practical guide to diagnosis and treatment of neuropathic pain ...

ORIGINAL RESEARCH
The impact of neuropathic pain on relationships
S. Jose Closs, Victoria Staples, Innes Reid, Michael I. Bennett & Michelle Briggs
Accepted for publication 10 October 2008
Correspondence to S.J. Closs:
e-mail: [email protected]
S. Jose Closs BSc PhD RN
Professor
Nursing Research, School of Healthcare,
University of Leeds, UK
V. Staples BSc MSc DHealth Psych
Senior Lecturer
Health Psychology, School of Social Sciences,
University of Derby, UK
I. Reid BSc MA RN
Critical Care Outreach Charge Nurse
Theatres, Anaesthetics and Critical Care,
Leeds Teaching Hospitals NHS Trust, UK
M.I. Bennett MBChB MD FRCP
Professor
Palliative Medicine, International
Observatory on End of Life Care, Institute for
Health Research, University of Lancaster, UK
M. Briggs MSc PhD RN
Senior Research Fellow
School of Healthcare, University of Leeds,
UK
CLOSS S.J . , STAPLES V. , REID I . , BENNETT M.I . & BRIGGS M. (2009)CLOSS S.J . , STAPLES V. , REID I . , BENNETT M.I . & BRIGGS M. (2009) The
impact of neuropathic pain on relationships. Journal of Advanced Nursing 65(2),
402–411
doi: 10.1111/j.1365-2648.2008.04892.x
AbstractTitle. The impact of neuropathic pain on relationships.
Aim. This paper is a report of a study exploring the impact of neuropathic pain on
family, social and working relationships among patients at a pain clinic serving a
large urban area.
Background. Neuropathic pain is a particularly distressing type of chronic pain
which is extremely difficult to manage successfully. It produces a range of
unpleasant symptoms and adversely affects patients’ quality of life, but little is
known about its personal impact.
Method. A descriptive and exploratory approach was used and 10 participants
participated in three focus groups in 2005. Because of the low response rate of 20%
from the initial sample, a second sample of 16 patients was invited to participate.
However, only one person responded and therefore it was not possible to convene
an additional group.
Findings. The unpleasant and bizarre nature of neuropathic pain underpinned much
of its impact in terms of respondents’ difficulties in maintaining a range of rela-
tionships. For closer relationships, key difficulties centred on the reduction in quality
and/or number of personal relationships. For more distant relationships and those
with professionals, frustration at the invisibility of their pain and their own failure
to communicate symptoms and its consequences were central.
Conclusion. More extensive work is needed to improve our understanding of how
neuropathic pain is experienced, how it affects close and more distant kinds of
relationships, and how healthcare professionals might best support people with
persistent neuropathic pain to maintain personal and social relationships, and to
communicate their pain effectively.
Keywords: communication, focus group, neuropathic pain, nursing, pain impact,
quality of life, relationships
Introduction
The impact of chronic pain on daily life is extensive, but most
research in this field has not differentiated between those who
have chronic nociceptive pain (in response to injury or
pathology) only and those who suffer from neuropathic pain
symptoms due to abnormal nerve function. The International
Association for the Study of Pain (IASP) defines neuropathic
402 � 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd
J A N JOURNAL OF ADVANCED NURSING

pain as ‘Pain initiated or caused by a primary lesion or
dysfunction in the nervous system… Peripheral neuropathic
pain occurs when the lesion or dysfunction affects the
peripheral nervous system. Pain initiated or caused by a
primary lesion or dysfunction in the nervous system…Peripheral neuropathic pain occurs when the lesion or
dysfunction affects the peripheral nervous system. Central
pain may be retained as the term when the lesion or
dysfunction affects the central nervous system.’ (IASP
2008). Persistent neuropathic pain is not uncommon, its
symptoms are frequently bizarre and distressing, and it is
notoriously refractory to treatment.
Most treatment is pharmacological, and little is known
about patients’ experiences of symptoms and how they affect
daily life. Improving our understanding of these issues might
provide a platform from which more effective interventions
and support could be developed and tested.
Background
Symptoms and prevalence of neuropathic pain
Chronic neuropathic pain has a wide range of unpleasant
symptoms, many of which are strange and unpredictable.
Neuropathic pain is typically reported as burning,
shooting, stabbing, random, sudden, or electrical. It is
associated with sensory changes such as dysaesthesias
(abnormal pain perception) or paraesthesias (abnormal
perception of a non-painful nature) and abnormal sensory
perception, such as allodynia or hyperalgesia (eg Mortimer
et al. 2002).
