Meditation Traditions in Fifth-Century Northern China (Buddhabhadra)
Upload
independentCategory
view
0download
0
Research report
The effect of body–mind relaxation meditation induction on majordepressive disorder: A resting-state fMRI study
Fangfang Chen a,b,1, Xueyu Lv c,1, Jiliang Fang g, Shan Yu d,e, Jing Sui d,e, Lingzhong Fan d,e,Tao Li c, Yang Hong g, XiaoLing Wang g, Weidong Wang c,nn, Tianzi Jiang d,e,f,n
a School of Mathematics and Computational Science, Sun Yat-Sen University of China, Guangzhou 510275, Chinab School of Mathematics and Computational Science, Shenzhen University of China, Shenzhen 518060, Chinac Psychology Department of Guang'anMen Hospital, China Academy of Chinese Medical Sciences, Beijing 100053, Chinad Brainnetome Center, Institute of Automation, Chinese Academy of Sciences, Beijing 100190, Chinae National Laboratory of Pattern Recognition, Institute of Automation, Chinese Academy of Sciences, Beijing 100190, Chinaf Queensland Brain Institute, The University of Queensland, Brisbane, QLD 4072, Australiag Radiology Department of Guang'anMen Hospital, China Academy of Chinese Medical Sciences, Beijing 100053, China
a r t i c l e i n f o
Article history:Received 8 December 2014Received in revised form25 March 2015Accepted 17 April 2015Available online 28 April 2015
Keywords:Major depressive disorderBody–mind relaxation meditationfMRICognitive reappraisalMedial frontal cortexOrbitofrontal cortex
a b s t r a c t
Background: Meditation has been increasingly evaluated as an important complementary therapeutictool for the treatment of depression. The present study employed resting-state functional magneticresonance imaging (rs-fMRI) to examine the effect of body–mind relaxation meditation induction(BMRMI) on the brain activity of depressed patients and to investigate possible mechanisms of action forthis complex intervention.Method: 21 major depressive disorder patients (MDDs) and 24 age and gender-matched healthy controls(HCs) received rs-fMRI scans at baseline and after listening to a selection of audio designed to inducebody–mind relaxation meditation. The rs-fMRI data were analyzed using Matlab toolbox to obtain theamplitude of low-frequency fluctuations (ALFF) of the BOLD signal for the whole brain. A mixed-designrepeated measures analysis of variance (ANOVA) was performed on the whole brain to find which brainregions were affected by the BMRMI. An additional functional connectivity analysis was used to identifyany atypical connection patterns after the BMRMI.Results: After the BMRMI experience, both the MDDs and HCs showed decreased ALFF values in thebilateral frontal pole (BA10). Additionally, increased functional connectivity from the right dorsal medialprefrontal cortex (dmPFC) to the left dorsal lateral prefrontal cortex (dlPFC) and the left lateralorbitofrontal cortex (OFC) was identified only in the MDDs after the BMRMI.Limitation: In order to exclude the impact of other events on the participants' brain activity, the HamiltonRating Scales for Depression (HDRS) was not measured after the body–mind relaxation induction.Conclusion: Our findings support the hypothesis that body–mind relaxation meditation induction mayregulate the activities of the prefrontal cortex and thus may have the potential to help patients constructreappraisal strategies that can modulate the brain activity in multiple emotion-processing systems.
& 2015 Elsevier B.V. All rights reserved.
1. Introduction
Major depressive disorder (MDD) is a serious clinical mood disordercharacterized by mood dysregulation and cognitive impairment.
According to the World Health Organization, MDD will be thesecond-leading cause of disability in the world by the year 2020,following heart disease (Sliz and Hayley, 2012). Despite this highprevalence, the pathogenesis of MDD remains unclear and the diagnosisof depression is often delayed or missed, leading to poor outcomes,including high relapse rates, suicide, and diminished psychosocialfunctioning.
The most frequently used treatment for MDD is antidepressantmedication. In spite of the development of new and effectivemedications for depression, as many as 30–50% of patients do notrespond to medication treatment (Baghai et al., 2006). Furthermore,medications may induce unwanted side effects that can impair
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jad
Journal of Affective Disorders
http://dx.doi.org/10.1016/j.jad.2015.04.0300165-0327/& 2015 Elsevier B.V. All rights reserved.
n Corresponding author at: Brainnetome Center and National Laboratory ofPattern Recognition, Institute of Automation, Chinese Academy of Sciences, Beijing100190, China.
nn Corresponding author.E-mail addresses: [email protected] (W. Wang),
[email protected] (T. Jiang).1 Co-first authors.
Journal of Affective Disorders 183 (2015) 75–82

patients' quality of life (Kupfer et al., 2012). As a result, they may notbe suitable for patients with mild to moderate depressive symptoms,which represent the majority of clinical cases.
In contrast, new non-pharmacological treatments strategies,including electroconvulsive therapy (ECT), cognitive behavioral ther-apy (CBT), repetitive transcranial magnetic stimulation (rTMS), andso on, are currently under development. Their clinical efficacy hasbeen confirmed at least in subgroups of depression, although moreinsight into the main mechanisms underlying their antidepressantefficacy is still necessary. Furthermore, depression is a highlyrecurrent disorder that causes great suffering for patients and theirfamilies. Even among patients who show improvement with short-term antidepressant use, there is a significant risk for relapse withinone year after treatment termination (Hsu and Lai, 2004).
