a kind of research design conducted in cycles and it is carried ...
Upload
ministryhighereducationscientificresearchCategory
view
0download
0
Field work report carried out from July 06th to 10th 2015 in the Mezam Division, North West
Region of Cameroon
REPUBLIQUE DU CAMEROUN
Paix – Paix – Patrie
----------
MINSTERE DE LA RECHERCHE
SCIENTIFIQUE ET DE L’INNOVATION
----------
CENTRE NATIONAL D’EDUCATION
----------
BP. 1721 Yaoundé-Cameroun
Tél. Tél +237 22 23 40 12.
REPUBLIC OF CAMEROON
Peace – Work – Fatherland
----------
MINISTRY OF SCIENTIFIC
RESEARCH AND INNOVATION
----------
NATIONAL CENTRE FOR EDUCATION
----------
Po Box 1721 Yaounde-Cameroon
Tel. +237 22 23 40 12.
THE FIELD WORK STUDY REPORT OF THE NORTH WEST REGION TEAM
(Mezam Division)
IN THE FRAMEWORK OF THE PROJECT CARRIED ON
« THE EVALUATION OF THE NON ACHIEVEMENT OF THE MILLENIUM
DEVELOPMENT GOALS IN CAMEROON »
August 2015
Research team
Fritz NGOE (Senior Researcher)
NZINO MUNONGO Victorine Ghislaine (Senior Researcher)
Euloge Thierry BISSAYA B. (Senior Researcher)
FOSSO SIMUN Reine (Researcher)

I- INTRODUCTION
1- CONTEXT AND JUSTIFICATION
Considering health as ‘one of the fundamental human right of every human being, the
WHO defines health as ‘a state of complete physical, social and mental well-being and not
merely the absence of disease or infirmity’1. Despite this sacred status granted to health, the
latter remains a privilege not accessible to all. As a remedy to this situation, the global
community came up with the MDGs.
The Millenium Development Goals (MDGs) were initiated by the United Nations in
the year 2000. The purpose of this initiative is to find measures contributing to find a way out
for developing countries of their precarious economic conditions. Therefore, eight goals were
adopted with focus on poverty reduction and the improvement of the population’s living2.
Cameroon notified its involvement in the MDGs implementation by the elaboration of a
strategy3 to achieve the fixed goals. The strategy adopted by Cameroon involved the holding
of an assessment exercise. Nwanolue and al. present assessment as being a sine qua non
exercise for any human enterprise whose purpose is success. Assessment has as target to
reveal difficulties which were not obvious at the outset in order to make adjustments4. The
deadline of achieving the different objectives was set for 2015; the time has then come for
assessment to be made.
The strategic Document for growth and employment is presented as an integrated
framework of human sustainable development in medium term in which the Cameroonian
Government outlined its progress towards the achievement of the MDGs 5. According to the
report by the National Institute of Statistics in 2012, Cameroon has honoured its commitment
1 Helena Legido-Quigley, ‘Health in developing countries’ in International Encyclopedia of the social sciences,
Macmillan Social Science Library, USA, 2nd
edition, 2008, pp. 441-442. 2 Nwanolue et al., Economic partnership agreement and sustainable development in Africa: an analysis of the
impact of eu-africa ‘first action plan 2008-2010’ on MDGs, pp.5-7,
http://scholar.google.com/scholar_url?url=http://www.nwanoluebog.net/wp-
content/uploads/2014/12/ECONOMIC-PARTNERSHIP-AGREEMENT-AND-SUSTAINABLE-
DEVELOPMENT-IN-
AFRICA.pdf&hl=fr&sa=X&scisig=AAGBfm1qIo6DFZSslJRA_nHJ_ooB8Cn_rw&nossl=1&oi=scholaralrt
(Consulté le 06/02/2015). 3 DSCE, http://www.minepat.gov.cm/index.php/fr/modules -menu/doc_download/108-document-de-strategies-
pour-la-cro issance-et-l-emploi-dsce (Consulté le 06/02/2015). 4 Nwanolue et al., op cit, p.5.
5 DSCE, p. 10, http://www.minepat.gov.cm/index.php/fr/modules -menu/doc_download/108-document-de-
strategies-pour-la-cro issance-et-l-emploi-dsce (Consulté le 06/02/2015).

to the integration of sustainable development principles in policies and programmes6.
However, the Strategic document for growth and employment also states that it is very
unlikely that the country could reach targets by 2015. What would be the reasons? In other
words, what are the reasons justifying the non achievement of MDGs 4 and 5 by the
Cameroonian Government and how to fix it?
In order to carry out a study that meets a precise physical demarcation, this study will
have as focus to seek the causes of the MDGs 4 and 5 non achievements in the North West
Region of Cameroon, precisely in the Mezam Division.
2- PRESENTATION OF SITE
The North West Region is constituted of seven administrative units: Boyo, Bui, Donga-
Mantung, Menchum, Momo and Ngo Ketunjia. Each division has sub-administrative units
called subdivisions. In sum, the North West Region has 34 subdivisions and 35 councils.
Mezam Division has as headtown Bamenda and a land surface of 1 745 km2 composed of 7
subdivisions.
DIVISION SURFACE
AREA KM2
SUB-DIVISION COUNCIL
MEZAM
1 745
BAFUT
7
BALI
BAMENDA 1
BAMENDA 2
BAMENDA 3
SANTA
TUBAH
NORTH WEST REGION 17 300 34 35
Source: RADEC 2013.
The North West Region is found between Latitudes 5◦40’ and 7◦ North of the prime Meridian,
with a land surface area of 17 300 km2. The Region is not easily accessible due to the abrupt
6 6 Rapport national de progrès des objectifs du millénaire pour le développement l’année 2012, réalisé sous la
coordination de l’Institut National de la Statistique, p.31,
http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0CB0QFjAA
&url=http%3A%2F%2Fwww.un.org%2Ffr%2Fmillenniumgoals%2Fpdf%2Fmdg_report2012.pdf&ei=E9XUV
KOcD9HdapGvgqAB&usg=AFQjCNGvLlKkcX9S2XH9yXqUZ -BO8f3pIw&sig2=8vWTYGQNKu1m-
c8xHwew4Q&bvm=bv.85464276,d.d2s ( Consulté le 06/02/2015).

escarpment of the landscape. Almost all the lands are located in altitudes above 900 m. Its
hydrology is made up of plateaus that are big water catchments, various water sources, large
rivers, waterfalls and artificial lakes with high potential to generate hydroelectricity and
enhance economic activities. Abundant rainfall contributes to the development of agriculture
and forest regeneration. Three kinds of vegetation are present in this region: lowland forest,
mountain forest and afro-alpine vegetation. They are mostly made of wildlife, crop
production, medicinal plants, fertile soils, Non Timber Forest Product and fishing points7.
Source:https://encrypted-tbn2.gstatic.com/images?q=tbn:ANd9GcTunEL-
QH5b9wMUr2TLbtcwYghicqnhS HIs7lzId8BdgO2-Htdl1A (Consulted on the August 07th
2015).
7 Economic development report of Cameroon: North west Region, Ministry of Economy, Planning and Regional
Development, 2013, pp. 11-25.

