Acupuncture for spinal cord injury survivors in Chinese literature: A systematic review
12
Complementary Therapies in Medicine (2009) 17, 316—327 available at www.sciencedirect.com journal homepage: www.elsevierhealth.com/journals/ctim Acupuncture for spinal cord injury survivors in Chinese literature: A systematic review Byung-Cheul Shin a , Myeong Soo Lee b , Jae Cheol Kong c , Insoo Jang d,e , Jongbae J. Park d,∗ a Department of Rehabilitation Medicine, School of Korean Medicine, Pusan National University, Yangsan, South Korea b Division of Standard Research, Korea Institute of Oriental Medicine, Daejeon, South Korea c Department of Rehabilitation Medicine, College of Korean Medicine, Wonkwang University, Iksan, South Korea d Asian Medicine and Acupuncture Research, Department of Physical Medicine & Rehabilitation, School of Medicine, the University of North Carolina, Chapel Hill, NC, USA e Department of Internal Medicine, College of Korean Medicine, Woosuk University, Jeonju, South Korea Available online 21 October 2009 KEYWORDS Spinal cord injury; Acupuncture; Rehabilitation; Bladder dysfunction; Systematic review Summary Objective(s): To systematically review Chinese literature on the effectiveness of acupuncture for treating patients with spinal cord injury (SCI). Data sources: The Chinese electronic databases (China National Knowledge Infrastructure) were searched from their inceptions to May 2008. Study selection: Trials reporting randomized controlled trials (RCTs) where patients with SCI (with or without operation) were treated with acupuncture including electroacupuncture. Data extraction: Methodological quality was assessed with the PEDro scale. Discrepancies were resolved through discussions and arbitration by two co-authors. Results: : The searches identified 236 potentially relevant studies, of which 7 RCTs met the inclusion criteria. Five studies assessed functional recovery, and two bladder dysfunction. All the studies reported favourable effects of acupuncture on functional recovery or urinary function; however methodological quality of studies is poor in general. Meanwhile, pooled anal- ysis of two trials assessing bladder dysfunction showed positive effectiveness compared with conventional treatment (n= 128, RR 1.51 [1.21, 1.90], P =0.0004, heterogeneity Tau 2 < 0.01, Chi 2 = 0.01, P = 0.94, I 2 = 0%). Conclusion(s): Based on 7 RCTs done in China, the effectiveness of acupuncture for functional recovery and bladder dysfunction in SCI is suggestive. With the methodological quality of the included studies on functional recovery and the small number of studies on bladder dysfunction taken into consideration, further rigorous studies prove needed. © 2009 Elsevier Ltd. All rights reserved. We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated. ∗ Corresponding author at: UNC-Chapel Hill, School of Medicine, Department of Physical Medicine and Rehabilitation, 1st Floor, North Wing, UNC Hospitals, Campus Box #7200, Chapel Hill, NC 27599-7200, USA. Tel.: +1 919 966 5164; fax: +1 919 843 0164. 0965-2299/$ — see front matter © 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.ctim.2009.09.001
-
Upload
independent -
Category
Documents
-
view
8 -
download
0
Transcript of Acupuncture for spinal cord injury survivors in Chinese literature: A systematic review
C
AC
BI
a
b
c
d
te
A
o
0d
omplementary Therapies in Medicine (2009) 17, 316—327
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ierhea l th .com/ journa ls /c t im
cupuncture for spinal cord injury survivors inhinese literature: A systematic review�
yung-Cheul Shina, Myeong Soo Leeb, Jae Cheol Kongc,nsoo Jangd,e, Jongbae J. Parkd,∗
Department of Rehabilitation Medicine, School of Korean Medicine, Pusan National University, Yangsan, South KoreaDivision of Standard Research, Korea Institute of Oriental Medicine, Daejeon, South KoreaDepartment of Rehabilitation Medicine, College of Korean Medicine, Wonkwang University, Iksan, South KoreaAsian Medicine and Acupuncture Research, Department of Physical Medicine & Rehabilitation, School of Medicine,he University of North Carolina, Chapel Hill, NC, USADepartment of Internal Medicine, College of Korean Medicine, Woosuk University, Jeonju, South Koreavailable online 21 October 2009
KEYWORDSSpinal cord injury;Acupuncture;Rehabilitation;Bladder dysfunction;Systematic review
SummaryObjective(s): To systematically review Chinese literature on the effectiveness of acupuncturefor treating patients with spinal cord injury (SCI).Data sources: The Chinese electronic databases (China National Knowledge Infrastructure) weresearched from their inceptions to May 2008.Study selection: Trials reporting randomized controlled trials (RCTs) where patients with SCI(with or without operation) were treated with acupuncture including electroacupuncture.Data extraction: Methodological quality was assessed with the PEDro scale. Discrepancies wereresolved through discussions and arbitration by two co-authors.Results: : The searches identified 236 potentially relevant studies, of which 7 RCTs met theinclusion criteria. Five studies assessed functional recovery, and two bladder dysfunction.All the studies reported favourable effects of acupuncture on functional recovery or urinaryfunction; however methodological quality of studies is poor in general. Meanwhile, pooled anal-ysis of two trials assessing bladder dysfunction showed positive effectiveness compared withconventional treatment (n = 128, RR 1.51 [1.21, 1.90], P = 0.0004, heterogeneity Tau2 < 0.01,
Chi2 = 0.01, P = 0.94, I2 = 0%).Conclusion(s): Based on 7 RCTs done in China, the effectiveness of acupuncture for functionalrecovery and bladder dysfunctioincluded studies on functional retaken into consideration, furthe© 2009 Elsevier Ltd. All rights re� We certify that no party having a direct interest in the results of ther on any organization with which we are associated.∗ Corresponding author at: UNC-Chapel Hill, School of Medicine, Depar
North Wing, UNC Hospitals, Campus Box #7200, Chapel Hill, NC 27599-7
965-2299/$ — see front matter © 2009 Elsevier Ltd. All rights reserved.oi:10.1016/j.ctim.2009.09.001
n in SCI is suggestive. With the methodological quality of the
covery and the small number of studies on bladder dysfunctionr rigorous studies prove needed.served.research supporting this article has or will confer a benefit on us
tment of Physical Medicine and Rehabilitation, 1st Floor,200, USA. Tel.: +1 919 966 5164; fax: +1 919 843 0164.

