Late-life depression, mild cognitive impairment, and dementia: possible continuum?
19
Late-Life Depression, Mild Cognitive Impairment, and Dementia: Possible Continuum? Francesco Panza, M.D., Ph.D., Vincenza Frisardi, M.D., Cristiano Capurso, M.D., Ph.D., Alessia D’Introno, Ph.D., Anna M. Colacicco, Ph.D., Bruno P. Imbimbo, Ph.D., Andrea Santamato, M.D., Gianluigi Vendemiale, M.D., Davide Seripa, Ph.D., Alberto Pilotto, M.D., Antonio Capurso, M.D., Vincenzo Solfrizzi, M.D., Ph.D. Clinical and epidemiologic research has focused on the identification of risk factors that may be modified in predementia syndromes, at a preclinical and early clinical stage of dementing disorders, with specific attention to the role of depression. Our goal was to provide an overview of these studies and more specifically to describe the prevalence and incidence of depression in individuals with mild cognitive impair- ment (MCI), the possible impact of depressive symptoms on incident MCI, or its progression to dementia and the possible mechanisms behind the observed associa- tions. Prevalence and incidence of depressive symptoms or syndromes in MCI vary as a result of different diagnostic criteria and different sampling and assessment procedures. The prevalence of depression in individuals with MCI was higher in hospital-based studies (median: 44.3%, range: 9%– 83%) than in population-based studies (median: 15.7%, range: 3%– 63%), reflecting different referral patterns and selection criteria. Incidence of depressive symptoms varied from 11.7 to 26.6/100 person-years in hospital-based and population-based studies. For depressed normal subjects and depressed patients with MCI, the findings on increased risk of incident MCI or its progression to dementia were conflicting. These contrasting findings suggested that the length of the follow-up period, the study design, the sample population, and methodological differences may be central for detecting an associ- ation between baseline depression and subsequent development of MCI or its pro- gression to dementia. Assuming that MCI may be the earliest identifiable clinical stage of dementia, depressive symptoms may be an early manifestation rather than a risk factor for dementia and Alzheimer disease, arguing that the underlying Received September 3, 2008; revised May 13, 2009; accepted May 21, 2009. From the Department of Geriatrics, Center for Aging Brain, Memory Unit, University of Bari, Bari (FP, VF, AD’I, AMC, AC, VS); Department of Geriatrics, University of Foggia, Foggia (CC, GV); Research and Development Department, Chiesi Farmaceutici, Parma (BPI); Department of Physical Medicine and Rehabilitation, University of Foggia, Foggia (AS); and Department of Medical Sciences, Geriatric Unit and Gerontology-Geriatrics Research Laboratory, IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo, Foggia (DS, AP), Italy. Send correspondence and reprint requests to Francesco Panza, M.D., Ph.D., Department of Geriatrics, Center for Aging Brain, Memory Unit, University of Bari, Policlinico, Piazza Giulio Cesare, Bari 11-70124, Italy. e-mail: [email protected] © 2009 American Association for Geriatric Psychiatry Am J Geriatr Psychiatry ●:●, ●●● 2009 1
Transcript of Late-life depression, mild cognitive impairment, and dementia: possible continuum?

Late-Life Depression, Mild CognitiveImpairment, and Dementia: Possible
Continuum?
Francesco Panza, M.D., Ph.D., Vincenza Frisardi, M.D.,Cristiano Capurso, M.D., Ph.D., Alessia D’Introno, Ph.D.,
Anna M. Colacicco, Ph.D., Bruno P. Imbimbo, Ph.D.,Andrea Santamato, M.D., Gianluigi Vendemiale, M.D.,
Davide Seripa, Ph.D., Alberto Pilotto, M.D.,Antonio Capurso, M.D., Vincenzo Solfrizzi, M.D., Ph.D.
Clinical and epidemiologic research has focused on the identification of risk factorsthat may be modified in predementia syndromes, at a preclinical and early clinicalstage of dementing disorders, with specific attention to the role of depression. Ourgoal was to provide an overview of these studies and more specifically to describe theprevalence and incidence of depression in individuals with mild cognitive impair-ment (MCI), the possible impact of depressive symptoms on incident MCI, or itsprogression to dementia and the possible mechanisms behind the observed associa-tions. Prevalence and incidence of depressive symptoms or syndromes in MCI vary asa result of different diagnostic criteria and different sampling and assessmentprocedures. The prevalence of depression in individuals with MCI was higher inhospital-based studies (median: 44.3%, range: 9%–83%) than in population-basedstudies (median: 15.7%, range: 3%–63%), reflecting different referral patterns andselection criteria. Incidence of depressive symptoms varied from 11.7 to 26.6/100person-years in hospital-based and population-based studies. For depressed normalsubjects and depressed patients with MCI, the findings on increased risk of incidentMCI or its progression to dementia were conflicting. These contrasting findingssuggested that the length of the follow-up period, the study design, the samplepopulation, and methodological differences may be central for detecting an associ-ation between baseline depression and subsequent development of MCI or its pro-gression to dementia. Assuming that MCI may be the earliest identifiable clinicalstage of dementia, depressive symptoms may be an early manifestation rather thana risk factor for dementia and Alzheimer disease, arguing that the underlying
Received September 3, 2008; revised May 13, 2009; accepted May 21, 2009. From the Department of Geriatrics, Center for Aging Brain, MemoryUnit, University of Bari, Bari (FP, VF, AD’I, AMC, AC, VS); Department of Geriatrics, University of Foggia, Foggia (CC, GV); Research andDevelopment Department, Chiesi Farmaceutici, Parma (BPI); Department of Physical Medicine and Rehabilitation, University of Foggia, Foggia(AS); and Department of Medical Sciences, Geriatric Unit and Gerontology-Geriatrics Research Laboratory, IRCCS Casa Sollievo della Sofferenza,San Giovanni Rotondo, Foggia (DS, AP), Italy. Send correspondence and reprint requests to Francesco Panza, M.D., Ph.D., Department ofGeriatrics, Center for Aging Brain, Memory Unit, University of Bari, Policlinico, Piazza Giulio Cesare, Bari 11-70124, Italy. e-mail:[email protected]
© 2009 American Association for Geriatric Psychiatry
Am J Geriatr Psychiatry ●:●, ●●● 2009 1

neuropathological condition that causes MCI or dementia also causes depressivesymptoms. In this scenario, at least in certain subsets of elderly patients, late-lifedepression, MCI, and dementia could represent a possible clinical continuum. (Am JGeriatr Psychiatry 2009; ●:000–000)
Key Words: Dementia, depression, epidemiology, mild cognitive impairment, prede-mentia syndromes
The transitional phase between mild nondisablingcognitive decline and disabling dementia is an
ambiguous diagnostic period during which it is un-clear whether mild cognitive deficits predict incipi-ent dementia or not. In this article, we will use theterm “predementia syndrome” to identify all condi-tions with age-related deficits in cognitive functionreported in the literature, including a mild stage ofcognitive impairment based on normal or patholog-ical conditions considered predictive or early stagesof dementia.1,2 Such predementia syndromes havebeen defined for Alzheimer disease (AD) but have notyet been operationalized for vascular dementia (VaD)and other specific forms of dementia. However, not allthese conditions are progressive (e.g., dementing), butthey may be stable or also reversible.1,2 Neuropsychi-atric symptoms may accompany these predementiasyndromes and help in identifying incipient dementia.In particular, in older adults, depression may be asso-ciated with an increased risk for dementia. It may be ofcrucial interest to determine what presentations of pre-dementia syndromes and depression are progressive/dementing and which are not.
First aim of this review article was to summarizethe findings of the studies of depressive symptomsor depression in patients with mild cognitive impair-ment (MCI) and other predementia syndromes. Fur-thermore, we attempted to clarify the relationshipsamong late-life depression, MCI, and dementia, re-viewing studies that examined the possible impact ofdepressive symptoms on incident MCI or its progres-sion to dementia, as well as the possible mechanismsbehind the observed associations. We reviewed clin-ical and epidemiologic studies from the English lit-erature published before September 2008, includingstudies that provided a description of the MCI ordepression diagnostic criteria used or describingthe means of collecting depressive symptoms. We
searched through the PubMed database of NationalCenter for Biotechnology Information (available at:http://www.ncbi.nlm.nih.gov) by author and thefollowing keywords: mild cognitive impairment, de-pression, depressive symptoms, predementia syn-dromes, prodromal Alzheimer disease, and MCI.Using the PubMed search engine, we found 37 peer-reviewed works that satisfied our inclusion criteria.The relevance of the aims of this review was under-lined in a recent article, the proceedings of the 2003National Institute of Mental Health (NIMH) confer-ence “Perspectives on Depression, Mild CognitiveImpairment, and Cognitive Decline.”3 The principalobjectives of the meeting were to examine how wemight better integrate the varied perspectives on as-sociations among depression, MCI, and cognitive de-cline and to illuminate the common or distinct mech-anisms involved in these associations.3
Predementia Syndromes and MCI
Many different diagnostic criteria and terms havebeen proposed over the years to describe predemen-tia syndromes in the elderly: age-associated memoryimpairment, aging-associated cognitive decline, cog-nitive impairment no dementia, and many others.1,2
Furthermore, numerous rating scales for staging de-mentia include a specific preclinical phase of demen-tia, e.g., “questionable dementia” in Clinical Demen-tia Rating Scale (0.5).4 At present, MCI is a clinicallabel that includes nondemented aged persons withmemory impairment and no significant disability.5–8
The criteria for MCI, as defined by Petersen et al. in1997, include: 1) memory complaint, 2) objectivememory disorder, 3) absence of other cognitive dis-orders or repercussions on daily life, 4) normal gen-eral cognitive function, and 5) absence of dementia.8
In 1997, the emphasis was placed on the compulsory
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 20092

