Depressive symptoms and bodily pain: the role of physical disability and social stress
17
Depressive symptoms and bodily pain: The role of physical disability and social stress Mathew D. Gayman 1 , Robyn Lewis Brown 2 , and Ming Cui 3 1 Department of Sociology, Georgia State University, GA, USA 2 Department of Sociology, DePaul University, IL, USA 3 Department of Family & Child Sciences, Florida State University, FL, USA Summary This study evaluates the bi-directional association between depressive symptoms and bodily pain, and examines the role of physical disability and perceived social stress in the depression—pain relationship. Data are employed from a two-wave panel study of Miami-Dade county residents (n = 1,459) that includes a substantial over-sampling of individuals who identify as physically- disabled. Findings indicate that the bi-directional relationship between depression and pain is similar for those with and without a physical disability. Results also demonstrate that stress exposure, specifically recent life events and daily discrimination, partially mediated the relationship between prior levels of depression and changes in pain. Directions for future research and the need for a more comprehensive model of health incorporating physical, psychological, and social factors are discussed. Keywords depression; bodily pain; social stress; physical disability Introduction The co-occurrence of depression and bodily pain is a major public health issue in the United States constituting substantial economic, social and personal costs (Gatchel, 2004). Although the association between depression and pain is consistently observed in the health literature (Baune et al., 2008; Benjamin et al., 2000; Gamsa, 1990; Gayman, Turner, & Cui, 2008; Harma et al., 2002; Lindsay & Wyckoff, 1981; Magni, Rigatti-Luchini, & Merskey, 1990; Magni et al., 1993; Mathew, Weinman, & Mirabi, 1981), the nature of this relationship is still not well understood. Indeed, further investigation into the depression— pain relationship remains of both theoretical and practical significance (Bair et al., 2003; Romano & Turner, 1985). The current investigation aims to further our understanding of the relationship between depression and pain by addressing three study objectives: First, evaluate the bi-directional relationship by modeling both pathways simultaneously using path analysis, as well as control for disability status in order to rule out the interpretation of spuriousness. Second, test whether the bi-directional relationship between depression and pain is moderated by Address correspondence to Mathew D. Gayman, Department of Sociology, Georgia State University, General Classroom Building, 38 Peachtree Center Ave., Room 1041, Atlanta, GA 30303, USA, [email protected]. NIH Public Access Author Manuscript Stress Health. Author manuscript; available in PMC 2012 February 1. Published in final edited form as: Stress Health. 2011 February ; 27(1): 52–53. doi:10.1002/smi.1319. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Depressive symptoms and bodily pain: the role of physical disability and social stress

Depressive symptoms and bodily pain: The role of physicaldisability and social stress
Mathew D. Gayman1, Robyn Lewis Brown2, and Ming Cui31 Department of Sociology, Georgia State University, GA, USA2 Department of Sociology, DePaul University, IL, USA3 Department of Family & Child Sciences, Florida State University, FL, USA
SummaryThis study evaluates the bi-directional association between depressive symptoms and bodily pain,and examines the role of physical disability and perceived social stress in the depression—painrelationship. Data are employed from a two-wave panel study of Miami-Dade county residents (n= 1,459) that includes a substantial over-sampling of individuals who identify as physically-disabled. Findings indicate that the bi-directional relationship between depression and pain issimilar for those with and without a physical disability. Results also demonstrate that stressexposure, specifically recent life events and daily discrimination, partially mediated therelationship between prior levels of depression and changes in pain. Directions for future researchand the need for a more comprehensive model of health incorporating physical, psychological, andsocial factors are discussed.
Keywordsdepression; bodily pain; social stress; physical disability
IntroductionThe co-occurrence of depression and bodily pain is a major public health issue in the UnitedStates constituting substantial economic, social and personal costs (Gatchel, 2004).Although the association between depression and pain is consistently observed in the healthliterature (Baune et al., 2008; Benjamin et al., 2000; Gamsa, 1990; Gayman, Turner, & Cui,2008; Harma et al., 2002; Lindsay & Wyckoff, 1981; Magni, Rigatti-Luchini, & Merskey,1990; Magni et al., 1993; Mathew, Weinman, & Mirabi, 1981), the nature of thisrelationship is still not well understood. Indeed, further investigation into the depression—pain relationship remains of both theoretical and practical significance (Bair et al., 2003;Romano & Turner, 1985).
The current investigation aims to further our understanding of the relationship betweendepression and pain by addressing three study objectives: First, evaluate the bi-directionalrelationship by modeling both pathways simultaneously using path analysis, as well ascontrol for disability status in order to rule out the interpretation of spuriousness. Second,test whether the bi-directional relationship between depression and pain is moderated by
Address correspondence to Mathew D. Gayman, Department of Sociology, Georgia State University, General Classroom Building, 38Peachtree Center Ave., Room 1041, Atlanta, GA 30303, USA, [email protected].
NIH Public AccessAuthor ManuscriptStress Health. Author manuscript; available in PMC 2012 February 1.
Published in final edited form as:Stress Health. 2011 February ; 27(1): 52–53. doi:10.1002/smi.1319.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

psychical disability status. Third, evaluate the mediating effects of social stress in thedepression—pain relationship.
Bi-directional relationship between depression and painRecent studies employing longitudinal designs have considered the temporal order of theassociation between depression and pain. While findings indicate that pain predictsdepression over time (Bair et al., 2004; Breslau & Davis, 1992; Brown, 1990; Corruble &Guelfi, 2000; Gallagher & Verna, 1999; Von Korff et al., 1993)and that pain appears to be astronger predictor of depression than vice versa (Cairns, Adkins, & Scott, 1996; Fishbain etal., 1997), evidence also demonstrates that depression is associated with an increase in pain(Leino and Magni, 1993; Ruoff, 1996; Von Korff et al., 1991). Breslau and colleagues(1994) found that prior pain predicted an increase in risk for major depression and thatdepression predicted an increase in bodily pain. Consequently, researchers have concludedthat the relationship between depression and pain is bi-directional (Bair et al., 2003; Leino &Magni, 1993; Von Korff & Simon, 1996). However, because a true test of a bi-directionalassociation necessitates that both pathways are modeled simultaneously researchers cannotanswer with confidence whether the depression—pain relationship is indeed bi-directional.