Acupuncture for spinal cord injury 317Contents
Introduction.............................................................................................................. 317Methods.................................................................................................................. 317
Data sources ........................................................................................................ 317Study selection...................................................................................................... 317Data extraction, quality, and validity assessment.................................................................... 317Data synthesis....................................................................................................... 318
Results ................................................................................................................... 318Study description.................................................................................................... 318Study quality ........................................................................................................ 318Descriptions of acupuncture......................................................................................... 318Outcomes ........................................................................................................... 318Adverse events ...................................................................................................... 324
Discussion................................................................................................................ 324Financial disclosure and conflict of interest .............................................................................. 326
.........
iFsio
S
AotciTaoas
D
AaiJifw((
eaio‘
Acknowledgements........................................References .................................................
Introduction
Spinal cord injury (SCI) is a major cause of disability, andits treatment of neurologic injury1 and various secondaryconditions including bladder and bowel complications, psy-chological changes and pain2 putting both economic andsocial burden on patients and their families.3 While careand treatment options such as spinal surgery,4 pharmacologi-cal interventions,5 and rehabilitation1 continue to improve,additional modalities are sought after. Acupuncture is oneof those modalities, and in fact, a recent review6 includingthree acupuncture studies on SCI patients, two with shoul-der pain7,8 and one dealing with motor recovery,9 suggestedthat acupuncture may have some beneficial effects on motorimprovement in SCI survivors. The small number of includedstudies was the major limitation of this review.
Despite the long use of acupuncture for varied clinicalconditions in China, most acupuncture research in China hasnot been easily detectable or introduced in western societydue to its publication in Chinese.10,11 Studies on acupunc-ture for SCI are not exceptional from this difficulty in beingdisseminated.
Therefore, the objective of this review is to system-atically review Chinese literature on the effectiveness ofacupuncture and its detailed interventions for patients withSCI. In addition, we intend to summarize the types ofacupuncture applied and commonly selected acupuncturepoints or locations of the body, so as to provide informa-tion on the current status in the treatment of SCI patientsin Chinese Medicine (CM).
Methods
Data sources
Databases accessed via China National Knowledge Infras-
tructure (CNKI: www.cnki.co.kr) searched from theirrespective inceptions to May 2008 include China AcademicJournal (CAJ), China Doctor/Master’s Dissertation database,and China Proceedings Conference database. The searchkeywords used were: ‘‘acupuncture’’ and (‘‘spinal cordcow0a
.......................................................... 326
.......................................................... 326
njury’’ OR ‘‘spinal injury’’) in both English and Chinese.urther, the references in all located articles were hand-earched to identify potentially relevant studies. Afternitial screening, hardcopies of all the relevant articles werebtained and read in full.
tudy selection
ll prospective randomized controlled clinical studies (RCTs)f needle acupuncture with or without electrical stimula-ion as a treatment of SCI (with or without operation) wereonsidered. Trials comparing needle acupuncture with var-ous forms of rehabilitation or drugs were also included.rials testing other forms of acupuncture, such as injectioncupuncture or laser acupuncture, and trials comparing twor more types of acupuncture were excluded. Dissertationsnd abstracts were also included as long as they containedufficient detail.
ata extraction, quality, and validity assessment
ll articles were read by two independent reviewers (B.C.S.nd J.C.K.), who extracted data from the articles accord-ng to predefined criteria. The PEDro scale12 and modifiedadad scale13 were used for assessing methodological qual-ty because it is the most comprehensive measure availableor assessing rehabilitation therapy studies.14 Disagreementsere resolved by discussion between the two reviewers
B.C.S. and J.C.K.), with the opinion of a third reviewerJ.P.) sought if necessary.
The quality of acupuncture was assessed by two review-rs (B.C.S. and J.C.K.) as described previously,15 assessmentnswered the questions, ‘how would you treat the patientsncluded in the study?’, on five ranks including ‘exactlyr almost exactly the same way’, ‘similarly’, ‘differently’,completely differently’, or ‘could not assess’ due insuffi-
ient information (on acupuncture or patient). The degreef confidence that acupuncture was applied appropriatelyas assessed on the 100 mm visual analogue scale (with= extremely inappropriate, and 100 = extremely appropri-te).
3 B.-C. Shin et al.
D
KttWffp(C
R
S
Sw((T1itotispowei
S
WadmM6tcmdaan
D
OaErriv
tatsdf(q‘sWv
O
Twruo
18
ata synthesis
ey data from the included studies were summarized andabulated, and study qualities and specifics of acupunc-ure were taken into consideration in drawing a conclusion.ith the intention to be informative, upon sufficing for per-
orming a meta-analysis, we calculated total efficacy rateor bladder dysfunction (BD) using random effect model ofooled data. Risk ratios with their 95% confidence intervalsCIs) were calculated using RevMan 5.0 software (The Nordicochrane Centre, Copenhagen, Denmark).