presence of memory complaint and memory disor-der.8 In 1999, these criteria were clarified, with MCIdefined solely in clinical terms.5 The absence of im-paired cognitive function in a domain other thanmemory is also required. The more recently pro-posed multiple subtypes of MCI were intended toreflect the heterogeneity of different types of demen-tia. Actually, there are at least three different subclas-sifications of MCI according to its cognitive features,8
clinical presentation,7 and probable etiology.1 Thereis now ample evidence that MCI is often a pathology-based condition with a high rate of progression toAD.1,2 MCI definitions can be broadly classified asamnestic (aMCI) and nonamnestic (naMCI). There-fore, aMCI, with a central role for memory disorderand with relative preservation of other cognitive do-mains, was identified as the predementia syndromefor AD. aMCI can be subdivided into a single do-main subtype with a pronounced memory deficit ora multiple-domain subtype that includes memoryimpairment along with some impairment in othercognitive domains such as language, executive func-tion, and visuospatial skills.8 The other major MCIsubtype is naMCI, which similarly can be subdividedinto single and multiple-domain subtypes.8 More-over, MCI can be further classified in different sub-types according to its cognitive features (dysexecu-tive MCI and aMCI8) or clinical presentations (MCIwith parkinsonism, cerebrovascular disease [CVD],depressive symptoms, or behavioral and psycholog-ical symptoms).7 Different MCI subtypes can be de-fined by probable etiology: MCI-AD, vascular MCI,or MCI-Lewy body dementia.1 A critical review re-cently took place in Stockholm, then in Montreal todefine a new consensus on MCI.7,9 Modification ofPetersen’s criteria5,8 was proposed during the confer-ence in Montreal, which was to not require the subjec-tive memory impairment criterion and intact instru-mental activities of daily living (Table 1). The EuropeanConsortium on Alzheimer’s Disease working group onMCI has very recently proposed a novel diagnosticprocedure with different stages, combining neuropsy-chological evaluation and family interview to detectMCI at the earliest possible stage10 (Table 1).
Late-Life Depression
In adults older than 65 years, late-life depressionrefers to depressive syndromes defined in the Diag-
nostic and Statistical Manual of Mental Disorders,4th Edition (DSM-IV11) and in the International Clas-sification of Disease-10 (ICD-1012) as a mood disor-der with symptoms of sadness, negative self-regard,loss of interest in life, and disruptions of sleep, ap-petite, thinking, and energy level for more than 2weeks that interfere with daily living. Late-life de-pression encompasses both late-onset cases and early-onset cases that recur or continue into later years oflife. Various studies present an age range from 45 to65 years as the lower limit for defining late age ofdepression onset.13 Late-life depressive syndromesoften arise in the context of medical and neurologicdisorders.14 The prevalence of major depressive disor-der (MDD) is about 17% in patients with AD15 and iseven higher in those with subcortical dementias.16 TheU.S. NIMH has developed provisional criteria for thediagnosis of depression in individuals with AD to iden-tify the problem and to promote research into the dis-order17 (Table 2). Several studies suggesting depression
TABLE 1. Proposed General Criteria for Mild CognitiveImpairment (MCI) According to theInternational Working Group on MCI7 and tothe MCI Working Group of the EuropeanConsortium on Alzheimer Disease10
International WorkingGroup on MCI Criteria
European Consortium onAlzheimer’s Disease MCIWorking Group Criteria
1. Not normal, notdemented; does not meetcriteria (DSM-IV, ICD 10)for a dementia syndrome
1. Cognitive complaintemanating from the patientand/or his/her family
2. Cognitive decline 2. The subject and/or informantreport a decline in cognitivefunctioning relative toprevious abilities during thepast year
3. Self and/or informantreport and impairment onobjective cognitive tasksand/or evidence of declineover time on objectivecognitive tasks
3. Cognitive disorders evidencedby clinical evaluation:impairment in memory and/oranother cognitive domain
4. Preserved basic activitiesof daily living/minimalimpairment in complexinstrumental functions
4. Cognitive impairment doesnot have major repercussionson daily life. However, thesubject may report difficultiesconcerning complex day-to-day activities
5. No dementia
Notes: Modified from J Intern Med7 and J Neurol Neurosurg.10
DSM-IV: Diagnostic and Stastical Manual of Mental Disorders, 4thEdition; ICD-10: International Statistical Classification of Diseases andRelated Health Problems, 10th Revision.
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 3

as a risk factor for dementia are based on early-onsetrecurrent or chronic depression rather than on depres-sion occurring for the first time shortly before the de-mentia is manifested.18 In fact, research suggests thatearly-onset depression that is untreated or recurrent isassociated with volume loss in the hippocampus13 andpossibly contributes to dysfunction of the hypothalam-ic-pituitary-adrenal-stress axis.19 On the other hand, ingeneral, individuals who present with first onset ofdepression in late life have the higher relative risk ofdeveloping some form of dementia.14
There is a general consensus on a syndromal ap-proach to depression, calling on DSM-IV,11 to iden-
tify symptom clusters such as MDD. In MDD, the useof structured clinical interviewing as the StructuredClinical Interview for DSM-IV allows data acquisi-tion from many sources about past and current psy-chiatric symptoms and about past and current Axis Idiagnoses.20 However, in the elderly, other depres-sion subtypes may be important to the relationshipwith functional disability and cognitive impairmentas MDD, including subsyndromal depression inwhich symptoms are present intermittently21 andnondysphoric depression in which feelings of sad-ness are denied.22 In this article, depression will referto clinically significant depressive symptoms andsubsumes MDD, dysthymia, and subsyndromal andother subtypes of depression.3 Furthermore, in manystudies of cooccurrence of cognitive impairment anddepression, the use of lengthy structured interviewssuch as the Structured Clinical Interview for DSM-IVis impractical, and researchers often struggle to iden-tify briefer instruments that aid in diagnosis and cantrack severity of symptoms.3 There are several in-struments that are useful for identifying symptomsconsistent with depression.13 The Geriatric Depres-sion Scale (GDS) was developed and validated spe-cifically for use with older adults, avoiding somaticand sexual symptoms, evaluating subjective experi-ence of cognitive impairment, and using a simple yesor no response format that decreases cognitive bur-den.23 There are 15- and 30-item versions of the GDS(GDS-15 and GDS-30), with sensitivities of 80%–100%.13 A very recent study demonstrated that theGDS-30 is a reliable screening tool for depressivesymptoms in MCI but not in patients with AD.24
Another widely used instrument is the Center forEpidemiological Studies Depression Scale (CES-D)composed of 20 items in a multiple-choice format.25
It also developed a 10-item modified version witha dichotomous response scale to avoid confusionamong depressed elderly subjects with the multiple-choice format, with comparable sensitivity and spec-ificity to the full version.26 The Beck Depression In-ventory is a widely used self-report questionnaire,not developed specifically for older adults but poten-tially useful, because item content was developed toconform to DSM-IV diagnostic criteria for depres-sion.27 The approach to screening for depression incognitively impaired individuals also depends inpart on the level of cognitive impairment, and formost subjects with even MCI, information from a
TABLE 2. Provisional Diagnostic Criteria for Depressionof Alzheimer Disease17
A. Three (or more) of the following symptoms have been presentduring the same 2-week period and represent a change fromprevious functioning: at least one of the symptoms is either 1)depressed mood or 2) decreased positive affect or pleasure1. Clinically significant depressed mood (e.g., depressed, sad,
hopeless, discouraged, and tearful)2. Decreased positive affect or pleasure in response to social
contacts and usual activities3. Social isolation or withdrawal4. Disruption in appetite5. Disruption in sleep6. Psychomotor changes (e.g., agitation or retardation)7. Irritability8. Fatigue or loss of energy9. Feelings of worthlessness, hopelessness, or excessive or
inappropriate guilt10. Recurrent thoughts of death, suicidal ideation, plan, or
attemptB. All criteria are met for dementia of the Alzheimer type (DSM-
IV-TR)C. The symptoms cause clinically significant distress or disruption
in functioningD. The symptoms do not occur exclusively during the course of a
deliriumE. The symptoms are not due to the direct physiological effects of
a substance (e.g., a drug of abuse or a medication)F. The symptoms are not better accounted for by other conditions
such as major depressive disorder, bipolar disorder,bereavement, schizophrenia, schizoaffective disorder, psychosisof Alzheimer disease, anxiety disorders, or substance-relateddisorder
Specify ifCooccurring onset: if onset antedates or cooccurs with the AD
symptomsPost-AD onset: if onset occurs after AD symptoms
SpecifyWith psychosis of Alzheimer diseaseWith other significant behavioral signs or symptomsWith history of mood disorder
Notes: Modified from Am J Geriatr Psychiatry.17 DSM-IV-TR: Di-agnostic and Statistical Manual of Mental Disorders, 4th Edition-TextRevision.
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 20094

