Gene Therapy for Chronic Neuropathic Pain: How Does It Work and Where Do We Stand Today
15
Review Article Gene Therapy for Chronic Neuropathic Pain: How Does It Work and Where Do We Stand Today?Sanjeev Kumar, MD,* Rupam Ruchi, MD, † Stephen R. James, MD,* ‡ and Elie J. Chidiac, MD* Departments of *Anesthesiology, † Internal Medicine, and ‡ Pain Medicine, Wayne State University/Detroit Medical Center, Detroit, Michigan, USA Reprint requests to: Sanjeev Kumar, MD, Department of Anesthesiology, Wayne State University/Detroit Medical Center, Harper University Hospital, 3990 John R., Box 162, Detroit, MI 48201, USA. Tel: 313-745-7233; Fax: 313-993-3889; E-mail: [email protected]. Disclosure: The authors have not received any financial support or grant of any kind for this review, nor have any financial relationships with any entities or organizations that have been named in this article. Abstract Objectives. Chronic neuropathic pain has been an enigma to physicians and researchers for decades. A better understanding of its pathophysiology has given us more insight into its various mechanisms and possible treatment options. We now have an understanding of the role of various ionic channels, biologically active molecules involved in pain, and also the intricate pain pathways where possible interventions might lead to substantial pain relief. The recent research on laboratory animals using virus-based vectors for gene transfer at targeted sites is very promising and may lead to additional human clinical trials. However, one needs to be aware that this “novel” approach is still in its infancy and that many of its details need to be further elu- cidated. The purpose of this article is to thoroughly review the current available literature and analyze the deficiencies in our current knowledge. Design. Literature review. Methods. After an extensive online literature search, a total of 133 articles were selected to syn- thesize a comprehensive review about chronic neuropathic pain and gene therapy in order to understand the concepts and mechanisms. Results. Most of the studies have shown benefits of gene therapy in animal models, and recently, phase 1 human trials using herpes simplex virus vector have started for intractable cancer pain. Conclusion. Although animal data have shown safety and efficacy, and initial human trials have been promising, additional studies in humans are required to more completely understand the actual benefits and risks of using gene therapy for the treatment of chronic neuropathic pain. Key Words. Chronic Neuropathic Pain; Gene Therapy Introduction The International Association for the Study of Pain (IASP) has defined neuropathic pain as “pain initiated or caused by a primary lesion or dysfunction in the nervous system” [1]. Recently, a task force in collaboration with the IASP Special Interest Group on Neuropathic Pain has proposed to replace the current definition of neuropathic pain by the following wording: “Pain arising as a direct consequence of a lesion or disease affecting the somatosensory system.” A grading system of certainty for presence of neuropathic pain has also been proposed according to which pain can be graded as being definite, probable, or possible neuropathic pain depending on four criteria based on clinical symptoms and signs [2]. Neuropathic pain is a fairly common condition with an estimated prevalence of 1.5% in the general population [3]. However, precise estimation of its incidence and prevalence is extremely difficult because of the lack of a standard definition and cutoff for diagnosis [4,5]. Recent studies have found the prevalence of pain of predomi- nantly neuropathic origin to be as high as 8.2% in the general population [6]. It is a cause of significant disability, decreases productivity and quality of life, and increases the cost of health care by approximately threefold [7]. Current pharmacological and interventional modalities available for the treatment of chronic neuropathic pain have variable efficacy. In addition, other problems with current therapy include intolerable adverse effects. Pain Medicine 2011; 12: 808–822 Wiley Periodicals, Inc. 808
Transcript of Gene Therapy for Chronic Neuropathic Pain: How Does It Work and Where Do We Stand Today

Review ArticleGene Therapy for Chronic Neuropathic Pain:How Does It Work and Where Do WeStand Today?pme_1120 808..822
Sanjeev Kumar, MD,* Rupam Ruchi, MD,†Stephen R. James, MD,*‡ and Elie J. Chidiac, MD*
Departments of *Anesthesiology,
†Internal Medicine, and
‡Pain Medicine, Wayne State University/DetroitMedical Center, Detroit, Michigan, USA
Reprint requests to: Sanjeev Kumar, MD, Departmentof Anesthesiology, Wayne State University/DetroitMedical Center, Harper University Hospital, 3990 JohnR., Box 162, Detroit, MI 48201, USA. Tel:313-745-7233; Fax: 313-993-3889; E-mail:[email protected].
Disclosure: The authors have not received anyfinancial support or grant of any kind for this review,nor have any financial relationships with any entitiesor organizations that have been named in this article.
Abstract
Objectives. Chronic neuropathic pain has been anenigma to physicians and researchers for decades.A better understanding of its pathophysiology hasgiven us more insight into its various mechanismsand possible treatment options. We now have anunderstanding of the role of various ionic channels,biologically active molecules involved in pain, andalso the intricate pain pathways where possibleinterventions might lead to substantial pain relief.The recent research on laboratory animals usingvirus-based vectors for gene transfer at targetedsites is very promising and may lead to additionalhuman clinical trials. However, one needs to beaware that this “novel” approach is still in its infancyand that many of its details need to be further elu-cidated. The purpose of this article is to thoroughlyreview the current available literature and analyzethe deficiencies in our current knowledge.
Design. Literature review.
Methods. After an extensive online literaturesearch, a total of 133 articles were selected to syn-
thesize a comprehensive review about chronicneuropathic pain and gene therapy in order tounderstand the concepts and mechanisms.
Results. Most of the studies have shown benefits ofgene therapy in animal models, and recently, phase1 human trials using herpes simplex virus vectorhave started for intractable cancer pain.
Conclusion. Although animal data have shownsafety and efficacy, and initial human trials havebeen promising, additional studies in humans arerequired to more completely understand the actualbenefits and risks of using gene therapy for thetreatment of chronic neuropathic pain.
Key Words. Chronic Neuropathic Pain; GeneTherapy
Introduction
The International Association for the Study of Pain (IASP)has defined neuropathic pain as “pain initiated or causedby a primary lesion or dysfunction in the nervous system”[1]. Recently, a task force in collaboration with the IASPSpecial Interest Group on Neuropathic Pain has proposedto replace the current definition of neuropathic pain by thefollowing wording: “Pain arising as a direct consequenceof a lesion or disease affecting the somatosensorysystem.” A grading system of certainty for presence ofneuropathic pain has also been proposed according towhich pain can be graded as being definite, probable, orpossible neuropathic pain depending on four criteriabased on clinical symptoms and signs [2].
Neuropathic pain is a fairly common condition with anestimated prevalence of 1.5% in the general population[3]. However, precise estimation of its incidence andprevalence is extremely difficult because of the lack of astandard definition and cutoff for diagnosis [4,5]. Recentstudies have found the prevalence of pain of predomi-nantly neuropathic origin to be as high as 8.2% in thegeneral population [6]. It is a cause of significant disability,decreases productivity and quality of life, and increasesthe cost of health care by approximately threefold [7].Current pharmacological and interventional modalitiesavailable for the treatment of chronic neuropathic painhave variable efficacy. In addition, other problems withcurrent therapy include intolerable adverse effects.
Pain Medicine 2011; 12: 808–822Wiley Periodicals, Inc.
808

Emerging modalities including gene therapy have shownconsiderable promise in this area; however, there areseveral aspects that need to be clarified regarding theiruse including mechanism of action, specific advantagesand disadvantages, as well as their practicality for generalclinical use. This article will review currently available lit-erature to highlight the state of our current knowledgeregarding the current and potential future role of genetherapy for chronic neuropathic pain.
Methods
An extensive literature search was completed by theauthors involved in the study. Medline was used as theprimary source of articles that were searched usingPubmed, the key words being various combinations of“neuralgia,” “chronic neuropathic pain,” “pathophysiol-ogy,” “mechanisms,” “treatment,” and “gene therapy.”Further information was obtained from Internet Websitesof the IASP (http://www.iasp-pain.org) and Kimball’sBiology Pages (http://biology-pages.info). Additionalarticles were identified by manual review of retrieved ref-erences. English language full-text articles ranging from1980 to November 2010 were selected based on theirquality, relevance to the subject with focus on pathophysi-ology of chronic neuropathic pain, and its application togene therapy for treatment of neuropathic pain.
Target Sites and Molecules for Gene Therapy ofChronic Neuropathic Pain
Gene therapy for chronic neuropathic pain encompassesthe introduction of specific genes into neurons, where theysynthesize specific proteins that interact with their recep-tors and/or ionic channels involved in the pathogenesis ofneuropathic pain. Hence, it is important to understand therole of key biologically active molecules and ionic channelsin causation of chronic neuropathic pain. This will bereviewed below.
Role of Biologically Active Molecules
Ongoing research has resulted in the identification ofseveral biologically active molecules that have been impli-cated in the causation of chronic neuropathic pain. Theycan be categorized as:
1. Excitatory amino acids (EAA), substance P (SP),neurokinin (NK) A: Persistent activation of afferent Cfibers causes the release of EAAs like glutamate, SP,and neurokinin A. Acting via the N-methyl D-aspartate(NMDA), NK-1, and NK-2 receptors, respectively, theyhave been shown to rapidly induce hyperalgesia andspinal facilitation [8,9]. Several studies have shown thatglutamate is involved in prolonged nociception [10–14].Intrathecal administration of nonselective NMDA andnon-NMDA (quisqualate/kainate) glutamate receptorantagonists in rats has been shown to effectivelyreduce the early as well as delayed peaks of chemicalnociception induced by formalin. Selective NMDAreceptor antagonism however produces a marked
decrease in the second delayed peak with little effecton the initial peak [11]. This suggests that activation ofthe NMDA receptor plays a significant role in inductionof central spinal facilitation and, once induced, couldprovide the foundation for further modulation and per-sistence of pain [11,15]. NMDA receptors are also thekey receptors in the “wind up” phenomenon of centralsensitization whereby each successive stimulus of apulse volley sensitizes the dorsal root neurons to gen-erate more action potential [15,16]. Other studies havealso suggested that EAA and SP do not actually play arole in pain transmission but in the central facilitation ofthe process, which, once activated, does not requiretheir continued presence [8].
2. Calcitonin gene-related peptide (CGRP): Data fromseveral animal studies implicate CGRP in the genera-tion and maintenance of hyperexcitability of spinal cordneurons in inflammatory models of hyperalgesia [17].Possible mechanisms may involve the release of SPand EAA in the dorsal horn neurons [18,19].
3. Inflammatory cytokines: Spinal inflammatory cytokinessuch as tumor necrosis factor-a (TNF-a) [20–24] andinterleukin-1 (Il-1) [25–27] have also been shown tocause hyperalgesia and enhance nociception at thespinal level. Intrathecal administration of Il-1 has beenshown to induce mechanical and thermal hyperalge-sia [28], the effect being antagonized by intrathecallyadministered Il-1 receptor antagonists [29] and neu-tralizing antibodies against it [9]. Intrathecal etaner-cept, a TNF-a inhibitor, administered before spinalnerve ligation decreases mechanical allodynia byalmost 50% [30]. A synergistic action between Il-1band TNF-a [29], and Il-1 and other neurotransmitters[31,32] have also been suggested. Il-10, however,has been shown to inhibit the expression of Il-1 andTNF-a [33], and has antinociceptive properties[34,35]. Il-2 also has antinociceptive properties [36]mediated via its binding to opioid receptors [37,38]and reversed by naloxone [38]. Il-4 is also a prototypeof an anti-inflammatory cytokine, which has beenshown to decrease the expression of Il-1 [39] andinhibit the induction of nitric oxide (NO) synthase [40]and cycloxygenase-2 enzymes [39]. Its antinocicep-tive properties have been well documented in priorstudies [34,41]. The source of these cytokines (Il-1band TNF-a) has been traced to spinal cord neurons,neuroglial cells, and vascular endothelial cells in ratspinal cord after acute spinal cord injury [20,42,43],and in spinal cord neurons and microglial cells inhumans after traumatic spinal cord injury [44,45].Studies have linked a chemokine called fractalkine tothe activation of glial cells that cause the release ofinflammatory mediators [46,47].
4. NO: Spinal NO has long been implicated in the centralmechanisms of inflammatory hyperalgesia. The induc-ible NO synthase activity has been demonstratedwithin 20 minutes [48] to 1 hour [9] of the application ofa nociceptive stimulus depending upon the type ofstimulus. NO further causes the release of SP, CGRP,and inflammatory cytokines, and helps in central facili-tation of synaptic transmission.
809
Gene Therapy of Pain