A recent survey of the general population in the United
Kingdom (UK) showed that of over 3000 patients, 48% had
chronic pain, of whom 8% had pain of predominantly
neuropathic origin. Those in the latter group suffered higher
pain intensity and higher levels of expressed need (Torrance
et al. 2006). Neuropathic pain is thought to be a particularly
distressing pain condition and is associated with a high
degree of suffering, not only because of the intensity of the
pain but also the long duration of the condition, as the pain
does not generally decline over time (Karlsten & Gordh
1997). Some elements of neuropathic pain are described as
constant, but it is more common for patients to describe
intermittent symptoms.
Impact of neuropathic pain symptoms on relationships
A large body of literature exists on the impact of chronic
pain in general on daily life (Gureje et al. 1998, Niv &
Kreitler 2001, Katz 2002). It can disrupt work, family and
social functioning and can lead to depression and with-
drawal from social activities (Breivik et al. 2006). Many
researchers who have explored the experience of living
with chronic pain have not differentiated between those
with predominantly nociceptive pain and those where
neuropathic symptoms dominated the experience (e.g.
Johansson et al. 1999).
Surveys of people with neuropathic pain suggest that the
majority experience severe discomfort which interferes with
general activity, work, sleep, mood and enjoyment of life (eg
Meyer-Rosberg et al. 2001, McDermott et al. 2006, Smith
et al. 2007). These people showed poorer physical and social
functioning and mental health than the general population.
The most bothersome symptoms were generally difficulty in
sleeping, lack of energy, difficulty in concentrating and
drowsiness, all of which might interfere with the ability to
integrate socially.
The expression of negative emotions such as frustration,
irritability and anger has been described in relation to the
impact on interpersonal relationships and increases the level
of stress within families (Henwood & Ellis 2004). Neuro-
pathic pain syndromes can affect job performance, work
absenteeism, reduced productivity and ultimately the ability
to maintain a work role, without which it is difficult to
maintain an ordinary life pattern (Liedberg & Henriksson
2002).
It is clear that chronic neuropathic pain can produce
many and various negative changes in sufferers. While the
broader population of those with chronic pain has received
some consideration, the more specific population of people
whose chronic pain has a neuropathic element has received
far less attention. The specific needs of such patients in
terms of psychological and social support are not known in
any detail.
The study
Aim
The aim of this sub-section of a wider study (Closs et al.
2007) reported in this paper was to explore the impact of
neuropathic pain on family, social and working relationships
among a sample of patients from a Pain Clinic serving a large
urban area.
Methodology
A descriptive and exploratory approach was used since the
purpose was to focus on the largely unexplored experience
and reported impact of neuropathic pain symptoms. Focus
JAN: ORIGINAL RESEARCH Neuropathic pain and relationships
� 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd 403

groups were selected as the method for generating data,
because these are particularly useful in identifying both
diverse individual accounts and shared experiences (Dawson
et al. 1993). Discussion with others may facilitate more
in-depth and meaningful discussions than one-to-one inter-
views with only a researcher present.
Since we anticipated that participants might be willing to
discuss intimate or embarrassing issues, the size of focus
groups was kept smaller than normal (typical groups include
5–12 participants). Generally the more sensitive the
topic under discussion, the smaller the group needs to be
(Goodman & Evans 2006, p. 357).
Participants
Participants for the focus groups were recruited from an
existing database of patients with chronic neuropathic pain.
They had previously been screened with the Leeds Assess-
ment of Neuropathic Symptoms and Signs (LANSS) pain
scale (Bennett 2001). We had no direct access to the database,
and patients were initially contacted on our behalf by a
specialist nurse. Exact diagnoses were unavailable due to
adherence to the Data Protection Act. Data collection took
place over six months in 2005.
Of the 99 patients on the database, 49 lived locally and
were considered by the specialist nurse to be well enough to
be approached. They were sent an information sheet
explaining the study, a consent form, contact details and a
reply-paid envelope. Ten participants took part in three focus
groups. The first comprised two men and two women; the
second two men and one woman; and the third three women.
Ages ranged from 24–60 years.
Due to the low response rate of 20% from the initial
sample, a second sample of 16 patients was identified from a
town further afield and invited to participate. Only one
person responded and therefore it was not possible to
convene an additional group.
Data collection
A comprehensive review of the current literature on
the impact of persistent neuropathic pain was undertaken as
a basis for developing the focus group schedule. One
hundred and ninety-seven abstracts were identified from
the initial search, in 22 of which a qualitative method
was used. The focus group schedule was developed to
facilitate discussion around the main domains related to
the impact of living with neuropathic pain symptoms,
as identified in the literature. We identified eight
such topics, of which three - impact on family life, impact
on social life and impact on working life - are explored
here.
