Technical factors affecting morbidity in definitive irradiation for localized carcinoma of the...
9
Pergamon ?? Clinical Original Contribution Int. J. Radiation Oncology Biol. Phys., Vol. 28. No. 4, pp. 81 I-819, 1994 Copyright 0 1994 Elsevier Science Ltd Printed in the USA. All rights reserved 0360-3016/94 $6.00 + .OO TECHNICAL FACTORS AFFECTING MORBIDITY IN DEFINITIVE IRRADIATION FOR LOCALIZED CARCINOMA OF THE PROSTATE CARLOS A. PEREZ, M.D., HENRY K. LEE, M.D., ANASTASIOS GEORGIOU, M.D. AND MARY ANN LOCKETT, M.B.A. Radiation Oncology Center, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO 63 108 Purpose: The impact of some technical factors on morbidity was analyzed in 738 patients with histologically confirmed carcinoma of the prostate treated with definitive irradiation. Methods and Materials: The records of all patients were reviewed, and morbidity of irradiation was evaluated according to severity. All patients were followed up for a minimum of 3 years (median observation, 6.5 years). Results: The most frequent Grade 2 (moderate) intestinal complication was proctitis, which was observed in i% of -patients, followed by enteritis (1%) and anal-rectal fibrosis or stricture (about 1%). Incidence of Grade 3 (severe) proctitis was less than 1% and small bowel obstruction, 0.2%. One patient developed radiation-induced ileitis complicated with peritonitis, which was fatal. The most frequent Grade 2 urinary complication was urethral stricture (5%) and cystitis with significant symptoms or hematuria (2%). A vesicosigmoid and a rectovesical fistula (.4%) were noted, which required colostomy. One patient with hemorrhagic cystitis (.2%) required an ileal bladder, and two cases of ureteral stricture (.3%) required surgical correction. Most cases of Grade 2-3 intestinal or urinary morbidity appeared within 2-5 years after therapy (8% moderate and 3% severe cumulative intestinal morbidity at 10 years, and 9% and 3%, urinary). The actuarial incidence of rectosigmoid Grade 2 and 3 morbidity was 10% for patients treated to the pelvic lymph nodes and the prostate and 3% for those treated to the prostate only (p = 0.04). The difference in urinary morbidity in these two groups of patients was not statistically significant. There was also no significant correlation of morbidity with boost portal size for prostate irradiation. Patients treated with a stationary portal technique that delivered higher doses to the urinary bladder had a significantly greater incidence of urinary morbidity (18% cumulative) compared with patients treated with rotational techniques (5%) (p < 0.1). However, patients treated with pelvic fields and rotational techniques had a higher intestinal and rectosigmoid morbidity (11%) than patients treated to the prostate only (5 5%) (p = 0.05). No statistically significant difference in intestinal or urinary morbidity was related to doses of irradiation (60-70 Gy). Conclusion: Volume treated and, to a lesser extent, dose of irradiation at tolerance levels are important factors influencing significant morbidity in patients with carcinoma of the prostate treated with definitive irradiation. With recent advances in three-dimensional (3-D) treatment planning and conformal radiation therapy techniques, it is imperative to precisely determine optimal volumes and doses of irradiation required to achieve the highest local- pelvic tumor control while minimizing morbidity to enhance the role of irradiation in the management of localized carcinoma of the prostate. Prostate, Radiation therapy, Technical factors, Morbidity. INTRODUCTION METHODS AND MATERIALS Definitive irradiation is increasingly used in the manage- ment of localized carcinoma of the prostate (3,23). Several factors have been reported to influence the morbidity of radiation therapy (6, 9, 18, 19). In this publication, we analyze the potential impact of some technical and do- simetry factors on the incidence and severity of sequelae. Reports from our previous experience are updated, with a larger number of patients ( 17). Between January 1967 and December 1988, 738 pa- tients with histologically proven adenocarcinoma of the prostate localized to the pelvis were treated with definitive radiation therapy at the Mallinckrodt Institute of Ra- diology Radiation Oncology Center, Washington Uni- versity Medical Center. All patients have been followed up for a minimum of 3 years, with a median follow-up of 6.5 years, and a maximum of 22 years. All radiation Reprint requests to: Carlos A. Perez, M.D., Radiation On- Accepted for publication 29 September 1993. cology Center, 45 11 Forest Park, St. Louis, MO 63 108. 811
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Technical factors affecting morbidity in definitive irradiation for localized carcinoma of the...

Pergamon
??Clinical Original Contribution
Int. J. Radiation Oncology Biol. Phys., Vol. 28. No. 4, pp. 81 I-819, 1994 Copyright 0 1994 Elsevier Science Ltd Printed in the USA. All rights reserved
0360-3016/94 $6.00 + .OO
TECHNICAL FACTORS AFFECTING MORBIDITY IN DEFINITIVE IRRADIATION FOR LOCALIZED CARCINOMA OF THE PROSTATE
CARLOS A. PEREZ, M.D., HENRY K. LEE, M.D., ANASTASIOS GEORGIOU, M.D. AND MARY ANN LOCKETT, M.B.A.
