
aacp members' offer - Acupuncture Association of Chartered ...
120
Freephone 0800 072 0202 www.balancehealthcare.com www.balancehealthcare.com Dedicated to providing an unrivalled service, Balance Healthcare partners with leading global practitioners, like GIOVANNI MACIOCIA, to supply high quality products, price commitment, product support and education. Expertise | Education | Service AACP MEMBERS’ OFFER * for orders placed in August & September Please quote AACP 01 when ordering * Buy 2 packs and get 3rd pack FREE! (of the same product) for orders placed in August and September 2008 Your perfect partner High quality Acupuncture, TCM and Phytotherapy products for professional practitioners and students SPECIAL NEEDLE PACKS OFFER Across the Balance Healthcare needles range. Including: Seirin, Carbo, Jia Chen, Natural and Sharp. Stock up now and let BALANCE HEALTHCARE help point you in the right direction Balance Healthcare
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of aacp members' offer - Acupuncture Association of Chartered ...

Freephone 0800 072 0202www.balancehealthcare.comwww.balancehealthcare.com
Dedicated to providing an unrivalled service,Balance Healthcarepartners with leading globalpractitioners, like GIOVANNIMACIOCIA, to supply high qualityproducts, price commitment,product support and education.
Expertise | Education | Service
AACP MEMBERS’ OFFER*
for orders placed in August & September
Please quote AACP 01when ordering
*Buy 2 packs and get 3rd pack FREE!
(of the same product)
for orders placed in August and September 2008
Your perfect partner
High quality Acupuncture,TCM and Phytotherapy
products for professionalpractitioners and students
SPECIAL NEEDLE PACKS
OFFERAcross the Balance Healthcare needles range. Including:
Seirin, Carbo, Jia Chen,Natural and Sharp.
Stock up now and let BALANCE HEALTHCAREhelp point you in the right direction
Balance Healthcare

HEGU P-type• Lightweight with longer, thicker plastic handles which make them
easier to manipulate. • Colour-coded handles make it easy to identify dimension.• High-precision nail head.• Micro-polished, DDS-plated for painless insertion.• 5 Years Sterility
Also available
HEGU XenoHEGU Xeno is a needle of the highest quality. • Japanese needle type.• Non-pyrogenic and non-toxic.• Spiral handle of surgical stainless steel for optimum grip.• Manufactured of surgical stainless spring steel, from Sweden.• Best electrical conductivity properties for electroacupuncture.
Barrier Healthcare are promoting the HEGU Svenska AB range of needles. HEGUhave been manufacturing sterile single-use acupuncture needles under its ownbrand at its plants in China and South Korea for over a decade. The needles aremanufactured in accordance with market specifications and adhere to the CE Mark (Europe), FDA (US) and the Swedish Medical Products Agency instructions and regulations.
HEGU family of needles

ContentsAutumn 2008
Editorial .........................................................5Chair report ...................................................7Business Manager report .............................11Finance and Secretariat report .....................13Webmaster report ........................................15Political Liaison Officer report ....................19Clinical Interest Group Liaison Officerreport ...........................................................21Education, Training and ResearchCommittee report ........................................23IAAPT Representative report ......................25Conference Coordinator report ...................27Regional reports ..........................................29Regional representatives ..............................35
Literature reviews
Acupuncture and its use in the managementof low back and pelvic girdle pain inpregnancy by Wendy Koch ..............................37Acupuncture in cardiology by Val Hopwood .49
Case reports
Treatment of cervical and posterior shoulderpain in a 57-year-old female with conventionalphysiotherapy and Western acupuncture by
Lotte Skjodt ...................................................53Acupuncture for the induction of labour by
Roseanne McEwan ..........................................61
AACP Annual Conference, 16–18 May 2008:The Five Principles .....................................69AACP Limited . . . the next 5 years ............83AACP clinical web audit .............................91Statutory regulation of practitioners ............97Book reviews ............................................. 101Letters ....................................................... 109News from the front ................................. 113Guidelines for authors ............................... 117
� 2008 Acupuncture Association of Chartered Physiotherapists 3


Editorial
Welcome to the Autumn 2008 Journal of the
Acupuncture Association of Chartered Physiotherapists.I hope that you have all had a wonderful summerand are feeling energized after your holidays.
I want to bid farewell to one Journal editor andwelcome another. This edition is the last that DrPennie Roberts will work on as acting ClinicalEditor. I can only second the following com-ments from the Chair, Jennie Longbotton: ‘‘Wewould sincerely like to thank Pennie for theextensive services that she has offered to theAACP over the past 2 years in her roles asClinical Editor of the Journal, and as a memberof both the AACP Board and the Education,Training and Research Committee. Her adviceand experience has been invaluable, and shewill be greatly missed.’’ It has been a pleasureworking with her.
While we wish Pennie all the best, I do hopethat she will grace these pages again with herpresence. After all, her predecessor, AndrewBannan, is still contributing conference reportsto the Journal (see pp. 69–72).
Pennie is handing the reins over to MajorSherin Roffey, who has contributed a letter tothis issue (see pp. 110–111). Sherin studiedphysiotherapy as a mature student at the WestYorkshire College of Health Studies (formerlyPinderfields School of Physiotherapy) and quali-fied as a chartered physiotherapist in 1997,gaining a BHSc(Hons) that was awarded by theUniversity of Leeds.
She joined the British Army upon qualifyingand completed junior rotations at the RoyalHospital Haslar, Gosport, Hampshire, in ortho-paedics, respiratory care, neurology and rehabili-tation (including hydrotherapy). In 1999, shewas posted to Plymouth and continued to gainrespiratory care experience at the Ministry ofDefence Hospital Unit at Derriford Hospital inthe Intensive Therapy Unit (ITU), the HighDependency Unit, and on the surgical and medi-cal wards, while furthering her musculoskeletalexperience at the Physiotherapy Department atHMS Drake (now the Regional RehabilitationUnit – HMS Drake). In the latter part of 1999,she deployed to Bosnia and Croatia in a stand-alone post covering the ITU, ward and physio-therapy outpatient department of a British field
� 2008 Acupuncture Association of Chartered Physiotherapists 5

hospital, treating international service personneland the indigenous population.
In 2000, Sherin was posted to the Duchess ofKent Military Hospital (now the Duchess ofKent Barracks) at Catterick Garrison, where shecompleted over 4 years in the PhysiotherapyOutpatient Department, including a small case-load of ward-based patients. During this time,she undertook a 9-month rotation at the Sportsand Training Injuries Centre (now the RegionalRehabilitation Unit – Catterick) and also com-pleted parts A–C of the Society of OrthopaedicMedicine courses. She began an MSc in Sportsand Exercise Injury Management in 2001, whichincluded an acupuncture foundation module,although she was forced to delay her dissertationfor one year because of deployment to Iraq in2003 during the initial phase of the war, whereshe was part of the furthest-forward 200-beddedfield hospital. Her role was that of senior in-patient physiotherapist, and she was responsiblefor the musculoskeletal and respiratory care ofinjured British troops and hostile combatants;however, during the later stages of hostilities, shewas also able to carry a small caseload of primarycare outpatients.
Sherin was posted to the Army TrainingRegiment at Winchester in 2004 as Officer inCommand of the Primary Care RehabilitationFacility, a position that consisted of a largermanagement role since she was the most seniormilitary medical personality within the regiment.She completed her MSc whilst in this post.
In 2006, she was posted to the Army PrimaryHealth Care Headquarters, Eastern Region(Colchester to Nottingham), as the RegionalClinical Governance coordinator, and there de-veloped her interest and experience in clinicalaudit. In this post, she was responsible for thedevelopment of clinical governance within 10Army medical centres, two medical receptionstations, one department of community mentalhealth and the Regional Rehabilitation Unit –Colchester. Whilst in this post, she maintained
her professional registration requirements bycarrying a small caseload, participating in regionalin-service training and completing an acupunc-ture course that involved the production of aclinically reasoned case study.
Sherin has a special interest in continuingprofessional development and teaching, and wasresponsible for the regional physiotherapy in-service training programme at Catterick for over2 years (involving approximately seven primarycare and rehabilitation departments), which in-cluded teaching clinical and academic subjects.Whilst at Colchester, she chaired the regionalclinical governance meetings, which includedteaching clinical audit, clinical risk manage-ment, promoting evidence-based practice andother aspects of clinical governance, such aspatient satisfaction and patient confidentiality(Caldicott).
Throughout her career, she has undertakenvarious short courses, including ‘‘Nags andSnags’’, hydrotherapy, respiratory ‘‘top-up’’,neurology and normal movement, taping andstrapping, biomechanics, ‘‘Get on the Ball’’, an-terior knee pain management, and acupuncture.
Sherin was posted to the Regional Rehabilita-tion Unit at Aldershot in late May 2008, whereshe will undertake a caseload of primary care andrehabilitation patients, be responsible for re-gional multidisciplinary assessment clinics (ArmyPrimary Healthcare Services, Southern Region),and further develop her role and interest inclinical governance and clinical audit. Duringthis posting, she plans to undertake a literaturereview focusing on acupuncture and women’shealth, and an acupuncture-based researchproject.
In her spare time, Sherin writes short stories,mainly in the crime genre. In the longer term, sheplans to undertake a further MSc – this time inacupuncture.
Andrew J. Wilson
Corporate Editor
Editorial
� 2008 Acupuncture Association of Chartered Physiotherapists6

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 7–9
Chair report
Once again, thanks to the hard work of theJournal Committee, this is a very full edition ofthe Journal. Rather than repeating too many ofthe facts, I will let you see for yourselves that thisissue offers detailed coverage of:+ Conference 2008 (pp. 69–81);+ the AACP 5-year plan (pp. 83–90); and+ the Association’s clinical web audit (pp.
91–96).These topics are all covered by extensive
reports, so I merely want to thank all thoseinvolved in the organization and delivery ofConference for their hard work and commit-ment. Special thanks go to Suzanne Charboneau,our Marketing Manager, for her impressive workin increasing the trade attendance by 50% thisyear, a difficult achievement in the current econ-omic and health climate. My sincere thanksalso go to the trade: without their support, wecould not organize such a successful event withsuch important speakers and subjects. The 2009Conference is already booked and speakers havebeen approached. If you feel that you would liketo be part of its future, please come forward andspeak with Sharon at the office. We welcomeyou!
Here is a question to be discussed on theJournal letter page:
Does the membership want two smaller conferences a
year, or a number of one-day clinical workshops
distributed around the country?
AACP top-up courses
My sincere thanks go to the following tutors,who have put the membership before their owninterests. Provision of the top-up courses chal-lenged both the Office staff, who organizedthem, and even more so, the tutors, who pro-vided them throughout the country. The tutorshave contributed their valuable time and effort toaccommodate the needs of lapsed or forgetfulmembers. My thanks go to:+ Dr Panos Barlas;+ Kam Mah Wak;
+ Lesley Pattenden;+ Adrian Yeoman;+ Jill Drew; and+ Jennifer Michie.
The top-up courses are now complete,although this seems to have come as a surprise tomany lapsed AACP members and trust man-agers. Forgive me for sounding somewhat cyni-cal, but we have advertised these facts for morethan 2 years and, yes indeed, the facts are:
All applicants for AACP membership from 1 April
2008 will be required to demonstrate a minimum of
80 h accredited acupuncture training. There will be no
provision of future top-up courses.
The 40-Hour Top-Up Course audit, which willbe published in the next edition of the Journal
(Spring 2009), has revealed a number of factsconcerning previous acupuncture basic trainingthat will be used to improve the current AACP-approved foundation training. These recommen-dations will be discussed at the forthcomingtutor meeting, and implemented by our Educa-tion, Training and Research Committee.
Clinical web audit resultsThis issue of the Journal presents the preliminaryresults from the web audit that was undertaken atthe end of 2007 (pp. 91–96). Unfortunately, sinceonly 3% of our membership took the time andeffort to complete the 5-min questionnaire, thefigures and outcomes reported have little value interms of statistical significance.
A clinical, financial or structural audit is under-taken in order to access, evaluate and determinethe delivery of future services to our members.Without an audit trail, we cannot determine thatwhat we do is having the desired effect ordetrimental one. How can the AACP improve,develop, establish or change membership ser-vices when:
(1) only 3% of the membership responded;(2) only 25% of the membership log on to the
AACP web; and
� 2008 Acupuncture Association of Chartered Physiotherapists 7

(3) only 3% of the membership accesses theresearch databases?
The web audit is cheap, efficient, practical andnecessary. Please take the time to use it. It willgenerate:+ AACP research;+ individual research;+ statistics to provide support for clinical use;+ statistics that will support your argument for
acupuncture within physiotherapy;+ knowledge and understanding; and+ improved membership services.
If we do not have your input we cannot provide the
relevant output.
Provision of research databasesAs you will have seen from the excited e-mailsfrom Sharon Fox, our Business Manager, we arenow able to offer AACP members access to thefollowing full-text research databases:+ Medline;+ AMED; and+ CINAHL.
I congratulate Sharon for pursuing this untilshe had the necessary results. It is a service thatprivate practitioners, AACP members and I havebeen waiting avidly for the Chartered Society ofPhysiotherapy (CSP) to provide for the past15 years. Sharon ensured that we didn’t have towait any longer: within 2 weeks of the idea beingfloated, she had dealt with it, and the facility waslive and running on AACP web. On behalf ofthe membership, I would like to thank her forproviding us with an essential resource. I hopethat this will now facilitate informed, evidence-based debate about the facts and statistics inorder to justify the use of acupuncture withinphysiotherapy. Since I am in danger of becom-ing even more cynical, I also hope that it willserve to prevent anecdotal discussion and theexpression of uninformed opinions!
I am particularly delighted to offer this facilitysince it is something that the membership hasbeen calling for. The provision of this servicewill bring about with both positive and negativechanges. The available evidence will serve manypurposes by:+ supporting acupuncture intervention;+ supporting clinical effectiveness;
+ providing the facts;+ providing evidence to answer some of the
questions that are posed on iCSP; and+ preventing anecdotal, opinionated responses,
which have no constructive part to play inclinical reasoning.
The online AACP database now includes thefull text of Acupuncture in Medicine, the journal ofthe British Medical Acupuncture Society(BMAS). The cost of providing the printedversion of this to AACP members is £32 000this year alone. Because we now have access tothis resource online, we have discussed the costof supplying the printed version at length andtaken advice from Jim Mandeville, our FinancialDirector, reaching the decision that, financiallyand ecologically, the Association cannot con-tinue to offer this service. For many, includingmyself, this will be a loss; I like to read a hardcopy on the train, in the bath, whenever I can.Nevertheless, for the reasons cited above, AACPmembers will cease to receive the printed versionof the BMAS journal from December 2008, andthe money saved will be used to offer increasededucational facilities at lower prices whilst main-taining the present cost of AACP membershipfor the next 12 months.
AACP 5-year planThis edition of the Journal includes the AACPBoard’s 5-year plan (pp. 83–90). Considerableeffort has been spent discussing and presentingthis strategy. At the very least, it is ambitious andwill stimulate a debate with some ‘‘fire’’, and nodoubt, a degree of ‘‘wind’’!
Discussion and opinions are welcome, butplease remember, with the membership require-ments at its heart, this plan is designed to offer asmany education, research, conference and mem-bership advantages as possible within the currenteconomic and health climate.
Dr Val Hopwood presents her last report asAACP Political Liaison Officer and member ofthe Government Stakeholder Group in thisedition (pp. 19–20). You will see that Val isresigning from the post to enable an active Boardmember to take negotiations to another level.The Association would like to thank Val for theincredible service and representation that she has
Chair report
� 2008 Acupuncture Association of Chartered Physiotherapists8

given the membership throughout these negotia-tions. Without her knowledge, expertise andpolitical attitude, the AACP would not be inthe favourable position it now commands. Oursincere thanks to Val for her commitment andpolitical negotiating skills. We are now in con-stant communication with Rachel Tripp from theHealth Professions Council (HPC), and haveasked her to present the future plans for statu-tory self-regulation and the HPC at the AnnualGeneral Meeting (AGM) in May 2008.
As you know, this will be my final year asAACP Chair. I will step down to allow younger,brighter leaders to take the Association forward.With this in mind, we must use 2008–2009 to
mentor, support and develop the next Chair andBoard members. I encourage you to step forwardand help to take the AACP forward. These arecrucial years, and the strategies, plans and organi-zations are now in place to support a new leader.We have made enormous strides over the past3 years and gone far beyond my expectations.This position is both challenging and incrediblyrewarding, and an honour to perform. . .
We need people to join us this year in order to take
AACP into the next 5 years.
Jennie Longbottom
Chair
Chair report
� 2008 Acupuncture Association of Chartered Physiotherapists 9

For all your professional needs –high quality acupuncture suppliesat competitive pricesWhy shop around when you canorder everything you need fromAcupuncture Supplies Porthcawl:
Acupuncture Supplies Porthcawl, 7 Sawmill Yard, Blair Atholl, Perthshire, PH18 5TL
Tel: 01796 482 114 Fax: 01796 481 493 Email: [email protected]: www.acupuncturedirect.co.uk
Extensive range of acupuncture needles, moxa and cupping sets always in stock. We supply to Practitionersand Professionals so you are assured of the best quality goods at the best prices.
For a free catalogue, contact us on 01797 482 114 or visit www.acupuncturedirect.co.uk
NEW DVD Range – including Anatomy for Acupuncture & Sports InjuriesFREE 1 week online trial
NEWDVDRange
SpecialOffer
Seirin Needles
Tai Chi Needles
Needle Moxa
Cupping Sets
Electro-acupuncture
Clinical Devices
Diagnostic Instruments
Acupuncture Accessories
Books and Charts
Wide Range of Models
Only £7.50 per box of 100.Order and receive FREEsamples of Tai Chi needles.
647 Acup_ad_a4 ED2:Layout 1 24/5/07 12:27 Page 1

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 11–12
Business Manager report
Office activities to Autumn 2008Well, I could say what a year it’s been – even ifthat might sound a bit self-satisfied consideringthat the AACP had a fabulous 2007 – but whatthe heck, it has!
I hope that you have all found the time to visitthe AACP website because we have introducedsome great member benefits that are only acces-sible if you log on to the site. If you haven’t doneso already, you will need your Association mem-bership number, which the AACP Office will behappy to provide if you do not have it to hand.
We have also published the 5-year plan (seepp. 83–90), and those that went to the AnnualGeneral Meeting at Conference in May 2008 willhave heard our Chair, Jennie Longbottom, say afew words about Association’s future direction.The plan provides us with a vital tool to focusour efforts on the areas that will best supportexisting and future members. It is important thatthe AACP does not lose sight of why it exists: tosupport you, the members, and represent yourprofessional interests. We can only achieve this ifwe are aware and informed of the issues that willaffect you.
So, how was your summer? I hope that,wherever you are sitting reading this, you feelthat the weather was better than 2007 and you atleast managed to get some sun. It has been abusy time for the Association over the springand summer. We have had our heads downdealing with the daily workload, enquiries andissues, but I was fortunate to meet some you atthe musculoskeletal roadshow, which took placein Bristol in March 2008.
This was my first attendance at a roadshow,and I thought it was great. Although, not being apractitioner, the clinical content of the presenta-tions was rather alien to me, I still found itfascinating watching the speakers and experienc-ing their different presentation styles – they wereall so different. We will have another event at theUniversity of Cambridge in November 2008, ofcourse, so I also hope to meet more membersthere. As for 2009 events, we hope to bring
you something a little different. There will still bea musculoskeletal bias, but there will be lesscontent and more focused sessions. We really dolook at your feedback and try to bring you thetype of events that you want to see. Watch theAACP website for announcements or let us haveyour up-to-date e-mail address because we notifyour members by e-mail of course availability andother member issues that need to be communi-cated quickly.
I’ve mentioned the word a couple of timesnow and I can’t contain it any longer: Confer-ence! Wow, what a weekend! It was fantastic tobe involved in such a good event once again. Itrivalled 2007 for success and I think I can saythat we now have an enviable reputation forholding successful events. I really hope thatthose of you who attended enjoyed the weekend.As ever, the speakers were compelling, theatmosphere was relaxed and informative, and thefood and entertainment superb. I was concernedthat a rock band might be a little too run-of-the-mill after we were treated to The Matzos in 2007,but Arizona Calling were excellent. Lookingforward to 2009, planning for this began in late2007, would you believe, and you will see fromthe enclosure with your copy of the Journal thatthe line-up of speakers for 2009 is absolutelyfantastic once again. The theme, ‘‘Acupuncture –Beyond Pain’’, will mean that there will besomething for everyone, and with a programmelike this, I expect bookings to go through theroof. Don’t delay in securing your place!
Whilst most things have been striding forwardin leaps and bounds, the one thing that has beena real disappointment from an uptake perspec-tive is the discussion forum on the AACPwebsite member area. Feedback from the mem-bership had identified that this was one ofmembership benefits that seemed to be reallyneeded. A lot of work was then done designingand testing the site, appointing a moderator, andpromoting its availability. Despite trying toencourage people to post their queries, there wasvery little uptake over the whole membership –just over 3%. The forum, whilst currently
� 2008 Acupuncture Association of Chartered Physiotherapists 11

removed from the website, remains in the back-ground as an inactive area and is ready to bereinstated at the click of a button. If you wouldlike to volunteer as a moderator, then please doget in touch. It’s such a shame that this greatfacility for the membership community has beenput on hold. You’ve paid for it, so let’s get it upand running again, if we can, and make sure thatwe use this focussed area for you, the members.
The availability of the AACP 40-HourTop-Up Course ceased at the end of March2008, although courses were almost fully bookeda few weeks beforehand. I want to extend apersonal thanks to my team in the Office, par-ticularly Diane Morgan, who I am sure many ofyou have spoken to whilst we have been estab-lished in Peterborough. Diane worked tirelesslyto ensure that as many courses ran for as manypeople as possible. Her hard work ensured thattutors had everything they needed and the stu-dents had the correct information at the righttime. The deadline for attendees of the top-upcourses to join the Association passed on 1 July2008. I am pleased to say that the take-up ofmembership by the group has been reasonablygood. Of course, those who did not join beforeJuly will now have to complete the AACP-approved 80-Hour Foundation Course, or arelevant acupuncture degree. Existing membersof the AACP do not need to do anything toremain a member other than maintain therequired 10 h of continuing professional devel-opment for every 2 years of membership.
The online clinical audit was extremely inter-esting, and among other things, has confirmedthe need for the Association to provide coursesthat take members beyond the basics. We will belooking to run more courses focussed on specificissues. Details of courses are always available inthe AACP website training area. Just click on theblue title of each of the courses to find out
details about course content, dates, location andhow to book.
The regional representatives pages on thewebsite are now up and running, so you will haveaccess to a dedicated area for your location whenyou log on to the website. Of course, you canalways look at the activities in other regions bynavigating around the regional representativespages. If you have an event, course or anythingelse that you think might be useful for othermembers within your region, please contact yourrepresentative, who will discuss your requestwith you.
I mentioned in the Spring 2008 Journal that wewere having a big drive to encourage members torenew their membership by direct debit (DD). Iam pleased to say that this has been a hugesuccess. The ratio of DD renewals versus chequerenewals is still three to one, but most peoplenow join by putting in place the DD. If yourenew your membership by cheque, why notswitch to DD at your next renewal. You will save£5.00 on the current annual subscription fee.New members can now join by DD, whichoffers greater convenience for both the newmember and the administration staff.
It would be great to hear from you. Let meknow if you have any burning issues, want to beinvolved, or have any questions or suggestions.You can also now write in to the Journal and haveyour letters published on the letters page (seepp. 109–111). Thank you for your continuedsupport and feedback, and do try to use thewebsite. Go on, just take a peek!
Finally, am I the first person to wish you ahappy Christmas? Well, season’s greetings for thecoming festivities. Have a wonderful break –you’ve earned it!
Sharon Fox
Business Manager AACP Ltd
Business Manager report
� 2008 Acupuncture Association of Chartered Physiotherapists12

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 13
Finance and Secretariat report
IntroductionIn order to meet the Journal deadline, this reportsummarizes all recent AACP Office activity up to30 April 2008.
Office changesThere have been no changes in staffing at theOffice because we have now reached our opti-mum staffing levels for managing the administra-tive activities of the Association.
Membership renewalMembership renewal activities remain steady,and there has been an improvement in the speedwith which individuals are renewing their mem-berships following efforts by the Office toencourage swift renewals and the introduction ofa late renewal charge. I am delighted that we arenow able to allow members to join using directdebit (DD), and 69% of members are now usingthe DD method of renewal.
Membership status to date is shown inTable 1.
Direct debit collection is running relativelysmoothly. However, many members are notletting us know when they change their bankdetails. Of course, this means that DDs arerejected, and the Office then has to establish thereason and contact the member. Please let usknow about any changes to your account so thatwe can ensure that your membership is notlapsed accidentally.
DatabaseThank you to all members who are updatingtheir details online via the AACP website.Renewals and those arriving each day are loggedinto the database within a couple of days.
New members are being sent joining packswithin 5 working days. Membership certificatesfor those renewing by DD are sent out immedi-ately after confirmation of the successful collec-tion of their subscription.
Current financial situation
General situationYou will see from the audit report on the websitethat the financial situation remains favourable,and following the publication of the AACP5-year plan (see pp. 83–90), initiatives and mem-bership benefits are being put in place to ensurethat funds are reinvested in membership servicesand opportunities.
Other issues
WebsiteYou will recall that the AACP websitee-commerce facility opened in October 2007.Only a small number of merchandise and coursebookings have been purchased using this facility.If there are any enhancements or amendmentsthat you wish to suggest, then please do so.
The Association have introduced access tothree academic databases via the member’s areaof the website.
Unfortunately, the discussion forum has lapsedbecause of inactivity by the membership. This is agreat shame since it could be an extremely usefulfacility for members to pass on guidance, experi-ences of treating patients and engage in generalinformation sharing. The facility can be resur-rected if necessary, but we do need a moderatorfor the site. If you have the relevant experienceand can commit to giving a couple of hours aweek to work in this role, please contact me.
Sharon Fox
Business Manager AACP Ltd
Table 1. Acupuncture Association of Chartered Physiotherapistsmembership status as of 30 April 2008
Membership category Number
Accredited Members 4617Advanced Members 227Probationary Members 34Honorary Members 17
Total number of active members* 4895
*Number of new members who have joined since 1 January 2007=819.
� 2008 Acupuncture Association of Chartered Physiotherapists 13


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 15–17
Webmaster report
IntroductionThis report covers the development of theAACP website in its second year. The level oftake-up is discussed, and an analysis of patternsof usage by members and the general public ispresented.
You can find our website at:http://www.aacp.uk.com
BackgroundThe previous AACP website had been in usesince its inception, back in 2000, and wasreplaced in February 2007. The new website wasthen developed in stages and completed laterthat year. The new site is graphics-oriented andprovides a wide range of member services,including online access to research databases, apractitioner search facility and details of theavailability of training courses. Members cannow order and pay for AACP publications,courses and conference places.
There are currently no further formallyplanned stages, but small improvements aremade regularly and any major additions can beplanned as required, subject to approval andfunding by the Board (see below).
The addition of reference documents to thesite can be made at any time and new infor-mation is added regularly. If any members haveitems that they would like added to the site,please contact the Webmaster (e-mail:[email protected]).
Website take-upThe first stage of the website finally went live on13 February 2007. The website is monitored in a
number of different ways and these are discussedbelow.
Website visitorsStatistics maintained by our Internet service pro-vider (ISP) demonstrate that the take-up is asshown in Table 1.
Members’ accessThe website itself tracks logins by members, andTable 2 shows the numbers of members loggingin against the number of times each has loggedin. From this table, it can be seen that, since thewebsite opened, some 868 members have loggedin one or two times, but just 80 members havelogged in between 11 and 20 times. Although thefigures are an improvement compared with lastyear, there are still more than 4000 memberswho have never logged in to the site.
Thus, this general level of website take-up bymembers remains disappointing. In view of therelative ease and low cost of using the website topromulgate information to members, the Boardwishes to make much more use of this mediumto provide an improved service to members.
Take-up from those who may be regardedas ‘‘senior members’’ (e.g. AACP tutors andregional representatives) also remains disappoint-ing (Table 3).
Table 1. Website total visitor count
PeriodUnique visitorsper day
Total visitorsper day
2007 58 962008 to date 62 92
Table 2. Access to the AACP website by members
Number of member logins
Time period 1–2 3–5 6–10 11–20 21–50 >51
Since 15 February 2007* 868 393 168 80 26 12007 718 305 96 35 12 12008 to date 510 175 58 26 2 1
*Start of website.
� 2008 Acupuncture Association of Chartered Physiotherapists 15

Members may wish to ask their tutors inparticular how they keep themselves up to datewith changes and the latest developments withinAACP.
Non-member accessThe ISP statistics reveal that, to date, there havebeen approximately 60 independent logins to thewebsite each day since its inception. Table 2shows that members account for about 20 ofthese a day, with the remainder, therefore, beingfrom non-members – this equates to an averageof around 40 per day.
I can’t judge whether this figure represents asatisfactory level of interest from non-members.Members may have their own views on thisaspect.
Website feedback from membersThe website has a feedback questionnaire thatgives members the opportunity to comment oftheir experience of using the site and to makerecommendations for future developments.Feedback on the new site has generally been verylow, but positive, with ratings in the onsitequestionnaire remaining at 85% and above.
The website was demonstrated at this year’sAACP Annual Conference, where comments onthe website from members were also very posi-tive. A number of members took the opportunityto access the website under supervision whilst atConference, indicating that a lack of confidencein using the web was a problem for quite a few.This had prompted the idea of demonstating thecapabilities of the website at future roadshowsand conferences. Regional representatives willalso be encouraged to make use of their regionalpages to make sure that their local members areup to speed in terms of using the facilities.
There have been very few expressions ofdissatisfaction, and almost all of those that havebeen made have been the result of members notbeing able to find themselves when carrying out
a practitioner search – regretfully, the old maximthat ‘‘physiotherapists never read instructions’’ isalive and well! Following on from this, severalmembers requested the facility to list all AACPmembers in a given area – the website wasoriginally configured for the general public to listup to 10 members in a random order againstdefined search criteria. Such an update has nowbeen implemented and provides regional repre-sentatives with the capability to list all membersin their areas. This will improve their ability tomake contact with members and promulgateinformation.
Website visibilitySurveys on Google are carried out using anumber of relevant search terms and the resultsare shown in Table 4.
Website promotionWays of promoting the website have been dis-cussed and the possibility of a ‘‘treasure hunt’’type competition, with members having to navi-gate through the site to find answers and ulti-mately to win a prize, has been suggested. TheBoard is considering this proposal. If agreed, itcould be implemented with little difficulty andcould perhaps develop into a regular feature. Ifmembers have any other ideas to stimulate inter-est, please let the Webmaster know.
Website contentThe content of the website has steadily increasedsince the launch, with many more referencedocuments and news items being made availableto members and the general public. However,there is still much to be done to provide all theinformation that members need.
Table 3. Take-up of the website by ‘‘senior’’ AACP members
GroupNumber ingroup
Neveraccessedwebsite
Fiveaccessesor less
Tutors 19 4 10Regional representatives 16 1 5
Table 4. Website search rankings: (N/R) not ranked
Date of ranking
Search term(s)June2007
December2007
June2008
Acupuncture 9 9 5Acupuncture physiotherapy 2 1 1Acupuncturist 36 N/R 8Acupuncture training 8 9 6Find acupuncturist 9 5 6
Webmaster report
� 2008 Acupuncture Association of Chartered Physiotherapists16

Website searchesSearches made on the website are tracked so thatit is possible to identify items for which visitorsare searching. The most common searches sincethe website inception are shown in Table 5.
These statistics are monitored and fed backregularly to the Board to guide the future devel-opment and content of the site.
Surveys: clinical auditA survey on members’ experience with acupunc-ture was launched with a view to a clinical auditof the results. To promote the survey, whichmembers have been notified of by e-mail, a prizeof £100 was offered to a member completing thesurvey, to be selected at random in January 2008.The results of the survey are available online and
are published elsewhere in this edition of theJournal (pp. 91–96).
Website updatesThe target for making simple changes to thewebsite (e.g. adding a course advertisement,research paper or a Frequently Asked Question)is 5 working days. At present, such additions arebeing done by the next working day in mostcases.
For more complex changes, the target is toanalyse the problem and provide a time scale forits implementation within 5 working days.
All changes to website content or structure aresubject to AACP Board approval.
ConclusionsThe new website, together with the members’database, allows the Association to offer mem-bers new facilities and gives the AACP scope toprovide many more in response to their require-ments, whilst keeping down its administrativecosts and, hence, member subscriptions.
Members are encouraged to have a look at thewebsite. It’s one of the benefits of membership,and the more interest that there is in its devel-opment, the more use it will be to all members.
J. D. Longbottom
Webmaster
Table 5. Website search results: (CPD) continuing professionaldevelopment
Search rating
Search term Since 15 February 2007* 2008
Consent 7.5% 6.4%CPD 4.6% 7.4%Safety standards 4.4% 3.4%Journal 2.7% 2.3%Courses 1.5% –Contraindications 1.2% 1.6%Fees – 1.4%
*Start of website.
Webmaster report
� 2008 Acupuncture Association of Chartered Physiotherapists 17


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 19–20
Political Liaison Officer report
Acupuncture, Herbal Medicineand Traditional Chinese MedicineRegulation Steering GroupYet again, all I really have to report is anotherdelay.
The final report to be submitted to theGovernment by the Department of HealthSteering Group on the Statutory Regulation ofAcupuncture, Herbal Medicine and TraditionalChinese Medicine (AHMTCM) is still in prep-aration. Even though the work of the SteeringGroup finished in November 2007, the docu-ment was still not available at the time of writing,but I believe that it was scheduled to be printedat the end of March 2008. At least a monthwas spent selecting the cover! (In fact, it waspublished in June; see pp. 97–99.)
There will be very few surprises when it doescome out. A greater emphasis than expected onherbal medicine may be evident, but this is partlybecause there is pressure on herbal practitionersto ensure that their regulation is up and run-ning before some important European Unionlegislation is due to be enacted in 2011.
I must emphasize that it is not known whatthe response of the Government will be to thereport. It very much depends on what is seen asa priority on the day of publication. In so far aswe can be certain of anything, it seems very likelythat the Health Professions Council (HPC) willbe tasked with becoming the regulatory body forthis group of complementary therapies. To thatend, Rachel Tripp from the HPC has attendedseveral meetings of the Steering Group toanswer questions about how the Council worksand allay fears that the smaller groups willeffectively vanish in the larger whole. One of themain worries has been the English-languagerequirement for Chinese practitioners working inshops across the UK. This problem is by nomeans solved, and it will be interesting to see theGovernment’s response. Rachel has emphasizedthat nothing will happen until 2010 at the earliest.
The Steering Group requested considerableinput from the smaller stakeholder groups
throughout the process, and the AACP has beenan influential contributor at all times. Physio-therapists are the largest single group of prac-titioners in any category, and indeed, they arehard to ignore. The report will include an overallsummary of the current situation with regard tothe three groups of practitioners, with specificdetails on training, accreditation and scope ofpractice. Annexes to the main document willcontain suggestions about how the ‘‘grandfather-ing’’ processes could be most effectively handled,and also information on the current trainingprogrammes for each profession.
The AHMTCM Steering Group is notscheduled to meet again. It has been both anhonour and a pleasure to represent physiothera-pists during this consultation process, and I amgrateful to the AACP Board for their confidencein me.
Acupuncture Stakeholders GroupIn the light of the above report, much of theurgency has gone out of the AcupunctureStakeholders Group meetings. The lengthy andoften tedious discussion of the minutiae of thesubmissions to the AHMTCM Steering Group isover now and we await the Governmentresponse. By and large, there has been consensuson all the issues. The group agreed that the needfor such regular meetings had passed, althoughone last meeting is scheduled for June 2008 todiscuss the fallout from the report.
However, the most important question hasstill not been decided: what will happen tophysiotherapists using acupuncture? As I havesaid before, it is more than likely that the HPCwill continue as our physiotherapy regulator,and we will be able to have an entry on boththe physiotherapy and acupuncture registers.The drawback is that we will have to pay forboth. This comes as no surprise, given thecurrent arrangements for physiotherapists whoalso practise podiatry, although it may be moreexpensive than some AACP members wouldlike.
� 2008 Acupuncture Association of Chartered Physiotherapists 19

The benefit is that when the acupuncture/herbal medicine register opens, there will be apainless transfer of all current, paid-up memberson the AACP register. The issue will be whethermembers wish to pay to retain themselves onboth registers when the first year or so iscomplete. The procedure for rejoining a list aftera lapse is much easier, and cheaper, than joiningfor the first time, and therefore, even if theychoose to leave for a while, the fact that theirtraining was sufficient for them to be acceptedfor the register the first time will make it easy torejoin.
The issue of whether AACP members will stillwant to opt out remains problematic. It will betheir own decision, but as we have said manytimes, it is very likely that National HealthService trusts and the Ministry of Defence, forexample, will insist that they are registered foracupuncture in addition to physiotherapy. It
cannot be said too often that these decisionsconcerning the HPC will depend entirely on theresponse of the Government to the SteeringGroup report.
Finally, it is with some regret that I haveto announce my resignation from the post ofPolitical Liaison Officer. It has been a greatpleasure and I have enjoyed the endless debatesbetween the different factions, but I feel that, ifthe Acupuncture Stakeholders Group continues,although meeting less regularly, we really need tobe represented by someone from the Associationwho is in touch with the Board and familiarwith the 5-year plan. Once again, I would like tothank the AACP for their confidence in me andwish them well in future dealings with the newacupuncture profession.
Dr Val Hopwood
Political Liaison Officer
Political Liaison Officer report
� 2008 Acupuncture Association of Chartered Physiotherapists20

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 21
Clinical Interest Group Liaison Officer report
The clinical interest groups (CIGs) represent allaspects of physiotherapy and demonstrate thewide diversity within the scope of physiotherapypractice: over 40 groups were represented at themost recent CIG meeting.
Members of the CIG Liaison Committee(CIGLC) also sit on eight other committees, themost influential being: the Annual Representa-tives Conference Agenda Committee; the Pro-fessional Practice Committee; and the Learningand Development Committee.
The most recent CIGLC meeting was one ofthe most eventful that I have ever attended, withthe election of a new Chair and Vice-Chair, andnew rules of engagement for the group. The
main item discussed was a Chartered Society ofPhysiotherapy (CSP) project called ‘‘Chartingthe Future’’, which highlights the need for theprofession to change. The other topic of interestwas the new e-portfolio that is being piloted atpresent. For further details of both projects, Idirect you to the CSP website and the relevantarticles in Frontline.
If anyone is interested in attending thesemeetings as my alternate, then please do contactme (e-mail: [email protected]).
Lesley Pattenden
Clinical Interest Group Liaison Officer
� 2008 Acupuncture Association of Chartered Physiotherapists 21


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 23
Education, Training and Research Committee report
The Education, Training and Research Com-mittee (ETRC) continues to meet quarterly toconduct its business. The membership has beenreviewed and increased to widen the range ofexpertise available, and Ann Green fromCoventry University is the new Vice-Chair of theCommittee.
The main business of the ETRC is still theapproval of courses and tutors, but the numberfor consideration has dropped considerably incomparison to last year. The approval processhas also been modified, and from now on, allmembers of the Committee will consider everycourse, rather than groups of three, since it is feltthat this will help to ensure the consistency ofthe validation process.
A new innovation this year has been theaddition of meetings with tutors. The validationprocess is explained at these sessions, and tutorsare given the opportunity to ask questions andput forward ideas. We plan to hold these tutormeetings regularly, usually in the afternoons
immediately following the ETRC’s morningsessions.
A meeting dedicated to the development ofresearch has recommended to the Board thatfunds should be made available to AACP mem-bers in order to support them in conductingresearch. The final details of how membersshould apply, the amount available and therequirements of the Association will bepublished in the Journal as soon as possible.
Assurance of the quality of provision of coursesthat are recognized by the ETRC and, thus, theAACP requires professional expertise from themembers of the Committee, all of whom areperforming this role in addition to their othercommitments. The Office staff at the AACPalso play an important role in ensuring that alldocumentation is distributed in a timely manner.
Professor Nigel Palastanga FCSP
Education, Training and Research Committee Chair
� 2008 Acupuncture Association of Chartered Physiotherapists 23

Acupuncture Association of Chartered Physiotherapists
MUSCULOSKELETAL ROADSHOW
7 November 2008
Cambridge University, Vivien Stewart Room, New Hall, Cambridge CB3 0DF
A selection of speakers and their topics includes:
ADRIAN YEOMAN Hip Joint
LYNN PEARCEThoracic Spine T6
DR VAL HOPWOOD Elbow
JENNIE LONGBOTTOM Myofascial Pelvic Pain
£95 (members)/£105 (non-members)
Telephone the AACP Administrative Office on (01733) 390012 or 390007 to book your place now!

