
Symptomatic and Asymptomatic Viral Recrudescence in Solid-Organ Transplant Recipients and Its...
6
Published Ahead of Print 8 August 2007. 2007, 81(20):11538. DOI: 10.1128/JVI.00581-07. J. Virol. Galbraith, Keith McNeil and Rajiv Khanna Campbell, Miles P. Davenport, Scott C. Bell, Andrew Tania Crough, Chrysa Fazou, Julissa Weiss, Scott T-Cell Response + Antigen-Specific CD8 Recipients and Its Relationship with the Recrudescence in Solid-Organ Transplant Symptomatic and Asymptomatic Viral http://jvi.asm.org/content/81/20/11538 Updated information and services can be found at: These include: REFERENCES http://jvi.asm.org/content/81/20/11538#ref-list-1 This article cites 20 articles, 5 of which can be accessed free at: CONTENT ALERTS more» articles cite this article), Receive: RSS Feeds, eTOCs, free email alerts (when new http://journals.asm.org/site/misc/reprints.xhtml Information about commercial reprint orders: http://journals.asm.org/site/subscriptions/ To subscribe to to another ASM Journal go to: on May 6, 2014 by guest http://jvi.asm.org/ Downloaded from on May 6, 2014 by guest http://jvi.asm.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Symptomatic and Asymptomatic Viral Recrudescence in Solid-Organ Transplant Recipients and Its...
Published Ahead of Print 8 August 2007. 2007, 81(20):11538. DOI: 10.1128/JVI.00581-07. J. Virol.
Galbraith, Keith McNeil and Rajiv KhannaCampbell, Miles P. Davenport, Scott C. Bell, Andrew Tania Crough, Chrysa Fazou, Julissa Weiss, Scott
T-Cell Response +Antigen-Specific CD8Recipients and Its Relationship with theRecrudescence in Solid-Organ Transplant Symptomatic and Asymptomatic Viral
http://jvi.asm.org/content/81/20/11538Updated information and services can be found at:
These include:
REFERENCEShttp://jvi.asm.org/content/81/20/11538#ref-list-1This article cites 20 articles, 5 of which can be accessed free at:
CONTENT ALERTS more»articles cite this article),
Receive: RSS Feeds, eTOCs, free email alerts (when new
http://journals.asm.org/site/misc/reprints.xhtmlInformation about commercial reprint orders: http://journals.asm.org/site/subscriptions/To subscribe to to another ASM Journal go to:
on May 6, 2014 by guest
http://jvi.asm.org/
Dow
nloaded from
on May 6, 2014 by guest
http://jvi.asm.org/
Dow
nloaded from

JOURNAL OF VIROLOGY, Oct. 2007, p. 11538–11542 Vol. 81, No. 200022-538X/07/$08.00�0 doi:10.1128/JVI.00581-07Copyright © 2007, American Society for Microbiology. All Rights Reserved.
Symptomatic and Asymptomatic Viral Recrudescence in Solid-OrganTransplant Recipients and Its Relationship with the Antigen-Specific
CD8� T-Cell Response�
Tania Crough,1,2 Chrysa Fazou,1 Julissa Weiss,1 Scott Campbell,3 Miles P. Davenport,4Scott C. Bell,5 Andrew Galbraith,5 Keith McNeil,5 and Rajiv Khanna1*
Australian Centre for Vaccine Development and Tumour Immunology Laboratory, Division of Infectious Diseases and Immunology,Queensland Institute of Medical Research, 300 Herston Road, Brisbane, Queensland 4029, Australia1; School of Medicine,
University of Queensland, Brisbane, Queensland, Australia2; Department of Haematology, Prince of Wales Hospital andCentre for Vascular Research, University of New South Wales, Kensington 2052, Australia4; The Prince Charles Hospital,
Rode Road, Chermside, and Department of Medicine, University of Queensland, Brisbane, Queensland, Australia5;and Department of Nephrology, Princess Alexandra Hospital, and Department of Medicine,
University of Queensland, Brisbane, Queensland, Australia3
Received 19 March 2007/Accepted 26 July 2007
Using ex vivo antigen-specific T-cell analysis, we found that symptomatic cytomegalovirus recrudescence intransplant recipients was coincident with reduced expression of gamma interferon (IFN-�) by virus-specificCD8� T cells and an up-regulation of CD38 expression on these T cells, although there was no significantchange in the absolute number of virus-specific cells (as assessed by major histocompatibility complex-peptidemultimers). In contrast, HLA class I-matched transplant patients with asymptomatic viral recrudescenceshowed increased expansion of antigen-specific T cells and highly stable IFN-� expression by epitope-specificT cells. These studies suggest that a strong functional T-cell response plays a crucial role in defining theclinical outcome of acute viral recrudescence.
