
The Health and Social Security Act 1984 and the price of spectacles among corporate practices in the...
11
Invited Review The Health and Social Security Act 1984 and the price of spectacles among corporate practices in the United Kingdom (1980–2007): a review Richard Calver 1,2 1 Department of Optometry and Ophthalmic Dispensing, Anglia Ruskin University, East Road, Cambridge, and 2 Vision and Eye Research Unit, Postgraduate Medical Institute, Anglia Ruskin University, East Road, Cambridge, UK Abstract The Health and Social Security Act 1984 deregulated certain aspects of optometry in the United Kingdom, including advertising and the supply of spectacles, in the hope that greater competition would reduce spectacle prices. The effects of this legislation are tested by plotting the mean prices of private spectacles purchased from corporate optometric practices, from 1980 to 2007. Historical evidence is used to gauge the effect on prices of other factors such as National Health Service (NHS) payments, sight test fees and pressure exerted by consumer organisations. The high prices in 1980 reduced markedly throughout the rest of the 1980s, remained low for most of the 1990s and rose between 1999 and 2003, before falling. Changes in price were associated with changes to the system of NHS payments and variations in private sight test fees, but prices have generally been lower since the deregulation of dispensing than they were before. Although the price of private spectacles remains heavily influenced by other factors, the deregulation of opticiansÕ services has benefited the public by maintaining lower prices, as intended by proponents of the legislation. Keywords: deregulation, Health and Social Security Act, ophthalmic dispensing, spectacles Introduction Optometry in the United Kingdom is regulated by the Opticians Act 1989. Section 21 of the original Opticians Act 1958 restricted the supply of spectacles to that by, or under the supervision of, registered medical practitio- ners and opticians (Taylor and Austen, 1992), creating a legal monopoly over the sale of spectacles. (The term ÔopticianÕ is used here to encompass both optometrists and dispensing opticians). After a series of consumer reports (ConsumersÕ Association, 1983) and official enquiries (Price Commission, 1976; Office of Fair Trading, 1982) scrutinised opticiansÕ prices in the 1970s and early 1980s, the UK parliament passed the Health and Social Security Act 1984 (see reviews by Brahams, 1984; Taylor, 1986, 1991; Taylor and Austen, 1986, 1992; Fulop and Warren, 1992, 1993). This revoked Section 21, permitting unregistered persons to supply spectacles, except to patients under the age of 16, or to those registered as partially-sighted or blind, effectively ending opticiansÕ monopoly. Section 25, which restricted opticiansÕ advertising, was also amended and the range of spectacles provided by the National Health Service (NHS) was replaced with a system of NHS vouchers, though this reform was not completed until 1986 (Taylor and Austen, 1986, 1992). Parliament hoped that deregulating advertising and dispensing would increase competition within optome- try, encouraging more entrants to the industry, leading to a cheaper and more efficient service (Taylor and Austen, 1986, 1992; Fulop and Warren, 1992, 1993). Opponents of the legislation believed that it would lead to a poorer service, as much dispensing would be Received: 19 May 2009 Revised form: 7 October 2009; 9 November 2009 Accepted: 15 November 2009 Correspondence and reprint requests to: Richard Calver, Department of Optometry and Ophthalmic Dispensing, Anglia Ruskin University, East Road, Cambridge, CB1 1PT, UK. Tel.: +44 0845 196 2506; Fax: +44(0)1223 417712. E-mail address: [email protected] Ophthal. Physiol. Opt. 2010 30: 113–123 ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists doi: 10.1111/j.1475-1313.2009.00709.x
Transcript of The Health and Social Security Act 1984 and the price of spectacles among corporate practices in the...

Invited Review
The Health and Social Security Act 1984 andthe price of spectacles among corporatepractices in the United Kingdom (1980–2007):a review
Richard Calver1,2
1Department of Optometry and Ophthalmic Dispensing, Anglia Ruskin University, East Road,
Cambridge, and 2Vision and Eye Research Unit, Postgraduate Medical Institute, Anglia Ruskin
University, East Road, Cambridge, UK
Abstract
The Health and Social Security Act 1984 deregulated certain aspects of optometry in the United
Kingdom, including advertising and the supply of spectacles, in the hope that greater competition
would reduce spectacle prices. The effects of this legislation are tested by plotting the mean prices of
private spectacles purchased from corporate optometric practices, from 1980 to 2007. Historical
evidence is used to gauge the effect on prices of other factors such as National Health Service (NHS)
payments, sight test fees and pressure exerted by consumer organisations. The high prices in 1980
reduced markedly throughout the rest of the 1980s, remained low for most of the 1990s and rose
between 1999 and 2003, before falling. Changes in price were associated with changes to the
system of NHS payments and variations in private sight test fees, but prices have generally been
lower since the deregulation of dispensing than they were before. Although the price of private
spectacles remains heavily influenced by other factors, the deregulation of opticians� services has
benefited the public by maintaining lower prices, as intended by proponents of the legislation.
Keywords: deregulation, Health and Social Security Act, ophthalmic dispensing, spectacles
Introduction
Optometry in the United Kingdom is regulated by theOpticians Act 1989. Section 21 of the original OpticiansAct 1958 restricted the supply of spectacles to that by, orunder the supervision of, registered medical practitio-ners and opticians (Taylor and Austen, 1992), creating alegal monopoly over the sale of spectacles. (The term�optician� is used here to encompass both optometristsand dispensing opticians). After a series of consumerreports (Consumers� Association, 1983) and officialenquiries (Price Commission, 1976; Office of Fair
Trading, 1982) scrutinised opticians� prices in the1970s and early 1980s, the UK parliament passed theHealth and Social Security Act 1984 (see reviews byBrahams, 1984; Taylor, 1986, 1991; Taylor and Austen,1986, 1992; Fulop and Warren, 1992, 1993). Thisrevoked Section 21, permitting unregistered persons tosupply spectacles, except to patients under the age of 16,or to those registered as partially-sighted or blind,effectively ending opticians� monopoly. Section 25,which restricted opticians� advertising, was alsoamended and the range of spectacles provided by theNational Health Service (NHS) was replaced with asystem of NHS vouchers, though this reform was notcompleted until 1986 (Taylor and Austen, 1986, 1992).
