Violence in first episode psychosis : a systematic review and meta-analysis
12
Review Violence in first-episode psychosis: A systematic review and meta-analysis Matthew M. Large a,b , Olav Nielssen c,d, ⁎ a The Prince of Wales Hospital, Randwick, Sydney, Australia b School of Psychiatry, University of New South Wales, Sydney, Australia c Clinical Research Unit for Anxiety and Depression at St Vincent's Hospital, Sydney, Australia d Discipline of Psychiatry, Sydney Medical School, University of Sydney, Sydney, Australia article info abstract Article history: Received 4 August 2010 Received in revised form 14 November 2010 Accepted 29 November 2010 Available online 5 January 2011 Background: Violence towards others is a recognised complication of first-episode psychosis. Aims: To estimate the rate of violence and the associations with violence in first-episode psychosis. Method: A systematic review and meta-analysis of 9 studies. Results: Pooled estimates of the proportion of patients with first-episode psychosis committing any violence, serious violence and severe violence were 34.5%, 16.6% and 0.6%, respectively. Violence of any severity was associated with involuntary treatment (OR = 3.84), a forensic history (OR = 3.28), hostile affect (OR = 3.52), symptoms of mania (OR = 2.86), illicit substance use (OR = 2.33), lower levels of education (OR = 1.99), younger age (OR = 1.85), male sex (OR = 1.61) and the duration of untreated psychosis (OR = 1.56). Serious violence was associated with a forensic history (OR = 4.42), the duration of untreated psychosis (OR = 2.76) and total symptom scores (OR = 2.05). Violence in the period after initiation of treatment for first-episode psychosis was associated with involuntary treatment (OR = 5.71). Conclusions: A substantial proportion of patients in first-episode psychosis commit an act of violence before presenting for treatment, including a number who commit an act of more serious violence causing injury to another person. However, severe violence resulting in serious or permanent injury to the victim is uncommon in this population. © 2010 Elsevier B.V. All rights reserved. Keywords: First-episode psychosis First-episode schizophrenia Schizophrenia Violence Aggression Risk assessment 1. Introduction Violence is defined in the Oxford Dictionary as “behaviour involving physical force intended to hurt, injure or kill” and denotes a wide range of behaviours from destructive acts, minor assaults, assaults using a weapon, sexual assaults, and severe violence causing injury or even death. The terms violence and aggression have sometimes been used synony- mously, but aggression is a broader term and includes a forceful or hostile attitude, whereas violence refers to the use of actual physical force. In this paper we report a meta-analysis of studies of physical violence occurring in association with first-episode psychosis. The vast majority of patients with schizophrenia will never commit an act of severe violence. However, most researchers agree that there is a modest but consistent association between psychosis and violent offending (Arseneault et al., 2000; Elbogen and Johnson, 2009; Fazel et al., 2009a; Modestin and Ammann, 1996; Wallace et al., 2004) and that rates of violence are particularly high among cohorts of patients who have both schizophrenia and substance abuse disorders (Elbogen and Johnson, 2009; Fazel et al., 2009b; Swanson et al., 2006). Although only a small proportion of all homicides are committed by patients with schizophrenia (Large et al., 2009b), there is a statistical association between homicide and schizophrenia (Fazel et al., 2009a), almost half of those homicides are committed before treatment with antipsychotic medication (Large and Nielssen, 2008), and the risk of homicide Schizophrenia Research 125 (2011) 209–220 ⁎ Corresponding author. Discipline of Psychiatry, Sydney Medical School, University of Sydney, Sydney, Australia. Tel.: +61 2 92210688. E-mail address: [email protected] (O. Nielssen). 0920-9964/$ – see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2010.11.026 Contents lists available at ScienceDirect Schizophrenia Research journal homepage: www.elsevier.com/locate/schres
Transcript of Violence in first episode psychosis : a systematic review and meta-analysis
Schizophrenia Research 125 (2011) 209–220
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r.com/ locate /schres
Review
Violence in first-episode psychosis: A systematic review and meta-analysis
Matthew M. Large a,b, Olav Nielssen c,d,⁎a The Prince of Wales Hospital, Randwick, Sydney, Australiab School of Psychiatry, University of New South Wales, Sydney, Australiac Clinical Research Unit for Anxiety and Depression at St Vincent's Hospital, Sydney, Australiad Discipline of Psychiatry, Sydney Medical School, University of Sydney, Sydney, Australia
a r t i c l e i n f o
⁎ Corresponding author. Discipline of Psychiatry, SyUniversity of Sydney, Sydney, Australia. Tel.: +61 2 9
E-mail address: [email protected] (O. Nielsse
0920-9964/$ – see front matter © 2010 Elsevier B.V.doi:10.1016/j.schres.2010.11.026
a b s t r a c t
Article history:Received 4 August 2010Received in revised form 14 November 2010Accepted 29 November 2010Available online 5 January 2011
Background: Violence towards others is a recognised complication of first-episode psychosis.Aims: To estimate the rate of violence and the associations with violence in first-episodepsychosis.Method: A systematic review and meta-analysis of 9 studies.Results: Pooled estimates of the proportion of patients with first-episode psychosis committingany violence, serious violence and severe violence were 34.5%, 16.6% and 0.6%, respectively.Violence of any severity was associated with involuntary treatment (OR=3.84), a forensichistory (OR=3.28), hostile affect (OR=3.52), symptoms of mania (OR=2.86), illicitsubstance use (OR=2.33), lower levels of education (OR=1.99), younger age (OR=1.85),male sex (OR =1.61) and the duration of untreated psychosis (OR=1.56). Serious violencewas associated with a forensic history (OR=4.42), the duration of untreated psychosis(OR=2.76) and total symptom scores (OR=2.05). Violence in the period after initiation oftreatment for first-episode psychosis was associated with involuntary treatment (OR=5.71).Conclusions: A substantial proportion of patients in first-episode psychosis commit an act ofviolence before presenting for treatment, including a number who commit an act of moreserious violence causing injury to another person. However, severe violence resulting in seriousor permanent injury to the victim is uncommon in this population.
© 2010 Elsevier B.V. All rights reserved.
Keywords:First-episode psychosisFirst-episode schizophreniaSchizophreniaViolenceAggressionRisk assessment
1. Introduction
Violence is defined in the Oxford Dictionary as “behaviourinvolving physical force intended to hurt, injure or kill” anddenotes a wide range of behaviours from destructive acts,minor assaults, assaults using a weapon, sexual assaults, andsevere violence causing injury or even death. The termsviolence and aggression have sometimes been used synony-mously, but aggression is a broader termand includes a forcefulor hostile attitude, whereas violence refers to the use of actualphysical force. In this paperwe report ameta-analysis of studies
dney Medical School,2210688.n).
All rights reserved.
of physical violence occurring in association with first-episodepsychosis.
