
Living Well: A Guide for Persons with Mild Cognitive Impairment (MCI) and Early Dementia
Upload
independentCategory
view
2download
0
Journal of Cardiovascular NursingVol. 00, No. 0, pp 00Y00 x Copyright B 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins
The Association Between Mild CognitiveImpairment and Self-care in Adults WithChronic Heart FailureA Systematic Review and Narrative Synthesis
Kay Currie, PhD, RN; Andrew Rideout, MPH, RN; Grace Lindsay, PhD, RN;Karen Harkness, PhD, RN
Background: Emerging evidence suggests that heart failure (HF) patients who have mild cognitive impairment
(MCI) may experience greater difficulty with self-care. Objective: This article reports a systematic review that
addressed the objective ‘‘What is the evidence for an association between MCI and self-care, measured in
1 or more of the self-care domains related to HF, in adults who have a diagnosis of chronic HF?’’ Method:
We adopted Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for the review and
synthesis of quantitative research studies that formally measured both cognitive function and self-care in HF
patients and sought to describe the relationship between these factors. Results: Ninety-one potentially relevant
studies were located; 10 studies (2006Y2014) were included. Because of heterogeneity in the retrieved studies,
meta-analysis was not possible. Narrative synthesis found growing evidence regarding the association between
MCI and adverse effects on self-care in HF. Nine studies reported significant positive associations between MCI
and self-care in HF, either specifically in relation to medication adherence or more generic measures of self-care
activity. One study reported a significant, negative correlation between cognitive function and self-care,
suggesting that worse cognitive function was associated with better self-care; however, this is partially explained
by a small sample size and mixed methodology. Conclusions: These findings have implications for clinical
practice. It is known that HF patients have difficulty with self-care, and the influence of cognitive function needs
to be considered when providing professional support. Further research to determine the feasibility and
acceptability of cognitive assessment in routine clinical care is recommended.
KEY WORDS: heart failure, mild cognitive impairment, review, self-care, systematic
Background
Heart failure (HF) is a syndrome of reduced cardiacoutput, such that the heart cannot maintain adequatetissue perfusion.1 Quality of life for individuals with
HF may be reduced by symptoms of breathlessness,limb edema, and fatigue, often resulting in disturbedsleep, reduced capacity for coping with normal daily ac-tivities or employment, and deteriorating mental well-being.2 The prevalence of HF is 1% to 2% of the generalpopulation, but that increases significantly with age, risingsharply to 10% for individuals around 70 years of age.3
In a comprehensive literature review of epidemiologicalstudies of HF, the overall prevalence ranges from 1% to12%, with variation caused mainly by methodologicaldifferences between studies.4 As the population ages,the burden of HF can be expected to increase in manycountries.3,5
There is growing recognition of the importance ofeffective self-care in the management of HF.3,6 The in-ability to undertake self-care activities is well recognizedas a contributing factor for increased hospital admissionin patients with HF.7,8 Self-care in this context has beendescribed as a naturalistic decision-making process involv-ing knowledge, experience, skill, and compatibility withpersonal values.9 Theoretically, the concept of self-care
1
Kay Currie, PhD, RNReader in Applied Health Research, Nursing & Community Health,Glasgow Caledonian University, Scotland, UK.
Andrew Rideout, MPH, RNResearcher, Nursing & Community Health, Glasgow CaledonianUniversity, Scotland, UK.
Grace Lindsay, PhD, RNReader in Nursing, Nursing & Community Health, GlasgowCaledonian University, Scotland, UK.
Karen Harkness, PhD, RNAssistant Clinical Professor, School of Nursing, McMaster University,Ontario, Canada.
The authors have no conflicts of interest to disclose.
CorrespondenceKay Currie, PhD, RN, School of Health & Life Sciences, GlasgowCaledonian University, Cowcaddens Road, Glasgow G4 0BA,Scotland, UK ([email protected]).
DOI: 10.1097/JCN.0000000000000173
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

in HF has been explained in terms of 3 discrete yet over-lapping components. These are self-care maintenance(involving activities associated with symptom monitoringand treatment adherence), self-care management (wherepatients recognize and respond to their symptoms by im-plementing self-care activities), and self-care confidence(acts as a mediator and moderator of the outcomes ofthe self-care process).9 Recommendations for patient be-haviors or activities to promote self-care include adviceregarding medication, fluid and sodium management,nutrition and weight management, smoking cessation,alcohol limitation, and physical activity,10 commonly de-scribed as the ‘‘domains’’ of self-care in the context of HF.
Specific tools have been developed and validated tomeasure self-care in patients with HF, the most com-monly cited being the Self-care in Heart Failure Index(SCHFI)11 and the European Heart Failure Self-care Be-haviour Scale.12 Both tools were developed based on aninitial concept analysis to construct scale items and sub-sequent psychometric testing using pooled data drawnfrom multicenter studies; however, it should be noted thatthese tools rely on patient self-report, which may under-report or overreport actual self-care ability, and a singleassessment may not reflect variation in self-care over time.
