SYDNEY MEDICAL PROGRAM
66
SYDNEY MEDICAL PROGRAM GDMP2012 LEARNING TOPICS Stage 1 BLOCK 1: Foundation Block Copyright © 2012 Sydney Medical Program, University of Sydney Compiled by A. K. Menezes for SUMS
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of SYDNEY MEDICAL PROGRAM
SYDNEY MEDICAL PROGRAM
GDMP2012
LEARNING TOPICS
Stage 1
BLOCK 1:
Foundation Block
Copyright © 2012 Sydney Medical Program, University of Sydney
Compiled by A. K. Menezes for SUMS
2
CONTENTS • 1.06 – I’ve been here before // Normal pregnancy 3
1. Antenatal care 4 2. Bio-psycho-social aspects of pregnancy 7 3. Overview: normal pregnancy 9 4. Screening in pregnancy 11 5. Anatomy of the urinary system and female genital tract 12 6. Screening for infection in pregnancy 14 7. Implications of UTI for pregnancy 16 8. Immune responses in the urinary tract 18
• 1.07 – Is this serious // Carcinoma 20
1. Structure and function of breast 21 2. Lumps in the breast 23 3. The nature of cancer 24 4. Lymphatic system and the spread of cancer 25 5. Responses to life-threatening illness 26 6. Team approaches to management of breast cancer 28 7. Principles of screening non-communicable diseases 29
• 1.08 – A question of communication // Tuberculosis 32
1. Systemic responses to infection 33 2. Structure of the respiratory tract 35 3. Chronic inflammation 37 4. Immune response to mycobacterium 39 5. TB: the global perspective 41 6. Outbreak: surveillance & control 43 7. Health System Structure: Access for Immigrants 45 8. Health and its determinants: Ethnicity 47
• 1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 49
1. Structures of the chest 50 2. Mechanisms of pain 52 3. Pathogenesis of arterial disease 54 4. Overview of management 55 5. Treatment adherence 57 6. Hypoxia ischaemia and cell death 60 7. Coronary artery disease in Australian Aborigines and Torres Strait Islanders 61 8. Patterns of non-communicable disease: cardiac disease 64
3
1.06 – I’VE BEEN HERE BEFORE // NORMAL PREGNANCY Learning objectives Detailed anatomical organisation of the muscles of the shoulder and arm; their attachments and functions. The functions for each individual muscle and its action on the major joints, namely shoulder, elbow, acromioclavicular and sternoclavicular.
Anatomy
Processes involved in cell division and growth, with reference to key mechanisms for normal and disordered events in the cell cycle.
Physiology
Principle maternal physiological adaptations to pregnancy. Physiology Meaning of neoplasia and nomenclature of tumours, the similarities and differences between benign and malignant tumours, the mechanism of underlying neoplastic transformation and accumulation of genetic damage, the basic morphology of tumours, both in macroscopic and microscopic terms, the mechanism underlying metastasis and finally, the overall risk factors for cancer.
Pathology
Major stages of early development of the human embryo. Embryology Major defects associated with the developing embryo during pregnancy. Embryology Major issues related to women's health: puberty, menstruation, contraception, fertility and infertility, pregnancy, childbirth, postpartum, menopause and old age.
Obstetrics, Gynaecology and Neonatology
Major issues related to men's health, from obesity to cardiac problems and from prostate cancer to sexual dysfunction.
Obstetrics, Gynaecology and Neonatology
Major issues related to child and adolescent health. Paediatrics Major issues related to child and adolescent health. Paediatrics Differentiation between investigating the presence of the pathogen and host responses to the pathogen, the differences between bacteria and viruses in relation to the lab techniques used for their cultivation and identification, the impact of characteristics of viruses in pathogenesis of infection, management and diagnostic procedures, practical methods used to identify pathogenic viruses and to assess their susceptibility to antivirals, and finally, the role of rapid point-of-care and molecular diagnostics in the management of infections.
Infectious Diseases
To introduce students to the measurement of height, body weight and waist circumference and calculation of Body Mass Index. Clinical usefulness and relevance of BMI. Consideration of other measures such as waist size and hip to waist ration in the estimation of obesity. Implications of ethnicity, age and body morphology on obesity score.
Medicine
At the end of this session, students should be able to: • Name the three levels of prevention • Define the three levels of prevention • Give examples of prevention strategies • State where in the life cycle of a disease secondary prevention strategies should be
implemented • Define screening • Describe a framework for critically appraising articles on screening interventions
Medicine, Public Health
An overview of HIV and health. Immunology, Public Health
1.06 – I’ve been here before // Normal pregnancy 4
1. Antenatal care Background The aim of antenatal care is to provide optimal outcomes for the mother and baby. Antenatal care should identify factors that place women and their babies at risk of adverse outcomes. Some factors may be present prior to pregnancy or recognised for the first time in pregnancy. Of the latter some may be specific to pregnancy. An important aspect of antenatal care is the first visit at which a full medical, obstetric and psychosocial history is obtained. Medical disorders may impact on the pregnancy or the pregnancy may impact on the medical disorder. Many pregnancy complications (e.g. growth restriction, preterm birth, placental abruption, pre-eclampsia) have a risk of recurrence. It is important to ascertain as much detail as possible about previous pregnancy complications. Psychosocial history may reveal a history of depression, personality traits or behaviours that may place a newborn child at potential risk. The physical examination at this visit is important to identify any co-existent medical disorders such as hypertension, thyroid or cardiac disease. A series of investigations are performed in normal pregnancy: these are summarised below. Some of these are optional and require careful discussion with the prospective parents.
The first visit is performed often in conjunction with a medical officer. A woman's risk is assigned and subsequent care planned. For the majority of women who are low risk their future antenatal care may not involve medical personnel. Midwives increasingly provide antenatal care to this group. Women at risk because of medical disorders, such as hypertension or diabetes, or a previous poor pregnancy outcome, most commonly have specialist led antenatal care. Continuity of care, where possible, is a desirable component of pregnancy care.
