
A hybrid BCI speller paradigm combining P300 potential and the SSVEP blocking feature

ELSEVIER Electroencephalography and clinical Neurophysiology 94 (1995) 163-174
Symptomatic and asymptomatic high-grade unilateral internal carotid artery stenosis: scalp topography of event-related potentials (P300)
and psychometric testing
A. Taghavy *, H. Hamer Department of Neurology, University of Erlangen, Schwabachanlage 6, 91054 Erlangen, Germany
Accepted for publication: 22 August 1994
Abstract
Unilateral internal carotid artery (ICA) stenosis may be accompanied by widespread atherosclerosis of extra- and intracranial vessels leading to subtle cognitive disorders. We applied multichannel recording of P300 in 28 patients (68.3 +_ 8.1 years; 15 asymptomatic, 13 with a history of transient ischemic attack (TIA)) and compared them with an age- and sex-matched control group. All underwent a visual "odd-ball paradigm" as well as a psychometric test, the Cognitive Performance Test (CPT), testing mainly visual attention and memory. The potentials were derived from 16 electrodes according to the 10//20 system against linked mastoids. The latencies and amplitudes of N250 and P300 were measured and their amplitudes additionally mapped. Furthermore, the early sensory exogenous potentials, P1 and N1, within the P300 potentials as well as conventional pattern reversal visual evoked potentials (PVEPs) were evaluated.
(1) Both the early exogenous potentials and the conventional PVEPs showed no significant differences among all groups. (2) There were no significant differences between asymptomatic patients and those with a TIA history in all parameters of the P300 complex so that one total patient group was constructed and compared to the controls. (3) Patients' P300 amplitudes showed significant reductions over hemispheres ipsilateral (P < 0.014) and contralateral (P < 0.044) to the stenosis. (4) The N250 amplitudes were reduced only in the central leads (P < 0.05). (5) The latencies of N250 potentials were significantly prolonged at many electrodes, not only ipsi- (P < 0.0007) but also contralateral (P _< 0.022) to the stenosis. (6) The patients' P300 latencies showed significant lengthening only at occipital sites (P < 0.05) compared to controls. (7) In all measured parameters, within the patient group, the differences between hemispheres ipsilateral versus contralateral to the ICA stenoses did not reach statistical significance. (8) The CPT values detected slight cognitive disorders for both patient groups and they correlated significantly with the latencies in many leads. (9) The highest test sensitivity to classify patient:~ versus controls (z score > 2) was reached in P300 maps of TIA patients (77%).
An altered P300 indicate,; electrophysiologically, and CPT behaviorally, subclinical cognitive deficits even in asymptomatic patients with unilateral tight ICA stenoses. Interestingly, no differences between asymptomatic and TIA patients with a high-grade unilateral ICA stenosis could be found.
Keywords: P300; Electrical brain mapping; Psychometry; Internal carotid artery stenosis; Asymptomatic; Transient ischemic attack ('HA)
1. Introduct ion
Stroke remains a leading cause of mortality in industri- alized countries and one of the most frequent cause of disabilities in elderly people. The neuropsychiatric implica-
* Corresponding author. Tel.: + + 49-9131-854310; Fax: + + 49-9131- 854436.
tions of cerebrovascular diseases, however, are relatively neglected, and only few empirical data are available about emotional and cognitive disturbances and their relationship to specific types of cerebrovascular disease. This is espe- cially true for tight carotid artery stenosis, with or without transient ischemic attacks (TIAs). Clinical impressions teach that these patients complain not infrequently of a decrease of concentration and memory, and a diminution in the level of performance and vigor. A recent study
0013-4694/95//$09.50 © 1995 Elsevier Science Ireland Ltd. All rights reserved SSDI 0013-4694(94)00241 -X EEG 93700
164 A. Taghat% H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174
(Oblak et al. 1992) tried to use scaled questionnaires to establish a profile of cognition of these patients, with inconclusive results.
Psychometric studies did not give unanimous results either. On the one hand, Kelly et al. (1980) used psycho- metric testing only in carotid stenoses with TIA symp- tomatology before carotid endarterectomy. They found no significant differences between these patients and controls consisting of patients with peripheral vascular disease. They did not compare the patients with a healthy control. Similarly, Williams and McGee (1964) found descrip- tively, in a group of patients with uni- or bilaterally stenotic carotid arteries, that they "stand up fairly well on intellectual and memorial functions." In contrast to these two studies, Jacobs et al. (1983) compared a group of patients with high-grade internal carotid artery (ICA) stenoses to a group of patients with hemodynamically insignificant lesions of the carotid artery and they were able to show that in several psychometric tests, patients with high-grade stenoses are significantly more impaired. They, however, included patients with "small, stable strokes." Furthermore, Parker et al. (1986) examined psy- chometrically "symptomat ic" patients with carotid disease of different degrees previous to endarterectomy and found them preoperatively significantly more impaired than gen- eral surgery patients. All these studies and several others suffer from the inhomogeneity of the patient populations in respect to the symptomatology and the degrees of their carotid disease. Also, the controls sometimes consisted of
hospital-based patients with or without generalized atherosclerosis. Additionally, a great variety of psychomet- ric tests of various time durations and heterogenous sensi- tivity to organicity were applied. For these reasons, clinical investigators looked for other possibilities, such as the conventional EEG, to evaluate cortical function. Since, however, the conventional EEG was not helpful in the majority of cases (Silva and Gross, 1983), there have been calls for development of new methods for repeatable, non-invasive and objective evaluation of cortical function (Editorial, 1981). We, therefore, used the visually elicited P300 potentials which are well known to correlate highly with cognitive function (Sutton et al., 1965; Gomer et al., 1976; Donchin et al., 1978; Taghavy and Kiigler, 1988; Kiigler et al., 1993). Using its most sensitive form of multichannel recording and electrical brain mapping, P300 was applied in combination with a short psychometric test to two distinct strictly homogenous groups of patients: asymptomatic tight unilateral ICA stenoses and ones with a TIA history. The latter group has a superior response to carotid endarterectomy in comparison to medical treatment as shown by the North American Symptomatic Carotid Endarterectomy Trial (NASCET) collaborators in 1991, whereas the former (asymptomatic tight unilateral ICA stenoses) are currently under intense investigation.
This study could be helpful not only in this regard but also contribute to the pathophysiology of both conditions, such as possible hemodynamic insufficiency under task processing or subtle parenchymal damage in the sense of
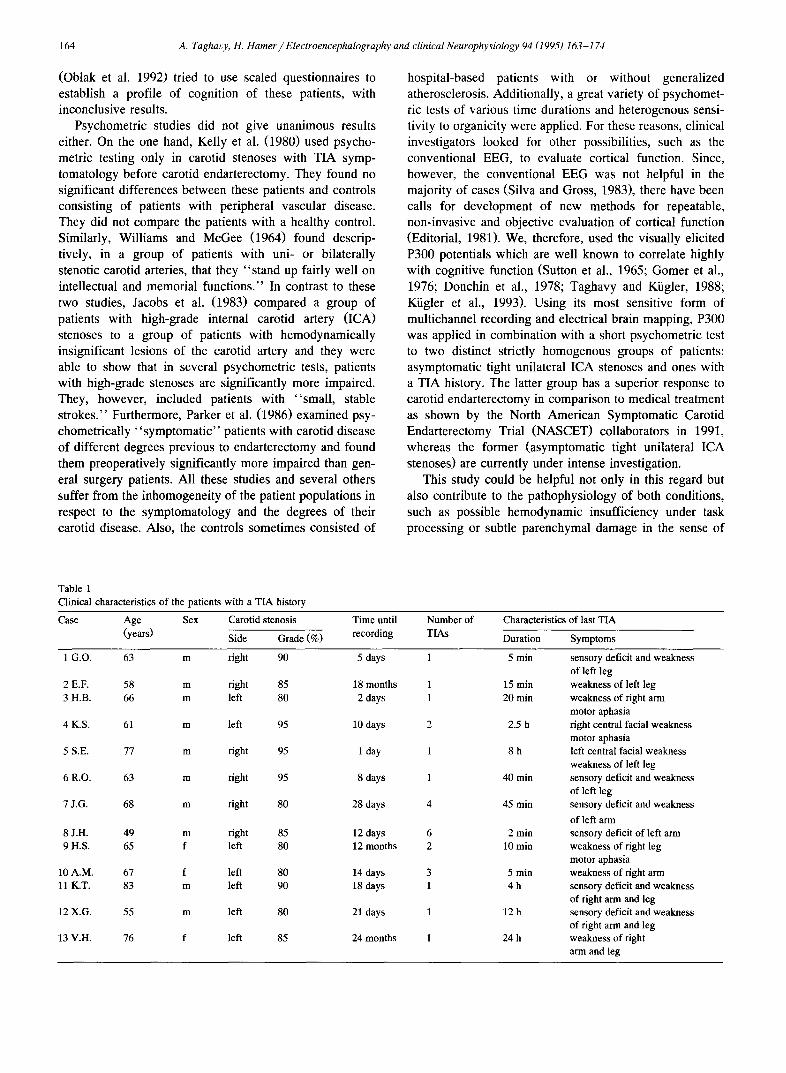
Table 1 Clinical characteristics of the patients with a TIA history
Case Age Sex Carotid stenosis Time until (years) Side Grade (%) recording
Number of Characteristics of last TIA
TIAs Duration Symptoms
1 G.O. 63 m right 90 5 days
2 E.F. 58 m right 85 18 months 3 H.B. 66 m left 80 2 days
4 K.S. 61 m left 95 10 days
5 S.E. 77 m right 95 1 day
6 R.O. 63 m right 95 8 days
7 J.G. 68 m right 80 28 days
8 J.H. 49 m right 85 12 days 9 H.S. 65 f left 80 12 months
10 A.M. 67 f left 80 14 days 11 K.T. 83 m left 90 18 days
12 X.G. 55 m left 80 21 days
13 V.H. 76 f left 85 24 months
1 5 min
1 15 min 1 20 rain
2 2.5 h
1 8h
1 40 min
4 45 min
6 2 min 2 10 min
3 5 min 1 4h
1 12 h
l 24 h
sensory deficit and weakness of left leg weakness of left leg weakness of right arm motor aphasia right central facial weakness motor aphasia left central facial weakness weakness of left leg sensory deficit and weakness of left leg sensory deficit and weakness of left arm sensory deficit of left arm weakness of right leg motor aphasia weakness of right arm sensory deficit and weakness of right arm and leg sensory deficit and weakness of right arm and leg weakness of right arm and leg
A. Taghavy, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174 165
neuronal fall-out. A short communication of the brain mapping part of this work: has been previously presented (Taghavy and Hamer, 1993a).