The clinical presentation of acute latent viral infections andits interaction with host T-cell responses have recently beeninvestigated in order to understand the dynamics of immuneregulation and to develop better therapeutic strategies (5, 9,10, 20). Previous studies have proposed a role for a number ofpotential factors, such as viral load and cytokine dysregulation,in controlling the symptoms of acute viral infection (1, 17). Itis entirely feasible that the dynamics of emergence of thevirus-specific T-cell response during the early stages of viralrecrudescence may delimitate the patterns of clinical symp-toms in different individuals (11, 13, 16). Indeed, massive ex-pansion of CD8� T cells specific for Epstein-Barr virus latent
and lytic antigens, which is often a feature of acute Epstein-Barr virus infection, suggests that these T-cell responses arerecruited to control the active viral infection (2). However,understanding the biological significance and the longitudinaldynamics of these T cells during acute viral infections in hu-mans is often difficult and is complicated by the nature ofimmune responses in naturally outbred individual patients. Wehave addressed some of these limitations by analyzing thedynamics of T-cell responses to a panel of CD8� T-cellepitopes in a group of HLA class I-matched unrelated humansubjects undergoing acute human cytomegalovirus (HCMV)infection with contrasting clinical symptoms. We studied three
* Corresponding author. Mailing address: Queensland Institute ofMedical Research, Bancroft Centre, 300 Herston Rd., Brisbane, Aus-tralia 4029. Phone: 61-7-3362 0385. Fax: 61-7-3845 3510. E-mail: [email protected].
� Published ahead of print on 8 August 2007.
TABLE 1. List of HLA class I-restricted HCMV epitopes used in this study
Epitope sequence (code) HLArestriction
Antigen Assay used:
Name Expression kinetics ELISPOT MHC-peptidetetramer
YSEHPTFTSQL (YSE) A1 pp65 Late/structural XRPHERNGFTVL (RPH) B7 pp65 Late/structural XNLVPMVATV (NLV) A2 pp65 Late/structural X XVTEHDTLLY (VTE) A1 pp50 Late/structural X XTPRVTGGAM (TPR) B7 pp65 Late/structural X XVLEETSVML (VLE) A2 IE-1 Immediate-early XELRRKMMYM (ELR) B8 IE-1 Immediate-early XQIKVRVDMV (QIK) B8 IE-1 Immediate-early X
11538
on May 6, 2014 by guest
http://jvi.asm.org/
Dow
nloaded from

broad groups of transplant patients: (i) individuals with asymp-tomatic viral recrudescence, (ii) individuals with symptomaticviral recrudescence, and (iii) individuals with no evidence ofviral recrudescence. In each of these groups of patients welongitudinally analyzed CD8� T-cell responses using ex vivoELISPOT assays and major histocompatibility complex(MHC)-peptide multimer analysis. In addition, we also as-sessed the viral load in these individuals to determine whetherthere was any correlation with T-cell dynamics and/or clinicalsymptoms.
Peripheral blood samples from a cohort of 15 HLA class
I-matched solid-organ transplant (SOT) patients (renal orheart and/or lung) were collected into EDTA collection tubes.These blood samples were collected at multiple time points(see Fig. 1), cryopreserved, and used for T-cell assays and viralload analysis. All blood samples were collected following in-formed consent, and the study was approved by the relevanthuman ethics committees. Clinical diagnosis of symptomaticviral recrudescence was based on laboratory diagnosis (pp65antigenemia; �10 positive cells/106 peripheral blood mononu-clear cells [PBMC]) and previously published clinical criteriaoutlined by the American Society of Transplantation (8). Pa-
FIG. 1. Longitudinal functional analysis of HCMV-specific T cells in HLA class I-matched SOT recipients using IFN-� ELISPOT assays andpeptide epitopes from HCMV antigens (Table 1). Data from an individual recipient are presented in each panel. Data from individuals with noevidence of viral recrudescence are presented in panels A to E, those from individuals with asymptomatic recrudescence are presented in panelsF to J, and those from individuals with symptomatic recrudescence are presented in panels K to O. Data presented in panels A to E, K, L, andN are based on SOT patients who received heart and/or lung transplants, while data in panels F to J, M, and O are based on renal transplantrecipients. Gray-shaded areas in panels K to O indicate the time period when clinically active HCMV disease was diagnosed and the patient wasbeing treated with antiviral medication (Table 2). Patients B, D, and E received antiviral prophylaxis based on oral ganciclovir. The results areexpressed as spot-forming cells (SFC) per 106 CD3�/CD8� T cells. Also shown in panels F to O is the HCMV load in peripheral blood of thesepatients as HCMV copies/106 PBMC. Blood sample collection time points (weeks) for each of the donors are indicated on the x axis.