The vast majority of patients with schizophrenia will nevercommit an act of severe violence. However, most researchersagree that there is amodest but consistent association betweenpsychosis and violent offending (Arseneault et al., 2000;Elbogen and Johnson, 2009; Fazel et al., 2009a; Modestin andAmmann, 1996;Wallace et al., 2004) and that rates of violenceare particularly high among cohorts of patients who have bothschizophrenia and substance abuse disorders (Elbogen andJohnson, 2009; Fazel et al., 2009b; Swanson et al., 2006).Although only a small proportion of all homicides arecommitted by patients with schizophrenia (Large et al.,2009b), there is a statistical association between homicideand schizophrenia (Fazel et al., 2009a), almost half of thosehomicides are committed before treatment with antipsychoticmedication (Large andNielssen, 2008), and the riskof homicide

210 M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
in never-treated schizophrenia has been estimated to be one in630 presentations (Nielssen and Large, 2010). Case linkagestudies have found that up to half of the offending by peoplewith schizophrenia occurs before contact with mental healthservices (Munkner et al., 2003;Wallace et al., 2004), suggestingthat early psychosis could also be a time of increased risk forless severe forms of violence. A number of factors have beenidentified as being associatedwith violence in psychotic illness,including aspects of the patients’ circumstances, substance useand antisocial personality traits. However, change in behaviourarising from emerging psychosis is likely to be an importantfactor in many cases.
Minor forms of violence and assaults that have notnecessarily resulted in criminal charges are often reported atthe time of initial presentation of psychotic illness (Humphreyset al., 1992; Volavka et al., 1997). Several recent studies haveexamined the rates of violence prior to treatment and thefactors associated with violence in samples of patients withfirst-episode schizophrenia (Deanet al., 2007; Foleyet al., 2005;Harris et al., 2010; Milton et al., 2001; Steinert et al., 1999;Verma et al., 2005). A better understanding of the factorsassociated with violence prior to treatment could help preventsome acts of violence, including severe forms of violence suchas homicide and violence resulting in serious criminal charges,which are more common in first-episode psychosis.
We present a systematic review and meta-analysis of theclinical and other factors associated with violence amongcohorts of patients with first-episode psychosis. Meta-analysis summarises the findings of earlier research andminimises the likelihood of both type-I errors due to chancefindings and of type-II errors arising when true associationsare not detected in individual studies (Stroup et al., 2000).
Fig. 1. Flow chart
2. Methods
2.1. Search strategies
For the purpose of this review, three data-bases (Medline,Embase and Psycinfo) were searched for papers publishedbefore July 2010, using a broad range of search terms (seeFig. 1 for search terms and search time frames). ON and MLconducted the searches independently, locating the same setof abstracts and full-text papers. All but one recent study hadbeen previously located during systematic searches con-ducted for earlier reviews (Large and Nielssen, 2008; Largeet al., 2009b; Nielssen et al., in press; Nielssen and Large,2010). No additional studies were located by hand searchingthe reference lists of included studies or by examining thetitles of the first 1000 hits in Google Scholar using the terms“first-episode psychosis AND aggression”.
2.2. Inclusion and exclusion criteria
The definition of violence and the inclusion and exclusioncriteria were agreed upon prior to the searches and selection ofstudies.
Studies were included if they reported a cohort of patientswith first-episode psychosis and compared the characteristicsof the patients who had committed an act of violence withthose of non-violent controls. We included studies of patientswith schizophrenia, non-affective psychosis, bipolar disorderand psychotic depression. Studies reporting violent behaviourprior to contact with health services or violence during theinitial period of treatment for psychotic illness were included.
of searches.

211M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
Studies examining aggressive attitude or hostility withoutspecifying whether any violence took place were excluded, aswere studies of psychosis among those charged with criminaloffences if they did not differentiate between violent andnon-violent offences.
2.3. Definitions of less serious, more serious and severe violence
Less serious violence was defined as physical violenceagainst objects and assault not causing physical injury.
Serious violencewasdefinedalong the lines suggestedby theMacarthur violence risk assessment study (Steadman et al.,1998) as assault causing any degree of injury, any use of aweapon, or any sexual assault. The term any violence was usedwhen the severity of the violence was not specified, althoughourdefinitionof anyviolencediffered fromthat of theMacarthurstudy because we did not include verbal aggression. A plannedsubgroup analysis of the factors associated with seriousviolence used the definition of serious violence contained inthe Macarthur study.
Severe violence was defined as violence resulting inserious injury that required treatment in hospital or resultedin permanent physical harm to the victim.
2.4. Data extraction
Data were extracted independently by ON and ML. Therewas disagreement about the value in 12 of approximately 450data points, most of which related to the value of thedenominators in some studies. Disagreements were resolvedby a further joint examination of the papers and clarificationby email correspondence with the authors of several studies.Variables reported in two or more studies were included inthe meta-analysis. The definitions of the included variableswere taken from the studies themselves. For example, therewere a range of definitions of long duration of untreatedpsychosis, with some studies recording counts above andbelow median values and other studies providing means andstandard deviations in violent and non-violent groups. Thevariable ‘forensic history’ included studies reporting a historyof prior violence or any criminal convictions.
2.5. Meta-analysis
Comprehensive Meta-Analysis (CMA) version 2.2 software(Borenstein et al., 2005)was used to calculate pooled estimatesof the proportion of patients with a history of violence and theassociations with violence. An a priori choice of a random-effects model was made because the studies differed in theirinclusion criteria with respect to diagnosis, age and otherfactors. In these circumstances, a random-effects modelincreases the confidence in any statistically significant associa-tions foundbymeta-analysis, although it has reduced statisticalpower when compared with a fixed-effects model when thereare a small number of studies. Odds ratios were used to expressthe effect size because almost all of the data were categorical.Effect sizes were classified as weak (OR between 1.5 and 2.5),moderate (OR, between 2.5 and 4), strong (OR, between 4 and10) or very strong (OR, greater than 10) (Rosenthal, 1996). Nocorrectionwasmade to significance testing because ofmultiplemeta-analyses. However, assuming 20 independent observa-
tions, a P-value of b0.0025 would be unlikely to result from atype-I error. Statistical heterogeneity was assessed using a Q-value and I-square statistic or each factor. An I-square of over 50and significant Q-value indicate that the study parametersbeing considered were not randomly drawn from a singleunderlyingpopulation—anassumption thatwehadmade on ana priori basis when choosing a random-effects model. I-squarestatistics are a more reliable guide to between study heteroge-neity than other statistics when there are a small number ofstudies. Possible publication biaswas assessedwith a fail-safeNfor significant variables, where N is the number of studies withan effect size of zero needed to reduce P to ≤0.05.
2.6. Subgroup analysis
A subgroup analysis was performed using data fromstudies that separately reported patients who committedmore serious forms of violence, as defined by the MacArthurstudy (Steadman et al., 1998). In the subgroup analysis,patients responsible for less serious violence were included inthe control group to minimise the risk of type one error.
A further subgroup analysis examined the characteristics ofpatientswhowere violent in theperiod after initial presentation.
3. Results
3.1. Searches
Systematic searches yielded 56 articles thatwere thought tobe relevant, of which 24 were examined in full text afterviewing the abstract (Fig. 1, flow chart of searches). One studythat examined aggressive attitude or hostility without specify-ing whether any violence took place was excluded (Ceskovaet al., 2008). Several studies reporting rates of criminalconviction in cohorts of first-episode psychosis that didnot report the characteristics of the violent and non-violentsubjects separately were also excluded (Bhugra et al., 2000;Payne et al., 2006; Rowlands, 2001). No studies from forensicsettings could be included because none of those studiesreported a control group of non-violent subjects.