2. Methods and materials
From among the patients with carotid vascular disease to be operated upon (carotid endarterectomy) in our uni- versity hospital, we studied 28 patients over a period of 2 years (1991-1992) using the following strict criteria:
(1) A 4-vessel angiography had to prove the existence of every ICA stenosis. (2) Only high-grade ICA stenoses (> 80%) were included. (3) The stenosis had to be unilat- eral. The opposite side had to be normal or to have a stenosis of less than 25%. The vertebro-basilar system had to be normal. (4) Only patients considered to be asymp- tomatic or with a history of TIA were included. TIAs referred to the distribution of the vertebro-basilar artery and the posterior cerebral arteries were excluded. All patients in this study had their TIAs referrable to the territories of the carotid arteries. All patients with brain infarction diagnosed clinically or detected in cranial com- puted axial tomography (CAT) scans were excluded. A TIA was defined as a suddenly occurring loss of neurologi- cal function without a precipitant and was characterized as a temporary, completely reversible and non-convulsive focal event secondary to a failure of sufficient blood supply to the brain. By definition, it is agreed that symp- toms and signs of a TIA have to disappear completely within 24 h (Taghavy and Hamer, 1992), this being the case for all of the TIA patients in this study (Table 1). (5) Patients with amaurosis fugax were excluded. All patients and controls had no retinal dysfunction, and possible opti- cal abnormalities were co::rected by glasses. (6) The rou- tine neurological examination was normal in all the pa- tients and no patient received a medication suppressing or activating the brain.
Only 5 of the included patients had cranial CAT scans. All these 5 CAT scans were normal and no CAT scan was performed on controls. The 28 patients included in this study (21 males, 7 female.';, 68.3 _ 8.1 years; mean unilat- eral stenosis: 8 5 _ 5.8%) were divided into 2 subgroups: (I) asymptomatic ICA sl:enoses (11 males, 4 females, 70.7 __+ 6.3 years; mean unilateral stenosis: 84 __+ 5.4%); (II) ICA stenoses with a TIA history (10 males, 3 females, 65.5 + 9.3 years; mean unilateral stenosis: 86 .2_ 6.2%). Between these subgroups there were no significant differ- ences in the age or sex distribution. Fifteen (54%) of the 28 patients had a history of hypertension (7 (54%) of the 13 TIA patients and 8 (153%) of the 15 asymptomatic patients), and 11 (39%) were diabetic (5 (38%) of the TIA and 6 (40%) of the asymptomatic patients). The diabetic patients did not have signs or symptoms of a peripheral neuropathy. Ophthalmologically, there was no evidence of diabetic or hypertensive retinopathy. Ten patients (35%)
had a hypercholesterolemia (6 of the TIA (46%) and 4 of the asymptomatic patients (27%)). All these conditions were adequately treated and all patients received between 250 mg and 500 mg acetylsalicylic acid daily. Nineteen patients (69%) had previously been heavy smokers (10 (77%) of the TIA and 9 (62%) of the asymptomatic patients). No patient had a history of acute or gradual diminution of vision of either eye, which would indicate an acute or chronic anterior ischemic optic neuropathy (AION).
In group I, there were 10 patients with left-sided stenoses and 5 with right-sided ones. The degrees of the stenoses were between 80% and 95%. The clinical conditions which led to the checking of the carotid vessels in group I included coronary heart disease (5 X ), dizziness with or without headache (5 × ), intermittent claudication (3 × ), collapse (1 × ) and hypercholesterolemia (1 x ). Side, grade and clinical characteristics of all ICA stenoses with a TIA history (group II) are listed in Table 1. All patients gave their informed consent to the study.
The patients' data were compared with the data of controls (n = 15). The control group consisted of paid volunteers who did not have any neurological disease or any vascular insufficiency. They did not receive any medi- cation affecting the brain and their neurological examina- tion was completely normal. The controls were sex- and age-matched to all patient groups. Before the electrophysi- ological and psychometric tests, all subjects were given enough time to familiarize themselves with the methods of investigation.
During recording of the P300 complex, the patients, as well as the controls, sat in a darkened room 1 m in front of a TV set and had to fixate on a red L.E.D. lamp in the center of the screen. Both eyes were stimulated. Generated by a NIC-1015 stimulator, 2 different kinds of randomly presented checkerboard patterns, A and B of 120 msec duration each, were flashed at a rate of 1.0 Hz on a grey background. The ratio between the A stimuli, which were to be disregarded, and the task-relevant B stimuli was 4 to 1. The size of the squares of the A stimuli was 48.6' of visual angle (16 × 16 squares) and of the B stimuli 12.5' (64 X 64 squares). The subjects had to keep a silent run- ning count of the infrequent B stimuli (Taghavy and Kiigler, 1988).
Twenty-two silver chloride electrodes were used. The potentials were derived simultaneously from 16 electrodes on the scalp (Fpl, Fp2, F3, F4, F7, F8, Fz, C3, C4, P3, P4, Pz, T5, T6, O1 and 02) according to the international 10/20 system against linked mastoids (ground electrode at the arm; sensitivity: + 50 gV; filter frequency: 1-30 Hz). A vertical and a horizontal electro-oculogram (4 elec- trodes) were recorded for additional artefact rejection (sensitivity: _ 100 /zV). Care was taken that the electrode resistances were persistently under 5 k T2. The potentials were averaged over 250 artefact-free sweeps of 750 msec duration, including a 10% prestimulus interval. The electri-
166 A. TaghaL,y, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (I995) 163-174
cal responses to the A and B stimuli were averaged separately in 2 different 16-channel memory blocks of the 32-channel Nicolet Pathfinder II. We studied the early sensory exogenous potentials (P1 and N1) in the A poten- tials related to the frequent stimuli and the P300 complex (N250 and P300 potential) in the B potentials related to the target stimuli. After the intrasessional psychometric test- ing, the recordings were repeated at least once. The poten- tials averaged from both records were used for statistical measurements.
The amplitudes of P1, N1, N250 and P300 were mea- sured and mapped peak to baseline. P1 was the first positive peak around 90 msec in the A potentials of the occipital region. N1 was the following negative potential around 115 msec. N250 potential was defined as the immediately preceding negative peak to P300. P1, N1 and N250 were mapped from the peak in the occipital lead and P300 from the peak in Pz. The latencies of the potentials were measured in frontal, central, parietal, temporal and occipital leads.
Additionally, conventional pattern reversal visual evoked potentials (PVEPs) were recorded binocularly in all subjects after a period of rest. A black and white checkerboard pattern with a checksize of 48.6' of visual angle reversed at a rate of 1.9 Hz (sensitivity: 25 /zV; number of averages: twice 100). All other experimental conditions were identical to the P300 recordings.
In respect to each patient there were 2 variables to consider: "hemispheres ipsilateral or contralateral to the ICA stenosis" and "left or right hemispheres." This would have resulted in at least 4 groups of TIA patients and 4 groups of asymptomatic patients. However, to avoid multiple comparisons as much as possible, we performed the following procedure to keep the number of different groups at a reasonable level.
For the statistical analysis of the potentials we collected all curves which were derived over hemispheres ipsilateral to the ICA stenosis in corresponding leads of one side. For example, in respect of the parietal leads P3 and P4, we derived in the 17 cases with a left-sided stenosis the potentials ipsilateral to the ICA stenosis in the lead P3 and in the remaining 11 cases (with right-sided ICA stenoses), the potentials ipsilateral to the stenosis were derived in P4. Since ipsilaterality to the stenosis was one of the main issues in this study, we grouped the above mentioned 17 potentials of P3 and the 11 potentials of P4 into one lead: P3/4-ipsilateral. Likewise, we obtained: O1/2-ipsilateral, T5/6-ipsilateral , P3/4-ipsilateral, C3/4-ipsilateral, F3/4-ipsilateral, F7/8-ipsilateral, Fpl/2-ipsilateral. Con- versely, the same procedure was applied to curves derived over hemispheres contralateral to the stenosis: O1/2-con- tralateral, T5/6-contralateral. etc.. In midline electrodes Pz and Fz, there was no need to employ this procedure.
