
The Iowa Longitudinal Study of Recent Onset Psychosis: One-year follow-up of first episode patients
13
SCHIZOPHRENIA RESEARCH ELSEVIER Schizophrenia Research 23 (1997) 1-13 The Iowa Longitudinal Study of Recent Onset Psychosis: one-year follow-up of first episode patients’ Sanjay Gupta a**, Nancy C. Andreasen a, Stephan Arndt a, Michael Flaum b, William C. Hubbard a, Steven Ziebell a aMental Health ClinicalResearch Center,The University of Iowa College of Medicine,Room 2911 JPP, 200 Hawkins Drive, Iowa City, IA 52242-1057, USA bDepartment of Psychiatry, The University of Iowa College of Medicine,Room 2911JPP, 200Hawkins Drive, Iowa City, IA 52242-1057, USA Received 2 November 1995; revision 15July 1996; accepted 22 July 1996 Abstract The natural history of schizophrenia remains unclear. One strategy to further inform this area is to prospectively evaluateindividuals early in the course of the disorder, both in terms of symptomaticand psychosocial/occupational functioning. Subjects were recruited into the study if they were in the midst of their first psychiatric hospitalization for a non-‘organic’ psychotic disorder. Subjects were extensively evaluatedat index with semi-structured interviews including the Comprehensive Assessment of Symptomsand History (CASH), and followed at 6-month intervals. Data are presented on 35 subjects who were followed through 1 year. There was a significant improvementin overall symptomatology during index hospitalization, but this was accounted for primarily by improvement of positive symptoms, with negativesymptoms remaining prominent. No further improvement wasnoted between discharge and l-year follow-up in any of the symptom measures. Employment, interpersonal relationships, and sexual activity remained markedly impairedthroughout the follow-up period. These data demonstrate that; (1) negative symptoms are prominent and stable early in the course of the disorder; (2) symptom severity at dischargefrom index hospitalization ispredictive of symptomseverityat 1year; and (3) despite substantial overall symptomatic improvement during the first hospitalization, psychosocial and occupationalfunctioning were found to be markedly impaired at l-year follow-up. Keywor& Schizophrenia; First-episode; Quality of life; Symptomatology; Longitudinal study * Corresponding author. Present address: Olean General Hospital West, 2221 West State Street, Olean, NY 14760, USA. Tel.: (1-716) 375-7324; Fax: (1-716) 375-7591. ‘These data were presented at the Winter Workshop On Schizophrenia, Les Diablerets, Switzerland, January 23-28, 1994. 0920-9964/97/$17.00 Copyright 0 1997 Elsevier Science B.V. All rights reserved PII SO920-9964(96)00078-3
Transcript of The Iowa Longitudinal Study of Recent Onset Psychosis: One-year follow-up of first episode patients
SCHIZOPHRENIA RESEARCH
ELSEVIER Schizophrenia Research 23 (1997) 1-13
The Iowa Longitudinal Study of Recent Onset Psychosis: one-year follow-up of first episode patients’
Sanjay Gupta a**, Nancy C. Andreasen a, Stephan Arndt a, Michael Flaum b, William C. Hubbard a, Steven Ziebell a
a Mental Health Clinical Research Center, The University of Iowa College of Medicine, Room 2911 JPP, 200 Hawkins Drive, Iowa City, IA 52242-1057, USA
b Department of Psychiatry, The University of Iowa College of Medicine, Room 2911 JPP, 200 Hawkins Drive, Iowa City, IA 52242-1057, USA
Received 2 November 1995; revision 15 July 1996; accepted 22 July 1996
Abstract
The natural history of schizophrenia remains unclear. One strategy to further inform this area is to prospectively evaluate individuals early in the course of the disorder, both in terms of symptomatic and psychosocial/occupational functioning. Subjects were recruited into the study if they were in the midst of their first psychiatric hospitalization for a non-‘organic’ psychotic disorder. Subjects were extensively evaluated at index with semi-structured interviews including the Comprehensive Assessment of Symptoms and History (CASH), and followed at 6-month intervals. Data are presented on 35 subjects who were followed through 1 year. There was a significant improvement in overall symptomatology during index hospitalization, but this was accounted for primarily by improvement of positive symptoms, with negative symptoms remaining prominent. No further improvement was noted between discharge and l-year follow-up in any of the symptom measures. Employment, interpersonal relationships, and sexual activity remained markedly impaired throughout the follow-up period. These data demonstrate that; (1) negative symptoms are prominent and stable early in the course of the disorder; (2) symptom severity at discharge from index hospitalization is predictive of symptom severity at 1 year; and (3) despite substantial overall symptomatic improvement during the first hospitalization, psychosocial and occupational functioning were found to be markedly impaired at l-year follow-up.
Keywor& Schizophrenia; First-episode; Quality of life; Symptomatology; Longitudinal study
* Corresponding author. Present address: Olean General Hospital West, 2221 West State Street, Olean, NY 14760, USA. Tel.: (1-716) 375-7324; Fax: (1-716) 375-7591. ‘These data were presented at the Winter Workshop On Schizophrenia, Les Diablerets, Switzerland, January 23-28, 1994.
0920-9964/97/$17.00 Copyright 0 1997 Elsevier Science B.V. All rights reserved PII SO920-9964(96)00078-3

2 S. Gupta et al. JSchizophrenia Research 23 (1997J I-13
1. Introduction
Emil Kraepelin was one of the earliest propo- nents of using longitudinal observation of clinical features to understand the outcome of psychosis and to develop improved classifications of diseases with greater prognostic power (Kraepelin et al., 1919). By monitoring the evolution of symptoms over time, he classified psychosis into dementia praecox, manic depressive illness, and paranoia. Our current nosological system is still based on his observations. Following his example, numerous subsequent longitudinal studies have been con- ducted to define and validate psychotic syndromes (Bleuler, 1911; Vaillant, 1964; Astrup and Noreik, 1966; Stephens et al., 1966; Garmezy, 1970; Strauss and Carpenter, 1972; Harrow et al., 1974; Huber et al., 1975; Tsuang et al., 1979; McGlashan, 1984; Harding et al., 1987; Carpenter and Kirkpatrick, 1988; Ciompi, 1988; Bromet et al., 1992).