5. Prostaglandins: The fact that the prostaglandins stimu-late the peripheral afferent fibers and cause painin inflammatory conditions is well known. However,recent evidence has also implicated them in centralsensitization [49]. Membrane depolarization and acti-vation of NMDA receptors increase the concentrationof arachidonic acid in the neurons, which, when actedupon by enzyme cyclooxygenase-2, forms prostaglan-dins [50]. Prostaglandins then diffuse into the extracel-lular space and cause the release of neurotransmitterssuch as EAA, SP, CGRP, and NO. These neurotrans-mitters can further increase the release of prostaglan-dins [51].
6. Melanocortin: The role of the melanocortin system inneuropathic pain is being actively explored. As early as1981, Sandman and Kastin had demonstrated thehyperalgesic effect of intraventricular injections of asubtype of melanocyte-stimulating hormone (MSH)in rats in a double-blind study and suggested theirrole in the body as endogenous anti-opiates [52]. Itis well known that the precursor molecule pro-opiomelanocortin (POMC) is cleaved to the peptidesadrenocorticotropic hormone (ACTH) and MSH, and ispresent in the pituitary. However, recent work has dem-onstrated the presence of mRNA of POMC in the ratspinal cord and also the presence of MSH receptors,specifically the subtype MS4, in the lamina I, II, and X ofthe spinal gray mater that are involved in nociception[53,54]. Intrathecal administration of a melanocortinreceptor antagonist effectively decreases the sensitivityto cold and mechanical stimulation in animal models ofchronic neuropathic pain. In contrast, a melanocortinreceptor agonist has the opposite effect [55]. Interest-ingly, g subtype of MSH acts via g-amino butyric acid(GABA) receptor pathway rather than melanocortinpathway and has analgesic activity [56]. Even moreintriguing is the interaction between melanocortins andopioids. Apart from producing MSH, cleavage ofPOMC also produces b-endorphin, which is an endog-enous opioid. This opioid along with its m- andd-receptor subtypes are present in lamina X of thespinal gray mater involved in nociception. Whereasa-MSH acts via melanocortin G-protein-coupledreceptor to increase the activity of adenylate cyclase,b-endorphin acts via d-receptor to decrease its activity.Thus, adenylate cyclase is the intracellular integrator ofboth pathways and, depending upon which pathwaypredominates, can lead to nociception or analgesia[55]. There is downregulation of m-opioid receptors andincrease in MS4 receptor gene expression in the spinalcord of rats tolerant to morphine [57]. Kalange et al.found that chronic intracerebroventricular administra-tion of an MS4 receptor antagonist along with mor-phine in rats delayed the development of tolerance andreduced the dependence on morphine [58].
7. Endogenous opioids: The central pain inhibitorymechanisms involve the endogenous opioids(b-endorphins, dynorphins, enkephalins), and noradr-energic and serotoninergic systems. Endogenousenkephalins are synthesized from a precursor moleculecalled preproenkephalin that, upon processing, pro-
duces met-enkephalin and leu-enkephalin [59]. Thesehave been demonstrated in a wide variety of centraland peripheral neurons including those of thesubstantia gelatinosa (lamina II) and dorsal root gan-glion [60]. They also have been shown to be decreasedin chronic inflammatory pain states [61]. The endog-enous opioids act on the m-, d-, or k-receptors presentmostly in the presynaptic terminals of the primary affer-ents. The receptors are coupled to G-proteins that,upon activation, inhibit calcium channels and adenylatecyclase, and also open up the potassium channels,leading to reduced neuronal excitability [60]. Interest-ingly, studies have shown the presence of opioidreceptors on peripheral nerve terminals as well. Thesereceptors are of subtypes mu, lambda, and kappa [62],and assume an important antinociceptive role duringinflammation when they bind to opioid peptidesreleased from inflammatory cells [63]. Perineural dis-ruption due to inflammation improves the access ofthese peptides to the opioid receptors. New opioidreceptors are also synthesized over the next few daysand are transported to the nerve endings by axonaltransport [64]. This is important because targeted genetherapy can be used to increase the concentration ofopioid receptors at peripheral nerve terminals asdetailed later.The antihyperalgesic effect of endogenous opioids hasbeen well substantiated. However, dynorphin has alsobeen found to demonstrate significant non-opioid pro-nociceptive activity. It acts via kappa receptors toproduce analgesia but, at the same time, increases therelease of excitatory neurotransmitters, SP, and CGRPfrom primary afferent neurons. Studies have shownthat prolonged opioid administration increases thespinal dynorphin expression [65]. This has been pos-tulated to play a major role in opioid-induced pain,possibly resulting in behavioral pattern of tolerance tothese drugs.
8. Norepinephrine: Norepinephrine plays a very complexrole in pain modulation. Its various receptors are widelydistributed in the central nervous system and periph-eral tissues. At the peripheral level, norepinephrinemay have both pain facilitatory and inhibitory actiondepending on the type of receptors it acts upon[66–70]. At the spinal level, norepinephrine releasedfrom descending pathways cause inhibition of pain atpresynaptic and postsynaptic level [71]. At supraspinallevels, norepinephrine has variable pain modulatoryeffects depending on factors like the supraspinal site ofaction, the duration and chronicity of pain, and the typeof adrenergic receptor present [72,73].
9. GABA: Various studies have shown that GABA, theprincipal neurotransmitter of the spinal interneurons,plays an important role in pain inhibition. In fact, partialnerve injury has been shown to promote a selectiveloss of GABAergic synaptic pathways in the dorsalhorn of the spinal cord [74]. GABA is synthesized fromglutamate in the presence of a rate-limiting enzymeglutamic acid decarboxylase (GAD), which exists in twoisoforms: 65 and 67. Most studies of gene therapyhave been done with GAD67, which is expressed in
810
Kumar et al.