The focus groups were undertaken at a locality convenient
for participants and audio-taped with their consent. Each
discussion lasted for 1–1Æ5 hours. The three questions posed
relevant to this paper were: ‘Thinking now about these
symptoms, what influence do you feel they have on your
family life’; ‘Do these symptoms influence your social life in
the same ways they influence family life, or do they have a
different influence on your social life?’ and ‘Do or did these
symptoms have any influence on your working life and if so,
in what ways?’. Between two and six prompts were planned
for each section. VS acted as moderator and IR as facilitator.
Ethical considerations
The study was approved by the appropriate ethics committee.
Participants were informed about the study and gave consent
as described above. At the start of each focus group all
participants agreed that the content of the discussion would
remain confidential among themselves.
Data analysis and validity
The audio-taped discussions were transcribed verbatim and
organised using QSR NVIVO version 2 (QSR NVIVO
International Pty Ltd, Victoria, Australia). Data were analy-
sed using the straightforward approach of qualitative descrip-
tion. This method was selected because it allows researchers
to stay close to the data, which were from a smaller than
anticipated sample. It is less interpretive than approaches such
as grounded theory and phenomenology, not requiring
‘conceptual or other highly abstract renderings of data’
(Sandelowski 2000, p. 335). This analysis was undertaken
by the focus group moderator VS) and independently by
another researcher (IR). Open coding was used within and
across the groups to identify common or contrasting themes,
which were then labelled and assigned codes.
Agreement was high between the two sets of codes and
categories derived. The few disagreements were resolved
through discussion between the two coders and, where these
were unresolved, consensus was sought through discussion
with the wider research team. An overall thematic framework
was developed and then reviewed by two independent pain
nurse specialists with experience of working with patients’
with neuropathic pain to establish its face validity.
The findings are presented as descriptive summaries and
interpretations of key emergent themes, illustrated by data
extracts from the transcripts. Quotes have been anonymised
to maintain participant confidentiality. Each quote is
S.J. Closs et al.
404 � 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd

identified only by the focus group number, participant
number and gender, e.g. FG1, P2, female.
Results
In each of the groups, participants developed considerable
rapport with one another, which appeared to have two
effects. First, it allowed them to feel that they were not alone
and that they ‘were not going mad’ trying to cope with their
distressing symptoms on their own. Second, by disclosing
personal information, they encouraged one another to discuss
topics that they had felt unable to divulge in any forum
previously. Once one person had been brave enough to reveal
sensitive information, others felt that they had ‘permission’ to
do the same. All took a full part in their focus groups.
The discussions produced wide-ranging content, including
data on the nature of the pain experienced and how
participants managed this (Closs et al. 2007). The key
aspects of the pain experience were its very unpleasant and
unpredictable nature, together with the difficulty of describ-
ing its often bizarre characteristics to other people (Closs
et al. 2006). It appeared that the relentless unpleasantness of
neuropathic pain had a profound effect on all kinds of
relationship.
Participants described some of the difficulties they had
experienced with intimate relationships and the strains placed
on relationships within their families. They also described
difficulties in maintaining, and the loss of, relationships with
friends, as well as frustration in their dealings with uncom-
prehending healthcare professionals, disability services, ben-
efits agencies and employment services, which was common.
Impact of pain on spouses/partners
Several participants reported that the relationships that they
were in when they developed neuropathic pain had broken
down because of the impact of living with the pain and their
symptoms:
I and my husband split up and we’d been married 36 years. We split
up because my husband couldn’t stand it any more. [FG1, P2, female]
Those who were still in their relationships or who had
established new ones had difficulties related to physical
intimacy:
You know, if you’re just sort of laid in bed and he puts his hand on
my hip to give me a cuddle or anything I say, ‘Don’t touch me’
because it’s just, it’s just I can’t even put my own hand there. I
certainly don’t want anybody else’s big hand on me as it were…
‘Don’t touch me, but you’ve still got to love me’ [laugh] – strange
isn’t it?... And half of the time you’re in so much pain you can’t be
bothered anyway [FG3, P1, female]
Others described how new relationships had failed because of
the impact of the pain, and for some patients it was
impossible to establish new relationships, again because of
the impact of living with neuropathic pain:
When this pain comes bad it has spoilt, spoilt relationships because
it’s really hard for somebody to understand how it debilitates, how
you become miserable. [FG2, P1, female]
Impact on relationships with family
For the men, the loss of physical capacity was particularly
difficult to accept. They felt unable to perform traditional
male tasks and fulfil their roles as sons, partners and fathers.