Meditation, an easy, low cost practice that seems to have theability to regulate emotion, has been used in the treatment ofdepression (Goyal et al., 2014; Little et al., 2009). Meditation hasbeen shown to produce benefits for anxiety, depression, and othernegative emotional symptoms (Jain et al., 2015; Simkin and Black,2014). Review studies have pointed out that adding mindfulnessmeditation to conventional CBT offers a promising, cost-efficientpsychological approach for preventing relapse/recurrence in recov-ered recurrently depressed patients (Beshai et al., 2011; Shelton,2004). Prior exposure to mindfulness-based cognitive therapy(MBCT) appears to be about as efficacious as keeping patients onmedications; in fact, most of the patients exposed to MBCT in onestudy were able to discontinue medications (Kuyken et al., 2008). Aprevious review study indicated that alterations in attention,memory specificity, self-discrepancy, activity-pleasantness apprai-sal, emotional reactivity, and momentary positive and negativeaffect may play a role in how MBCT exerts clinical effects in MDDtreatment (van der Velden et al., 2015).
A version of mindfulness meditation, body–mind relaxationmeditation, which originates from ancient Eastern traditions, hasbeen showed to be an important complementary therapy for boththe treatment and prevention of many stress-related conditions(Tang, 2011). This type of meditation does not stress controllingthoughts, but instead encourages a state of restful alertness thatallows for a high degree of awareness of the body, of breathing, andof external instructions. The inducing passage helps trainees to relax,adjust their breathing, and use mental imagery to achieve a balancedstate of relaxation while focusing attention. This approach is suitablefor novices and MDD patients, who might have difficulty sponta-neously entering into and remaining in a state of mindfulness.
Despite the various benefits of body–mind relaxation meditationinduction for depression, its effects on brain activity have not beenadequately established. In the current study, we used a brief, guidedbody–mind relaxation intervention, based on observations that shortmeditation interventions have significant effects on mood (Zeidanet al., 2010b), cognition (Zeidan et al., 2010a), and self-regulation (Tanget al., 2007). Our hypothesis was that after a single brief session of guidedmeditation, participants would show functional changes in the brain. Wecollected rs-fMRI data before and after a body–mind relaxation medita-tion induction session to identify the affected brain regions.
The amplitude of low-frequency fluctuations (ALFF) of the BOLDsignal, an index that measures the total power of a given time coursewithin a specific frequency range (0.01–0.08 Hz) (Zang et al., 2007),was employed to compare the resting-state brain activity before andafter body–mind relaxation meditation induction. Due to its hightemporal stability (Kublbock et al., 2014) and test–retest reliability(Zuo and Xing, 2014), ALFF has been suggested as a biologicallymeaningful index for assessing the altered neural activity associatedwith behavioral performance or psychiatric disorders (Hoptmanet al., 2010; Yan et al., 2009; Yang et al., 2007).
Functional connectivity (FC) is another widely-used fMRI dataanalysis method, which measures the temporal correlation between
different brain regions. Although either standard seed-ROI-basedfunctional connectivity or whole brain functional connectivity canprovide more holistic information about a set of brain regions withina network, they do not reveal the BOLD signal change of the regionalspontaneous activity. Moreover, altered connectivity between brainregions cannot precisely reveal which brain region has alteredspontaneous activity (Jiang et al., 2011). In contrast, ALFF analysesare only concerned with the activity level of each area of the brainwithout taking into account the activity in other brain areas.
The purpose of the present study was to assess whethersubsequent rs-fMRI scanning could detect changes in the brainactivity of the participants after experiencing BMRMI. We choseALFF combined with functional connectivity as our analysismethod. In light of the previous studies mentioned above, wehypothesized that the BMRMI might affect people with MDD andhealthy controls (HC) differently. The general method used in theBMRMI is briefly described in the next section.
2. Materials and methods
2.1. Participants
The study was approved by the Institute of Medicine ReviewBoard, Guang'anmen Hospital, China Academy of Chinese MedicalSciences. Patients meeting the following criteria were recruited:SCID-IV diagnostic criteria for depression; Hamilton Rating Scalesfor Depression (HDRS) score420; age range from 18 to 50 yearsold; medication naive or withdrawn for 2 weeks before the rs-fMRI scanning; no other drug therapy; no other psychiatric ill-nesses or severe physical illness; disease course longer than2 weeks; right-handed; no history of qigong practice, yogapractice, or relaxation training; and no contradiction to undergoan MRI scan based on an MRI screening questionnaire. The criteriafor the healthy controls were as follows: no psychiatric disordersor severe physical disorders; right-handed; no history of qigongpractice, yoga practice, or relaxation training.
Two patients with MDD were excluded from the analyses dueto excessive head motion during the image acquisition. The patientgroup and the control group did not differ significantly in age (twotailed two sample t test: p¼0.74) or gender (Pearson chi-squaret test: p¼0.81) (Table 1).
The depressed patients and the healthy controls were scannedfor rs-fMRI data before and after body–mind relaxation meditation(BMRM) induction. During the BMRM induction, the participantslay still in a bed. The BMRM induction adopted in our experimentcontained background music and a human voice reading relaxing-inducing passages, which were read by a woman broadcaster instandard Chinese Mandarin. A type of soft and slow Chinese lutemusic called Saishangqu was the background music. The inductionpassage included two sessions: a whole body relaxation inductionwith words such as “Relax your head, …, relax your neck, …”, anda mind relaxation session with words such as “Now calm yourmind, …, remove all your worries, … ”. Each subject listened to the
Table 1Group demographics and clinical measures.
Characteristics MDD patients Healthy controls p Value
Age, year (mean7SD) 36.0579.18 35.2177.92 0.74 a
HAMD (mean7SD) 30.4875.86 2.0072.02 o0.001a
Gender(female/male) 16/5 19/5 0.811b
Abbreviations: SD: standard deviation; HAMD: Hamilton Depression Rating Scale.a Indicates p values for two-sample t-test.b Indicates p values for Pearson chi-square t-test.
F. Chen et al. / Journal of Affective Disorders 183 (2015) 75–8276

BMRM induction for 15 min with the goal of becoming completelyrelaxed.