reliable informant is necessary to assess depression.The Cornell Scale for Depression in Dementia wasdesigned for use in dementia and specifically in-cludes caregivers in the evaluation.28 The Neuropsy-chiatric Inventory (NPI) is an informant-based inter-view that assesses neuropsychiatric disturbancescommonly seen in patients with dementia.29 Otherclinician-based instruments that have been used instudies on MCI and other predementia syndromesinclude the Hamilton Depression Rating Scale(HDRS),30 the Montgomery-Asberg Depression Rat-ing Scale (MADRS),31 the Comprehensive Psycho-pathological Rating Scale,32 the Goldberg DepressionScale,33 and the Consortium to Establish a Registryfor Alzheimer’s Disease Behavioral Rating Scale forDementia.34 These instruments are suitable for usewith cognitively impaired individuals, but these re-quire training to achieve acceptable reliability foradministration and scoring.13
PREVALENCE AND INCIDENCE OF DEPRESSIONIN PREDEMENTIA SYNDROMES
Prevalence of Depression in Patients With MCI
Depression has often been excluded from the def-inition of MCI, creating a bias in studies on therelationship of depression with predementia syn-dromes. However, research now indicates a high rateof cooccurrence between depression and MCI thatseems to raise the risk for persistent cognitive im-pairment and dementia.13 Among population-basedstudies, in the Italian Longitudinal Study on Aging(ILSA), the diagnosis of MCI was associated with ahigh prevalence of depressive symptoms, with ahigher prevalence of mild depressive symptoms(GDS-30: between 10 and 19 points). A prevalencerate of 63.3% of depressive symptoms among pa-tients with MCI was found: 49.3% had mild and14.0% had severe depressive symptoms (GDS-30 �20points).35 Findings have been inconsistent mainlybecause of different procedures in both assessmentof depression and MCI definition. In fact, the Car-diovascular Health Study (CHS) Cognition Studywas nested within the original CHS cohort, and asubset of demented patients and patients with MCIwere assessed with the NPI (Table 3). The CHS Cog-nition Study reported a cumulative prevalence of26% for depression among individuals with MCI
(amnestic or multiple-domain subtypes) relative to32% in demented subjects.36 Accepting some differ-ences in methodology, the prevalence rates of de-pressive symptoms assessed with the GDS-30 amongpatients with MCI in the ILSA were more than twicethat found in the CHS Cognition Study. In anotherstudy, those classified as MCI had an even lowerprevalence of depressive symptoms: only 15.7% as aNPI symptom in the past month.37 In the Kungshol-men project, a Swedish population-based study, thereported prevalence of depression (according toDSM–III–R criteria) in MCI was 10%: 20% reportedloss of initiative, 9% loss of interest, 9% suicidalthoughts, 4% depressive thoughts, and 11% reportedsadness, as rated using the Comprehensive Psycho-pathological Rating Scale 38 (Table 3). More recently,two Australian population-based studies assesseddepressive symptoms in patients with MCI.39,40 TheGoldberg Depression Scale demonstrated limitedsensitivity for detection of depressive symptoms inboth the patients with MCI (3%) and a healthy con-trol group (2%).39 Using DSM-IV criteria resulted insuperior sensitivity in diagnosing minor depressionin patients with MCI (17.2%) and control group(3.5%)40 (Table 3). In a Thai population-based study,patients with MCI had higher incidence of anxiety(53%) and dysphoria (46%) measured with the NPI,when compared with normal subjects. Althoughmarginally significant, apathy (12%) was also morecommon in patients with MCI41 (Table 3).
Among hospital-based studies, in a sample of vol-unteers who responded to advertisements for sub-jects, nondemented subjects (Clinical Dementia Rat-ing � 0.5) who progressed to AD had more depressivesymptoms and symptoms of personality changes (suchas agitation and passivity) at baseline than those whodid not progress to AD42 (Table 3). Hwang et al.,43
utilizing the NPI for behavioral assessment, foundthat the most significant differences between MCIand controls were mood symptoms, including dys-phoria, anxiety, and irritability. The larger study byGeda et al.44 reported the substantially lower rate of9% for depressive symptoms in MCI with the NPI,which was not statistically different from the rate innormal controls. These inconsistent results were de-rived from methodological differences, with differ-ent MCI diagnostic criteria used in these two case–control studies43,44 (Table 3) and with the exclusionof subjects who have concomitant untreated depres-
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 5

TABLE 3. Principal Prevalence Studies of Depressive Symptoms or Syndromes in Patients With Mild CognitiveImpairment (MCI)
Reference Setting and Study Design Subjects
Tools, Procedure, or Diagnostic
Criteria
Reported Prevalence
of Depressive
Symptoms or
Depression
Population-based studiesLyketsos et al.36 Cross-sectional, population
based
From a total of 3,608 participants,
824 individuals completed the
behavioral assessment. Of
these, 362 were demented,
320 were MCI, and 142 did not
meet criteria for MCI or
dementia
MCI criteria: �1.5 SD below age- and
education-adjusted norms on
standard neuropsychological tests,
and depressive symptoms
measured with the NPI
26%
Chan et al.37 Cross-sectional, population
based
A total of 454 subjects (dementia,
n � 333; MCI, n � 121) and
their knowledgeable
informants
MCI criteria: �1.5 SD on one test or
�1 SD on two or more tests
below age- and education-adjusted
norms on standard
neuropsychological tests and
depressive symptoms measured
with the NPI and BSRS
15.7%
Forsell et al.38 Cross-sectional, population
based
In a population of 443
nondemented persons aged 75
years and older, 89 fulfilled the
criteria of MCI and had
sufficient data from the
psychiatric examination
MCI criteria: 1 SD below age- and
education-adjusted norms on
MMSE score; depressive symptoms
measured with CPRS and
diagnoses of depression, anxiety
and psychosis were made
according to DSM-III-R
Depression: 11%;
depressive symptoms:
4%
Kumar et al.39,40 Cross-sectional, population
based
2,551 community-dwelling
individuals in the age range of
60–64 years
MCI criteria: SMC, objective memory
impairment (score 2 or below on
delayed CVLT), normal general
cognitive function (MMSE 26 or
above), intact ADL; depressive
symptoms measured with the
GoDS, depressive syndromes
diagnosed with DSM-IV
Depressive symptoms:
3%; minor
depression: 17.2%
Solfrizzi et al.35 Cross-sectional and longitudinal,
population based (3.5 years)
2,963 subjects from population-
register (including institutions)
aged from 65 to 84 years
MCI criteria: 1.5 SDs below mean
age- and education-adjusted on the
MMSE and 10th percentile below
age- and education-adjusted on
memory test, without SMC and
intact ADL/IADL); depressive
symptoms measured with the
GDS-30
63.3%
Muangpaisan et al.41 Cross-sectional, population
based
107 community-dwelling
individuals aged 50 years and
older diagnosed with MCI
(N � 77) and normal (N � 30)
MCI criteria: clinical diagnosis
according to Petersen’s criteria;
depressive symptoms measured
with the NPI
46%
Hospital-based studies
and clinical trialsLi et al.55 Cross-sectional and longitudinal,
case–control, hospital based
(3.5 years)
294 subjects at baseline: 19
patients with MCI followed up
for a mean of 3.5 years
MCI criteria: cognitive capacity
screening examination or MMSE
scores between 24 and 26;
depressive symptoms measured
with the HDRS
29%
Copeland et al.42 Cross-sectional and longitudinal,
convenience sample
recruited through
advertisements (3 years)
A total of 165 elderly individuals,
from 1,095 who were screened
MCI criteria: CDR � 0.5; depressive
symptoms measured with a
semistructured interview with
nine questions based on the DSM
III-R criteria
Questionable dementia
(stable CDR � 0.5):
43.5% of depressive
symptoms at baseline
converters (progressed
to probable AD):
45.5% of depressive
symptoms at baseline(Continued)
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 20096

TABLE 3. (Continued)
Reference Setting and Study Design Subjects
Tools, Procedure, or Diagnostic
Criteria
Reported Prevalence
of Depressive
Symptoms or
Depression
Hwang et al.3 Cross-sectional, hospital based Three age and education
comparable groups, i.e., 28
patients with MCI, 124 patients
with mild AD, and 50 normal
subjects
MCI criteria: �1.5 SD below age- and
education-adjusted norms on
standard neuropsychological tests;
depressive symptoms measured
with the NPI
39%
Feldman et al.49 Cross-sectional, clinical trial 1,010 patients with MCI MCI criteria: CDR � 0.5 and
impaired performance on NYU
delayed paragraph recall;
depressive symptoms measured
with the NPI
45%
Geda et al.44 Cross-sectional, hospital based Data collected on 514 normal
controls, 54 patients with MCI,
and 87 patients with mild AD
MCI criteria: clinical diagnosis
according to Petersen’s criteria;
depressive symptoms measured
with the NPI
9%
Gabryelewicz et al.46 Longitudinal, hospital based
(3 years)
102 patients with MCI MCI criteria: clinical diagnosis
according to Petersen’s criteria
and CDR � 0.5; depressive
symptoms measured with the
MADRS, depressive syndromes
diagnosed with DSM-IV
minor depression: 27%;
major depression: 20%
Lopez et al.45 Cross-sectional, hospital based A total of 655 subjects, of these
228 were patients with MCI
and 427 were probable
mild AD
MCI criteria: �1.5 SD below age- and
education-adjusted norms on
standard neuropsychological tests;
depressive symptoms measured
with the CERAD BRSD
53%
Rozzini et al.47 Cross-sectional, hospital based A total of 120 subjects were
analyzed: 94 of these were
classified as aMCI, and 26 as
naMCI
MCI criteria: cognitive complaint, no
dementia, intact general
functioning, objective impairment
in at least 1 of 4 cognitive
domains (cutoff of 1.5 SD with
normative corrections for age,
years of education, and sex). aMCI
criteria: memory impairment
either alone or with other
cognitive impairments (multiple
domains with amnesia); naMCI
criteria: single nonmemory domain
impaired alone or with other
nonmemory deficits (multiple
domains without amnesia);
depressive symptoms measured
with the NPI
MCI: 68.8%;
aMCI: 83%;
naMCI: 73.1%
Ellison et al.48 Cross-sectional, hospital based A total of 116 screened patients,
of these 59 were patients with
MCI (only 38 had also NPI
data). Twenty-two of these 38
patients with MCI met criteria
for aMCI, whereas 16 met
criteria for naMCI
MCI criteria: clinical diagnosis
according to Petersen’s criteria. A
diagnosis of aMCI required low
performance on the CVLT or a
six-item word list recall task,
whereas patients with naMCI
scored within the normal range on
the memory test but at least 1.5
SD below appropriate norms on
any of a series of nonmemory
cognitive tests; depressive
symptoms measured with NPI
MCI: 63.3%;
aMCI: 59.1%;
naMCI: 68.8%
Notes: BSRS: Behavior Symptom Rating Scale; MMSE: Mini-mental State Examination; CPRS: Comprehensive Psychopathological Rating Scale;SMC: subjective memory complaint; CVLT: California Verbal Learning Test; ADL: activities of daily living; GoDS: Goldberg Depression Scale; IADL:instrumental activities of daily living; CDR: Clinical Dementia rating Scale; NYU: New York University; CERAD BRSD: Consortium to Establish aRegistry for Alzheimer’s Disease Behavioral Rating Scale for Dementia.
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 7