Moderation of physical disabilityThere are also grounds to anticipate that the relationship between depression and pain maybe moderated (or conditioned) by disability status: whereby the relationship variessignificantly for those with and without a physical disability. Prior research demonstratesthat persons with physical disabilities are more prone to experiencing co-occurring pain anddepression (Dickens et al., 2000; Gatchel & Dersh, 2002; Polatin et al., 1993). Persons witha disability who experience considerable bodily pain may have greater difficulty in meetingthe requirements of social roles and, consequently, increase risk for depressive mood.Similarly, persons with disabilities who experience higher levels of depressive symptomsmay experience greater obstacles in the ability and motivation to engage in physical andsocial activities conducive to physical well-being, thus increasing risk for bodily pain.However, due to the paucity of research specifically testing for a bi-directional associationbetween depression and pain, the potential significance of disability for understanding theshared linkage between these health indicators has also received little attention.
Mediation of social stressThe hypothesis that pain may increase risk for depression and depression may increase riskfor pain, vis-à-vis associated difficulties in overcoming life’s hardships, is consistent withresearch in the stress process tradition. Stress process theory posits that social experiencesare translated into health outcomes through exposure to social stress and one’s ability toeffectively cope with stress (Pearlin et al., 1981, Pearlin, 1989). Because depression isassociated with increased stress exposure (Hammen 1991, 2006) and psychological stress isrelated to physical pain (Diepenmaat et al., 2006; Hwang et al., 2008; Ullrich et al., 2005),social stress may mediate the relationship between prior depression and changes in pain.Conversely, to the extent that bodily pain increases risk for failure to meet the requirementsof social roles, pain may increase risk for role-related chronic stressors and, in turn, increasedepressive mood.
The potential mediating effects of social stress in the depression—pain relationship is alsosupported by research examining shared physiological attributes between depression andpain (Bair et al., 2003) and shared biological pathways that respond similarly to clinicaltreatment (Blier & Abbott, 2001; Gallagher & Verna, 1999). Evidence from research onallostatic load (Geronimus et al., 2006; McEwen & Seeman, 1999; Seeman et al., 1997) and
Gayman et al. Page 2
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

psychoneuroimmunology (Benham, Nash, & Baldwin, 2009; Glaser, 2005; Fan et al., 2009)have specified a range of biomarkers that are affected by social stress and that mediate thelinkage between stress exposure and health. Schell and colleagues (2008) recentlydemonstrated an association between stress biomarkers and bodily pain. In the case ofdepression, stress has been shown to influence neuroendocrine responses that are correlatesor expressions of depressive symptoms (Nierop et al., 2006; Robles, Glaser, & Kiecolt-Glaser 2005). Because symptoms of depression and pain may follow the same pathways inthe central nervous system(Bair et al., 2003), it seems likely that stress plays an importantrole in shaping the influence of depression on pain and vice versa.
MethodStudy Procedures and Sample
The data employed in this study were from a two-wave (W1 and W2) panel study of MiamiDade County residents that included a substantial oversampling of individuals with aphysical disability. This study was approved by the Institutional Review Board (IRB) at theUniversity of Miami and has been described in detail elsewhere (Gayman et al., 2008;Turner, Lloyd, & Taylor, 2006). Described in the sampling framework illustrated below, atotal of 10,000 randomly selected households were screened with respect to gender, age,ethnicity, disability status, and language preference. Using this sampling frame, the studysample was drawn such that there were even numbers of women and men, even numbers ofpeople screened as having a physical disability and those not, and equivalent numbers of thefour major ethnic groups comprising more than 90% of all Miami-Dade County residents(non-Hispanic Whites, Cubans, non-Cuban Hispanics, and African Americans). Thepresence of disability status was established in responses to the question: “Do any adults inthe household have a physical health condition or physical handicap that has resulted in achange in their daily routine or that limits the kind of or amount of activity they can carryout?”
From 2000–2001, 1,986 interviews were completed, with a success rate of 82 percent.Included in the study were 1,086 adults who screened as having no physical disability and900 individuals who screened as having a disability. Of the 900 reported by a familymember as having activity limitations within the screening process, only 559 confirmed thisstatus within the actual interview. Presumably, this discrepancy arises from differing viewsabout the level of activity limitation that defines disability.
Second-wave interviews of 1,495 W1 participants were completed approximately threeyears later (2003–2004). Excluding 100 W1 participants who had died and 59 who were tooill to be interviewed, the second-wave success rate was 82.5 percent. Those lost to attritionat W2 reported lower levels of social stress, socioeconomic status, and pain, and slightlyhigher levels of both physical limitations and depressive symptoms at W1. The magnitude ofthese differences varied from 0.10 SD to slightly more than 0.30 SD. In our view, the natureand magnitude of these differences do not seriously challenge the representativeness of thesubpopulation employed in these analyses or in any way suggest that selection biases mayhave accounted for the results presented.
A total of 1,459 study participants provided valid data across all study variables employed inthe current analysis. The working sample included 786 females (54%), 345 non-HispanicWhites (24%), 351 Cuban-Americans (24%), 320 non-Cuban Hispanics (22%), and 443African Americans (30%). The sample distribution by physical disability status was 410disabled (28%) and 1,049 non-disabled (72%). The average age of respondents at Wave 1was 57 years (S.D. = 17 years; range = 18–93 years).
Gayman et al. Page 3
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

MeasuresDepressive symptoms—Depressive symptomatology was assessed at W1 and W2 usingthe highly reliable and widely used Center for Epidemiologic Studies Depression Scale(CES-D) (Radloff, 1977). From the original 20-item CES-D index, six items related tosomatic problems were omitted from analyses to avoid measurement confounding betweendepression and physical health (Ormel et al., 2002). These omitted items include problemswith eating, keeping your mind on what you are doing, effort, restlessness, talking, andgetting going. In completing the CES-D items, participants were asked about theirexperiences over the past month using response categories of “not at all” (1) to “almost allthe time” (4) (range = 0–56). Items were coded such that higher scores indicated higherlevels of depressive symptoms and summed for analysis (Wave 1 α = .81; Wave 2 α = .84).
Bodily pain—Indicators of physical pain were assessed by asking respondents at W1 andW2 whether they had experienced any bodily pain over the preceding four weeks. Thosewho answered affirmatively were questioned on the frequency and average intensity of painexperienced. Response categories for the intensity item ranged from “very mild” (1) to “verysevere” (5). Those for frequency ranged from “once or twice” (1) to “everyday or almosteveryday” (5). Respondents who reported no pain over the past four weeks were coded as“none” (0) for intensity of pain and “never” (0) for frequency of pain. Both items werecoded so that higher values indicate greater intensity and frequency of pain. While themeasurement of pain varies widely across studies, the severity of pain has importantimplications for depression (Bair et al., 2003). As used in prior research (Gayman et al.,2008), we derive the pain measure by multiplying scores on the two dimensions as anindicator of pain severity (range = 0–25).