Nine studies met the inclusion criteria (Dean et al., 2007;Foley et al., 2005; Harris et al., 2010; Humphreys et al., 1992;Milton et al., 2001; Spidel et al., 2010; Steinert et al., 1999;Verma et al., 2005; Volavka et al., 1997) (Table 1). Furtherinformation about the subjects of five of these studies wasavailable from related publications (Brewin et al., 1997; Foleyet al., 2007; Harris et al., 2005; Johnstone et al., 1986; Sartoriuset al., 1986). The studies were all of high quality and usedsystematic methods to determine the diagnosis of psychosis,record the clinical data and collect information about violence.The studies reported overlapping sets of variables andnot everystudy made a distinction between less and more seriousviolence. Eight studies examined violence before or duringinitial treatment for psychosis and three studies examinedviolence in the period after initial treatment.
3.2. Meta-analysis of rates of less serious, more serious and severeviolence
Meta-analysis of six studies (Dean et al., 2007; Foley et al.,2005; Harris et al., 2010; Milton et al., 2001; Steinert et al.,
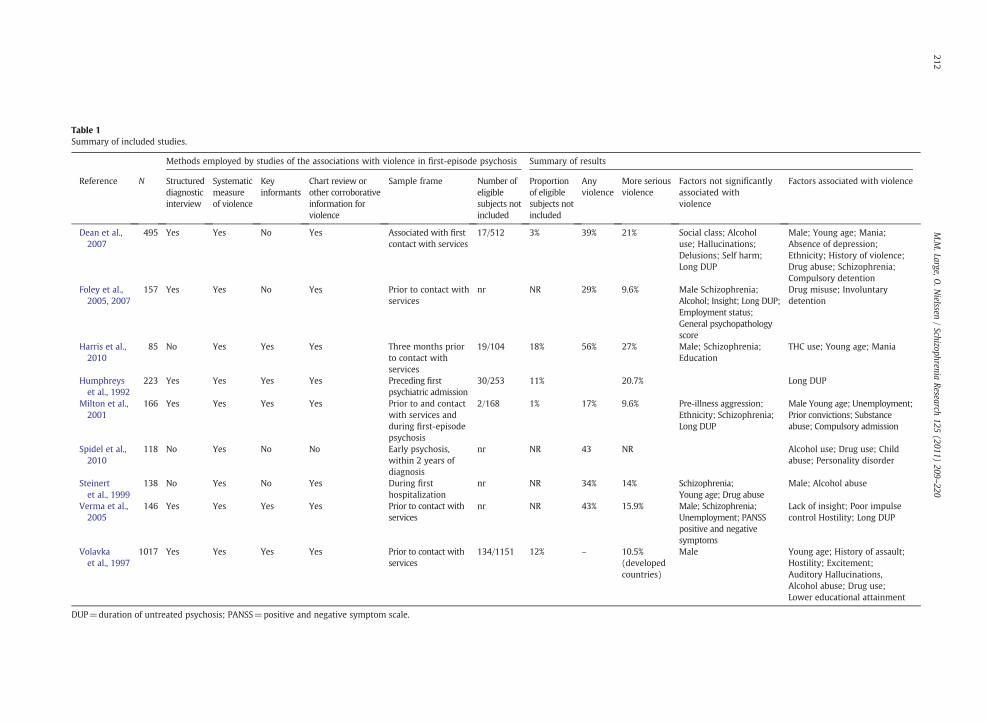
Table 1Summary of included studies.
Methods employed by studies of the associations with violence in first-episode psychosis Summary of results
Reference N Structureddiagnosticinterview
Systematicmeasureof violence
Keyinformants
Chart review orother corroborativeinformation forviolence
Sample frame Number ofeligiblesubjects notincluded
Proportionof eligiblesubjects notincluded
Anyviolence
More seriousviolence
Factors not significantlyassociated withviolence
Factors associated with violence
Dean et al.,2007
495 Yes Yes No Yes Associated with firstcontact with services
17/512 3% 39% 21% Social class; Alcoholuse; Hallucinations;Delusions; Self harm;Long DUP
Male; Young age; Mania;Absence of depression;Ethnicity; History of violence;Drug abuse; Schizophrenia;Compulsory detention
Foley et al.,2005, 2007
157 Yes Yes No Yes Prior to contact withservices
nr NR 29% 9.6% Male Schizophrenia;Alcohol; Insight; Long DUP;Employment status;General psychopathologyscore
Drug misuse; Involuntarydetention
Harris et al.,2010
85 No Yes Yes Yes Three months priorto contact withservices
19/104 18% 56% 27% Male; Schizophrenia;Education
THC use; Young age; Mania
Humphreyset al., 1992
223 Yes Yes Yes Yes Preceding firstpsychiatric admission
30/253 11% 20.7% Long DUP
Milton et al.,2001
166 Yes Yes Yes Yes Prior to and contactwith services andduring first-episodepsychosis
2/168 1% 17% 9.6% Pre-illness aggression;Ethnicity; Schizophrenia;Long DUP
Male Young age; Unemployment;Prior convictions; Substanceabuse; Compulsory admission
Spidel et al.,2010
118 No Yes No No Early psychosis,within 2 years ofdiagnosis
nr NR 43 NR Alcohol use; Drug use; Childabuse; Personality disorder
Steinertet al., 1999
138 No Yes No Yes During firsthospitalization
nr NR 34% 14% Schizophrenia;Young age; Drug abuse
Male; Alcohol abuse
Verma et al.,2005
146 Yes Yes Yes Yes Prior to contact withservices
nr NR 43% 15.9% Male; Schizophrenia;Unemployment; PANSSpositive and negativesymptoms
Lack of insight; Poor impulsecontrol Hostility; Long DUP
Volavkaet al., 1997
1017 Yes Yes Yes Yes Prior to contact withservices
134/1151 12% – 10.5%(developedcountries)
Male Young age; History of assault;Hostility; Excitement;Auditory Hallucinations,Alcohol abuse; Drug use;Lower educational attainment
DUP=duration of untreated psychosis; PANSS=positive and negative symptom scale.
212M.M
.Large,O.N
ielssen/Schizophrenia
Research125
(2011)209
–220

213M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
1999; Verma et al., 2005) found the pooled estimate ofthe proportion of patients with any degree of violence priorto contact with mental health services or during the firstepisode of psychosis to be 35.4% (95% CI 26.8–45.1%; heteroge-neity, I-square=89.2, Q-value=46.7, df=5, P≤0.001). Thisfigure included less and more serious violence and a smallnumber of cases of severe violence.
Meta-analysis of eight studies (Dean et al., 2007; Foley et al.,2005; Harris et al., 2010; Humphreys et al., 1992; Milton et al.,2001; Steinert et al., 1999; Verma et al., 2005; Volavka et al.,1997) found that the pooled estimate for the rate ofmore seriousviolence (excluding less serious violence and including casesof severe violence)was 16.6% (95%CI 12.9–21.3%; heterogeneity,I-square=81.5, Q-value=37.8, df=7, P≤0.001). One studythat reportedassaults of unspecified severitywas included in thisgroup (Volavka et al., 1997).
Three studies with a total of 527 patients each reportedone patient who committed an act of severe violenceresulting in the victim sustaining permanent injury (Foleyet al., 2005; Humphreys et al., 1992; Steinert et al., 1999) anda fourth study (Harris et al., 2010) noted the absence of anyepisodes of severe violence among 85 subjects. Meta-analysisof these 4 studies found a pooled estimate of 0.6% of subjectscommitted acts of severe violence (95% 0.2–1.7%; heteroge-neity, I-square=0.00, Q-value =0.15, df=3, P=0.99).