esults
tudy description
earches identified 236 potentially relevant articles, 211ere excluded because they were: not related to SCI
n = 31), duplicated publications (n = 61), not clinical trialsn = 19), animal studies (n = 56), and case reports (n = 44).wo independent reviewers read in full 25 articles, of which8 were excluded because 8 were not RCTs, three were RCTsnvolving stroke patients,16—18 three tested mixed interven-ions of treatments,19—21 one used injection acupuncture,22
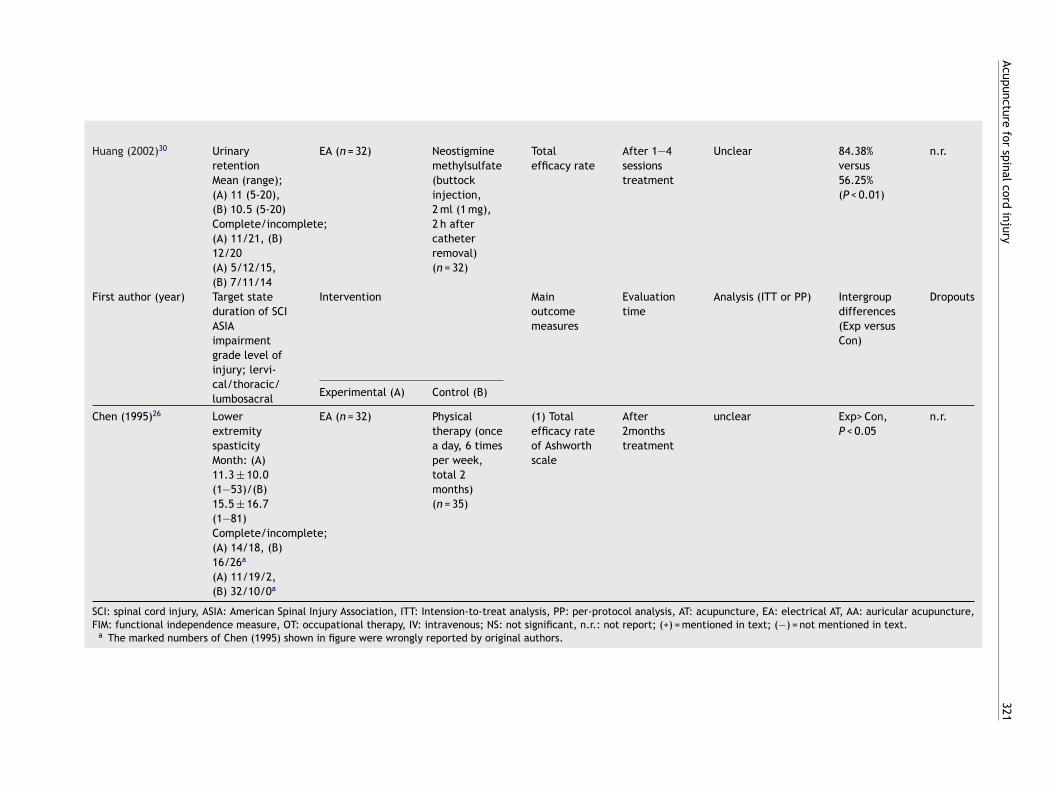
ne provided an insufficient report,20 and two comparedwo different types of acupuncture.23,24 Of the seven stud-es meeting our inclusion criteria (Fig. 1), the key data areummarized in Table 1.25—31 All included trials were two-arallel arm studies. Four trials studied functional recoveryf SCI; one acute SCI,25 two traumatic SCI,27,29 and the otheras unspecified SCI.31 One trial26 studied the antispasmodicffect of acupuncture on SCI patients and two trials28,30 stud-ed BD secondary to SCI.
tudy quality
hile all the included trials reported favourable effects ofcupuncture on function recovery or urinary dysfunctionue to SCI, quality scores derived from the two differentethodological quality scales present a different picture.ean scores (SD) for PEDro scale and the Jadad scale were(1.4) and 1.1 (0.9), respectively (Table 2). Only one of
he included trials31 reported the implementation of allo-ation concealment without detailed description of theethod, and subjects- and assessor blind. All seven trials areescribed as randomized, yet the randomization methodsre not mentioned. One of the trials29 reports inappropri-te randomization, in which researchers used admission bedumber (odd or even) for randomization.
escriptions of acupuncture
ne study comparatively tested electroacupuncture (EA)gainst physical therapy for spasticity,26 and another tested
A against drug injection for urinary retention.30 In theemaining five studies effectiveness of EA was tested versusehabilitation for functional recovery,25,27,31 versus rehabil-tation and drug for the same functional recovery,29 andersus BD.28etteo
Figure 1 Flowchart of trials selection process.
Total body acupuncture points included were 39. Ofhese, the majority are located in the limbs, with 13 (33.3%)nd 12 (30.8%) in the lower and upper extremity, respec-ively. The intended conceptual purpose ranges motor andensory recovery (n = 23, 59%), with 10 for bladder and bowelysfunction (25.6%), 9 for motor recovery (23.1%), threeor bladder or bowel dysfunction and one for anti-spasticityTables 3 and 4). In terms of the fidelity of acupunctureuality assessed by the two authors, four trials revealedexactly or almost exactly the same way’,28—31 one trialhowed ‘similarly’,27 and two trials proved ‘differently’.25,26
hile the degree of confidence of described acupuncturearies from 60% to 90% (mean: 82.1%).
utcomes
he Functional Independence Measure (FIM) score wasidely used as the main outcome measure for functional
ecovery, while two trials related to bladder dysfunctionsed total efficacy rate for main outcomes.28,30 The extentf heterogeneity among the studies testing for motor recov-
ry prohibited them from being pooled together. However,rials assessing the effect of EA for BD,28,30 was qualifiedo perform a pooled quantitative analysis, hence their totalfficacy rate was compared against conventional treatmentnly (n = 128, RR 1.51 [1.21, 1.90], P = 0.0004, heterogene-
Acupuncturefor
spinalcordinjury
319
Table 1 Summary of randomized clinical trials of acupuncture for spinal cord injury in China.
First author (year) Target stateduration of SCIASIAimpairmentgrade level ofinjury; lervi-cal/thoracic/lumbosacral
Intervention Mainoutcomemeasures
Evaluationtime
Analysis(ITT or PP)
Intergroupdifferences(Exp versusCon)
Dropouts
Experimental (A) Control (B)
Chen(2005)25 Acute SCIn.r.A and Bn.r.
