The longitudinal association between inflammation and incident depressive symptoms in men: The...
8
The longitudinal association between inflammation and incident depressive symptoms in men: The effects of hs-CRP are independent of abdominal obesity and metabolic disturbances Phillip J. Tully a,b, ⁎, Harald Baumeister b,c , Jürgen Bengel b , Alicia Jenkins d , Andrzej Januszewski d , Sean Martin a , Gary A. Wittert a a Freemasons Foundation Centre for Men's Health, Discipline of Medicine, School of Medicine, The University of Adelaide, Adelaide, Australia b Department of Rehabilitation Psychology and Psychotherapy, Institute of Psychology, University of Freiburg, Freiburg, Germany c Medical Psychology and Medical Sociology, Medical Faculty, University of Freiburg, Freiburg, Germany d University of Sydney, NHMRC Clinical Trials Centre, Sydney, NSW, Australia HIGHLIGHTS • We examine whether obesity alters the inflammation–depression association. • 5-year associations between hsCRP, IL-6, TNF-α and depression are reported. • hsCRP was associated with depression, and an increase in depressive symptoms. • Effects were upheld only in men without abdominal obesity and metabolic risk. • We show that metabolic factors alter the association between hsCRP and depression. abstract article info Article history: Received 8 August 2014 Received in revised form 17 November 2014 Accepted 18 November 2014 Available online 22 November 2014 Keywords: Depression Inflammation Abdominal adiposity Longitudinal C-reactive protein Interleukin-6 Tumor necrosis factor-alpha Obesity Body mass index Metabolic syndrome Background: This cohort study evaluates whether the association between low-grade inflammation and incident depressive symptoms is independent of abdominal obesity and metabolic disturbances. Methods: A cohort of 1167 non-depressed men aged 35 to 80 years were followed up over 5 years to assess incident depressive symptoms measured by the Centre for Epidemiology Scale—Depression or Beck Depression Inventory—I. Venous tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6) and high sensitivity C-reactive protein (hsCRP) were quantified at baseline and 5 years. Logistic regression determined whether hsCRP, IL-6 and TNF-α were associated with incident depressive symptoms independent of abdominal obesity and metabolic factors. Ancillary analysis uti- lizing depression z scores stratified participants by waist circumference ≥ 102 cm and ≥2 metabolic disturbances. Results: Incident depressive symptoms occurred in 95 men at 5 years (8.14% of total). Clinically relevant depressive symptoms were associated with baseline hsCRP (adjusted OR = 1.04; 95% CI 1.00–1.07, p = .03) and annualized ΔhsCRP (adjusted OR = 1.04; 95% CI 1.01–1.08, p = .02). Ancillary analysis showed that the association between annualized ΔhsCRP and depression z score was only significant in men with waist circumference b 102 cm (β = .19, p b .001) and ≤1 metabolic disturbance (β = .18, p b .001). None of the measured cytokines were significantly associated with depression. Conclusions: hsCRP and annualized ΔhsCRP were positively associated with depressive symptoms in a cohort of men. Further investigation into the role of abdominal obesity and metabolic disturbances in the inflammation– depression hypothesis is warranted. © 2014 Elsevier Inc. All rights reserved. 1. Introduction The prevalence of overweight body mass index criteria (BMI N 25) exceeds 37% prevalence in most developing and developed countries according to the Global Burden of Disease Study 2013 [1], indicating a burgeoning global obesity epidemic. High comorbidity between depres- sion and obesity in the extant literature is suggestive of shared behav- ioral and pathophysiological mechanisms [2,3]. With respect to the latter, chronic low grade systemic inflammation has been extensively documented in both obesity [4,5] and depression [6–11], and has thus been proposed as possible mechanisms [12,13]. The directionality of this complex association has been examined in at least two ways, Physiology & Behavior 139 (2015) 328–335 ⁎ Corresponding author at: Discipline of Medicine, School of Medicine, The University of Adelaide, South Australia 5005, Australia. E-mail address: [email protected] (P.J. Tully). http://dx.doi.org/10.1016/j.physbeh.2014.11.058 0031-9384/© 2014 Elsevier Inc. All rights reserved. Contents lists available at ScienceDirect Physiology & Behavior journal homepage: www.elsevier.com/locate/phb
Transcript of The longitudinal association between inflammation and incident depressive symptoms in men: The...

Physiology & Behavior 139 (2015) 328–335
Contents lists available at ScienceDirect
Physiology & Behavior
j ourna l homepage: www.e lsev ie r .com/ locate /phb
The longitudinal association between inflammation and incidentdepressive symptoms in men: The effects of hs-CRP are independentof abdominal obesity and metabolic disturbances
Phillip J. Tully a,b,⁎, Harald Baumeister b,c, Jürgen Bengel b, Alicia Jenkins d, Andrzej Januszewski d,Sean Martin a, Gary A. Wittert a
a Freemasons Foundation Centre for Men's Health, Discipline of Medicine, School of Medicine, The University of Adelaide, Adelaide, Australiab Department of Rehabilitation Psychology and Psychotherapy, Institute of Psychology, University of Freiburg, Freiburg, Germanyc Medical Psychology and Medical Sociology, Medical Faculty, University of Freiburg, Freiburg, Germanyd University of Sydney, NHMRC Clinical Trials Centre, Sydney, NSW, Australia
H I G H L I G H T S
• We examine whether obesity alters the inflammation–depression association.• 5-year associations between hsCRP, IL-6, TNF-α and depression are reported.• hsCRP was associated with depression, and an increase in depressive symptoms.• Effects were upheld only in men without abdominal obesity and metabolic risk.• We show that metabolic factors alter the association between hsCRP and depression.
⁎ Corresponding author at: Discipline ofMedicine, SchoAdelaide, South Australia 5005, Australia.
E-mail address: [email protected] (P.J. Tull
http://dx.doi.org/10.1016/j.physbeh.2014.11.0580031-9384/© 2014 Elsevier Inc. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 8 August 2014Received in revised form 17 November 2014Accepted 18 November 2014Available online 22 November 2014Keywords:DepressionInflammationAbdominal adiposityLongitudinalC-reactive proteinInterleukin-6Tumor necrosis factor-alphaObesityBody mass indexMetabolic syndrome
Background: This cohort study evaluates whether the association between low-grade inflammation and incidentdepressive symptoms is independent of abdominal obesity and metabolic disturbances.Methods:A cohort of 1167 non-depressedmen aged 35 to 80 yearswere followed up over 5 years to assess incidentdepressive symptomsmeasured by the Centre for Epidemiology Scale—Depression or BeckDepression Inventory—I.Venous tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6) and high sensitivity C-reactive protein (hsCRP) werequantified at baseline and 5 years. Logistic regression determined whether hsCRP, IL-6 and TNF-αwere associatedwith incident depressive symptoms independent of abdominal obesity andmetabolic factors. Ancillary analysis uti-lizing depression z scores stratified participants by waist circumference≥ 102 cm and ≥2 metabolic disturbances.Results: Incident depressive symptoms occurred in 95 men at 5 years (8.14% of total). Clinically relevantdepressive symptoms were associated with baseline hsCRP (adjusted OR = 1.04; 95% CI 1.00–1.07, p = .03)and annualized ΔhsCRP (adjusted OR = 1.04; 95% CI 1.01–1.08, p = .02). Ancillary analysis showed that theassociation between annualized ΔhsCRP and depression z score was only significant in men with waistcircumference b 102 cm (β = .19, p b .001) and ≤1 metabolic disturbance (β = .18, p b .001). None of themeasured cytokines were significantly associated with depression.Conclusions: hsCRP and annualized ΔhsCRP were positively associated with depressive symptoms in a cohort of
men. Further investigation into the role of abdominal obesity and metabolic disturbances in the inflammation–depression hypothesis is warranted.© 2014 Elsevier Inc. All rights reserved.
