
The evolution of health care reforms in Greece: charting a course of change
24
THE EVOLUTION OF HEALTH CARE REFORMS IN GREECE: CHARTING A COURSE OF CHANGE ELLIE TRAGAKES 1 * AND NICHOLAS POLYZOS 2 1 WHO, Regional Oce for Europe, 4 Papastratou Str., Kifissia, Athens, 14562, Greece 2 Ministry of Health, Athens, Greece; University of Athens Researcher, 1–3 Triantafyllopoulou Str., Athens 10443, Greece SUMMARY An examination of Greece’s experience with health care reform planning over the past half century reveals a remarkable consistency in reform themes pursued by planners. However, few of the plans resulted in legislation, and of the legislation that was passed even fewer were implemented. The present paper traces out reform plans since the early 1950s and argues that legislative and implementation failures have been due to a lack of political will, insucient attention to consensus-forming mechanisms, and inadequate consideration of the technical, administrative, and institutional feasibility of reform plans. By contrast, developments in the 1990s, which have seen three pieces of health care reform legislation, suggest that processes of health care planning and change are becoming more focused, rational and pragmatic. Macroeconomic constraints, and con- sensus on broader economic policies focusing on the EU convergence requirements have produced a consensus regarding the imperative of change in the health sector, and have given rise to mechanisms which facilitate the task of implementation. The most recent health care reform act (of 17 July 1997) is less radical than many of its predecessors, but includes issues that had entered the health care reform agenda as early as 1952, as well as the more current issues of health sector rationalization. Implementation of the most recent legislative act has already begun. # 1998 John Wiley & Sons, Ltd. KEY WORDS: health care reform; Greece; legislation; policy; reform planning INTRODUCTION On 17 July 1997, Greece enacted a major piece of health care reform legislation. This was the culmination of four years of discussions and reform planning, during which several reform proposals had been formulated and subsequently rejected. The purpose of this article is to place this most recent legislative act in the historical context of Greece’s health care reform experiences. CCC 0749–6753/98/020107–24$17.50 # 1998 John Wiley & Sons, Ltd. INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT Int. J. Health Plann. Mgmt. 13, 107–130 (1998) *Correspondence to: Ellie Tragakes, 4 Papastratou Street, Kifissia, Athens, 14562, Greece. The views expressed here are solely those of the authors. In no way do they represent the World Health Organization or the Ministry of Health (Greece).
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The evolution of health care reforms in Greece: charting a course of change

THE EVOLUTION OF HEALTH CARE REFORMSIN GREECE: CHARTING A COURSE
OF CHANGE
ELLIE TRAGAKES1* AND NICHOLAS POLYZOS2
1WHO, Regional O�ce for Europe, 4 Papastratou Str., Ki®ssia, Athens, 14562, Greece2Ministry of Health, Athens, Greece; University of Athens Researcher,
1±3 Triantafyllopoulou Str., Athens 10443, Greece
SUMMARY
An examination of Greece's experience with health care reform planning over the pasthalf century reveals a remarkable consistency in reform themes pursued by planners.However, few of the plans resulted in legislation, and of the legislation that was passedeven fewer were implemented. The present paper traces out reform plans since the early1950s and argues that legislative and implementation failures have been due to a lack ofpolitical will, insu�cient attention to consensus-forming mechanisms, and inadequateconsideration of the technical, administrative, and institutional feasibility of reformplans. By contrast, developments in the 1990s, which have seen three pieces of healthcare reform legislation, suggest that processes of health care planning and change arebecoming more focused, rational and pragmatic. Macroeconomic constraints, and con-sensus on broader economic policies focusing on the EU convergence requirements haveproduced a consensus regarding the imperative of change in the health sector, and havegiven rise to mechanisms which facilitate the task of implementation. The most recenthealth care reform act (of 17 July 1997) is less radical than many of its predecessors, butincludes issues that had entered the health care reform agenda as early as 1952, as well asthe more current issues of health sector rationalization. Implementation of the mostrecent legislative act has already begun. # 1998 John Wiley & Sons, Ltd.
KEY WORDS: health care reform; Greece; legislation; policy; reform planning
INTRODUCTION
On 17 July 1997, Greece enacted a major piece of health care reform legislation.This was the culmination of four years of discussions and reform planning,during which several reform proposals had been formulated and subsequentlyrejected. The purpose of this article is to place this most recent legislative act inthe historical context of Greece's health care reform experiences.
CCC 0749±6753/98/020107±24$17.50# 1998 John Wiley & Sons, Ltd.
INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT
Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
*Correspondence to: Ellie Tragakes, 4 Papastratou Street, Ki®ssia, Athens, 14562, Greece.The views expressed here are solely those of the authors. In no way do they represent the WorldHealth Organization or the Ministry of Health (Greece).
In the course of the last several decades, a number of plans and legislativeproposals for health care reform have periodically appeared in Greece under avariety of governments. Examination of these proposals reveals that reformplanners, regardless of their political orientation, have displayed a remarkableconsistency in their evaluation of Greece's health care reform needs. Ofthese proposals, however, few have successfully passed into legislation. Of thelegislation that was passed, even fewer proposed changes were successfullyimplemented. As a result, change in the health care system until recently has notbeen the result of rational planning, but rather an ad hoc process arising frompartially implemented legislative acts in combination with the behaviour ofdiverse actors operating autonomously within the system.
Whereas the system is highly centralized, with the Ministry of Healthexercising strong control over activities in the health sector, it has nonethelessbeen characterized by the absence of a steering mechanism where change isconcerned. The present paper will trace out the major reform plans which haveappeared in Greece since the early 1950s, and will identify the factors makingfor the inability of successive governments to pass health care reform legislationand implement change. It will be argued that reform planning in the health caresystem has historically and until recently been undertaken as a top-downprocess, by groups in theMinistry of Health or in government planning agenciesworking in relative isolation, with minimal input from broader segments of thepopulation and particularly from those actors who are most directly andintimately a�ected by processes of change. In part, the failure to pass legislationin the early years of reform planning was due to a lack of a political will, and alack of commitment to change in the health sector.
Until the decade of the 1990s, legislation that was successfully passed did soonly when the government in power was exceptionally strong. Whatever imple-mentation occurred following passage was in proportion to the strength of thegovernment in Parliament, to the degree of achievement of a consensus amongthe numerous actors involved in the process of change, and to the technical,institutional and administrative feasibility of the reform plan. The second andthird factors were as a rule ignored in reform planning, thus severely weakeningimplementation. This led to a strong divergence of actual developments in thehealth sector from the objectives of reform planners.
During the 1990s, however, there are strong indications that Greece hasentered a new policy phase, marked by increased constancy and stability. It willbe argued that the most recent health care reform legislation constitutes adeparture from the above pattern of change. While it is fairly ambitious in termsof what it aims to achieve, the legislation of 1997 is less radical in the means itpurports to use, and more pragmatic in that it takes into consideration thetraditional inertia of actors who are less bent towards change. In this process itis aided by the constraining in¯uence of the European Union on domesticpolicy-making, which tends to dilute the historical di�erences between politicalparties. In addition, the health care system in Greece, as elsewhere, is facing thepressures of ®scal constraints. It will be argued that these factors have had apositive in¯uence on policy-making processes in the Greek health sector.
108 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
A BRIEF OVERVIEW OF THE GREEK HEALTH CARE SYSTEMa
The Greek health care system is ®nanced both through taxation and socialinsurance sources, supplemented by a high proportion of voluntary ®nancing. Itdoes not therefore fall neatly into either the `Beveridge' or `Bismarck' mode of®nancing. Reforms of 1983 established a National Health System and attemptedto increase the share of state funding of the health care (Maniadakis andYfantopoulos, 1996), but fell short of achieving a full transition from predomin-antly insurance-based to predominantly tax-based ®nancing of health care.