Bamenda, Santa, North West Region, Cameroon July 2015.
The North West Region has about 1.8 million inhabitants with a density of about 99: 7.95% in
the urban area and the rural growth rate is at 1.16%. The population dens ity of Mezam
division is of 300.36 inhabitants per km2. The female population is predominant. The
population is largely young with over 62% of citizens aged less than 20 years and 4.2% of
citizens of 60 years old. Hence, according to the standards of the International Bureau of
Labour, the active population represents about 52.20% of the total population. According to
the North West regional delegation of MINEFOP, the rate of active citizens was 76.2 in 2013:
79% for men and 73.4% for women. The population of Mezam Division is estimated to 56
6921 inhabitants with a density of 324.9 inhabitants / km8.
Christianity (Baptist, Presbyterian, Catholic, etc.) with 80% and Islam with 20% are dominant
in the region; though there is a very common practice of ancestral worship in most of ethnic
groups. These religious organizations are considered as development driving forces in the
health and education fields in remote areas9.
8 Economic development report of Cameroon: North West Region, Ministry of Economy, Planning and Regional
Development, 2013, pp. 11-25. 9 Idem.

In the course of achieving the MDGs 4 and 5, the North West Region has been rated among
the regions that excelled in the achievement of great progress.
Table 1: Percentage of children under 5 underweight
Moderate or severe Severe
2006 2011 2006 2011
North West 12.1 7.1 3.1 1.5
Cameroon 19.3 14.6 5.2 4.5
Source: National Report MINEPAT 2012.
Table 2: Percentage of children 12-23 months fully vaccinated by region or site of residence
2004 2011
North West Region 71.7 82.5
Cameroon 48.2 53.2
Source: National Report MINEPAT 2012.
Table3: Proportion of deliveries assisted by skilled health personnel (% )
2004 2011
North West Region 87,5 93,6
Cameroon 61.8 63.6
Source: National Report MINEPAT 2012.
Despite this significant progress at the regional level, they are still insufficient on the national
map. There is hence the need to consider the features specific to the North West Region that
permitted the latter to excel in the achievement of the Millennium Development Goals in
order to consider an extension of positive practices. And thus bring more light on the shadow
areas that prevented an absolute achievement of the objectives set.
3- STUDY OBJECTIVE
The objective of this study is to determine the causes contributing to the infringement of the
successful achievement of the MDGs 4 & 5 and setting out adjustment measures. In other
words, it is about:
- Describing the investigations on the basis of some socio-economic and cultural
characteristics;

- Analyzing the representations of the beneficiaries on approaches to implementation of the
MDGs 4 & 5 in Cameroon;
- Determining different observed deadlocks, as well as the reasons attached thereto;
- Identifying key lessons related to non-achieved MDGs in the health sector.
4- METHODOLOGY
a. Data collection process
The data collected in the course of this study are both primary and secondary. For they are
derived on one hand from a survey conducted on the North West Region in the Department of
Mezam( Bamenda 1, Bamenda 2, Bamenda 3, Bali, Tubah and Santa), from July 6th to 10th
2015 and on the other hand from documentation of precedent surveys carried on the same
study field.
The coverage involved the organisation of focus groups, interviews with key resource
persons, administration of questionnaires to the populations of the areas mentioned above.
The sample consisted of 40 individuals on average and 12 key resource persons (sector
officials/authorities, administrative staff, authorities of municipalities, o fficials in charge of
health centres, and managers of NGOs in the field of health).
Interviews with key resource persons were carried out in offices. Generally contacts with
various officials were quite easy; interviewees demonstrated much courtesy and availability
and especially showed a great interest for the research theme. The time devoted to conduct an
interview was about 30 minutes.
Two focus groups were held in the course of this study. The first focus group was held on July
07th 2015 in the subdivision of Bamenda 2. Seven (07) people were present at this meeting,
among whom 04 (four) women and 03 (three) men. The second focus group was held on July
08th 2015 in the subdivision of Tubah, Bambui. Eight (08) people were present at this
meeting, seven (07) women and one (01) man. The time devoted to conduct a focus group
was about 1 hour 30 minutes.
b. Analysis grid

Considering the interdisciplinary nature of this study, the analysis of data collected on the
field is made through the Conflict theory and the Health belief model.
Health belief Model (HBM) is known as a “psychological model that attempts to explain and
predict health behaviors [of individual]”10. Promoted by authors as Hochbaum, Rosenstock
and Kegels, HBM is based “on understanding that a person will take a health related action if
that person:
- Feels that a negative health condition can be avoided;
- Has a positive expectation that by taking a recommended action, he/she will avoid a
negative health condition and;
- Believes that he/she can successfully take a recommended health action.”
In the course of this study, the HBM will hence contribute in bringing out the perception in
various aspects of the population concerning the MDGs 4 and 5:
- The degree of susceptibility of the population to the various health programs carried in
achieving the MDGs 4&5;
- The level of perceived severity of maternal health and infant mortality by the
population;
- The population’s belief in the efficacy of the advised actions to reduce infant mortality
and improve maternal health;
- The population’s opinion on the tangible and psychological costs of the advised
actions;
- The strategies to take to successfully achieve the expected MDGs;
- To rate the population’s capacity to take action.
Diagram1: Conceptual Model
10
Charles K. Atkin and Ronald E. Rice, Theory and Principles of Public Communication Campaigns, p.3. http://www.sagepub.com/upm-data/46948_CH_1. (Consulted on the 27/07/2015).
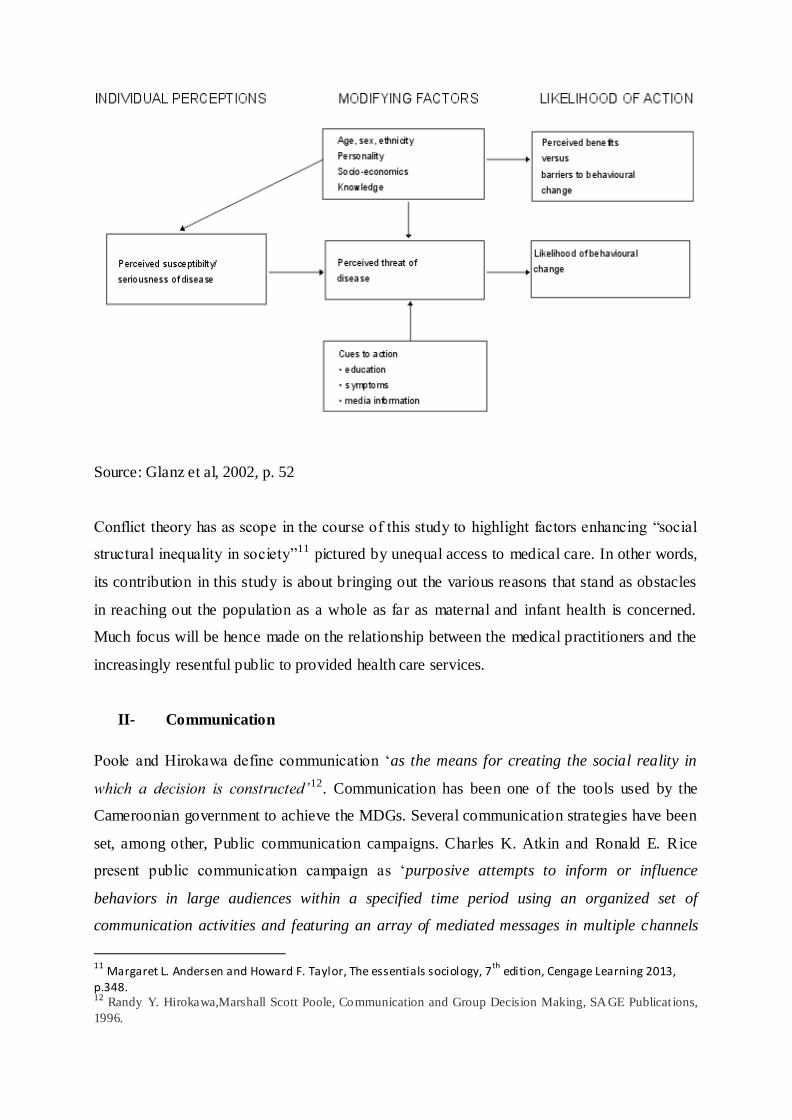
Source: Glanz et al, 2002, p. 52
Conflict theory has as scope in the course of this study to highlight factors enhancing “social
structural inequality in society”11 pictured by unequal access to medical care. In other words,
its contribution in this study is about bringing out the various reasons that stand as obstacles
in reaching out the population as a whole as far as maternal and infant health is concerned.
Much focus will be hence made on the relationship between the medical practitioners and the
increasingly resentful public to provided health care services.
II- Communication
Poole and Hirokawa define communication ‘as the means for creating the social reality in
which a decision is constructed’12. Communication has been one of the tools used by the
Cameroonian government to achieve the MDGs. Several communication strategies have been
set, among other, Public communication campaigns. Charles K. Atkin and Ronald E. Rice
present public communication campaign as ‘purposive attempts to inform or influence
behaviors in large audiences within a specified time period using an organized set of
communication activities and featuring an array of mediated messages in multiple channels
11
Margaret L. Andersen and Howard F. Taylor, The essentials sociology, 7th
edition, Cengage Learning 2013, p.348. 12
Randy Y. Hirokawa,Marshall Scott Poole, Communication and Group Decision Making, SAGE Publicat ions,
1996.