3.3. Meta-analysis of the associationswith violence infirst-episodepsychosis
Meta-analysis was used to pool the findings of eightstudies examining the clinical factors associated with anyform of violence. A total of 23 factors that were reported in 2
Table 2Meta-analysis of factors associated with any violence during first-episode psychosi
Groups Effect size and 95% interval Teshy(tw
Group Point estimate Lower limit Upper limit Z-v
Alcohol use 1.43 0.91 2.24 1.Depressed mood 0.57 0.31 1.06 -1.Drug use 2.33 1.49 3.63 3.Duration of untreated psychosis(DUP)
1.56 1.05 2.31 2.
Ethnic minority 1.26 0.74 2.15 0.Forensic history 3.28 1.75 6.14 3.General psychopathology 1.40 0.85 2.29 1.Hostility 3.52 2.09 5.92 4.Insidious onset of psychosis 1.15 0.61 2.17 0.Less education 1.99 1.06 3.70 2.Less insight 1.31 0.69 2.51 0.Lives alone 1.04 0.34 3.17 0.Low socio-economic status 1.55 0.90 2.66 1.Male 1.61 1.15 2.26 2.Manic symptoms 2.86 1.87 4.38 4.Involuntary treatment 3.84 2.19 6.73 4.Negative symptoms 0.82 0.44 1.54 -0.Positive symptoms 1.20 0.85 1.71 1.Schizophrenia 1.02 0.65 1.58 0.Self harm 1.22 0.41 2.36 -0.Single 1.56 0.73 3.35 1.Unemployment 1.35 0.73 2.49 0.Younger age 1.85 1.28 2.69 3.
or more studies were included in the meta-analysis. Thesewere grouped into demographic factors (Table 2, Fig. 2),factors in the patients’ history (Table 2, Fig. 3) and factors inthe patients’ mental state (Table 2, Fig. 4).
Moderate associations (defined as an ORN2.5) were foundbetween any violence and the following factors: a forensichistory (including a history of earlier violence), hostility,manic symptoms and the need for involuntary treatment.Weak associations (OR 1.5–2.5) were found between anyviolence and the following factors: younger age, male sex,lower levels of education, the duration of untreated psychosisand illegal drug use.
3.4. Meta-analysis of associations with serious violence
Meta-analysis of three studies (Harris et al., 2010; Miltonet al., 2001; Verma et al., 2005) found that the factors associatedwith more serious forms of violence differed from thoseassociatedwith anyviolence. A forensic history, longerdurationof untreated psychosis and higher levels of psychopathologywere associated with more serious violence (Table 3, Fig. 5).
3.5. Meta-analysis of associationswith any violence after treatmentfor first-episode psychosis
Meta-analysis of three studies (Foley et al., 2005; Miltonet al., 2001; Spidel et al., 2010) reporting the factorsassociated with violence in the period following the initialtreatment of first-episode psychosis found that involuntarytreatment was the only factor found to be associated withsubsequent violence (Table 4, Fig. 6).
s.
t of nullpothesiso-tailed)
Heterogeneity Failsafe N
alue P-value Q-value df (Q) P-value I-Squared Missing studies
55 0.12 2.49 4.00 0.65 0.0077 0.08 4.52 1.00 0.03 77.8772 0.0002 10.43 4.00 0.03 61.64 3622 0.03 25.27 5.00 0.00 80.21 11
85 0.40 3.60 2.00 0.17 44.4772 0.0002 5.18 2.00 0.08 61.37 1533 0.18 6.79 4.00 0.15 41.0574 b0.0001 6.15 3.00 0.10 51.25 4445 0.66 3.11 1.00 0.08 67.8716 0.03 0.20 1.00 0.66 0.0083 0.41 3.37 2.00 0.19 40.5907 0.94 4.08 1.00 0.04 75.4758 0.11 7.48 1.00 0.01 86.6379 0.01 6.57 7.00 0.48 0.00 3283 b0.0001 2.67 4.00 0.62 0.00 7371 b0.0001 0.22 2.00 0.90 0.00 3861 0.54 0.12 2.00 0.94 0.0003 0.30 18.65 6.00 0.001 67.8307 0.95 0.89 4.00 0.93 0.0003 0.98 9.05 1.00 0.001 88.9515 0.25 2.51 1.00 0.11 60.2396 0.34 6.39 2.00 0.04 68.6925 0.001 4.26 5.00 0.51 0.00 43
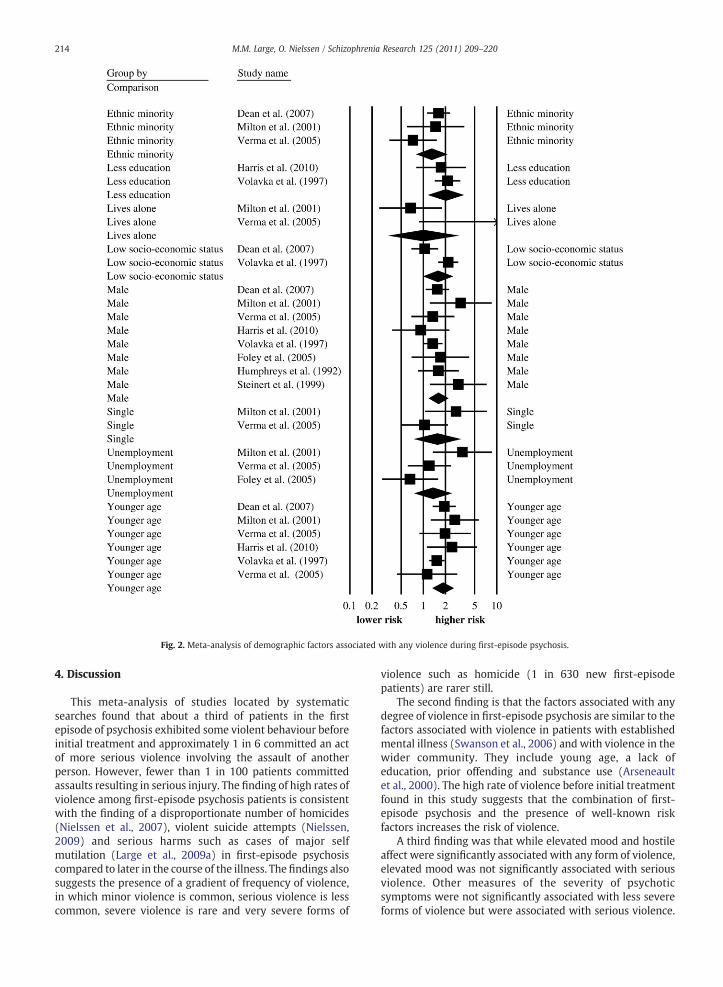
Fig. 2. Meta-analysis of demographic factors associated with any violence during first-episode psychosis.