The system can therefore be characterized as a complicated mixture of thepublic integrated model and the public contract model, with the former pre-domination over the latter (OECD, 1994). Secondary care and tertiary careare provided by the state and are ®nanced primarily by the state (approximately70 per cent of total NHS funding, along the lines of the integrated model)but also to a signi®cant degree by social insurance funds (about 30 per cent ofthe total, along the lines of the contract model; Ranos and Polyzos, 1994).Primary care is provided both by the state (for farmers and civil servants) andby social insurance funds (blue and white collar workers) and is also ®nanced byboth (about 10 per cent by the state and 50 per cent by social insurance funds).In addition, in view of the signi®cant size of private sector provision and out-of-pocket payments, the voluntary out-of-pocket mode of ®nance is also relevantin characterizing the system.b
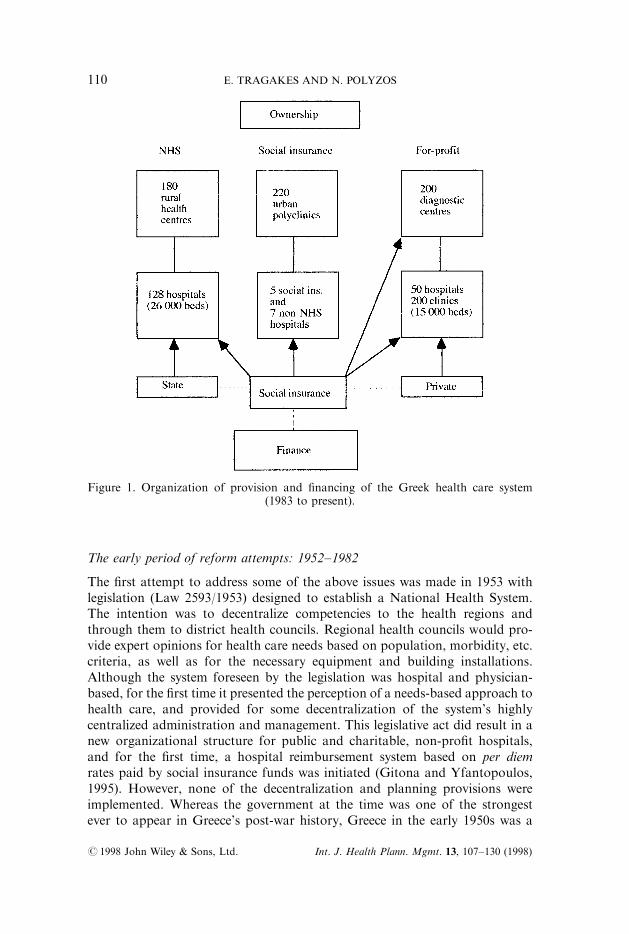
Organizationally, the system is highly centralized and regulated, with virtuallyevery aspect relating to health care and social care ®nancing and provisionsubject to control by the Ministry of Health and Welfare. The structure ofthe National Health Service is based on the regional and district division of thecountry, i.e. the 13 regions and 52 districts (Figure 1).
POST-WAR EFFORTS TO ACHIEVE COMPREHENSIVEHEALTH SYSTEM REFORM
The reform proposals put forward during the post-war decades in Greece looklike an unending process to try to reform the system, on the one hand, and toimpose obstacles in implementing these reforms, on the other. Although theemphasis has varied somewhat from proposal to proposal, the main themes ofthe proposed reforms have been remarkably similar: establishing a nationalhealth service; expanding public sector provision; achieving equity in accessand provision; consolidating the disparate and multiple sources of funding;addressing the weaknesses of primary health care; establishing a family doctorsystem based on general practice; instituting a referral system; and achievingsome degree of decentralization.
aFor a more thorough description of the Greek health care system, see WHO (1996).bPrivate expenditure on health constitutes about 40 per cent of total health care expenditure(Liaropoulos and Tragakes, 1998).
HEALTH CARE REFORMS IN GREECE 109
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
The early period of reform attempts: 1952±1982
The ®rst attempt to address some of the above issues was made in 1953 withlegislation (Law 2593/1953) designed to establish a National Health System.The intention was to decentralize competencies to the health regions andthrough them to district health councils. Regional health councils would pro-vide expert opinions for health care needs based on population, morbidity, etc.criteria, as well as for the necessary equipment and building installations.Although the system foreseen by the legislation was hospital and physician-based, for the ®rst time it presented the perception of a needs-based approach tohealth care, and provided for some decentralization of the system's highlycentralized administration and management. This legislative act did result in anew organizational structure for public and charitable, non-pro®t hospitals,and for the ®rst time, a hospital reimbursement system based on per diemrates paid by social insurance funds was initiated (Gitona and Yfantopoulos,1995). However, none of the decentralization and planning provisions wereimplemented. Whereas the government at the time was one of the strongestever to appear in Greece's post-war history, Greece in the early 1950s was a
Figure 1. Organization of provision and ®nancing of the Greek health care system(1983 to present).
110 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

war-ravaged country, lacking in even the most rudimentary institutionalinfrastructure that could have made the planned organizational and planningchanges possible. Moreover, the provisions of the legislation were viewed asbeing `too socialist' in the view of the highly conservative ideology of the time(Niakas, 1993).
Despite the very high rates of growth during the decades of the 1960s and1970s, public health care expenditure remained less than 2.5 per cent of GDP(Ministry of Health, 1994). The private sector in health care expanded rapidlyduring that period as a result of growth in numbers of physicians in soloprivate practice, as well as the erection of a number of small-scale privatehospitals. The state, by contrast, had developed only some public hospitals inlarge cities, while continuing to subsidize a number of charity hospitals(Yfantopoulos, 1994). Financing of the statutory system took place predomi-nantly through the numerous social health insurance funds that had graduallybeen formed over the years, the largest one of which (IKA) also directly pro-vided primary care services to its members. This pattern of services provisionwas consolidated during the dictatorship of 1967±74. At this time, anothermajor e�ort to organize a comprehensive health care system was made. In 1968a plan for health care reform was presented by the Minister of Health (PatrasPlan; Patras, 1970), aiming to reduce regional inequalities in provision throughthe geographical redistribution of services; expand public sector provision ofservices through the establishment of new public hospitals; introduce a familydoctor system and primary care based on general practitioners; improve healthcare services for the rural population; harmonize insurance fund regulationsand introduce an agency that would be the sole source of funding. However,the proposals never passed into legislation. Whereas there was no e�ectiveopposition to the junta government, the planned market elements of the pro-posal were highly incongruous with the pro-free market, private provisionmodel prevailing at the time. In addition, the proposed changes faced insur-mountable di�culties in view of the lack of necessary planning and manage-ment capabilities. By the end of the pilot period (1973) only a small portion ofthe plan had been implemented, publicly funded health care expenditures hadactually declined and the reform proposals were dropped.c
Following the restoration of democracy in 1974, social issues were for the newgovernment an area of signi®cant priority in view of increasing social andpolitical pressures and a growing number of unresolved problems intensifyingthe need for reform. In 1976, a working party of the Centre for Planning andEconomic Research (KEPE) prepared a study identifying the main problems ofthe health care system and proposing measures for their solution (Centerof Planning and Economic Research, 1976). The reform aims of the KEPEworking party were similar to those of the Patras Plan of 1968 and were viewedas entailing the necessary steps in a transition period that would eventually lead
cHowever, as a result of this legislation, graduating doctors were required to spend a 2-year periodpractising in rural areas. This was intended to alleviate the serious geographical maldistribution ofdoctors, characterized by high concentration in urban areas and pronounced shortages in ruralareas.
HEALTH CARE REFORMS IN GREECE 111
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

to the establishment of a National Health System. The proposals thereforecentred on the uni®cation of the services of the three major insurance funds(IKA, OGA and TEVE), covering roughly 85 per cent of the population, as wellas any other fund that wanted to join; and the establishment of a uni®ed fund.Implementation of these measures would be accompanied by the e�orts to traingeneral practitioners and increase the relative importance of public sector®nancing in health care. However, the plan remained an academic exercisewhich never became part of the political agenda. Political priorities at the timeincluded the restoration of democratic institutions, restructuring of theeconomy, and pursuit of broader social policy objectives.
