] Ries LAG, Melbert D, Krapcho M, Mariotto A, Miller BA, Feuer EJ,
et al., editors. SEER cancer statistics review, 1975e2004. Bethesda,
MD: National Cancer Institute. http://seer.cancer.gov/csr/1975_2004/,
based on November 2006 SEER data submission, posted to the SEER
web site, 2007.
[13] Sorensen TI, Nielsen GG, Andersen PK, Teasdale TW. Genetic and en-
vironmental influences on premature death in adult adoptees. N Engl J
Med 1988;318(12):727e32.
[14] Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J,
Koskenvuo M, et al. Environmental and heritable factors in the causation
of cancer e analysis of cohorts of twins from Sweden, Denmark and Fin-
land. N Engl J Med 2000;343(2):78e85.
[15] Hoover RN. Cancer e nature, nurture or both. N Engl J Med
2000;343(2):135e6.
[16] Hemminki K, Li X. Cancer risks in second-generation immigrants to
Sweden. Int J Cancer 2002;99(2):229e37.
[17] Ziegler RG, Hoover RN, Nomura A, et al. Relative weight, weight
change, height, and breast cancer risk in Asian-American women.
J Natl Cancer Inst 1996;88:650e60.
[18] Fox AJ, Collier PF. Low mortality rates in industrial cohort studies due to
selection for work and survival in the industry. Br J Prev Soc Med
1976;30:225e30.
[19] Rothman N, Smith MT, Hayes RB, et al. Benzene poisoning, a risk factor
for hematologic malignancy, is associated with the NQO1 609C/T mu-
tation and rapid fractional excretion of chlorzoxazone. Cancer Res
1997;57:2839e42.
[20] Gorelik E, Landsittel D, Marrangoni A, et al. Multiplexed immunobead-
based cytokine profiling for early detection of ovarian cancer. Cancer
Epidemiol Biomarkers Prev 2005 Apr;14(4):981e7.
[21] King MC, Marks JH, Mandell JB, et al. Breast and ovarian cancer risks
due to inherited mutations in BRCA1 & BRCA2. Science
2003;302:643e6.
[22] Jemal A, Clegg LX, Ward E, et al. Annual report to the nation on the sta-
tus of cancer 1975e2001, with a special feature regarding survival.
Cancer 2004;101(1):3e27.
[23] Davis DL, Hoel D, Fox J, Lopez A. International trends in cancer mor-
tality in France, West Germany, Italy, Japan, England and Wales, and
the USA. Lancet 1990;366(8713):474e81.
[24] Blair A, Zahm SH, Pearch NE, Heneman EF, Fraumeni Jr JF. Clues to
cancer etiology from studies of farmers. Scan J Work Environ Health
1992;18(4):209e15.
[25] Hayes HM, Tarone RE, Cantor KP, Jessen CR, McCurnin DM,
Richardson RC. Case-control study of canine malignant lymphoma: pos-
itive association with dog owners’ use of 2,4-dichlorophenoxyacetic acid
herbicides. J Natl Cancer Inst 1991;83(17):1226e31.
[26] Howe HL, Wingo PA, Thun MJ, et al. Annual report to the nation on the
status of cancer 1973e1998, featuring cancers with recent increasing
trends. J Natl Cancer Inst 2001;93:824e42.
[27] Dinse GE, Umbach DM, Sasco AJ, Hoel DG, Davis DL. Unexplained in-
creases in cancer incidence in the US from 1975e94. Annu Rev Public
Health 1999;20:173e209.
[28] Devesa SS, Blot WJ, Stone BJ, et al. Recent cancer trends in the US.
J Natl Cancer Inst 1995;87:175e82.
[29] CDC. 95th percentiles for blood and urine levels of chemicals measured
in CDC’s third national report on human exposure to environmental
chemicals. Available at, http://www.cdc.gov/exposurereport/ 2007.
Accessed May 14.
[30] Living beyond cancer: finding a new balance. President’s Cancer panel
annual report, 2003e2004. Available at: http://deainfo.nci.nih.gov/
ADVISORY/pcp/pcp03-04rpt/Survivorship.pdf. Accessed May 14, 2007.
Please cite this article in press as: Davis D.L. et al., The need to develop cen
j.biopha.2007.06.006
[31] Jemal A, Clegg L, Ward E, et al. Annual report to the nation on the status
of cancer, 1975e2001, with a special feature regarding survival. Cancer.
2004. Available at http://www3.interscience.wiley.com/cgi-bin/fulltext/
108567706/PDFSTART. Accessed May 14, 2007.
[32] Environmental health. Available at: http://www.healthypeople.gov/
document/HTML/Volume1/08Environmental.htm. Accessed May 14,
2007.
[33] The Provincial Cancer Prevention and Screening Council, Canadian Can-
cer Society and Cancer Care Ontario. A call for renewed action on cancer
prevention and detection in Ontario. Report on Cancer 2020, Issue 1,
June 2006.
[34] Kessler DA. Question of intent. New York: Public Affairs; 2001.
[35] Mehlman M. Benzene: a haematopoietic and multi-organ carcinogen at
any level above zero. Eur J Oncol 2004;9(1):15e36.
[36] Kessler E, Brandt-Rauf PW. Occupational cancers of the nervous system.
Semin Occup Med 1987;2:311e4.