1. Introduction
The prevalence of overweight body mass index criteria (BMI N 25)exceeds 37% prevalence in most developing and developed countries
ol ofMedicine, TheUniversity of
y).
according to the Global Burden of Disease Study 2013 [1], indicating aburgeoning global obesity epidemic. High comorbidity between depres-sion and obesity in the extant literature is suggestive of shared behav-ioral and pathophysiological mechanisms [2,3]. With respect to thelatter, chronic low grade systemic inflammation has been extensivelydocumented in both obesity [4,5] and depression [6–11], and has thusbeen proposed as possible mechanisms [12,13]. The directionality ofthis complex association has been examined in at least two ways,

Time 1 Assessment n = 2569
Time 2 Not Eligible
Did not complete depression
questionnaire n = 52
Withdrawn from study n = 18
Time 1 Completed Baseline
n = 1237
Time 1 Excluded
Cardiovascular disease n = 269
Glucocorticoid n = 28
Depression in past 12 months n = 219
Symptomatic depression n = 190
Anti-psychotic medication n = 1
No inflammation markers n = 616
Time 2 Completed Study
n = 1167
Eligible n = 4524
Excluded
Non-contactable / no reply n = 499
Refused n = 425
Incomplete / withdrawn n = 606
Refused clinic visit n = 425
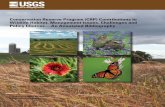
Fig. 1. Flow chart of patients through the study.
329P.J. Tully et al. / Physiology & Behavior 139 (2015) 328–335
depression leading to incident obesity and heightened inflammation,and alternatively, inflammation inherent to obesity leading to incidentdepression. This longitudinal report concerns only the latter.
To date inflammation–depression research has particularly fo-cused on two pro-inflammatory cytokines, interleukin-6 (IL-6),tumor necrosis factor-α (TNF-α), and also the acute phase reactantprotein C-reactive protein (CRP) [14,15]. Some longitudinal studiessuggest that CRP and IL-6 in particular precede a depressive stateand that this association is upheld after adjustment for baselineBMI [16–19]. However a 2013 meta-analysis [20] highlighted apaucity of longitudinal research in this area, considering that only 8CRP studies, 3 IL-6 studies, and no TNF-α studies were analyzed.
It is important to further investigate whether inflammationprecedes depression as recent evidence highlights that metabolicfactors alter and may confound these purported etiological linksmore than first thought [12,20,21]. Specifically, a meta-analysis[22] of cross-sectional studies showed that adjustment for BMI ledto a significant reduction in effect sizes reflecting the association be-tween CRP and IL-6 with depression. Despite the apparent reductionin association between inflammation and depressionwhen adjustingfor BMI, no longitudinal cohort studies have evaluatedwhether othermeasures of visceral fat [23], such as waist circumference [24], alsolead to a substantial attenuation of effect sizes. Such a longitudinalexamination of this type is important considering that abdominaladipose tissue is partly comprised of visceral fat, a known sourceof inflammatory adipokines, and together abdominal obesity andadipokines portend heightened risk to the constituent diseases ofthe metabolic syndrome [3,12,20,21,25].
In addition to the likely role of abdominal obesity as a confoundingsource of low-grade inflammation, it has been recently shown thatonly the specific combination of BMI ≥ 30 and poor metabolic healthis associated with incident depressive symptoms in a pooled-cohortmeta-analysis [26]. Taken together, findings to date suggest that, it isnot yet established whether depression is preceded by low-grade in-flammation (i.e. CRP, IL-6, TNF-α) independent of abdominal obesity,metabolic disturbance, and their combination, in longitudinal studies,as most research to date has adjusted for BMI only.
To our knowledge this study is first to report the longitudinal asso-ciation between changes in inflammation (i.e. CRP, IL-6, TNF-α) andincident depressive symptoms, controlling for the discrete effects ofabdominal obesity, metabolic disturbance and their combination. Wereport findings from the Men Androgen Inflammation LifestyleEnvironment and Stress (MAILES) Study [27]. Considering that malesexperience a higher proportion of cardiovascular disease, obesity,physical inactivity and smoking compared to females, the findingsmight serve to address male-specific health inequalities [27]. Here wehypothesize that a positive association between inflammation and inci-dent depressive symptoms at 5 years is attenuated when adjustment ismade for abdominal obesity and comorbid metabolic disturbance.
2. Materials and methods
2.1. Study design, recruitment strategy and population
This study employed data from MAILES Study, as describedelsewhere [27,28]. Briefly, a representative sample of males between35 and 80 years of age were recruited from a pre-specified catchmentarea of North andWest Adelaide, South Australia, Australia. Participantswere recruited at random based on having a residential telephonenumber listed in the electronic white pages. Residential householdswere then selected at random, and the male person within thehousehold aged between 35 and 80 years to last have his birthdaywas invited for interview and study participation.
Participants were excluded when they: (1) had limited mental orphysical capacity (e.g. due to illness) to partake in the study; (2) wereinstitutionalized at the time of the study; and (3) did not speak English.
For the current analysis participants were also excluded for any of thefollowing at the time of baseline assessment: (1) the presence of cardio-vascular disease (CVD) including angina; (2) a physician-diagnosis fordepression within the preceding 12 months; (3) had clinically relevantdepressive symptoms (based on either Center for Epidemiologic StudiesDepression Scale ≥ 16 [CES-D] or the Beck Depression Inventory ≥ 10[BDI-I]); (4) anti-psychotic medication use; and (5) glucocorticoidmedication use.
The sample recruitment strategy and generalizability was assessedaccording to the 2008 Estimated Resident Population [27]. Accordingly,data were weighted by age group, sex, region, and probability ofselection in the household. Data collected for the MAILES studyincluded questionnaire-based information and a baseline clinicvisit between 2002 and 2006 (Baseline) and rolling follow-upoccurred between 2007 and 2010 (median 4.94 year follow-up,interquartile range 4.34–5.00). A flow chart of patients through thestudy is provided in Fig. 1.