Following the KEPE proposals, a team of experts in the Ministry ofHealth (1978±81) worked out a legislative proposal entitled `Measures forHealth Promotion' for the reorganization of the health care system (DoxiadesPlan). The proposal anticipated the creation of a planning agency for the co-ordination of health care provision and the development of a network of ruralhealth centres, sta�ed mainly by family physicians. However when the bill waspresented in Parliament it faced strong opposition by doctors' unions (whichwere controlled by the opposition party), as well as members of Parliament ofthe ruling party (Liaropoulos, 1992), and was rejected. The failure of this bill topass was largely due to the fact that it made its appearance in Parliament on theeve of national elections.d One may well ask why the bill was delayed and wasunder preparation for a period of about 3 years. The answer lies in the di�-culties that were encountered in the process of reaching a consensus between thedoctors' unions and the political parties.
These four reform plans illustrate the broad agreement among policy plannersregarding both the need for change and the direction of needed change. Thefactors behind the failure to implement legislation in the ®rst case and to passlegislation in the latter three can be summed up as political and ideologicalopposition to the reforms or lack of a political consensus, doctors' opposition,and lack of institutional infrastructure and administrative and planning capa-bilities, as well as lack of political will to address the problems of the healthsector. In brief, reform planners failed to base the proposals on political,ideological, and administrative/institutional/technical realities (Papoulias andTsoukas, 1994), while each of the governments involved was not su�cientlycommitted to change in the health sector.
The health care reform of 1983
By the early 1980s, widespread dissatisfaction with health care services andthe severity of problems in the system once again gave prominence to the issueof need for reforms. The new PASOK government which came to power in1981 stressed `change' in the broader social and political spheres. In 1982 theNational Drug Organisation (NDO), responsible for the administration and
dNo major legislative act has ever been passed in the Greek Parliament within a year or so prior tonational elections.
112 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
supervision of the pharmaceutical sector, and the Central Health Council(KESY), with an advisory function to the Ministry of Health, were formed.The latter was composed of representatives of doctors' and other health pro-fessionals' unions, representatives of university faculties, the governors of thelargest insurance funds, the chairman of the newly established NDO, andsenior o�cers of the Ministry of Health. KESY played a major role in thedevelopment of a new reform plan, which incorporated the main core of pro-posals that had been included in the earlier Doxiades Plan. In 1983 Law 1397,introducing a National Health System, was passed. It embodied the followingprinciples:
. Equity in ®nancing and delivery of health care services: there was to beuniversal coverage and equal access to health care services; the state was to befully responsible for the provision of health care services for the population;
. A new public±private mix: primary and secondary health services were to bemainly provided by health centres and public hospitals; publicly providedhealth services were to be expanded; establishment of private hospitals wasprohibited and those already in existence were to either close down or be soldto the public sector;
. Decentralization in the planning process, management improvement andcommunity participation: the Central Health Council (KESY) was to play anadvisory role to the Minister in health policy and research issues; healthcouncils (PESY) were to be established at a regional level with planning andadministrative responsibilities;
. Primary health care development: special emphasis was to be placed on thedevelopment of primary health care; a system of referral was to be estab-lished; a network of urban and rural health centres was to be establishedproviding comprehensive primary care services and implementing healthpromotion and disease prevention programmes;
. Labour relation and payment methods for health care providers: NHSdoctors and other health care sta� would be fully and exclusively employedby the NHS, and would be paid by salary, with signi®cant salary increases;
. New ®nancing mechanisms: a low tari� policy for health care services wouldbe imposed and incentives for greater use of the public sector would beintroduced; a process was to be set into motion leading to the uni®cation ofthe main insurance funds (especially IKA, OGA, and the state).
Seen in historical context, the 1983 reform represents the passing of a reformbill that was in preparation since the early 1950s, re¯ecting the same principlesembraced by reform planners over a span of 30 years. Its success in Parliamentand its subsequent partial implementation were on the whole due to the broadpolitical consensus that had been achieved by the early 1980s which included thehighly in¯uential doctors' unions, the strength of the government at that time,as well as the consensus on the need for reform.
The successful features of the reform can be brie¯y summarized to haveincluded the partial establishment of the NHS; the expansion of public
HEALTH CARE REFORMS IN GREECE 113
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

expenditure on health care; the construction of rural health centres as well as anumber of hospitals which contributed to an improvement in access to healthcare services especially for the rural population; and improved labour relations(mainly in the case of doctors) during the initial 5 years of implementation(Karokis et al., 1992).
Yet despite the highly favourable conditions, certain key legislative provisionswere never implemented: the family doctor system was not established; a referralsystem was not initiated; the urban health centres were not developed;e thepublic health system was not developed; inequalities in provision throughvariable fund bene®t packages persisted; the ®nancial footing of the NHSand the social insurance funds became increasingly unstable; decentralizationprocesses were not initiated; the rapid growth of the underground economyin health worked to undermine many of the achievements in equity; privateexpenditures on health increased signi®cantly and in fact did so more rapidlythan public expenditures; and there were additional perverse e�ciency develop-ments.
Implementation failures can be attributed to systemic rigidities, excessivelybureaucratic administrative and institutional infrastructure, poor planning andmanagement capabilities, the lack of technical manpower and expertise in themanagement of change, and doctors' resistance to the prospect of losing theirmanagerial positions, within hospitals, since it was customary to appointmedical personnel to managerial and administrative positions on the basis ofpolitical considerations (Yfantopoulos, 1988). The reform was therefore unableto address the key issues of managerial and ®nancial change, as well as severede®ciencies in provision.
In spite of its limitations, the 1983 reform did represent major change in thesystem as a result of the introduction of the NHS. Health policy in the decade ofthe 1980s was dominated by e�orts to alter the public±private mix in provisionin favour of the former. However no evaluation of the reform was ever under-taken in subsequent years. Concerning the public±private mix in provision,there is little question that the reform did result in a signi®cant shift in favour ofpublic provision (Kyriopoulos and Tsalikis, 1993; Ministry of Health, 1994).
REFORM INITIATIVES OF THE 1990s
At the end of the 1980s, there followed a 2-year period of political instability. In1989±90 there was a succession of governments, as a result of which there was aminimum of health policy. The election of the Conservative government in 1990marked an ideological shift which coincided with the onset of a period of ®scalrestraint. These factors were clearly re¯ected in a marked change in Greece'shealth policy orientation.
eExisting IKA polyclinics have played the role of the planned urban health centres, but do not coverthe entire urban population.
114 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
The health care reform acts of 1992 and 1994
In 1992 the Conservative government introduced a new health care reformact altering certain of the 1983 legislative provisions. The new legislative act(Law 2071), together with a new ®nancial policy for health care, focused mainlyon the following areas of change:
. The role of the citizen versus the state: Whereas the legislation of 1983 stressedthe role of the state in guaranteeing universal coverage and equity in healthservices provision, the 1992 Act (Article 1) presents the state as a guarantor ofthe citizen's right to seek preventive and curative care in accordance with theprinciples of freedom of choice and respect of human dignity.
. Freedom of choice: The legislation introduced freedom of choice of doctorand hospital institution.f
. Patients' rights: The legislation introduced rights of hospitalized patients,based on the European Charter of Patients' Rights.
. Managerial change: The legislation introduced certain managerial changesincluding the introduction of chief executives of hospitals; a manager fortechnical services; organizational changes in health centres; the introductionof managerial bodies in the Ministry of Health; and changes in the organiza-tional structure.
. Labour relations: As a result of the Act, doctors employed in public hospitalsbecame free to choose full or part-time employment within the NHS, withthe latter permitted to also practise privately.g
. Private versus public provision: The legislation abolished the restrictions of the1983 Act concerning the establishment and development of private hospitalsand clinics.