Social stress—Measured at W1 and W2, stress exposure was measured using threeseparate indicators of perceived social stress: chronic stress, daily discrimination and recentlife events. The chronic stress measure is an adaptation of Wheaton’s (1994) scale, modifiedto better capture the kinds of enduring stressors older individuals are likely to experience.This index includes 39 items (0–1 scale; range = 0–39) relating to general experiences,employment/unemployment, intimate partnerships/no partners, children, recreation, andhealth concerns. Daily discrimination (9 items; 1–5 point scale; range = 9–45) and lifeevents within the past 12-moths (32 items; 0–1 scale; range = 0–32) were indexed bypreviously employed measures (Turner & Avison, 2003; Williams et al., 1997). Indicators ofdaily discrimination include statements such as “You are treated with less courtesy thanother people,” “People act as if they think you are dishonest,” and “You are called names orinsulted.” Recent life events involve undesirable experiences that occur to the respondent orthose close to them and include, for example: being in a serious accident, death of spouse/partner, death of child, and major financial crisis. A detailed list of all stress items includedin this study was previously published by Turner and Avison (2003).
Physical disability status—At Wave 1 interviewers asked the following question ofrespondents who were classified as having a disability in the screening process: “Earliersomeone in your household [or the respondent] told us that you had a condition or physicalhealth problem that limits the kind or amount of activity that you can carry out (such aswork, housework, school, recreation, shopping, or participation in social or communityactivities). I just want to confirm with you now whether that is correct.” Respondents whoresponded affirmatively were coded as 1 for disability; those who did not were coded as 0.
Controls—The control variables were assessed at Wave 1 and included gender, age, race-ethnicity, and socioeconomic status (SES). Gender is coded 1 for females and 0 for males.Age was measured in years as a continuous variable. Race-ethnicity is measured using a set
Gayman et al. Page 4
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
of dummy variables for non-Hispanic Whites (reference group), African Americans,Cubans, and non-Cuban Hispanics. Estimates of SES were based on a composite score thatequally weights occupational level (Hollingshead, 1957), educational attainment, andhousehold income of each participant. To avoid problems of missing data, particularly onthe variable of household income, scores on each of these dimensions were standardized,summed and divided by the number of dimensions on which data were available.
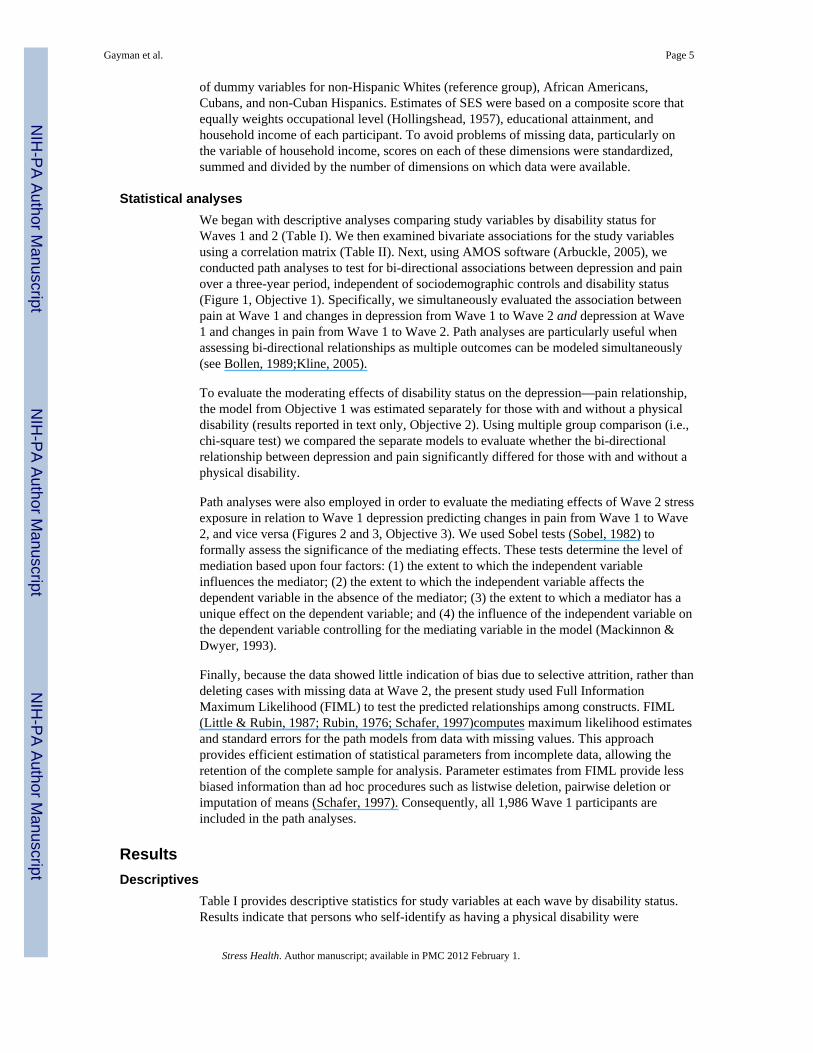
Statistical analysesWe began with descriptive analyses comparing study variables by disability status forWaves 1 and 2 (Table I). We then examined bivariate associations for the study variablesusing a correlation matrix (Table II). Next, using AMOS software (Arbuckle, 2005), weconducted path analyses to test for bi-directional associations between depression and painover a three-year period, independent of sociodemographic controls and disability status(Figure 1, Objective 1). Specifically, we simultaneously evaluated the association betweenpain at Wave 1 and changes in depression from Wave 1 to Wave 2 and depression at Wave1 and changes in pain from Wave 1 to Wave 2. Path analyses are particularly useful whenassessing bi-directional relationships as multiple outcomes can be modeled simultaneously(see Bollen, 1989;Kline, 2005).
To evaluate the moderating effects of disability status on the depression—pain relationship,the model from Objective 1 was estimated separately for those with and without a physicaldisability (results reported in text only, Objective 2). Using multiple group comparison (i.e.,chi-square test) we compared the separate models to evaluate whether the bi-directionalrelationship between depression and pain significantly differed for those with and without aphysical disability.
Path analyses were also employed in order to evaluate the mediating effects of Wave 2 stressexposure in relation to Wave 1 depression predicting changes in pain from Wave 1 to Wave2, and vice versa (Figures 2 and 3, Objective 3). We used Sobel tests (Sobel, 1982) toformally assess the significance of the mediating effects. These tests determine the level ofmediation based upon four factors: (1) the extent to which the independent variableinfluences the mediator; (2) the extent to which the independent variable affects thedependent variable in the absence of the mediator; (3) the extent to which a mediator has aunique effect on the dependent variable; and (4) the influence of the independent variable onthe dependent variable controlling for the mediating variable in the model (Mackinnon &Dwyer, 1993).