A previous MAILES report [27] shows that non-respondents to the5 year follow-up were, at baseline; more likely to be in the N75 yearage group (16.6% vs. 5.8%, p b .001), less likely to have attained abachelor university degree or higher (6.3% vs. 12.9%, p b .001), less likelyto have an annual gross income N AUD $80,000 (9.3% vs. 16.3%, p b .05),less likely to been born in Australia (59.8% vs. 67.0%, p b .05), less likelyto be married (62.5% vs. 76.3%, p b .05), and less likely to be employedfull-time (31.4% vs. 51.7%, p b .05).With respect to comorbid conditionsnon-respondents at 5 year follow-up were more likely to have diabetes(14.1% vs. 9.5%, p b .001), cardiovascular disease (13.5% vs. 9.7%, p b .01),physician diagnosed depression (13.1% vs. 9.1%, p b .01), be currentsmokers (26.1% vs. 18.5%) and be overweight or obese (67.8% vs.77.9%, p b .05).

330 P.J. Tully et al. / Physiology & Behavior 139 (2015) 328–335
2.2. Systemic inflammation
Blood samples were drawn between 8 and 11 a.m. after a 12 hovernight fast. Samples were kept on ice until centrifuged, separated,and stored at −80 °C. High sensitivity CRP mg/L (hsCRP), TNF-α pg/L,and IL-6 pg/L, were quantitatedwith an enzyme linked immunosorbentassay (ELISA) and Cobas autoanalyzer (Roche Diagnostics, FlorhamPark, New Jersey, US). The inter-assay change values (CVs) were 2.1%for hsCRP, 10.6% for TNF-α, and 7.8% for IL-6. Plasma glucose wasdetermined using an automated chemistry analyzer system (OlympusAU5400; Olympus Corp., Tokyo, Japan), and glycated hemoglobin(HbA1c) was measured by high performance liquid chromatographyusing a spherical cation exchange gel (CV, 2% at 6% of total hemoglobin).Blood samples were analyzed in the same laboratory.
2.3. Anthropometry
Waist circumference wasmeasured to the nearest 0.1 cm using an in-elastic tapemaintained in a horizontal plane at the level of the narrowestpart of the waist, and read from the mid-axillary line, with the subjectstanding comfortably with weight distributed evenly on both feet.Abdominal adiposity was defined as waist circumference ≥ 102 cmaccording to guidelines [24].
2.4. Chronic conditions at baseline
Blood pressure was measured at the clinic visit and hypertensionwas defined as systolic blood pressure N 140 mm Hg and/or diastolicblood pressure N 90 mm Hg, or use of antihypertensive medication.Range for high triglycerides was ≥2.0 mmol/L, and for low high-density lipoprotein (HDL) b0.9 mmol/L. Diabetes was defined asfasting blood glucose ≥ 7.0 mmol/L, having known diabetes (physiciandiagnosed or use of medications), or HbA1c ≥ 6.2 mmol/L [29]. Thepresence of CVD was based on self-report. The validity of self-reporteddiabetes and CVD compared to medical records has been demonstratedpreviously [30,31]. Medication use was obtained from MedicareAustralia by confidential unit record linkage, classified according tothe Anatomical Therapeutic Chemical (ATC) Classification [28].
2.5. Behavioral/lifestyle factors
The physical activity questions from the Australian National HealthSurveys were used to classify participants as sedentary or having low,moderate, or high levels of physical activity calculated with metabolicequivalents [32]. Smoking behavior was recorded as nonsmoker,ex-smoker, and current smoker. Alcohol use was determined at clinicalinterview and recorded in standard drinks consumed per day; low ≤2,moderate 3–4, high ≥5.
2.6. Stratification by abdominal obesity and metabolic health
The metabolically unhealthy variable constituted ≥2 metabolicrisk factors including hypertension, diabetes, low HDL and hightriglycerides, similar to that reported previously [21]. To determinethe effects of abdominal adiposity ≥102 cm in combination withmetabolic health participants were allocated into one of four groupsas follows: no-abdominal obesity and metabolically healthy, no-abdominal obesity and metabolically unhealthy, abdominal obesityand metabolically healthy, and abdominal obesity and metabolicallyunhealthy.
2.7. Endpoint: depressive symptoms at five year follow-up
The endpoint was incident depressive symptoms at five yearfollow-up, determined by either the CES-D [33] or BDI-I [34,35].The cut-off scores for clinically relevant depression symptoms were
set at ≥16 and ≥10 for the CES-D and BDI-I respectively whichreflect at least mild depression symptoms [33–35]. The selectedcut-off scores have been shown to reflect clinically relevant depres-sive symptoms and are comparable for the separate depressionmeasures [33–35]. Prevalence rates of depressive symptoms didnot differ in the baseline sample when the CES-D or BDI was used.An open-ended question was asked to participants to determinewhether a physician had ever told them that they were depressedin the previous 12-months. This was excluded from the depressionendpoint for a number of reasons. Physician reports at 5 yearfollow-up were based on preceding 12 month history and werethus not contemporaneous with participant completion of CES-Dand BDI. This would likely explain why 12-month physician reportof depression at 5 year follow-up was not associated with 2-weekself-reported depressive symptoms.
2.8. Statistical analysis
Data analysis was performed with SPSS® 20.0 statistical softwarepackage (SPSS Inc., Chicago, IL). A p-value of b0.05 was consideredsignificant. No adjustment was made for multiple comparisons basedon the recommendation of Rothman [36] that fewer errors of inter-pretation will be made when observing interrelated phenomena.Log and back transformation was applied to baseline hsCRP, IL-6 andTNF-α because of skewness of the data. To incorporate the change be-tween baseline andmedian 5-year follow-upmeasures of inflammationin a single analysis, annualized Δ inflammation was calculated forhsCRP, IL-6 and TNF-α as; e.g. ΔhsCRP= hsCRPTime 2 − hsCRPTime 1 di-vided by number of years between clinical assessments [28]. Such anal-yses permit an examination of change in inflammation as opposed tocross-sectional analysis of Time 2 inflammation.
Analyses concerning clinically relevant depressive symptoms at5 year follow-up were assessed with logistic regression showing theodds ratio (OR) and 95% confidence interval (CI) (Table 1). To avoidoverfitting themodels, only covariates associated with incident depres-sive symptoms (p b .20) were retained for multivariate analysis [37].The first logistic regression models consisted of stepped entry of demo-graphic andmedical comorbidity covariates followedbyhsCRP, IL-6 andTNF-αwhich were forced into the models. The secondmodel consistedof stepped entry of demographic, medical comorbidity covariates, andthe abdominal obesity–metabolic health variable followed by hsCRP,IL-6 and TNF-α. The two types of models specified above wereperformed with baseline inflammation, and then repeated withannualized Δ inflammation. In all models regression coefficientmulticollinearity was within acceptable thresholds b .50; inspectionof regression model discriminatory and fit indices included the Hosmerand Lemeshow χ2 test and the c-index. Sensitivity analysis proceededby excluding participants according to comorbid conditions; rheuma-toid arthritis, osteoarthritis, diabetes mellitus, medication use, andage b 60 years, consistent with another study [16].