Parliament hoped that deregulating advertising anddispensing would increase competition within optome-try, encouraging more entrants to the industry, leadingto a cheaper and more efficient service (Taylor andAusten, 1986, 1992; Fulop and Warren, 1992, 1993).Opponents of the legislation believed that it would leadto a poorer service, as much dispensing would be
Received: 19 May 2009
Revised form: 7 October 2009; 9 November 2009
Accepted: 15 November 2009
Correspondence and reprint requests to: Richard Calver, Department of
Optometry and Ophthalmic Dispensing, Anglia Ruskin University,
East Road, Cambridge, CB1 1PT, UK.
Tel.: +44 0845 196 2506; Fax: +44(0)1223 417712.
E-mail address: [email protected]
Ophthal. Physiol. Opt. 2010 30: 113–123
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists doi: 10.1111/j.1475-1313.2009.00709.x

undertaken by unregistered personnel, without neces-sarily reducing prices (e.g. Federation of IndependentBritish Optometrists, 1983; Scott, 1983; Trybuchowski,1983; Taylor, 1986). For summaries of proponents� andopponents� views see Brahams (1984) and Fulop andWarren (1993).
Even after 25 years the deregulation of spectacledispensing, perhaps the most contentious reform, con-tinues to frustrate opticians. Baker (1983) was opposedto the legislation at the time and, when interviewed over20 years later, still regarded it as �foolish� (Johnson,2006). Pike (2006) and Hunt (2007) claim that thelegislation acted against the interests of consumers.Longhurst (2007a,b) believes that only registered dis-pensing opticians should be permitted to dispensespectacles, claiming that poorly fitted spectacles endan-ger the wearer and have caused amblyopia in children(Longhurst, 2007b). Longhurst failed to substantiate hisassertion that amblyopia had been caused by inaccuratedispensing, and his opinions appear naı̈ve to othercommentators (Little, 2007), but these comments illus-trate a perception among opticians that the deregulationof spectacle dispensing has led to the sale of poor qualityspectacles. The College of Optometrists and the Asso-ciation of British Dispensing Opticians still advise theirmembers that spectacles should be supplied by, or underthe supervision of, a registered optician even though thisis no longer legally necessary (Association of BritishDispensing Opticians, 2008; College of Optometrists,2009). Nevertheless, other commentators regard thelegislation as exemplifying the beneficial effects ofcompetition in the health sector (Spiers, 2003).
Despite the enduring interest in this legislation,surprisingly few studies have investigated its effects.Taylor (1986, 1991) considered its potential conse-quences but did not examine its actual effects. Fulopand Warren (1992, 1993) studying the variation inspectacle prices from 1981 to 1990, observed a reductionin prices �in real terms� post-deregulation and concludedthat deregulation had benefited the public withoutundermining standards of service. Davies et al. (2004)and Davies and Olczak (2006) were more cautious. Theyobserved a short-term reduction in prices, followed by asmall increase, and concluded that it was not possible toprove an obvious long-term benefit. These studies(Fulop and Warren, 1992, 1993; Davies et al., 2004;Davies and Olczak, 2006) made the interesting pointthat prices had begun to fall in the 2 years immediatelybefore deregulation, suggesting that other factors causedthis price reduction, but neither study provided asatisfactory explanation. Fulop and Warren (1992,1993) attributed it to a combination of back-datedpayments from the NHS in 1982 and 1983, whichpermitted opticians to lower the prices of their privatespectacles, and their eagerness to reduce prices in
anticipation of the increased competition from deregu-lation, but provided no evidence to substantiate theseideas. Davies et al. (2004) concurred, again withoutgiving evidence.
Price variations are hard to explain without consid-ering the broad range of factors that might haveinfluenced opticians� prices. This review examines thefactors affecting the price of private spectacles from1980 to 2007. Historical evidence is presented ofopticians� views on NHS funding and the threat ofderegulation in the early 1980s: these clarify the reasonsunderlying the pre-deregulation drop in prices, as well asthe impact of NHS fees and the prevailing economicclimate, on private prices. In contrast to Davies et al.(2004), who ignored these factors, it will be argued thatthere is good evidence that the deregulation of spectacledispensing has benefited the public by constraining pricerises.
Variation in the price of private spectacles
As deregulation was primarily aimed at reducing theprice of spectacles (Taylor and Austen, 1986), itssuccess can be tested by comparing prices of spectaclesbefore and since the amendments took effect. TheFederation of Optical Corporate Bodies (FOCB) and itssuccessor the Federation of Ophthalmic and DispensingOpticians (FODO) have published spectacle price dataannually since 1982 (FOCB, 1982–1985; FODO, 1986–2008), and older surveys include data for 1980 and 1981(FOCB, 1982). The surveys are based on analyses ofbetween 2.5 million (FOCB, 1982) and 5.5 million(FODO, 2002) sight tests conducted by members ofFOCB and FODO, i.e. the corporate sector, whichconsists of national chains of opticians, and excludesindependent practices. Although the surveys do notrepresent all types of optometric practice, the corporatesector is large, rising from 45% (FOCB, 1982) to 75%(FODO, 2007) of the optometric market during theperiod under consideration. These surveys have beenused before by academic researchers (Fulop and War-ren, 1992, 1993; Davies et al., 2004; Davies and Olczak,2006) and market researchers (Euromonitor, 1985; KeyNote, 2008).
Figure 1 shows the mean prices of private spectaclessupplied for each year from 1980 to 2007. Value AddedTax (VAT) was imposed on spectacles at a rate of 15%in 1988 and 17.5% in 1991 (FODO, 1988–1993), andFigure 1 depicts prices including and excluding VAT.There is a clear upward trend in prices, but a realisticview of price changes must consider the effects ofinflation. Figure 2 shows the rate of inflation asmeasured by the Retail Price Index (RPI) for each yearunder review (Office for National Statistics, 2008). TheRPI for a particular year expresses the price of goods as
114 Ophthal. Physiol. Opt. 2010 30: No. 2
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

a percentage increase or decrease from the price at thesame point in the previous year. This information can beused to compare the actual price changes with theirchange in �real terms�, i.e. after inflation has beenconsidered, which allows the prices of spectacles to becompared with those of other goods. Initial surveyscover the calendar year, but from 1989/90 surveys(FODO, 1990), covered the financial year (April toMarch). This introduces uncertainty to the followinganalysis because monthly fluctuations in the RPI causeits value calculated over the calendar year to differ fromthat calculated over the financial year. However, thisdifference is small: the largest difference in the yearsunder review was 1.5% in 1980/81.Figure 3 plots the variation in price in real terms with
respect to a 1983 baseline using a method similar to that
adopted by Davies et al. (2004) as described in theAppendix. It expresses the actual price of spectacles in aparticular year in terms of the amount by which itexceeds the inflated price, as a percentage proportion ofthe inflated price. Inflation is cumulative, so any inflatedprice must be considered with respect to a baseline priceinflated by the RPI year-on-year. The year 1983 hasbeen chosen as the baseline because this is the last fullyear before the Health and Social Security Act 1984 wasenacted. Any subsequent change in the graph will showthe price changes with respect to the last year in whichspectacles were supplied under full regulation. A nega-tive data point indicates that the actual price was lowerthan the inflated price. Figure 3 shows that the price ofspectacles fell in real terms after deregulation and thatthe price remained below inflation up to and including
Figure 1. Variation in the mean price of private spectacles purchased from 1980 to 2007 using data taken from FOCB (1982–1985) and FODO
(1986–2008). Note that Value Added Tax (VAT) was imposed on spectacles from 1988.
