Symptoms of depression and stress mediate the effect of pain on disability
8
Symptoms of depression and stress mediate the effect of pain on disability Amanda M. Hall a,⇑ , Steven J. Kamper a , Chris G. Maher a,b , Jane Latimer a,b , Manuela L. Ferreira c , Michael K. Nicholas d a The George Institute for Global Health, PO Box M201, Missenden Road, NSW 2050, Australia b Sydney Medical School, The University of Sydney, St. Leonard’s, NSW 2065, Australia c Faculty of Health Sciences, The University of Sydney, St. Leonard’s, NSW 2065, Australia d Pain Management Research Institute, The University of Sydney at Royal North Shore Hospital, St. Leonard’s, NSW 2065, Australia Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article. article info Article history: Received 8 October 2010 Received in revised form 24 December 2010 Accepted 7 January 2011 Keywords: Pain Disability Chronicity Psychological distress Depression Mediation abstract The mechanism or mechanisms involved in the development of pain-related disability in people with low back pain is unclear. Psychological distress has been identified as one potential pathway by which an epi- sode of pain influences the development of persistent disabling symptoms; however, the relationship has not been formally investigated. This study investigated the causal relationship between pain and disabil- ity via psychological distress (and its components depression, stress, and anxiety) by using mediation path analysis. The study sample included 231 participants with subacute low back pain (6 to 12 weeks’ pain duration) who had been recruited for an exercise-based randomised, controlled trial. All participants completed self-report assessments of pain (0–10 numerical rating scale), disability (Roland Morris Dis- ability Questionnaire), and psychological distress (Depression Anxiety and Stress Scale) at baseline and again at 2 follow-up time points (6 and 12 weeks after baseline). The results of the mediation analysis suggest that approximately 30% of the relationship between subacute pain and later disability is depen- dent on the level of patients’ psychological distress. The finding that psychological distress only partially (30%) mediated the pain-disability relationship indicates that other factors should also be explored. Fur- ther analysis into the components of psychological distress revealed that the symptoms of depression and stress, but not anxiety, are responsible for mediation of the pain-disability relationship. These find- ings provide an opportunity to decrease the risk of long-term disability through early identification and management of depressive and stress symptoms. Crown Copyright Ó 2011 Published by Elsevier B.V. on behalf of International Association for the Study of Pain. All rights reserved. 1. Introduction Low back pain (LBP) affects 22% to 65% of people worldwide [19], ranking in the top 7 most common reasons for consulting a general practitioner in Australia [20] and the United States [2]. Despite the multitude of treatments for people with LBP, few seem to be particularly successful in preventing the transition to chronicity. This is evidenced by approximately one-third of acute episodes resulting in persistent symptoms including re- duced work productivity and physical function [5]. Although high initial pain intensity is associated with longer recovery time for patients with acute LBP [5], the mechanisms by which initial pain contributes to the development of subsequent disability are unclear. It is widely accepted that psychological factors are potentially influential in the development of pain-related disabil- ity and work loss [7], and assessment of these factors has been recommended to help predict long-term outcome [8]. However, failure of many previous studies to recruit subjects with uniform durations of LBP means that the predictive value of psychosocial factors in the early stages of the condition remains unclear [14]. Three recent studies enrolled an inception cohort to investigate the association of psychosocial factors at pain onset with outcome at long-term follow-up [4,5,17]. These studies reported significant independent associations between psychological distress and non- recovery at 3 months. For instance, people with nonspecific back pain presenting to primary care were 4.1 times more likely to still have symptoms at 3 months if they reported high levels of distress at presentation [4]. Likewise, people with work-related back pain seeking outpatient care who reported ‘‘feeling under stress most or all of the time’’ were 4.45 times more likely to have unresolved pain at 3 months compared to those who reported ‘‘feeling under 0304-3959/$36.00 Crown Copyright Ó 2011 Published by Elsevier B.V. on behalf of International Association for the Study of Pain. All rights reserved. doi:10.1016/j.pain.2011.01.014 ⇑ Corresponding author. Tel.: +61 2 9657 0391; fax: +61 2 9657 0301. E-mail address: [email protected] (A.M. Hall). www.elsevier.com/locate/pain PAIN Ò 152 (2011) 1044–1051
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Symptoms of depression and stress mediate the effect of pain on disability

w w w . e l s e v i e r . c o m / l o c a t e / p a i n
PAIN�
152 (2011) 1044–1051
Symptoms of depression and stress mediate the effect of pain on disability
Amanda M. Hall a,⇑, Steven J. Kamper a, Chris G. Maher a,b, Jane Latimer a,b,Manuela L. Ferreira c, Michael K. Nicholas d
a The George Institute for Global Health, PO Box M201, Missenden Road, NSW 2050, Australiab Sydney Medical School, The University of Sydney, St. Leonard’s, NSW 2065, Australiac Faculty of Health Sciences, The University of Sydney, St. Leonard’s, NSW 2065, Australiad Pain Management Research Institute, The University of Sydney at Royal North Shore Hospital, St. Leonard’s, NSW 2065, Australia
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
a r t i c l e i n f o a b s t r a c t
Article history:Received 8 October 2010Received in revised form 24 December 2010Accepted 7 January 2011
Keywords:PainDisabilityChronicityPsychological distressDepressionMediation
0304-3959/$36.00 Crown Copyright � 2011 Publishedoi:10.1016/j.pain.2011.01.014
⇑ Corresponding author. Tel.: +61 2 9657 0391; faxE-mail address: [email protected] (A.M. H
The mechanism or mechanisms involved in the development of pain-related disability in people with lowback pain is unclear. Psychological distress has been identified as one potential pathway by which an epi-sode of pain influences the development of persistent disabling symptoms; however, the relationship hasnot been formally investigated. This study investigated the causal relationship between pain and disabil-ity via psychological distress (and its components depression, stress, and anxiety) by using mediationpath analysis. The study sample included 231 participants with subacute low back pain (6 to 12 weeks’pain duration) who had been recruited for an exercise-based randomised, controlled trial. All participantscompleted self-report assessments of pain (0–10 numerical rating scale), disability (Roland Morris Dis-ability Questionnaire), and psychological distress (Depression Anxiety and Stress Scale) at baseline andagain at 2 follow-up time points (6 and 12 weeks after baseline). The results of the mediation analysissuggest that approximately 30% of the relationship between subacute pain and later disability is depen-dent on the level of patients’ psychological distress. The finding that psychological distress only partially(30%) mediated the pain-disability relationship indicates that other factors should also be explored. Fur-ther analysis into the components of psychological distress revealed that the symptoms of depressionand stress, but not anxiety, are responsible for mediation of the pain-disability relationship. These find-ings provide an opportunity to decrease the risk of long-term disability through early identification andmanagement of depressive and stress symptoms.Crown Copyright � 2011 Published by Elsevier B.V. on behalf of International Association for the Study of
Pain. All rights reserved.