sion in one of the studies.43 Another case–controlstudy reported a prevalence of 53% of depressivesymptoms among patients with MCI,45 using the Con-sortium to Establish a Registry for Alzheimer’s DiseaseBehavioral Rating Scale for Dementia and MCI criteriaidentical to those used by Hwang et al.43 (Table 3). Themost common depressive symptoms were hopeless-ness and crying spells, with crying spells more com-monly identified in patients with aMCI.45 In their MCIcohort, Gabryelewicz et al.46 showed that as almost halfof all patients met DSM-IV criteria for depression: 27%suffered from minor and 20% from MDD (Table 3). Themost common symptoms were sadness, poor concen-tration, inner tension, pessimistic thoughts, lassitude,and reduced sleep.
Furthermore, two very recent studies investigatedthe prevalence in MCI subtypes of neuropsychiatricsymptoms and particularly depression47,48 (Table 3).In fact, in another hospital-based study, about 85% ofpatients with aMCI had some neuropsychiatricsymptoms evaluated with the NPI, and the mostprevalent symptom was depression, followed byanxiety. A significantly higher prevalence of halluci-nations and sleep disorders has been observed in thenaMCI group in comparison with the aMCI group.47
Moreover, using NPI, depression/dysphoria (63.3%),apathy (60.5%), anxiety (47.4%), irritability (44.7%), andnighttime behaviors (42.1%) were the most frequentneuropsychiatric symptoms. Although depression/dysphoria was distributed similarly between aMCIand naMCI, apathy was significantly more fre-quently associated with aMCI, and nighttime behav-iors were more frequently associated with naMCI.48
In these two studies, there were no significant differ-ences in depression rates between patients withaMCI and naMCI.47,48 In a international multicenter,long-term, randomized, placebo-controlled clinicaltrial, the Investigation in the Delay to Diagnosis ofAD with Exelon trial, about 60% of patients withaMCI reported some neuropsychiatric symptomsassessed with the NPI and almost half of the grouphad reported depressive symptoms (�45%)49 (Table 3).
Prevalence of MCI in Depressed Patients
All the studies cited earlier examined the preva-lence of depression or depressive symptoms in pa-tients with MCI; conversely, some studies deter-mined the prevalence of MCI in older patients with
depression. In fact, elderly patients may have symp-toms of both depression and mild cognitive defi-cits,50 whereas other studies have identified persis-tent cognitive impairment in depression.51–53 It isimportant to note that in some of these studies, MCIdiagnosis was based on neuropsychological algo-rithms and not on a traditional clinical definition ofMCI.50,51,53 In particular, Reischies and Neu50 founda diffuse mild cognitive disorder in 102 consecutive,depressed elderly patients and 18%–35% of impairedneuropsychological tests in 57 patients with MDD.No improvement in cognitive performance was foundat the time of remission of depressive symptoms up tothe level of control subjects, suggesting that these pa-tients may suffer from comorbidity of both depressionand mild cognitive disorder.50 Butters et al. found thatamong 45 elderly patients who met DSM-IV criteriafor MDD, who had no cognitive impairment at studyentry, and who were remitted after a 12-week treat-ment with nortriptyline or paroxetine had no changein cognitive function as a result of treatment (N � 35;77%); in contrast, successful depression treatment ledto significantly improved cognitive functioningamong elderly depressed patients with baseline cog-nitive impairment (N � 10; 23%).51 Adler et al. en-rolled 34 depressed elderly of whom 53% with MCIwere all treated for depression. At a 6-month follow-up, the HDRS scores improved in the entire group,whereas cognitive performance remained un-changed and 44% of patients still fulfilled the MCIcriteria.52 In another study, 61 depressed patientsaged more than 60 years who met DSM-IV criteriafor MDD and 40 healthy subjects underwent struc-tural MRI, neuropsychological testing, apolipopro-tein E (APOE) genotyping, and salivary cortisol as-sessment (more than 3 days) with follow-up 6months later. Persisting MCI according to Petersen’scriteria5,8 was diagnosed in 20 of 49 subjects (41%) at6 months and was associated with reduced hip-pocampal volume but not severity of depression,cortisol levels, or APOE genotype.54 In a recentstudy, Lee et al. enrolled 142 elderly patients withMDD by DSM-IV criteria, instituted antidepressanttherapy, and reassessed them a year later. Fifty-fivepercent of depressed patients who remitted at 1-yearfollow-up were classified as having MCI at baselineassessment, whereas 44.8% had MCI after 1 year. Ofthe participants classified as MCI at baseline, 59.4%remained cognitively impaired at 1-year follow-up.
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 20098

By contrast, of the subjects not meeting MCI criteria atbaseline, only 26.7% were classified as MCI after 1 year.53
Incidence of Depression in Patients With MCI
Very limited evidence is available on the incidenceof depression or depressive symptoms in patientswith MCI in population-based or hospital-basedstudies35,55 (Table 4). In the ILSA cohort, an esti-mated incidence rate of depressive symptoms of29.6/100 person-years was found, with 8.2/100 per-son-years of mild new-onset depressive symptomsand 21.4/100 person-years of severe new-onset de-pressive symptoms.35 A prior nonpopulation-basedstudy of elderly volunteers estimated the incidenceof depressive symptoms in patients with MCI to be11.7/100 person-years,55 which is less than half of theILSA incidence rate of depressive symptoms of 29.6/100 person-years. This underscores the importance ofthe distinction between population-based and hospi-tal-based settings. The differences between these twoincidence studies may arise from selected groupsand the different assessment of depression (GDS-30versus HDRS). The findings from the ILSA suggesteda borderline nonsignificant trend for a protectiveeffect against the new-onset of total depressivesymptoms in subjects with MCI who reverted to
normal cognition in comparison with cognitively sta-ble patients with MCI.35 In conclusion, although hos-pital-based studies on MCI reported a higher preva-lence of depressive symptoms (median value: 44.3%),population-based studies reported a prevalence of3%–63.3% (median value: 15.7%) for depressionamong patients with MCI. Incidence of depressivesymptoms varied from 11.7 to 26.6/100 person-yearsin hospital-based and population-based studies. Fur-thermore, it seems that another important source ofdiscrepancy in prevalence rates of depression in MCIare due more to the operational definition and as-sessment of depression than the definition of MCI(Table 3). This was also confirmed by the limitedevidence coming from studies reporting the inci-dence of depressive symptoms among patients withprevalent MCI35,55 (Table 4). In particular, use of theNPI seemed to produce higher prevalence of depres-sion, except for the study of Geda et al.44 where themost pure and restrictive definition of MCI accord-ing to the Petersen’s criteria was used5,8 (Table 3).
DEPRESSION AND RISK PREDEMENTIASYNDROMES
Converging evidence suggests that late-onset de-pressive symptoms or syndromes often are a pro-
TABLE 4. Principal Incidence Studies of Depressive Symptoms in Patients With Mild Cognitive Impairment (MCI)
Reference Setting and Study Design SubjectsTools, Procedure, orDiagnostic Criteria
Reported Incidence ofDepressive Symptoms
or Depression
Population-basedstudies
Solfrizzi et al.35 Cross-sectional and longitudinal,population based (3.5 years)
2,963 subjects frompopulation-register(includinginstitutions) agedfrom 65 to 84years
MCI criteria: 1.5 SDs belowmean age- and education-adjusted on the MMSE and10th percentile below age-and education-adjusted onmemory test, withoutSMC and intactADL/IADL); depressivesymptoms measured withthe GDS-30
29.6/100 person-years
Hospital-basedstudies
Li et al.55 Cross-sectional and longitudinal,hospital based (3.5 years)
294 subjects atbaseline: 19patients withMCI followed upfor a mean of 3.5years
MCI criteria: cognitivecapacity screeningexamination or MMSEscores between 24 and26; depressive symptomsmeasured with the HDRS
11.7/100 person-years
Notes: SMC: subjective memory complaint; ADL: activities of daily living; IADL: instrumental activities of daily living.
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 9