Finally, because the data showed little indication of bias due to selective attrition, rather thandeleting cases with missing data at Wave 2, the present study used Full InformationMaximum Likelihood (FIML) to test the predicted relationships among constructs. FIML(Little & Rubin, 1987; Rubin, 1976; Schafer, 1997)computes maximum likelihood estimatesand standard errors for the path models from data with missing values. This approachprovides efficient estimation of statistical parameters from incomplete data, allowing theretention of the complete sample for analysis. Parameter estimates from FIML provide lessbiased information than ad hoc procedures such as listwise deletion, pairwise deletion orimputation of means (Schafer, 1997). Consequently, all 1,986 Wave 1 participants areincluded in the path analyses.
ResultsDescriptives
Table I provides descriptive statistics for study variables at each wave by disability status.Results indicate that persons who self-identify as having a physical disability were
Gayman et al. Page 5
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

disadvantaged in terms of pain, depression and stress exposure at both Wave 1 and 2. Forexample, persons with a physical disability reported significantly greater bodily pain atWave 1 (M=8.63) and Wave 2 (M=2.71) than their non-physically limited counterparts(M=5.24 and M=1.90, respectively).
Table II provides correlations among study variables; indicating significant bivariateassociations between study variables at both Wave 1 and 2. Of interest, Wave 1 pain wasassociated with Wave 2 depressive symptoms, and vice versa. The results also showedsignificant stability in both pain (r = .42, p < .001) and depressive symptoms (r = .35, p < .001) over a three-year period. In addition, measures of social stress were associated withboth pain and depressive symptoms. Together, the correlations provided initial support forthe bi-directional and mediation hypotheses.
Bi-directional relationship between depression and painFigure 1 provides results from path analysis examining the hypothesized bidirectionalassociation between depressive symptoms and bodily pain. We included age, gender, race/ethnicity, SES, and disability status as control variables but do not show them in order tomore clearly convey the primary findings. Several findings are noteworthy. First, controllingfor demographics and disability status, the stability coefficients for depression and painremained statistically significant for depressive symptoms (b = .27, p < .01) and pain (b = .33, p < .01). Second, independent of disability status, the level of depressive symptoms atWave 1 predicts changes in bodily pain from Wave 1 to Wave 2 (b = .05, p < .05), and viceversa (b = .04, p < .05).
Moderation of psychical disabilityIn order to evaluate whether the bi-directional association between depression and pain ismoderated by disability status, multiple group comparisons were conducted (not shown).Specifically, the sample was divided by physical status to create two subsamples: oneincluded those with a physical disability (N = 559) and the other included those without aphysical disability (N = 1,427). First the model in Figure 1 was evaluated for both groupssimultaneously with corresponding paths in the model for the two groups freely estimated.Second, corresponding pairs of paths were constrained to be equal and chi-square changesbetween models were evaluated to test the difference. The findings indicate that thebidirectional relationship between depression and pain statistically equivalent—in bothdirection and strength—for those with and without a physical disability. In other words, therelationship between depression and pain is both bi-directional and equally robust for thosewith and without a physical disability.
Mediation of social stressWe next tested the mediating hypotheses. We proposed that the association between priordepression and changes in pain, and vice versa, would be attenuated by Wave 2 social stress(Figures 2 and 3). Again, we included age, gender, race/ethnicity, SES, and disability statusas control variables (not shown).
Figure 2 shows that Wave 1 depression predicted each measure of Wave 2 stress and thatWave 2 stress (recent life events, daily discrimination) was associated with Wave 2 pain.Compared to Figure 1, the direct path from Wave 1 depression to Wave 2 pain was reducedfrom .05 to .03. With respect to mediating effects, Sobel tests revealed that both recent lifeevents (z=2.792, p=.005) and daily discrimination (z=1.939; p=.052) significantly mediatedthe relationship between prior depression and changes in bodily pain. Chronic stress,however, was not found to be a significant mediator between prior depression and changesin bodily pain
Gayman et al. Page 6
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Conversely, Figure 3 evaluated the mediating effects of social stress for the influence ofprior pain for changes in depressive symptoms. With demographic controls and all Wave 2stress measures modeled simultaneously, Wave 1 pain was not associated with Wave 2stressors and stress was not associated with Wave 2 depressive symptoms. In addition torevealing no changes in the relationship between prior pain and changes in depression, theresults failed to meet the requirements of mediation effects. We therefore conclude that theeffects of pain on changes in depressive symptoms were not mediated by the stress indictorsin this study.
DiscussionThe present study addressed three research questions. Is the relationship between depressivesymptoms and bodily pain bi-directional, independent of sociodemographic characteristicsand physical disability status? Is the bi-directional association between depression and painmoderated by disability status? And, does perceived social stress mediate the depression—pain relationship?
Regarding the first research question, the current investigation builds on previous studies(Breslau et al., 1994) by simultaneously modeling the pathway from depression to pain andfrom pain to depression. The results support the conclusion that the relationship betweendepression and pain is bi-directional. In addition, although prior research has shown that thedepression—pain relationship is partially explained by disability status (Dickens et al.,2000), the current investigation demonstrates that the bi-directional relationship betweendepression and pain is independent of physical disability status.
It should be noted that, although the reported effect sizes for the cross-lagged associationsfor depression and pain were modest, small bi-directional effects are common in this kind ofmodel given the high stability coefficients between adjacent waves of data (Cui, Donnellaan,& Conger, 2007). Moreover, small effects are not necessarily indicative of trivialassociations, especially when such relationships reflect an ongoing process that is related tothe health and well-being of individuals (see Rosenthal and Rubin 1979 for a discussion ofthe importance of small effects). Simply put, the observed bi-directional relationship mayhave a substantial and clinically significant impact on individual functioning over time. Inaddition, given that the data employed here were based on a community sample, the bi-directional and exacerbating effects of depression on pain (and vice versa) may be evenmore robust among clinical populations.
The bi-directionality between depression and pain identified here is in contrast with a recentreport employing the same sample but that assessed the relationship between depressivesymptoms and physical limitations. Specifically, Gayman and colleagues (2008)demonstrated that physical limitations predict changes in depressive symptoms, but foundno evidence of the reverse association over the three-year period. They concluded that thetranslation of depression to physical limitations is likely to occur over an extended period oftime.