. Financial policy: Other adjustments (in addition to the legislation) included:(a) a huge increase in per diem hospital reimbursement rates (600 per cent)which created de®cits in the insurance funds for the ®rst time;h (b) thegranting of permission to insurance funds to contract with private clinicsand diagnostic centres; (c) the imposition of certain co-payments and fees inthe case of drugs, visits to outpatient departments and inpatient admissions;(d) increases in social insurance contributions; and (e) tax deductions forprivate insurance premiums.
Quite clearly, the above changes re¯ect three basic policy shifts: from stateto individual responsibility for health, from public to private sector provision,and from public (budgetary) to social insurance and private ®nancing of healthcare. The increased emphasis placed on private provision and ®nancing after
fThis had few practical implications because patient choice was largely free to begin with, due to thestructure of provision and the lack of a referral system (Kyriopoulos et al., 1994).gOnly 5 per cent of NHS doctors actually opted for part-time NHS employment.hBeginning in 1994, the inability of the state budget to provide subsidies and social insurance funds'inability to pay higher reimbursement rates to the hospitals have led to the creation of huge de®citsin hospital budgets. The increasingly unstable ®nancial footing of hospitals is an issue of majorconcern today.
HEALTH CARE REFORMS IN GREECE 115
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

1992 is closely linked to the increase in hospital reimbursement rates notedabove and the expansion of private insurance (Liaropoulos, 1995). Duringthe decade of the 1980s, the number of private hospital beds had declineddramatically as a result not only of restrictions imposed on the establishment ofprivate hospitals and clinics, but also through the maintenance of arti®cially lowhospital reimbursement rates, which forced private hospitals and clinics toeither close down, become absorbed by the public sector, or operate as littlemore than nursing homes. The huge (600 per cent) increase in hospitalreimbursement rates which occurred after 1992 permitted private clinics andhospitals to resume their operation.
The above changes did not represent an e�ort to introduce major systemreform, but were rather of an incremental nature. The 1992 legislative Act did notattempt to alter the basic structure of the NHS, nor to correct its unsound®nancial footing. Rather, e�orts focused on introducing new issues into thepolicy agenda and on dealing with ®scal priorities by reducing the scope of publicresponsibility. Thus, equity ceased to be a priority, while attention turned to thenew themes of e�ciency (through managerial changes) and cost-containment(through the introduction of cost-sharing arrangements) for the ®rst time. Theincreased ®nancial burden placed on the social insurance funds was the result ofthe need to lessen the pressures on budgetary ®nancing.
Some of the 1992 legislative and policy changes were short-lived. In January1994, the PASOK government (re-elected in October 1993) enacted new legisla-tion (Law 2194) which abolished certain of the articles of the 1992 legislationand returned to some of the 1983±89 regulations. Speci®cally, doctors once againhad to be fully and exclusively employed by the NHS; all managerial changesintroduced in 1992 were abolished except that regarding the chief executivesof hospitals (although that had never been implemented), and licences thathad been given to non-pro®t hospitals and the private ambulance sector wererevoked. In addition, the 1983 provision regarding equity in access wasre-introduced. However, the 1994 legislation did not abolish the new freedomsgranted in 1992 to private clinics, hospitals and diagnostic centres, and it main-tained all the ®nancial arrangements introduced by the Conservative govern-ment regarding cost-sharing, social insurance fund contracting with privatehospitals and diagnostic centres, and greatly increased hospital reimbursementrates burdening the social insurance funds. It also maintained the 1992 pro-visions on freedom of choice and patients' rights.
Clearly, the new policy orientation of PASOK was in agreement with therapidly growing role of private sector provision and ®nancing made possible bythe 1992 legislative and policy changes.
The 1994±96 legislative proposals
Since 1994, a number of factors once again combined to push the reform processforward. These included the changing international environment, persistentmacroeconomic constraints, the lack of policy formulation mechanisms inthe health sector, and persistent technical and administrative ine�ciencies. The
116 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
reform discussions which began in 1994 focused on several of the initial reformthemes which were prominent during the pre-1983 period, while at the sametime giving more emphasis to managerial and administrative aspects associatedwith e�ciency and productivity considerations. In addition, for the ®rst timethere appeared a concern for quality of health care services.
The issues underlying this reform drive included the following:
. absence of appropriate funding mechanisms in connection with levels of care,regions or social insurance funds, resulting in inequalities in populationcoverage and access to services;
. high system centralization, precluding local evaluation and decision-makingfollowing needs-based priority setting;
. absence of e�ective managerial structures and organizational±administrativepolicies leading to incentives for more e�cient and productive behaviour byhealth care personnel;
. absence of su�cient cost-containment measures, co-ordination of payments,e�ective incentives to providers, pricing policies, etc.;
. absence of a referral system associated with the weak primary care system;
. unequal distribution and education of health manpower, characterized bythe oversupply of doctors, dentists and pharmacists, and great shortages ofproperly trained nurses, technicians, managers and other highly specializedsta�;
. old-fashioned and bureaucratic role of public health at the central govern-mental level and the districts;
. lack of quality and audit control programmes resulting in low credibility ofthe system and low citizens' satisfaction.
In January 1994, the Minister of Health (under the PASOK government) setup two committees to investigate the reform options of the Greek health caresystem: a local committee including Greek experts from Greece and abroad(Ministry of Health, 1994), which produced an extensive report on the healthcare system and its shortcomings, and an international committee which visitedmany health services, and informed by the local committee, produced its ownrecommendations (Abel-Smith et al., 1994). The main points of the latter reportwere for the most part subsequently incorporated in a new reform plan whichappeared in 1995. In addition, the Minster of Health established three localcommittees to study the following areas:
. uni®cation of sickness fundsÐdecentralization (Sissouras et al., 1995);
. organization and management of the systemÐmanpower (Dervenis andPolyzos, 1995);
. GP networkÐprimary health careÐpublic health (Moraitis et al., 1995).
These committees, composed of politicians and social and professionalrepresentatives, made recommendations in each of the above areas. On thebasis of these recommendations, the local committee of Greek experts, togetherwith members of the three local committees, legal advisors of the Ministry of
HEALTH CARE REFORMS IN GREECE 117
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
Health and the Parliamentary Health Commission, prepared a new proposalconsisting of 100 articles (Kremastinos Plan, May 1995) that was to be sub-mitted to Parliament. The key elements were the following:
Financial change. The main social insurance funds were to transfer their fundsfor health care to one Uni®ed Sickness Fund (EFY) , which was to purchaseservices for its members. The government would transfer all subsidies allocatedto health care to this fund. The EFY was to be directly accountable to theMinister of Health, although it would be an independent public agency. Inaddition, global budgets for hospitals, as well as productivity incentives forpersonnel, were to introduced.
Organizational change and a purchaser±provider split. The provision and®nancing of health care was to be split, with the Ministry of Health responsiblefor provision and the Uni®ed Sickness Fund for ®nancing. New organizationalstructures would be established for the supervision of NHS services provisionand for assessing population needs locally as the basis for allocating the centralfund's resources across the regions.
Hospital management. Structural and ®nancial changes were to lead to thedevelopment of a managerial culture.
A family doctor system. A family doctor system, beginning with urban areas,was to be established. The country was to be divided into 400 `primary healthcare sectors' in which GPs would work in groups or solo practice with lists ofabout 1500 registered residents. There was to be free choice of GP. Existingurban polyclinics and rural health centres, as well as ambulance centres were tobe upgraded.
Focus on public health. Plans focusing on health promotion and preventionwere to be developed, with the establishment of: a multi-disciplinary publichealth service with trained public health doctors working at the new regionallevel in collaboration with the existing district level; at least one public healthlaboratory in every region; a national committee and a special directorate in theMinistry of Health to make speci®c planning arrangements; crash programmesfor the training of managers, public health doctors and GPs.
Rationalization of drug policy. New costing techniques, the introduction ofpositive lists and some cost containment through reference pricing.