drome of cognitive decline. Recent history of depres-sion is associated with increased incidence of AD.18
Individuals with late-life depression and transientcognitive impairment frequently develop AD or VaDwithin a few years after the onset of depression.13
Together, these observations suggest that some late-life depressive syndromes may be early manifesta-tions of dementing disorders.56 In contrast to thistheory, depression may represent an independentrisk factor predisposing to dementing disorders,18
even when depressive symptoms occur more than 10years before the onset of dementia.57 Lifetime historyof depression increases the risk of AD, regardless ofthe presence or absence of family history of dement-ing disorders,58 and depression may be also a riskfactor for VaD.59 Moreover, the findings reviewedsuggested that in primary MDD, the task is to figureout if the cognitive impairment is reversible or pro-gressive in nature.50,51,53 In primary MCI, the taskmay be to figure out if depressive symptoms or aparticular depressive pattern may predict progres-sion to dementia.
The findings from the ILSA showed that higherdepressive symptoms at baseline (moderate or highdepressive symptoms: GDS-30 �10 points) were notassociated with the development of incident MCI60
or the progression of patients with MCI to demen-tia.61 At present, only in the CHS Cognition Study,the development of MCI was associated cross-sec-tionally with racial and constitutional factors, CVD,and measurements of cognition and depression.62
Very recently, the CHS Cognition Study confirmedthese findings in a prospective study in which de-pressive symptoms at baseline (moderate or highdepressive symptoms: CES-D �8 points) were asso-ciated with increased risk of MCI, and this associa-tion was independent of underlying vascular dis-ease.63 In a cohort of cognitively normal elderlysubjects without depression at recruitment, individ-uals in the depression cohort (GDS-15 �6 points)were at significantly increased risk of subsequentincident MCI, and a synergistic interaction betweendepression and APOE genotype was also found64
(Table 5).The findings from the ILSA suggested that de-
pression and MCI may cooccur but failed to dem-onstrate a causal link between depressive symp-toms and incident MCI,60 at least in a shorterfollow-up. A possible role of depressive symptoms
was recently evaluated in preclinical AD,65 sug-gesting that depressive symptoms may be a part ofthe preclinical phase of dementia. Furthermore,Wilson et al., in two cohort studies (the ReligiousOrder Study and the Rush Memory and AgingProject) found that the risk of MCI increased byabout 2% for each one-unit increase on an indicatorof the tendency to experience psychological dis-tress. Depressive symptoms evaluated with the 10-item CES-D were also related to risk of MCI butnot after controlling for distress score66 (Table 5).Furthermore, only among the participants from theReligious Order Study, depressive symptoms didnot increase in those who subsequently developedMCI in a 13-year follow-up. However, the samplewas very mildly depressed at baseline (mean 10-item CES-D � SD: 1.0 � 1.5), and the participantswere all highly educated.67
In the ILSA, depressive symptoms also failed topredict the conversion of MCI to dementia.61
Nonetheless, these findings are in contrast withthose of another recent study in which patientswith MCI and depression are at more than twicethe risk of developing AD as those without depres-sion68 (Table 5). However, in this study, a clinicaldiagnosis of depressive disorder (DSM-IV) wasperformed, and the subjects were from a commu-nity general hospital and not from a population-based study. Furthermore, the results of the ILSAconfirmed those of another recent study in whichpatients with MCI who had concurrent depressiondid not have an increased risk of incident AD,when compared with nondepressed patients withMCI.69 More recently, in a Polish study, multiple-domain patients with aMCI had significantlyhigher MADRS baseline scores relative to singledomain aMCI, and after a mean 3-year follow-upperiod, more severe depression (higher MADRSscore) at baseline was a significant predictor forprogression to dementia.70 On the contrary, in aFrench study, no difference was found in the prev-alence of depressive symptoms (MADRS scores)between subjects with MCI converted to dementiaand those who did not. Of the patients with apathyat baseline, 15.1% developed AD in comparisonwith 6.9% of the nonapathetic patients71 (Table 5).
Furthermore, other recent data suggested thatthe anxiety-related or motivational (apathetic)symptoms of depression may be relevant to MCI
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 200910

TABLE 5. Principal Studies Examining the Possible Role of Depressive Symptoms or Syndromes in Predicting Incident MildCognitive Impairment (MCI) and Its Progression to Dementia
ReferencesSetting and Study
Design SubjectsTools, Procedure, orDiagnostic Criteria
Reported Risk of Incident MCIor Its Progression to
Dementia in Relation toDepressive Symptoms orDepression at Baseline
Risk of incident MCIBarnes et al.63 Cross-sectional and
longitudinal,populationbased (6 years)
2,220 subjects from 4 U.S.communities aged 65years or older
MCI criteria: clinical diagnosisaccording to Petersen’scriteria without intactIADL; depressive symptomsmeasured with the CES-D
Low depressive symptoms:unadjusted OR: 1.38, 95% CI:1.03–1.85
Moderate or high depressivesymptoms: unadjusted OR:2.20, 95% CI: 1.59–3.03
These associations werediminished only slightly byadjustment for vascular diseasemeasures and demographics
Geda et al.64 Longitudinal,hospital based(3.5 years)
840 subjects from primarycare clinic, median age(range) 77 (50–98)
MCI criteria: clinical diagnosisaccording to Petersen’scriteria withoutmodifications; depressivesymptoms measured withthe GDS-15
HR: 2.2; 95% CI: 1.2–4.1 (afteradjusting for possiblecounfounders)
HR: 5.1; 95% CI, 1.9–13.6)(interaction between APOEgenotype �3/�4 or �4/�4 anddepression)
Panza et al.60 Cross-sectional andlongitudinal,populationbased (3.5 years)
2,963 subjects frompopulation-register(including institutions)aged from 65 to 84years
MCI criteria: 1.5 SDs belowmean age- and education-adjusted on the MMSE and10th percentile below age-and education-adjusted onmemory test, without SMCand intact ADL/IADL);depressive symptomsmeasured with the GDS-30
RR: 1.25; 95% CI: 0.85–1.84
Wilson et al.66 Longitudinal,populationbased (12 years)
1,256 subjects frompopulation-register;mean � SD age: 78.6 �7.6 years
MCI criteria: clinical diagnosisaccording to Petersen’scriteria; depressivesymptoms measured withthe 10-item CES-D
RR: 1.06; 95% CI: 1.002–1.120RR: 1.02; 95% CI: 0.96–1.09
(after adjusting forpsychological distress score)
Risk of progression fromMCI to AD ordementia
Modrego et al.68 Longitudinal,hospital based(3 years)
114 patients with aMCIfrom a communitygeneral hospital; mean� SD age: 72.8 � 5.3years
aMCI criteria: clinicaldiagnosis according toPetersen’s criteria withoutmodifications; majordepression was carried outby means of a half-hourstructured interview toelicit at least 5 depressivesymptoms according to theDSM-IV criteria
RR: 2.6; 95% CI: 1.8–3.6
Robert et al.71 Cross-sectional andlongitudinal,hospital based(1 year)
251 patients with aMCIfrom the referralpopulations of the 14centers with memoryconsultation facilities;aged 58 years and older
aMCI criteria: patients withmemory complaints andpatients presenting at leastone error to the MMSEthree word recall, or ascore lower than 29 to theIsaac-set test; depressivesymptoms measured withthe MADRS. Apathy wasassessed with the ApathyInventory
After a 1-year follow-up, 10.2% ofpatients developed AD and194 did not develop AD. Therewere no differences at baselinebetween the two groups forMADRS total score. Of thepatients with apathy atbaseline, 15.1% developed ADin comparison with 6.9% ofthe non-apathetic patients
(Continued)
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 11

TABLE 5. (Continued)
ReferencesSetting and Study
Design SubjectsTools, Procedure, orDiagnostic Criteria
Reported Risk of Incident MCIor Its Progression to
Dementia in Relation toDepressive Symptoms orDepression at Baseline
Gabryelewicz et al.70 Longitudinal,hospital based(3 years)
105 patients with MCI MCI criteria: clinical diagnosisaccording to Petersen’scriteria, with asubclassification in singleand multiple domain aMCI;depressive symptomsmeasured with the MADRS
After 3 years of follow-up,multiple domain patients withaMCI had significantly higherMADRS baseline scores relativeto single domain aMCI andmore severe depressivesymptoms at baseline inmultiple domain patients withaMCI were a significantpredictor for progression todementia
Teng et al.73 Longitudinal,hospital based(2 years)
51 patients with aMCIfrom a tertiary carecenter; mean � SD age:73.9 � 6.7 years
MCI criteria: clinical diagnosisaccording to modifiedPetersen’s criteria with 1.5SD below age- andeducation-adjusted normson neuropsychological testscores; depressivesymptoms measured withthe NPI
Subjects with MCI progressing toAD had a significantly higherprevalence of neuropsychiatricsymptoms than subjects whoremained stable or improved(100 vs. 59%). In particular,depression (67 vs. 31%) andapathy (50 vs. 18%) were morecommon in subjects who werelater diagnosed with AD
Palmer et al.75 Cross-sectional andlongitudinal,populationbased (3 years)
In a population of 628persons aged 75 yearsand older, 47 personsfulfilled the criteria ofMCI (amnestic ormultidomains) and 185were cognitivelyunimpaired at baseline
MCI criteria: 1 SD below age-and education-adjustednorms on MMSE score;aMCI criteria: objectiveimpairment in episodicmemory task but normalfunctioning on visuospatialand language tasks;multidomains MCI criteria:impairment in two or moreof the episodic memory,language, and visuospatialdomains; depressive andanxiety symptoms weremeasured with CPRS
Mood-related depressivesymptoms RR: 0.9; 95% CI:0.6–1.5
Motivation-related depressivesymptoms RR: 1.1; 95% CI:0.7–1.8
Panza et al.61 Cross-sectional andlongitudinal,populationbased (3.5 years)
2,963 subjects frompopulation-register(including institutions)aged from 65 to 84years
MCI criteria: 1.5 SDs belowmean age- and education-adjusted on the MMSE and10th percentile below age-and education-adjusted onmemory test, without SMCand intact ADL/IADL);depressive symptomsmeasured with the GDS-30
RR: 1.42; 95% CI: 0.48–4.23
Houde et al.76 Longitudinal,hospital based(4.3 years)
60 patients with aMCIfrom a tertiary carecenter; mean � SD age:74.5 � 6.5 years
aMCI criteria: clinicaldiagnosis according toPetersen’s criteria withoutmodifications; depressivesymptoms measured withthe GDS-30
HR: 1.07; 95% CI: 0.99–1.15
IADL: instrumental activities of daily living; CES-D: Center for Epidemiological Studies Depression Scale 10-item questionnaire; OR: odds ratio;HR: hazard ratio; ADL: activities of daily living; RR: relative risk; MMSE: Mini-mental State Examination; SMC: subjective memory complaint; CPRS:Comprehensive Psychopathological Rating Scale.
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 200912