These studies have expanded our knowledge of the course of psychotic illnesses and have helped to identify positive prognostic indicators such as good premorbid adjustment, acute onset, promi- nent psychotic (positive) symptoms, being married, female gender, and the presence of affective symp- toms (Gittelman-Klein and Klein, 1969; Haas and Sweeny, 1992; Gupta et al., 1995). The symptoms of psychosis in first episode patients can be con- founded by comorbidity, particularly by substance abuse. Studying comorbidity associated with first episode psychosis, Strakowski et al. (1995) found that the comorbid diagnosis was antecedent in 80% of first episode patients. Substance abuse, particularly alcohol, was noted to be the most common comorbid diagnosis (Strakowski et al., 1995).
Early longitudinal studies tended to ascertain subjects at variable times during the course of illness, making interpretation of results potentially equivocal (Bleuler, 1911; Vaillant, 1964). That is, when acute and relatively chronic patients are mixed together it is more difficult to obtain a ‘pure’ evaluation of the natural history of psychosis that is independent of the effects of existing chro- nicity (Ram et al., 1992). A review of previous studies revealed marked variability in the defini- tions used for diagnosis, sampling, and data collec-
tion which led to differences in findings; these being attributed to the presumed heterogeneity of the illness (Keshavan and Schooler, 1992). An example of variability would be a difference in the definition of age of onset as pointed out by DeLisi (1992). The ideal sample for such a study consists of patients ascertained during the first episode of illness, preferably prior to the initiation of treat- ment with neuroleptic medications (Kirch et al., 1992; Lieberman et al., 1992a,b; Shtasel et al., 1992).
It is only in the first episode group that the specificity of prodromal symptoms for schizophre- nia can be examined because the confounding effects of chronicity are not present (Jackson et al., 1995). The f&t episode group has also been an ideal one for studying intellectual deficits, eye movement abnormalities, and electrodermal ano- malies because of the lack of confounding effects of medication, chronicity, and institutionalization (Bilder et al., 1992; Dawson et al., 1992; Hoff et al., 1992; Sweeny et al., 1992). First episode subjects are also ideal for studying risk of rehospi- talization following the index hospitalization (Eaton et al., 1992).
In this study, we seek to explore a variety of fundamental questions concerning the natural his- tory of acute psychotic illness. What is the diagnos- tic evolution over time, particularly when the now widely used criteria of the Diagnostic and Statistical Manual (DSM-III-R and IV) are applied (APA, 1987, 1994)? How often do acute psychotic disorders evolve into schizophrenia, and how often do they remit fully? Does the pattern of symptoms present at the time of onset predict subsequent course, subsequent symptomatology, or subsequent psychosocial functioning? Given the recent re-emergence of interest in the negative symptoms of schizophrenia, which are often per- ceived as ‘end stage’ symptoms, that occur in patients as they evolve into chronicity, what is their frequency and prognostic significance early in the illness?
This study applies six measures for outcome: stability and ‘severity’ of diagnosis, severity of symptoms, changing course and pattern of symp- toms, frequency of relapse, frequency of rehospital- ization, and quality of life as measured by multiple

S. Gupta et al./Schizophrenia Research 23 (1997) I-13 3
domains (e.g., employment, recreational interest, social interactions). All these issues are addressed within the context of the Iowa Prospective Longitudinal Study of Recent Onset Psychoses which was designed for the long-term study of psychotic disorders (Flaum et al., 1992). The overall purpose is to ascertain a large sample of subjects early in the course of a psychotic disorder and to follow them prospectively, gathering biolog- ical and phenomenological data. This combines first episode and recent onset (i.e., duration 5 years or less) patients. The Iowa sample has a variety of special strengths such as a low rate of attrition due to population stability within the Iowa region and referral patterns that lead psychiatrists throughout the state to routinely refer recent onset psychotic patients to University of Iowa Hospitals and Clinics and the Mental Health Clinical Research Center for diagnostic consultation.
2. Methods
2.1. Subjects
Subjects in the Iowa Prospective Longitudinal Study, which is being conducted at the Mental Health Clinical Research Center (MH-CRC) at the University of Iowa Hospitals and Clinics, are drawn from our research inpatient unit, the psychi- atric inpatient units, and outpatient referrals, The study evaluates both recent onset and first episode patients (Arndt et al., 1995). For these analyses we evaluated a subset of 41 patients to focus on relatively young first episode subjects. Selection was based on the following criteria: (1) at intake subjects were in the midst of their first psychiatric hospitalization and were not older than 35 years; (2) subjects were experiencing their first episode of psychosis, i.e., there had been no remission in psychotic symptoms since the onset of the syn- drome (defined as global rating of three or higher on any item of the Scale for the Assessment of Positive Symptoms (SAPS); (3) subjects were enrolled in the study for at least one year following intake; (4) at follow-up, subjects had a DSM- III-R diagnosis of a psychotic disorder not due to an ‘organic’ cause (e.g., schizophrenia, delusional
disorder, psychotic disorders not otherwise speci- fied, and mood disorders with mood incongruent psychotic features).
These criteria were used in an attempt to resolve some of the problems relating to the various definitions of first episode. By adding the criterion of nonremission of the syndrome prior to first hospitalization, we eliminated subjects who may have had multiple exacerbations and remissions of psychotic syndromes prior to first hospitalization. Also, by using follow-up diagnoses as entrance criteria, we did not exclude subjects who may have had confusing clinical presentations at intake. This also allowed us to explore the boundaries of diag- nostic categories. This study has a naturalistic design with respect to treatment, with all subjects treated in a noncontrolled fashion in the com- munity by their psychiatrists. The MH-CRC serves as a tertiary referral center for consultations. Patient follow-up by community psychiatrists was encouraged for purposes of therapeutic alliance.
2.2. Clinical assessment
2.2.1. Intake The diagnosis at entry into the study was based
on clinical information obtained from a structured interview, known as the Comprehensive Assessment of Symptoms and History (CASH) using DSM-III-R criteria. The information was collected from clinical interviews, comprehensive physical and neurological examination, from col- lateral sources, and available records. The team consisted of a research psychiatrist, research asso- ciates, and nursing staff at the MH-CRC. None of the subjects had mental retardation, dementia, or serious medical or neurological illnesses. Subjects were also excluded if psychotic symptoms occurred immediately following head trauma or epilepsy. Treatment was not a controlled variable in this study. The patients were treated using ‘clinicians choice’ medications. All subjects gave informed consent before entry into the study.