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 25
IAAPT Representative report
There is very little to report on the internationalfront.
In February, the AACP Board members werefortunate to receive a talk from Mrs BrendaMyers, Secretary General of the World Congressof Physiotherapy (WCPT). Mrs Myers gave us ashort history of the organization, explained itscurrent aims and then went on to explain thenature of the special interest groups that existunder the WCPT umbrella. It was a very inter-esting presentation and helped the Board tobetter understand the role of the WCPT and
the International Association of AcupuncturePhysical Therapists (IAAPT) Representative infostering international collaboration.
The AACP are currently in discussion withIAAPT regarding next year’s conference, whichwe hope will be a collaborative event withIAAPT and, therefore, have an internationalflavour. Watch this space!
Merian Denning
Vice-Chair and IAAPT Representative
� 2008 Acupuncture Association of Chartered Physiotherapists 25

Acupuncture Association of Chartered Physiotherapists
AACP CONFERENCE 2009
“Acupuncture – Beyond Pain”
15–17 May 2009
Robinson Executive Centre, Wyboston, Bedfordshire
Confirmed speakers include:
PROFESSOR GRAHAM SMITH
ROSA N. SCHYNER
PROFESSOR GRACE DOREY
PETER DEADMAN
Watch out for reservation information and weekend schedules on a PC near you – soon!

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 27
Conference Coordinator report
AACP Conference, ‘‘Acupuncture– Beyond Pain’’, RobinsonExecutive Centre, WybostonLakes, Bedfordshire, 15–17 May2009I am sure that you are all eagerly awaiting1 October 2008, when you can pick up thephone and secure your place at next year’sconference at the customary ‘‘early bird’’ dis-counted price. After another superb event thisyear, we have an outstanding variety of speakersconfirmed for 2009 who will surely rival thepopularity of past presenters.
Those of you who are still to attend one ofthese meetings have yet to experience a greatweekend. It’s an informal chance to networkwith other AACP members, guest speakers, andthe Board and subcommittee members. Thanksto all of you who have supported these events todate: these are superb weekends, and it’s fun tomeet everyone and see people having a goodtime.
Once again, my work on Conference 2009started very early on, and I was relieved thatmost of the speakers whom I approached didn’thave any commitments for the dates when wewanted them to attend. I think the theme for2009, ‘‘Acupuncture – Beyond Pain’’, will be very
popular, and there will be something for every-one, whether you are interested in women’shealth, sports injury or mental health.
This year’s conference ran smoothly and ourrelationship with Wyboston Lakes ensures thatthey know exactly what we expect from them.Using the same venue over a few years doesmean that both parties know how the otheroperates and what they need. However, it alsomeans that you have to work hard at not takingthings for granted and resting on your laurels!
Over the coming months, the AACP willbegin the task of compiling documentation forthe delegate folders, making final checks onattendee requirements, contacting the trade,organizing helpers and generally making sureeverything is in place for a fabulous conferenceweekend. I hope that will be with your help: theAssociation needs members to participate in theorganization and coordination of future confer-ence events. If you have the time to attend upto four meetings a year at our head office inPeterborough, have ideas for potential speakersor possible event formats, and the commitmentto help contribute to the delivery of conferences,then I’d really like to hear from you.
Sharon Fox
Business Manager AACP Ltd
� 2008 Acupuncture Association of Chartered Physiotherapists 27

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 29–34
Regional reports
East Anglia
West
Kim Wager andSue Cox fromSubstance MisuseAcupuncture Reg-ister and Training(SMART) gave apresentation inPeterborough, out-lining their use ofauricular acupunc-
ture for drug addiction. They use the NationalAcupuncture Detoxification Association protocol,i.e. five points in each ear, and have achieved someencouraging results in a difficult patient group.Interestingly, SMART train various non-healthprofessionals within the prison system, such asprison officers, to perform the acupuncture.
In December 2007, Jennie Longbottom ran asession on the medicolegal aspects of acupunc-ture that covered issues such as careful docu-mentation, what an expert witness would lookfor and the various policies related to the use ofacupuncture. This was all useful information, andthe event was surprisingly well attended for anon-clinical workshop!
February 2008 saw Lynn Pearce running aworkshop on headaches in Bedford, and boththe topic and speaker were hugely popular! A lotof people were very disappointed not to get aplace at this workshop, so we are planning tohold it again in the autumn.
The regional representatives area on theAACP website is now up and running, and this isthe best place to find details of forthcomingcontinuing professional development (CPD)sessions. The website is very user-friendly, andan excellent source of information for allacupuncture-related issues, from courses andsharps policies to news and events. It also givesyou access to the research databases – so, go on,check it out!
Debbie Yates
EastThank you to the new members in the regionwho have contacted me. Please continue to do soif you think that I can help in any way. Forexample, I can lend a hand if you want to set upa course or find a mentor.
An active National Health Service (NHS) acu-puncture special interest group meets at theNorwich Community Hospital, Norwich. AnnWilliams gave the members a report about LynnPearce’s review course in December 2007, andmost recently, Ann and I gave a presentation onbi syndrome that will be followed up with apractical session at the next meeting.
Please get in touch if you have any infor-mation for members that I can post on thewebsite or if you have any queries.
Lynne Fanning
InternationalMy name is Felicity Edwards. One day, not solong ago, I received an e-mail from the AACPasking for volunteers for the post of inter-national representative. In a sudden and un-characteristic fit of civic duty, I pressed thereply button. When I thought about it later, Itook comfort from the likelihood that I wouldnot stand out among the hundreds of otherresponses – only to discover that I was the onlyone to step into the breach!
Although I now live and work in the UK,I grew up in Kenya and went to school inQueensland, Australia. After training and quali-fying in the UK, I went back to Africa to workin Rhodesia and stayed on when it becameZimbabwe, moving to South Africa later. Withsuch a chequered background, I hope that I willbe able to serve members abroad well as theirrepresentative.
For the past 4 years, I have worked as a clinicalspinal specialist in Kings Lynn, Norfolk. Prior tothis, I worked in Gloucestershire for 5 years. Thefirst acupuncture course I took was with CharlesLiggins in Durban, South Africa. It made a big
� 2008 Acupuncture Association of Chartered Physiotherapists 29

impression on me and I have since done manyother courses. I find acupuncture to be one of themost useful modalities in my treatment arsenal.
Because we are such a disparate group, regularphysical meetings are not possible, but we canuse the Internet to get to know each other. Someof you will already have received a communi-cation from me. As a means of getting to knoweach other, I am planning to initiate a round-robin letter. Everyone will be able to write a littleabout themselves, and air their knowledge or askquestions. If anyone has any other suggestions,I would be only too pleased to hear from you.I will forward any new information (e.g. guide-lines) that I receive to each member individually,of course. If any of you reading this have notgiven the AACP your e-mail address, but wouldlike to join in, you are very welcome to doso – this is the most cost-effective means ofexchanging information and news.
I also plan to pass on any interesting titbitsthat glean at Conference to internationalmembers via e-mail.
Felicity Edwards
Midlands WestI am pleased toannounce that,since my last re-port, 23 new mem-bers have joinedthe AACP in theWest Midlands re-gion. I would liketo take this oppor-tunity to welcome
you all and hope that you fully utilize the benefitsof being members of the Association.
As promised, the quarterly acupuncture clini-cal interest group (CIG) has now begun meeting.The first discussion was led by Catherine Plant,and focused on safety standards and protocols.This was very well received by the 14 attendeesand it highlighted some important issues regard-ing AACP safe practice guidelines. Another CIGevent on electroacupuncture was scheduled forearly July. These meetings are open to all acu-puncturists, so do come along if you can. Pleasesee the AACP website for further details. I would
also like you to tell me about any courses beingheld in the West Midlands region that membersshould know about, or any speakers who youwould like to hear.
It is and will continue to be an excellent yearfor the Association and its members. We arestrengthening our lines of communicationthrough the new website, increasing our rep-resentative and membership base, and in turn,enhancing the depth and breadth of support andcourses available to members. I am very muchlooking forward to putting faces to names atConference and hearing from you all soon.
Get involved!
Jamie Holder
North East EnglandGreetings from theNorth East tomembers from fur-ther afield! Partici-pants from as faraway as Devon andFrance have at-tended our coursesin Morpeth thisyear, along with
our neighbours from Scotland. As a result of thisinterest, we have had to ‘‘google’’ for maps ofHadrian’s Wall and directions to the GatesheadMetroCentre since many of attendees wanted togo sightseeing. I was quite surprised by this, butthen, I suppose that everyone tends to ignore thebeauty of their own surroundings. Now I need tofind my local tourist information point so that Ican grab a load of leaflets in preparation for thenext course!
Morpeth is a medieval market town that isvery quiet during the daytime, but becomesa ‘‘party town’’ on Nurses’ Night (the lastWednesday of the month) and at weekends. Ifit’s a quiet country pub that you want when youcome here, let me know! Morpeth does have awebsite that you can access (www.morpeth-online.co.uk).
Unfortunately for Kam Mak-Wah’s group,their course was held on the same weekend asthe Morpeth Northumbrian Gathering, one ofthe town’s celebrations, so many of the hotels
Regional reports
� 2008 Acupuncture Association of Chartered Physiotherapists30

were booked a long time in advance, the pubswere busier, the bells rang most of the day, anda mock battle with cannon fire belted outthrough out the afternoon. It may be wise toavoid that weekend next year, as well as the otherissues that arose during our first official AACPcourse, but it was all a learning experience formyself, Kam and the course participants.
I would like to welcome all new members, andhope that you will contact me with your viewsregarding future regional meetings, speakers andfuture courses in our area. This also applies toour current members, of course. The AACPwebsite makes this very easy to do.
This year, we hosted the last 40-Hour Top-UpCourse, tutored by Kam, and ‘‘Women’s Health’’and ‘‘Anxiety and Depression’’, both run byJennie Longbottom, and by popular request, wealso hope to run a return fixture featuring BryanRouse and Jong Baik. Kam has volunteered togive us an evening session, and we didn’t evenhave to twist his arm!
I was contacted by many acupuncture studygroups last year, but unfortunately, a computervirus deleted many contact details. I do apologiseif you have not received a reply to your e-mail.Please get in touch again.
Finally, if you have any ideas, know a speakeror are able to volunteer to give a talk at a regionalmeeting, then do get in touch – many heads arebetter than one!
I hope to meet more of our members at futuremeetings.
Karen Ogle
North West EnglandAll informationI receive fromCumbrian mem-bers about courses,meetings and otherrelevant issues isbeing circulated onmy e-mail contactlist. I am veryhappy to expand
this list and the topics that it covers, so pleasecontact me via the website if you want to join orgive me input.
Local meetings are proving to be an excellentopportunity for NHS and independent physio-therapists to find common ground in our mutualquest for improved practice and education.
I hope that everyone is visiting the website. Itcontains a lot of useful information and can beeasily accessed, even by an information tech-nology novice like myself!
Dianne Allan
Hello to you all!My first 6 months as the shared representative
for the North West have been busy ones, takenup with arranging courses and contacting thelocal membership. After close liaison with RuthHeaton, our Cheshire and Merseyside Acupunc-ture Representative, three subsidized NHScourses for local members due to be run in Mayand June 2008 have been organized. We havemanaged to pin down Jennie Longbottom to atrip up north to present her medicolegal lecture,which I am sure will be well attended. There willalso be a day course on stress and anxiety withNeil Quinton and a headache course with LynnPearce. These courses were filled rapidly, whichshows how much we continue to need to runevents in the North West region.
If anyone wants to help organize a course,please get in touch with me. I now have anup-to-date e-mail list of members, so news aboutany local meetings can be passed to me forforwarding to the list.
As Dianne Allen says in her report above, localmeetings and courses are a very good way ofboth private practitioners and NHS staff gettingtogether, so please keep organizing these!
Over the next 6 months, I will put any relevantinformation up on the North West regionalrepresentatives web page – sorry for not doingso as yet. I am looking forward to meeting asmany of you as I can at this year’s conference.
Janet Wiggins
Northern IrelandThere is not much to report from NorthernIreland at the moment. We are continuing towork with the significant number of memberswho are updating, and once this processnears completion, we will contact members
Regional reports
� 2008 Acupuncture Association of Chartered Physiotherapists 31

regarding what they want in terms of teachingand follow-up.
Kay McLorn and Maggi Holmes
South Central England
Hello, everybody! First of all, I would like towelcome all our new members. I look forward tocontacting you with about future events andmeetings, and offering help when I can.
It has been relatively quiet over the past fewmonths, but I hope that we can create anddevelop a network to facilitate communicationand the exchange of ideas within the SouthCentral region.
I look forward to helping many of you overthe coming months. However, please continue toconsult the AACP Office or refer to the AACPwebsite with regard to any urgent matters.
Ahmed Osman
South East EnglandHello to you all, Iam Moira Tunstall,a private prac-titioner working in asmall rural practicein Horsmonden,Kent. I work part-time, but fill myspare days withmany other activi-ties, including per-sonal study. I amcurrently in myfirst academic year
at Coventry University, Coventry, studying forthe MSc in Acupuncture. It is a daunting butmost enjoyable task, and I can highly recom-mend it to any of you who are consideringit. The MSc adds a whole new dimension toacupuncture practice and its future within ourprofession. I also have time for other, lesscranial, pursuits. As I write, I am dressed for atrip to the gym for a hour of tai chi, followed bya workout. I believe that tai chi and acupunctureare complementary.
As you know, I have only started, so I havelittle to report to you about regional activities.Jennie Longbottom ran a foundation courseat Maidstone in May and June 2008, which Ihope will inspire more people to join theAACP.
I have a list of the postal addresses of mem-bers in the region, but no e-mail contact details.Can you send these to me ([email protected])? It will make any future correspon-dence much easier. Please let me know about thetype of CPD that would be of benefit to you. Iwould also be happy to learn of any specialinterest groups in the region.
I look forward to receiving your news and Ihope that I can be of help to all members in theSouth East area.
Moira Tunstall
South WalesHello, all, I am the South Wales regional rep-resentative, and I work in sunny Swansea. Since
Regional reports
� 2008 Acupuncture Association of Chartered Physiotherapists32

my last report, Ihave been con-tinuing to try todevelop an effec-tive e-mail com-munication toolfor networking inWales. As withmost things, theidea was simple,but it has provedto be is a tad morecomplicated inpractice! Still, I ampersevering, andwould ask those of
you who have not yet checked or provided ane-mail address to do so as soon as you can.
I have started to put up some messages onthe Wales portion of the website, but I canonly add what I know. Please tell what’s goingon so that I can make everyone aware of yournews. Do this via <www.aacp.uk.com> . Itseems that there are quite a few courses goingon in Wales, and if you are thinking of runninganything, do get in touch and I will see what Ican do to help.
There is now an extra representative in Wales:Paul Battersby is taking on the North Wales areaand will be contactable via the web page in thenear future.
Not much else happening at the moment – butdo let me know what you want and I will try tohelp.
Dave Graham-Woollard
South West England
Devon, Somerset and BristolI am pleased toreport that ourDevon PrimaryCare Trust (PCT)and Ministry ofDefence (MOD)regional meetingscontinue to thriveand be well sup-ported.
A practical needling day at Honiton inFebruary 2008 was highly successful, with a fullattendance of 20 physiotherapists from aroundthe region. Another day has been arranged forMay 2008 to cater for another 20 members whomissed out the first time.
The MOD group will also have met again inlate May 2008 for a training day dedicated to bisyndrome, its clinical implications, practical pointfinding and needling of appropriate formulae.We plan to run this session again later in the yearfor the Devon group to foster a pattern ofcontinual development.
I try to send a mailshot to all new members,but ultimately, communication is down to you.This is a huge area that, for the time being, alsoincludes Gloucestershire, Herefordshire andDorset. Let me know what you want and I willtry to facilitate a response where possible.
Please take the time to log on to the AACPwebsite, which is fast developing into a first-classinformation service. Amongst many other things,you are now able to access research databasesand interact via a discussion forum.
For information on any regional matter andthe MOD Group, please contact me at my newe-mail address ([email protected]). Forinformation, about the Devon PCT group, getin touch with Nicola Parfitt ([email protected]).
Mike Chapman
CornwallI am continuing toact as joint regionalrepresentative withMike Chapman forthe South West,covering themembership inCornwall.
I am pleased toreport that the
Cornwall Acupuncture Group continues to holdquarterly meetings in Truro. These have beenscheduled for February, June and October 2008.As an offshoot of the February meeting, threevolunteers have offered to arrange and coordi-nate half-day practical acupuncture sessions:there will be one each for the central, eastern and
Regional reports
� 2008 Acupuncture Association of Chartered Physiotherapists 33

western parts of the county. The meetings are agreat forum for discussion and the disseminationof information, as well as providing sup-port for the attendees. Contact Sophie Down([email protected]) or myself([email protected]) via e-mail toget details of upcoming meetings.
Please continue to check the website forupcoming events, and let me know of any localnews or queries that you may have.
Averil Bainbridge
Regional reports
� 2008 Acupuncture Association of Chartered Physiotherapists34

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 35–36
Regional representatives
The following table details the regional representatives and how to contact them.
Contact details
Name E-mail Telephone
East AngliaDebbie Yates [email protected] 01480 462112Lynne Fanning [email protected] –
InternationalFelicity Edwards [email protected] –
JerseyVacant – –
LondonVacant – –
Midlands EastVacant – –
Midlands WestJamie Holder [email protected] 07915 615625
North East EnglandKaren Ogle [email protected] 01670 511930
North WalesVacant – –
North West EnglandDianne Allan [email protected] 01946 820483Janet Wiggins [email protected] –
Northern IrelandMaggi Holmes [email protected] 02893 372089Kay McLorn [email protected] 02892 611211
Republic of IrelandVacant – –
ScotlandTheresa Sheldon [email protected] 01506 834148Wendy Rarity [email protected] –
South Central EnglandAhmed Osman* [email protected] –
*Alternate required.
� 2008 Acupuncture Association of Chartered Physiotherapists 35
Contact details
Name E-mail Telephone
South East EnglandMoira Tunstall [email protected] –
South WalesDave Graham-Woollard [email protected] 01792 537648
(link to AACP web)/[email protected]
South West EnglandAveril Bainbridge [email protected] 0121 286 8243
(link to AACP web)/[email protected]
Mike Chapman [email protected] 01392 414067
Regional representatives
� 2008 Acupuncture Association of Chartered Physiotherapists36

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 37–47
LITERATURE REVIEW
Acupuncture and its use in the management of low back andpelvic girdle pain in pregnancy
Wendy KochPrivate Practice, London, UK
AbstractThis literature review examines four freely available studies that relate to the management oflow back and pelvic girdle pain in pregnancy. Two of these publications are case reports,another describes a quasi-randomized trial and the fourth paper is concerned with a single-blindrandomized controlled trial. A comparison of the use of acupuncture in these studies ispresented. The results of these investigations challenge the traditionally held belief thatacupuncture is contraindicated during pregnancy.
Keywords: acupuncture, low back pain, pelvic girdle pain, pregnancy.
IntroductionLow back pain (LBP) and pelvic girdle pain(PGP) are two of the most common complaintsin pregnancy (Björklund & Bergström 2000);studies have reported that these problems affectbetween 48% and 76% of all pregnant women(Fast et al. 1987; Berg et al. 1988; Östgaard et al.
1991; Kristiansson et al. 1996). The purpose ofthe present literature review is to provide anoverview of LBP and PGP in pregnancy, andreview four freely available articles that describethe use of acupuncture for LBP and/or PGP inpregnancy.
The exact aetiology of LBP and PGP inpregnancy remains unclear. It has been proposedthat pain develops as a result of mechanical,complex hormonal or circulatory changes, ora combination of these factors (MacEvilly &Buggy 1996). As the pregnancy progresses,ligaments become lax as a result of complexhormonal changes and the increasing weight ofthe uterus. The centre of gravity shifts forwardsto accommodate the expanding abdomen, thelumbar curve becomes hyperlordotic, the pelvicposition alters and the rib angles change. Muscu-
lar support is reduced as length–tension relation-ships alter in the abdominal, pelvic and thoracicregions. Increased blood volume, laxity in bloodvessels and the weight of the gravid uterus on theabdominal great vessels combine to alter bloodflow and impede venous return. The weight ofthe uterus and position of the foetus can alsocompress lumbosacral nerve roots, and may alsocontribute to the development of LBP andposterior PGP in pregnancy. Factors thatincrease the likelihood of developing LBP orPGP in pregnancy include a previous history ofthese conditions, pelvic symmetry, smoking andstrenuous work (Östgaard et al. 1994; Wu et al.
2004).Symptoms usually start between the sixth and
ninth month of pregnancy, but can occur as earlyas the first trimester. These symptoms canworsen as the pregnancy progresses and physicalchanges become more pronounced. Pain is oftenaggravated by prolonged weight-bearing, changesin position and activities of daily living. Thesymptoms are often worse in the evening, andmay disturb sleep in combination with otherfactors, such as an increasing frequency of uri-nation (Wu et al. 2004).
Low back pain and PGP are often treated asminor and inevitable consequences of the hor-monal and mechanical changes that occur during
Correspondence: Wendy Koch, Pilates Art Physiotherapy,
1 Thornton Road, Wimbledon Village, London SW19
4NB, UK (e-mail: [email protected]).
� 2008 Acupuncture Association of Chartered Physiotherapists 37

pregnancy; however, the symptoms can lead tosignificant pain, distress and disability (Perkinset al. 1998). Women can become distressed bythe likelihood that their pain may worsenthroughout the pregnancy, and that this painmay adversely affect labour and the postnatalperiod. They can also be concerned by thepossibility that the pain will return and worsen insubsequent pregnancies.
The revised guidelines on pregnancy-relatedPGP published by the Association of CharteredPhysiotherapists in Women’s Health (ACPWH)advocate that women reporting musculoskeletalsymptoms in pregnancy should undergo individ-ual assessment (ACPWH 2007a). The recom-mended treatment for PGP includes adviceregarding positioning and support before andduring labour, the possible use of a sacroiliacjoint (SIJ) belt, as well as stretches, stabilizingexercises and hydrotherapy, if available. Heat canalso be used for pain relief and transcutaneouselectrical nerve stimulation may also be used inthe third trimester (ACPWH 2007b). The useof heat creams, anti-inflammatory gels, non-steroidal anti-inflammatory medications andmost other medications are limited because ofconcerns regarding the effect of active ingredi-ents on the developing foetus. Paracetamol isconsidered to be the safest analgesic, but is onlyrecommended for use if it is taken under medicalsupervision. Stronger analgesics (e.g. codeine-based preparations) may be prescribed whenother measures prove inadequate, but these cancause further complications (e.g. constipationand pelvic discomfort).
Acupuncture has been extensively studied inthe management of LBP in the general popu-lation and some positive results have beenrecorded (Furlan et al. 2004; Manheimer et al.2005). The underlying mechanisms of acupunc-ture are rather complex and still not fully under-stood; however, it is clear that the somatic andautonomic nervous system, neuroendocrine sys-tems, endogenous opioids and central nervoussystem all play a key role in its effects at the local,regional and central levels (Karavis 1997).
The Western and Eastern approaches to acu-puncture vary considerably and a wide range oftreatment approaches exist. In simplistic terms,traditional Chinese medicine (TCM) acupunctureinvolves diagnosis according to patient presenta-
tion and history, as well as objective examination,including general observation, tongue, pulse andskin analysis, and palpation (Stux et al. 2003). Thechoice of acupuncture points is dependent onpatient presentation, identification of ‘‘patho-gens’’, and consideration of inter-relationshipsbetween the acupuncture meridians and organfunction. Recognized treatment regimes for par-ticular complaints are often considered withinthe framework of the individual. Identificationand needling of local tender points (Ah Shipoints) is also a recognized traditional technique.
In Western healthcare, acupuncture is used bya wide variety of health professionals, and theassessment of patients varies according to thetraining and medical background of the individ-ual practitioner. The Western use of acupuncturesometimes utilizes TCM approaches; however,practitioners often select traditional acupuncturepoints within areas of segmental innervation inorder to achieve an effect without always consid-ering the TCM meridian or channel theories andinter-relationships. Local needling of musculartrigger points is also relatively common.
It has been reported that acupuncture hasbeen widely used during pregnancy in TCM formany years. A range of problems have beentreated in this way, including pain, nausea andvomiting, turning breech babies, induction oflabour, and pain relief during labour. Acupunc-ture has also reportedly been used to stimulatespontaneous pregnancy loss (abortion). As aresult of the different effects of discrete acupunc-ture points, various guidelines exist within theTCM literature relating to ‘‘forbidden points’’during pregnancy. Consequently, concerns existin Western medicine regarding the safety ofacupuncture in pregnancy.
There is limited published research assessingthe effects of acupuncture on LBP and PGP inthe pregnant population. This may partly bebecause of the research challenge of assessingthe effect of any form of therapy in pregnantwomen because of the risks associated withharming the foetus.
The present literature review examines fourfreely available studies that relate to the manage-ment of LBP and PGP in pregnancy. Two ofthese publications are case reports, one describesa quasi-randomized trial and the fourth paperis concerned with a single-blind randomized
Low back and pelvic girdle pain in pregnancy
� 2008 Acupuncture Association of Chartered Physiotherapists38

controlled trial (RCT). A comparison of the useof acupuncture in these studies is presented inTable 1.
Literature reviewA case study by Cummings (2003) reported theuse of acupuncture in a female subject duringtwo separate episodes of symptoms thatoccurred one year apart.
The first course of treatment was for LBP andtook place when the patient was not pregnant.During this episode, tender sites were needled inthe gluteus medius and quadratus lumborum,causing an 85% reduction in symptoms over twosessions.
The second course of acupuncture was forunilateral LBP and leg pain. Treatment wasundertaken without knowledge of the pregnancy,which was only discovered six sessions later. Itconsisted of local periosteal needling to theL5–S1 facet joint, and local tender points in thequadratus lumborum and gluteus medius. Fol-lowing a discussion about the benefits and risksof treatment between the subject and therapist,the patient opted to continue treatment through-out her pregnancy to the third trimester, whentreatment ceased. At this time, the subject startedusing crutches with a good effect. During thesecond episode, she was also undertaking chiro-practic treatment and exercise, which reportedlyaggravated symptoms.
Cummings (2003) listed a number of adverseevents that took place during the sessions,including ‘‘tattooing’’ of the skin as a result of theemployment of stainless-steel needles that werefound to have a residue on the shaft. The use ofthese needles was discontinued and the batchwas discarded. Other reported adverse eventsincluded local pain on needling and the inadvert-ent needling of the left L5 spinal nerve rootduring one session, which produced sudden andsevere pain referral. The symptoms were onlytemporary and ceased once the needle was with-drawn. The subject reportedly opted to continuetreatment and gave full consent. No adverseevents relating to the pregnancy were reported;however, the birth outcomes were unknown.
A single case study by Forrester (2003)described the management of incapacitating LBPin a 21-year-old female from 24 weeks’ gestation
until the end of the pregnancy. The initial treat-ment focused on LBP; however, as this resolved,it was focused on leg pain and cramps. A positiveoutcome was reported, and no treatment givenbeyond 33 weeks gestation until a review thattook place 3 weeks postnatally.
Treatment started at 24 weeks’ gestation. Itwas provided on a weekly basis to 29 weeks, thenat 31 and 34 weeks, and finally, at 3 and 9 weekspostnatally. The treatment involved usingmanual acupuncture bilaterally to traditionalpoints for LBP or points connected via segmen-tal innervation, including Bladder (BL) 23, BL25,and BL57, and Huatuojiaji (HTJ) points at the L2and L4 levels. Outcome was measured accordingto patient-reported pain symptoms and a VisualAnalogue Scale (VAS; range=0–100). Noadverse effects were reportedly experienced bythe woman or her infant.
Guerreiro et al. (2004) undertook a prospectivequasi-randomized controlled study. This studyrecruited females with LBP or PGP who wereattending the hospital antenatal programme. Outof a group of 79 women, 61 (77.2%) reported atleast mild LBP or PGP. These subjects wereallocated to either ‘‘conventional’’ management(the control group) or ‘‘conventional’’ manage-ment plus acupuncture (the treatment group).Women attending a Monday–Wednesday classwere allocated to the control group, whereasthose attending a Tuesday–Thursday class wereallocated to the treatment group. Prospectivesubjects were excluded if they had experiencedany chronic or handicapping LBP before becom-ing pregnant, if they were in a high-risk preg-nancy group, or if they had been treated withacupuncture in the preceding year.
Both groups were given ‘‘conventional’’ treat-ment, which consisted of prescribing analgesicmedication (500 mg paracetamol) and anti-spasmodic medication (10 mg hyoscine). Thetreatment group also received acupuncture,which involved the use of eight standard acu-puncture points as well as the option of fouradditional points to individualize the treatmentto each patient’s presentation. Commonly usedpoints included Kidney (KI) 3, Small Intestine(SI) 3, BL62, BL40, Triple Energizer (TE) 5, GallBladder (GB) 30, GB41 and HTJ points overbetween eight and 12 treatments on a once- ortwice-weekly basis.
W. Koch
� 2008 Acupuncture Association of Chartered Physiotherapists 39
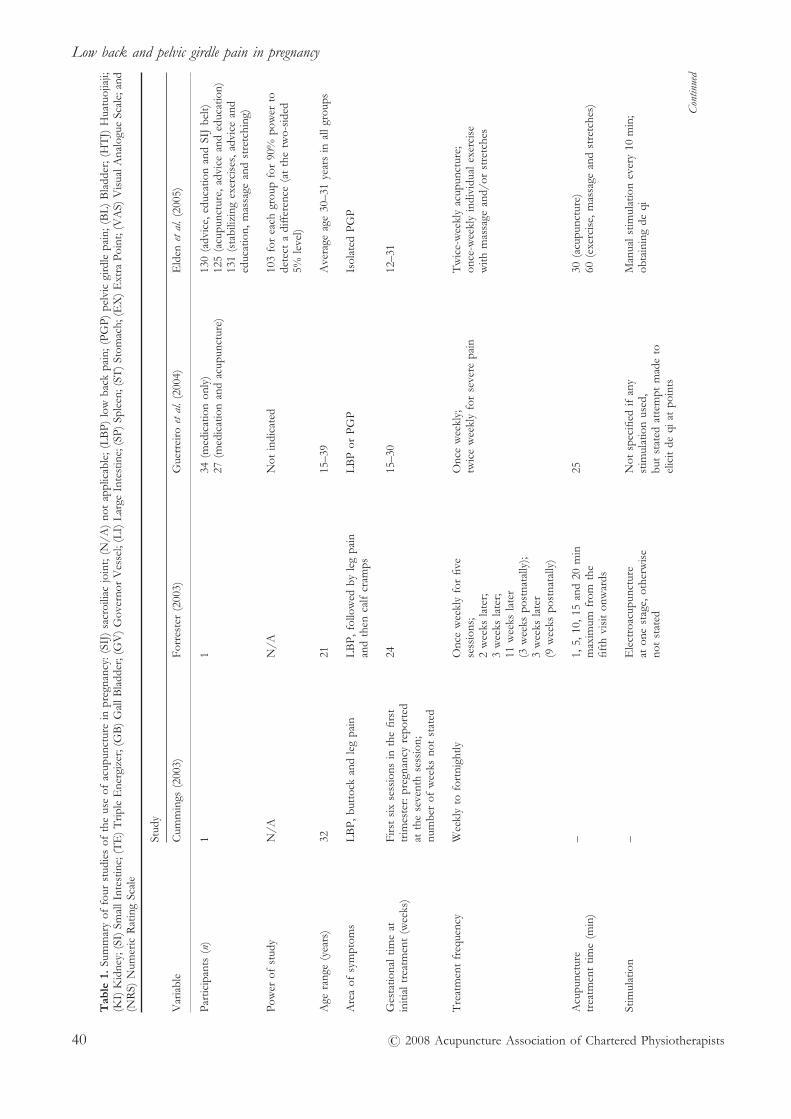
Ta
ble
1.
Sum
mar
yof
four
stud
ies
ofth
eus
eof
acup
unct
ure
inpr
egna
ncy:
(SIJ
)sa
croi
liac
join
t;(N
/A)
not
appl
icab
le;(
LB
P)lo
wba
ckpa
in;(
PGP)
pelv
icgi
rdle
pain
;(B
L)
Bla
dder
;(H
TJ)
Hua
tuoj
iaji;
(KI)
Kid
ney;
(SI)
Smal
lInt
estin
e;(T
E)
Trip
leE
nerg
izer
;(G
B)
Gal
lBla
dder
;(G
V)
Gov
erno
rV
esse
l;(L
I)L
arge
Inte
stin
e;(S
P)Sp
leen
;(ST
)St
omac
h;(E
X)
Ext
raPo
int;
(VA
S)V
isua
lAna
logu
eSc
ale;
and
(NR
S)N
umer
icR
atin
gSc
ale
Stud
y
Var
iabl
eC
umm
ings
(200
3)Fo
rres
ter
(200
3)G
uerr
eiro
etal
.(2
004)
Eld
enet
al.
(200
5)
Part
icip
ants
(n)
11
34(m
edic
atio
non
ly)
130
(adv
ice,
educ
atio
nan
dSI
Jbe
lt)27
(med
icat
ion
and
acup
unct
ure)
125
(acu
punc
ture
,adv
ice
and
educ
atio
n)13
1(s
tabi
lizin
gex
erci
ses,
advi
cean
ded
ucat
ion,
mas
sage
and
stre
tchi
ng)
Pow
erof
stud
yN
/AN
/AN
otin
dica
ted
103
for
each
grou
pfo
r90
%po
wer
tode
tect
adi
ffer
ence
(at
the
two-
side
d5%
leve
l)
Age
rang
e(y
ears
)32
2115
–39
Ave
rage
age
30–3
1ye
ars
inal
lgro
ups
Are
aof
sym
ptom
sL
BP,
butt
ock
and
leg
pain
LB
P,fo
llow
edby
leg
pain
LB
Por
PGP
Isol
ated
PGP
and
then
calf
cram
ps
Ges
tatio
nalt
ime
atFi
rst
six
sess
ions
inth
efir
st24
15–3
012
–31
initi
altr
eatm
ent
(wee
ks)
trim
este
r:pr
egna
ncy
repo
rted
atth
ese
vent
hse
ssio
n;nu
mbe
rof
wee
ksno
tst
ated
Tre
atm
ent
freq
uenc
yW
eekl
yto
fort
nigh
tlyO
nce
wee
kly
for
five
Onc
ew
eekl
y;T
wic
e-w
eekl
yac
upun
ctur
e;se
ssio
ns;
twic
ew
eekl
yfo
rse
vere
pain
once
-wee
kly
indi
vidu
alex
erci
se2
wee
ksla
ter;
with
mas
sage
and/
orst
retc
hes
3w
eeks
late
r;11
wee
ksla
ter
(3w
eeks
post
nata
lly);
3w
eeks
late
r(9
wee
kspo
stna
tally
)
Acu
punc
ture
–1,
5,10
,15
and
20m
in25
30(a
cupu
nctu
re)
trea
tmen
ttim
e(m
in)
max
imum
from
the
60(e
xerc
ise,
mas
sage
and
stre
tche
s)fif
thvi
sit
onw
ards
Stim
ulat
ion
–E
lect
roac
upun
ctur
eN
otsp
ecifi
edif
any
Man
uals
timul
atio
nev
ery
10m
in;
aton
est
age,
othe
rwis
est
imul
atio
nus
ed,
obta
inin
gde
qino
tst
ated
but
stat
edat
tem
ptm
ade
toel
icit
deqi
atpo
ints
Con
tinu
ed
Low back and pelvic girdle pain in pregnancy
� 2008 Acupuncture Association of Chartered Physiotherapists40

