The effect of geometric and topologic differences in boundary element models on magnetocardiographic...
11
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 47, NO. 9, SEPTEMBER 2000 1237 The Effect of Geometric and Topologic Differences in Boundary Element Models on Magnetocardiographic Localization Accuracy Katja Pesola*, Jyrki Lötjönen, Associate Member, IEEE, Jukka Nenonen, Isabelle E. Magnin, Member, IEEE, Kirsi Lauerma, Riccardo Fenici, and Toivo Katila Abstract—This study was performed to evaluate the changes in magnetocardiographic (MCG) source localization results when the geometry and the topology of the volume conductor model were altered. Boundary element volume conductor models of three patients were first constructed. These so-called reference torso models were then manipulated to mimic various sources of error in the measurement and analysis procedures. Next, equivalent current dipole localizations were calculated from simulated and measured multichannel MCG data. The localizations obtained with the reference models were regarded as the “gold standard.” The effect of each modification was investigated by calculating three-dimensional distances from the gold standard localizations to the locations obtained with the modified model. The results show that the effect of the lungs and the intra-ven- tricular blood masses is significant for deep source locations and, therefore, the torso model should preferably contain internal inho- mogeneities. However, superficial sources could be localized within a few millimeters even with nonindividual, so called standard torso models. In addition, the torso model should extend long enough in the pelvic region, and the positions of the lungs and the ventricles inside the model should be known in order to obtain accurate lo- calizations. Index Terms—Boundary element modeling, equivalent current dipole localization, magnetocardiography. I. INTRODUCTION M AGNETOCARDIOGRAPHIC (MCG) source imaging has received increasing interest in recent years [1]. In particular, the ability of MCG to locate current sources, com- bined with precise timing of events, is valuable both in basic re- Manuscript received September 23, 1999; revised April 25, 2000. This work was partly supported by the Academy of Finland and by the Finnish Cultural Foundation. Asterisk indicates corresponding author. *K. Pesola is with the Laboratory of Biomedical Engineering, Helsinki University of Technology, 02150 Espoo, Finland, and the BioMag Laboratory, Helsinki University Central Hospital (HUCH), 00290 Helsinki, Finland (e-mail: [email protected]). J. Lötjönen is with the Laboratory of Biomedical Engineering, Helsinki University of Technology, 02150 Espoo, Finland, and the BioMag Laboratory, Helsinki University Central Hospital (HUCH), 00290 Helsinki, Finland. He is also with the Creatis, Insa 502, 69621 Villeurbanne Cedex, France. J. Nenonen and T. Katila are with the Laboratory of Biomedical Engineering, Helsinki University of Technology, 02150 Espoo, Finland, and the BioMag Lab- oratory, Helsinki University Central Hospital (HUCH), 00290 Helsinki, Fin- land. I. E. Magnin is with the Creatis, Insa 502, 69621 Villeurbanne Cedex, France. K. Lauerma is with the Department of Radiology, HUCH, 00290 Helsinki, Finland. R. Fenici is with the Clinical Physiology - Biomagnetism Center, Catholic University of Rome, 00168 Rome, Italy. Publisher Item Identifier S 0018-9294(00)08002-2. search and in clinical studies [2], [3]. MCG localization studies based on an equivalent current dipole (ECD) source model are useful in finding focal sources associated with cardiac arrhyth- mias or other pathologies [4]–[6]. The accuracy of ECD local- ization in these studies has been found to vary between 7–20 mm. In source localization studies, the forward problem has to be solved first, i.e., one has to calculate the electromagnetic field on the surface and outside of the body for the selected source and volume conductor model. Therefore, the forward problem for ECD in boundary element (BE) volume conductors has been investigated as a function of the complexity of the torso model [7]–[9]. In the inverse problem, the aim is to solve for the param- eters of an ECD (the position and the dipole moment) from mea- sured MCG data. Several studies have been reported concerning the effects of inhomogeneities on the MCG ECD localization accuracy [10]–[14]. To our knowledge, systematic studies have still not been reported on establishing the relationship between the geometric and topologic errors of the BE models, and the accuracy of ECD inverse solutions. The purpose of the present study was to specify the effect of various sources of error in BE model construction, in order to obtain accurate dipole localizations from multichannel MCG recordings. The required accuracy in clinical MCG studies is strongly dependent on the application; however, the result should point to the correct anatomical region of the heart. An accuracy of 10 mm is usually considered high enough for most clinical purposes. Another aim of this study was to establish practical guidelines for flexible, automated BE model generation. Three patients (two males and one female) were selected for the study. Individual thorax models of the patients were built using the segmentation and triangulation methods developed earlier in our laboratory [15], [16]. These torso models served as reference models throughout this study. The reference models were modified to represent different aspects of the model gen- eration process. The resulting changes in the localization ac- curacy were determined by computing the three-dimensional (3-D) distances from the ECD localizations obtained with the reference models to the ECD locations produced by the modi- fied models. Both simulated and measured multichannel MCG data were used in the calculations. II. CONSTRUCTION OF THE REFERENCE MODELS In our MCG studies, the BE models are constructed using magnetic resonance (MR) images providing detailed 3-D geom- 0018–9294/00$10.00 © 2000 IEEE
Transcript of The effect of geometric and topologic differences in boundary element models on magnetocardiographic...

IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 47, NO. 9, SEPTEMBER 2000 1237
The Effect of Geometric and Topologic Differences inBoundary Element Models on Magnetocardiographic
Localization AccuracyKatja Pesola*, Jyrki Lötjönen, Associate Member, IEEE, Jukka Nenonen, Isabelle E. Magnin, Member, IEEE,
Kirsi Lauerma, Riccardo Fenici, and Toivo Katila
Abstract—This study was performed to evaluate the changesin magnetocardiographic (MCG) source localization results whenthe geometry and the topology of the volume conductor modelwere altered. Boundary element volume conductor models of threepatients were first constructed. These so-called reference torsomodels were then manipulated to mimic various sources of errorin the measurement and analysis procedures. Next, equivalentcurrent dipole localizations were calculated from simulated andmeasured multichannel MCG data. The localizations obtainedwith the reference models were regarded as the “gold standard.”The effect of each modification was investigated by calculatingthree-dimensional distances from the gold standard localizationsto the locations obtained with the modified model.
The results show that the effect of the lungs and the intra-ven-tricular blood masses is significant for deep source locations and,therefore, the torso model should preferably contain internal inho-mogeneities. However, superficial sources could be localized withina few millimeters even with nonindividual, so called standard torsomodels. In addition, the torso model should extend long enough inthe pelvic region, and the positions of the lungs and the ventriclesinside the model should be known in order to obtain accurate lo-calizations.
Index Terms—Boundary element modeling, equivalent currentdipole localization, magnetocardiography.
I. INTRODUCTION
M AGNETOCARDIOGRAPHIC (MCG) source imaginghas received increasing interest in recent years [1]. In
particular, the ability of MCG to locate current sources, com-bined with precise timing of events, is valuable both in basic re-
Manuscript received September 23, 1999; revised April 25, 2000. This workwas partly supported by the Academy of Finland and by the Finnish CulturalFoundation.Asterisk indicates corresponding author.
*K. Pesola is with the Laboratory of Biomedical Engineering, HelsinkiUniversity of Technology, 02150 Espoo, Finland, and the BioMag Laboratory,Helsinki University Central Hospital (HUCH), 00290 Helsinki, Finland(e-mail: [email protected]).