interneurons and other neurons that fire tonically, andsynthesizes cytosolic GABA involved in general meta-bolic activity [75].
Role of Ionic Channels
After a nerve injury, the regenerating sprouts of the primaryafferent fiber have shown abnormal excitability withmechanical stimulation and spontaneous erratic dis-charge characteristics [76]. These are in part mediated bythe ionic channels [76,77]. Several subtypes of voltage-gated sodium channels have been characterized, eachhaving different properties. Nerve injury triggers mem-brane remodeling, which leads to membrane hyperexcit-ability. This is in part attributed to expression of differentsubtypes of sodium channels in the membrane withabnormal inactivation kinetics, allowing for repetitive firing.Subtypes 1.3 and 1.7 are examples of such channels andhence can be a target for gene therapy [78]. An interactionbetween opioid receptor activation and voltage-gatedsodium channels has also been suggested [79].
Expression of calcium channels also allows for calciumentry into the neurons where it modulates the regulation ofgrowth related proteins. It is shown to increase the releaseof SP and CGRP from rat nerve neuromas [76].
Gene Therapy—Current Insights Regarding ItsMechanism(s) of Action
Delivery of genes that encode proteins with antinocicep-tive properties or those that can antagonize nociceptivemolecules into the neurons forms the basis of genetherapy of neuropathic pain. The delivery of geneshowever requires a vehicle, which could be a virus or anon-virus.
1. Viral vectors: The advantages of using recombinantviruses as vectors are their natural capacity to enterthe cells and deliver their genome to the host cell.However, the main drawbacks are their natural infec-tivity and their limited capacity to carry the genome.Also, the lytic effect of the virus on the host cell com-bined with the immune response mounted against thevirus or the newly expressed gene product may limitthe duration for which such a therapy is effective [80].Various viruses have been studied and modified toovercome these limitations. These include herpessimplex virus (HSV), adenovirus, adeno-associatedvirus (AAV), and retroviruses.(i) HSV: The genome of HSV has been completely
sequenced. It is relatively large (152 kb) and has 72genes organized as double-stranded DNA [81].Some of the important genes of the virus include theinfected cell polypeptides (ICP) 4 gene, thymidinekinase (Tk) gene, and the latency-associated tran-script (Lat). The ICP 4 gene is expressed immedi-ately after the viral entry into the nucleus and isresponsible for initiating and controlling the expres-sion of genes vital for viral replication [82]. The Tkgene is responsible for causing reactivation of the
virus from the latent stage [83]. The Lat gene is theonly gene that is actively transcribed during latency,hence indicating its role in maintaining latency of thevirus [60,84]. Because almost half of the HSV genesare nonessential and can be replaced by the trans-gene, it enables the virus to carry inserts of about30–40 kb [85]. One advantage of using HSV as avector is that it is a neurotropic virus that can beapplied directly on the abraded skin or given byintradermal injections. It multiplies in the skin epithe-lia for a few cycles, penetrates the peripheral nerveendings, and travels retrogradely to the cell bodiesof the sensory neurons, where it establishes a latentinfection in the form of episome, without integratingwith the host genome. Another advantage with HSVis that the release of gene product is restricted toonly those areas of spinal cord where the nocicep-tive neurons are projecting. Also, the axonal trans-port of gene product to the nerve endings mayprovide additional reduction in pain [87].
(ii) AAV: The recombinant AAV vectors are nonpatho-genic and replication defective, and integrateinto the host genome, hence allowing long-termexpression of the gene [87]. When AAV was usedas a vector to transfer opioid gene, it was observedthat it causes the expression of gene only in dorsalroot ganglion (DRG) and peripheral afferentssparing the spinal cord. This may help preventstimulation of central compensatory mechanismsmediated via dynorphin, which can lead to opioidtolerance over time, as discussed above.One disadvantage of using AAV as vector is the factthat it is not neurotropic. For this reason, delivery ofthe virus to the target site poses a difficulty. Animalstudies have experimented with direct injections ofthe recombinant virus into the DRGs and also withintrathecal and intraneuronal routes of administra-tion. For practical purposes, the intrathecal routeseems to be the most appropriate choice. In aseries of experiments, Storek et al. tried to identifythe efficacy of intrathecal delivery of recombinantAAV and ways to make it more effective anddurable [88,89]. They found that upon intrathecalinjection of the commonly employed recombinantAAV serotype into rats, the neuronal tissues did notshow an expression of the marker protein greenfluorescent marker protein (GFP) at the end of 4weeks. They postulated that this could be second-ary to the limited capacity of the capsid proteins tomediate transfer of genome to the target cells orbecause of limited capacity of the target cellmachinery to convert AAV’s single-stranded DNAto double stranded. To overcome these obstacles,the authors modified the vector by pseudotyping it(a process by which different viral serotypes arephenotypically mixed, and capsid glycoproteins areexchanged) to generate a new capsid and, at thesame time, modifying the genome to make itdouble stranded. This self-complementary recom-binant AAV serotype 8 (scAAV8) was shown to beeffective in causing marker protein expression for at
811
Gene Therapy of Pain

least 12 weeks upon intrathecal injection. None oftheir studies reported any cytotoxicity or activationof immune response in the host. However, a fewqueries regarding the rostrocaudal extent of trans-gene expression in the DRG, effect on brain andother organs outside the nervous system, and tox-icity of single injection vs two sequential injectionsinto cerebrospinal fluid (CSF) are still unanswered,and further studies are needed in this respect [90].
(iii) Retrovirus: A novel vector called human foamy virus(HFV) has also been recently studied. It is a retro-virus that can transduce different types of cellsincluding neurons across various mammalianspecies [91,92]. It is nonpathogenic, not inactivatedby human serum [91], can transduce nondividingcells effectively [93], has a large genome, and,unlike other retroviruses, has a second promotercalled internal promoter at the end of env geneproviding for additional regulation [94].
2. Nonviral vectors: Some studies have experimentedwith injecting naked plasmid, liposomal-complexedDNA, or polymer-complexed DNA intrathecally, eachwith their own merits and demerits [95,96]. These non-viral vectors have the advantage that they do not carrythe inherent risk of infection, which does exist with anyviral vector; in addition, they can be used for genes thatare too large to be carried by viruses. While thesevectors have been shown to be safe end extremelyeffective in transfecting the cells in vitro, their in vivoefficiency has been found to be rather low [97].Although research designed to improve their cellularuptake is ongoing, and few studies have found somesuccess by addition of a pH-sensitive fusogenicsegment to the liposomal complex [98], as of now, theirlimitations still preclude their use for therapeuticpurposes.
Basics of Gene Therapy Using Viral Vectors
The gene to be inserted into the viral genome (calledtransgene) is first placed under the control of a promoter,
which will regulate its expression. Some studies have useda modified HSV latency promoter consisting of a fusionbetween the region upstream from the HSV Lat corepromoter and elements of Moloney murine leukemia virus(MLV) long terminal repeat (LTR) [85]. Others have usedthe human cytomegaloviral immediate-early promoter/enhancer, which has been shown to drive transgeneexpression both acutely and after establishment of latency(Figure 1). It is then recombined with the viral genome byuse of site-specific recombination (e.g., the recombinationoccurring at a specific site called LoxP mediated via Crerecombinase enzyme) [84].
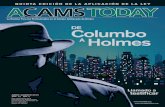
Sometimes, the transgene may be the one that encodesprotein, which is actually pro-nociceptive (e.g., CGRP).However, it is inserted into the viral genome in such a waythat upon transcription, the mRNA synthesized has asequence opposite to that of mRNA synthesized in thehost cell from native DNA (“antisense sequence”). Hence,the virally encoded mRNA hybridizes the native hostmRNA by simple Watson–Crick interaction and effectivelyblocks its translation into the biologically active proteinwith pro-nociceptive properties, thus reducing its concen-tration within the cell (Figure 2).
Clinical Trials of Gene Therapy for Treatment ofNeuropathic Pain
Several clinical trials have been carried out in animalmodels of neuropathic pain and have demonstrated theefficacy and safety of gene therapy in them. A few humanclinical trials are also underway. These trials will bereviewed based on the molecules they target with genetherapy.
Studies Targeting the Opioid Pathways UsingGene Therapy
Genes that direct the synthesis of opioid and their recep-tors have been introduced into the neurons of variousanimals using viral vector, and the effects were studied.
Figure 1 Schematic representation of recombinant herpes virus (adapted with permission from Wilson et al.[60]). The viral genome is comprised of a unique long segment (UL) and a unique short segment (US). Humanpreproenkephalin cDNA (hPPE) is placed under the control of human cytomegaloviral immediate-earlypromoter/enhancer (hCMV-P). The transgene–promoter construct is then inserted into the viral thymidinekinase gene, which is the gene responsible for reactivation of virus from latent stage. This insertion of transgeneinto the viral gene thus disables the virus from replicating in nondividing cells such as neurons. Polyadenylationsequence (PA) (simian virus—40 polyadenylation sequence) increases transcription and protein production.
812
Kumar et al.

Wilson et al. introduced the complementary DNA (cDNA)for human preproenkephalin into the sensory neurons ofmice using recombinant HSV1 as the vehicle [60]. Thetransgene was placed under the control of cytomegalovi-ral immediate-early promoter/enhancer, and the micewere infected by application on abraded skin. Immunohis-tochemistry successfully demonstrated the synthesis andprocessing of the opioid precursor in the mouse sensoryneurons. Study of the animal behavioral responses sug-gested reduced responsiveness of both C and Ad fibers tonociceptive stimuli. The biological effect of therapy wasfirst seen 4–5 days post-infection with its magnitudeincreasing in the next 2 weeks and remaining robust untilat least 7 weeks of observation, despite the fact that bythis time, the transgene expression had been reduced by75%. This discrepancy was postulated to be because ofthe ability of low levels of proenkephalin to modulatesensory neurons and their effect on neuronal plasticity.Another mechanism could be that the active enkephalinsare synthesized and stored in secretory vesicles in thenerve endings to be released only with robust activation ofperipheral nerve afferents. This analgesic effect was
blocked by intrathecal naloxone only when the fibers werepre-sensitized by capsaicin and dimethyl sulfoxide with noeffect on basal withdrawal latencies, indicating thatendogenous opioids are released only with substantialactivation of the primary afferents and baseline nocicep-tion is not altered. The study overall suggests that thetargeted application of this virus could result in antihype-ralgesia mediated via opioids without their antecedentsystemic toxicity and longer duration of action withoutdisrupting normal sensory transmission in chronic neuro-pathic pain.
Similar results were substantiated by another study, whichused the rat proenkephalin gene placed under the regula-tion of binary promoter [99] (HSV Lat core promoter andMLV LTR, as described above). This recombinant HSV1KOS strain (known for its extremely low neurovirulence[100]) was applied to abraded skin of rats. Three weekspost-infection, they observed a 7-fold increase in thenumber of proenkephalin mRNA-expressing neurons, a24-fold increase in the levels of proenkephalin mRNA, anda 160% increase in concentration of met-enkephalin-likematerial in DRG. Reversed-phase high-performance liquidchromatography and immunohistochemistry demon-strated that the overexpressed proenkephalin was com-pletely processed into active peptides. These activepeptides were preferentially transported to the peripheralprocesses of primary afferent neurons, where they accu-mulated in secretory vesicles to be released by electricalstimulation of dorsal roots or peripheral nerve. Like theprevious study, this study also showed that basal nocice-ption was not affected by this therapy. However, theauthors went one step ahead to demonstrate its therapeu-tic application in rats [85]. They applied this recombinantvirus to increase the expression of proenkephalin gene inDRG of rats with adjuvant-induced polyarthritis and studiedthe effect of this therapy on their functional disability. Theyfound that the locomotor activity of polyarthritic ratsreached up to 70% of that of healthy rats, which was highlysignificant. The effect was also long standing and persisteduntil at least 8 weeks of observation.
Finegold et al. used an adenovirus as a vector to introducethe artificial fusion gene encoding the secreted form ofb-endorphin (preprobeta-endorphin) into the meningealcells [101]. The gene was under the regulatory control of acytomegaloviral promoter, and the recombinant viruswas injected intrathecally. The CSF concentration ofb-endorphin increased fourfold 1 week after infection butdeclined to control levels within 15 days because of animmune response against the vector. Like other studies,an antihyperalgesic effect to inflammatory stimulus wasobserved without effect on basal nociception. Yeomanset al. tested the efficacy of this therapy in monkeys [102].They found that upon topical application of recombinantHSV carrying the human preproenkephalin on the dorsalsurface of monkeys’ feet, there was a significant analgesiain response to periodic sensitization and activation of Cnociceptors. The effect was sustained for 20 weeks.Immunohistochemistry and radioimmunoassay confirmedthe production of enkephalin peptides by the DRG cells.
(Native gene) (Antisense gene)
Transcription
(Native mRNA) (Antisense mRNA)
Hybridization
(Duplex formation by simple Watson-Crick base pairing)
Translation blocked
Figure 2 Adapted with permission from Kimball’sBiology Pages. The antisense gene sequence tran-scribes to antisense RNA and hybridizes the mRNAfor the gene, hence blocking translation and synthe-sis of that specific protein.
813
Gene Therapy of Pain