and progression of MCI to dementia.72–75 In fact, in51 subjects with MCI assessed for neuropsychiatricsymptoms using the NPI and followed for an av-erage of 2 years, subjects progressing to AD had asignificantly higher prevalence of psychopathol-ogy than subjects who remained stable or im-proved (100% versus 59%). In particular, depres-sion (67% versus 31%) and apathy (50% versus18%) were more common in subjects who werelater diagnosed with AD.73 Robert et al.,74 in alongitudinal study with a 3-year follow-up on 214patients with aMCI with depressive symptoms,found that the risk of progression to AD was sig-nificantly higher for patients with lack of interest,one dimension of apathy. Findings from the pop-ulation-based Kungsholmen project suggested thatsubjects with MCI plus anxiety symptomatologyhad an increased risk of progressing to AD over 3years compared with that of subjects with MCI andwithout anxiety problems. Furthermore, depressedmood was predictive of AD in subjects with nor-mal levels of baseline cognition and being frequentin subjects with MCI75 (Table 5). In 60 patientswith MCI from a hospital-based study with a 4.3-year follow-up, simple presence or absence of de-pression at referral (moderate or high depressivesymptoms: GDS-30 �10 points) did not predictprogression of MCI to AD. Positive answers tospecific GDS-30 questions referring to a pattern ofmelancholia and the persistence of depression over2–3 years significantly predicted cognitive deteri-oration leading to AD76 (Table 5). At present, fordepressed normal subjects and depressed patientswith MCI, the findings on increased risk of inci-dent MCI or its progression to dementia seem to beconflicting. However, future work will have toassess participants using more comprehensivescreening tools for depressive symptoms, com-bined with instruments that show good validity forexamination of anxiety and apathy. In patients withMCI with these mood symptoms, executive functionsseem especially vulnerable.77 More cross-sectional andlongitudinal studies would help to clarify whether thisgroup of dysexecutive patients with MCI plus anxiety-related or apathetic symptoms of depression should beconsidered as having subclinical late-life depression orat higher risk of progression to dementia, and particu-larly AD.
DEPRESSION AND PREDEMENTIA SYNDROMES:POSSIBLE MECHANISMS
Depression and MCI: Shared Risk Factors orConfounding
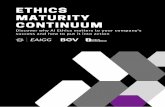
At present, the mechanisms on the possible role ofdepression and depressive symptoms in the devel-opment of predementia syndromes or their progres-sion to dementia are still under investigation. Onepossibility is that depression and predementia syn-dromes share the same risk factors or confounding.In fact, additional factors, genetic, environmental, orboth may lead to the genesis of both MCI and de-pression (Fig. 1). Current etiological models of late-life depression and cognitive decline focus on thepotential role of vascular risk factors and suggestedpossible opportunities for specific prevention andintervention strategies in high-risk populations.2 Infact, some late-life depressive syndromes might pre-dispose, precipitate, or perpetuate by CVD, the socalled “vascular depression” hypothesis.78 This no-tion is based on the comorbidity of depressive syn-dromes with cerebrovascular lesions and cerebrovas-cular risk factors and on the fact that depressionoften develops after a stroke.14 Elderly people withvascular depression have greater disability andcognitive impairment than those who are de-pressed but who do not have comorbid vascularstigmata.14 Furthermore, previous studies haveshown a correlation between MCI and vascularrisk factors, such as hypertension, total cholesterol,and coronary artery disease.2
However, in the ILSA, no sociodemographicvariables or vascular risk factors modified the as-sociation between depressive symptoms and inci-dent MCI or between depressive symptoms andconversion to dementia.60,61 Furthermore, in theILSA, vascular disease or vascular risk factors didnot have any impact on the onset of depressivesymptoms in both cognitively stable patients withMCI and in patients with MCI who reverted tonormal cognition after a 3.5-year follow-up.35 Pos-sibly, a longer follow-up would reveal that vascu-lar factors might influence the incidence of MCI indepressed patients, its progression to dementia, orthe onset of mood disturbances in patients withMCI. Butters et al.18 suggested two possible path-ways linking depression, vascular disease, MCI,
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 13

and dementia: 1) individuals who accumulate ADneuropathology over many years along with cooc-curring CVD, which damages the frontostriatal cir-cuitry, leading to late-life depression. The totalneuropathologic burden, combined with depressedmood, lowers brain reserve capacity, leads to expres-sion of MCI (e.g., memory and executive dysfunction)earlier than otherwise would be the case, and, given theunderlying neuropathology, progresses to AD alongwith cooccurring CVD and 2) individuals who developCVD (with variable neuropathologic burden) leadingto late-life depression and MCI (e.g., executive dys-function), which will follow the course of the under-lying CVD. However, at present, epidemiologic stud-ies suggest that the possible association betweendepressive symptoms and MCI seems not attribut-able to vascular disease or risk,60,61,63 and severalother hypotheses on the underlying mechanism havebeen proposed (Fig. 1).
Coexistence of Depression and MCI
Another hypothesis is that development of late-lifedepressive symptoms may reflect an underlying neu-
ropathologic condition that will develop also cognitivedecline over time. Therefore, depressive symptomswithout clinically significant cognitive impairmentmay be the early signs of a neurodegenerative disease56
(Fig. 1). Alternatively, depression may “unmask” theclinical manifestations of MCI in individuals with lim-ited cognitive reserve,79 or depressive symptomsmay overlap to some extent with the symptoms ofcognitive decline (Fig. 1). It is also possible that in-dividuals with some degree of cognitive decline maydevelop depression as a reaction to the cognitivesymptoms (Fig. 1). In fact, some evidence suggestedthat patients with MDD reported in self and observerratings cognitive problems exceeded neuropsycho-logical deficits in standardized tests, and these re-sults could be additionally influenced by patientsnegative self-perception.80 Furthermore, some find-ings suggest that anxiety or apathetic symptoms ofdepression in MCI may be a response to the initialphases of cognitive impairment in neurodegenera-tion,71–74 whereas mood-related depressive symp-toms may be a preclinical sign of AD related to theneuropathologic mechanism, present even in indi-viduals with prodromal AD who have no detectable
FIGURE 1. Synopsis of the Principal Hypotheses on the Possible Mechanisms Linking Depression to Mild Cognitive Impairment (MCI)
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 200914

cognitive impairment.75 Several other hypothesesmay explain the relationship between depressionand predementia syndromes. One possibility is thatdepression may be a causal factor leading to hip-pocampal damage through a glucocorticoid cas-cade19 (Fig. 1). In fact, older adults with high orrising cortisol levels during 5 years had poorer mem-ory and greater hippocampal atrophy.81 Depressioncould produce degenerative lesions in the hippocam-pus mediated by the excess of glucocorticoids,82 neu-ronal loss in the aminergic nuclei of the brainstem,18
and a fall in the levels of noradrenaline and serotoninin the cerebral cortex and hippocampus.18 Butters etal.18 suggested two possible pathways linking de-pression, hypothalamic-pituitary-adrenal-stress axis,MCI, and dementia: 1) individuals who develop de-pression at any point and who experience depres-sion-related neuropathology (e.g., hippocampal vol-ume loss) that results in MCI that is stable (unlessthey experience additional depressive episodes) and2) individuals who accumulate AD neuropathologyover many years and who develop late-life depres-sion (related or unrelated to AD pathology), thatlowers brain reserve capacity, and results in expres-sion of MCI earlier than otherwise would be thecase, and given the underlying neuropathology,progress to AD. An important implication of this hy-pothesis is that an intervention targeting depressionmay lead to primary prevention of MCI and subse-quent dementia.
Depression and MCI: Interaction With a GeneticSusceptibility Factor
Another hypothesis is a possible interaction inwhich depression leads to cognitive decline only inthe presence of a genetic susceptibility factor (Fig. 1).In fact, a recent study found evidence of a synergisticinteraction between APOE genotype and depression.63
There also may be a genetic link between depressivesymptoms and dementia in some patients. For exam-ple, a study of women at high risk of carrying thepresenilin 1 mutation for dementia showed that carri-ers of this mutation had significantly more depressivesymptoms than noncarriers and were more likely tohave sought help from a psychiatric professional.83 Ofcourse, all these hypotheses and other possible mech-anisms are not mutually exclusive,18 may act in com-
bination, and need clinical or experimental confirma-tion in the near future.
CONCLUSIONS
Prevalence rates of depressive syndromes orsymptoms vary widely among studies, as a resultof different diagnostic criteria and operational def-initions of depression (MDD versus depressivesymptoms) and different sampling and assessmentprocedures. In fact, although hospital-based stud-ies on MCI reported a higher prevalence of depres-sive symptoms (median value: 44.3%), population-based studies reported a prevalence of 3%– 63.3%(median value: 15.7%) for depression among pa-tients with MCI. Avoiding a subclassification forstudy setting, the median value of depressivesymptoms in patients with MCI was, therefore,34%. At present, incidence of depressive symp-toms varied from 11.7 to 26.6 per 100 person-yearsin the very few hospital-based and population-based studies available, suggesting the need foradditional research in this area to describe alsoprevalence and incidence of depressive symptomsor syndromes in MCI subtypes. Furthermore, per-sistent cognitive deficits in the context of MDD area significant clinical concern because they mayreflect underlying structural changes that increasean individual’s risk of progression to AD or an-other form of dementia.13 The tripled prevalence ofdepression of patients with MCI in hospital-basedsamples versus population-based samples may re-flect different referral patterns, selection criteriaand tools, and different stages of cognitive decline.Nonetheless, in the studies reviewed, prevalenceand incidence estimates of depressive symptoms inMCI had important limitations, because it was im-possible to establish a precise link between MCIand neuropsychiatric symptoms. Future studiesshould include a standardization of settings, diagnos-tic criteria for predementia, and depression syndromesor the means of collecting depressive symptoms.
At present, for depressed normal subjects anddepressed patients with MCI, the findings on in-creased risk of incident MCI or its progression todementia seem to be conflicting. Converging evi-dence suggests that late-onset depressive symp-toms or syndromes often are a prodrome of cogni-
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 15