2.2. rs-fMRI data acquisition
Functional images were acquired on a 1.5T GE Signal scannerusing a standard GE whole-head coil. A custom-built head holderwas used to prevent head movement. The echo planar imaging(EPI) sequence was acquired in 41 axial slices with TR¼2500 ms,TE¼30 ms, flip angle¼901, field of view¼24 cm; 3 mm thicknessand 0.5 mm gap; the sequence duration was 370 s for each subject,150 time points were acquired, and the voxel dimensions were64�64�20. All the subjects were asked to close their eyes,remain awake, not think about anything specific, and not movewhile scanning. All the subjects were scanned twice: before andafter the BMRM induction session.
2.3. Functional image analysis
We utilized two rs-fMRI metrics: the amplitude of low-frequency fluctuation (ALFF) and functional connectivity (FC), toassess the effects of BMRMI experience on brain activity. Incontrast to FC, ALFF requires no a priori definition of ROIs andcan provide information about the local activity of separate brainregions. We first performed a voxel-based ANOVA analysis on thefour groups of mALFF maps, that is, the MDD patients' mALFFmaps before the BMRMI (denoted as DP_01), the MDD patients'mALFF maps after the BMRMI (denoted as DP_02), the healthycontrols' mALFF maps before the BMRMI (denoted as HC_01), andthe healthy controls' mALFF maps after the BMRMI (denoted asHC_02), to identify the ROIs with a main effect of diagnosis, a maineffect of BMRMI, and an interaction effect of diagnosis�BMRMI.For the ROIs showing a significant interaction effect, furtherfunctional connectivity analysis was performed to find differencesbetween the effects of the BMRMI on the MDD patients and HCs.This process is described in detail below.
2.3.1. Data preprocessingThe image data were preprocessed using SPM8 (http://www.fil.
ion.ucl.ac.uk/spm) and MATLAB R2009a (The Mathworks, Natick,MA). The first 10 volumes from each participant were discarded. Thefunctional images underwent slice-timing correction and realign-ment for head motion correction. Data from participants whose headmotion during scanning exceeded 2 mm or rotation exceeded 21were excluded. The motion-corrected functional volumes were thenspatially normalized to a standard EPI template and resampled to avoxel size of 3� 3� 3 mm3. Subsequently, the functional imageswere spatially smoothed with a Gaussian kernel of 6 mm full-widthat half maximum. Finally, the linear trend of the time series wasremoved, and band-pass filtering (0.01–0.08 Hz) was performed toreduce the effects of low-frequency drift and high-frequency noises,such as from respiratory and cardiac rhythms.
2.3.2. Individual ALFF map calculationAfter band-pass filtering and linear trend removal, the time series
were transformed to the frequency domain using a fast Fouriertransform (FFT) and the power spectrum was obtained. Since thepower of a given frequency is proportional to the square of theamplitude of this frequency component in the original time series,the square root of the power spectrum obtained by FFT was takenand was then averaged across 0.01–0.08 Hz at each voxel.
For the purpose of standardization, the ALFF for each voxel wasdivided by the mean ALFF value within the same brain mask. MeanALFF (mALFF) maps were calculated for each subject and then fourgroups of data were created: the MDD patients' mALFF maps before
the BMRMI (denoted as DP_01), the MDD patients' mALFF maps afterthe BMRMI (denoted as DP_02), the healthy controls' mALFF mapsbefore the BMRMI (denoted as HC_01) and the healthy controls'mALFF maps after the BMRMI (denoted as HC_02). All furtherstatistical analyses were performed based on these four groups of data.
2.3.3. Seed-ROI functional connectivityRegions showing a significant interaction effect were defined as
seed-ROIs. After normalization and smoothing, the time series for thewhole brain were further preprocessed as follows: first, six headmotion parameters, the averaged signals from the CSF and whitematter, and the global brain signal were regressed. Second, to reducethe effects of low-frequency drifts and high frequency noise, the timeseries were band filtered (0.01–0.08 Hz) and linearly detrended. Theregional mean time series were obtained by averaging the fMRI timeseries over all the voxels in the seed region. Then, functionalconnectivity maps were produced by computing the Pearson corre-lation coefficients between each averaged seed-ROI signal and thetime series from all other voxels within the brain mask. In addition,all correlation coefficients were converted to z-scores by applying theFisher r-to-z transformation.
2.3.4. Statistical analysisA two way mixed design repeated ANOVA with a between-
subjects factor of diagnosis and a within-subjects factor of BMRMIwas performed using SPM software to identify the ROIs with a maineffect of diagnosis, a main effect of BMRMI, and an interaction effectof diagnosis�BMRMI. Significance was first assessed at the wholebrain level. The resulting maps were formed using a threshold ofpo0.001 at the voxel level and po0.05 at the cluster level (minimalcluster volume of 13 contiguous voxels). The significance thresholdswere determined by Monte Carlo simulations and corrected formultiple comparisons using the Alphasim tool in AFNI (http://afni.nih.gov/afni/docpdf/AlphaSim.pdf) within the whole brain mask(size: 61� 73� 61 mm3). A post-hoc analysis was performed tofind the average mALFF value for each ROI, the resulting averagemALFF values for the four groups of data (DP_01, DP_02, HC_01,HC_02) are displayed in Figs. 1–3.
To further explore how BMRMI can affect functional connectivitypatterns, the brain region showing significant interaction effect wasidentified as a seed-ROI, and whole brain functional connectivitymaps of this seed-ROI were calculated. Further paired t-tests wereperformed separately on the MDD and HC groups to compare theirconnectivity maps before and after the BMRM induction. Thesignificance level was set at po0:05 (corrected for AlphaSimcorrection, with a combined individual voxel po0.001 and a clustersize Z13 voxels).