Self-care in HF patients involves a complex cognitivedecision-making process; however, the pathophysiologyand symptoms associated with HF may have an adverseimpact on cognitive functioning.13 Therefore, it is rea-sonable to consider the potential contribution of cognitivefunction on engagement in self-care in HF. Cognitiondescribes the intellectual functions required to manageindependently within one’s environment. These includememory, language, attention, visuospatial ability, behav-ior, and executive functions.13 Cognition in aging per-sons follows along a spectrum ranging from normalfunction to severe impairment, known as dementia. Mildcognitive impairment (MCI) is described as an interme-diate step between normal cognitive function and de-mentia that make performance of some activities of dailyliving more difficult than usual (eg, unable to organizemedications or appointments without a memory aid ortake care of finances) but are not severe enough to im-pair basic activities of daily living (eg, dressing, eating,toileting).14 Formal diagnosis of MCI requires evidenceof abnormalities on neuropsychological testing (1.5 SDbelow age-standardized mean) in at least 1 cognitivedomain, with or without memory impairment.15
The presence of cognitive impairment is well docu-mented in patients with HF, with a prevalence rangingbetween 25% and 75%,16Y19 depending on the defi-nition used and the cognitive domains tested. The Mini-Mental State Examination (MMSE)20 is a widely usedinstrument for cognitive testing in older persons, with orwithout HF.16,21,22 However, it is acknowledged thatthe MMSE is not sensitive for detecting MCI and haslimited sensitivity to executive functions.22,23 In other
words, people with HF and MCI will often score withinthe normal range on the MMSE, and therefore, the pre-sence of MCI is missed.21,24,25 The Montreal CognitiveAssessment (MoCA) is recommended for use in patientswith vascular disease26 and is sensitive to cognitive de-ficits detected in older HF patients. Recent studies havereported a prevalence of MCI, as defined by a totalMoCA score lower than 26, in 54% to 75% of olderpatients with HF.27Y29 Difficulties with memory, atten-tion, psychomotor speed, verbal learning, and executivefunctions are the most common types of cognitive de-ficits reported.30,31 It is often difficult to detect MCI ina clinical setting without formal cognitive testing or spe-cifically asking about signs such as a decline in managingfinances, organizing medications, or performing otherusual instrumental activities.14
Self-care imposes a high cognitive demand on patientswith HF, and emerging evidence suggests that patientswith MCI may experience difficulty with self-care,25,32,33
although the evidence for this association is arguablylimited. Evaluation and synthesis of current evidenceare important to inform clinical practice; identifyingwhether MCI can affect specific domains or generalaspects of self-care in patients with HF will enable clin-icians who support patients in developing knowledge,skill, and confidence in self-care to take account of theinfluence of cognitive function.
This article reports a systematic review that aimedto synthesize the best available evidence for an asso-ciation between MCI and self-care in adults who havebeen diagnosed with chronic HF. The review questionwas as follows: What is the evidence for an associationbetween MCI and self-care, measured in 1 or more of theself-care domains related to HF, in adults who have adiagnosis of chronic HF? A review protocol was reg-istered with the Joanna Briggs Institute (protocol 642).
Methods
We adopted the Preferred Reporting Items for System-atic Reviews and Meta-Analyses approach34 to system-atic review and narrative synthesis. The inclusion criteriawere primary quantitative studies that recruited adultpatients (Q18 years) who have a diagnosis of chronicHF, at any stage of the New York Heart Association(NYHA) classification of HF, regardless of sex, age,ethnic origin, or any comorbidity. Our inclusion criteriawere articles that excluded patients who had preexistingdementia or known severe cognitive impairment and thatused validated instruments to measure cognitive functionor impairment that were sensitive to MCI and also mea-sured self-care capability or activities then sought todescribe the relationship between these factors. For thepurposes of this review, MCI was defined as evidence ofimpairment on a validated tool or diagnostic battery inindividuals whodo not have cognitive impairment that
2 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

is severe enough to interfere with their basic activitiesof daily living; studies that conducted cognitive testingusing only the MMSE were excluded, as this test is notsensitive to MCI. Definitions of self-care could includemanagement of diet (including healthy diet, salt, and fluidintake), medicines management, avoidance of risk factorsfor disease progression/deterioration, and symptom aware-ness and management. Measurement of self-care may beperformed using validated tools, or more simple mea-sures (such as percentage of missed medications).
Our search strategy was reviewed by an informationmanagement specialist and aimed to find both publishedand unpublished (indexed) studies. We conducted a sys-tematic search of electronic databases, including Medline,EMBASE, CINAHL, PsycINFO, CSA Sociological Ab-stracts, AARPAgeline, SocINDEX, ISI Web of Science:Social Sciences Citation Index and Science Citation IndexExpanded, Ethos, and MedNar. As the concept of self-care in HF developed in the mid-1990s, a date limit of1995 was set for the database search; because of re-source constraints, only articles with English abstractwere included in the search. A 3-phase search strategywas used. The initial search used 3 keywords or phrases:heart failure, cognitive, and self-care. These terms werecombined using the ‘‘AND’’ Boolean operator and en-tered into Medline, CINAHL, and MedNar databases.Retrieved articles were reviewed to identify keywordscontained in the title and abstract, as well as index termsused to describe the article. A second search using allidentified keywords and index terms plus theoreticallyderived terms from the self-care literature was then per-formed across all included databases (Table 1). Third,the reference list of all identified reports was searchedfor additional studies. There was no other attempt toidentify gray literature in the area of interest (search com-pleted March 14, 2014).
All citations located by the search were screened by2 reviewers for relevance based on the title and abstract.Thereafter, the full text of selected articles or theses wasassessed independently by 2 reviewers using the speci-fied inclusion criteria, before appraisal of methodologicalquality using a standardized critical appraisal instru-ment from the Joanna Briggs Institute (JBI-MAStARI).The Figure demonstrates the selection process adopted.
Data from included studies were extracted onto astandardized template by 1 reviewer and independentlyconfirmed by a second, with any discrepancies resolvedthrough discussion with a third reviewer. Data itemsincluded study setting; method; demographic data suchas age, sex, and cohabitation status; disease-specificdata (commonly NYHA classification); and a wide va-riety of outcome measures pertaining to the 2 areas ofinterest for this review (cognitive impairment and self-care), including descriptive statistics and results fromregression analyses indicating association between out-come measures.
A heterogeneous range of data collection tools wereused for assessment of variables and data aggregationor meta-analysis was not possible; instead, findings ex-tracted from all included studies were inserted into amatrix for ease of comparison for narrative synthesis.Measures used to assess cognitive function and self-carewere highlighted to identify possible similarities; outcomeswere classified as self-care related to either medicationadherence (a specific focus of several studies) or a broaderrange of self-care activities. Studies were further cate-gorized into those that demonstrated a statistically sig-nificant association between MCI and self-care and thosethat did not. Table 2 presents summary details of the10 studies25,35,39Y43 included in this comparative matrix.All were observational correlation designs, published asfull-text articles between 2006 and 2014; 2 studies42,43
included mixed methods; and 1 study38 was a compa-rative cohort design. Eight studies were conducted in theUnited States,35Y39,41,43 1 was conducted in Australia,25
and 1 in Canada.40
Results
Ten studies were included in the review, involving atotal of 1842 patients. Sample size ranged from 29 to557 participants. One study42 purposively sampled ex-treme cases (poor or expert in self-care; n = 29), andanother43 used a purposive homogenous sampling tech-nique. All other studies recruited convenience samplesthat met inclusion criteria.