All patients received a structured interview with the CASH (Andreasen, 1985; Andreasen et al., 1992). The CASH includes the Scale for the Assessment of Negative Symptoms (SANS) and the Scale for the Assessment of Positive Symptoms

4 S. Gupta et al./Schizophrenia Research 23 (1997) I-13
(SAPS). The PSYCH-base (an acronym for psychosocial symptoms you currently have at base- line), a companion instrument to the CASH was also administered concurrently to assess psychoso- cial functioning and record details of psychiatric treatment (Andreasen, 1987a). Detailed informa- tion was obtained through ongoing interviews with the subjects, informants, and hospital staff, as well as a comprehensive review of all available medical records. To obtain a thorough evaluation, data were collected during the entire hospitalization. Ratings including those for negative symptoms were conducted by research associates. All attempts were made to maintain the same raters over time. To maintain interrater reliability and address issues pertaining to rater drift there is an ongoing program of checks on interrater reliability (Andreasen et al., 1992; Flaum et al., 1992).
2.2.2. Follow-up Interviews were conducted with the patient and
best informant, and medical records were also reviewed at 6-month intervals dated from discharge at index hospitalization. Modified versions of the CASH and PSYCH-base were used at follow-up to record cross-sectional and longitudinal informa- tion pertaining to symptomatology and psychoso- cial functioning. The CASH-Up is a shortened version of the CASH that records information about positive (SAPS) and negative symptoms @ANSI, mood symptoms and syndromes, schizotypal and residual symptoms, and substance abuse. It is designed as a cross-sectional instrument that documents current levels of symptoms inclu- sive of the month prior to the interview.
The PSYCH-Up is an expanded version of the PSYCH-base that documents psychosocial func- tioning (quality of life) during each month of the 6-month follow-up period (Andreasen, 1987b). The level of impairment in the areas of employ- ment, household duties, education, sources of income, relationships with family and friends, sexual functioning, and satisfaction are recorded for each month. We chose to look at symptomatol- ogy on the basis of total SANS and SAPS scores and also in the context of psychotic, disorganized, and negative symptom dimensions which have been proposed on the basis of factor analytic
studies (Andreasen, 1983, 1984; Kulhara et al., 1986; Arndt et al., 1991; Minas et al., 1992; Peralta et al., 1992; Miller et al., 1993).
2.3. Statistical analysis
Means and standard deviations were calculated on all sociodemographic and clinical data. Frequency distributions were computed for levels of impairment of psychosocial variables. Mann- Whitney U-tests were performed to determine if group differences existed between the patients who were ill for less than 6 months and those who had unremitting symptoms for greater than 6 months prior to index hospitalization. These same nonpar- ametric tests were performed on additional groups consisting of subjects who dropped out of the study after intake and those who remained in the study at one year follow-up. Wilcoxon Signed Rank Statistic was used to test changes in the severity of the three symptom dimension ratings (negative, psychotic, and disorganized) made during index hospitalization and discharge. Nonparametric statistics were used because the distribution of symptom severity were often non- normal, and previous data from our group has shown nonparametric tests to be more powerful for these data (Arndt et al., 1993). We used Spearman Rank correlation to assess predictive relationships between the three symptom dimen- sions at intake and l-year follow-up.
3. Results
Thirty-five subjects remained in the study at 1 year out of a total of 41 enrolled at discharge from index hospitalization. Four subjects refused follow-up, one committed suicide, and the sixth was dropped because subsequent evaluations indi- cated that the psychotic symptoms were feigned. All follow-up data presented are based on the 35 subjects remaining in the study at 1 year.
3.1. Sociodemographic and clinical characteristics
The sample at intake was diagnostically diverse (schizophrenia spectrum disorders, bipolar affec-

S. Gupta et al.lSchizophrenia Research 23 (1997) l-13 5
tive disorder, major depression, and psychosis NOS). The follow-up group (n = 35) had a signifi- cantly higher (t = - 2.4, df = 39, p < 0.02) rating on the psychotic dimension at discharge than those lost (n =6) to follow-up. These two groups also differed on the number of months on neuroleptics. None of the subjects who dropped out had taken neuroleptics prior to intake hospitalization. No group differences were found between the subjects who had unremitting symptoms for greater than 6 months prior to index hospitalization and those whose symptoms were of less than 6-months dura- tion. Majority of the subjects in the study were neuroleptic naive (7 l%), severely ill, all with prom- inent positive and negative symptoms, and with varying degrees of psychosocial impairment. At one year 90% of the subjects were on neuroleptic medication. The mean duration of index hospital- ization was 37.2 (34.3) days. Two-thirds of the sample (66%) was male with the mean age being 24 years (5.9). The majority of the patients were never married (78%), and approximately half were unemployed. The educational achievement was 12.1 (1.7) years. Drug and alcohol related prob- lems, which included DSM-III-R diagnoses of drug/alcohol abuse or dependence, were present in eight subjects (22.85% of the sample). Detailed socio-demographic and clinical characteristics of the sample are presented in Table 1.
3.2. Diagnostic categories
In assessing the diagnostic categories at intake and follow-up (Table 2) our results revealed that
Table 1 Summary of sociodemographic variables for all subjects at index hospitalization (n = 41)
Variable Mean SD.
Age Percent male Educational achievement of subject Educational achievement of father Percent never married Age at first outpatient contact Duration of illness (months) Global assessment scale at intake Drug/alcohol abuse or dependence
24.0 5.9 66.0% 12.1 1.7 12.8 3.7 78.0% 23.6 5.5 19.6 33.2 32.6 8.3 22.85%
approximately half (48.4%) of the patients had a diagnosis of schizophrenia at intake while a large proportion (72.2%) of the remaining patients were within the schizophrenia spectrum. One hundred percent of patients diagnosed at intake with schizo- phreniform (n = 1 l), schizoaffective (n = 1 ), or schizotypal personality (n = 1) disorders were rediagnosed at follow-up. The remaining patients in this category were rediagnosed as having psychotic disorder not otherwise specified. At follow-up, 94% of the subjects had a diagnosis within the schizophrenia spectrum, 83% of them being diagnosed as having schizophrenia.
3.3. Course of symptoms
These data were summarized by using three symptom dimensions which have been established on the basis of factor analytic studies of the SANS and SAPS. The psychotic dimension was the sum of the global ratings for SAPS items for hallucina- tions and delusions (Arndt et al., 1995). The disorganized dimension was defined as the sum of the global ratings for SAPS items for bizarre behavior, positive formal thought disorder, and inappropriate affect. The negative dimension con- sisted of the global rating for SANS items alogia, affective flattening or blunting, avolition-apathy, and anhedonia-asociality.
We found significant changes (p ~0.01, Wilcoxon Signed Rank Statistic, n = 35) in all three symptom dimensions between ratings made during index hospitalization and at discharge. However, symptom severity showed no significant changes between discharge and l-year follow-up. Fig. 1 illustrates the finding that symptom improvement occurs primarily during index hospitalization and that symptoms remain relatively stable during l-year follow-up.