Radiation Oncology Center, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO 63 108
Purpose: The impact of some technical factors on morbidity was analyzed in 738 patients with histologically confirmed carcinoma of the prostate treated with definitive irradiation. Methods and Materials: The records of all patients were reviewed, and morbidity of irradiation was evaluated according to severity. All patients were followed up for a minimum of 3 years (median observation, 6.5 years). Results: The most frequent Grade 2 (moderate) intestinal complication was proctitis, which was observed in i% of -patients, followed by enteritis (1%) and anal-rectal fibrosis or stricture (about 1%). Incidence of Grade 3 (severe) proctitis was less than 1% and small bowel obstruction, 0.2%. One patient developed radiation-induced ileitis complicated with peritonitis, which was fatal. The most frequent Grade 2 urinary complication was urethral stricture (5%) and cystitis with significant symptoms or hematuria (2%). A vesicosigmoid and a rectovesical fistula (.4%) were noted, which required colostomy. One patient with hemorrhagic cystitis (.2%) required an ileal bladder, and two cases of ureteral stricture (.3%) required surgical correction. Most cases of Grade 2-3 intestinal or urinary morbidity appeared within 2-5 years after therapy (8% moderate and 3% severe cumulative intestinal morbidity at 10 years, and 9% and 3%, urinary). The actuarial incidence of rectosigmoid Grade 2 and 3 morbidity was 10% for patients treated to the pelvic lymph nodes and the prostate and 3% for those treated to the prostate only (p = 0.04). The difference in urinary morbidity in these two groups of patients was not statistically significant. There was also no significant correlation of morbidity with boost portal size for prostate irradiation. Patients treated with a stationary portal technique that delivered higher doses to the urinary bladder had a significantly greater incidence of urinary morbidity (18% cumulative) compared with patients treated with rotational techniques (5%) (p < 0.1). However, patients treated with pelvic fields and rotational techniques had a higher intestinal and rectosigmoid morbidity (11%) than patients treated to the prostate only (5 5%) (p = 0.05). No statistically significant difference in intestinal or urinary morbidity was related to doses of irradiation (60-70 Gy). Conclusion: Volume treated and, to a lesser extent, dose of irradiation at tolerance levels are important factors influencing significant morbidity in patients with carcinoma of the prostate treated with definitive irradiation. With recent advances in three-dimensional (3-D) treatment planning and conformal radiation therapy techniques, it is imperative to precisely determine optimal volumes and doses of irradiation required to achieve the highest local- pelvic tumor control while minimizing morbidity to enhance the role of irradiation in the management of localized carcinoma of the prostate.
Prostate, Radiation therapy, Technical factors, Morbidity.
INTRODUCTION METHODS AND MATERIALS
Definitive irradiation is increasingly used in the manage- ment of localized carcinoma of the prostate (3,23). Several factors have been reported to influence the morbidity of radiation therapy (6, 9, 18, 19). In this publication, we analyze the potential impact of some technical and do- simetry factors on the incidence and severity of sequelae. Reports from our previous experience are updated, with a larger number of patients ( 17).
Between January 1967 and December 1988, 738 pa- tients with histologically proven adenocarcinoma of the prostate localized to the pelvis were treated with definitive radiation therapy at the Mallinckrodt Institute of Ra- diology Radiation Oncology Center, Washington Uni- versity Medical Center. All patients have been followed up for a minimum of 3 years, with a median follow-up of 6.5 years, and a maximum of 22 years. All radiation
Reprint requests to: Carlos A. Perez, M.D., Radiation On- Accepted for publication 29 September 1993. cology Center, 45 11 Forest Park, St. Louis, MO 63 108.
811
812 I. J. Radiation Oncology 0 Biology 0 Physics Volume 28, Number 4, 1994
oncology records were reviewed; the information was coded on computer-compatible forms and analyzed on a computer program with multiple cross-reference checks to ensure reliability of the data. A Biomedical Department Program (BMDP) statistical package was used for com- putation of the data (4, 5). All survival functions use the actuarial life-table as applied by Cutler and Ederer (4) and test statistics were determined by the methods of Generalized Wilcoxon (Breslow), Generalized Savage (Mantel-Cox), and Tarone-Ware ( 12,27). Trend analysis was performed by the Tarone method (26). The Mantel- Cox method was used to test for potentially significant factors for survival.
All patients had a complete physical and rectal exam- ination, routine blood count, chemistry profile, urinalysis, determination of serum prostatic acid phosphatases and alkaline phosphatases, chest X ray, intravenous pyelo- gram, and radioisotope bone scan, as previously reported ( 16, 17). The patients were initially staged according to a modification of the American Urological Association classification of 1978 (17) and restaged according to the American Joint Committee (AJC) guidelines (2). The clinical stage D 1 designation was used for locally extensive tumors in the pelvis or those invading the bladder neck (AJC T4). The tumors were classified according to the degree of histological differentiation into well, moderately, or poorly differentiated. Techniques of irradiation using 18-25 MV betatron or linear accelerator photons have been described previously ( 13, 14, 17). Stationary anterior- posterior portals were used to treat the pelvic lymph nodes to 40-45 Gy; in various groups decreasing anterior fields or 240” anterior or 120” bilateral arc rotation was used to irradiate the prostatic volume with 2 cm margins (Fig. 1). Total dose to the prostate in most patients was 62-66 Gy for A2 (Tl b) and B (T2) and 65-7 1 Gy for Stage C (T3) tumors. Daily dose was 1.8-2 Gy, five fractions-per- week (13, 14).
Patients were followed up periodically during and after therapy or until death by the staff of the Radiation On- cology Center, the referring urologist, and occasionally the family physician. When this information was not available, contact was made directly with the patient or relatives. Follow-up was obtained in 98% of the patients: those lost to follow-up were considered dead with disease. Morbidity was periodically assessed (1 month after com- pletion of irradiation, at 4- to 6-month intervals for the first 3 years, and yearly thereafter). Significant sequelae were classified as moderate (Grade 2) when the symptoms persisted for longer than 30 days and required medication or minor surgical procedures (i.e., cauterization of bleed- ing telangiectasis or ulcers in the bladder or rectum) or hospitalization of fewer than 30 days; severe (Grade 3) when treatment required a major surgical procedure or repeated or prolonged hospitalization (> 30 days); or fatal (Grade 4). Morbidity and specific treatment data were recorded on computer-compatible forms and analyzed as described previously.