Ancillary analysis sought to stratify patient groups based on waistcircumference ≥ 102 cm, and ≥2 metabolic risk factors to identifypossible discrete effects within these sub-groups [23]. Owing to thelimited number of participants in these groups, and limited numberof persons with clinically significant depressive symptoms, linearregression models were used. Consequently, raw depression scoresfor the BDI and CESD were converted into z scores for interpretabil-ity. Linear regression models were conducted adjusted for age,marital status, rheumatoid arthritis, exercise level and smokingstatus. In the linear regression analyses a positive and significantstandardized β value indicates an increase in depression symptoms(z score). To avoid multicollinearity, tolerance, the variance inflationfactor (VIF) and eigen values were used to measure the strength ofthe linear relationships between the independent variables; a toler-ance value of ≥0.2 and/or VIF ≤ 4 and/or an eigen value N .01 wasregarded as acceptable [38].

Table 1Descriptives for sample and odds ratio for incident depression at follow-up.
Time 1 variables No depression Incident depression p OR 95% CI lower 95% CI upper p
Age, M(SD) 54.1 ± 11.3 51.5 ± 10.8 .03 .99 .97 1.00 .10Co-habitation status
Married/partner (reference) 874 (81.5) 68 (71.6) .02 – – – –
Living alone 198 (18.5) 27 (28.4) 2.03 1.33 3.09 b .001Waist circumference ≥ 102 cm 423 (39.5) 48 (50.5) .04 1.55 1.02 2.34 .04Hypertension 535 (49.9) 48 (50.5) .91 1.11 .78 1.60 .58Triglycerides N 2.0 mmol/L 313 (29.2) 24 (25.3) .42 .89 .59 1.35 .60High density lipoprotein b .9 65 (6.1) 5 (5.3) .75 .66 .26 1.67 .38Diabetes 137 (12.8) 14 (14.7) .59 1.31 .79 2.18 .29Abdominal adiposity–metabolic health variable .11
No-abdominal adiposity and metabolically healthy (reference) 554 (51.7) 42 (44.2) – – – –
No-abdominal adiposity and metabolically unhealthy 95 (8.9) 5 (5.3) .69 .27 1.80 .45Abdominal adiposity and metabolically healthy 248 (23.1) 31 (32.6) 1.65 1.01 2.69 .04Abdominal adiposity and metabolically unhealthy 175 (16.3) 17 (17.9) 1.28 .71 2.31 .41
Physical activity levelHigh (reference) 250 (23.3) 30 (31.6) .07 – – – –
Moderate 398 (37.1) 34 (35.8) 1.30 .58 2.91 .53Low 313 (29.2) 24 (25.3) 1.29 .58 2.88 .53Sedentary 111 (10.4) 7 (7.4) 1.82 .82 4.05 .14
Osteoarthritis 64 (6.0) 4 (4.2) .48 .55 .20 1.54 .26Rheumatoid arthritis 29 (2.7) 4 (4.2) .34 1.89 .78 4.59 .16Smoking status .13
Non-smoker (reference) 440 39 – – – –
Past 454 (42.5) 31 (32.6) .80 .51 1.26 .33Current 177 (16.6) 26 (27.4) 1.69 1.03 2.76 .04
Alcohol intake (standard drinks)Low b2 (reference) 636 (59.3) 51 (53.7) .40 – – – –
Moderate 3–4 247 (23.0) 26 (27.4) 1.23 .77 1.96 .39High N5 189 (17.6) 18 (18.9) 1.25 .74 2.10 .41
Diagnosed anxiety 25 (2.3) 2 (2.1) N .99 1.53 .71 3.28 .28Log hsCRP (mg/L), M(SD) .11 ± .47 .18 ± .52 .20 1.38 .92 2.08 .12Log IL-6 (pg/L), M(SD) .42 ± .19 .43 ± .18 .61 1.32 .79 2.18 .29Log TNF-α (pg/L), M(SD) .42 ± .17 .39 ± .12 .08 .34 .09 1.30 .11Δ hsCRP (mg/L), M(SD) 1.70 ± 3.84 3.01 ± 10.21 .009 1.03 1.00 1.07 .03Δ IL-6 (pg/L), M(SD) 1.54 ± 1.74 1.52 ± 1.21 .92 .99 .88 1.13 .92Δ TNF-α (pg/L), M(SD) 1.42 ± 1.41 1.14 ± .60 .06 .76 .59 1.00 .05
Acronyms: CI, confidence interval; hsCRP, high sensitivity C-reactive protein; IL-6, interleukin-6; M, mean; OR, odds ratio; SD, standard deviation, TNF-α, tumor necrosis factor-α.
331P.J. Tully et al. / Physiology & Behavior 139 (2015) 328–335
2.9. Statistical power
The cohort size was determined to detect a minimum detectablerelative risk of chronic disease exceeding 1 in 1.22 and less than 1 in0.81 between groups of participants with and without risk-factorexposure in multivariate analyses [27]. In the present study a sampleof 951 was required for the continuous inflammatory measures basedon an unbalanced design and low event rates for incident depressivesymptoms assuming criteria of a: (i) 80% power; (ii) use of a two-tailed test; (iii) a 5% chance of type 1 error; and (iv) a conservativeestimate event rate 1 SD above the reference group.
Table 2Adjusted model showing odds ratio for incident depression by inflammatory markers.
Model 1
Variable OR 95% CI lower 95% CI upper
Baseline inflammationhsCRP 1.04 1.00 1.07TNF-α .81 .63 1.04IL-6 .97 .84 1.13
Annualized inflammationhsCRP 1.04 1.01 1.08TNF-α .80 .61 1.06IL-6 .95 .81 1.13
Acronyms: CI, confidence interval; hsCRP, high sensitivity C-reactive protein; IL-6, interleukin-Model 1. Adjusted for age, marital status, rheumatoid arthritis, exercise level, smoking status.Model 2. Adjusted for age, marital status, rheumatoid arthritis, exercise level, smoking status, aa. Annualized change in hsCRP, IL-6 and TNF-α calculated as; Inflammation markerTime 2 − In
3. Results
3.1. Descriptives
Descriptive characteristics of the sample are shown in Table 1 forthe final sample (N = 1167). Incident depressive symptoms devel-oped in 95 men (8.14% of total). At baseline, it was found that menwho developed depressive symptoms were significantly younger,more likely to live alone, were characterized by a higher proportionof waist circumference ≥ 102 cm at baseline, and higher ΔhsCRP atfollow-up. It was also found that incident depressive symptoms
Model 2
p OR 95% CI lower 95% CI upper p
.03 1.04 1.00 1.07 .03
.10 .81 .63 1.05 .11
.70 .96 .82 1.11 .58
.02 1.04 1.01 1.08 .02
.12 .81 .61 1.07 .14
.58 .94 .80 1.12 .49
6; OR, odds ratio; TNF-α, tumor necrosis factor-α.
nd abdominal obesity–metabolic health.flammation markerTime 1 divided by number of years between clinical assessments.