These included heavier household chores such as gardening,
being able to protect their loved ones and being able to
perform sexually:
Yes, it’s a man thing - you’ve lost all that what men stand for, if you
know what I mean/If my daughter gets in to trouble, I’m not in a
position now to go and sort it out. [FG1, P3, male]
Men found it particularly difficult to accept help from people
whom they felt they should be supporting:
My parents have been there for me all my life and they’re at an age
now where they should be able to take it easy and rely on their son
occasionally to help them out with stuff, and I can’t do it for them…
You feel guilty. [FG1, P3, male]
Women also described their inability to perform their usual
roles and participate in normal family activities. The impact
on children was particularly noted:
I’m a single mum. It affected them [the children] because who wants
to come home with your mum tucked up in bed not well? [FG2, P1,
female]
Participants recognised their negative emotions and behav-
iour, expressed concern that they might react physically
aggressively and worried that family members would not
tolerate their behaviour indefinitely:
I do flare up, do get so frustrated. I don’t throw things, but I do bang
things. If you understand me, the table like that… I’ve never been
physically violent, thank goodness, but you never know how long
they’re going to stand it - so you’re living in the fear. [FG1, P4, male]
Impact on relationships with friends
Participants described how their friends found it difficult to
‘see’ the problems they were experiencing:
JAN: ORIGINAL RESEARCH Neuropathic pain and relationships
� 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd 405

You find that people don’t believe you a lot of the time. They can’t
see it, so they don’t think there’s anything the matter with you. [FG1,
P3, male]
Despite the loss of a many relationships, participants reported
receiving a great deal of support from their families and
friends, even though they felt that most people did not
understand what they were going through.
The nature of the disability resulting from neuropathic pain
is further complicated by the invisibility of pain. The com-
plexity of the sensory impairments and bizarre feelings added
to lack of understanding of what it took to live their lives.
Having to ask for assistance was particularly frustrating:
And when I’ve got to go shopping, I got to have someone to help me
lift, I’ve got to ask … to have someone to lift, and they look at you as
if to say, ‘Are you kidding me’... I just need the help there and then
and it gets so frustrating. [FG1, P1, female]
Everyone in the focus groups reported that their social lives
had been affected to some extent by the pain. This was often
seen as the starting point for the loss of social relationships:
Yeah, because they ask you out and you’re in agony, and nine times
out of ten you have to turn round and say, ‘I’m sorry, I can’t make it.’
So in the end they think, ‘What’s the point?’ [FG1, P3, male]
Preoccupied with their own experiences, participants
reported not having the emotional energy to deal with other
people’s concerns, and expressed how they had become
resentful towards others who relied on them. Paradoxically,
they were also able to identify positive changes within
themselves and described how they had become more patient
with others, more tolerant and less concerned about issues
that would previously have been a cause for worry:
I’ve got a bit more patience where people are concerned. I listen more
intently … and therefore I’ve got more patience with people. [FG1,
P1, female]
Impact of pain on relationships with professionals
Most participants were unable to work, and so focused on
their dealings with healthcare professionals and staff in
statutory agencies. Lack of understanding by these profes-
sionals, together with not being believed, was a major
problem for many:
It’s just people’s [doctors’] off the cuff ‘Just get on with it’… You
wouldn’t say that if I came in and I had a bloody leg missing or
something … You wouldn’t react like that if I came in and I had
multiple sclerosis or if I had cancer. You don’t say to them, ‘Just
bloody get on with it’ and leave it... so put up with it, there’s no
choice. It isn’t that bloody easy - if it were that easy I’d do it, I’d grit
my teeth and I’d bloody get on with it. [FG2, P3, male]
This lack of professional understanding had negative
practical consequences for some. There was a perceived lack
of understanding from general practitioners (GPs) or family
physicians of the severity and consequences of pain. The
inability to communicate the nature of pain successfully to
these people might have led to a cut in social security benefits
for one participant:
He hasn’t got your medical records … then he writes a report and
sends it to the benefits people. And whether you get your benefits or
not is purely and simply on what that GP has said after ten minutes.
[FG1, P3, male]
Continual re-assessment by seemingly ill-informed staff at
disability services, benefits agencies and employment services
was described as very stressful. In one case this lack
of understanding was reported to produce inconsistency
between judgements by professionals’, who were then
perceived as untrustworthy:
I find that the different people you see, you get so many different
opinions. … you’re swapping about and for me, now, I got finished in
my job from Dr A in Derby [who] did a medical [for my job] and then
… they said, ‘You can’t work anymore.…. Then Dr B at Leeds did the
medical for my pension and said, ‘Oh you should go to work’. So I
lost my job and then I didn’t get my pension. So I ended up with
nothing, and all on the fact that two people in the same bloody jobs
got different opinions. [FG2, P3, male]
Any suggestion that the pain was psychological fed into
participants’ difficulties in understanding their experiences.