RESULTS
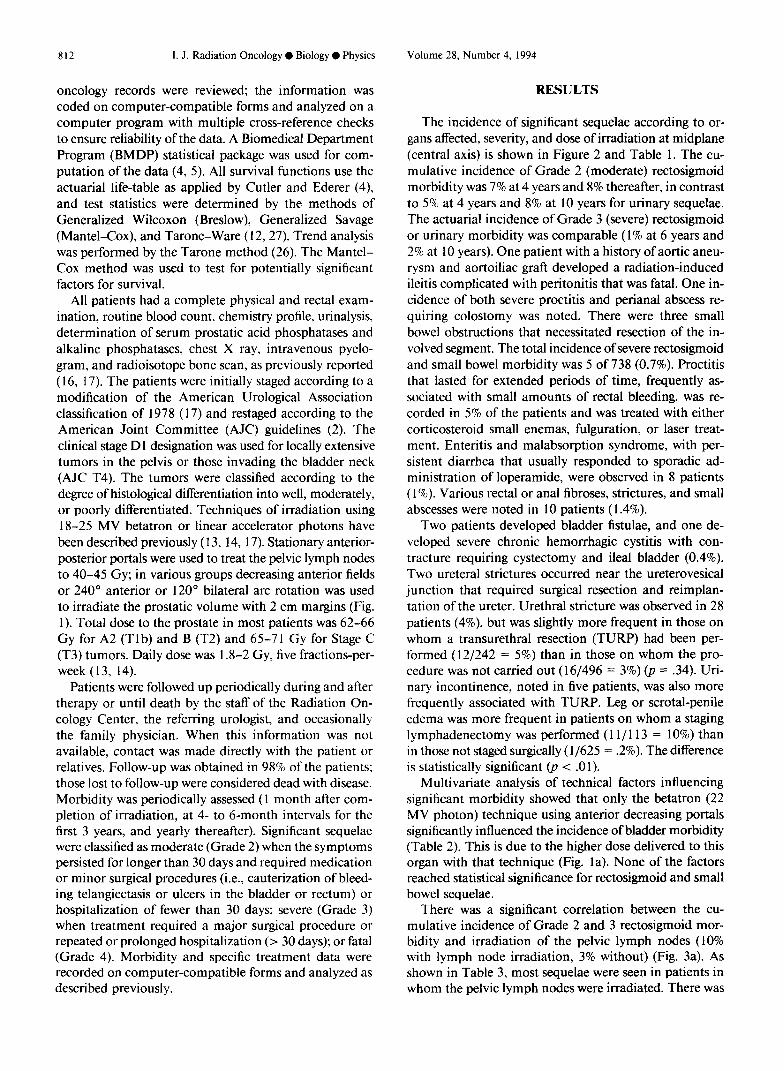
The incidence of significant sequelae according to or- gans affected, severity, and dose of irradiation at midplane (central axis) is shown in Figure 2 and Table 1. The cu- mulative incidence of Grade 2 (moderate) rectosigmoid morbidity was 7% at 4 years and 8% thereafter, in contrast to 5% at 4 years and 8% at 10 years for urinary sequelae. The actuarial incidence of Grade 3 (severe) rectosigmoid or urinary morbidity was comparable (1% at 6 years and 2% at 10 years). One patient with a history of aortic aneu- rysm and aortoiliac graft developed a radiation-induced ileitis complicated with peritonitis that was fatal. One in- cidence of both severe proctitis and perianal abscess re- quiring colostomy was noted. There were three small bowel obstructions that necessitated resection of the in- volved segment. The total incidence of severe rectosigmoid and small bowel morbidity was 5 of 738 (0.7%). Proctitis that lasted for extended periods of time, frequently as- sociated with small amounts of rectal bleeding, was re- corded in 5% of the patients and was treated with either corticosteroid small enemas, fulguration, or laser treat- ment. Enteritis and malabsorption syndrome, with per- sistent diarrhea that usually responded to sporadic ad- ministration of loperamide, were observed in 8 patients ( 1%). Various rectal or anal fibroses, strictures, and small abscesses were noted in 10 patients ( 1.4%).
Two patients developed bladder fistulae, and one de- veloped severe chronic hemorrhagic cystitis with con- tracture requiring cystectomy and ileal bladder (0.4%). Two ureteral strictures occurred near the ureterovesical junction that required surgical resection and reimplan- tation of the ureter. Urethral stricture was observed in 28 patients (4%) but was slightly more frequent in those on whom a transurethral resection (TURP) had been per- formed ( 12/242 = 5%) than in those on whom the pro- cedure was not carried out (16/496 = 3%) (p = .34). Uri- nary incontinence, noted in five patients, was also more frequently associated with TURP. Leg or scrotal-penile edema was more frequent in patients on whom a staging lymphadenectomy was performed ( 1 l/ 113 = 10%) than in those not staged surgically (l/625 = .2%). The difference is statistically significant 0, < .Ol).
Multivariate analysis of technical factors influencing significant morbidity showed that only the betatron (22 MV photon) technique using anterior decreasing portals significantly influenced the incidence of bladder morbidity (Table 2). This is due to the higher dose delivered to this organ with that technique (Fig. la). None of the factors reached statistical significance for rectosigmoid and small bowel sequelae.