1. Introduction
Low back pain (LBP) affects 22% to 65% of people worldwide[19], ranking in the top 7 most common reasons for consulting ageneral practitioner in Australia [20] and the United States [2].Despite the multitude of treatments for people with LBP, fewseem to be particularly successful in preventing the transitionto chronicity. This is evidenced by approximately one-third ofacute episodes resulting in persistent symptoms including re-duced work productivity and physical function [5]. Althoughhigh initial pain intensity is associated with longer recovery timefor patients with acute LBP [5], the mechanisms by which initialpain contributes to the development of subsequent disability areunclear. It is widely accepted that psychological factors are
d by Elsevier B.V. on behalf of Inte
: +61 2 9657 0301.all).
potentially influential in the development of pain-related disabil-ity and work loss [7], and assessment of these factors has beenrecommended to help predict long-term outcome [8]. However,failure of many previous studies to recruit subjects with uniformdurations of LBP means that the predictive value of psychosocialfactors in the early stages of the condition remains unclear [14].
Three recent studies enrolled an inception cohort to investigatethe association of psychosocial factors at pain onset with outcomeat long-term follow-up [4,5,17]. These studies reported significantindependent associations between psychological distress and non-recovery at 3 months. For instance, people with nonspecific backpain presenting to primary care were 4.1 times more likely to stillhave symptoms at 3 months if they reported high levels of distressat presentation [4]. Likewise, people with work-related back painseeking outpatient care who reported ‘‘feeling under stress mostor all of the time’’ were 4.45 times more likely to have unresolvedpain at 3 months compared to those who reported ‘‘feeling under
rnational Association for the Study of Pain. All rights reserved.

A.M. Hall et al. / PAIN�
152 (2011) 1044–1051 1045
stress none or little of the time’’ [17]. Additionally, each unit of in-crease reported by patients on a depression scale decreased therate of recovery by 9% [5]. Although these data clearly identifythe association between psychological distress and outcome, itdoes not provide information on how they are related.
Attempting to explore the development of chronic disability,researchers have proposed a theoretical model linking initial painwith long-term disability via psychological distress, whereby thepresence of pain induces psychological distress leading to ongoingdisability [16]. However, this model remains untested. Explorationof this model could provide insight into the development of pa-tient-relevant outcomes and lead to improved management forthis prevalent condition.
One way to determine whether symptoms of psychological dis-tress are indeed along the causal pathway between initial pain andlater disability is via mediation analyses [1]. This process allowsexploration of 2 pathways by which the independent variable (pain)affects the dependent variable (disability): via a direct path as well asvia an indirect path through a mediating variable (psychologicaldistress).
The primary aim of this study was to test the hypothesis thatpsychological distress mediates the relationship between painand disability. If psychological distress was confirmed as amediating variable, secondary analyses explored the contribu-tions of the following constituent factors: depression, anxiety,and stress.
2. Methods
2.1. Participants
Data used in this analysis were collected as part of a random-ised placebo-controlled trial investigating the effectiveness ofexercise and/or advice for people with subacute LBP (6 to 12weeks’ pain duration) [15]. Participants were recruited from hospi-tal waiting lists, community advertisements, and referrals fromhealth care professionals in Australia and New Zealand. The exclu-sion criteria included serious spinal pathology, previous spinal sur-gery, and pregnancy. Participants were assessed at baseline (t1),directly after the treatment (t2, 6 weeks after randomization),and again at follow-up (t3, after 12 weeks).
2.2. Measurements
At each assessment point, subjects rated their pain intensity ona numerical rating scale (NRS), disability on the Roland Morris Dis-ability Questionnaire (RMDQ), and psychological distress on theDepression Anxiety and Stress Scale (DASS). The pain intensityNRS measures the participant’s average pain in the past 24 h on a0–10 scale where 0 is ‘‘no pain’’ and 10 is ‘‘worst pain possible’’[13]. The RMDQ consists of 24 yes/no items regarding the impactof back pain on activities of daily living. Each item that is answered‘‘yes’’ is scored 1 point, with scores ranging from 0, representing‘‘no disability,’’ to 24, representing ‘‘extremely severe disability’’[12]. The DASS-21 is a set of 3 self-report scales designed to mea-sure symptoms of psychological distress including depression, anx-iety, and stress [11]. The Depression scale assesses low positiveaffect, loss of self-esteem and incentive, and sense of hopelessness.The Anxiety scale assesses autonomic arousal and fearfulness(physiological hyperarousal). The Stress scale assesses difficultyrelaxing, persistent tension, irritability, and low threshold forbecoming upset or frustrated. Each of the 3 scales contains 7 itemsthat can be summed to represent a composite measure of negativeemotional symptoms or psychological distress [11].