generally to produce non commercial benefits to individuals and society’13. It is in view of
implementing this strategy that the Medical personnel of the PMI Nkwen (Infant Welfare
Unit) has been carrying out outreach programs in the community, about 4 (four) times a
month. The tools used during outreach programs are megaphones; the media, volunteers are
trained, mouth to mouth information. The medical personnel of the District hospital of Santa
said ‘sensitizations activities are carried out through community outreach, radio talk shows’.
However, these measures have produced limited results.
According to World Health Organization Consultant attached to the North West regional
delegation of the Ministry of Health, ‘communication is not effective from the base’:
- The nuclear cell of society is not involved;
- Schools are not involved;
- Communities are not involved;
- In between actors in the domain, there is a lack of dialog;
- The communication mechanism set in place is not appropriate for the targeted
population.
All the officials of the various subdivisions, namely, 1st Deputy Mayor of Bamenda 1, Mayor
of Bamenda 3, Mayor of Bamenda 2 were unanimous on the fact that information concerning
the MDGs did not get to the grassroots population because the councils were not involved in
the communication campaigns. According to the 1st Deputy Mayor of Bamenda 1, ‘linguistic
barrier has been very obvious in the communication field’ despite the openness of the
population to every initiative carried in the said domain.
Moreover, some citizens during focus groups discussions clearly stated to have heard about
the MDGs but were not able to name its contents in detail. Meanwhile others clearly knew
about its content but had no clue it was linked to MDGs. Most of our informants made us to
understand that there is little or no communication on issues concerning the millennium
development goals. Some of the women said all what they head concerning these goals came
from the hospitals, some said they heard it from the radio while others from their neighbours.
We realized that most of the informants had knowledge about the products offered by the
13
Charles K. Atkin and Ronald E. Rice, Theory and Principles of Public Communication Campaigns, SAGE
Publications, 2012, fourth edit ion, p.1.

goals but did not know about the goals. Actually in the hospitals there is health talk once in a
week for pregnant women and breast feeding mothers. These talks are on the importance of
nutrition and Antenatal care, there is also health education on preventable diseases and
preventive treatment, hygiene, HIV screening and preparation for birth. In all of these, there
are still some obstacles because most patients do not accompany their partners especially
when tested positive. Other informants said most patients are not willing to give information
about their health situations.
In the interview with the national Director of Women’s Union of the Cameroon Baptist
Convention, she said the Baptist women have inserted the MDGs in their activities 4 (four)
years ago. They annually carry out an assessment exercise of the various goals set by the
MDGs 4 and 5. The activities carried out are teaching sessions on diverse platforms
(women’s meetings, forums, conferences, etc.) in order to alleviate maternal and infant
mortality.
III- Achievements/products
Addressing the issue of the MDGs 4 and 5 is talking about reducing infant mortality through
vaccines, fight against infant diseases and malnutrition; improving maternal health via
rendering medical services accessible, namely, neonatal and antenatal obstetrical care and
campaigns for the accelerated reduction of maternal mortality known as CARMMA.
a. Achievements on Maternal health improvements
Considering that maternal health has a heavy influence on the health state of the family as
whole, maternal health has been set as one of the major levers of Cameroon’s health sectoral
strategy. Hence, several products have been offered in view of reducing by 3/4 the maternal
mortality rate (1900 – 2015).
Policies regarding the information and education of the population in link with family
planning have been set in place by the Cameroonian government. According to the national
report of progress of The MDGs produced in 2012, the contraceptive prevalence has been
improved. The use of modern contraceptive methods among women in union aged between
15 and 49 years of age rose from 12% in 2004 to 14% in 2011.

The medical personnel of the Regional hospital of Bamenda (Family Planning Unit) Ajehua
Elsie- Kake Elizabeth elaborated their various activities in the medical domain in these words:
‘In the hospital, Family Planning is considered as the entrance way to have access to maternal
health care attention. The goals are to:
- Help individual choose in a proper way a good sexual attitude
- Prevent unwanted pregnancies/ undesirable effects of wrongly conducted abortions
- Healthy infants for couples
Women welcome the information they receive and the response is immediate. 6 (Six) weeks
after delivery, they come for contraceptive services. In the hospital, services are intergraded.
When women come for Antenatal consultations or post natal consultations, they are called for
Family Planning. 60% of women who come for delivery are informed and respond positively
to the Family planning session invitation. There has been a reduction of abortions carried out
in the hospital since 2009. As far as Antenatal consultations are concerned, 85% of the
population will seek for medical attention.
According to the national Director of Women’s Union of the Cameroon Baptist Convention,
women receive training on maternal health issues and react promptly. There has been a major