Investigation Reason
Blood Group Antigen Screen Rhesus negative women are at risk of alloimmunisation/ possible sensitisation
FBC Screen for anaemia/thalassaemia
Rubella Rubella causes congenital anomalies
Hepatitis B Baby at risk of infection in newborn period
HIV Measures can be taken to reduce risk of congenital infection
VDRL Treatment in pregnancy reduces risk of congenital infection
MSU Asymptomatic bacteriuria is associated with preterm delivery and development of pyelonephritis.
Screening for Down syndrome This may be via an ultrasound assessment at 12-14 weeks or a blood test. This is optional and its uptake will depend on the parents' view about giving birth to a child with Down Syndrome.
Ultrasound at 18-20 weeks To assess fetal anatomy and placental position
Glucose tolerance testing Screening for glucose intolerance in pregnancy is advocated by some and is common but not universal practice. A 50 g glucose load is administered and if abnormal (≥ 7.8 mmol) a formal GTT is performed. Hyperglycaemia in the mother is associated with large birthweight babies (macrosomia). Appropriate dietary intervention reduces blood sugar levels in most women. Insulin is used in those women who remain hyperglycaemic.
Vaginal swab for Group B streptococci
Screening for GBS in pregnancy is another common but not universal practice. Approximately 10% of women carry GBS in the vagina. Of these women 1% may have a baby that will face life-threatening sepsis from infection transmitted as the baby descends through the birth canal. Intravenous penicillin is effective at reducing the transmission risk. Some advocate giving antibiotics only to high-risk women (those in preterm labour or with prolonged ruptured membranes).
1.06 – I’ve been here before // Normal pregnancy 5
In the absence of pregnancy complications the frequency of visits has generally been every four weeks up until 28 weeks, every 2 weeks up until 36 weeks, then weekly visits until delivery. At each visit the blood pressure is checked and fundal height assessed. Weight and urinalysis are no longer routinely performed at each visit. It should be remembered that proteinuria might be a sign of the pregnancy-specific disorder pre-eclampsia. Urinary tract infection in pregnancy Women are at risk of urinary tract infection in pregnancy due to stasis and dilatation of the renal collecting system. This is caused both by a mechanical obstruction to the ureters and also by a direct dilatation mediated through the action of progesterone. The dilatation is often more marked on the right. Asymptomatic bacteriuria is the presence of bacteria in the urine without clinical signs or symptoms of infection. It usually is found on random urine screening in pregnancy. Asymptomatic bacteriuria is screened for in pregnancy since it is present in up to 5% of pregnancies. If untreated, asymptomatic bacteruria can develop into acute cystitis (40%) and pyelonephritis (25%) in pregnancy. In addition, the relative risk of preterm birth is doubled in a woman with bacteriuria. Asymptomatic bacteriuria is best screened for by performing a urine culture. Urinalysis with a dip stick has a high specificity but a low sensitivity for bacteriuria. Antibiotic treatment for women with asymptomatic bacteruria is effective in reducing cystitis, pyelonephritis and preterm labour. Urinary tract infection (cystitis) presents with symptoms of dysuria, urgency, incontinence, and frequency. The diagnosis is suspected when a urine dipstick shows leukocytes, nitrite, hematuria, or protein and is confirmed by a positive urine culture. Pyelonephritis is characterised by the presence of fever, loin pain and tenderness. Nausea, vomiting, urinary frequency, urgency, and dysuria may also be present. If a woman presents with symptoms and signs of pyelonephritis in pregnancy, a urine sample should be obtained and intravenous antibiotics commenced. When the organism responsible is identified its sensitivity to the chosen antibiotic should be confirmed. Patients with recurrent UTIs or pyelonephritis should be maintained on prophylactic antibiotics throughout pregnancy. Antenatal care Pregnant women prefer continuity of care in the antenatal, intrapartum and postnatal periods. This may be offered either by specialists, general practitioners or midwives. In Australia private obstetric care has been shown to be associated with increased birth interventions. This may be due to these practitioners offering more intervention. Alternatively consumers may choose this type of care because they feel that they have more input into decisions regarding birth or because of a difficult past obstetric history, intervention is indicated. The schedule of antenatal visits that sees women reviewed monthly to 28 weeks, fortnightly to 36 weeks and weekly thereafter has not been shown to be associated with improved outcomes compared with less frequent antenatal visits.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Villar J, Carroli G, Khan-Neelofur D, Piaggio G, Gulmezoglu M. Patterns of routine antenatal care for low-
risk pregnancy. Cochrane Database of Systematic Reviews, 2004, 2. • Waldenstrom U, Nilsson CA. No effect of birth centre care on either duration or experience of breast
feeding, but more complications: findings from a randomised controlled trial. Midwifery 1994 Mar;10(1):8-17
• Roberts CL, Tracy S, Peat B. Rates for obstetric intervention among private and public patients in Australia: population based descriptive study. BMJ 2000; 321(7254):137-41
• Carroli G, Villar J, Piaggio G, Khan-Neelofur D, Gulmezoglu M, Mugford M, Lumbiganon P, Farnot U, Bersgjo P; WHO Antenatal Care Trial Research Group. WHO systematic review of randomised controlled trials of routine antenatal care. Lancet 2001; 357(9268):1565-70
• Antenatal care: Routine care for the healthy pregnant woman – National Institute for Health and Clinical Excellence
• Villar J, Carroli G, Khan-Neelofur D, Piaggio G, Gulmezoglu M. Patterns of routine antenatal care for low-risk pregnancy. Cochrane Database of Systematic Reviews, 2004, 2.