J. Lötjönen is with the Laboratory of Biomedical Engineering, HelsinkiUniversity of Technology, 02150 Espoo, Finland, and the BioMag Laboratory,Helsinki University Central Hospital (HUCH), 00290 Helsinki, Finland. He isalso with the Creatis, Insa 502, 69621 Villeurbanne Cedex, France.
J. Nenonen and T. Katila are with the Laboratory of Biomedical Engineering,Helsinki University of Technology, 02150 Espoo, Finland, and the BioMag Lab-oratory, Helsinki University Central Hospital (HUCH), 00290 Helsinki, Fin-land.
I. E. Magnin is with the Creatis, Insa 502, 69621 Villeurbanne Cedex, France.K. Lauerma is with the Department of Radiology, HUCH, 00290 Helsinki,
Finland.R. Fenici is with the Clinical Physiology - Biomagnetism Center, Catholic
University of Rome, 00168 Rome, Italy.Publisher Item Identifier S 0018-9294(00)08002-2.
search and in clinical studies [2], [3]. MCG localization studiesbased on an equivalent current dipole (ECD) source model areuseful in finding focal sources associated with cardiac arrhyth-mias or other pathologies [4]–[6]. The accuracy of ECD local-ization in these studies has been found to vary between 7–20mm.
In source localization studies, theforward problemhas to besolved first, i.e., one has to calculate the electromagnetic fieldon the surface and outside of the body for the selected sourceand volume conductor model. Therefore, the forward problemfor ECD in boundary element (BE) volume conductors has beeninvestigated as a function of the complexity of the torso model[7]–[9]. In theinverse problem, the aim is to solve for the param-eters of an ECD (the position and the dipole moment) from mea-sured MCG data. Several studies have been reported concerningthe effects of inhomogeneities on the MCG ECD localizationaccuracy [10]–[14]. To our knowledge, systematic studies havestill not been reported on establishing the relationship betweenthe geometric and topologic errors of the BE models, and theaccuracy of ECD inverse solutions.
The purpose of the present study was to specify the effect ofvarious sources of error in BE model construction, in order toobtain accurate dipole localizations from multichannel MCGrecordings. The required accuracy in clinical MCG studiesis strongly dependent on the application; however, the resultshould point to the correct anatomical region of the heart.An accuracy of 10 mm is usually considered high enoughfor most clinical purposes. Another aim of this study was toestablish practical guidelines for flexible, automated BE modelgeneration.
Three patients (two males and one female) were selected forthe study. Individual thorax models of the patients were builtusing the segmentation and triangulation methods developedearlier in our laboratory [15], [16]. These torso models servedasreference modelsthroughout this study. The reference modelswere modified to represent different aspects of the model gen-eration process. The resulting changes in the localization ac-curacy were determined by computing the three-dimensional(3-D) distances from the ECD localizations obtained with thereference models to the ECD locations produced by the modi-fied models. Both simulated and measured multichannel MCGdata were used in the calculations.
II. CONSTRUCTION OF THEREFERENCEMODELS
In our MCG studies, the BE models are constructed usingmagnetic resonance (MR) images providing detailed 3-D geom-
0018–9294/00$10.00 © 2000 IEEE

1238 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 47, NO. 9, SEPTEMBER 2000
etry. The MR images of the three patients included in this studywere taken at the Helsinki University Central Hospital (HUCH)with a 1.5 T device (Magnetom Vision, Siemens AG, Erlangen,Germany). The objects of interest were segmented from MRimages using a method based on a deformable pyramid [15].The method elastically matches boundary element templates,i.e., triangulated surfaces representing the typical size and shapeof the objects of interest, to noisy edges extracted from MRimages. In the triangulation stage [16], a marching cubes tri-angulation, containing several hundreds of thousands of trian-gles, was produced. Thereafter, a mesh-simplification methodwas applied, resulting in the final set of triangles. Finally, theBE model was aligned with the MCG coordinate system usingexternal markers.
The BE models contained the following surfaces: outer bodysurface (B), left lung (LL), right lung (RL), left ventricle (LV),and right ventricle (RV). In our reference models, the numberof triangles in B, LL, RL, LV, and RV were 700, 200, 200, 200,and 200, respectively. The solid angle of the triangles, calculatedfrom the center of the heart, was approximately constant on theB, LL, and RL surfaces. Thus, in B, LL and RL the size of thetriangles was smallest near to the heart where the electromag-netic gradients show largest spatial variation. The length of theedge (LE) of the smallest triangles in B was about 1.6 cm. Alltriangulations were closed, and approximated by a tessellationof triangles.
III. FORWARD AND INVERSECOMPUTATIONS
In the calculations, the volume conductor was assumed to bepiecewise homogeneous with respect to the electrical conduc-tivity, each region having a constant conductivityand beingbounded by the surface . In this case, the magnetic field dueto the internal current sources can be expressed as [17]
(1)
where and are the conductivities inside and outside ofthe surface , respectively, and is the number of regions.Vector refers to the observation point, vector to the inte-gration point, and is a vector element of surface
, oriented along the outward unit normal. is the mag-netic field produced by the current sources in an infinite ho-mogeneous volume conductor. The electric potentialon thesurface can be obtained from the integral equation [18]
(2)
where is the electric conductivity at the source location, andis the electric potential produced by the current sources in
an infinite homogeneous volume conductor.
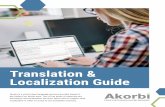
Fig. 1. The positions of the dipoles used in generating the MCG data forthe first patient are presented with the triangulated heart (a) in an anteriorprojection and (b) in a projection visualized as looking from the feet to thehead of the patient. (e= the direction of the dipoles, SA= sino-atrial node, AV= atrio-ventricular ring, CS= coronary sinus, Q= origin of activation in theinterventricular septum, RV= right ventricle, LVA= anterior left ventricle,LVP = posterior left ventricle, and AP= apex)
The discretization of (1) and (2) is based on the BE method,assuming triangulated surfaces and linearly varying surface po-tentials over the triangles. The accuracy of constant vs. linearpotential approximation functions has been investigated, e.g.,by de Munck [19] and by Ferguson and Stroink [20], who foundthat the linear approach is more accurate than the constant one incalculating surface potentials. In addition, linear basis functionsallow the use of twice as many triangle elements as the constantfunctions with the same system matrix dimension. Therefore,linear potential approximation was used in this study when theeffect of the boundaries was included in the solution.
Following de Munck [19] and Fergusonet al. [21], we eval-uated the surface integrals in (1) and (2) over each triangle an-alytically. This evaluation included the calculation of the solidangle subtended by a plane triangle [22]. The singularity of theresulting system of equations was removed by using the defla-tion technique [23]. Thereafter, (1) and (2) were transformedinto matrix equations [24].
In this study, constant conductivities of 0.2 S/m, 0.05 S/m,and 0.6 S/m were assigned to the torso, to the lungs and to theblood masses, respectively. The conductivity in the myocardiumwas the same as in the torso. These are the values most fre-quently used in the literature. The errors in assumed conductivi-ties have been addressed, e.g., by Throne and Olson [25] who in-vestigated their effect on electrocardiographic inverse solutions.
To investigate a variety of different source locations, a currentdipole was placed at eight different positions inside the heart: 1)sino-atrial node (SA), 2) left lateral atrio-ventricular ring (AV),3) coronary sinus (CS), 4) the site of origin of the activation inthe interventricular septum (Q), 5) the mid-anterior wall of theRV, 6) the antero-lateral wall of the left ventricle (LVA), 7) themid-posterior wall of the left ventricle (LVP) and 8) the apex(AP). The source positions for the first patient are presented inFig. 1.