Figure 2. Variation in the Retail Price Index (RPI) from 1980 to 2007 using data taken from the Office for National Statistics (2008).
Deregulation and spectacle prices: R. Calver 115
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

the year 1999. The fall was particularly pronounced inthe years between 1984 and 1990: the price of spectaclesin 1990 was 24% lower than that predicted by inflationfrom 1983 to 1990. After a rise in 1990, prices from 1991to 1999 remained stable but still lay 6–8% below theinflated price, apart from the year beginning 1996 whichappears anomalous. Between 2000 and 2005 the actualprice exceeded the inflated price, as noted before (Davieset al., 2004), but the actual price has been declining since2003.
The low post-deregulation prices do not necessarilyindicate a causative effect. Figure 3 lacks a clear trendand also shows that prices were falling with respect toinflation even before deregulation took place, asobserved before (Fulop and Warren, 1992, 1993; Davieset al., 2004). This observation can be interpreted indifferent ways. One argument, advanced by opticians inthe years immediately following deregulation (FODO,1986), is that prices were already falling and thatderegulation was not beneficial, merely maintaining anestablished effect. A counter-argument is that priceswere indeed falling by 1983, but from a level which wasalready too high because of the opticians� monopolywhich then existed. Prices were approaching a morerealistic level by 1983 and were prevented from return-ing to such high levels when deregulation was imple-mented, proving its value. For example, had the changein prices between 1980 and 1983 exactly matchedinflation, the 1983 price of £56.39 would have beenreached if spectacles had been priced at £44.36 in 1980:in fact, the mean price in 1980 was 23% higher at£54.71.
This controversy is important. If the cause of the pre-1983 fall can be identified, the likelihood that deregu-lation benefited the consumer can be established withgreater confidence. The data in Figure 3 give some
support to the view that deregulation was beneficial. Theprice in 1983 was 19% lower than that in 1980 in realterms; by 1985 it was as much as 35% lower than 1980 inreal terms, and it remained lower than the inflated priceuntil the end of the 1990s. The drop in prices just before1983 was mainly due to a particularly marked fallbetween 1981 and 1982 when the price fell by approx-imately 15% in real terms, supported by two smallerfalls of less than 4% (Figure 3). In contrast, the realterms price often fell by more than 5% in the mid- tolate-1980s and sometimes by more than 10%. Pricesonly began to rise regularly from 1998, but havedecreased since 2003. These figures hint that lowerprices have been normal since 1983 and that deregula-tion probably prevented excessive price rises until thelate 1990s. Overall, prices fell in real terms in nine of the15 years from 1983 to 1998 and have fallen each yearsince 2003, and this seems to support the argument thatderegulation has generally been associated with lowerprices.
However, this support remains weak because there isno price data prior to 1980 and because the cause of thepre-1983 fall remains uncertain. Previous work hasclaimed that private prices in the early 1980s were usedto subsidise the low payments made by the NHS (Fulopand Warren, 1992, 1993; Davies et al., 2004). Thisimplies that private prices were artificially high in theearly 1980s, and that an increase in NHS paymentscould reduce the need for a subsidy, allowing privateprices to fall. There is some evidence that prices from1980 to 1982 were particularly high. Figure 1 shows thatactual prices fell between 1981 and 1983, even withoutconsidering inflation. This is surprising because theprices of commodities would usually be expected to rise,especially at times of high inflation. Perhaps the 1981price of £59.26 was unusually high and a fall was likely
Figure 3. Variation in the mean price of private spectacles purchased from 1980 to 2007 with respect to inflation at 1983 baseline. The horizontal
line at y = 0 indicates a price varying in line with inflation.
116 Ophthal. Physiol. Opt. 2010 30: No. 2
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

after opticians received increased fees for NHS work in1982, backdated to 1978: Fulop and Warren (1992,1993) believed that this explained the fall in pricesbetween 1981 and 1983, but provided no evidence.However, an earlier investigation by the Price Commis-sion reported that the prices of private spectacles in themid-1970s were �higher than they needed to be�, partlybecause of a lack of competition in the industry but alsobecause NHS dispensing was �insufficiently rewarded�(Price Commission, 1976). To gauge fully the effects ofderegulation on the price of spectacles, and to explainwhat drove opticians to change their prices, it isnecessary to examine some of the history of the yearsimmediately preceding the deregulation of spectacledispensing, paying attention to other factors that mighthave influenced spectacle prices and to the contempo-rary views and actions of opticians.
General economic conditions
The British economy lay in recession between 1979 and1981 (Cairncross, 1994; Pemberton, 2005). Inflation(Figure 2) and unemployment were high during thisperiod (Cairncross, 1994; Pemberton, 2005) and con-sumer spending was low, falling by £0.8 billion between1979 and 1981 (Worswick, 1984; Cairncross, 1994).These economic problems may have influenced spectaclepurchases in the early 1980s (Euromonitor, 1985) andare relevant to this review because the data collected byFODO records the mean amount of money spent onspectacles, not the mean price of a �standard� pair ofspectacles. The 1980–1983 fall in Figure 3 might bepartly caused by the public, concerned about theeconomic climate, choosing cheaper spectacles. Thislatter explanation seems more plausible than the alter-native, i.e. that opticians lowered their prices at a time ofhigh inflation. Figure 1 shows that the actual prices ofprivate spectacles increased slightly by about 3%between 1980 and 1983: the apparently large fall shownin Figure 3 is partly due to the high inflation between1980 and 1983.