2.3. Analysis
The criteria for mediation as proposed by Baron and Kenny[1] were used to test whether psychological distress mediatesthe relationship between the independent and the dependentvariable. The criteria require that 4 conditions be met to estab-lish mediation between the independent (pain) and dependent(disability) variables: (1) pain is related to disability, (2) painis related to the mediator (psychological distress), (3) psycholog-ical distress is related to disability when pain is controlled, and(4) the effect of pain on disability is reduced or eliminated aftercontrolling for psychological distress. The different pathways bywhich these variables are related are termed as follows: the rela-tionship between pain and disability without adjustment is thetotal effect; the effect of pain on disability via psychological dis-tress is the indirect effect; and the effect of pain on disability,adjusted for psychological distress is the direct effect. Theseterms have been derived from Cole and Maxwell and reportedby Baron and Kenny [1]. These pathways are depicted in Table 1.All analyses were preplanned and were conducted by linearregression with SPSS software, version 16.0.
2.4. Longitudinal analysis
To explore the causal pathways from the independent variable(pain) to the dependent variable (disability) via the mediating var-iable (psychological distress), longitudinal data at 3 time points arerequired to provide information regarding temporal precedence.The analysis of covariance method uses scores from each of the 3time points and includes the baseline values of the mediator andindependent variable as covariates in the analysis. Using data from3 time points accounts for the time the independent variable (mea-sured at t1) takes to exert an effect on the mediating variable(measured at t2) and then for the time the mediating variable takesto exert an effect on the dependent variable (measured at t3). Inthis method, the mediated or indirect path (a � b) reflects the prod-uct of (a) the association between the pain at t1 and psychologicaldistress at t2 after adjustment for psychological distress at t1 and(b) the association between psychological distress at t2 and dis-ability at t3 after adjustment for both pain and psychological dis-tress at t1. This method may underestimate the magnitude of thetrue mediated effect if the effect of pain on psychological distresshas already occurred before measurement at t1. At t1, patientshad experienced pain for 6 to 12 weeks; t2 was 6 weeks later,and t3 was 6 weeks after that.
Evidence suggests that symptoms of psychological distress arepresent in patients within the first few weeks after an acute epi-sode of pain [5]. To determine whether this was the case in ourdata set, we also planned an analysis using psychological distressat t1 (rather than t2) as the mediating variable. In this analysis,the mediated or indirect path (a � b) reflects the product of (a)the association between the pain at t1 and psychological distressat t1 and (b) the association between psychological distress at t1and disability at t3 after adjustment for pain at t1 (Table 2). Thisanalysis method does limit the ability to infer causation, in termsof confirming whether pain causes symptoms of psychological dis-tress, because both variables are measured at the same time point.However, the DASS measurement of symptoms of psychologicaldistress was derived specifically for people with physical rehabili-tation conditions and is aimed at measuring distress symptoms asa result of the pain experience. We recognise that future research,with rigorous methods to measure variables at earlier time points,would be necessary to investigate any interaction effects and con-firm a causal relationship between pain and psychological distress.
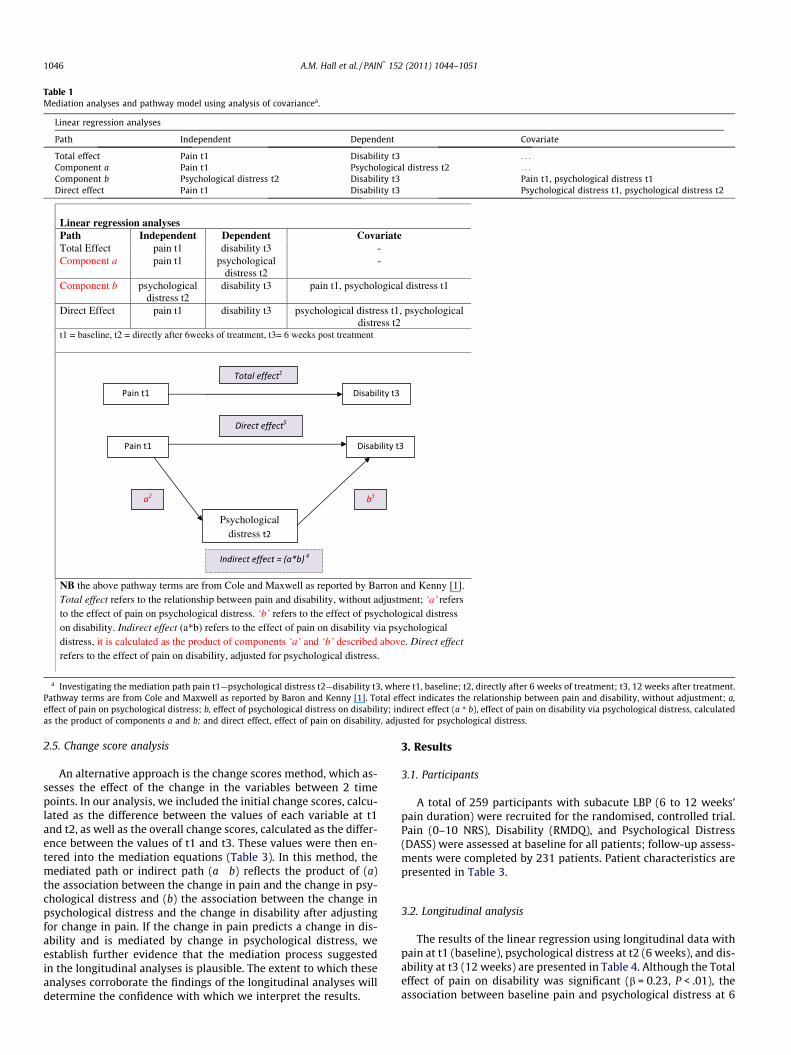
Table 1Mediation analyses and pathway model using analysis of covariancea.