Other experiments have also been done to introduce am-opioid receptor gene into neurons. Zhang et al. [103]used two recombinant viruses, one with the m-receptorgene (SGMOR) and another with the antisense sequenceof gene (SGAMOR), placed under the cytomegaloviralpromoter. They also inserted cDNA for GFP flanked byinternal ribosome entry site, which could allow initiation oftranslation of GFP from the middle. The co-expression ofGFP with the m-receptor helped to deduce whether thechanges in receptor expression were due to infection withtheir HSV constructs. The study demonstrated a signifi-cant increase in m-receptor immunoreactivity in the skinwhere the virus was applied, in the dorsal root ganglion, aswell as in the dorsal horn of the spinal cord with SGMORand the opposite with SGAMOR. This showed that them-receptors not only were synthesized in the DRG, butalso transported anterograde and retrograde, and thuscan modulate pain and analgesia at both spinal andperipheral sites. With respect to DRG, the increase inm-receptor immunoreactivity related to SGMOR was seenmostly in large-diameter neurons (which normally do notexpress endogenous m-receptor), whereas the decreaseassociated with SGAMOR was seen in small- andmedium-diameter neurons (which normally expressendogenous receptors and are presumably nociceptive).The analysis of GFP expression revealed that 75% of theincrease in m-receptor expression in the peripheral affer-ents could be attributed to the viral constructs. Theauthors also demonstrated the effect of increasing dosesof subcutaneous loperamide, which is a selectivem-receptor agonist, on paw withdrawal latencies in theSGMOR-infected, SGAMOR-infected, and the controlrats, and the resultant dose–response curve was ana-lyzed. As expected, the half-maximal effective concentra-tion of loperamide (EC50) significantly decreased in ratsthat were infected with SGMOR as compared with that inrats infected with SGAMOR, and the changes wereequivalent albeit opposite. They concluded that the effectof m-receptor gene insertion and its knockdown is not onlymolecular but also functional, thus paving a way for itstherapeutic application.
Xu et al. [104] used recombinant AAV to transferm-receptor gene placed under the control of rat neuron-specific enolase promoter [105] into the DRG of rats. Theyfound that the viral system induced an effective expressionof m-receptors not only in small- and medium-sizedneurons, but also in large neurons. This intervention thusincreases the number of neurons that are sensitive toopioids as well as increase the sensitivity of individualneurons to opioids. The study also found that the therapysensitizes the neurons to opioid-mediated calciumchannel inhibition. The m-receptor expression was longlasting (6 months after the initial infection) and wasrestricted to DRG cells and their presynaptic terminals,unlike studies using HSV that have found gene expressioneven in the spinal cord, thus having the potential advan-tage of not invoking mechanism causing opioid tolerance.However, as discussed above, one disadvantage of usingAAV as vector is that it is not neurotropic, hence makingthe delivery of virus to the neurons difficult. For this study,
the researchers had to remove a small piece of vertebra toinject the virus directly into the DRG. As was discussed,intrathecally injected recombinant scAAV8 was used byStorek et al. and found to be effective in transducing noci-ceptive neurons in DRG to produce b-endorphin and Il-10.It caused significant analgesia in chronic neuropathic painmodel of rats. The effect was sustained for at least 3months [89].
Studies Targeting the Interplay Between InflammatoryCytokines Using Gene Therapy
Studies have also been conducted on the gene transferof immune mediators of chronic neuropathic pain.Because these mediators of nociception have a veryshort half-life, their therapeutic application requires theircontinuous intrathecal infusion, which causes a lot ofinconvenience to the patients, is costly, and therefore isnot very practical. Induction of meningeal or DRG cellsto produce these cytokines by gene therapy has there-fore attracted a lot of attention. Hao et al. transducedthe DRG neurons of rats to produce p55 TNF receptor(TNFR) by using recombinant HSV as a vector [106].They placed this gene under the control of an HSVimmediate/early promoter and delivered the virus subcu-taneously. They found that release of TNFR from theneurons reduced the expression of membrane TNF andIl-1, presumably by binding to membrane TNF andinducing reverse signaling [107] into the cells. It mani-fested as reduced thermal hyperalgesia in the infectedanimals. Another study used HSV-based vectors todeliver soluble TNFR and Il-1 receptor antagonist tonerve fibers in the joint cavity in the arthritis model ofrats, and successfully demonstrated the expression ofTNFR in significant concentration in the joint fluid andreported significant reduction of leukocytosis and syno-vitis. However, the effect on functional status of the jointswas not studied [108]. Several studies have tried toutilize anti-inflammatory properties of Il-10 to combatpain. Intrathecal injections of Il-10 have prevented andreversed Il-1-induced pain in different animal models, butits short half-life (2 hours) limits clinical application. Il-10gene transfer using viral vectors show considerablepromise but again are effective only for approximately 2weeks due to activation of host immune system or inef-ficient promoter activity. Intrathecal injections of nakedplasmid DNA encoding Il-10 have found considerablepromise. Whereas anti-allodynic effect of a single injec-tion may not be long lasting, a second injection at aninterval of 2–3 days potentiates the effect of the first, andthe intervention remains effective even after 40 days[109]. The study found its efficacy in both acute andchronic neuropathic pain. Intrathecal injection of plasmidDNA encoding Il-10 was also found to be effective inpreventing and reversing allodynia in a paclitaxel-inducedperipheral neuropathy model of pain in rat [110]. Theauthors found increased levels of Il-10 mRNA in thelumbar DRG and meninges, and decreased expressionof Il-1 and TNF-a mRNA, 2 weeks after initial therapy.Because the Il-10 receptors are only expressed by glialcells and not the neurons, this therapy does not interfere
814
Kumar et al.