VOL. 81, 2007 NOTES 11539
on May 6, 2014 by guest
http://jvi.asm.org/
Dow
nloaded from

tients with symptomatic HCMV disease were treated with oraland intravenous ganciclovir (the exact period of HCMV dis-ease and treatment is indicated in Fig. 1 as a shaded area) withthe exception of patient N, who received cidofovir. Patient Lalso received foscarnet and valganciclovir. The transplant im-munosuppressive regimens have been outlined elsewhere (14).Briefly, these patients received cyclosporine, mycophenolatemofetil, and prednisolone.
In the first set of studies, we longitudinally analyzed theHCMV-specific T-cell responses using ELISPOT assays andMHC-peptide pentamer/tetramer staining in these transplantpatients as described previously (3, 4). For these assays,HCMV epitopes restricted through various HLA class I alleles(HLA-A1, HLA-A2, HLA-B7, and HLA-B8) were used (Table1). Data from each of these SOT recipients are presented inFig. 1A to O. Longitudinal analysis of immune responsesclearly illustrated that those SOT patients who either showedno evidence of viral recrudescence (Fig. 1A to E) or showedasymptomatic viral recrudescence (Fig. 1F to J) maintained astable virus-specific gamma interferon (IFN-�) expression byCD8� T cells throughout the follow-up period. These re-sponses were towards epitopes derived from both structuraland/or IE-1 antigens. In contrast, HLA-matched SOT recipi-ents who were diagnosed with symptomatic viral recrudescence(Fig. 1K to O; Table 2) showed significant fluctuations of theirvirus-specific IFN-� expression by CD8� T cells. These fluctu-ations ranged from a 3- to 120,000-fold reduction in the virus-specific CD8� T-cell responses. One of the interesting aspectsof this longitudinal analysis was that patients with symptomaticviral recrudescence showed reduced IFN-� expression (�5-fold reduction) by virus-specific CD8� T cells in �70% of theirblood samples, while �10% of the blood samples from SOTrecipients with no viral recrudescence or with asymptomaticviral recrudescence showed reduced IFN-� expression by virus-specific CD8� T cells. Furthermore, T-cell responses towardsmultiple epitopes showed a contemporaneous pattern of fluc-tuation which is consistent with our previous findings forhealthy virus carriers (3). Most importantly, the reduction inthe IFN-� expression by antigen-specific T cells in four of thefive symptomatic recipients preceded the clinical diagnosis ofactive disease. It is important to mention here that the viralload in asymptomatic or symptomatic recipients showed nocorrelation with either IFN-� expression by HCMV-specific T
cells or clinical symptoms. Taken together, these analysesstrongly suggest that a stable antigen-specific CD8� T-cell re-sponse is crucial to prevent symptomatic clinical syndromesfollowing latent viral recrudescence.