Linear regression analyses
Path Independent Dependent Covariate
Total effect Pain t1 Disability t3 . . .
Component a Pain t1 Psychological distress t2 . . .
Component b Psychological distress t2 Disability t3 Pain t1, psychological distress t1Direct effect Pain t1 Disability t3 Psychological distress t1, psychological distress t2
Linear regression analyses Path Independent Dependent Covariate Total Effect pain t1 disability t3 - Component a pain t1 psychological
distress t2 -
Component b psychological distress t2
disability t3 pain t1, psychological distress t1
Direct Effect pain t1 disability t3 psychological distress t1, psychological distress t2
t1 = baseline, t2 = directly after 6weeks of treatment, t3= 6 weeks post treatment
NB the above pathway terms are from Cole and Maxwell as reported by Barron and Kenny [1]. Total effect refers to the relationship between pain and disability, without adjustment; ‘a’ refers to the effect of pain on psychological distress. ‘b’ refers to the effect of psychological distress on disability. Indirect effect (a*b) refers to the effect of pain on disability via psychological distress, it is calculated as the product of components ‘a’ and ‘b’ described above. Direct effect refers to the effect of pain on disability, adjusted for psychological distress.
Psychological distress
a Investigating the mediation path pain t1—psychological distress t2—disability t3, where t1, baseline; t2, directly after 6 weeks of treatment; t3, 12 weeks after treatment.Pathway terms are from Cole and Maxwell as reported by Baron and Kenny [1]. Total effect indicates the relationship between pain and disability, without adjustment; a,effect of pain on psychological distress; b, effect of psychological distress on disability; indirect effect (a * b), effect of pain on disability via psychological distress, calculatedas the product of components a and b; and direct effect, effect of pain on disability, adjusted for psychological distress.
1046 A.M. Hall et al. / PAIN�
152 (2011) 1044–1051
2.5. Change score analysis
An alternative approach is the change scores method, which as-sesses the effect of the change in the variables between 2 timepoints. In our analysis, we included the initial change scores, calcu-lated as the difference between the values of each variable at t1and t2, as well as the overall change scores, calculated as the differ-ence between the values of t1 and t3. These values were then en-tered into the mediation equations (Table 3). In this method, themediated path or indirect path (a � b) reflects the product of (a)the association between the change in pain and the change in psy-chological distress and (b) the association between the change inpsychological distress and the change in disability after adjustingfor change in pain. If the change in pain predicts a change in dis-ability and is mediated by change in psychological distress, weestablish further evidence that the mediation process suggestedin the longitudinal analyses is plausible. The extent to which theseanalyses corroborate the findings of the longitudinal analyses willdetermine the confidence with which we interpret the results.
3. Results
3.1. Participants
A total of 259 participants with subacute LBP (6 to 12 weeks’pain duration) were recruited for the randomised, controlled trial.Pain (0–10 NRS), Disability (RMDQ), and Psychological Distress(DASS) were assessed at baseline for all patients; follow-up assess-ments were completed by 231 patients. Patient characteristics arepresented in Table 3.
3.2. Longitudinal analysis
The results of the linear regression using longitudinal data withpain at t1 (baseline), psychological distress at t2 (6 weeks), and dis-ability at t3 (12 weeks) are presented in Table 4. Although the Totaleffect of pain on disability was significant (b = 0.23, P < .01), theassociation between baseline pain and psychological distress at 6
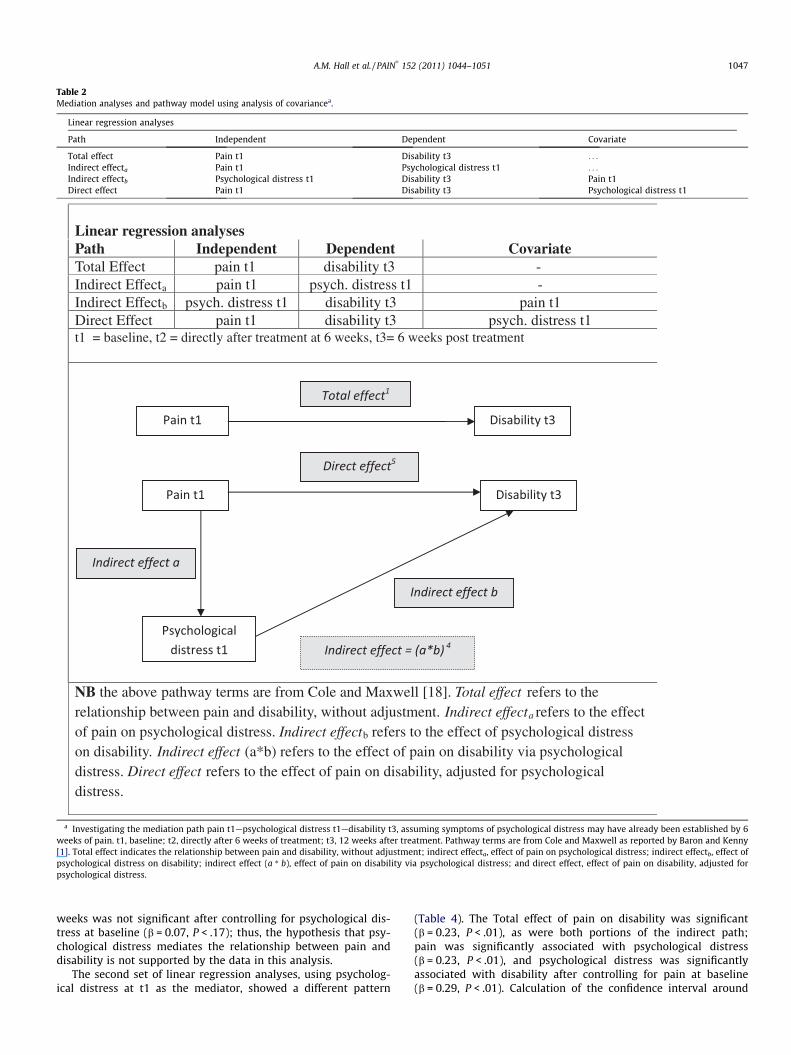
Table 2Mediation analyses and pathway model using analysis of covariancea.