1.06 – I’ve been here before // Normal pregnancy 6
• Waldenstrom U, Nilsson CA. No effect of birth centre care on either duration or experience of breast feeding, but more complications: findings from a randomised controlled trial. Midwifery 1994 Mar;10(1):8-17
• Roberts CL, Tracy S, Peat B. Rates for obstetric intervention among private and public patients in Australia: population based descriptive study. BMJ 2000; 321(7254):137-41
• Carroli G, Villar J, Piaggio G, Khan-Neelofur D, Gulmezoglu M, Mugford M, Lumbiganon P, Farnot U, Bersgjo P; WHO Antenatal Care Trial Research Group. WHO systematic review of randomised controlled trials of routine antenatal care. Lancet 2001; 357(9268):1565-70
• Antenatal care: Routine care for the healthy pregnant woman – National Institute for Health and Clinical Excellence
Author: Dr Kirsten Black, Obstetrics and Gynaecology
1.06 – I’ve been here before // Normal pregnancy 7
2. Bio-psycho-social aspects of pregnancy Pregnancy and the postpartum period are times of change. There are changes in physical symptoms, body image, moods, feelings, concerns and sexuality. These interact with the hormonal changes of pregnancy. Every woman is different and each pregnancy is different. The common early symptoms of pregnancy which can occur are; an increase in the size and tenderness of the breasts, nausea (not necessarily in the morning) and for some women vomiting, urinary frequency, constipation, backache, dizziness and fatigue. For most women nausea and vomiting occurs during the first 12 to 14 weeks of pregnancy but some women report vomiting for longer periods of time. Hyperemesis gravidaruum is the term used to describe women who require treatment in hospital for their vomiting. This occurs in 0.1% of pregnant women and may have psychosocial aspects to the presentation. The variables that have most effect on women during pregnancy and are predictive of a good outcome and less problems with somatic and psychological symptoms are; whether the pregnancy was wanted (even if not planned), if the mother feels she has good support available during and after her pregnancy, if she has good antenatal care, if her mental health before her pregnancy is good (including no drug or alcohol abuse) and if she is not of lower socioeconomic status. The common later symptoms of pregnancy that can occur are; urinary frequency, incontinence, weight gain, binge eating, pica, edema, sweating, breathlessness, heartburn, hemorrhoids and varicose veins, muscle spasm and back pain. Most of these can be explained by the size and position of the baby in relation to the maternal organs. Women report feeling relaxed, passive and tired. This hormonal effect is protective for growth and development and allows weight gain. Good antenatal care provides the opportunity for women to ask questions about their pregnancy and childbirth, provides education about women's health, assesses the women's mood throughout pregnancy, gives the woman choices about the events of pregnancy, such as, the choice to use analgesia and the types of pain relief available during childbirth. The choices must be given impartially so women are not made to feel guilty if they are unable to fit in with the prevailing fashions, for example, epidural anesthesia. Women have fears and worries during their pregnancy. The most common are; 'will I lose my baby?' will my baby be normal?' 'Is my baby still alive?' 'Will I/we be able to cope with a baby?' 'Will I be a good enough mother?' 'Have I done anything to hurt my baby?' 'Will sex hurt my baby?' ' Will I lose the weight gained after my pregnancy? Pregnancy is a challenge to the body image of many women, not only those with eating disorders before pregnancy. The increase in blood volume, fluid retention, fat deposition on the thighs and breasts and increase in the size of the organs associated with pregnancy all contribute to this challenge. A good physical outcome of pregnancy is the birth of a healthy baby of normal weight for sex, and gestational age and a healthy mother. Intrauterine growth retardation is associated with; low maternal pre-pregnancy weight, failure to gain adequate weight during pregnancy, smoking cigarettes and in many studies; excess coffee, alcohol and drug abuse, excessive exercise and vomiting. Maternal obesity may be associated with birth of either large or growth retarded babies. Although the hormones of pregnancy can affect mood and behaviour psychosocial factors frequently predominate. Interest and responsiveness in sex during pregnancy will depend on cultural beliefs, the acceptance of using different positions during sexual intercourse, concerns about contractions (Braxton Hicks) during arousal, fear of hurting the baby during sexual intercourse and orgasm, attitude of partner to pregnant women and the couples prepregnancy attitudes and feeling about sex. The additional factors that effect mood and sexuality following pregnancy can depend on the events at childbirth, fatigue and breastfeeding. Recovery from childbirth may take many months. Three months after the vaginal birth of their first child 20% of women still feel general discomfort in the vulvovaginal area and 50% still have some discomfort during sexual intercourse. The recovery time is longer if sutures are required, forceps are needed and other more extensive vaginal trauma occurs. Parents 'at risk' of a poor outcome following childbirth are those who have poor coping skills, have a poor relationship with each other, who had parents who were poor role models, who have unrealistic expectations of parenthood, who have a baby who is in poor health or 'failing to thrive' and who lose their baby. The risk factors for postnatal depression are poor perceived supports during and after pregnancy, prior history of depression or other psychological problem, such as an eating disorder. Postpartum depression may be a misnomer as at least one third of women are already depressed during pregnancy and others do not develop symptoms until a year later.