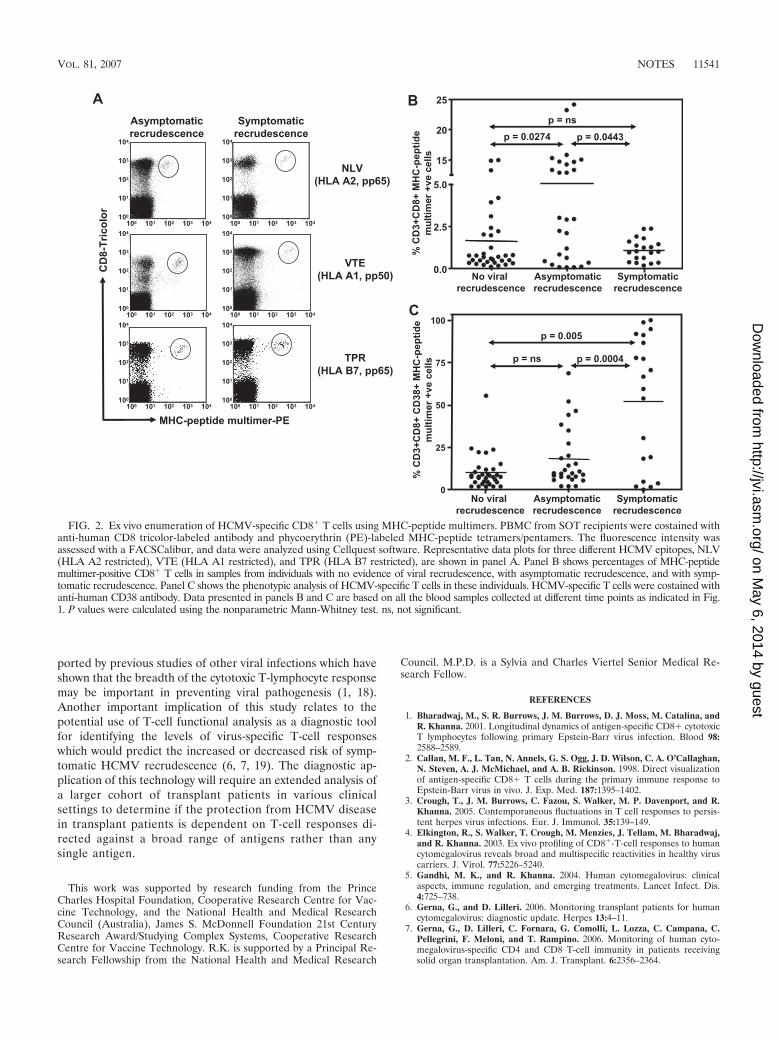
To determine whether the reduced IFN-� expression byvirus-specific T cells in individuals with symptomatic viral re-crudescence was due to the loss of HCMV-specific T cells,PBMC from all SOT recipients were stained with MHC-pep-tide tetramers/pentamers and anti-CD8 antibody (Fig. 2A).Data presented in Fig. 2B show that although there was verylittle difference in the overall numbers of HCMV-specific Tcells between SOT recipients who showed no viral recrudes-cence and those who showed symptomatic recrudescence, asignificant increase in the number of HCMV-specific T cellswas observed in individuals with asymptomatic recrudescence.We hypothesize that this increase in the HCMV-specific T cellsin these individuals is not unexpected, as the viral recrudes-cence would provide increased stimulation to these cells, re-sulting in their expansion, and thus provide protection fromclinical disease. It is highly likely that in addition to the re-duced IFN-� expression, the lack of expansion of HCMV-specific T cells in individuals with symptomatic recrudescencemay also contribute towards the development of clinical dis-ease. Furthermore, we also observed a significant increase inthe expression of CD38 on the HCMV-specific CD8� T cells inSOT recipients with symptomatic viral recrudescence com-pared to recipients who either showed no viral recrudescenceor showed asymptomatic recrudescence (Fig. 2C). No signifi-cant difference in the expression of CD62L or CD27 onHCMV-specific CD8� T cells was observed during or afterantiviral prophylaxis (data not shown). Previous studies of hu-man immunodeficiency virus-infected individuals have shownthat increased expression of CD38 on CD8� T cells is coinci-dent with chronic human immunodeficiency virus disease pro-gression to AIDS (12, 15).
In conclusion, this study is the first to demonstrate directlythat a broadly directed CD8� T-cell response with strong func-tional activity was coincident with the protection from symp-tomatic viral recrudescence. In addition, we have also shownthat terminal differentiation/exhaustion of antigen-specific Tcells (as indicated by the increased CD38 expression) maycontribute towards the development of clinical symptoms fol-lowing viral recrudescence. These conclusions are strongly sup-
TABLE 2. Clinical syndrome in active HCMV disease
Patient codea Clinical syndrome Antiviral therapyb
K (D�/R�) Systemic HCMV infection without defined end organinvolvement
Treatment with ganciclovir (i.v., 400 mg b.i.d.) followed byoral ganciclovir (1,000 mg t.i.d.)
L (D�/R�) Clinical disease with very high viral load and antigenemia Treatment with ganciclovir (i.v., 400 mg b.i.d., followed byvalganciclovir at 450 mg b.i.d.); also treatment with acombination of foscarnet (4 g), i.v. ganciclovir (460 mg),and CMV hyperimmunoglobulin
M (D�/R�) Systemic HCMV infection with gastric involvement Treatment with ganciclovir (i.v., 160 mg b.i.d.) followed byoral ganciclovir (1,000 mg t.i.d.)