There was a significant correlation between the cu- mulative incidence of Grade 2 and 3 rectosigmoid mor- bidity and irradiation of the pelvic lymph nodes (10% with lymph node irradiation, 3% without) (Fig. 3a). As shown in Table 3, most sequelae were seen in patients in whom the pelvic lymph nodes were irradiated. There was

Prostate: Radiation therapy and morbidity 0 C. A. PEREZ et al. 813
WASHINGTON U. - MIR. ST. LOUIS, MO. CARCINOMA OF PROSTATE PORTALS
AP 15x18 cm 14x 14 cm
6x 6 cm
PA 15x l8cm
a
b
ANT
22-25 MV X-RAYS
AP-PA- ISxlScm
240. ANT ARC
POST
d
PROSTATE 16 MVX
150’ BILATERAL ARCS
AP
e
16 MV X-RAYS
c f
Fig. 1. (a) Progressively decreasing treatment portals used with 22 MeV betatron X rays. (b) Dose to the bladder is 70-72 Gy and to the rectum between 60 and 65 Gy (14). (c) Portals used to irradiate the pelvic lymph nodes and prostate. (d) Isodose curves for 22-25 MV X rays using 18 X 15 cm AP-PA portals to deliver 50 Gy to the pelvis. Additional 15-20 Gy is given using 240” anterior arc. (e) Isodose curves for plan delivering 65-70 Gy to the prostate with 18 MV photons, bilateral 120” arcs, skipping 60” anterior and posterior vectors. (f) AP-PA and lateral fields used to deliver 45 Gy to the pelvis and 20-26 Gy to prostate with reduced fields, bilateral 120” arcs (13).

Volume 28, Number 4, 1994 814 I. J. Radiation Oncology 0 Biology 0 Physics
Table I. Carcinoma of the Prostate (MIR 1967- 1988): Seauelae correlated with central axis dose
Dose (Gv)
< 60 65 70 n = 52 n = 92 n = 594
(%) (%) (%)
Rectosigmoid and small bowel Moderate (Grade 2)
Proctitis Enteritis Rectal fibrosis/stricture Rectal ulcer Anal stricture/fissure Perianal abscess
Severe (Grade 3) Perianal abscess Proctitis Small bowel obstruction
Fatal (Grade 4) Radiation-induced ileitis’
Urinary Moderate (Grade 2)
Urethral stricture Cystitis (+- hematuria) Urinary incontinence Ureteral stricture
Severe (Grade 3) Vesicosigmoid fistula’ Rectovesical fistula Cystitis (hemorrhagic) Ureteral stricture
Other Moderate (Grade 2)
Subcutaneous fibrosis Scrotal ulcer Leg/scrotal/penile edema Impotence3
Severe (Grade 3) Pubic bone necrosis Pelvic soft tissue necrosis
1 (2) 5 (6) 30 (5) 8 (1) 3 (.5) 3 (.5) 3 (.5) 1 (4
1 (4 1 (2 3 (.5)
1 (3
1 (2) 27 (5) 1 (2) 2 (2) 11 (2) 1 (2) I(1) 3 (.5)
1 (3
1 C.2) 1 (3 1 t.21 2 (.3)
2 (.3) 1 C.2)
1 (2) 11 (2) 2 (4) 81 (14)
1 (2) 1 (3
’ History of aortic aneurysm and aortoiliac graft. ’ Sigmoid diverticulitis. 3 Only patients who were potent at the time of radiation ther-
apy.
CARCINOMA OF THE PROSTATE MIR 1967 - 1986
AECTOSIGMOID and URINARY SEQUELAE
I P- P 6c 4 2 4
0 2 4 6 8 10
YEARS AFTER TREATMENT
Fig. 2. Actuarial incidence of Grade 2 and 3 rectosigmoid and urinary sequelae.
no significant correlation between the volume irradiated (pelvic lymph nodes and prostate or prostate only) and the incidence of urinary sequelae (Fig. 3b). The size of the prostate boost field had no significant impact on the incidence of rectosigmoid or urinary morbidity, with or without pelvic lymph node irradiation (Figs. 4 and 5). In a univariate analysis, the cumulative incidence of recto- sigmoid Grade 2 and 3 morbidity was greater in patients treated to the pelvic lymph nodes with anterior-posterior (AP-PA) portals and rotational fields to the prostate than with other techniques (Fig. 6a). However, a higher inci- dence of urinary morbidity was observed with the betatron anterior decreasing fields technique (Fig. 6b). There is a somewhat higher incidence of rectosigmoid and urinary morbidity with doses over 69 Gy when the pelvic nodes are irradiated than in patients treated with lower doses, but the differences are not statistically significant (Fig. 7).
DISCUSSION
Because of the reported incidence of local-regional postirradiation recurrences (or positive needle biopsies)
Table 2. Carcinoma of the prostate (MIR 1967- 1988): Multivariate analysis of factors affecting Grade 2 and 3 genitourinary morbidity
Final model p-value of variables regression Exponent of the
entered into the coefficient regression Factor model (-t SE) coefficient
Decreasing fields vs. arc rotation .005 1.2836 + .3920 3.6096 Pelvic node irradiation ,131 -1.2950 f .6493 0.2739 Boost field size .622 -0.0049 I!I .0087 0.995 1 Treatment time < 7 weeks vs. > 7 weeks .607 0.4100 * .9193 1.5068 Daily fraction 1.8 vs. 2 Gy .733 -0.1249 f .3675 0.8826 Total tumor dose .I65 0.0003 f .0005 1.0003 Clinical stage .I94 0.2035 f .1444 1.2257 Pelvic lymphadenectomy .05 1 -1.0418 + .4578 0.3528 Age .I73 0.0293 f .0220 1.0297

Prostate: Radiation therapy and morbidity 0 C. A. PEREZ et al. 815
VEARSAFTERTHERAPV
a
CARCINOMA OF THE PROSTATE MIR 1967 - 1999
Urlnaty Grada 2 and 3 Sequelae Cormlat6d with Irradiated Volume
F 2 4 6 6 10 YEARS AFTER THERAPY
b
Fig. 3. Incidence of rectosigmoid (a) and urinary (b) Grade 2 and 3 sequelae correlated with irradiated volume.
