aacp members' offer - Acupuncture Association of Chartered ...
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.www.acupunctureinmedicine.org.uk/volindex.php 121
Papers
Stephanie L Pradydoctoral studentDepartment of HealthSciencesUniversity of York, UK
Kate Thomasprofessor(CAM research)
Lisa Esmonderesearch officer
School of HealthcareUniversity of Leeds, UK
Simon Crouchsenior research fellow
Hugh MacPhersonsenior research fellow
Department of HealthSciencesUniversity of York, UK
Correspondence:Stephanie L Prady
The natural history of back pain after arandomised controlled trial of acupuncture vsusual care – long term outcomesStephanie L Prady, Kate Thomas, Lisa Esmonde, Simon Crouch, Hugh MacPherson
AbstractIntroduction There is growing evidence about the effectiveness of acupuncture in the short term treatment
of chronic low back pain but little is known about long term outcomes. To address this question we followed
up participants of a past randomised controlled trial of acupuncture to assess outcomes after 5.5 to 7 years.
Methods A postal questionnaire assessing pain, quality of life, disability, experience with back pain and
healthcare resource use was sent to all 239 participants of the York Acupuncture for Back Pain trial.
Results Response to the survey was low at 43.9%. Pain measured by the SF-36 Bodily Pain dimension was
maintained in the acupuncture group since the last follow up 3.5 to 5 years previously. The usual care group
had improved over the intervening years and there was now no evidence of a difference between the groups
(difference -0.4 points, 95% confidence interval -10.1 to 9.7). The results were unchanged on sensitivity
analysis using multiple imputation. In both groups back pain had not completely resolved and worry about
back health was moderate. Physiotherapy and acupuncture were used at similar rates for continuing treatment.
Discussion We theorise that exposure to a short course of acupuncture speeds natural recovery from a back
pain episode, but improvements plateau after two years. Acupuncture is often accessed privately for long term
management of back pain but is rarely available within the health service. While our study methods were robust,
the low response rate means that our findings should be interpreted with caution.
KeywordsBack pain, acupuncture, long term effects, randomised controlled trial.
IntroductionBack pain affects 59% of UK adults at some point in
their lives and results in significant personal and
societal burdens.1 The precise cause of the pain is
often difficult to diagnose and may be related to
ligamentous or muscular strains and sprains,
fibromuscular problems or osteoarthritic processes.2
The natural history of back pain is not well
understood although some data indicate that it is
rarely a self limiting condition.3;4 In 1994 the
estimated cost of low back pain to a UK GP practice
of 10,000 patients was £88,000,5 and it is among the
most costly conditions studied in the UK.6
There are a range of treatment options but
research into the most effective therapy is continuing
and evidence based effectiveness guidelines for
treatment have yet to be implemented in the UK.
Acupuncture is one choice that patients are seeking
out; an estimated 1.6% of the British population
consulted an acupuncturist in 2001 and back
complaints account for more than 12% of
consultations to traditional acupuncture practitioners
in the UK.7;8 Most acupuncture consultations are in
the private sector, with only 14% of primary care
practices offering access within the National Health
Service (NHS) in 2001.9 There is a growing body of
evidence on the effectiveness of acupuncture in the
treatment of chronic low back pain; systematic
reviews have found that acupuncture may be more
effective in the short term relief of pain than sham
treatment or no treatment.10-12 However, these
conclusions are tempered by low study quality and
there are few data on long term (>3 months)
outcomes. To address this gap in the literature, the
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 121

current study sought to examine the long term effects
of acupuncture treatment.
The study was based upon a previous trial
conducted by two of us (KT and HM) and reported
elsewhere.13 Briefly, during 1999 and 2001, 241 adults
who had recently consulted their GP about low back
pain were recruited to a pragmatic trial. Participants
were randomised to either the offer of up to 10
acupuncture treatments, or usual GP care. After 12
months there was a difference of 5.6 points in favour
of acupuncture on the primary measure (SF-36 Bodily
Pain dimension) (95% Confidence Interval, -1.3 to
12.5; P=0.1). At 24 months there was an 8 point
difference (95% CI, 0.7 to 15.3; P=0.03) and at this
time point acupuncture was also found to be cost
effective.14 An intriguing finding from this trial was that
the authors found more evidence of an improvement
between the groups at 24 months than at 12.Apossible
explanation of this is that the positive effects of
acupuncture continue to accumulate over time.
The aim of the current study was to follow up
with the participants of this trial and examine whether
the difference between the groups persisted 5.5 to 7
years after randomisation. We also planned to
examine healthcare resource use and self
management techniques.
MethodsEthical approval
Approval for the project was obtained from York
Local Research Ethics Committee (06/Q1108/31)
and the North Yorkshire Alliance Research and
Development Unit.
Data collection
In July 2006, 239 of the 241 participants in the
original trial were sent a letter informing them of the
new study, together with a participant information
sheet. The two participants who had withdrawn their
informed consent from the original study were not
contacted. Potential participants whose letters were
returned undelivered were contacted by telephone
where possible to establish a new address. Two weeks
after the initial letter was mailed, a questionnaire
together with a participant information sheet was
sent to all addresses that were known or presumed
viable.