Since there were now in every "lead ipsilateral to the stenosis" (for example P3/4-ipsilateral) 17 left hemi- spheric (61%) and 11 right hemispheric (39%) curves, we
had to exclude the possible effect of a physiological hemispheric asymmetry of the potentials since this has been shown in younger adults (Taghavy and Hamer, 1993b) but not conclusively in the study's age group. This was done by grouping the left hemispheric potentials of 61% of the control cases together with the right hemispheric poten- tials of the remaining 39% of the controls. The newly arranged group of 61% left and 39% right hemispheric potentials was gathered in corresponding leads of one side of the control's scalp; this acting as the matched control leads for the patients' "leads ipsilateral to the stenosis." Conversely, 39% left and 61% right hemispheric potentials were grouped on the other side of the control's scalp, providing the matched control leads for the patients' hemi- spheres contralateral to the stenosis.
The statistical analysis was performed according to Breslau et al. (1989). Differences between groups were assessed separately for the latency and the amplitude of each measured potential. A 2-way analysis of variance (ANOVA: lead (1-16)X group) for repeated measures was used. The Greenhouse-Geisser correction to reduce degrees of freedom was performed to avoid type I errors caused by falsely increased degrees of freedom in repeated measures ANOVA. Where significant ( P < 0.05) results were found, the ANOVA was repeated with values normal- ized with a z transformation. This was done to correct for the multiplicative effect on event-related potential voltages produced by differences in source strength (McCarthy and Wood, 1985). Within the z transformation, each value was re-expressed as (va lue - mean across all leads)/standard deviation. The z transformed latencies and amplitudes with significant lead x group interactions were chosen for post hoc 2-tailed t tests between corresponding leads to illustrate the regional effects of the overall significant interaction.
In order to assess possible differences between poten- tials derived over hemispheres ipsilateral versus contralat- eral to the stenosis within the patient group, we used the A_NOVA design "within-subjects (repeated measures) ANOVA with multiple dependent measures (MANOVA)." Electrical brain mapping of the amplitudes was used to exhibit graphically the statistically confirmed significance patterns. Figures were developed showing the distribution of the amplitudes in each group in addition to "maps" based exclusively on the 16 t values from the t tests between corresponding leads. Furthermore, we compared critically the results of the ANOVA as a profile analysis to the commonly accepted procedure of t test comparisons within electrical brain mapping.
Twenty-six of the patients and all of the controls under- went a psychometric test of 10-15 min duration during the pause between the two P300 recordings. In 2 patients, the test could not be performed because their native language was not German. The psychometric test CPT ( = cognitive performance test = Syndromkurztest (SKT); Erzigkeit, 1989; Overall and Schaltenbrand, 1992) is a specially
A. Taghavy, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174
Grand-Averages of event related visual P300 potentials r e l a t e d t o n o n - t a r g e t a n d t a r g e t s t i m u l i
167
P 3 O O - p o t e n t i a l s
r e l a t e d t o n o n -
t a r g e t s t i m u l i
j lO~V
150ms
P3OO-potentials related to target
stimuli
control-hemispheres nsymptomntic patients: TIA patients: (n = 15) h~d~acres il~ilntarnl to hemisi~a~ il~ilatcral to
the l e a steaasis (n - 15) the 1CA stenosis (n - 13)
F / / I
O V I
I I I i i i i i i i * l
P l | NI
P ~ 4
l I I I i i i I I I
o i I N250 P300
I I I I , i i i i I I i i i i i i I I
0 | 0 Pi i el 1
NI NI
i i i I I i 1 i i i I I I I I I I I I I
* I I * 1 1 N250 P300 N250 P300
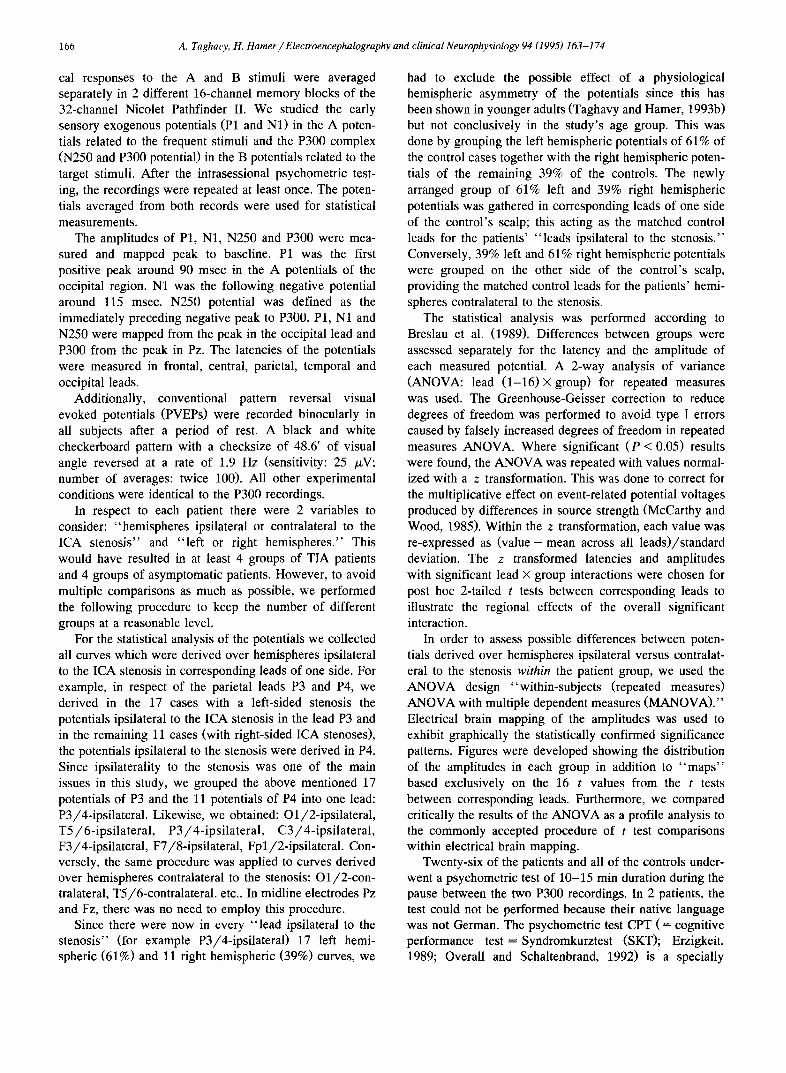
Fig. 1. The early sensory exogenous potentials (P1 and N1) were evaluated in the A potentials related to the frequent st imuli (above) and the P300 complex
(N250 and P300 potential) was :measured in the B potentials related to the target stimuli (below). Note that in comparison to the controls ' potentials, the potentials of both patient groups are visual ly flattened and in case of the P300 complex also prolonged.
devised test, extensively validated and adjusted according to age, intelligence and social background, used for the evaluation of visual attention, memory, visuo-motor skills and symbol handling. It consists of 9 subtests: naming
objects, immediate recall, naming numerals, arranging blocks, replacing blocks, counting symbols, reversal nam- ing, delayed recall, and recognition memory. Norms based on German data stratified into 4 age intervals and 3 levels
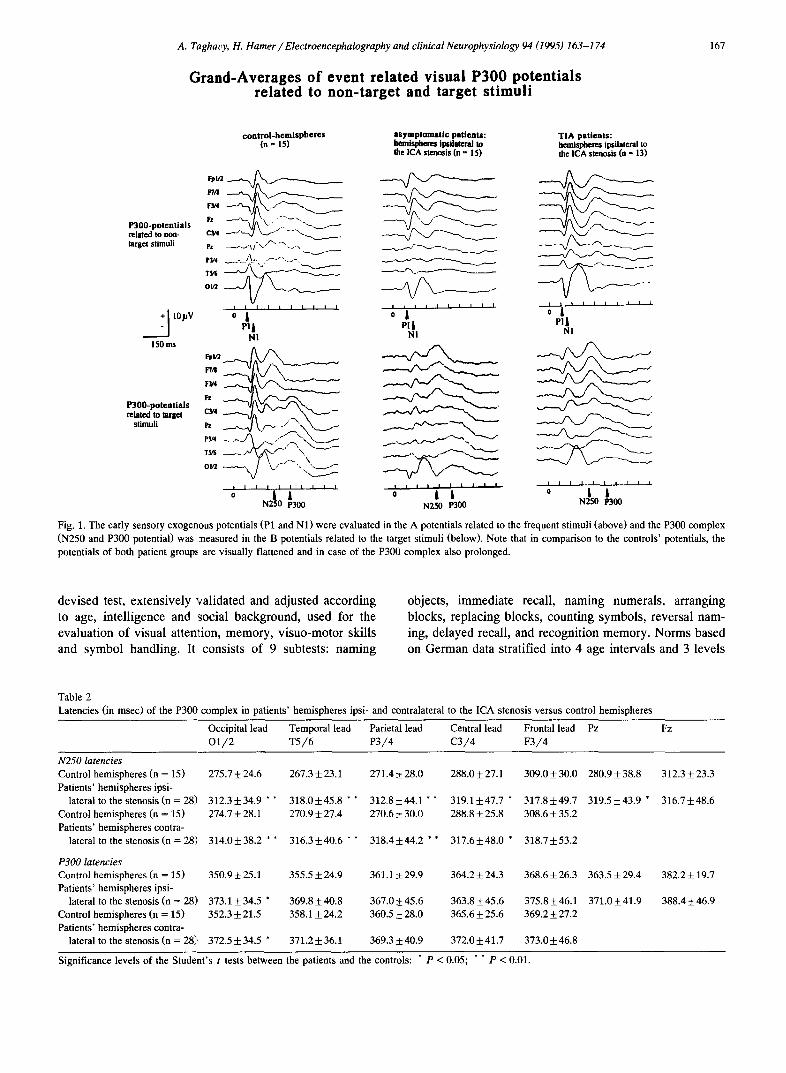
Table 2 Latencies (in msec) of the P300 complex in patients ' hemispheres ipsi- and contralateral to the ICA stenosis versus control hemispheres
Occipital lead Temporal lead Parietal lead Central lead Frontal lead Pz Fz O 1 / 2 T 5 / 6 P 3 / 4 C 3 / 4 F 3 / 4
N250 latencies Control hemispheres (n = 15) 275.7 + 24.6
Patients ' hemispheres ipsi- lateral to the stenosis (n = 28) 312.3 +_ 34.9 * *
Control hemispheres (n = 15) 274.7 + 28.1
Patients ' hemispheres contra- lateral to the stenosis (n = 28) 314.0 + 38.2 * *
P300 latencies Control hemispheres (n = 15) 350.9 ± 25.1 Patients ' hemispheres ipsi-
lateral to the stenosis (n = 28), 373.1 + 34.5 * Control hemispheres (n = 15) 352.3 + 21.5
Patients ' hemispheres contra- lateral to the stenosis (n = 28], 372.5 +- 34.5 *
267.3 ___ 23.1 271.4 + 28.0 288.0 + 27.1 309.0 + 30.0 280.9 + 38.8 312.3 + 23.3
318 .0+45 .8 * * 312 .8+44 .1 * * 319 .1+47 .7 * 317 .8+49 .7 319 .5+43 .9 * 316.7+_48.6 270.9 _+ 27.4 270.6 _+ 30.0 288.8 + 25.8 308.6 + 35.2
316 .3+40 .6 * * 318.4::1:44.2 * * 317 .6+48 .0 * 318 .7+53 .2
355.5 _+ 24.9 361.1 +,+_ 29.9 364.2 -t- 24.3 368.6 _+ 26.3 363.5 _+ 29.4 382.2 +_ 19.7
369.8 + 40.8 367.0 _+ 45.6 363.8 + 45.6 375.8 + 46.1 371.0 + 41.9 388.4 + 46.9 358.1 + 24.2 360.5 _+ 28.0 365.6 + 25.6 369.2 + 27.2
371.2 + 36.1 369.3 + 40.9 372.0 +__ 41.7 373.0 _+ 46.8
Significance levels of the Student 's t tests between the patients and the controls: * P < 0.05; * * P < 0.01.