1.06 – I’ve been here before // Normal pregnancy 8
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Abraham and Oats ‘Llewelyn-Jones Fundamentals of Obstetrics and Gynaecology’, 9th edition, Elsevier
Mosby 2010
Author: Associate Professor Suzanne Abraham, Obstetrics and Gynaecology
1.06 – I’ve been here before // Normal pregnancy 9
3. Overview: normal pregnancy Pregnancy is characterised by multiple changes in anatomy, physiology, biochemistry and psychology. The effects of these changes are to: • Protect the fetus in an optimal environment • Protect the mother from the risks posed by the pregnancy and delivery • Prepare the mother for the delivery process and • Prepare the mother for breast-feeding Points to note are: • Preparation precedes demands • Changes exceed the fetal needs • Nearly all changes are completely reversible • Nutritional and blood reserves accumulate at a rate that matches the fetal size Most changes are hormone related. Major hormones from varying sites: • Placenta - human chorionic gonadotropin, human placental lactogen, progesterone • Feto-placental unit: oestrogens • Endometrium - prolactin, renin • Mother - cortisol, angiotensin/aldosterone Human chorionic gonadotropin has 2 subunits (a and à Ÿ) that combine to form an active hormone. Detection of the beta-subunit is the basis of the modern pregnancy test. The action of this hormone is ovarian support, sexual differentiation of the male fetus, regulation of the fetal adrenal cortex and possibly thyroid stimulation in the mother. Human placental lactogen alters maternal metabolism to ensure a glucose supply to the fetus. Progesterone relaxes smooth muscle (in part to allow for uterine enlargement, but also to cause increased blood flow to the peripheral circulation), causes alteration in the metabolism of the mother by diminishing carbon dioxide production and antagonising insulin, aids breast development for breast-feeding, and alters the mothers' ability to concentrate and recall facts. The maternal response to the hormones of pregnancy leads to an increase in maternal weight. This arises from increased fat deposits, increased breast and uterine size, fetal and placental mass, and fluid retention, which is both intravascular and extravascular. The average weight gain in pregnancy is about 12.5 kg. To cope with the vasodilation associated with progesterone, cardiac output increases and an increase in intravascular volume occurs. Peripheral resistance is reduced. Blood volume may increase by up to 50% at term. There is also an increase in red cell mass by about 33%. There is an increase in the depth of breathing by the mother due to a rise in the basal metabolic rate and the progesterone effect on the maternal brain stem. This results in a fall in her carbon dioxide levels and a small rise in her oxygen levels. These are to the benefit of the baby. Renal function in terms of creatinine clearance increases by 40% due to increased renal blood flow and liver function also increases in terms of enzyme activity allowing for detoxification of drugs etc.. There are complex changes in the immune system. A diminution of cell-mediated immunity is noted with a rise in humoral immunity. In part this helps in ensuring the pregnancy is not rejected; placental antigens are much less immunogenic than fetal organs. Maternal appetite is usually increased to meet increased nutritional demands. The gut increases in efficiency in nutritional absorption, but there is a decrease in motility due to the rise in progesterone. Constipation often occurs.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue

1.06 – I’ve been here before // Normal pregnancy 10
• Rohen JW, Yokochi C. Colour Atlas of Anatomy. New York: Igaju-Shoin, 1988;326-333. • Fisher C. Normal Pregnancy. In: Wreen BG and Lobo RA, ed. Handbook of Obstetrics and Gynaecology.
Australia: Cassell, 3rd Edition, 1989; 46-68. • Hytten, Chambolain, eds. Clinical Physiology. (4th ed.) Oxford: Blackwell Scientific, 1991; 53-79. • Leif Skamris Matthiesen. Immune Changes in Pregnancy.
http://www.bibl.liu.se/liupubl/disp/disp98/med563s.htm
Author: Clinical Associate Professor Max Mongelli, Obstetrics and Gynaecology Author: Dr Henry Murray, Obstetrics and Gynaecology

1.06 – I’ve been here before // Normal pregnancy 11
4. Screening in pregnancy Screening tests serve to detect a disease or condition in early stages of pregnancy, before it may generate major problems. In the first instance, a medical, family and social history should be taken. Subsequently, the following major tests should be undertaken. Weight and height. This should be checked in the early stages. Assessing baby growth. This is done during routine antenatal checks. A tape measure is used to measure from the top of the growing uterus (womb) to the pubic bone. Blood pressure. This is measured regularly during routine antenatal checks. Examination of baby position. At ~36 wks, abdomen will be examined to feel if the baby is lying breech (bottom down). If so, treatment to turn the baby to a head down position may be considered. Urine tests. Urine is examined at antenatal checks using a simple dipstick test to detect: Protein (protein in urine may indicate early pre-eclampsia) and Bacteria (during pregnancy an asymptomatic infection of the urine may develop, which may increase the risk of problems in childbirth). Blood tests. To check for the following: • Anaemia: Most commonly, lack of iron. • Blood group: including rhesus D status and red cell antibodies. If mother is rhesus D negative and baby is
rhesus positive then mother may form D antibodies in her bloodstream. These not dangerous in first pregnancy, but may attack blood cells of baby that is rhesus D positive in any future pregnancy. To prevent this mother will be offered anti-D injections later in pregnancy.
• Rubella status. Checks for antibodies to rubella virus (German measles). • Infections. Including: HIV - One may be infected with HIV for years before it shows symptoms. The risk of
passing this virus on to baby may be reduced with treatment during pregnancy and delivery by caesarean section. Hepatitis B - Many people carry this virus, but have no symptoms. In some may case cause liver damage. Syphilis - This is an uncommon sexually transmitted infection. Again, mother may be infected without realising and pass it on to baby. A repeat blood test at ~28 weeks is usually offered, for example to re-check for anaemia.
Routine ultrasound scans. Usually offered at: 10-13weeks to date baby and expected time of birth, also checks for twins: 18-20 weeks to examine for physical abnormalities of baby. Screening for Down syndrome. They include a blood test and a special ultrasound test, or both. Screening for Down syndrome is offered between 11-20 weeks, depending on the type of test used. Note that the screening test is not a clear-cut diagnostic test. Screening for placenta previa (placenta is covering opening from uterus to cervix). If an earlier ultrasound indicates that mother may have a placenta previa, a repeat scan at 36 weeks may be advised to clarify the position of placenta before delivery.