with neuronal function and acts only to alter the localcytokine milieu in favor of anti-inflammatory mediatorsthat prevent/reduce acute as well as chronic neuropathicpain. Gene therapy has also been used to transduceneuronal cells to produce Il-2, another inhibitory cytok-ine. Yao et al. injected recombinant adenovirus carryingIl-2 transgene under the control of cytomegaloviralimmediate/early promoter enhancer into the lumbar sub-arachnoid space of rats and detected the mRNA in thecells of pia mater as well as dorsal horn of spinal cord[111]. Behavioral experiments showed that the infectionof the rats with recombinant adenovirus increased thebasal nociceptive pain threshold and also had analgesiceffect on chronic neuropathic pain; the response wasmaintained for 4 weeks. In another study, naked plasmidDNA encoding Il-2 was injected into the subarachnoidspace, and the researchers found that the antinocicep-tive effect could be maintained for up to 6 days [112].Hao et al. subcutaneously injected recombinant HSVcarrying Il-4 gene under the regulation of HSV ICP 4promoter and observed that it had a significant reductionin mechanical allodynia and thermal hyperalgesia, theeffect peaking at 2 weeks and lasting for 5 weeks [86].A second inoculation was equally effective in producinganti-allodynia, which also lasted for a similar duration,indicating no immune response to the first inoculation.The researchers also established that the interventionhad resulted in reduced levels of PGE2 and Il-1 in thedorsal horn. Studies have also been done to increasethe expression of glial-derived neurotrophic factor(GDNF) in the neurons, using recombinant HSV[113,114]. One study found that this intervention had ananti-allodynic effect that was maintained for 3–4 weeksand also upon subsequent inoculation [113].
Studies Targeting the GABA Pathway UsingGene Therapy
Transduction of DRG neurons to produce GAD67 forGABA synthesis has also been effective in reducing pain.The synthesized GABA is released from interneurons viareversal of GABA transporter and is independent of elec-trical depolarization [115]. Studies have used HSV as avehicle to deliver gene encoding GAD67 and demon-strated decreased mechanical allodynia as well as thermalhyperalgesia in rats [116,117]. Another study comparedthe efficacy of analgesia between HSV-transduced pro-duction of GAD and proenkephalin, and found that reduc-tion in pain-related behavior (mechanical allodynia) wasmore profound and prolonged with GAD than with proen-kephalin [118]. In one of the studies, researchers wereable to transduce DRG neurons of rats by subcutaneousinoculation of recombinant HFV containing GAD67 gene[119]. They could detect GAD expression in the DRG thatmanifested as an increased synthesis of GABA. This inter-vention significantly reduced the mechanical allodynia aswell as thermal hyperalgesia in the spinal cord injury modelof rats. The therapeutic effect lasted for 5 weeks, and asecond inoculation produced effects of similar magnitude,indicating lack of immune response and tolerance to firstinoculation.
Studies Targeting CGRP Using Gene Therapy
Pohl and Braz placed an antisense sequence to CGRPunder the control of modified HSV latency promoter con-sisting of a fusion between the region upstream from theHSV Lat core promoter and elements of Moloney MLV LTR[85]. The antisense sequence was the complete sequenceof the exon 5 of the rat CGRP gene in an antisenseorientation. This transcriptional unit was then recombinedwith the HSV genome at the glycoprotein C locus usinghomologous recombination. This recombinant virus wasthen inoculated on the slightly scarified footpad surface ofrat hind limbs. The study demonstrated that the concen-tration of CGRP in ipsilateral lumbar DRG of rats inocu-lated with the recombinant virus was significantly lowerthan the control rats after induction of inflammationachieved by subcutaneous injection of Freund’s adjuvantinto the hind paw of rats. They also observed that thoughthe biological efficacy of the therapy (as measured by pawvolumes indicating local edema) was sustained for all ofthe 16 days’ period of observation, the biochemical effi-cacy (measured by reduction in the levels of CGRP in theDRG) lasted for only 12 days after induction of inflamma-tion. They suggested that limited variations in the level ofendogenous neuropeptides were sufficient to sustain afunctional effect.
A similar study was carried out by Tzabazis et al. [120]using a slightly different viral construct. They placed thetransgene with antisense sequence to CGRP under thecontrol of human cytomegaloviral immediate-earlypromoter/enhancer and then recombined it with the ICP4-negative HSV genome at the Tk locus, thus inactivatingit, in order to disrupt the capacity of the virus to replicatein nondividing cells. The recombinant virus was thus iso-lated, purified, and rescued by introduction of ICP 4 DNA.The ICP 4 protein represses the latency-associated pro-moter, hence helping in viral replication. This virus wasapplied to the abraded skin of mice. The study demon-strated that such mice showed reduced thermal C fiberhyperalgesia after capsaicin application as compared withcontrols, comparable with the effect of intrathecal CGRPantagonist but longer lasting. They quantified the extent ofCGRP knockdown to be approximately 80%, which wascomparable to another study that used antisensesequence to NMDA receptor NR1 subunit delivered tocultured neurons via recombinant HSV [121]. The effect ofa single application of the virus lasted for 14 weeks. Boththe studies established the effectiveness of transdermalroute of viral delivery, which is highly desirable.
CGRP appears to be an attractive target for gene therapybecause it has been shown to prevent the development oftolerance to antinociceptive effects of morphine [122].
Studies Targeting Norepinephrine Pathway UsingGene Therapy
Inhibition of norepinephrine synthesis by gene therapy inareas of brain involved in pain facilitation is a novelapproach to treatment of pain. In a recent study, Martins
815
Gene Therapy of Pain

et al. [72] used HSV-1 as a vector for delivery of tyrosinehydroxylase transgene inserted in an antisense orientationdirectly to dorsal reticular nucleus of the rat brain. Tyrosinehydroxylase is an enzyme that catalyzes the rate-limitingstep in norepinephrine synthesis. Dorsal reticular nucleusis involved in supraspinal pain facilitation and receives astrong input from noradrenergic cell groups in the brainstem. Neuropathic pain was induced in these rats usingspared nerve injury. The authors successfully demon-strated not only a significant decrease in norepinephrineassociated with gene expression in this area, but also asignificant inhibition of mechanical allodynia, cold allo-dynia, and mechanical hyperalgesia. The ability of thevector to transduce only the noradrenergic neurons in thesupraspinal areas and to have sustained analgesic effectfor almost 2 months was remarkable. Although still experi-mental, the study is very promising and has opened newpotential mechanisms to target noradrenergic modulationof neuropathic pain.
Studies Targeting Ionic Channels Using Gene Therapy
Very few studies have examined the effects of targetingionic channels with gene therapy. One such study usedHSV as a vector to transfer the antisense sequence ofgene encoding subtype 1.7 of voltage-gated sodiumchannels in mice. Application of the recombinant virus onthe skin of the animals before treatment with completeFreund’s adjuvant blocked the upregulation of thischannel in DRG and also effectively prevented the devel-opment of thermal hyperalgesia after inflammation [123].
Chattopadhyay and colleagues established thattransgene-mediated expression of enkephalin in rodentmodels of diabetic neuropathy prevented the increase inexpression of neuronal sodium channels, subtype 1.7 byinhibition of protein kinase C, and p38 mitogen-activatedprotein kinase [79].
Advantages and Disadvantages Peculiar to GeneTherapy for Chronic Neuropathic Pain
The existing treatment modalities for the treatment ofchronic neuropathic pain are limited by adverse effectsand, for certain treatments, tolerance. Too often we feel,and most pain practitioners would agree, that evenoptimal utilization of current treatment modalities does notresult in effective pain relief. Gene therapy conceptuallyoffers the advantages of being localized, hence minimizingthe adverse effects. Also, it aims to target the biomol-ecules that are directly involved in pathophysiology ofchronic neuropathic pain and hence should be moreeffective. Several animal studies have shown biochemicalevidence of efficacy and safety; however, human trials arejust beginning to be completed. Some of the prior clinicaltrials on humans for conditions other than neuropathicpain have raised concerns about safety, and more clinicaltrials are needed before gene therapy can be deemed safeand effective for the use of humans, both for terminal andnonterminal causes of neuropathic pain. Another concernwith gene therapy is the regulation of gene expression.
The transduced cells constitutively synthesize the respec-tive protein that is beyond any physiological control. Con-tinuous production of TNFR, for example, may causeimmunosuppresion and increased susceptibility to infec-tions [124]. A physiologically responsive gene therapy,which targets the specific tissue, is inducible by a specificstimulus only, produces the effector protein in therapeuticconcentration, and has a rapid responsiveness that wouldbe an ideal system [125]. With respect to chronic neuro-pathic pain, however, this concern may not be very rel-evant because we actually require a constitutiveexpression of the gene. But this may be relevant forinflammatory pain conditions like rheumatoid arthritis,which has intermittent flares of inflammation [126].
Gene Therapy of Neuropathic Pain: Where Do WeStand Today?
Gene therapy with all its unique advantages seems to bean attractive modality for treatment of chronic neuropathicpain. However, most of the data regarding its safety andefficacy available to us today are from studies conductedon animals, mostly mice and rats. None of the studieshave been conducted to assess these effects of genetherapy in humans with chronic neuropathic pain.However, a trial of intrathecally injected plasmid encodingIl-10 in patients with chronic neuropathic pain has beenproposed [127]. Wolfe et al. have recently begun a phase1 human trial (began enrolling in December 2008) withreplication-defective HSV encoding enkephalin for treat-ment of moderate to severe intractable pain due to malig-nancy anatomically located below the angle of the jaw. It isprimarily a safety study, and per protocol, the eligiblepatients will be injected transdermally with escalating doseof the vector. The study is still ongoing and currentlyrecruiting patients [128,129]. An efficacy study with HSVencoding GAD67 is being planned [129].
Evans et al. [130] conducted a study on postmenopausalwomen who were undergoing joint replacement surgeriesfor advanced rheumatoid arthritis. One week before thesurgery, they injected those joints with autologous synovialfibroblasts transduced with retrovirus containing the Il-1receptor antagonist gene. This retrovirus was derived fromMLV. At surgery, results showed that the synovia of thesejoints produced more Il-1 receptor antagonist, and less ofIl-6 and prostaglandin E2 than those from control joints.This was an indirect indication of the biological activity ofthe transgene product. They observed these patients for 5years and did not find any evidence of delayed adverseeffects related to the virus itself. This study does showthe ability of gene transfer to induce production ofgene product; however, its functional efficacy was notassessed. Also, in this study, the joints were removed after1 week of injections; hence, concerns of safety if thesejoints were not removed, which would be the case moreoften in clinical practice, could not be addressed. A similarstudy was carried out by Wehling et al. [131] in twopatients with rheumatoid arthritis. They used the samevirus, transgene, and procedure to inject joints thatwere to undergo surgical synovectomy. However, they
816
Kumar et al.