TABLE 1 Summary of Search Terms Used Across
All Included Databases
S1 MM ‘‘Heart Failure +’’S2 ‘‘Cardiac failure’’S3 ‘‘Ventricular failure’’S4 ‘‘Pulmonary oedema’’ OR ‘‘Pulmonary Edema’’S5 ‘‘Dyspnoea+’’S6 S1 OR S2 OR S3 OR S4 OR S5S7 MM ‘‘cognitive impairment’’S8 ‘‘Mild cognitive impairment’’S9 ‘‘Cognitive disorders+’’
S10 ‘‘Cognitive dysfunction’’S11 ‘‘Cognitive function’’S12 ‘‘Executive function’’S13 S7 OR S8 OR S9 OR S10 OR S11 OR S12S14 MM ‘‘Self-care+’’S12 ‘‘Self-management’’S13 ‘‘Medicines management’’S14 ‘‘Medication management’’S15 ‘‘Medication adherence’’S16 ‘‘Exercise’’S17 ‘‘Diet’’S18 ‘‘Diet, sodium-restricted’’S19 ‘‘Fluid intake’’S20 ‘‘Fluid restriction’’S21 ‘‘Smoking’’S22 S14ORS15ORS16S17ORS17ORS18ORS19ORS20ORS21S23 S6 AND S13 AND S22
Mild Cognitive Impairment and Self-care in Chronic HF 3
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Two studies25,39 recruited HF patients during anhospital admission; the other 8 studies recruited from HFoutpatient clinics or management programs.35Y38,40Y43
Most of both inpatient and clinic participants were re-cruited from single facilities, with only 3 studies25,38,43
recruiting from more than 1 site. Participant ages rangedfrom 25 to 93 years, with mean ages of 49 to 73 yearsreported. Two studies targeted older patients (945 years25
and 955 years40) to increase representativeness of theHF population. Most participants were male. One largersample study36 recruited from a veterans’ facility, and menconstituted 99% of the sample. Eight studies25,35,36,38,40Y43
provided NYHA classification details for participants,indicating functional severity of HF; most participantshad at least NYHA stage III HF, suggesting marked lim-itation in activity due to HF symptoms. Where reported,participants were urban dwelling and predominantlywhite, although minority groups were represented inmost studies. Five studies25,37,39,41,42 reported whetherparticipants lived alone or with another person; in thesesamples, most lived with another person, with 13% to49.7% living alone.
A variety of cognitive assessment tools were used inthe reported studies; each included study used at least1 technique known to be sensitive in detecting MCI.One study used MMSE and MoCA25; 2 used MoCAalone40,41; 1 used MMSE in combination with a range
of other cognitive assessment tools35; and the remaining6 studies used various other assessment tools excludingthe more commonly applied MMSE or MoCA.36Y39,42,43
Most articles did not differentiate between degrees ofcognitive impairment in their findings (except for Hawkinset al37). However, as we included only studies that ex-cluded people with dementia or significant cognitive im-pairment and that used tools sensitive to MCI, we caninfer that the findings represent the association betweenMCI and self-care.
All included studies measured some dimension ofself-care capability or activities as outcomes of interest,addressing either medication adherence or a more com-prehensive assessment of self-care activities. Four studiesmeasured medication adherence using various report-ing scales35Y38; 3 studies used the validated SCHFIalone25,40,42; 1 study used the European Heart FailureSelf-care Behaviour scale39; 1 study used SCHFI and theEuropean Heart Failure Self-care Behaviour scale41; and1 study used SCHFI and the Dutch Heart Failure Knowl-edge Scale.43
Review Findings
From the 10 studies reviewed, 8 studies25,35Y41 reportedstatistically significant results indicating a positive corre-lation between MCI and self-care ability, with 1 study43
reporting a negative correlation between MCI and self-care (suggesting poorer cognitive function leads to betterself-care). One study42 did not report P values. Only4 studies37,39,40,43 reported confidence intervals for thefindings related to cognitive function alone; these werewide, suggesting that the effect size may be rather smallor of poor precision because of small sample size. How-ever, there is persuasive evidence that MCI affects HF-self-care ability adversely.
Measurement of selected variables was largely hetero-geneous in the included studies, with the variety of as-sessment tools and outcome measures, meaning thatmeta-analysis was not possible. Therefore, the follow-ing results are presented as a narrative synthesis of (a)those studies that found a statistically significant asso-ciation between MCI and some dimension of self-careand (b) the single study that reported a negative cor-relation between MCI and self-care (see Table 2).
Impaired Cognitive Function Leads toPoorer Self-care
Four studies35Y38 demonstrated a statistically significantassociation between MCI and poorer medication ad-herence. These studies had reasonable sample sizes (n =122Y280), and each used a combination of validated teststo measure cognitive function, thus increasing the like-lihood of detection of MCI. In 3 of 4 studies, medication
FIGURE. Selection process.
4 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE2
IncludedStu
dies
Author
Design
Setting
Age;Gender
NYHA
Class
Lived
Alone
Cognition
Outcome
Measu
res
Self-care
Outcome
Measu
res
Resu
ltsand
Conclusions
Studiesthatdemonstratedpositive
correlationbetw
eenMCIandpoorermedicationadherence
1.
Aloscoetal
(2012)35
Retrospective
observational
correlational
studyvia
hierarchical
regression
analysis
HFmanagement
program
inOhio,
United
States
59Y7
7y
(mean,68y)
F:M
29:93
2Y3
Notgiven
MMSE
TMT-A,
TMT-B
LawtonBrody
ADLScale
Functionalability
measuredand
arangeof
activities
including
medication
management
Cognitivefunctionshowed
increm
entalp
redictive
validityfor
medicationmanagement(R
2
change=0.14,PG.001;no
confidence
intervalsreported).
Significan
tassociationsare
TMT-A
withmed
ications,MMSEwith
driving,andgenderwithfinances.
Convenience
sample
of
consecutive
casesfrom
largeHF
database
InpersonswithHF,
cognitive
perform
ance
isanindependent
predictorofindependence
inmedicationmanagement.Persons
withpoorercognitivetest
perform
ance
(TMT-A)reported
greaterdifficultywithmed
ication
management.
Exclusioncriteria
relatedto
brain
function,
eg,stroke,
headinjury
withLO
CN=122
2.