N (D�/R�) HCMV syndrome with end organ disease (liver, pancreas,brain, and gut)
Treatment with cidofovir (200 mg weekly)
O (D�/R�) HCMV syndrome without defined end organ involvement Treatment with ganciclovir (i.v., 325 mg b.i.d.) followed byoral ganciclovir (1,000 mg t.i.d.)
a Patient code refers to the panels in Fig. 1.b Abbreviations: i.v., intravenous(ly); b.i.d., twice daily; t.i.d., three times daily; D, donor; R, recipient.
11540 NOTES J. VIROL.
on May 6, 2014 by guest
http://jvi.asm.org/
Dow
nloaded from
ported by previous studies of other viral infections which haveshown that the breadth of the cytotoxic T-lymphocyte responsemay be important in preventing viral pathogenesis (1, 18).Another important implication of this study relates to thepotential use of T-cell functional analysis as a diagnostic toolfor identifying the levels of virus-specific T-cell responseswhich would predict the increased or decreased risk of symp-tomatic HCMV recrudescence (6, 7, 19). The diagnostic ap-plication of this technology will require an extended analysis ofa larger cohort of transplant patients in various clinicalsettings to determine if the protection from HCMV diseasein transplant patients is dependent on T-cell responses di-rected against a broad range of antigens rather than anysingle antigen.
This work was supported by research funding from the PrinceCharles Hospital Foundation, Cooperative Research Centre for Vac-cine Technology, and the National Health and Medical ResearchCouncil (Australia), James S. McDonnell Foundation 21st CenturyResearch Award/Studying Complex Systems, Cooperative ResearchCentre for Vaccine Technology. R.K. is supported by a Principal Re-search Fellowship from the National Health and Medical Research
Council. M.P.D. is a Sylvia and Charles Viertel Senior Medical Re-search Fellow.
REFERENCES
1. Bharadwaj, M., S. R. Burrows, J. M. Burrows, D. J. Moss, M. Catalina, andR. Khanna. 2001. Longitudinal dynamics of antigen-specific CD8� cytotoxicT lymphocytes following primary Epstein-Barr virus infection. Blood 98:2588–2589.
2. Callan, M. F., L. Tan, N. Annels, G. S. Ogg, J. D. Wilson, C. A. O’Callaghan,N. Steven, A. J. McMichael, and A. B. Rickinson. 1998. Direct visualizationof antigen-specific CD8� T cells during the primary immune response toEpstein-Barr virus in vivo. J. Exp. Med. 187:1395–1402.
3. Crough, T., J. M. Burrows, C. Fazou, S. Walker, M. P. Davenport, and R.Khanna. 2005. Contemporaneous fluctuations in T cell responses to persis-tent herpes virus infections. Eur. J. Immunol. 35:139–149.
4. Elkington, R., S. Walker, T. Crough, M. Menzies, J. Tellam, M. Bharadwaj,and R. Khanna. 2003. Ex vivo profiling of CD8�-T-cell responses to humancytomegalovirus reveals broad and multispecific reactivities in healthy viruscarriers. J. Virol. 77:5226–5240.
5. Gandhi, M. K., and R. Khanna. 2004. Human cytomegalovirus: clinicalaspects, immune regulation, and emerging treatments. Lancet Infect. Dis.4:725–738.
6. Gerna, G., and D. Lilleri. 2006. Monitoring transplant patients for humancytomegalovirus: diagnostic update. Herpes 13:4–11.
7. Gerna, G., D. Lilleri, C. Fornara, G. Comolli, L. Lozza, C. Campana, C.Pellegrini, F. Meloni, and T. Rampino. 2006. Monitoring of human cyto-megalovirus-specific CD4 and CD8 T-cell immunity in patients receivingsolid organ transplantation. Am. J. Transplant. 6:2356–2364.
FIG. 2. Ex vivo enumeration of HCMV-specific CD8� T cells using MHC-peptide multimers. PBMC from SOT recipients were costained withanti-human CD8 tricolor-labeled antibody and phycoerythrin (PE)-labeled MHC-peptide tetramers/pentamers. The fluorescence intensity wasassessed with a FACSCalibur, and data were analyzed using Cellquest software. Representative data plots for three different HCMV epitopes, NLV(HLA A2 restricted), VTE (HLA A1 restricted), and TPR (HLA B7 restricted), are shown in panel A. Panel B shows percentages of MHC-peptidemultimer-positive CD8� T cells in samples from individuals with no evidence of viral recrudescence, with asymptomatic recrudescence, and with symp-tomatic recrudescence. Panel C shows the phenotypic analysis of HCMV-specific T cells in these individuals. HCMV-specific T cells were costained withanti-human CD38 antibody. Data presented in panels B and C are based on all the blood samples collected at different time points as indicated in Fig.1. P values were calculated using the nonparametric Mann-Whitney test. ns, not significant.
