
Responsiveness of the Neck Disability Index in patients with mechanical neck disorders
Upload
independentCategory
view
1download
0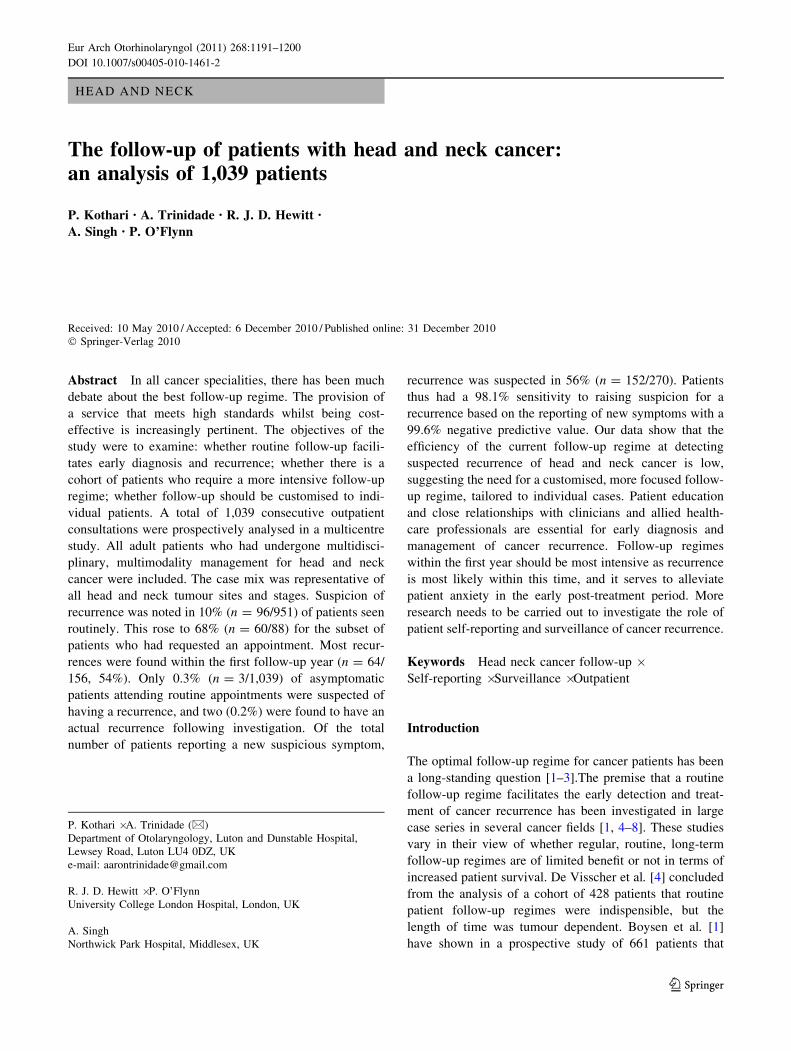
HEAD AND NECK
The follow-up of patients with head and neck cancer:an analysis of 1,039 patients
P. Kothari • A. Trinidade • R. J. D. Hewitt •
A. Singh • P. O’Flynn
Received: 10 May 2010 / Accepted: 6 December 2010 / Published online: 31 December 2010
� Springer-Verlag 2010
Abstract In all cancer specialities, there has been much
debate about the best follow-up regime. The provision of
a service that meets high standards whilst being cost-
effective is increasingly pertinent. The objectives of the
study were to examine: whether routine follow-up facili-
tates early diagnosis and recurrence; whether there is a
cohort of patients who require a more intensive follow-up
regime; whether follow-up should be customised to indi-
vidual patients. A total of 1,039 consecutive outpatient
consultations were prospectively analysed in a multicentre
study. All adult patients who had undergone multidisci-
plinary, multimodality management for head and neck
cancer were included. The case mix was representative of
all head and neck tumour sites and stages. Suspicion of
recurrence was noted in 10% (n = 96/951) of patients seen
routinely. This rose to 68% (n = 60/88) for the subset of
patients who had requested an appointment. Most recur-
rences were found within the first follow-up year (n = 64/
156, 54%). Only 0.3% (n = 3/1,039) of asymptomatic
patients attending routine appointments were suspected of
having a recurrence, and two (0.2%) were found to have an
actual recurrence following investigation. Of the total
number of patients reporting a new suspicious symptom,
recurrence was suspected in 56% (n = 152/270). Patients
thus had a 98.1% sensitivity to raising suspicion for a
recurrence based on the reporting of new symptoms with a
99.6% negative predictive value. Our data show that the
efficiency of the current follow-up regime at detecting
suspected recurrence of head and neck cancer is low,
suggesting the need for a customised, more focused follow-
up regime, tailored to individual cases. Patient education
and close relationships with clinicians and allied health-
care professionals are essential for early diagnosis and
management of cancer recurrence. Follow-up regimes
within the first year should be most intensive as recurrence
is most likely within this time, and it serves to alleviate
patient anxiety in the early post-treatment period. More
research needs to be carried out to investigate the role of
patient self-reporting and surveillance of cancer recurrence.