Some of the bizarre features of their neuropathic pain left
them questioning its reality and whether they were somehow
diminished in their capacity to cope with it. Not wanting to
be labelled as mentally ill was also expressed in relation to
any suggestion that their pain was psychological in nature:
They try and say there’s nothing, so I thought it must be psycho-
logical and that was the biggest insult for me. [FG2, P1, female]
Discussion
Study limitations
The findings of this exploratory study are limited by the
smaller than anticipated sample size, since we cannot be
certain that data saturation had been reached. Additional
work and more sophisticated analysis would therefore be
valuable, although our findings were supported by the
S.J. Closs et al.
406 � 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd

existing literature. It would be necessary to confirm or refute
the validity of these findings before considering how best to
intervene to help people with neuropathic pain.
Discussion of findings
Many of the issues identified by this sample of people with
neuropathic pain were similar to those in the wider popula-
tion of chronic pain sufferers (e.g. Breivik et al. 2006). Our
findings showed clearly that they had experienced many
distressing problems due to the impact of neuropathic pain on
all sorts of relationships, but they reported no formal access
to much-needed psychological or social support to help them
manage these problems (Closs et al. 2007).
Our findings mirror to a great extent those of Sofaer-
Bennett et al. (2007), who explored the social consequences
of neuropathic pain with older people. They found limita-
tions (related to physical constraints, reduced activities and
family contacts, sadness and loss) and social isolation
(waning friendships, strained personal and intimate relation-
ships). We found many similar themes, in that neuropathic
pain appeared to produce four key overlapping areas of
negative impact on participants’ relationships. These were
strained intimate relationships, loss of family roles, social
withdrawal and being believed/understood.
Loss of family roles
A common issue resulting from chronic neuropathic pain was
the inability to maintain roles in relation to family members,
and the breakdown of marriages and similar relationships
was common. This is an under-researched area for those with
neuropathic pain, although the role of spousal responses to
chronic pain has been studied in some detail. It has been
shown that both solicitous (engaged and caring) and punish-
ing responses from significant others can be negatively
associated with acceptance of chronic pain (McCracken
2005). Conversely, the notion of ‘carer burnout’ may apply to
spouses in this group, who may well have suffered physical
and mental strain as a result of providing long-term support.
It has been estimated that 20–50% of spouses of those with
chronic pain exhibit significant depressive symptoms
(Shwartz & Slater 1991).
Loss of feelings of masculinity or femininity was a central
aspect of the loss of traditional family roles, and was something
which participants had not felt able to discuss in other forums.
This has received little attention in the pain literature. Those
who were still in relationships with spouses or partners
described difficulties with physical intimacy, increasing levels
of dependency and not being able to reciprocate support.
The inability to maintain other roles in the family also
caused great distress. Fathers who were unable to protect
their daughters, sons who were unable to support their
elderly parents and mothers who could not play with their
children found this highly problematic. The inability to
participate in normal family activities was recognised as
having a major impact on children in particular, and
participants described how they often felt like a burden on
others, in keeping with the findings of Bakitas (2007). This
has also been shown to be an issue for older people with
neuropathic pain, who lose contact with their grandchildren,
as well as suffering strained personal relationships with
spouses and losing friendships (Sofaer-Bennett et al. 2007).
It appears that there may be scope for providing additional
support for people with neuropathic pain patients and their
families. Spouses may need as much help as sufferes to cope
with the physical and psychological demands of living with
such a distressing condition. It may be that participation in
pain management programmes would benefit them.
Social withdrawal
Solicitousness is conceptually related to social support, in
part referring to the provision of various kinds of assistance.
This may come from any number of people within the
relevant social network, including friends, neighbours and
work colleagues. Social networks are emerging as an impor-
tant factor in mitigating the interference of pain with daily
activities (Peat et al. 2004). For most people, any attempt to
maintain a normal life includes the maintenance of social
networks, but this becomes increasingly difficult with the
establishment of neuropathic pain symptoms.
Several participants in the study reported difficulties with
planning ahead because of the unpredictable nature of the
pain. They sought to identify possible triggers for their pain,
and expressed frustration at its unpredictability. This sup-
ports earlier work describing how people became despondent
at not being able to identify the cause of their problem, and
felt depressed by their failed attempts to relieve symptoms
over prolonged periods of time (Hunt & Bogg 2000).
Participants reported that family activities were often dis-
rupted because of their symptoms, but they also described
how they had become more spontaneous, engaging in family
activities as and when they felt able. Advance knowledge, in
terms of the environment or facilities, was identified as an
important aid in identifying suitable locations for activities,
but not in relation to daily fluctuations in the pain experience.
In some cases triggers were identified, such as physical,
emotional or environmental factors, including increased
activity, physical contact, stress and climatic change. Many
JAN: ORIGINAL RESEARCH Neuropathic pain and relationships
� 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd 407

of these occurred in social situations, potentially making
patients choose to avoid socialising.