improvement on maternal health through Family Planning sessions in that more women
control child birth.
Nevertheless, fertility remains early and at a high level; hence the exposure of women to the
risk of maternal mortality. In the interview with the national Director of Women’s Union of
the Cameroon Baptist Convention, she said the phenomenon of ‘single mothers’ is very
rampant; the latter lack means to take care of their children and sometimes abandon them in
public premises as churches. The mortality rate among adolescents aged between 15 and 19
years was 127 births per 1000 in 201114. According to the medical personnel of the Regional
hospital of Bamenda (Family Planning Unit) Ajehua Elsie- Kake Elizabeth, despite the
positive respond of women, 40% are still reluctant to family planning due to religious
(catholic) considerations or prejudices. The single adolescent will not seek for medical
attention due to lack of finances, fear of being judged and condemned and ignorance. Women
are very secretive concerning Family Planning issues. The reason behind this is that they
don’t want to make a public show of the contraceptive method they have chosen. Considering
this fact on one hand and on the other that the Family planning Unit in the Regional hospital
of Bamenda is set in an open space deprived of all intimacy, women feel uncomfortable
during discussions and do not easily confide in the medical personnel. And this contributes to
alter the services rendered by the Family Planning unit. Home visits are carried out but are not
effective. As a response to the lacks observed in this domain, it has been recommended that
Family Planning be carried out as community project. The proposal of the project is still
under consideration at the medical district level. Other factors could be considered as being
major barriers to the effective implementation of family planning activities:
- Husbands are not involved or show very poor interest in Family Planning.
- The medical personnel lack support mechanisms and structures (finances of activities
like field work, lack of didactic material, etc.)
The medical personnel of the District hospital of Santa said women are responding but not
efficiently. Antenatal care is the gate way to maternal health care in the hospital. When
14
Rapport national de progrès des objectifs du millénaire pour le développement l’année 2012, réalisé sous la
coordination de l’Institut National de la Statistique,
http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0CB0QFjAA
&url=http%3A%2F%2Fwww.un.org%2Ffr%2Fmillenniumgoals%2Fpdf%2Fmdg_report2012.pdf&ei=E9XUV
KOcD9HdapGvgqAB&usg=AFQjCNGvLlKkcX9S2XH9yXqUZ-BO8f3pIw&sig2=8vWTYGQNKu1m-
c8xHwew4Q&bvm=bv.85464276,d.d2s ( Consulté le 06/02/2015).

women begin with the Antenatal care, they are carried through the whole process. Antenatal
coverage has increased. Santa subdivision was cited as having the highest coverage in the
North West region. This is thanks to the change of strategy at the national level; from Massive
Antenatal Care to focalized Antenatal care. Women are much more treated as individual and
no more collectively. The delivery kit which is provided at low cost has helped reduce the
mortality rate. In 2014, 60% of women in the subdivision of Santa were registered for
Antenatal consultations; in 2011, 30% at the national level.
In the focus group carried out in Bambui, the participants said Family Planning se nsitizations
are only made in clinics for pregnant women and nursing mothers. Thus in Bambui District
hospital, Family planning sessions are conducted every Thursdays. Contraceptives methods
are well received but controversial. This is caused by the fact that women are not given the
opportunity to choose a contraceptive method having received all information on the matter.
One contraceptive method is often imposed to them. Catholic converts are not encouraged by
their clergy to use contraceptive methods. Some men are said to be cooperative in the use of
contraceptive methods by their women. According to participants, there are specialized health
care unit which take care of pregnant women called maternity, where these women go for
check up every week, complicated pregnancy cases that cannot be handled by these doctors
are transferred to the regional hospital in Bamenda. Though some pregnant women may lose
their lives, this is not as rampant as before. These women think that doctors in this area have
embarked on carrying out surgical operation on pregnant women instead of giving birth
normally; they think that it is strategy that the doctors have put in play to make much money
because operations are more expensive. On the other hand most mothers have become very
negligent with their health and come to the hospital only when the situation has become
worst, this is very common with mothers who have many children. Family planning lectures
are given in the hospital but most women complained that, it does not correspond with their
system, since there are different types, they find themselves taking all the various types and it
still does not work with them.
In the Focus Group Bamenda 2 Council (bojong junction), the women present in the Focus
group discussion confessed that all the Antenatal consultation sessions were respected by
them. But still, women lose their life due to pregnancy complications (bleeding after the
child’s birth), in great number. Some of these women are said to have closely followed all
their Antenatal Consultation sessions. The participants link this fact with the money
consciousness of the medical personnel, lack of availability and competence.

In the other hand, the medical personnel of the District hospital of Santa said women do not
faithfully respect appointments for Antenatal consultations, and medical practices as
Caesarean section are not welcomed in the community. The population fails to understand
that Caesarean sections are mostly conducted to save the life of the baby in other to fight
infant mortality. Thus the next step they take is the way to traditional practices.
b- Infant mortality reduction achievements
In Cameroon, the target has been to reduce the mortality rate of infant below five years by 2/3
between 1990 and 2015: 76°/◦◦. According to the national report on the progress of MDGs in
2012, the mortality rate of children below five years has gone from 146°/◦◦ between the
period of 1996 – 2001 to 122°/◦◦ from 2006 – 201115. Despise the notable changes, much still
need to be done.
In the course of achieving infant mortality reduction, the medical personnel of the PMI
Nkwen (Infant Welfare Unit) said in the hospital, services are integrated so women are given
information concerning the various programs oriented to infant health as they go from one
medical service to another.
15
Rapport national de progrès des objectifs du millénaire pour le développement l’année 2012, réalisé sous la
coordination de l’Institut National de la Statistique,
http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0CB0QFjAA
&url=http%3A%2F%2Fwww.un.org%2Ffr%2Fmillenniumgoals%2Fpdf%2Fmdg_report2012.pdf&ei=E9XUV
KOcD9HdapGvgqAB&usg=AFQjCNGvLlKkcX9S2XH9yXqUZ -BO8f3pIw&sig2=8vWTYGQNKu1m-
c8xHwew4Q&bvm=bv.85464276,d.d2s ( Consulté le 06/02/2015).

In the interview with the Mayor of Bamenda 2, Lord Mayor Balick Awa Fidelis and
collaborators (1st 2nd 3rd Deputy Mayor) , services provided in regard to the MDGs
(mosquito net, vaccines) are well received but do not reach remote areas, rural areas are left
out. A study carried out by students of the University of Bamenda showed that 85% of
children were immunized in the North West Region. However most of the coverage was done
in urban areas. Agents on the field thus turn towards the Council to request assistance in
reaching out the hinterlands.
From the focus group discussion in Bambui, though government launched a campaign to fight
against malaria by distributing mosquito net to household, vaccinating children against
poliomyelitis and yellow fever, some people still complain of not having mosquito net in their
homes. Many children have been immunized due to constant sensitization. Governmental
programs and interventions are effective. Vaccines campaigns are carried out and in unism
women present in the discussion agreed to have received the services provided by this
campaign. The drugs sold in public hospitals are of cheap value, which is not the case of
laboratory tests. This has contributed to reduction of maternal and infant dead rate.
In the focus group of Bamenda 2 Council, according to the participants, there has been polio
campaign, free malaria treatment, measles campaigns launched by the government. These
programs have been of great help but due to the lack of understanding by the population,
children still die. In some areas vaccine campaigns were not carried out; so children still die in
those areas. But in some areas of the council, some people have grown to be very reluctant
concerning vaccine campaigns because they thought these vaccine were 100% immunization
for their children. So when their children develop illnesses still after the campaigns. They feel
the program did not work.
The participants confessed to be satisfied with the various programs organized by the
government but unfortunately children still die due to the negligence of parents. Women do
not attain all the 3 sessions of the Antenatal Consultations prescribed by hospitals; hence, they
are faced with complications. The participants concluded that the government is doing its best
but the people also have to do their own part.
IV- Support mechanisms/structures