Keywords Head neck cancer follow-up �Self-reporting � Surveillance � Outpatient
Introduction
The optimal follow-up regime for cancer patients has been
a long-standing question [1–3].The premise that a routine
follow-up regime facilitates the early detection and treat-
ment of cancer recurrence has been investigated in large
case series in several cancer fields [1, 4–8]. These studies
vary in their view of whether regular, routine, long-term
follow-up regimes are of limited benefit or not in terms of
increased patient survival. De Visscher et al. [4] concluded
from the analysis of a cohort of 428 patients that routine
patient follow-up regimes were indispensible, but the
length of time was tumour dependent. Boysen et al. [1]
have shown in a prospective study of 661 patients that
P. Kothari � A. Trinidade (&)
Department of Otolaryngology, Luton and Dunstable Hospital,
Lewsey Road, Luton LU4 0DZ, UK
e-mail: [email protected]
R. J. D. Hewitt � P. O’Flynn
University College London Hospital, London, UK
A. Singh
Northwick Park Hospital, Middlesex, UK
123
Eur Arch Otorhinolaryngol (2011) 268:1191–1200
DOI 10.1007/s00405-010-1461-2

routine follow-up regimes are rarely indicated beyond the
third year post-treatment, and that 61% of patients with
recurrence reported their symptoms. They recommend a
focus on patient education in recognition of the signs and
symptoms or recurrence. Conversely, in a more recent
study, Lester et al. [5] concluded that based on the local
prospective data of 676 patients and published evidence,
laryngeal primaries should be followed up for 7 years,
whilst oropharyngeal and hypopharyngeal primaries should
be followed up for 3 years. They also felt that relying on
good patient education for the detection of recurrence
through self-presentation was an unacceptable practice, as
it would lead to the detection of less than two-thirds of
recurrences [5].
The issue is further highlighted by the financial impli-
cations of long-term follow-up for health-care trusts and
patients alike. The cost of medical, allied health-care,
nursing and clerical staff, in addition to patient costs
incurred in accessing the service, is considerable. The
question of whether the time commitment and psycholog-
ical stress involved in such regular clinic visits by patients
is warranted must also be taken into account.
At present, there are three main national guidelines
available in the UK that outline suggested follow-up
regimes for head and neck cancer patients: (1) the con-
sensus document of the British Association of Otorhino-
laryngologists and Head and Neck Surgeons (BAO-HNS),
(2) the Scottish Intercollegiate Guidelines Network (SIGN)
guidelines, and (3) the National Institute for Clinical
Excellence (NICE) guidelines [9–12] (Table 1). This
study’s main focus is on clinician-suspected recurrences of
disease rather than actual recurrences. It aims to determine
how early cancer recurrence is most likely to be identified
by the clinician at a routine outpatient visit, or by the
patient who notices a new symptom.
Setting
The study was conducted across three northwest London-
based head and neck cancer units: the University College
London Hospital (UCLH), Northwick Park Hospital (NPH)
and Mount Vernon Hospital (MVH). The three hospitals
serve as the main centres for head and neck cancer man-
agement for a catchment population of approximately
1.7 million. UCLH and NPH serve as the tertiary referral
and surgical centres where patients are first seen and
diagnostics and surgery are performed. MVH is the onco-
logical centre. The population includes several areas with a
high deprivation index. Patients with head and neck cancer
are under the care of otorhinolaryngology, head and neck
surgery (ORL-HNS), oral and maxillofacial surgery
(OMFS) and oncology. Consultants and allied health pro-
fessionals from all three hospitals participate in a weekly
joint multidisciplinary meeting held via videoconferencing.