Being believed/understood
The invisibility of the pain increased the need for sufferers to
be able to demonstrate its presence verbally. The negative
impact of the failure to communicate clearly and successfully
about pain occurred in relationships with family and
friends as well as with government agencies and healthcare
professionals.
Unfortunately, the diverse and peculiar symptoms of
neuropathic pain are difficult to understand and describe,
even for those with an excellent vocabulary and verbal
skills. Metaphors were often used by participants (eg like a
balloon that’s under half pressure) and this has been
observed previously (Schaefer 1995, Soderberg & Norberg
1995).
Frustration was expressed at the inability of healthcare
professionals, particularly GPs and family physicians, to
understand the pain. This had the potential to result in poor
diagnosis and treatment. Loeser (1991) proposed that a key
difficulty for physicians is the differentiation between impair-
ment and disability. If impairment is defined as any loss or
abnormality of psychological, physiological or anatomic
structure or function, and disability is defined as any
restriction or lack (resulting from impairment) of ability to
perform an activity in the manner or within the range
considered normal for a human being, the problem becomes
clearer.
A person with chronic neuropathic pain may have no
discernable impairment underlying their disability due to the
pain and, while doctors are trained to identify impairment,
for the most part it is only specialists in rehabilitation who
have adequate understanding of disability. It has been
suggested that when a chronic pain sufferer is asked to
NEGATIVE IMPACTS OF
NEUROPATHIC PAIN:
Type of relationship
ProfessionalsFriendsFamilySpouse/partner
Intimate relationships
unsustainable due to
pain
Failure of existing
marriage or partnership
Failure to establish new
relationships
Loss of family roles (reduced
ability to act as father, mother,
son etc)
guilt
Feelings of inadequacy and
Frustration and fear of
expressing anger to family
members
Withdrawal from social
activities
Frustration at invisibility of
symptoms and inability of
friends to understand
Inability to plan activities due
to unpredictability of pain
Change in attitude to friends
(more tolerant/resentful)
Frustration at doctors’ apparent
lack of understanding of their
situation
Loss of trust where no
consistency between doctors’
judgements
Frustration at dealing with
statutory agencies (benefits etc)
who did not understand/believe
them
Fear of being labelled mentally ill
Figure 1 The impact of neuropathic pain on relationships.
S.J. Closs et al.
408 � 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd

demonstrate their physical capacity, it is not an objective
diagnostic procedure which ensues, but ‘an interesting social
interaction, based on the beliefs, knowledge, affect and
physical characteristics of the patient’ (Loeser 1991, p218). It
is hardly surprising, then, that different doctors may come to
different conclusions about the same patient. Benefits agen-
cies may have no choice but to rely on the diagnoses of GPs
who lack expert knowledge. The ramifications of this go
beyond treatment to the employment and economic aspects
of sufferers’ lives. The extent of GPs’ need for information is
unknown, they need to have the appropriate knowledge if
patients are to get the support they need.
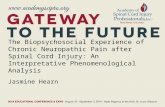
Two key negative impacts on relationships
Although our participants varied in terms of condition and
demographic factors, some commonalities did emerge.
Figure 1 summarises the reported impact of neuropathic
pain on the range of relationships. If relationships are
considered as a continuum, ranging from the closest to the
most distant, two key factors may be considered to have had
graduated impacts, starting at opposite ends of this contin-
uum (Figure 2).
At the more intimate end of the relationship spectrum,
profound reductions in the quality of relationships with
partners and families were seen, together with a reduction in
the number of personal relationships which participants
could sustain. At the opposite end, where relationships were
more formal, the main negative impact appeared to be
frustration at failure to communicate the nature of their
condition successfully. This did not appear to be a major
difficulty within intimate relationships, although the fear of
expressing anger due to frustration was a concern. Difficulty
in communicating pain symptoms produced varying degrees
of social withdrawal from friendships and was a major
problem when dealing with healthcare professionals and staff
at statutory agencies. The consequences in terms of being
misunderstood by the latter were profound in terms of the
potential for losing employment and other benefits which
might otherwise have supported them in maintaining the
normal aspects of their lives.
Conclusion
Neuropathic pain was reported to produce negative impacts
on a range of relationships, in terms of loss of family roles,
social withdrawal and frustration about being understood
and believed by family, friends and professionals. Many of
these issues are not new in the US and European pain
literature and suggest that little progress has been made in
supporting those with disabling chronic pain to maintain as
normal a life as possible.
However, it may be that focusing on two key areas of
concern to these patients, that is preventing relationship
breakdown or loss, and effectively communicating about
neuropathic pain, would have the greatest potential for
Continuum of ‘closeness’ of relationships:
Spouse/partner Family Friends Professionals
2. Frustration at invisibility of
pain and failure to communicate
symptoms – and the
consequences
1. Reduction in quality
and/or number of
personal relationships
Figure 2 Two key areas of negative impact
on the continuum of relationships. The
graduated shading in the triangular areas
indicates the suggested strength of the two
types of negative impacts on different types
of relationship; the darker the shading, the
greater the impact.