after definitive irradiation of localized prostatic carcinoma (7, 2 1 ), an attempt has been made to deliver higher irra- diation doses in an effort to improve local-regional tumor control. This objective must be accomplished without in-
Table 3. Carcinoma of the prostate (MIR 1967-1988): Rectosigmoid and small bowel sequelae correlated
with pelvic node/prostate irradiation
Pelvis and prostate Prostate only n = 608 n= 130
(%) (%)
Moderate (Grade 2) Proctitis Rectal fibrosis/stricture Rectal ulcer Anal stricture/fissure Perianal abscess Enteritis
Severe (Grade 3) Perianal abscess Proctitis Small bowel obstruction
33 (5) 4 (3) 4 05) 2 (.3) 2 (.3) 1 (3 8 (5)
1 (3 1 t.3 3 U)
creasing morbidity that may affect the patient’s quality of life. As emphasized by Lawton et al. (9), there were only two treatment-related deaths in 1020 patients (one in our experience), demonstrating the low mortality rate with irradiation. The reported overall incidence of sig- nificant rectosigmoid or urinary sequelae in our experi- ence (3% severe and 7-10% moderate) is similar to that reported by others ( 1, 6, 9, 18, 19, 23).
In our patients, as in the analysis by Lawton et al. (9) of the RTOG randomized protocols, the most frequently noted rectosigmoid sequela was proctitis and in the uri- nary tract, urethral stricture and cystitis with bleeding (3- 6%). The incidence of intestinal obstruction-perforation in their series is comparable to ours (less than 1%).
We observed only one of 625 patients (. 1%) treated with irradiation alone who had leg or scrotal-penile edema in contrast to 10% (11 of 113) in those who underwent a staging lymphadenectomy (p < .O 1). This observation is consistent with that of Pilepich et al. (20) who found a positive correlation between the incidence of leg-penile edema and the extent of the pelvic lymphadenectomy.
CARCINOMA OF THE PROSTATE MIA 1967 - 1999
Rectoaigmokl Gmda 2 and 3 Saquelae Cormlated with Booat FleM Size
Pelvic Lymph Node lrmdlatlon Patients
VEARSAFTERTHERAPV
a
CARCINOMA OF THE PROSTATE MIR 1997 - 1999
Ractoaigmoid Grade 2 and 3 Sequclae Correlated with Booat Field Size
No Pelvic Lymph Nods lrradlatlon
0 2 4 6 6 10
YEARS AFTER THERAPY
b
Fig. 4. Incidence of rectosigmoid Grade 2 and 3 sequelae cor- related with boost field size. (a) Patients receiving pelvic lymph node and prostate irradiation. (b) Patients treated to the prostate only.
816 1. J. Radiation Oncology 0 Biology 0 Physics Volume 28, Number 4, 1994
CARCINOMA OF THE PROSTATE MIR 1667 - 1666
Urinary Grade 2 and 3 Sequelae Cornlated with Boost Field Size
Pelvic Lymph Node lrrsdlation Patients 30 -
4 5
YEARS AFTER THERAPY
a
20 -
CARCINOMA OF THE PROSTATE MIR lS67 - 1668
Urinary Grsde 2 and 3 Sequelaa Correlated with Boost Field Size
No Pelvic Lymph Node Irradiation
YEARS AFTER THERAPY
b
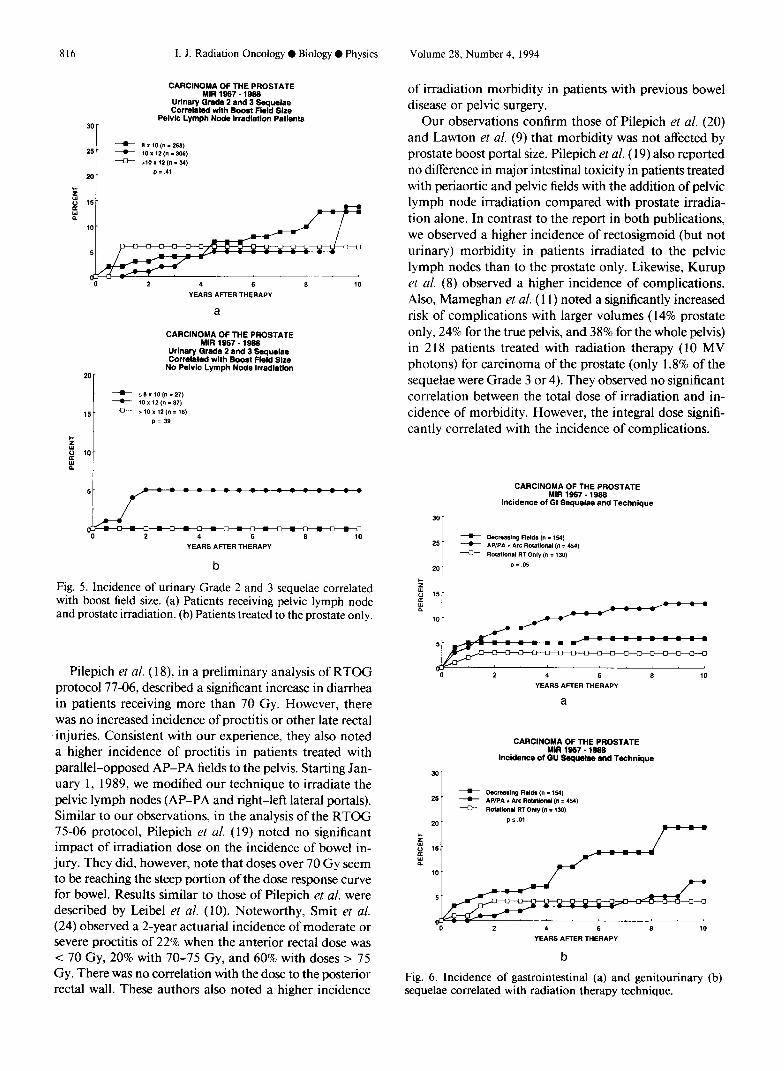
Fig. 5. Incidence of urinary Grade 2 and 3 sequelae correlated with boost field size. (a) Patients receiving pelvic lymph node and prostate irradiation. (b) Patients treated to the prostate only.