EA + AA +rehabilitation(n = 28)
Rehabilitationonly (n = 28)
(1) ASIAneurologicandfunctionalscore(2) FIMscore
(1)Discharge/1year afterdischarge(2)Discharge/1year afterdischarge
Unclear AllExp > Con,P < 0.05
n.r.
Gu (2005)a29 Traumatic SCI(A) 30.3±17.6,(B) 28.8±11.7A/B/C/D; (A):11/15/4/2, (B):9/16/3/2(A) 4/24/4, (B)2/26/2
EA + (B) (n = 32) Kinesitherapy+OT +neurotrophicdrugs(Methycobal,50�g × 3/days)(n = 30)
(1) FIMscore(2) Rehabili-tationeffective-ness (=[FIMdischarge— FIM admis-sion]/hospitalizationday)
After 6monthstreatment
Unclear (1)97.78 ± 19.55versus87.53 ± 16.67(P < 0.05)(2)0.63 ± 0.21versus0.51 ± 0.25(P < 0.05)
n.r.
Cui (2004)27 Traumatic SCI(A) 12.9 ± 5.1,(B) 13.4 ± 6.2A:15, B:25,C:19, D:13(A)20/T1-L4:17,(B) 18/T1-L4:17
EA + (B) (n = 37) Nursing careplus exercisetherapy(n = 35)
(1) FIMscore (3, 6session)(2) Sensoryrecovery (3,6 session)
(1) After 3,6 monthstreatment(2) After 3,6monthstreatment
Unclear (1)Exp > Con,P < 0.05(2)Exp > Con,P < 0.05
n.r.

320B.-C.
Shinet
al.
Table 1(Continued)
First author (year) Target stateduration of SCIASIAimpairmentgrade level ofinjury; lervi-cal/thoracic/lumbosacral
Intervention Mainoutcomemeasures
Evaluationtime
Analysis(ITT or PP)
Intergroupdifferences(Exp versusCon)
Dropouts
Experimental (A) Control (B)
First author (year) Target stateduration of SCIASIAimpairmentgrade level ofinjury; lervi-cal/thoracic/lumbosacral
Intervention Mainoutcomemeasures
Evaluationtime
Analysis(ITT or PP)
Intergroupdifferences(Exp versusCon)
Dropouts
Experimental (A) Control (B)
Ma (2005)31 SCI (Walkingfunction)n.r.C 0/18/12
EA + (B) (n = 15) Weight liftwalkingexercise(15—30 min, 5times perweek, for 6months)(n = 15)
(1)Fugl-Meyerscore(2)Lindmarkscore
After 6monthstreatment
Unclear (1)23.8 ± 4.1versus17.2 ± 5.0(P < 0.01)(2)140.0 ± 3.8versus112.0 ± 2.6(P < 0.01)
n.r.
Gu (2005)b28 Bladderdysfunctionn.r.Complete/incomplete;37/2736/4/24
EA + (B) (n = 32) Intermittentcatheteriza-tion(n = 32)
Totalefficacy rate
After 2—8weekstreatment
Unclear 90.6% versus59.4%(P < 0.05)
n.r.
Acupuncturefor
spinalcordinjury
321
Huang (2002)30 UrinaryretentionMean (range);(A) 11 (5-20),(B) 10.5 (5-20)Complete/incomplete;(A) 11/21, (B)12/20(A) 5/12/15,(B) 7/11/14
EA (n = 32) Neostigminemethylsulfate(buttockinjection,2 ml (1 mg),2 h aftercatheterremoval)(n = 32)
Totalefficacy rate
After 1—4sessionstreatment
Unclear 84.38%versus56.25%(P < 0.01)
n.r.
First author (year) Target stateduration of SCIASIAimpairmentgrade level ofinjury; lervi-cal/thoracic/lumbosacral
Intervention Mainoutcomemeasures
Evaluationtime
Analysis (ITT or PP) Intergroupdifferences(Exp versusCon)
Dropouts
Experimental (A) Control (B)
Chen (1995)26 LowerextremityspasticityMonth: (A)11.3 ± 10.0(1—53)/(B)15.5 ± 16.7(1—81)Complete/incomplete;(A) 14/18, (B)16/26a
(A) 11/19/2,(B) 32/10/0a
EA (n = 32) Physicaltherapy (oncea day, 6 timesper week,total 2months)(n = 35)
(1) Totalefficacy rateof Ashworthscale
After2monthstreatment
unclear Exp> Con,P < 0.05
n.r.
SCI: spinal cord injury, ASIA: American Spinal Injury Association, ITT: Intension-to-treat analysis, PP: per-protocol analysis, AT: acupuncture, EA: electrical AT, AA: auricular acupuncture,FIM: functional independence measure, OT: occupational therapy, IV: intravenous; NS: not significant, n.r.: not report; (+) = mentioned in text; (−) = not mentioned in text.
a The marked numbers of Chen (1995) shown in figure were wrongly reported by original authors.

322B.-C.
Shinet
al.
Table 2 Quality assessment of internal validity of included randomized controlled trials with PEDro Scale and Jadad scale.