Patients and methods
The study was conducted between January 2007 and
October 2007: 1,039 consecutive patients attending the
outpatient department who were undergoing multidisci-
plinary, multimodality management for head and neck
cancer were prospectively collected. Data included patient
age, original stage of cancer, treatment, patient-reported
symptoms and signs, clinician-reported symptoms and
signs and established follow-up plan. A ‘suspicion of
recurrence’ was defined as a sign or symptom noticed by
either the patient or the clinician that led to further inves-
tigation into whether the patient’s cancer had recurred.
These signs and symptoms were often disease specific and
included new onset of dysphonia and/or dysphagia, a new
Table 1 Summary of UK national guidelines for follow-up of head and neck tumour patients
Governing
body
Guidelines
BAO-HNS (1998) Squamous cell carcinoma (SCC): 2–4 weeks post-radiotherapy; year 1, every 1–3 months; year 2, every 2–4 months;
year 3 and 4, every 6 months; discharge at the end of year 5
Adenoid cystic carcinoma: as for SCC, but 6 monthly after year 4 until year 10
Pleomorphic adenoma: 2–4 weeks post-treatment; 6 monthly once effects of surgery ± radiotherapy have settled; discharge at
the end of 5 years
(2002) All guidelines remain unchanged, except for pleomorphic adenoma: monthly follow-up in year 1, decreasing to annually
by year 5 with option of annual visits offered to patients following this
SIGN (2006) Patients to be seen frequently and regularly within first 3 years post-treatment. Based on study by Boysen et al. [1], which
concludes that follow-up on a regular basis is rarely indicated beyond the third year. Follow-up should be limited to patients
where treatment options still remain [13, 14]
NICE (2004) Regular examinations in the first 2 years post-treatment with periods increased between consultations; discharge to be
considered at year 5
1192 Eur Arch Otorhinolaryngol (2011) 268:1191–1200
123
neck lump, new pain within the aerodigestive tract or neck
or positive nasendoscopic findings. All patients underwent
a full examination of the head, neck, oral cavity and
pharynx by a specialist surgeon, which included a routine
nasendoscopic examination. All data, suspicion of recur-
rence and appointment status (whether routine or patient
requested) were collected for all 1,039 patients and entered
into a standard proforma, from which data were later col-
lated and analysed (Appendix 1). A non-validated survey
was also conducted on the final 263 consecutive patients
attending the outpatient setting during the study period
regarding various aspects of their outpatient follow-up
experience, which the authors felt were relevant to this
study (Appendix 2). It was not conducted on the other
patients, as the idea of conducting the survey only occurred
to the authors towards the end of the study period. All data
were analysed using SPSS for Windows statistical package
(SPSS Inc., Chicago, IL, USA) and Microsoft Excel 2007.
Ethical considerations
All data were collected routinely as part of the clinical care
of the patients. No patient records or extra patient data
were accessed, and all collected data were anonymised
before analysis. The survey was reviewed by the ethics
department before distribution.
Results
Demographic data
Approximately, three-quarters of the population were male
(M = 763, 73.4%; F = 276, 26.6%), the overall average
patient age being 62 years (M = 62; F = 59). The youn-
gest patients were 19-year-old males with T3N3M0 naso-
pharyngeal carcinoma (n = 6), and the oldest patient was a
96-year-old male with T3N0M0 oropharyngeal carcinoma.
Tumour type and treatment data
The most common cancer was glottic (n = 369, 35.5%),
followed by oropharyngeal (n = 168, 16.2%) and naso-
pharyngeal (n = 100, 9.6%) (Fig. 1). Most tumours found
were classified as T2 (n = 293, 28%), followed by T3
(n = 275, 26.5%), T4 (n = 223, 21.5%), T1 (n = 177,
17%) and T9 (n = 18, 1.7%). The TNM classification for
all tumours in this study are shown in Table 2. One-quarter
of patients had surgery as their primary modality of treat-
ment (n = 260, 25%); 356 (n = 34.3%) underwent radio-
therapy and/or chemotherapy; 420 (n = 40%) underwent
both modalities.