Pilepich et al. ( 18), in a preliminary analysis of RTOG protocol 77-06, described a significant increase in diarrhea in patients receiving more than 70 Gy. However, there was no increased incidence of proctitis or other late rectal injuries. Consistent with our experience, they also noted a higher incidence of proctitis in patients treated with parallel-opposed AP-PA fields to the pelvis. Starting Jan- uary 1, 1989, we modified our technique to irradiate the pelvic lymph nodes (AP-PA and right-left lateral portals). Similar to our observations, in the analysis of the RTOG 75-06 protocol, Pilepich et al. (19) noted no significant impact of irradiation dose on the incidence of bowel in- jury. They did, however, note that doses over 70 Gy seem to be reaching the steep portion of the dose response curve for bowel. Results similar to those of Pilepich et al. were described by Leibel et al. ( 10). Noteworthy, Smit et al. (24) observed a 2-year actuarial incidence of moderate or severe proctitis of 22% when the anterior rectal dose was < 70 Gy, 20% with 70-75 Gy, and 60% with doses > 75 Gy. There was no correlation with the dose to the posterior rectal wall. These authors also noted a higher incidence
of irradiation morbidity in patients with previous bowel disease or pelvic surgery.
Our observations confirm those of Pilepich et al. (20) and Lawton et al. (9) that morbidity was not affected by prostate boost portal size. Pilepich et al. ( 19) also reported no difference in major intestinal toxicity in patients treated with periaortic and pelvic fields with the addition of pelvic lymph node irradiation compared with prostate irradia- tion alone. In contrast to the report in both publications, we observed a higher incidence of rectosigmoid (but not urinary) morbidity in patients irradiated to the pelvic lymph nodes than to the prostate only. Likewise, Kurup et al. (8) observed a higher incidence of complications. Also, Mameghan et al. (11) noted a significantly increased risk of complications with larger volumes (14% prostate only, 24% for the true pelvis, and 38% for the whole pelvis) in 2 18 patients treated with radiation therapy ( 10 MV photons) for carcinoma of the prostate (only 1.8% of the sequelae were Grade 3 or 4). They observed no significant correlation between the total dose of irradiation and in- cidence of morbidity. However, the integral dose signifi- cantly correlated with the incidence of complications.
CARCINOMA OF THE PROSTATE MIR 1667 - 1666
Incidence of Gl Sequelae and Technique
2 4 5 8 10
YEARS AFTER THERAPY
a
CARCINOMA OF THE PROSTATE MlR 1667 - 1666
Incidence of GU Saquelae and Technique
30 -
- 25. -
-
YEARS AFTER THERAPY
b
Fig. 6. Incidence of gastrointestinal (a) and genitourinaty (b) sequelae correlated with radiation therapy technique.

Prostate: Radiation therapy and morbidity 0 C. A. PEREZ et nl. 817
CARCINOMA OF THE PROSTATE MIR 1987 - 1988
Grade 2-3 Sequelae Correlated with Dose
PROSTATE ONLY Rectosiamoid
3or PELVIS AND PROSTATE
--- 3 ̂ 3 0
*=zc=-==- Ot5z-~==OQ
-=‘==-=--I-=* 0 2 4 6 8
YEARS AFTER THERAPY
“0 2 4 5 8 10
YEARS AFTER THERAPY
Urinary PROSTATF ONI Y PFLVIS AND PROSTAIE
30
0 0 2 4 6 * 10
YEARS AFTER THERAPY YEARS AFTER THERAPY
Fig. 7. Incidence of rectosigmoid or urinary Grade 2 and 3 sequelae correlated with dose of irradiation in patients treated to the pelvis and prostate or to the-prostate only.
Rosen et al. (22) reported, in 229 patients treated with definitive irradiation, an incidence of urinary or bowel complications similar to ours. The authors described a higher incidence of significant complications with fields larger than 150 cm* (8.7% vs. 1.6%). For fields 150 cm* or smaller, treatment with bilateral arcs was associated with a lower complication rate than with opposed ante- rior-posterior or other rotational fields. Hanks et al. (6) and Lawton et al. (9) noted a significantly increased in- cidence of Grade 3, 4, and 5 urinary toxicity in patients receiving over 70 Gy (a = .03); in contrast, we did not observe a difference in Grade 2 and 3 urinary sequelae with increasing doses of irradiation up to 7 1 Gy. We did note a difference in Grade 2 and 3 urinary morbidity when correlated with the irradiation techniques (anterior-pos- terior reduced portals vs. rotational fields), the former de- livering higher doses of irradiation to the bladder.
As in our experience, Rosen et al. (22) reported that a higher proportion of patients with significant complica- tions had surgical staging procedures in addition to irra- diation.