The direction of the dipoles () was constant in all simula-tions; , (see Fig. 1).The strength of the source was varied as a sinusoidal wave, withthe dipole amplitudes ranging from 0.2 to 10Am. The forwardMCG solutions were calculated with the densest triangulationsused in this study, the surfaces B, LL, RL, LV and RV consistingof 1000, 300, 300, 300, and 300 triangles, respectively. No noisewas added to simulated data because in this case, only the effect

PESOLAet al.: EFFECT OF GEOMETRIC AND TOPOLOGIC DIFFERENCES IN BEMs ON MCG LOCALIZATION ACCURACY 1239
Fig. 2. An MCG signal from the central channel of the dewar (a) simulatedby placing a current dipole in the apex area and (b) averaged after pacing theheart in the right ventricle. The time interval of the localizations calculated frommeasured data is marked in the beginning of the cardiac evoked field.
of BE modeling on dipole localizations was studied. However,the measured MCG data contained a realistic amount of noise,as well. An example of the simulated data in one MCG channel,originating from a dipole in the apex of the first patient, is pre-sented in Fig. 2(a).
In the generation of the simulated multichannel MCG data,a 99-channel cardiomagnetometer was simulated, including 33planar gradiometer pairs, each containing two figure-of-eightloops, and 33 magnetometers positioned on top of the planarunits. This sensor configuration combines the advantages ofdifferent sensor types, and is more optimal for cardiomagneticstudies than a system consisting solely of planar gradiometers[26].
In addition to simulated data, measured multichannel MCGrecordings from the three patients included in this study wereutilized. The MCG data were recorded with a 67-channelcardiomagnetometer (Neuromag Ltd., Helsinki, Finland) atthe BioMag Laboratory [27] of HUCH. Both the 99-channelconfiguration used in the simulations and the 67-channel devicewere similarly positioned with respect to the anterior surfaceof the torso.
Before the MCG recordings, a nonmagnetic stimulationcatheter [28] was inserted in the right ventricle of two patientsand in the coronary sinus of one patient. The catheter pulsestimulated the myocardial cells near the tip of the catheter,causing an evoked response in the myocardium. The my-ocardial evoked response is reflected in the measured MCGdata as a cardiac evoked field [5]. The MCG recording wascarried out in a magnetically shielded room during cardiacpacing (see [5] and [6]). In this study, dipole localizationswere calculated for the initial phase of the paced activationsequence from signal-averaged MCG data. As the recordingsof paced activation lasted for 30 s with a 0.5–0.6 s stimulusinterval, altogether 50–60 cycles were included in the averages.The first two right-ventricular catheter positions representedsuperficial sources, located close to the anterior surface of theheart. The coronary sinus position represented a deep sourcelocation close to the posterior surface of the heart. An exampleof the measured MCG signals, used in calculating localizationsfor the first patient, is presented in Fig. 2(b). The time interval(5 ms) during which the localizations were calculated, is alsopresented. Since the sampling frequency used in the recordingswas 2 kHz, altogether ten localizations were calculated frommeasured MCG data with each modified BE model.
The ECD parameters were estimated with the iterative Leven-berg–Marquardt (LM) nonlinear least squares fitting [29]. TheLM-algorithm minimizes the squared differencebetween themeasured and the calculated magnetic field
(3)
where denotes to the number of sensors,to the measuredand to the calculated field at theth sensor, respectively.Theparameter vector contains the six parameters of a dipole. Thecurrent values of the parameters are updated with a stepwhich is determined from
(4)
where is the Jacobian of and is the identity matrix. Thevalue of the constant is chosen so that the approximation ofthe Hessian matrix on the left-hand side is positive definite. TheLM-algorithm was realized with the Minpack routines in Netlib.
In the LM-algorithm, an initial set of values for the dipoleparameters is required. Often it was found that the localizationresults were dependent on the initial guess. This phenomenon ismostly due to the secondary sources on the ventricular bound-aries which are located close to the actual source. These sec-ondary sources may increase the number of local minima inthe biomagnetic cost function to which the LM-algorithm mayincorrectly converge. In addition, numerical difficulties in thecalculations may occur if the source is located very close to aboundary. Therefore, multiple initial guesses were used in thelocalizations, and the goodness-of-fit value was used to evaluatethe quality of the localizations. Typically, the initial position forthe dipole fitting had to be close, within 1–2 cm from the truelocation of the source to obtain a good localization result.
IV. GENERATION OF THEMODIFIED MODELS
In this study, the dipole localizations calculated with the ref-erence models were regarded as thegold standard(GS). Fourgroups of BE models were created by modifying the referencemodels in a controlled way. The effect of BE model propertieson the localization accuracy was studied by calculating 3-D dis-tances from the GS locations to the localizations obtained withthe modified BE models. Therefore, the correctness of GS lo-calizations was not emphasized. For each patient, about 100different BE models were constructed. The purpose was notto build a detailed quantitative correlation between the modelproperties and the localization accuracy, but to establish guide-lines for their relationship.
The modifications in reference models simulated varioussources of error in the BE model construction. The purpose wasto find out the effect of modifications on the MCG localizationaccuracy, in order to eliminate the most significant error sourcesin the future. In the first group of modifications (Group A), thegeometric accuracy of BE models was studied. The final sizeand shape of the BE model with respect to the size and shape ofthe patient during MCG measurements may differ due to, e.g.,the protocol applied in the anatomical imaging, the positioning

1240 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 47, NO. 9, SEPTEMBER 2000
of the patient, breathing, and segmentation accuracy. In thesecond group of modifications (Group B), the effects of thetriangulation protocol, such as the number and the shape ofthe triangles, were considered. The third group (Group C)demonstrated the effect of errors in rigid registration, i.e., whenthe model was misaligned by rotation and translation. In thefourth group of modifications (Group D), the combinations ofdifferent error sources were studied.
A. Geometric Accuracy—Group A
In group A, the effect of the geometric accuracy of the BEmodel on the localization results was studied. When MR im-ages are utilized in the BE model construction, several factorsaffect the final geometry of the model. These factors include,e.g., the MR imaging (MRI) protocol, the position of the pa-tient during the imaging, and the segmentation of the anatom-ical images. In addition to MR images, an approximation of theindividual BE model can also be constructed from two orthog-onal X-ray projections [30]. The advantage of X-ray imageswith respect to MR images is that they are easily available atlow cost. If no anatomical information is available, astandardmodel, i.e., a model which is not patient-specific but representsan average shape of each object of interest, is usually applied inMCG studies. In group A, the geometric properties of the refer-ence model were varied to simulate some of the modeling errorsrelated to the X-ray reconstruction and to the standard models.The effects caused by using an X-ray-based model or a standardmodel were studied in group D, because these models were con-sidered to include several error sources affecting the localizationaccuracy.
The first problem of the whole modeling process is to estab-lish the MR imaging protocol. The selection of the field of view(FOV) strongly affects the geometry of the model to be con-structed. To investigate which parts of the thorax should be in-cluded in the model, the reference model was modified in threeways: 1) The arms were included in the model ( , i.e., groupA, modification 01). 2) The neck was removed from the modelby excluding 3 cm from the superior part of the MR volume( ). 3) B was shortened and lengthened by 5 cm in the pelvic
). In the reference models, the lowest part of themodel was about 15 cm below the apex of the heart.