Continuing education of health care professionals. Focus on doctors, nurses andmanagers.
Quality of care. Within hospitals through committees on evaluation ofutilization and on a national level through the establishment of an appropriateagency.
118 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
Prime Minister Papandreou approved the plan, together with 5000 appoint-ments of new NHS sta� (mostly quali®ed nurses, physicians, and a fewmanagers). A National Committee and a special Directorate in the Ministry ofHealth were established in order to make speci®c planning arrangements.Upgrading of the National School of Public Health was initiated. Despite someopposition to the reform plan shown by doctors' unions and the oppositionpolitical party, the proposals would have been submitted to Parliament inDecember 1995 had it not been for Prime Minister Papandreou's illness at thattime. The considerable disruption to the governing process which ensued,together with changes in the government (a new Prime Minister, a new Ministerof Health, etc.) resulted in postponement of the legislation.
The new PASOK government which was formed in early 1996 under PrimeMinister Costas Simitis a�rmed its strong interest in continuing the processof reform planning. However, under a new Minister of Health the earlierreform plan was modi®ed into a less radical and more pragmatic proposal(Peponis-Papadellis Plan). It was felt necessary to introduce changes intothe Kremastinos plan due to the usual practice whereby each Minister prefers toput his or her own personal touch into a reform plan. In addition, the new PrimeMinister had been appointed to replace the previous one, and had not yet beenelected by either the Party or the people through general elections; hence thegovernment was too weak to impose radical changes. Thus, relatively lessemphasis was placed on far-reaching organizational changes, and more onmeasures that would promote cost containment, e�ciency and productivity inthe health care system. In the actual process of modifying the Kremastinos plan,the initial health planning group was maintained, with additional inputs intoplanning from the academic sector and unions of health professionals. Theunions of doctors were opposed to those aspects of the earlier reform plan(particularly the foreign experts' proposals) which promoted rationalization ofthe health sector, and particularly to managerial changes which would restrictor change the relative hierarchy within hospitals.i In addition, doctors sought tosecure salary increases through promotions. Unions of other health careprofessionals were in favour of the reforms.
The modi®ed proposal focused on the following additional areas of change:
. rationalization of resources on the ®nancing side (while postponing theuni®cation of the biggest social insurance funds) and allocation of resourcesvia regional global budgets based on speci®c criteria;
. encouraging social insurance funds to establish a GP network beginning fromurban areas;
. upgrading emergency care (ambulances, mobile cardio-surgical units,helicopters, telematics, etc.) starting from the Aegean Islands;
. changing the ®nancing principles of the health care system by intro-ducing global budgets, cost accounting per department or case, productivity
iThe Panhellenic union of doctors was controlled by the Conservatives, while the union of hospitaldoctors was controlled by PASOK. Despite their di�ering political orientations the unions wereunited in their opposition to the reforms.
HEALTH CARE REFORMS IN GREECE 119
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
incentives for health care professionals, and by ®nding additional resourcesthrough speci®cally targeted state subsidies or cost savings from rationaliz-ation of expenses in drugs and medical supplies;
. abolishing the full-life tenure for new doctors entering into the NHS andopening the hierarchy for physicians already working in the NHS;
. focus on issues of quality of care and quality assurance through the establish-ment of a National Centre of Quality Control;
. rationalization of expenditures on drugs through costing based on realexpenditures and updating the role of the NDO.
By the summer of 1996, it appeared likely that these proposals wouldpass into legislation. As in the early 1980s, pressure was mounting for changein the health care system, and the less radical nature of the measures (comparedto the Kremastinos Plan of 1995) rendered them more easily acceptable bybroader segments of the population. Some opposition was shown by thedoctors' union, but only with respect to the provision abolishing full-life tenurefor new doctors entering the NHS. There was no other opposition to theproposals.
However, due to sudden general elections which were held in September1996, the above proposals were not submitted to Parliament. PASOK wasre-elected and a government was again formed under the leadership of PrimeMinister Costas Simitis who had replaced Andreas Papandreou earlier in theyear. The arrival of a new Minister of Health, however, once more signalled are-evaluation of the earlier reform proposals.
The health care reform legislation of July 1997 and implementation
The new government stressed `modernization' in all areas of public services, andthe Minister of Health declared the government's strong commitment to changein the health care system. Two committees were established: one to examine theNHS hospital de®cits (that had become a major issue since 1994) and another torevise the existing legislative proposal.
The ®rst committee concluded that there is wide scope for rationalization ofprocurement processes in public hospitals if decentralization and local manage-ment are implemented. Its early unpublished ®ndings suggested the need for aloan to be negotiated between the state on behalf of the hospitals as a whole andthe creditors in order to secure a signi®cant discount, and its proposals were infact implemented in 1997.
The second committee noted above made certain revisions to the earlierproposal. The new draft legislation (Gitonas Plan) was submitted to Parliamentin June 1997 and was passed into legislation on 17 July 1997 (N. 2519/21-8-97).Its provisions can be summarized as follows:
Patients' rights. The rights of hospital patients (granted by the legislation of1992) will be extended to cover all patients seeking primary care as well. Inaddition, each hospital is to set up a committee concerned with the protection of
120 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
patients' rights. A `National Committee of Bioethics and Deontology' (foreseenby the 1992 legislation) is to be made operational.
Public health. One central and 13 regional laboratories (corresponding toeach of the 13 regions of the country) are to be established and sta�ed withpublic health doctors, for the purpose of carrying out regional health policy; anagency for quality and accreditation of health services is to be established; and asystem of school doctors with lists is to be established. In addition and mostimportantly, the legislation established public health doctors and other scienti®cpositions to create public health networks in all regions.
Organization of the health care system, and decentralization. The legislationforesees the establishment of the NHS Management Executive in the Ministry;the appointment of regional directors for health care and welfare; and theestablishment of a Council for Co-ordination and Concerted Action in HealthServices which is to co-ordinate policy between the NHS and the socialinsurance funds. Decentralization is initially to take the form of deconcentra-tion, which is eventually intended to lead to devolution.j
Hospital management. The aim is to promote more democratic and e�cientmanagement practices, through the introduction of a chief executive, and anincrease in the number of executives who are no longer to be appointed by theMinister of Health.
Hospital ®nancing. The legislation foresees the introduction of global depart-mental budgets, a new costing system based on cost accounting per departmentor case (DRGs), productivity incentives for health care professionals.
Financing of the health care system. There is a vaguely formulated provisionallowing for the future possibility of a uni®cation of the social insurance funds.In addition, there are provisions allowing for negotiations on zero-based pricingfor private insurance companies intending to base prices on real costs andincrease hospital revenues.
Primary health care. `Primary health care networks' are to be established overa 3-year period throughout the country. These will consist of existing poly-clinics of social insurance funds in urban areas, and the existing health centres ofrural areas and will be sta�ed by GPs as well as a range of specialists. A systemof family physicians is to be instituted, each of whom will have a patient list ofa maximum of 2000 persons; family paediatricians will have patient lists of1600 persons. Each family will be free to choose its family physician andpaediatrician of the polyclinic or health centre in its area, as well as free toremain outside of the network if it so chooses. Individuals/families that partici-pate in the networks will be guaranteed easier access to services, reduced waiting
jThis is in accordance with the terminology of Mills et al. (1990).
HEALTH CARE REFORMS IN GREECE 121
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
periods and a well-integrated, holistic approach to care. Any person/familymay choose to participate in the system, regardless of fund membership.k
The networks are to operate through contractual agreements between socialinsurance funds, or the Ministry and insurance funds (in the case of the NHSrural health centres). Referral to higher levels of care will be part of the system,but will not be compulsory (hence there is to be no gatekeeping role of primarycare physicians).
Hospital care. NHS hospitals are to establish rehabilitation units; home careis to be promoted; afternoon outpatient services on a private basis are to bepermitted.