Table 4Adjusted model showing standardized regression coefficient for five year depressionsymptoms by inflammatory markers according to waist circumference, body mass indexand metabolic health.
BaselineinflammationModel 1
AnnualizedinflammationModel 2a
Sub-sample (analysis N) β p β p
332 P.J. Tully et al. / Physiology & Behavior 139 (2015) 328–335
were associated with abdominal obesity when not in conjunctionwith metabolic disturbances (OR = 1.65; 95% CI 1.01–2.69, p = .04).
3.2. Incident clinically relevant depressive symptoms
The adjusted logistic regression for incident clinically relevantdepressive symptoms according to inflammatory markers is shownin Table 2. These analyses showed that baseline hsCRP was associatedwith increased risk for incident depressive symptoms adjusted forcovariates (adjusted OR = 1.04; 95% CI 1.00–1.07, p = .03). The oddsratio for hsCRP was not attenuated when the abdominal obesity–metabolic health variable was entered into the model. The associationbetween hsCRP and incident depressive symptoms translates to a 4%increase in odds for depressive symptoms for every 1 mg/L increase inhsCRP. The findings for baseline TNF-α tended to suggest a reducedrisk in incident depressive symptoms however these findings failed toattain conventional significance when adjusted for covariates includingthe abdominal obesity–metabolic health variable (adjusted OR = .81;95% CI .63–1.05. p = .11).
The annualized change in inflammation is shown in Table 2.The findings corroborated that ΔhsCRPwas associated with clinicallyrelevant depressive symptoms at five year follow-up even afteradjustment for abdominal obesity–metabolic health. Specifically,this model suggested that increase in annualized ΔhsCRP over five-years was associated with incident depressive symptoms (adjustedOR = 1.04; 95% CI 1.01–1.08, p = .02). The association betweenannualized change in IL-6 and TNF-α with incident depressivesymptoms failed to attain conventional significance.
3.3. Sensitivity analyses
In sensitivity analyses we first assessed the level of inflammationacross the abdominal obesity–metabolic health groups. There was amain between-group effect for hsCRP (F (3, 1165) = 50.69, p b .001).Post-hoc analyses showed that the abdominal obesity patients,irrespective of metabolic health, had significantly higher hsCRP atbaseline (Bonferroni correction p b .01). There was also a mainbetween-group effect for IL-6 (F (3, 1165) = 22.59, p b .001). Post-hocanalyses again suggested that the abdominal obesity patients,irrespective of metabolic health, had significantly higher IL-6 atbaseline (Bonferroni correction p b .001). There was also a main
Table 3Sensitivity analysis showing adjusted odds ratio for incident depression by hsCRP excludingpersons with specified covariates.
Sensitivity exclusioncovariate
Depressedcases
OR 95% CIlower
95% CIupper
p
hsCRPRheumatoid arthritisa 81 1.04 1.00 1.07 .03Osteoarthritis 80 1.04 1.00 1.07 .03Diabetes 57 1.05 1.01 1.09 .02Medication use 85 1.04 1.00 1.07 .03Age b 60 68 1.05 1.00 1.09 .04
Annualized hsCRPb
Rheumatoid arthritisa 81 1.04 1.01 1.08 .02Osteoarthritis 80 1.04 1.01 1.08 .02Diabetes 57 1.05 1.01 1.10 .02Medication use 85 1.04 1.01 1.08 .02Age b 60 68 1.05 1.00 1.10 .04
Models adjusted for age, marital status, rheumatoid arthritis, exercise level, smokingstatus, abdominal obesity–metabolic health.a. Rheumatoid arthritis not adjusted for in this analysis as it was a pre-specified exclusioncovariate.b. Annualized change in hsCRP, IL-6 and TNF-α calculated as; InflammationmarkerTime 2 − Inflammation markerTime 1 divided by number of years betweenclinical assessments.Medication use inclusive of any antileptic, sex hormone, antiandrogen, no patients weretaking opiates, anti-psychotics or glucocorticoids.
between-group effect for TNF-α (p b .001). Post-hoc analyses suggestedthat the non-obese and metabolically healthy group had significantlylower TNF-α than the non-obese-metabolically unhealthy and theobese-metabolically unhealthy group (Bonferroni correction p b .01).
Sensitivity analyses excluding pre-specified participant subgroupsare shown in Table 3. The results supported a significant association be-tween baseline hsCRP and ΔhsCRP with incident clinically relevant de-pressive symptoms when participants were excluded with rheumatoidarthritis, osteoarthritis, diabetes,medication use and age b 60 years (ad-justed ORs 1.04). In these analyses both IL-6 and TNF-αwere not signif-icantly associated with depressive symptoms in sensitivity analysis(data not shown).
3.4. Linear models of depressive symptoms (z-scores)
3.4.1. Total sampleThe linear regression results are shown in Table 4. The linear regres-
sion analyses did not support an association between baseline hsCRPand depressive symptoms at five-year follow-up (β = .07, p = .06).However a significant and positive association was evident for annual-ized ΔhsCRP (β= .15, p b .001). None of the IL-6 or TNF-α associationswere significant.
3.4.2. Waist circumferenceStratification according to participants with waist circumference b
102 cm (n = 598) did not support an association between baselinehsCRP and depressive symptoms at five-year follow-up (β = .05,p = .26). A significant association was evident however for annual-ized ΔhsCRP (β = .19, p b .001). Stratification according to waistcircumference ≥ 102 cm (n = 587) also did not support an associa-tion between baseline hsCRP and depressive symptoms at five-year
All patients (n = 1185)b
hsCRP .07 .06 .15 b .001IL-6 .02 .50 − .04 .24TNF-α − .05 .09 − .03 .41
Waist circumference b 102 cm (n = 598)c
hsCRP .05 .26 .19 b .001IL-6 .01 .86 − .02 .55TNF-α − .05 .28 .02 .72
Waist circumference ≥ 102 cm (n = 587)c
hsCRP .08 .14 .09 .11IL-6 .02 .70 − .06 .28TNF-α − .07 .21 − .06 .28
b1 metabolically risk factors (n = 641)c
hsCRP .08 .04 .18 b .001IL-6 .02 .71 − .03 .45TNF-α − .05 .19 − .04 .32
≥2 metabolically risk factors (n = 542)c
hsCRP .07 .28 .05 .44IL-6 .06 .35 − .07 .29TNF-α − .07 .29 .05 .49
Acronyms: β, standardized regression coefficient; hsCRP, high sensitivity C-reactiveprotein; IL-6, interleukin-6; TNF-α, tumor necrosis factor-α.a. Annualized change in hsCRP, IL-6 and TNF-α calculated as; InflammationmarkerTime 2 − Inflammation markerTime 1 divided by number of years betweenclinical assessments.b. Analyses adjusted for age, marital status, rheumatoid arthritis, exercise level, smokingstatus, abdominal obesity–metabolic health variable.c. Analyses adjusted for age, marital status, rheumatoid arthritis, exercise level,smoking status.