Linear regression analyses
Path Independent Dependent Covariate
Total effect Pain t1 Disability t3 . . .
Indirect effecta Pain t1 Psychological distress t1 . . .
Indirect effectb Psychological distress t1 Disability t3 Pain t1Direct effect Pain t1 Disability t3 Psychological distress t1
Linear regression analyses Path Independent Dependent Covariate Total Effect pain t1 disability t3 - Indirect Effecta pain t1 psych. distress t1 - Indirect Effectb psych. distress t1 disability t3 pain t1 Direct Effect pain t1 disability t3 psych. distress t1 t1 = baseline, t2 = directly after treatment at 6 weeks, t3= 6 weeks post treatment
NB the above pathway terms are from Cole and Maxwell [18]. Total effect refers to the relationship between pain and disability, without adjustment. Indirect effecta refers to the effect of pain on psychological distress. Indirect effectb refers to the effect of psychological distress on disability. Indirect effect (a*b) refers to the effect of pain on disability via psychological distress. Direct effect refers to the effect of pain on disability, adjusted for psychological distress.
a Investigating the mediation path pain t1—psychological distress t1—disability t3, assuming symptoms of psychological distress may have already been established by 6weeks of pain. t1, baseline; t2, directly after 6 weeks of treatment; t3, 12 weeks after treatment. Pathway terms are from Cole and Maxwell as reported by Baron and Kenny[1]. Total effect indicates the relationship between pain and disability, without adjustment; indirect effecta, effect of pain on psychological distress; indirect effectb, effect ofpsychological distress on disability; indirect effect (a * b), effect of pain on disability via psychological distress; and direct effect, effect of pain on disability, adjusted forpsychological distress.
A.M. Hall et al. / PAIN�
152 (2011) 1044–1051 1047
weeks was not significant after controlling for psychological dis-tress at baseline (b = 0.07, P < .17); thus, the hypothesis that psy-chological distress mediates the relationship between pain anddisability is not supported by the data in this analysis.
The second set of linear regression analyses, using psycholog-ical distress at t1 as the mediator, showed a different pattern
(Table 4). The Total effect of pain on disability was significant(b = 0.23, P < .01), as were both portions of the indirect path;pain was significantly associated with psychological distress(b = 0.23, P < .01), and psychological distress was significantlyassociated with disability after controlling for pain at baseline(b = 0.29, P < .01). Calculation of the confidence interval around
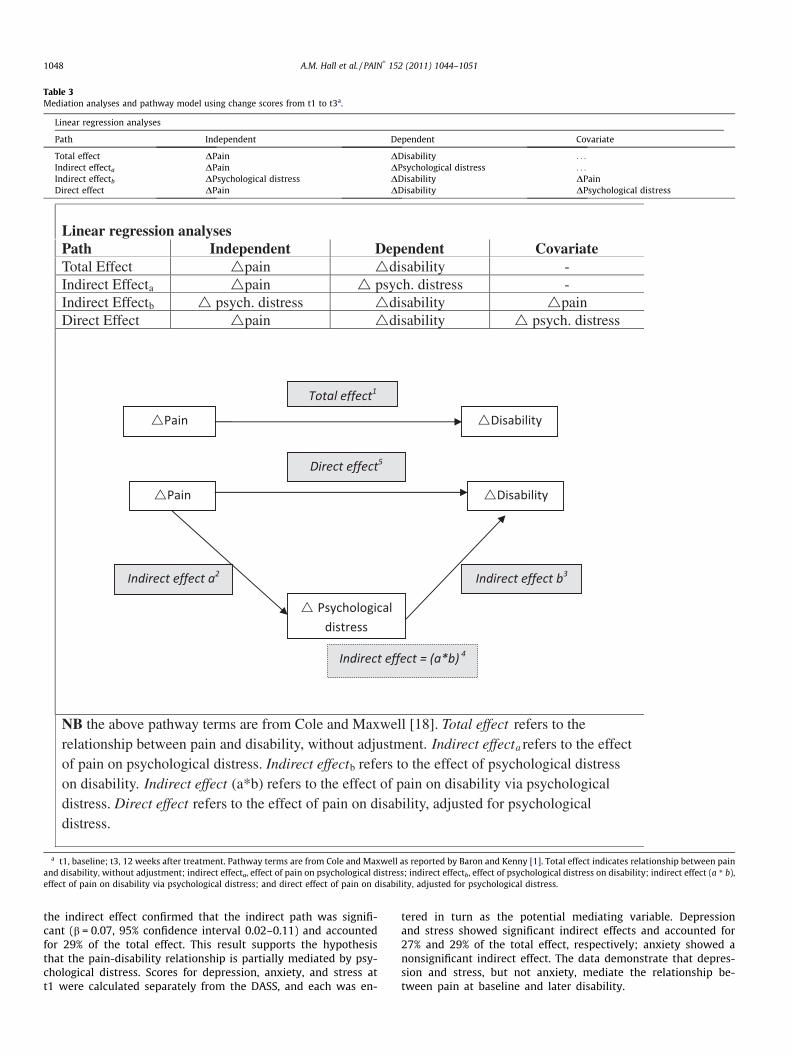
Table 3Mediation analyses and pathway model using change scores from t1 to t3a.