3. Results
3.1. ANOVA analysis
A whole brain ANOVA analysis on the mALFF revealed a significantmain effect of diagnosis (F1;86 ¼ 11:6096; po :001; cluster sizeZ13)in three structures, see Table 2 and Fig. 1. The MDD patients exhibitedhigher mALFF values in the right insular (BA13) cortex extending to theright inferior frontal cortex as well as lower mALFF values in the rightprecuneus (BA7) and the right supplementary motor area.
The bilateral frontal polar cortex (BA10) showed a main effect ofBMRMI (Table 2, Fig. 1). Both sides showed decreased mALFF valuesafter the BMRM induction in both the MDD and HC groups.
The interaction between diagnosis and BMRMI showed a singlecluster in the right dorsal medial frontal cortex (BA8/9). The BMRMIdecreased the mALFF value for this structure in the MDD patients
F. Chen et al. / Journal of Affective Disorders 183 (2015) 75–82 77

while increasing the mALFF value of the same region for the HCs(Table 2, Fig. 3).3.2. Seed-based resting-state functional connectivity
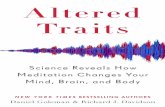
After the BMRM induction, the MDD patients demonstratedsignificantly increased functional connectivity (FC) between the rightdorsal medial prefrontal cortex (dmPFC) and the left dorsal lateralprefrontal cortex (dlPFC). The BMRMI experience also seemed to alterthe functional connectivity of MDDs from negative to positivebetween the right dorsal medial prefrontal cortex (dmPFC) and theleft lateral orbitofrontal cortex (OFC). This alteration was detected inboth the MDD patients and the HCs, albeit much more significantlyin the MDDs (Table 3 and Fig. 4). The two significantly increased FCsobserved in the MDDs were interhemispheric and were located inthe frontal lobes.
4. Discussion
In this paper, we investigated the effects of BMRMI on brainactivity in MDD patients and HCs. We found (1) an effect of BMRMIthat was similar between the MDD patients and the HCs, (2) aspecific effect of BMRMI on the MDD patients, and (3) group
Fig. 1. Main effect of diagnosis: MDD patients exhibited higher mALFF values in the right dorsal anterior insula/BA13 extending to the right inferior frontal gyrus, and lowermALFF values in the right precuneus/BA7 and right supplementary motor area. L¼ left, R¼right. n0 :01rpo0:05, nn0 :001rpo0:01, nnnpo0:001.
Fig. 2. Main effect of BMRMI: BMRMI had the same effect on the healthy controls andMDD patients in the bilateral superior frontal cortex (BA10/BA11). Decreased mALFFvalues were observed after the BMRMI. Abbreviations: BMRMI: body–mind relaxationmeditation induction; L¼ left, R¼right. *0.01rpo0.05, **0.001rpo0.01, ***po0.001.
Fig. 3. Interaction effect of diagnosis�BMRMI: BMRMI had a different effect on thehealthy controls and the MDD patients in right superior medial frontal cortex: afterthe body–mind relaxation meditation induction, the MDD patients showedincreased mALFF values in the area, whereas the healthy controls showeddecreased mALFF values. Abbreviations: BMRMI: body–mind relaxation meditationinduction; L¼ left, R¼right. *0.01rpo0.05, **0.001rpo0.01.
Table 2Brain areas showing significant ALFF differences in 2 groups (MDD/HC)�2conditions (before BMRMI/after BMRMI) repeated measure ANOVA.
Brain region Side BA MNIcoordinates
Voxels F value
x y z
Main effect of diagnosisDorsal anterior insula R 13 36 9 15 20 20.8946Precuneus R 7 6 �66 45 129 27.0126Supplementary motor area R 6 6 �24 63 13 16.0003
Main effect of BMRMIFrontal pole L 10 �6 69 �9 115 24.9416Frontal pole R 10 12 72 3 22 17.9954
Interaction effect of diagnosis�BMRMIDorsal medial prefrontal cortex R 8,9 9 33 36 13 16.6908
Abbreviations: BMRMI: body–mind relaxation meditation induction; ANOVA:analysis of variance; ALFF: amplitude of low-frequency fluctuation; BA: Brodmannarea; MNI: Montreal Neurological Institute; L¼ left; R¼right.
F. Chen et al. / Journal of Affective Disorders 183 (2015) 75–8278

differences in the mALFF maps between the MDD patients and thecontrols.
4.1. Similar effect of BMRMI on MDDs and HCs
After the BMRM induction, the mALFF in the bilateral fronto-polar cortex (FPC) (rostrolateral prefrontal cortex) decreased inboth the MDD and the HC groups, although this decrease showed alower level of statistical significance in the HC group. Numerousneuroimaging studies have provided support for the role of thebilateral rostral prefrontal cortex in “evaluation, monitoring, ormanipulation of internally generated information” (Burgess et al.,
2007). The FPC (BA10) receives no direct input from the sensorycortex leaving it well-positioned to consider events beyond thepresent moment: self-reflection, long-term goals, past or futureevents, or hypothetical scenarios (Downar and Daskalakis, 2013). Ameta-analysis demonstrated increased resting-state activity inthe BA10 as a consistent finding in patients with depression(Fitzgerald et al., 2008). Correcting the excessive activity in theFPC has also been correlated with the success of MDD treatment intherapy modalities such as rTMS, DBS, and CBT (Bewernick et al.,2010; Goldapple et al., 2004; Henry et al., 2001).
The anterior prefrontal cortex (frontopolar cortex) is also ameditation-related region. Anatomical likelihood estimation (ALE)
Table 3Functional connectivity alterations after BMRMI on MDDs and HCs.