214 M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
4. Discussion
This meta-analysis of studies located by systematicsearches found that about a third of patients in the firstepisode of psychosis exhibited some violent behaviour beforeinitial treatment and approximately 1 in 6 committed an actof more serious violence involving the assault of anotherperson. However, fewer than 1 in 100 patients committedassaults resulting in serious injury. The finding of high rates ofviolence among first-episode psychosis patients is consistentwith the finding of a disproportionate number of homicides(Nielssen et al., 2007), violent suicide attempts (Nielssen,2009) and serious harms such as cases of major selfmutilation (Large et al., 2009a) in first-episode psychosiscompared to later in the course of the illness. The findings alsosuggests the presence of a gradient of frequency of violence,in which minor violence is common, serious violence is lesscommon, severe violence is rare and very severe forms of
violence such as homicide (1 in 630 new first-episodepatients) are rarer still.
The second finding is that the factors associated with anydegree of violence in first-episode psychosis are similar to thefactors associated with violence in patients with establishedmental illness (Swanson et al., 2006) and with violence in thewider community. They include young age, a lack ofeducation, prior offending and substance use (Arseneaultet al., 2000). The high rate of violence before initial treatmentfound in this study suggests that the combination of first-episode psychosis and the presence of well-known riskfactors increases the risk of violence.
A third finding was that while elevated mood and hostileaffect were significantly associated with any form of violence,elevated mood was not significantly associated with seriousviolence. Other measures of the severity of psychoticsymptoms were not significantly associated with less severeforms of violence but were associated with serious violence.
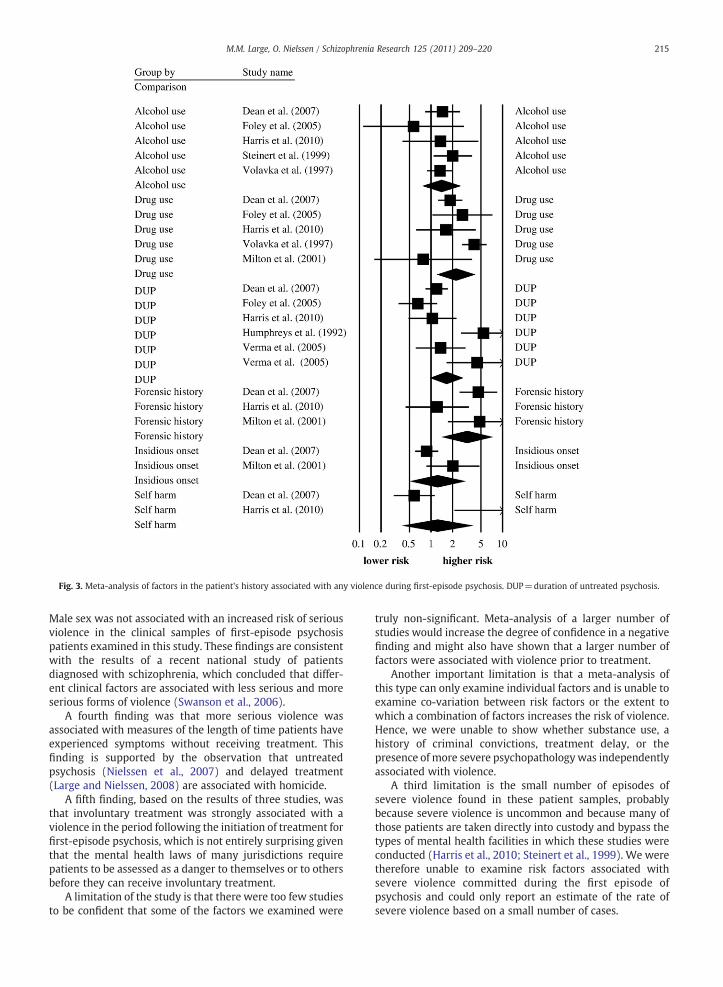
Fig. 3. Meta-analysis of factors in the patient's history associated with any violence during first-episode psychosis. DUP=duration of untreated psychosis.
215M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
Male sex was not associated with an increased risk of seriousviolence in the clinical samples of first-episode psychosispatients examined in this study. These findings are consistentwith the results of a recent national study of patientsdiagnosed with schizophrenia, which concluded that differ-ent clinical factors are associated with less serious and moreserious forms of violence (Swanson et al., 2006).
A fourth finding was that more serious violence wasassociated with measures of the length of time patients haveexperienced symptoms without receiving treatment. Thisfinding is supported by the observation that untreatedpsychosis (Nielssen et al., 2007) and delayed treatment(Large and Nielssen, 2008) are associated with homicide.
A fifth finding, based on the results of three studies, wasthat involuntary treatment was strongly associated with aviolence in the period following the initiation of treatment forfirst-episode psychosis, which is not entirely surprising giventhat the mental health laws of many jurisdictions requirepatients to be assessed as a danger to themselves or to othersbefore they can receive involuntary treatment.
A limitation of the study is that there were too few studiesto be confident that some of the factors we examined were
truly non-significant. Meta-analysis of a larger number ofstudies would increase the degree of confidence in a negativefinding and might also have shown that a larger number offactors were associated with violence prior to treatment.
Another important limitation is that a meta-analysis ofthis type can only examine individual factors and is unable toexamine co-variation between risk factors or the extent towhich a combination of factors increases the risk of violence.Hence, we were unable to show whether substance use, ahistory of criminal convictions, treatment delay, or thepresence of more severe psychopathology was independentlyassociated with violence.
A third limitation is the small number of episodes ofsevere violence found in these patient samples, probablybecause severe violence is uncommon and because many ofthose patients are taken directly into custody and bypass thetypes of mental health facilities in which these studies wereconducted (Harris et al., 2010; Steinert et al., 1999). We weretherefore unable to examine risk factors associated withsevere violence committed during the first episode ofpsychosis and could only report an estimate of the rate ofsevere violence based on a small number of cases.
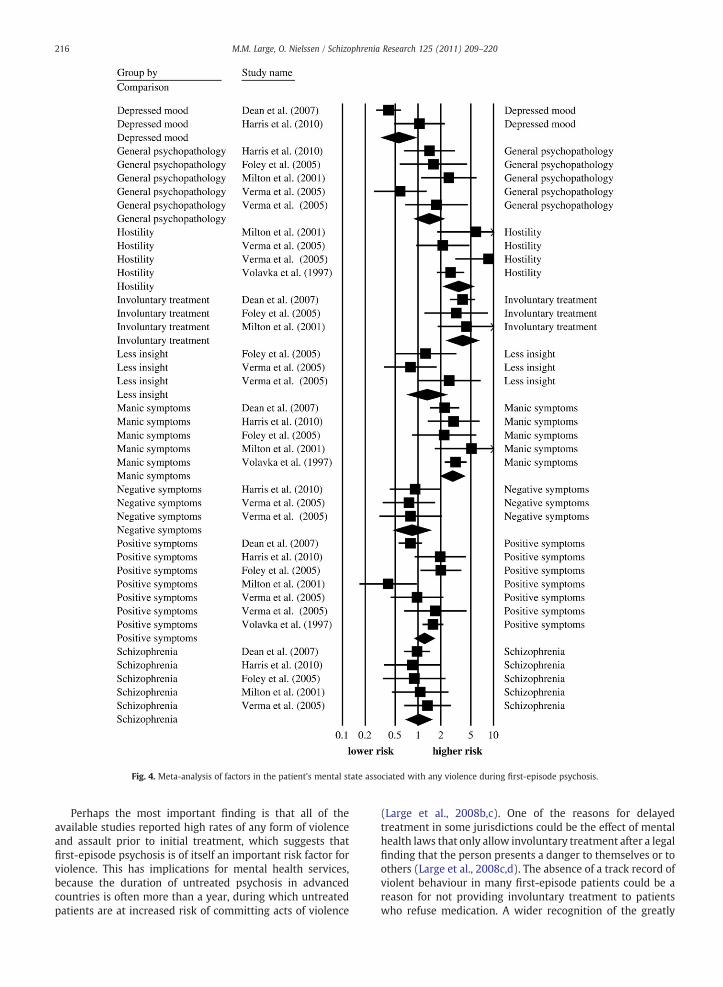
Fig. 4. Meta-analysis of factors in the patient's mental state associated with any violence during first-episode psychosis.