In addition, Spearman Rank correlations between symptom dimensions at intake and l-year follow-up indicated that the presence of negative symptoms at index hospitalization (intake) corre- lated significantly (r = 0.44, n = 35, p < 0.01) with the presence of negative symptoms at one year, while the psychotic and disorganized dimension showed no correlations between intake and one year. Neuroleptic medication status is an impor-

6
Table 2
S. Gupta et al. JSchizophrenia Research 23 (1997) I-13
Frequency and change of DSM-III-R diagnosis at intake and one year (n = 35)
Intake diagnosis 1 -year diagnosis Total at index (%)
Schizophrenia Psychosis Bipolar Delusional SchizoaITective NOS disorder disorder disorder
Schizophrenia 17 0 0 0 0 17 (48.4) Schizoaffective disorder 9 2 0 0 0 11 (31.3) Schizotypal personality disorder 1 0 0 0 0 1 (2.9) Psychosis NOS 1 0 0 0 0 1 (2.9) Delusional disorder 0 0 0 1 0 1 (2.9) Bipolar disorder 0 0 1 0 0 1 (2.9) Major depression 0 0 0 0 1 1 (2.9) Bipolar disorder NOS 0 0 1 0 0 1 (2.9) Total at follow-up (%) 29 (82.8) 2 (5.7) 2 (5.7) 1 (2.9) 1 (2.9) 35 (100.0)
Plot of Group Average Symptom Dimension Severity Rating vs. Time
5
I- Diihargefrom
t Index Haspitaliiation
Index Hospitaliition
Disorganized Dimension
, I I 0 4 8 12 16 20 24 28 32 36 40 44 48 52
Weeks
Fig. 1. Plot of group average symptom dimension severity vs. time.
tant confounding factor in the assessment of nega- tive symptoms. We examined the neuroleptic naive and the non-naive patients separately at index for negative symptoms. There was a significant differ- ence (x2=4.02, df= 1, p ~0.045) in the sum of negative symptoms between the two groups (naive and non-naive), with the non-naive group having a higher score. The data suggest that negative
symptoms are present early in the illness. However, neuroleptic medication can be a contributing factor.
We explored the prevalence of a depressive syndrome as defined in the CASH. It required the presence of dysphoric mood of a moderate degree or higher for a 2-week period along with four vegetative symptoms of at least a moderate degree.

S. Gupra et al./Schizophrenia Research 23 (1997) l-13 I
Eleven subjects met the criteria at 6 months while only three experienced it at 1 year. No significant differences were found in the negative symptoms scores between patients who met the CASH criteria for a depressive syndrome and those who did not (Mann-Whitney U-test z approximation = 1.58, p>O.ll).
from the negative syndrome lasting the entire follow-up period. These data seem to indicate that positive syndromes were more likely to remit than negative syndromes. This hypothesis was verified using McNemar’s test of correlated proportions (;‘=5.8, df= 1, ~~0.017) (Siegel, 1956).
3.4. Remissions and relapse
A remission from the positive syndrome was defined as a period of at least 12 consecutive weeks during which none of the SAPS global items were rated higher than mild in severity. This definition combines the psychotic and disorganized dimen- sions since they are conventionally combined in the determination of need for hospitalization, med- ication dosage increase, or other clinical decisions. For the negative syndrome it was defined as a period of 12 consecutive weeks during which three of the four SANS global items were rated no higher than mild severity.
The analyses revealed that approximately one- third (31.4%) of the subjects had no remission from the positive syndrome (Table 3). In contrast, over one-half (57.1%) of the subjects had no remission of the negative syndrome. Conversely, 20% (n=7) of all subjects had a full remission from the positive syndrome for the entire follow-up period. Only one subject had a complete remission
Relapse of both positive and negative syndromes was determined for subjects who underwent an initial complete remission in the 1 year period of follow-up. Relapse of positive syndrome was defined as a score of three or more on any global rating of the SAPS following a remission period of 12 weeks. Negative syndrome relapse was defined as a symptom score of three or greater on any two SANS global items after a remission period of 12 weeks. There were seven subjects who had a relapse characterized by positive symptoms and five who had a relapse of negative symptoms during the l-year follow-up period. One of the seven subjects had relapsed twice (positive symp- toms) during the follow-up period. Medication noncompliance or lowering of the neuroleptic dosage was the predominant cause for relapse.
Over half (n = 18, 5 1.4%) of the sample remained out of the hospital during the l-year follow-up period. Of the 17 individuals that were rehospital- ized, 82% (n = 14) of them were hospitalized only once and over one-half (n = 10, 58.8%) were rehos- pitalized for a total of ~5 weeks. Only 20% (n= 7) of all subjects were hospitalized for longer than
Table 3 Total number of remissions from positive” and negativeb syndrome per subject by total duration of remissions during l-year follow-up period (n = 35)
Total number of remissions per subject Syndrome Total duration of all remissions (weeks) Total
No remissions 12-19 20-29 30-39 40-51 52
0
1
2
Total
Positive 11 - - 31.4% Negative 20 - - 57.1% Positive - 5 1 0 7 I 57.2% Negative ~ 5 4 3 2 1 42.9% Positive - 0 0 2 2 0 11.4% Negative - 0 0 0 0 0 0.0% Positive 31.4% 14.3% 2.9% 5.7% 25.7% 20.0% Negative 57.1% 14.3% 11.4% 8.6% 5.7% 2.9%
“A remission from positive syndrome is defined as a period of 12 or more consecutive weeks during which time no SAPS global items were rated higher than mild severity. “A remission from negative syndrome is defined as a period of 12 or more consecutive weeks during which time three of the four SANS global items were rated no higher than mild severity.

8 S. Gupta et al./Schizophrenia Research 23 (1997) I-13
5 weeks. Two of these patients remained hospital- ized for the entire follow-up period after being transferred to institutional care following index hospitalization.
3.5. Quality of life
Quality of life is a key area in the assessment of long-term treatment outcome in schizophrenia. The main issue is how close do patients get to their premorbid level of functioning in the context of areas such as interpersonal relationships, employment, and sexual activity. The best level of functioning in the 5 years preceding entry into the study was used as the baseline for comparisons made at 6 and 12 months. A Scale for the Assessment of Psychosocial functioning is embed- ded in The Psych Base and Psych Up. It contains ratings from 0 to 5, with higher numbers represent- ing increasing impairment.