[37] Markowitz D, Rosner D. Deceit and denial: the deadly politics of indus-
trial pollution. New York: Milbank Memorial Fund; 2003.
[38] Peipins LA, Lewin M, Campolucci S, et al. Radiographic abnormalities
and exposure to asbestos-contaminated vermiculite in the community
of Libby, Montana, USA. Environ Health Perspect 2003;
111(14):1753e9.
[39] Schneider A, McCumber D. An air that kills: how the asbestos poisoning
of Libby, Montana uncovered a national scandal. New York: Putnam;
2004.
[40] International Agency for Research on Cancer. IARC monographs on the
evaluation of carcinogenic risks to humans. Some pharmaceutical drugs
e summary of data reported and evaluation, http://monographs.iarc.fr/
ENG/Monographs/vol66/volume66.pdf 1996.
[41] Salaries and expenses. Occupation Safety and Health Administration.
Available at: http://www.congress.gov/cgi-bin/cpquery/?&;dbname¼cp105&&r_n¼hr635.105&sel¼TOC_80167&. Accessed May 14, 2007.
[42] Report on carcinogens, 11th ed. US Department of Health and Human
Services, Public Health Service, National Toxicology Program. Available
at: http://ntp.niehs.nih.gov/index.cfm?objectid¼32BA9724eA97F1F6-
975E-7FCE50709CB4C932. Accessed May 14, 2007.
[43] International Agency for Research on Cancer. IARC monographs on the
evaluation of carcinogenic risks to humans. Available at http://monographs.
iarc.fr/ENG/Monographs/allmonos90.php.
[44] Environmental chemicals and breast cancer risk: why is there concern?
Cornell University. Available at: http://envirocancer.cornell.edu/
FactSheet/General/fs45.chemical.cfm. Accessed May 14, 2007.
[45] Banks’ green pledge earns mixed response. The equator principles.
Available at: http://www.equator-principles.com/si.shtml. Accessed
May 14, 2007.
[46] Leadership in Energy and Environmental Design (LEED), a voluntary,
consensus-based national standard for developing high-performance, sus-
tainable buildings. Available at: http://www.usgbc.org/DisplayPage.
aspx?CategoryID¼19. Accessed May 14, 2007.
[47] Health Care Without Harm is an international coalition of 431 organiza-
tions in 52 countries working to reduce the use of toxins and promote ef-
ficiency in the health care industry. Available at: http://www.noharm.org.
Accessed May 14, 2007.
[48] Four ways to find alternative products. Sustainable hospitals. Available at
http://www.sustainablehospitals.org/cgi-bin/DB_Index.cgi. Accessed
May 14, 2007.
[49] Mercury Elimination and Reduction Challenge (MERC), Mercury in the
health care sector: the cost of alternative products. November, 1996, p.
14e24 as cited at http://www.geocities.com/RainForest/Wetlands/7756/
EPP1.htm. Accessed May 14, 2007.
[50] National Toxicology Program. Report on carcinogens. 10th ed. Washing-
ton, DC: Department of Health and Human Services; 2002.
[51] Jonas H. The imperative of responsibility: in search of ethics for the tech-
nological age. Chicago, IL: University of Chicago Press; 1984. 1.
[52] Jonas H. The imperative of responsibility: in search of ethics for the tech-
nological age. Chicago, IL: University of Chicago Press; 1984. 11.
[53] Cranor CF. Toxic torts: science, law, and the possibility of justice.
Cambridge: Cambridge University Press; 2006.
ters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/

9D. L. Davis et al. / Biomedicine & Pharmacotherapy xx (2007) 1e9
ARTICLE IN PRESS
[54] Melquiot P. Jacques Chirac warns of the need to fight against environ-
mentally-linked cancers. Actualites News Environnement. Translated
by Mary Sheehan. Available at, http://www.healthandenvironment.org/
articles/homepage/1071 2007. Accessed May 14.
[55] The Provincial Cancer Prevention and Screening Council, Canadian
Cancer Society and Cancer Care Ontario. A call for renewed
action on cancer prevention and detection in Ontario. Report on
cancer 2020, Issue 1, June 2006; Strategies for the reduction and
control of environmental carcinogens in Canada: What’s happening?
What’s missing? Prepared for Cancer Care Ontario by Brian Hy-
ndman. September 28, 2005; and see http://www.cancer.ca/ccs/
Please cite this article in press as: Davis D.L. et al., The need to develop cen
j.biopha.2007.06.006
internet/standard/0, 3182, 3172_1434293210__langId-en,00.html.
Accessed May 14, 2007.
[56] See http://www.newrules.org/environment/wapbde.html and http://
www.newrules.org/environment/cachem.html. Accessed May 14, 2007.
[57] Devesa SS, Silverman DT, Young Jr JL, Pollack ES, Brown CC,
Horm JW, et al. Cancer incidence and mortality trends among whites
in the United States, 1947e48. J Natl Cancer Inst 1987;79:701e70.
[58] Chemicals associated with site-specific tumor induction in mammary
gland. National Toxicology Program. Available at: http://ntp.niehs.nih.
gov/index.cfm?objectid¼0723C503-E864-262E-EE6B8B34B6F0C5D1.
Accessed May 14, 2007.
ters for environmental oncology, Biomed Pharmacother (2007), doi:10.1016/