JAN: ORIGINAL RESEARCH Neuropathic pain and relationships
� 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd 409

improving their quality of life. These issues would need to
be pursued in a range of international settings since family
and social relationships, as well as attitudes and beliefs
about pain, vary considerably according to ethnicity and
faith. Furthermore, culturally-acceptable ways of expressing
pain also vary a great deal, and so the mode and
significance of pain communications require exploration
in different contexts. Different kinds of support are likely
to be needed in different cultures. Use of cognitive
behavioural therapies with patients and/or spouses and
perhaps other family members might help to rebuild
damaged relationships and help to normalise family func-
tioning. Neuropathic pain sufferers could be trained to
manage interactions with family, friends and professionals
who appear not to understand or believe their symptoms.
This might involve developing their communication skills
and/or support in adjusting more positively to the notion
that they may not be understood.
Larger studies are needed to explore in more depth the
personal and interpersonal impacts of neuropathic pain on
different types of relationship.
Acknowledgements
We would like to thank the British Pain Society and Pfizer,
who funded this research; all the participants who gave their
valuable time to participate in the focus groups; Helen
Radford and the medical and nursing staff who supported the
study; members of the advisory group for their help
throughout the project, in particular Helen Poole and Kath
Marczewski; and we would like to thank Ruth Allcroft for
her support with administration.
Funding
This research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
Author contributions
SJC, MIB & MB were responsible for the study conception
and design. VS & IR performed the data collection. SJC, VS
& IR performed the data analysis. SJC was responsible for
the drafting of the manuscript. SJC, VS, IR, MIB & MB made
critical revisions to the paper for important intellectual
content. SJC, MIB & MB obtained funding. SJC, MIB & MB
supervised the study.
References
Bakitas M.A. (2007) Background noise. The experience of chemo-
therapy-induced peripheral neuropathy. Nursing Research 56(5),
323–331.
What is already known about this topic
• Persistent neuropathic pain is not uncommon and its
symptoms are frequently bizarre and distressing and its
unpredictability presents unique challenges which dif-
ferentiate it from other types of chronic pain.
• Persistent neuropathic pain is not widely understood
by health care professionals and is notoriously refrac-
tory to treatment.
• Surveys of people with neuropathic pain suggest that
the majority experience severe discomfort which
interferes with general activity, work, sleep, mood and
enjoyment of life.
What this paper adds
• Participants reported many distressing problems
related to the impact of neuropathic pain, including its
negative impacts on relationships with the spouse/
partner and wider family and loss of ability to main-
tain established roles, leading to feelings of inade-
quacy, guilt, frustration and fear of expressing anger.
• The pain and its unpredictability interfered with the
ability to maintain existing social contacts and pre-
vented the development of new ones, thereby increas-
ing social isolation.
• A major problem was the invisibility of pain and the
problem of communicating it successfully to friends
and professionals, leading to misunderstanding linked
to fear of being labelled mentally ill.
Implications for practice and/or policy
• Focusing on two key areas of concern to these patients,
that is preventing relationship breakdown or loss, and
effectively communicating about neuropathic pain,
might have the greatest potential for improving their
quality of life.
• Use of cognitive behavioural therapies with patients
and/or spouses and perhaps other family members
might help to rebuild damaged relationships and help
to normalise family functioning.
• Neuropathic pain sufferers could be trained to manage
interactions with family, friends and professionals who
appear not to understand or believe their symptoms.
S.J. Closs et al.
410 � 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd

Bennett M. (2001) The LANSS Pain Scale: the Leeds assessment of
neuropathic symptoms and signs. Pain 92(1–2), 147–157.
Breivik H., Collett B., Ventafridda V., Cohen R. & Gallacher D.
(2006) Survey of chronic pain in Europe: prevalence, impact on
daily life and treatment. European Journal of Pain 10(4), 287–333.
Closs S.J., Staples V., Reid I., Bennett M.I. & Briggs M. (2006) An
exploratory study of patients’ accounts of managing the symptoms
of neuropathic pain. Presentation at the 9th International confer-
ence: Mechanisms and treatment of neuropathic pain, Bermuda.
Closs S.J., Staples V., Reid I., Bennett M.I. & Briggs M. (2007)
Managing the symptoms of neuropathic pain: an exploration of
patients’ experiences. Journal of Pain and Symptom Management
34(4), 422–433.
Dawson S., Manderson L. & Tallo V.L. (1993) A Manual for the Use
of Focus Groups. International nutrition foundation for developing
countries, Boston, MA.