Seed region FC sig. region BA MNI Coordinates Voxels T value
x y z
MDD groupRight dmPFC (BA8/9) Left dorsal LPFC 8 �36 15 48 13 4.9025Right dmPFC (BA8/9) Left lateral OFC 47/12 �39 54 �9 13 5.5586
HC groupRight dmPFC (BA8/9) No significant region
Abbreviations: BMRMI: body–mind relaxation meditation induction; dmPFC: dorsal medial prefrontal cortex; LPFC: lateral prefrontal cortex; OFC: orbitofrontal cortex; BA:Brodmann area; MNI: Montreal Neurological Institute; L¼ left; R¼right
Fig. 4. Functional connectivity alterations after BMRMI on MDDs and HCs. Abbreviations: BMRMI: body–mind relaxation meditation induction; dmPFC: dorsal medialprefrontal cortex; LPFC: lateral prefrontal cortex; OFC: orbitofrontal cortex. L¼ left; R¼right; ***po0.001.
F. Chen et al. / Journal of Affective Disorders 183 (2015) 75–82 79

meta-analysis found consistent morphological differences in thefrontopolar cortex (BA10) in meditators compared with controlswith no meditation experience or short term meditators(Fox et al., 2014). Other research indicated that long-term medita-tion practice is associated with altered cortical thickness in thefrontopolar cortex (Lazar et al., 2005). Based on these previousstudies and our findings, we suggest that BMRMI decreases theactivity of the anterior superior prefrontal cortex. This loweredactivity may contribute to weakening of the rumination processand short circuiting of complex thought, helping participants stayrelaxed.
4.2. Specific effect of BMRMI on MDDs
We also detected three brain regions, the right dmPFC, leftdorsal dlPFC, and left lateral OFC, that showed effects of theBMRMI that were specific to the MDD patients.
The particular regions of the dmPFC, dlPFC, and lateral OFC thatwe detected are similar to regions commonly activated by cogni-tive reappraisal, an emotion regulation strategy that involveschanging the trajectory of an emotional response by reinterpretingthe meaning of the emotional stimulus (Kalisch et al., 2006;Ochsner et al., 2002; Smoski et al., 2013). This reappraisal processis an important mechanism of self-regulation that has conse-quences for mental and physical well-being, as being exemplifiedby the central role of reappraisal processes in cognitive behavioraltherapy (Willner et al., 2013).
In general, cognitive reappraisal has been shown to dependupon interactions between prefrontal systems that support controlprocesses and posterior cortical and subcortical systems that formrepresentations of the different types of modality specific (e.g.visual, spatial, auditory) information (Ochsner and Gross, 2005). Arecent meta-analysis identified the dorsolateral and dorsomedialprefrontal cortex (dlPFC and dmPFC), the orbitofrontal cortex(OFC), and the parietal cortex as the most important nodes ofthe cognitive reappraisal network (Kalisch, 2009). A study byGolkar et al. confirmed that both the dorsolateral prefrontal cortex(DLPFC) and the lateral orbitofrontal cortex (OFC) contribute toemotion regulation through reappraisal (Golkar et al., 2012). Areview study by Ridderinkhof and others concluded that conver-ging evidence points to the presence of functional interactionsbetween the posterior medial frontal cortex (pMFC) and the lateralprefrontal cortex (LPFC), such that monitoring-related pMFCactivity serves as a signal that engages regulatory process in theLPFC that implement adjustments in cognitive control perfor-mance (Ridderinkhof et al., 2004).
A previous study found decreases in the gamma oscillation inthe frontal regions of MDD patients, indicating that the top-downinhibitory control systems involved in emotion regulation areimpaired (Lee et al., 2010). The prefrontal cortex (PFC) governsthe executive control of information processing and behavioralexpression, including the ability to selectively attend to andmaintain information, to inhibit irrelevant stimuli and impulses,and to evaluate and select appropriate responses. In thecurrent study, increased functional connectivity between theinterhemispheric prefrontal nodes of MDD patients was observedafter BMRMI, a finding which may suggest that BMRMI couldmodulate cognitive reappraisal through regulating functionalinteractions in the prefrontal cortex. A recent study demonstratedthat MDD patients showed lower voxel-mirrored homotopicconnectivity (VMHC) in the medial prefrontal cortex (MPFC) thanhealthy subjects (Guo et al., 2013). Decreased connectivityin the frontal regions has been related to cognitive deficits indepression, and successful treatments appear to normalize theserelationships (Beall et al., 2012). The present findings in ourresearch raise the possibility that BMRMI may improve the
cognitive reappraisal ability of MDD patients by regulating thefunctional interactions in the prefrontal cortex. However, morerigorous designs will be needed to assess greater levels of causalspecificity.
4.3. Group differences in mALFF maps between MDDs and HCs
In addition, an ANOVA analysis found group differencesbetween the MDD patients and the healthly controls. Threeregions, the right anterior insula, the right precuneus, and theright supplementary motor area, showed significantly differentmALFF values.
The anterior insular cortex (AIC) has been reported to be animportant cortical structure involved in awareness, pain, attention,and interoception (Craig, 2009). The AIC is also considered to be alimbic-related cortex. Major depressive disorder is characterizedby a dysregulated fronto-limbic network. Hyperactivation of thelimbic regions leads to increased attention and processing ofemotional information, with a bias toward negative stimuli. Inthe current study, the right anterior insula showed greater activityin the resting state in the MDD patients than in the HCs,supporting the concept that MDD patients are unable to disengagefrom externally cued events and negative emotions, a combinationwhich may lead to pathologically self-focused mental ruminativebehaviors.