The number of health centres at the national level has increased from 3 039 to 3 370 in the
period of 2007 and 200916.
Table 7: Physical capital for the provision of care and services
Health Centre
categories
2001 2007 2009
Hospitals of 1st
category
4 4 4
Hospitals of 2nd
category
3 3 4
Regional hospitals
and assimilated
8 11 11
District hospitals 130 154 164
District medical
centres
/ 155 155
Integrated health
centres
1 689
1 888 1 888
Not-for-profit health
private centres
…
599 …
Healthcare practices
… … 384
Private non-profit
hospitals
… 93 …
Source: MINSANTE/DOSTS
In 2010, 75% of health centres have said to have a box delivery, 88% a delivery tables and
32% boxes for caesarean section17.
16
2e enquête sur le suivi des dépenses publiques et le niveau de satisfaction des bénéficiaires dans les secteurs
de l éducation et de la sante au Cameroun, INS, Décembre 2010, p. 11. 17
2e enquête sur le suivi des dépenses publiques et le niveau de satisfaction des bénéficiaires dans les secteurs
de l éducation et de la sante au Cameroun, INS, Décembre 2010, p. xvii .
From the focus group discussion in Bambui, The women said though all of these are taking
place, they are not still satisfied with the infrastructure in this area. The population has over
grown the present infrastructure. These women said one of the reasons why many people
abandon the hospital and seek health care elsewhere because of high bills they are charged to
pay in carrying out laboratory test. They said doctors sell their drugs to patients and even
direct the patients to particular pharmacies to purchase their drugs, they also complained that
there is shortage of trained personnel’s in the hospital and since most of them are not well
paid, they become very rude to the patients.
Interview with the 1st Deputy Mayor of Bamenda 1, there are various programs/support
structures for the implementation of the MDGs 4 and 5, but the government has lofty project.
If followed properly it will be very beneficial to the population. These programs do not reach
the roots of the population. Government should have a mechanism of follow up.
In the interview with the Mayor of Bamenda 3, Lord Mayor Fongu Cletus Tawe, The Council
has health centres (public, private). Good numbers of these health centres are private.
However, they are insufficiently equipped in human resource (doctor, nurse), in
infrastructures (wards are small and not healthy, insufficient water supply), logistics. They
deal with minor cases and always refer major cases to more equipped hospitals like the
Regional hospital of Bamenda, Shisong and Bingo Baptist hospital.
The major complains of the population is the lack of finances to go in for health basic
services. Due to lack of finance, some women give birth home and develop complications.
Government has to create a conducive atmosphere in order to regain the confidence of
citizens in governmental actions: no interest in governmental programs because no direct gain
is seen. Sometimes the Council grants support (drugs, medical equipments) to health centres.
In the interview with the Mayor of Bamenda 2, Lord Mayor Balick Awa Fidelis and
collaborators (1st 2nd 3rd Deputy Mayor), Health centres are existant in the Council of
Bamenda 2. Nevertheless, various complains are mention: the lack of equipments (lack of
electricity to sustain vaccines and sometimes generators are purchased by the council), lack of
funding (in order to ensure free or services of low cost), lack of human resources (Doctors are
posted to places they do not like and hence do not get to their post of service at the same time,
some of the medical personnel are indexed of being more interested in self money than
rendering medical attention).

In the interview with the national Director of Women’s Union of the Cameroon Baptist
Convention, One of the obstacles to the full accomplishment of the set goals is the absence of
health centres in some remote areas. The response of CBC health Unit has been the
elaboration of the “Life Abundant Program”. Hence, where there are no institutions, local
agents are trained to attain to the population in remote areas.
In the interview with the personnel in charge of sanitation and hygiene at the Council of
Santa, the latter said they work in collaboration with the district hospital. The following
activities are carried out:
- Ensure the population’s health improvement
- Control food handlers in public places and possession of medical certificate provided
by the hospital personnel
- Management of the hospital committee in which the Mayor is the chairman
- Assist with medical equipments and personnel (the council recruits medical staff in the
hospital present in the council).
The difficulties faced in this council are:
- The lack of access to medical services due to lack of finances.
- The lack of knowledge on Family Planning issues due to illiteracy.
- The lack of medical equipment in some health centres. Women give birth on ordinary
tables.
- Poor infrastructures of health centres (no windows, etc.)
However, the hospital is solely in charge of the education of the population on health issues.
In the interview with the medical personnel of the District hospital of Santa, Most women
complain of distance between their homes and the hospital, lack of finance for consultations
and transportation. There is a great lack of competent medical personne l in remote areas.
Antenatal consultations are not free (5000 francs excluding other medical tests).
In the focus group Discussions in Bambui, Women have access to health centres and
sometimes go to these health centres for consultation and treatment. They don’t go always to
health centres because doctors are not often available, the medical personnel is too money

conscious and sell drugs on their personal account, the medical personnel shows flaws in the
rendering medical attention (wrong diagnosis, wrong treatment, wrong manner of
psychological approach in dialogs with patients), lack of money of patients for laboratory
tests, lack of medical equipments (major cases are referred to more equipped hospitals), lack
of electricity ( sometimes, child delivery is conducted in the light of cellular phones. So the
alternatives are traditional treatments (herbs medicine), the purchase of drugs by the road side.
In one week, a traditional practionner is said to receive about18 women. The population is
faced with hygiene problems. Campaigns are being carried but are not effective. Mosquito
nets are not enough when shared. Mosquito nets not used because the users complain of the
heat it produce. Sometimes, people are not met at home during sensitizing campaigns.
In the Focus Group Bamenda 2 Council, The women present at the focus group said they
delivered their children in hospitals. Some preferred private hospitals (St Mary) and others
public hospitals (Regional hospitals). When women are unable to deliver due to complications
or lack of medical personnel, they are taken to the regional hospital.
They said the tropical diseases from which they suffer are due typhoid, diarrhoea, malaria,
yellow fever and measles. Due to poverty, they are unable to follow the treatment of these
various diseases. Water is available but very scarce. It has been 2 (months) now that water has
not been available. It has not been easy.
As preventive measures, the participants confessed that they use mosquito net, they keep their
environment clean. When confronted to the lack of means they refer to alternative methods,
like putting on electricity light during the night to chase mosquitoes.
Due to the various shortages shown by medical personnel in hospitals, like brutal approach
towards patients, wrong diagnosis and wrong treatment given in hospitals, they prefer
alternative health care measures. A woman confessed to have suffered of this; she was driven
out by the nurses because she did not have money and her pregnancy was due. She almost
gave birth on the street. Another woman said her child was at the point of dying and
according to her, the nurses did not have a good approach towards them. Some times
electricity shortage happens in the middle of a chirurgical intervention in the theatre room.
According to the participants, medical personnel in public hospitals (Regional hospital) are so
money conscious that they do not focus on providing health services to patients. Meanwhile,
in private hospitals (St Mary), the patients are taken care of in the first position before being