Inaccuracies in the torso modeling are also caused by the dif-ferent positioning of the patient in the MRI tube with respectto the conditions during MCG recordings. The errors producedby the positioning of the patient were simulated by a deforma-tion grid Fig. 3. A grid was set around the model.By displacing a grid point, the model was deformed utilizingtrilinear interpolation [15]. Three kinds of elastic deformationswere produced.
1) The shoulders are most sensitive to positioning errors.The errors in the positioning of the shoulders weresimulated by raising both shoulders by 3 cm ( ),by lowering both shoulders by 3 cm ( ), by raisingone shoulder and lowering the other by 3 cm ( );these modifications were accomplished by moving gridpoints near both shoulders, i.e., the points and
in Fig. 3.
Fig. 3. Elastic deformation of a reference model using a deformation grid.Both shoulders were raised by 3 cm from their original position, thus simulatingthe positioning differences during the MRI and the MCG measurements.
2) The MRI bed is concave whereas the MCG bed is flat.The center of the MRI bed is about 3 cm lower than thesides of the bed. Concavity of the MRI bed was simulatedby displacing the grid points on both the left and the rightside of the body by 3 cm in the antero-posterior direction( ) [the points and ].
3) The phase of breathing in the model defined from MRimages usually differs from the phase during MCG local-ization. The effect of breathing in the model defined fromMR images was studied by moving the grid point (1, 0, 0)by 1.5 cm in the antero-posterior direction ( ).The movement of the heart, caused by breathing, was notconsidered here. However, it may considerably affect theMCG localization accuracy. Variation in the position ofthe heart was studied in group C, presented later.
Next, more general differences in geometry during anatom-ical imaging and MCG measurements, as well as segmentationerrors related to constructing the BE model from MR images,were studied. First, the reference model was scaled using anisotropic scaling, i.e., a constant coefficient for all coordinateaxes. Second, each coordinate axis was scaled separately whilekeeping the other directions constant. The body surface, thelungs and the ventricles were studied separately. The scaling co-efficients were chosen in such a way that the surfaces B, LL andRL, and LV and RV in each direction were displaced maximallyby 15, 15, and 5 mm, respectively. The isotropic scalingof the body produced the models , and the anisotropicscaling the models – . The models – were gen-erated similarly by scaling the lungs and the models–by scaling the ventricles. After the scaling, possible overlapswith other surfaces were corrected by minimal interactive andelastic deformations.
Previously, the segmentation error caused by our automaticMR image segmentation tool with respect to a manual segmen-

PESOLAet al.: EFFECT OF GEOMETRIC AND TOPOLOGIC DIFFERENCES IN BEMs ON MCG LOCALIZATION ACCURACY 1241
tation was found to be about 4 mm for volumes[15]. However, the estimation of the final segmentation accuracyis difficult since it depends on several reasons, e.g., on the ob-ject to be segmented, on the properties of the anatomical data,and on the users/experts segmenting the data. It is worth notingthat in addition to segmentation errors, the BE model containsother geometrical inaccuracies, e.g., arising from patient posi-tioning, which cannot be simulated by the simple modificationsof – . Considering the technique in which the models arebuilt from two orthogonal X-ray projections, the error arisingfrom the method itself was found to be about 5 mm [30]. There-fore, the magnitudes of changes related to the scaling of the BEmodel were reasonably high in the present study. Although theapplied modifications were larger than the geometric errors dis-cussed above, they give an idea how sensitive the localizationresult is to the geometry of each object of interest.
When using a standard torso model, the relative position ofthe lungs and the ventricles with respect to the body surface areoften incorrect. The distance from the sternum to the apex of theheart was defined from 18 sets of MR images to get an idea ofthe variability in the location of the heart between patients. Thedifference between the minimum and the maximum distancewas about 8 cm. This individual variability was simulated bydisplacing the lungs and the ventricles by15 mm ( – )and by 30 mm ( – ). Only the direction was studied asthe objects were assumed to be centered in the body. The objectswere displaced simultaneously because the overlapping of thesurfaces could not be avoided while moving them separately.
To deform the reference model including all objects in amore realistic way, a deformation grid was utilized.Different ways to change the positions of grid points weretested. A method where a grid point was moved along a linepassing through the point itself and the center of the grid waschosen. Two displacement magnitudes were used, 7.5 mmand 15.0 mm. The direction of the movement on the line wasrandomized. Two different models were produced with bothmagnitudes ( – ). When the grid points were displacedby 7.5 mm and by 15.0 mm, the average errors of the deformedmodel, compared to the reference model, were about 3 mm and6 mm, respectively. The modifications of models –can be considered to represent various nonlinear geometricalerrors in segmentation. When the model with a 3-mm errorwas superimposed on the MR images, the modifications weredifficult to recognize. Therefore, this kind of geometrical erroris easily generated in the BE model construction process.
B. Triangulation—Group B
Group B demonstrated the effect of different point sets andcorresponding triangulations on the MCG localization accuracy.
First, the density and the shape of triangles inwere variedlocally while keeping the total number of triangles constant: 1)The area of triangles was constant ( ). 2) The area of thesmallest triangle was smaller than in the reference model (
cm) ( ). 3) The area of the smallest triangle was largerthan in the reference model ( cm) ( ).
Second, two models were generated using a method based ontriangulating a set of contours. A contour is a nonoverlappingconnected point set on a plane. The contours were extracted
from the MR slices. In contour-based methods, the nodes inneighboring contours are connected by edges. The edges areadded sequentially in such a way that triangles are produced.In the simplest form, an edge , between the nodeof thecontour and the node of the contour , is first defined to be,e.g., the shortest edge between the nodes of the contours. There-after, the next edge is the shorter one from the edgesand . The contour-based methods are relatively easy toimplement because only the connectivity between the contours,not between the nodes inside a contour, has to be defined. How-ever, if the problem of branching exists, i.e., the connectivitybetween the contours is not aone-to-onemapping, the imple-mentation is more difficult. Another problem in contour-basedmethods is that sharp-angled triangles may appear, since the po-sitions of the nodes cannot be chosen arbitrarily. These problemsare automatically taken into account in the triangulation methodpresented in [16]. In contour-based methods, the first and the lastcontours have to be triangulated separately in order to produceclosed triangulations. The triangulations were closed by a point( ) and a set of points ( ).
Third, triangulations with 1000 and 400 triangles for B (700in the reference model) ( ), and 300 and 100 for theother objects (200 in the reference model) were produced (
, , , and). Models – were constructed in such a way
that only the triangulation of one object was different from thereference model. In the last model of group B ( ), the densesttriangulations were used for all objects.
C. Registration—Group C
In group C, the effect of errors in rigid registration were in-vestigated. The average RMS registration error using nine ex-ternal markers is about 6 mm in our MCG studies. The mag-nitude of different registration error sources has not been ana-lyzed, but we presume that the two most important sources are:1) the different orientation of the patient during MRI and MCGmeasurements and 2) the nonoptimal attachment of the externalmarkers in MRI and/or in MCG measurements. In addition, thepositions of the markers may change because of the elasticity ofthe skin. Case 1 is included in the models of group A, i.e., if thegeometry of the BE model does not correspond to the geometryof the patient during MCG recordings, the external markers arenot at corresponding positions. For example, the RMS errors ofthe markers in the models and comparedto the markers in the reference model were about 4 mm and 10mm, respectively. This error can be reduced by rigid registra-tion, but cannot be eliminated. In case 2, the geometry of theBE model is correct, but because of the incorrect positions ofthe markers, the BE model will be misaligned by rotation andtranslation.