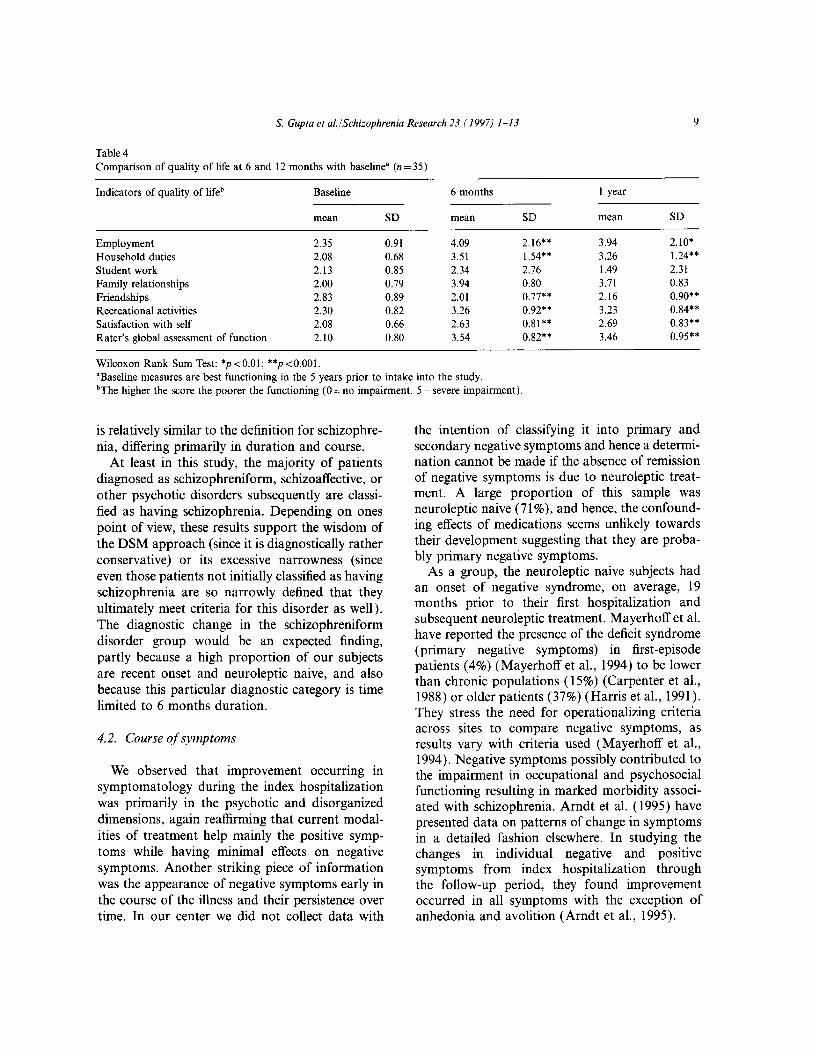
At baseline, the subjects were in the range between normality and mild dysfunction (~2.5) on most items. The majority of the subjects evi- denced high levels of impairment in the areas of family relationships, recreational activities, sexual activity, and household duties during the follow-up period. A substantial number were unemployed at both 6- and 12-month follow-up (49.0% at 6 months and 43.0% at 12 months). There was marked lack of sexual activity which worsened with time, at baseline 62%, at 6 months 79%, and at 12 months 86% of the subjects were sexually inactive. There was a statistically significant differ- ence in the number of sexually inactive subjects at baseline (n = 18) when compared to the 12-month (n=30) time frame (x2=4.729, @=I, ~~0.03). The analyses did not reach significance when com- paring baseline with 6 months (x2=2.52, df= 1, p < 0.11). Many subjects also reported a high degree of dissatisfaction (49%) with their function- ing in these psychosocial domains used to assess quality of life. The comparison of psychosocial functioning at baseline with that at 6 and 12 months indicated a decline which was statistically significant (Table 4) for the items of employment, household duties, recreational activities, satisfac- tion with self, and the raters global assessment of function. The findings indicated a statistically sig-
nificant improvement in friendships (Table 4). Overall, the patients were markedly impaired at 1 year in social, occupational, sexual, and interper- sonal functioning despite significant improvement in psychotic symptomatology during index hos- pitalization.
4. Discussion
This is an initial report on the Iowa Prospective Longitudinal Study focusing on 1 -year follow-up of first episode patients. We have presented hnd- ings on the demographic, diagnostic, clinical, and quality of life of these patients. The findings at 1 year revealed there was a significant improvement in the overall symptomatology during index hospi- talization. The quality of life assessed by factors such as employment, interpersonal relationships, and sexual activity remained markedly poor throughout the follow-up period. This study like most other first episode studies also tended to have more male (66%) than female subjects (Iacono and Beiser, 1992; Wahl and Hunter, 1992).
4.1. Stability of diagnosis
Evaluating changes in diagnosis provides a mea- sure of outcome at the simplest descriptive level. This study was designed in order to ascertain psychotic patients with a relatively broad range of presentations. In spite of this breadth, by l-year follow-up the majority of patients were given a diagnosis of schizophrenia: 48.4% of patients received this diagnosis at index evaluation, com- pared to 82.8% by l-year follow-up. These findings are consistent with those of Ganguli and Brar who found that 81.3% of their first episode subjects met criteria for schizophrenia at the end of 15 months (Ganguli and Brar, 1992). Many of our patients who were admitted to the hospital with a diagnosis in the psychotic disorders spectrum con- verted to the relatively narrow diagnosis of DSM schizophrenia. In all likelihood, this outcome reflects the stringency of definition even for the nonschizophrenic psychotic disorders. The cross- sectional syndromal definition of these disorders
S. Gupta et al./Schizophrenia Research 23 (1997) 1-13 9
Table 4 Comparison of quality of life at 6 and 12 months with baseline” (n = 35)
Indicators of quality of lifeb Baseline 6 months
mean SD mean SD
Employment 2.35 0.91 4.09 2.16** Household duties 2.08 0.68 3.51 1.54** Student work 2.13 0.85 2.34 2.76 Family relationships 2.00 0.79 3.94 0.80 Friendships 2.83 0.89 2.01 0.77** Recreational activities 2.30 0.82 3.26 0.92** Satisfaction with self 2.08 0.66 2.63 0.81** Rater’s global assessment of function 2.10 0.80 3.54 0.82**
Wilcoxon Rank Sum Test: *p<O.Ol; **p<O.OOl. “Baseline measures are best functioning in the 5 years prior to intake into the study. ‘The higher the score the poorer the functioning (0 =no impairment, 5 = severe impairment).