Doctors' labour relations. The legislation provides for abolishing full-life tenureof all newly appointed NHS hospital doctors (thus maintaining full-life tenurefor those already employed within NHS hospitals). In addition, it provides forincreased salaries for hospital doctors based on their promotion.
Payment methods for doctors. New payment methods are to be initiated in thePHC networks, consisting of fees per registered patient for speci®c services andcapitation.
Drugs. More responsibilities are to be given to the NDO. In addition, thelegislation provides for a reduction of the pro®t margin on drugs (approxi-mately a 20 per cent reduction) based on costing on actual prices, and theintroduction of a positive list and a hospital list.
Implementation of the legislation has already begun. First, the position of theNHS management executive, and those of chief executives in NHS hospitals,have been announced. Second, the Ministry has announced an internationaltender for a study investigating the restructuring of NHS hospitals (organizationand ®nancing dimensions within hospitals, as well as redistribution of resourcesacross regions). Moreover, in the light of a governmental decision to start aprocess of mergers or closures of public organizations for the purpose of pro-moting e�ciency in the larger public sector, this study is to investigate the meansby which such mergers can take place within the NHS hospital system. In thecase of the provisions dealing with primary health care and public healthnetworks, two committees have already begun to construct implementationplans. Further, in January 1998 a national positive drug list was announced,including 3200 drugs of a total of about 6000 available in the Greek market.
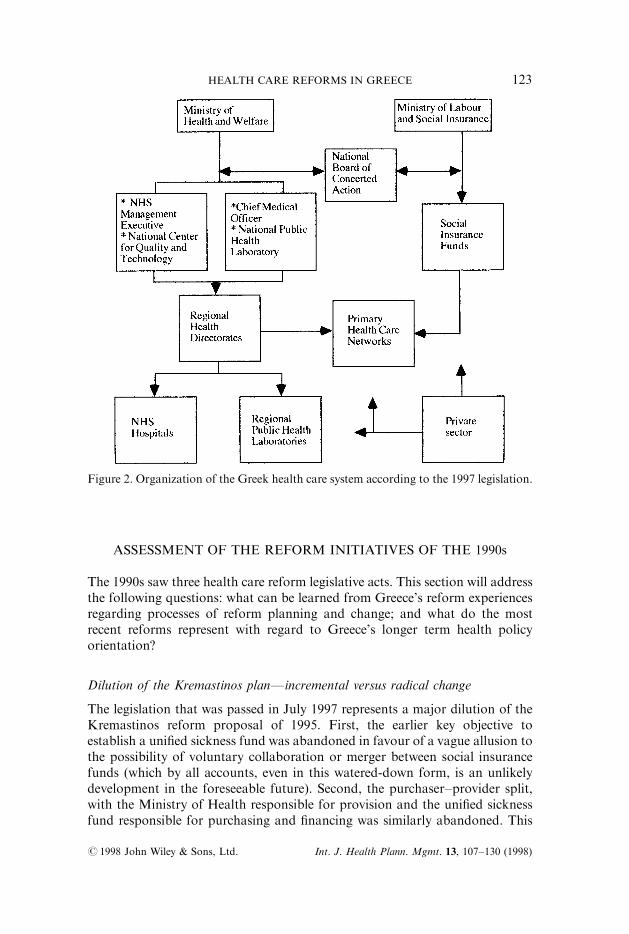
Figure 2 shows the organizational structure of the health care system asforeseen by the 1997 legislation.
kAt the present time, only members of the insurance fund IKA have access to the IKA polyclinics(about 50 per cent of the population). All others receive primary care services either at rural healthcentres, outpatient hospital departments, or private physicians contracted with the patient'srespective fund (other than IKA).
122 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
ASSESSMENT OF THE REFORM INITIATIVES OF THE 1990s
The 1990s saw three health care reform legislative acts. This section will addressthe following questions: what can be learned from Greece's reform experiencesregarding processes of reform planning and change; and what do the mostrecent reforms represent with regard to Greece's longer term health policyorientation?
Dilution of the Kremastinos planÐincremental versus radical change
The legislation that was passed in July 1997 represents a major dilution of theKremastinos reform proposal of 1995. First, the earlier key objective toestablish a uni®ed sickness fund was abandoned in favour of a vague allusion tothe possibility of voluntary collaboration or merger between social insurancefunds (which by all accounts, even in this watered-down form, is an unlikelydevelopment in the foreseeable future). Second, the purchaser±provider split,with the Ministry of Health responsible for provision and the uni®ed sicknessfund responsible for purchasing and ®nancing was similarly abandoned. This
Figure 2. Organization of the Greek health care system according to the 1997 legislation.
HEALTH CARE REFORMS IN GREECE 123
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

was replaced by provisions allowing for the possibility of selective contractingwith the social insurance funds as purchasers and the public and private pro-viders.l Third, concerning the establishment of a family doctor system, thepresent reform bill is far less radical in that it attempts to build on theexisting organizational structures of existing social insurance fund polyclinicsand health centres, and does not attempt a radical restructuring of PHC as inthe case of the `primary health care sectors' in the Kremastinos plan.
While abandoning or seriously modifying the above features of theKremastinos plan, the 1997 reform act maintains other key points. Speci®cally,it focuses on change in the areas of hospital management, public health, qualityof care, hospital ®nancing methods, payment methods for physicians, rational-ization of drug expenditures, and decentralization. These main issues arethe same between the two plans, though some of the details on how change isto be brought about may be di�erent. In addition to maintaining the focus onthe above issues, the 1997 legislation introduces one further issue which was notincluded in the Kremastinos plan, namely that of patients' rights which had ®rstappeared in the 1992 Act for hospital patients, and which is now extended tocover the rights of all patients. The important point to note here is that all theseareas of change (with the exception of decentralization), entail incrementalchange in the sense that it involves marginal changes within existing institu-tional structures as opposed to changes in the structures themselves (Duncanet al., 1995).
The case of decentralization is di�erent, in that it involves far-reachinginstitutional changes that depend heavily on both technical resources as well asa nation-wide institutional and organizational structure on which it can bebased. There cannot be decentralization of any kind in health services within asystem of public administration which is characterized by a high degree ofcentralization. Given the high degree of centralization which has prevailedhistorically in the Greek system of public administration, it is hardly surprisingthat all earlier plans to decentralize health care services failed to result inany concrete change. The current situation is likely to be di�erent, however,in view of a major plan to initiate a process of decentralization (in the sense of`deconcentration') in the country's entire system of public administration inJanuary 1998. Decentralization of health services as planned in the 1997 reformlegislation is therefore likely to follow as part of this larger process.
It follows that virtually all the features of the 1997 reform plan involve`incremental' (Lee and Mills, 1982) rather than radical change, at least as far as
lIt is being stressed here that selective contracting remains a possibility which could perhaps developin the major urban areas. Contracting has for many years been a feature of the Greek system, but itentails no competition whatever between providers. Such competition could develop if thepurchasers (the social insurance funds) decide to engage in selective contracting. Certain recentdevelopments suggest that a move in this direction is already taking place. IKA and other socialinsurance funds have begun to look for lower cost and higher quality providers of specializedservices (for example, cardio-surgery and orthopaedics). Also, private insurance companies thatwere previously contracting only with private hospitals, following the 1997 legislation, are obligatedto contract also with public hospitals which are reimbursed at full cost, and are also looking forlower cost, higher quality providers.
124 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
all change which originates from within the health sector. As such, they are farmore easily acceptable by the broader public in general, and by the communityof health professionals in particular. They are also much easier to implement, asthey do not entail any major mobilization of technical and ®nancial resources.