Return of the questionnaire included consent for
the questionnaire portion of the study. The contact
details of the study coordinator were made available
for participants to discuss any concerns. If participants
did not return their questionnaire within four weeks
of mailing, they were sent a second packet with a
friendly reminder letter. Finally, non-responders were
contacted by telephone in an attempt to elicit key
outcomes.
Participants who returned a completed
questionnaire or provided outcome data over the
telephone were sent a £5 retail voucher and a copy of
a specially written summary of the trial results. At that
stage participants were informed whether or not they
would be invited for a qualitative interview to talk
about their experiences, which is a parallel study
reported elsewhere.15
Primary outcome measure
In the interest of comparability, the measures and
algorithms used in this follow up were similar to
those used to collect data in the original trial.
The primary clinical outcome measure was the
Bodily Pain dimension of a developmental version of
the Mosby Short Form 36 item non-specific quality
of life questionnaire (SF-36 V1)16 adapted and
validated for the UK population.17 One of the eight
subscales, the Bodily Pain dimension, measures two
items: the amount of bodily pain experienced and
interference of the pain on activities over the previous
four weeks. Higher scores indicate better health
status, and a five point difference in before and after
scores on this dimension is considered the minimum
clinically important change (MCIC) with 10 points
indicating moderate differences.18 The Bodily Pain
dimension has proved sensitive as an overall measure
in back pain.19-21
Secondary outcome measures
The Back Pain Experience Questionnaire is an
unvalidated battery of questions including some
asked previously, such as: presence of back pain;
steps taken to control or prevent pain; worry and
feelings about acupuncture. A numerical rating scale
of the degree of worry felt about back pain was added
for this time point.22
The Oswestry Disability Index (ODI) is a
validated disease-specific measure for back or leg
pain that discriminates change.23;24 An improved 10-
item measure is now validated and recommended;25
however, participants were previously administered
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.122 www.acupunctureinmedicine.org.uk/volindex.php
Papers
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 122

the original nine-item version that was used for this
follow up. The MCIC for the ODI is considered to be
greater than 10 points.26 The remaining seven
dimensions of the SF-36 were scored,18 and data
pertaining to healthcare resource use and work status
were collected.
Statistical procedures
Data were single-entered into SPSS and the primary
outcome data double-entered. Demographic and
clinical outcome profiles were reported using mean
(continuous variables) or percentage (categorical)
differences. Between group differences for all
continuous measures were analysed using linear
regression adjusting for age and baseline score.
Categorical variables from the Back Pain Experience