216 M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
Perhaps the most important finding is that all of theavailable studies reported high rates of any form of violenceand assault prior to initial treatment, which suggests thatfirst-episode psychosis is of itself an important risk factor forviolence. This has implications for mental health services,because the duration of untreated psychosis in advancedcountries is often more than a year, during which untreatedpatients are at increased risk of committing acts of violence
(Large et al., 2008b,c). One of the reasons for delayedtreatment in some jurisdictions could be the effect of mentalhealth laws that only allow involuntary treatment after a legalfinding that the person presents a danger to themselves or toothers (Large et al., 2008c,d). The absence of a track record ofviolent behaviour in many first-episode patients could be areason for not providing involuntary treatment to patientswho refuse medication. A wider recognition of the greatly
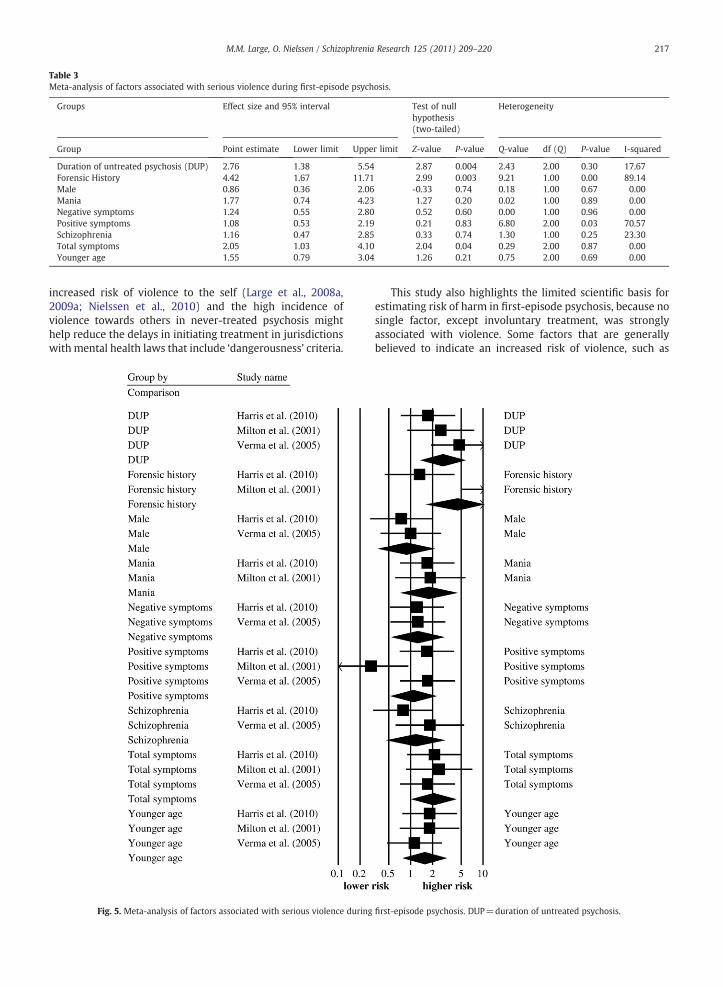
Table 3Meta-analysis of factors associated with serious violence during first-episode psychosis.
Groups Effect size and 95% interval Test of nullhypothesis(two-tailed)
Heterogeneity
Group Point estimate Lower limit Upper limit Z-value P-value Q-value df (Q) P-value I-squared
Duration of untreated psychosis (DUP) 2.76 1.38 5.54 2.87 0.004 2.43 2.00 0.30 17.67Forensic History 4.42 1.67 11.71 2.99 0.003 9.21 1.00 0.00 89.14Male 0.86 0.36 2.06 -0.33 0.74 0.18 1.00 0.67 0.00Mania 1.77 0.74 4.23 1.27 0.20 0.02 1.00 0.89 0.00Negative symptoms 1.24 0.55 2.80 0.52 0.60 0.00 1.00 0.96 0.00Positive symptoms 1.08 0.53 2.19 0.21 0.83 6.80 2.00 0.03 70.57Schizophrenia 1.16 0.47 2.85 0.33 0.74 1.30 1.00 0.25 23.30Total symptoms 2.05 1.03 4.10 2.04 0.04 0.29 2.00 0.87 0.00Younger age 1.55 0.79 3.04 1.26 0.21 0.75 2.00 0.69 0.00
217M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
increased risk of violence to the self (Large et al., 2008a,2009a; Nielssen et al., 2010) and the high incidence ofviolence towards others in never-treated psychosis mighthelp reduce the delays in initiating treatment in jurisdictionswith mental health laws that include ‘dangerousness’ criteria.
Fig. 5. Meta-analysis of factors associated with serious violence during
This study also highlights the limited scientific basis forestimating risk of harm in first-episode psychosis, because nosingle factor, except involuntary treatment, was stronglyassociated with violence. Some factors that are generallybelieved to indicate an increased risk of violence, such as
first-episode psychosis. DUP=duration of untreated psychosis.
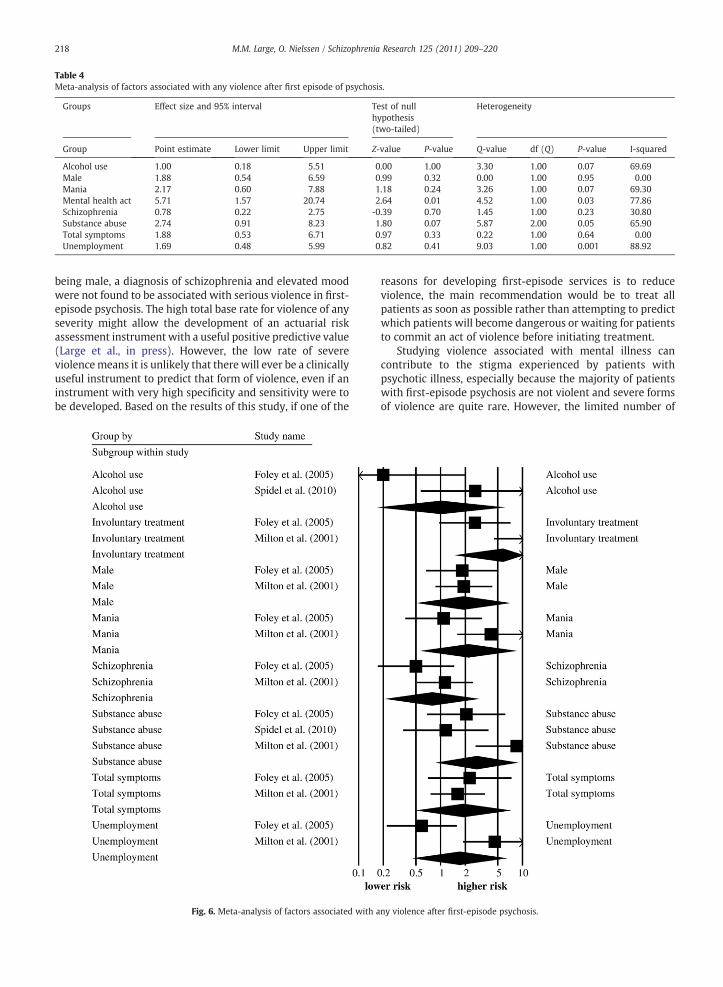
Table 4Meta-analysis of factors associated with any violence after first episode of psychosis.