Tumour recurrence and outpatient follow-up data
The mean follow-up period of our patients in the outpatient
department was approximately 40 months (3.34 years)
following completion of treatment, regardless of modality.
Most follow-ups were routine (n = 951, 91.5%) and the
remainder were patient-requested appointments (n = 88,
8.5%).
Overall, the rate of suspected recurrence of cancer
during the study period was 15% (n = 156/1,039). Glottic
cancer was the most commonly suspected site of recur-
rence (n = 62, 40%) (Fig. 2). When suspected recurrence
was stratified by treatment modality, it was found to be
most common in those patients who had undergone surgery
and adjuvant chemoradiotherapy (n = 72, 46%). When
stratified by original disease stage, T2 tumours were found
to be most commonly suspected of recurrence (n = 43,
28%) (Table 3). Of the suspected recurrences, 64 (56%)
were suspected within the first year of follow-up, followed
by 21 (14%) in the second year and 23 (15%) in the third
year. The overall trend was a decrease in suspicion of
recurrence with time, dropping to 6% (n = 10) by the
fourth year (Fig. 3). The shortest follow-up period until a
recurrence was suspected was 2 months for oropharyngeal
cancer (n = 2). Both patients had macroscopically clear
surgical margins at the time of operation. Histology and
radiology supported this post-operatively, and both patients
were deemed to be disease free following adjuvant therapy.
This strengthened the case against the possibility of this
representing residual or persistent disease as opposed to
recurrence given the short period of time.
The longest was 220 months (18.3 years) for laryngeal
cancer (n = 4). In the case of the latter four patients, none
was part of a routine follow-up regime, but requested an
appointment reporting a change in their voice. Again, given
the length of time to new findings, it is possible that these
patients could have developed second primary tumours as
opposed to recurrences. However, both can be considered
Fig. 1 Distribution of primary cancer site by type
Eur Arch Otorhinolaryngol (2011) 268:1191–1200 1193
123

Ta
ble
2T
NM
clas
sifi
cati
on
of
all
can
cers
Glo
ttis
Oro
-phar
ynx
Nas
ophar
ynx
Hypophar
ynx
Supra
glo
ttis
Ora
lT
hyro
idS
aliv
ary
Sin
onas
alU
nknow
nN
ose
Ear
Tra
chea
Skull
bas
eT
ota
l
T9
N1M
06
6
T9
N2M
04
4
T9
N2bM
04
4
T9
N3M
04
4
T1N
0M
080
52
29
32
6127
T1aN
0M
012
12
T1bN
0M
02
2
T1N
1M
06
22
21
13
T1N
2M
04
4
T1N
2bM
010
10
T2N
0M
0120
24
16
11
16
12
616
33
2229
T2N
1M
07
14
22
46
136
T2N
2M
04
22
513
T2bN
2M
02
2
T2N
2aM
02
2
T2N
2bM
02
68
T2N
2cM
02
57
T2N
3M
02
2
T3N
0M
030
11
13
33
36
410
16
24
159
T3N
1M
012
45
28
22
338
T3N
2M
04
12
65
431
T3N
2bM
017
17
T3N
2cM
08
42
14
T3N
3M
06
10
16
T4N
9M
02
24
T4N
0M
029
110
68
48
12
21
81
T4N
1M
014
11
65
24
143
T4N
1M
12
2
T4N
1aM
92
2
T4N
1bM
02
2
T4N
1cM
03
3
T4N
2M
026
25
21
238
T4N
2bM
021
44
29
T4N
2cM
02
24
412
T4N
3M
02
24
T4N
3M
14
4
TN
Mnot
reco
rded
311
82
10
46
246
Tota
l370
168
92
86
83
58
49
46
33
20
11
10
22
1194 Eur Arch Otorhinolaryngol (2011) 268:1191–1200
123

as ‘new cancer events’. The authors felt that such distinc-
tion would have made little difference in the overall
treatment decisions proposed at the time of discovery and
considered them as recurrences in view of their individual
past oncological histories.