The precuneus, which is centrally located in the default modenetwork, has consistently been reported to be involved in thepathophysiology of depression. Resting electroencephalographyhas showed hypoactivity of the precuneus in depressed subjects(Pizzagalli et al., 2002). Patients with MDD have also showedsignificantly lower signal intensities in the precuneus during aparadigm that focused on judgments about self-relatedness(Grimm et al., 2009). Moreover, decreased gray matter density inthe precuneus (BA 7) has been showed to contribute to thediagnosis of depression (Costafreda et al., 2009). A recent studyalso found decreased regional amplitudes (fALFF and ALFF) inMDD patients in the precuneus (Jing et al., 2013), a finding whichis consistent with our findings.
The supplementary motor area (SMA) (including BA6), is abrain area that has been given little attention in emotion proces-sing. However, recent studies have suggested that this region isrelated to MDD. Indeed, a reduced gray matter volume was foundin the right SMA (BA 6) of depressed patients (Cheng et al., 2010;Yuan et al., 2008). Abnormal activity in the SMA (BA6) wasobserved when MDD patients performed an emotion recognitiontask (Scheuerecker et al., 2010; Stuhrmann et al., 2011). Our studydetected a decrease in the mALFF value for the right SMA of MDDpatients using resting-state fMRI.
4.4. Limitations
In addition to the relatively small sample size, a few limitationsto this study should be noted. In order to exclude the impact ofother events on the participants' brain activity, we opted not tomeasure the Hamilton Rating Scales for Depression (HDRS) afterthe body–mind relaxation induction. This made it difficult toestimate the clinical efficacy of the BMRMI. Therefore, althoughour results suggest that the BMRMI experience may improve MDDpatients' cognitive reappraisal, this hypothesis has to be consid-ered as preliminary. Other analytical techniques such as dynamiccausal modeling or network-based analysis might be helpful foridentifying a more specific role for BMRM induction in MDDtreatment.
F. Chen et al. / Journal of Affective Disorders 183 (2015) 75–8280

5. Conclusions
In this study, we sought to detect how body–mind relaxationmeditation induction (BMRMI) influences resting-state brain activityin MDD patients and HCs. Our results revealed altered regional brainactivity in both groups after the BMRMI. In summary, the BMRMIdecreased the activity of the anterior superior prefrontal cortex inboth groups, a finding which implies a role for this region in keepingthe mind in a relaxed state. Moreover, the BMRMI enhanced theresting-state functional connectivity in the MDD group between theright dmPFC and the left dlPFC and between the right dmPFC andthe left lateral OFC, all regions which play important roles incognitive reappraisal. This suggests that BMRMI may improve thecognitive reappraisal ability of MDD patients by regulating thefunctional interactions in their prefrontal cortex. Taken together,our findings provide new insights into possible mechanisms of actionfor body–mind relaxation meditation induction in MDD therapy.
Role of funding sourceThis work was partially supported by the National Key Basic Research and
Development Program (973) (Grant no. 2011CB707800), the Strategic Priority ResearchProgram of the Chinese Academy of Sciences (Grant no. XDB02030300),“100 TalentsPlan” of Chinese Academy of Sciences to J Sui, the State High-Tech Development Plan(863) (Grant no. 2015AA020513), and the National Natural Science Foundation ofChina (Grant nos. 81471367, 91132301, 11371017 and 61303102).
Conflict of interestThe Authors have declared that there are no conflicts of interest in relation to
the subject of this study.
AcknowledgmentsThe authors wish to acknowledge the precious help of Dr. Chunhong Liu for
advice on fMRI data analysis. Moreover, we would like to thank Drs. Rhoda E. andEdmund F. Perozzi for a critical reading of the manuscript and kindly giving helpfuladvice.
References
Baghai, T.C., Moller, H.J., Rupprecht, R., 2006. Recent progress in pharmacologicaland non-pharmacological treatment options of major depression. Curr. Pharm.Des. 12, 503–515.
Beall, E.B., Malone, D.A., Dale, R.M., Muzina, D.J., Koenig, K.A., Bhattacharrya, P.K.,Jones, S.E., Phillips, M.D., Lowe, M.J., 2012. Effects of electroconvulsive therapyon brain functional activation and connectivity in depression. J. ECT 28,234–241.
Beshai, S., Dobson, K.S., Bockting, C.L., Quigley, L., 2011. Relapse and recurrenceprevention in depression: current research and future prospects. Clin. Psychol.Rev. 31, 1349–1360.
Bewernick, B.H., Hurlemann, R., Matusch, A., Kayser, S., Grubert, C., Hadrysiewicz, B.,Axmacher, N., Lemke, M., Cooper-Mahkorn, D., Cohen, M.X., Brockmann, H.,Lenartz, D., Sturm, V., Schlaepfer, T.E., 2010. Nucleus accumbens deep brainstimulation decreases ratings of depression and anxiety in treatment-resistantdepression. Biol. Psychiatry 67, 110–116.
Burgess, P.W., Dumontheil, I., Gilbert, S.J., 2007. The gateway hypothesis of rostralprefrontal cortex (area 10) function. Trends Cogn. Sci. 11, 290–298.
Cheng, Y.Q., Xu, J., Chai, P., Li, H.J., Luo, C.R., Yang, T., Li, L., Shan, B.C., Xu, X.F., Xu, L.,2010. Brain volume alteration and the correlations with the clinical character-istics in drug-naive first-episode MDD patients: a voxel-based morphometrystudy. Neurosci. Lett. 480, 30–34.
Costafreda, S.G., Chu, C., Ashburner, J., Fu, C.H., 2009. Prognostic and diagnosticpotential of the structural neuroanatomy of depression. PLoS One 4, e6353.
Craig, A.D., 2009. How do you feel — now? The anterior insula and humanawareness. Nat. Rev. Neurosci. 10, 59–70.