Groups Effect size and 95% interval Test of nullhypothesis(two-tailed)
Heterogeneity
Group Point estimate Lower limit Upper limit Z-value P-value Q-value df (Q) P-value I-squared
Alcohol use 1.00 0.18 5.51 0.00 1.00 3.30 1.00 0.07 69.69Male 1.88 0.54 6.59 0.99 0.32 0.00 1.00 0.95 0.00Mania 2.17 0.60 7.88 1.18 0.24 3.26 1.00 0.07 69.30Mental health act 5.71 1.57 20.74 2.64 0.01 4.52 1.00 0.03 77.86Schizophrenia 0.78 0.22 2.75 -0.39 0.70 1.45 1.00 0.23 30.80Substance abuse 2.74 0.91 8.23 1.80 0.07 5.87 2.00 0.05 65.90Total symptoms 1.88 0.53 6.71 0.97 0.33 0.22 1.00 0.64 0.00Unemployment 1.69 0.48 5.99 0.82 0.41 9.03 1.00 0.001 88.92
218 M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
being male, a diagnosis of schizophrenia and elevated moodwere not found to be associated with serious violence in first-episode psychosis. The high total base rate for violence of anyseverity might allow the development of an actuarial riskassessment instrument with a useful positive predictive value(Large et al., in press). However, the low rate of severeviolencemeans it is unlikely that there will ever be a clinicallyuseful instrument to predict that form of violence, even if aninstrument with very high specificity and sensitivity were tobe developed. Based on the results of this study, if one of the
Fig. 6. Meta-analysis of factors associated with a
reasons for developing first-episode services is to reduceviolence, the main recommendation would be to treat allpatients as soon as possible rather than attempting to predictwhich patients will become dangerous or waiting for patientsto commit an act of violence before initiating treatment.
Studying violence associated with mental illness cancontribute to the stigma experienced by patients withpsychotic illness, especially because the majority of patientswith first-episode psychosis are not violent and severe formsof violence are quite rare. However, the limited number of
ny violence after first-episode psychosis.

219M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
studies of violence in first-episode and early schizophreniaand the absence of empirical data showing how violence byfirst-episode patients can be reduced indicate the need forfurther research examining a comprehensive range of factorsthatmight be associatedwith or protective against violence. Alarge multi-centre study employing standardised definitionsof violence could be included in a meta-analysis of individualsubjects that would allow an examination of the interactionof risk factors (Riley et al., 2010). A multi-centre studycollecting data from both civil and forensic settings could alsoprovide information about the factors associated with therare forms of severe violence.
Role of the funding sourceI can confirm that the study was unfunded and that we have no conflicts
of interest.
ContributorsM.L. and O.N. conceived the study, performed the searches, extracted the
data and wrote the paper. M.L. performed the analysis and takesresponsibility for the data.
Conflict of interestI can confirm that we have no conflicts of interest.
AcknowledgementsWe thank Dr. Peter Arnold for his assistance with the manuscript and Dr.
Tracy Anderson for her advice about the presentation of the data. We alsothank Dr. J Milton, Dr. S Foley, Dr. K Dean, and Dr. Humphreys for emailcorrespondence about the their studies included in the meta-analysis.
References
Arseneault, L., Moffitt, T.E., Caspi, A., Taylor, P.J., Silva, P.A., 2000. Mentaldisorders and violence in a total birth cohort: results from the DunedinStudy. Arch. Gen. Psychiatry 57 (10), 979–986.
Bhugra, D., Hilwig, M., Mallett, R., Corridan, B., Leff, J., Neehall, J., Rudge, S.,2000. Factors in the onset of schizophrenia: a comparison betweenLondon and Trinidad samples. Acta Psychiatr. Scand. 101 (2), 135–141.
Borenstein, M., Hedges, L., Higgins, J., 2005. Comprehensive meta-analysis.Biostat, Engelwood, NJ. (Version 2).
Brewin, J., Cantwell, R., Dalkin, T., Fox, R., Medley, I., Glazebrook, C.,Kwiecinski, R., Harrison, G., 1997. Incidence of schizophrenia inNottingham. A comparison of two cohorts, 1978–80 and 1992–94. Br. J.Psychiatry 171, 140–144.
Ceskova, E., Prikryl, R., Kasparek, T., Kucerova, H., 2008. Aggression in first-episode schizophrenia. Prim. Care Community Psychiatry 13 (3), 134–137.
Dean, K., Walsh, E., Morgan, C., Demjaha, A., Dazzan, P., Morgan, K., Lloyd, T.,Fearon, P., Jones, P.B., Murray, R.M., 2007. Aggressive behaviour at firstcontact with services: findings from the AESOP First Episode PsychosisStudy. Psychol. Med. 37 (4), 547–557.
Elbogen, E.B., Johnson, S.C., 2009. The intricate link between violence andmental disorder: results from the National Epidemiologic Survey onAlcohol and Related Conditions. Arch. Gen. Psychiatry 66 (2), 152–161.
Fazel, S., Gulati, G., Linsell, L., Geddes, J.R., Grann, M., 2009a. Schizophreniaand violence: systematic review and meta-analysis. PLoS Med. 6 (8),e1000120.
Fazel, S., Langstrom, N., Hjern, A., Grann, M., Lichtenstein, P., 2009b. Schizophre-nia, substance abuse, and violent crime. JAMA 301 (19), 2016–2023.
Foley, S.R., Kelly, B.D., Clarke, M., McTigue, O., Gervin, M., Kamali, M., Larkin,C., O'Callaghan, E., Browne, S., 2005. Incidence and clinical correlates ofaggression and violence at presentation in patients with first episodepsychosis. Schizophr. Res. 72 (2–3), 161–168.
Foley, S.R., Browne, S., Clarke, M., Kinsella, A., Larkin, C., O'Callaghan, E., 2007. Isviolence at presentation bypatientswithfirst-episode psychosis associatedwith duration of untreated psychosis? Soc. Psychiatry Psychiatr. Epidemiol.42 (8), 606–610.
Harris, A., Brennan, J., Anderson, J., Taylor, A., Sanbrook, M., Fitzgerald, D.,Lucas, S., Redoblado-Hodge, A., Gomes, L., Gordon, E., 2005. Clinicalprofiles, scope and general findings of the Western Sydney First EpisodePsychosis Project. Aust. N Z J. Psychiatry 39 (1–2), 36–43.
Harris, A.W., Large, M.M., Redoblado-Hodge, A., Nielssen, O., Anderson, J.,Brennan, J., 2010. Clinical and cognitive associations with aggression inthe first episode of psychosis. Aust. N. Z. J. Psychiatry 44 (1), 85–93.