Questionnaire were dichotomised and analysed using
percentage differences and Fisher’s exact test and
quoted with odds ratios. A question about degree of
worry collected on an ordinal scale was analysed
using Student’s t test. Reports of steps taken to
prevent or minimise the impact of back pain were
analysed using percentage difference.
Data were analysed on complete cases using the
intention-to-treat principle (ITT). Statistical analysis
was carried out using SPSS 14 (SPSS, Inc, Chicago,
Illinois) and R version 2.4.1. Multiple imputation
analyses were carried out using the R libraries ‘mice’
and ‘mitools’. All analyses were two tailed and the αset at 0.05. Ninety-five percent confidence intervals
were calculated for all estimates. Analysis of the
effect of missing data was carried out under the
assumption that missing data were ‘missing at
random’ (MAR) that is, missingness could be
dependent on covariates and clinical outcomes but not
on unobserved outcomes.27 Multiple imputed datasets
were calculated using the method of ‘multiple
imputation by chained equations’ (MICE) using the
default imputation methods provided by the mice
library. Regression results from the multiple
imputations were combined using mitools.
Sample size and study power
Based on pilot data, the original acupuncture trial
was powered to detect a 10 point change (SD 19.3)
on the SF-36 Bodily Pain dimension with α of 0.05
and β-1 of 90%.14 Based on prior attrition of 23.9%
at 24 months, the anticipated response rate for this 5.5
to 7 year follow up was estimated at 50% of the
original study population. The power to detect
differences between groups was retrospectively
calculated from actual response rates using G*Power
for Windows.28
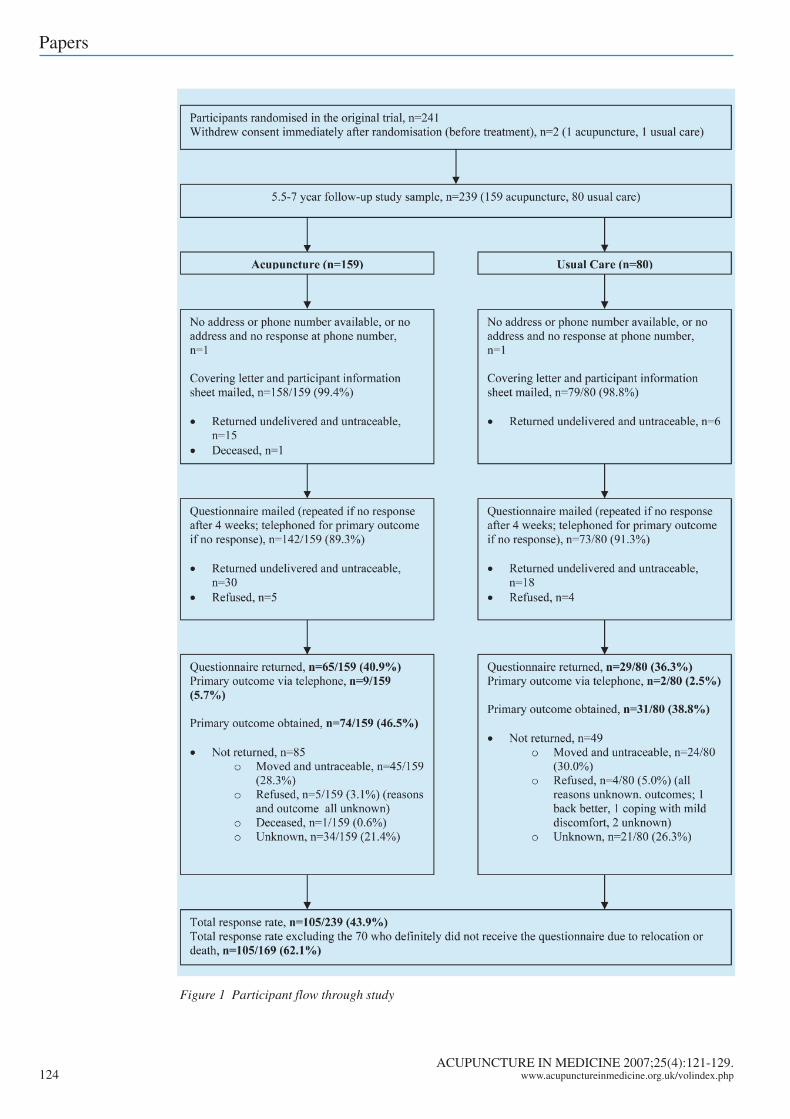
ResultsFlow of participants through the study
At this time point of up to seven years post-
randomisation, we achieved an overall response rate
of 43.9% (105/239) (Figure 1). However, excluding
the 70 people who definitely did not receive the
questionnaire (ie envelopes returned ‘addressee
unknown’ and known deceased), the response rate
was 62.1% (105/169). We feel that this is an
acceptable rate of return given that we did not attempt
to contact or locate respondents in the intervening
years. Similar rates of response were observed in
both randomisation groups. Upon telephone contact,
12 people volunteered the reason why they did not
complete the questionnaire: forgot or had no time
(n=5); pain gone/changed and didn’t think their input
would be relevant (n=2); questionnaire too long
(n=2); done enough for this study already (n=2);
didn’t want to be reminded of current pain (n=1).
Eleven of the 12 volunteered primary outcome data
over the telephone.
Characteristics of respondents and non-
respondents
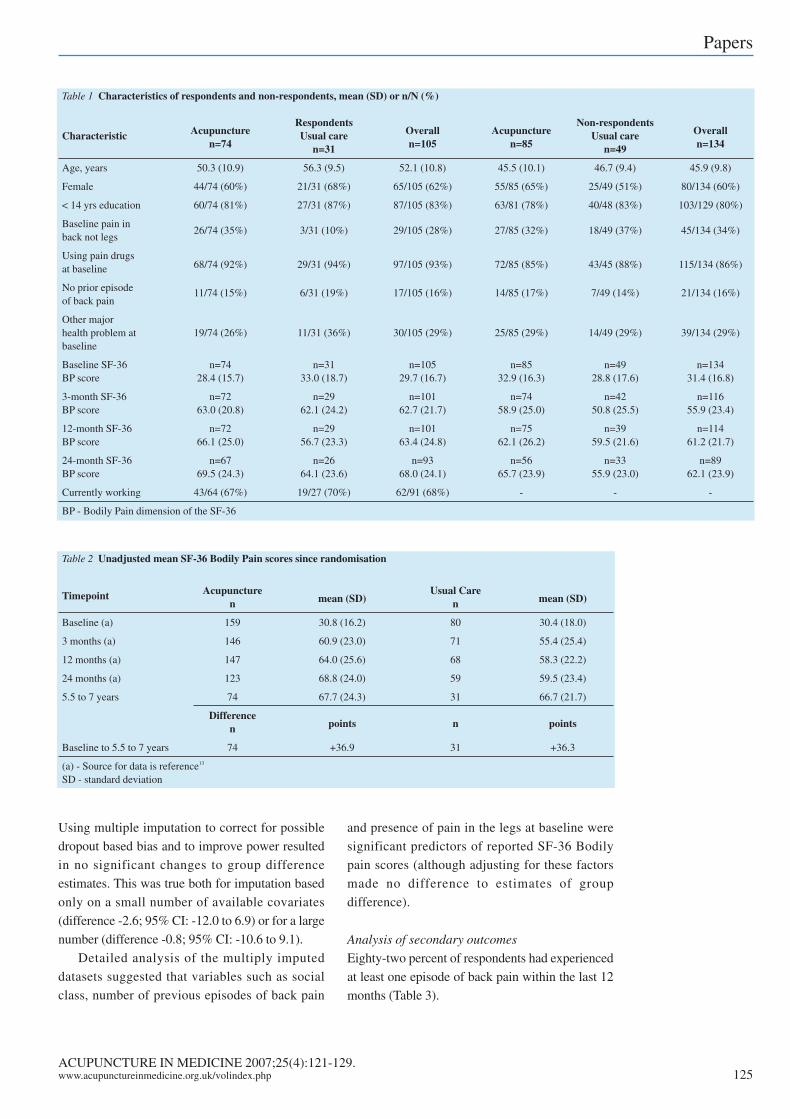
The characteristics of respondents and non-
respondents are shown in Table 1. Respondents
appeared to be older than non-respondents, and usual
care respondents older than respondents in the
acupuncture group. Respondents may have reported
less pain at the 3-month data collection point than
non-respondents but otherwise characteristics
between groups appeared similar.