asked to pay medical bills. But still, they concluded that medical services offered in Bamenda,
are far better than the ones offered in Yaounde.
Actually there is a support program for women in most of the district hospital and health
centres. There are support groups for those who are suffering from HIV; the structures have
been divided into adult group and children group, where they meet once every month.
According to Mrs Mofor, there is no close contact between the stake holders and
beneficiaries. The stakeholders are more interested in their political campaign rather than
issues concerning health but at the level of the hospitals, doctors and nurses are close to the
patients. Small health committees are formed in the interior of most villages that help to take
care of HIV patients.
V- Cost for change
This part of the study deals with the cost to make a change in the health social habitus of the
population of the Mezam division. According to Kathleen Dannemiller, ‘three factors must be
present for meaningful organizational change to take place. These factors are: D =
Dissatisfaction with how things are now; V = Vision of what is possible; F = First, concrete
steps that can be taken towards the vision; If the product of these three factors is greater than
R = Resistance then change is possible. Because D, V, and F are multiplied, if anyone is
absent (zero) or low, then the product will be zero or low and therefore not capable of
overcoming the resistance’18.
Based on the recent evaluation of the MDGs’ achievement by Cameroon, results have shown
that Cameroon will not be able to achieve the MDGs by 2015 (D). Hence, a new resolution
was taken at UN Conference on September 22nd 2010 in New York to postpone the
achievement point to 2020 (V). The 2012 MINEPAT report shows that Cameroon will
certainly achieve one objective on eight and could realise four on eight if efforts towards the
implementation of the growth and employment strategy are maintained 19. In view of meeting
the challenge, concrete steps are taken, among which the present study (F). Through this
study, the resistance factors are to be identified and converted to benefits for the achievement
of the MDGs in Cameroon, specifically in the Mezam division (R).
18
Philip E. Flora, Ensure change management, 2010 Annual Conference Association of Pacific Island Public Auditors (APIPA), July 19, 2010, http://apipa2010.pitiviti.org/files/changemgt.ppt (Consulté le 06/08/2015). 19
INS/MINEPAT : Rapport Nat ional de Progrès des Objectifs du Millénaire pour le Développement, Année
2012, p.10.

In the interview with the authorities of municipalities, here are the various statements that
were made:
The 1st Deputy Mayor of Bamenda 1 said the MDGs are not seen for the ordinary person, so
not understood. The State should maximize in sensitization. The Mayor of Bamenda 3, Lord
Mayor Fongu Cletus Tawe said MDGs are seen as ideas, theories of the government and not
of the people. And finally, the Mayor of Bamenda 2, Lord Mayor Balick Awa Fidelis and
collaborators (1st 2nd 3rd Deputy Mayor) focused on the fact that monitoring and evaluation
steps are not followed; they reiterated on the fact that the MDGs are seen as a theory. Hence,
goals set are not implemented and thus remain slogans.
According to our informants, the procedure in acquiring the MDG 4 and 5 are very
complicated, there are times that many of the people at the grass root do not benefit from it at
all. Some people are ignorant about these services. One of our informants from an NGO in
Bambui called Angel of Mercy said that there is a lot of mixed information, at times they say
drugs to treat malaria in infants are free but they still buy these drugs in the hospital. They
also say drugs are cheap at the hospital pharmacy but they go there these drugs are not
available.
According to Dr Tankou, every program that the government implement on the field has a
training session and there is evaluation but the problems encountered on the field are not
usually addresses immediately. There is no clear data base of the health personnel’s in the
country, there is also a lot of movement of health personel’s, the government spend much
money in training a lot of nurses but only few of them are employed. Those who are sent to
remote area find it very difficult to live there.
From the focus group discussion in Bambui, we realized that there are two health care
systems in this area, the traditional and the biomedical system. Though patient visit hospital
when they are sick, they still hold on to their traditional believe about illness causation and
treatment. Our informants made us to understand that health facilities are present in the
hospital but they are not enough for the population. Due to the presences of these two health
systems in this area, when the child is ill, he/she is first taken to the traditional healer if the
sickness cannot be treated there, they move to the hospital. They made us to understand that
not all diseases results from unhygienic condition, some are due to witch craft practices.

Most of the informants think that the millennium goal failed because of embezzlement in the
health sector. On the other hand, some patients are still negligent with their health. These
women said the only way to improve on infants health is subsidies their drugs and new
infrastructures be put in place that reflect the population size. The people don’t feel at the
centre but feel that all these slogans are just for political purposes.
In the interview with the Medical personnel of the Regional hospital of Bamenda (Family
Planning Unit) Ajehua Elsie- Kake Elizabeth, Concerning the MDGs, the package is known
but not really considered because not carried out as a program on its own.
VI- LESSONS FOR THE FUTURE
According to Kathleen Dannemiller, ‘to ensure a successful change it is necessary to use
influence and strategic thinking in order to create vision and identify those crucial, early
steps towards it. In addition, the organization must recognize and accept the dissatisfaction
that exists by listening to the [citizens’] voice while sharing [society] trends, leadership ideas,
best practice and competitive analysis to identify the necessity for change’.
Before proceeding to the deduction of lessons for the future based on the observation that was
made on the field, a review of the various suggestions made by the citizens of Mezam division
will be made.
In interviews with the personnel in charge of sanitation and hygiene at the Council of Santa
and the national Director of Women’s Union of the Cameroon Baptist Convention the
following suggestions were made:
- Education of the population with illustrations;
- Make use of traditional authorities to get to the people because they are very influential;
- Carry out sensitization in associations;
- Government should work in close collaboration with mayors and Chiefs.
Moreover, were mentioned:
- The building of more health centres;
- The employment of qualified personnel in the medical field;
- The involvement of grass root population in the implementation of various programs;

- The provision of education to grass root population on vaccines;
- Give allowances to discourage high rate of uncontrolled child birth;
- Carry out sensitization in associations;
- Unemployment and idleness being the main cause of the lack of birth control,
strategies to occupy the population have to be found;
- Set up more health units in the hinterlands;
- Ensure accessible roads in cases of evacuations towards urban areas.
The Medical personnel of the Regional hospital of Bamenda (Family Planning Unit) Ajehua
Elsie- Kake Elizabeth suggested that in view of a better rendering of services, the hospital
should create a reproductive health care Unit and thus unify all the units active in maternal
care issues in respect with the secretive social habitus of patients. And also, it has been
recommended that Family Planning be carried out as community project. The proposal of the
project is still under consideration at the medical district level.
The medical personnel of the District hospital of Santa suggested that:
- the financing of the programmes must be focused on the performance;
- there should be a recruitment of community agents to follow up patients from the
hospital to their homes; in collaboration with hospitals;
- Group discussions should be created in the order of HIV programs.
The 1st Deputy Mayor of Bamenda 1, suggested that the State should carry out monitoring
and evaluation of its various programs at various steps of their implementation and get
involved other people committed to reach out the beneficiaries (the root people,
communities).
The Mayor of Bamenda 3, Lord Mayor Fongu Cletus Tawe said the Government has to create
a conducive atmosphere in order to regain the confidence of citizens in governmental actions;
effective devolution of powers and resources to councils to pursue the goals of Cameroonian
government could be considered as a solution.
The Mayor of Bamenda 2, Lord Mayor Balick Awa Fidelis and collaborators (1st 2nd 3rd
Deputy Mayor) agreed on the fact that the Government should associate local government to
the implementation of national project.