Aloscoetal
(2013)36
Cross-sectional,
descriptive
studyusing
hierarchical
regression
analysis
OPDcardiology
clinicsin
Ohio
Mean,68y
As%
:1,0.5%
;2,84%;3,14%;
4,1.5%
Notgiven
TMT-A,
TMT-B
LawtonBrody
ADLScale
Significantbivariate
correlationan
dbetween(a)executive
function
(TMT-A)andmedicationmanagem
ent
(correlationcoefficient=0.18,
PG.05)and(b)attention(LNS)
and
medicationmanagem
ent(correlation
coefficient=0.15;PG.05).
Hierarchicalregressionsrevealed
that
reducedexecutive
functionwas
indepen
den
tlyassociated
witha
decreasedabilitytomanagemedications.
Noconfidence
intervalgiven.
N=197
F:M
70:127
DigitSymbol
Coding
Functionalability
measuredand
arangeof
activities
including
medication
management
Excluded
peo
ple
withdementia,
otherneurological
history
LNS
3.
Haw
kinsetal
(2012)37
Prospective
observational
correlational
studyvialinear
regression
HFveterans
OPDfacilityin
theUnited
States
33Y9
3y
(mean,66y)
Notgiven
27.3%
(68)
SaintLouis
University
Mental
Status
MA
Estim
ator
Compared
withnoCI,MAsignifican
tly
worsen
edby8percentagepoints
(78%
to70%,P
=.017)forpatients
withMCIbutdid
notcontinueto
worsen
forpatients
withsevere
CI
inthedem
entiarange.
(continues)
Mild Cognitive Impairment and Self-care in Chronic HF 5
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE2
Included
Stu
dies,
Continued
Author
Design
Setting
Age;Gender
NYHA
Class
LivedAlone
CognitionOutcome
Measu
res
Self-care
Outcome
Measu
res
Resu
ltsand
Conclusions
Convenience
sample
F:M
4:247
Battery
ofAssessmentof
neuropsychologicalstatus;
TMTs;Wechsler
TestofAdult
Reading;GroovedPegboard
Test;phonem
icandsemantic
verbalfluency
tasks;
Similarities,Matrix
Reasoning,
LNS,andDigitSpansubtests
from
theWechsler
Adult
Intelligence
Scale,4
thed
ition
Reg
ressionan
alyses
revealed
arobustassociationbetween
thepresence
ofCIandMA
(P=.017).Amongthe
studyvariab
les,onlyCIw
asfoundto
haveastatistically
significantassociationwith
MA.
Nosubjectshad
knownCI
beforeenrolment
Studyfoundthatunrecognized
CIw
ashighlyprevalent
andassociated
withpoorer
adheren
ceto
med
ication.
(Theseresultsarenot
necessarilysupported
bythe
confidence
intervals,which
suggestnodifference
betweengroups)
N=251
4.
Riegeletal
(2011)38
Prospective
comparative
observational
correlationstudy
vialogistic
regressionmodels
HFoutpatient
clinicsin
3UShospitals
50Y7
4(m
ean62)
Majority
3Notgiven
TelephoneInterview
of
CognitiveStatus
MAVBasel
Assessm
entof
Adherence
Scale
Theonlycognitionmeasure
significan
tlyassociated
withMAwas
attentionPV
T(P
=.047;noconfiden
ceintervalsreported).
Astratified
sampling
techniquewas
used,based
on
EDSan
dCI
F:M
100:180
PVT
Nonadherence
was
significantly
more
commonin
those
withEDS,
regardless
of
cognitivestatus(P
=.035).
N=280(242
completed)
TMT-B
Secondary
modelsusingthe
EDSscoreandtheindividual
cognitiontestscores
showed
thatcognitive
status
wasnotsignificantlyassociated
withMA(P
=.752).
Reportedattrition
andstates
cohorts
becam
esaturated
butnospecific
justificationfor
samplesize
DigitSymbol-SubstitutionTest
EDSmay
causelack
ofvigilance/
attentionan
dmedication
nonadherence,ie,picture
morecomplexthan
CIalone.
Theau
thorsacknowledge
thatthose
withCIm
ay
beunderreportingtheir
medicationnonad
heren
ce.
Excluded
ifdem
entia
orneurological
even
t
Probed-M
emory
RecallTask
LNStest
(continues)
6 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE2
Included
Stu
dies,
Continued
Author
Design
Setting
Age;Gender
NYHA
Class
LivedAlone
Cognition
Outcome
Measu
res
Self-care
Outcome
Measu
res
Resu
ltsand
Conclusions
Studiesthatdemonstratedpositive
correlationbetw
eenMCIandpoorercomprehensive
self-care
activity
5.
Cameronetal
(2010)25
Prospective
observational
correlational
studyvia
multiplelinear
regression
analysis
1inpatient
facilityin
Australia
62Y8
4y
(mean,73y)
45%
NYHA
Class
342%
(39)
MMSEandMoCA
SCHFI
Sixty-eightpatients
(75%
)were
codedashavingMCIandhad
significantlylowerself-care
management(P
=.01)and
self-confidence
scoresP=.05)
(noconfidence
intervalsgiven).
Convenience
sample
of
consecutive
patients
F:M
27:66
5%
NYHA
Class
4
MCImadethelargest
contribution,
explaining9%
ofthevariance
inself-care
management.
N=93
CI,ahiddencomorbidity,may
imped
epatients’abilityto
make
appropriate
self-caredecisions.
Dementia,
neurological
excluded
6.
Hadjuketal
(2013)39
Prospective
observational
cohortstudy
Patients
hospitalized
with
prim
ary
orsecondary
diagnosis
ofHF
Meanage,71y
Notgiven
287(49.7%
)5word
immediate
anddelayed
memory
test
(MoCA),
ControlledOral
Word
Association
Test,DSST
EHFScBS-9
Memory,processingspeed,and
executive
functionwere
impairedin
33.3%
,40.0%
,and
56.0%
ofpatients,respectively;
more
thanthree-quarters
(79%
)ofpatients
were
impairedin
at
least
1ofthe3domains.Overall
cognitive
statuswas
notassociated
withperform
ance
ofself-care
activities
inmultivariableadjusted
regressionmodels;however,
impairmentin
specificdomains
affectedself-care.
n=577
Multiple
linear
regression
analysis
Screenedfor
delirium
5inpatient
facilities
inthe
UnitedStates
F:M
254:323
Memory
impairm
entwas
associated
withsignifican
tlypoorerself-care
(P=.006)("
=j1.87;95%
confiden
ceinterval,j3.20to
j0.54).Im
pairmentsin
processing
speedandexecutive
function
were
notsignificantlyassociated
withself-care
intheadjusted
models.