References Use the textbooks in your Tutorial Room
Author: Dr Kirsten Black, Obstetrics and Gynaecology
1.06 – I’ve been here before // Normal pregnancy 12
5. Anatomy of the urinary system and female genital tract The URINARY TRACT is important in the excretion and elimination of waste. It comprises kidneys, ureters, bladder and urethra. The upper urinary tract (kidneys, ureters) is paired while the lower urinary tract (bladder, urethra) is unpaired. The kidneys filter blood, maintain water and electrolyte balance and excrete nitrogenous wastes. The ureters conduct urine to the bladder by peristalsis and the bladder stores urine and expels it through the urethra. The kidneys are reddish-brown, bean-shaped organs lying on the posterior wall of the upper abdominal cavity. They lie behind the gastrointestinal viscera and behind the peritoneum. Each kidney is surrounded by a capsule, fat and fascia. The medial border of kidney presents a vertical slit, the hilum, which transmits the renal vein, artery and renal pelvis from before backwards. The ureter is a 25 cm long, thick-walled muscular tube. It descends almost vertically in the abdominal cavity and enters the bladder wall at an angle. The obliquity of their passage helps to prevent reflux into the ureter as the bladder fills. The bladder is a highly distensible muscular sac situated in the pelvis in the empty state, but rising into the abdominal cavity as it fills. It rests on the pubic bones and adjacent pelvic floor muscles. The bladder lies anterior to the rectum in the male, and anterior to the uterus and vagina in the female. The male urethra is 20 cm long and comprises 4 parts: preprostatic (1cm), prostatic (3cm), membranous (1cm) and penile or spongy (15cm), which reflects the passage of the urethra through the internal urethral sphincter, the prostate, perineal membrane, and corpus spongiosum of the penis respectively. The urethra opens externally on the glans penis. The male urethra also forms part of the reproductive system; sperm and seminal fluid enter the prostatic part of the urethra. The female urethra is only 4 cm long. It extends down and forward from the neck of the bladder, through the perineum, to open anterior to the vagina between the labia minora. The urethra is fused with the anterior wall of the vagina. The short length of the urethra and the location of its external opening makes the female more prone to lower urinary tract infections. The urethra is surrounded by an internal urethral sphincter (involuntary control) at the bladder neck and an external urethral sphincter (voluntary control) above the perineal membrane. The FEMALE GENITALIA can be divided into internal and external parts, which are located in the pelvic cavity and perineum respectively. The internal genitalia comprise the ovaries, uterine tubes, uterus and vagina. The external genitalia are collectively called the vulva or pudendum and comprise the mons pubis, labia majora and minora, vestibule of the vagina, erectile tissue and greater vestibular gland. Note that the upper vagina is in the pelvic cavity and the lower vagina is in the perineum. The birth canal comprises the cervix and vagina. The adult, non-pregnant uterus is a pear-shaped structure (7.5 x 5 x 2.5 cm) comprising a fibromuscular cervix, a body and fundus. During pregnancy the fundus and body undergo great expansion, and the fundus comes to lie in contact with the anterior abdominal wall; the small and large intestines are displaced upward, outward and backwards. The upper third of the cervix (isthmus of cervix) is gradually taken up into the uterus in the second month of pregnancy to form the 'lower uterine segment'. The layers of the uterus include the endometrium (lining which undergoes cyclical change), myometrium (muscle) and perimetrium (serosa). Uterine (fallopian) tubes (10 cm long) extend laterally from the junction of the body and fundus of the uterus. The uterine tube comprises, from medial to lateral, an intramural part, isthmus, ampulla and infundibulum. Fertilisation normally takes place in the ampulla. Fimbriae are the finger-like extensions at the distal end of the infundibulum, one of which normally attaches to the ovary (ovarian fimbria). The ovary (3 x 1.5 x 1cm) is initially smooth and pink, later becoming grey and puckered from successive ovulations. It is attached to the uterus by the ovarian ligament. The peritoneum, a serous membrane, drapes like a sheet over the uterine tubes and uterus. Lateral to the uterus and below the uterine tube the peritoneum forms a double-layered sheet called the broad ligament. The ovaries are attached to the posterior surface of the broad ligament. The vagina (8 x 4 cm) lies posterior to the bladder and urethra, and anterior to the rectum. It is directed down and forward. The cervix projects through its upper anterior wall creating the fornices. Below this level the anterior and posterior walls of the vagina are in contact. The opening of the vagina is between the labia minora. The urethral opening is anterior, and the anal canal posterior. Lateral to the lower walls of the vagina are erectile

1.06 – I’ve been here before // Normal pregnancy 13
tissue covered by muscle. During childbirth the pelvic floor may be torn and weakened and perineal structures, like the anal sphincters, may be damaged. In the female there is a pathway of communication from the peritoneal cavity to the exterior of the body by way of the uterine tube, uterus and vagina, presenting a potential route of infection into the peritoneal cavity (peritonitis). Note that there is no communication between the peritoneal cavity and the exterior in the male.
References Use the textbooks in your Tutorial Room Optional references Online: • Prosections, Models, CDROMs
o Anatomy glossary - http://www.anatomy.usyd.edu.au/glossary o Online Wilson Museum of Anatomy - http://www.anatomy.usyd.edu.au/wilson_henle/ see Bottles
320, 67, 629, 269 (kidneys and ureter); 320 medial (bladder, urethra) o Prosections, skeleton, computer-based resources available in J. T. Wilson Museum of Anatomy
room W401, Anderson Stuart Bldg, open 8.30 am - 5.30pm o Model of the trunk - Medical library o Interactive Atlas of Anatomy (Netter) CDROM - Wilson Museum or Medical Library (611.00222
32) Netter plates 350 A,B, 351, 370 AB (kidneys), 346A, 347A (bladder, urethra).
Author: Professor John Mitrofanis, Anatomy and Histology
1.06 – I’ve been here before // Normal pregnancy 14
6. Screening for infection in pregnancy Several infections which are asymptomatic or nonspecific in the mother can cause devastating effects on the fetus or infant and/or long-term sequelae for the mother. Routine antenatal screening for infection or for susceptibility to infection in the mother potentially allows preventative intervention. Whether screening is cost-effective depends on many factors: • Prevalence/incidence of infection - this varies in different populations (risk factors include ethnicity, life-
style, sexual activity and socioeconomic status) and geographic areas • Incidence and severity of potential fetal damage or sequelae (in infant or mother) - depends on gestation at
which maternal infection occurs and/or stage or nature of maternal infection; these may be difficult to determine and fetal risk unpredictable
• Likelihood of transmission of infection to fetus or infant • Whether there is a suitable screening test (and confirmatory test if required) available; criteria for suitability
include: o Sensitivity, specificity and predictive values of test o Ability of test to distinguish current/recent or primary infection from past, chronic, or reactivated
infection o Type of specimen required and practicalities of routine collection, transport and storage (serum vs.