The Effect of NHS Payments
By the end of 1982, inflation was falling close to the levelat which it would remain for most of the 1980s, andincome increased markedly (Muellbauer and Murphy,1997). These conditions encouraged higher consumerspending (Worswick, 1984; Cairncross, 1994), yetspending on spectacles fell with respect to inflation.The effects of deregulation cannot yet be invoked toexplain this fall, but the system of NHS fees may behighly relevant. In the 1970s and early 1980s, it waspossible to buy spectacles consisting of private framesand lenses, NHS frames and lenses, or private frames
and NHS lenses, with the NHS paying the optician a setfee for NHS work (Office of Fair Trading, 1982). NHSfees had remained unchanged since 1978 (Office of FairTrading, 1982), but were raised in 1982 and 1983, andthe differential was backdated to 1978. Fulop andWarren (1992, 1993) claimed that this increase in NHSpayments lessened the need for a cross-subsidy fromprivate spectacle charges and, although they providedno supporting evidence, their hypothesis should betaken seriously. Editorials in the optometric pressillustrate the importance of NHS payments. For exam-ple the editor of The Optician, when discussing the feesfor a new NHS frame, warned that opticians� represen-tatives would not want �to lumber the profession withanother service for the Government which it mustsubsidise by its private dispensing� (Anon, 1983a).Letters submitted to The Optician also provide strongevidence that opticians reduced their prices in responseto the higher NHS payments. A representative ofDollond and Aitchison, a large corporate optician,explained how the increased payments in 1982 hadalready affected the prices of many private frames:
�Following the increases, in April [1982], of NHSsight test and dispensing payments, our companyimmediately reduced private frame prices by up to20% on over 500 frame styles� (Stone, 1983).Stone also estimated that restricting NHS glasses to
10% of the market (e.g. children and �free category�patients) would allow his company to reduce pricesfurther by approximately 25%. He pointed out that thelow NHS fees had distorted the range of privatespectacle fees and �the shortfall has to be made up onthe higher priced spectacles. […] It has been necessaryfor private sales in the UK to subsidise the NHSshortfall� (Stone, 1983).
Other opticians took similar action when NHSpayments increased further in 1983. One describedforthcoming changes in his prices:
�The recent announcement regarding increased fees,together with back payments, goes some way tocorrect anomalies. Accordingly, we feel that there isnow a real need to express not only satisfaction butalso financial adjustment and as such we areinforming patients as follows:For many years the fees paid for an eye examinationunder the NHS have been grossly inadequate andhave had to be subsidised by additional charges forprivate dispensing, a situation we dislike very much.The Government have now partially accepted thisfact and as from February 1 are increasing Fees.Accordingly as from this date we shall reduce ourprivate charges for spectacles� (Hart, 1983).Hart�s decision to reduce his prices was clearly
prompted by the backdating of NHS fees. He alsoimplies that private fees for spectacles were indeed too
Deregulation and spectacle prices: R. Calver 117
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

high, hence the need to �correct anomalies� by way of�financial adjustment�. If this approach had beenadopted by other opticians, the prices of privatespectacles would have fallen throughout the countryand this could have plausibly explained the reduction ofprices in 1982 and 1983. However, opticians stillbelieved that the new fees were �unrealistic� (Chappell,1983), maintaining that �even with the latest fees aGeneral Ophthalmic Services (GOS) eye examinationhas to be subsidised by private dispensing� and that�GOS dispensing too has to be further subsidised byprivate dispensing� (Owen, 1983). The prevailing viewwas that these subsidies had led to private patientsinevitably being overcharged, and that this situationwould continue, given the inadequate GOS payments.
These opinions clearly illustrate opticians� view thatpoor NHS fees had led to inflated private fees. Althoughthis might have been unavoidable, it created a situationwhere private fees were particularly high until opticianstook the chance to lower them after receiving higherNHS fees, supporting Fulop and Warren�s (1992, 1993)hypothesis. The effect of backdated payments waspotentially very significant: the Price Commission(1976) had previously estimated that backdating NHSpayments by 2 years could have increased opticians�profit margins by almost 15%, and the Office of FairTrading (1982) would later conclude that private pricescould fall by a similar amount if NHS fees were fairer.
It could be argued that prices in 1980 would have beenlower had NHS fees increased more fairly in the late1970s, and that opticians were not to blame forunavoidable price rises. However, the Office of FairTrading (1982) rejected this notion, identifying a lack ofcompetition as a significant factor. There was alreadyevidence that opticians in the 1970s were, at least tosome extent, charging �what the market would bear�(Price Commission, 1976). These observations suggestthat prices would have risen, even if NHS fees hadincreased in the later 1970s.
Changes to the NHS payments system
Since low NHS fees in the 1970s and early 1980s had ledto high private spectacle prices, and a large increase inNHS fees led to a fall in private prices, it is instructive toexamine the changes in NHS fees in the years since 1984.
In July 1986, NHS spectacles were replaced with NHSvouchers which contributed a fixed value towards thecost of a pair of private spectacles (Taylor and Austen,1992). Some authors seem to have regarded the vouchersystem as a continuation of the NHS system (Davieset al., 2004), but this interpretation is incorrect: vouch-ers broke down the barrier between NHS and privatespectacles (Spiers, 2003), allowing patients to buyprivate spectacles at a lower price whilst enabling the
optician to receive the same payment. Since this effec-tively meant that all spectacles were now privatelypurchased, the voucher system should obviate the needfor private spectacles to subsidise the perceived lowNHS fees (since there are now no NHS fees), avoidinghigh private prices. This contrasts with the situation in1981, when only 30% of dispensing was private (Officeof Fair Trading, 1982), and Stone (1983) probably hadthis in mind when he recommended limiting NHSspectacles to specific types of patients. The introductionof vouchers is therefore likely to have played a part inpreventing high private charges.