Top-down versus horizontal planning processes and the place of concessions
The 1997 reform act illustrates the importance of bringing diverse actorsfrom di�erent levels into the reform planning process. The Kremastinosproposal was based on planning by domestic and international academic circles.They produced a radical reform plan relative to the inertial frame of mind ofmany of the key actors of the system, which was based extensively oninternational knowledge and experience with health care reforms. The approachtaken was manifestly a top-down planning process with inadequate input fromkey domestic actors. There was little public debate on the areas of change thatwere being pursued, little e�ort to incorporate the voices of actors whowere to bea�ected by the proposed changes. The successive rounds of reform planningwhich followed, brought on by a series of accidental happenings in the politicalsphere, permitted the original plan to be modi®ed in accordance with thedemands of key actors, not least of whom are the doctors' unions. It is thusinteresting to note that the 1997 Act passed with a minimum of discussion andvirtually no opposition within Parliament.
The incorporation of diverse actors' voices into a reform planning processmay involve making concessions and providing inducements to potential foes ofthe reform (WHO, 1997). The most obvious inducement that was provided inthe Greek case, which made the passing of the 1997 Act possible, involved theinclusion of the provision which allowed increases in doctors' salaries based ontheir promotion and a new salary scale, as well as that which abolished full-lifetenure for only new doctors entering the NHS, thus safeguarding the positionsof doctors already employed within the NHS. Union support for otherunpopular measures (such as managerial changes in hospitals) was thus securedby the inclusion of these two measures. The dilution of the Kremastinos plandiscussed above, whereby the uni®ed fund, the purchaser±provider split, andthe comprehensive family doctor system were altered in favour of milderchanges, can also be looked upon as concessions which secured support for thereform.
The process of making concessions can have the e�ect of watering-down ordiluting original reform objectives, as discussed above. This could be seen as anegative development in the reform process, but it should be assessed relative torealistic alternatives. Judging from Greece's history with reform planning, thealternatives would appear to be the formulation of reform plans which donot get passed into legislation, or passing legislation which is subsequentlynot implemented. Thus, reform plans representing change which is of anincremental nature and incorporating compromise elements, may be the onlypragmatic route for a country like Greece, where entrenched interests preventthe formulation of a consensus for radical change (Walt and Gilson, 1994). This
HEALTH CARE REFORMS IN GREECE 125
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

is especially the case when a country does not have a very strong government.It might perhaps be argued that a strong government could act as a substitutefor consensus in enacting radical change, as it can minimize the in¯uences andcompeting demands of powerful interest groups. However, whereas a stronggovernment may more easily impose its own version of reform legislation, thisdoes not guarantee that the legislation will be implemented as planned, unlessother important conditions are satis®ed. If a consensus has been build into thereform plan, the changes for its successful implementation are greatly increased.
The relevance of international experiences
Greece is following current international trends with respect to health carereforms that focus increasingly on the larger issues of cost-containment, pro-motion of e�cient practices, decentralization, public health, quality assurance,and increased private responsibility for health and health care ®nancing. Inaddition, Greece appears to be attempting to selectively incorporate some morespeci®c elements of international experiences into its own institutional andorganizational structures. For example, it is borrowing somewhat from thenotion of purchaser functions for social insurance funds which may developinto provider competition, from the HMO experience which is being adapted toGreece's social insurance type of PHC, from UK-type regional authorities andNHS management as a basis for its plan to decentralize health care compe-tencies, and the establishment of a German-type Concerted Action Committeeto coordinate the functions of the social insurance funds with the NHS. What isimportant to note here is that each of these elements does not representindiscriminate imitation of institutions and practices of other countries, whichwould be unlikely to succeed in a foreign setting, but rather a cautious attemptto incorporate them into its own organizational and institutional structure suchthat they can be realistically adapted to the peculiarities of its own uniqueconditions.
Toward a more stable policy orientation
The 1997 legislative act undertaken by the PASOK government shows aclear continuity in health policy from the policy shift which occurred in 1992(under the Conservative government) and less from 1983 when the NHS wasestablished under the PASOK government.
Speci®cally, the 1997 Act appears to pay less attention to the equity principlewhich laid the foundation for the establishment of the NHS in 1983. The focuson individual responsibility for health is maintained, as is the issue of patients'rights which are now expanded to apply to all patients, while institutionalstructures strengthening patients' ability to exercise rights are providedfor. There is an emphasis on management and organizational structures forthe NHS as a whole and hospitals in particular with a view to promotingmore e�cient practices, and there are numerous measures in support of cost-containment policies and improved system e�ciency (hospital and physician
126 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

payment methods, rationalization of drug expenditures, an increased role forprivate insurance, continuation of cost-sharing arrangements, etc.). Regardingpublic versus private provision, the shift toward private provision which wasinitiated in 1992 continues unabated. Similarly, the shift away from public andtoward social insurance and private ®nancing is maintained; in fact the shifttoward private ®nancing is strengthened under the provisions allowing NHShospitals to receive afternoon visits on a private basis and the encouragement ofprivate insurance.
All of the above issues represent a continuity from 1992. At the same time, the1997 legislation picks up certain issues of the 1983 reform (mainly decentraliza-tion and management of the system and primary health care) which were notimplemented during the 1980s. Additional issues in the reform agenda of 1997which did not come from 1992 include public health and quality assurance,which are carry-overs from the Kremastinos plan. Thus, the key challengesfaced by the Greek health care system today, as in the case of many other Euro-pean countries, include the pursuit of e�ciency and e�ectiveness-promotingmeasures in the context of a greater focus on public health and quality assurance(Tountas, 1996).
The fact that the 1997 reform has essentially the same policy lime as the 1992reform has crucial implications for a country like Greece where traditionally,party politics polarized society and precluded the formation of a consensusacross political or ideological lines. It suggests quite clearly that party politicsare ceasing to play an overriding role in determining the course of policy. Itimplies that for the ®rst time in its post-war history Greece may be in a positionto embark upon a long-term, stable process of change, as opposed to short-term, erratic, and party-driven change. The ideological di�erences between thetwo main political parties of Greece (PASOK and New Democracy) havetended to diminish under the constraining in¯uence of the European Unionwhose convergence policy and dictates on structural transformation of theGreek economy and society lessen the scope for domestic di�erences. Ideo-logically inspired policies tend to be transformed into technocratic problemsand solutions, and this may facilitate the processes of conceptualization,planning, implementation and management of change.
CONCLUSIONS
Macroeconomic constraints currently faced by many countries operate as adeterrent to reform planning and implementation, as economic retrenchmentposes obstacles to the room for manoeuvre and provides less scope foropportunities for change (WHO, 1997). Periods of economic expansion tendto be more appropriate for reform undertakings, particularly if these requireincreases in ®nancial resources. The historical examination of Greece's experi-ence with health care reforms indicates that Greece di�ers from the abovepattern. The period of time from the 1950s through the 1970s was a time of
HEALTH CARE REFORMS IN GREECE 127
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)

signi®cant economic expansion for Greece.m There were numerous opportun-ities for change in the health care system, and there was considerable agreementamong reform planners across the political spectrum on both the need forchange and the direction of change. However, the low priority attached bygovernments at the time to change in health care, and the failure to ground theplans in political, institutional and technical realities, resulted in their totalfailure.
Ironically, the 1983 reform plan and its subsequent partial implementationcoincided with the ®rst period of major economic retrenchment that appearedin Greece in its post-war history. The government of the time was highly com-mitted to change, however, and large increases in public expenditure for socialpurposes (including health) that occurred during the 1980s were debt-®nanced.n
Economic constraints were therefore not responsible for the only partial imple-mentation of the 1983 reform plans. Rather, reasons must be sought in poorplanning and implementation capabilities, technical and institutional con-straints, and doctors' and their unions' control of managerial and politicalstructures. In brief, the reform plan was once again not su�ciently grounded ininstitutional and technical realities, while the in¯uential position of doctors wasnot adequately heeded.