Analysis of the primary outcome
All 105 respondents completed the two questions
on the SF-36 that made up the primary outcome. The
primary indication was that both groups had retained
improvements in their pain since randomisation
(Table 2).
The adjusted mean score difference at this time
point was -0.4 points (95% CI, -10.1 to 9.7, P=0.9).
This result should be interpreted with caution as post
hoc calculations indicated the study was only
powered at 64%.
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.www.acupunctureinmedicine.org.uk/volindex.php 123
Papers
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 123
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.124 www.acupunctureinmedicine.org.uk/volindex.php
Papers
Figure 1 Participant flow through study
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 124
Using multiple imputation to correct for possible
dropout based bias and to improve power resulted
in no significant changes to group difference
estimates. This was true both for imputation based
only on a small number of available covariates
(difference -2.6; 95% CI: -12.0 to 6.9) or for a large
number (difference -0.8; 95% CI: -10.6 to 9.1).
Detailed analysis of the multiply imputed
datasets suggested that variables such as social
class, number of previous episodes of back pain
and presence of pain in the legs at baseline were
significant predictors of reported SF-36 Bodily
pain scores (although adjusting for these factors
made no difference to estimates of group
difference).
Analysis of secondary outcomes
Eighty-two percent of respondents had experienced
at least one episode of back pain within the last 12
months (Table 3).
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.www.acupunctureinmedicine.org.uk/volindex.php 125
Papers
Table 1 Characteristics of respondents and non-respondents, mean (SD) or n/N (%)
Respondents Non-respondentsCharacteristic Acupuncture Usual care Overall Acupuncture Usual care Overall
n=74 n=31 n=105 n=85 n=49 n=134
Age, years 50.3 (10.9) 56.3 (9.5) 52.1 (10.8) 45.5 (10.1) 46.7 (9.4) 45.9 (9.8)
Female 44/74 (60%) 21/31 (68%) 65/105 (62%) 55/85 (65%) 25/49 (51%) 80/134 (60%)
< 14 yrs education 60/74 (81%) 27/31 (87%) 87/105 (83%) 63/81 (78%) 40/48 (83%) 103/129 (80%)
Baseline pain in26/74 (35%) 3/31 (10%) 29/105 (28%) 27/85 (32%) 18/49 (37%) 45/134 (34%)
back not legs
Using pain drugs68/74 (92%) 29/31 (94%) 97/105 (93%) 72/85 (85%) 43/45 (88%) 115/134 (86%)at baseline
No prior episode 11/74 (15%) 6/31 (19%) 17/105 (16%) 14/85 (17%) 7/49 (14%) 21/134 (16%)of back pain