Linear regression analyses
Path Independent Dependent Covariate
Total effect DPain DDisability . . .
Indirect effecta DPain DPsychological distress . . .
Indirect effectb DPsychological distress DDisability DPainDirect effect DPain DDisability DPsychological distress
Linear regression analyses Path Independent Dependent Covariate Total Effect pain disability - Indirect Effecta pain psych. distress - Indirect Effectb psych. distress disability pain Direct Effect pain disability psych. distress
NB the above pathway terms are from Cole and Maxwell [18]. Total effect refers to the relationship between pain and disability, without adjustment. Indirect effecta refers to the effect of pain on psychological distress. Indirect effectb refers to the effect of psychological distress on disability. Indirect effect (a*b) refers to the effect of pain on disability via psychological distress. Direct effect refers to the effect of pain on disability, adjusted for psychological distress.
a t1, baseline; t3, 12 weeks after treatment. Pathway terms are from Cole and Maxwell as reported by Baron and Kenny [1]. Total effect indicates relationship between painand disability, without adjustment; indirect effecta, effect of pain on psychological distress; indirect effectb, effect of psychological distress on disability; indirect effect (a * b),effect of pain on disability via psychological distress; and direct effect of pain on disability, adjusted for psychological distress.
1048 A.M. Hall et al. / PAIN�
152 (2011) 1044–1051
the indirect effect confirmed that the indirect path was signifi-cant (b = 0.07, 95% confidence interval 0.02–0.11) and accountedfor 29% of the total effect. This result supports the hypothesisthat the pain-disability relationship is partially mediated by psy-chological distress. Scores for depression, anxiety, and stress att1 were calculated separately from the DASS, and each was en-
tered in turn as the potential mediating variable. Depressionand stress showed significant indirect effects and accounted for27% and 29% of the total effect, respectively; anxiety showed anonsignificant indirect effect. The data demonstrate that depres-sion and stress, but not anxiety, mediate the relationship be-tween pain at baseline and later disability.

Table 4Mediation effect using analysis of covariance.a
Psychologicaldistress measure
Totaleffect
Directeffect
Indirecteffect
95%Confidenceinterval
Proportionmediated(%)
DepressionAnxiety andStress Scale
0.23 0.16 0.07 0.02 to 0.11 30.0
Depression 0.23 0.16 0.06 0.02 to 0.11 26.8Anxiety 0.23 0.20 0.03 �0.00 to 0.06 12.9Stress 0.23 0.16 0.06 0.02 to 0.11 28.0
a Investigating the mediation path pain t1—psychological distress t1—disabilityt3, where t1, baseline; t2, directly after 6 weeks of treatment; t3, 12 weeks aftertreatment. All effects are reported as standardized b. Total effect indicates rela-tionship between pain and disability, without adjustment; direct effect, effect ofpain on disability, adjusted for mediator; indirect effect, effect of pain on disabilityvia mediator. Support for meditation: if the indirect effect (a * b) is significant, thensupport significant partial mediation.
Table 5Mediation effect using change scores.a
Psychologicaldistress measure
Totaleffect
Directeffect
Indirecteffect
95%Confidenceinterval
Proportionmediated(%)
t1–t3DTotal Depression
Anxiety andStress Scale
0.53 0.48 0.05 0.01 to 0.08 9.0
DDepression 0.53 0.50 0.06 0.00 to 0.06 5.5DAnxiety 0.53 0.51 0.04 �0.00 to 0.04 3.7DStress 0.53 0.48 0.09 0.01 to 0.08 8.9
t1–t2DTotal Depression
Anxiety andStress Scale
0.48 0.42 0.06 0.02 to 0.11 13.0
DDepression 0.48 0.43 0.06 0.02 to 0.10 12.2DAnxiety 0.48 0.47 0.01 �0.004 to 0.04 2.5DStress 0.48 0.43 0.05 0.01 to 0.10 11.4
a Investigating the mediation path Dpain—Dpsychological distress—Ddisability.t1, baseline; t2, directly after 6 weeks of treatment; t3, 12 weeks after treatment. Alleffects are reported as standardized b. Total effect indicates relationship betweenpain and disability, without adjustment; direct effect, effect of pain on disability,adjusted for mediator; indirect effect, effect of pain on disability via mediator.Support for mediation: if indirect effect (a * b) is significant, then support signifi-cant partial mediation.
A.M. Hall et al. / PAIN�
152 (2011) 1044–1051 1049
3.3. Change score analysis
Results of the analyses using the overall change scores (be-tween t1 and t3) showed a similar pattern to the second longitudi-nal analysis. The Total effect of pain on disability was significant(b = 0.53, P < 0.01), as were both portions of the indirect path; painwas significantly associated with psychological distress (b = 0.20,P < 0.01), and psychological distress was significantly associatedwith disability after controlling for pain at baseline (b = 0.24,P < 0.01). The confidence interval around the indirect effect con-firmed that the indirect path was significant (b = 0.05, 95% confi-dence interval 0.01–0.08) and accounted for 9% of the total effect.This result supports the hypothesis that the pain-disability rela-tionship is partially mediated by a change in psychological distress.Change scores for each of the variables of depression, anxiety, andstress were entered in turn as the potential mediating variable.Depression and stress showed a significant indirect effect account-ing for 6% and 9% of the total effect, respectively; anxiety had anonsignificant indirect effect.
A subsequent analysis of the initial change scores (between t1and t3) was performed, and the results were not different to thosefrom the overall change scores analysis (Table 5).