Of those patients routinely seen, 10% (n = 96/951)
were suspected of having a recurrence. Of those patients
requesting an appointment to report new or changing
symptoms, the suspicion rate of recurrence rose to 68%
(n = 60/88). The sensitivity of a patient’s reported symp-
toms, resulting in a clinician’s suspicion of recurrence, was
thus 98.1% (152/155), with a specificity of 86.6% (766/
884). The probability of a suspected recurrence occurring
in a patient who had reported symptoms (PPV) was 56.3%
(152/270). However, the probability of a clinician having
no suspicion of recurrence in an asymptomatic patient
(NPV) was 99.6% (766/769) (Table 4). Of the asymp-
tomatic patients attending a routine follow-up regime, only
three (0.3%) were suspected of having a recurrence (two
nasopharyngeal, one glottic), and two (0.2%) were found to
have an actual recurrence on investigation (glottis and
nasopharynx).
Regarding the patient survey, 67% (n = 176/263) of
patients felt that the multidisciplinary team (MDT) clinic
met the goals they hoped would be achieved during their
visit. Of all, 84% (n = 221/263) of patients felt that their
head and neck follow-up visits were too frequent; 60%
(n = 159/263) of patients were also booked to see an allied
health professional in addition to the attending clinician on
their day of attendance to the clinic. Of these, 84%
(n = 134/159) felt that issues addressed at follow-up with
the clinician overlapped or duplicated those addressed by
the allied health-care professionals. When asked about their
0 10 20 30 40 50 60 70
Ear
Sinonasal
Unknown primary
Salivary gland
Supraglottis
Thyroid
Oral cavity
Hypopharynx
Sinonasal
Nasopharynx
Oropharynx
GlottisS
usp
ecte
d t
um
ou
r re
curr
ence
n
Fig. 2 Distribution of tumour types by suspicion of recurrence
Table 3 Suspicion of recurrence stratified by treatment modality and
original tumour stage
n (%)a
Treatment modality
Surgery ? chemoradiotherapy 72 (46)
Chemoradiotherapy 35 (22)
Radiotherapy 29 (19)
Surgery 18 (12)
Chemotherapy 2 (1)
Original tumour stage
T9 2 (1)
T1 26 (17)
T2 43 (28)
T3 40 (26)
T4 36 (23)
Data not available 9 (6)
a Total = 156
0
20
40
60
80
100
120
140
160
180
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Time to suspicion of recurrence (years)
n (
cum
ula
tive
)
Fig. 3 Overall suspected
recurrences from completion of
treatment with respect to time
(years)
Eur Arch Otorhinolaryngol (2011) 268:1191–1200 1195
123

opinion of a less intensive follow-up system based on
patients reporting problems and requesting appointments,
73% (n = 192/263) were in favour of it. When asked who
they would like to contact first in such a system, most
patients (n = 118/263, 45%) stated a clinical nurse spe-
cialist, followed by the medical secretary (n = 58/263,
22%). Clinicians ranked third (n = 42/263, 16%). Other
contacts included a speech and language therapist (n = 21/
263, 8%), their GP (n = 18/263, 7%) and a dietician
(n = 5/263, 2%).
Discussion
This study stemmed from the authors’ belief that there was
a dichotomy between the historic follow-up regime of head
and neck patients currently employed in the UK and the
more recent introduction of a multidisciplinary approach to
its management. The latter seems to have evolved in par-
allel to the former, instead of having been effectively
integrated into it, therefore allowing itself to the possibility
of multiplicity and repetition in patient follow-ups with the
surgeon and the various allied health-care professionals
who act independently of the surgeon and deal with the
various aspects of post-treatment rehabilitation. These
include clinical nurse specialists, speech and language
therapists, dieticians and, where appropriate, palliative care
nurses. Their input ensures a more holistic patient
approach, and many rehabilitative issues traditionally dis-
cussed with the surgeon are more efficiently addressed
through their own individual systems.
The guidelines outlined in Table 1 differ in their advice
as there is currently no high-level evidence to support any
one given regime, and many variations exist from region to
region [5, 13]. The authors believe that a streamlining of
the current system to a more modern, efficient one that
takes into account geographical variations and individual
patient requirements is needed.
From our data, the average age, sex ratio and distribution
of our population are similar to other data published else-
where in literature and is therefore a representative popu-
lation of adults with head and neck cancer. The data suggest
that the reporting of new symptoms by a patient provides a
very sensitive predictor for the suspicion of a recurrence. In
turn, this suggests that a less rigid, patient-oriented system
would have a very low chance of missing patients with a
suspected recurrence. The introduction of such a system
would require patient education of the symptoms and signs
of recurrence. Patients unable to achieve this would need to
be readily identifiable and managed accordingly. Allied
health-care professionals will also play an important role in
addressing other arising issues.