In order to study the effects of rigid registration errors,the model was displaced by3 mm and by 6 mm fromits original position in each coordinate direction separately.Models – , – and – were translatedin the -, - and directions, respectively. Next, the referencemodel was misaligned using 3 and 6 rotations. Models
– , – , and – were rotated aroundthe , , and axes, respectively. It should be noted that the

1242 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 47, NO. 9, SEPTEMBER 2000
registration error of the reference model cannot be excludedwhen real patient data are used in the inverse calculations.However, this is not important in the present study because thelocalizations obtained with the reference model are defined asthe gold standard.
D. Combination—Group D
The directions of the changes in the MCG localization results,produced by different modifications, were not investigated inthis study. Only the magnitudes of the displacements were com-puted. Since the errors are not cumulative, at least as scalars,the effect of each different modification appearing simultane-ously in the model has to be investigated separately. There-fore, we built eight combinations with a different selection oferror sources. The magnitudes of the modifications were slightlyover-estimated to give a worst case scenario. Only modificationssimulating error sources, which cannot be avoided during themodeling procedure, were chosen. For example, modificationsfrom group B were not included in group D as the number andthe density of the triangles can be kept as constants. In addi-tion, the effects caused by using an X-ray-based model and astandard model were studied in group D because these modelsinclude several differences with respect to the reference models.Finally, the effect of inhomogeneities was investigated.
Models – were produced as follows: The effectsof misaligned shoulders ( ), concave MRI bed ( ) andbreathing ( ) were included in all models. Geometric errorswere generated using a deformation grid (– ), thusproducing the four models. Finally, each of these four modelswas displaced by 6 mm indirection ( ) and rotated around
and axes by 6 ( ).Models and were created as models – but
contained only the smaller deformations ( – ). In addi-tion, the 6 mm displacement was selected to be in thedirection( ), and smaller 3 rotations were used around theandaxes ( ). Models and were created withoutthe errors from – but contained the errors from and
, respectively. Both models were rotated by 3( )around the and axes.
Real X-ray images were not available for the patients studiedin this paper. Therefore, we created virtual X-ray images fromsegmented MR images, simulating real X-ray imaging condi-tions as explained in [30]. The surfaces of the body and lungsof model were generated using these virtual X-ray images.The ventricles of model were created by coarsely matchingventricles from a standard model inside the epicardium. Finally,the model was manually matched with the external markers usedin the MCG/MRI-registration.
To investigate the errors caused by using a standard torsomodel, model was constructed from a thorax library to rep-resent the average shape of the thorax [30]. Another standardtorso model by Horácek [18] was utilized in to check thevariability between the standard torso models. Models and
were coarsely matched with the external markers by trans-lation and rotation, as is done in our measurement procedure.To investigate the effect caused by the incorrect locations of thelungs and the ventricles inside , model was created bypositioning them correctly by translation.
The effect of inhomogeneities was studied by omitting theventricles of the reference model in . In model , thelungs were also left out, i.e., it contained only B from the refer-ence model. Model was also a homogeneous model but thebody surface was extracted from the Horácek standard thoraxmodel.
V. RESULTS AND DISCUSSION
The results obtained with simulated data describe only the ef-fect of a specific modification in the BE model because the sim-ulated data contained no noise. The results for measured MCGdata also include the effect of measurement noise and a true car-diac signal generator, which is not an ideal dipole. It is worthnoting that, in clinical practice, the localizations obtained withthe reference models are not “gold standard” but are affected bythe simplifications made in the volume conductor model and inthe calculation methods. However, the difference approach al-lowed us to specify the effect of each modification in millimeterscale.
The results from all four BE model groups, obtained usingsimulated and measured MCG data, are presented in Figs. 4–7.In these figures, the upper graph is generated from the results ob-tained with simulated data and the bottom graph from the resultsof measured data. The black bars display the average 3-D dis-tances from the calculated dipole locations to the correspondingGS localizations. On top of the average error bars, the standarddeviations (SDs) of the results are plotted with gray bars. Theresults for each of the three patients are shown separately for aparticular modification of the reference model. From simulateddata it was found that the dipole amplitudes have no effect onthe results, as no noise was added to the data. Thus, the resultsobtained with simulated data were independent of the sourcestrength and present the average change in localizations overthe different source locations (see Fig. 1). In this case, the stan-dard deviation describes the effect of different source positionson the localizations results. From measured data, the averageerrors and the standard deviations of the errors were calculatedfrom the ten localizations, computed at the onset of paced acti-vation Fig. 2(b). Therefore, the SDs of measured data only in-dicate variability in the localization results over the 5-ms timeinterval.
The results among the patients were relatively uniform whensimulated data were used in the calculations. Therefore, evenwith only three cases, a consistent analysis of the simulateddata can be given. With measured MCG data, the variabilityincreased slightly, but the results were still consistent amongpatients, and also with the results obtained with simulated data.The differences in results between simulated and measureddata are due to the different source locations and to the limitedsignal-to-noise ratio of the measured data. In the following, aqualitative description of the results is provided, giving an ideawhether a particular property of the BE model is importantwhen considering the MCG dipole localization accuracy.Possible differences in the results obtained with simulated andmeasured data are also addressed.
A. Geometric Accuracy—Group A
Fig. 4 presents the results of group A. The effect of mod-ifications arising from MR imaging was studied with models

PESOLAet al.: EFFECT OF GEOMETRIC AND TOPOLOGIC DIFFERENCES IN BEMs ON MCG LOCALIZATION ACCURACY 1243
Fig. 4. The average differences of all dipole locations to GS localizations within the first group of BE models (Group A). The average changes in the localizations,due to different modifications, are visualized with black bars. The standard deviations of the changes are shown with gray bars, on top of the averagedresults.
– . Including the arms in the BE model ( ) had a neg-ligible effect on localization results. The magnitude of changeslightly increased when the neck was removed from the model( ). Shortening the model by 5 cm in the pelvic region ( )increased the difference by over 10 mm. The correspondinglengthening ( ) did not have as large an effect. The verticalextent of B has also been studied, e.g., by Czapskiet al. [31]who used the finite element method (FEM) in the forward cal-culations. They suggested that a 3-cm vertical extension of thetorso above and below the heart is sufficient for obtaining a re-alistic spatial variability in the magnetic field data. However,our results suggest that in order to obtain accurate ECD local-izations, the model should be extended to the pelvic region, i.e.,at least 20–25 cm below the apex of the heart. Otherwise, thelocalization results will be affected by the artificial boundary atthe inferior part of the torso.
The misalignment of a patient inside the MRI tube, simulatedby raising and lowering the shoulders ( – ), had a negli-gible effect on localizations. However, the alignment errors maychange the positions of the external markers which affect the lo-calization by producing a registration error. The curved shape ofthe MRI bed ( ) changed the geometry of the patient com-pared to the MCG measurements. The effect of this error sourceon the localization accuracy was about 7 mm in the simulations,but exceeded 10 mm with the measured MCG data. Althoughthe curved shape was possibly over-estimated, the results sug-
gest that the shape of the bed should be taken into account inthe measurements. This can be accomplished, for example, bychanging the shape of the MCG bed to resemble the MRI bed.
The effect of breathing ( – ) was about 5 mm. If thephase of breathing is recorded during MCG measurements, thiserror source can be at least partly eliminated. Using averagedMCG data also removes the effect of breathing. In models
– the effect of breathing was studied by modifyingonly the body surface. However, the position of the heart mayvary by a few centimeters in the direction (head–feet) dueto breathing, as mentioned above. This phenomenon is partlyincluded in models – .