These findings are highly relevant in light of recent at- tempts to increase the dose of irradiation delivered to the
prostate using 3-D treatment planning and conformal de- livery techniques. Soffen et al. (25) noted a 14% reduction of bladder and rectal volume included in the treated vol- ume using conformally blocked fields with a 1.5 cm mar- gin around the prostate contour in comparison with matched controls treated with conventional techniques. Acute urinary symptoms occurred in 77% and 80% of the patients, respectively, but only 3 1% of the patients treated with conformal technique required medication vs. 60% of the conventionally treated patients. Persistent symp- toms at or beyond the one-month follow-up were present in 11% of the former and 20% of the latter group. Late toxicity has not been evaluated because of the short follow- up. Likewise, Vijayakumar et al. (28) observed less acute bladder and rectal toxicity in 43 patients treated with beam’s eye view-based conformal irradiation than in 16 patients treated with conventional or 57 patients irradiated with computed tomography-based conventional tech- niques. The authors noted increased severity of toxicity with larger treated volume.
Our analysis, as well as reports from others ( 1,6,9, 16, 18, 19), documents an incidence of about 5% of Grade 2 and 3 rectosigmoid or urinary morbidity with doses of
818 I. J. Radiation Oncology 0 Biology 0 Physics Volume 28, Number 4, 1994
65-71 Gy. These findings are similar to those reported for carcinoma of the uterine cervix ( 15) in which a greater incidence of significant rectal morbidity was observed with doses > 75 Gy and for the bladder-ureter with doses of 80 Gy. Similar correlation was noted by Smit et al. (24) in patients irradiated for carcinoma of the prostate. Therefore, it should be possible to increase the dose of irradiation with 3-D treatment planning conformal therapy techniques to doses of at least 75 Gy without a substantial increase in morbidity, but extreme caution must be ex- ercised as we design dose escalation studies. It must be recognized that it will be impossible to substantially spare the trigone portion of the bladder or the anterior rectal wall since they are in close proximity to the prostate, without severely compromising adequate coverage of the target volume with a margin for position error. Neverthe- less, more precise treatment planning and better immo- bilization techniques, such as with an alpha cradle, should decrease systematic errors in repositioning and improve dose distribution in the volume of interest.
The present techniques of irradiation at our institution in patients treated to the pelvic lymph nodes is admin- istration of 45 Gy to the pelvic lymph nodes ( 1.8 Gy daily) with AP-PA and lateral fields, followed by a boost dose to the prostatic bed (22 Gy for Stage A2 and B and 26 Gy for Stage C) with bilateral 120” arc rotation. Patients treated to the prostate only for Stage A2 and B tumors receive 68 Gy with bilateral 120” arcs (2 Gy daily). Other techniques of irradiation including the box technique with reduced fields have been used at other institutions with satisfactory results.
CONCLUSION
This therapeutic approach is a reasonable alternative to nerve-sparing radical prostatectomy in patients with Stage A and B (T 1, T2) tumors and is the treatment of choice in patients with Stage C (T3, T4) lesions (1, 17, 24). Efforts to improve local-regional tumor control with higher doses of irradiation are in progress with appropri- ately designed clinical trials that will assess the potential of 3-D treatment planning and conformal delivery tech- niques to enhance our ability to more effectively treat these patients without increasing morbidity or decreasing their quality of life.
Our experience in a large number of patients treated At the present time we are conducting a prospective at a single institution, as well as that of others (6, 9, 18, randomized comparison of conventional therapy and 3- 19) in multiinstitutional studies, documents an acceptable D conformal therapy in localized carcinoma of the pros- incidence of treatment morbidity with definitive irradia- tate, incorporating cost effectiveness as an endpoint to be tion in patients with localized carcinoma of the prostate. analyzed.
REFERENCES
1. Bagshaw, M. A.; Cox, R. S.; Ramback, J. E. Radiation ther- apy for localized prostate cancer: Justification by long-term follow-up. Urol. Clin. N. Am. 17:787-802; 1990.
2. Beahrs, 0. H.; Henson, D. E.; Hutter, R. V. P.; Kennedy. B. J., eds. Manual for staging of cancer, 4th ed. Philadelphia, PA: J.B. Lippincott; 1992.
3. Cutler, S. J.; Ederer, F. Maximum utilization of the life table method in analyzing survival. J. Chron. Dis. 8:699- 713; 1958.
4. Dixon, W. J., ed. BMDP statistical software. Los Angeles. CA: University of California Press; 1982.
5. Dixon, W. J., ed. NEWS for 1987 release of BMDP statistical software. Los Angeles, CA: University of California Press; 1986.
6. Hanks, E. G.; Leibel, S. A.; Krall, J. M.; Kramer, S. Patterns of Care Studies: Dose-response observations for local control of adenocarcinoma of the prostate. Int. J. Radiat. Oncol. Biol. Phys. 11:153; 1985.
7. Kuban, D.; El-Mahdi, A. M.; Schellhammer, P. The signif- icance of postirradiation prostate biopsy with long-term follow-up. Int. J. Radiat. Oncol. Biol. Phys. 24(3):409-4 14; 1992.
8. Kurup, P.; Kramer, T. S.; Lee, M. S.; Phillips, R. External beam irradiation of prostate cancer: Experience in 163 pa- tients. Cancer 53:37-43; 1984.
9. Lawton, C. A.; Won, M.; Pilepich, M. V.; Asbell, S. 0.; Shipley, W. U.; Hanks, G. E.; Cox, J. D.; Perez, C. A.; Sause, W. T.; Doggett, S. R. L.; Rubin, P. Long-term treatment sequelae following external beam irradiation for adenocar- cinema of the prostate: Analysis of RTOG studies 7506 and 7706. Int. J. Radiat. Oncol. Biol. Phys. 21:935-939; 1991.
10. Leibel, S. A.; Hanks, G. E.; Kramer, S. Patterns of Care
Outcome Studies: Results of the national practice in ade- nocarcinoma of the prostate. Int. J. Radiat. Oncol. Biol. Phys. lo:40 l-409; 1984.