4. Discussion
Previous research reports psychological distress to be an obsta-cle to recovery for LBP patients and was recently proposed as amechanism to explain how pain leads to subsequent disability[16]. The longitudinal mediation analyses performed on 231 pa-tients with subacute LBP in this study provide some support forthe Pincus theoretical model. Our data suggest that psychologicaldistress explains approximately 30% of the relationship betweeninitial pain and later disability, implying that a person’s disabilitylevel is influenced by the degree to which their psychological statehas been affected by their pain experience. Our analyses supportpartial and not total mediation, which indicates that psychologicaldistress explains only a portion of how pain affects disability, andother factors should be explored.
Although the meditation model proposed by Baron and Kenny[1] may seem a succinct method to explore mechanism, interpreta-tion of the results in terms of causal inferences is more difficult.This requires careful consideration of timing of both outcome mea-surement and presentation of symptoms. For instance, if pain haselicited symptoms of psychological distress before the initial mea-surement, we no longer capture the entire process, and the modelmay underestimate the mediating effect. One way to gather moreconclusive information regarding the causal pathways would beto gather data at regular and closer time intervals from the onset
of pain. Another problem in interpretation of causality can occureven if we were able to obtain initial measures of the variablesat the onset of pain—for example, if measures of psychological dis-tress and pain were obtained within 24 h of the onset of pain. Inthis case, it would still be unclear whether these symptoms of dis-tress were present before the onset of pain or whether they wereindeed caused by the pain. It is plausible that symptoms of distresscould be present in a proportion of patients with back pain as acoexisting health problem; thus the model would potentially over-estimate the mediating effect. In this case, gathering informationon medical history would be advantageous to help exclude preex-isting conditions of distress. In the current study, the sample in-cluded patients with subacute pain, meaning the initialassessment was performed a minimum of 6 weeks after the onsetof pain. Symptoms of psychological distress have been reported tooccur in first few weeks after the onset of pain [5]. Therefore, ourinterpretation of the longitudinal mediation models based on thissample is limited by the timing of the measurements of distressand may provide an imprecise estimate of the mediating effect.By using the change scores, we gain another perspective intohow the changes in pain and distress exert influence on changein disability. In our study, this analysis reported a similar patternto the original longitudinal analyses, with change in psychologicaldistress partially mediating the relationship between pain anddisability.
Our exploratory investigation of how specific components ofpsychological distress impact long-term disability consistentlyshowed that depression and stress individually were both partialmediators in the pain-disability relationship. Therefore, pain mea-sured at 6 weeks after the onset of pain indirectly affects futuredisability by influencing symptoms of depression and symptomsof stress, but not symptoms of anxiety. Although it is generally ac-cepted that each of these components may share a similar elementof affective distress [11], each can be distinguished by certain un-ique features, and arguably, these defining features may help toshed more light the management and/or prevention of long-termdisability. For example, depression is characterised by low positiveaffect, loss of self-esteem, and a decreased incentive, potentiallydecreasing motivation for activity, thus affecting productivity anddisability [11]. These symptoms would differ from those of stressthat are characterized by a persistent tension, irritability, and a

1050 A.M. Hall et al. / PAIN�
152 (2011) 1044–1051
low threshold for becoming upset [11]. Therefore, deeper under-standing of the components of psychological distress and how theyinfluence disability can help guide appropriate patient-centredtreatment. In this case, on the basis of the symptoms associatedwith depression and stress, interventions to improve social partic-ipation, self-esteem, and energy levels, and to encourage treat-ments geared to learning relaxation strategies may be helpful.Future research to investigate how depression and stress and affectdisability is required for appropriate treatment planning.
Anxiety, on the other hand, differs from depression and stress,with symptoms characterized by autonomic arousal and fearful-ness [11]. Although anxiety has been hypothesized to predict dis-ability and poor prognosis [10], in our analyses, anxiety did nothave a significant mediating effect. This may be in part to the sub-acute nature of the study sample; with subjects already having hadpain for at least 6 weeks, it is possible that anxiety plays a role inthe very early/acute stages of pain-disability relationship, but notto the same extent in cases of longer duration.
Interventions that use a cognitive-behavioural approach havebeen recommended as a part of second-line care for patientswhose symptoms persist at least 6 months beyond onset [9]. Thisrecommendation is based on the theory that psychological, as op-posed to purely physical, factors play an increasing role in themaintenance of symptoms as time progresses. This study providessupport for this general theory in showing that psychological dis-tress is a mediating variable in the pain-disability relationship.However, the data also indicate that the various elements contrib-uting to psychological distress may differ (particularly in their timeof onset) with respect to how they influence this relationship.Although a recent systematic review [6] has shown some benefitof cognitive-behavioural strategies for patients with chronic LBPcompared to usual care, the effects are small, and there is littleor no benefit when compared to exercise therapy and inpatientrehabilitation. This finding highlights the need for future researchdesigned specifically to partition all the steps and or mechanismsby which psychological distress actually affects disability. In thisway, interventions may be designed to specifically target theappropriate elements, which should increase the chance of positiveoutcome.
Our findings suggest that symptoms of depression and stressare present as early as 6 weeks after the onset of pain and play arole in developing chronicity by 12 weeks. This would align withrecommendations to use cognitive-behavioural strategies as a pre-ventative method for those who have been identified as likely todevelop chronic symptoms [3], rather than solely as a treatmentfor patients with chronic symptoms. Currently, the bulk of cogni-tive-behavioural interventions for acute and subacute LBP popula-tions have been aimed at reductions in fear avoidance using gradedexposure techniques. Considering that our results indicate thatsymptoms of depression and stress are present as early as 6 weeksafter onset of LBP and are likely to contribute to the developmentof persistent symptoms of disability, we recommend that futureresearch focus on the early identification of these symptoms aswell as other prognostic factors associated with chronic disability(such as high pain intensity and work absence [5]) and test theeffectiveness of cognitive-behavioural treatment plans for thosewho are found to be at risk on these symptoms.