The scaling of B with global scaling factors ( – ) pro-duced differences of 6–10 mm. The localizations were espe-cially affected by using an under-scaled torso (). The ef-fect of scaling B has been investigated, e.g., by Tanet al. [11]who found comparable changes (around 10 mm) in localizationsusing scaling factors of 0.9 and 1.1. Scaling B in each coordi-nate direction separately ( – ) did not have as large ef-fects. Global scaling of LL and RL ( – ) resulted in abouta 6-mm change with simulated data, while the variability washigher with measured data. Scaling the lungs in each coordi-nate direction separately ( – ) and scaling the ventricles( – ) affected the localization results by less than 5 mm.
A 15 mm error in the position of the lungs and the ventri-cles ( – ) affected the localizations by about 10 mm, and

1244 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 47, NO. 9, SEPTEMBER 2000
Fig. 5. The average 3-D distances of dipole locations from the GS localizationswithin group B. Format as in Fig. 4.
a 30 mm error ( – ) by about 15 mm. Therefore, theirpositions need to be accurate in order to calculate reliable local-izations. If standard models are used in the calculations withoutpatient-specific knowledge of the position of the lungs and theventricles, errors in the positions cannot be avoided.
Deforming the reference model by moving the grid points by7.5 mm ( – ) changed the localizations by about 5 mm.With the larger displacement of 15 mm ( – ), the resultswere affected by about 10 mm, and as much as 15 mm withmeasured data. As mentioned earlier, the geometric errors pro-duced by modifications – were very small. Therefore,even if the BE model is built as accurately as possible from MRimages, a few millimeter inaccuracies in the localization resultsare difficult to avoid.
B. Triangulation—Group B
In group B, the effects of different point sets and corre-sponding triangulations were investigated. The average changesin the localization results due to the modifications in this groupare presented in Fig. 5. Changing the size of the triangles( – ) had a negligible effect in simulations. However,using constant size triangles ( ) showed a larger effectwith measured data. The two triangulations generated using amethod based on a triangulation of a set of contours (– )showed a maximum effect of 10 mm in simulations. This islikely caused by the sharp-angled triangles appearing in models
and and, therefore, they should be avoided in thetorso models. With measured data, however, the effect wassmaller.
Changing the number of triangles in B ( ) seemedto have a negligible effect on the localization results, as
Fig. 6. The average 3-D distances of dipole locations from the GS localizationswithin group C. Format as in Fig. 4.
did changing the number of triangles in RL, LV, and RV( – ). However, the effect of LL changes ( )was larger, as high as 10 mm with measured data. When thedensest triangulations were used for all objects (), theresults were changed less than 5 mm with simulated data butup to 10 mm with measured data.
The density of triangulation has been investigated previously.Ferguson and Stroink [20] found that, approximately, the errorin surface potential distributions is inversively proportional tothe number of triangle elements. As the number of triangleswas increased by a factor of four, the error of the surface poten-tial was also reduced approximately fourfold. They also inves-tigated the behavior of the error as a function of the mean edgelength of the elements and found that the error was quadraticwith respect to the mean edge length, i.e., proportional to thearea of the elements. Therefore, surfaces should be tessellatedusing equilateral triangles to minimize the mean edge length. Inour study, however, the effect of the number and the size of tri-angles was found to be, in general, much smaller than the effectof geometric errors, investigated in group A.
C. Registration—Group C
In group C, the effect of errors in rigid registration on thelocalization accuracy was investigated. The results of this groupare presented in Fig. 6. When all objects were displaced by3mm and by 6 mm in each direction separately ( – ),the localization results were affected by 2–7 mm. The rotationof the BE model by 3 and by 6 ( – ) changed the

PESOLAet al.: EFFECT OF GEOMETRIC AND TOPOLOGIC DIFFERENCES IN BEMs ON MCG LOCALIZATION ACCURACY 1245
Fig. 7. The average 3-D distances of dipole locations from the GS localizationswithin group D. Format as in Fig. 4, withy axis scaling changed.
localizations by 2–9 mm. The results obtained with simulatedand measured data were highly reproducible in this group ofBE models. Overall, no specific coordinate axis was found tobe sensitive to translation or rotation, and the localization resultswere not very sensitive to small registration errors.
However, it is worth noting that the effect of registration er-rors is bipartite. First, the misaligned BE model affects the MCGlocalization accuracy. Second, when the localization result istransformed back to the MRI coordinate system and visualizedon the images, the registration error is automatically added to theresult. In other words, if the model is misaligned by 5 mm, thelocalization result will be viewed by a cardiologist with a 5 mmoffset from the correct position, even if the misalignment wouldnot change the localization result in MCG coordinate system.The same problem occurs also with standard models. Geometricinaccuracies in such a model may change the localization resultonly by a few millimeters in the MCG coordinate system. How-ever, if the lungs and ventricles are, for example, 3 cm off fromtheir correct position, this error will be added to the localizationresult, when it is visualized in the model or on the MR images.
D. Combination—Group D
In group D, different combinations of the error sources werestudied. This group exhibited the largest changes in the local-
ization results, and therefore, the scale in Fig. 7 differs from thescale used in Figs. 4–6. In order not to increase the scale toomuch, the SDs of the last two models are clipped for the simu-lated data.
The magnitudes of the modifications in the first six models,especially in models – , were somewhat over-esti-mated to give an upper limit for the localization error. Withmodels – , the localizations were affected by 6–18mm, which shows the increased effect as several error sourceswere combined in the models. The changes in localizationswere decreased by about 5 mm with the smaller rotations inmodels – . The effects caused by models –were found to be less than 10 mm as the models did not containthe effects of misaligning the shoulders, concave MRI bed andbreathing.
With the model generated from X-ray images ( ), the lo-calization results changed by about 10 mm with simulated data,and slightly less with measured data. Therefore, X-ray-basedmodel construction could be used, if MR images are not avail-able, and still a sufficient localization accuracy could be ac-quired for most clinical purposes. In addition, the positions ofthe heart and the lungs are approximately correct, which is usu-ally not the case in standard models. Using standard models( – ), the changes in simulated localization results wereabout 15 mm and even over 20 mm in one case. With measureddata, the corresponding change varied between 3 mm and 15mm for the first two catheter positions, and was about 20 mm forthe third (deep) catheter position. The effect of using a standardmodel was surprisingly small compared to the changes pro-duced by the X-ray-based model. When model was com-pared to the reference model of each patient, by chance the lungsappeared to be almost in the correct position for the first twopatients. When the lungs and the ventricles were correctly posi-tioned in model and scaling was used in coarse matching( ), the changes in the localization results were slightly de-creased, especially with measured data. However, the results forthe third patient with model showed the complexity of theinverse problem. The geometric accuracy of model wasworse than in model , but the localizations calculated withmodel were found to be more accurate than with model
in the case with simulated data.Models – showed the effect of removing the inho-
mogeneities from the torso model. If only the ventricles wereomitted ( ), the average change in the simulated data wasfound to be 5–17 mm. From the results obtained with the mea-sured data, it can be seen how sensitive this result was for the lo-cation of the source. The two RV cases with superficial sourceswere only affected by 4 mm and 12 mm, whereas the CS casewas affected by over 30 mm. When the lungs were also removedfrom the model ( ), the average changes in the simulated lo-calizations increased at times to over 60 mm. The strong effectcaused by the inhomogeneities of the BE model in the case ofdeep sources has also been found previously, e.g., by Forsmanet al. [10] who reported that removing the ventricles altered thelocalization results of deep sources by around 10 mm, and whenalso the lungs were removed, the changes increased to severalcentimeters. However, in the present study it was found that thetwo RV cases were only affected by around 10 mm in the mea-

1246 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 47, NO. 9, SEPTEMBER 2000
sured data. A comparable result with superficial sources in caseof measured data has also been found previously [6], where re-moving the lungs from individual BE models altered the local-izations only by a few millimeters. Therefore, for deep sourcesthe effect of inhomogeneities is too significant to be neglected,but superficial sources can be localized within a few millimeterseven with homogeneous BE models.