The Health and Medicines Act 1988 abolished NHSsight tests for many patients from April 1989 (Taylorand Austen, 1992), and opticians introduced privatecharges for sight tests. The variation in NHS andprivate sight test fees are shown in Figure 4, and theirvariations in real terms are shown in Figure 5 whichdepicts the data using a similar method to that used forFigure 3, assuming a 1989 baseline. NHS sight test feeshave risen very slightly in real terms, but rises in privatesight test fees have tended to lag well behind inflation,particularly between 2003 and 2005 when the private feelay more than 10% below the inflated fee. Althoughprivate fees actually remain higher than NHS fees,opticians generally believe that neither NHS nor privatesight tests are adequately funded (FODO, 2008; Spiers,2003), meaning that sales of spectacles must subsidisethe sight test. Sheinman (2006) estimated that the costof conducting an eye examination lay between £50 and£100 at a time when the mean private fee was £21.10(Figure 4; FODO, 2007), and claimed that spectacleprices could be reduced if this cost were met in full.Other opticians were vocal in criticising �the ludicrouscross-subsidy of inadequate eye examination fees by theovercharging for optical product� (Llewellyn, 2006). It istherefore clear that private spectacle prices are heavilyinfluenced by apparently low sight test fees. The relativereduction in private sight test fees since 1989 might haveled to an increase in spectacle prices, yet Figure 3 showsthat this did not happen. Although sales of privatespectacles subsidise both NHS and private sight tests,the perceived poor sight test remuneration from 1989 todate has not generally been associated with a rise inprivate spectacle prices, apart from the years 1990–1991and 1999–2003. Sight test numbers fell just after theavailability of NHS sight tests was restricted (FODO,1991, 1992) and this could explain the rise in spectaclesprices between 1990 and 1991 since opticians, receivingless income from sight tests, became more dependent onsales of spectacles. The period from 1999 to 2003, whenspectacle prices rose sharply, coincided with the rein-troduction in 1999 of NHS sight tests for certaingroups, which transferred relatively highly remuneratedprivate work to less lucrative NHS work (FODO, 2001;
118 Ophthal. Physiol. Opt. 2010 30: No. 2
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists
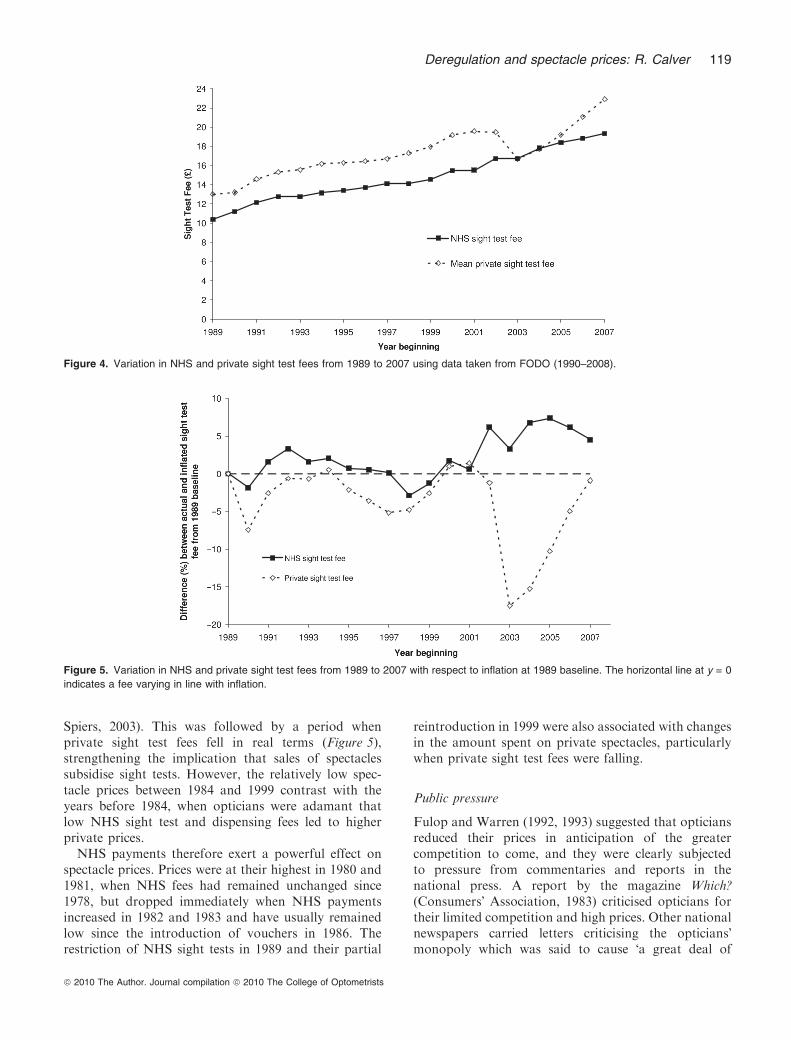
Spiers, 2003). This was followed by a period whenprivate sight test fees fell in real terms (Figure 5),strengthening the implication that sales of spectaclessubsidise sight tests. However, the relatively low spec-tacle prices between 1984 and 1999 contrast with theyears before 1984, when opticians were adamant thatlow NHS sight test and dispensing fees led to higherprivate prices.NHS payments therefore exert a powerful effect on
spectacle prices. Prices were at their highest in 1980 and1981, when NHS fees had remained unchanged since1978, but dropped immediately when NHS paymentsincreased in 1982 and 1983 and have usually remainedlow since the introduction of vouchers in 1986. Therestriction of NHS sight tests in 1989 and their partial
reintroduction in 1999 were also associated with changesin the amount spent on private spectacles, particularlywhen private sight test fees were falling.
Public pressure
Fulop and Warren (1992, 1993) suggested that opticiansreduced their prices in anticipation of the greatercompetition to come, and they were clearly subjectedto pressure from commentaries and reports in thenational press. A report by the magazine Which?(Consumers� Association, 1983) criticised opticians fortheir limited competition and high prices. Other nationalnewspapers carried letters criticising the opticians�monopoly which was said to cause �a great deal of
Figure 5. Variation in NHS and private sight test fees from 1989 to 2007 with respect to inflation at 1989 baseline. The horizontal line at y = 0
indicates a fee varying in line with inflation.
Figure 4. Variation in NHS and private sight test fees from 1989 to 2007 using data taken from FODO (1990–2008).