genital swab) - dependence of test result on specimen quality o Cost of screening test and confirmatory test (if applicable)
• Whether intervention is possible and safe, effective, acceptable and inexpensive; possible interventions include:
o Antibiotic therapy o Immunisation o Termination of pregnancy o Modification of obstetric management (method of delivery; breast feeding)
It is important that the aim of screening is understood - eg whether it is to detect active current infection or susceptibility to infection - and what action is required when "cases" are detected. Recommendations vary in different circumstances and over time; they should be reviewed regularly Infections for which routine screening is currently advocated • Syphilis - screening for active infection: infection is uncommon but, if present, can cause serious effects on
fetus and long-term sequelae in infant; sensitive, inexpensive screening and confirmatory tests and safe effective antibiotic therapy are available
• Rubella - screening for maternal susceptibility; rubella still occurs occasionally during pregnancy, despite good childhood immunisation rates; severe predictable effects on fetus from first trimester infection; effective immunisation available (given postpartum to susceptible women - see Case 1.07)
• Hepatitis B antigen - screening for chronic carriage - carriage not uncommon (<0.1->1%, depending on ethnic origin and other factors); sensitive, specific, inexpensive tests available; predictable high incidence of transmission to infant with serious long-term sequelae; effective immunisation available (given to infant at birth)
• Screening for hepatitis C antibody should be offered during pregnancy and actively encouraged for women in high risk groups e.g. those with a history of IV drug use. The risk of transmission to the fetus/infant is low, even in the presence of active infection
• Human immunodeficiency virus - it there is still no definite recommendation for routine HIV antibody screening, in Australia; it is recommended that it should be "offered", but issues such as informed consent, counselling and funding have not been addressed. This is currently (December 2006) under review. The incidence of HIV infection in women is very low in Australia and those in recognised risk groups have usually been detected before pregnancy. Nevertheless, the consequences of unrecognised maternal and neonatal HIV infection are serious and it has been established that antiretroviral therapy during pregnancy can prevent vertical transmission of HIV infection in a high proportion of cases.
• Varicella - maternal varicella during pregnancy can cause non-specific adverse effects on pregnancy outcome, intrauterine infection with developmental abnormalities or serious neonatal infection. It is recommended that women who have no history of chicken pox be screened during pregnancy and, if susceptible, offered vaccination during the postpartum period.
Vertically transmissible infections for which routine screening is currently not advocated because of inadequacies of available tests, low prevalence of infection and/or lack of suitable intervention • Genital chlamydial infection - this is currently under review because of the availability of relatively
inexpensive and sensitive screening tests. Currently screening is largely confined to women in high risk groups for sexually transmissible infections.

1.06 – I’ve been here before // Normal pregnancy 15
• Toxoplasmosis • CMV infection
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library; see Library Catalogue • Royal Australian & New Zealand College of Obstetricians & Gynaecologists. Antenatal Screening Tests
(2006). • Kirkham C, Harris S, Grzybowski S. Evidence-based prenatal care: part II. Third-trimester care and
prevention of infectious diseases. American Family Physician 2005, 71(8):1555. • Giles ML, Hellard ME, Lewin SR, Mijch AM. The evidence for a change in antenatal HIV screening policy
in Australia. Med J Aust 2006; 185(4):217-220 • Gilbert, G.L., Infections in Pregnant Women. MJA 2002 176(5):229-236 • Sackett DL, Haynes RB, Guyatt GH, Tugwell P, eds. Early Diagnosis. In: Clinical Epidemiology: A Basic
Science for Clinical Medicine. Boston: Little Brown Co, 1991; 153-170. • Gilbert GL. Routine antenatal screening and prenatal diagnosis of vertically transmissible infection.
Bailliere's Clinical Obstetrics and Gynaecology 1993; 7(1): 1-23.
Author: Clinical Professor Gwendolyn Gilbert, Institute of Clinical Pathology and Medical Research
1.06 – I’ve been here before // Normal pregnancy 16
7. Implications of UTI for pregnancy There is no significant increase in the incidence of asymptomatic bacteriuria (AB) during pregnancy. Incidence 3-6%; risk factors include - increased age and parity, sexual activity, anaemia (incl. sickle cell trait), previous UTIs or urinary tract abnormalities, low socioeconomic status, diabetes. Significance of AB and UTI during pregnancy • AB in pregnancy women is associated with increased risk of acute UTI (occurs in up to one third of
pregnant women with AB compared with 1% of those without AB). Reasons for increased risk of UTI during pregnancy include:
o Physiological dilatation of ureters and reduced bladder tone (throughout pregnancy; due to oestrogen effects)
o Obstruction of ureters by pressure from uterus at pelvic brim (later in pregnancy) • Potentially serious maternal effects of UTI:
o Increased risk of spread to upper urinary tract and septicaemia o Maternal fever, endotoxaemia/septic shock, adult respiratory distress syndrome (ARDS); o Onset of premature labour due to production of inflammatory mediators and arachidonic acid
metabolites (especially prostaglandins, which stimulate uterine contractions) o Initiation or exacerbation of renal damage o Increased risk of hypertension and anaemia
• Potentially serious fetal effects of maternal UTI: o Prematurity o Low birth weight o Sepsis
• Possible independent risk of prematurity and low birth weight associated with AB per se (?both independently related to underlying renal disease).
Acute UTI requires urgent investigation, effective therapy and follow-up Routine antenatal screening for AB and treatment of those affected can prevent development of acute UTI - ? Also reduces incidence of prematurity and low birth weight not associated with UTI. Controversies related to routine screening. • Should screening (by examination of urine) be universal or confined to women with risk factors for UTI
(mainly past history), i.e. initial screening by history? What screening method for urine examination should be used? Dipstick method for detection of (some or all of) protein, nitrates, blood and leucocyte esterase; or routine microscopy and culture - there are conflicting data re sensitivity, specificity and cost-effectiveness of each • Practicalities of ensuring recognition and follow-up of abnormal results - confirmatory testing and therapy • Management of AB and UTI - antibiotic use during pregnancy; choice, dose and duration of antibiotic
therapy (AB vs. UTI; pregnant vs. non-pregnant); follow-up tests of cure; long-term prophylaxis; follow-up investigation of renal tract (types, indications and timing)
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library; see Library Catalogue • Several recent papers and reviews outline problems associated with evaluation of the significance of AB
and UTI in pregnancy and some of the issues related to antenatal screening for AB. o Devillé, Walter LJM., Yzermans JC, van Duijn NP et al. The urine dipstick test useful to rule out
infections. A meta-analysis of the accuracy. BMC Urology 2004, 4:4. o Mittal P, Wing DA. Urinary Tract Infections in Pregnancy. Clin Perinatol 2005; 32(3): 749-764. o Romero R, Chaiworapongsa T, Espinoza J, Kalache K. Infection and prematurity and the role of
preventive strategies. Semin Neonatol 2002, 7(4): 259-274. o Rouse DJ, Andrews WM, Goldenberg RL, Owen. Screening and treatment of asymptomatic
bacteriuria of pregnancy to prevent pyelonephritis: a cost-effectiveness and cost-benefit analysis. Obstetrics and Gynaecology 1995; 86(1): 119-123.
o Schieve LA, Handler A, Hershow, Persky V, Davis F. Urinary tract infection during pregnancy: its association with maternal morbidity and perinatal outcome. American Journal of Public Health 1994; 84(3): 405-410.