Currently, there are many approaches for implementing cogni-tive-behavioural strategies, ranging and from intensive cognitive-behavioural therapy delivered by mental health specialists seenin second-line care to less sophisticated interventions that can beadopted by other health professionals, including cognitive-behav-ioural-trained general practitioners, physiotherapists, occupationaltherapists, chiropractors, and exercise therapists. Although thebest method remains unclear, the latter method, which uses sim-ple, low-cost interventions, has been recently suggested as cost-
effective option for delivery in primary care to address a wider tar-get population early with the aim of preventing chronic disability[18]. We would further recommend that research regarding thetime of delivery and the effectiveness of well-designed, simple cog-nitive-behavioural interventions be undertaken to provide appro-priate evidence-based recommendations.
In conclusion, prevention of chronic disability associated withLBP is a necessity for improving overall well-being, productivity,and health care costs for individuals and for society. Although afew prognostic studies have attempted to describe the course ofLBP, none have formally investigated the underlying mechanismsof how acute LBP results in chronic disability. On the basis of thefindings of prognostic research, it has been proposed that presenceof pain can induce psychological distress, which can influence thedevelopment of disability. Our study evaluated this hypothesis inpatients with subacute LBP and found that psychological distresswas a partial mediator in the relationship between initial painand future disability. Further exploration into the components ofpsychological distress revealed that the symptoms of depressionand stress, but not anxiety, in part determine how pain influenceschronic disability. These findings provide an opportunity to de-crease the risk of chronicity by further exploring the effects ofhow and when these elements actually influence disability, whichcan determine appropriate screening times and implementation ofinterventions.
Conflict of interest statement
There are no known conflicts of interest associated with thisstudy.
Acknowledgments
AMH is funded by an Endeavour International Postgraduate Re-search Scholarship from the Australian government. SJK is fundedby the National Health and Medical Research Council of Australia.CGM is funded by the National Health and Medical Research Coun-cil of Australia. JL is funded by the Australian Research Council.
References
[1] Baron RM, Kenny DA. The moderator mediator variable distinction in socialpsychological-research, conceptual, strategic and statistical considerations. JPers Soc Psychol 1986;51:1173–82.
[2] Deyo RA. Low-back pain. Sci Am 1998;279:48–53.[3] Frank JW, Brooker AS, Demaio SE. Disability resulting from occupational low
back pain. Part II. What do we know about secondary prevention? A review ofthe scientific evidence on prevention after disability begins. Spine1996;21:2918–29.
[4] Grotle M, Brox JI, Veierod M, Glomsrad B, Lonn J, Vollestad NK. Clinical courseand prognostic factors in acute low back pain. Spine 2005;30:976–82.
[5] Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J,York J, Das A, McAuley JH. Prognosis in patients with recent onset low backpain in Australian primary care: inception cohort study. Br Med J 2008:337.
[6] Henschke N, Ostelo RWJG, van Tukder MW, Vlaeyen JWS, Morley S, AssendelftWJJ, Main CJ. Behavioural treatment for chronic low-back pain [review].Cochrane Database Sys Rev 2010:CD002014.
[7] Kendall NAS. Psychosocial approaches to the prevention of chronic pain: thelow back paradigm. Best Pract Res Clin Rheumatol 1999;13:545–54.
[8] Koes B, van Tulder M, Lin C, Macedo L, McAuley JH, Maher C. An updatedoverview of clinical guidelines for the management of nonspecific low backpain in primary care. Eur Spine J 2010;19:2075–94.
[9] Koes BW, van Tulder MW, Thomas S. Diagnosis and treatment of low back pain.Br Med J 2006;332:1430–4.
[10] Lethem J, Slade PD, Troup JDG, Bentley G. Outline of a fear-avoidance model ofexaggerated pain perception. Behav Res Ther 1983;21:401–8.
[11] Lovibond SH, Lovibond PF. Manual for the Depression Anxiety StressScales. Syndey: Psychology Foundation; 1995.
[12] Morris R. A study of the natural-history of back pain. 1. Development of areliable and sensitive measure of disability in low-back pain. Spine1983;8:141–4.
[13] Ostelo R, de Vet HCW. Clinically important outcomes in low back pain. BestPract Res Clin Rheumatol 2005;19:593–607.

A.M. Hall et al. / PAIN�
152 (2011) 1044–1051 1051
[14] Pengel LHM, Herbert RD, Maher CG, Refshauge KM. Acute low back pain:systematic review of its prognosis. Br Med J 2003;327:323–5.
[15] Pengel LHM, Refshauge KM, Maher CG, Nicholas MK, Herbert RD, McNair P.Physiotherapist-directed exercise, advice, or both for subacute low back pain—a randomized trial. Ann Intern Med 2007;146:787–96.
[16] Pincus T, Vogel S, Burton AK, Santos R, Field AP. Fear avoidance and prognosisin back pain—a systematic review and synthesis of current evidence. ArthritisRheum 2006;54:3999–4010.
[17] Shaw WS, Pransky G, Winters T. The Back Disability Risk Questionnaire forwork-related, acute back pain: prediction of unresolved problems at 3-monthfollow-up. J Occup Environ Med 2009;51:185–94.
[18] van der Windt D, Hay E, Jellema P, Main C. Psychosocial interventions for lowback pain in primary care—lessons learned from recent trials. Spine2008;33:81–9.
[19] Walker B. The prevalence of low back pain: a systematic review of theliterature from 1966 to 1998. J Spinal Disord 2000;13:205–17.
[20] Williams CM, Maher CG, Hancock MJ, McAuley JH, McLachlan AJ, BrittH, Fahridin S, Harrison C, Latimer J. Low back pain and best practicecare. A survey of general practice physicians. Arch Intern Med2010;170:271–7.