First author (year)ref Chen (2005)25 Gu (2005)a29 Cui (2004)27 Ma (2005)31 Gu (2005)b28 Huang (2002)30 Chen (1995)26
Allocation concealment n.r. n.r. n.r. Yes n.r. n.r. n.r.Acupuncture validity [quality ofacupuncture,a degree of confidence(%)b]
56/56 [2, 60] 62/62 [4,90] 72/72 [3, 85] 30/30 [4, 90] 64/64 [4,90] 64/64 [4, 85] 67/67 [2,75]
PEDro Scale itemsEligibility criteria specified 1 1 1 1 1 1 1Randomization 1 1 1 1 1 1 1Allocation concealment 0 0 0 1 0 0 0Groups similar at baseline 0 1 1 1 0 1 0Blinded subjects 0 0 0 1 0 0 0Blinded therapists 0 0 0 0 0 0 0Blinded assessors 0 0 0 1 0 0 085% of subjects on main outcomemeasure
1 1 1 1 1 1 1
Intention-to-treat analysis 1 1 1 1 1 1 1Between-group comparison 1 1 1 1 1 1 1Point and variability measures 1 1 1 1 1 1 1Total 5 6 6 9 5 6 5
Jadad Scale itemsStudy described as randomized 1 1 1 1 1 1 1Appropriate method 0 0 0 0 0 0 0Inappropriate method 0 -1 0 0 0 0 0Subject blinded to intervention 0 0 0 1 0 1 0Evaluator blinded to intervention 0 0 0 1 0 0 0Description of withdrawals or dropouts 0 0 0 0 0 0 0Total 1 0 1 3 1 1 1
Note. Quality Scale: PEDro Scale (Range 0 to 10 points; item 1 is related to external validity and not included in score), Jadad score (randomization + randomization method + drop outor withdraw + assessor blind + patients’ blind, maximum 5). PEDro Scale: 1, item positive; 0, item negative or unknown; Jadad score: 1, described in text, 0, not described in text, −1,deducted because of inappropriateness.
a Quality of acupuncture: 0, could not assess; 1, completely differently; 2, differently; 3, similarly; 4, exactly or almost exactly the same way.b Degree of confidence: degree of confidence that acupuncture was applied appropriate manner 100 mm visual scale (with 0% = complete absence of evidence that the acupuncture was
appropriate, and 100% = total certainty that the acupuncture was appropriate).

Acupuncture for spinal cord injury 323
Table 3 Summary of acupuncture intervention for spinal cord injury in China.
First author(year)
Modified Jadadscore (total)
Acupuncture Total treatment Acupuncture pointsDeqi sensation
Adverseevents
Type ofacupuncture
Regimen
Chen(2005)25
1 EA + AA EA (30 min,1—5 Hz, daily 6days/week, 3months/session,session interval:1—2 weeks) AA(daily, each earalternately, 10times/session,total 2—3 session)
3 months EA: Both SI3, BL62AA: brain, subcortex,sympathetic,Shenmen(Authors reported:impossible in SCIpatients because ofsensory impairment)
No adverseevents (+)
Gu(2005)a29 0 EA 1 Hz, 3—5 V,30 min, daily for 1month, 1 weekrest, total 6months
6months Huatuojiaji, LI15,LI11, TE5, LI4, GB30,GB31, GB34, ST36,GB39, BL60, ST41,LR3(EA applied to majorextrimity points)Evacuation disorders;plus eight-liao point,BL25, SP6, GB34n.r.
n.r.
Cui(2004)27 1 EA 30 min, daily,1month/session,total 3—6 sessions
3—6 months Arm: HT1, LU5, PC3,HT3Leg: SP12, BL37 orGB30, BL40,Other peroneal nervestimulation point (noreports about whereEA was applied)Considered
n.r.
Ma (2005)31 3 EA(scalp) + bodyAT
Scalp (5 min,daily), Body(25 min, daily), for6 months
6 months EA; scalpacupuncture: motorarea (MS6),equilibrium area(MS14)Arm: LI10, LI11, TE8,SI5Leg: LR12, GB34,GB39, BL54, BL60,LR3Considered (authorsdid not describe, butmight be considered)
n.r.
Gu(2005)b28
1 EA 30 min, continuouswave, daily, 2weeks/session/total1—4 sessions
2—8 weeks Eight-liao point (EA),if excess syndrome:plus BL23, CV6, BL20,BL22, if deficiencysyndrome: plus SP6,BL28, SP9, CV3Considered
n.r.

324 B.-C. Shin et al.
Table 3(Continued)
First author(year)
Modified Jadadscore (total)
Acupuncture Total treatment Acupuncture pointsDeqi sensation
Adverseevents
Type ofacupuncture
Regimen
Huang(2002)30
1 EA 30 min, continuouswave, 5days/session, 3days rest, total1—4 sessions
1—4 sessions EA: Bilateral; BL54,ST28, BL32, BL34,T12-L2 Huatuojiaji,SP9, SP6Considered (authorsdid not describe, butmight be considered)
n.r.
Chen(1995)26
1 EA 30 min, 1—2 Hz,daily, 6times/week /for 2months
2 months EA: Injured spinallevel; upper 1point &lower 1 point ofGoverner vessel ofinjured level (interspinous process)
n.r.
.; no
irts
A
Owo
D
Tshoi
fqMoPnP
fsnio
aooFutsara
stlba
AT: acupuncture; EA: electrical AT; AA: auricular acupuncture, n.r
ty Tau2 < 0.01, Chi2 = 0.01, P = 0.94, I2 = 0%) (Fig. 2). All trialseported positive effects of acupuncture treatment on func-ional recovery or urinary dysfunction due to SCI with limitedtrength of evidence.
dverse events
nly one trial25 mentioned adverse events stating that thereas no adverse reaction reported during the trial, whilethers studies did not report on this at all (Table 3).
iscussion
he key findings of this review are as follows: while it isuggestive that acupuncture may be an effective adjunct toelp motor and sensory recovery and BD after surviving SCI,utstanding quality issues of the studies so far carried outn China prevent us from drawing any firm conclusion.
Five RCTs25,27—29,31 testing the additional effect of EA forunctional recovery and BD, indicate that use of a low fre-uency (1—5 Hz) may result in significantly better outcomes.
eanwhile, none of these studies use a rigorous controlr blinding, except one study reporting assessor blinding.31erhaps the positive findings include a broad range ofon-specific effects including suggestion, and expectation.erhaps these rather pragmatic trials could have only been
b
wet
Figure 2 Meta-analysis of acupuncture for b
n.r.
t report; (+) = mentioned in text; (−) = not mentioned in text.
easible in China since acupuncture is a major part of healthervices. In fact, these findings may provide rationale for aew study outside of China; therefore the suggestive find-ngs from these Chinese studies lend support for a new seriesf rigorous studies.