1.06 – I’ve been here before // Normal pregnancy 17
o Smaill F. Antibiotics for asymptomatic bacteriuria in pregnancy. The Cochrane Database of Systematic Reviews. [update of Cochrane Database Syst Rev. 2000;(2):CD000490; PMID: 10796206].The Cochrane Library, Copyright 2006, The Cochrane Collaboration Volume (4), 2006.
Author: Associate Professor Philip Siddall, Pain Management and Research Institute
1.06 – I’ve been here before // Normal pregnancy 18
8. Immune responses in the urinary tract Innate defense mechanisms [pH of the urinary tract, its chemical content and periodic flushing] render the urinary tract relatively resistant to pathogenic bacterial infections. Should these occur and 'ascend' from urethra to bladder and kidney, the host may respond by initiating a humoral immune response with the formation of antibodies in the circulation [IgM and IgG] and urine [IgA]. The antibodies bind to the pathogen [antigen-antibody interaction]. Urinary tract infections are mainly caused by Escherichia coli and generate only a weak antibody response in the host. While UTIs perse are not life threatening, they can be complicated by septicaeima which is potentially fatal, especially in pregnancy and they are common complaints which recur frequently in some individuals and which can cause kidney damage if untreated. All these factors indicate that development of protective vaccination procedures would be beneficial. Experiments in a mouse model of UTI infection showed that immunisation with a protein essential for the binding of E. coli to host cells elicited IgG antibodies which leaked into the mucosal lining of the urinary tract, preventing the organisms binding onto target cells and providing long-term protection against infection, (Service 1997). Phase II clinical trials of vaginal vaccination have reported success in limiting recurrent UTI infections (Uehling et al. 2003). Effector Function of Antibodies Antibodies do not directly damage antigens. The binding of antigen-antibody in combination leads to a variety of biological events, which ultimately lead to the removal of the pathogen [antigen]. Antibodies alone may physically block receptor-ligand interactions such as those required for toxins and viruses to enter cells i.e. neutralize bacterial exotoxins and so limit the pathological activities of the toxins, or block virus infection. Tetanus anti-toxin, the IgA produced in the gut by the oral polio vaccine and the experimental protective vaccine described above are good examples of this. Removal of systemic antigen, however, requires the involvement of other cells and molecules of the immune system. Antibodies are recognition molecules that specifically bind to a target and 'mark' it for disposal by non-specific [innate] mechanisms such as complement and phagocytosis. The constant or Fc parts of antibody molecules determine this involvement in secondary interactions leading to the removal and destruction of the antigen. Phagocytic cells [e.g. macrophages, polymorphonuclear neutrophils] possess receptors for immunoglobulin Fc. These receptors bind with high affinity only to antibodies complexed to antigen. Pathogens coated with specific antibodies bind to Fc receptors and the efficiency of phagocytic processes is greatly enhanced (a process called opsonisation. Once inside the cell the phagosome binds to the lysosome that contains microbicidal components such as oxygen free radicals, various toxic proteins and digestive enzymes. Within the phagolysosome pathogens are killed and digested. Antibody-coated microorganisms also activate the complement cascade. The pathogen coated with antibody and activated complement components can then be killed via enhanced phagocytosis (another type of opsonisation) or by direct complement-mediated lysis. [More details of the complement cascade are given below and are illustrated in the BCS theme session] What is complement? The complement system comprises about 20 proteins present in the plasma. Activation is sequential, with each component splitting into a larger enzymic fragment (responsible for activating the next protein in the sequence) and a smaller fragment (with other biological activity). The sequential activation of complement components forms a cascade, with amplification (increasing numbers of activated molecules) at each step. Activation can be initiated via three pathways: 1. The alternative pathway - this is a more "primitive" activation-mechanism which is not dependent on
antibodies. It occurs in solution or on the surface of bacteria, triggered by chemical components of bacterial cell walls [e.g. peptidoglycans on gram positive, and lipopolysaccharide on gram negative, bacteria]. Initiation involves factors B and D and properdin.
2. The classical pathway - is triggered when IgG or IgM antibodies bind antigen, activating in sequence the "classical" components C1(q,r,s), C4 and C2. This is a principal effector mechanism of adaptive humoral immune responses.
3. The lectin pathway is a third recently discovered mechanism for activation of the complement cascade. It involves a mannose-binding protein (lectin) which attaches to mannose-containing glycoproteins or carbohydrates on bacteria and viruses.