A World Health Organization consultant attached to the Regional Delegation of Public
Health, suggested that it will be proper for politics to give way to technicians on the field and
in decision making.
In the Focus group Discussions in Bambui, suggestions were also made:
- Reduction of the prices of medical services (laboratory tests, consultations,etc.)
- Building of public toilets for good sanitary (markets,etc.).
- Discipline wrong attitude of the medical personnel.
In the Focus Group Bamenda 2 Council, The people suggested that the government should get
more involved in sensitizing the local population on research topics that are carried out on
health issues. Sometimes these information are passed on but do not reach the root people.
Considering the various statements that were made by the various respondents on the field, it
could be said that despite the large exposure of the population to messages linked to the
MDGs, few were able to pay attention and capture their content to a high degree. Hence, more
emphasis has to be made on communications’ strategies. More highlights have to be made in
the exposure of the Cameroonians to simple reception of messages with as focus a generation
of related cognitions, image formation, skills acquisition, change in attitudes, beliefs and
values. This can be done in addition to the classic communication media, via informal
interpersonal influences and social engineering policy initiatives20.
More highlights have to be made on behaviors in the health care system. Patients, no matter
their age, should be treated like children ‘a behavior called infantilization’ 21. Hence, emphasis
should be laid on the cultural competency of the Health care professionals which is said to
result in increasing empathy with patients ‘whose cultural frameworks may differ from that of
the physician and thus could compromise communication between the patient and the
doctor’22. However, there is a great need for vigorous supervision and medical staffs
motivation, because the latter carry out much work with little payments.
20
Charles K. Atkin and Ronald E. Rice ,Theory and Principles of Public Communication Campaigns, SAGE
Publications, 2012, fourth edit ion, p.13. 21
Margaret L. Andersen and Howard F. Taylor, The essentials sociology, 7th
edition, Cengage Learning 2013,
p.348. 22
idem.

At the local level, more health posts should be constructed in grass root areas. There is a need
to work with local population, to train them on the dangers of not attending antenatal and
postnatal Consultations; on the importance of vaccination.
At the level of the council, mayors and local chiefs should be involved in the fight against ill
health social habitus at the community level and counselors should receive the ability of
training other members of the community.
At the regional level, chief medical officers, chief of centers should be involved in training
seminars and not only the district health officers.
Nationally, when programs are conceived there should be a long term and a short term
evaluation, the government should not wait and come at the end to carry out final evaluations
after several years. Delegates and security officers should be able to give health information
to the people at the grass root level.
Considering the high potential of the Region in solar energy, this energy can be transformed
into electricity in order to remedy to the frequent electricity shortages in health centres. Also,
the abundance of raw material due to the high practice of farming and animal husbandry
(organic waste material from animals, fowl dung, etc.) could give way to the provision of bio-
gas.
Considering the great vegetation resources of the North West Region, more focus can be laid
on the development of the agro-sylvo-pastoral resources in order to enhance the fight against
poverty, idleness and joblessness.
VII- Bibliography
- 2e enquête sur le suivi des dépenses publiques et le niveau de satisfaction des
bénéficiaires dans les secteurs de l’éducation et de la santé au Cameroun, INS,
Décembre 2010, 119 pages.
- Charles K. Atkin and Ronald E. Rice, Theory and Principles of Public Communication
Campaigns, 17 pages. http://www.sagepub.com/upm-data/46948_CH_1. (Consulted
on the 27/07/2015).
- DSCE, 167 pages, http://www.minepat.gov.cm/index.php/fr/modules-
menu/doc_download/108-document-de-strategies-pour- la-croissance-et- l-emploi-dsce
(Consulted on 06/02/2015).

- Economic development report of Cameroon: North West Region, Ministry of
Economy, Planning and Regional Development, 2013, 117 pages.
- Glanz, K., Rimer, B.K., & Lezism F.M. (Eds)m (2002). Health Behavior and Health
Education (3rd ed.). San Francisco: Jossey-Bass.
- Margaret L. Andersen and Howard F. Taylor, The essentials sociology, 7 th edition,
Cengage Learning 2013, 512 pages.
- Nwanolue et al., Economic partnership agreement and sustainable development in
Africa: an analysis of the impact of eu-africa ‘first action plan 2008-2010’ on MDGs,
23 pages, http://scholar.google.com/scholar_url?url=http://www.nwanoluebog.net/wp-
content/uploads/2014/12/ECONOMIC-PARTNERSHIP-AGREEMENT-AND-
SUSTAINABLE-DEVELOPMENT-IN-
AFRICA.pdf&hl=fr&sa=X&scisig=AAGBfm1qIo6DFZSslJRA_nHJ_ooB8Cn_rw&n
ossl=1&oi=scholaralrt (consulted on 06/02/2015).
- Philip E. Flora, Ensure change management, 2010 Annual Conference Association of
Pacific Island Public Auditors (APIPA), July 19, 2010,
http://apipa2010.pitiviti.org/files/changemgt.ppt (Consulted on 06/08/2015).
- Randy Y. Hirokawa,Marshall Scott Poole, Communication and Group Decision
Making, SAGE Publications, 1996, 315 pages.
- Rapport national de progrès des objectifs du millénaire pour le développement l’année
2012, réalisé sous la coordination de l’Institut National de la Statistique, 50 pages,
http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&ua
ct=8&ved=0CB0QFjAA&url=http%3A%2F%2Fwww.un.org%2Ffr%2Fmillenniumg
oals%2Fpdf%2Fmdg_report2012.pdf&ei=E9XUVKOcD9HdapGvgqAB&usg=AFQj
CNGvLlKkcX9S2XH9yXqUZ-BO8f3pIw&sig2=8vWTYGQNKu1m-
c8xHwew4Q&bvm=bv.85464276,d.d2s ( Consulté le 06/02/2015).
- William A. Darity Jr., International Encyclopedia of the social sciences, Macmillan
Social Science Library, USA, 2nd edition, 2008, 531pages.

VIII- Annex
1- Main agricultural products, quantities produced, average yield and production areas are
summarized in the table below after:
Type of crop main
products
Production (in ton) Average yield
(t/ha)
Area of production
2012 2013 2012 2013
Export crops
Arabica
coffee
2250 2701 All the Divisions
Robusta
coffee
8150 8166 All Divisions
Cocoa 344 357 Momo, mezam, menchum, Donga Mantung, bui,
ngokentunjia.
Tea 3161 3320 1.4 Boyo, Donga Mantung, santa
Palm oil 25700 26123 3 3.1
Cereals Rice 28150 30615 1 1.2 Ndop, Mezam, menchum-
valley, mbaw plain
Maize 180502 195300 2.3 2.3 All Divisions
roots and tubers Cocoyam/
Taro
105259 102041 5.6 5 All Divisions
Cassava 175439 178310 12.4 12.4 All Divisions
plantain 111200 109062 8 8 All Divisions
Potato 66560 67560 8 8 Mezam, boyo, Bui, Donga Mantung, Momo
Potato 24177 26238 5.4 7 All Divisions
Yam 75936 77111 10 10 All Divisions
legume
Groundnu
ts
7807 7917 0.8 0.85 All Divisions
Beans 125180 126020 1.1 1.1 All Divisions
Soya 2458 2315 1.2 1.2 All Divisions
vegetable crops Okro
Tomato 38756 39164 8.4 8.6 All Divisions
Pepper 280 281 All Divisions
Onion 130 135 Mezam
Cabbage 225 262 All Divisions
Lettuce
eggplant
Carrot
Green
spices
Source : RADEC 2013, p. 34 – 35.