Downar, J., Daskalakis, Z.J., 2013. New targets for rTMS in depression: a review ofconvergent evidence. Brain Stimul. 6, 231–240.
Fitzgerald, P.B., Laird, A.R., Maller, J., Daskalakis, Z.J., 2008. A meta-analytic study ofchanges in brain activation in depression. Hum. Brain Mapp. 29, 683–695.
Fox, K.C., Nijeboer, S., Dixon, M.L., Floman, J.L., Ellamil, M., Rumak, S.P., Sedlmeier, P.,Christoff, K., 2014. Is meditation associated with altered brain structure? Asystematic review and meta-analysis of morphometric neuroimaging in med-itation practitioners. Neurosci. Biobehav. Rev. 43, 48–73.
Goldapple, K., Segal, Z., Garson, C., Lau, M., Bieling, P., Kennedy, S., Mayberg, H.,2004. Modulation of cortical-limbic pathways in major depression: treatment-specific effects of cognitive behavior therapy. Arch. Gen. Psychiatry 61, 34–41.
Golkar, A., Lonsdorf, T.B., Olsson, A., Lindstrom, K.M., Berrebi, J., Fransson, P.,Schalling, M., Ingvar, M., Ohman, A., 2012. Distinct contributions of thedorsolateral prefrontal and orbitofrontal cortex during emotion regulation.PLoS One 7, e48107.
Goyal, M., Singh, S., Sibinga, E.M., Gould, N.F., Rowland-Seymour, A., Sharma, R.,Berger, Z., Sleicher, D., Maron, D.D., Shihab, H.M., Ranasinghe, P.D., Linn, S.,Saha, S., Bass, E.B., Haythornthwaite, J.A., 2014. Meditation programs forpsychological stress and well-being: a systematic review and meta-analysis.JAMA Intern. Med. 174, 357–368.
Grimm, S., Ernst, J., Boesiger, P., Schuepbach, D., Hell, D., Boeker, H., Northoff, G.,2009. Increased self-focus in major depressive disorder is related to neuralabnormalities in subcortical–cortical midline structures. Hum. Brain Mapp. 30,2617–2627.
Guo, W., Liu, F., Dai, Y., Jiang, M., Zhang, J., Yu, L., Long, L., Chen, H., Gao, Q., Xiao, C.,2013. Decreased interhemispheric resting-state functional connectivity in first-episode, drug-naive major depressive disorder. Prog. Neuropsychopharmacol.Biol. Psychiatry 41, 24–29.
Henry, M.E., Schmidt, M.E., Matochik, J.A., Stoddard, E.P., Potter, W.Z., 2001. Theeffects of ECT on brain glucose: a pilot FDG PET study. J. ECT 17, 33–40.
Hoptman, M.J., Zuo, X.N., Butler, P.D., Javitt, D.C., D'Angelo, D., Mauro, C.J., Milham,M.P., 2010. Amplitude of low-frequency oscillations in schizophrenia: a restingstate fMRI study. Schizophr. Res. 117, 13–20.
Hsu, W.C., Lai, H.L., 2004. Effects of music on major depression in psychiatricinpatients. Arch. Psychiatr. Nurs. 18, 193–199.
Jain, F.A., Walsh, R.N., Eisendrath, S.J., Christensen, S., Rael Cahn, B., 2014. Criticalanalysis of the efficacy of meditation therapies for acute and subacute phasetreatment of depressive disorders: a systematic review. Psychosomatics 56,140–152.
Jiang, G.H., Qiu, Y.W., Zhang, X.L., Han, L.J., Lv, X.F., Li, L.M., Lin, C.L., Zhuo, F.Z., Hu, S.Y., Tian, J.Z., 2011. Amplitude low-frequency oscillation abnormalities in theheroin users: a resting state fMRI study. NeuroImage 57, 149–154.
Jing, B., Liu, C.-H., Ma, X., Yan, H.-G., Zhuo, Z.-Z., Zhang, Y., Wang, S.-H., Li, H.-Y.,Wang, C.-Y., 2013. Difference in amplitude of low-frequency fluctuationbetween currently depressed and remitted females with major depressivedisorder. Brain Res. 1540, 74–83.
Kalisch, R., 2009. The functional neuroanatomy of reappraisal: time matters.Neurosci. Biobehav Rev. 33, 1215–1226.
Kalisch, R., Wiech, K., Critchley, H.D., Dolan, R.J., 2006. Levels of appraisal: a medialprefrontal role in high-level appraisal of emotional material. NeuroImage 30,1458–1466.
Kublbock, M., Woletz, M., Hoflich, A., Sladky, R., Kranz, G.S., Hoffmann, A.,Lanzenberger, R., Windischberger, C., 2014. Stability of low-frequency fluctua-tion amplitudes in prolonged resting-state fMRI. NeuroImage 103, 249–257.
Kupfer, D.J., Frank, E., Phillips, M.L., 2012. Major depressive disorder: new clinical,neurobiological, and treatment perspectives. Lancet 379, 1045–1055.
Kuyken, W., Byford, S., Taylor, R.S., Watkins, E., Holden, E., White, K., Barrett, B.,Byng, R., Evans, A., Mullan, E., Teasdale, J.D., 2008. Mindfulness-based cognitivetherapy to prevent relapse in recurrent depression. J. Consult. Clin. Psychol. 76,966–978.
Lazar, S.W., Kerr, C.E., Wasserman, R.H., Gray, J.R., Greve, D.N., Treadway, M.T., McGarvey,M., Quinn, B.T., Dusek, J.A., Benson, H., Rauch, S.L., Moore, C.I., Fischl, B., 2005.Meditation experience is associated with increased cortical thickness. NeuroReport16, 1893–1897.