In light of the current findings, we posit that the influence of depression on bodily pain, andvice versa, may reflect a more pervasive linkage between mental and physical health—alinkage that may arise partly from shared biological pathways, as previously noted (Blier &Abbott, 2001; Gallagher & Verna, 1999). Thus the time it takes for depression to translateinto perceptions of pain may be relatively short, at least compared to the time needed fordepression to manifest into physical limitations. In addition, depression may translate intophysical limitations through experiences of bodily pain. Though data limitations prevent usfrom testing these hypotheses, we recommend future research to consider the linkage
Gayman et al. Page 7
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
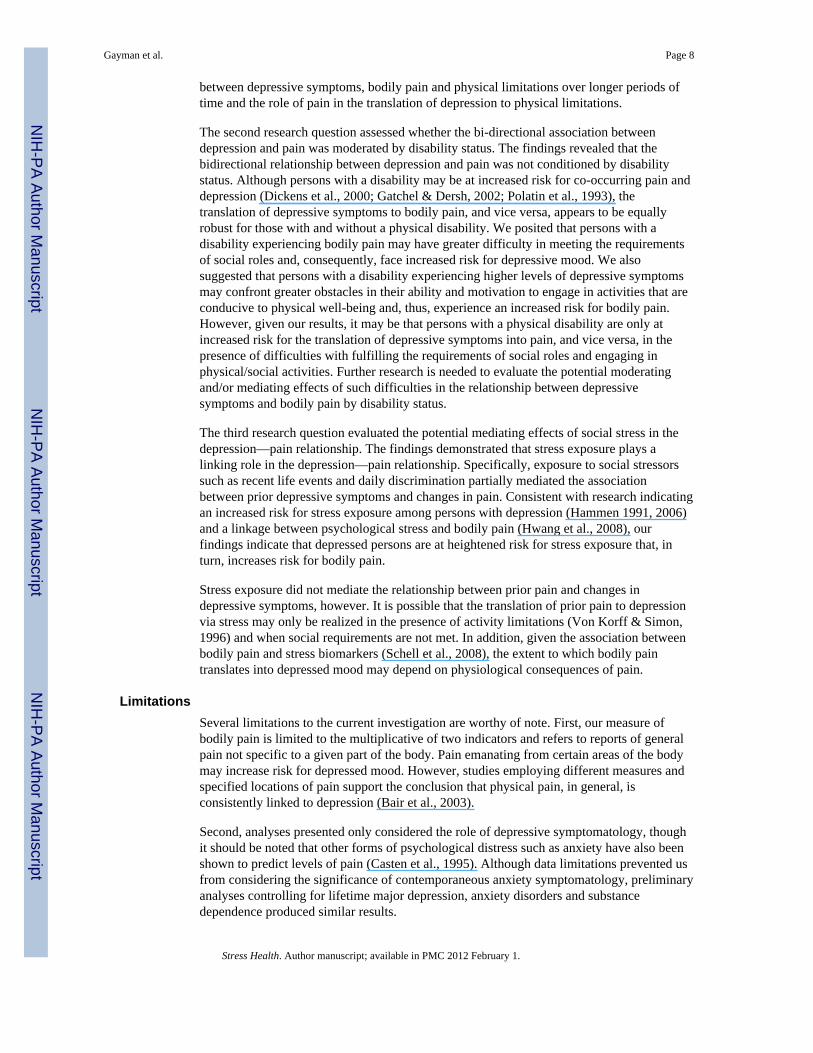
between depressive symptoms, bodily pain and physical limitations over longer periods oftime and the role of pain in the translation of depression to physical limitations.
The second research question assessed whether the bi-directional association betweendepression and pain was moderated by disability status. The findings revealed that thebidirectional relationship between depression and pain was not conditioned by disabilitystatus. Although persons with a disability may be at increased risk for co-occurring pain anddepression (Dickens et al., 2000; Gatchel & Dersh, 2002; Polatin et al., 1993), thetranslation of depressive symptoms to bodily pain, and vice versa, appears to be equallyrobust for those with and without a physical disability. We posited that persons with adisability experiencing bodily pain may have greater difficulty in meeting the requirementsof social roles and, consequently, face increased risk for depressive mood. We alsosuggested that persons with a disability experiencing higher levels of depressive symptomsmay confront greater obstacles in their ability and motivation to engage in activities that areconducive to physical well-being and, thus, experience an increased risk for bodily pain.However, given our results, it may be that persons with a physical disability are only atincreased risk for the translation of depressive symptoms into pain, and vice versa, in thepresence of difficulties with fulfilling the requirements of social roles and engaging inphysical/social activities. Further research is needed to evaluate the potential moderatingand/or mediating effects of such difficulties in the relationship between depressivesymptoms and bodily pain by disability status.
The third research question evaluated the potential mediating effects of social stress in thedepression—pain relationship. The findings demonstrated that stress exposure plays alinking role in the depression—pain relationship. Specifically, exposure to social stressorssuch as recent life events and daily discrimination partially mediated the associationbetween prior depressive symptoms and changes in pain. Consistent with research indicatingan increased risk for stress exposure among persons with depression (Hammen 1991, 2006)and a linkage between psychological stress and bodily pain (Hwang et al., 2008), ourfindings indicate that depressed persons are at heightened risk for stress exposure that, inturn, increases risk for bodily pain.
Stress exposure did not mediate the relationship between prior pain and changes indepressive symptoms, however. It is possible that the translation of prior pain to depressionvia stress may only be realized in the presence of activity limitations (Von Korff & Simon,1996) and when social requirements are not met. In addition, given the association betweenbodily pain and stress biomarkers (Schell et al., 2008), the extent to which bodily paintranslates into depressed mood may depend on physiological consequences of pain.
LimitationsSeveral limitations to the current investigation are worthy of note. First, our measure ofbodily pain is limited to the multiplicative of two indicators and refers to reports of generalpain not specific to a given part of the body. Pain emanating from certain areas of the bodymay increase risk for depressed mood. However, studies employing different measures andspecified locations of pain support the conclusion that physical pain, in general, isconsistently linked to depression (Bair et al., 2003).
Second, analyses presented only considered the role of depressive symptomatology, thoughit should be noted that other forms of psychological distress such as anxiety have also beenshown to predict levels of pain (Casten et al., 1995). Although data limitations prevented usfrom considering the significance of contemporaneous anxiety symptomatology, preliminaryanalyses controlling for lifetime major depression, anxiety disorders and substancedependence produced similar results.
Gayman et al. Page 8
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Third, the relationship between physical and mental health may also stem from statedependence bias—those who currently experience higher levels of depressive symptoms, forexample, report higher levels of social stress and bodily pain. Although we can not rule outthis alterative interpretation, the longitudinal nature of the study helps temper this concern.At a minimum, this builds upon prior cross-sectional studies on the relationship betweendepression and bodily pain.