VOL. 81, 2007 NOTES 11541
on May 6, 2014 by guest
http://jvi.asm.org/
Dow
nloaded from

8. Humar, A., and M. Michaels. 2006. American Society of Transplantationrecommendations for screening, monitoring and reporting of infectious com-plications in immunosuppression trials in recipients of organ transplantation.Am. J. Transplant. 6:262–274.
9. Khanna, R., and D. J. Diamond. 2006. Human cytomegalovirus vaccine: timeto look for alternative options. Trends Mol. Med. 12:26–33.
10. Khanna, R., D. J. Moss, and M. Gandhi. 2005. Applications of emergingimmunotherapeutic strategies for Epstein-Barr virus-associated malignan-cies. Nat. Clin. Pract. Oncol. 2:138–149.
11. Lacey, S. F., D. J. Diamond, and J. A. Zaia. 2004. Assessment of cellularimmunity to human cytomegalovirus in recipients of allogeneic stem celltransplants. Biol. Blood Marrow Transplant. 10:433–447.
12. Liu, Z., W. G. Cumberland, L. E. Hultin, H. E. Prince, R. Detels, and J. V.Giorgi. 1997. Elevated CD38 antigen expression on CD8� T cells is astronger marker for the risk of chronic HIV disease progression to AIDS anddeath in the Multicenter AIDS Cohort Study than CD4� cell count, solubleimmune activation markers, or combinations of HLA-DR and CD38 expres-sion. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 16:83–92.
13. Ljungman, P. 2006. Would monitoring CMV immune responses allow im-proved control of CMV in stem cell transplant patients. J. Clin. Virol.35:493–495.
14. McNeil, K., G. A. Wahlers, T. Knoop, C. Speich, R. Mamelok, R. D. Maurer,J. Ives, and P. A. Corris. 2006. Comparison of mycophenolate mofetil and
azathioprine for prevention of bronchiolitis obliterans syndrome in de novolung transplant recipients. Transplantation 81:998–1003.
15. Paul, M. E., W. T. Shearer, C. A. Kozinetz, and D. E. Lewis. 2001. Compar-ison of CD8� T-cell subsets in HIV-infected rapid progressor children versusnon-rapid progressor children. J. Allergy Clin. Immunol. 108:258–264.
16. Radha, R., S. Jordan, D. Puliyanda, S. Bunnapradist, A. Petrosyan, N. Amet,and M. Toyoda. 2005. Cellular immune responses to cytomegalovirus inrenal transplant recipients. Am. J. Transplant. 5:110–117.
17. Silins, S. L., M. A. Sherritt, J. M. Silleri, S. M. Cross, S. L. Elliott, M.Bharadwaj, T. T. Le, L. E. Morrison, R. Khanna, D. J. Moss, A. Suhrbier,and I. S. Misko. 2001. Asymptomatic primary Epstein-Barr virus infectionoccurs in the absence of blood T-cell repertoire perturbations despite highlevels of systemic viral load. Blood 98:3739–3744.
18. Thimme, R., D. Oldach, K. M. Chang, C. Steiger, S. C. Ray, and F. V.Chisari. 2001. Determinants of viral clearance and persistence during acutehepatitis C virus infection. J. Exp. Med. 194:1395–1406.
19. Walker, S., C. Fazou, T. Crough, R. Holdsworth, P. Kiely, M. Veale, S. Bell,A. Gailbraith, K. McNeil, S. Jones, and R. Khanna. 2007. Ex vivo monitoring ofhuman cytomegalovirus-specific CD8� T-cell responses using QuantiFERON-CMV. Transpl. Infect. Dis. 9:165–170.
20. Zhong, J., and R. Khanna. 2007. Vaccine strategies against human cytomeg-alovirus infection. Expert Rev. Anti-Infect. Ther. 5:449–459.
11542 NOTES J. VIROL.
on May 6, 2014 by guest
http://jvi.asm.org/
Dow
nloaded from




