Ta
ble
1.
Con
tinu
ed
Stud
y
Var
iabl
eC
umm
ings
(200
3)Fo
rres
ter
(200
3)G
uerr
eiro
etal
.(2
004)
Eld
enet
al.
(200
5)
Tre
atm
ents
(n)
189
8–12
12(a
cupu
nctu
re)
6(e
xerc
ise)
1(a
dvic
e)
Nee
dlin
gte
chni
que
Perio
stea
lfac
etjo
int
need
ling,
‘‘Cla
ssic
al’’
acup
unct
ure
Tra
ditio
nala
cupu
nctu
reL
ocal
acup
unct
ure
poin
tsat
site
dry
need
ling
ofm
yofa
scia
lpo
ints
for
low
back
pain
and
usin
gcl
assi
cala
cupu
nctu
reof
loca
lsen
sitiv
itytr
igge
rpo
ints
‘‘seg
men
tald
ysfu
nctio
n’’
poin
ts
Ave
rage
poin
ts(n
)�
6–8
2,4,
6or
1012
(8st
anda
rdpo
ints
with
Loc
alin
divi
dual
sele
ctio
n�
4ad
ditio
nalp
oint
s)ac
cord
ing
todi
agno
stic
palp
atio
n:10
segm
enta
lpoi
nts
and
7ex
tra-
segm
enta
lpoi
nts
used
Mos
tco
mm
only
used
Lef
tL
5–S1
face
tjo
int;
Bila
tera
lpoi
nts:
KI1
3,SI
3;G
V20
;po
ints
bila
tera
lglu
teus
med
ius
BL
23,B
L25
,BL
57;
BL
62,B
L40
;bi
late
ralp
oint
s:(t
wo
poin
ts);
HT
Jpo
ints
atsi
mila
rle
vels
:T
E5,
GB
30,G
B4;
LI4
,BL
26,B
L32
,BL
54,B
L60
;bi
late
ralq
uadr
atus
L2,
L4
HT
Jpo
ints
KI1
1,G
B30
,SP1
2,ST
36,E
X21
lum
boru
m
Out
com
em
easu
res
Patie
ntsy
mpt
omre
port
ing
Pain
scor
e:V
AS
(0–1
00);
Pain
scor
e:N
RS
(0–1
0);
Pain
scor
e:V
AS
(0–1
00)
ever
yan
dge
nera
lrea
sses
smen
tsy
mpt
omre
port
ing
each
use
ofm
edic
atio
ns;
afte
rnoo
nan
dev
enin
g;fo
rtni
ght
func
tiona
lcap
acity
(0–1
0)ph
ysic
alre
asse
ssm
ent
for
gene
rala
ctiv
ities
,wal
king
and
wor
king
;bi
rth
wei
ghts
and
Apg
arsc
ores
Res
ults
No
stat
istic
alan
alys
isof
chan
ge;
No
stat
istic
alan
alys
isof
chan
ge;
Stat
istic
ally
sign
ifica
ntre
duct
ion
Red
uctio
nin
repo
rted
pain
intr
eatm
ent
stop
ped
atar
ound
VA
Sno
tst
ated
atth
ela
stin
acup
unct
ure
grou
p’s
pain
acup
unct
ure
grou
pco
mpa
red
to27
–29
wee
ksof
preg
nanc
yw
hen
trea
tmen
tdu
ring
preg
nanc
yle
vels
(P<0
.000
1);
educ
atio
n/SI
Jbe
ltgr
oup
(P<0
.001
);th
epa
tient
deci
ded
that
she
at33
wee
ks,a
lthou
ghth
ere
duce
dus
eof
para
ceta
mol
redu
ctio
nin
pain
inex
erci
segr
oup
was
com
fort
able
enou
ghto
patie
ntre
port
ed‘‘t
wo
bad
(P=
0.00
5);
com
pare
dto
educ
atio
n/SI
Jbe
ltgr
oup
cont
inue
with
out
trea
tmen
tda
ysin
2w
eeks
’’;im
prov
edfu
nctio
nalc
apac
ity(P
<0.0
4);
with
the
aid
ofcr
utch
espo
stna
talV
AS=
5–10
with
(P=
0.01
gene
rala
ctiv
ities
;no
stat
istic
aldi
ffer
ence
betw
een
inte
rmitt
ent
LB
Pon
liftin
g;P
<0.0
01w
ork
and
wal
king
)ac
upun
ctur
ean
dex
erci
segr
oups
;no
leg
pain
orcr
amps
No
diff
eren
cein
infa
ntm
easu
res
redu
ctio
nin
pain
mos
tpr
onou
nced
inth
eev
enin
gin
acup
unct
ure
grou
pat
revi
ewon
ew
eek
afte
ren
dof
trea
tmen
t
Sign
ifica
ntad
vers
eef
fect
sN
ilN
ilN
ilin
fem
ales
and
infa
nts
Nil
infe
mal
esan
din
fant
s
W. Koch
� 2008 Acupuncture Association of Chartered Physiotherapists 41

Guerreiro et al. (2004) measured outcomesincluding pain levels (score=0–10), the use ofmedication and self-reported functional capacityfor three areas of function (score=0–10). Stat-istically significant reductions were reported inthe acupuncture group with respect to pain andthe use of paracetamol. Statistically significantimprovements were also reported in this groupwith respect to functional capacity. Birth weightsand Apgar scores were similar between the twogroups. No adverse effects were reported ineither the subjects or their infants.
Elden et al. (2005) reported an extensivesingle-blind RCT in which 386 pregnant womenwith isolated PGP were randomly assigned toeither standard treatment (education, advice andsacroiliac belt), acupuncture (including standardtreatment) or stabilization exercises (includingstandard treatment with some individual massageand stretching). Prospective subjects wereexcluded if they had another pain condition,systemic disorders, multiple pregnancy or con-traindications to treatment.
Acupuncture treatment was determinedaccording to points of local sensitivity. Tensegmental and seven extrasegmental points wereused. Commonly used points included GovernorVessel (GV) 20, bilateral Large Intestine (LI) 4,BL26, BL32, BL54, BL60, KI11, GB30, Spleen(SP) 12, Stomach (ST) 36 and Extra Point 21.The outcome measures included reported painscores (VAS=0–100) and physical reassessmentby an independent examiner. The reportedresults included a statistically significant reduc-tion in pain for both the acupuncture and exer-cise groups compared to the standard treatmentgroup, but no statistical difference between theacupuncture and exercise groups, although theacupuncture group showed more positive out-comes. No adverse effects were reported ineither the subjects or their infants.
DiscussionOne major criticism regarding research in aclinical population relates to the use of smallsample sizes, which results in a lack of statisticalpower to detect change. With regard to thepresent literature review, the single case reportshad major limitations; however, these studiesreported the use of different forms of acupunc-
ture application and contribute to a growingbody of evidence describing the safe applicationof acupuncture in pregnancy. Guerreiro et al.
(2004) used a relatively small sample size, buttook the importance of power into considerationin their study; they were still able to detectstatistically significant changes between the treat-ment groups. Elden et al. (2005) also consideredstatistical power and ensured that their samplesizes were appropriate to achieve a 90% powerfor detecting a significant change.
All four studies varied widely in terms offrequency of treatment, the time for which thetreatment was provided and the acupuncturetechnique used. Not all of the authors consideredTCM principles in the selection of points. Allfour reports initially administered treatment on aweekly or fortnightly basis, but the times givenfor treatment varied significantly. All sessionslasted no longer than 30 min.
Current theories in acupuncture suggest thattreatment times of under 20 min predominantlyaffect local tissue and spinal cord mechanisms,whereas longer sessions begin to augment thecentral nervous system and neuroendocrine sys-tem. However, since there are so many physio-logical changes during pregnancy, it is unclearwhether this results in different levels of sensi-tivity and different responses to the varioussystems. This is evidently an area that requiresfurther research.
Notably, all the acupuncture treatmentsreported in the four studies involved more thansix sessions. Current research suggests that aminimum of six treatments is required to achievea positive result in treating chronic pain. To date,the number of sessions, and the time requiredfor treating acute episodes of pain and otherconditions (e.g. pregnancy) has not been studiedor documented thoroughly.
Interestingly, although Cummings (2003)administered the greatest number of treatmentsduring pregnancy, the efficacy of the acupunc-ture treatment is questionable because the sub-ject was also undertaking other forms oftherapy (e.g. chiropractic manipulation andexercises). Furthermore, the use of crutchesfrom 25 weeks’ gestation significantly reducedsymptoms and acupuncture treatment wasstopped. However, the inclusion of Cummings’(2003) case report in the present literature
Low back and pelvic girdle pain in pregnancy
� 2008 Acupuncture Association of Chartered Physiotherapists42

review is not intended to provide a comparisonwith the most effective treatment methods, butis meant to recognize that acupuncture duringpregnancy does not result in any knownadverse effects, and to document the pointsand techniques used.
Three out of the four articles described in thepresent literature review indicate that treatmentwas begun in the second trimester; however, nospecific reasoning for this decision is discussed inany of these articles. Cummings (2003) inadvert-ently treated a subject with acupuncture duringher pregnancy, although it was not known at thetime. Forrester (2003) acknowledged that it isusual practice to commence treatment once ahealthy pregnancy has been established and thefirst trimester is complete. He cited that 15% ofknown pregnancies result in spontaneous mis-carriage in the first trimester, and highlightedthat, because of concerns with litigation, clini-cians are wary of initiating a treatment during thefirst trimester since it could be blamed for anysubsequent miscarriage. However, treatment issometimes commenced with the subject’s fullinformed consent if the benefits of the treatmentoutweigh the risks involved.
There was also significant variation in thetreatment approach and amount of stimulationreported in the four papers. This probablyreflects the wide range of schools of acupuncturetraining and the variety of techniques utilized inthe clinical environment. Cummings (2003)adopted a dry needling/intramuscular and perio-steal needling approach, and also tried someelectroacupuncture, but he considered it lesseffective for this particular patient and returnedto vigorous manual acupuncture. However,details of the techniques and progression at eachsession are scant.
By comparison, Forrester (2003), Guerreiroet al. (2004) and Elden et al. (2005) selectedtraditional acupuncture points and someintended to elicit de qi. Ah Shi (tender) pointswere also used. Forrester (2003) clearly docu-mented that point selection had been based ontraditional acupuncture principles and conceptsof segmental innervation, and considered theconcept of ‘‘forbidden points’’ in pregnancy. Hemainly used a small selection of Bladder (BL23,BL25 and BL57) and corresponding HTJ pointsat the L2 and L4 levels. While these points are
commonly used in the general LBP population,TCM literature and the AACP FoundationAcupuncture Course guidelines (Pearce 2007)suggest that points over the lumbosacral areashould not be used during pregnancy because ofshared segmental innervation with the uterus,cervix and pelvis.
Guerreiro et al. (2004) did not provide clearreasoning for the points that they selected anddid not document all the points that were used.These authors indicated that the commonly usedpoints were KI3, SI3, BL62, BL40, TE5, GB30,GB 41 and HTJ points along the spine. Eldenet al. (2005) selected points according to localsensitivity following diagnostic palpation andindicated that they were trying to access thesegmental inhibition systems to provide painrelief.
A number of ‘‘forbidden points’’ in pregnancyare well documented in the literature (Dale1997). These points are largely based on a wealthof historical and authoritative literature, and varydepending on which text is consulted; however,there is currently little research evidence forthese directives. The ‘‘forbidden points’’ includethose over the abdomen, those with a strongeffect on the autonomic nervous system, thosewith shared segmental innervation with theuterus and cervix, and points that have report-edly been used to terminate pregnancies.Another example of TCM reasoning is the avoid-ance of the yin channels in the lower limbs.Some points are considered completely contrain-dicated, whilst others are considered appropriatefor moxibustion only. Certain points are con-traindicated until the pregnancy reaches aspecific milestone (e.g. 33 weeks for points usedto turn a breech presentation and 36 weeks forpoints associated with the induction of labour).The AACP Foundation Acupuncture Courseguidelines (AACP 2007) recommend that LI4,Lung 11, Liver (LV) 1, LV3, KI11, SP6, BL60,BL67, GV22 and GB21 are specifically avoidedduring pregnancy, in addition to normal TCM‘‘forbidden points’’.
Notably, Elden et al. (2005) used LI4 andBL60, which are considered to be contraindi-cated during pregnancy in TCM and AACPFoundation Acupuncture Course literature(Pearce 2007). These authors also used BL32 andST36, which are also points described by some
W. Koch
� 2008 Acupuncture Association of Chartered Physiotherapists 43

traditional sources as being ‘‘forbidden’’ duringpregnancy (Becke 1988, cited in Forrester 2003;Lian et al. 2005).
Large Intestine 4 is contraindicated duringpregnancy because strong manipulations havebeen reported to cause uterine contractions,although this point is used for analgesia in labour(Stux et al. 2003; Lian et al. 2005). Additionally,BL60 is contraindicated until a pregnancy is fullterm since it is also used in TCM to induce orincrease contractions during labour (Lian et al.
2005).Out of the four studies, only Forrester (2003)
reported reviewing TCM literature relating to‘‘forbidden points’’ in pregnancy (Table 2).Cummings (2003) alluded to concerns associatedwith spontaneous pregnancy loss and othercomplications of pregnancy that could be attrib-uted to acupuncture treatment, but he did notspecifically address the issue of ‘‘forbiddenpoints’’ in pregnancy in the paper. It is surprisingthat these points were not given due consider-ation in light of the paucity of quality researchdocumenting the safe use of acupuncture during
pregnancy for LBP and PGP, and the risksassociated with trialing treatments on a pregnantpopulation.
Notably, although Pericardium 6 is listed ascontraindicated in Table 2, this point has beenextensively studied in the management of nauseaand vomiting associated with pregnancy, and isnow considered to be safe and effective to use.Other points listed above have also been used invarious studies without adverse effects beingreported.
Interestingly, some other authors havereported needling a number of ‘‘forbiddenpoints’’ judiciously without observing anyadverse effects to the mother or unborn foetus(Becke 1988, as cited in Forrester 2003). Conse-quently, questions are now arising relating towhether points are completely or only relativelycontraindicated (i.e. appropriate for gentlemanipulation only) and further research isrequired in this area. In the four studies reviewedin the present paper, no adverse effects werereported relating to the women or their infants.
Other issuesThere are a number of difficulties associated withresearch into acupuncture. First, acupuncture isstill considered to be a ‘‘novel’’ treatment inWestern medicine, and in itself, this can create asignificant treatment effect regardless of thepoints used, the method of stimulation or theother treatment parameters that are selected.Consequently, studies that do not include a shamacupuncture group are often criticized and anysignificant results are dismissed as placeboeffects. However, it is very difficult forresearchers to deceive patients into believing thatthey have undergone an acupuncture treatmentthat penetrates the skin at specified sites whenthey have not. Additionally, even a gentle touchhas a physiological effect. Furthermore, it is alsoethically difficult to justify providing a sham orcontrol treatment that does not have a clinicaleffect to women who have need therapy during atime of immense change, especially when it iswell documented that there are treatments thatare effective in the management of PGP andLBP in pregnancy. As acupuncture becomesmore widely known, it is also difficult to find agroup of patients who are naïve about it.
Table 2. Forbidden points in pregnancy (cited by Forrester2003): (CV) Conception Vessel; (PC) Pericardium; (GB) GallBladder; (GV) Governor Vessel; (HTJ) Huatuojiaji; (KI) Kidney;(LI) Large Intestine; (LU) Lung; (LV) Liver; (SI) Small Intestine;(SP) Spleen; (ST) Stomach; (TE) Triple Energizer; (BL) Bladder;(T) Thoracic; (L) Lumbar; and (S) Sacral
Acupuncture points
CV2, CV3, CV4, CV5, CV6, CV7PC6, PC8GB2, GB9, GB21, GB34GV3, GV4, GV5, GV6, GV7All HTJ pointsKI1, KI2, KI4, KI7LI2, LI4, LI10LU7, LU11LV1SI7, SI10SP1, SP2, SP6, SP13, SP14ST4, ST12, ST24, ST25, ST36, ST45TE4, TE10BL60, BL67Points with shared segmental innervation to the uterus andcervix, i.e.:
T11, T12L1, L2S2, S3, S4
All leg and hand points, and low back, loin, and abdominalpoints, especially:
LI4,GB3, GB21, GB31ST25, ST30, ST36, ST44SP6KI3, KI6GV20
Low back and pelvic girdle pain in pregnancy
� 2008 Acupuncture Association of Chartered Physiotherapists44

Some of the control ‘‘treatments’’ described inthe articles reviewed in the present study werequestionable. Guerreiro et al. (2005) used para-cetamol and hyoscine as the control treatment;however, these authors did not provideevidence-based justification of this regimen as aneffective treatment for LBP and PGP in preg-nancy. Furthermore, some patients included intheir groups may have been averse to takingmedications during pregnancy because of per-ceived risks. However, Guerreiro et al. (2005)highlighted the ethical issue regarding the needto provide treatment for patients in a real-lifesituation, and justified their approach by explain-ing that both groups were offered medication asstandard treatment and acupuncture was addedto the standard treatment in the treatment group.
Elden et al. (2005) attempted to compare theeffect of recognized treatments used in the clini-cal setting; however, the treatments in thesegroups were not completely standardized. Theseauthors briefly documented that some patients inthe exercise group also received stretching andmassage, which confounds the results, but thismore accurately reflects the kind of multi-treatment approach commonly used in clinicalsettings. In this group, Elden et al. (2005) high-lighted that the manual treatment was onlyundertaken once weekly, whereas the main treat-ment (exercises) were performed at least daily.Surprisingly, although these authors stated thatprevious research highlighted that their standardtreatment including education and a SIJ belt isineffective, they opted to use this approach in thecontrol group. Elden et al. (2005) also concludedthat this was not an effective form of treatmentin the pregnancy population.
In the two case studies, both women were intheir first pregnancy. Elden et al. (2005) studiedwomen who were in different pregnancies (justover one-third in each group were in their firstpregnancy); however, Guereiro et al. (2004) didnot indicate whether women were in their first ora subsequent pregnancy. Since mechanical andhormonal influences are enhanced with eachsubsequent pregnancy, these factors may poten-tially also confound results. This was not high-lighted in the above authors’ discussion.
Overall, Cummings (2003) presented a rathernarrow discussion of the mechanics of applyingperiosteal needling in pregnancy, briefly high-
lighting that no adverse effects occurred, eventhough treatment had been unwittingly com-menced during the first trimester. In contrast,Forrester (2003) provided an extensive andwell-researched summary relating to safety risks,‘‘forbidden points’’, litigation and the evidencefor the number of treatment sessions, and high-lighted relative contraindications to acupuncturein pregnancy. Forrester (2003) also discussedpotential direct and indirect mechanisms (e.g.segmental, hormonal and autonomic systemschanges) during pregnancy. Guerreiro et al.
(2004) highlighted the limitations of not usingsham acupuncture, but discussed the ethical needto be providing some form of recognized treat-ment in a clinical population with a real-life need.There was only minimal discussion of the mecha-nisms of the treatment effects; Guerreiro et al.
(2004) focused on the results of their study dem-onstrating that no adverse effects occurred as aconsequence of acupuncture in pregnancy. Eldenet al. (2005) provided a brief discussion regardingthe effects of stabilizing exercise, the absence ofevidence for ‘‘standard’’ treatment, and the acu-puncture mechanisms and concepts of segmentalpain inhibition and the activation of central painsystems via endogenous opioid activation.
ConclusionsAlthough there are a few other papers describingthe use of acupuncture in pregnancy in additionto the four reviewed in the present study, it isapparent that further research regarding safepoints and the use of acupuncture in the man-agement of PGP and LBP needs to be under-taken. Because LBP and PGP are two differentpresentations that require different treatmentapproaches from the exercise and manual treat-ment standpoints, it may be clinically useful iffuture studies separate the two presentations intodifferent treatment groups in order to elucidate ifa different approach is required from an acu-puncture perspective. It may also be useful ifgroups of pregnant women are separated intofirst, second or subsequent pregnancies since thehormonal and mechanical responses to preg-nancy increase with each subsequent pregnancy,and the inclusion of a range of women indifferent pregnancies may confound results. Inaddition, further studies require significant
W. Koch
� 2008 Acupuncture Association of Chartered Physiotherapists 45

numbers of subjects and researchers must con-sider the statistical power of the sample size.Preferably, these studies should be RCTs; how-ever, case reports continue to add to the body ofliterature documenting the safe use of acupunc-ture in pregnancy.
Whilst the results of the studies discussed inthe present literature review cannot be extrapo-lated to the general population of pregnantwomen in the clinical setting, these four paperscontribute to the growing literature that suggeststhat acupuncture can be safely administeredduring pregnancy, given that the therapist hasadequate training and knowledge of its use.Although some aspects of the methodologiesand discussions can be criticized, the four studieschallenge the historical beliefs that some pointsare absolutely contraindicated during pregnancy.Some of the papers also highlighted that furtherresearch is required to establish safe parametersfor stimulation and length of time for treatment.These findings are further supported by a recentextensive Cochrane review of RCTs relating tointerventions for preventing and treating LBP inpregnancy that concluded that, although furtherhigh-quality research was required, the indica-tions were that acupuncture was useful in themanagement of PGP and LBP in pregnancy(Pennick & Young 2007).
AcknowledgementsI would like to thank Lynn Pearce, my tutor onthe Foundation Course in Acupuncture that Iattended at Westminster Primary Care Trust,London, UK, in October–November 2007.
ReferencesAssociation of Chartered Physiotherapists in Women’s
Health (ACPWH) (2007a) Pregnancy-Related Pelvic Girdle
Pain. [WWW document.] URL http://www.acpwh.org.uk/docs/ACPWH-PGP_HP.pdf
Association of Chartered Physiotherapists in Women’sHealth (ACPWH) (2007b) ACPWH guidance on thesafe use of transcutaneous electrical nerve stimulation(TENS) for musculoskeletal pain during pregnancy.Journal of the Association of Chartered Physiotherapists in
Women’s Health 101, 102–105.Becke H. (1988) Dangerous acupuncture points in preg-
nancy. Deutsche Zeitschrift für Akupunktur 31 (5), 110–111.Berg G., Hammar M., Möller-Nielsen J., Lindén U. &
Thorblad J. (1988) Low back pain during pregnancy.Obstetrics and Gynecology 71 (1), 71–75.
Björklund K. & Bergström S. (2000) Is pelvic pain inpregnancy a welfare complaint? Acta Obstetricia et Gyneco-
logica Scandinavica 79 (1), 24–30.Cummings M. (2003) Acupuncture for low back pain in
pregnancy. Acupuncture in Medicine 21 (1–2), 42–46.Dale R. A. (1997) The contraindicated (forbidden) points
of acupuncture for needling, moxibustion and preg-nancy. American Journal of Acupuncture 25 (1), 51–57.
Elden H., Ladfors L., Olsen M. F., Östgaard H.-C. &Hagberg H. (2005) Effects of acupuncture and stabilis-ing exercises as adjunct to standard treatment in preg-nant women with pelvic girdle pain: randomised singleblind controlled trial. British Medical Journal 330 (7494),761–765.
Fast A., Shapiro D., Ducommun E. J., et al. (1987)Low-back pain in pregnancy. Spine 12 (4), 368–371.
Forrester M. (2003) Low back pain in pregnancy. Acupunc-
ture in Medicine 21 (1–2), 36–41.Furlan A. D., van Tulder M. W., Cherkin D. C., et al. (2004)
Acupuncture and dry-needling for low back pain.Cochrane Database of Systematic Reviews 2004, Issue 4. Art.No.: CD001351. DOI: 10.1002/14651858.CD001351.pub2.
Guerreiro da Silva J. B., Nakamura M. U., Cordeiro J. A. &Kulay L., Jr (2004) Acupuncture for low back pain inpregnancy – a prospective, quasi-randomised, controlledstudy. Acupuncture in Medicine 22 (2), 60–67.
Karavis M. (1997) The neurophysiology of acupuncture: aviewpoint. Acupuncture in Medicine 15 (1), 33–42.
Kristiansson P., Swärdsudd K. & von Schoultz B. (1996)Back pain during pregnancy: a prospective study. Spine
21 (6), 702–709.Lian Y.-L., Chen C.-Y., Hammes M. & Kolster B. C.
(2005) The Pictorial Atlas of Acupuncture: An Illustrated
Manual of Acupuncture Points. Könemann Verlagsgesell-schaft, Cologne.
MacEvilly M. & Buggy D. (1996) Back pain and pregnancy:a review. Pain 64 (3), 405–414.
Manheimer E., White A., Berman B., Forys K. & Ernst E.(2005) Meta-analysis: acupuncture for low back pain.Annals of Internal Medicine 142 (8), 651–663.
Östgaard H.-C., Andersson G. B. J. & Karlsson K. (1991)Prevalence of back pain in pregnancy. Spine 16 (5),549–552.
Östgaard H.-C., Zetherström G., Roos-Hansson E. &Svanberg B. (1994) Reduction of back and posteriorpelvic pain in pregnancy. Spine 19 (8), 894–900.
Pearce L. (2007) Acupuncture Association of Chartered Physio-
therapists Foundation Acupuncture Manual. Acupuncture As-sociation of Chartered Physiotherapists, Peterborough.
Pennick V. E. & Young G. (2007) Interventions forpreventing and treating pelvic and back pain in preg-nancy. Cochrane Database of Systematic Reviews 2007, Issue3. Art. No.: CD001139. DOI: 10.1002/14651858.CD001139.pub2.
Perkins J., Hammer R. L. & Loubert P. V. (1998) Identi-fication and management of pregnancy-related low backpain – a common, treatable cause of low-back pain inpregnancy. Journal of Nurse-Midwifery 43 (5), 331–340.
Low back and pelvic girdle pain in pregnancy
� 2008 Acupuncture Association of Chartered Physiotherapists46

Stux G., Berman B. & Pomeranz B. (eds) (2003) Basics of
Acupuncture, 5th edn. Springer-Verlag, Berlin.Wu W. H., Meijer M. O., Uegaki K., et al. (2004)
Pregnancy-related pelvic girdle pain (PPP), I: terminol-ogy, clinical presentation and prevalence. European Spine
Journal 13 (7), 575–589.
Wendy Koch graduated as a Bachelor of Applied Science
(Physio) with First-Class Honours from the University
of South Australia in 1996. She has spent more than a
decade working in musculoskeletal physiotherapy, and
over the past 9 years, has further specialized in the
management of musculoskeletal disorders during preg-
nancy and the postnatal phase, providing individual
treatments, and running pregnancy and postnatal aqua-
natal and Pilates classes in Australia and the UK.
Since moving to the UK in 2006, Wendy has also
pursued an interest in acupuncture, and its application in
the management of musculoskeletal and women’s health
disorders. She undertook the AACP Foundation Acu-
puncture Course with Lynn Pearce in 2007, and
completed specific training in the use of acupuncture in
women’s health with Professor Elisabet Stenin-Victorin
and Dr Panos Barlas in 2008. This review was
undertaken as part of the requirement for completion of
the Foundation Acupuncture Training Course. Wendy
is currently working in private practice for Pilates
Art Physiotherapy and London Sports Medicine in
Wimbledon Village, London.
W. Koch
� 2008 Acupuncture Association of Chartered Physiotherapists 47


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 49–52
BRIEF LITERATURE REVIEW
Acupuncture in cardiology
Val HopwoodHealth and Life Sciences, Coventry University, Coventry, UK
AbstractAcupuncture is not usually associated with cardiology, but when the physiological mechanismsthrough which acupuncture is thought to work are carefully examined, the possibility emerges.This paper discusses some speculative ideas that explore how acupuncture might work in thiscontext, and more specifically, in the field of stroke.
Keywords: acupuncture, cardiology, stroke.
IntroductionAcupuncture is not usually associated with car-diology by anyone other than an acupuncturepractitioner. However, when the physiologicalmechanisms through which acupuncture isthought to work are carefully examined, thepossibility emerges.
Acupuncture is best defined as a potent formof sensory stimulation. It is derived from thetraditional Chinese medicine (TCM) paradigm,and associated with ideas about life force, and yinand yang. However the acupoints are chosen,whether by Chinese tradition and their positionon an acupuncture meridian, or Western theoriesof segmental distribution, the insertion of aneedle into the skin and underlying tissues pro-duces a clear pattern of afferent responses inperipheral nerves.
The basic science of acupuncture has beensubject to much research with regard to itsanalgesic effect, and the studies have mainlyexamined the effect of acupuncture on the cen-tral, peripheral and autonomic nervous systems,together with related neurohumoral effects andchanges in blood biochemicals. Other effects,such as those on the vascular system, have alsobeen investigated, but not to such a great extent.
The first research studies looked at the effect
of acupuncture on the nervous system, and themodel proposed by Pomeranz (1996) indicatedjust how acupuncture could affect this system,increasing the secretion of neuropeptides andmonoamines in the bloodstream or cerebrospinalfluid. These include the endorphins, enkephalins,dynorphins, serotonin and epinephrines. In hispresentations and publications, Bruce Pomeranzhas documented 17 convergent lines of evidencesupporting the claim that acupuncture releasesendorphins, producing acupuncture analgesia,which is naloxone reversible (Pomeranz 1996).This work played a major part in convincingthe Consensus Development Conference of theNational Institutes of Health in the USA of thescientific credibility of acupuncture for pain reliefin 1997 (NIHCDPA 1998).
While we have a relatively good understandingof how acupuncture may work in pain, ourunderstanding of the overall effects is far morefragmented. We are aware that acupuncture maybe having an effect on the circulation in general,including both the microcirculation and thecerebral circulation. We are also aware thatacupuncture may influence recovery from neuro-logical damage, and may have direct effects onmuscle tissue as well as mood (Ludwig 2000;Mukherjee et al. 2007).
However, there is no coherent physiological orimmunological theory that unites these variousdisparate observations. Furthermore, much ofthe research in this area is limited and has notbeen reproduced independently; some of the
Correspondence: Dr Val Hopwood FCSP, Acupuncture
MSc Course Director, Health and Life Sciences, Coventry
University, Priory Street, Coventry CV1 5FB, UK
(e-mail: [email protected]).
� 2007 Sovereign Publications 49

science, particularly from the Chinese studies, isvery poor. The following are some speculativeideas that explore how acupuncture might beworking in the context of cardiology, and morespecifically, the field of stroke.
General circulationThe Chinese have long claimed that acupunctureproduces changes in circulation, but tend toassert that these are only a normalization pro-cess, restoring the characteristics of healthy cir-culation both in mechanical flow and the state ofthe blood cells. Research into acupuncture andthe cardiovascular system has the advantage thatthis system is capable of reliable and relativelyconvenient monitoring.
It has been remarked that patients frequentlycomment that they feel warm after acupuncture(Filshie & White 1998). Indeed, Cao et al. (1983),measuring changes in skin temperature andassessing blood flow by finger plethysmography,suggested that patients who responded to acu-puncture analgesia tended to show a measurableincrease in the skin temperature of the palms.
Some recent work on acupuncture for reflexsympathetic dystrophy has investigated thereported sensation of warmth when acupunctureis given for this condition (Bar et al. 2002). Tenhealthy age- and sex-matched patients were usedas controls. The 10 patients received acupunc-ture to the affected limb. The participants in thecontrol group were matched for limb and side.Blood flow was measured by duplex sonographyof either the brachial of the femoral arterybefore, during and after the third session ofacupuncture. Ten treatments were given in total.Blood flow increased significantly in the patients’affected limbs compared with their untreated(unaffected limb). All but one patient reportedimproved symptoms. Interestingly, only animprovement in subjective function, not subjec-tive pain, was positively correlated with theincrease in blood volume flow.
HypertensionHypertension has also been investigated inhuman subjects by several researchers, one of theearliest being Tam & Yiu (1975). In this study,28 patients with essential hypertension were
treated with acupuncture. Sixteen showed excel-lent improvement in terms of the lowering ofblood pressure to normal and the disappearanceof original symptoms. Eight had moderateimprovement and four showed no response. Theresults of treatment seem to indicate thatimprovement is closely related to the durationof disease and history of drug treatment. Theselection of acupuncture loci, and the techniquesof needle insertion and manipulation were dis-cussed in detail, but there was no controlgroup. Also, the descriptions of the results as‘‘excellent’’, ‘‘moderate’’ etc. are not sufficientlyobjective to draw any definite conclusions.
A more rigorous recent study (Ballegaard et al.
1993) found that acupuncture tends to regulateresponses towards the norm, i.e. high bloodpressure is lowered, possibly because of therelease of endorphins and serotonin, and raisedwhen it is low, possibly through the release ofcentral acetylcholine and vasopressin. Ballegaardet al.’s (1993) results were highly significant incomparison to placebo. This type of finding alsotends to support the original Chinese theory thatacupuncture has no effect in a healthy person.Also, the influence of acupuncture on the auto-nomic nervous system is reflected in heart ratevariability, depending on the site of stimulation(Haker et al. 2000).
A very recent trial (Flachskampf et al. 2007)showed that acupuncture according to traditionalChinese medicine theories significantly loweredmean 24-h ambulatory blood pressure in patientswith uncomplicated arterial hypertension. How-ever, the effect disappeared after the 6 weeks ofacupuncture treatment.
There is a lot of interest in research circles, andthe use of acupuncture as an adjunctive therapyfor essential hypertension is being carefullyexamined (Yin et al. 2007). Yin et al. (2007)integrated acupuncture with conventional phar-maceutical therapy, lifestyle management, easy-walking and breathing exercises, and suggestedthat a modulation of the autonomic nervoussystem is the primary mechanism responsible fortheir good results.
Ear acupunctureAuricular acupuncture has also been shown tohave an effect on blood pressure by Gaponjuk &
Acupuncture in cardiology
� 2007 Sovereign Publications50

Sherkovina (1994). In a study of 104 patients bythe above authors, the haemodynamic influenceof each of 16 pairs of auricular acupuncturepoints was observed in hypertensive patients.Changes in heart rate, stroke output and periph-eral vascular resistance were measured, so thatthe degree of change could be charted for eachacupuncture point. It became clear that certaingroups of ear points induced a fall in bloodpressure by influencing changes in one or moreof these cardiac perimeters.
The ear has a particularly rich nerve supplyderived from several cranial and upper cranialnerves, and it is possible to explain the hypoten-sive action of specific groups of acupuncturepoints by reference to their innervation.Branches of the trigeminal, facial, glossopharyn-geal, vagus and cervical nerves are all present onthe ear surface. Gaponjuk & Sherkovina (1994)claimed that the most effective auricular acu-puncture points for hypertensive patients couldthus be accurately predicted.
StrokeAn important clinical result of this work is thepossibility of stroke prevention. By loweringblood pressure (Yin et al. 2007), decreasingviscosity (Jiao et al. 1992) and increasing the rateof blood flow (Yuan et al. 1998), the likelihood ofstroke should be diminished.
Perhaps surprisingly, TCM ideas about thecauses of stroke have a lot in common withWestern medicine. While the primary cause ofstroke is believed to be an uncontrolled andcatastrophic rush of pathological heat to thebrain, the reasons for this include a poor diet,with too much rich or fatty food, excess alcohol,decreased activity, and general stress.
There have been several recent controlledtrials of acupuncture as a treatment after stroke,the best of which were analysed in a Cochranereview by Zhang et al. (2005). Their main find-ings were that, in spite of no significant differ-ence between acupuncture and the controlinterventions, fewer deaths occurred in the acu-puncture groups. There has been some sugges-tion that a greater percentage of stroke survivorstreated with acupuncture return to, or remain in,their own homes (Hopwood & Lewith 2005).Whether this is the result of an increase in
motivation and a decrease in the widely recog-nized problem of post-stroke depression is hardto say.
Some researchers have indicated that theremight be an increase in muscle strength and adecrease in spasticity, particularly in the earlystages of recovery (Park et al. 2005; Mukherjeeet al. 2007; Hopwood et al. 2008). Others haveclaimed an improvement in well-establishedsymptoms of physical disability with increasedfunctional movement after several years (Naeseret al. 1994). Most dramatically, a study publishedrecently (Schaechter et al. 2007) indicated thatthere is a positive correlation between changes infunction of the affected upper limb (spasticityand range of motion) and activation in a regionof the ipsilesional motor cortex, perhaps indicat-ing that acupuncture may improve function ofthe affected upper limb in chronic hemipareticstroke patients by this mechanism.
Further large, well-controlled studies areneeded to confirm this, but clinicians are agreedthat the potential for acupuncture to increasephysical recovery from stroke is worth seriousinvestigation. The Chinese, of course, will saythat they have known this for years.
ReferencesBallegaard S., Muteki T., Harada H., et al. (1993) Modula-
tory effects of acupuncture on the cardiovascular system:a cross-over study. Acupuncture and Electro-Therapeutics
Research 18 (2), 103–115.Bar A., Li Y., Eichlisberger R., Angst F. & Aeshlimann A.
(2002) Acupuncture improves peripheral perfusion inpatients with reflex sympathetic dystrophy. Journal of
Clinical Rheumatology 8 (1), 6–12.Cao X.-D., Xu S.-F. & Lu W.-X. (1983) Inhibition of
sympathetic nervous system by acupuncture. Acupuncture
and Electro-Therapeutics Research 8 (1), 25–35.Filshie J. & White A. (eds) (1998) Medical Acupuncture:
A Western Scientific Approach. Churchill Livingstone,Edinburgh.
Flachskampf F. A., Gallasch J., Gefeller O., et al. (2007)Randomized trial of acupuncture to lower blood press-ure. Circulation 115 (24), 3121–3129.
Gaponjuk P. J. & Sherkovina T. J. (1994) The clinical andphysiological foundation of auricular acupuncturetherapy in patients with hypertensive disease. Acupuncture
in Medicine 12 (1), 2–5.Haker E., Egekvist H. & Bjerring P. (2000) Effect of
sensory stimulation (acupuncture) on sympathetic andparasympathetic activities in healthy subjects. Journal of
the Autonomic Nervous System 79 (1), 52–59.
V. Hopwood
� 2007 Sovereign Publications 51