ConclusionSuch limitations notwithstanding, the present study builds on prior research in severalimportant ways. First, it offers a prospective assessment to evaluate the bidirectionalrelationship between depressive symptoms and bodily pain by modeling both pathwayssimultaneously. Second, the oversampling of persons with a physical disability living in thecommunity provides a unique opportunity to evaluate whether the bidirectional relationshipbetween depression and pain is an artifact of disability status and/or whether the relationshipis moderated by disability status. In this vein, results from this study can be generalized tothe community from which the sample was drawn, as opposed to being limited to a clinicalpopulation characteristic of many prior studies. Third, few community-based studies accountfor such a wide array of stressors allowing for a more comprehensive understanding of themediating effects of social stress in the depression—pain relationship.
In sum, the findings leave little doubt that the relationship between depression and pain is,indeed, bi-directional and that this bi-directional linkage is not an artifact of having aphysical disability. In addition, the bi-directional relationship between depression and painwas similar for those with and without a physical disability, further highlighting thepervasive nature of the relationship. The findings also demonstrate that stress exposureamong those with a history of depression has important implications for experiencingpersistent and increasing levels of physical pain. Although the current investigation couldnot account for biological indicators of health, taken together, the findings support the callfor a more comprehensive model of health incorporating physical, psychological, and socialfactors.
AcknowledgmentsThe authors would like to thank Dr. Tim Carey for his critiques on an earlier draft of this manuscript. This workwas supported by grants R01DA13292 and R01DA16429 from The National Institute on Drug Abuse to R. JayTurner. This research was also supported by the National Research Service Award Postdoctoral Traineeship fromthe National Institute of Mental Health sponsored by Cecil G. Sheps Center for Health Services Research,University of North Carolina at Chapel Hill (Grant No: T32 MH019117).
ReferencesArbuckle, JL. Amos 6.0 user’s guide. Chicago, IL: SPSS, Inc; 2005.Bair MJ, Robinson RL, Eckert GJ, Stang PE, Croghan TW, Kroenke K. Impact of pain on depression
treatment response in primary care. Psychosomatic Medicine. 2004; 66:17–22. [PubMed:14747633]
Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: A literature review.Archives of Internal Medicine. 2003; 163:2433–2445. [PubMed: 14609780]
Baune BT, Caniato RN, Garcia-Alcaraz MA, Berger K. Combined effects of major depression, painand somatic disorders on general functioning in the general adult population. Pain. 2008; 138:310–317. [PubMed: 18258371]
Benham G, Nash MR, Baldwin DR. A comparison of changes in secretory immunoglobulin Afollowing a stress-inducing and stress-reducing task. Stress and Health. 2009; 25:81–90.
Gayman et al. Page 9
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Benjamin S, Morris S, McBeth J, MacFarlane GJ, Silman AJ. The association between chronicwidespread pain and mental disorder. Arthritis and Rheumatism. 2000; 43:561–567. [PubMed:10728749]
Blier P, Abbott FV. Putative mechanisms of action of antidepressant drugs in affective and anxietydisorders and pain. Journal of Psychiatry and Neuroscience. 2001; 26:37–43. [PubMed: 11212592]
Bollen, KA. Structural equations with latent variables. New York: Wiley; 1989.Breslau N, Davis G. Migraine, major depression and panic disorder: A prospective epidemiological
study of young adults. Cephalalgia. 1992; 12:85–90. [PubMed: 1576649]Breslau N, Davis GG, Schultz LR, Peterson EL. Migraine and major depression: a longitudinal study.
Headache. 1994; 12:387–393. [PubMed: 7928322]Brown GK. A causal analysis of chronic pain and depression. Journal of Abnormal Psychology. 1990;
99:127–137. [PubMed: 2348006]Cairns DM, Adkins RH, Scott MD. Pain and depression in acute traumatic spinal cord injury: Origins
of chronic problematic pain? Archives of Physical Medicine and Rehabilitation. 1996; 77:329–335. [PubMed: 8607754]
Casten RJ, Parmelee PA, Kleban MH, Lawton MP, Katz IR. The relationships among anxiety,depression, and pain in a geriatric institutionalized sample. Pain. 1995; 61:271–276. [PubMed:7659437]
Corruble E, Guelfi JD. Pain complaints in depressed inpatients. Psychopathology. 2000; 33:307–309.[PubMed: 11060514]
Cui M, Donnellan MB, Conger RD. Reciprocal influences between parents’ marital problems andadolescent internalizing and externalizing behavior. Developmental Psychology. 2007; 43:1544–1552. [PubMed: 18020831]
Dickens C, Jayson M, Sutton C, Creed F. The relationship between pain and depression in a trial usingparoxetine in sufferers of chronic low back pain. Psychosomatics. 2000; 41:490–499. [PubMed:11110112]
Diepenmaat AC, van der Wal MF, de Vet HC, Hirasing RA. Neck/shoulder, low back, and arm pain inrelation to computer use, physical activity, stress, and depression among Dutch adolescents.Pediatrics. 2006; 117(2):412–416. [PubMed: 16452360]
Fan Y, Tang Y, Lu Q, Feng S, Yu Q, Sui D, Zhao Q, Ma Y, Li S. Dynamic changes in salivary cortisoland secretory immunoglobulin A response to acute stress. Stress and Health. 2009; 25:189–194.
Fishbain DA, Cutler R, Rosomoff HL, Steele-Rosomoff R. Chronic pain associated depression:antecedent or consequence of chronic pain? A review. Clinical Journal of Pain. 1997; 13:116–137.[PubMed: 9186019]
Gallagher RM, Verna S. Managing pain and comorbid depression: a public health challenge. Seminarsin Clinical Neuropsychiatry. 1999; 4:203–220. [PubMed: 10498788]
Gamsa A. Is emotional disturbance a precipitator or a consequence of chronic pain? Pain. 1990;42:183–195. [PubMed: 2247316]
Gatchel RJ. Comorbidity of chronic pain and mental health disorders: The biopsychosocialperspective. American Psychologist. 2004; 59(8):795–805. [PubMed: 15554853]
Gatchel, RJ.; Dersh, J. Psychological disorders and chronic pain: Are there cause-and-effectrelationships?. In: Turk, DC.; Gatchel, RJ., editors. Psychological approaches to pain management.New York: Guilford Press; 2002. p. 30-51.
Gayman MD, Turner RJ, Cui M. Physical limitations and depressive symptoms: Exploring the natureof the association. Journal of Gerontology: Social Sciences. 2008; 63B:S219–S228.