168 A. Taghavy, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174
of estimated intelligence are included in the test manual (Erzigkeit, 1989).
3 . R e s u l t s
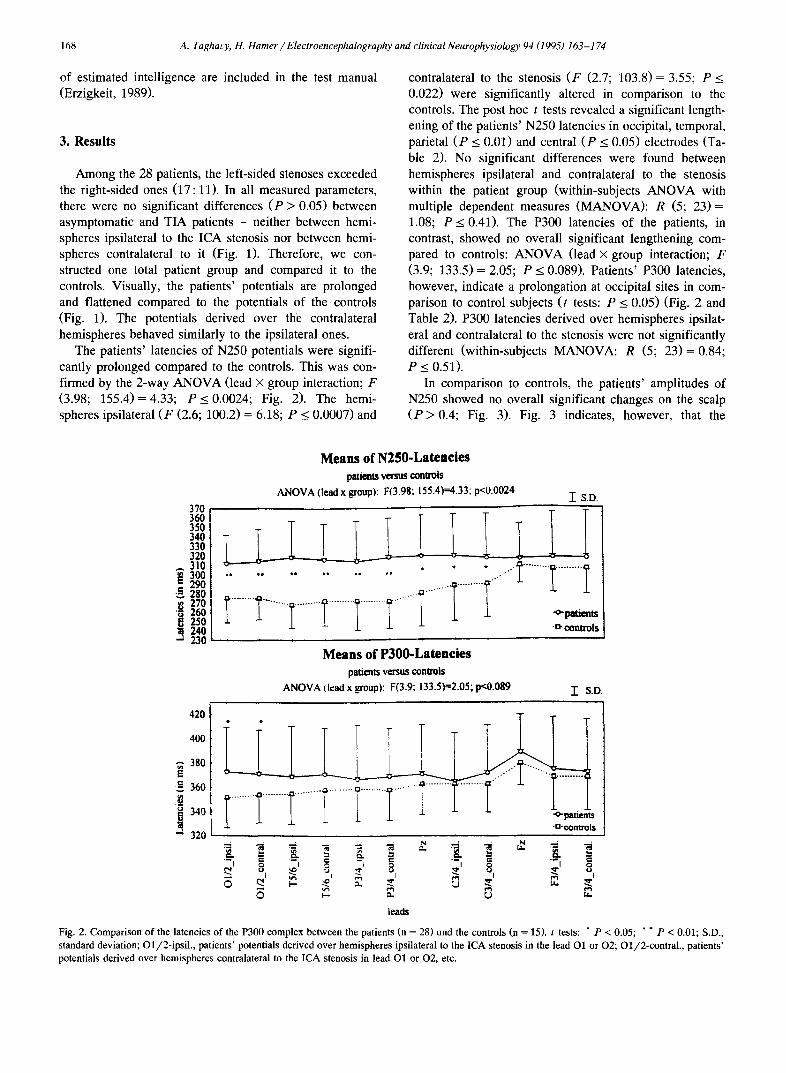
Among the 28 patients, the left-sided stenoses exceeded the right-sided ones (17: 11). In all measured parameters, there were no significant differences ( P > 0.05) between asymptomatic and TIA patients - neither between hemi- spheres ipsilateral to the ICA stenosis nor between hemi- spheres contralateral to it (Fig. 1). Therefore, we con- structed one total patient group and compared it to the controls. Visually, the patients' potentials are prolonged and flattened compared to the potentials of the controls (Fig. 1). The potentials derived over the contralateral hemispheres behaved similarly to the ipsilateral ones.
The patients' latencies of N250 potentials were signifi- cantly prolonged compared to the controls. This was con- firmed by the 2-way ANOVA (lead × group interaction; F (3.98; 155.4)=4.33; P < 0.0024; Fig. 2). The hemi- spheres ipsilateral ( F (2.6; 100.2) = 6.18; P < 0.0007) and
contralateral to the stenosis ( F (2.7; 103.8)= 3.55; P < 0.022) were significantly altered in comparison to the controls. The post hoc t tests revealed a significant length- ening of the patients' N250 latencies in occipital, temporal, parietal ( P < 0.01) and central ( P < 0.05) electrodes (Ta- ble 2). No significant differences were found between hemispheres ipsilateral and contralateral to the stenosis within the patient group (within-subjects ANOVA with multiple dependent measures (MANOVA): R (5; 2 3 ) = 1.08; P < 0.41). The P300 latencies of the patients, in contrast, showed no overall significant lengthening com- pared to controls: ANOVA (lead × group interaction; F (3.9; 133.5) = 2.05; P < 0.089). Patients' P300 latencies, however, indicate a prolongation at occipital sites in com- parison to control subjects (t tests: P < 0.05) (Fig. 2 and Table 2). P300 latencies derived over hemispheres ipsilat- eral and contralateral to the stenosis were not significantly different (within-subjects MANOVA: R (5; 2 3 ) = 0.84; P < 0.51).
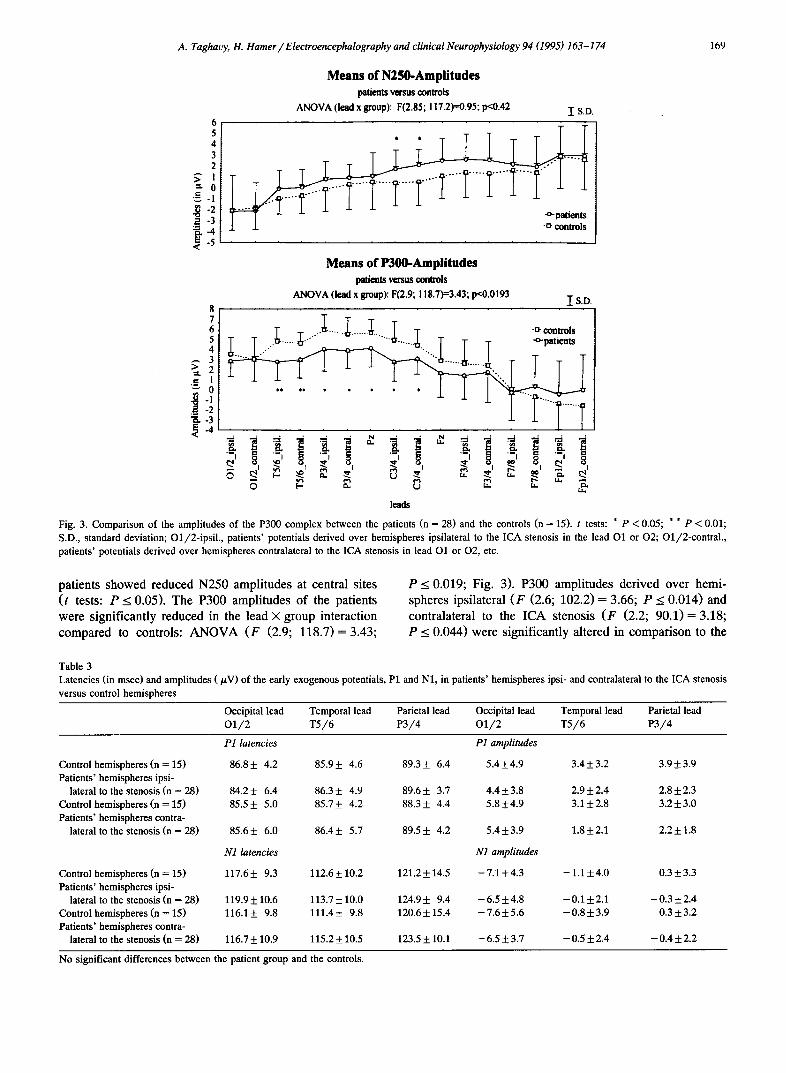
In comparison to controls, the patients' amplitudes of N250 showed no overall significant changes on the scalp ( P > 0.4; Fig. 3). Fig. 3 indicates, however, that the
M e a n s o f N 2 5 0 - L a t e n c i e s
patients versus conu~ls
ANOVA (lead x groupl: F(3.98; 155.4)=4.33; p<0.0024 -[ S.D 370
ai2222 350 3411 330 320 , -
310 I i I
280 ...................