tive decline. These contrasting findings suggested that thelength of the follow-up period, the study design, thesample population, the level of education, the setting(population based versus hospital based), and method-ological differences (measurement of depressive symp-toms or diagnosis of depressive disorders and levelof depressive symptoms or particular patterns ofdepressive symptoms) may be central for detectingan association between baseline depression andsubsequent development of MCI or its progressionto dementia. Furthermore, self-report measurescould overestimate MCI in patients with depres-sion as some of the reported cognitive impairmentmay be related to negative self-appraisal.80 Exam-ining the reviewed measures of risk of incidentMCI or its progression to dementia (Table 5), wenoted that all are �1, suggesting that discrepancyamong study findings may be attributable also torandom variation/low power. The development ofuniversal diagnostic tools or more precise mea-surements of both depressive and cognitive symp-toms could help the researchers to overcome thismethodological bias, avoiding to report such dis-parate findings. In particular, a battery of testswith sensitivity to change over time could be de-veloped for the assessment of mood and behav-ioral symptoms in clinical MCI studies, with abriefer screening version that could be used inepidemiologic studies and in primary care settings,combined with instruments with good validity forexamination of anxiety and apathy in depression.
These observations suggested that late-life de-pressive syndromes may be early manifestations ofdementing disorders, suggesting that depressivesymptoms might be included in MCI diagnosticcriteria. In fact, in the proceedings of the 2003NIMH conference on this topic, Steffens et al.3
suggested specifically that research is needed toclarify whether mood symptoms might be in-cluded in diagnostic criteria sets (e.g., MCI andmood disorder), act as a modifier (e.g., MCI withdepression), be excluded from the MCI diagnosis,or be seen as one of two distinct but not mutuallyexclusive diagnoses (e.g., MCI and major or minordepression). Furthermore, the European Consor-tium on Alzheimer’s Disease Working Group onMCI has very recently proposed that psychologicaland behavioral symptoms have to be taken in ac-count too and should not systematically be an
“exclusion criteria” for the diagnosis.10 Subjectsmay have depressive symptoms related to cogni-tive impairment or to the underlying process.13 Ofcourse, it also should be clarified that this contin-uum would only apply in particular subgroups ofelders. In fact, depressive symptoms may be highboth in patients with MCI who remained demen-tia-free and in patients with MCI who progressedto dementia or AD. In the first group of subjects,MCI could be related to an underlying psychiatricdisorder, and in the second group, MCI and depressionmay be associated with neurodegeneration.
In conclusion, the critical question is how thepresence of depression modifies the risk of inci-dent MCI or progression of MCI to dementia. Cen-tral to this question is determining the extent towhich depression is a true risk factor versus anearly symptom occurring in the prodromal phaseof dementia, particularly AD (e.g., aMCI). Substan-tial support exists for both hypotheses, and theyare not mutually exclusive. Some findings suggestthat when depressive and cognitive symptoms ap-pear close in time they likely arise from commonneuropathologic processes.18This is an importantcompeting hypothesis to the concept of depressionas a risk factor for progression of MCI to dementia.Therefore, assuming that MCI may be the earliestidentifiable clinical stage of dementia, depressivesymptoms may be an early manifestation rather thana risk factor for dementia and AD,56 arguing that theunderlying neuropathologic condition that causesMCI or dementia also causes depressive symptoms,rather than depressive symptoms causing or exacer-bating MCI. In this picture, at least in certain subsetsof elderly patients (e.g., dysexecutive MCI plus anx-iety related or apathetic symptoms of depression),late-life depression, MCI, and dementia could repre-sent a possible clinical continuum with indefinitebounds.
This work was supported by the Italian Longitudi-nal Study on Aging (ILSA) (Italian National ResearchCouncil—CNR-Targeted Project on Ageing— grants9400419PF40 and 95973PF40).
The CNR had no further role in study design; in thecollection, analysis, and interpretation of data; in writingof the report; and in the decision to submit the paper forpublication.
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 200916

References
1. Panza F, D’Introno A, Colacicco AM, et al: Current epidemiologyof mild cognitive impairment and other predementia syndromes.Am J Geriatr Psychiatry 2005; 13:633–644
2. Panza F, D’Introno A, Colacicco AM, et al: Cognitive frailty:Predementia syndrome and vascular risk factors. Neurobiol Aging2006; 27:933–940
3. Steffens DC, Otey E, Alexopoulos GS, et al: Perspectives ondepression, mild cognitive impairment, and cognitive decline.Arch Gen Psychiatry 2006; 63:130–138
4. Hughes CP, Berg L, Danziger WL, et al: A new clinical scale for thestaging of dementia. Br J Psychiatry 1982; 140:566–572
5. Petersen RC, Smith GE, Waring SC, et al: Mild cognitive impair-ment: clinical characterization and outcome. Arch Neurol 1999;56:303–308
6. Petersen RC, Doody R, Kurz A, et al: Current concepts in mildcognitive decline. Arch Neurol 2001; 58:1985–1992
7. Winblad B, Palmer K, Kivipelto M, et al: Mild cognitive impair-ment–beyond controversies, towards a consensus: report of theInternational Working Group on mild cognitive impairment. J In-tern Med 2004; 256:240–246
8. Petersen RC, Smith GE, Waring SC, et al: Aging, memory, andmild cognitive impairment. Int Psychogeriatr 1997; 9:65–69
9. Gauthier S, Reisberg B, Zaudig M; International PsychogeriatricAssociation Expert Conference on mild cognitive impairment:Mild cognitive impairment. Lancet 2006; 367:1262–1270
10. Portet F, Ousset PJ, Visser PJ, et al; MCI Working Group of theEuropean Consortium on Alzheimer’s Disease (EADC): Mild cog-nitive impairment (MCI) in medical practice: a critical review ofthe concept and new diagnostic procedure report of the MCIWorking Group of the European Consortium on Alzheimer’sDisease. J Neurol Neurosurg Psychiatry 2006; 77:714–718
11. American Psychiatric Association Committee on Nomenclatureand Statistics: Diagnostic and Statistical Manual of Mental Disor-ders. 4th edition (DSM-IV). Washington, DC, American Psychiat-ric Association, 1994
12. World Health Organization: International Statistical Classificationof Diseases and Related Health Problems, 10th Revision (ICD-10).Chapter V, categories F00–F99: Mental, Behavioural, and Devel-opmental Disorders, Clinical Description and Diagnostic Guide-lines. Geneva, Switzerland, World Health Organization, 1992
13. Potter GG, Steffens DC: Contribution of depression to cognitiveimpairment and dementia in older adults. Neurologist 2007; 13:105–117
14. Alexopoulos GS: Depression in the elderly. Lancet 2005; 365:1961–1970
15. Wragg RE, Jeste DV: Overview of depression and psychosis inAlzheimer’s disease. Am J Psychiatry 1989; 146:577–589
16. Sobin C, Sacheim HA: Psychomotor symptoms of depression.Am J Psychiatry 1997; 154:4–17
17. Olin JT, Schneider LS, Katz IR, et al: Provisional diagnostic criteriafor depression of Alzheimer’s disease. Am J Geriatr Psychiatry2002; 10:125–128
18. Butters MA, Young JB, Lopez O, et al: Pathways linking late-lifedepression to persistent cognitive impairment and dementia.Dialogues Clin Neurosci 2008; 10:345–357
19. Sapolsky RM: Depression, antidepressants, and the shrinking hip-pocampus. Proc Natl Acad Sci USA 2001; 98:12320–12322
20. First MB, Spitzer RL, Gibbon M, et al: Structured Clinical Inter-view for DSM-IV Axis I Disorders (SCID I), Clinician Version,Administration Booklet. Washington, DC: American PsychiatricPress, 1997
21. Lyness JM, King DA, Cox C, et al: The importance of subsyn-dromal depression in older primary care patients: prevalenceand associated functional disability. J Am Geriatr Soc 1999;47:647– 652
22. Gallo JJ, Rabins PV, Lyketsos LG, et al: Depression without sad-ness: functional outcomes of nondysphoric depression in laterlife. J Am Geriatr Soc 1997; 45:570–578
23. Yesavage JA, Brink TL, Rose TL, et al: Development and validationof a geriatric depression screening scale: a preliminary report.J Psychiatr Res 1982–83; 17:37–49
24. Debruyne H, Van Buggenhout M, Le Bastard N, et al: Is thegeriatric depression scale a reliable screening tool for depressivesymptoms in elderly patients with cognitive impairment? Int JGeriatr Psychiatry 2009; 24:556–662
25. Radloff LS: The CES-D scale: a self-report depression scale forresearch in the general population. Appl Psychol Measurement1977; 1:385–401
26. Irwin M, Artin KH, Oxman MN: Screening for depression in theolder adult: criterion validity of the 10-item Center for Epidemi-ological Studies Depression Scale (CES-D). Arch Intern Med 1999;159:1701–1704
27. Beck AT, Steer RA, Brown GK: Beck Depression Inventory-IIManual. San Antonio, TX: Psychological Corporation, 1996
28. Alexopoulos GS, Abrams RC, Young RC, et al: Cornell scale fordepression in dementia. Biol Psychiatry 1988; 23:271–284
29. Cummings JL, Mega M, Gray K, et al: The NeuropsychiatricInventory: comprehensive assessment of psychopathology in de-mentia. Neurology 1994; 44:2308–2314
30. Hamilton M: A rating scale for depression. J Neurol NeurosurgPsychiatry 1960; 23:56–62
31. Montgomery SA, Asberg M: A new depression scale designed tobe sensitive to change. Br J Psychiatry 1979; 134:382–389
32. Asberg M, Montgomery SA, Perris C, et al: A comprehensivepsychopathological rating scale. Acta Psychiatr Scand 1978; suppl271:5–27
33. Goldberg D, Bridges K, Duncan-Jones P, et al: Detecting anx-iety and depression in general medical settings. BMJ 1988;297:897– 899
34. Tariot PN: CERAD behavior rating scale for dementia. Int Psy-chogeriatr 1996; 8(suppl 3):317–320
35. Solfrizzi V, D’Introno A, Colacicco AM, et al: Italian LongitudinalStudy on Aging Working Group. Incident occurrence of depres-sive symptoms among patients with mild cognitive impairment—the Italian Longitudinal Study on Aging. Dement Geriatr CognDisord 2007; 24:55–64
36. Lyketsos CG, Lopez O, Jones B, et al: Prevalence of neuropsychi-atric symptoms in dementia and mild cognitive impairment: re-sults from the cardiovascular health study. JAMA 2002; 288:1475–1483
37. Chan DC, Kasper JD, Black BS, et al: Prevalence and correlatesof behavioral and psychiatric symptoms in community-dwell-ing elders with dementia or mild cognitive impairment: theMemory and Medical Care Study. Int J Geriatr Psychiatry 2003;18:174 –182
38. Forsell Y, Palmer K, Fratiglioni L: Psychiatric symptoms/syn-dromes in elderly persons with mild cognitive impairment. Datafrom a cross-sectional study. Acta Neurol Scand 2003; suppl179:25–28
39. Kumar R, Jorm AF, Parslow RA, et al: Depression in mild cogni-tive impairment in a community sample of individuals 60–64years old. Int Psychogeriatr 2006; 18:471–480
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 17