1 year
mean
3.94 3.26 1.49 3.71 2.16 3.23 2.69 3.46
SD
2.10* 1.24** 2.31 0.83 0.90** 0.84** 0.83** 0.95**
is relatively similar to the definition for schizophre- nia, differing primarily in duration and course.
At least in this study, the majority of patients diagnosed as schizophreniform, schizoaffective, or other psychotic disorders subsequently are classi- fied as having schizophrenia. Depending on ones point of view, these results support the wisdom of the DSM approach (since it is diagnostically rather conservative) or its excessive narrowness (since even those patients not initially classified as having schizophrenia are so narrowly defined that they ultimately meet criteria for this disorder as well). The diagnostic change in the schizophreniform disorder group would be an expected finding, partly because a high proportion of our subjects are recent onset and neuroleptic naive, and also because this particular diagnostic category is time limited to 6 months duration.
4.2. Course of symptoms
We observed that improvement occurring in symptomatology during the index hospitalization was primarily in the psychotic and disorganized dimensions, again reaffirming that current modal- ities of treatment help mainly the positive symp- toms while having minimal effects on negative symptoms. Another striking piece of information was the appearance of negative symptoms early in the course of the illness and their persistence over time. In our center we did not collect data with
the intention of classifying it into primary and secondary negative symptoms and hence a determi- nation cannot be made if the absence of remission of negative symptoms is due to neuroleptic treat- ment. A large proportion of this sample was neuroleptic naive (7 1 %), and hence, the confound- ing effects of medications seems unlikely towards their development suggesting that they are proba- bly primary negative symptoms.
As a group, the neuroleptic naive subjects had an onset of negative syndrome, on average, 19 months prior to their first hospitalization and subsequent neuroleptic treatment. Mayerhoff et al. have reported the presence of the deficit syndrome (primary negative symptoms) in first-episode patients (4%) (Mayerhoff et al., 1994) to be lower than chronic populations (15%) (Carpenter et al., 1988) or older patients (37%) (Harris et al., 1991). They stress the need for operationalizing criteria across sites to compare negative symptoms, as results vary with criteria used (Mayerhoff et al., 1994). Negative symptoms possibly contributed to the impairment in occupational and psychosocial functioning resulting in marked morbidity associ- ated with schizophrenia. Arndt et al. (1995) have presented data on patterns of change in symptoms in a detailed fashion elsewhere. In studying the changes in individual negative and positive symptoms from index hospitalization through the follow-up period, they found improvement occurred in all symptoms with the exception of anhedonia and avolition (Arndt et al., 1995).

10 S. Gupta et al.lSchizophrenia Research 23 (1997) I-13
There is a slight worsening of symptoms immedi- ately following discharge (Fig. 1) which may be due to symptom minimization by the patient just prior to discharge, or to the need for adjustment at the place of residence following discharge from a structured therapeutic inpatient milieu.
4.3. Remissions and relapse
This study indicates that psychotic (delusions and hallucinations) and disorganization symptoms (thought disorder and inappropriate affect) respond to the current treatment modalities while negative symptoms are refractory. It suggests the need to focus research on the development of successful treatments for negative symptoms. The results suggest that the ‘rule of thirds’ is not really true. In particular, the outcome of schizophrenia might be poor early in the illness possibly due to the persistence of negative symptoms which are considered to be ‘core’.
4.4. Quality of l$e
The recovery in symptoms was not paralleled by recovery in psychosocial functioning: a finding similar to the reports of Tohen et al. (1992). Most of these individuals continued to be moderately to severely impaired in the arena of occupational functioning, family relationships, sexual activity, and household chores, a picture very congruent with observations made in clinical practice. The improvement noticed with regard to friendships may be due to neuroleptic treatment resulting in reduction of psychosis and attendance at day pro- grams following discharge from the hospital. This indicates that the decline in psychosocial, sexual, and occupational functioning (quality of life) in schizophrenia is present early in the course of the disorder with little scope for improvement even after discharge from the hospital. We have noted in this mostly neuroleptic naive sample (7 1%) that negative symptoms are present early in the course and are persistent despite treatment. This is some- what contrary to the clinical belief that these patients deteriorate over time. Neuroleptic-induced side-effects and institutionalization are only con- tributing factors to a process that begins early in
the illness. These data project a bleak outlook for patients early in the course of schizophrenia. It is interesting to note that many of the findings of Fenton and McGlashan in a chronic schizophrenic sample, such as poor outcome in terms of employ- ment, social functioning, and intimacy, have been replicated in this first episode sample consisting predominantly of neuroleptic naive (7 1%) patients (Fenton and McGlashan, 1991). These findings suggest that the quality of life declines early in the illness.
4.5. Limitations
Limiting factors include a relatively small sample size (n=35) and nearly one-quarter of these patients had drug/alcohol abuse or dependence which may influence results. This sample was obtained primarily from hospitalized patients (whose symptoms may be unusually severe) and, hence, is not an epidemiological one. This is a naturalistic study where treatment of these first episode patients was started after index and the results of the study tell the story of outcome in the context of modern day treatment approaches. There may have been variations in treatment prac- tice (e.g., maintenance medication dosage, dura- tion, emphasis on continued treatment) among the community psychiatrists which could influence outcome.
4.6. Strengths
Ram et al. (1992), in a review of first admission studies, have mentioned six limitations of the currently designed studies which are: (1) failure to analyze separately first episode from multi-episode patients; (2) reliance on cross-sectionally deter- mined diagnosis; (3) small samples; (4) lack of treatment data before, during, and after hospital- ization; (5) drawing of samples from single treat- ment facilities; (6) exclusion of patients with substance abuse. The Iowa study has taken into account most of these limitations in design. We have separately analyzed the first episode patients from the multi-episode ones, and our study design allows for diagnostic assessment on a longitudinal and not a cross-sectional basis by starting with a

S. Gupta et al. JSchizophrenia Research 23 (1997) 1-13 11
broad sampling strategy. Using the CASH and PSYCH base and its companion instruments, we continue to gather complete data on treatments, symptomatology, and psychosocial functioning before, during, and after hospitalization. Also, at Iowa we do not exclude patients with substance abuse from the study. The strengths of this study are: ( 1) first episode patients, with 71% being neuroleptic naive, which reduces to a great extent the confounding effects of medication and institu- tionalization; (2) the study is a naturalistic one as the patients are followed by their community psy- chiatrists; (3) use of the first set of measurements designed specifically for the purpose of longitudi- nal studies which have undergone validation (Flaum et al., 1993). The clinical ratings used in this study are from the consensus CASH which is based on pooled information obtained indepen- dently from the patient and the best informant by two raters who then jointly complete the consensus CASH. This procedure provides information of high accuracy; (4) The patients were followed at 6-month intervals by the same rater which helps in establishing rapport with the subject, the family, and other care givers, which promotes cooperation and facilitates extraction of important information.