11. Mameghan, H.; Fisher, R.; Mameghan, J.; Watt, W. H.; Tynan, A. Bowel complications after radiotherapy for car- cinoma of the prostate: The volume effect. Int. J. Radiat. Oncol. Biol. Phys. 18:3 15-320; 1990.
12. Miller, R. Survival analysis. New York, NY: John Wiley and Sons; 198 1.
13. Perez, C. A. Prostate. In: Perez, C. A., Brady, L. W., eds. Principles and practice of radiation oncology, 2nd ed. Phil- adelphia, PA: Lippincott Co.; 1992: 1067- 1116.
14. Perez, C. A.; Ackerman, L. V.; Silber, I.; Royce R. K. Ra- diation therapy in the treatment of localized carcinoma of the prostate: Preliminary report using 22 MeV photons. Cancer 34:1059-1068; 1974.
15. Perez, C. A.; Fox, S.; Lockett, M. A.; Grigsby, P. W.; Camel, H. M.; Galakatos A.; Kao, M.-S.; Williamson, J. Impact of dose in outcome of irradiation alone in carcinoma of the uterine cervix: Analysis of two different methods. Int. J. Radiat. Oncol. Biol. Phys. 21:885-898; 199 1.
16. Perez, C. A.; Lee, H. K.; Georgiou A.; Logsdon, M. D.; Lai, P. P.; Locket& M. A. Technical and tumor-related factors affecting outcome of definitive irradiation for localized car- cinoma of the prostate. Int. J. Radiat. Oncol. Biol. Phys. 26:581-591; 1993.
17. Perez, C. A.; Pilepich, M. V.; Garcia, D.; Simpson, J. R.; Zivnuska, F. Definitive radiation therapy in carcinoma of the prostate localized to the pelvis: Experience at the Mal- linckrodt Institute of Radiology. N.C.I. Monogr. 7:85-94; 1988.
18. Pilepich, M. V.; Asbell, S. 0.; Krall, J. M.; Baerwald, W. H.;

Prostate: Radiation therapy and morbidity 0 C. A. PEREZ et al. 819
19.
20.
21.
22.
Sause, W. T.; Rubin, P.; Emami, B. N.; Pidcock, G. M. Correlation of radiotherapeutic parameters and treatment related morbidity: Analysis of RTOG study 77-06. Int. J. Radiat. Oncol. Biol. Phys. 13:1007-1012; 1987.
Pilepich, M. V.; Krall, J. M.; Sause, W. T.; Johnson, R. J.; Russ, H. H.; Hanks, G. E.; Perez, C. A.; Zinninger, M.; Martz, K. L.; Gardner, P. Correlation of radiotherapeutic parameters and treatment related morbidity in carcinoma of the prostate: Analysis of RTOG study 75-06. Int. J. Ra- diat. Oncol. Biol. Phys. 13:35 l-357; 1987. Pilepich, M. V.; Pajak, T.; George, F. W.; Asbell, S. 0.; Stetz, J.; Zinninger, M.; Plenk, H. P.; Johnson, R. J.; Mul- holland, S. G.; Walz, B. J.; Kalish, L. Preliminary report on phase III RTOG studies of extended-field irradiation in car- cinoma of the prostate. Am. J. Clin. Oncol. (CCT) 6:485- 491; 1983. Prestidge, B.; Kaplan, I.; Cox, R. S.; Bagshaw, M. A. The clinical significance of a positive postirradiation prostatic biopsy without metastases. Int. J. Radiat. Oncol. Biol. Phys. 24( 3):403-408; 1992.
Rosen, E.; Cassady, R.; Connolly, J. R.; Chaffey, J. T. Ra- diotherapy for prostate carcinoma: The JCRT experience ( 1968- 1978). II. Factors related to tumor control and com- plications. Int. J. Radiat. Oncol. Biol. Phys. I1:725-730; 1985.
23.
24.
25.
26.
27.
28.
Shipley, W. U.; Prout, G. R., Jr.; Coachman, N. M.; McManus, P. L.; Healey, E. A.; Althausen, A. F.; Heney, N. M.; Parkhurst, E. C.; Young, H. H.; Shipley, J. W.; Kaufman, S. D. Radiation therapy for localized prostate carcinoma: Experience at the Massachusetts General Hos- pital (1973-1981). N.C.I. Monogr. 7:67-73; 1988. Smit, W. G. J. M.; Helle, P. A.; van Putten, W. L. J.; Wijnmaalen, A. J.; Seldenrath, J. J.; van der Werf-Messing, B. H. P. Late radiation damage in prostate cancer patients treated by high dose external radiotherapy in relation to rectal dose. Int. J. Radiat. Oncol. Biol. Phys. 18:23-29; 1990. Soffen, E. M.; Hanks, G. E.; Hunt, M. A.; Epstein, B. E. Conformal static field radiation therapy treatment of early prostate cancer vs. nonconformal techniques: A reduction in acute morbidity. Int. J. Radiat. Oncol. Biol. Phys. 24(3): 485-488; 1992. Tarone, R. Tests for trend in life table analysis. Biometrika 62:679-682; 1975. Tarone, R.; Ware, J. On distribution free tests for equality of survival distributions. Biometrika 64: 156- 160; 1977. Vijayakumar, K.; Awan, A.; Karrison, T.; Culbert, H.; Chan, S.: Kolker, J.; Low, N.; Halpern, H.; Rubin, S.; Chen, G. T. Y.; Weichselbaum, R. R. Acute toxicity during ex- ternal-beam radiotherapy for localized prostate cancer: Comparison of different techniques. Int. J. Radiat. Oncol. Biol. Phys. 25:359-37 I ; 1993.