Hopwood V. & Lewith G. T. (2005) Does acupuncturehelp stroke patients become more independent? Journal
of Alternative and Complementary Medicine 11 (1), 175–177.Hopwood V., Lewith G. T., Prescott P. & Campbell M. J.
(2008) Evaluating the efficacy of acupuncture in definedaspects of stroke recovery: a randomized, placebo-controlled, single-blind study. Journal of Neurology 255, inpress.
Jiao X., Chang X., Yin K. & Gao Y. (1992) Clinical andexperimental studies on acupuncture therapy of stroke-related blood stasis. International Journal of Clinical Acu-
puncture 3 (3), 231–241.Ludwig M. (2000) Einfluss der Akupunktur auf die
Leistungsfähigkeit der Quadrizepsmuskulatur. [Influenceof acupuncture on the performance of the quadricepsmuscles.] Deutsche Zeitschrift für Akupunktur 43 (2), 104–107. [In German.]
Mukherjee M., McPeak L. K., Redford J. B., Sun C. & LiuW. (2007) The effect of electro-acupuncture on spastic-ity of the wrist joint in chronic stroke survivors. Archives
of Physical and Medical Rehabilitation 88 (2), 159–166.Naeser M. A., Alexander M. P., Stiassny-Eder D., Lannin
L. N. & Bachman D. (1994) Acupuncture in thetreatment of hand paresis in chronic and acute strokepatients – improvement observed in all cases. Clinical
Rehabilitation 8 (2), 127–141.NIH Consensus Development Panel on Acupuncture
(NIHCDPA) (1998) Acupuncture. Journal of the American
Medical Association 280 (17), 1518–1524.Park J., White A. R., James M. A., et al. (2005) Acupuncture
for subacute stroke rehabilitation. Archives of Internal
Medicine 165 (17), 2026–2031.Pomeranz B. (1996) Scientific research into acupuncture
for the relief of pain. Journal of Alternative and Complemen-
tary Medicine 2 (1), 53–60.
Schaechter J. D., Connell B. D., Stason W. B., et al. (2007)Correlated change in upper limb function and motorcortex activation after verum and sham acupuncture inpatients with chronic stroke. Journal of Alternative and
Complementary Medicine 13 (5), 527–532.Tam K.-C. & Yiu H.-H. (1975) The effect of acupuncture
on essential hypertension. American Journal of Chinese
Medicine 3 (4), 369–375.Yin C., Seo B., Park H. J., et al. (2007) Acupuncture, a
promising adjunctive therapy for essential hypertension:a double-blind, randomized, controlled trial. Neurological
Research 29 (Suppl. 1), S98–S103.Yuan X., Hao X., Lai Z., Zhao H. & Liu W. (1998) Effects
of acupuncture at Fengchi point (GB 20) on cerebralblood flow. Journal of Traditional Chinese Medicine 18 (2),102–105.
Zhang S. H., Liu M., Asplund K. & Li L. (2005) Acupunc-ture for acute stroke. Cochrane Database of Systematic
Reviews 2005, Issue 2. Art. No.: CD003317. DOI:10.1002/14651858.CD003317.pub2.
Dr Val Hopwood FCSP is the Course Director of the
Acupuncture MSc at Coventry University and is also
an Honorary Research Fellow at the University of
Southampton. She has written a wide variety of publica-
tions, including both books and scientific papers. Val was
Chair of the AACP from 1997 to 2003. She was
awarded a Chartered Society of Physiotherapy Fellowship
in 2000 for services to acupuncture education.
This article is reprinted from The National Associ-ation of Primary Care Review by kind permission of
Sovereign Publications. Original publication: TheNAPC Review, Summer 2007, pp. 37–39.
Acupuncture in cardiology
� 2007 Sovereign Publications52

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 53–60
CASE REPORT
Treatment of cervical and posterior shoulder pain in a57-year-old female with conventional physiotherapy andWestern acupuncture
Lotte SkjodtDepartment of Physiotherapy, Addenbrooke’s Hospital, Cambridge, UK
AbstractThe case of a 57-year-old female with predominantly centrally evoked cervical and posteriorshoulder pain is described. The primary outcome measure was the Numerical Rating Scale; thesecondary outcome measures were the Neck Disability Index (NDI), cervical range of movementand intake of co-codamol. The treatment modalities were conventional physiotherapy andWestern acupuncture. The results show that the subject’s pain score improved by 5 points, whichis considered to be clinically significant. There was no clinical improvement in the NDI score, butthe intake of analgesia decreased by 33% and the patient achieved full range of movement.
Keywords: manual therapy, neck pain, physiological mechanisms, Western acupuncture.
IntroductionThe present case study describes a 57-year-oldfemale who was referred to the Departmentof Physiotherapy, Addenbrooke’s Hospital, Cam-bridge, UK, by the Rheumatology Department.She presented in December 2007 with a history ofneck and bilateral posterior shoulder pain, as wellas depression. The subject’s symptoms had begungradually approximately 12 months before, coin-ciding with problems at her place of employment:she reported that ‘‘work wants to finish me off’’.In the previous year, her local occupational healthteam had recommended light duties, but the painand severity of her symptoms persisted.
The subject’s past medical history consisted ofa troublesome left knee and mild bilateral carpaltunnel syndrome.
Case report
Subjective presentationThe initial physiotherapy assessment tookplace in February 2008. The subject’s pain had
worsened since her referral, and additionally, shecomplained of intermittent bouts of dizziness.She also reported intermittent headaches thatwere apparently unrelated to her neck and shoul-der pain. The subject thought these could bestress-induced. Further questioning revealed thatshe felt hot and sweaty, although her urineoutput was normal. The subject described herselfas ‘‘not feeling well’’ and ‘‘a wreck’’, and men-tioned that she had a tendency to pull her hairout.
A body chart identifying the anatomicallocations and providing descriptions of the sub-ject’s various types of pain is shown in Figure 1.Table 1 lists the factors that either aggravated oralleviated the pain. Table 2 details the course ofher pain during the day. At night, the subjectpreferred to sleep on either side with one good-sized pillow under her head, and complained ofintermittent sleep disturbance.
In terms of medication, the subject used10 mg of amitriptyline at night to help with thesleep disturbance, co-codamol (paracetamol andcodeine) six times a day for pain relief, andetodolac, a non-steroidal anti-inflammatory drug.
She had worked as a care assistant in a daycentre for 25 h a week since 1986. Her duties
Correspondence: L. Skjodt MCSP SRP, Department of
Physiotherapy, Addenbrooke’s Hospital, Hills Road,
Cambridge, Cambridgeshire CB2 0QQ, UK (e-mail:
� 2008 Acupuncture Association of Chartered Physiotherapists 53
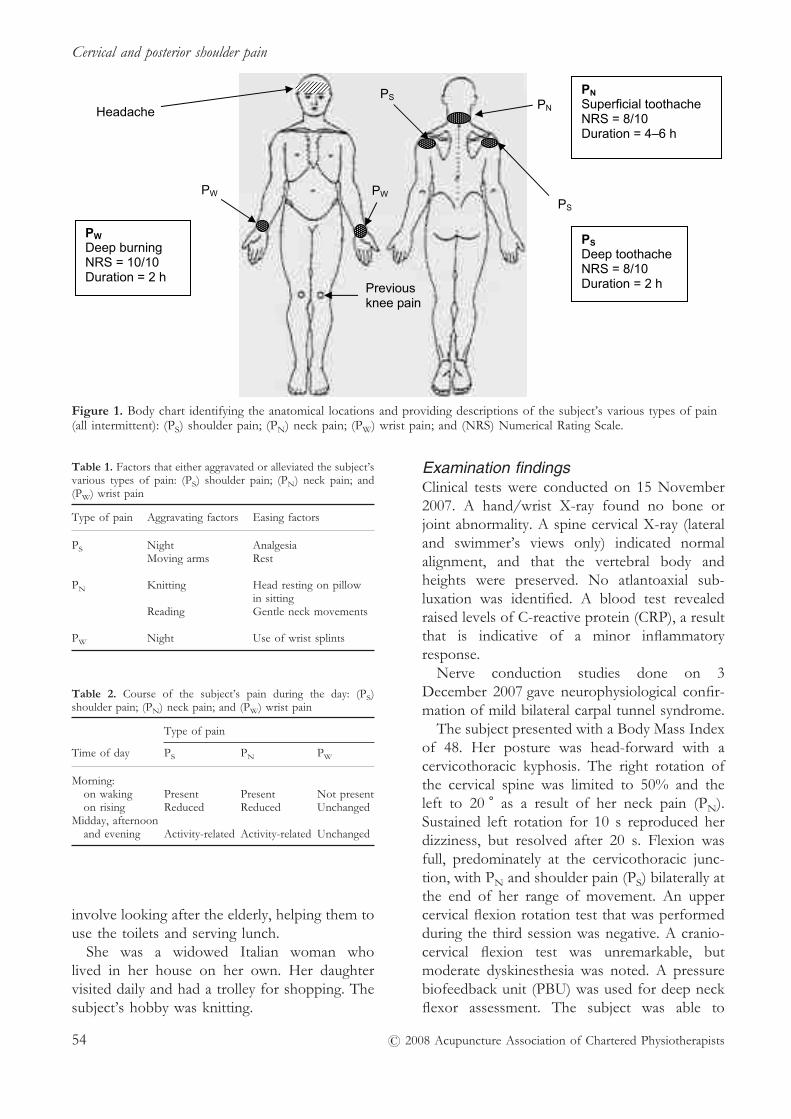
involve looking after the elderly, helping them touse the toilets and serving lunch.
She was a widowed Italian woman wholived in her house on her own. Her daughtervisited daily and had a trolley for shopping. Thesubject’s hobby was knitting.
Examination findingsClinical tests were conducted on 15 November2007. A hand/wrist X-ray found no bone orjoint abnormality. A spine cervical X-ray (lateraland swimmer’s views only) indicated normalalignment, and that the vertebral body andheights were preserved. No atlantoaxial sub-luxation was identified. A blood test revealedraised levels of C-reactive protein (CRP), a resultthat is indicative of a minor inflammatoryresponse.
Nerve conduction studies done on 3December 2007 gave neurophysiological confir-mation of mild bilateral carpal tunnel syndrome.
The subject presented with a Body Mass Indexof 48. Her posture was head-forward with acervicothoracic kyphosis. The right rotation ofthe cervical spine was limited to 50% and theleft to 20 � as a result of her neck pain (PN).Sustained left rotation for 10 s reproduced herdizziness, but resolved after 20 s. Flexion wasfull, predominately at the cervicothoracic junc-tion, with PN and shoulder pain (PS) bilaterally atthe end of her range of movement. An uppercervical flexion rotation test that was performedduring the third session was negative. A cranio-cervical flexion test was unremarkable, butmoderate dyskinesthesia was noted. A pressurebiofeedback unit (PBU) was used for deep neckflexor assessment. The subject was able to
Figure 1. Body chart identifying the anatomical locations and providing descriptions of the subject’s various types of pain(all intermittent): (PS) shoulder pain; (PN) neck pain; (PW) wrist pain; and (NRS) Numerical Rating Scale.
Table 1. Factors that either aggravated or alleviated the subject’svarious types of pain: (PS) shoulder pain; (PN) neck pain; and(PW) wrist pain
Type of pain Aggravating factors Easing factors
PS Night AnalgesiaMoving arms Rest
PN Knitting Head resting on pillowin sitting
Reading Gentle neck movements
PW Night Use of wrist splints
Table 2. Course of the subject’s pain during the day: (PS)shoulder pain; (PN) neck pain; and (PW) wrist pain
Type of pain
Time of day PS PN PW
Morning:on waking Present Present Not presenton rising Reduced Reduced Unchanged
Midday, afternoonand evening Activity-related Activity-related Unchanged
Cervical and posterior shoulder pain
� 2008 Acupuncture Association of Chartered Physiotherapists54

achieve a pressure of 24 mmHg, and the PBUwas then selected as a training tool. Combinedmovements were not performed because sheshowed signs of vertebrobasilar insufficiency andmoderate irritability.
Furthermore, the subject had full range ofmovement (ROM) of the shoulders, with nodefinite rotator cuff signs. A neurological exami-nation was unremarkable, and upper limbtension test (ULTT) 1 and ULTT2a reproducedher wrist pain (PW) at the end of her range ofmovement, but with no change during sensitiza-tion. Motion palpation confirmed hypomobilityin cranial nerve 7 (C7), and thoracic spinal nerve1 (T1) and T2; PN and PS manifested onpalpation. Both Phalen’s test and Tinel’s signwere positive bilaterally, and Adson’s test wasnegative.
The Numerical Rating Scale (NRS) is a vali-dated tool that is used to obtain verbal reportsabout pain levels. Pain is recorded on a 10-pointscale: (0) no indication of pain; (10) worst painimaginable (Paice & Cohen 1997).
The Neck Disability Index (NDI), which thesubject completed during her second visit, gave ascore of 20. The NDI is a validated, disease-specific quality-of-life measurement. Each of the10 items is scored from 0 to 5: the maximumscore of 50 indicates the worst level of disability;a score of between 15 and 24 suggests moderatedisability (Vernon & Mior 1991).
Clinical reasoning for acupunctureAcupuncture is commonly used to treat PN
(Wadlow & Peringer 1996). In a recent study ofthe reduction of PN, Western acupuncture wasreported to be statistically significantly moreeffective than placebo at both 5 and 12 weeks(White et al. 2004). Because of the clinicalpresentation of the symptoms, acupuncture wasdeemed to be an appropriate choice of treatmentin this case.
The present author postulated that the sub-ject’s most dominant pain mechanism was thatof centrally evoked pain because of the longevityof her symptoms, which had continued longafter tissue healing would have been expected tooccur (Gifford & Butler 1997). Other symptomsthat she experienced included hypervigilance,and sympathetic changes, such as sweating and
feeling hot, which are also indicative of centrallymaintained pain (CMP). Acupuncture has beenshown to be an effective treatment for CMP.
Another feature of CMP that was evident wasthe inflammatory response demonstrated by thesubject’s raised levels of CRP. The sympatheticnervous system (SNS) is thought to contribute toinflammation via activation of the lateral sympa-thetic horn in the spinal cord or by a centrallymediated autonomic response, which could con-tribute to this type of pain (Coderre et al. 1993).The raised levels of CRP, and the subject’ssymptoms of heat and sweating can all be treatedwith etodolac, a non-steroidal anti-inflammatorydrug (Mehta 2007).
The subject also complained of mood andsleep disturbance. However, she reported that afull dose of amitriptyline caused her to experi-ence dizziness. Amitriptyline is known to causeblood pressure to drop when an individualmoves from a lying or sitting position to sittingor standing (Mehta 2007). This is experienced asdizziness or unsteadiness, and is a well-documented side effect of this medication. Acu-puncture could alleviate these symptoms since ithas been demonstrated to release neurochemicalsin the brain that may regulate mood and sleep.
There was also a mechanical nociceptive com-ponent to the subject’s pain, as demonstrated bythe intermittent nature of the PN and PS, whichwere aggravated by forward head postures, thebiomechanical fault in the excessive cervico-thoracic kyphosis, and the lack of motor control.Acupuncture has been shown to be effective inthe treatment of nociceptive pain (Lundeberget al. 1988). The burning sensation in herwrists, which was caused by mild carpal tunnelsyndrome, was another neurogenic component.
Acupuncture began to capture the popularimagination in the West in the early 1970s, and itis now one of the most widely used alternativemedical interventions (Kaptchuk 2002). Acu-puncture is a relatively quick treatment to whichpatients are generally well disposed, and it cancomplement conventional physiotherapy.
After the initial assessment and an explanationof acupuncture, the present subject consentedto acupuncture treatment. The acupuncturepoints employed at each treatment session andthe rationale for their use are shown in Tables 3and 4.
L. Skjodt
� 2008 Acupuncture Association of Chartered Physiotherapists 55

The other treatment modalities that were usedincluded oscillatory physiological movements ofthe cervical and upper thoracic spine, PBU,
proprioceptive exercises for the rectus capitismuscules, and taping.
Physiological reasoning for acupuncturepoint selectionAcupuncture with manual stimulation via theneedles is an effective way to initiate nerveimpulses and the activation of the endogenousantinociceptive system (Alied Training 2005).De qi a sign of the activation of the presumedthin myelinated A� fibres that is experienced as afeeling of heaviness and numbness, a sensationsimilar to the deep muscle pain that is experi-enced when muscles points are stimulated(Andersson 1993).
However, acupuncture is thought to stimulatemany descending inhibitory systems from thebrain. These include diffuse noxious inhibitorycontrols, descending pathways from the arcuatenucleus in the hypothalamus and the control ofthe autonomic nervous system (Bradnam 2003,2007). A study by Melzack & Wall (1984) dem-onstrated that an injection of morphine or elec-trical stimulation of the periaqueductal greymatter in animals inhibits noxious stimuli atspinal cord level. Nerve fibres descend to thenucleus raphe magnus in the medulla oblongata,which sends its axons to the substantia gelati-nosa. This activation acts on the serotoninergic
Table 3. Acupuncture points used at each treatment session: (GB) Gall Bladder; (LI) Large Intestine; (BL) Bladder; (GV) Governor Vessel;(Ex-HN) Yintang; (SI) Small Intestine; (LV) Liver; (PC) Pericardium; (SP) Spleen; (B) bilateral; (R) right; (L) left; (NG) needle grasp; (PN)neck pain; (PS) shoulder pain; (PW) wrist pain; (CF) cervical flexion; and (T12) thoracic spinal nerve 12
Treatmentsession Acupuncture point De qi Outcome Adverse effect
1 GB20, GB34 (B) Yes PN, PS, PW=0/10 NoneLI4 (B) Yes CF √√BL10, BL11 (B) Yes Feels heavyGV14 NoShenmen* Self-stimulated
2 GB20, GB21, GB34 (B) Yes (NG) PN, PS, PW=0/10 NoneLI4 (B) Yes CF √√BL10, BL11 Yes Feels coolGV14 No
3 ‘‘Four gates’’ Yes PN, PS, PW=0/10 NoneEx-HN3 No CF
Feels relaxed
4 SI3 (R) Yes PN pull to T12 Bruise [LV3 (R)]BL62 (B) Yes PS, PW=0/10LV3 (B) Yes (R)/no (L) No headachePC6 (R) Yes CF full,LI4, LI11 Yes pulling sensationSP6 No Feels relaxed
*Ear.
Table 4. Acupuncture point rationale (Alied Training 2005; YinYang House 2006; Hecker et al. 2008): (GB) Gall Bladder; (LI)Large Intestine; (BL) Bladder; (GV) Governor Vessel; (LV) Liver;(Ex-HN) Yintang; (SI) Small Intestine; (SP) Spleen; (PSNS)parasympathetic nervous system; and (C7) cranial nerve 7
SessionAcupuncturepoint Rationale
1 GB20 Head and shoulder, master point ofPSNS
GB34 He Sea point, distal point for headacheLI4 Most important analgesia pointBL10, BL11 Neck painGV14 Complements BL11 (the dorsal magic
triangle)Shenmen Tranquilizing point, similar to LI4 and
LV3
2 GB21 Neck and shoulder painEx-HN3 Headache, soothing Shen point;
self-acupressure before sleep taught
3 SI3 Pain in back and shoulders, clears themind;self-acupressure taught with matchstick;dermatomal distribution
BL62 Together with SI3, major anti-inflammatory point
LV3 Major analgesic pointPC6 Harmonizing effect, point on the C7
distributionLI11 He Sea pointSP6 Major point for maintaining high
endorphin levels
Cervical and posterior shoulder pain
� 2008 Acupuncture Association of Chartered Physiotherapists56

system, which is known to modulate mood,emotion, sleep and appetite, and thus, is impli-cated in the control of numerous behaviouraland physiological functions. Melzack & Wall(1984) proposed that transcutaneous electricalnerve stimulation (TENS) shares some aspectsof pain modulation with acupuncture.
Decreased serotoninergic neurotransmissionhas been proposed to play a key role in theaetiology of depression. The concentration ofsynaptic serotonin is controlled directly by itsreuptake into the presynaptic terminal, and thus,drugs blocking serotonin transport have beensuccessfully used in the treatment of depression.The assessment of depressed mood is importantbecause 50% of people with chronic pain syn-dromes are significantly depressed (Romano &Turner 1985).
Needling Large Intestine 4 may activate thesympathetic lateral horn at the T1 level, and alterthe sympathetic outflow to the head and neckbecause the autonomic outflow is under thecontrol of the hypothalamus (Bradnam 2003,2007), and thereby, inhibits noxious stimulationin the dorsal horn. This may be of benefit if thepatient has an injury that is slow to heal or ispartly sympathetically driven.
The present treatment was intended to stimu-late the subject’s supraspinal mechanisms toengage the descending inhibitory systems fromthe brain, which acupuncture is thought to acti-vate. Since the central response may be morelikely to be evoked when strong points, such asthe feet and hands, are needled (Bradnam 2003,2007), the present author selected strong periph-eral points from the beginning. Because therewas also a nociceptive component to the presen-tation and biomechanical faults were involved,some very gentle physiological manual treatmentof the lower cervical spine was administered. Indoing so, simultaneously, the parasympatheticnervous system (PSNS) was also engaged in thehandling of the subject, since part of the PSNS islocated in the brainstem and includes cranialnerves C3, C7, C9 and C10. At the end of thefirst session, the subject burst into tears. Theexplanation for this reaction could be thatthe cranial nerve innervates the eye, is part of thePSNS and is responsible for secretion of tears.
Even though Bladder (BL) 11 is located lateralto T1, and thus, in theory, could stimulate the
somatic afferents in the region and potentiallyinfluence the sympathetic chain, the presentauthor was confident that the relaxing effect ofthe bilateral use of BL11 and Governor Vessel14 would produce the calming and relaxing effectintended. By the third session, the subjectreported a 50% subjective improvement in PN
and PS, and that her co-codamol intake had beenreduced to two tablets a day.
Needling of Yintang stimulates the pinealgland, which secretes melatonin. Several clinicalstudies have indicated that supplementation withmelatonin is an effective preventative treatmentfor migraine and headache (Gagnier 2001).
Outcome measures and resultsThe primary outcome measure was the NRS, andsecondary outcome measures were the NDI,cervical ROM and intake of co-codamol.
The subject presented with a pain score of 8 atthe initial assessment; by the fourth treatmentsession, she reported a pain score of 3. Her dailyanalgesic intake had been reduced from sixtablets to only two, an improvement of 33%.
The NDI was completed during the subject’ssecond and fourth treatment sessions. This is avalidated instrument for measuring self-rateddisability caused by neck pain. She initially scored20 (40%), but her score of 17 points (34%)2 weeks later suggested some improvement.Vernon & Mior (1991) proposed that at least afive-point change is required for results to beclinical meaningful.
Cervical ROM improved significantly in alldirections. Initially, the subject had movementdysfunction in both rotation and flexion, but shehad regained full ROM by the last treatmentsession.
A total of four treatment sessions, approxi-mately one a week, have been administered todate. Acupuncture was performed in the second,third and fourth sessions, manual treatment hasbeen given from the beginning, and PBU andproprioceptive retraining were employed in thethird and fourth sessions. The subject subjec-tively reported that she felt 50% better after thethird and then fourth sessions. She reported nopain whatsoever immediately after the acupunc-ture was performed, and described feeling heavy,cool and relaxed.
The subject remained on light duties at work.
L. Skjodt
� 2008 Acupuncture Association of Chartered Physiotherapists 57

DiscussionFour treatment sessions of acupuncture, manualtherapy and proprioceptive training reduced thepresent subject’s various types of pain substan-tially from the initial levels. It seems clinicallysignificant that her pain score has improved intandem with a 33% reduction in her intake ofco-codamol.
It is interesting that the subject’s NDI scoredid not significantly improve despite the decreasein her pain levels and the fact that she regainedfull ROM of the cervical spine. It is possible thatthe reduction of co-codamol evoked a greater‘‘fear of moving’’ or a fear of relapse, or that thepatient simply developed a pacing strategy.
The acupuncture treatment was planned usingthe ‘‘layering method’’ described by Bradnam(2003, 2007). The above author suggested thattreatment plans should be formulated based onthe predominant pain mechanism. As the painmechanics change with time or treatment, theacupuncture intervention may be altered toreflect the changing physiology.
Initially, the SNS and CMP were the predomi-nant mechanisms affecting the present subject,and hence, points intended to activate thedescending inhibitory systems were used. Seg-mental and local points were also employed astreatment progressed.
An analysis of the few studies that haveinvestigated the effect of acupuncture on PN isinconclusive because there appear to be equalnumbers that report positive and negativeresults. A larger, higher-quality study by White& Ernest (1999) suggested that the efficacy ofacupuncture is unsubstantiated. Despite theirfindings, the above authors results showed thatacupuncture was superior to waiting list control,and was superior or equivalent to physiotherapy.
It is interesting to note that, although thepresent subject achieved a 33% reduction in heranalgesic intake by the end of the fourth treat-ment session, she was still on light duties atwork. There could be several reasons for this: thesubject might not have felt ready to take onheavier tasks; she might simply not enjoy them;or her communication with her employer mighthave been strained. The subject stated that‘‘work wants to finish me off’’ and, therefore,might have thought that the management would
not support her. She did report that her workwas enjoyable, even though she was lookingforward to retirement in a couple of years, butunfortunately, she will not be able to retire earlybecause of her financial situation. The subjectalso mentioned that her daughter came to visiton a daily basis, but it might be possible that shewas seeking a secondary gain by suffering afunctional limitation that made this necessary. Ofcourse, her daughter might still have visited everyday even if this had not been the case.
Pulling hair out can be a sign of self-harmingor attention-seeking behaviour, but these issueswere never fully discussed in the treatmentsessions. With hindsight, it might have beenuseful to liaise with the subject’s general prac-titioner regarding these psychological issues.
In retrospect, the length of the treatmentsessions sometimes limited the treatment modali-ties, and the present author now feels that sheshould have booked longer appointments.
Therapeutic and functional modulation hasbeen observed in both acupuncture and exercise.Both modalities release endogenous opiates thatgive rise to a central inhibition of pain. Anincrease in endorphin levels has been observedin the brain tissue of animals after acupunctureand muscle exercise (Andersson 1993). As partof the present subject’s continuing treatment, itmay become necessary to refer her to an exerciseclass.
There are inevitably many limitations to thiscase study. One was that the subject’s limitedEnglish initially made taking an accurate historydifficult. There was also a limitation on time,partly because of pressure on the NationalHealth Service (NHS) to meet the 18-weekwaiting list target (DH 2005, 2006) and partlybecause of the subject’s work commitments,which meant that she only received acupunctureon a weekly basis.
Since descending inhibition lasts for approxi-mately only 16 h (Alied Training 2005), a homeprogramme using a TENS machine could havebeen beneficial in this case and might havecompensated for the limitations described above.Unfortunately, this treatment option could notbe pursued because the present subject could notunderstand how to use it. Furthermore, she didnot follow the set-up of the PBU when it wasdemonstrated to her, and therefore, the training
Cervical and posterior shoulder pain
� 2008 Acupuncture Association of Chartered Physiotherapists58

had to be carried out during the treatmentsessions, which was time-consuming. The prop-rioceptive training was achieved by placing a doton the wall, where the intention was to keeplooking at the dot whilst turning the head. Thisexercise was slightly modified because the sub-ject had recently had an eye test that confirmedher need for stronger spectacles.
The final limitation was the combination ofconventional physiotherapy treatment and West-ern acupuncture, which begs the question ofwhich modality brought about the improvement.The subject’s treatment has been successful todate, but this remains ongoing and, therefore, itis very hard to conclude which modality isresponsible for her improvement.
ConclusionsThe present subject’s expectation was that hertreatment would bring about a reduction in pain,and this was successfully achieved by stimulatingthe descending inhibitory systems. The passivephysiological treatment and resultant stimulationof the PSNS initially seemed to interrupt thevicious pain cycle with which she had initiallypresented.
The subject has benefited from conventionalphysiotherapy and Western acupuncture, and theselected treatments seem to be complementary.The layered approach suggested by Bradnam(2003, 2007) initially appears to be a differentapproach to identifying this problem, but in fact,it is very similar to the standard physiotherapyback classifications that were proposed byPetersen et al. (2004). However, the problem withclassification by syndrome is that this might notexplain pain since there is a poor correlationbetween pain and pathology. Unsurprisingly,further research is needed in this area.
AcknowledgementsI would like to thank the pleasant Italian ladywho was the subject of this case study and thosewho supported me in the writing of the presentreport. The text employs material drawn fromLongbottom (2007).
This study was conducted in part-completionof the AACP-approved 40-Hour Top-Up Coursefor pain relief.
ReferencesAlied Training (2005) Foundation Acupuncture Course for Pain
Relief, Issue 1.1. Alied Training, St Neots, Cambridge-shire.
Andersson S. (1993) The functional background inacupuncture effects. Scandinavian Journal of Rehabilitation
Medicine 29 (Suppl.), 31–60.Bradnam L. (2003) A proposed clinical reasoning model
for Western acupuncture. New Zealand Journal of
Physiotherapy 31 (1), 40–45.Bradnam L. (2007) A proposed clinical reasoning model
for Western acupuncture. Journal of the Acupuncture
Association of Chartered Physiotherapists February, 21–30.Coderre T. J., Katz J., Vaccarino A. L. & Melzack R. (1993)
Contribution of central neuroplasticity to pathologicalpain: review of clinical and experimental evidence. Pain
52 (3), 259–285.Department of Health (DH) (2005) Commissioning an 18
Week Patient Pathway – Proposed Principles and Definitions: A
Discussion Document. [WWW document.] URL http://www.dh.gov.uk/en/Publicationsandstatistics/Publica-tions/PublicationsPolicyAndGuidance/DH_4122312
Department of Health (DH) (2006) The Musculoskeletal
Services Framework. [WWW document.] URL http://www.dh.gov.uk/en/Publicationsandstatistics/Publica-tions/PublicationsPolicyAndGuidance/DH_4138413
Gagnier J. J. (2001) The therapeutic potential of melatoninin migraines and other headache types. Alternative
Medicine Review 6 (4), 383–389.Gifford L. S. & Butler D. S. (1997) The integration of pain
sciences into clinical practice. Journal of Hand Therapy 10
(2), 86–95.Hecker H.-U., Steveling A., Peuker E., Kastner J. &
Liebchen K. (2008) Colour Atlas of Acupuncture:
Body Points, Ear Points, Trigger Points, 2nd edn. Thieme,Stuttgart.
Kaptchuk T. J. (2002) Acupuncture: theory, efficacy, andpractice. Annals of Internal Medicine 136 (5), 374–383.
Longbottom J. (2007) Case reports: JAACP author guide-lines. Journal of the Acupuncture Association of Chartered
Physiotherapists January, 67–68.Lundeberg T., Hurtig T., Lundeberg S. & Thomas M.
(1988) Long-term results of acupuncture in chronic headand neck pain. The Pain Clinic 2 (1), 15–31.
Mehta D. K. (ed.) (2007) British National Formulary, No. 54.British Medical Association and the Royal Pharmaceuti-cal Society of Great Britain, London.
Melzack R. & Wall P. D. (1984) Acupuncture andtranscutaneous electrical nerve stimulation. Postgraduate
Medical Journal 60 (710), 893–896.Paice J. A. & Cohen F. L. (1997) Validity of a verbally
administered numerical rating scale to measure cancerpain intensity. Cancer Nursing 20 (2), 88–93.
Petersen T., Olsen S., Laslett M., et al. (2004) Inter-testingreliability of a new diagnostic classification system forpatients with non-specific low back pain. Australian
Journal of Physiotherapy 50 (2), 85–91.
L. Skjodt
� 2008 Acupuncture Association of Chartered Physiotherapists 59

Romano J. M. & Turner J. A. (1985) Chronic pain anddepression: does the evidence support a relationship?Psychological Bulletin 97 (1), 18–34.
Vernon H. & Mior S. (1991) The Neck Disability Index: astudy of reliability and validity. Journal of Manipulative and
Physiological Therapeutics 14 (7), 409–415.Wadlow G. & Peringer E. (1996) Retrospective survey of
patients of practitioners of traditional Chinese acupunc-ture in the UK. Complementary Therapies in Medicine 4 (1),1–7.
White A. R. & Ernest E. (1999) A systematic review ofrandomized controlled trials of acupuncture for neckpain. Rheumatology 38 (2), 143–147.
White P., Lewith G., Prescott P. & Conway J. (2004)Acupuncture versus placebo for the treatment ofchronic mechanical neck pain. Annals of Internal Medicine
141 (12), 911–919.Yin Yang House (2006) Acupuncture Points Database:
Locations, Functions and Clinical Applications. [WWW
document.] URL http://www.yinyanghouse.com/acupuncturepoints/locations_theory_and_clinical_applications
Lotte Skjodt trained as a physiotherapist in Denmark,
her native country, and became state-registered in the UK
in 2000. She has since gained experience in the NHS,
and has specialized in musculoskeletal disorders since
2002. Lotte is currently the lead physiotherapist in the
Acute Sports Injury Clinic at Addenbrooke’s Hospital,
Cambridge, UK, and is the chair of the local
Musculoskeletal Educational Committee. In 2007, she
gained her Certificate in Orthopaedic Manual Therapy
after completing the renowned postgraduate course run by
Toby Hall and Kim Robinson in Perth, Western
Australia.
Cervical and posterior shoulder pain
� 2008 Acupuncture Association of Chartered Physiotherapists60

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 61–67
CASE REPORT
Acupuncture for the induction of labour
Roseanne McEwanPrivate Practice, Lee-on-Solent, Hampshire, UK
AbstractThis case report describes two pregnant females who, having reached full term, elected to haveacupuncture to induce their labours. Following a thorough assessment, it was decided to treatthese subjects with acupuncture and then assess the effectiveness of this form of therapeuticintervention. One of the women had three sessions of acupuncture with a gap of 3 days inbetween, while the other had four sessions spread over 8 days. The subjects were exclusivelytreated with acupuncture. Both women went into labour naturally and their labours were lessthan 9 h long. The subjects needed only a relatively small amount of pain relief during labourand both babies were born vaginally. It is concluded that acupuncture can be a useful techniquein the management of labour and its associated problems.
Keywords: acupuncture, induction, labour, pregnancy.
IntroductionLabour induction is the process by whichmedical or surgical intervention initiates uterinecontractions (Tenore 2003). Several differentmethods of inducing labour have been proposed,but there have been relatively few clinical studiesin this area (Smith & Crowther 2007) and manyof those that have been published are compro-mised by poor design (Tenore 2003). Currentresearch suggests that between 9.5% and 33.7%of labours need to be induced (Tenore 2003),and that cervical ripening fails to occur in 5%of women experiencing their first pregnancy(Summers 1997). Although many pregnantfemales would prefer to go into labour naturally,interventions are on the increase (Evans 2007),and women are increasingly requesting infor-mation on alternative ways to start the process oflabour (Tenore 2003).
Acupuncture has been proposed as onemethod of inducing labour, but again, there islittle evidence upon which to base practice.Physiotherapists who have completed the neces-sary courses are qualified to practise acupuncture
for pain relief. However, an increasing numberof professionally run courses are being madeavailable that allow physiotherapists to furtherextend their roles. One such course is ‘‘Acupunc-ture in Pregnancy’’, which qualifies physiothera-pists who complete the programme to practisethis technique on pregnant patients. This role hasbeen expanded further as woman who are at fullterm in their pregnancy are now approachingphysiotherapists in order to have their labourinduced, often with the encouragement ofmidwives and consultants (Summers 1997).
After a thorough subjective and objectiveexamination, physiotherapists use their clinicaljudgement, drawing on their prior knowledge,experience and skill, to decide which techniqueis most suitable for a particular patient (Jones1995). Evidence-based practice is essential andthe treatments chosen need to be effective.Acupuncture is one such technique, and whenemployed correctly, it can be a very usefultreatment tool (Bradnam 2001).
The aim of the present case study is toevaluate the effects of acupuncture on two sub-jects at the full term of their pregnancies. Bothwomen wanted to try a natural method ofinducing labour, and acupuncture had beenrecommended by a private physiotherapy clinic
Correspondence: Roseanne McEwan, Coates Mill Dairy,
2 Gloucester Street, Winchcombe, Gloucestershire GL54
5LU, UK (e-mail: [email protected]).
� 2008 Acupuncture Association of Chartered Physiotherapists 61

that employed a physiotherapist who hadrecently completed the ‘‘Acupuncture inPregnancy’’ course (Longbottom 2007).
Case reports
Case 1Mrs W. was a 33-year-old married woman with a2-year-old son who was pregnant with hersecond child. She had recently started hermaternity leave, but had previously had a full-time and often stressful job in medical sales. Thesubject was kept busy by her lively young son,but enjoyed socializing and reading when she hadany spare time.
She had always enjoyed a healthy active life-style and had no significant past medical historybarring minor headaches, occasional migrainesand recurrent cystitis. Her general practitionerhad suggested that these problems were probablystress-related, and had prescribed painkillers forthe headaches, to be taken when needed. Mrs W.had also taken antibiotics for cystitis in the past.She had had difficulty sleeping, but assumed thatthis was because she was heavily pregnant.
At her initial physiotherapy assessment, thesubject reported that she was anxious about theforthcoming birth of her second child becauseher first labour had been long and painful(>24 h). Mrs W. had to be induced, and requiredepidural anaesthesia and a forceps delivery. Shebelieved that this experience had resulted in hermild postnatal depression. Her 2-year-old sonhad always had problems settling and she wasconvinced that this was because of his traumaticbirth. When her son was younger, she had takenhim to a cranial osteopath and she believedthat the treatment had helped to alleviate theproblem.
Mrs W. attended the present author’s physi-otherapy clinic at the suggestion of one of herfriends. This friend was convinced that her ownpregnancy had been induced with acupuncture.The subject and her husband decided to try thistherapeutic intervention because she did notwant to repeat the traumatic experience of thebirth of her son.
Mrs W. was 40 weeks into her pregnancy whenshe attended the clinic for treatment, and aninduction date was scheduled 14 days later. Afterthe initial assessment, the intended benefits and
precautions were discussed. The treatment wasexplained to the subject, and an informationsheet was provided that described the possibleside effects and risks. A medical questionnairewas filled out as per the recommendation of thepractice, and a consent form was signed anddated. There were no contraindications to treat-ment and Mrs W. was eager to proceed with it.The aim of the treatment was to induce thesubject’s labour, but other potential benefitsincluded lessening her anxiety by promotingrelaxation, alleviating the headaches and helpingher to sleep.
On the morning after her third session, MrsW. woke up with stomach cramps. As themorning progressed, these became contractions,and by lunchtime, the contractions were less than5 min apart. The only pain relief that sherequired during labour was gas and air, and herdaughter was born naturally in hospital at 17:30 hthat day.
Mrs W. visited the clinic 6 weeks after thebirth of her child and said she could not believethe difference that her treatment had made to herexperience of labour in comparison to her firstbirth. The subject reported that she felt morerelaxed, and although she admitted that it washard work looking after two children, she saidthat was enjoying it much more than she haddone before. Mrs W. also showed no signs of thepostnatal depression that she had suffered afterthe birth of her first child, but she said that,if she did, then she would try acupuncturetreatment before anything else.
Case 2Mrs P. was also pregnant for the second time.Unlike the case described above, she had had aquick and easy first delivery (3 h, with gas and aironly), but it should be noted that this subject hadreceived a course of acupuncture from her mid-wife in the 2 weeks before she gave birth. Shewas attended by a new midwife during hersecond pregnancy, one who was supportive ofacupuncture, but did not actually practise it.
Mrs P. attended the present author’s practicebecause she was convinced that it was theacupuncture treatment that had made her firstbirth such a pleasurable one. She wanted torepeat the experience, but hoped to be able to
Acupuncture for the induction of labour
� 2008 Acupuncture Association of Chartered Physiotherapists62

have a home birth on this occasion. The subjectwas 39 weeks and 5 days into her pregnancywhen she attended her first assessment. She wasfit and well and had no contraindications toacupuncture. As with the first case, she was givena leaflet describing the intended benefits andpossible drawbacks of the treatment.
Over the course of 8 days, Mrs P. receivedfour sessions of acupuncture and went intolabour naturally. Everything progressed well andher second son was born after a labour of just4 h. This subject also only needed gas and air forpain relief, but she did not have the home birthshe desired because not enough midwives wereon shift.
Outcome measures and resultsBoth patients felt a tingling sensation as theneedles were inserted and turned. This responseindicates that the sensory neurones had beenstimulated. Different sensations or de qi mayoccur when a patient receives acupuncture, andthese can be used as outcome measures. Theseunpleasant feelings have a physiological signifi-cance (Melzack et al. 1977). Other commonsensations that are experienced include soreness,numbness, distension, warmth, radiation andtenderness (Gunn 1976). Subjective outcomemeasures may also include feedback frompatients when they attend further treatmentsessions.
Mrs W. found that she slept much better andfelt more relaxed after her first acupuncturesession. After her second treatment, she reportedthat she did not have any headaches in betweensessions. Mrs P. stated that her baby was veryactive when the needles were in situ and thatshe also slept well between sessions. Both sub-jects went into labour naturally and had rela-tively pain-free births, and this could be anoutcome measure in itself since the aim of theacupuncture was to induce their labours.
Acupuncture physiologyAlthough the reason why acupuncture induceslabour is a matter for speculation at present(Smith & Crowther 2007), it is thought that theuterus is stimulated by hormonal changes or bythe nervous system. It is also believed thatacupuncture can stimulate the release of prosta-
glandins and oxytocin (Tenore 2003), and thatneuronal stimulation may act on the para-sympathetic system to induce a contraction(Smith & Crowther 2007). Both these factorsplay important roles in cervical ripening, whichleads, in turn, to increased uterine contractilityand labour induction (Summers 1997). Levels ofinterleukin-8, prostaglandin F2� and �-endorphinare thought to be important regulators in cervicalripening, and in a study by Tempfer et al. (1998),the acupuncture group had a significantly shorterlabour than the control group. The aboveauthors concluded that the release of oxytocin orthe stimulation of the parasympathetic systemmay induce contractions.
Bradnam (2001) referred to a ‘‘layering tech-nique for acupuncture treatment of musculo-skeletal conditions’’, and provided a useful guideto the progression of treatment and its effects.The first layer, which is an effect of the mech-anical stimulation of the needle, is the tripleresponse (Gunn 1976). This produces histamine-like substances, which act on local changesaround the area.
Melzack et al. (1977) stated that acupuncturepoints have a similar effect to trigger points inproducing prolonged pain relief by disrupting theabnormal pain response that subjects experience.It is thought that acupuncture points work byblocking the pain pathway, a hypothesis knownas the Gate Control Theory, which inhibits thefiring of the pain signalling system. Many acu-puncture points are known motor points, andwhen needled, these act on the mechanorecep-tors. Such large-diameter afferent fibres travelfaster than the nociceptors, and when thesesynapse in the dorsal horn, the fibres bring aboutan overall inhibitory gate closure effect onnociceptive input and ascending transmission(Gunn 1976). The points can also send ‘‘fastpain’’ stimulation via the ascending pathway tothe brainstem, which acts on the periaqueductalgrey neurones, releasing opioids. The transmis-sion of pain can be influenced in the descendingcentral control by activating the enkephalininterneuron to produce encephalin, therebyreleasing endorphins that have an analgesiceffect. This theory may explain why both sub-jects’ labour pains were less intense and moreshort lived than they had expected.
R. McEwan
� 2008 Acupuncture Association of Chartered Physiotherapists 63