assessed the functional effect of this therapy on the jointsby considering reduction in pain and joint swelling; also,they followed the patients for 4 weeks instead of 1 week.The study showed reduction in both parameters, whichwas maintained for 4 weeks with no adverse effectsreported for the duration. Recently, however, one of theclinical trials reported death in a young patient with rheu-matoid arthritis who received genetically engineered AAVwith the cDNA for TNFR. The cause of death was reportedto be disseminated histoplasmosis, and the patient wassimultaneously taking adalimumab (a TNF-a inhibitor). Thedirect role of gene therapy in causation of this death isdifficult to determine; however, Food and Drug Adminis-tration gave a go-ahead to this study after some modifi-cations in the protocol [132]. Other clinical trials done onhumans have shown adverse effects related to the virus,for example, the development of acute lymphocytic leu-kemia in a patient with severe combined immunodefi-ciency injected with a transduced retrovirus [133].
Summary and Future Perspectives
Management of chronic neuropathic pain has been chal-lenging for treatment providers and patients alike. Exist-ing therapies pose problems with their adverse effects;possibility of treatment tolerance; short duration ofaction; in many instances, suboptimal pain reduction;and need for repeated administration often via invasiveroutes, thus adding to the patients’ burden. Elucidationof the pain pathways and understanding of the patho-physiology at molecular level have enriched our knowl-edge of chronic pain and led to development of noveltreatment strategies that can overcome most of theshortcomings of standard treatment. In the current sce-nario, gene therapy may be a very promising therapeuticoption for chronic neuropathic pain. HSV and HFV holdconsiderable promise as vectors for gene transferbecause of their ease of administration and efficacy.However, scAAV8 offers the advantage of long-termtransduction of target cells albeit at the cost of takingintrathecal injections. As reviewed, studies have shownthe efficacy of gene transfer in neurons to produceendogenous opioids, m-opioid receptor TNFR, Il-2, Il-4,Il-10, GABA, and GDNF, or to decrease the productionof CGRP in alleviating mechanical allodynia and thermalhyperalgesia in response to various experimental painsyndromes. Moreover, enhanced synthesis of opioids ortheir receptors does not affect basal nociception; hence,the protective role of acute pain in response to acuteinjury is still retained. m-Receptor expression has beenshown to increase the potency of intrathecal morphineand also to decrease the EC50 of its agonist. Inhibitionof CGRP synthesis additionally prevents the develop-ment of tolerance to opioids. So far, results from animalstudies have been very encouraging. Initial human trialswith regard to gene therapy have shown efficacy, butacceptable safety is yet to be established. Furtherstudies are needed to establish the safety and adverseeffects of such a therapy, and to elucidate the dosingand monitoring patterns in humans.
References1 Merskey H, Bogduk N. Classification of Chronic Pain.
Seattle, WA: IASP Press; 1994.
2 Treede RD, Jensen TS, Campbell JN, et al. Neuro-pathic pain: Redefinition and a grading system forclinical and research purposes. Neurology2008;70(18):1630–5.
3 Bennett GJ. Neuropathic pain: New insights, newinterventions. Hosp Pract (Minneap) 1998;33(10):95–8.
4 Backonja MM. Defining neuropathic pain. AnesthAnalg 2003;97:785–90.
5 Max MB. Clarifying the definition of neuropathic pain.Pain 2002;96:406–7.
6 Torrance N, Smith BH, Bennett MI, Lee AJ. The epi-demiology of chronic pain of predominantly neuro-pathic origin. Results from a general populationsurvey. J Pain 2006;7(4):281–9.
7 Berger A, Dukes EM, Oster G. Clinical characteristicsand economic costs of patients with painful neuro-pathic disorders. J Pain 2004;5(3):143–9.
8 Okano K, Kuraishi Y, Satoh M. Involvement of spinalsubstance P and excitatory amino acids in inflamma-tory hyperalgesia in rats. Jpn J Pharmacol 1998;76(1):15–22.
9 Zanchet EM, Longo I, Cury Y. Involvement of spinalneurokinins, excitatory amino acids, proinflammatorycytokines, nitric oxide and prostanoids in pain facili-tation induced by Phoneutria nigriventer spidervenom. Brain Res 2004;1021(1):101–11.
10 Coderre TJ, Melzack R. The contribution of excitatoryamino acids to central sensitization and persistentnociception after formalin-induced tissue injury. JNeurosci 1992;12:3665–70.
11 Haley JE, Sullivan AF, Dickenson AH. Evidence forspinal N-methyl-D-aspartate receptor involvement inprolonged chemical nociception in the rat. Brain Res1990;518(1–2):218–26.
12 Ren K, Dubner R. NMDA receptor antagonistsattenuate mechanical hyperalgesia in rats with unilat-eral inflammation of the hind paw. Neurosci Lett1993;163(1):22–6.
13 Sung B, Lim G, Mao J. Altered expression anduptake activity of spinal glutamate transporters afternerve injury contribute to the pathogenesis of neuro-pathic pain in rats. J Neurosci 2003;23(7):2899–910.
817
Gene Therapy of Pain

14 Sakurada T, Wako K, Sugiyama A, et al. Involvementof spinal NMDA receptors in capsaicin-induced noci-ception. Pharmacol Biochem Behav 1998;59(2):339–45.
15 Woolf CJ, Thompson SW. The induction and main-tenance of central sensitization is dependent onN-methyl-D-aspartic acid receptor activation; impli-cations for the treatment of post-injury pain hyper-sensitivity states. Pain 1991;44(3):293–9.
16 Baranauskas G, Nistri A. Sensitization of pain path-ways in the spinal cord: Cellular mechanisms. ProgNeurobiol 1998;54(3):349–65.
17 Neugebauer V, Rümenapp P, Schaible HG. Calcito-nin gene-related peptide is involved in the spinal pro-cessing of mechanosensory input from the rat’s kneejoint and in the generation and maintenance of hyper-excitability of dorsal horn-neurons during develop-ment of acute inflammation. Neuroscience 1996;71(4):1095–109.
18 Kangrga I, Randic M. Tachykinins and calcitoningene-related peptide enhance release of endog-enous glutamate and aspartate from the rat spinaldorsal horn slice. J Neurosci 1990;10(6):2026–38.
19 Oku R, Satoh M, Fujii N, et al. Calcitonin gene-relatedpeptide promotes mechanical nociception by poten-tiating release of substance P from the spinal dorsalhorn in rats. Brain Res 1987;403(2):350–4.
20 Ohtori S, Takahashi K, Moriya H, Myers RR. TNF-alpha and TNF-alpha receptor type 1 upregulation inglia and neurons after peripheral nerve injury: Studiesin murine DRG and spinal cord. Spine 2004;29(10):1082–8.
21 Wei XH, Zang Y, Wu CY, et al. Peri-sciatic adminis-tration of recombinant rat TNF-alpha inducesmechanical allodynia via upregulation of TNF-alpha indorsal root ganglia and in spinal dorsal horn: The roleof NF-kappa B pathway. Exp Neurol 2007;205(2):471–84. Epub March 23, 2007.
22 Nicol GD, Lopshire JC, Pafford CM. Tumor necrosisfactor enhances the capsaicin sensitivity of ratsensory neurons. J Neurosci 1997;17(3):975–82.
23 Sorkin LS, Xiao WH, Wagner R, Myers RR. Tumournecrosis factor-alpha induces ectopic activity in noci-ceptive primary afferent fibres. Neuroscience 1997;81(1):255–62.
24 Sorkin LS, Doom CM. Epineurial application of TNFelicits an acute mechanical hyperalgesia in the awakerat. J Peripher Nerv Syst 2000;5:96–100.
25 Kleibeuker W, Gabay E, Kavelaars A, et al. IL-1 betasignaling is required for mechanical allodynia induced
by nerve injury and for the ensuing reduction in spinalcord neuronal GRK2. Brain Behav Immun 2008;22(2):200–8. Epub Sep 14, 2007.
26 Wolf G, Gabay E, Tal M, Yirmiya R, Shavit Y. Geneticimpairment of interleukin-1 signaling attenuates neu-ropathic pain, autotomy, and spontaneous ectopicneuronal activity, following nerve injury in mice. Pain2006;120(3):315–24. Epub Jan 19, 2006.
27 Hashizume H, DeLeo JA, Colburn RW, Weinstein JN.Spinal glial activation and cytokine expression afterlumbar root injury in the rat. Spine 2000;25(10):1206–17.
28 Tadano T, Namioka M, Nakagawasai O, et al. Induc-tion of nociceptive responses by intrathecal injectionof interleukin-1 in mice. Life Sci 1999;65(3):255–61.
29 Sweitzer S, Martin D, DeLeo JA. Intrathecalinterleukin-1 receptor antagonist in combination withsoluble tumor necrosis factor receptor exhibits ananti-allodynic action in a rat model of neuropathicpain. Neuroscience 2001;103(2):529–39.
30 Svensson CI, Schäfers M, Jones TL, Powell H, SorkinLS. Spinal blockade of TNF blocks spinal nerveligation-induced increases in spinal P-p38. NeurosciLett 2005;379(3):209–13.
31 Jeanjean AP, Moussaoui SM, Maloteaux JM,Laduron PM. Interleukin-1 beta induces long-termincrease of axonally transported opiate receptors andsubstance P. Neuroscience 1995;68(1):151–7.
32 Inoue A, Ikoma K, Morioka N, et al. Interleukin-1betainduces substance P release from primary afferentneurons through the cyclooxygenase-2 system. JNeurochem 1999;73(5):2206–13.
33 Zhou Z, Peng X, Hao S, Fink DJ, Mata M. HSV-mediated transfer of interleukin-10 reduces inflam-matory pain through modulation of membrane tumornecrosis factor alpha in spinal cord microglia. GeneTher 2008;15(3):183–90. Epub Nov 22, 2007.
34 Vale ML, Marques JB, Moreira CA, et al. Antinocice-ptive effects of interleukin-4, -10, and -13 on thewrithing response in mice and zymosan-inducedknee joint incapacitation in rats. J Pharmacol ExpTher 2003;304:102–8.
35 Plunkett JA, Yu CG, Easton JM, Bethea JR, YezierskiRP. Effects of interleukin-10 (IL-10) on pain behaviorand gene expression following excitotoxic spinal cordinjury in the rat. Exp Neurol 2001;168(1):144–54.
36 Jiang CL, Xu D, Lu CL, et al. Interleukin-2: Structuraland biological relatedness to opioid peptides. Neu-roimmunomodulation 2000;8(1):20–4.
818
Kumar et al.