Regarding the types of acupuncture used, five trialsdopted EA on paralysed extremity or back injured site, 26—30
ne trial used EA plus AA (auricular acupuncture),25 and thether used scalp EA on the head plus body acupuncture.31
ive trials testing the effect of EA for functional recoverysed active control (exercise, rehabilitation and physicalherapy)25—27,29,31 and two RCTs testing BD adopted controluch as intermittent catheterization and drugs.28,30 Shamcupuncture is regarded as a valid control for acupunctureesearch,32—34 however, all the trials did not chose any shams control, which raises potential to bias.
Interestingly the acupuncture modality of all the includedtudies is EA. Why manual acupuncture was not studiedherefore seems a plausible question. It may be that theack of sensational response to manual acupuncture causedy sensory and motor loss following SCI prevented its use,nd that the use of EA in this case is found empirically more
eneficial.Of the seven RCTs, one study was assessor blind,27
hile six further studies did not make any attempt atither subjects or assessor blinding. One trial reportedhe concealment of treatment allocation,29 though the
ladder dysfunction of spinal cord injury.

Acupuncture for spinal cord injury 325
Table 4 Summary of acupoints selected in the studies included in the review.
Acupoints Location Intention touse (N)
Frequency ofappearance (N)
Percentagea
(%)
Classicacupuncture
Sanyinjiao (SP6) LL BBD (3) 3 42.9Eight-liao point (BL31-34) LA BBD (3) 3 42.9Huatuojiaji (EX) CS, TS or LS MSR (1), BD (2) 3 42.9Zhibian (BL54) Hip BD (1), MR (1) 2 28.6Kunlun (BL60) LL MSR (1), MR (1) 2 28.6Huantiao (GB30) Hip MSR (2), 2 28.6Yanglingquan (GB34) LL MSR (1), MR (1) 2 28.6Xuanzhong (GB39) LL MSR (1), MR (1) 2 28.6Quchi (LI11) UL MSR (1), MR (1) 2 28.6Taichong (LR3) LL MSR (1), MR (1) 2 28.6Yinlingquan (SP9) LL BD (2) 2 28.6Pishu (BL20) TS BD (1) 1 14.3Sanjiaoshu (BL22) LS BD (1) 1 14.3Shenshu (BL23) LS BD (1) 1 14.3Dachangshu (BL25) LA BBD (1) 1 14.3Pangguangshu (BL28) LA BD (1) 1 14.3Yinmen (BL37) LL MSR (1) 1 14.3Weizhong (BL40) LL MSR (1) 1 14.3Shenmai (BL62) LL MSR (1) 1 14.3Zhongji (CV3) AA BD (1) 1 14.3Qihai (CV6) AA BD (1) 1 14.3Fengshi (GB31) LL MSR (1) 1 14.3Governer vessel meridian CS, TS or LS
(injured level)Anti-spasticity 1 14.3
Jiquan (HT1) UL MSR (1) 1 14.3Shaohai (HT3) UL MSR (1) 1 14.3Shousanli (LI10) UL MR (1) 1 14.3Jianyu (LI15) UL MSR (1) 1 14.3Hegu (LI4) UL MSR (1) 1 14.3Jimai (LR12) AA MR (1) 1 14.3Chize (LU5) UL MSR (1) 1 14.3Quze (PC3) UL MSR (1) 1 14.3Houxi (SI3) UL MSR (1) 1 14.3Yanggu (SI5) UL MR (1) 1 14.3Chongmen (SP12) LL MSR (1) 1 14.3Shuidao (ST28) AA BD (1) 1 14.3Zusanli (ST36) LL MSR (1) 1 14.3Jiexi (ST41) LL MSR (1) 1 14.3Waiguan (TE5) UL MSR (1) 1 14.3Sanyangluo (TE8) UL MSR (1) 1 14.3
Auricularacupuncture
Brain Ear MSR (1) 1 14.3Subcortex MSR (1) 1 14.3Sympathetic MSR (1) 1 14.3Shenmen MSR (1) 1 14.3
Scalpacupuncture
Motor area (MS6) Scalp MR (1) 1 14.3Eequilibrium area (MS14) MR (1) 1 14.3
ical sdysfu
c
UL: upper limb, LL: lower limb, LA: lumbosacral area, CS: cervabdominal area, BBD: bladder or bowel dysfunction, BD: bladder
a Percentage = N/7 × 100.
method of allocation concealment was not described, while
others were unclear. Trials with inadequate blinding andinadequate allocation concealment are likely to show exag-gerated treatment effects.35,36 Most of the included trialsalso suffered from a lack of adequate allocation con-cioa
pine area, TS: thoracic spine area, LS: lumbar spine area, AA:nction, MSR: motor and sensory recovery, MR: motor recovery.
ealment and sufficient sample size to draw meaningful
onclusions, with no power analysis included. All of thencluded trials were rated as low methodological qualityn the score of PEDro and Jadad. These low quality tri-ls are more likely to over-estimate efficacy, and in our
3
rce
attecsii
fntwa
intcwomtapsloTaafp
iebAteaot
DpibroCaptn
pa
etlao
F
N
A
TRFm
R
26
eview, 100% of the included RCTs generated positive results,onfirming that low quality trials are more likely to over-stimate the effect size of a medical intervention.
Acupuncture stimulation elicits deqi, sensations that aresserted to be important for clinical effect in the concep-ual framework of traditional Chinese Medicine.37,38 Tworials27,28 reported deqi sensation, and two30,31 did notxplicitly describe deqi although they implied this within theontext of the report. In two other trials26,29 authors did notpare any significant importance to deqi, and in the remain-ng trial,25 the authors reported that elicitation of deqi wasmpossible in SCI patients because of sensory impairment.