Geronimus AT, Hicken M, Keene D, Bound J. ‘Weathering’ and age patterns of allostatic load scoresamong blacks and whites in the United States. American Journal of Public Health. 2006; 6:826–833. [PubMed: 16380565]
Glaser R. Stress-associated immune dysregulation and its importance for human health: a personalhistory of psychoneuroimmunology. Brain, Behavior, and Immunity. 2005; 19:3–11.
Hammen C. The generation of stress in the course of unipolar depression. Journal of AbnormalPsychology. 1991; 100:555–561. [PubMed: 1757669]
Gayman et al. Page 10
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Hammen C. Stress generation in depression: Reflections on origins, research, and future directions.Journal of Clinical Psychology. 2006; 62:1065–1082. [PubMed: 16810666]
Harma AM, Kaltiala-Heino R, Rimpela M, Rantanen P. Are adolescents with frequent pain symptomsmore depressed? Scandanavian Journal of Primary Health Care. 2002; 20:92–96.
Hollingshead, AB. Two factor index of social position. New Haven, CT: Author; 1957.Hwang G, Kim SK, Kim JH, Kim HR, Park SH, Kim SH. Influence of psychological stress on
physical pain. Stress and Health. 2008; 24:159–164.Kline, RB. Principles and practice of structural equation modeling. 2. New York: The Guilford Press;
2005.Leino P, Magni G. Depression and distress symptoms as predictors of low back pain, neck-shoulder
pain, and other musculoskeletal morbidity: A 10-year follow-up of metal industry employees.Pain. 1993; 53:89–94. [PubMed: 8316395]
Lindsay PG, Wyckoff M. The depression—pain syndrome and its responses to antidepressants.Psychosomatics. 1981; 22:571–573. [PubMed: 7267947]
Little, RJA.; Rubin, DB. Statistical analysis with missing data. New York: Wiley; 1987.Mackinnon DP, Dwyer JH. Estimating mediated effects in prevention studies. Evaluation Review.
1993; 17:144–158.Magni G, Caldleron C, Rigatti-Luchini S, Merskey H. Chronic musculoskeletal pain and depressive
symptoms in the general population: An analysis of the 1st National Health and NutritionExamination Survey data. Pain. 1990; 43:299–307. [PubMed: 2293141]
Magni G, Marchetti M, Morechi C, Merskey H, Luchini SR. Chronic musculoskeletal pain anddepressive symptoms in the National Health and Nutrition Examination, I: Epidemiologic follow-up study. Pain. 1993; 53:163–168. [PubMed: 8336986]
Mathew RJ, Weinman ML, Mirabi M. Physical symptoms of depression. British Journal of Psychiatry.1981; 139:293–296. [PubMed: 7326538]
McEwen BS, Seeman T. Protective and damaging effects of mediators of stress: Elaborating andtesting the concepts of allostasis and allostatic load. Annals of the New York Academy ofSciences. 1999; 896:30–47. [PubMed: 10681886]
Nierop A, Bratsikas A, Zimmerman R, Ehlert U. Are stress-induced cortisol changes during pregnancyassociated with postpartum depressive symptoms? Psychosomatic Medicine. 2006; 68:931–937.[PubMed: 17132840]
Ormel J, Rijsdijk FV, Sullivan M, van Sonderen E, Kempen GI. Temporal and reciprocal relationshipbetween IADL/ADL disability and depressive symptoms in late life. Journal of Gerontology:Psychological Sciences. 2002; 57B:P338–P347.
Pearlin LI. The sociological study of stress. Journal of Health and Social Behavior. 1989; 30:241–256.[PubMed: 2674272]
Pearlin LI, Lieberman MA, Menaghan EG, Mullan JT. The stress process. Journal of Health and SocialBehavior. 1981; 22:337–356. [PubMed: 7320473]
Polatin PB, Kinney RK, Gatchel RJ, Lillo E, Mayer TG. Psychiatric illness and chronic low-back pain.The mind and the spine – Which goes first? Spine. 1993; 18:66–71. [PubMed: 8434327]
Radloff LS. The CES-D scale: A self-report depression scale for research in the general population.Applied Psychological Measurement. 1977; 1:385–401.
Robles TF, Glaser R, Kiecolt-Glaser JK. Out of balance: A new look at chronic disease, depression,and immunity. Current Directions in Psychological Science. 2005; 14:111–115.
Romano JM, Turner JA. Chronic pain and depression: Does the evidence support a relationship?Psychological Bulletin. 1985; 97:18–34. [PubMed: 3983297]
Rosenthal R, Rubin DB. A note on percent variance explained as a measure of the importance ofeffects. Journal of Applied Social Psychology. 1979; 9:395–396.
Rubin DB. Inference and missing data. Biometrika. 1976; 63:581–592.Ruoff GE. Depression in the patient with chronic pain. Journal of Family Practice. 1996; 43:S25–S33.
[PubMed: 8969710]Schafer, JL. Analysis of incomplete multivariate data. London: Chapman & Hall; 1997.
Gayman et al. Page 11
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Schell E, Theorell T, Hasson D, Arnetz B, Saraste H. Stress biomarkers’ associations to pain in theneck, shoulder and back in healthy media workers: 12-month prospective follow-up. EuropeanSpine Journal. 2008; 17:393–405. [PubMed: 18075764]
Seeman TE, Singer BH, Rowe JW, Horwitz RI, McEwen BS. Price of adaptation—allostatic load andits health consequences. MacArthur Studies of Successful Aging. Archives of Internal Medicine.1997; 157:2259–2268. [PubMed: 9343003]
Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models.Sociological Methodology. 1982; 13:190–212.
Turner RJ, Avison WR. Status variations in stress exposure: Implications for the interpretation ofresearch on race, socioeconomic status, and gender. Journal of Health and Social Behavior. 2003;44:488–505. [PubMed: 15038145]
Turner RJ, Lloyd DA, Taylor J. Physical disability and mental health: An epidemiology of psychiatricand substance disorders. Rehabilitation Psychology. 2006; 51:214–223.
Turner RJ, McLean PD. Physical disability and psychological distress. Rehabilitation Psychology.1989; 34(4):225–242.
Turner RJ, Noh S. Physical disability and depression: A longitudinal analysis. Journal of Health andSocial Behavior. 1988; 29(1):23–37. [PubMed: 2966841]
Ullrich PM, Turner JA, Ciol M, Berger R. Stress is associated with subsequent pain and disabilityamong men with nonbacterial prostatitis/pelvic pain. Annals of Behavioral Medicine. 2005; 30(2):112–118. [PubMed: 16173907]
Verbrugge LM, Jette AM. The disablement process. Social Science and Medicine. 1994; 38:1–14.[PubMed: 8146699]
Von Korff M, Deyo RA, Cherkin D, Barlow W. Back pain in primary care: Outcomes at 1 year. Spine.1993; 18:855–862. [PubMed: 8316884]
Von Korff M, Ormel J, Katon W, Lin EHB. Disability and depression among high utilizers of healthcare: A longitudinal analysis. Archives of General Psychiatry. 1991; 49:91–100. [PubMed:1550468]
Von Korff M, Simon G. The relationship between pain and depression. British Journal of PsychiatrySupplement. 1996; 30:101–108. [PubMed: 8864155]
Wheaton, B. Sampling the stress universe. In: Avison, WR.; Gotlib, IH., editors. Stress and mentalhealth. New York: Plenum Press; 1994. p. 77-115.