37 Wang Y, Pei G, Cai YC, et al. Human interleukin-2could bind to opioid receptor and induce corre-sponding signal transduction. Neuroreport 1996;8(1):11–4.
38 Song P, Zhao Z. Interleukin 2-induced antinocicep-tion partially coupled with mu receptor. Cytokine2000;12(8):1240–2.
39 Hart PH, Vitti GF, Burgess DR, et al. Potential antiin-flammatory effects of interleukin 4: Suppression ofhuman monocyte tumor necrosis factor alpha, inter-leukin 1, and prostaglandin E2. Proc Natl Acad Sci US A 1989;86(10):3803–7.
40 Borderie D, Hilliquin P, Hernvann A, et al. Inhibition ofinducible NO synthase by TH2 cytokines and TGFbeta in rheumatoid arthritic synoviocytes: Effects onnitrosothiol production. Nitric Oxide 2002;6(3):271–82.
41 Cunha FQ, Poole S, Lorenzetti BB, Veiga FH, FerreiraSH. Cytokine-mediated inflammatory hyperalgesialimited by interleukin-4. Br J Pharmacol 1999;126(1):45–50.
42 Watkins LR, Hutchinson MR, Ledeboer A, et al. Gliaas the “bad guys”: Implications for improving clinicalpain control and the clinical utility of opioids. BrainBehav Immun 2007;21(2):131–46.
43 Wieseler-Frank J, Maier SF, Watkins LR. Glial activa-tion and pathological pain. Neurochem Int 2004;45(2–3):389–95.
44 Yan P, Li Q, Kim GM, et al. Cellular localization oftumor necrosis factor-alpha following acute spinalcord injury in adult rats. J Neurotrauma 2001;18(5):563–8.
45 Yang L, Blumbergs PC, Jones NR, et al. Earlyexpression and cellular localization of proinflamma-tory cytokines interleukin-1beta, interleukin-6, andtumor necrosis factor-alpha in human traumaticspinal cord injury. Spine 2004;29(9):966–71.
46 Verge GM, Milligan ED, Maier SF, et al. Fractalkine(CX3CL1) and fractalkine receptor (CX3CR1) distri-bution in spinal cord and dorsal root ganglia underbasal and neuropathic pain conditions. Eur J Neuro-sci 2004;20(5):1150–60.
47 Zhuang ZY, Kawasaki Y, Tan PH, et al. Role of theCX3CR1/p38 MAPK pathway in spinal microglia forthe development of neuropathic pain following nerveinjury- induced cleavage of fractalkine. Brain BehavImmun 2007;21(5):642–51.
48 Wu J, Fang L, Lin Q, Willis WD. Nitric oxide synthasein spinal cord central sensitization following intrader-mal injection of capsaicin. Pain 2001;94(1):47–58.
49 Malmberg AB, Yaksh TL. Hyperalgesia mediated byspinal glutamate or substance P receptor blocked byspinal cyclooxygenase inhibition. Science 1992;257(5074):1276–9.
50 Dumuis A, Sebben M, Haynes L, Pin JP, Bockaert J.NMDA receptors activate the arachidonic acidcascade system in striatal neurons. Nature 1988;336(6194):68–70.
51 Svensson CI, Yaksh TL. The spinal phospholipase-cyclooxygenase-prostanoid cascade in nociceptiveprocessing. Annu Rev Pharmacol Toxicol 2002;42:553–83.
52 Sandman CA, Kastin AJ. Intraventricular administra-tion of MSH induces hyperalgesia in rats. Peptides1981;2(2):231–3.
53 Plantinga LC, Verhaagen J, Edwards PM, et al.Expression of the pro-opiomelanocortin gene indorsal root ganglia, spinal cord and sciatic nerve aftersciatic nerve crush in the rat. Brain Res Mol Brain Res1992;16(1–2):135–42.
54 Van der Kraan M, Tatro JB, Entwistle ML, et al.Expression of melanocortin receptors and pro-opiomelanocortin in the rat spinal cord in relation toneurotrophic effects of melanocortins. Brain Res MolBrain Res 1999;63(2):276–86.
55 Vrinten DH, Kalkman CJ, Adan RA, Gispen WH. Neu-ropathic pain: A possible role for the melanocortinsystem? Eur J Pharmacol 2001;429(1–3):61–9.
56 Klusa V, Germane S, Svirskis S, Wikberg JE. Thegamma(2)-MSH peptide mediates a central analgesiceffect via a GABA-ergic mechanism that is indepen-dent from activation of melanocortin receptors. Neu-ropeptides 2001;35(1):50–7.
57 Starowicz K, Obara I, Przewłocki R, Przewlocka B.Inhibition of morphine tolerance by spinal melanocor-tin receptor blockade. Pain 2005;117(3):401–11.
58 Kalange AS, Kokare DM, Singru PS, et al. Centraladministration of selective melanocortin 4 receptorantagonist HS014 prevents morphine tolerance andwithdrawal hyperalgesia. Brain Res 2007;1181:10–20.
59 Comb M, Seeburg PH, Adelman J, Eiden L, HerbertE. Primary structure of the human Met- and Leu-enkephalin precursor and its mRNA. Nature 1982;295(5851):663–6.
60 Wilson SP, Yeomans DC, Bender MA, et al.Antihyperalgesic effects of infection with apreproenkephalin-encoding herpes virus. Proc NatlAcad Sci U S A 1999;96(6):3211–6.
819
Gene Therapy of Pain

61 Pohl M, Ballet S, Collin E, et al. Enkephalinergic anddynorphinergic neurons in the spinal cord and dorsalroot ganglia of the polyarthritic rat—In vivo releaseand cDNA hybridization studies. Brain Res 1997;749(1):18–28.
62 Stein C, Millan MJ, Shippenberg TS, Peter K, Herz A.Peripheral opioid receptors mediating antinocicep-tion in inflammation. Evidence for involvement of mu,delta and kappa receptors. J Pharmacol Exp Ther1989;248(3):1269–75.
63 Rittner HL, Labuz D, Richter JF, et al. CXCR1/2ligands induce p38 MAPK-dependent translocationand release of opioid peptides from primary granulesin vitro and in vivo. Brain Behav Immun 2007;21(8):1021–32.
64 Young WS 3rd, Wamsley JK, Zarbin MA, Kuhar MJ.Opioid receptors undergo axonal flow. Science1980;210(4465):76–8.
65 Gardell LR, Wang R, Burgess SE, et al. Sustainedmorphine exposure induces a spinal dynorphin-dependent enhancement of excitatory transmitterrelease from primary afferent fibers. J Neurosci2002;22(15):6747–55.
66 Ali Z, Raja SN, Wesselmann U, et al. Intradermalinjection of norepinephrine evokes pain in patientswith sympathetically maintained pain. Pain 2000;88(2):161–8.
67 Chabal C, Jacobson L, Russell LC, Burchiel KJ. Painresponse to perineuromal injection of normal saline,epinephrine, and lidocaine in humans. Pain 1992;49(1):9–12.
68 Choi B, Rowbotham MC. Effect of adrenergic recep-tor activation on post-herpetic neuralgia pain andsensory disturbances. Pain 1997;69(1–2):55–63.
69 Kress M, Fickenscher H. Infection by humanvaricella-zoster virus confers norepinephrine sensitiv-ity to sensory neurons from rat dorsal root ganglia.FASEB J 2001;15(6):1037–43.
70 Dogrul A, Uzbay IT. Topical clonidine antinociception.Pain 2004;111(3):385–91.
71 Obata H, Li X, Eisenach JC. Alpha2-adrenoceptoractivation by clonidine enhances stimulation-evokedacetylcholine release from spinal cord tissue afternerve ligation in rats. Anesthesiology 2005;102(3):657–62.
72 Martins I, Costa-Araújo S, Fadel J, et al. Reversal ofneuropathic pain by HSV-1-mediated decrease ofnoradrenaline in a pain facilitatory area of the brain.Pain 2010;151(1):137–45.
73 Zhang GW, Yang CX, Zhang D, et al. Noradrenergicmechanism involved in the nociceptive modulation ofnociceptive-related neurons in the caudate putamen.Neurosci Lett 2010;480(1):59–63.
74 Moore KA, Kohno T, Karchewski LA, et al. Partialperipheral nerve injury promotes a selective loss ofGABAergic inhibition in the superficial dorsal horn ofthe spinal cord. J Neurosci 2002;22(15):6724–31.
75 Soghomonian JJ, Martin DL. Two isoforms ofglutamate decarboxylase: Why? Trends PharmacolSci 1998;19(12):500–5.
76 Zimmermann M. Pathobiology of neuropathic pain.Eur J Pharmacol 2001;429(1–3):23–37.
77 Aurilio C, Pota V, Pace MC, Passavanti MB, BarbarisiM. Ionic channels and neuropathic pain: Physiopa-thology and applications. J Cell Physiol 2008;215(1):8–14.
78 Devor M. Sodium channels and mechanisms of neu-ropathic pain. J Pain 2006;7(1 suppl 1):S3–12.
79 Chattopadhyay M, Mata M, Fink DJ. Continuousdelta-opioid receptor activation reduces neuronalvoltage-gated sodium channel (NaV1.7) levelsthrough activation of protein kinase C in painful dia-betic neuropathy. J Neurosci 2008;28(26):6652–8.
80 Jani A, Menichella D, Jiang H, et al. Modulation ofcell-mediated immunity prolongs adenovirus-mediated transgene expression in sciatic nerve. HumGene Ther 1999;10(5):787–800.
81 Burton EA, Fink DJ, Glorioso JC. Gene delivery usingherpes simplex virus vectors. DNA Cell Biol 2002;21(12):915–36.
82 Glorioso JC, DeLuca NA, Fink DJ. Development andapplication of herpes simplex virus vectors for humangene therapy. Annu Rev Microbiol 1995;49:675–710.
83 Tenser RB. Role of herpes simplex virus thymidinekinase expression in viral pathogenesis and latency.Intervirology 1991;32(2):76–92.
84 Hamilton DL, Abremski K. Site-specific recombina-tion by the bacteriophage P1 lox-Cre system. Cre-mediated synapsis of two lox sites. J Mol Biol 1984;178(2):481–6.
85 Pohl M, Braz J. Gene therapy of pain: Emergingstrategies and future directions. Eur J Pharmacol2001;429(1–3):39–48.
86 Hao S, Mata M, Glorioso JC, Fink DJ. HSV-mediatedexpression of interleukin-4 in dorsal root ganglionneurons reduces neuropathic pain. Mol Pain 2006;2:6.
820
Kumar et al.