High-intensity needling (20–40 min) may pro-duce a stronger response, and points that have alarge representation in the somatosensory cortex(i.e. the hands and feet) will cause the desiredsupraspinal effect (Bradnam 2001). This could bea reason for choosing the ‘‘four gates’’ sincethese points can have a calming effect and inducerelaxation.
Acupuncture point rationaleThe acupuncture point rationale for the treat-ment of both subjects is described below and thepoints used are listed in Table 1.
When the needles were inserted at the firstsession, both subjects felt de qi, and by the endof the treatment, each was more relaxed. Sincethis was Mrs W.’s first experience of acupunc-ture, the needles were not stimulated and wereleft in situ for 20 min. After Mrs P.’s first sessionand during all of her subsequent treatments, thepoints were reinforced after insertion, and theneedles were turned quickly at a smallish ampli-tude approximately every 4 min to stimulate aresponse. The needles were left in situ forbetween 30–40 min. Both subjects felt morecomfortable in half-lying with pillows under theirknees. Other clinicians were nearby in case eitherwoman felt faint during their treatment.
After the first session, other points were addedand these remained the same for each furthertreatment (Table 1).
Guidelines for points chosenThe points chosen conformed to the recommen-dations made by the Acupuncture Association of
Chartered Physiotherapists ‘‘Acupuncture inPregnancy’’ course (Longbottom 2007). Thesepoints have also been referred to by otherauthors (Hecker et al. 2001) and recommendedfor use in labour. Spleen (SP) 6 and Liver (LV) 3have also been cited in the literature (Dunn et al.
1989), as has Large Intestine (LI) 4 (Rabl et al.
2001). Bladder 67 could have been used, butbecause there was no facility for using moxibus-tion and neither woman was thought to have abreech presentation baby, this point was avoided(Evans 2007). Bladder 28 was chosen bilaterallysince this point had been recommended as onethat could stimulate the parasympathetic system(Longbottom 2007). Gall Bladder 21 is thoughtto promote labour and lactation (Hecker et al.
2001). According to Longbottom (2007), SP6affects blood flow and nourishes the kidney,spleen and liver, and may have an importantrole to play in inducing labour. It is believed thatSP6 can increase contractions (Hecker et al.
2001). Duyin (Ex-LE11) was used according toLongbottom’s (2007) recommendation.
Relevant research to support treatmentRabl et al. (2001) studied at 56 women in order tocompare whether a group receiving acupunctureto induce labour would experience more of aneffect from the stimulation of cervical ripeningthan a control group. This was a single-blindedcontrolled study, and those receiving acupunc-ture did so on their estimated date of confine-ment and at 2-day intervals thereafter. Sufficientexclusion and inclusion criteria were used in thisstudy. Only two points were used, LI4 and SP6.The treatment duration was only 20 min. How-ever, the results showed that those women whoreceived pre-labour acupuncture experiencedimproved cervical ripening and a significantshortening of the time from the expected date ofconfinement to delivery. No significant findingswere found in the active phase of labour.
A randomized controlled trial by Gaudernacket al. (2006) found that women with pre-labourrupture of membranes may benefit from acu-puncture. Out of 100 subjects, 91 completed thestudy. Forty-three women were in the acupunc-ture group and 48 in the control group. The mainfinding in this study was that the active phase oflabour was significantly shorter in the acupunc-ture group (P=0.027). It was also found that the
Table 1. Acupuncture points used in the two subjects: (GB) GallBladder; (SP) Spleen; (LI) Large Intestine; (LV) Liver; (BL)Bladder; and (Ex-LE) Duyin
Treatment session Acupuncture points
Session 1:points (bilateral) GB21
SP6distal points (bilateral) LI4
LV3Subsequent sessions:
points (bilateral) GB21SP6BL28BL60
distal points (bilateral) LI4LV3Ex-LE11
Acupuncture for the induction of labour
� 2008 Acupuncture Association of Chartered Physiotherapists64

subjects who received acupuncture needed lessoxytocin infusion when labour was augmentedthan the control group.
DiscussionPatients are becoming more interested in alter-native therapies as a method of treatment forpain-related disorders, especially headaches, backpain and arthritis (Berman 2004). These modali-ties may alleviate the discomfort and pain ofmusculoskeletal conditions in the short term(Bullock et al. 1999). However, few studies haveassessed the role of acupuncture in the inductionof labour and for pain relief during labour(Tenore 2003). The present case report suggeststhat acupuncture could be used successfully as analternative method of bringing on cervical ripen-ing and induction. It also demonstrates thatother benefits were derived from acupuncture;for example, Mrs W.’s sleep improved and herheadaches were reduced.
Clinicians are becoming more aware of therole that complementary and alternative medi-cine can play, and it is gradually being embracedmore wholeheartedly (Gatchel 2003). Acupunc-ture may be an additional tool in the holisticapproach to treating the whole person (Berman2004). It has been suggested by Gaudernack et al.
(2006) that acupuncture should be offered topregnant women to help facilitate a natural birth.
Before women do decide on acupuncture, theyneed to be aware of and understand the processof acupuncture and its possible side effects, aswell as its intended benefits (Summers 2007).It is worth mentioning that there are fewerconcerns about side effects in complementarymedicines than in conventional medicine (Smith& Crowther 2007).
Only manual acupuncture was used in thepresent case report, but other studies haveemployed transcutaneous electrical nerve stimu-lation (TENS) on acupuncture points (Dunnet al. 1989). The above authors used SP6 andLV3 to induce uterine contractions, but onlyover a 4-h period on the day before their labourwas scheduled to be induced. Although Dunnet al. (1989) did not report any significant out-comes, stronger contractions were found in thestudy group. It may be not necessary to use aTENS machine because results may be more
dependent on using a greater number of pointsor carrying out acupuncture over a longer period.
The number of needles used may also berelevant, and research needs be carried out bothto confirm this and also to identify the areawhere these should be placed. This may have animpact on the reaction of the patient andwhether it stimulates the beginning of labour.
It could be argued that labour could havestarted spontaneously for both the casesdescribed in the present report. Because theywere at full term in their pregnancy, the resultscould be seen as a coincidence, especially sincethe numbers in the study are so small. However,each of the women had positive experiences oftheir deliveries and both believed that it wasacupuncture that helped.
Acupuncture is a cost-effective form of painrelief that reduces the need for a more-expensivereferral if used on appropriately selected patients(Lindall 1999). Furthermore, this form of treat-ment is cost-effective in comparison to a patientattending hospital for an induction. Acupuncturealso has other, additional benefits over medicalintervention in that it does not need to take placein a hospital, and the mother and foetus do notneed to be monitored (Gaudernack et al. 2006).Mothers-to-be may not like the idea of acupunc-ture, but it is only one of many alternativetherapies that are available to help with theinduction of labour (Summers 1997).
Specialized clinicians in this particular fieldshould only practice acupuncture in pregnancy ifthey understand the underlying physiology anddo not allow the contractions to become toostrong (Evans 2007). However, once they haveundergone their training, this can be an area ofgreat interest and a popular method of induction(Summers 1997).
There are several limitations to the presentstudy. Both patients underwent private treatmentbecause National Health Service (NHS) policiesdo not allow acupuncture because of its possibleadverse effects. Furthermore, there are time con-straints on treatment sessions within the NHS,and there may not be long enough to allow theneedles to work. Some follow-up sessions in theNHS are only 20 min, which may mean thatneedles are only in situ for 10–15 min during asingle session. Only two patients are described inthe present report and this small number means
R. McEwan
� 2008 Acupuncture Association of Chartered Physiotherapists 65

that it is not statistically significant. More clinicaltrials are required to assess the benefits andpitfalls of acupuncture in the induction of labour(Smith & Crowther 2007), especially since publicdemand is increasing, with an estimated 30–70%of patients turning to complementary and alter-native medicine (Soeken 2004). Finally, there islittle guidance regarding the length of time thatneedles should be left in, and it should be notedthat this could have had an effect on the induc-tion of labour.
ConclusionAs acupuncture becomes more popular in theinduction of labour, more randomized controlledtrials are needed to evaluate its efficacy (Tenore2003). Although several clinical trials have beenpublished, there is still a lack of strong evidenceto support its use and many trials have beenflawed (Smith & Crowther 2004).
Nevertheless, even if it can be argued that itwas not the process of acupuncture that startedlabour, both of the present subjects found thattheir birthing experiences were swift and rela-tively pain free. The reason that they hadrequested such an intervention was in order toavoid medical treatment. Women should havethe freedom to choose and access the method ofinduction that they prefer. Acupuncture appearsto be a safer and cheaper approach that may alsohave other benefits, which may be significantwhen the efficient use of resources can oftenbe more important factor than scientific evidencein clinical practice (Kovacs & Gil del Real2000).
AcknowledgementsI would like to express my appreciation toGeorge Chia and Adrian Yeoman, who taughtthe initial acupuncture courses that I attended,and to my colleagues at St Mary’s Hospital,Portsmouth, for regular in-service training for con-tinuing professional development requirements.A thank-you also goes to Jennie Longbottom,who taught the Physio First ‘‘Acupuncture inPregnancy’’ course; this has broadened mythought processes and increased my scope ofpractice.
ReferencesBerman B. (2004) Complementary and alternative medi-
cine: is it just a case of more tools for the medical bag?Clinical Journal of Pain 20 (1), 1–2.
Bradnam L. (2001) Western acupuncture point selection: ascientific clinical reasoning model. Meridian Worldwide –
Newsletter of the International Acupuncture Association of
Physical Therapists 10 (2), 9–18.Bullock M. L., Pheley A. M., Lenz S. K. & Culliton P. D.
(1999) Short-term outcomes of treatment for muscu-loskeletal disorders in a hospital-based alternative andcomplementary medicine clinic. Journal of Alternative and
Complementary Medicine 5 (3), 253–260.Dunn P. A., App M., Rogers D. & Halford K. (1989)
Trancutaneous electrical nerve stimulation at acupunc-ture points in the induction of uterine contractions.Obstetrics and Gynecology 73 (2), 286–290.
Evans J. M. (2007) Why we need holism in pregnancy care:a review. Alternative Therapies in Health and Medicine 13 (3),60–63.
Gatchel R. J. (2003) Chronic spinal pain: a randomizedclinical trial comparing medication, acupuncture, andspinal manipulation – point of view. Spine 28 (14),1502–1503.
Gaudernack L. C., Forbord S. & Hole E. (2006) Acupunc-ture administered after spontaneous rupture of mem-branes at term significantly reduces the length ofbirth and oxytocin. A randomized controlled trial. Acta
Obstetricia et Gynecologica Scandinavica 85 (11), 1348–1353.Gunn C. C. (1976) Trancultaneous neural stimulation,
needle acupuncture and ‘‘Teh Ch’i’’ phenomenon.American Journal of Acupuncture 4 (4), 317–322.
Hecker H.-U., Steveling A., Peuker E., Kastner J. &Liebchen K. (2001) Color Atlas of Acupuncture. Thieme,Stuttgart.
Jones M. (1995) Clinical reasoning and pain. Manual Therapy
1 (1), 17–24.Lindall S. (1999) Is acupuncture for pain relief in general
practice cost-effective. Acupuncture in Medicine 17 (2),97–100.
Longbottom J. (2007) Physio First Course Handbook. PhysioFirst, Towcester, Northants.
Kovacs F. M. & Gil del Real M. T. (2000) BMA approvesacupuncture: is approval of acupuncture for back painreally evidence based? [Letter.] British Medical Journal 321
(7270), 1220.Melzack R., Stillwell D. M. & Fox E. J. (1977) Trigger
points and acupuncture points for pain: correlations andimplications. Pain 3 (1), 3–23.
Rabl M., Ahner R., Bitschnau M., Zaisler H. & Husslein P.(2001) Acupuncture for cervical ripening and inductionof labour at term: a randomized controlled trial. Wiener
Klinische Wochenschrift 113 (23–24), 942–946.Smith C. A. & Crowther C. A. (2007) Acupuncture for
induction of labour. In: Cochrane Database of Systematic
Reviews 2007, Issue 1. Art. No.: CD002962. DOI:10.1002/14651858.CD002962.pub2
Acupuncture for the induction of labour
� 2008 Acupuncture Association of Chartered Physiotherapists66

Soeken K. L. (2004) Selected CAM therapies for arthritis-related pain: the evidence from systematic reviews.Clinical Journal of Pain 20 (1), 13–18.
Summers L. (1997) Methods of cervical ripening andlabour induction. Journal of Nurse-Midwifery 42 (2), 71–85.
Tempfer C., Zeisler H., Heinzl H., et al. (1998) Influence ofacupuncture on maternal serum levels of interleukin-8,prostaglandin F2alpha and beta-endorphin: a matchedpair study. Obstetrics and Gynecology 92 (2), 245–248.
Tenore J. L. (2003) Methods for cervical ripening andinduction of labor. American Family Physician 67 (10),2123–2128.
Roseanne McEwan studied Physiotherapy at the Univer-
sity of Wales College of Medicine, Cardiff, between 1997
and 2000. After attaining a 2:1 with distinction,
she completed her Junior and Senior II notations at
Cheltenham General Hospital. Roseanne has since
worked at Rutherglen Health Centre, Glasgow, and
part-time at DDB Physiotherapy Clinic, Lee-on-Solent,
Hampshire, and at St Mary’s Hospital, Portsmouth. She
is currently on maternity leave following the birth of her
second child.
R. McEwan
� 2008 Acupuncture Association of Chartered Physiotherapists 67


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 69–81
AACP Annual Conference, 16–18 May 2008: The Five Principles
Introduction and overviewOnce again, all the preparation and organizationthat must have gone into yet another excellentweekend Conference has proved to be time verywell spent indeed. As always, the RobinsonExecutive Centre, Wyboston, Bedfordshire, pro-vided the ideal venue not just for the Conferencesessions, but also in terms of accommodation,catering and overall service. I for one wouldcertainly be in favour of another pilgrimage toWyboston Lakes next year.
Friday’s keynote sessions began shortly afterthe timetable indicated to allow the modestcollective of Friday delegates to be divided upinto two groups. The first session I will mentiondealt with the perennial topic of legal issuesrelating to clinical practice. Mr Andrew Andrewsof Bond Solon Training Ltd shared his consider-able insight into and knowledge of the subject,and this lively and, as I later discovered,impromptu session was very well received.
The other keynote session was shared betweenMr Kim Wager and Mrs Sue Cox, both ofSubstance Misuse Acupuncture Register andTraining (SMART UK). In essence, their sessionhighlighted the prevalence of substance misuseand noted the common pathways of all addictivebehaviours. Unfortunately, I and some of theother delegates whom I spoke to felt that theremay have been a mismatch between the audienceand the speakers. Much of what was covered wasnot news to the majority of the audience and thepresentation tended to come across as a pre-amble to attendance at one of SMART UK’scourses. The prescriptive nature of the courseswas also notable because these are aimed atlaypersons and not clinicians. This is an issuethat I feel may not sit well with the majority ofphysiotherapists practicing acupuncture whovalue their autonomy and are self-governing interms of scope of practice.
Friday evening allowed delegates some freetime, during which use could be made of thefitness centre facilities on offer, and this wasfollowed by a barbeque by the lakeside. Again,
like last year, the food on offer was of a very highstandard and was accompanied by a few drinksand some relaxed conversation.
Professor Thomas Lundeberg (Fig. 1) kickedoff Saturday’s sessions, and displayed an enviableconfidence and knowledge of physiology, bothin general and as it related to acupuncture.Although perhaps an acquired taste, his presen-tation style of writing on blank transparencieswas lively, fresh and engaging. As the chair,Professor Graham Smith (Figs 2 & 3), com-mented at the end of his presentation, we wouldall have been lucky to have had someone with hisenthusiasm and knowledge teach us physiology.
Although Thomas could have been a hard actto follow, Dr Hugh MacPherson (Fig. 4) did justthat by leading us through the salient findings of
Figure 1. Professor Thomas Lundeberg fascinatesProfessor Graham Smith.
Figure 2. Professor Graham Smith commandingSaturday with style and skill.
� 2008 Acupuncture Association of Chartered Physiotherapists 69

his research into the long-term effects of acu-puncture treatment of low back pain. As always,Hugh presented some of the less-familiar con-cepts of the research process in a clear andsuccinct manner without talking down to hisaudience. Following a short break, and our firstchance to meet and speak with the trade repre-sentatives, Hugh returned to speak about a topicthat was, perhaps, somewhat outside his comfortzone: neuroimaging and acupuncture. This pres-entation brought to light some of the realities ofresearch utilizing functional magnetic resonanceimaging (fMRI) in addition to the notion thatminimal needling and deep needling may bothproduce clinically relevant effects.
A question-and-answer session followed be-tween the audience and the previous two speak-ers. Although this ended up lasting about 45 min,the time flew by as both Thomas and Hughexpertly responded to questions both passed onin writing to the session chair and from the floor.
A choice of hot or cold lunch with desertsfollowed, along with some more mingling with
the trade representatives (Fig. 5) and somesharing of feedback from the morning’s sessions.
For the Saturday afternoon workshops, thedelegates were again divided into two groups. Thefirst of the two sessions that I attended was led byMr Tom Lawrence, who spoke about treatingchildren with acupuncture. One of the essentialtake-home messages of this workshop was toidentify two main subtypes of children: thosefailing to thrive and listless (Xu); and those failingto relax and restless (Shi). It seemed fundamentalthat varying degrees of these characteristics haveto be considered when treating children. Whilethis was an interesting and, to some extent, aninteractive session, I feel that it had most rel-evance to those who treat children under 3 yearsof age with acupuncture on a regular basis;unfortunately I suspect that such clinicians didnot make up the bulk of the audience.
The second workshop saw the return ofProfessor Thomas Lundeberg (Fig. 6), this timetaking us on yet another enlightening journeythrough the world of acupuncture in the treat-ment of stress-related disorders. This insight into
Figure 3. Professor Graham Smith captivating theaudience.
Figure 4. Dr Hugh MacPherson discussing how to doresearch that is significant to clinical practice.
Figure 5. Trade stands at Conference.
Figure 6. Professor Thomas Lundeberg informs andentertains.
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists70

the complex but elegant physiology of ourin-built stress mechanisms and the influence thatacupuncture can have upon them was, I believe,a highlight of the day.
The Annual General Meeting (AGM) was heldat the close of the day (Figs 7 & 8) as many of thedelegates took their leave, and it proceeded expe-diently with a minimum of fuss or argument.
Delegates again had some free time to makeuse of the facilities at Wyboston Lakes after theclose of the AGM, but many focused on gettingready for the evening meal and the followingentertainment (Figs 9–12). As always, the foodand service were both excellent and the livemusic courtesy of Arizona Calling saw somedelegates throw a few shapes on the dancefloor.However, the real talking only started in thesmall hours, when a select few of the remainingdelegates made significant inroads into the last ofthe red wine.
Sunday’s sessions began brighter and earlierthan I’m sure many would have hoped, and again
saw Professor Thomas Lundeberg presenting,this time questioning the validity of sham acu-puncture procedures (Fig. 13). As has beendemonstrated and outlined by research, it is clearthat the concept of using so-called ‘‘sham’’ acu-puncture in comparative research studies is in-trinsically flawed and has no physiological basis.
Figure 7. Janice Booth, President of the BritishAcupuncture Council, thanking us and invitingphysiotherapists to the BAcC Conference to promoteintegration.
Figure 8. Your AACP Board.
Figure 9. Integrating with the British AcupuncureCouncil.
Figure 10. Integrating with PhysioFirst.
Figure 11. Fun and frolics.
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists 71

Once Thomas had got the ball rolling, it was upto Dr Nadine Foster and Dr Panos Barlas to keepit going. They did so by presenting the highlightsof their research into acupuncture for the treat-ment of osteoarthritis. Not only did Nadine andPanos present a clear and comprehensive accountof their investigations, they responded admirablyto the barrage of questions from the audience thatfollowed. This took us up to break time, duringwhich checkout time elapsed, and so the journeyto wherever home was and the beginning of theend of Conference 2008 felt already upon us.
After the break, we were again taken on whatcan only be described as a physiological roller-coaster with Professor Walter Zieglgansberger atthe controls. His talk investigated the topic ofre-learning in chronic pain. Walter somehowmanaged to elucidate the essence of memoryphysiology and how it plays a role in chronicpain in addition to outlining the beneficial effectsthat acupuncture may have in such cases.
A lively question-and-answer session precededlunch, and a further opportunity to meet with
fellow delegates and trade representatives. Afterlunch, the final two workshops saw the delegatesdivided into two groups once again.
The group I was in were first treated to asession shared by Ms Jennie Longbottom and MsJane Dixon on the treatment of pelvic pain withacupuncture, and the ups and downs of thefemale pelvic floor. Both presenters spoke froma very practical standpoint, but this was sup-ported at all times by an evidence base andclinical reasoning. While, perhaps, some of thestrictly women’s health content may not besomething that the majority of physiotherapistshave practical clinical experience of, it is, none-theless, a topic that, one way of another, is areality for over half the population, and at thevery least, should be acknowledged by all.
Finally, Mr Neil Quinton delivered a very wellreceived presentation dealing with the treatmentof mental and emotional conditions with acu-puncture. While some may argue that Neil’sapproach was point-specific and prescriptive,others may applaud him for his practical advice,which was justified and clinically reasoned,drawing from a mix of traditional Chinese andWestern medical perspectives.
All in all, this was a very successful Confer-ence, and I’m sure that I’ll be back next year fora number of reasons, including the quality of thevenue, the variety and authority of the speakers,and the relaxed atmosphere, which was condu-cive to debate and the exchange of ideas.
Andrew Bannan
Auricular acupuncture: anintegrated approach to addiction
Kim Wagner & Sue Cox
AbstractThis presentation is not intended to be a practi-cal instruction course. The treatment of addic-tion is far too complex to explain in a short time.However, it provides an overview of current au-ricular acupuncture in addiction practice as taughtby SMART UK. The presentation discusses:+ the difference between addiction and misuse;+ the brain and behaviour;+ the neurochemical basis for addictive behav-
iour;
Figure 12. Do you know these men?
Figure 13. The Chair both speechless and enthralled.
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists72

+ comprehensive, integrated drug addictiontreatment;
+ modern theories of auricular acupuncture andmechanisms of action;
+ how acupuncture may contribute to a treat-ment programme; and
+ the current evidence base.
ReportWhilst both Sue Cox and Kim Wager fromSMART UK are registered acupuncturists, Sue’sexperience is in addiction and counselling, andKim’s background is in biological sciences.
The abstract for this session promised todiscuss a number of interesting topics, includingthe brain and behaviour, and modern theories ofauricular acupuncture and mechanisms of action.It also promised to provide an introduction tothe neurochemical basis for addictive behaviourand a synopsis of the current evidence base.
However, the event turned out to be more ofa sales presentation on behalf of their coursesand lacked any real substance. I have heardpositive comments about the SMART UK train-ing courses, and it would have been interesting tohave heard Sue and Kim discuss either someaspects of their courses in more detail or any ofthe topics listed in the abstract.
Debbie Yates
Ignorance of the law: a gooddefence?
Andrew Andrews
AbstractThis presentation deals with the medicolegalimplications of treatment intervention. Issuesrelating to best practice are addressed withrespect to a number of areas, including consentand duty of care. The topics of consent, safepractice and scope of practice are highlighted.
ReportAndrew Andrews from Bond Solon Ltd gave apresentation on what could have been a veryfactual and indigestible subject that held theaudience spellbound. He discussed the medico-legal minefield of areas such as:
+ academic practice;+ scope of practice;+ consent; and+ duty of care.
Andrew’s charismatic and experienced styleoffered the audience the chance to understandcurrent medicolegal issues pertaining to ‘‘bestpractice’’, whilst reinforcing the AACP guidelinesfor safe and effective practice at the same time.He placed great emphasis on guidelines for:+ consent;+ safe practice; and+ scope of practice.
It was stressed that these were guidelines andadvisory documents, but at the end of the day, asautonomous practitioners, the emphasis lay withour own:+ professional knowledge and interaction;+ effective practice; and+ current best practice.
Andrew provided a highly entertaining andinformative presentation, and having attendedBond Solon expert witness courses in the past,I would wholeheartedly recommend these fortraining or personal interest.
The AACP and the Chartered Society ofPhysiotherapy are always interested in trainingfurther expert witnesses, and so, if you werestimulated by this workshop, please get in touchwith the Office to learn more about training inthis field.
Jennie Longbottom
Acupuncture: self-appraisal andthe reward system
Thomas Lundeberg
AbstractAcupuncture is an ancient therapy with a varietyof different explanatory models. A cascade ofphysiological effects have been reported in boththe peripheral and the central nervous systemsfollowing the insertion of a needle or lighttapping of the skin. Clinical trials testing thespecific claims of acupuncture have generallytried to focus on testing the efficacy of applyingspecific techniques and/or specified points.However, different conditions may respond dif-ferently to different modes of stimulation.
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists 73

It has recently been demonstrated that bothsuperficial and deep needling (with de qi/Hibiki)result in amelioration of patellofemoral pain andunpleasantness. The pleasurable aspect of theacupuncture experience has largely been ignoredbecause it has been considered secondary to itspain-alleviating effects. These latter aspects arelikely related to the activation of self-appraisaland the reward system.
When a patient seeks a therapist, there areexpectations of a specific effect. Also, when askedabout the effect of the treatment, processes thatorient pre-attentive anticipatory or mnemonicinformation (self-relevant phenomena), and pro-cesses that mediate self-reflection and recollection(self-referential introspection) are integrated toenable a decision to be made about the effect.These ‘‘self-appraisal’’ processes are dependenton two integrated networks: a ventral medialprefrontal cortex–paralimbic–limbic ‘‘affective’’pathway; and a dorsal medial prefrontal cortex–cortical–hippocampal ‘‘cognitive’’ pathway.
The limbic structures are implicated in thereward system and play a key role in most diseaseand illness responses, including chronic pain anddepression, by regulating mood and neuromodu-latory responses (e.g. sensory, autonomic andendocrine reactions). The pleasurable and neuro-modulatory aspects of acupuncture, as well as‘‘placebo needling’’, may partly be explained bythe activation or deactivation of limbic struc-tures, including the hippocampus, amygdala andtheir connections with the hypothalamus.
In patients with patellofemoral pain, theeffects of superficial and deep needling remainfor 6 months. These long-term pain-alleviatingeffects have been attributed to the activation ofpain-inhibiting systems in the cortical and sub-cortical pathways. When considering long-termeffects, the cortical–cerebellar system needs tobe taken into account. The cortical–cerebellarsystem is probably central to the development ofneural models that learn and eventually stimulateroutinely executed (e.g. motor skills) and long-term (e.g. pain alleviation) cognitive processes.These higher-order cognitive processes are ini-tially mediated in prefrontal cortical loci, but latershift control iteratively to internal cerebellarrepresentations of these processes. Some of thelong-term healing effects of acupuncture maypossibly be attributed to changes in the cerebellar
system, thereby reducing the processing load inthe cortical and subcortical areas.
Since cortical and subcortical structures areactivated and/or de-activated following thestimulation of receptors in the skin irrespective ofsite, it must be concluded that ‘‘placebo- or sham-needling’’ does not exist and conclusions drawnon the basis that it is an inert control are invalid.
ReportProfessor Thomas Lundeberg delivered his pres-entation on a complicated topic with humourand scientific depth, ably describing the corticalchanges that occur during acute and long-termpain and stress. He began his talk by explainingthat the treatment of a patient’s pain was moreabout the treatment of the patient and theirexpectations, and less about the treatment oftheir pain per se. We are all so used to slickPowerPoint presentations that I was initiallytaken aback by his old-fashioned use of anoverhead projector and hand-written notes.However, this was very soon forgotten as Ifocused on the information being presented. Heused simple language to talk about a compli-cated subject, illustrating many points with clearexamples that we could all relate to.
Thomas described how the limbic systemplays a key role in disease and illness response,especially in chronic pain and stress, and how thefrontal cortex and the cerebellum also link inwith patients’ expectations about treatment. Hefinished his talk by linking together these effects,and how acupuncture may partly be explainedby its activation or deactivation on the limbicsystem, as well as its likely effects on the cortical–cerebellar system.
Janet Wiggins
Acupuncture for low back pain inprimary care: evidence over thelonger term from a randomizedcontrolled trial
Hugh MacPherson
AbstractPatients with chronic low back pain (LBP)often seem to respond relatively quickly to
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists74

acupuncture. Nevertheless, if you look at thedata from systematic reviews, you could beforgiven for thinking that the evidence just doesnot make sense. With this concern in mind, atrial was conducted of acupuncture for LBP inpatients referred by their general practitioner inYork, UK. The aim was to gather the highestquality of evidence possible, while maximizingthe ecological validity of the study, in order toensure a fair comparison between acupuncturebased on traditional principles and a usual-caregroup acting as a control. This presentationdescribes both the quantitative and qualitative dataassociated with patients’ experiences of acupunc-ture and their practitioners’ roles in providing it.New data on longer-term outcomes are presented,along with data that were collected 6 years afterthe start of the trial. The key factors that mightbe associated with the longer-term benefits ofacupuncture were identified from relevant inter-view data and from practitioners’ reports.
ReportHugh MacPherson began by asking, ‘‘Does acu-puncture have a long-term effect in the manage-ment of low back pain in primary care?’’ Arandomized controlled trial (RCT) has been doneto find out the answer.
It involved 241 subjects who were randomlydivided into two treatment groups, acupunctureand usual management (randomization ratio=2:1). The inclusion criteria selected patientsbetween 20 and 65 years of age with currentepisodes of LBP of at least 4 weeks in duration;the exclusion criteria rejected patients with acurrent episode of LBP of more than 3 monthsin duration and those with possible serious spinalpathology. Clinical outcomes were measured at3, 12 and 24 months using the ‘‘Bodily Pain’’subscale of the Medical Outcomes Study 36-ItemShort-Form Health Survey (SF-36).
During the RCT, the acupuncture treatmentinvolved:+ an average of eight treatment sessions per
patient, usually on a weekly basis;+ an average of 10 needles per patient;+ the following local points: Hiatuo at L3, L4
and L5; Bladder (BL) 23, BL26 and Ah-shipoints; and adjacent points BL53 and GallBladder (GB) 30; and
+ the following distal points: BL40, GB34 andKidney 3.
Hugh reported the following findings:+ Many of the subjects who participated in the
trial were unable to work because of LBP.+ The two-thirds of the sample who believed
that acupuncture could help them had betteroutcomes, while the one-third of subjectswho were sceptical about acupuncture hadless-positive results.
+ There was heterogeneity between the acu-puncturists: with regard to the effect of indi-vidual practitioners compared to all controls,it was found that there were no statisticaldifferences between the practitioners.
+ The results of the SF-36 ‘‘Bodily Pain’’ scorewere as follows:+ both groups demonstrated very good
progress at 3 months;+ the acupuncture group scored slightly
better at 12 months; and+ there was a greater between-group differ-
ence at 24 months favouring the acu-puncture group, providing evidence thatacupuncture may have a beneficial long-term effect over usual care.
Hugh concluded that a short course of indi-vidualized acupuncture treatment can providehighly cost-effective results. Acupuncture effec-tiveness in the longer-term management of LBPin primary care is, therefore, supported by thisstudy.
Ahmed Osman
The neuroimaging ofacupuncture: comparingsuperficial needling (Japanesestyle) to deep needling(traditional Chinese medicinestyle)
Hugh MacPherson
AbstractPractitioners trained in Japanese styles ofacupuncture commonly insert their needlessuperficially just below the skin to a depth ofapproximately 1–2 mm. In contrast, practitionerstrained in what has become known as traditional
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists 75
Chinese medicine (TCM) hold the view thattherapeutic responses are associated with nee-dling depths that are relatively deep, usually1–2 cm, depending upon the local musculature.Practitioners of both acupuncture styles claimtherapeutic benefits while insisting that the depthof needling is integral to the putative therapeuticgain. To explore this divergence of opinion andpractice, we compared the impact of needlingat two different depths at Liver (LI) 4 (Hegu)using fMRI. We mapped the brain images associ-ated with both increases (activations) anddecreases (deactivations) in the blood oxygenlevel dependant (BOLD) response. The resultsof this comparison are presented, as well asvariations associated with the de qi sensation.This project resulted in a steep learning curve forthe investigators. A clearer understanding of theopportunities, challenges and limitations of uti-lizing neuroimaging in gaining knowledge abouthow acupuncture might work is also presented.
ReportHugh MacPherson’s second session was deliv-ered in the manner that one has come to expectfrom such an eminent researcher in the field ofacupuncture. His subject matter was clear andconcise, and he ably juxtaposed the boundariesof science and pragmatism. Hugh described thebackground to the research, essentially a favour-able opportunity to utilize a new imaging centreat the University of York on a gratis basis(MacPherson et al. 2008).
Seventeen subjects, naïve to acupuncture, werechosen and recruited to a randomized blockdesign involving either superficial or deep nee-dling at LI4 (Hegu). Imaging provided successivesnapshots of brain activity over a period of16 min. Despite this artificial constraint, thefindings proved most interesting.
It was found that activation in the cerebellumproved to be roughly identical with deep orsuperficial needling, while a greater margin ofdeactivation, more so with deep needling thansuperficial, was discovered in the frontal andoccipital lobes, and what appeared to be thelimbic system. The findings suggest that deacti-vation occurs more than activation, which maywell correlate with the frequently reported out-come of sedation post-treatment.
The impact of de qi proved challenging. Hughdevised a questionnaire and canvassed 30 TCMpractitioners to ascertain their thoughts on theimportance of de qi for effective treatment (85%confirmed de qi as essential), asking them todocument their patient’s subjective descriptionsof the needling sensation. Having extrapolatedand matched this information to the imaging, itwas clear that those subjects who experienced deqi demonstrated a stronger cluster of deactiva-tion at both the superficial and deep levels. It wasalso noted that there was a small gender vari-ation, with more deactivation in women, perhapsbecause of gender-based differences in neuralprocessing.
In summary, Hugh tabulated criticism of thestudy:+ Only short-term responses were recorded.+ The scanning environment itself was far
removed from that of a clinical setting.+ Was the needling reaction in response to
pain?+ The subjects were all healthy, so would find-
ings vary with acute and chronic conditions?+ Hegu (LI4) seems to activate not only the
somatosensory system, but also deeper, inter-connecting pathways (i.e. the limbic system).
+ This single point was also subject to longperiods of stimulation, which is atypical ofmost treatments.
Hugh’s conclusions were that:+ Depth of needling does have an impact upon
the BOLD response, but there is no overallstatistical difference.
+ There was a prevalence of deactivation inresponse to needling.
+ Needle sensation was found to mediate theBOLD response.
+ There was a tendency to deactivation inresponse to de qi and activation in responseto pain.
+ Superficial needling is not appropriate forsham trials because its outcome is similar tothat of deep needling.
Hugh’s presentation met with clear approvalfrom the audience and demonstrated the poten-tial scope of fMRI research to map patterns ofhigher-centre activation during the admin-istration of acupuncture.
Mike Chapman
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists76