The efficacy of the current routine follow-up regime in
our institution at detecting a suspected recurrence is 10
versus 68% in follow-ups concerning patient-reported
symptoms. This suggests the need for a more focused
follow-up regime. It again suggests that the patient rather
than the clinician is better able to identify a suspected
recurrence and therefore facilitate early detection.
Three patients within a routine follow-up regime were
suspected of having a recurrence and, on investigation, two
of them were confirmed to have recurrence. These patients
represent the most difficult cases of recurrence for the
clinician to identify and therefore a possible limitation of a
less rigid, patient-oriented system as they would potentially
be overlooked in the initial stages of disease when their
treatment options would be greatest.
A clear definition of recurrence versus persistence of
disease is desirable in the management of head and neck
cancer and its follow-up. The authors accept that micro-
scopic disease can remain even in the face of negative
random biopsies of the macroscopically clear surgical
margins, representing persistent disease rather than a
recurrence. However, no uniform criteria to define a clear
surgical margin exist among practising head and neck
surgeons and the definition of a clear tumour margin after
chemoradiation is unclear. Most surgeons rely on frozen
section, but this view is not held by all [14].
Whilst not validated, the results of the survey are
interesting as they provide an insight into the patients’
perspective of the current follow-up regime. Research
suggests that the incidence of patients’ under-reporting
symptoms and signs is far increased with more frequent
follow-up [1]. In general, patients felt that being seen
intensively for the first year, then having visits tapered off
over the next 2 years and finally being seen according to
symptoms thereafter was appropriate and felt that this
represented an overall better system. Most felt that overall,
visits were too frequent and intensive and felt that different
aspects of the MDT clinic needed to communicate better to
avoid replication. The authors stress that whilst these data
can by no means form the sole basis for implementing
Table 4 Statistical analysis of
patient-reported new/changing
symptoms versus clinician-
suspected recurrence rates
Suspected
recurrence
No suspected
recurrence
Total
Patient reporting symptoms 152 118 270
Asymptomatic patient 3 766 769
Total 155 884 1,039
1196 Eur Arch Otorhinolaryngol (2011) 268:1191–1200
123

changes into current follow-up regimes, it does suggest that
an updated system might take into consideration an indi-
vidual patient’s attitude to his or her disease when tailoring
the follow-up plan.
Comparison with other studies
Our data are similar to those of Boysen et al. [1] (see
Fig. 3), showing a marked reduction in suspected recur-
rence after the third year. This seems to support their claim
that in general, routine follow-up regimes are rarely indi-
cated after the third year. However, four patients were
suspected of recurrence of laryngeal cancer at 220 months;
therefore, seemingly supporting claims by Lester et al. and
Spector et al. [5, 15] that laryngeal primaries should be
followed up for 7 years. Marchant et al. [16] suggest that
follow-up for life should be considered if detrimental
habits such as smoking and alcohol use persist. However,
these four patients were not routinely seen over
220 months, but instead requested an appointment to have
new symptoms reviewed. It therefore supports an argument
against routine follow-up regimes for such an extended
length of time. Nonetheless, this study does not have a
sufficiently large population number to accurately delineate
specific subsets of patients, but the authors feel that it does
highlight the need for flexibility in any chosen system of
follow-up. In a large chart review of 2,550 patients, again
by Spector et al. [16] it was found that the incidence of
distant metastases in squamous cell carcinomas of the
larynx and pharynx was greatest between 1.5 and 6 years
after initial treatment with the mean incidence being less
than or equal to 3.2 years. Our data support this claim.
They also found that delayed and distant lymph node
metastases were significantly higher in advanced primary
disease (T4 stage), locoregional recurrences and regional
disease (N2 and N3) in both the larynx and hypopharynx,
and that metastases occurring in hypopharyngeal tumours
were three times greater than in laryngeal cancers [16].