333P.J. Tully et al. / Physiology & Behavior 139 (2015) 328–335
follow-up (β = .08, p = .14) or annualized ΔhsCRP (β = .09, p =.11). None of the IL-6 or TNF-α associations were significant.
3.4.3. Metabolic healthStratification by ≤1 metabolic disturbances (n = 641) showed that
a positive association was evident between depressive symptomsat five-year follow-up and baseline hsCRP (β = .08, p = .04) andannualized ΔhsCRP (β = .18, p b .001). Stratification by ≥2 metabolicdisturbances (n = 542) showed that there was no significantassociation between depressive symptoms at five-year follow-upand baseline or annualized ΔhsCRP. None of the IL-6 or TNF-αassociations were significant.
4. Discussion
This longitudinal cohort study adds to previous research byshowing that annualized increase in ΔhsCRP over five years, andto a lesser extent, baseline hsCRP was significantly associated withincident depressive symptoms. These data showed a significant asso-ciation between hsCRP and incident depressive symptoms indepen-dent of age, smoking, exercise level, rheumatoid arthritis, centralobesity and N2 metabolic risk factors. Though the findings are inline with prior studies implicating cardiometabolic and inflammato-ry biomarkers in depression [17,20,39] a discrete finding was therelationship between annualized ΔhsCRP, and to a lesser extentbaseline hsCRP, with five-year depressive symptoms in personswith waist circumference b 102 cm and with ≤1 metabolic distur-bance. The general absence of association between TNF-α and IL-6with incident depressive symptoms contrasts to several longitudinalstudies [25,40,41], while is in line with others [42,43], reflecting thelack of consensus in this area.
The current findings with regard to hsCRP align closely with Au'sreport [44] from the English Longitudinal Study of Ageing which alsoshowed that hsCRP was only related to elevated depressive symptomsin personswithoutmetabolic syndrome. The importance and potential-ly confounding role of central obesity and metabolic risk factors isunderscored by our discrete findings which suggested that these partic-ular factors altered the longitudinal association between inflammationand incident depressive symptoms. The role of hsCRP in incidentdepressive symptoms appears less clear, and in contrast to, prior studiesreporting particular strong associations among males [45]. The non-significant association between hsCRP and incident depressive symp-toms in males with abdominal obesity or metabolic disturbance indi-cates that metabolic factors may alter the hsCRP–depression link morethan previously recognized. Moreover, it was evident that abdominalobesity was significantly associated with hsCRP, IL-6 and TNF-α. Yetthe non-significant association with depression among males withabdominal obesity and metabolic disturbance extends further Howrenet al.'s [22] finding for a significant attenuation of effect sizes withadjustment for BMI in their pooled meta-analysis. Collectively thesefindings suggest that the association between chronic low-grade in-flammation and subsequent depressive symptoms is partly obscuredby abdominal obesity and metabolic risk factors. Inconsistent findingsto date are conceivably due to the initial assumption that circulatingcytokine activity in depression is predominantly a marker of anup-regulated immune-response and not part of a broader neuroendo-crine response [10].
The current study simplified potential etiological links in four ways.Firstly, this study examined only one direction of the inflammation–depression link when bidirectional associations are established. Sec-ondly, this study focused on the hypothesis that, for example,cytokines are pro-inflammatory when evidence supports that IL-6is implicated in immune down-regulation [46], and furthermore,that depression is associated with immune-suppression [14]. Thirdly,a number of demographic and behavioral factors are implicated inincident depressive symptoms including age, living alone and social
supports, sedentary behaviors and current smoking [3,39,44,47]. Yetseveral of these behavioral factors, particularly sedentary behaviorand smoking, are known to increase low-grade inflammation [19,48]and thus we could not rule out the possibility that incident depres-sive symptoms were mediated by such behavioral risk factors.Fourthly, this study measured a heterogeneous constellation ofdepressive symptoms and it is plausible that cytokines are discretelyassociated with subsets of depressive symptoms, and depressiondisorder subtypes. Supporting this Capuron and colleagues [49]reported that CRP and IL-6 were associated with neurovegetativedepressive symptoms and to a lesser extent, total BDI scores incross-sectional analysis of 323 male twin-pairs. It is possible thatthe findings are representative for clinically relevant depressivesymptoms in general, but do not necessarily translate to other studiesfocusing on cognitive depressive symptoms [16] ormelancholic depres-sion subtypes [50]. Thereby, analysis of depression subtypes may helpto further disentangle the association between inflammation and inci-dent depressive symptoms, by dismantling subtype specific effectsthat might be leveled out on a general depression level [51]. In a similarline, it cannot be ruled out that incident depressive symptoms were amanifestation of broader environmental or social stressors, consideringthat stress more generally is associated with obesity and inflammatorymarkers [52,53].
The lack of association between hsCRP, IL-6 and TNF-αwith depres-sive symptomswas limited to personswith abdominal obesity andmet-abolic disturbance, as evidenced by sensitivity analyses and ancillaryanalyses. The findings with respect to IL-6 and TNF-α in particular con-trast to the extant meta-analysis data which was inclusive of studiescontemporaneously adjusting for BMI [22] albeit not the combinationof abdominal obesity and metabolic risk factors. Nonetheless, the cur-rent findings utilizing depressive symptoms do not parallel thoseamong persons with major depression whom reportedly exhibit signif-icantly higher TNF-α and IL-6 [15]. It is plausible that mild depressivesymptoms are less strongly associated with TNF-α and IL-6 thanepisodes of major depression. In a similar line, longitudinal associ-ations between CRP and IL-6 with depressive symptoms are typicallysmall [20].
A strength of the study is measurement of a comprehensive set ofcardiometabolic factors longitudinally among a representative sampleof Australian men. Consequently these findings may not generalize topopulations comprised by females [18,54] or older adults [55]. Thesedata are presented with a number of limitations that may increasethe risk of bias including the observational and longitudinal design,while a higher proportion of comorbidities characterized men lostto follow-up. It was possible that physician diagnosis of depressionreflected non-current or treated episodes of depression, the latterwhich is known to alter inflammatory responses [47,56]. Also, thestudy utilized two different questionnaire reports of depressionsymptoms rather than structured interview, and as such, the find-ings may not reflect clinically diagnosed episodes of depression.Inflammation–depression links are strongest for clinical depression[20,22] and those using antidepressants [56], while obesity andmetabolic health also increase risk for major depression [57,58].Likewise, depression–metabolic associations are strongest for clini-cal depression [2,59]. Here, less than 8% of males reported incidentdepressive symptoms at 5 year follow-up. As a consequence ofthe limited statistical power afforded by regression analyses withfew incident depression cases the results should be interpretedcautiously. The present study only examined one direction of theinflammation–incident depressive symptom hypothesis. Consider-ing that the association between inflammation, abdominal obesity,metabolic factors and depression is undoubtedly complex andbidirectional, it is possible that discrete effects between these riskfactors would be uncovered longitudinally with structural equationmodels [25]. Similarly, it is plausible that the depression responseassociated with inflammation and metabolic factors is reversible [60].