ReferenceMacPherson H., Green G., Nevado A., et al. (2008) Brain
imaging of acupuncture: comparing superficial with deepneedling. Neuroscience Letters 434 (1), 144–149.
Treating children withacupuncture: an overview
Tom Lawrence
AbstractIn TCM, children are treated quite differently toadults: their problems are congruent withimmune and digestive systems that are still indevelopment; their emotions are transient anddon’t cause disease in the way that these can inadults; and they have not learnt how to erectenergetic barriers to cope with the world, and assuch, their energy is vulnerable but much easierto work with. This presentation provides aninsight into how acupuncture, when adminis-tered with appropriate sensitivity and technique,can change the course of a young human being’slife forever. Participants will learn how to recog-nize the basic energetic types in children, how toapproach treatment and how children can beneedled painlessly.
ReportTom Lawrence gave an enlightening presentationon how TCM acupuncture can be a valuabletreatment for children. He spent time explainingthe two basic energetic types of children, i.e. full(Shi), and empty or deficient (Xu), and how torecognize these clinically. Tom stated that, obvi-ously, not every child or situation fits completelyinto one of the two types. His treatment thenworks on the principle of either giving or takingaway energy.
We had a practical component on correctneedling techniques for children, using oranges,and were instructed to ‘‘be swift, gentle andkind’’.
Numerous diverse examples of pathologywere illustrated using the model and rationalesfor treatment were given. The conditions dis-cussed included asthma, gastrointestinal dis-orders, juvenile arthritis, cancer, ear problemsand behavioural problems. Tom also includesdietary and/or lifestyle changes in his treatment
plans, and perhaps most importantly, treatmentof the parent!
This was a well-presented and thought-provoking lecture and workshop session.
Averil Bainbridge
Acupuncture in the treatment ofstress-related disorders: abiological and genderperspective
Thomas Lundeberg
AbstractStress is a unique personal experience showingvariability where gender-related effects contrib-ute. The mechanisms underlying the differencesbetween women and men are currently un-known, but are likely to be complex and involveinteractions between biological, sociocultural andpsychological aspects.
In women, painful experimental stimuli (acutestress) are generally reported to produce a greaterintensity of pain than in men. Clinical pain andstress are often reported with higher severity andfrequency, as well as a longer duration, in womenthan in men. Women are also more likely toexperience a number of stressful conditions suchas post-traumatic stress disorder, chronic fatigueand irritable bowel syndrome. With regard tobiological factors, quantitative as well as qualita-tive differences in the limbic–hypothalamic con-nectivity and autonomic systems have beenimplicated, as well as the influence of gonadalhormones. Psychosocial factors like sex-rolebeliefs, stress coping strategies and stress-relatedexpectancies may also contribute to the differ-ences. Being exposed to repeated stressful vis-ceral events (e.g. menstruation and labour)during life may contribute to an increased sensi-tivity to, and greater prevalence of, stress con-ditions and pain among women.
When assessing the outcome of pharmacologi-cal and non-pharmacological therapies in stressand pain treatment, the factor of gender shouldbe taken into account since responses to anintervention may differ. Preferably, treatmentrecommendations should be based on studiesusing both women and men as the norm.
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists 77

Because of the variability in results, findingsfrom animal studies and experiments in healthysubjects should be interpreted with care.
The use of acupuncture and cognitive behav-ioural therapy in post-traumatic stress disorder isdiscussed and demonstrated.
ReportThe aim of this workshop was to illustrate atreatment concept based on acupuncture forstress-related disorders. Thomas Lundebergwarned us that this might become confusing, butas with his previous session, we journeyedthrough the brain, its chemistry and processeseffortlessly. With his excellent use of acetates, heensured that everyone joined him as he took usthrough the effects of stress on the central andautonomic nervous systems. Thomas inter-spersed his presentation with up-to-date scien-tific evidence, and related these physiologicalprocesses to clinical signs and symptoms. Hisability to link these seemingly complex processesto a treatment concept with a clear evidencebase with humour and pictorial diagrams kepteveryone entertained, thoroughly enthused andinterested.
The concluding message was the importanceof the segmental innervation of our patients’affected organs and their relationship to acu-puncture. Prior to this session, many of us mighthave found this message rather dull and seem-ingly irrelevant to the treatment of our patients.Following this workshop, I know that there arenow a lot of us who are keen to use thistreatment concept with the many patients we seewho are struggling to deal with the effects ofacute and chronic stress.
Lynne Fanning
Are reviews based on shamacupuncture procedures infibromyalgia valid?
Thomas Lundeberg
AbstractIn recent reviews of the efficacy of acupuncturein fibromyalgia, it has been concluded that acu-puncture has no specific effect because the
control procedure (i.e. superficial needlingand/or needling outside the ‘‘specific’’ points)had similar effects. It may be questioned if theseconclusions are valid since superficial needlingand/or needling outside the specific trigger pointis not inert. Furthermore, manual acupuncturemay not be sufficient when trying to activate theendogenous pain inhibiting system.
Studies of subjects with fibromyalgia havedemonstrated that they suffer from general allo-dynia. This would suggest that light stimulationof the skin might have as strong an effect asregular needling on the pain inhibitory system inthese patients. This conclusion is supported bystudies measuring blood flow in individuals withfibromyalgia where superficial needling of theskin resulted in as strong an increase in bloodflow as stimulation of muscle tissue. In healthysubjects, superficial needling had no effect onblood flow.
Furthermore, patients with fibromyalgia haveincreased receptive fields. This would suggestthat controls using needling away from the‘‘specific site’’ might have as strong an effect asneedling within the painful myotome/dermatome. In healthy subjects, needling withinthe myotome/dermatome induces the mostmarked increase in pain thresholds.
In fibromyalgia, there is a dysregulation ofthe pain inhibitory system. Therefore, strongstimulation is probably needed to activate thedescending pain inhibitory system. This sugges-tion is supported by a study showing thatstrong electroacupuncture stimulation is neededto obtain pain alleviation in fibromyalgia. Instudies using manual acupuncture or weakelectroacupuncture stimulation, optimal paininhibition may, therefore, not have beenobtained.
Chronic sleep disturbances are also character-istic of fibromyalgia, and it has been suggestedthat these sleep disturbances are the result of asleep disorder in which deep sleep is frequentlyinterrupted. Most of the previous reviews on theefficacy of acupuncture in fibromyalgia havefocused on pain alleviation. We have observedthat both sleep and cognitive dysfunction may beameliorated with acupuncture, suggesting thatthese parameters should also be taken intoaccount when assessing the effects of acupunc-ture in fibromyalgia.
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists78

Taken together, this would suggest that, whenconducting studies on acupuncture, one needs totake the clinical condition/syndrome into accountand design the control procedure appropriately.
ReportIn an unusual departure from Thomas Lundeberg’susual illustration of his lectures with whimsicalfreehand drawings, this was a standard Power-Point presentation. The former usually capturesthe attention of the audience and most heads aredown scribbling as he goes, but this one allowedthe attention to wander in spite of the interestingtopic. I hope that he returns to his usual type ofpresentation because I know that I was not theonly one to miss it.
The topic that Thomas covered in this sessionwas the validity of reviews based on shamacupuncture procedures in fibromyalgia. He cov-ered the dysfunction of the autonomic nervoussystem characteristic of fibromyalgia and pre-sented findings from an experiment with healthyvolunteers. When placebo needling was used,there was no change in blood flow, but when realacupuncture was employed, there was an effect.Furthermore, in subjects with fibromyalgia, therewere changes in both the placebo and realacupuncture treatments, indicating that placeboin this condition is not a placebo at all. In thesecircumstances, sham acupuncture trials are notvalid because any intervention cannot bedescribed as inert and expectations about acu-puncture also play a key role triggering similarresponses to true acupuncture.
Felicity Edwards
Acupuncture for osteoarthritis
Nadine Foster & Panos Barlos
AbstractOsteoarthritis (OA) results in 2 million generalpractitioner consultations annually, and is thecommonest cause of chronic pain and mobilitylimitation among older adults. Disability relatedto OA is set to increase as the population agesand obesity levels rise. Physiotherapy has asignificant role to play, given that recentevidence-based National Institute for Health and
Clinical Excellence guidelines recommend non-pharmacological interventions in both ‘‘core’’treatments for all patients and ‘‘optional’’additional therapies.
This presentation provides a summary of therole of acupuncture for OA, and using its mostcommon presentation, knee OA, discussesrecent evidence underpinning the use of acu-puncture. The results of a recent UK trial thatinvestigated the benefit of adding acupuncture toa course of advice and exercise (A&E) forpatients with knee OA are also described.
The trial recruited 352 patients, all of whomwere naïve to acupuncture treatment. The sub-jects were randomized to one of three treat-ments: a course of A&E; A&E plus trueacupuncture; or A&E plus non-penetrating acu-puncture delivered by 67 physiotherapists across37 clinics. Follow-up took place at 2 and 6weeks, and 6 and 12 months. The primary out-come measure was change in Western Ontarioand McMaster Universities Osteoarthritis Index(WOMAC) ‘‘Pain’’ subscale at 6 months, andsecondary outcomes included pain intensity andunpleasantness, and function.
ReportThis was an interesting, thought-provoking andat times emotive lecture regarding acupuncturefor OA. Nadine Foster began with an overviewof her role at Keele University, Keele, UK, andthe importance of support of groups such as theArthritis Research Campaign to further research.As evidenced-based practice becomes the norm,the value of clinical trials and epidemiologicalstudies was emphasized.
Osteoarthritis was highlighted as a conditionworthy of particular attention, although the dif-ficulty of making a differential diagnosis wasidentified, leading to some problems when defin-ing parameters for clinical guidelines and trials.Advice regarding the use of acupuncture for OAseems varied, with national and internationalguidelines often giving differing advice regardingthe effectiveness of acupuncture as an intervention.
Panos Barlos reviewed the potential physio-logical actions, and therefore, the possible ben-efits of using acupuncture in OA. As well as theperipheral effects, autonomic, central, descend-ing inhibition and mood effects were briefly
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists 79

considered, fitting in nicely with other lectures atConference this year. However, his recommen-dation of between eight and 12, 30-min treat-ment sessions may be a contentious one formanagers in the National Health Service!
Nadine finished with a summary of the multi-centre pragmatic trial into acupuncture and OAknee pain and function. The presentation stimu-lated some animated debate and I’m sure we alldeveloped a better understanding of the limits ofpragmatic trials. As Nadine said, the more of uswho get involved in research the better becausethis will help to provide a more accurate evi-dence base for the future.
Dave Graham-Woollard
Treatment of chronic pain: isrelearning a therapeutic option?
Walter Zieglgansberger
AbstractRecent advances in pain research illustrate theanalytical power of modern neurosciences in afield that was previously accessible only tomethods of systems biology. Novel electro-physiological, molecular and cellular biologicaltechniques have changed the face of painresearch by detailing systems acting in concert tohelp the individual to cope with pain.
The introduction of these concepts ofneuronal plasticity has already led to importanttherapeutic consequences: novel compounds andnew regimes for drug treatment to preventactivity-dependent long-term changes are beingdeveloped. Emerging knowledge related to thediversity of pain-related systems in the centraland peripheral nervous systems suggests that,besides ‘‘classical’’ neurotransmitters, biologicallyactive molecules such as peptide hormones, neu-rosteroids, trophic factors or cytokines releasedsynaptically or non-synaptically from terminals,neighbouring neurons, glial cells, or componentsof the immune system or the circulation, partici-pate in the integration of somatosensory infor-mation in the pain matrix.
Research over the past decade has shown thatpain states may arise from a variety of pharmaco-logically distinct systems. Some of these discretesystems appear sensitive to novel families of
agents that were otherwise not predicted by tra-ditional preclinical pain models as well as humanpain states. The multitude of dynamic changesthat occur during chronic pain offer novel targetsfor selective pharmacotherapy and treatment byvarious forms of acupuncture that are among theoldest healing practices in the world.
This lecture addresses therapeutically relevantmolecular, cellular and psychological mecha-nisms of pain processing and perception. Anattempt is made to interpret some of the obser-vations in complementary medicine in the lightof modern neurosciences.
ReportWalter Zieglgansberger delivered an entertainingand thought-provoking lecture on chronic painand relearning. He used some ‘‘state of the art’’technology to guide us through the pain-relatedsystems in the central and peripheral nervoussystems. His impressive PowerPoint presentationillustrated therapeutically relevant molecular,cellular and psychological mechanisms of painprocessing and perception. He informed us thatthe brain does not forget, it relearns to overrideadverse memories triggered by pain. Hedescribed chronic pain as ‘‘the dark side ofneuronal plasticity’’ and advocated a ‘‘pain holi-day’’ for chronic pain sufferers. In conclusion,Walter advised that acupuncture was veryimportant to modern neuroscience: as a methodof pain relief, it leaves the patient alert and com-pliant, in contrast to drug-induced pain relief,and decreases anxiety, which is a prerequisite forrelearning.
Wendy Rarity
Treating mental emotionalconditions using acupuncture
Neil Quinton
AbstractBased on my experience of working with patientswith severe and enduring mental health problemsin Walsall, UK, for the past 6 years, this work-shop focuses on a six-point acupuncture pointcombination that can be used to treat generalizedanxiety disorder with considerable success. It
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists80

begins with an outline of the condition thatcompares the perspectives of Western psychiatryand TCM. It then covers the location and actionof the points, and examines how this six-pointcombination addresses the root of the presentingsigns and symptoms. This workshop also coversthe important role that diet, relaxation and exer-cise can play in empowering our patients andaiding their recovery.
ReportNeil Quinton brought together the East andWest in his workshop on treating generalizedanxiety disorder. He began by outlining theWestern conceptualization of anxiety, and itsconcentration on physiological symptoms, thecontent and history of the patients’ problemsnotwithstanding. His calm and relaxed approachto the technical difficulties that threatened tointerrupt the smooth flow of his first session,and the interesting discussions regarding qi (is it‘‘energy’’ or ‘‘influence’’?) ensured an enthusiasticreception by the audience, as exemplified by thequestions at the end of the session. Neil’srefreshing take on the problem of syndromes/patterns and the need to look at how the patternsinteract, as opposed to trying to fit a patient intoa pattern/syndrome will have been gratefullyreceived by anyone present who is tussling withsuch difficulties. The presentation of a treatmentconcept that we can rationally use and incorpor-ate into our current practice made sure that thisworkshop was extremely well received.
Lynne Fanning
Treating pelvic pain withacupuncture and the femalepelvic floor: its ups and downs
Jennie Longbottom & Jane Dixon
AbstractThis theoretical presentation offers participantsan overview of the use of acupuncture in the
management of pelvic pain in the field ofwomen’s health. It encompasses Western acu-puncture analgesia, myofascial trigger pointrelease and Chinese acupuncture incorporatingpattern differentiation in the management ofthree specific conditions, i.e. endometriosis,chronic pelvic pain and pubic symphysis dys-function in pregnancy. An evidence-basedapproach using a clinical reasoning model is putforward throughout the presentation.
ReportPelvic pain is at the bottom (pardon the pun) ofmost people’s lists of desired specialities, butthank goodness there are people like JennieLongbottom and Jane Dixon who approach asubject bordering on social taboo in such arefreshing practical manner. Jane’s mention ofGrace Dorey as one of the leading lights in thisfield rang a bell. I had attended one of Grace’scourses on male and female incontinence manyyears ago and she had the same pragmaticapproach.
The discussion of the anatomy of the pelvicfloor was well presented and featured someinteresting original drawings. Jane’s descriptionof her work with real-time ultrasound and herpractical advice in response to questions werebacked up by Jennie’s slick and well-presentedacupuncture discussion. This presentation cer-tainly hit home, and will, I hope, encourage moremusculoskeletal physiotherapists to consider theclose relationship between the pelvic floor mus-culature and many sites of pain that may notrespond to therapy. All in all, there were moreups than downs to this fascinating session. I forone will be even more evangelical in preachingthe importance of the pelvic floor and its role,not just for women’s health, but also for goodposture and the health of the nation’s backs.
Felicity Edwards
Conference 2008
� 2008 Acupuncture Association of Chartered Physiotherapists 81


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 83–90
AACP Limited . . . the next 5 years
IntroductionOver the past few years, there has been consider-able progress in moving the AACP to where weare now, an effective, efficient and well-recognized clinical interest group (CIG) of theChartered Society of Physiotherapy (CSP). Wenow have the Association on a relatively soundfooting, with well-defined training and educa-tional standards, and systems that should serveus well as we move into the future of acupunc-ture regulation. We are grateful to all thosewith vision and commitment who have made ithappen. We thank those with the early idea ofbringing acupuncture into the scope of physio-therapy practice and those who participated inthe development of the AACP as a CIG of theCSP. We congratulate the members of the presentAACP Board for taking this vision even furtherover the past 3 years and making the outstandingprogress we now see in AACP Limited.
The progress that we have made was difficult,in that we had many hurdles to overcome, buteasy in that we could see clearly what we neededto do. Having got this far, however, we do notthink that it is quite so easy to see where we gofrom here, and consequently, what resources weneed to get there.
BackgroundFirst and foremost, the AACP is a CIG of theCSP that provides a range of supports andservices to physiotherapists with an interest inthe use of acupuncture. It is one of a number ofCIGs that have been formed to supplement theefforts of the CSP, providing support to thoseinterested in specific clinical techniques or areasof physiotherapy. Clinical interest groups caninevitably be more focused than a society thathas to represent all facets of physiotherapy.
Since its inception over 25 years ago, theAACP has grown in size and is now one of thetwo largest CSP CIGs, with some 5000 mem-bers. One unique difference between the AACPand other CIGs is the potential involvement ofthe Association in the regulation of physio-
therapists who practise acupuncture, and theimplications that this may have for the AACPand the membership.
The Government announced its intention tobring in regulation of those practising acupunc-ture (regulation) following earlier programmes toregulate other health professionals, includingpodiatrists and physiotherapists, through theHealth Professions Council (HPC). The AACPExecutive, having foreseen the need to beinvolved in the consultation from the beginning,was part of the Joint Working Group (JWG) forStatutory Self-Regulation (SSR) of the Acupunc-ture Profession. It was realized immediately thatpossible involvement in regulation would resultin closer scrutiny of AACP organization andgovernance, and therefore, the Executivecommissioned an independent study of theAssociation. The study recommended that theAACP should become a limited company, togive a focus to the development of appropriategovernance, and provide those running theAssociation with some protection in the event ofchallenges made about regulation or training.
AACP Limited was finally incorporated inJanuary 2006, with a board of directors (Board)made up of AACP members and some externalspecialist support. Shortly afterwards, the AACPintroduced its Training Framework (Frame-work), which set out the requirements for thetraining of physiotherapists in acupuncture, thestandards required from those who were to beallowed to teach acupuncture to physio-therapists, and the procedures under which bothtraining and trainers would be assessed. Therewas some initial opposition from some whostood to lose out because of the new standards,and from others who did not understand theimplications if physiotherapists could not dem-onstrate to the HPC that their training wasrigorous and independently assessed. Neverthe-less, by the end of 2006, the new procedureshad been widely accepted and endorsed by theCSP. Acupuncture training could no longer beadvertised in Frontline unless it was approved by
� 2008 Acupuncture Association of Chartered Physiotherapists 83
the AACP, and physiotherapists being trained inacupuncture were required to undertake accred-ited AACP courses.
Under its Board, the AACP has introduceda number of subcommittees, including thefollowing:+ the Education, Training and Research
Committee (ETRC);+ the Journal Committee;+ the Audit Committee;+ the Regional Representatives Committee; and+ the Conference Committee.
The Office in Peterborough offers an efficient,cost-effective hub of information and member-ship resources that is deftly managed by SharonFox, Business Manager, who is supported by onefull-time and two part-time members of staff.
Statutory regulationDiscussions involving the HPC about regulationhave progressed slowly, with complicationsintroduced via the regulation of Chinese herbalmedicine, with which many acupuncture prac-titioners outside the AACP are also involved.The forecast dates for the introduction of regu-lation have come and gone, with no decisionsmade. Today, it is still not clear how regulationwill be managed, or when regulation will beintroduced. What is going on is seriously ham-pered by our lack of contact or representationwithin the HPC.
It appears that the HPC will hold registers ofthose allowed to practise acupuncture by boththe British Acupuncture Council (BAcC) and theAACP, but not by the British Medical Acupunc-ture Society (BMAS), whose information will beheld by the General Medical Council or othersuch medical regulatory body. The HPC willtake, via the CSP, a register of those physio-therapists who are qualified to practise acupunc-ture. Effectively, this should mean that allmembers of the AACP will be transferred to theHPC register. Other physiotherapists wishing topractise acupuncture, but who are not AACPmembers, will be required to produce a portfolioof training and experience and apply to begrandparented onto the register. Details of whowill assess these portfolios are yet to be agreed.
There appear to be two options for regulationas far as physiotherapists are concerned:
+ The HPC will look to the CSP/AACP tomaintain the register.
+ The HPC will set up their own procedures formaintenance of the register.
It is not clear which of the two options will beadopted by the HPC, although the former optionis cheaper and less time-consuming for the HPCand is believed to be the option of choice.
At present, membership of the AACP or CSPis not compulsory for physiotherapists whopractise acupuncture, although only charteredphysiotherapists are allowed to join theAACP.
If the HPC look to the CSP/AACP to main-tain the register, it might be expected that theHPC registration fee would be less. It might benecessary for physiotherapists to be allowed onto the register, even if they were not alsomembers of the CSP or AACP. Membership ofthe AACP potentially should remain a desirableoption for physiotherapists wishing to practiseacupuncture, since continuing membershipwould automatically ensure appearance on theregister. Importantly, it would be necessary forthe AACP to clarify its relationship with the CSPin this process.
If the HPC decide to maintain the register,they would have to set up their own organizationand the role of the AACP would diminish.Whilst it has never been compulsory to join theAACP, the fact that the register was independentof the Association would act as a disincentive tocontinuing AACP membership, especially asphysiotherapists would then have to pay asignificant fee to both the AACP and HPC.
Therefore, we believe that the outcome of theHPC deliberations on regulation will have aprofound effect on the future of the AACP (seepp. 97–99).
The role of AACPAs a CIG, the primary role of the Associationis to provide services for its members. We feelthat this is an important point to make becausewe sometimes think that the fact that we havebecome a limited company can give the impres-sion that we aspire to be a profit-makingbusiness, like most other limited companies. Likethese other companies, we have to run our affairsin an efficient and effective way, but we are
AACP Limited . . .the next 5 years
� 2008 Acupuncture Association of Chartered Physiotherapists84

fundamentally different from these companies inthat we do not exist to make a profit. Indeed, ifwe do make a profit, then we shall incur aliability to pay tax.
If the AACP does play a part in the regulatoryprocess, it is likely that existing membershiplevels will be sustained or even increased, andthis economy of scale will enable us to developan increasingly wide range of services. On theother hand, if we were to be outside the regulat-ory process, it is likely that our membershipwould be reduced, since we should then only beable to attract members if they really valued theservices that we provided. We should then haveto look much more carefully at our basic runningcosts because these would become a muchlarger part of our income than is currently thecase.
Where now? AACP objectives
Quality-assured training standards
The AACP needs to provide quality-assured training
standards for its members and for other practitioners.
Quality training standards are essential if theAACP is to demonstrate that its members aresafe and effective in their practice of acupunc-ture. These are essential if physiotherapists whopractise acupuncture are to be able to developtheir skills and capabilities.
AACP Limited commissioned an independentconsultant to produce a defined set of proce-dures, with appropriate specifications for trainingcourses and tutors. This Framework was pub-lished in 2006 and defined the requirements forfoundation and post-foundation courses, and fortutors themselves. A governing committee, theETRC, was set up, reporting to the AACPBoard, under an independent Chair. A timescalefor the introduction of the new framework waspublished and it finally came into operation inspring 2007. Since then, although there wasinitially some opposition from those findingdifficulty meeting the new standards, these havegenerally been accepted. The CSP has endorsedthe standards and the Framework has beenscrutinized by the HPC.
The process is effectively run by the ETRC,with administrative support from the AACP
Office. It provides for tutors to submit theircourses and teaching portfolios for approval: theETRC handles these in a cycle that takesapproximately 3 months from submission toformal approval. There is a published list ofAACP-approved tutors and training courses, soto that extent the process is meeting our require-ments and we have sufficient resource tocontinue this process.
The ETRC now needs to determine whetherthese standards are indeed being met via internaland external audit of:+ courses;+ tutors; and+ case study standards.
Support of this type would appear to bestobtained from an external, suitably qualifiedindividual. We envisage that the results of thisexercise should result in additional procedures inthe Framework, which would be implementedwith the resources of the ETRC and AuditCommittee, although it is possible that oneoutcome could be the identification of additionalpermanent resources required by AACP.
Policy and political liaison
The AACP needs to have a clear insight into what is
going on within the CSP, the HPC and other areas that
may impinge on the practice of acupuncture.
The AACP is a CIG of the CSP, and thus, it isessential that the Association maintains goodcommunication with the Society, so that theAACP knows what is going on within the CSPand so that the it may exert appropriate influencewhen required. The current Chair and Boardhave made considerable efforts to improve com-munication via the CSP main managerial struc-ture, the Professional Practice Committee (PPC)and the CSP Council. The AACP has tradition-ally had a liaison officer who has attendedmeetings at the CSP and, to an extent, kept aneye on developments within the CSP. However,the Association no longer has a seat on the PPCand we have just been advised that the CSPapparently no longer require a liaison officerfrom the AACP. These developments clearlyneed to be investigated. Surely, as the largestCIG, the Association should be offered at leastsome representation at the decision-making endof the CSP? Furthermore, if the HPC opts to
AACP Limited . . . the next 5 years
� 2008 Acupuncture Association of Chartered Physiotherapists 85

allow the register of physiotherapists practisingacupuncture to be maintained by the CSP/AACP, it will be essential that the exact role ofthe Association in this process is defined and ourinterests safeguarded.
The AACP has had a representative at anumber of JWG and SSR meetings associatedwith the development of regulatory procedures.The Association has not managed to obtain anyform of representation within the HPC, despiteour efforts to do so. With regulation comingin soon, it is clearly essential that the AACPhas good communication with the HPC andrepresentation at the decision-making end of thisorganization. Latest developments give somegrounds for optimism, with the HPC advisingthe AACP that they will accept representation indiscussion groups.
Therefore, we judge that we are not meetingthis objective and we consider that we urgentlyneed to develop our liaison with both the CSPand HPC.
To do this, we should put forward AACPrepresentatives to stand for election at:+ the CSP Council;+ the PPC;+ the CIG liaison group;+ the Research and Development Committee;+ the Strategic Management Group of the CSP;
and+ the HPC.
The Board should have a representative withaccess to both the CSP and HPC, so that we areat least called for consultation during decisionsthat may influence acupuncture and physio-therapy. We believe that this requires a consult-ant who has advanced acupuncture skills toMSc/PhD level, has research understanding, andabove all, has enough knowledge of CSP andHPC working mechanisms to gain access tothese organizations. This person will requirepolitical knowledge, a reputation beyond theAACP, both at the HPC and with externalacupuncture groups, and a reputation thatdemands respect and support. This must be aphysiotherapist and this post must be paidaccording to experience.
It is also essential that the AACP develops andmaintains its good working relationships withboth the BAcC and BMAS.
Conferences, roadshows, workshops andcourses
The AACP should provide members with a range of
attractive conferences, roadshows, workshops and courses.
Past experience of organizing conferenceswith other CIGs and the CSP indicates that,for the long term, a well-resourced, proactiveConference Committee with access to a databaseof speakers, traders and venues is an essentialrequirement of any organization. We shouldstrive to develop a Conference Committee thathas access and attendance at international andnational acupuncture conferences.
Such a Conference Committee would thendetermine the theme and speakers, and direct theoperation of the Annual Conferences. In orderto achieve this, we need greater input and AACPrepresentatives in this Committee, and we wouldsuggest that we target new recruits to undertakethis role.
If the AACP were to opt to run additionalconferences, this would require additional effortfrom the Business Manager and Office staff, andadditional support from the Marketing Consult-ant, although an economy of scale would prevailbecause the methods and contacts built up forone conference would transfer to others. TheMarketing Consultant, Suzanne Charboneau, hasmade enormous strides with trade and confer-ence venue interaction, and she has become avaluable member of the AACP team. We suggestthat, in the light of her success, we use her skillsto take over the management of trade for bothConference and the AACP Journal so that thelevel of continuity, efficiency and respect isfurther developed and maintained.
Roadshows and workshops. There have been a fewroadshows in different parts of the country,organized by the Business Manager and consist-ing of a number of tutors presenting papersgenerally on musculoskeletal subjects. Thesehave been reasonably popular, but there has beenconsiderable difficulty in persuading tutors andothers to become involved, and the Office hasspent considerable time and effort in findingappropriate venues and available tutors.
The AACP could move to providing work-shops throughout the country rather than road-shows. Tutors, working with the Business
AACP Limited . . .the next 5 years
� 2008 Acupuncture Association of Chartered Physiotherapists86

Manager, could work towards a specialist one-day workshop, which would offer elements ofpractical and theoretical knowledge. Here theskills of AACP tutors, licensed acupuncturistsand BMAS specialists using acupuncture in anumber of clinical settings, and for a numberof conditions, may have greater appeal to theclinical membership than the present roadshowtheme. The use of outpatient facilities in differingregions, together with the input from regionalrepresentatives, may encourage better attend-ance, cheaper venues and provide greater clinicalbenefit for those attending. This suggestion hasmet with great interest from a number of trustmanagers and the Educational Officer of Physio-first. This would also ease the load carried by theBusiness Manager, who currently has to placateand accommodate numerous tutors at onevenue.
Training courses. The AACP has taken on theorganization and running of courses, both at theOffice in Peterborough and at other locationsthroughout the country. Profits from thesecourses are available for the development of awider range of services, as discussed in thispaper.
Up to now, the courses that have been runhave been owned by individual tutors, with theexception of a 40-Hour Top-Up Course. Thiscourse has been run by several AACP-approvedtutors, to whom we are very grateful for takingthe time to accommodate the needs of lapsedand forgetful members. The tutors have workedvery hard this year, but the course has beenextremely well received by those who haveundertaken it.
The new Framework does not restrict tutorsfrom running their own courses, unlike coursesrun by other CIGs, which have taken totalownership of all relevant courses given tophysiotherapists. These tutors may only teach theapproved courses and fees are fixed, any excessreturning to the CIG for further development.This approach is one that we believe the AACPshould consider.
There are two further concerns about trainingcourses:+ The AACP should consider carefully whether
there is sufficient clinical involvement inacupuncture training courses. The approach
taken by many CIGs has distinct advantagesin that courses are run with common stan-dards, ensuring that students gain direct clini-cal experience; indeed, the clinical placementis an essential component of these courses.Such clinical involvement is almost totallylacking in AACP courses and is a majorcriticism made by students undertakingAcupuncture MSc courses. The Associationwill consider whether clinical placement andclinical assessment are not only necessary, butindeed, essential to good clinical practice andknowledge for the graduating student.
+ Integration of AACP Foundation courses athigher educational level is essential for thedevelopment and emphasis of specializationwithin professional practice. There is a needfor healthcare professionals to developspecialized knowledge and skills (NHSExecutive 1999). This emphasis has changedthe career structure of healthcare profession-als, resulting in the specialized clinical prac-titioner, extended scope practitioner andconsultant posts. There has been a prolifer-ation of courses at the Master’s level aimingto develop clinical expertise. The Associationshould be at the forefront of this prolifer-ation, especially in the area of pain manage-ment, and as such, should be pioneeringAACP Master’s courses throughout thecountry by providing quality assurance,quality control, external inspection andmonitoring processes.
Research sponsorship
The AACP should sponsor acupuncture research for the
benefit of its members and the general public.
The Association offers the facility to provideresearch funding to members, but there is nocurrent research funded by the AACP.
The ETRC is nominated to manage theresearch budget, but this is an area that has beenneglected collectively by the Association. As amajor CIG of the CSP, it is essential that we leadthe field, and offer advice, guidance and supportto those wishing to turn to the field of acupunc-ture research. It is essential that the AACPbe seen to be encouraging and supporting themembership for the benefit of effectivenesswithin acupuncture and physiotherapy. We must
AACP Limited . . . the next 5 years
� 2008 Acupuncture Association of Chartered Physiotherapists 87

consider whether there is a need to take on adesignated AACP research consultant who hasexperience within the research field and exper-tise within the research community in order tofacilitate AACP-sourced research projects.
The post should also develop communicationswith the research and development committeesof the CSP, BAcC, BMAS and other researchresources that may offer the membership addedbenefits for the use of acupuncture within theclinical setting.
Communications
The AACP needs effective communications so that its
views are made well known and taken into account by its
required audiences:
+ the Government, including the HPC;+ the CSP;+ other acupuncture groups;+ AACP members; and+ the general public.
Public relations. The communication networkwithin the AACP and, indeed, within the CSPfalls short of achieving any impact both inter-nally and externally. Physiotherapy in generaldoes not have an effective, well-projected imagein the UK, and partly as a result of this, theAssociation has struggled to get its views acrossto its target audiences, although we have madesome progress in recent years. It must be remem-bered that acupuncture is one of the modalitiesused by physiotherapists to manage pain andachieve rehabilitation in a number of patients,but our views are rarely sought either from mediasources or within our own profession. Forexample, the CSP guidelines on low back pain(LBP) make no reference to systematic reviewson acupuncture use within a physiotherapy man-agement programme. International guidelines onLBP do not refer to any evidence for theintegration of acupuncture into a managementprotocol.
Press and media statements referring to break-throughs in acupuncture for a variety of diseaseand pain processes automatically contact theBAcC or BMAS for statements supporting thefacts. The AACP must attempt to lift its headabove the media parapet and offer effectivecommunication networks to ensure that both
the public and health professionals use theAssociation as one of its main resources in thisarea. In 2007, the AACP commissioned a studyby a public relations adviser. This initially ident-ified that the Association has a huge variety ofcontacts and associates, ranging from theDepartment of Health (DH) to the generalpublic, and that it was necessary to obtain ahigher calibre of professional individual to leadthe development of the AACP profile, influencekey audiences, including public and privatepurchasers, consumers and members, and pro-mote the Association with statutory and regulat-ory bodies, together with other groups andprofessions. Unfortunately, this study did notprogress.
We must consider taking on a professionalpublic relations officer (PRO), who would ini-tially work part-time for the AACP. The role ofthis PRO must be that of a proactive individualwith the ability to develop media strategy, state-ments and timely responses who has a highlyinformed professional background. This personmust be responsible for:+ the development and provision of AACP
strategies to internal and external stake-holders;
+ the setting up and development of a pressfunction in coordination with the AACPOffice;
+ the development and maintenance of a data-base of contacts, i.e. spokespeople fromwithin and without the AACP who representthe collective voice of the Association;
+ the initiation, development and implementa-tion of promotional strategies for externalconferences, training and relevant eventswhere the AACP need to be represented;
+ the development and promotion of educa-tional literature, videos and all relevantadvances that promote AACP business;
+ ensuring that all AACP committee membersare familiar with the strategies, developmentsand requirements of the business;
+ the establishment and maintenance of com-munications between all groups at all times,both nationally and internationally;
+ the promotion of the AACP within healthcareinitiatives, patient groups and primary carecontracts; and
AACP Limited . . .the next 5 years
� 2008 Acupuncture Association of Chartered Physiotherapists88

+ the promotion of internal influence andaccess to all policy changes within healthcareat the DH and HPC levels.
This is an important requirement for theAACP to safeguard our professional statuswithin acupuncture and future healthcare.
Website. The AACP has had a website for10 years, and at the start of 2007, a new websitewas specified by the AACP Board and designedby Summit Directions. The new website wasdesigned to be integrated with the membershipmanagement system so that much of the routinework associated with membership and subscrip-tions could be automated. Development of thewebsite took place in stages and was completedby the end of 2007.
The site now provides the following facilities:+ membership services;+ course and Conference booking;+ document purchase;+ reference documents;+ course advertising (free for AACP tutors);+ standards and guidance;+ relevant political and clinical news;+ audit; and+ research databases.
Day-to-day administration of the website isdone by the Webmaster, who is able to add allrequired information to the site, usually within aday or two of the requirement arising. What theWebmaster cannot do is to invent or generateinformation that should be available on the site.However, the proposed PRO and ResearchOfficer posts could ensure that the Webmasterwas fed with up-to-date news for the benefit ofmembers and the general public.
The website provides an ideal low-costapproach to providing information to membersand to accommodating the needs of the businessin the future, especially when moving into thearea of clinical and evidence-based database pro-vision. This is essential for academic access forour members and for those AACP membersworking outside the National Health Service.
The website also contains a bulletin board toallow members to discuss a range of issues. Thishas not been successful, with limited generaltake-up, and the take-up from AACP-approvedtutors being particularly disappointing. If thebulletin board is to succeed, the Association will
need to recruit and pay moderators to take thelead in getting this service up and running. If thisis not done, the bulletin board will not succeedand should be abandoned.
We will propose that the AACP website nowcharge for tutor advertising of courses, as is doneby the iCSP web service. Fees could be relativelysmall, and could be offset by support from tutorsfor roadshows, workshops or the bulletin board.
Enhanced membership facilities
The AACP should seek to provide a range of enhanced
membership services, over and above routine admin-
istration, an Annual Conference and quality training.
As a CIG, the Association’s purpose should bethe provision of a wide range of services to itsmembers. It is not sufficient simply to provideroutine membership administration, togetherwith an Annual Conference and expect thatmembers should be satisfied, especially whenregulation comes and they have to pay additionalfees to the HPC as well as membership feesto the AACP. Ideally, members should seeclear benefits from their membership of theAssociation, such that they would wish to remainmembers, even if their membership is notessential for them to practise acupuncture.
We have made a start on providing theseservices, with the website, regional roadshowsand others in the pipeline, but we think we stillhave a long way to go. Among the enhancedservices that we should consider providing arethe following:+ improved access to mentors;+ improved access to clinical reasoning and
problem-solving sessions;+ clinical experience on courses;+ clinical practice;+ web answers to questions;+ medicolegal courses for AACP members;+ an acupuncture resource centre;+ research papers on AACP web;+ advice on negotiating skills for primary care
trusts;+ marketing members’ skills;+ improved numbers of AACP expert wit-
nesses;+ report writing;+ negotiating contracts with private insurers;
AACP Limited . . . the next 5 years
� 2008 Acupuncture Association of Chartered Physiotherapists 89