Goodman C. & Evans C. (2006) Chapter 23: Using Focus Groups. In
The Research Process in Nursing, 5th edn (Gerrish K. & Lacey A.,
eds), Blackwell Publishing, Oxford, pp. 353–366.
Gureje O., von Korff M., Simon G.E. & Gater R. (1998) Persistent
pain and well being: a World Health Organisation study in primary
care. Journal of the American Medical Association 280, 147–151.
Henwood P. & Ellis J.A. (2004) Chronic neuropathic pain in spinal
cord injury: the patient’s perspective. Pain Research Management
9(1), 34–49.
Hunt J. & Bogg J. (2000) An evaluation of the impact of a fibrom-
yalgia self-management programme on patient morbidity and
coping. Advances in Physiotherapy 2, 168–175.
International Association for the Study of Pain (2008) IASP
Pain Terminology. Retrieved from http://www.iasp-pain.org/AM/
Template.cfm?Section=Pain_Definitions&Template=/CM/HTML-
Display.cfm&ContentID=1728#Neuropathic on 30 September
2008.
Johansson E.E., Hamberg K., Westman G. & Lindgren G. (1999)
The meanings of pain: an exploration of women’s descriptions of
symptoms. Social Science & Medicine 48, 1791–1802.
Karlsten R. & Gordh T. (1997) How do drugs relieve neurogenic
pain? Drugs and Aging 11, 398–412.
Katz N. (2002) The impact of pain management on quality of life.
Journal of Pain and Symptom Management 24(1), S38–S47.
Liedberg G. & Henriksson C. (2002) Factors of importance for work
disability in women with fibromyalgia: an interview study.
Arthritis and Rheumatism (Arthritis Care and Research) 47(3),
266–274.
Loeser J.D. (1991) What is chronic pain? Theoretical Medicine 12,
213–225.
McCracken L. (2005) Social context and acceptance of chronic
pain: the role of solicitous and punishing responses. Pain 113,
155–159.
McDermott A.M., Toelle T.R., Rowbotham D.J., Schaefer C.P. &
Dukes E.M. (2006) The burden of neuropathic pain: results from a
cross-sectional survey. European Journal of Pain 10, 127–135.
Meyer-Rosberg K., Kvarnstrom A., Kinnman E., Gordh T., Nordfors
L. & Kristofferson A. (2001) Peripheral neuropathic pain – a
multidimensional burden for patients. European Journal of Pain 5,
379–389.
Mortimer C.M., Steedman W.M., McMillan I.R., Martin D.J. &
Ravey J. (2002) Patient information on phantom limb pain: a focus
group study of patient experiences, perceptions and opinions.
Health Education Research 17(3), 291–304.
Niv D. & Kreitler S. (2001) Pain and quality of life. Pain Practice
1(2), 150–161.
Peat G., Thomas E., Handy J. & Croft P. (2004) Social networks and
pain interference with daily activities in middle and old age. Pain
112, 397–405.
Sandelowski M. (2000) Focus on Research Methods. Whatever
happened to qualitative description? Research in Nursing and
Health 23, 334–340.
Schaefer K.M. (1995) Struggling to maintain balance: a study of
women living with fibromyalgia. Journal of Advanced Nursing 21,
95–102.
Shwartz L. & Slater M.A. (1991) The impact of chronic pain on the
spouse: research and clinical implications. Holistic Nursing Prac-
tice 6, 9–16.
Smith B.H., Torrance N., Bennett M.I. & Lee A.J. (2007) Health and
quality of life associated with chronic pain of predominantly
neuropathic origin in the community. Clinical Journal of Pain
23(2), 143–149.
Soderberg S. & Norberg A. (1995) Metaphorical pain language
among fibromyalgia patients. Scandinavian Journal of Caring
Sciences 9, 55–59.
Sofaer-Bennett B., Walker J., Moore A., Lamberty J., Thorp T. &
O’Dwyer J. (2007) The social consequences for older people of
neuropathic pain: a qualitative study. Pain Medicine 8(3), 263–270.
Torrance N., Smith B.H., Bennett M.I. & Lee A.J. (2006) The
epidemiology of chronic pain of predominantly neuropathic origin.
Results from a general population survey. Journal of Pain 7(4),
281–289.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the
advancement of evidence-based nursing, midwifery and health care by disseminating high quality research and
scholarship of contemporary relevance and with potential to advance knowledge for practice, education, management
or policy. JAN publishes research reviews, original research reports and methodological and theoretical papers.
For further information, please visit the journal web-site: http://www.journalofadvancednursing.com
JAN: ORIGINAL RESEARCH Neuropathic pain and relationships
� 2009 The Authors. Journal compilation � 2009 Blackwell Publishing Ltd 411
Copyright © 2022 FDOKUMEN