Regarding the importance of patient education and can-
cer detection in the follow-up system, there is conflicting
evidence as to whether patient surveillance versus routine
clinic surveillance results in a survival advantage [4, 5, 17,
18]. Some authors claim that up to two-thirds of recurrences
can be detected through increased patient self-awareness
[1, 4]. Lester et al. [5] state that this level of detection is
unacceptable. Our data of a sensitivity of 98.1% and an
NPV of 99.6% suggest that patient surveillance is not only
an acceptable measure of cancer recurrence, but a highly
sensitive and specific one that could potentially be incor-
porated into follow-up regimes that are tailored based on the
MDT’s perceived reliability of an individual patient’s
likelihood to report symptoms and signs.
Clinical applicability of this study
The authors feel that this study supports the notion of an
intensive follow-up regime for the first year post-treatment
for all cancers. It also suggests that intensive follow-up
after 3 years is not necessary. Patient education still plays
an important role in identifying recurrence of disease and
placing emphasis on this will allow for a more flexible
approach to follow-up, especially beyond 3 years post-
treatment. Once appropriately educated, patients can con-
tinue to bring worrisome symptoms to the clinicians’
attention, even many years post-treatment, without detri-
ment to overall care. Fostering a truly multidisciplinary
approach, involving greater patient responsibility to allied
health-care professionals and increased patient access to
members such as the clinical nurse specialist, would also
complement such a service, avoid repetition and, based on
the survey, approximate the service closer to patients’
expectations.
Limitations of this study
This study does not confirm that self-reporting is the best
follow-up method, but does suggest that this is a potential
area of study. Another limitation is that our sample size
precludes subset analysis. There were 18 patients identified
with unknown primaries in our population (see Table 2).
These patients pose a special problem as they do require
close monitoring and thus represent a confounding factor
of our study. However, it is still not known whether such a
follow up regime confers any benefit, and further research
into this subpopulation is needed. Disease-specific survival
data were not available. Finally, the survey used in this
study, though yielding interesting data, was non-validated.
Conclusion
Follow-up policies for head and neck cancer patients must
necessarily vary from centre to centre and must be the
product of agreed local practice and distinctive population
demographics. A shorter, flexible, individualised, inte-
grated multidisciplinary approach would seem to be more
favourable than a lengthy, prescriptive one that encour-
ages clinicians to practise independently of the rest of the
MDT. The result would be less over-subscribed clinics
and better-informed, less anxious patients with individu-
ally tailored follow-up regimes and greater clinic access if
needed.
Conflict of interest None to declare.
Eur Arch Otorhinolaryngol (2011) 268:1191–1200 1197
123
Appendix 1: Data collection proforma
Date of consult: DD/MM/YYYY
Age: Sex:
Primary site: Oral Cavity Oropharynx Supraglottis Glottis
Hypopharynx Thyroid Salivary Gland Sinonasal
Nasopharynx Unknown Primary Other _____________
T: N: M:
Patient seen by: Surgeon Oncologist
Treatment completion date: Surgery: DD/MM/YYYY
Radiotherapy: DD/MM/YYYY
Chemoradiation: DD/MM/YYYY
Current follow-up plan (months): 1 2 3 6 12 Discharged
Routine follow-up? Yes No If no, requested by who? _________
Patient reported symptoms? No Yes If yes, symptom? _______________
Clinical findings: No recurrence Suspicion of recurrence
Management decision: Imaging EUA/Bxa Reassurance
Additional consult by: Dietitian SALTb CNSc Palliative care
Other _________________
Proposed follow-up plan (months) 1 2 3 6 12 Discharge
Comments: __________________________________________________________________________
a Examination under anaesthesia / biopsy
b Speech & Language Therapist
c Clinical Nurse Specialist
1198 Eur Arch Otorhinolaryngol (2011) 268:1191–1200
123
Appendix 2: Patient survey
1. How do you view the number of follow-up visits you make to the head and neck clinic?
Too frequent Just about right Not frequently enough No opinion
2. Are you being seen by anyone else in the head and neck clinic today besides the doctor?
Clinical nurse specialist
Speech & Language Therapist
Dietitian
Dental/Oral hygienist
Other Please state who:________________________
None
3. If you are seeing someone else besides the doctor, do you think that the issues usually covered with
them overlaps with or duplicates the issues covered with the doctor?
Yes No Don’t know Not applicable
4. Do you feel that by coming to this clinic , you are able to adequately resolve any issues you may
have?