+ improving the profile of the AACP in themarket-place;
+ setting up in private practice;+ the use of acupuncture within pain clinics;+ acupuncture beyond pain; and+ first aid training.
Just how far we can go in implementing theabove will depend on the decisions made aboutregulation, but this does not mean that wecannot work to develop these ideas now.
New ideas – continuity and succession
The AACP needs to generate new ideas for the benefit of
the membership. It needs to ensure that the organization
builds on the success achieved and attracts new blood to
keep its development going.
We firmly believe that the responsibility forthe generation of new ideas and member benefitslies with the Board. Members of the Boardshould have vision, experience and businessskills in order to maximize benefits for themembership. The Board are supported asrequired by external independent consultants,who will bring particular skills, experience andstrategic planning beyond the realms of physio-therapy and acupuncture. The skills of a financialconsultant, business adviser, marketing consult-ant and company secretary are available to offera wider view and an independent voice. How-ever, the skills required for acupuncture advance-ment within the membership must come fromthose experienced within the acupuncture world.This then rests with AACP members on theBoard.
It has to be a role of the Board in general to:identify AACP members who offer particularskills, either in the clinical setting, business oracademic worlds; target these members; andencourage their membership of committees andthe Board. Similarly, we rely on the goodwill ofsuch members coming forward to offer theseskills. If we don’t know you are out there andinterested, how can we encourage and supportyour Board involvement?
The way aheadIn this paper, we have identified seven objectivesthat we believe the AACP should strive to meet.For convenience, these are summarized below:+ quality-assured training standards;+ policy and political liaison;+ conferences, roadshows, workshops and
courses;+ research sponsorship;+ communications;+ enhanced membership services; and+ new ideas – continuity and succession.
These ideas and suggestions have beendebated by the Board and voted to be actionedwithin the next 5 years. Members will beinformed at each stage of the attainment of theseobjectives and the availability additional benefits,which we hope will enhance your clinical andacademic requirements within acupuncture andphysiotherapy.
AACP Board
AACP Limited . . .the next 5 years
� 2008 Acupuncture Association of Chartered Physiotherapists90

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 91–96
AACP clinical web audit
IntroductionThe AACP has carried out an audit of members’use of acupuncture in clinical practice. Thisreview was conducted using the AACP website,and members were requested to complete arange of questions presented online.
Unfortunately, the response was disappoint-ing, with only 137 completed responses out ofthe Association’s membership of some 5000 – amere 3% of the total voice of the AACP.As a result of the low response rate, it is notappropriate to draw firm conclusions aboutthe experience of the membership as a whole.However, after discussion with the Journal,Board and Educational committees, it was agreedto print an overview of the responses in theAACP Journal in order to facilitate discussion anddebate, and we hope, encourage a more positiveresponse to future clinical audits.
The AACP web audit tool is fast, efficientand a very inexpensive way to steer theAssociation’s research and training programmes.We do need information to inform decisions,and if we cannot generate sufficient responsesfrom our membership, we cannot attempt tointerpret:+ the clinical shortfalls of acupuncture within
physiotherapy;+ the clinical advantages of acupuncture within
physiotherapy;+ the clinical or educational requirements of our
membership; or+ the future avenues for AACP research and
clinical effectiveness.These are necessary requirements that must
be fulfilled in order for the profession to con-tinue to defend the evidence-based use of acu-puncture in the musculoskeletal management ofpain within clinical practice. It is also essentialthat these requirements are fulfilled in order toestablish the clinical use of acupuncture in gen-eral, which may go further than musculoskeletalmanagement, encompassing the holistic andhomeostatic management of patients beyondpain.
During the interpretation of figures, readers are
reminded that these results only represent the views of 3%
of the membership of the AACP.
Practice areaThere does appear to be a fairly even distributionof those responding between members workingin the National Health Service (NHS) (52%) andprivate practice (44%), a much closer ratio thandemonstrated by the wider membership of theAssociation (Fig. 1). Within the past 2 years, wehave seen greater demands from private insur-ance companies insisting that physiotherapistsusing acupuncture are members of the AACP,and similarly, 32 NHS trusts and the whole ofthe Ministry of Defence have introduced thesestandards. With forthcoming statutory regula-tion, it is impossible to determine whether thiswill remain the norm, or whether the HealthProfessions Council will oversee the future regu-lation and educational standards of acupuncturewithin physiotherapy.
The Association must continue to monitor:+ the standard of courses provided;+ the standard of tutors presenting courses;+ the standards of safety for acupuncture within
physiotherapy; and+ the standards of clinical effectiveness.
Membership categoryThe ratio of accredited to advanced to proba-tionary membership within the AACP as a wholeis 100:5:1. From the response illustrated in Fig-ure 2, we can see a ratio of 100:20:2.5, indicatingthat the relative response rates from advancedand probationary members was higher than thatof accredited members.
Probationary membership is a temporary sta-tus awarded whilst prospective members aretaking the 40-Hour Top-Up Course required foraccredited membership. It is to be hoped that, asprobationary members complete their top-upcourses and become fully accredited, their levelof interest will remain high.
� 2008 Acupuncture Association of Chartered Physiotherapists 91

The current ratio of advanced to accreditedmembers and the feedback gained from thetop-up courses beg the following question:
Is the AACP providing sufficient, quality advanced
courses to facilitate advanced status?
The Association’s requirement for advancedstatus is 200 h of training after the initial trainingrequired to become an accredited member.Traditionally, this has been via an acupuncturedegree training, but not all members have thetime or are in a financial position to undertakeprolonged acupuncture degree courses.
I believe that the AACP should be facilitating a
modular system of advanced training via external, accred-
ited courses offering Master’s-level points and an Accredi-
tation of Prior Experiential Learning system. I open this
to further discussion.
Figure 1. Main practice area of physiotherapists usingacupuncture: (NHS) National Health Service.
Figure 2. Membership category of respondents.
Figure 3. Proportion of practitioners using acupuncturefor pain management.
Figure 4. Support for acupuncture in clinical practice.
Figure 5. Source of support for acupuncture.
Figure 6. Opposition to acupuncture in clinical practice.
Figure 7. Source of opposition to acupuncture.
AACP clinical web audit
� 2008 Acupuncture Association of Chartered Physiotherapists92

Scope of acupuncture useOf those replying, it can be seen that the majority(51%) use acupuncture for pain management,but this does not take into account how or wherethey do this, and requires further investigation
(Fig. 3). Of far more concern are the results forthose using acupuncture for systemic disease(�1%) or neurological conditions (�1%),although these figures are at odds with responsesto other questions indicating that acupuncture isused in:+ anxiety and stress;+ relaxation and well-being;+ hormonal disturbance and menstrual cycle
management;+ sleep disturbance; and+ women’s health and incontinence training.
Again, a further in-depth response is required,together with clinical audit, to determine out-comes and results from these interventions.
Figure 8. Use of standard acupuncture point protocol.
Figure 9. Use of clinical reasoning in point selection.
Figure 10. Treatment of inflammation with acupuncture.
Figure 11. Use of acupuncture in stress and anxiety.
Figure 12. Use of acupuncture in insomnia.
Figure 13. Use of acupuncture in circulatory or tissuehealing enhancement.
Figure 14. Treatment of pregnancy-related disorderswith acupuncture.
AACP clinical web audit
� 2008 Acupuncture Association of Chartered Physiotherapists 93

From the in-depth questions answered, itwould appear that the majority of respondentsbelieved that acupuncture:+ facilitated pain management;+ facilitated rehabilitation;+ facilitated manual therapy;+ was cheap and effective; and+ offered speedier benefits than electrotherapy
modalities.
Support and oppositionFigures 4 and 5 offer some insight into supportand sources of support for acupuncture, themajority of support arising from patients (58%)and peers (48%), whereas the amount of supportarising from trust involvement is less than 20%.This has some very strong implications forwhether the Association should be supportingmembers at the trust level with evidence base,clinical effectiveness and cost-effective researchevidence, and presentations.
Figures 6 and 7 give an indication of thesources of opposition to acupuncture, peersbeing apparently the largest group here. Perhapscontrary to expectations, trusts appear less nega-tive than peers – although, with the low responserate, this conclusion cannot be definitive. Whathas to be determined is the source of ‘‘otheropposition’’, and this will require more in-depthquestions to determine whether this may arisefrom:+ medical referral sources;+ private insurance sources;+ management; and/or+ unknown sources.
I pose the following question: Would the membership
welcome AACP involvement at the senior management
level with the availability of presentations on clinical
effectiveness, cost-effectiveness and evidence base?
Clinical reasoningFigures 8 and 9 should give tutors within theAssociation some cause for concern. More than50% of respondents used a standard point pro-tocol in treatment management, whereas Figure9 suggests that more than 50% do not use aclinical reasoning model in choosing acupunctureor points.
I would raise the question of whether we are teaching
an adequate clinical reasoning model of pain presentation
against acupuncture intervention within the Foundation
Training. Should we reappraise the courses to ascertain
whether standards are being met and fulfilled?
Other conditionsFigure 10 suggests that more than 50% of thoseresponding would not use acupuncture in thetreatment of inflammatory dysfunction despitethe copious evidence to suggest that it is aclinically effective modality in the treatmentof inflammatory processes (Lundeberg 1993;Sato et al. 1994; Ceccherelli et al. 2002; Wolfe2005).
Are members taught to integrate acupuncture within
the first stages of nociception and inflammation in order to
facilitate rehabilitation, healing and recovery rather than
as an adjunct to treatment or after manual therapy has
provided the required results?
Once again, over 50% of respondents failed touse acupuncture in the management of stress oranxiety (48%), despite the existence of excellentphysiological evidence to suggest its use in stress(Fig. 11) (Garvey et al. 1997; White 2002; Heine2006) and anxiety (Sher 1998; White 2001; Linde2002; Pilkington et al. 2007).
Are members being taught the important application of
acupuncture in stress and anxiety as a precursor or
adjunct to physiotherapy and rehabilitation?
Figure 12 demonstrates that over 50% ofrespondents do not to choose acupuncture in themanagement of sleep disturbance or insomniadespite the evidence (Spence et al. 2004;Guerreiro da Silva et al. 2005; Chen et al. 2007;Kalavapalli & Singareddy 2007; Kim & Sok2007). We are fully aware that pain managementand tissue healing – whether acute or chronic –can only be enhanced by sleep and normalcircadian rhythm.
Figure 13 suggests that some 60% of thosewho replied would not incorporate acupunctureas a circulatory enhancement despite the evi-dence to support its effectiveness in woundhealing, skin disorders and tissue repair (Ulettet al. 1998; Sumano & Mateos 1999; Sandberg &Lindberg 2003; Sandberg et al. 2004).
Should acupuncture not be an integral part of any
surgical, systemic or physiological process where healing is
required?
AACP clinical web audit
� 2008 Acupuncture Association of Chartered Physiotherapists94

Finally, Figure 14 indicates that 64% ofrespondents do not offer acupuncture duringpregnancy. It seems that scepticisms and miscon-ceptions concerning the dangers of acupuncturewithin pregnancy are causing physiotherapistsnot to use what can be a very valuable tool forthe management of pain within pregnancy (Betts2003; Manber et al. 2004; Guerreiro da Silva et al.
2007).
Conclusion and discussionMy thanks are due to those who took part in thesurvey. As I have discussed, with such a lowresponse rate, we cannot draw too heavily on theinformation presented, but I do hope that thefigures will provide some ‘‘food for thought’’.The AACP would like to take this audit muchfurther in order to obtain much more defini-tive results in greater depth, but we can onlydo this with your help. Please give this yourconsideration.
Jennie Longbottom
Chair
ReferencesBetts D. (2006) A review of research into the application
of acupuncture in pregnancy. Journal of Chinese Medicine
80 (February), 50–55.Ceccherelli F., Gagliardi G., Ruzzante L. & Giron G.
(2002) Acupuncture modulation of capsaicin-inducedinflammation: effect of intraperitoneal and local admin-istration of naloxone in rats. A blinded controlled study.Journal of Alternative and Complementary Medicine 8 (3):341–349.
Chen H. Y., Shi Y., Ng C. S., et al. (2007) Auricularacupuncture treatment for insomnia: a systematicreview. Journal of Alternative and Complementary Medicine 13
(6), 669–676.Garvey M., Rogers C., Ryan D., Congxing Y. & Zaslawski
C. (1997) Toward development of appropriate clinicaltrail methodology for acupuncture: considerations anddesign of a research project on stress. American Journal of
Acupuncture 25 (2–3), 161–167.Guerreiro da Silva J. B., Nakamura M. U., Cordeiro J. A. &
Kulay L., Jr (2005) Acupuncture for insomnia in preg-nancy – a prospective, quasi-randomised, controlledstudy. Acupuncture in Medicine 23 (2), 47–51.
Guerreiro da Silva J. B., Nakamura M. U., Cordeiro J. A. &Kulay L., Jr (2007) Acupuncture for low back pain onpregnancy – a prospective, quasi-randomised controlledstudy. Acupuncture in Medicine 22 (2), 60–67.
Heine H. (2006) Bedeutung der Grundregulation für dasStressgeschehen unter besonderer Berücksichtigung vonNeuraltherapie und Akupunktur. [Regulation of theextracellular matrix: significance for stress reactionsparticularly in neuraltherapy acupuncture.] Schweizerische
Zeitschrift für GanzheitsMedizin 18 (6), 328–332. [InGerman.]
Kalavapalli R. & Singareddy R. (2007) Role of acupunc-ture in the treatment of insomnia: a comprehensivereview. Complementary Therapies in Clinical Practice 13 (3),184–193.
Kim K. B. & Sok S. R. (2007) Auricular acupuncture forinsomnia: duration and effects in Korean older adults.Journal of Gerontological Nursing 33 (8), 23–28.
Linde K. (2002) Ear acupuncture reduces preoperativeanxiety. Focus on Alternative and Complementary Therapies 7
(2), 130–131.Lundeberg T. (1993) Peripheral effects of sensory nerve
stimulation (acupuncture) in inflammation and ischemia.Scandinavian Journal of Rehabilitation Medicine 29 (Suppl.),61–86.
Manber R., Schnyer R. N., Allen J. J., Rush A. J. & BlaseyC. M. (2004) Acupuncture: a promising treatment fordepression during pregnancy. Journal of Affective Disorders
83 (1), 89–95.Pilkington K., Kirkwood G., Rampes H., Cummings M. &
Richardson J. (2007) Acupuncture for anxiety andanxiety disorders – a systematic literature review.Acupuncture in Medicine 25 (1–2), 1–10.
Sandberg M. & Lindberg L.-G. (2003) Effects of acupunc-ture on skin and muscle blood flow in healthy subjects.European Journal of Applied Physiology 90 (1–2), 114–119.
Sandberg M., Lindberg L.-G. & Gerdle B. (2004) Periph-eral effects of needle stimulation (acupuncture) on skinand muscle blood flow in fibromyalgia. European Journal
of Pain 8 (2), 163–171.Sato T., Kawatani M., Takeshige C. & Matsumoto I. (1994)
Ga-Al-As laser irradiation inhibits neuronal activityassociated with inflammation. Acupuncture and Electro-
therapeutics Research 19 (2–3), 141–151.Sher L. (1998) Acupuncture, endogenous opiods and anxi-
ety disorders. American Journal of Acupuncture 26 (4), 307.Spence D. W., Kayumov L., Chen A., et al. (2004)
Acupuncture increases nocturnal melatonin secretionand reduces insomnia and anxiety: a preliminary report.Journal of Neuropsychiatry and Clinical Neurosciences 16 (1),19–28.
Sumano H. & Mateos G. (1999) The use of acupuncture-like electrical stimulation for wound healing of lesionsunresponsive to conventional treatment. American Journal
of Acupuncture 27 (1–2), 5–14.Ulett G. A., Han J. S. & Han S. (1998) Traditional and
evidence-based acupuncture: history, mechanisms, andpresent status. Southern Medical Journal 91 (12), 1115–1120.
White A. R. (2001) Some evidence that auricular acupunc-ture points are specific for anxiety. Focus on Alternative
and Complementary Therapies 6 (3), 188–189.
AACP clinical web audit
� 2008 Acupuncture Association of Chartered Physiotherapists 95

White A. R. (2002) Acupuncture prevents hyperventilationduring mental stress. Focus on Alternative and Complemen-
tary Medicine 7 (1), 10–11.
Wolfe H. L. (2005) The concept of inflammation and itsrelationship to acupuncture. Townsend Letter for Doctors
and Patients 262 (May), 52–53.
AACP clinical web audit
� 2008 Acupuncture Association of Chartered Physiotherapists96

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 97–99
Statutory regulation of practitioners
IntroductionThe Report to Ministers from The Department of Health
Steering Group on the Statutory Regulation of Prac-
titioners of Acupuncture, Herbal Medicine, Traditional
Chinese Medicine and Other Traditional Medicine Sys-
tems Practised in the UK (Pittilo 2008) was launchedat a press conference at the King’s Fund, London,on 16 June 2008. The document consists of themain report, which makes specific recommenda-tions for regulation, outlining relevant infor-mation on the development of a research andevidence base for health professionals, trainingprovision and accreditation arrangements, to-gether with criteria used by the Steering Group(SG) to assess the potential of ‘‘professionalpractitioner associations’’ to qualify for directtransfer to the chosen regulatory body, identifiedas the Health Professions Council (HPC).
The report is vast, and the AACP congratu-lates the SG for an extensive, detailed andprofessional document. The report was informedby expert input from practitioners, health profes-sionals and statutory regulators, and by indepen-dent lay members of the SG. Because the reportis extensive, I will attempt to summarize themain points that pertain to physiotherapistsusing acupuncture within their profession andthose who may have the dual qualification ofLicensed Acupuncturist and Physiotherapist.
The role of the HealthProfessions CouncilThe SG takes the view that effective, safe andcost-effective statutory regulation (SR) has beendemonstrated by the HPC, and that this shouldbe extended to cover practitioners of:+ acupuncture;+ herbal medicine;+ traditional Chinese medicine (TCM); and+ other traditional medicine systems practised
in the UK.
Health Professions Councilcriteria for aspirant professionalsThe following criteria are outlined of aspirantprofessionals, who should:
(1) cover a discrete area of activity displayingsome homogeneity;
(2) apply a defined body of knowledge;(3) practice evidence, based upon evidence of
efficacy;(4) have at least one established professional
body that accounts for a significant pro-portion of that occupational group;
(5) operate a voluntary register;(6) have defined routes of entry to the profes-
sion;(7) have independently assessed entry qualifica-
tions;(8) have standards in relation to conduct, per-
formance and ethics;(9) have Fitness to Practise procedures to
enforce these standards; and(10) be committed to continuing professional
development (CPD).
Physiotherapists who are members of theHPC and who use acupuncture within theirscope and competency to practise are con-forming to these criteria by virtue of theirmembership of:+ the AACP;+ the Chartered Society of Physiotherapy (CSP);
and+ the HPC.
None of the professions considered in thisreport has a single voluntary regulatory body.The evidence base for the effectiveness ofacupuncture, herbal medicine and TCM is notwidely accepted in the way that it is for manyother professions regulated by the HPC.
However, the SG recommends that ‘‘in the interest of
public safety, SR should proceed with all possible speed’’.
GrandparentingWhenever a profession is protected, there isopportunity for individuals who have been usingthe skills safely and effectively to become regis-tered, a ‘‘one-off’’ window of time during whichindividuals can apply for registration. Duringthis period, there is an opportunity for membersof voluntary registers to be transferred directly
� 2008 Acupuncture Association of Chartered Physiotherapists 97

onto the HPC register without going throughindividual registration and assessment. The SGformally recommends a number of voluntaryregisters where there is evidence that these havebeen effectively and rigorously operated to highstandards. Those registrants, subject to HPCagreement, automatically transfer to the HPCregister when it is established. These acupunc-ture organizations are:+ the AACP;+ the British Medical Acupuncture Society; and+ the British Dental Acupuncture Association.
These professional bodies will be required tocontinue to:+ promote and develop the profession;+ represent members’ interests;+ publish journals;+ provide CPD training programmes;+ provide support;+ develop curriculum framework documents
for educational providers;+ develop standards of Best Practice;+ develop research and audit;+ provide minimum threshold standards neces-
sary for public safety; and+ provide Best Practice.
Professional body liaison withthe Health Professions CouncilAssociations representing acupuncture shouldengage with the HPC through regular, informalliaison in areas of:+ revalidation;+ reviews of standards of education and train-
ing;+ post-registration qualifications; and+ CPD standards.
The AACP has made provision for all thesecriteria to be in place and for effective, ongoingHPC liaison to take place.
Acupuncture within physiotherapyAcupuncture training within physiotherapy isnow undertaken post-registration and requires adifferent standard of definition as follows:
‘‘Acupuncture is premised on the scope ofpractice of the primary discipline and cannotbe offered without the basic professionalqualification to support it.’’
‘‘The appropriate qualification ranges froma certificate of qualification of safe, effectivetraining and competence (AACP FoundationTraining) to a University validated MSc.’’
The fundamental Physiotherapy degree educa-tional qualification is already subject to HPCregulation, its emphasis being research based,and thus, facilitating the adjunct of acupuncture,as a clinically effective modality, to be integratedwithin National Health Service and privatephysiotherapy practice. Recent work undertakento formulate National Occupational Standardshas established professional acupuncture compe-tencies. Compliance with these is inherent in allforms of training, although it may be supportedby different and profession-specific definitionsof the knowledge and understanding of acu-puncture required to practise. In the case ofphysiotherapy, emphasis may be placed onWestern neurophysiological processes (Han &Terenius 1982), and/or TCM philosophical prin-ciples of natural law and movement of qi (Qiu1993).
The SG recommends, in the interest of public safety, to
have all those practising acupuncture, even as an adjunc-
tive technique, on the same list with the same title.
The report has reinforced the combined workof the AACP and CSP to ensure that thefollowing standards are in place for membersalready placed on the AACP register to receiveautomatic transfer to the HPC SR register foracupuncture.
The AACP/CSP/HPC register ensures thatthe following standards are in place:+ the register has been in place for more than
5 years;+ the AACP has been established for more than
5 years prior to SR;+ the AACP membership is able to speak with a
unified voice;+ the AACP has a code of ethics informing a
code of conduct;+ AACP educational standards are established
with transparent and rigorous processes inplace to monitor the quality of training;
+ there is an effective arrangement for accredi-tation of educational programmes;
+ there is evidence of policies and proceduresthat would facilitate removal of individualsfrom the register;
Statutory regulation of practitioners
� 2008 Acupuncture Association of Chartered Physiotherapists98

+ there is evidence of CPD; and+ there is the involvement of lay members on
key committees who are able to have input.
ConclusionThe AACP, in liaison with the CSP and theHPC, are confident that all measures have beentaken to ease the transfer of the AACP registerfor automatic registration. What is essential isthat the AACP continues its active collaborationwith the HPC in order to ensure that the highstandards that have been set are maintained andchanged with emerging evidence in order toprotect the general public and ensure continuingscope of practice for those physiotherapists
using a clinically effective tool as a means to themanagement of patient rehabilitation.
Jennie Longbottom
Chair
ReferencesHan J. S. & Terenius L. (1982) Neurochemical basis of
acupuncture analgesia. Annual Review of Pharmacology and
Toxicology 22, 193–220.Pittilo R. M. (2008) Report to Ministers from The Department of
Health Steering Group on the Statutory Regulation of Prac-
titioners of Acupuncture, Herbal Medicine, Traditional Chinese
Medicine and Other Traditional Medicine Systems Practised in the
UK. Department of Health, London.Qiu M.-L. (ed.) (1993) Chinese Acupuncture and Moxibustion.
Churchill Livingstone, Edinburgh.
Statutory regulation of practitioners
� 2008 Acupuncture Association of Chartered Physiotherapists 99


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 101–107
Book reviews
The Practice of Chinese Medicine,2nd edn: The Treatment of Diseaseswith Acupuncture and Chinese HerbsBy Giovanni MaciociaChurchill Livingstone, London, 2008,1546 pages, hardback, £89.99ISBN 978-0-443-07490-5
The first edition of The Practice of Chinese Medicine
(Maciocia 1994), published 14 years ago, wasintended to be the companion volume to The
Foundations of Chinese Medicine (Maciocia 1989),and described the application of the theory oftraditional Chinese medicine (TCM) to the treat-ment of specific diseases with both acupunctureand Chinese herbs. Now, following the publica-tion of the excellent second edition of the latterbook (Maciocia 2005), an extended, 1546-page,revised edition of The Practice of Chinese Medicine
has been released by the publisher to completethis popular and successful series.
Giovanni Maciocia is probably the best-knownauthor and lecturer on Chinese medicine inthe West. What makes his books so popular?Clarity and system: his works are easy to read,using clear and simple English, and are set outin such a way that all kinds of readers can findthe answers that they need quickly andefficiently. However, the most important factorin Maciocia’s popularity is the reflection of thecultural context that all of us, as Westerners,share.
In our societies, which are shaped by thedominant paradigm of Western medicine, wedeal with complaints that are not what thepatients themselves feel, but rather a labelapplied through that paradigm. This is where The
Practice of Chinese Medicine provides an interfacebetween the Western medical understanding of adisease, and the TCM view and handling of thesame patient. There is a lot of debate regardingthe above approach, and many commentatorshave characterized Maciocia as a TCM ‘‘heretic’’.Nevertheless, TCM is a clinical discipline thatnot only welcomes, but in fact, demandsinnovation and creativity.
Giovanni has once more invested his clinicalheart and soul in the pages of the second editionof The Practice of Chinese Medicine. Readers whowant to expand their knowledge and experienceare provided with both new and refreshedmaterial to help them understand the mech-anisms that create the various conditions in ourpatients.
This book is about Nei Ke, i.e. internal medi-cine, which is the core of everyday generalpractice. Giovanni describes the application ofTCM theory to the diagnosis and treatment of48 diseases and conditions. In addition to the34 topics that were covered in the first edition,there are 14 new chapters. These include anexpanded and in-depth discussion of the ‘‘psyche’’in TCM, as well as sections on anxiety, depression,chronic fatigue, hypertension, thyroid conditions,nausea/vomiting, acid reflux, mouth ulcers, uri-nary retention, interstitial cystitis, benign prostatichyperplasia, fibromyalgia and erectile dysfunction.There is also a notable expansion of materialpublished in the first edition, such as the chapteron the differentiation and treatment of nasalpolyps. New theories presented in the secondedition include models of allergic asthma, allergicrhinitis and multiple sclerosis, although thelatter is mostly based on the pathology andsymptomatology of atrophy syndrome.
There are some major changes and additionsto the new edition of The Practice of Chinese
Medicine. The text has been revised throughoutand has expanded on the Chinese sources. A lotof new references have been added in compari-son to the first edition. Many new patterns,formulae, case histories and clinical trials havebeen added to several chapters. A colourfulsection dealing with the pathological colours andshapes of the tongue is also included. The threegynaecological diseases, i.e. premenstrual syn-drome, painful periods and menorrhagia, thatwere included in the first edition have beenremoved because these conditions are now dis-cussed in detail in the author’s gynaecologicaltext, Obstetrics and Gynecology in Chinese Medicine
(Maciocia 1998).
� 2008 Acupuncture Association of Chartered Physiotherapists 101

A lot of the extracts from modern TCMjournal articles suffer from poor design andmethodology. Maciocia notes that he includesthese articles not for the value of the clinicaltrials reported, but mostly to gain from theexperience and treatment principles adopted bydifferent famous doctors in the treatment ofvarious conditions.
This edition of The Practice of Chinese Medicine
has the same design and layout as Maciocia’sother works published by Elsevier, and it sharesthe very professionally designed diagrams, boxesand illustrations that make those books bothunique, and very easily read and understood.
As in the first edition of this text, most of the‘‘diseases’’ are discussed only in the context ofTCM. For example, cough or abdominal pain arenot ‘‘diseases’’, but symptoms in Western medi-cine; in TCM, they are diseases (binq) of internalmedicine. However, in some cases, the treatmentof Western-defined diseases (e.g. Parkinson’sdisease and multiple sclerosis) is thoroughlydiscussed.
Readers should note that some herbal pre-scriptions may contain substances that are nowillegal in the UK. The author mentions that thesereferences do not signify an endorsement ofthe use of banned substances, and readers arestrongly advised to enquire about the lawsgoverning the use of certain herbs and sub-stances in their country. Maciocia’s intention wasto present traditional formulae without alterationin order to give the reader an idea of the actionof these prescriptions. It is only when we knowthe original ingredients of a formula that wecan make appropriate substitutions based onthe action of the ingredient that we intend toreplace. For that particular reason, the wholeof Appendix 6, ‘‘Suggested substitutions ofChinese herbs’’, is dedicated to providing all theappropriate information.
The acupuncture points indicated for eachpattern are not given formulae, but rather, serveas a list of possible points from which prac-titioners can choose when determining an acu-puncture treatment. Nevertheless, there are a fewexceptions, and these are indicated as ‘‘generalprescription’’ or ‘‘ancient prescription’’.
Finally, I have to mention that each chapterincludes a Western differentiation of the symp-tom discussed in order to provide practitioners
with a quick checklist of the possible Westerncauses of that particular condition. Anotherreason for practitioners to be more familiar withthe Western differentiation of symptoms is prog-nosis. Although TCM is excellent at providingnot only a diagnosis, but also a reasonableprognosis by carefully examining symptoms,signs, tongue and pulse, in many cases, theprognosis also depends on the Western diagno-sis. For example, it makes a big difference toprognosis whether an oedema in a limb is causedby a ‘‘simple’’ qi-stagnation deficiency, or bycardiac problems or nephritis.
With this comprehensive and scholarly work,Maciocia has brought his extensive clinicalexperience as a practitioner and lecturer to theWestern reader. The second edition of The
Practice of Chinese Medicine presents an excellentexplanation of the theories of TCM in relation toclinical practice, as well as information oncreative adaptation of TCM theory to Westernclinical conditions.
George Marcos MSc BSc(Hons)
MAACP MBAcC
Private Practice
London
ReferencesMaciocia G. (1989) The Foundations of Chinese Medicine: A
Comprehensive Text for Acupuncturists and Herbalists.Churchill Livingstone, Edinburgh.
Maciocia G. (1994) The Practice of Chinese Medicine: The
Treatment of Diseases with Acupuncture and Chinese Herbs.Churchill Livingstone, Edinburgh.
Maciocia G. (1998) Obstetrics and Gynecology in Chinese
Medicine. Elsevier, New York, NY.Maciocia G. (2005) The Foundations of Chinese Medicine: A
Comprehensive Text for Acupuncturists and Herbalists, 2ndedn. Churchill Livingstone, London.
The Management of Post-operativePain with AcupunctureBy Sun PeilinChurchill Livingstone, London, 2007,384 pages, hardback, £34.99ISBN 0-443-10361-5
This is an interesting book masquerading under arather misleading title. The scientific evidence forpostoperative acupuncture is very poor. Onlya few published studies indicate any kind of a
Book reviews
� 2008 Acupuncture Association of Chartered Physiotherapists102

favourable outcome and most of these have usedauriculotherapy (Wang H. H. et al. 1997;Usichenko et al. 2006; Wang S. M. et al. 2007). Ithas to be added that acupuncture has not beenwidely used or studied for this type of painwithin Western medical circles.
The author’s main argument seems to be thatthese postoperative situations should be consid-ered on an individual basis, and purely from aTCM point of view. To that end, The Management
of Post-operative Pain with Acupuncture begins with along chapter on TCM theory, offering knowledgeand practical skills for treatment with acupunc-ture in order to obtain better therapeutic results,and then considers the body region by region,comprehensively covering all kinds of pain afterany operation. The meridians that may beinvolved are described, together with the symp-toms and possible syndromes that may be associ-ated. In this section, the points suggested are notalways very different from those that might beselected by an acupuncturist applying segmentalacupuncture.
Sun Peilin highlights the importance of treat-ment differentiation, point selection, point expla-nations and modifications, thereby providing asmuch information about treatment as possible.In addition to acupuncture treatment, the authoralso includes relevant facts about, for example,auricular acupuncture, electroacupuncture andpoint injection. He also includes detailed modi-fications of the treatments in order to aid clinicalpractice.
The section on general complications is wellorganized and full of helpful information. It issubdivided into those problems that may occurimmediately, others that may follow a little laterand long-term complications. Specific complica-tions that may be life-threatening are dealt within a final section, and the advice that they shouldreceive emergency treatment in hospital is madevery clear.
I was made very uneasy when I read aboutacupuncture treatment in some circumstances,particularly that of a deep vein thrombosis. To hiscredit, Sun does discuss compression stockings,positioning and exercise, but the impressiongiven is that acupuncture can help prevent furtherepisodes. In the absence of any evidence to sup-port this, I would be wary of relying on acupunc-ture in this potentially dangerous situation.
This book is written by an experienced andwell-known author in the field, and is supportedby the experience of acupuncturists in Chineseuniversities. However, it will find few friends inthe world of medical acupuncture because of thelack of any evidence base, and this is a shame sincethere is a treasury of information within its pages.
Taken as a textbook for treating pain ingeneral, The Management of Post-operative Pain with
Acupuncture is an excellent source of ideas. Iwould have no hesitation in recommending it fora pain clinic. It might also be useful to colleagueswho work in palliative care. Both groups arelikely to meet complex pain symptoms moreoften than those of us dealing with relativelysimple joint and muscle pain in outpatients, andthey could find the detailed differentiation of theTCM syndromes a very good starting point foreffective treatments.
Dr Val Hopwood
Course Director
MSc Acupuncture
Department of Physiotherapy and Dietetics
Coventry University
Coventry
UK
ReferencesUsichenko T. I., Dinse M., Lysenyuk V. P., et al. (2006)
Auricular acupuncture reduces intraoperative fentanylrequirement during hip arthroplasty – a randomizeddouble-blinded study. Acupuncture and Electro-Therapeutics
Research 31 (3–4), 213–221.Wang H. H., Chang Y. H., Liu D. M. & Ho Y. J. (1997) A
clinical study on physiological response in electroacu-puncture analgesia and meperidine analgesia for colon-oscopy. American Journal of Chinese Medicine 25 (1), 13–20.
Wang S. M., Punjala M., Weiss D., Anderson K. & KainZ. N. (2007) Acupuncture as an adjunct for sedationduring lithotripsy. Journal of Alternative and Complementary
Medicine 13 (2), 241–246.
Teaching Atlas of Acupuncture,Volume 2: Clinical IndicationsBy Piero Ettore QuiricoThieme Medical Publishers, Stuttgart, 2007,272 pages, hardback, £100.00ISBN 978-3-131-41261-4
This is a very odd publication. Readers mayremember my review of the first book in this
Book reviews
� 2008 Acupuncture Association of Chartered Physiotherapists 103

series, Teaching Atlas of Acupuncture, Volume 1:Channels and Points (Quirico & Pedrali 2007) inthe last AACP Journal (Spring 2008, pp. 97–98),where I posed the questions with answersbelow:
‘‘Does the acupuncture world really needanother atlas of acupuncture points? Does thisbeautifully produced volume add anything towhat we already know? The answers wouldhave to be ‘not really’ and ‘not much’.’’
Sadly, I think that the answers have to be thesame this time. Quirico has provided a bookcontaining only acupoint indications. Since Imade much the same notes when I studied inNanjing, China, I fear that the four-volume set(two more are still to come) will be a reproduc-tion of the total teaching from the World HealthOrganization-collaborating college based there.Even if Teaching Atlas of Acupuncture, Volume 2,may be a valuable source of knowledge to abeginner in the acupuncture field – and as such,it is a beautifully produced book, well bound andlikely to last a long time – it will add little to theexisting literature.
The text deals with the acupuncture points,detailing names, meanings and locations. Clinicalindications are described, and data taken fromTCM are compared with the clinical signs andsymptoms of Western medicine.
The first of the four chapters deals with theacupuncture points of the 12 main channels. Thesecond describes acupuncture points on the Ren(Conception Vessel) and Du (Governor Vessel)meridians. Chapter 3 deals with the Extra acu-puncture points, listing them by region. Thefinal, very short chapter talks about the system ofpoints and channels, discussing the characteris-tics of the different kind of points (e.g. He Sea,Spring and Yuan source).
There are no illustrations. There is some brieftext on the physical location of each point,together with indications and main combina-tions. The general tone of this book is bestillustrated by an example in the next column.
It can be seen that there is quite a lot ofinformation in Teaching Atlas of Acupuncture, Vol-ume 2, but I feel that other books have done thisbetter, the main rival being that written byDeadman et al. (1998), which has, in addition,beautiful illustrations.
Again, if you are buying for the first time, thisbook might be a good investment. Most of usdon’t have time to read extensively about singlepoints while working in a busy outpatient depart-ment, but maybe in a coffee break? I wouldsuggest that Teaching Atlas of Acupuncture, Volume2, would be a useful book to have as a referencein the physiotherapy department. It is quiteexpensive, but is nicely bound and would lastwell with regular use.
Dr Val Hopwood
Course Director
MSc Acupuncture
Department of Physiotherapy and Dietetics
Coventry University
Coventry
UK
ReferencesDeadman P., Al-Khafaji M. & Baker K. (1998) A Manual of
Acupuncture. Journal of Chinese Medicine Publications,Hove.
Quirico P. E. & Pedrali T. (2007) Teaching Atlas of Acupunc-
ture, Volume 1: Channels and Points. Thieme MedicalPublishers, Stuttgart.
TB 8 San Yang Luo – Three Yang Connection
san = three: yang = yang: luo=convergence.At this point the three yang channels of the upper limbs meetand converge.Location: 2 cun above TB 5 Waiguan at the lower third of thedorsal aspect of the forearm.
Western medicine Traditional Chinese Medicine
Tinnitus, loss of hearing,sudden aphonia
Local effect on the ears andthroat
Pain and stiffness of the Bi syndromeforearm, shoulder and neck.Toothache
Obstruction of the three yangchannels of the arm
Thoracic operations(surgical analgesia)
Remarks: In clinical practice this acupuncture point is not used much– even though it acts on the territory of all the yang channels –becauseTB 5 Waiguan is usually preferred.
TCM functions
Crossing of the three yang channels of the arm.
TB 8 San Yang Luo Main Combinations
+ GB 20, CV 23 Sudden aphonia+ GV 15 Sudden aphonia+ TB 2 Sudden deafness+ LI 4 Toothache
Book reviews
� 2008 Acupuncture Association of Chartered Physiotherapists104