Deregulation and spectacle prices: R. Calver 119
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

inconvenience and extra cost to the general public�(Wright, 1982). Editorials expressed similar sympathies(Anon, 1982) and these attacks cannot have goneunnoticed by opticians. A commentary in The Opticianreferred to an article in the Yorkshire Evening Newsurging opticians to reflect on their prices before it wastoo late:
�There is precedent in other countries for the sale ofhigh quality spectacles by non-qualified people madeto the requirements of a proper prescription – and atprices much lower than the going rate in this coun-try. While acknowledging the professional servicesoffered by opticians, it has to be said that some ofthem must look to their prices if they are to resist theimplications of the Which report� (�Nemo�, 1983).When the Health and Social Security Bill was
presented to Parliament in November 1983, The Opti-cian published extracts from several national andregional newspapers, many of which sympathised withthe Bill�s proposals. The Daily Telegraph predicted �bigfalls in the price of spectacles�; the Daily Star believedthat the measures would be to �slash prices, which havebeen kept far too high by restrictive trading�; theSheffield Morning Telegraph thought that opticians�prices were �astronomical� (Anon, 1983b). These criti-cisms must have been difficult to ignore and it isplausible that opticians felt sufficiently pressured bythese comments in the general and optometric press toreduce their prices, though I have found no concreteevidence that they actually did so.
Discussion
Considering the effects of public pressure, the generaleconomic climate and opticians� attitudes towards NHSfees, the following observations can be made:(1) By 1980, opticians had resorted to charging high feesfor private spectacles to subsidise inadequate NHSremuneration. The price of private spectacles apparentlyfell between 1980 and 1983, during times of lowconsumer spending and after opticians received higher,backdated NHS payments. These factors plausiblyexplain the price changes. The high inflation between1980 and 1982 also distorts the notion of �real terms� andexaggerates the apparent size of the price fall.(2) Between 1983 and 1986, prices fell further eventhough rising consumer spending and still-inadequateNHS fees might have been expected to result in higherprivate prices. The Health and Social Security Act 1984,with its implications for deregulation of dispensing andadvertising, and modifications to NHS payments, is theonly obvious intervention that might plausibly havecaused prices to fall.(3) From 1986 onwards, opticians have no longerneeded to subsidise NHS spectacle fees by sales of
private spectacles, but they must instead use similarmethods to subsidise their sight tests. However, this hasrarely been associated with a rise in spending on privatespectacles, apart from a period between 1999 and 2003,shortly after NHS sight tests were reintroduced for somepatients and when the private sight test fees fell sharplyin real terms.
Spending on private spectacles fell between 1980 and1983, before deregulation but due to factors largelybeyond opticians� control. Opticians reduced their pricesafter receiving a large windfall from the NHS, and Hart(1983) and Stone (1983) imply that their prices wouldotherwise have remained high. The poor economicconditions of the early 1980s also probably contributedto the low spending in 1981 and 1982. Opticians havecontinued to complain of low NHS payments which,along with the higher consumer spending since the early1980s, would be expected to increase spending onprivate spectacles. This has rarely happened, and it islikely that deregulating advertising and the supply ofspectacles, helped to prevent prices from escalating asthey had previously done, though the level of sight testfees strongly influences spectacle prices and the removalof NHS spectacles has also contributed to the lowprivate prices. The association between spectacle prices,deregulation and NHS fees does not necessarily imply acausal relationship but the Health and Social SecurityAct 1984 seems the only factor that could haveprevented price increases after 1984, given that sales ofspectacles continued to subsidise sight tests.
It is hard to separate the effects of deregulatingspectacle dispensing, deregulating advertising and abol-ishing NHS spectacles. The deregulation of dispensing,but not advertising, would have permitted new compet-itors to enter the market, but would have preventedthem from advertising their services and prices. Permit-ting advertising without the deregulation of dispensingwould have allowed opticians to advertise their services,but would not have introduced more competitors.Several new entrants did emerge in the early 1980s(Euromonitor, 1985) and exploited the relaxation ofadvertising restrictions by promoting innovative pricingstrategies, such as �buy one get one free� offers (Fulopand Warren, 1992), which appear to be important to thepublic (Key Note, 2008) and have since been embracedby the independent sector (Fulop and Warren, 1992).These strategies would have been impossible to imple-ment had advertising remained tightly regulated. There-fore, the deregulation of advertising and dispensing wereclosely linked, as noted by Spiers (2003) and Davieset al. (2004) who regard the deregulation of advertisingas highly important. The abolition of NHS spectacleswas also crucial because it obviated the need for asubsidy from private spectacles and should have helpedprices remain low.
120 Ophthal. Physiol. Opt. 2010 30: No. 2
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

This review demonstrates the usefulness of historicalevidence in examining a variety of factors and clarifyingthe reasons for price fluctuations. Davies et al. (2004)did not exploit this evidence and were unable to examinethe price variations in detail; had they done so, theirconclusions might have been less cautious. There arestill certain limitations. Since the data ignores indepen-dent opticians, the conclusions are applicable only to thecorporate sector. No similar survey of independentpractices has been undertaken, however, and the datareviewed here represents the only long-term, ongoingsurvey of prices amongst UK opticians. Davies et al.(2004) regarded it as the best available data for studyinglong-term price trends. The corporate sector is respon-sible for such a large volume of optometric activity thatthe data are likely to reflect the experience of a largeproportion of the UK spectacle-wearing population,even if it is not necessarily representative of all types ofoptometric practice. Since the data are based on moneyspent on spectacles, rather than the prices of actualspectacles, it could be argued that it fails to reveal thechanges in price of specific types of spectacles. This istrue, but knowledge of the retail price of spectaclesacross the 27 year period covered can only be obtainedfrom practice records stretching back to 1980. Suchrecords must undoubtedly exist, but probably in rathersparse numbers as opticians are advised to retainrecords for only 10 years after they have completedtheir patient�s treatment (College of Optometrists,2009). Even with extensive records, a comparison of�typical� or �standard� spectacles over such a long periodwould be difficult: with advances in spectacle lenstechnology and the growing popularity of progressivepower lenses, aspheric lenses and anti-reflection coat-ings, the �standard� spectacle lens of 1980 might havebeen very different to that supplied in 2007. The meanprice paid by patients therefore seems a reasonablemeasure of spectacle prices over time. If more techno-logically advanced lenses now make up a higherproportion of lenses supplied, the absence of an obviousprice increase suggests that a quality-adjusted price,accounting for more advanced lenses, might actuallyshow a downward trend (Spiers, 2003; Davies et al.,2004). The qualitative nature of aspects of this reviewalso limit its conclusions: I have not examined, forexample, the exact amount by which spectacle prices areraised to subsidise sight tests. However, this type ofexercise would also require comprehensive knowledge ofoperating costs, staff salaries and other data whichwould be difficult or impossible to obtain retrospec-tively. Modern electronic accounting systems maypermit more sophisticated price research but may notextend back as far as the data in this survey. Finally, thereview ignores the introduction of ready-made readingspectacles in 1989 following the legislative changes
effected by the Health and Medicines Act 1988. Between5% and 11% of adults bought these spectacles by theearly 1990s (FODO, 1990, 1991; Office for PopulationCensuses and Surveys, 1996) and, although their pres-ence might have affected the prices of prescribedspectacles, any precise effects are unclear.