334 P.J. Tully et al. / Physiology & Behavior 139 (2015) 328–335
5. Conclusions
In conclusion heightened baseline and annualized change inhsCRP were associated with incident depressive symptoms at 5 yearfollow-up in males. This study adds to previous literature by highlight-ing that the association between hsCRP and depression was not upheldin participantswithwaist circumference≥ 102 cmor≥2metabolic dis-turbances. The findings that heightened hsCRP precedes depressivesymptoms only among males whom are free from abdominal obesityor metabolic disturbance suggest that further investigation should ex-amine the role of these particular metabolic factors in the hypothesizedinflammation–depression link.
Acknowledgments
The authors thank the MAILES investigators for their role in thestudy.
Role of the funding sourceThis work was supported by the National Health and Medical
Research Council of Australia (NHMRC Project Grant # 627227;NHMRC Clinical Overseas Fellowship # 1053578). The funding bodyhad no role in the design and conduct of the study; in the collection,analysis, and interpretation of the data; or in the preparation, review,or approval of the manuscript.
References
[1] NgM, Fleming T, RobinsonM, Thomson B, Graetz N,Margono C, et al. Global, regional,and national prevalence of overweight and obesity in children and adults during1980–2013: a systematic analysis for the Global Burden of Disease Study. Lancet2013:2014.
[2] Luppino FS, de Wit LM, Bouvy PF, Stijnen T, Cuijpers P, Penninx BW, et al.Overweight, obesity, and depression: a systematic review and meta-analysis oflongitudinal studies. Arch Gen Psychiatry 2010;67:220–9.
[3] Valtonen MK, Laaksonen DE, Laukkanen JA, Tolmunen T, Viinamaki H, Lakka HM,et al. Low-grade inflammation and depressive symptoms as predictors of abdominalobesity. Scand J Public Health 2012;40:674–80.
[4] Cartier A, Cote M, Lemieux I, Perusse L, Tremblay A, Bouchard C, et al. Age-relateddifferences in inflammatory markers in men: contribution of visceral adiposity.Metabolism 2009;58:1452–8.
[5] SmithMM,Minson CT. Obesity and adipokines: effects on sympathetic overactivity. JPhysiol 2012;590:1787–801.
[6] Maes M. Depression is an inflammatory disease, but cell-mediated immuneactivation is the key component of depression. Prog NeuropsychopharmacolBiol Psychiatry 2011;35:664–75.
[7] Leonard B,MaesM.Mechanistic explanations how cell-mediated immune activation,inflammation and oxidative and nitrosative stress pathways and their sequels andconcomitants play a role in the pathophysiology of unipolar depression. NeurosciBiobehav Rev 2012;36:764–85.
[8] Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry 2010;67:446–57.
[9] Dantzer R, O'Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation tosickness and depression: when the immune system subjugates the brain. Nat RevNeurosci 2008;9:46–56.
[10] Messay B, Lim A, Marsland A. Current understanding of the bi-directional relation-ship of major depression with inflammation. Biol Mood Anxiety Disord 2012;2:4.
[11] Dantzer R, Kelley KW. Twenty years of research on cytokine-induced sicknessbehavior. Brain Behav Immun 2007;21:153–60.
[12] Penninx BW, Milaneschi Y, Lamers F, Vogelzangs N. Understanding the somaticconsequences of depression: biological mechanisms and the role of depressionsymptom profile. BMC Med 2013;11:129.
[13] van Reedt Dortland AK, Vreeburg SA, Giltay EJ, Licht CM, Vogelzangs N, van Veen T,et al. The impact of stress systems and lifestyle on dyslipidemia and obesity inanxiety and depression. Psychoneuroendocrinology 2013;38:209–18.
[14] Blume J, Douglas SD, Evans DL. Immune suppression and immune activation indepression. Brain Behav Immun 2011;25:221–9.
[15] Liu Y, Ho RC, Mak A. Interleukin (IL)-6, tumour necrosis factor alpha (TNF-α) andsoluble interleukin-2 receptors (sIL-2R) are elevated in patients with majordepressive disorder: a meta-analysis and meta-regression. J Affect Disord2012;139:230–9.
[16] GimenoD,KivimakiM, Brunner EJ, ElovainioM,DeVogli R, SteptoeA, et al. Associationsof C-reactive protein and interleukin-6 with cognitive symptoms of depression:12-year follow-up of the Whitehall II study. Psychol Med 2009;39:413–23.
[17] Deverts DJ, Cohen S, DiLillo VG, Lewis CE, Kiefe C, Whooley M, et al. Depressivesymptoms, race, and circulating C-reactive protein: the Coronary Artery RiskDevelopment in Young Adults (CARDIA) study. Psychosom Med 2010;72:734–41.
[18] Matthews KA, Schott LL, Bromberger JT, Cyranowski JM, Everson-Rose SA, SowersM.Are there bi-directional associations between depressive symptoms and C-reactiveprotein in mid-life women? Brain Behav Immun 2010;24:96–101.
[19] Hamer M, Molloy GJ, de Oliveira C, Demakakos P. Persistent depressive symptom-atology and inflammation: to what extent do health behaviours and weight controlmediate this relationship? Brain Behav Immun 2009;23:413–8.
[20] Valkanova V, Ebmeier KP, Allan CL. CRP, IL-6 and depression: a systematic reviewand meta-analysis of longitudinal studies. J Affect Disord 2013;150:736–44.
[21] Hamer M, Batty GD, Kivimaki M. Risk of future depression in people who are obesebut metabolically healthy: the English longitudinal study of ageing. Mol Psychiatry2012;17:940–5.
[22] Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive protein,IL-1, and IL-6: a meta-analysis. Psychosom Med 2009;71:171–86.
[23] Bouchard C. BMI, fat mass, abdominal adiposity and visceral fat: where is the beef?Int J Obes 2007;31:1552–3.
[24] Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al.Diagnosis and management of the metabolic syndrome: an American HeartAssociation/National Heart, Lung, and Blood Institute Scientific Statement.Circulation 2005;112:2735–52.
[25] Stewart JC, Rand KL, Muldoon MF, Kamarck TW. A prospective evaluation of thedirectionality of the depression–inflammation relationship. Brain Behav Immun2009;23:936–44.
[26] Jokela M, Hamer M, Singh-Manoux A, Batty GD, Kivimaki M. Association of metabol-ically healthy obesity with depressive symptoms: pooled analysis of eight studies.Mol Psychiatry 2014;19:910–4.
[27] Grant JF, Martin SA, Taylor AW, Wilson DH, Araujo A, Adams RJ, et al. Cohort Profile:The Men Androgen Inflammation Lifestyle Environment and Stress (MAILES) Study.Int J Epidemiol 2014;43:1040–53.