- I I I I I I ......... ......... 270 ......................................
250 240 -o- controls
.a 230 M e a n s o f P 3 0 0 - L a t e n e i e s
patients versus controls
A N O V A (lead x #oup): F(3.9; 133.5)=2.05; p<0.089 1" S.D.
420 • .
4OO
380 e -
-~ 360
340 -o-patients =~ 320 -n-controls
• =. ~ N . . . . ~ ~ . ~ g .-g ,..,
leads
Fig. 2. Comparison o f the latoncies of the P300 complex between the patients (n = 2S) und the controls (n = ]5) . t tests: * P < 0.05; * * P < 0.01; S.D., standard deviation; O1/2-ipsil., patients' potentials derived over hemispheres ipsilateral to the ICA stenosis in the lead O1 or 02; Ol/2-contral., patients' potentials derived over hemispheres contralateral to the ICA stenosis in lead O1 or 02, etc.
A. Tag~avy, It. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174 169
6 5 4 3 2
ff i "~ 0
~ . - 4
Means of N250-Amplitudes patients versus controls
ANOVA (lead x group): F(2.85; 117.2)=0.95; p<0.42 IS.D.
t Means of P300-Amplitudes
patients venus ¢mntrols
ANOVA (le.ad x group): F(2.9; 118.7)=3.43; p<0.0193 I S.D. 8 7 6 T T ...... ....... T T 5 T T i n - - ] ] - . 6 . . . . _ . . . . ~ - I i l l • . ~ T T T patients
2
~.
_ ' , - s ,
leads
Fig. 3. Comparison of the amplitttdes of the P300 complex between the patients (n = 28) and the controls (n = 15). t tests: * P < 0.05; * * P < 0.01; S.D., standard deviation; O1/2-ipfil., patients' potentials derived over hemispheres ipsilateral to the ICA stenosis in the lead O1 or 02; O1/2-contral., patients' potentials derived over hemispheres contralateral to the ICA stenosis in lead O1 or O2, etc.
patients showed reduced N250 amplitudes at central sites (t tests: P < 0.05). The P300 amplitudes of the patients were significantly reduced in the lead × group interaction compared to controls: ANOVA (F (2.9; 118.7)= 3.43;
P < 0.019; Fig. 3). P300 amplitudes derived over hemi- spheres ipsilateral (F (2.6; 102.2) = 3.66; P < 0.014) and contralateral to the ICA stenosis (F (2.2; 90.1)= 3.18; P < 0.044) were significantly altered in comparison to the
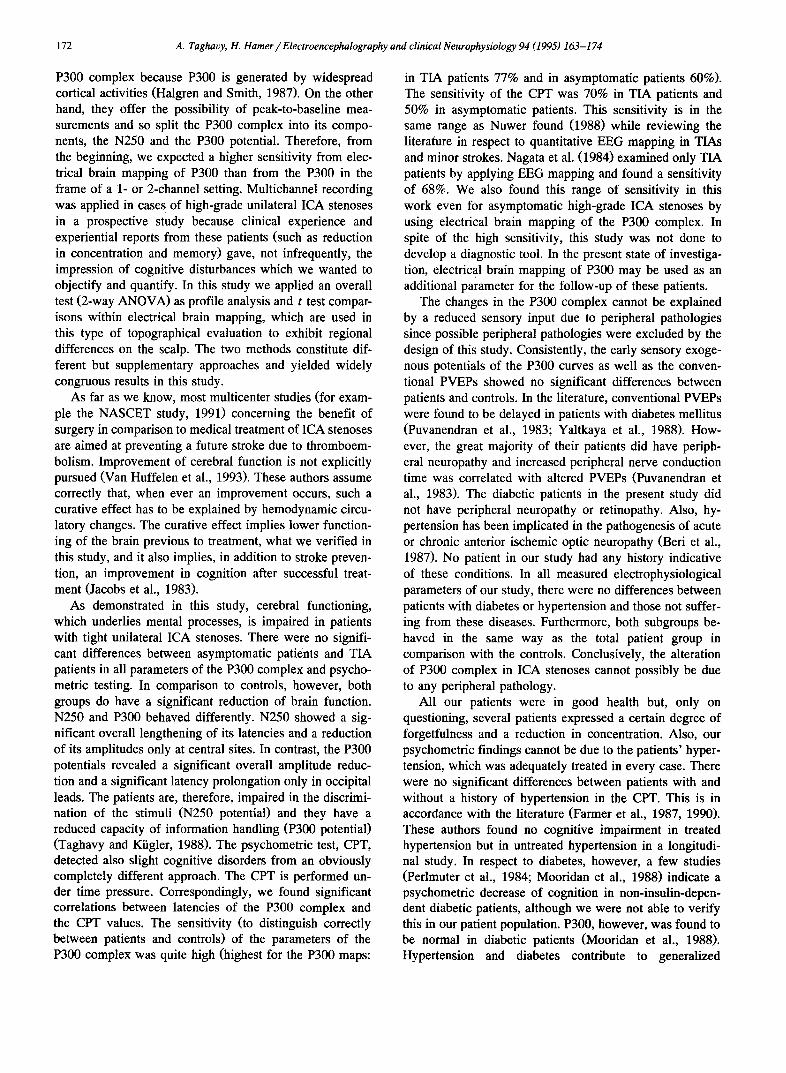
Table 3 Latencies (in msec) and amplitudes (pV) of the early exogenous potentials, P1 and N1, in patients' hemispheres ±psi- and contralateral to the ICA stenosis versus control hemispheres
Occipital lead Temporal lead Parietal lead Occipital lead Temporal lead Parietal lead O1 /2 T5 /6 P3 /4 O1 /2 T5/6 P3 /4
Control hemispheres (n = 15) Patients' hemispheres ±psi-
lateral to the stenosis (n = 28) Control hemispheres (n = 15) Patients' hemispheres contra-
lateral to the stenosis (n = 28)
Control hemispheres (n = 15) Patients' hemispheres ±psi-
lateral to the stenosis (n = 28) Control hemispheres (n = 15) Patients' hemispheres contra-
lateral to the stenosis (n = 28)
H ~tencies ~ amp~mdes
86.8± 4.2 85.9± 4.6 89.3± 6.4 5.4±4.9 3.4±3.2 3.9±3.9
84.2± 6.4 86.3± 4.9 89.6± 3.7 4.4±3.8 2.9±2.4 2.8±2.3 85.5± 5.0 85.7± 4.2 88.3± 4.4 5.8±4.9 3.1±2.8 3.2±3.0
85.6± 6.0 86.4± 5.7 89.5± 4.2 5.4±3.9 1.8±2.1 2.2±1.8
Nl~tencies NlampHmdes
117.6± 9.3 112.6±10.2 121.2±14.5 - 7 . 1 ± 4 . 3 - 1 . 1 ± 4 . 0 0.3±3.3
119.9±10.6 113.7±10.0 1 ~ . 9 ± 9.4 - 6 . 5 ± 4 . 8 - 0 . 1 ± 2 . 1 - 0 . 3 ± 2 . 4 116.1± 9.8 111.4± 9.8 1~ .6±15 .4 - 7 . 6 ± 5 . 6 - 0 . 8 ± 3 . 9 0.3±3.2
116.7±10.9 115.2±10.5 123.5±10.1 - 6 . 5 ± 3 . 7 - 0 . 5 ± 2 . 4 - 0 . 4 ± 2 . 2
No significant differences between the patient group and the controls.