It is worth briefly looking at one of the objections toderegulation, namely that it put the public at risk frominaccurately-fitted spectacles sold by unqualified sup-pliers (Baker, 1983; Trybuchowski, 1983; Longhurst,2007a,b). This review has not examined the supposedrisk, and I have found no studies which have assessedthe accuracy of spectacles fitted by unqualified staff,but the risks may be small. Inaccurate spectacleprescriptions are known to cause visual problems(Atchison et al., 2001; Hrynchak, 2006; Freeman andEvans, 2010) but inaccurate spectacle dispensing oftendoes not. Hrynchak (2006) found that dispensing-related errors, such as �ineffective education regardinglens design� and �appliance problems�, were responsiblefor only 15% of the 1.6% of patients who experienceddifficulties with their spectacles, representing only0.24% of prescriptions dispensed. Freeman and Evans(2010) found that dispensing-related errors were pres-ent in about 22% of cases of intolerance to spectacles,i.e. about 0.4% of all prescriptions they surveyed,although they pointed out that their methodologymight underestimate the true proportion of theseerrors. Inaccurate lens centration, a potential dispens-ing error, is traditionally regarded as a potential causeof discomfort and diplopia (Brooks and Borish, 1996),yet it not only appears to be ubiquitous but can oftenbe tolerated without discomfort (Osuobeni andal-Zughaibi, 1993; du Toit et al., 2007). A survey ofchildren�s spectacles by Drack et al. (2006) found thatthree out of 79 pairs were so inaccurate as to be�potentially amblyogenic�, but these errors related tolens power, not fitting. The one pair of inaccurately-centred spectacles was not regarded as amblyogenic.These findings suggest that dispensing-related errors,including inaccurate lens centration, do not often causeproblems to spectacle wearers, although wearers ofmore complex lenses may be less tolerant since theperformance of such lenses is more severely compro-mised by poor centration (Atchison and Tame, 1993).
Registered opticians themselves may not necessarilydispense spectacles accurately. The Office of FairTrading (1982) noted the variable standards amongopticians, and this variability appears to extend toopticians� measurements of interpupillary distance(Osuobeni and al-Fahdi, 1994; Holland and Siderov,1999), which are less reliable than is sometimes believed(Walsh and Pearce, 2009). This suggests that accuratespectacle fitting is not always possible, even in the handsof registered opticians, in which case there may be little
Deregulation and spectacle prices: R. Calver 121
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

disadvantage in entrusting spectacle dispensing tounregistered suppliers.
Conclusion
Spectacle prices in the UK corporate sector from 1980to 2007 were affected by various factors, includingsupply regulations, NHS payments and the price of eyeexaminations. The amendments introduced by theHealth and Social Security Act 1984 appear to havebeen successful in constraining rises in the prices ofprivate spectacles.
Acknowledgement
I would like to thank Helen Bowman of the Federationof Ophthalmic and Dispensing Opticians for providingme with copies of �Optics at a Glance�.
References
Anon (1982) An optical monopoly. Times 12th January, 1982,9.
Anon (1983a) What price NHS fashion? Optician 185, 28th
Feb 1983, 5.Anon (1983b) What the papers said. Optician 186, 9thDecember 1983, 10–11.
Association of British Dispensing Opticians (2008) Advice &Guidelines on Professional Conduct for Dispensing Opticians.http://www.abdo.org.uk/adviceandguidelines.php (last acce-ssed 27 April 2009).
Atchison, D. A. and Tame, S. A. (1993) Sensitivity of off-axisperformance of aspheric spectacle lenses to tilt and decen-tration. Ophthalmic. Physiol. Opt. 13, 415–421.
Atchison, D. A., Schmid, K. L., Edwards, K. P., Muller, S. M.and Robotham, J. (2001) The effect of under and overrefractive correction on visual performance and spectacle
lens acceptance. Ophthalmic. Physiol. Opt. 21, 255–261.Baker, J. (1983) The dispensing viewpoint. Optician 185, 3rdJune 1983, 26, 29.
Brahams, D. (1984) Opticians and competition. Lancet 1, 14thApril, 1984, 861–862.
Brooks, C. W. and Borish, I. M. (1996) System for OphthalmicDispensing, 2nd edn. Butterworth-Heinemann, Boston.
Cairncross, A. (1994) Economic policy and performance,1964–1990. In: The Economic History of Britain since 1700.Volume 3: 1939–1992, 2nd edn (eds R. Floud and D.
McLoskey), Cambridge University Press, Cambridge, pp.67–94.
Chappell, N. W. (1983) Burden of industry. Optician 186, 29th
July, 1983, 28.College of Optometrists (2009) Good Optometric Practice:Guidance for Professional Conduct. http://www.college-optometrists.org/index.aspx/pcms/site.publication.Ethics_
Guidelines.recent/ last accessed 27 April 2009.Consumers� Association (1983) Opticians� prices. Which?March 1983, 102–103.
Davies, S. and Olczak, M. (2006) Benefiting from competition:
some UK cases. Econ. Rev. (UK) 24, 17–20.Davies, S., Coles, H., Olczak, M., Pike, C. and Wilson, C.
(2004) DTI Economics Paper No. 9. The Benefits from
Competition: Some Illustrative UK Cases. Department ofTrade and Industry, HMSO, London.
Drack, A. V., Sands, R., Smith, C., Curtis, T., Moore, C. and
O�Donnell, C. (2006) How often are our patients� spectaclelenses dispensed as prescribed? J. AAPOS 10, 72.
Euromonitor (1985) The Optical Goods Report. EuromonitorPublications, London.
Federation of Independent British Optometrists (1983) State-ment by the Federation of Independent British Optome-trists. Optician 186, 1st July 1983, 23–24.