Other majorhealth problem at 19/74 (26%) 11/31 (36%) 30/105 (29%) 25/85 (29%) 14/49 (29%) 39/134 (29%)baseline
Baseline SF-36 n=74 n=31 n=105 n=85 n=49 n=134BP score 28.4 (15.7) 33.0 (18.7) 29.7 (16.7) 32.9 (16.3) 28.8 (17.6) 31.4 (16.8)
3-month SF-36 n=72 n=29 n=101 n=74 n=42 n=116BP score 63.0 (20.8) 62.1 (24.2) 62.7 (21.7) 58.9 (25.0) 50.8 (25.5) 55.9 (23.4)
12-month SF-36 n=72 n=29 n=101 n=75 n=39 n=114BP score 66.1 (25.0) 56.7 (23.3) 63.4 (24.8) 62.1 (26.2) 59.5 (21.6) 61.2 (21.7)
24-month SF-36 n=67 n=26 n=93 n=56 n=33 n=89BP score 69.5 (24.3) 64.1 (23.6) 68.0 (24.1) 65.7 (23.9) 55.9 (23.0) 62.1 (23.9)
Currently working 43/64 (67%) 19/27 (70%) 62/91 (68%) - - -
BP - Bodily Pain dimension of the SF-36
Table 2 Unadjusted mean SF-36 Bodily Pain scores since randomisation
Timepoint Acupuncture Usual Caren mean (SD) n mean (SD)
Baseline (a) 159 30.8 (16.2) 80 30.4 (18.0)
3 months (a) 146 60.9 (23.0) 71 55.4 (25.4)
12 months (a) 147 64.0 (25.6) 68 58.3 (22.2)
24 months (a) 123 68.8 (24.0) 59 59.5 (23.4)
5.5 to 7 years 74 67.7 (24.3) 31 66.7 (21.7)
Differencen points n points
Baseline to 5.5 to 7 years 74 +36.9 31 +36.3
(a) - Source for data is reference13
SD - standard deviation
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 125
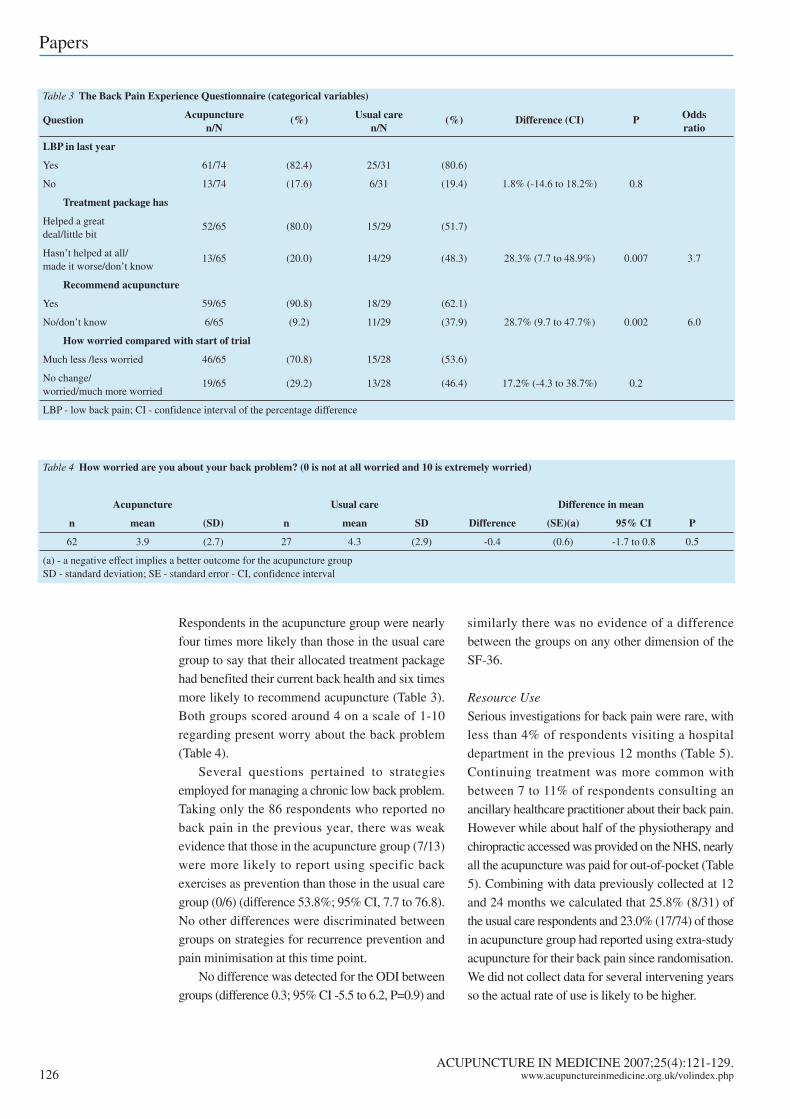
Respondents in the acupuncture group were nearly
four times more likely than those in the usual care
group to say that their allocated treatment package
had benefited their current back health and six times
more likely to recommend acupuncture (Table 3).
Both groups scored around 4 on a scale of 1-10
regarding present worry about the back problem
(Table 4).
Several questions pertained to strategies
employed for managing a chronic low back problem.
Taking only the 86 respondents who reported no
back pain in the previous year, there was weak
evidence that those in the acupuncture group (7/13)
were more likely to report using specific back
exercises as prevention than those in the usual care
group (0/6) (difference 53.8%; 95% CI, 7.7 to 76.8).
No other differences were discriminated between
groups on strategies for recurrence prevention and
pain minimisation at this time point.
No difference was detected for the ODI between
groups (difference 0.3; 95% CI -5.5 to 6.2, P=0.9) and
similarly there was no evidence of a difference
between the groups on any other dimension of the
SF-36.
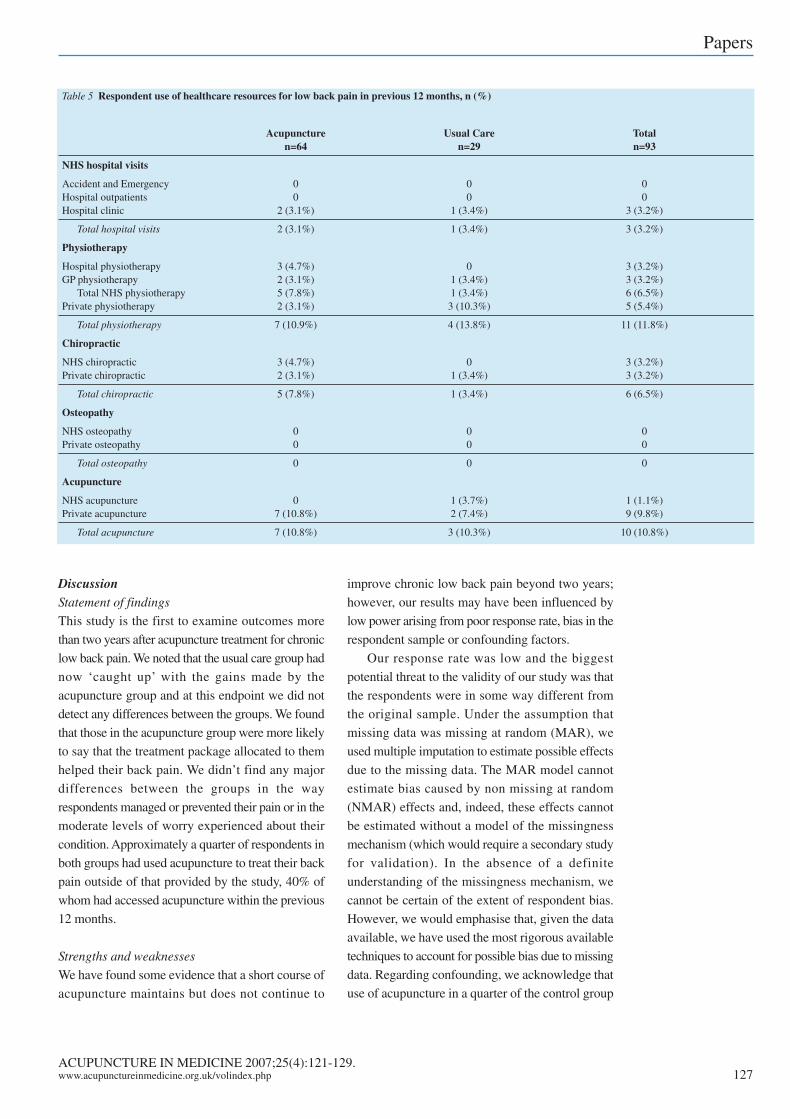
Resource Use
Serious investigations for back pain were rare, with
less than 4% of respondents visiting a hospital
department in the previous 12 months (Table 5).