5. Conclusions
These data demonstrate that: ( 1) negative symp- toms are prominent early in the course of the disorder and not necessarily due to neuroleptic treatment; (2) despite substantial overall symp- tomatic improvement during the first hospitaliza- tion, psychosocial and occupational functioning were found to be markedly impaired at l-year follow-up. As appears from these data, the natural- istic course of first episode psychotic illness in ‘modern times’ is a conversion of diagnosis from a ‘holding pattern’ to schizophrenia, substantial reduction in psychotic and disorganized symptoms, persistent negative symptoms and early psychoso- cial morbidity.
Acknowledgment
This work is supported in part by NIMH Grants MH3 1593, MH40856, MH-CRC 43271; the Nellie Ball Trust Fund, Iowa State Bank and Trust Company.
References
Andreasen, N.C. (1983) The Scale for the Assessment of Negative Symptoms (SANS). The University of Iowa, Iowa City, IA.
Andreasen, N.C. (1984) The Scale for the Assessment of Positive Symptoms (SAPS). The University of Iowa, Iowa City, IA.
Andreasen, N.C. (1985) Comprehensive Assessment of Symptoms and History (CASH). The University of Iowa, Iowa City, IA.
Andreasen, N.C. (1987a) Psychiatric Symptoms You Currently have-Baseline (PSYCH-base). The University of Iowa, Iowa City, IA.
Andreasen, N.C. (1987b) Psychiatric Symptoms You Currently have-Follow-up (PSYCH-UP). The University of Iowa, Iowa City, IA.
Andreasen, N.C., Flaum, M. and Arndt, S. (1992) The compre- hensive assessment of symptoms and history (CASH): An instrument for assessing psychopathology and diagnosis. Arch. Gen. Psychiatry 49, 615-623.
APA, (1987) Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R). American Psychiatric Association, Washington, DC.
APA, (1994) Diagnostic and Statistical Manual of Mental Disorders (DSM IV). American Psychiatric Association, Washington, DC.
Amdt, S., Alliger, R.J. and Andreasen, N.C. (1991) The distinc- tion of positive and negative symptoms: The failure of a two- dimensional model. Br. J. Psychiatry 158, 317-322.
Arndt, S., Davis, C., Miller, D. and Andreasen, N. (1993) Effect of antipsychotic withdrawal on extrapyramidal symptoms: Statistical methods for analysis of single sample repeated measures data. Neuropsychopharmacology 8, 67.
Amdt, S., Andreasen, N.C., Flaum, M., Miller, D. and Nopoulos, P. (1995) A longitudinal study of symptom dimen- sions in schizophrenia. Arch. Gen. Psychiatry 52, 352-360.
Astrup, C. and Noreik, K. (1966) Functional Psychoses: Diagnostic and Prognostic Models. Charles C. Thomas, Springfield. IL.
Bilder, R.M., Lipshultz-Broth, L., Reiter, G., Geisler, S.H., Mayerhoff, D.I. and Lieberman. J.A. (1992) Intellectual deficits in first-episode schizophrenia: Evidence for pro- gressive deterioration. Schizophr. Bull. 18, 437-448.
Bleuler, E. ( 1911) (Translated by J. Zinkin; 1950) Dementia Praecox of the Group of Schizophrenias. International Universities Press, New York, NY.
12 S. Gupta et al./Schizophrenia Research 23 (1997) I-13
Bromet, E.J., Schwarrtz, J.E., Fennig, S., Geller, L., Jandorf, L., Kovasznay, B., Lavalle, J., Miller, A., Pato, C., Ram, R. and Rich, R. (1992) The epidemiology of psychosis: The Suffolk County Mental Health Project. Schizophr. Bull. 18, 243-255.
Carpenter, W.T. and Kirkpatrick, B. (1988) The heterogeneity of the long-term course of schizophrenia. Schizophr. Bull. 14, 645-659.
Carpenter, W.T. Jr., Heinrichs, D.W. and Wagman, A.M.I. (1988) Deficit and nondeficit forms of schizophrenia: The concept. Am. J. Psychiatry 145, 578583.
Ciompi, L. (1988) Learning from outcome studies: Towards a comprehensive biological-psychosocial understanding of schizophrenia. Schizophr. Res. 1, 3733384.
Dawson, M.E., Nuechterieien, H., Schell, N.K.H. and Schell, A.M. (1992) Electrodermal anomalies in recent onset schizo- phrenia: Relationships to symptoms and prognosis. Schizophr. Bull. 18, 295-311.
DeLisi, L.E. (1992) The significance of the age of onset of schizophrenia. Schizophr. Bull. 18, 209.
Eaton, W.W., Bilker, W., Haro, J.M., Herrman. H., Mortensen, P.B., Freeman, H. and Burgess, P. (1992) Long-term course of hospitalization for schizophrenia: Part II. Change with passage of time. Schizophr. Bull. 18, 229-241.
Fenton, W.S. and McGlashan, T.H. (1991) Natural history of schizophrenia, II. Positive and negative symptoms and long- term course. Arch. Gen. Psychiatry 48, 978-986.
Flaum, M., Andreasen, N.C. and Amdt, S. (1992) The Iowa Prospective Longitudinal Study of Recent Onset Psychoses: Methodological and statistical strategies. Schizophr. Bull. 18, 481-490.
Flaum, M., Hubbard, W.H., Amdt, S. and Andreasen, N.C. (1993) The validity of subjective reporting of positive and negative symptoms in schizophrenia. Schizophr. Res. 9, 92.
Ganguli, R. and Brar, J.S. (1992) Generalizability of first-epi- sode studies in schizophrenia. Schizophr. Bull. 18, 463-469.
Garmezy, N. (1970) Process and reactive schizophrenia: Some conceptions and issues. Schizophr. Bull. 3, 30-74.
Gittehnan-Klein, R. and Klein, D.F. ( 1969) Premorbid asocial adjustment and prognosis in schizophrenia. J. Psychiatr. Res. 7, 35-53.
Gupta, S., Rajaprabhakaran, R., Amdt, S., Flaum, M. and Andreasen, NC. (1995) Premorbid adjustment as a predictor of phenomenological and neurobiological indices in schizo- phrenia. Schizophr. Res. 16, 189-197.