While ethical issue grows more important in clinical trialsor assuring the safety and human right of study participants,o included trial reported any approval of their investiga-ional review board (IRB) or an informed consent process,ith only one trial stating they attempted to explain thegreement of participation verbally.31
It would be meaningful to compare the studies includedn this review and those published in the West albeit less inumber. Four RCTs were published in English up to date7—9,39;wo assessed effects of acupuncture on pain reduction ofhronic shoulder pain in wheelchair users following SCI,here both did not show favourable effects of acupuncturen pain level compared with sham acupuncture or Trageranual therapy.7,8 Wong et al. evaluated effects of acupunc-
ure as an adjunct to standard therapy, and concludedcupuncture as beneficial adjunct.9 The above three studiesrovide more or less accordant insights from those Chinesetudies included in this review.27,29 Cheng et al.39 despiteimited quality, showed favourable effects of acupuncturen neurogenic bladder symptom control in 80 SCI patients.his study is in support of the included Chinese studies,28,30
nd the modality of acupuncture was very similar to Chinesepproach in that EA was used on Conception vessel (mid-rontal line of the body) and Bladder meridian (bilateraleri-spinal vertebral lines of the body) for treating BD.28,30,39
A bright side of using acupuncture for SCI survivors is thatt causes very few adverse effects, i.e. minimal risk. In gen-ral, acupuncture, when used according to safety standardsy qualified health professionals, is known to be safe.40,41
ssuming that acupuncture was beneficial for treating SCI,he possible mechanisms of action are of interest. The recov-ry effects of acupuncture treatment for SCI postulate thatcupuncture can facilitate nerve regeneration, stimulation,r regulation of the nerve conduction in damaged nerveshrough EA.42,43
Our review has a number of important limitations.espite our efforts, our included study pool may be open toublication bias. Moreover, selective publishing and report-ng are potentially major causes for bias, which have toe considered. It is conceivable that several negative RCTsemained unpublished and thus distort the overall.44,45 Mostf the included RCTs that report positive results come fromhina, a country which has been shown to produce no neg-tive acupuncture studies.46 Further limitations include theaucity and the often suboptimal methodological quality of
he primary data. In total, these facts limit the conclusive-ess of this systematic review considerably.In conclusion, the results of our systematic reviewrovide suggestive evidence for the effectiveness ofcupuncture as adjunctive therapy in treating SCI. How-
B.-C. Shin et al.
ver, the total number of RCTs included in the analysis, theotal sample size and the methodological quality were tooow to draw firm conclusions about the effectiveness of thispproach. Further rigorous RCTs are warranted but need tovercome the many limitations of the current evidence.
inancial disclosure and conflict of interest
one.
cknowledgements
his work was supported by Pusan National Universityesearch Grant, 2008. All the authors thank Stephenlaherty for his editorial assistance in preparing theanuscript.
eferences
1. Sipski ML, Richards JS. Spinal cord injury rehabilitation: stateof the science. Am J Phys Med Rehabil 2006;85(4):310—42.
2. Sawatzky B, Bishop CM, Miller WC. Classification and measure-ment of pain in the spinal cord-injured population. Spinal Cord2008;46(1):2—10.
3. Krause JS, DeVivo MJ, Jackson AB. Health status, communityintegration, and economic risk factors for mortality after spinalcord injury. Arch Phys Med Rehabil 2004;85(11):1764—73.
4. Bridwell KH, Anderson PA, Boden SD, Vaccaro AR, WangJC. What’s new in spine surgery. J Bone Joint Surg Am2008;90(7):1609—19.
5. Taricco M, Pagliacci MC, Telaro E, Adone R. Pharmacologi-cal interventions for spasticity following spinal cord injury:results of a Cochrane systematic review. Eura Medicophys2006;42(1):5—15.
6. Harvey LA, Lin CW, Glinsky JV, De Wolf A. The effectiveness ofphysical interventions for people with spinal cord injuries: asystematic review. Spinal Cord 2009;47(3):184—95.
7. Dyson-Hudson TA, Kadar P, LaFountaine M, Emmons R, Kirsh-blum SC, Tulsky D, et al. Acupuncture for chronic shoulder painin persons with spinal cord injury: a small-scale clinical trial.Arch Phys Med Rehabil 2007;88(10):1276—83.
8. Dyson-Hudson TA, Shiflett SC, Kirshblum SC, Bowen JE, DruinEL. Acupuncture and Trager psychophysical integration in thetreatment of wheelchair user’s shoulder pain in individuals withspinal cord injury. Arch Phys Med Rehabil 2001;82(8):1038—46.
9. Wong AM, Leong CP, Su TY, Yu SW, Tsai WC, Chen CP. Clinicaltrial of acupuncture for patients with spinal cord injuries. AmJ Phys Med Rehabil 2003;82(1):21—7.
10. Fan WY, Tong YY, Pan YL, Shang WL, Shen JY, Li W, et al. Tradi-tional Chinese Medical Journals currently published in mainlandChina. J Altern Complement Med 2008;14(5):595—609.
11. Wang J. Major Chinese full-text electronic informa-tion resources for researchers and scholars. Serials Rev2006;32(3):164—71.
12. Physiotherapy Evidence Database. PEDro Scale.http://wwwpedrofhsusydeduau/scale itemhtml. Accessed at26, September; 2008.
13. White AR, Ernst E. A systematic review of randomized con-trolled trials of acupuncture for neck pain. Rheumatology
1999;38(2):143—7.14. Bhogal SK, Teasell RW, Foley NC, Speechley MR. The PEDro scaleprovides a more comprehensive measure of methodologicalquality than the Jadad scale in stroke rehabilitation literature.J Clin Epidemiol 2005;58(7):668—73.
trolled clinical trials of complementary/alternative therapies.J Clin Epidemiol 2000;53(5):485—9.
46. Vickers A, Goyal N, Harland R, Rees R. Do certain countries
Acupuncture for spinal cord injury
15. Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, WhiteAR. Acupuncture for migraine prophylaxis. Cochrane DatabaseSyst Rev 2009;(1). CD001218.
16. Teng XY. Clinical effects of acupuncture treatment on the blad-der dysfunction. Clin J Acupunct Moxibustion 2003;19(4):17.