(continues)
Mild Cognitive Impairment and Self-care in Chronic HF 7
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
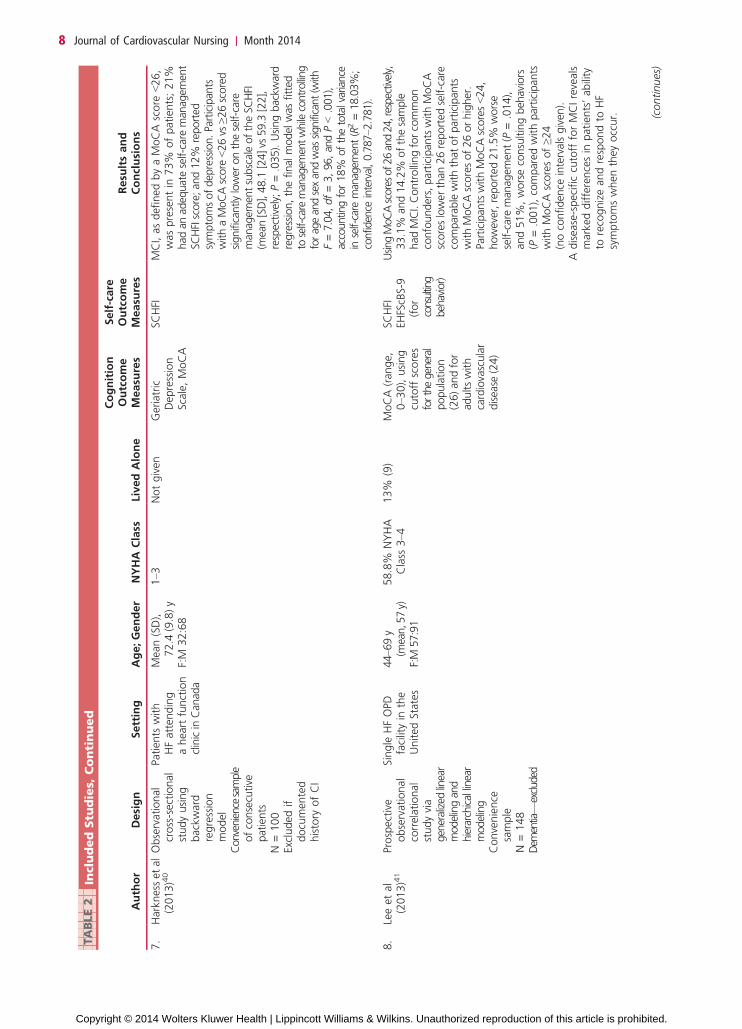
TABLE2
IncludedStu
dies,
Continued
Author
Design
Setting
Age;Gender
NYHA
Class
LivedAlone
Cognition
Outcome
Measu
res
Self-care
Outcome
Measu
res
Resu
ltsand
Conclusions
7.
Harkness
etal
(2013)40
Observational
cross-sectional
studyusing
backward
regression
model
Patients
with
HFattending
aheartfunction
clinicinCan
ada
Mean(SD),
72.4
(9.8)y
1Y3
Notgiven
Geriatric
Depression
Scale,MoCA
SCHFI
MCI,asdefinedbyaMoCAscore
G26,
waspresentin
73%
ofpatients;21%
had
anad
equateself-careman
agem
ent
SCHFIscore;an
d12%
reported
symptomsofdep
ression.Participan
tswithaMoCAscore
G26vs
Q26scored
significan
tlylower
ontheself-care
man
agem
entsubscaleoftheSC
HFI
(mean[SD],48.1
[24]vs
59.3
[22],
respectively;P=.035).Usingbackw
ard
regression,thefinal
model
was
fitted
toself-caremanagem
entwhile
controlling
forageandsexandwas
significant(with
F=7.04,df=3,96,andPG.001),
accountingfor18%
ofthetotalvariance
inself-care
managem
ent(R2=18.03%;
confidence
interval,0.787Y2
.781).
Convenience
sample
ofconsecutive
patients
F:M
32:68
N=100
Excludedif
documented
history
ofCI
8.
Leeetal
(2013)41
Prospective
observational
correlational
studyvia
generalized
linear
modelingand
hierarchicallinear
modeling
Single
HFOPD
facilityin
the
UnitedStates
44Y6
9y
(mean,57y)
F:M
57:91
58.8%
NYHA
Class
3Y4
13%
(9)
MoCA(range,
0Y3
0),using
cutoffscores
forthegeneral
population
(26)andfor
adultswith
cardiovascular
disease
(24)
SCHFI
UsingMoCAscoresof26and24,respectively,
33.1%
and14.2%
ofthesample
hadMCI.Controllingforcommon
confounders,participantswithMoCA
scoreslowerthan
26reported
self-care
comparablewiththat
ofparticipan
tswithMoCAscoresof26orhigher.
ParticipantswithMoCAscoresG24,
however,reported21.5%
worse
self-care
man
agem
ent(P
=.014),
and51%,worseconsultingbehaviors
(P=.001),comparedwithparticipants
withMoCAscoresofQ24
(noconfidence
intervalsgiven
).
Convenience
sample
N=148
EHFScBS-9
(for
consulting
behavior)
Adisease-specificcutoff
forMCIreveals
markeddifferencesin
patients’ability
torecognizeandrespondto
HF
symptomswhentheyoccur.
Dem
entiaV
excluded
(continues)
8 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE2
IncludedStu
dies,
Continued
Author
Design
Setting
Age;Gender
NYHA
Class
LivedAlone
Cognition
Outcome
Measu
res
Self-care
Outcome
Measu
res
Resu
ltsand
Conclusions
9.
Riegeletal
(2007)42
Cross-sectional
mixed-m
ethods
designusing
extremecase
sampling
Single
HF
OPDfacility
intheUnited
States
Givenper
category
F:M
11:18
Majority
3Y4
21%
(6)
PMRTask
DSST
SCHFI
Patients
poorin
HFself-care
had
worsecognition,more
sleepiness,
higherdepression,andpoorerfamily
functioning.Theprim
aryfactors
distinguishingthose
goodvs
expert
inself-careweresleepinessandfamily
engagem
ent(althoughnotestsof
statisticalsignificance
wereconducted).