Haas, G.L. and Sweeny, J.A. (1992) Premorbid and onset fea- tures of first-episode schizophrenia. Schizophr. Bull. 18, 373-386.
Harding, C.M., Brooks, G.W., Ashikaga, T., Strauss, J.S. and Breier, A. (1987) The Vermont longitudinal study of persons with severe mental illness, I: Methodology, study sample, and overall status 32 years later. Am. J. Psychiatry 144, 718-726.
Harris, M.J., Jeste, D.V., Krull, A., Montague, J. and Heaton, R.D. (1991) Deficit syndrome in older schizophrenic patients. Psychiatr. Res. 39, 285-292.
Harrow, M., Bromet, E. and Quinlan, D. (1974) Predictors of
posthospital adjustment in schizophrenia. J. Nerv. Ment. Dis. 158, 25-36.
Hoff, A.L., Riordan, H., O’Donnell, D., Stritzke, P., Neale, C., Boccio, A., Anand, A.K. and Delisi, L.E. (1992) Anomalous lateral sulcus asymmetry and cognitive function in first-epi- sode schizophrenia. Schizophr. Bull. 18, 257-270.
Huber, G., Gross, G. and Schuttler, R. (1975) A long-term follow-up study of schizophrenia: Psychiatric course of illness and prognosis. Acta Psychiatr. Stand. 52, 49957.
Iacono, W.G. and Beiser, M. (1992) Where are the women in first-episode studies of schizophrenia. Schizophr. Bull. 18, 471-513.
Jackson, H.J., McGorry, P.D. and Dudgeon, P. (1995) Prodromal symptoms of schizophrenia in first-episode psy- chosis: prevalence and specificity. Comp. Psychiatry 36, 241-50.
Keshavan, M.S. and Schooler, N.R. (1992) First-episode studies in schizophrenia. Schizophr. Bull, 18, 491-513.
Kirch, D.G., Keith, S.M. and Mathews, M. (1992) Research on first episode psychosis: Report on a National Institute of Mental Health Workshop. Schizophr. Bull. 18, 179-184.
Kraepelin, E., Barclay, R.M. and Robertson, G.M. (1919) Dementia Praecox and Paraphrenia. E&S Livingstone, Edinburgh.
Kulhara, P., Kota, S.K. and Joseph, S. (1986) Positive and negative subtypes of schizophrenia: A study from India. Acta Psychiatr. Stand. 74, 3533359.
Lieberman, J.A., Alvir, M.J., Woemer, M., Degreef, G., Bilder, R.M., Ashtari, M., Bogerts, B., Mayerhoff, D.I., Geisler, S.H., Loebel, A., Levy, D.L., Hinrichsen, G., Szymanski, S., Chakos, M., Koreen, A., Borenstein, M. and Kane, J.M. (1992a) Prospective study of psychobiology in first-episode schizophrenia at Hillside Hospital. Schizophr. Bull. 18, 351-371.
Lieberman, J.A., Matthews, S.M. and Kirch, D.G. (1992b) First-episode psychosis: Part II. Editors’ introduction. Schizophr. Bull. 18, 349-350.
Mayerhoff, D.I., Loebel, A.D., Alvir, J.M.J., Szymanski, S., Geisler, S.H., Borenstein, M. and Lieberman, J.A. (1994) The deficit state in first-episode schizophrenia. Am. J. Psychiatry 151, 1417-1422.
McGlashan, T.H. (1984) The chestnut lodge follow-up study: I. Follow-up methodology and study sample. Arch. Gen. Psychiatry 41, 573-585.
Miller, D.D., Arndt, S. and Andreasen, N.C. (1993) Alogia, attentional impairment, and inappropriate affect: Their status in the dimensions of schizophrenia. Comp. Psychiatry 34, 221-226.
Minas, I.H., Stuart, G.W., Klimidis, S., Jackson, H.J., Singh, B.S. and Copolov, D.L. (1992) Positive and negative symp- toms in the psychoses: Multidimensional scaling of SAPS and SANS items. Schizophr. Res. 8, 1433156.
Peralta, V., De Leon, J. and Cuesta, M.J. (1992) Are there more than two syndromes in schizophrenia: A critique of the positive-negative dichotomy. Br. J. Psychiatry 161, 335-343.
Ram, R., Bromet, E.J., Eaton, W.W., Pato, C. and Schwartz,

S. Gupta et al./Schizophrenia Research 23 (1997) l-13 13
J.E. (1992) The natural course of schizophrenia: A review of first-admission studies. Schizophr. Bull. 18, 185-207.
Shtasel, D.L., Gur, R.E., Gallacher, F., Heimberg, C., Cannon, T. and Gur, R.C. (1992) Phenomenology and functioning in first-episode schizophrenia. Schizophr. Bull. 18, 4499462.
Siegel, S. (1956) The case of two related samples. In: Nonparametric Statistics for the Behavioral Sciences. McGraw-Hill, New York, NY, pp. 63-67.
Stephens, J.H., Astrup, C. and Mangrum, J.C. (1966) Prognostic factors in recovered and deteriorated schizophre- nics. Am. J. Psychiatry 122, 1116-1121.
Strakowski, SM., Keck, P.E.J., Lonczak, H.S. and West, S.A. (1995) Chronology of comorbid and principal syndromes in first-episode psychosis. Comp. Psychiatry 36, 106-l 12.
Strauss, J.S. and Carpenter, W.T. (1972) The prediction of out- come in schizophrenia. Arch. Gen. Psychiatry 27, 739-746.
Sweeny, J.A., Haas, G.L. and Li, S. (1992) Neuropsychological
and eye movement abnormalities in first-episode and chronic schizophrenia. Schizophr. Bull. 18, 283-293.
Tohen, M., Stoll, A.L., Strakowski, S.M., Faedda, G.L., Mayer, P.V., Goodwin, D.C., Kolbrener, M.L. and Madigan, A.M. (1992) The McLean first-episode psychosis project: Six month recovery and recurrence outcome. Schizophr. Bull. 18, 273-282.
Tsuang, M.T., Woolson, R.F. and Fleming, J.A. ( 1979) Long- term outcome of major psychoses: I. Schizophrenia and affective disorders compared with psychiatrically symptom- free surgical conditions. Arch. Gen. Psychiatry 36, 1295-1301.
Vaillant, G.E. (1964) Prospective prediction of schizophrenic remission. Arch. Gen. Psychiatry 11, 5099518.
Wahl, O.F. and Hunter, J. (1992) Are gender effects being neglected in schizophrenia research? Schizophr. Bull. 18, 313-318.




