87 Gu Y, Xu Y, Li GW, Huang LY. Remote nerve injectionof mu opioid receptor adeno-associated viral vectorincreases antinociception of intrathecal morphine. JPain 2005;6(7):447–54.
88 Storek B, Harder NM, Banck MS, et al. Intrathecallong-term gene expression by self-complementaryadeno-associated virus type 1 suitable for chronicpain studies in rats. Mol Pain 2006;2:4.
89 Storek B, Reinhardt M, Wang C, et al. Sensoryneuron targeting by self-complementary AAV8 vialumbar puncture for chronic pain. Proc Natl Acad SciU S A 2008;105(3):1055–60.
90 Pohl M, Fink DJ. A new player in gene therapy forpain. Gene Ther 2008;15:953–4.
91 Russell DW, Miller AD. Foamy virus vectors. J Virol1996;70:217–22.
92 Liu W, He X, Cao Z, et al. Efficient therapeutic geneexpression in cultured rat hippocampal neuronsmediated by human foamy virus vectors: A potentialfor the treatment of neurological diseases. Intervirol-ogy 2005;48(5):329–35.
93 Mergia A, Chari S, Kolson DL, Goodenow MM, Cic-carone T. The efficiency of simian foamy virus vectortype-1 (SFV-1) in nondividing cells and in humanPBLs. Virology 2001;280(2):243–52.
94 Lochelt M, Muranyi W, Flugel RM. Human foamyvirus genome possesses an internal, Bel-1-dependent and functional promoter. Proc Natl AcadSci U S A 1993;90:7317–21.
95 Abdallah B, Sachs L, Demeneix BA. Non-viral genetransfer: Applications in developmental biology andgene therapy. Biol Cell 1995;85(1):1–7.
96 Milligan ED, Soderquist RG, Malone SM, et al.Intrathecal polymer-based interleukin-10 gene deliv-ery for neuropathic pain. Neuron Glia Biol 2006;2(4):293–308.
97 Remy JS, Kichler A, Mordvinov V, Schuber F, BehrJP. Targeted gene transfer into hepatoma cells withlipopolyamine-condensed DNA particles presentinggalactose ligands: A stage toward artificial viruses.Proc Natl Acad Sci U S A 1995;92(5):1744–8.
98 Tu Y, Kim JS. A fusogenic segment of glycoprotein Hfrom herpes simplex virus enhances transfection effi-ciency of cationic liposomes (abstract). J Gene Med2008;10(6):646–54.
99 Antunes Bras JM, Epstein AL, Bourgoin S, et al.Herpes simplex virus 1-mediated transfer of pre-proenkephalin A in rat dorsal root ganglia. J Neuro-chem 1998;70(3):1299–303.
100 Thompson RL, Cook ML, Devi-Rao GB, Wagner EK,Stevens JG. Functional and molecular analyses ofthe avirulent wild-type herpes simplex virus type 1strain KOS. J Virol 1986;58(1):203–11.
101 Finegold AA, Mannes AJ, Iadarola MJ. A paracrineparadigm for in vivo gene therapy in the centralnervous system: Treatment of chronic pain. HumGene Ther 1999;10(7):1251–7.
102 Yeomans DC, Lu Y, Laurito CE, et al. Recombinantherpes vector-mediated analgesia in a primate modelof hyperalgesia. Mol Ther 2006;13(3):589–97.
103 Zhang G, Mohammad H, Peper BD, et al. Enhancedperipheral analgesia using virally mediated genetransfer of the mu-opioid receptor in mice. Anesthe-siology 2008;108(2):305–13.
104 Xu Y, Gu Y, Xu GY, et al. Adeno-associated viraltransfer of opioid receptor gene to primary sensoryneurons: A strategy to increase opioid antinocicep-tion. Proc Natl Acad Sci U S A 2003;100(10):6204–9.
105 Navarro V, Millecamps S, Geoffroy M-C, et al. Effi-cient gene transfer and long-term expression inneurons using a recombinant adenovirus with aneuron-specific promoter. Gene Ther 1999;6(11):1884–92.
106 Hao S, Mata M, Glorioso JC, Fink DJ. Gene transferto interfere with TNFalpha signaling in neuropathicpain. Gene Ther 2007;14(13):1010–6.
107 Eissner G, Kolch W, Scheurich P. Ligands workingas receptors: Reverse signaling by members of theTNF superfamily enhance the plasticity of theimmune system. Cytokine Growth Factor Rev 2004;15(5):353–66.
108 Oligino T, Ghivizzani S, Wolfe D, et al. Intra-articulardelivery of a herpes simplex virus IL-1Ra gene vectorreduces inflammation in a rabbit model of arthritis.Gene Ther 1999;6(10):1713–20.
109 Milligan ED, Sloane EM, Langer SJ, et al. Repeatedintrathecal injections of plasmid DNA encodinginterleukin-10 produce prolonged reversal of neuro-pathic pain. Pain 2006;126(1–3):294–308.
110 Ledeboer A, Jekich BM, Sloane EM, et al. Intrathecalinterleukin-10 gene therapy attenuates paclitaxel-induced mechanical allodynia and proinflammatorycytokine expression in dorsal root ganglia in rats.Brain Behav Immun 2007;21(5):686–98.
111 Yao MZ, Gu JF, Wang JH, et al. Adenovirus-mediated interleukin-2 gene therapy of nociception.Gene Ther 2003;10(16):1392–9.
821
Gene Therapy of Pain

112 Yao MZ, Wang JH, Gu JF, et al. Interleukin-2 genehas superior antinociceptive effects when deliveredintrathecally. Neuroreport 2002;13(6):791–4.
113 Hao S, Mata M, Wolfe D, et al. V-mediated genetransfer of the glial cell-derived neurotrophic factorprovides an antiallodynic effect on neuropathic pain.Mol Ther 2003;8(3):367–75.
114 Natsume A, Mata M, Wolfe D, et al. Bcl-2 and GDNFdelivered by HSV-mediated gene transfer after spinalroot avulsion provide a synergistic effect. J Neu-rotrauma 2002;19(1):61–8.
115 Liu J, Tai C, de Groat WC, et al. Release of GABAfrom sensory neurons transduced with a GAD67-expressing vector occurs by non-vesicular mecha-nisms. Brain Res 2006;1073–1074:297–304.
116 Liu J, Wolfe D, Hao S, et al. Peripherally deliveredglutamic acid decarboxylase gene therapy for spinalcord injury pain. Mol Ther 2004;10(1):57–66.
117 Hao S, Mata M, Wolfe D, et al. Gene transfer ofglutamic acid decarboxylase reduces neuropathicpain. Ann Neurol 2005;57(6):914–8.
118 Lee JY, Fink DJ, Mata M. Vector-mediated genetransfer to express inhibitory neurotransmitters indorsal root ganglion reduces pain in a rodent modelof lumbar radiculopathy. Spine 2006;31(14):1555–8.
119 Liu W, Liu Z, Liu L, et al. A novel human foamy virusmediated gene transfer of GAD67 reduces neuro-pathic pain following spinal cord injury. Neurosci Lett2008;432(1):13–8.
120 Tzabazis AZ, Pirc G, Votta-Velis E, et al. Antihyperal-gesic effect of a recombinant herpes virus encodingantisense for calcitonin gene-related peptide. Anes-thesiology 2007;106(6):1196–203.
121 Cheli V, Adrover M, Blanco C, et al. Knocking-downthe NMDAR1 subunit in a limited amount of neuronsin the rat hippocampus impairs learning. J Neuro-chem 2006;97(suppl 1):68–73.
122 Menard DP, van Rossum D, Kar S, et al. A calcitoningene-related peptide receptor antagonist prevents
the development of tolerance to spinal morphineanalgesia. J Neurosci 1996;16(7):2342–51.
123 Yeomans DC, Levinson SR, Peters MC, et al.Decrease in inflammatory hyperalgesia by herpesvector-mediated knockdown of Nav1.7 sodiumchannels in primary afferents. Hum Gene Ther 2005;16(2):271–7.
124 Kolls J, Peppel K, Silva M, Beutler B. Prolonged andeffective blockade of tumor necrosis factor activitythrough adenovirus-mediated gene transfer. ProcNatl Acad Sci U S A 1994;91(1):215–9.
125 Varley AW, Munford RS. Physiologically responsivegene therapy. Mol Med Today 1998;4(10):445–51.
126 Van de Loo FA. Inflammation-responsive promotersfor fine-tuned gene therapy in rheumatoid arthritis.Curr Opin Mol Ther 2004;6(5):537–45.
127 Mata M, Fink DJ. Gene therapy for pain. Anesthesi-ology 2007;106:1079–80.
128 Wolfe D, Wechuck J, Krisky D, Mata M, Fink DJ. Aclinical trial of gene therapy for chronic pain. PainMed 2009;10(7):1325–30.
129 Wolfe D, Mata M, Fink DJ. A human trial of HSV-mediated gene transfer for the treatment of chronicpain. Gene Ther 2009;16(4):455–60.
130 Evans CH, Robbins PD, Ghivizzani SC, et al. Genetransfer to human joints: Progress toward a genetherapy of arthritis. Proc Natl Acad Sci U S A 2005;102(24):8698–703.
131 Wehling P, Reinecke J, Baltzer AA, et al. Clinicalresponses to gene therapy in joints of two subjectswith rheumatoid arthritis. Hum Gene Ther 2009;20:97–101.
132 Evans CH, Ghivizzani SC, Robbins PD. Arthritis genetherapy’s first death. Arthritis Res Ther 2008;10(3):110.
133 Hacein-Bey-Abina S, von Kalle C, Schmidt M, et al. Aserious adverse event after successful gene therapyfor X-linked severe combined immunodeficiency. NEngl J Med 2003;348(3):255–6.
822
Kumar et al.