FOCB (1982–1985) Optics at a Glance.FODO (1986–2008) Optics at a Glance.Freeman, C. E. and Evans, B. J. W. (2010) Investigation of the
causes on non-tolerance to optometric prescriptions forspectacles. Ophthalmic. Physiol. Opt. 30, 1–11.
Fulop, C. and Warren, K. (1992) The marketing of aprofessional service: opticians. Int. J. Advert. 11, 287–
305.Fulop, C. and Warren, K. (1993) Deregulation and its impact
on the opticians� market: a comparison of the forecasts of
both proponents and opponents with events in practice. Int.J. Advert. 12, 257–278.
Hart, J. (1983) Private charges reduced. Optician 185, 18th
February, 1983, 31.Holland, B. J. and Siderov, J. (1999) Repeatability of
measurements of interpupillary distance. Ophthalmic. Phys-
iol. Opt. 19, 74–78.Hrynchak, P. (2006) Prescribing spectacles: reasons for failure
of spectacle lens acceptance. Ophthalmic. Physiol. Opt. 26,111–115.
Hunt, C. (2007) Disjointed jottings. Dispensing Optics 22,
March 2007, 22–23.Johnson, A. (2006) Master builder. Dispensing Optics 21,
March 2006, 16–18.Key Note (2008) Market Assessment 2008: Opticians and
Optical Goods. Key Note Publications, Hampton, UK.
Little, S. (2007) Why the multiples are to blame for thepublic�s poor perception of DOs. Optician 233, 9th March2007, 11.
Llewellyn, R. (2006) Working smarter. Optician 231, 17th
March 2006, 11–12.Longhurst, R. (2007a) Recognition we deserve. Optician 233,
9th February 2007, 14.
Longhurst, R. (2007b) The importance of dispensing opticians.Optician 233, 30th March 2007, 12.
Muellbauer, J. and Murphy, A. (1997) Booms and busts in the
UK housing market. Econ. J. 107, 1701–1727.�Nemo� (1983) To the point! Optician 185, 1st April, 1983, 34.Office for National Statistics (2008) Retail Prices Index all
items: Table RP04. http://www.statistics.gov.uk/down-loads/theme_economy/RP04.pdf (last accessed 24 March2009).
Office for Population Censuses and Surveys (1996) Living in
Britain. Results from the 1994 General Household Survey.HMSO, London.
122 Ophthal. Physiol. Opt. 2010 30: No. 2
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists

Office of Fair Trading (1982) Opticians and Competition. A
Report by the Director General of Fair Trading on Sections 21and 25 of the Opticians Act 1958. HMSO, London.
Osuobeni, E. P. and al-Fahdi, M. (1994) Differences between
anatomical and physiological interpupillary distance. J. Am.Optom. Assoc. 65, 265–271.
Osuobeni, E. P. and al-Zughaibi, A. M. (1993) Induced
prismatic effect in spectacle prescriptions sampled in SaudiArabia. Optom. Vis. Sci. 70, 160–166.
Owen, R. (1983) The role of the GOS. Optician 186, 22nd July1983, 32.
Pemberton, H. (2005) The transformation of the economy. In:A Companion to Contemporary Britain 1939–2000 (edsP. Addison and H. Jones), Blackwell, Malden, MA, pp.
180–202.Pike, J. (2006) Disjointed jottings. Dispensing Optics 21,
February 2006, 24.
Price Commission (1976) Prices of Private Spectacles andContact Lenses. Report No. 20. HMSO, London.
Scott, H. A. (1983) Not the time to submit. Optician 185, 4thMarch 1983, 32.
Sheinman, J. (2006) Consensus needed on what we charge.Optician 231, 14th April 2006, 11–12.
Spiers, J. (2003) Patients, Power and Responsibility. The First
Principles of Consumer-driven Reform. Radcliffe MedicalPress, Oxford.
Stone, C. G. (1983) 924 – the fight for financing. Optician 186,
15th July 1983, 11–12, 25–26.Taylor, S. P. (1986) Effect of the Health and SocialSecurity Bill 1984 on the profession of optometry in the
United Kingdom. Am. J. Optom. Physiol. Opt. 63, 377–381.
Taylor, S. P. (1991) The Opticians Act 1989 and UKoptometry. Ophthalmic. Physiol. Opt. 11, 185–190.
Taylor, S. P. and Austen, D. P. (1986) Law and Management inOptometric Practice. Butterworths, London.
Taylor, S. P. and Austen, D. P. (1992) Law and Management
in Optometric Practice, 2nd edn. Butterworth-Heinemann,Oxford.
du Toit, R., Ramke, J. and Brian, G. (2007) Tolerance to
prism induced by readymade spectacles: setting and using astandard. Optom. Vis. Sci. 84, 1053–1059.
Trybuchowski, B. M. (1983) A case of amateur glazing.Optician 185, 4th March 1983, 32.
Walsh, G. and Pearce, E. I. (2009) The difference between belief
and reality for Viktorin�s method of inter-pupillary distancemeasurement. Ophthalmic. Physiol. Opt. 29, 150–154.
Worswick, G. D. N. (1984) Two great recessions: the 1980s
and the 1930s in Britain. Scot J. Polit. Econ. 31, 209–228.Wright, B. M. (1982) An optical monopoly. Times 20thJanuary, 1982, 11.
Appendix
Figures 3 and 5 require the cumulative effects ofinflation to be calculated.
If a price x0 at baseline is inflated by the percentageRetail Price Index (RPI1%) for the following year, theinflated price x1 at the same point in the following yearis given by:
x1 ¼ x0 1þ RPI1%100
� �ð1Þ
The price xn in any subsequent year is:
xn ¼ x0 1þ RPI1%100
� �1þ RPI2%
100
� �1þ RPI3%
100
� �� . . .
� 1þ RPIn%
100
� �; ð2Þ
where RPIn% is the RPI in the nth year after baseline.For inflation to result in a price x0, the �deflated� price
x)1 for the previous year is:
x�1 ¼x0
1þ RPI0%100
� � : ð3Þ
The price x)n in any previous year is:
x�n
¼ x0
1þRPI0%100
� �1þRPI�1%
100
� �1þRPI�2%
100
� ��...� 1þRPI�nþ1%
100
� �
ð4Þ
where RPI)n% is the RPI in the nth year beforebaseline.
Deregulation and spectacle prices: R. Calver 123
ª 2010 The Author. Journal compilation ª 2010 The College of Optometrists




