During the 1990s, a new con®guration of conditions has appeared. Macro-economic constraints are of paramount importance as the EU convergencerequirements leave no room for delays. Agreement between the two mainpolitical parties of Greece concerning the need to meet the convergence require-ments has meant that ideological di�erences between them have been reduced.This point, together with the prevailing consensus on the imperative to conserveresources in all spheres of social and economic life have forced a situation whererationalization of the health sector (as in other social spheres) is deemednecessary. Thus, the three pieces of health care reform legislation passed in the1990s show continuity in the issues on the agenda and consistency in the policyorientation, even as governments have changed. Political will for change in thehealth sector has been mobilized by factors external to the sector itself. Still,political will is not by itself enough. The experience of the 1990s suggests thatthe presence of other conditions can facilitate the passing of a piece of legisla-tion. The conditions include the provision of incremental change as this is lessthreatening to entrenched interests, the incorporation of concessions andcompromise elements which will secure the support of otherwise hostile parties,and the selective incorporation of international experiences which are relevantto Greek needs as perceived by the key actors involved in the process of change.These conditions will also facilitate the process of change on the technical,institutional and administrative sides, which in the past have been constrainingfactors to successful implementation of reforms in Greece.
mDuring this period, Greece experienced the highest growth rates in real terms in Europe(Economist Intelligence Unit, 1989).nThe considerable debt-®nancing which began at this time laid the grounds for Greece's huge publicde®cit and high rates of in¯ation, which in later years and to the present have necessitated thepursuit of restrictive macroeconomic policies.
128 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
The same factors which have made the passing of recent legislation possibleare also likely to increase the chances of its successful implementation. Alreadya number of steps have been taken in this direction at a high level ofgovernment, indicating that reforms in health care have become a high priority.
The 1997 health care reform, even if implemented fully, by no means o�ersto solve some of the health sector's pressing problems. It could be argued that itis inadequate to solve the weaknesses in primary care as well as weaknesses onthe ®nancing side associated with the operation of disparate social insurancefunds. Moreover, it is silent on the issue of widespread uno�cial payments todoctors,o which is the greatest source of patient dissatisfaction in Greece.p
Nevertheless, it can be seen as an initial step in the right direction, beginning toaddress some of the problems, and as such, it may mark the start of a longerterm, focused, rational and pragmatic process of planning and change.
REFERENCES
Abel-Smith, B., Calltrop, J., Dixon, M. et al. (1994). Report on the Greek HealthServices. Athens: Ministry of Health and Social Welfare of Greece.
Besis, N. (1993). Private Health Services. Athens: Institute of Economic and IndustrialResearch (in Greek).
Center of Planning and Economic Research (KEPE) (1976). Programme for Economicand Social Development 1976±80: Health. Athens: KEPE (in Greek).
Dervenis, C., Polyzos, N. (1995). Study and Proposal on the Organization and Manage-ment of the NHS and the Development of Health Care Personnel. Athens: Ministry ofHealth and Welfare 2 (in Greek).
Duncan, J., Ginter, P., Swayne, L. (1995). Strategic Management of Health CareOrganizations, 2nd edition, Cambridge, Massachusetts: Blackwell.
Economist Intelligence Unit (1989). Country Pro®le, Greece, 1989±90. London:Economist Intelligence Unit, Ltd.
Gitona, M., Yfantopoulos, J. (1995). Management of public hospitals in Greece (1922±1992). Medicine, 67, 133±141 (in Greek).
Karokis, A., Mossialos, E., Sissouras, A. (1992) Achilles' heel. Health Service Journal102(5307), 22±25.
Kyriopoulos, J. (1993). Health Expenditures in Greece. Athens: Centre of Social andHealth Sciences (in Greek).
Kyriopoulos, J., Tsalikis, G. (1993). Public and private imperatives of Greek healthpolicies. Health Policy, 26, 105±117.
Kyriopoulos, J., Georgousi, E., Genimata, A. (1994). User satisfaction with healthservices in public hospitals. Patients and Health Care Professions in Greece. Athens:Academy of Health Professions (in Greek).
oIt is estimated that the black economy in health amounts to about 1.2 per cent of GDP(Kyriopoulos and Karalis, 1997).pThe 1983 reform had tried to address this problem indirectly, by attempting to make provision thealmost exclusive responsibility of the public sector, however it was largely unsuccessful, andaccording to all indications the uno�cial economy in health care is larger today than ever before(Kyriopoulos, 1993; Besis, 1993). However, this is a general problem in the Greek economy, and assuch its presence in the health sector is unlikely to be resovlved through action in the health sectoralone. Like the case of decentralization, which is being pursued in the wider national context, so it iswith the underground economy, which is being countered through tax policies a�ecting virtuallyevery sphere of economic activity.
HEALTH CARE REFORMS IN GREECE 129
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)
Kyriopoulos, J., Karalis, G. (1997). Current trends in the underground activities of thehealth care sector. Health Review, 8(49), 46±53 (in Greek).
Lee, K., Mills, A. (1982). Policy Making and Planning in the Health Sector. London:Croom Helm
Liaropoulos, L. L. (1992). Health policy: the Doxiades legislation. Medicine 61(4),367±371 (in Greek).
Liaropoulos, L. L. (1995). Health services ®nancing in Greece: a role for private healthinsurance. Health Policy 34, 53±62.
Liaropoulos, L., Tragakes, E. (1998). Public-private ®nancing in the Greek health caresystem: implications of equity. Health Policy 43(2), 153±169.
Maniadakis, N., Yfantopoulos, J. (1996). The phenomenon of induced demand inhealth services. Archives of Hellenic Medicine 13(1), 58±68 (in Greek).
Mills, et al. (Eds) (1990). Health System Decentralization: Concepts, Issues, and CountryExperience. Geneva: World Health Organization.
Ministry of Health (1994). Report on the Planning and Organization of Health Services inGreece. Athens: Ministry of Health and Social Welfare of Greece.
Moraitis, E., Georgousi, E., Zilides, C., Theodorou, M., Polyzos, N. (1995). Study onthe Organization and Function of a Primary Health Care System. Athens: Ministry ofHealth and Welfare 3 (in Greek).
Niakas, D. (1993). Health and Regional Development: Regional Health Policy in Greece.Athens: Centre of Social Sciences in Health (in Greek).
OECD (1994). The Reform of Health Systems: A Review of Seventeen OECD Countries.Paris: Health Policy Studies No. 5.
Papoulias, D., Tsoukas, H. (1994). Managing reforms on a large scale: what role forOR/MS? Journal of Operational Research Society 45, 977±986.
Patras, L. P. (1970). Planning of Social Policy. Athens: Greek Publishing Organisation(in Greek).
Ranos, C., Polyzos, N. (1994). Pharmaceutical policy within the Greek NHS.In: Mossialos, E., Ranos, C., Abel-Smith, B. (Eds). Cost Containment, Pricing andFinancing of Pharmaceuticals in the European Union. Athens: LSE Health andPharmetrica.
Sissouras, A., Karokis, A., Polyzos, N., Theodorou, M. (1995). Uni®ed Sickness Fund:Decentralization of Financing and organization of the System. Athens: Ministry ofHealth and Welfare 1 (in Greek).
Tountas, J. (1996). New strategies for primary health care. New Health 13, 1 (in Greek).Walt, G., Gilson, L. (1994). Reforming the health sector in developing countries. HealthPolicy and Planning 9(4), 353±370.
WHO (1996). Health Care Systems in Transition: Greece. Copenhagen: WHO, RegionalO�ce for Europe.
WHO (1997). European Health Care Reform: Analysis of Current Strategies.Copenhagen: WHO Regional Publications, European Series No. 72.
Yfantopoulos, J. (1988). Programming the Health Sector in Greece. Athens: NationalCenter of Social Research (in Greek).
Yfantopoulos, J. (1994). Economic and legal aspects of mental health policies in Greece.International Journal of Social Psychiatry 40(4), 296±305.
130 E. TRAGAKES AND N. POLYZOS
# 1998 John Wiley & Sons, Ltd. Int. J. Health Plann. Mgmt. 13, 107±130 (1998)












![“Yunanistan” [Greece]](https://static.fdokumen.com/doc/165x107/63250e4a85efe380f30680d9/yunanistan-greece.jpg)