Lee, P.S., Chen, Y.S., Hsieh, J.C., Su, T.P., Chen, L.F., 2010. Distinct neuronal oscillatoryresponses between patients with bipolar and unipolar disorders: a magne-toencephalographic study. J. Affect. Disord. 123, 270–275.
Little, S.A., Kligler, B., Homel, P., Belisle, S.S., Merrell, W., 2009. Multimodal mind/body group therapy for chronic depression: a pilot study. Explore 5, 330–337.
Ochsner, K.N., Bunge, S.A., Gross, J.J., Gabrieli, J.D., 2002. Rethinking feelings: anfMRI study of the cognitive regulation of emotion. J. Cogn. Neurosci. 14,1215–1229.
Ochsner, K.N., Gross, J.J., 2005. The cognitive control of emotion. Trends Cogn. Sci. 9,242–249.
Pizzagalli, D.A., Nitschke, J.B., Oakes, T.R., Hendrick, A.M., Horras, K.A., Larson, C.L.,Abercrombie, H.C., Schaefer, S.M., Koger, J.V., Benca, R.M., Pascual-Marqui, R.D.,Davidson, R.J., 2002. Brain electrical tomography in depression: the importanceof symptom severity, anxiety, and melancholic features. Biol. Psychiatry 52,73–85.
Ridderinkhof, K.R., Ullsperger, M., Crone, E.A., Nieuwenhuis, S., 2004. The role of themedial frontal cortex in cognitive control. Science 306, 443–447.
Scheuerecker, J., Meisenzahl, E.M., Koutsouleris, N., Roesner, M., Schopf, V., Linn, J.,Wiesmann, M., Bruckmann, H., Moller, H.J., Frodl, T., 2010. Orbitofrontal volumereductions during emotion recognition in patients with major depression.J. Psychiatry Neurosci. 35, 311–320.
Shelton, C.I., 2004. Long-term management of major depressive disorder: aredifferences among antidepressant treatments meaningful? J. Clin. Psychiatry65 (Suppl. 17), S29–S33.
Simkin, D.R., Black, N.B., 2014. Meditation and mindfulness in clinical practice. ChildAdolesc. Psychiatr. Clin. N. Am. 23, 487–534.
Sliz, D., Hayley, S., 2012. Major depressive disorder and alterations in insularcortical activity: a review of current functional magnetic imaging research.Front. Hum. Neurosci. 6, 323.
Smoski, M.J., Keng, S.L., Schiller, C.E., Minkel, J., Dichter, G.S., 2013. Neuralmechanisms of cognitive reappraisal in remitted major depressive disorder.J. Affect. Disord. 151, 171–177.
F. Chen et al. / Journal of Affective Disorders 183 (2015) 75–82 81

Stuhrmann, A., Suslow, T., Dannlowski, U., 2011. Facial emotion processing in majordepression: a systematic review of neuroimaging findings. Biol. Mood AnxietyDisord. 1, 10.
Tang, Y.Y., 2011. Mechanism of integrative body-mind training. Neurosci. Bull. 27,383–388.
Tang, Y.Y., Ma, Y., Wang, J., Fan, Y., Feng, S., Lu, Q., Yu, Q., Sui, D., Rothbart, M.K., Fan, M.,Posner, M.I., 2007. Short-term meditation training improves attention and self-regulation. Proc. Natl. Acad. Sci. USA 104, 17152–17156.
van der Velden, A.M., Kuyken, W., Wattar, U., Crane, C., Pallesen, K.J., Dahlgaard, J.,Fjorback, L.O., Piet, J., 2015. A systematic review of mechanisms of change inmindfulness-based cognitive therapy in the treatment of recurrent majordepressive disorder. Clin. Psychol. Rev..
Willner, P., Scheel-Kruger, J., Belzung, C., 2013. The neurobiology of depression andantidepressant action. Neurosci. Biobehav. Rev. 37, 2331–2371.
Yan, C., Liu, D., He, Y., Zou, Q., Zhu, C., Zuo, X., Long, X., Zang, Y., 2009. Spontaneousbrain activity in the default mode network is sensitive to different resting-stateconditions with limited cognitive load. PLoS One 4, e5743.
Yang, H., Long, X.Y., Yang, Y., Yan, H., Zhu, C.Z., Zhou, X.P., Zang, Y.F., Gong, Q.Y., 2007.Amplitude of low frequency fluctuation within visual areas revealed by resting-state functional MRI. NeuroImage 36, 144–152.
Yuan, Y., Zhu, W., Zhang, Z., Bai, F., Yu, H., Shi, Y., Qian, Y., Liu, W., Jiang, T., You, J., Liu, Z.,2008. Regional gray matter changes are associated with cognitive deficits inremitted geriatric depression: an optimized voxel-based morphometry study. Biol.Psychiatry 64, 541–544.
Zang, Y.F., He, Y., Zhu, C.Z., Cao, Q.J., Sui, M.Q., Liang, M., Tian, L.X., Jiang, T.Z., Wang, Y.F.,2007. Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev. 29, 83–91.
Zeidan, F., Johnson, S.K., Diamond, B.J., David, Z., Goolkasian, P., 2010a. Mindfulnessmeditation improves cognition: evidence of brief mental training. Conscious.Cogn. 19, 597–605.
Zeidan, F., Johnson, S.K., Gordon, N.S., Goolkasian, P., 2010b. Effects of brief andsham mindfulness meditation on mood and cardiovascular variables. J. Altern.Complement. Med. 16, 867–873.
Zuo, X.N., Xing, X.X., 2014. Test–retest reliabilities of resting-state fMRI measure-ments in human brain functional connectomics: a systems neuroscienceperspective. Neurosci. Biobehav. Rev. 45, 100–118.
F. Chen et al. / Journal of Affective Disorders 183 (2015) 75–8282
Copyright © 2022 FDOKUMEN