Williams DR, Yu Y, Jackson JS, Anderson NB. Racial differences in physical and mental health:Socioeconomic status, stress and discrimination. Journal of Health Psychology. 1997; 2:335–351.
Gayman et al. Page 12
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Reciprocal effects between depressive symptoms and bodily pain. Standardized regressioncoefficients are shown. N = 1,986. Age, gender, race-ethnicity, socioeconomic status, andphysical disability are controlled for in the model but not shown. Model is saturated. W =wave; e1 = error 1; e2 = error 2. *p ≤ .05; **p ≤ .01.
Gayman et al. Page 13
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Depressive symptoms predicting changes in bodily pain: mediating effects of social stress.Standardized regression coefficients are shown. N = 1,986. Age, gender, race-ethnicity,socioeconomic status, and physical disability are controlled for in the model but not shown.Model is saturated. Mediation effects using Sobel test: chronic stress z = .359, p = .720;recent life events z = 2.793, p = .005; daily discrimination z = 1.939, p = .052. W = wave. *p≤ .05; **p ≤ .01.
Gayman et al. Page 14
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Bodily pain predicting changes in depressive symptoms: mediating effects of social stress.Standardized regression coefficients are shown. N = 1,986. Age, gender, race-ethnicity,socioeconomic status, and physical disability are controlled for in the model but not shown.Model is saturated. W = wave. *p ≤ .05; **p ≤ .01.
Gayman et al. Page 15
Stress Health. Author manuscript; available in PMC 2012 February 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gayman et al. Page 16
Tabl
e I
Des
crip
tion
of S
tudy
Var
iabl
es b
y D
isab
ility
Sta
tus
Phys
ical
Dis
abili
ty (N
= 4
10)
No
Phys
ical
Dis
abili
ty (N
= 1,
049)
Tot
al (N
= 1
,459
)
Var
iabl
eW
ave
1 M
ean
(SD
)W
ave
2 M
ean
(SD
)W
ave
1 M
ean
(SD
)W
ave
2 M
ean
(SD
)W
ave
1 M
ean
(SD
)W
ave
2 M
ean
(SD
)
Bod
ily P
aina
8.63
** (8
.28)
5.24
** (6
.12)
2.71
(5.4
9)1.
90 (4
.03)
4.37
(6.9
2)2.
84 (4
.94)
Dep
ress
ive
Sym
ptom
sb23
.26*
* (7
.07)
23.2
4**
(7.2
5)20
.93
(6.3
9)20
.86
(6.3
4)21
.59
(6.6
7)21
.53
(6.6
9)
Chr
onic
Stre
ssc
4.90
* (5
.24)
5.07
** (5
.15)
4.21
(4.7
7)6.
27 (5
.39)
4.40
(4.9
2)5.
93 (5
.35)
Rec
ent L
ife E
vent
sd1.
19*
(1.5
4).9
9 (1
.49)
.99
(1.4
9).8
6 (1
.26)
1.05
(1.5
1).8
9 (1
.33)
Dai
ly D
iscr
imin
atio
ne14
.41*
* (5
.54)
14.3
0**
(5.3
6)13
.30
(4.8
1)13
.38
(4.7
4)13
.61
(5.0
5)13
.64
(4.9
4)
Not
es: N
= 1
,459
. Sho
wn
are
unst
anda
rdiz
ed m
ean
scor
es (S
D) f
or th
ose
who
par
ticip
ated
at b
oth
stud
y w
aves
and
had
val
id d
ata
on a
ll st
udy
varia
bles
. Sig
nific
ant t
ests
com
pare
thos
e w
ho se
lf-co
nfirm
aph
ysic
al d
isab
ility
to th
ose
with
out a
phy
sica
l dis
abili
ty b
y st
udy
wav
e.
a Freq
uenc
y ×
inte
nsity
of b
odily
pai
n ov
er p
revi
ous f
our w
eeks
(ran
ge =
0–2
5).
b Cen
ter f
or E
pide
mio
logi
c St
udie
s Dep
ress
ion
scal
e (r
ange
= 0
–56)
c Ran
ge =
0–3
9.
d Ran
ge =
0–3
2.
e Ran
ge =
9–4
5.
* p<.0
5;
**p<
.01.
Stress Health. Author manuscript; available in PMC 2012 February 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gayman et al. Page 17
Tabl
e II
Cor
rela
tion
mat
rix fo
r stu
dy v
aria
bles
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(1)
P (W
1)-
(2)
P (W
2).4
2-
(3)
DS
(W1)
.12
.12
-
(4)
DS
(W2)
.09
.16
.35
-
(5)
CS
(W1)
.16
.06
.25
.12
-
(6)
CS
(W2)
-.05
.08
.29
-
(7)
RLE
(W1)
.14
.10
.18
.47
.15
-
(8)
RLE
(W2)
.05
.13
.08
.05
.18
.37
.18
-
(9)
DD
(W1)
.12
.15
.34
.17
.29
.14
-
(10)
DD
(W2)
.06
.07
.12
.30
.13
.17
.35
-
(11)
PD (W
1).3
8.3
0.1
6.1
6.0
6-.1
0.0
6.1
0.0
8-
Not
es: N
= 1
,459
. Onl
y si
gnifi
cant
cor
rela
tions
are
show
n (p≤.
05) f
or th
ose
who
par
ticip
ated
at b
oth
stud
y w
aves
and
had
val
id d
ata
on a
ll st
udy
varia
bles
. W =
wav
e. P
= fr
eque
ncy
× in
tens
ity o
f bod
ilypa
in; D
S =
depr
essi
ve sy
mpt
oms (
Cen
ter f
or E
pide
mio
logi
c St
udie
s—D
epre
ssio
n sc
ale)
; CS
= ch
roni
c st
ress
; RLE
= re
cent
life
eve
nts;
DD
= d
aily
dis
crim
inat
ion;
PD
= se
lf-re
porte
d ph
ysic
al d
isab
ility
.
Stress Health. Author manuscript; available in PMC 2012 February 1.