N=29
Patientswith
severely
impairedcognition
wereexcluded.
Studythatfoundnostatistically
significantcorrelationbetw
eenCIandpoorercomprehensive
self-care
activity
10.
Dicksonetal
(2011)43
Concurrent
triangulation
mixed-m
ethods
design;contentand
correlationalanalysis
with
linearregression
2OPD
HFclinics
inalarge
urbanmedical
centerin
theUnited
States
25Y6
5y
(mean,49y)
F:M
15:26
41.5%
NYHA
Class
258.5%
NYHA
Class
3
Notgiven
DSST
PMR
DutchHeart
Failure
Knowledge
Scale
There
wasasignificantnegative
correlationbetw
eencognitive
function(DSST)andself-care
maintenance
(r=j0.33P=.03).
Purposive
homogenous
sampling
technique
Excluded
those
withdementiaor
neurologicalevent
SCHFI
95%
Confidence
intervalsareallnegative
(ie,d
onotcross0as
theothersdo),
sothisresultmaybeconsidered
significant,althoughtheconfid
ence
intervalsareverywide,suggestin
gpoorprecisiondueto
smallsam
ple
size
(n=41).Therewas
also
asignificant,negativecorrelationbetween
cognitive
function(PMR)andself-care
managem
ent(r=j0.39,P=.049),
indicatingthatworsecognitive
functionwas
associated
withbetter
self-care,
explained
inpartby
mixed
methodologyan
dthe
qualitativenarratives.Itcouldbe
that
someindividualswithMCI
overestim
ated
theirresponseson
theSC
HFI.Reexaminationofqualitative
resultsrevealed
that
socialsupport
(eg,spouses,children,andfriends)
playedim
portan
trolesin
self-care.
N=41
Excludetestsnot
welldescribedin
thesis
Abbreviations:
ADL,
activitiesofdaily
living;CI,cognitiveim
pairment;DSST,DigitSym
bolSubstitutionTest;EDS,excessivedaytim
esleepiness;EHFScBS-9,EuropeanHeartFailure
Self-care
BehaviourScale;
HF,
heartfailure;LN
S,LetterNumberSequencing;LO
C,loss
ofconsciousness;MA,medicationadherence;MCI,mild
cognitiveim
pairment;MMSE,Mini-MentalState
Examination;MoCA,MontrealCognitive
Assessment;NYHA,New
York
Heart
Association;OPD,outpatient;PMR,ProbedMemory
Recall;
PVT,PsychomotorVigilance
Task;SCHFI,Self-care
inHeartFailure
Index;
TMT,TrailMakingTest.
Mild Cognitive Impairment and Self-care in Chronic HF 9
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

adherence was found to be adversely affected by MCI35Y37;however, although the fourth38 found a relationshipbetween the cognitive function of attention, as measuredby the Psychomotor Vigilance Test, results indicated thatexcessive daytime sleepiness, rather than measured cog-nitive status, is more influential on medication adherence.These findings suggest that the concepts and measure-ment of cognitive function and excessive daytime sleep-iness may require further study to untangle their relativeinfluence.
A further 5 studies25,39Y42 used the Self-care Heart Fail-ure Index or European Heart Failure Self-care BehaviourScale to measure self-care and demonstrated a statisticallysignificant association between MCI and an adverse ef-fecton self-careactivities. Four studies25,39Y41 had relativelylarge samples (n = 93Y577) and reported a statisticallysignificant negative association between MCI (based onMoCA score) and self-care management and help-seekingbehaviors. The other study in this grouping, a mixed-methods descriptive study,42 had a smaller sample size(n = 29), and although reporting that ‘‘Patients poor inHF self-care had worse cognition, more sleepiness, higherdepression, and poorer family functioning’’ (p. 235), onlymean scores for each type of patient (poor, good, ex-pert in self-care) were provided and statistical testingfor differences in scores between patient types was notconducted,
Impaired Cognitive Function Is Not Relatedto Poorer Self-care
Despite the significant association between MCI andself-care described above, 1 study43 did not detect thisrelationship.
Dickson et al43 acknowledge the ‘‘surprising’’ findingof a negative correlation between their measures of cog-nitive function and self-care, indicating that poorer cog-nitive function improves self-care ability, which is intuitivelyperverse. However, this mixed-methods study had asmall sample (n = 41) of relatively young (25Y65 years)participants, which may affect the generalizability of find-ings. In addition, the authors note, ‘‘It could be that someindividuals with MCI overestimated their responses onthe SCHFII Re-examination of qualitative results rev-ealed that social support (eg, spouses, children, and friends)played important roles in self-care’’ (p. 183).
Discussion
Despite the established relationship between HF andcognitive impairment, there is a limited body of evidenceinvestigating the association between MCI and self-carein HF; sensitive measurement of both MCI and self-carecan be challenging, and the lack of consistency in thetools used in existing studies hampers the synthesis or
comparison of findings. In addition, the quality of thestudies reviewed here may have been affected in somecases by the use of small convenience samples drawnfrom single sites and the use of multiple regression whereexplanatory variables were not conditioned to removeimplicit bias, as discussed below.
In relation to the influence of sample size, the resultsof studies reported here have been obtained largelythrough the use of various regression methodologies.Regression is an appropriate methodology and buildson the concept that changes in explanatory variablestypically generate proportionate changes in the outcome(or response) process. Broadly speaking, the accuracywith which a regression coefficient is identified is pro-portional to the square root of the sample size; only themost influential explanatory variables are likely to beidentified from small samples. On the basis of the rec-ommendations of Good and Hardin,44 judging by thesample sizes and number of explanatory variables usedin the included articles, at least 2 studies,37,43 may havesome multiple regressions that were potentially tooambitious.
One potential weakness in a number of the arti-cles25,36,41Y43 under review is the absence of multipleregressions in which the explanatory variables are con-ditioned to remove implicit bias; when investigating thedependence of self-care on explanatory variables, a hier-archical multiple regression is preferable, where the ex-planatory variables are modified, or conditioned, to removethe effect of explanatory variables that potentially intro-duce bias, for example, age, gender, depression, and ex-cessive daytime sleepiness.