Continuing treatment was more common with
between 7 to 11% of respondents consulting an
ancillary healthcare practitioner about their back pain.
However while about half of the physiotherapy and
chiropractic accessed was provided on the NHS, nearly
all the acupuncture was paid for out-of-pocket (Table
5). Combining with data previously collected at 12
and 24 months we calculated that 25.8% (8/31) of
the usual care respondents and 23.0% (17/74) of those
in acupuncture group had reported using extra-study
acupuncture for their back pain since randomisation.
We did not collect data for several intervening years
so the actual rate of use is likely to be higher.
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.126 www.acupunctureinmedicine.org.uk/volindex.php
Papers
Table 3 The Back Pain Experience Questionnaire (categorical variables)
Question Acupuncture (%) Usual care (%) Difference (CI) P Oddsn/N n/N ratio
LBP in last year
Yes 61/74 (82.4) 25/31 (80.6)
No 13/74 (17.6) 6/31 (19.4) 1.8% (-14.6 to 18.2%) 0.8
Treatment package has
Helped a great 52/65 (80.0) 15/29 (51.7)deal/little bit
Hasn’t helped at all/ 13/65 (20.0) 14/29 (48.3) 28.3% (7.7 to 48.9%) 0.007 3.7made it worse/don’t know
Recommend acupuncture
Yes 59/65 (90.8) 18/29 (62.1)
No/don’t know 6/65 (9.2) 11/29 (37.9) 28.7% (9.7 to 47.7%) 0.002 6.0
How worried compared with start of trial
Much less /less worried 46/65 (70.8) 15/28 (53.6)
No change/ 19/65 (29.2) 13/28 (46.4) 17.2% (-4.3 to 38.7%) 0.2worried/much more worried
LBP - low back pain; CI - confidence interval of the percentage difference
Table 4 How worried are you about your back problem? (0 is not at all worried and 10 is extremely worried)
Acupuncture Usual care Difference in mean
n mean (SD) n mean SD Difference (SE)(a) 95% CI P
62 3.9 (2.7) 27 4.3 (2.9) -0.4 (0.6) -1.7 to 0.8 0.5
(a) - a negative effect implies a better outcome for the acupuncture groupSD - standard deviation; SE - standard error - CI, confidence interval
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 126
DiscussionStatement of findings
This study is the first to examine outcomes more
than two years after acupuncture treatment for chronic
low back pain. We noted that the usual care group had
now ‘caught up’ with the gains made by the
acupuncture group and at this endpoint we did not
detect any differences between the groups. We found
that those in the acupuncture group were more likely
to say that the treatment package allocated to them
helped their back pain. We didn’t find any major
differences between the groups in the way
respondents managed or prevented their pain or in the
moderate levels of worry experienced about their
condition. Approximately a quarter of respondents in
both groups had used acupuncture to treat their back
pain outside of that provided by the study, 40% of
whom had accessed acupuncture within the previous
12 months.
Strengths and weaknesses
We have found some evidence that a short course of
acupuncture maintains but does not continue to
improve chronic low back pain beyond two years;
however, our results may have been influenced by
low power arising from poor response rate, bias in the
respondent sample or confounding factors.
Our response rate was low and the biggest
potential threat to the validity of our study was that
the respondents were in some way different from
the original sample. Under the assumption that
missing data was missing at random (MAR), we
used multiple imputation to estimate possible effects
due to the missing data. The MAR model cannot
estimate bias caused by non missing at random
(NMAR) effects and, indeed, these effects cannot
be estimated without a model of the missingness
mechanism (which would require a secondary study
for validation). In the absence of a definite
understanding of the missingness mechanism, we
cannot be certain of the extent of respondent bias.