When a homogeneous, standard torso model () was used,the results obtained with simulated data were comparable tothose of model , e.g., the localizations were affected by sev-eral centimeters. With measured data, however, the localizationresults with were more affected than with in the twoRV cases, by about 20 mm.
VI. CONCLUSION
Error sources in the modeling process are numerous, andtheir relative contributions are difficult to determine exactly.Moreover, the bioelectromagnetic inverse problem is typicallya highly nonlinear process. As the changes in the localizations,resulting from modifications in the BE models, are not cumula-tive, the effect of combining different modifications cannot beestimated from separate results. Even though the formulation ofthe problem is difficult, we wanted to establish some guidelinesfor BE model construction. Three patients were selected forthe study. The reference model of each patient was modifiedin a controlled way, thus producing around 100 modified BEmodels for each patient. The effect of the modifications in thetorso model was monitored by calculating dipole localizationsfrom simulated and measured MCG data. The localizationsobtained with the modified models were compared with thegold standard results, obtained with the reference models.
The results showed that the magnitudes of the changes inthe dipole localizations, calculated from simulated and mea-sured data, were in quantitative agreement and, therefore, sim-ilar results were produced with the simulated 99-channel andwith the 67-channel sensor configurations. Qualitative relationsof the model properties and the localization accuracy could befound from the results. Due to the large number of modifica-tions studied, a short conclusion about the results is difficult topresent. However, a few general guidelines can be drawn: 1) thestandard inhomogeneities (lungs and ventricular blood masses)are required in the localization of deep sources, 2) the positionsof the lungs and the ventricles should be known and therefore,all possible information, e.g., X-ray images, about the anatomyof the patient should be used, 3) the torso model should extendto shoulders and to pelvic region, 4) the positioning of the pa-tient during the MCG recordings should be as similar as pos-sible to the positioning during MRI, and 5) sharp-angled trian-gles should be avoided in the torso models. However, any directgeneralization of the results of the present study on other sourcemodels, such as the ventricular activation time map [32], cannotbe made.
The present study showed the sensitivity and the nonlineardependence of MCG dipole localizations on the BE model prop-erties. Slight changes in the BE models could result in severalmillimeters changes in the localization results. For example,
the small random point modifications in models andcaused a 5 mm change in the localization results. On the otherhand, relatively large changes in the BE models, for exampleswitching to a standard model without any information aboutthe anatomy of the patient, did not alter some localization re-sults by more than a few millimeters. In this case, certain errorsources most likely cancelled the effect of others, and thus re-sulted in smaller alterations in the localizations than what couldbe expected from the separate results.
REFERENCES
[1] M. Hämäläinen and J. Nenonen, “Magnetic source imaging,” inEncy-clopedia of Electrical Engineering, J. Webster, Ed. New York: Wiley,1999, vol. 12, pp. 133–148.
[2] G. Stroink, W. Moshage, and S. Achenbach, “Cardiomagnetism,” inMagnetism in Medicine, W. Andrä and H. Nowak, Eds. Berlin, Ger-many: Wiley VCH, 1998, pp. 136–189.
[3] M. Mäkijärvi, J. Montonen, and J. Nenonen, “Clinical application ofmagnetocardiographic mapping,” in Cardiac Mapping, M. Shenasa, M.Borgreffe, and G. Breithardt, Eds. Mt. Kisco, NY: Futura, to be pub-lished.
[4] J. Nenonen, M. Mäkijärvi, L. Toivonen, K. Forsman, M. Leiniö, J. Mon-tonen, A. Järvinen, P. Keto, P. Hekali, T. Katila, and P. Siltanen, “Non-in-vasive magnetocardiographic localization of ventricular pre-excitationin the Wolff–Parkinson–White syndrome using a realistic torso model,”Eur. Heart J., vol. 14, pp. 168–174, 1993.
[5] R. Fenici, J. Nenonen, K. Pesola, P. Korhonen, J. lötjönen, M. Mäkijärvi,L. Toivonen, V. P. Poutanen, P. Keto, and T. Katila, “Non-fluoroscopiclocalization of an amagnetic stimulation catheter by multichannel mag-netocardiography,”PACE, vol. 22, pp. 1210–1220, 1999.
[6] K. Pesola, J. Nenonen, R. Fenici, J. Lötjönen, M. Mäkijärvi, P. Fenici, P.Korhonen, K. Lauerma, M. Valkonen, L. Toivonen, and T. Katila, “Bio-electromagnetic localization of a pacing catheter in the heart,”Phys.Med. Biol., vol. 44, pp. 2565–2578, 1999.
[7] B. M. Horácek, C. Purcell, R. Lamothe, R. Merritt, C. Kafer, S.Periyalwar, S. Dey, L. J. Leon, and G. Stroink G, “The effect of torsogeometry on magnetocardiographic isofield maps,”Phys. Med. Biol.,vol. 32, pp. 121–124, 1987.
[8] C. Purcell, G. Stroink, and B. M. Horácek, “Effect of torso boundaries onelectric potential and magnetic field of a dipole,”IEEE Trans. Biomed.Eng., vol. 35, pp. 671–678, Sept. 1988.
[9] R. Hren, G. Stroink, and B. M. Horácek, “Spatial resolution of body sur-face potential maps and magnetic field maps: A simulation study appliedto the identification of ventricular pre-excitation sites,”Med. Biol. Eng.Comput., vol. 36, pp. 145–157, 1998.
[10] K. Forsman, J. Nenonen, C. Purcell, and G. Stroinket al., “Biomagneticinverse solution with a realistic torso model,” inAdvances in Biomag-netism ’91: Clinical Aspects, M. Hoke et al., Eds. Amsterdam, TheNetherlands: Elsevier, 1992, pp. 819–823.
[11] G. Tan, F. Brauer, G. Stroink, and C. Purcell, “The effect of measurementconditions on MCG inverse solutions,”IEEE Trans. Biomed. Eng., vol.39, pp. 921–927, Sept. 1992.
[12] H. Bruder, B. Scholtz, and K. Abraham-Fuchs, “The influence of in-homogeneous volume conductor models on the ECG and MCG,”Phys.Med. Biol., vol. 39, pp. 1949–1968, 1994.
[13] R. Hren, X. Zhang, and G. Stroink, “Comparison between electrocardio-graphic and magnetocardiographic inverse solutions using the boundaryelement method,”Med. Biol. Eng. Comput., vol. 34, pp. 110–114, 1996.
[14] R. Hren, G. Stroink, and B. M. Horácek, “Accuracy of single-dipoleinverse solution when localizing ventricular pre-excitation sites: Simu-lation study,”Med. Biol. Eng. Comput., vol. 36, pp. 323–329, 1998.
[15] J. Lötjönen, P.-J. Reissman, I. E. Magnin, and T. Katila, “Model ex-traction from magnetic resonance volume data using the deformablepyramid,”Med. Image Anal., vol. 3, pp. 387–406, 1999.
[16] J. Lötjönen, P.-J. Reissman, I. E. Magnin, J. Nenonen, and T. Katila,“A triangulation method of an arbitrary point set for biomagnetic prob-lems,” IEEE Trans. Magn., vol. 34, pp. 2228–2233, Apr. 1998.