2- In 2013, major livestock and fishing products registered in the region are contained in the
following table with the main production areas:
Main Products Quantities Area of Production
Cattle 391518 (Head) Donga, Boyo, Menchum, Bui
Sheep 213092 (Heads) Donga, Menchum, Bui
Goats 319609(Heads) Donga, Boyo, Mezam, Bui
Pigs 169303(Heads) Mezam, Ngokentunjia, Momo
Fowls 818642 (Heads) Mezam, Ngokentunjia, Bui
Honey 1406095(Litres) Boyo, Menchum, Bui
Milk 2854489(Litres) Boyo, Mezam, Bui
Eggs 43540430(Unities) Mezam, Ngokentunjia, Bui
Fresh Fish 295572(Kilogrammes) Donga, Mezam, Ngokentunjia, Momo
Smoked fish 1805600 Kilogrammes) Donga, Mezam, Ngokentunjia,
Momo
Source: RADEC 2013, p. 35.
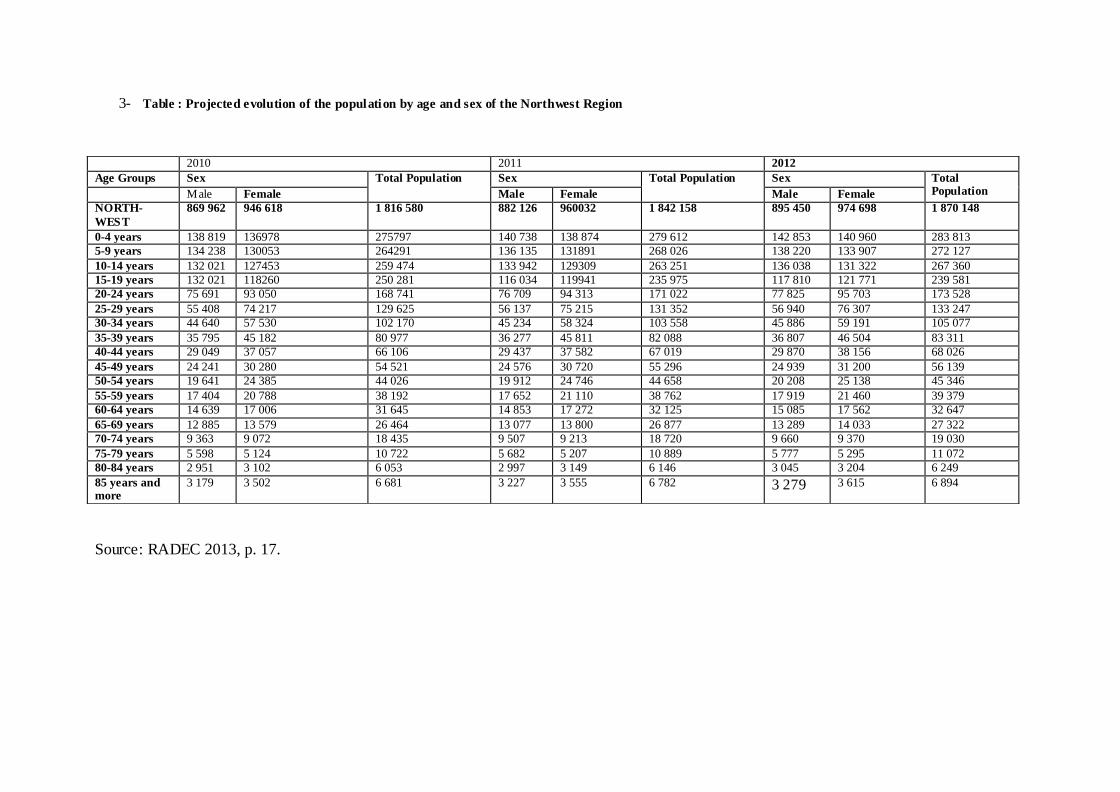
3- Table : Projected evolution of the population by age and sex of the Northwest Region
Source: RADEC 2013, p. 17.
2010 2011 2012
Age Groups Sex Total Population Sex Total Population Sex Total Population Male Female Male Female Male Female
NORTH-
WEST
869 962 946 618 1 816 580 882 126 960032 1 842 158 895 450 974 698 1 870 148
0-4 years 138 819 136978 275797 140 738 138 874 279 612 142 853 140 960 283 813
5-9 years 134 238 130053 264291 136 135 131891 268 026 138 220 133 907 272 127
10-14 years 132 021 127453 259 474 133 942 129309 263 251 136 038 131 322 267 360
15-19 years 132 021 118260 250 281 116 034 119941 235 975 117 810 121 771 239 581
20-24 years 75 691 93 050 168 741 76 709 94 313 171 022 77 825 95 703 173 528
25-29 years 55 408 74 217 129 625 56 137 75 215 131 352 56 940 76 307 133 247
30-34 years 44 640 57 530 102 170 45 234 58 324 103 558 45 886 59 191 105 077
35-39 years 35 795 45 182 80 977 36 277 45 811 82 088 36 807 46 504 83 311
40-44 years 29 049 37 057 66 106 29 437 37 582 67 019 29 870 38 156 68 026
45-49 years 24 241 30 280 54 521 24 576 30 720 55 296 24 939 31 200 56 139
50-54 years 19 641 24 385 44 026 19 912 24 746 44 658 20 208 25 138 45 346
55-59 years 17 404 20 788 38 192 17 652 21 110 38 762 17 919 21 460 39 379
60-64 years 14 639 17 006 31 645 14 853 17 272 32 125 15 085 17 562 32 647
65-69 years 12 885 13 579 26 464 13 077 13 800 26 877 13 289 14 033 27 322
70-74 years 9 363 9 072 18 435 9 507 9 213 18 720 9 660 9 370 19 030
75-79 years 5 598 5 124 10 722 5 682 5 207 10 889 5 777 5 295 11 072
80-84 years 2 951 3 102 6 053 2 997 3 149 6 146 3 045 3 204 6 249
85 years and more
3 179 3 502 6 681 3 227 3 555 6 782 3 279 3 615 6 894

Structure Programs Actions Projects Allocation (in Millions
FCFA)
State of realization(%
physical CP)
MO THER, ADO LESCENT AND CHILD HEALTH
Amount AE Amount
CP
MINSANTE Improving maternal health Construction and equipment of mother and child pavilions
185 000
185 000
81,08
Subtotal action 185 000 185 000 81,08
SUB TO TAL PROGRAM 185 000 185 000 81,08
DEVELO PMENT O F HEALTH DISTRICT
Construction, rehabilitation and equipping of proximity health facilities
Development of the technical plateau of CMA of Belo
20 000 20 000 100
Development of the technical plateau of CMA of Njinikom
20 000 20 000 100
Development of the technical plateau
of CMA of Kumbo
35 000 35 000 100
Development of the technical plateau of CMA of Andek
65 000 65 000 63,08
Development of the technical plateau tof the CMA of Pinyin
20 000 20 000 100
Development of the technical plateau
of CMA of Awing
35 000 35 000 100
Development of the technical plateau of HD of Oku
70 000 45 000 80
construction and équipment of CSI 112 900 112 900 60,14
Subtotal action 377 900 352 900 77,9
SUB TO TAL PROGRAM 377 900 352 900 77,9
GOVERNANCE AND IMPROVEMENT O F
Strengthening of human construction/réhabilitation/extension
of training schools
5 000 5 000 100
Working conditions in
MINSANTE
Resources Subtotal action 6 000 6 000 100
Subtotal program 5 000 5 000 100
TOTAL MINSANTE 567 900 542 900 79,19
4- GLOBAL STATE OF THE PUBLICS INVESTMENTS PROJECTS IN THE NORTH WEST REGION: YEAR2013
SOCIAL SECTOR
Source : RADEC 2013, pp. 99-100.
Copyright © 2022 FDOKUMEN