However, we would emphasise that, given the data
available, we have used the most rigorous available
techniques to account for possible bias due to missing
data. Regarding confounding, we acknowledge that
use of acupuncture in a quarter of the control group
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.www.acupunctureinmedicine.org.uk/volindex.php 127
Papers
Table 5 Respondent use of healthcare resources for low back pain in previous 12 months, n (%)
Acupuncture Usual Care Totaln=64 n=29 n=93
NHS hospital visits
Accident and Emergency 0 0 0Hospital outpatients 0 0 0Hospital clinic 2 (3.1%) 1 (3.4%) 3 (3.2%)
Total hospital visits 2 (3.1%) 1 (3.4%) 3 (3.2%)
Physiotherapy
Hospital physiotherapy 3 (4.7%) 0 3 (3.2%)GP physiotherapy 2 (3.1%) 1 (3.4%) 3 (3.2%)
Total NHS physiotherapy 5 (7.8%) 1 (3.4%) 6 (6.5%)Private physiotherapy 2 (3.1%) 3 (10.3%) 5 (5.4%)
Total physiotherapy 7 (10.9%) 4 (13.8%) 11 (11.8%)
Chiropractic
NHS chiropractic 3 (4.7%) 0 3 (3.2%)Private chiropractic 2 (3.1%) 1 (3.4%) 3 (3.2%)
Total chiropractic 5 (7.8%) 1 (3.4%) 6 (6.5%)
Osteopathy
NHS osteopathy 0 0 0Private osteopathy 0 0 0
Total osteopathy 0 0 0
Acupuncture
NHS acupuncture 0 1 (3.7%) 1 (1.1%)Private acupuncture 7 (10.8%) 2 (7.4%) 9 (9.8%)
Total acupuncture 7 (10.8%) 3 (10.3%) 10 (10.8%)
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 127

respondents, along with other potential confounders,
may have obscured any between group differences.
Meaning of our results
The data we have collected adds to the literature on
the natural history of low back pain. At some point
between two to five years after randomisation the
usual care group have improved to the gains seen at
two years in the acupuncture group. We theorise that
exposure to acupuncture speeds recovery from a back
pain episode. Several years after randomisation the
respondents scored 12.2 points lower on the SF-36
Bodily Pain dimension than the age adjusted norm,29
and worry about back health was moderate. This
concurs with other data showing that severity of back
pain fluctuates, and only completely resolves in 10-
31% of cases.3;4;30 A proportion of respondents use
acupuncture as a continuing treatment for their back
pain, the majority of whom pay for it privately. A
concurrent qualitative exploration found that some
of the respondents felt the cost of private acupuncture
treatment was prohibitive, although many believed
acupuncture had been helpful or even pivotal in the
treatment of their pain.15
Unanswered questions and future research
This study raises several interesting questions to be
addressed by future research. We theorise that
acupuncture helped participants to achieve and
maintain a level of pain relief more quickly. However,
we found relatively high utilisation of extra-study
acupuncture in both arms of our trial. Has this extra
acupuncture allowed the usual care group to catch up,
or was the passage of time or other factors responsible?
Our results highlight the question of whether
acupuncture offered as a short course over three months
is an appropriate design for research into a chronic
condition. We recommend that further trials allow
participants to access treatments after an initial course
at ‘point of need’ over a year or more, a design that
may more accurately reflect the actual pattern of use
among back pain patients. Examining the effect of an
intervention over a longer time period will enable long
term treatment strategies to be developed and
compared, an especially important consideration for
chronically fluctuating conditions such as back pain.
Second, we found that social class, area of pain and
chronicity of the condition emerged as predictors of SF-
36 Bodily Pain scores and these factors should be
explored in subsequent research. Third, we found there
was less NHS-provided acupuncture for back pain
than physiotherapy for our respondent sample. We
think the issue of access merits consideration given
the evidence for effectiveness and cost effectiveness for
acupuncture in the short and medium term.13;14;31;32
Finally, more long term studies on acupuncture for
back pain are needed to refute or validate this study’s
findings. To prevent low response rates and plan for an
adequate sample size, planning for long term follow up
should be built into trials at the design stage.
Conflicts of interest
None declared.
Sources of support
The project was supported by a research grant from
BackCare.
AcknowledgementsWe would like to thank all the participants of the
YACBAC trial for contributing to this study.
Reference list1. Dunn KM, Croft PR. Epidemiology and natural history of
low back pain. Eura Medicophys 2004;40(1):9-13.2. Beers MH, Berkow R. The Merck Manual of Diagnosis and
Therapy Section 5. Musculoskeletal And Connective TissueDisorders, Chapter 59. Nonarticular Rheumatism: Low backpain. 2006, 17th Edition.; Available at:http://www.merck.com/mrkshared/mmanual/sections.jsp.(Accessed 13 Sept 2006.).
3. Hestbaek L, Leboeuf-Yde C, Engberg M, Lauritzen T, BruunNH, Manniche C. The course of low back pain in a generalpopulation. Results from a 5-year prospective study.J Manipulative Physiol Ther 2003;26(4):213-9.
4. Von Korff M, Deyo RA, Cherkin D, Barlow W. Back pain inprimary care. Outcomes at 1 year. Spine 1993;18(7):855-862.
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.128 www.acupunctureinmedicine.org.uk/volindex.php
Papers
Summary points
There is some evidence for the effectiveness and costeffectiveness of acupuncture in the short term treatment ofpersistent low back pain
No studies have involved more than two years’ follow up
Up to seven years after an RCT comparing acupuncturewith usual care, we found no differences between thegroups (but the response rate was low)
About a quarter of patients from both groups chose to useacupuncture outside the study, usually paying for it
Trials of acupuncture for back pain should have extendedtreatment and follow up
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 128
5. Clinical Standards Advisory Group. Back Pain. Report of aCSAG committee on back pain. 1994 London: HMSO.
6. Maniadakis N, Gray A. The economic burden of back painin the UK. Pain 2000;84(1):95-103.
7. Thomas K, Coleman P. Use of complementary or alternativemedicine in a general population in Great Britain. Resultsfrom the National Omnibus survey. J Public Health (Oxf)2004;26(2):152-7.