[28] Shi Z, Araujo AB, Martin S, O'Loughlin P, Wittert GA. Longitudinal changes intestosterone over five years in community-dwelling men. J Clin EndocrinolMetab 2013;98:3289–97.
[29] Jesudason DR, Dunstan K, Leong D, Wittert GA. Macrovascular risk and diagnosticcriteria for type 2 diabetes: implications for the use of FPG and HbA(1c) for cost-effective screening. Diabetes Care 2003;26:485–90.
[30] Schneider AL, Pankow JS, Heiss G, Selvin E. Validity and reliability of self-reporteddiabetes in the Atherosclerosis Risk in Communities Study. Am J Epidemiol 2012;176:743.
[31] Okura Y, Urban LH, Mahoney DW, Jacobsen SJ, Rodeheffer RJ. Agreement betweenself-report questionnaires and medical record data was substantial for diabetes,hypertension, myocardial infarction and stroke but not for heart failure. J ClinEpidemiol 2004;57:1096–103.
[32] Australian Bureau of Statistics. National Health Survey: users' guide; 2003[Canberra,Australia].
[33] Radloff LS. The CES-D scale: a self-report depression scale for research in the generalpopulation. Appl Psychol Meas 1977;1:385–401.
[34] Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuringdepression. Arch Gen Psychiatry 1961;4:561–71.
[35] Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck DepressionInventory: twenty-five years of evaluation. Clin Psychol Rev 1988;8:77–100.
[36] Rothman KJ. No adjustments are needed for multiple comparisons. Epidemiology1990;1:43–6.
[37] BabyakMA.What you seemay not bewhat youget: a brief, nontechnical introductionto overfitting in regression-type models. Psychosom Med 2004;66:411–21.
[38] Tabachnick BG, Fidell LS. Using multivariate statistics. 4th ed. Boston, MA: Allyn andBacon; 2000.
[39] Daly M. The relationship of C-reactive protein to obesity-related depressivesymptoms: a longitudinal study. Obesity (Silver Spring, Md) 2013;21:248–50.
[40] van den Biggelaar AHJ, Gussekloo J, de Craen AJM, Frölich M, Stek ML, van derMast RC, et al. Inflammation and interleukin-1 signaling network contribute todepressive symptoms but not cognitive decline in old age. Exp Gerontol 2007;42:693–701.
[41] Baune BT, Smith E, Reppermund S, Air T, Samaras K, Lux O, et al. Inflammatorybiomarkers predict depressive, but not anxiety symptoms during aging: theprospective Sydney Memory and Aging Study. Psychoneuroendocrinology2012;37:1521–30.
[42] Chocano-Bedoya PO, Mirzaei F, O'Reilly EJ, Lucas M, Okereke OI, Hu FB, et al.C-reactive protein, interleukin-6, soluble tumor necrosis factor α receptor 2 andincident clinical depression. J Affect Disord 2014;163:25–32.
[43] Vetter ML, Wadden TA, Vinnard C, Moore RH, Khan Z, Volger S, et al. Genderdifferences in the relationship between symptoms of depression and high-sensitivity CRP. Int J Obes (Lond) 2013;37(Suppl. 1):S38–43.
[44] Au B, Schmitz N. Association of C-reactive protein with metabolic syndrome anddepressive symptoms in the English longitudinal study of ageing. J EpidemiolCommunity Health 2013;67:e2.
[45] Luukinen H, Jokelainen F, Hedberg P. The relationships between high-sensitivityC-reactive protein and incident depressed mood among older adults. Scand J ClinLab Invest 2010;70:75–9.
[46] Baune BT, Konrad C, Grotegerd D, Suslow T, Birosova E, Ohrmann P, et al.Interleukin-6 gene (IL-6): a possible role in brain morphology in the healthy adultbrain. J Neuroinflammation 2012;9:125.
[47] Vogelzangs N, Duivis HE, Beekman AT, Kluft C, Neuteboom J, HoogendijkW, et al.Association of depressive disorders, depression characteristics and antidepressantmedication with inflammation. Transl Psychiatry 2012;2:e79.
[48] Hamer M, Sabia S, Batty GD, Shipley MJ, Tabak AG, Singh-Manoux A, et al. Physicalactivity and inflammatory markers over 10 years: follow-up in men and womenfrom the Whitehall II cohort study. Circulation 2012;126:928–33.

335P.J. Tully et al. / Physiology & Behavior 139 (2015) 328–335
[49] Capuron L, Su S, Miller AH, Bremner JD, Goldberg J, Vogt GJ, et al. Depressivesymptoms and metabolic syndrome: is inflammation the underlying link? BiolPsychiatry 2008;64:896–900.
[50] Patas K, Penninx BWJH, Bus BAA, Vogelzangs N, Molendijk ML, Elzinga BM, et al.Association between serum brain-derived neurotrophic factor and plasmainterleukin-6 in major depressive disorder with melancholic features. BrainBehav Immun 2014;36:71–9.
[51] Baumeister H, Parker G.Meta-review of depressive subtypingmodels. J Affect Disord2012;139:126–40.
[52] Rosmond R, Dallman MF, Bjorntorp P. Stress-related cortisol secretion in men:relationships with abdominal obesity and endocrine, metabolic and hemodynamicabnormalities. J Clin Endocrinol Metabol 1998;83:1853–9.
[53] Bjorntorp P. Do stress reactions cause abdominal obesity and comorbidities? ObesRev 2001;2:73–86.
[54] Pasco JA, Nicholson GC, Williams LJ, Jacka FN, Henry MJ, Kotowicz MA, et al.Association of high-sensitivity C-reactive protein with de novo major depression.Br J Psychiatry 2010;197:372–7.
[55] Milaneschi Y, Corsi AM, Penninx BW, Bandinelli S, Guralnik JM, Ferrucci L.Interleukin-1 receptor antagonist and incident depressive symptoms over 6 yearsin older persons: the InCHIANTI study. Biol Psychiatry 2009;65:973–8.
[56] Hamer M, Batty GD, Marmot MG, Singh-Manoux A, Kivimaki M. Anti-depressantmedication use and C-reactive protein: results from two population-based studies.Brain Behav Immun 2011;25:168–73.
[57] Almeida OP, Calver J, Jamrozik K, Hankey GJ, Flicker L. Obesity and metabolicsyndrome increase the risk of incident depression in older men: the health in menstudy. Am J Geriatr Psychiatry 2009;17:889–98.
[58] Chaput JP, Drapeau V, Hetherington M, Lemieux S, Provencher V, Tremblay A.Psychobiological effects observed in obese men experiencing body weight lossplateau. Depress Anxiety 2007;24:518–21.
[59] Butnoriene J, Bunevicius A, Norkus A, Bunevicius R. Depression but not anxiety isassociated with metabolic syndrome in primary care based community sample.Psychoneuroendocrinology 2014;40:269–76.
[60] Grillo CA, Mulder P, Macht VA, Kaigler KF, Wilson SP, Wilson MA, et al. Dietaryrestriction reverses obesity-induced anhedonia. Physiol Behav 2014;128:126–32.