17. Yue ZH, Liu WL, Jiang JM. Acupuncture treatment and func-tional assessment on the spasticity of extremity. J Chin RehabilMed 2002;17(3):177—8.
18. Zhang W, Liu WL, Zhao YL. Clinical study of 52 cases of spas-modic paralysis. Zhong Guo Yi Kan 1999;34(3):52—3.
19. Shan LM, Wu XJ, Yang CM. Clinical effects of acupuncture com-bined with Tuina manipulation for the treatment of paralysisinduced by traumatic spinal cord injury. Zhong Yi Zheng Gu1999;11(9):14—5.
20. Yan CF. The effect of antispasmodic on the physical functions ofcases with spinal paraplegia. Mod Rehabil 1999;3(10):1162—3.
21. Zhang GH, Sun SF. Clinical effects of Yi-qi-huo-Xue-tang plusacupuncture treatment on the 20 patients with spinal cordinjury. Hebei Chin Med 2004;26(1):21—2.
22. Liu XF, Liao ZA, Deng WH, Guan XL, Luo J. Effects of drug injec-tion at eight-liao point combined with bladder function trainingon bladder sysfunction due to spinal cord injury. Chin J ClinRehabil 2005;9(25):142—3.
23. Zhang Y. Relationship between acupuncture and recoveryof spinal cord injury. Chin J Trad Med Traum Orthop2002;10(6):58—9.
24. Zhou LY, Li J, Li CM, Yu ZG, Zhang WL, Zheng M, etal. Observation on therapeutic effect of electroacupunctureat points Baliao and Huiyang (BL35) on retention of urineinduced by spinal cord injury. Chin Acupunct Moxibustion2006;26(4):237—9.
25. Chen LX, Duan JF, Zhan XR, Xie Q, Long QH. Electrical andauricular acupucture for patients with acute spinal cord injury.Clin J Rehabil Theory Pract 2005;11(11):934—5.
26. Chen ZG, Zhang JJ, Wong ZM, Li HL, Zhang AL. The clinicalstudy of Governer vessel electroacupuncture treatment on thelower extremity spasticity in patients with spinal cord injury.Clin J Acupunct Moxibustion 1995;11(6):6—7.
27. Cui XM, Pan XM, Zhang XM, Deng HZ, Yao SY. The rehabili-tation function of electroacupuncture treatment in patientswith traumatic spinal cord injury. J Guangdong Med Coll2004;22(2):170—1.
28. Gu XD, Fu JM, Yao YH. Clinical observation of elec-troacupuncture on eight-liao points in 64 bladder dysfunctionpatients with spinal cord injury. J Clin Acupunct Moxibustion2005;21(4):47—8.
29. Gu XD, Yao YH, Gu M, Fu JM, Ren Y, Yin HK. Clinical study onfunctional independence measure for patients with spinal cord
injury of trauma treated by electroacupuncture. Acupunct Res2005;30(3):175—8.30. Huang ZG, You B. Acupuncture treatment on 32 cases of uri-nary retention after spinal cord injury. J Shanhai AcupunctMoxibustion 2002;21(2):31.
327
31. Ma CH. The effects of combination treatment of elec-troacupuncture and weight lift walking exercise on the walkingfunction of spinal cord injury patients. Chin J Clin Rehabil2005;9(17):186.
32. Fink M, Gutenbrunner C, Rollnik J, Karst M. Credibility of anewly designed placebo needle for clinical trials in acupunc-ture research. Forsch Komplementarmed Klass Naturheilkd2001;8(6):368—72.
33. Park J, White A, Stevinson C, Ernst E, James M. Validating a newnon-penetrating sham acupuncture device: two randomisedcontrolled trials. Acupunct Med 2002;20(4):168—74.
34. Streitberger K, Kleinhenz J. Introducing a placebo needle intoacupuncture research. Lancet 1998;352(9125):364—5.
35. Day SJ, Altman DG. Statistics notes: blinding in clinical trialsand other studies. BMJ 2000;321(7259):504.
36. Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evi-dence of bias. Dimensions of methodological quality associatedwith estimates of treatment effects in controlled trials. JAMA1995;273(5):408—12.
37. Hui KK, Nixon EE, Vangel MG, Liu J, Marina O, Napadow V, etal. Characterization of the ‘‘deqi’’ response in acupuncture.BMC Complement Altern Med 2007;7:33.
38. White P, Bishop F, Hardy H, Abdollahian S, White A, Park J,et al. Southampton needle sensation questionnaire: develop-ment and validation of a measure to gauge acupuncture needlesensation. J Altern Complement Med 2008;14(4):373—9.
39. Cheng PT, Wong MK, Chang PL. A therapeutic trial of acupunc-ture in neurogenic bladder of spinal cord injured patients—–apreliminary report. Spinal Cord 1998;36(7):476—80.
40. Vincent C. The safety of acupuncture. BMJ2001;323(7311):467—8.
41. White A. A cumulative review of the range and incidence of sig-nificant adverse events associated with acupuncture. AcupunctMed 2004;22(3):122—33.
42. Chen YY, Zhang W, Chen YL, Chen SJ, Dong H, Zeng YS. Electro-acupuncture improves survival and migration of transplantedneural stem cells in injured spinal cord in rats. Acupunct Elec-trother Res 2008;33(1-2):19—31.
43. Peng B, Meng XF, Li M, Luo Y, Li LL, Zhang J, et al. Effectsof electroacupuncture on the expression of epidermal growthfactor receptor and glial fibrillary acidic protein after spinalcord injury in rats. Zhen Ci Yan Jiu 2007;32(4):219—23.
44. Ernst E, Pittler MH. Alternative therapy bias. Nature1997;385(6616):480.
45. Pittler MH, Abbot NC, Harkness EF, Ernst E. Location bias in con-
produce only positive results? A systematic review of controlledtrials. Control Clin Trials 1998;19(2):159—66.