8. MacPherson H, Sinclair-Lian N, Thomas K. Patients seekingcare from acupuncture practitioners in the UK: a nationalsurvey. Complement Ther Med 2006;14(1):20-30.
9. Thomas KJ, Coleman P, Nicholl JP. Trends in access tocomplementary or alternative medicines via primary carein England: 1995-2001 results from a follow up nationalsurvey. Fam Pract 2003;20(5):575-7.
10. Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: acupuncture for low back pain. Ann Intern Med2005;142(8):651-63.
11. Furlan AD, van Tulder MW, Cherkin DC, Tsukayama H,Lao L, Koes BW, et al. Acupuncture and dry-needling forlow back pain. Cochrane Database Syst Rev 2005, (1)CD001351.
12. van Tulder MW, Furlan AD, Gagnier JJ. Complementaryand alternative therapies for low back pain. Best Pract ResClin Rheumatol 2005;19(4):639-54.
13. Thomas KJ, MacPherson H, Thorpe L, Brazier J, Fitter M,Campbell MJ, et al. Randomised controlled trial of a shortcourse of traditional acupuncture compared with usual carefor persistent non-specific low back pain. BMJ2006;333(7569):623.
14. Ratcliffe J, Thomas KJ, MacPherson H, Brazier J.A randomised controlled trial of acupuncture care forpersistent low back pain: cost effectiveness analysis. BMJ2006;333(7569):626.
15. Esmond LE, Thomas K, Prady SL, MacPherson H. Patientexperiences of longer term effects of acupuncture for chronicpersistent low back pain. In preparation.
16. Ware JE,Jr, Sherbourne CD. The MOS 36-item short-formhealth survey (SF-36). I. Conceptual framework and itemselection. Med Care 1992;30(6):473-83.
17. Brazier JE, Harper R, Jones NM, O’Cathain A, Thomas KJ,Usherwood T, et al. Validating the SF-36 health surveyquestionnaire: new outcome measure for primary care. BMJ1992;305(6846):160-4.
18. Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 HealthSurvey. Manual and interpretation guide. Boston: MedicalOutcomes Trust; The Health Institute; 1993.
19. Gilbert FJ, Grant AM, Gillan MG, Vale LD, Campbell MK,Scott NW, et al. Low back pain: influence of early MRimaging or CT on treatment and outcome – multicenterrandomized trial. Radiology 2004;231(2):343-51.
20. Patrick DL, Deyo RA, Atlas SJ, Singer DE,Chapin A,Keller,RB. Assessing health-related quality of life in patients withsciatica. Spine 1995;20(17):1899-908.
21. Walsh TL, Hanscom B, Lurie JD, Weinstein JN. Is acondition-specific instrument for patients with low backpain/leg symptoms really necessary? The responsivenessof the Oswestry Disability Index, MODEMS, and the SF-36.Spine 2003;28(6):607-15.
22. Moore JE, Von Korff M, Cherkin D, Saunders K, Lorig K.A randomized trial of a cognitive-behavioral program forenhancing back pain self care in a primary care setting. Pain2000;88(2):145-53.
23. Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestrylow back pain disability questionnaire. Physiotherapy1980;66(8):271-3.
24. Taylor SJ, Taylor AE, Foy MA, Fogg AJ, et al.Responsiveness of common outcome measures for patientswith low back pain. Spine 1999;24(17):1805-12.
25. Roland M, Fairbank J. The Roland-Morris DisabilityQuestionnaire and the Oswestry Disability Questionnaire.Spine 2000;25(24):3115-24.
26. Ostelo RW, de Vet HC. Clinically important outcomes inlow back pain. Best Pract Res Clin Rheumatol2005.19(4):593-607.
27. Little RJA, Rubin DB. Statistical analysis with missing data.2nd ed. New York: John Wiley & Sons, Inc.; 2002.
28. Erdfelder E, Faul F, Buchner A. GPOWER: A general poweranalysis program. Behavior Research Methods, Instruments,& Computers 1996;28(1):1-11.
29. Jenkinson C, Coulter A, Wright L. Short form 36 (SF36)health survey questionnaire: normative data for adults ofworking age. BMJ 1993;306(6890):1437-40.
30. Hestbaek L, Leboeuf-Yde C, Manniche C. Low back pain:what is the long term course? A review of studies of generalpatient populations. Eur Spine J 2003;12(2):149-65.
31. Brinkhaus B, Witt CM, Jena S, Linde K, Streng A,Wagenpfeil S, et al. Acupuncture in patients with chroniclow back pain: a randomized controlled trial. Arch InternMed 2006;166(4):450-7.
32. Witt CM, Jena S, Selim D, Brinkhaus B, Reinhold T, WruckK, et al. Pragmatic randomized trial evaluating the clinicaland economic effectiveness of acupuncture for chronic lowback pain. Am J Epidemiol 2006;164(5):487-96.
ACUPUNCTURE IN MEDICINE 2007;25(4):121-129.www.acupunctureinmedicine.org.uk/volindex.php 129
Papers
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 129
Copyright © 2022 FDOKUMEN