170 A. Taghavy, 1"1. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174
o f 1'300 potential : patients, with stenosis versus controls
p a t i e n t s w i t h left con t ro l - IP~ |tOgA ~:t~nn~i~ h p m ~ c n h ~ r ~
-1 4 ~ 5 9
right control- h e m i s p h e r e s
- 3 ¢ ~ 3 4
h e m i s p h e r e s con t ra l~ te ra l t o t h e s t e n o s i s
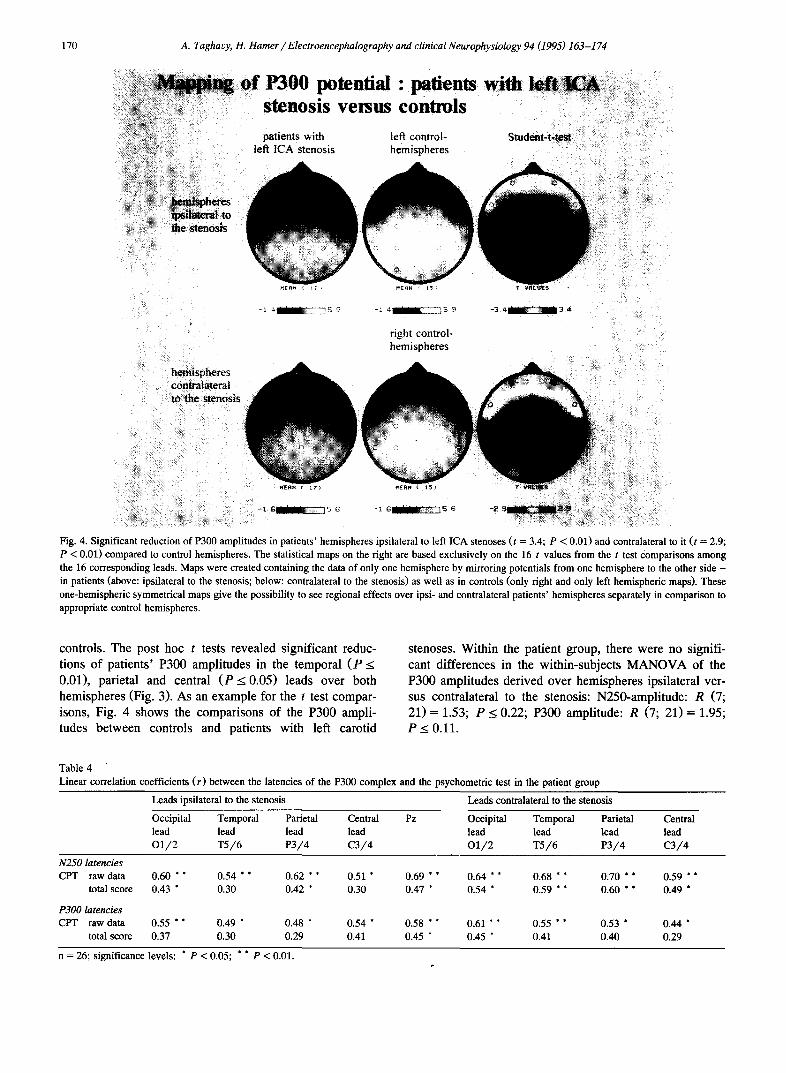
Fig. 4. Significant reduction of P300 ampli tudes in patients ' hemispheres ipsilateral to left ICA stenoses (t = 3.4; P < 0.01) and contralateral to it ( t = 2.9;
P < 0.01) compared to control hemispheres. The statistical maps on the right are based exclusively on the 16 t values from the t test Comparisons among
the 16 corresponding leads. Maps were created containing the data of only one hemisphere by mirroring potentials from one hemisphere to the other side -
in patients (above: ipsilateral to the stenosis; below: contralateral to the stenosis) as well as in controls (only right and only left hemispheric maps). These
one-hemispheric symmetrical maps give the possibil i ty to see regional effects over ipsi- and contralateral patients ' hemispheres separately in comparison to appropriate control hemispheres.
controls. The post hoc t tests revealed significant reduc- tions of patients' P300 amplitudes in the temporal ( P < 0.01), parietal and central ( P < 0.05) leads over both hemispheres (Fig. 3). As an example for the t test compar- isons, Fig. 4 shows the comparisons of the P300 ampli- tudes between controls and patients with left carotid
stenoses. Within the patient group, there were no signifi- cant differences in the within-subjects MANOVA of the P300 amplitudes derived over hemispheres ipsilateral ver- sus contralateral to the stenosis: N250-amplitude: R (7; 21) = 1.53; P < 0.22; P300 amplitude: R (7; 21)= 1.95; P < 0.11.
Table 4
Linear correlation coefficients ( r ) between the latencies of the P300 complex and the psychometric test in the patient group
Leads ipsilateral to the stenosis Leads contralateral to the stenosis
Occipital Temporal Parietal Central Pz Occipital Temporal Parietal Central
lead lead lead lead lead lead lead lead O 1 / 2 T 5 / 6 P 3 / 4 C 3 / 4 O 1 / 2 T 5 / 6 P 3 / 4 C 3 / 4
N250 latencies CPT raw data 0.60 * * 0.54 * * 0.62 * * 0.51 * 0.69 * * 0.64 * * 0.68 * * 0.70 * * 0.59 ° *
total score 0.43 * 0.30 0.42 * 0.30 0.47 * 0.54 * 0.59 * * 0.60 * * 0.49 *
P300 latencies CPT raw data 0.55 * * 0.49 * 0.48 * 0.54 * 0.58 * * 0.61 * * 0.55 * * 0.53 * 0.44 °
total score 0.37 0.30 0.29 0.41 0.45 * 0.45 ° 0.41 0.40 0.29
n = 26; significance levels: * P < 0.05; * * P < 0.01.

A. Tag,~avy, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174 171
Although the data shown in Fig. 1 suggest that the early sensory exogenous potentia]ts, P1 and N1, may be reduced in the patients, no signific, ant differences ( P > 0.05) of both these potentials could be established in the statistical tests between patients and controls or within the patient group - either for their latencies or for their amplitudes in all leads (Table 3 gives the data of the occipital, temporal and parietal leads). Similarly, there were no significant differences ( P > 0 . 0 5 ) in the lead×group interaction (ANOVA) of the conventional PVEPs, N80 and P100 potentials, between the patient group and the controls.
Furthermore, we divided the patient group in 2 sub- groups: carotid stenoses witi~ diabetes and/or hypertension and those not sufferering from these conditions. In all measured parameters, there were no significant differences ( P > 0.05) between these 2 subgroups. In comparison to the controls, however, both subgroups behaved statistically in the same way as the total patient group.
The cognitive performance test (CPT) revealed a score of 7.1 +_ 3.9 for TIA patients and 5 . 2 _ 3.2 for asymp- tomatic patients. These scores were not significantly differ- ent from each other but both were well above the accepted normal range according to the test manual (normal range: 0-4) (Erzigkeit, 1989), indicating a slight cognitive disor- der for both groups of patients. In addition to the normal range in the test manual, our. own controls' CPT score was 1.6 ___ 1.2, staying significantly (t = 5.21; resp. t = 4.07; P < 0.001) below the scores of both groups of patients. Significant linear correlation coefficients between .the la- tencies of the potentials and the CPT scores were found in the patients (Table 4). Asymptomatic and TIA patients behaved in the same way. /vlany leads ipsi- and contralat- eral to the stenosis revealed significantly (P < 0.01) posi- tive correlation coefficients between the CPT raw data and the latencies of both potentials, meaning the longer the 'latencies the higher the cFq ~ scores and the more severe the cognitive disorders. In every case, the total scores of the CPT displayed smaller correlation coefficients than the raw data. This can be because, in contrast to the total scores, the raw data are not age- and intelligence-corrected like the potentials' latencies. The correlation coefficients between CPT and N250 latencies were higher (up to r = + 0.70; P < 0.01) than between CPT and P300 (up to r = +0.61; P < 0.01) (Table 4).
As regards hypertension and diabetes among the pa- tients, there were no significant differences ( P > 0.05) between the CPT scores of patients with a history of hypertension and/or diabetes and the scores of those patients not suffering from these conditions. Both sub- groups behaved in the same., way as the total patient group in comparison to the controls.
Z scores of all parameters of the patients were calcu- lated: 77% of the P300 maps in TIA patients and 60% in asymptomatic patients deviated more than 2 S.D. from the control average (z score > 2), whereas in the case of N250 maps only 46% resp. 40% showed a z score> 2. In
respect to the N250 latencies, 69% of the TIA and 40% of the asymptomatic patients revealed a z score > 2. This was true for only 39% resp. 33% of the patients in regard to the P300 latencies. For the CPT values, z scores > 2 were obtained in 70% for TIA and 50% for asymptomatic patients.
4. Discussion
To the best of our knowledge, this is the first study applying P300 potentials to two distinct groups of patients with a severe unilateral ICA stenosis: asymptomatic pa- tients and patients with a TIA history. Additionally, we performed a short psychometric test. We intentionally selected this test of 10-15 min duration to avoid the decreasing attention span and fatigue over time of elderly people (Overall and Schaltenbrand, 1992). In the literature (Kelly et al., 1980; Jacobs et al., 1983; Parker et al., 1986; Oblak et al., 1992), such psychometric tests abound and reveal contradictory results so that the necessity was evi- dent for applying an objective, basically biological, repro- ducible and repeatable test such as offered by P300. Addi- tionally, compared to psychometric tests, P300 is more independent of patients' motivation (Wine, 1971), has less practice effect and only negligible test-retest variations. Furthermore, it is a method which is widely independent of language. Therefore, P300 may be a proper tool for the follow-up of patients pre- and postoperatively to a carotid endarterectomy. The P300 complex reflects cognitive func- tion of the brain, and ever since it was discovered by Sutton et al. (1965), it has been the most widely studied potential among the cognitive event-related potentials. It is not a unitary phenomenon but rather consists of overlap- ping late negative and positive potentials related to differ- ent processes (Neville and Lawson, 1987). We were able to show in 1988 (Taghavy and Kiigler, 1988) that the N250 potential, which is the preceding negativity to P300, is related to stimulus discrimination and evaluation (dis- crimination potential) whereas the P300 potential reflects task processing (task processing potential) and represents, therefore, a real endogenous potential. Knight et al. (1989) studied differential effects of parietal or temporo-parietal lesions on N250 and P300 in humans. They found that lesions of the mid and superior parietal cortex do not affect P300 but abolish or markedly reduce the preceding nega- tive component. Lesions in the temporo-parietal region, however, abolished P300 but did not affect N250. Thus, they confirmed that P300 and its preceding negativity, N250, have different cortical generators and reflect differ- ent states of mental processes (Taghavy and Kiigler, 1985). Additionally, as shown in this study, the two potentials are differently affected by the same pathological process (see below).