Humphreys, M.S., Johnstone, E.C., MacMillan, J.F., Taylor, P.J., 1992.Dangerous behaviour preceding first admissions for schizophrenia. Br.J. Psychiatry 161, 501–505.
Johnstone, E.C., Crow, T.J., Johnson, A.L., MacMillan, J.F., 1986. The North-wick Park Study of first episodes of schizophrenia. I. Presentation ofthe illness and problems relating to admission. Br. J. Psychiatry 148,115–120.
Large, M., Nielssen, O., 2008. Evidence for a relationship between the durationof untreated psychosis and the proportion of psychotic homicides prior totreatment. Soc. Psychiatry Psychiatr. Epidemiol. 43 (1), 37–44.
Large, M., Andrews, D., Babidge, N., Hume, F., Nielssen, O., 2008a. Self-inflicted eye injuries in first-episode and previously treated psychosis.Aust. N. Z. J. Psychiatry 42 (3), 183–191.
Large, M., Nielssen, O., Slade, T., Harris, A., 2008b. Measurement andreporting of the duration of untreated psychosis. Early Interv. Psychiatry2 (4), 201–211.
Large, M.M., Nielssen, O., Ryan, C.J., Hayes, R., 2008c. Mental health laws thatrequire dangerousness for involuntary admission may delay the initialtreatment of schizophrenia. Soc. Psychiatry Psychiatr. Epidemiol. 43 (3),251–256.
Large, M.M., Ryan, C.J., Nielssen, O.B., Hayes, R.A., 2008d. The danger ofdangerousness: why we must remove the dangerousness criterion fromour mental health acts. J. Med. Ethics 34 (12), 877–881.
Large, M., Babidge, N., Andrews, D., Storey, P., Nielssen, O., 2009a. Major self-mutilation in the first episode of psychosis. Schizophr. Bull. 35 (5),1012–1021.
Large, M., Smith, G., Nielssen, O., 2009b. The relationship between the rateof homicide by those with schizophrenia and the overall homicide rate:a systematic review and meta-analysis. Schizophr. Res. 112 (1–3),123–129.
Large, M. M., Ryan, C. J., Singh, S. P., Paton, M. B. & Nielssen, O. B. (in press).The predictive value of risk categorisation in schizophrenia. Harv. Rev.Psychiatry.
Milton, J., Amin, S., Singh, S.P., Harrison, G., Jones, P., Croudace, T., Medley, I.,Brewin, J., 2001. Aggressive incidents in first-episode psychosis. Br. J.Psychiatry 178, 433–440.
Modestin, J., Ammann, R., 1996. Mental disorder and criminality: maleschizophrenia. Schizophr. Bull. 22 (1), 69–82.
Munkner, R., Haastrup, S., Joergensen, T., Kramp, P., 2003. The temporalrelationship between schizophrenia and crime. Soc. Psychiatry Psychiatr.Epidemiol. 38 (7), 347–353.
Nielssen, O., Large, M., 2009. Untreated psychotic illness in the survivors ofviolent suicide attempts. Early Interv. Psychiatry 3 (2), 116–122.
Nielssen, O., Large, M., 2010. Rates of homicide during the first episode ofpsychosis and after treatment: a systematic review and meta-analysis.Schizophr. Bull. 36 (4), 702–712.
Nielssen, O.B., Westmore, B.D., Large, M.M., Hayes, R.A., 2007. Homicideduring psychotic illness in New South Wales between 1993 and 2002.Med. J. Aust. 186 (6), 301–304.
Nielssen, O., Glozier, N., Babidge, N., Reutens, S., Andrews, D., Gerard, A.,Mahli, G., Large, M., 2010. Suicide attempts by jumping and psychoticillness. Aust. N. Z. J. Psychiatry. 44 (6), 568–573.
Nielssen, O., Bourget, D., Laajasalo, T., Liem, M., Labelle, A., Hakkanen-Nyholm, H., Koenraadt, F. & Large, M. M. (in press). Homicide ofStrangers by People with a Psychotic Illness. Schizophr Bull.
Payne, J., Malla, A., Norman, R., Windell, D., Nicole, B., 2006. Status of first-episode psychosis patients presenting for routine care in a definedcatchment area. Can. J. Psychiatry 51 (5), 42–47.
Riley, R.D., Lambert, P.C., Abo-Zaid, G., 2010. Meta-analysis of individualparticipant data: rationale, conduct, and reporting. BMJ 340, c221.
Rosenthal, J.A., 1996. Qualitative descriptors of strength of association andeffect size. J. Soc. Serv. Res. 21 (4), 37–59.
Rowlands, R.P., 2001. Auditing first episode psychosis: giving meaning toclinical governance. Int. J. Clin. Pract. 55 (10), 669–672.
Sartorius, N., Jablensky, A., Korten, A., Ernberg, G., Anker, M., Cooper, J.E., Day,R., 1986. Early manifestations and first-contact incidence of schizophre-nia in different cultures. A preliminary report on the initial evaluationphase of the WHO Collaborative Study on determinants of outcome ofsevere mental disorders. Psychol. Med. 16 (4), 909–928.
Spidel, A., Lecomte, T., Greaves, C., Sahlstrom, K., Yuille, J.C., 2010. Earlypsychosis and aggression: predictors and prevalence of violent behaviouramongst individuals with early onset psychosis. Int. J. Law Psychiatry 33 (3),171–176.
Steadman, H.J., Mulvey, E.P., Monahan, J., Robbins, P.C., Appelbaum, P.S.,Grisso, T., Roth, L.H., Silver, E., 1998. Violence by people discharged fromacute psychiatric inpatient facilities and by others in the sameneighborhoods. Arch. Gen. Psychiatry 55 (5), 393–401.

220 M.M. Large, O. Nielssen / Schizophrenia Research 125 (2011) 209–220
Steinert, T.,Wiebe, C., Gebhardt, R.P., 1999. Aggressive behavior against self andothers among first-admission patients with schizophrenia. Psychiatr. Serv.50 (1), 85–90.
Stroup, D.F., Berlin, J.A., Morton, S.C., Olkin, I., Williamson, G.D., Rennie, D.,Moher, D., Becker, B.J., Sipe, T.A., Thacker, S.B., 2000. Meta-analysis ofobservational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group.JAMA 283 (15), 2008–2012.
Swanson, J.W., Swartz, M.S., Van Dorn, R.A., Elbogen, E.B., Wagner, H.R.,Rosenheck, R.A., Stroup, T.S., McEvoy, J.P., Lieberman, J.A., 2006. Anational study of violent behavior in persons with schizophrenia. Arch.Gen. Psychiatry 63 (5), 490–499.
Verma, S., Poon, L.Y., Subramaniam, M., Chong, S.A., 2005. Aggression in Asianpatientswith first-episode psychosis. Int. J. Soc. Psychiatry 51 (4), 365–371.
Volavka, J., Laska, E., Baker, S., Meisner, M., Czobor, P., Krivelevich, I., 1997.History of violent behaviour and schizophrenia in different cultures.Analyses based on the WHO study on Determinants of Outcome ofSevere Mental Disorders. Br. J. Psychiatry 171, 9–14.
Wallace, C., Mullen, P.E., Burgess, P., 2004. Criminal offending in schizophreniaover a 25-year period marked by deinstitutionalization and increasingprevalence of comorbid substance use disorders. Am. J. Psychiatry 161 (4),716–727.