Yes No Don’t know
5. Would you prefer a less intensive follow-up sy stem that based on you reporting any problems and
requesting an appointment?
Yes No Don’t know
6. If you prefer such a system, who would you like to contact in the first instance?
Doctor GP
Clinical Nurse Specialist Speech & Language Therapist
Dietitian Dental/Oral hygienist
Doctor’s secretary
Other Please state who:__________________________
Eur Arch Otorhinolaryngol (2011) 268:1191–1200 1199
123

References
1. Boysen M, Lovdal O, Tausjo J, Winther F (1992) The value of
follow-up in patients treated for squamous cell carcinoma of the
head and neck. Eur J Cancer 28:426–430
2. Boysen M, Natvig K, Winther F, Taujso J (1985) Value of routine
follow-up in patients treated for squamous cell carcinoma of the
head and neck. J Otolaryngol 14:211–214
3. Vikram B, Strong E, Shah J, Spiro R (1984) Second malignant
neoplasms in patients successfully treated with multimodality
treatment for advanced head and neck cancer. Head Neck Surg
6:734–737
4. de Visscher AV, Manni JJ (1994) Routine long-term follow-up in
patients treated with curative intent for squamous cell carcinoma
of the larynx, pharynx and oral cavity. Does it make sense? Arch
Otolaryngol Head Neck Surg 120:934–939
5. Lester SE, Wright RG (2009) ‘When will I see you again?’ Using local
recurrence data to develop a regime for routine surveillance in post-
treatment head and neck cancer patients. Clin Otolaryngol 34:546–551
6. Broyn T, Froyen J (1982) Evaluation of routine follow-up after
surgery for breast carcinoma. Acta Chir Scand 148:401–404
7. Cochrane JPS, Williams JT, Faber RG, Slack WW (1980) Value
of outpatient follow-up after curative surgery for carcinoma of
the large bowel. BMJ 280:593–595
8. Dewar JR, Kerr GR (1985) Value of routine follow-up of women
treated for early carcinoma of the breast. BMJ 291:1464–1467
9. BAO-HNS Effective Head and Neck Cancer Management
(1998) 1st consensus document. British Association of Otorhi-
nolaryngologists, Head and Neck Surgeons. Royal College of
Surgeons of England, London
10. BAO-HNS Effective Head and Neck Cancer Management.
(2002) 3rd consensus document. British Association of Otorhi-
nolaryngologists, Head and Neck Surgeons. Royal College of
Surgeons of England, London
11. Scottish Intercollegiate Guidelines Network (SIGN) (2006)
Diagnosis and management of head and neck cancer: a national
clinical guideline
12. Improving outcomes in head and neck cancers: the manual, 2004.
National institute for health and clinical excellence
13. Marchant FE, Lowry LD, Moffitt JJ, Sabbagh R (1993) Current
national trends in the post-treatment follow-up of patients with
squamous cell carcinoma of the head and neck. Am J Otolaryngol
14:88–93
14. Meier JD, Oliver DA, Varvares MA (2005) Surgical margin
determination in head and neck oncology: current clinical prac-
tice. The results of an International American Head and Neck
Society Member Survey. Head Neck 27:952–958
15. Spector GJ, Sessions DG, Lenox J, Newland D, Simpson J,
Haughey BH (2004) Management of stage IV glottic carcinoma:
therapeutic outcomes. Laryngoscope 114:1438–1446
16. Spector JG, Sessions DG, Haughey BH, Chao KS, Simpson J, El
Mofty S et al (2001) Delayed regional metastases, distant metas-
tases, and second primary malignancies in squamous cell carcino-
mas of the larynx and hypopharynx. Laryngoscope 111:1079–1087
17. Cooney TR, Poulsen MG (1999) Is routine follow-up useful after
combined-modality therapy for advanced head and neck cancer?
Arch Otolaryngol Head Neck Surg 125:379–382
18. Virgo KS, Paniello RC, Johnson FE (1998) Costs of post-treat-
ment surveillance for patients with upper aero-digestive tract
cancer. Arch Otolaryngol Head Neck Surg 124:564–572
1200 Eur Arch Otorhinolaryngol (2011) 268:1191–1200
123
Copyright © 2022 FDOKUMEN




