40. Kumar R, Parslow RA, Jorm AF, et al: Clinical and neuroimagingcorrelates of mild cognitive impairment in a middle-aged commu-nity sample: the personality and total health through life 60�study. Dement Geriatr Cogn Disord 2006; 21:44–50
41. Muangpaisan W, Intalapaporn S, Assantachai P: Neuropsychiatricsymptoms in the community-based patients with mild cognitiveimpairment and the influence of demographic factors. Int J Geri-atr Psychiatry 2008; 23:699–703
42. Copeland MP, Daly E, Hines V, et al: Psychiatric symptomatologyand prodromal Alzheimer’s disease. Alzheimer Dis Assoc Disord2003; 17:1–8
43. Hwang TJ, Masterman DL, Ortiz F, et al: Mild cognitive impair-ment is associated with characteristic neuropsychiatric symp-toms. Alzheimer Dis Assoc Disord 2004; 18:17–21
44. Geda YE, Smith GE, Knopman DS, et al: De novo genesis ofneuropsychiatric symptoms in mild cognitive impairment. IntPsychogeriatr 2004; 16:51–60
45. Lopez OL, Becker JT, Sweet RA: Non-cognitive symptoms in mildcognitive impairment subjects. Neurocase 2005; 11:65–71
46. Gabryelewicz T, Styczynska M, Pfeffer A, et al: Prevalence ofmajor and minor depression in elderly persons with mild cogni-tive impairment: MADRS factor analysis. Int J Geriatr Psychiatry2004; 19:1168–1172
47. Rozzini L, Vicini Chilovi B, Conti M, et al: Neuropsychiatricsymptoms in amnestic and nonamnestic mild cognitive impair-ment. Dement Geriatr Cogn Disord 2008; 25:32–36
48. Ellison JM, Harper DG, Berlow Y, et al: Beyond the “C” in MCI:noncognitive symptoms in amnestic and non-amnestic mild cog-nitive impairment. CNS Spectr 2008; 13:66–72
49. Feldman H, Scheltens P, Scarpini E, et al: Behavioral symptoms inmild cognitive impairment. Neurology 2004; 62:1199–1201
50. Reischies FM, Neu P: Comorbidity of mild cognitive disorder anddepression—a neuropsychological analysis. Eur Arch PsychiatryClin Neurosci 2000; 250:186–193
51. Butters MA, Becker JT, Nebes RD, et al: Changes in cognitivefunctioning following treatment of late-life depression. Am J Psy-chiatry 2000; 157:1949–1954
52. Adler G, Chwalek K, Jajcevic A: Six-month course of mild cogni-tive impairment and affective symptoms in late-life depression.Eur Psychiatry 2004; 19:502–505
53. Lee JS, Potter GG, Wagner HR, et al: Persistent mild cognitiveimpairment in geriatric depression. Int Psychogeriatr 2007; 19:125–135
54. O’Brien JT, Lloyd A, McKeith I, et al: A longitudinal study ofhippocampal volume, cortisol levels, and cognition in older de-pressed subjects. Am J Psychiatry 2004; 161:2081–2090
55. Li YS, Meyer JS, Thornby J: Longitudinal follow-up of depressivesymptoms among normal versus cognitively impaired elderly. IntJ Geriatr Psychiatry 2001; 16:718–727
56. Chen P, Ganguli M, Mulsant BH, et al: The temporal relationshipbetween depressive symptoms and dementia: a community-basedprospective study. Arch Gen Psychiatry 1999; 56:261–266
57. Steffens DC, Plassman BL, Helms MJ, et al: A twin study oflate-onset depression and apolipoprotein E �4 as risk factors forAlzheimer’s disease. Biol Psychiatry 1997; 41:851–856
58. van Duijn CM, Clayton DG, Chandra V: Interaction between geneticand environmental risk factors for Alzheimer’s disease: a reanalysisof case-control studies. Genet Epidemiol 1994; 11:539–551
59. Canadian Study of Health and Aging Working Group: The inci-dence of dementia in Canada. Neurology 2000; 55:66–73
60. Panza F, D’Introno A, Colacicco AM, et al: Italian LongitudinalStudy on Aging Working Group. Depressive symptoms, vascu-lar risk factors and mild cognitive impairment. The Italian
longitudinal study on aging. Dement Geriatr Cogn Disord2008; 25:336 –346
61. Panza F, Capurso C, D’Introno A, et al: Impact of depressivesymptoms on the rate of progression to dementia in patientsaffected by mild cognitive impairment. The Italian longitudinalstudy on aging. Int J Geriatr Psychiatry 2008; 23:726 –734
62. Lopez OL, Jagust WJ, Dulberg C, et al: Risk factors for mildcognitive impairment in the Cardiovascular Health Study Cogni-tion Study: part 2. Arch Neurol 2003; 60:1394–1399
63. Barnes DE, Alexopoulos GS, Lopez OL, et al: Depressive symp-toms, vascular disease, and mild cognitive impairment: findingsfrom the Cardiovascular Health Study. Arch Gen Psychiatry 2006;63:273–279
64. Geda YE, Knopman DS, Mrazek DA, et al: Depression, apoli-poprotein E genotype, and the incidence of mild cognitive im-pairment: a prospective cohort study. Arch Neurol 2006; 63:435–440 entity. J Intern Med 2004; 256:183–194
65. Berger AK, Fratiglioni L, Forsell Y, et al: The occurrence ofdepressive symptoms in the preclinical phase of AD: a popula-tion-based study. Neurology 1999; 53:1998–2002
66. Wilson RS, Schneider JA, Boyle PA, et al: Chronic distress andincidence of mild cognitive impairment. Neurology 2007; 68:2085–2092
67. Wilson RS, Arnold SE, Beck TL, et al: Change in depressivesymptoms during the prodromal phase of Alzheimer disease.Arch Gen Psychiatry 2008; 65:439–446
68. Modrego PJ, Ferrandez J: Depression in patients with mild cog-nitive impairment increases the risk of developing dementia ofAlzheimer type: a prospective cohort study. Arch Neurol 2004;61:1290–1293
69. Rozzini L, Vicini Chilovi B, Trabucchi M, et al: Depression isunrelated to conversion to dementia in patients with mild cogni-tive impairment. Arch Neurol 2005; 62:505
70. Gabryelewicz T, Styczynska M, Luczywek E: The rate of conver-sion of mild cognitive impairment to dementia: predictive role ofdepression. Int J Geriatr Psychiatry 2007; 22:563–567
71. Robert PH, Berr C, Volteau M, et al: The PreAL study: apathy inpatients with mild cognitive impairment and the risk of develop-ing dementia of Alzheimer’s disease: a one-year follow-up study.Clin Neurol Neurosurg 2006; 108:733–736
72. Ready RE, Ott BR, Grace J, et al: Apathy and executive dysfunc-tion in mild cognitive impairment and Alzheimer disease. Am JGeriatr Psychiatry 2003; 11:222–228
73. Teng E, Lu PH, Cummings JL: Neuropsychiatric symptoms areassociated with progression from mild cognitive impairmentto Alzheimer’s disease. Dement Geriatr Cogn Disord 2007;24:253–259
74. Robert PH, Berr C, Volteau M, et al: Importance of lack of interestin patients with mild cognitive impairment. Am J Geriatr Psychi-atry 2008; 16:770–776
75. Palmer K, Berger AK, Monastero R, et al: Predictors of progres-sion from mild cognitive impairment to Alzheimer disease. Neu-rology 2007; 68:1596–1602
76. Houde M, Bergman H, Whitehead V, et al: A predictive depres-sion pattern in mild cognitive impairment. Int J Geriatr Psychiatry2008; 23:1028–1033
77. Hudon C, Belleville S, Gauthier S: The association between de-pressive and cognitive symptoms in amnestic mild cognitiveimpairment. Int Psychogeriatr 2008; 20:710–723
78. Alexopoulos GS, Meyers BS, Young RC, et al: Clinically definedvascular depression. Am J Psychiatry 1997; 154:562–565
79. Jorm AF, van Duijn CM, Chandra V; EURODEM Risk Factors Re-search Group. Psychiatric history and related exposures as risk
Depression and Predementia Syndromes
Am J Geriatr Psychiatry ●:●, ●●● 200918

factors for Alzheimer’s disease: a collaborative re-analysis of case-control studies. Int J Epidemiol 1991; 20(suppl 2):S43–S47
80. Lahr D, Beblo T, Hartje W: Cognitive performance and subjectivecomplaints before and after remission of major depression. CognNeuropsychiatry 2007; 12:25–45
81. Lupien SJ, de Leon M, de Santi S, et al: Cortisol levels duringhuman aging predict hippocampal atrophy and memory deficits.Nat Neurosci 1998; 1:69–73
82. Steffens DC, Payne ME, Greenberg DL, et al: Hippocampal vol-ume and incident dementia in geriatric depression. Am J GeriatrPsychiatry 2002; 10:62–71
83. Ringman JM, Diaz-Olavarrieta C, Rodriguez Y, et al: Femalepreclinical presenilin-1 mutation carriers unaware of their ge-netic status have higher levels of depression than their non-mutation carrying kin. J Neurol Neurosurg Psychiatry 2004;75:500 –502
Panza et al.
Am J Geriatr Psychiatry ●:●, ●●● 2009 19