Acupuncture Research: Strategies forEstablishing an Evidence BaseEdited by Hugh MacPherson,Richard Hammerschlag, George Lewithand Rosa SchnyerChurchill Livingstone, London, 2007,288 pages, paperback, £29.99ISBN 0-443-10029-2
The editors of this long-awaited book have dem-onstrated expertise in both research into acu-puncture intervention and its clinical application.Acupuncture Research is welcome not only becauseit offers such easy reading while engaging thereader’s total interest, but also because it managesto offer the struggling clinician, eager to makesense of acupuncture intervention and clinicaleffectiveness, a lifeline. The book encourages itsreaders to ‘‘have a go’’, to initiate small-scaleresearch in order to be heard, which is especiallyimportant in today’s healthcare arena.
Acupuncture Research provides a logical journeythrough the areas of research courtesy of anumber of well-known experts who have clearlycollaborated and not merely contributed eachchapter in isolation. The most important aspectof this book for my purposes is that it managesto adopt a global approach to research, usingeasy, bite-sized pieces, whilst integrating bothTCM and Western acupuncture management.It makes no attempt to segregate these twophilosophies, something I welcome in ourpresent, evidence-based society, and a positionthat is particularly welcome within physiotherapymanagement.
As those of you who know me and listen tome teach will appreciate, I feel passionately aboutsupporting the need to move away from pointprescription, from sham versus real acupuncture,from the ever-varying and confusing methodsand ideas of acupuncture interventions. We mustdevelop and maintain good research thatinvolves clinical effectiveness, cost-effectivenessand clinical reasoning for the disease processpresented at the time of intervention. We mustinvestigate and research the effectiveness of inte-grating acupuncture alongside and adjacent toother physiotherapy management skills, not as analternative or as a last resort, but as mainstreammanagement within physiotherapy healthcaretoday.
Acupuncture Research supports these views whileequally identifying the complexity of acupunctureresearch when reduced to the randomized con-trolled trial. Each chapter leads the reader throughthe initial concepts and investigations, which I amsure we have all experienced within our clinicalworkload. It encourages practitioners to takeeasy steps via case studies or single-series studieswithout losing sight of patients’ perspectives. Itencourages both qualitative and quantitativeresearch methodology as a means of getting closerto answers for more extensive research trials.
The contributors discuss at length the difficul-ties of controlling for placebo while investigatinga dynamic and interactive intervention, andadhering to rules of rigor and elimination of biaswhile simultaneously challenging the biomedicalmodel of health and disease, and supportingand reinforcing the credibility of acupunctureintervention.
I welcome Acupuncture Research and would sug-gest that this is an invaluable text for all thosewho are about to embark upon research, whetherwithin a National Health Service or privateclinical setting, or an academic environment viathe undergraduate or MSc routes. I would alsorecommend it to those who are keen to investi-gate their own clinical results via small studiesand case reports. This book will be an invaluableaddition to any personal, clinical or universitylibrary, and on a personal note, this has suddenlyfuelled my own interest in research again.
Acupuncture Research is essential to any physio-therapist who is interested in taking their clinicalacupuncture knowledge into another investiga-tive dimension, and I thank the authors for theirclear insight, expert advice and encouragementto all those who feel wary about taking this step.
Jennie Longbottom
Chair
Chinese Auricular AcupunctureBy Skya AbbateCRC Press, Boca Raton, FL, 2003, 240 pages,hardback, £37.99ISBN 0-8493-2052-6
In classical Chinese medicine, the ear is consid-ered to be one of the acupuncture microsystems,an extraordinarily powerful nexus of energy
Book reviews
� 2008 Acupuncture Association of Chartered Physiotherapists 105

through which the entire body can be treated.Unlike the many current texts that apply Westernapproaches to Eastern medicine, Chinese Auricular
Acupuncture explains ear acupuncture within aframework of traditional Oriental energetics con-sistent with the general use of TCM approaches.
Written by an experienced practitioner andteacher of auricular acupuncture, this modern,user-friendly guide provides students and prac-titioners with a concise manual of ear acupunc-ture. This book has been in print for a few years,but remains unique because it simplifies the artof auricular acupuncture by relying solely on theTCM ear map rather than a set of complex chartsand systems.
The location of the points is dealt with in astraightforward style, with groups of points beinglocalized within each anatomical zone of the ear.This makes the location of what are termed the100 common points relatively easy to learn fromthe small local diagrams. Points are numberedand then named according to Chinese conven-tion, but English names are used throughout.
Photographs are used to illustrate commontypes of ear pathology and include instruction ondiagnosis. Some of these pictures are a little dark,but they do serve as useful indicators of some ofthe features described. The text features theChinese clinical energetics of ear acupoints inter-faced with the most common diagnostic para-digms. It also contains a detailed discussion ofhow to construct prescriptions tailored to thepatient rather than the disease process. Infor-mation is given on the different methods oftreating the ear points, dealing with tacks, seeds,magnets, laser and electroacupuncture.
There are some oddities in several of theformulae that are given. For instance, there is aspecific prescription of seven points for theelderly patient. These are Shenmen, Sympathetic,Kidney, Spleen, Stomach, Brain and Liver. It issuggested that seeds or pellets are used and leftin situ, rather than needles. There is also aprescription intended for use in palliative careincluding, in addition to the previous points,Lung (Upper and/or Lower).
Another gem is the Nanking Army ear acu-puncture prescription developed in China in the1960s, a variation on the theme mentioned above.This is now generally considered to be a ‘‘preven-tion of disease’’ treatment, having been tested by
the army as a defence against both malaria andinfluenza (Huang 1974, quoted also in the reviewof ear acupuncture by Gori & Firenzuoli 2007).
This approach explains the practical utilizationof auricular therapy in a manner that is memo-rable, clinically useful and based on the under-pinnings of an education in TCM. Mostimportantly, Chinese Auricular Acupuncture alsoincludes a wide-ranging and comprehensive setof research references, particularly in the lastchapter, ‘‘Clinical research and effective points’’.
This book is also available as an e-book,costing US$93.27 to download from:
http://ebooks.ebookmall.com/title/chinese-auricular-acupuncture-abbate-ebooks.htm
Dr Val Hopwood
Course Director
MSc Acupuncture
Department of Physiotherapy and Dietetics
Coventry University
Coventry
UK
ReferencesGori L. & Firenzuoli F. (2007) Ear acupuncture in Euro-
pean traditional medicine. Evidence-based Complementary
and Alternative Medicine 4 (Suppl. 1), 13–16.Huang H. (1974) Nanking Army Ear Acupuncture Team.
Rodale Press, Emmaus, PA.
Talking about Acupuncture inNew York, 5th revised ednBy J. R. WorsleyWorsley Inc., London, 2004, 109 pages,paperback, £14.99ISBN 0-9545939-1-X
This charming little book is a verbatim record ofa series of lectures given over just one day byJ. R. Worsley, one of the most famous foundersof acupuncture in the UK. This one-day seminarwas held in New York on 20 October 1980, andthe book is a transcript of a recording madeat the time. Thus, Talking about Acupuncture in
New York captures the flavour of the spirit andanimation shown by the speaker, right down tosome pretty feeble jokes!
Most physiotherapists don’t tackle the com-plexities of Five Element acupuncture, oftenperceiving it as being very complex and difficult.
Book reviews
� 2008 Acupuncture Association of Chartered Physiotherapists106

These short talks are a very good introductionand may change your mind. The language is clearand there are no obscure philosophies to grapplewith. Interestingly, the author was originally aphysiotherapist himself.
The fundamentals of his acupuncture theorieslie within nature itself. Worsley postulates that agreat deal of human sickness is caused by ourloss of ‘‘oneness’’ with nature and our failure torecognize the natural processes of disease. Hediscusses the five basic laws: the Law of the FiveElements; the Law of Mother/Child; the Law ofMidday/Midnight; the Law of Husband/Wife;and the Law of Cure. His careful explanations ofthe relationships of the organs to one anotherwill certainly shed light on difficult diagnosticproblems. There are some very useful ideascontained in his discussion of the functions ofthe Pericardium (he calls this Circulation/Sex)and the Triple Burner (or Sanjiao), both of whichcause confusion in the medically trained mind.
It makes uncomfortable reading at times.Worsley’s belief that much our modern disease isself-inflicted rings true. He also has no time forabbreviated versions of the great Chinese art andmight have been unhappy with what the AACPoffers as a foundation course. His point of viewis that this ‘‘barefoot doctor’’ technique is onlyconcerned with temporary pain relief and herefers to it as only first-aid, failing to address theroot causes of the problems. Personally, I thinkthat physiotherapists have proved that, far fromputting patients off the idea of acupuncture, theirversion of it has done a great deal of good: it hasboth popularized the technique and encouragedfurther research over the years. Of course, thereis no question of research evidence being pro-vided for the author’s assertions of long-lastingclinical effectiveness.
Worsley’s sometimes controversial opinionsshould not dissuade you from reading an enter-taining collection of ideas explaining and illustrat-ing some of the fundamental Chinese concepts.
Dr Val Hopwood
Course Director
MSc Acupuncture
Department of Physiotherapy and Dietetics
Coventry University
Coventry
UK
Gynaecology Revisited: Obstetrics andGynaecology for Practitioners ofChinese MedicineBy Robin MarchmentChurchill Livingstone, London, 2007,250 pages, paperback, £40.99ISBN 0-729-53858-3
This book is a welcome change from the vastscripts often presented in the field of gynae-cology and TCM. It is also a welcome surprisebecause it announces on the cover what it doesinside: it presents a succinct account of obstetricsand gynaecology for practitioners of TCM, butnot for those who are not well versed in thismodel of acupuncture and herbal medicine.
Gynaecology Revisited succeeds in encapsulatingthe relevant facts concerning the more ‘‘common’’presentations of women’s health and disease pro-cesses that pertain to the biomedical model, theTCM model and herbal medicine management. Iapplaud this integrated approach, and encourageall those involved in the complex world of wom-en’s health, both the clinician and the researcherwho is attempting to integrate clinical interven-tions within a holistic approach, to adopt it.
This book is an attempt to transcend thehistorical concepts of TCM and herbal medicinewhile embracing current physiological andpsychological processes, and I believe that itsuccessfully integrates the ‘‘mind and body’’interaction, which is so very pertinent togynaecological dysfunction.
One disappointing aspect of Gynaecology Revisited
is that the chapter layout and text become veryhaphazard and difficult to read at times, especiallywith the variation in font styles and sizes through-out each chapter. I believe that the book wouldhave benefited from a more systematic approachto each treatment category under discussion.
The appendix offers the clinician excellentreferences for treatment, but fails to cite anyevidence for point contraindication in pregnancyor the safety issues regarding acupuncture withinpregnancy.
This said, Gynaecology Revisited is a valuablebook for those experienced TCM practitionerswho work in the field of women’s health.
Jennie Longbottom
Chair
Book reviews
� 2008 Acupuncture Association of Chartered Physiotherapists 107


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 109–111
Letters
Self-acupunctureI read with interest the position statementsfrom the British Medical Acupuncture Society(Cummings 2008) and the British AcupunctureCouncil (Bishop 2008) that were published in theSpring 2008 edition of the Journal.
To summarize their views concerning thethorny subject of teaching patients ‘‘self-needling’’:+ neither group has a policy;+ neither sees that the process of self-
acupuncture should not be considered if thecircumstances are appropriate, the properguidance is given and the procedure isaudited; and
+ both groups are rightly concerned aboutmonitoring the process.
Assuming that the AACP is reviewing its ownpolicy, then perhaps the Association shouldreassess the recently published AACP Guidelines
for Safe Practice (AACP 2007). The Associationappears to be happy to provide guidance for apatient using moxa, a treatment that has, in itself,as much potential to harm as self-acupuncture.
Perhaps we should all remember the day whenwe learned to insert a needle. . . This was some-thing that was worse for us, as both therapistsand individuals, because we had knowledge of allkinds of possible reactions (e.g. serotonin andmuscle twitch), and at the same time, weremembers of the public with our own anxieties. Idare to suggest that we were probably moreanxious than our patient/colleague when we puta needle into an individual for the first time.
Yet we knew that the technique was safe,effective and could bring lasting relief.
We used our education.Surely that’s what it’s about? Education of
the appropriate patient or patient’s partner – theprecise control of a treatment remaining with thetherapist and being monitored by phone, e-mail,follow-up appointments, and by changing treat-ment as necessary.
Here’s an example: a colleague of mineworked in London in an office environment.
She wasn’t a therapist, but a sensible, motivatedlady with chronic tennis elbow. Appointmentswere difficult – one every 3 weeks was achiev-able, as long as a late slot was available. I askedthis patient if she would have been happydoing some of her own treatment, under strictinstruction. ‘‘Absolutely,’’ she told me – shewould have jumped at the chance! And I wouldhave had no qualms about showing her how todo it since I would have retained control of theintervention.
Mike Cummings’ (2008, p. 48) last paragraphsmacks of good old common sense. He doesn’tsuggest that we shy away from giving the rightpatient some control over their treatment whilstproviding a service designed to empower theirrecovery. Like any clinical decision, this has tocome from ourselves, as independent prac-titioners – it’s about our judgement of thesituation and sensible application. It’s intriguingthat Cummings (2008) mentions a hospital thatteaches self-auricular acupuncture – this tech-nique has far more chance of causing lasting andunpleasant tissue damage!
Ronald Bishop’s (2008) view regarding theenergetic aspect of the intervention does, ofcourse, also have some credence, and in general,the therapeutic session is better when performedby someone other than yourself. This is to dowith the bioelectrical change associated withtissue injury and how we influence that (Becker& Selden 1985; Lee et al. 2005). Nevertheless,affecting tissue impedance is all important, asrecent research into the role of fascia and trans-mission is showing (Ahn et al. 2005; Kao et al.
2006). Therefore, surely, the more we canencourage and manipulate that physiology, thequicker things will recover?
However, if we keep it simple and within thephysical framework within which many of uswork, the questions should be: what are wesuggesting that the patient goes away and nee-dles, and why? We are not going to propose thatpeople start furiously needling their spinal Blad-der line, but conditions that might come underconsideration include:
� 2008 Acupuncture Association of Chartered Physiotherapists 109

+ knee pain;+ shin splints;+ Achilles tendon;+ tennis elbow; and+ finger pain.
(These are only suggestions – not an exhaus-tive list!)
The sad fact is that anyone can go on Amazonand buy a book entitled Teach Yourself Acupuncture
(Weaver 1998) – and anyone can buy needlesfrom the myriad of suppliers on the Internet.
It would be much better if we could providecredible guidance based on relevant researchfindings within the health service in which wework.
One of Cummings’ (2008) phrases thatdeserves highlighting is the ‘‘well-managed thera-peutic process’’. This sums up how, perhaps, weshould reconsider the value of teaching the rightpatient self-acupuncture within a precise frame-work based on our clinical experience.
Lynn Pearce MCSP LicAc Cert Med Ed
Chartered Physiotherapist and Licensed Acupuncturist
AACP Tutor and Senior Part-time Lecturer
Coventry University
Coventry
UK
E-mail: [email protected]
ReferencesAcupuncture Association of Chartered Physiotherapists
(AACP) (2007) AACP Guidelines for Safe Practice, RevisedEdition. Acupuncture Association of Chartered Physio-therapists, Peterborough.
Ahn A. C., Wu J., Badger G. J., Hammerschlag R. &Langevin M. H. (2005) Electrical impedance alongconnective tissue planes associated with acupuncturemeridians. BMC Complementary and Alternative Medicine 5
(10), DOI: 10.1186/1472-6882-5-10.Becker R. O. & Selden G. (1985) The Body Electric:
Electromagnetism and the Foundation of Life. Quill, NewYork, NY.
Bishop R. (2008) Self-needling: a British AcupunctureCouncil position. Journal of the Acupuncture Association of
Chartered Physiotherapists Spring, 51–52.Cummings M. (2008) Self-needling: a British Medical
Acupuncture Society position. Journal of the Acupuncture
Association of Chartered Physiotherapists Spring, 47–49.Kao M.-J., Hsieh Y.-L., Kuo F.-J. & Hong C.-Z. (2006)
Electrophysiological assessment of acupuncture points.American Journal of Physical Medicine and Rehabilitation 85
(5), 443–448.
Lee M. S., Lee Y.-H., Shin B.-C., et al. (2005) Is there anyenergy transference during acupuncture? American Journal
of Chinese Medicine 33 (3), 507–512.Weaver P. R. (1998) Teach Yourself Acupuncture: A Beginner’s
Guide for the Busy Health Professional. Spinal PublicationsNew Zealand, Raumati Beach.
Doctoral researchI am a physiotherapist who has practised acu-puncture since 2001. I intend to undertake anMSc in Acupuncture in the near future, andduring a discussion with a course tutor, a bookentitled The Unwritten Rules of PhD Research (Rugg& Petre 2004) was recommended to me. Ipresent the following review of this work in thehope that other readers of the Journal will find ituseful if they are contemplating a researchproject of their own.
The Unwritten Rules of PhD Research is not aheavyweight academic text, but rather, a com-panion guide that aims to help the reader navi-gate through what may be uncharted waters.The authors start by describing the two maincategories of problems for PhD students: ‘‘bigpicture knowledge’’ and ‘‘craft skills’’. In the firstcase, readers are asked to consider what theywant to do with their PhD once they have beenawarded it, and thus, are forced to think clearlyabout whether the project will achieve itsintended outcome or if a slightly different coursewould be more appropriate. Secondly, theauthors discuss a variety of skills that can help toprevent researchers from getting bogged down.Some of these competencies are obvious, such asremembering to back up your work, and someare more obscure – and all the more useful for it.
Subsequent chapters focus on the procedures,milestones and systems that research studentswill encounter. Once you have gone through theprocess, a great deal of this will become obvious.Nevertheless, it is useful for the uninitiated tolearn not only what they have to plan for next,but also what they must start thinking about inorder that they do not run out of time or capacityat a later date. Underpinning this are regularreferences to dealing with the enormity of theproject; for example, how to cope with criticism,and the problem of ‘‘taking ages to go nowhere’’,a situation that I am sure will be familiar to manyin academia. The authors also discuss getting thebest from your supervisor.
Letters
� 2008 Acupuncture Association of Chartered Physiotherapists110

Despite its title, the advice given in The Unwrit-
ten Rules of PhD Research is equally applicable tonon-PhD-level students. The chapter on per-sonal support networks provides an insight intohow the burden can be lessened – if not lifted –during the process. Equally, the chapters onreading provide the researcher with a reasonablyquick reference guide to searching for and scru-tinizing the relevant literature in an effective andtime-efficient manner.
The greater part of the book is devoted toacademic writing, and what this means in termsof structure and style. There is also advice onhow to move forward when the words just won’tcome. This latter concept is probably theauthors’ greatest strength. A research studentmay reasonably expect to receive guidance fromtheir supervisor or course leader about what theyshould do when the work is going well, butadvice about what to do when things go wrongmay be less forthcoming. Frequent references tohow to deal with these situations are made.Unusually for a book on academic research, theauthors have included a chapter called ‘‘WhatNext?’’, covering career goals, job interviews andcurricula vitae, which may or may not be relevantto the non-PhD student.
I will conclude by answering three questions.First, is this book just for PhD students? No, I
can recommend it anyone embarking on post-graduate academic study. Secondly, since thisbook was published 4 years ago, is it worth thetrouble? In my opinion, it is: this is by no meansthe only text dealing with this subject; however,it is a useful and often humorous companion tothe more weighty subject matter that theresearch student will require. Thirdly, do I reallyneed to read a book like this before I embarkupon my research project when I have so manyothers to get through? The answer to that mustbe no. However, investing a little time in thisvery readable book at the beginning of such aproject may well save you a lot of heartache inthe long run. I certainly wish that I had read The
Unwritten Rules of PhD Research at the start of myfirst MSc and I’m glad to have it at the beginningof my second.
Sherin Roffey
RRU Aldershot
Aldershot
UK
E-mail: [email protected]
ReferenceRugg G. & Petre M. (2004) The Unwritten Rules of PhD
Research. Open University Press, Maidenhead.
Letters
� 2008 Acupuncture Association of Chartered Physiotherapists 111


Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 113–116
News from the front
AACP website: www.aacp.comWhilst members may be aware of the AACPwebsite, it may surprise you to learn that, out ofthe total membership of 4891, only 808 hadvisited the site as of 19 March 2008, with afurther 583 repeat visits. This is an astonishingand puzzling finding: why are so few membersusing the site? If you are one of those who haveyet to access www.aacp.com, please let us knowwhy. The Webmaster has worked extremely hardto ensure that the site is accessible, informativeand useful (see pp. 15–17).
For those of you who have either neveraccessed the website or have not visited it sincethe upgrade, there are a number of new features,including:+ Continuing professional development (CPD) records.
If you are looking for somewhere to log yourCPD, look no further than the ‘‘My member-ship’’ section. Here you can easily andconveniently enter all your CPD activities.
+ Online research databases. A new function allowsyou to access the CINAHL, Medline andAMED databases. This enables you to haveinstant access to current research papers thatwill enhance your research-based practisetechniques. To access this function, look in‘‘References’’ and follow the link to ‘‘Onlineresearch databases’’.
Rosemary Lillie
News Editor
Acupuncture and IVFThere have recently been conflicting reports inthe press concerning the effects of acupunctureon the success rates of in vitro fertilization (IVF).In October last year, BBC News online led with‘‘Acupuncture ‘may cut IVF chances’’’ (BBCNews 2007), and the Telegraph online reportedthat ‘‘Acupuncture does not aid IVF’’ (TelegraphNewspaper 2007). In contrast, BBC News andTimes Online respectively announced thisFebruary that ‘‘Acupuncture boosts IVFchances’’ (BBC News 2008) and ‘‘Course of
acupuncture may raise success of IVF treatmentby 65%’’ (Times Online 2008). Therefore, it isnecessary to look beyond the headlines and studythe evidence.
The reports published in October 2007 relateto an oral presentation at the 63rd AnnualMeeting of the American Society for Reproduc-tive Medicine (Craig et al. 2007). This describeda multicentre, prospective randomized studyinvolving 107 patients. The proportion ofpatients with a positive pregnancy test was higher(78.3%) in the control group than the acupunc-ture group (52.1%). However, this study has notas yet been published in full, so it is not possibleto critically analyse the results.
The February 2008 headlines refer to an articleby Manheimer et al. (2008) that was published inthe British Medical Journal in March. This was asystematic review and meta-analysis of seventrials involving 1366 women. The conclusion ofthe authors is: ‘‘Current preliminary evidencesuggests that acupuncture given with embryotransfer improves the rate of pregnancy and livebirth among women undergoing in vitro fertilis-ation.’’ The clinical findings of the study demon-strated an odds ratio of more than 1:6 forpregnancy after IVF with adjuvant acupuncture,which suggests that acupuncture increases theodds by 65% when compared with controlgroups. However, the odds ratio significantlyoverestimates the rate ratio in this context, inwhich pregnancy is relatively frequent anyway.Therefore, in absolute terms, an average of 10patients would need to be treated with acupunc-ture to result in one extra pregnancy. Further-more, in in vitro settings where the baselinepregnancy rate is already high, the relative addedvalue of acupuncture may be reduced.
In terms of the hierarchy of evidence, asystematic review and meta-analysis is a robustand powerful method, and this research shouldbe regarded as indicating that there is a positiveeffect when acupuncture used in conjunctionwith IVF. However, if acupuncture is adminis-tered, it is vital that it is done with the fullcooperation and agreement of the IVF centre.
� 2008 Acupuncture Association of Chartered Physiotherapists 113

Furthermore, this treatment should only becarried out by an experienced practitioner whohas been trained to understand and evaluatephysiological changes, and who adapts any treat-ment according to the results of laboratorytesting and hormonal readings. The practitionermust work in close collaboration with consult-ants, midwives and the trained staff of an assistedconception unit.
Rosemary Lillie
News Editor
ReferencesBBC News (2007) Acupuncture ‘‘may cut IVF chances’’.
[WWW document.] URL http://news.bbc.co.uk/1/hi/health/7047431.stm (Accessed 20 October 2007.)
BBC News (2008) Acupuncture ‘‘boosts IVF chances’’. [WWWdocument.] URL http://news.bbc.co.uk/1/hi/health/7233500.stm (Accessed 8 February 2008.)
Craig L. B., Criniti A. R., Hansen K. R., Marshall L. A. &Soules M. R. (2007) Acupuncture lowers pregnancy rateswhen performed before and after embryo transfer.Paper presented at the American Society for Reproduc-tive Medicine 63rd Annual Meeting, Washington, DC,16 October 2007.
Manheimer E., Zhang G., Udoff L., et al. (2008) Effects ofacupuncture on rates of pregnancy and live birth amongwomen undergoing in vitro fertilisation: systematic reviewand meta-analysis. British Medical Journal 336 (7643),545–549.
Telegraph Newspaper (2007) Acupuncture does not aid IVF.[WWW document.] URL http://www.telegraph.co.uk/news/main.jhtml?xml=news/2007/10/17nbirth217.xml (Accessed 20 October 2007.)
Times Online (2008) Course of acupuncture may raise success of
IVF treatment by 65%. [WWW document.] URL http://www.timesonline.co.uk/tol/life_and_style/health/article3327648.ece (Accessed 8 February 2008.)
Recording acupuncture: is therea place for proformas?The document section of iCSP contains a seriesof proformas designed by the Pennine AcuteHospitals NHS Trust physiotherapy departmentsthat include input from AACP members.Although the documents that have beenpublished are intended to record treatment forpain, the proformas can be adapted for otherconditions.
Accompanying this material is a documentoutlining the areas incorporated into the pro-forma, which include patient and therapist
details, consent, treatment approach,experience/expectation of acupuncture, con-traindications and adverse effects, point selec-tion, outcomes, and a body chart.
These proformas have presumably beendesigned and published to fulfil a perceived need,but do they have a place in clinical practice?
‘‘For many years, those who have pioneeredacupuncture within physiotherapy have workedto integrate the modality as a means of effective,evidence-based physiotherapeutic interventionfor the management of pain,’’ responds JennieLongbottom, AACP Chair. ‘‘This pioneeringwork undertaken by Dr Val Hopwood and hercolleagues in 1986 attempted at all times to bringtogether the art and science of acupuncture,which is proven to offer physiotherapists trainedto a standard set by the AACP a safe, effectivemodality within the physiotherapy tool box. Thiswas the main aim of the AACP: safe, effectiveacupuncture when used by trained physio-therapists. Above all, it was viewed as a main-
stream physiotherapy modality. This enabled theAACP to achieve clinical interest group statuswithin the CSP and acupuncture to be consid-ered within the scope of CSP practice.
‘‘Why then are we attempting to make this mainstream
modality more complex by producing lengthy proforma,
which merely offer a separate case for acupuncture?’’
Jennie poses the following questions:+ Do we have body charts and line drawings to
indicate where ultrasound is being given?+ Do we leave a lengthy proforma for the next
physiotherapist to continue ad infinitum with-out clinical assessment at each patientappointment?
+ Do we continue with the same points whenpatients are transferred from one therapist toanother, or do we reassess and use a clinicalreasoning model to determine the painpresentation, the points used to address thepain on the day of assessment and thechanges in the patients’ conditions?
+ Do we record interferential/transcutaneouselectrical nerve stimulation electrode place-ment with the same vigorous routine andprescription?
Within the medicolegal aspect of recordingtreatment, Jennie points out, physiotherapists arerequired to record the following:
News from the front
� 2008 Acupuncture Association of Chartered Physiotherapists114

+ Acupuncture point number with side of application,
and adverse effects, if found. The length of needle,date of sterilization and depth of needling arenot required. These are taught to AACPstandards on the Foundation courses and arerecognized by the World Health Organizationas established points within acupunctureintervention.
+ Trigger point application. The named musclebeing needled is required, and the number oftrigger points deactivated, adverse effects andthe outcome must be recorded. Once again,depth, angle and needling are taught to AACPstandards on the Trigger Point Course, and assuch, practitioners should be trained in thisapplication. If not, they should not use it untilthey have been.
+ Periosteal pecking. The site, number of needles,adverse effects and outcome are required.These are all taught by AACP tutors on theAssociation’s courses.
‘‘I will not continue to mention each acupunc-ture technique,’’ Jennie adds, ‘‘but suffice to say,the act of recording drawing and documentingeach point on numerous body charts merelyserves to deprive the physiotherapist of valuabletreatment time; it provides little else in the realmsof medicolegal requirements. As a paper exercise,it provides no facts regarding effectiveness oftreatment and merely serves to enable anotherphysiotherapist to pick up the identical pointswhen this is not the required standard of clinicalreasoning within acupuncture.
‘‘As a means of education and offering anaide-mémoire for those therapists starting out ontheir clinical acupuncture careers, this may havesome use, but as a standard proforma, I wouldsuggest that this may also prevent us from‘thinking outside the point prescription box’.’’
What do you think, readers? Do you useproformas? Perhaps you could let us know aboutyour experience of recording acupuncture bywriting a letter for publication in the Journal.
Rosemary Lillie
News Editor
In the news: Peter ButcherPeter Butcher MCSP MMACP GradDipPhyssuccessfully completed the AACP Foundation
Course in September/October 2007. There’snothing remarkable about that, you might think,but as a result of this qualification, he was notonly featured in his local newspaper, the Bexhill-
on-Sea Observer, in December 2007 (Lake 2007),but also appeared on the BBC’s South East Today
news programme on 27 March 2008.Peter qualified in 1979 from the North
London School of Physiotherapy, and specializesin manipulative and manual therapy. In 1985,he became a member of the ManipulationAssociation of the Chartered Association ofPhysiotherapy, and worked at St CharlesHospital, West London, and Bexhill Hospitalbefore setting up in private practice in 1993. Hisintention is to develop and consolidate his use ofacupuncture over the next 3 years, particularlywith respect to trigger point therapy.
When Peter was first approached by the BBC,he declined to be involved because he wasworried that the emphasis would be on thefact that he is a blind person who uses acu-puncture. His wife suggested that it might beakin to watching somebody pin the tail on thedonkey.
It took at least a month of persuasion by theBBC before he agreed to participate in filming.Peter did not want the story to be screened forits novelty value and end up following theweather forecast as a kind of novelty item. Heexplained to the production team that approxi-mately 15 000 physiotherapists in the countrypractise acupuncture, and that some of his blindcolleagues have been using it for 20–30 years.
Peter treated a patient for tennis elbow duringfilming, which took nearly 3 h. The item omittedhis examination and treatment of the patient’sneck and thoracic spine, as well as his demon-stration of a muscle re-education programmeand neural mobilization exercises. He detectedthe cameraman’s rather morbid curiosity as theneedles were inserted into the patient. As Petertapped the needle lightly through the dermallayers of the skin, the patient gave quite a jolt,and he was more than a little concerned that thegeneral public viewing this might think that hewas using a knitting needle!
Peter wanted to avoid the issue of blindness,and concentrate on acupuncture and its useful-ness as a tool in physiotherapy. He intendedto highlight the fact that physiotherapists use
News from the front
� 2008 Acupuncture Association of Chartered Physiotherapists 115

acupuncture in their everyday settings and workprimarily on pain relief.
Peter is particularly grateful to both JennieLongbottom and the Organisation of CharteredPhysiotherapists in Private Practice (PhysioFirst)Education Committee for giving him theopportunity to participate in the course.
If you would like to view the short film, youcan now access it online (YouTube 2008).
Rosemary Lillie
News Editor
ReferencesLake C. (2007) How Peter the blind physio is helping to
ease patients’ pain. Bexhill-on-Sea Observer 28 December2007, 7.
YouTube (2008) Peter Butcher physio & acupuncture. [WWWdocument.] URL http://www.youtube.com/watch?v=AhsUuWMXsyM (Accessed 6 June 2008.)
News from the front
� 2008 Acupuncture Association of Chartered Physiotherapists116

Journal of the Acupuncture Association of Chartered Physiotherapists, Autumn 2008, 117–118
Guidelines for authors
IntroductionAlways refer to a recent issue of the AACPJournal. Please follow the style and layout of anarticle or item that is similar to your contribution.If a paper is submitted for publication, then itis implied that it has not been simultaneouslysubmitted to another journal or any other type ofpublication. Academic and clinical papers aresubject to review by the editorial committee andmay require revision before being accepted.
Offprints are available free of charge if notice isgiven to the Clinical Editor when the article issubmitted. The Journal can also supply a PortableDocument Format (PDF) file of any article uponrequest.
Preparation of manuscriptsAll articles must be typed double-spaced withwide (3-cm) margins all round on one side ofA4-size paper. The pages should be numberedconsecutively, and two hard copies of the articleand a disk version (text saved in Rich TextFormat) should be submitted to the editor.Articles should be a maximum of 7500 words(excluding abstract and references).
Papers should be arranged as follows:
AbstractA summary of not more than 200 words shouldbe submitted on a separate sheet outlining thepurpose, scope and conclusions of the paper.This should be followed by a minimum of threeand a maximum of five keywords that bestrepresent the contents.
TitleThe title of the article should be in sentence case,bold and left-justified, as in the title above: notethat there is no full stop and no underlining. Theauthor’s name(s) and place(s) of work should runconsecutively below the title. Again, there shouldbe no full stops.
TextThe layout of the Journal is that the main headingof each section is in sentence case and bold.
Notice that, again, there are no full stops and nounderlining.
The first paragraph is left-justified; subsequentparagraphs in the same section are indented, as isthis part of the guidelines. When including tables,diagrams and figures, these should be numberedin the order in which they appear in the text, andshould be submitted, in duplicate, on separatesheets. Please indicate their placing in the text(e.g. ‘‘Fig. 1’’). Any caption should be left-justified below the relevant table or diagram. Allfigures and tables must be referred to in the text.When using numbers in the text, these should bewritten out as words up to and including nineunless they are measurements, numbers in tablesor units of time. Always use International Systemof Units (SI).
Clinical papers: referencingAll clinical papers must be fully referenced andthe references verified by the author. The refer-ence list must be double-spaced on separatesheets, and arranged alphabetically by the sur-name of the first author or editor, following theHarvard style. In the text, give the author(s) anddate of publication in brackets (e.g. ‘‘Smith1998’’), or if the main author’s name is part of asentence, then only the year is in brackets [e.g.‘‘as described by Smith (1998)’’]. For more thanone author, reference can be made in the text to‘‘Smith et al. (1998)’’ (note the italics). However,when writing the reference list, the convention isas follows: for up to five authors, write all theauthors’ names; for six or more authors, writethe first three author’s names, followed by et al.
For journals, give the author’s surname andinitials, the year of publication, the title of thepaper, the full name of the journal in italics, thevolume number, the issue number in brackets,and the first and last page numbers of the article:
Ceccherelli F., Rigoni M. T., Gagliardi G. & Ruzzante L.(2002) Comparison of superficial and deep acupuncturein the treatment of lumbar myofascial pain: a double-blind randomized controlled study. Clinical Journal of Pain
18 (3), 149–153.
� 2008 Acupuncture Association of Chartered Physiotherapists 117

For books, give the author’s/editor’s surnameand initials, the year of publication, the booktitle in italics, and the publisher and city ofpublication:
Williams P. L. & Warwick R. (eds) (1986) Gray’s Anatomy,36th edn. Churchill Livingstone, Edinburgh.
For a chapter or section in a book by a namedauthor (who may be one of several contributors),both chapter and book title in italics should begiven, along with the editor’s name(s) in brack-ets, and the first and last page numbers of thechapter:
Bekkering R. & van Bussel R. (1998) Segmental acupunc-ture. In: Medical Acupuncture: A Western Scientific Approach
(eds J. Filshie & A. White), pp. 105–135. ChurchillLivingstone, Edinburgh.
Please adhere strictly to this style of referenc-ing in any contribution to the Journal.
AcknowledgementsPlease state any funding sources, or companiesproviding technical or equipment support.
PhotographsThese can be colour or monochrome, but mustbe in sharp focus. If you are supplying prints,please write any caption on the back in softpencil since ball-point and felt-tipped penssmudge and leave an impression. If digital pho-tographs are submitted, these should be of highresolution (minimum 300 dots per inch), savedto floppy disk or CD-ROM, and accompanied byhard copies.
The photographs should also be numberedif there are more than one and their placingindicated in the text. All photos will be returned.
Case reportsThe Journal welcomes case reports of up to 2500words. These should be structured as follows:
title, abstract and keywords, a brief introduction,a concise description of the patient and con-dition, and an explanation of the assessment,treatment and progress, followed finally by adiscussion and evaluation of the implications forpractice. The report must be referenced through-out. Further guidance is available on request.
Book and software reviewsAt the beginning of the review, give all details ofthe book including the title in bold, the author/editor’s full name(s), publisher, city and year ofpublication, price, whether hardback or paper-back, number of pages, and ISBN number. Thereviewer’s name should appear at the end of thereview in bold, right-justified, followed by theirtitle and place of work in italics.
General points to notePlease enclose your home, work and e-mailaddresses, and telephone number(s).
It is the author’s responsibility to obtainand acknowledge permission to reproduce anymaterial that has appeared in another journal ortextbook.
A brief biographical note about the authorshould be included at the end of a clinical paperin italics.
All notes and news should have clinical rel-evance to the AACP. Please refer at all timesto the style and layout of previous issues ofthe Journal for whatever you are writing. Usingthese guidelines will save time for the editorialteam.
Any further enquiries should be addressed tothe Clinical Editor, whose name, address andcontact details appear on the contents page.
Guidelines for authors
� 2008 Acupuncture Association of Chartered Physiotherapists118

•
•
•
•
•
•
•
•
•
••••

��� ��������� �� � ���� ������������ ������ ����� �� ����������� ��� ��� �� ��������� �� ��� �� ����� ��� �������� ������ ��� ��� ���� ��� �� �� ��� ����� ��� �� �� � ��� � �� ���� ���
� � �� �� � �� ����� �� ���� ����� ��� ���� �� ���� ������ ���� � ��� �� ���� ���������� ����� ��� �� ����� ����
� �� � �� �� �� � ��� �� ������ ����! " #$�#$�� �� %& �������� �� ���
� '��� (���� � ���� ��� ) ����
� "��� �$� � �� � ����� �� ��� � ����
��� �� �������� ���������� ������ ���������� ������� �� ��� ��!��� ����� ���� �����
*��+ ,-$).#&/
��� � ����� ��
����




