Multichannel recording and subsequent electrical brain mapping are especially suited to the investigation of the
172 A. Taghavy, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174
P300 complex because P300 is generated by widespread cortical activities (Halgren and Smith, 1987). On the other hand, they offer the possibility of peak-to-baseline mea- surements and so split the P300 complex into its compo- nents, the N250 and the P300 potential. Therefore, from the beginning, we expected a higher sensitivity from elec- trical brain mapping of P300 than from the P300 in the frame of a 1- or 2-channel setting. Multichannel recording was applied in case s of high-grade unilateral ICA stenoses in a prospective study because clinical experience and experiential reports from these patients (such as reduction in concentration and memory) gave, not infrequently, the impression of cognitive disturbances which we wanted to objectify and quantify. In this study we applied an overall test (2-way ANOVA) as profile analysis and t test compar- isons within electrical brain mapping, which are used in this type of topographical evaluation to exhibit regional differences on the scalp. The two methods constitute dif- ferent but supplementary approaches and yielded widely congruous results in this study.
As far as we know, most multicenter studies (for exam- ple the NASCET study, 1991) concerning the benefit of surgery in comparison to medical treatment of ICA stenoses are aimed at preventing a future stroke due to thromboem- bolism. Improvement of cerebral function is not explicitly pursued (Van Huffelen et al., 1993). These authors assume correctly that, when ever an improvement occurs, such a curative effect has to be explained by hemodynamic circu- latory changes. The curative effect implies lower function- ing of the brain previous to treatment, what we verified in this study, and it also implies, in addition to stroke preven- tion, an improvement in cognition after successful treat- ment (Jacobs et al., 1983).
As demonstrated in this study, cerebral functioning, which underlies mental processes, is impaired in patients with tight unilateral ICA stenoses. There were no signifi- cant differences between asymptomatic patients and TIA patients in all parameters of the P300 complex and psycho- metric testing. In comparison to controls, however, both groups do have a significant reduction of brain function. N250 and P300 behaved differently. N250 showed a sig- nificant overall lengthening of its latencies and a reduction of its amplitudes only at central sites. In contrast, the P300 potentials revealed a significant overall amplitude reduc- tion and a significant latency prolongation only in occipital leads. The patients are, therefore, impaired in the discrimi- nation of the stimuli (N250 potential) and they have a reduced capacity of information handling (P300 potential) (Taghavy and Kiigler, 1988). The psychometric test, CPT, detected also slight cognitive disorders from an obviously completely different approach. The CPT is performed un- der time pressure. Correspondingly, we found significant correlations between latencies of the P300 complex and the CPT values. The sensitivity (to distinguish correctly between patients and controls) of the parameters of the P300 complex was quite high (highest for the P300 maps:
in TIA patients 77% and in asymptomatic patients 60%). The sensitivity of the CPT was 70% in TIA patients and 50% in asymptomatic patients. This sensitivity is in the same range as Nuwer found (1988) while reviewing the literature in respect to quantitative EEG mapping in TIAs and minor strokes. Nagata et al. (1984) examined only TIA patients by applying EEG mapping and found a sensitivity of 68%. We also found this range of sensitivity in this work even for asymptomatic high-grade ICA stenoses by using electrical brain mapping of the P300 complex. In spite of the high sensitivity, this study was not done to develop a diagnostic tool. In the present state of investiga- tion, electrical brain mapping of P300 may be used as an additional parameter for the follow-up of these patients.
The changes in the P300 complex cannot be explained by a reduced sensory input due to peripheral pathologies since possible peripheral pathologies were excluded by the design of this study. Consistently, the early sensory exoge- nous potentials of the P300 curves as well as the conven- tional PVEPs showed no significant differences between patients and controls. In the literature, conventional PVEPs were found to be delayed in patients with diabetes mellitus (Puvanendran et al., 1983; Yaltkaya et al., 1988). How- ever, the great majority of their patients did have periph- eral neuropathy and increased peripheral nerve conduction time was correlated with altered PVEPs (Puvanendran et al., 1983). The diabetic patients in the present study did not have peripheral neuropathy or retinopathy. Also, hy- pertension has been implicated in the pathogenesis of acute or chronic anterior ischemic optic neuropathy (Beri et al., 1987). No patient in our study had any history indicative of these conditions. In all measured electrophysiological parameters of our study, there were no differences between patients with diabetes or hypertension and those not suffer- ing from these diseases. Furthermore, both subgroups be- haved in the same way as the total patient group in comparison with the controls. Conclusively, the alteration of P300 complex in ICA stenoses cannot possibly be due to any peripheral pathology.
All our patients were in good health but, only on questioning, several patients expressed a certain degree of forgetfulness and a reduction in concentration. Also, our psychometric findings cannot be due to the patients' hyper- tension, which was adequately treated in every case. There were no significant differences between patients with and without a history of hypertension in the CPT. This is in accordance with the literature (Farmer et al., 1987, 1990). These authors found no cognitive impairment in treated hypertension but in untreated hypertension in a longitudi- nal study. In respect to diabetes, however, a few studies (Perlmuter et al., 1984; Mooridan et al., 1988) indicate a psychometric decrease of cognition in non-insulin-depen- dent diabetic patients, although we were not able to verify this in our patient population. P300, however, was found to be normal in diabetic patients (Mooridan et al., 1988). Hypertension and diabetes contribute to generalized

A. Taghavy, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174 173
atherosclerosis and to ICA stenoses, but they are not as such primarily responsible for our findings. Generalized cerebral atherosclerosis undetected by angiography, how- ever, may contribute pav:ially to our findings but to a lesser degree than the hemodynamic insufficiency due to the ICA stenosis since Vail Huffelen et al. (1993) found in a preliminary electrophysiological study that cerebral ac- tivity improved after carotid endarterectomy.
Although we support performing a CAT scan in every patient before carotid endarterectomy, there were only 5 patients with a cranial CAT scan in this study; all were normal. We cannot exclude, however, that minor cerebral infarctions had occurred in some of the remaining patients. Norris and Zhu (1992) found cerebral infarctions in 30% of the CAT scans of patients with high-grade carotid stenoses - comparable to our patients. On the other hand, asymptomatic brain infarctions are fairly common in ap- parently normal elderly subjects (Awad et al., 1986a) so that Hougaku et al. (1992) found asymptomatic infarctions in 43% of the magnetic resonance imagings (MRIs) of 42 healthy elderly subjects. Awad et al. (1986b) compared the findings in MRIs to the findings in CAT scans in TIA patients and found a 2.4 times higher sensitivity of MRIs to detect focal abnormalities. Thus, it is not unlikely that a few of our controls would have shown also signs of infarctions in cranial CAT scans.
Most important of all, however, multichannel recording of P300 in high-grade unilateral ICA stenoses illuminates the pathophysiology of carotid artery disease. Neither in all examined electrophysiolog;ical parameters nor in the psy- chometric testing were there any significant differences between the patients considered to be asymptomatic and the patients with a TIA history. The clinical presentation of high-grade ICA stenoSes :may consist mainly of (subjec- tive) symptoms detected by the above mentioned methods or mainly of (objective) neurological signs such as TIAs observed by patients and at times also by the physician. From this point of view, the so-called asymptomatic tight carotid artery stenosis lends itself to carotid endarterec- tomy as is already the case with symptomatic (TIA) ICA stenoses. The lack of any significant differences between "asymptomatic" and TIA patients contributes to the old dispute between the embolic (Millikan et al., 1955; Cas- taigne et al., 1965) and hemodynamic theory of TIAs (Denny-Brown, 1951). It :is doubtful that there are really asymptomatic high-grade unilateral ICA stenoses in the age group studied, and this is more likely to be due to hemodynamic insufficiency than to emboli of the ICA stenoses, especially in the face of a higher metabolic demand under stimulus conditions or under task solving processes, leading to longer lasting slight cognitive disor- ders in both groups of patients. An additional point is that all patients were treated with acetylsalicylic acid which reduces the risk of emboli. This, together with the anatom- ical study of Fisher and Ojemann in 1986, constitutes a revival of the hemodynamic theory of severe ICA stenoses.
In a study of 90 carotid endarterectomy specimens, those authors found evidence that hemodynamic insufficiency may be responsible for transient symptoms. We cannot exclude from our data, however, that in either case em- bolic phenomena may be involved - more so in TIAs than in so-called asymptomatic patients. In contrast to the TIA symptomatology, the cognitive deficit may not be readily apparent and escapes the attention of the physicians.