There are challenges in measuring both cognitive func-tion and self-care in HF; the reported studies used a widevariety of tools to measure cognitive function, limitingcomparability and preventing meta-analysis. The MMSEwas used in combination with other cognitive tests in2 of the studies25,35 included in this review. The MMSEis not sensitive for detecting MCI that impacts on self-care in HF,21Y25 and studies exploring the relationshipbetween cognitive function and self-care need to sup-plement the MMSE with cognitive tests sensitive to MCI.The MoCA has been shown to be a more sensitiveindicator of MCI in HF.26 The 4 studies25,39Y41 that usedMoCA demonstrated an association between MCI andpoorer self-care.
Self-care measures in all studies were self-reports,and, as acknowledged by some authors38,43 reviewedhere, individuals may not reliably report self-care, witheither overreporting or underreporting of ability orlack of acknowledgement of the role of carers in sup-porting self-care activities, particularly when MCI ispresent.
Finally, evidence presented in some studies suggeststhat predictors of poor self-care are more complexthan MCI alone with depression and excessive daytime
10 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

sleepiness also being implicated and their relative influ-ence difficult to untangle from cognitive function.
Conclusions
This systematic review and narrative synthesis has founda growing body of evidence regarding the associationbetween MCI and adverse effects on self-care in HF,either in its broadest sense or more specifically in re-lation to medication adherence. Although some of theresearch conducted thus far may have limitations dueto small sample size and design, the stronger evidence(produced by the use of a wider range of more sensitivemeasures of MCI, within larger sample studies) sug-gests that MCI does adversely affect self-care; however,this is based on findings from only 9 studies, 4 of whichrelate specifically to medication adherence. Further re-search using sensitive measures to detect MCI in ap-propriately selected and sized samples for multiple/hierarchical regressions is warranted. While acknowl-edging the limitations of the studies included in this re-view, nevertheless, our report represents a useful state ofbest evidence in this important aspect of HF.
These findings have implications for clinical practice.It is known that HF patients have difficulty with self-care and the influence of cognitive function needs to beconsidered when providing professional support for self-care in HF, with further research to determine the fea-sibility and acceptability of cognitive assessment inroutine clinical care. Once MCI is recognized, tailoredstrategies should be developed and evaluated to helppatients adapt to the increased challenges in self-carecaused by MCI, to improve clinical outcomes for thispatient group.
Acknowledgment
We acknowledge the support and advice offered by Pro-fessor Alex Clark, University of Alberta, in the prepara-tion of this article.
REFERENCES
1. ICD-10 [Database on the Internet]. World Health Orga-nization. 2010. http://apps.who.int/classifications/icd10/browse/2010/en#/I30-I52. Accessed February 3, 2012.
2. Zambroski C, Moser DK, Bhat G, Zeigler C. Impact ofsymptom prevalence and symptom burden on quality of lifein patients with heart failure. Eur J Card Nurs. 2005;4:198Y206.
3. McMurray JJ, Adamopoulos S, Anker SD, et al. ESC guide-lines for the diagnosis and treatment of acute and chronic heartfailure 2012: the Task Force for the Diagnosis and Treatmentof Acute and Chronic Heart Failure 2012 of the EuropeanSociety of Cardiology. Developed in collaboration with theHeart Failure Association (HFA) of the ESC. Eur Heart J.2012;14:803Y869.
4. Roger VL. Epidemiology of heart failure. Circ Res. 2013;113(6):646Y659. doi:10.1161/CIRCRESAHA.113.300268.
5. McCullough P, Philbin E, Spertus J, Kaatz S, Sandberg K,Weaver W. Confirmation of a heart failure epidemic: findingsfrom the Resource Utilization Among Congestive Heart Failure(REACH) study. J Am Coll Cardiol. 2002;39(1):60Y69.
6. Riegel B, Moser DK, Anker SD, et al. State of the science:promoting self-care in persons with heart failure: a scientificstatement from the American Heart Association. Circulation.2009;120(12):1141Y1163.
7. Riegel B, Dickson VV, Goldberg LR, Deatrick JA. Factorsassociated with the development of expertise in health failureself-care. Nurs Res. 2007;56(4):235Y243.
8. Silcock J. The Self Management of Heart Failure: A Placein Practice? [dissertation]. Leeds: University of Leeds; 2009.
9. Riegel B, Jaarsma T, Stromberg A. A middle-range theory ofself-care of chronic illness. ANS Adv Nurs Sci. 2012;35(3):194Y204.
10. Lainscak M, Blue L, Clark A, et al. Self-care managementof heart failure: practical recommendations from the PatientCare Committee of the Heart Failure Association of the EuropeanSociety of Cardiology. Eur J Heart Fail. 2011;13(2):115Y126.
11. Riegel B, Lee CS, Dickson VV, Carlson B. An update on theself-care of heart failure index. J Cardiovasc Nurs. 2009;24(6):485Y497.
12. Jaarsma T, Arestedt K, Martensson J, Dracup K, Stromberg A.The European Heart Failure Self-care Behaviour scale revisedinto a nine-item scale (EHFScB-9): a reliable and valid interna-tional instrument. Eur J Heart Fail. 2009;11:99Y105.
13. Harkness K, Heckman G, Akhtar-Danesh N, Gunn E, Demers C,McKelvie R. Cognitive function and self-management inolder patients with heart failure [published online aheadof print June 3, 2013]. Eur J Cardiovasc Nurs. doi:10.1177/1474515113492603.
14. Chertkow H, Nasreddine Z, Joanette Y. Mild cognitive im-pairment and cognitive impairment, no dementia, part A:concept and diagnosis. Alzheimer Dement. 2007;3(4):266Y282.
15. Petersen RC, Knopman DS, Boeve BF, et al. Mild cognitiveimpairment: tenyears later.ArchNeurol. 2009;66(12):1447Y1455.
16. Bennett SJ, Sauve MJ. Cognitive deficits in patients with heartfailure: a review of the literature. J Cardiovasc Nurs. 2003;18(3):219Y242.
17. Pressler SJ. Cognitive functioning and chronic heart failure:a review of the literature (2002YJuly 2007). J Cardiovasc Nurs.2008;23(3):239Y249.