[17] D. Geselowitz, “On the magnetic field generated outside an inhomo-geneous volume conductor by internal current sources,”IEEE Trans.Magn., vol. 6, pp. 346–347, 1970.
[18] B. M. Horácek, “Digital model for studies in magnetocardiography,”IEEE Trans. Magn., vol. MAG-9, pp. 440–444, 1973.

PESOLAet al.: EFFECT OF GEOMETRIC AND TOPOLOGIC DIFFERENCES IN BEMs ON MCG LOCALIZATION ACCURACY 1247
[19] J. de Munck, “A linear discretization of the volume conductor boundaryintegral equation using analytically integrated elements,”IEEE Trans.Biomed. Eng., vol. 39, pp. 986–990, Sept. 1992.
[20] S. Ferguson and G. Stroink, “Factors affecting the accuracy of theboundary element method in the forward problem—I: Calculatingsurface potentials,”IEEE Trans. Biomed. Eng., vol. 44, pp. 1139–1155,Nov. 1997.
[21] S. Ferguson, X. Zhang, and G. Stroink, “A complete linear discretizationfor calculating the magnetic field using the boundary element method,”IEEE Trans. Biomed. Eng., vol. 41, pp. 455–460, May 1994.
[22] A. van Oosterom and J. Strackee, “The solid angle of a plane triangle,”IEEE Trans. Biomed. Eng., vol. BME-30, pp. 125–126, Feb. 1983.
[23] M. Lynn and W. Timlake, “The use of multiple deflations in the nu-merical solution of singular systems of equations, with applications topotential theory,”SIAM J. Numer. Anal., vol. 5, pp. 303–322, 1968.
[24] J. Nenonen, C. Purcell, B. M. Horácek, G. Stroink, and T. Katila, “Mag-netocardiographic functional localization using a current dipole in a real-istic torso,”IEEE Trans. Biomed. Eng., vol. 38, pp. 658–664, July 1991.
[25] R. Throne and L. Olson, “The effects of errors in assumed conductivitiesand geometry on numerical solutions to the inverse problem of electro-cardiography,”IEEE Trans. Biomed. Eng., vol. 42, pp. 1192–1200, Dec.1995.
[26] P. Laine, M. Hämäläinen, and A. Ahonenet al., “Combination of mag-netometers and planar gradiometers in an MEG system,” inRecent Ad-vances in Biomagnetism: Proceedings of the 11th International Confer-ence on Biomagnetism, T. Yoshimotoet al., Eds. Sendai, Japan: To-hoku Univ. Press, 1999, pp. 47–50.
[27] J. Montonen, A. Ahonen, M. Hämäläinen, R. Ilmoniemi, P. Laine,J. Nenonen, M. Paavola, K. Simelius, J. Simola, and T. Katilaetal., “Magnetocardiographic functional imaging studies in BioMagLaboratory,” in Advances in Biomagnetism Research: Biomag96, C.Aine et al., Eds. New York: Springer Verlag, to be published.
[28] R. Fenici, P. Fenici, and J. Van Bosheide, “Amagnetic catheter for bio-magnetically guided endocardial mapping and ablation of cardiac ar-rhythmias,” inMicro System Technologies, H. Reichl and A. Heuberger,Eds. Berlin, Germany: VDE-Verlag GmbH, 1996, pp. 711–716.
[29] D. Marquardt, “An algorithm for least-squares estimation of nonlinearparameters,”J. Soc. Ind. Applicat. Math., vol. 11, pp. 431–441, 1963.
[30] J. Lötjönen, I. E. Magnin, L. Reinhardt, J. Nenonen, and T. Katila, “Re-construction of 3-D geometry using 2-D profiles and a geometric priormodel,” IEEE Trans. Med. Imag., vol. 18, pp. 992–1002, Oct. 1999.
[31] P. Czapski, C. Ramon, L. L. Huntsman, G. H. Bardy, and Y. Kim, “On thecontribution of volume currents to the total magnetic field resulting fromthe heart excitation process: A simulation study,”IEEE Trans. Biomed.Eng., vol. 43, pp. 95–104, Jan. 1996.
[32] G. Huiskamp and A. van Oosterom, “The depolarization sequence of thehuman heart surface computed from measured body surface potentials,”IEEE Trans. Biomed. Eng., vol. 35, pp. 1047–1058, Dec. 1988.
Katja Pesola received the M.Sc. (Tech.) degree inengineering physics and mathematics from HelsinkiUniversity of Technology, Espoo, Finland, in 1996.She is presently a Ph.D. Candidate at the Laboratoryof Biomedical Engineering of the same university.
Her research interests are the bioelectromagneticinverse problem and its applications in magneto- andelectrocardiography.
Jyrki Lötjönen (S’96–A’00) received the M.Sc.(Tech.) degree from Helsinki University of Tech-nology, Espoo, Finland, in 1994. He is workingtoward the Ph.D. degree at at INSA of Lyon, France.
His main interest concerns medical imageprocessing.
Jukka Nenonen was born in Joensuu, Finland in1961. He received the M.Sc. (Tech.) degree andthe D.Sc. (Tech.) degree in technical physics fromHelsinki University of Technology, Espoo, Finland,in 1988 and 1992, respectively.
Currently, he is working as a Senior Researcherat the Laboratory of Biomedical Engineeringof Helsinki University of Technology. His mainresearch interests include bioelectricity and biomag-netism, cardiac modeling, and inverse problem.
Isabelle E. Magnin (M’85) received the ECAM engineering degree in 1977and the “Doctor at d’état ès Sciences” in 1987 from INSA-Lyon Scientific andTechnical University, Lyon, France.
Since 1982, she has been a Researcher with the National Institute for Healthand Medical Research (INSERM) at CREATIS, UMR CNRS 5515. She is Headof the Dynamic Imaging Group at CREATIS. She is involved in more than 90publications. Her main interest concerns modeling, medical image processing,dynamic imaging, and three-dimensional reconstruction.
Kirsi Lauerma received the M.D. degree in 1988,and Ph.D. degree in 1999 from the Medical Schoolof Helsinki University, Espoo, Finland.
She is currently a last year resident and is workingas an Assistant Professor in the Department of Radi-ology, in Helsinki University Central Hospital. Herresearch interests are the applications of magneticresonance imagining to the assessment of ischemicheart disease and other myocardial diseases.
Riccardo Fenicireceived the M.D. degree in general medicine and surgery fromCatholic University of Sacred Heart (CUSH), Rome, Italy, in 1969.
He has been Professor of Cardiology at CUSH, since 1993 and is the headof the bioelectromagnetism, signal and image processing. He is the Head of theBiomagnetism and Clinical Physiology Center of CUSH. His major interests arestudies of clinical electrophysiology, cardiac arrhythmias, bioelectromagnetism,and signal and image processing.
Dr. Fenici is a Specialist in Cardiology since 1972 and in Vascular Surgerysince 1979.
Toivo Katila received the M.Sc. (Tech.) and D.Sc.(Tech.) degrees in engineering physics from HelsinkiUniversity of Technology, Espoo, Finland, in 1966and 1970, respectively.
He has been an Associate Professor of TechnicalPhysics at Helsinki University of Technology since1973 and Professor since 1990. He is the Headof the Laboratory of Biomedical Engineering atthe same university. His major interests of studyare bioelectricity and biomagnetism, biomedicalsignal and image processing, and spectroscopic
measurements.