In final analysis, high-grade unilateral carotid artery stenoses affect the brain even in asymptomatic patients. Its mechanism, however, still remains not totally clear since widely spread smaller vessel disease or intracerebral steal phenomena could be an additional cause for our findings. This would explain the involvement of the hemispheres contralateral to the ICA stenosis. For further clarification of this mechanism, the application of positron emission tomography or functional MRI may be helpful.
References
Awad, I., Spetzler, R., Hodak, J., Awad, R. and Carey, R. Incidental subcortical lesions identified on magnetic resonance imaging in the elderly, correlation with age and cerebrovascular risk factors. Stroke, 1986a, 17: 1084-1089.
Awad, I., Modic, M., Little, J., Furlan, A. and Weinstein, M. Focal parenchymal lesions in transient ischemic attacks: correlation of computed tomography and magnetic resonance imaging. Stroke, 1986b, 17: 399-403.
Beri, M., Klugman, M., Kohler, J. and Hayreh, S. Anterior ischemic optic neuropathy. VII. Incidence of bilaterality and various influencing factors. Ophthalmology, 1987, 94: 1020-1028.
Breslau, J., Starr, A., Sicotte, N., Higa, J. and Buchsbaum, M.S. Topo- graphic EEG changes with normal aging and SDAT. Electroenceph. clin. Neurophysiol., 1989, 72: 281-289.
Castaigne, P., Lhermitte, F. and Gautier, J.C. RSle des 16sions art6rielles darts les accidents isch6miques c6r6breux de l'ath6rosd6rose. Rev. Neurol., 1965, 113: 5-32.
Denny-Brown, D. The treatment of recurrent cerebrovaseular symptoms and the question of vasospasm. Med. Clin. N.Am., 1951, 35: 1457- 1475.
Donchin, E., Ritter, W. and McCallum, W. Cognitive psychophysiology: the endogenous components of the ERP. In: E. Callaway, P. Tueting and S. Koslow (Eds.), Event-Related Brain Potentials in Man. Aca- demic Press, New York, 1978: 1-79.
Editorial. Thresholds in cerebral ischemia - the ischemic penumbra. Stroke, 1981, 12: 723-725.
Erzigkeit, H. SKT Manual, Beltz Test. VEB Verlag, Weinheim, 1989. Farmer, M., White, L., Kittner, S., Kaplan, E., Moes, E., McNamara, P.,
Wolz, M., Wolf, P. and Feinleib, M. Neuropsychological test perfor- mance in Framingham: a descriptive study. Psychol. Rep., 1987, 60: 1023-1040.
Farmer, M., Kittner, S., Abbott, R., Wolz, M,, Wolf, P. and White, L. Longitudinally measured blood pressure, anithypertensive medication use and cognitive performance: the Framingham study. J. Clin. Epi- demiol., 1990, 43: 475-480.
Fisher, C.M. and Ojemann, R.G. A clinico-pathologic study of carotid endarterectomy plaques. Rev. Neurol., 1986, 142: 573-589.
Gomer, F., Spicuzza, R. and O'Donnell, P. Evoked potential correlates of visual item recognition during memory-scanning tasks. Physiol. Psy- chol., 1976, 4: 61-65.
Halgren, E. and Smith, M.E. Cognitive evoked potentials as modulatory
174 A. Taghavy, H. Hamer / Electroencephalography and clinical Neurophysiology 94 (1995) 163-174
processes in human memory formation and retrieval. Hum. Neurobiol., 1987, 6: 129-139.
Hougaku, H., Matsumoto, M., Kitagawa, K., Harada. K., Oku, N., Itoh, T., Maeda, H., Handa, N. and Kamada, T. Silent cerebral infarction as a form of hypertensive target organ damage in the brain. Hyperten- sion, 1992, 20: 816-820.
Jacobs, L.A., Ganji, S., Shirley, J.G., Morrell, R.M. and Brinkman, S.D. Cognitive improvement after extracranial reconstruction for the low flow-endangered brain. Surgery, 1983, 93: 683-687.
Kelly, M.P., David, C.G. and Javid, H. Carotid artery disease, carotid endarterectomy, and behaviour. Arch. Neurol., 1980, 37: 743-748.
Knight, R.T., Scabini, D., Woods, D.L. and Clayworth, C.C. Contribu- tions of temporal-parietal function to the human auditory P3. Brain Res., 1989, 502: 109-116.
Kiigler, C., Taghavy, A. and Platt, D. The event-related P300 potential - an analysis of cognitive human brain aging: a review. Gerontology, 1993, 39: 280-303.
McCarthy, G. and Wood, C.C. Scalp distributions of event-related poten- tials: an ambiguity associated with analysis of variance models. Electroenceph. clin. Neurophysiol., 1985, 62: 203-208.
Millikan, C.H., Siekert, R.C. and Shick, R.M. Studies in cerebro-vascular disease. V. The use of anticoagulant drugs in the treatment of intermittent insufficiency of the internal carotid arterial system. Mayo Clin. Proc., 1955, 30: 578-586.
Mooridan, A., Perryman, K., Fitten, J., Kavonian, G. and Morley, J. Cortical function in elderly non-insulin dependent diabetic patients: behavioral and electrophysiologic studies. Arch. Intern. Med., 1988, 148: 2369-2372.
Nagata, K., Yunoki, K., Araki, G. and Mizukami, M. Topographic electroencephalographic study of transient ischemic attacks. Elec- troenceph, clin. Neurophysiol., 1984, 58: 291-301.
Neville, H.J. and Lawson, D. Attention to central and peripheral visual space in a movement detection task: an event-related potential and behavioral study. I. Normal hearing adults. Brain Res., 1987, 405: 253-267.
Norris, J. and Zhu, C. Silent stroke and carotid stenosis. Stroke, 1992, 23: 483-485.
North American Symptomatic Carotid Endarterectomy Trial (NASCET) collaborators. Beneficial effect of carotid endarterectomy in symp- tomatic patients with high-grade carotid stenosis. New Engl. J. Med., 1991, 325: 445-453.
Nuwer, M.R. Quantitative EEG. II. Frequency analysis and topographic mapping in clinical settings. J. Clin. Neurophysiol., 1988, 5: 45-85.
Oblak, G., Egger, J., Freidl, F. and Stix, P. Befindlichkeit und neuropsy- chologische Leistung nach Karotis-Endarterektomien. Psycho, 1992, 18: 840-847.
Overall, J. and Schaltenbrand, R. The SKT neuropsychological test battery. J. Geriat. Psychiat. Neurol., 1992, 5: 220-227.
Parker, J.C., Smart, K.L., Granberg, B.W., Nichols, W.K. and Hewett, J.E. Neuropsychological parameters of carotid endarterectomy: a two-year prospective analysis. J. Cons. Clin. Psychol., 1986, 54: 676-681.
Perlmuter, L., Hakami, M., Hodgson-Harrington, C., Ginsberg, J., Katz, J., Singer, D. and Nathan, D. Decreased cognitive function in aging non-insulin-dependent diabetic patients. Am. J. Med., 1984, 77: 1043-1048.
Puvanendran, K., Devathasan, G. and Wong, P.K. Visual evoked re- sponses in diabetes. J. Neurol. Neurosurg. Psychiat., 1983, 46: 643- 647.
Silva, A. and Gross, P.T. Use of the EEG in the evaluation of TIAs. Electroenceph. clin. Neurophysiol., 1983, 56: 13P.
Sutton, S., Braren, M., Zubin, J. and John, E.R. Evoked potential correlates of stimulus uncertainty. Science, 1965, 150: 1187-1188.
Taghavy, A. and Hamer, H. Parenchymal "damage" in transient is- chemic attacks (TIAs) and prolonged reversible ischemic neurologic deficits (PRINDs): - the role of cranial CT and EEG. Int. J. Neurosci., 1992, 66: 251-261.
Taghavy, A. and Hamer, H. Symptomatic (TIA) and asymptomatic tight unilateral internal carotid artery (ICA) stenosis and electrical brain mapping of event related potentials (P300). Can. J. Neurol. Sci., 1993a, 20 (Suppl. 4): S140.
Taghavy, A. and Hamer, H. Hemispheric differences of visual P300 in a normal group in respect to latency, amplitude and area measure. In: M. Rother and U. Zwiener (Eds.), Quantitative EEG Analysis: Clini- cal Utility and New Methods. Universit~itsverlag, Jena, 1993b: 322- 324.
Taghavy, A. and Kiigler, C. The influence of different visual discrimina- tion tasks on the pattern flash P300 complex. Pfliigers Arch., 1985, 405 (Suppl. 2): R66.
Taghavy, A. and Kiigler, C. The pattern flash elicited P300 complex (PF-P300): a new method for studying cognitive processes of the brain. Int. J. Neurosci., 1988, 38: 179-188.
Van Huffelen, A.C., Vriens, E.M., Wieneke, G.H., Touwotten, F. and Eikelboom, B.C. Carotid endarterectomy: a three month follow-up study. Electroenceph. clin. Neurolophysiol., 1993, 87: $52-$53.
Williams, M. and McGee, T. Psychological study of carotid artery occlusion and endarterectomy. Arch. Neurol., 1964, 10: 293-297.
Wine, J. Test anxiety and direction of attention. Psychol. Bull., 1971, 76: 92-104.
Yaltkaya, K., Ballan, S. and Baysal, A.I. Visual evoked potentials in diabetes mellitus. Acta Neurol. Scand., 1988, 77: 239-241.
Copyright © 2022 FDOKUMEN




