18. Vogels RL, Scheltens P, Schroeder-Tanka JM, Weinstein HC.Cognitive impairment in heart failure: a systematic review ofthe literature. Eur J Heart Fail. 2007;9(5):440Y449.
19. Athilingam P, King KB. Heart and brain matters in heart failure:a literature review. J N Y State Nurses Assoc. 2007;38(2):13Y19.
What’s New and Important
h This article represents a useful and important ‘‘stateof best evidence’’ on the association between MCI andself-care in HF.
h The evidence for such an association is limited at present;however, 8 studies that used larger samples and moresensitive indicators of MCI found a statistically significantassociation suggesting that MCI has an adverse impacton self-care in HF.
h We recommend further research to investigate thefeasibility and acceptability of routine assessment ofcognitive function in HF patients to enable practitionersto tailor interventions to support self-care in the presenceof MCI.
Mild Cognitive Impairment and Self-care in Chronic HF 11
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

20. Folstein M, Folstein S, McHugh P. ‘‘Mini-mental state’’: apractical method for grading the cognitive state of pa-tients for the clinician. J Psychiatric Res. 1975;12(3):189Y198.
21. Riegel B, Bennett JA, Davis A, et al. Cognitive impairmentin heart failure: issues of measurement and etiology. Am JCrit Care. 2002;11(6):520Y528.
22. Tombaugh T, McIntyre N. The Mini-Mental State Examina-tion: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922Y935.
23. Bauer LC, Johnson JK, Pozehl BJ. Cognition in heart failure:an overview of the concepts and their measures. J Am AcadNurs Pract. 2011;23(11):577Y585.
24. Athilingam P, King KB, Burgin S, Ackerman M, Cushman L,Chen L. Montreal Cognitive Assessment and Mini-mentalStatus Examination compared as cognitive screening toolsin heart failure. Heart & Lung. 2011;40(6):521Y529.
25. Cameron J, Worrall-Carter L, Page K, Riegel B, Lo SK,Stewart S. Does cognitive impairment predict poor self-carein patients with heart failure? Eur J Heart Fail. 2010;12(5):508Y515.
26. Nasreddine Z, Phillips N, Bedirian V, et al. The MontrealCognitive Assessment, MoCA: a brief screening tool for mildcognitive impairment. J AmGeriatr Soc. 2005;53(4):695Y699.
27. Athilingam P. Validation of an Instrument to Measure Cog-nitive Function in PatientsWith Heart Failure [dissertation].Rochester, NY: University of Rochester School of Nursing;2008.
28. Cameron J, Worrall-Carter L, Page K, Stewart S, Ski C.Screening for mild cognitive impairment in patients with heartfailure: Montreal Cognitive Assessment versus Mini MentalState Exam.Eur J Cardiovasc Nurs. 2012;11(2). doi: 10.1177/1474515111435606.
29. Harkness K, Demers C, Heckman GA, McKelvie RS. Screen-ing for cognitive deficits using the Montreal Cognitive Assess-ment tool in outpatients 9=65 years of age with heart failure.Am J Cardiol. 2011;107(8):1203Y1207.
30. Bauer LC, Pozehl B, Hertzog M, Johnson JA, Zimmerman L,Filipi M. A brief neuropsychological battery for use in chronicheart failure population. Eur J Cardiovasc Nurs. 2012;11:23.doi:10.1016/j.ejcnurse.2011.03.007.
31. Vogels RL, Oosterman JM, van Harten B, et al. Profile ofcognitive impairment in chronic heart failure. J Am GeriatrSoc. 2007;55(11):1764Y1770.
32. Dickson VV, Tkacs N, Riegel B. Cognitive influences on self-care decision making in persons with heart failure.AmHeart J.2007;154(3):424Y431.
33. Sloan RS, Pressler SJ. Cognitive deficits in heart failure: re-cognition of vulnerability as a strange new world. J CardiovascNurs. 2009;24(3):241Y248.
34. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA state-ment for reporting systematic reviews and meta-analyses ofstudies that evaluate health care interventions: explanationand elaboration. PLOS Med. 2009;7:e1000100. doi:http://dx.doi.org/10.1136/bmj.b2700.
35. Alosco ML, Spitznagel MB, Cohen R, et al. Cognitive im-pairment is independently associated with reduced instrumen-tal activities of daily living in persons with heart failure.J Cardiovasc Nurs. 2012;27(1):44Y50.
36. Alosco ML, Spitznagel MB, Naftali R, et al. Executive dys-function is independently associated with reduced functionalindependence in heart failure. J Clin Nurs. 2013;23:829Y836.
37. Hawkins LA, Kilian S, Firek A, Kashner TM, Firek CJ, Silvet H.Cognitive impairment and medication adherence in outpatientswith heart failure. Heart Lung. 2012;41(6):572Y582.
38. Riegel B, Moelter ST, Ratcliffe SJ, et al. Excessive daytimesleepiness is associated with poor medication adherence inadults with heart failure. J Card Fail. 2011;7(4):340Y348.
39. Hadjuk AM, Lemon SC, McManus DD, et al. Cognitiveimpairment and self-care in heart failure. Clin Epidemiol.2013;5:407Y416.
40. Harkness K, Heckman GA, Akhtar-Danesh N, Demers C,Gunn E, McKelvie RS. Cognitive function and self-caremanagement in older patients with heart failure [publishedonline ahead of print June 3, 2013]. Eur J Cardiovasc Nurs.doi:10.1177/1474515113492603.
41. Lee CS, Gelow JM, Bidwell JT, et al. Blunted responses toheart failure symptoms in adults with mild cognitive dysfunc-tion. J Cardiovasc Nurs. 2013;28(6):534Y540. doi:10.1097/JCN.0b013e31826620fa.
42. Riegel B, Vaughan Dickson V, Goldberg LR, Deatrick JA.Factors associated with the development of expertise in heartfailure self-care. Nurs Res. 2007;56(4):235Y243.
43. Dickson VV, Lee CS, Riegel B. How do cognitive functionand knowledge affect heart failure self-care? J Mixed MethodsRes. 2011;5(2):167Y189.
44. Good PI, Hardin JW. Common Errors in Statistics (andHow to Avoid Them). 3rd ed. Hoboken, NJ: Wiley; 2009.
12 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Copyright © 2022 FDOKUMEN




