These three pathways converge on the C3 component which is a central player in the complement system. It is a major serum protein (concentration ~ 1g/litre). When activated, the larger fragment (C3b) attaches to the bacterial cell wall. Phagocytes have receptors for C3b and its presence further enhances bacterial opsonisation. C3b also triggers activation of the remaining complement components C5, 6, 7, 8, 9 (the "terminal sequence") which assemble to form a membrane attack complex. This creates pore-like holes in the bacterial cell wall, killing the pathogen a process known as complement-dependent lysis. Opsonisation is responsible for
1.06 – I’ve been here before // Normal pregnancy 19
elimination of many bacterial and fungal infections. Lysis appears less generally important but is essential for elimination of Neisserial infections genetic deficiencies of terminal complement components may lead to recurrent Neisserial infection. The smaller fragments cleaved from C3 and C5 (C3a and C5a) promote inflammation by causing mast cell degranulation, increased vascular permeability and chemotaxis of polymorphonuclear neutrophils and other inflammatory cells. Because of these actions, C3a and C5a are sometimes referred to as anaphylatoxins. The complement system has an enormous potential to cause inflammation and so requires tight regulation to limit its activity. Under normal circumstances, where there is no infection, a series of regulatory and inhibitory proteins ensure that complement components remain inactive.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library; see Library Catalogue • Roitt, Brostoff, Male. Immunology. (6th ed.) 2001; chapters 4 Antibodies and 15 Immunity to bacteria and
fungi. o If you can only locate the previous (5th edition 1998) of Roitt et al. then please consult: chapters 6
Antibodies and 17 Immunity to bacteria and fungi. • Service R, "Medical research: new vaccines may ward off urinary tract infections", Science, 1997
276(5312):533. • Uehling DT, Hopkins WJ, Elkahwaji JE, Schmidt DM, Leverson GE. 'Phase 2 clinical trial of a vaginal
mucosal vaccine for urinary tract infections' Journal of Urology, 2003. 170(3): 867 – 869 • Walport MJ. Complement: First of two parts. New England Journal of Medicine, 2001, 344(14): 1058-
1066. • Walport MJ. Complement: Second of two parts. New England Journal of Medicine, 2001, 344(15): 1140-
1144.
Author: Dr Rob Loblay, Medicine
20
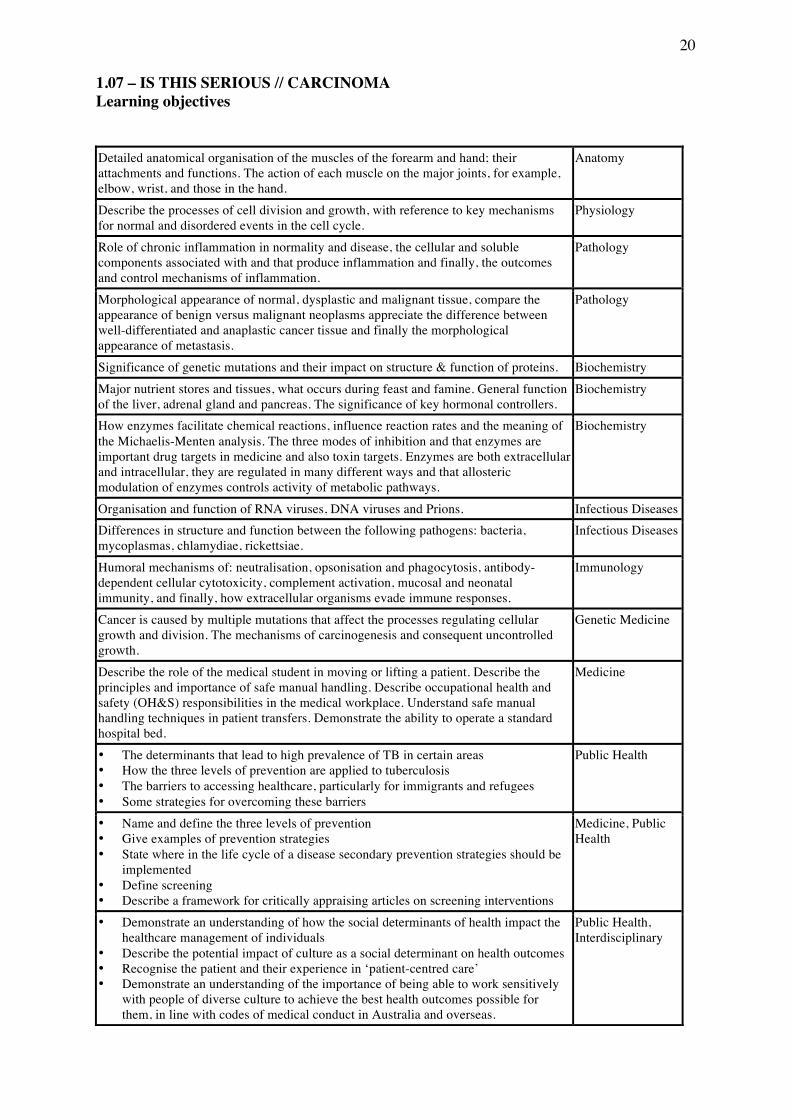
1.07 – IS THIS SERIOUS // CARCINOMA Learning objectives
Detailed anatomical organisation of the muscles of the forearm and hand; their attachments and functions. The action of each muscle on the major joints, for example, elbow, wrist, and those in the hand.
Anatomy
Describe the processes of cell division and growth, with reference to key mechanisms for normal and disordered events in the cell cycle.
Physiology
Role of chronic inflammation in normality and disease, the cellular and soluble components associated with and that produce inflammation and finally, the outcomes and control mechanisms of inflammation.
Pathology
Morphological appearance of normal, dysplastic and malignant tissue, compare the appearance of benign versus malignant neoplasms appreciate the difference between well-differentiated and anaplastic cancer tissue and finally the morphological appearance of metastasis.
Pathology
Significance of genetic mutations and their impact on structure & function of proteins. Biochemistry Major nutrient stores and tissues, what occurs during feast and famine. General function of the liver, adrenal gland and pancreas. The significance of key hormonal controllers.
Biochemistry
How enzymes facilitate chemical reactions, influence reaction rates and the meaning of the Michaelis-Menten analysis. The three modes of inhibition and that enzymes are important drug targets in medicine and also toxin targets. Enzymes are both extracellular and intracellular, they are regulated in many different ways and that allosteric modulation of enzymes controls activity of metabolic pathways.
Biochemistry
Organisation and function of RNA viruses, DNA viruses and Prions. Infectious Diseases Differences in structure and function between the following pathogens: bacteria, mycoplasmas, chlamydiae, rickettsiae.
Infectious Diseases
Humoral mechanisms of: neutralisation, opsonisation and phagocytosis, antibody-dependent cellular cytotoxicity, complement activation, mucosal and neonatal immunity, and finally, how extracellular organisms evade immune responses.
Immunology
Cancer is caused by multiple mutations that affect the processes regulating cellular growth and division. The mechanisms of carcinogenesis and consequent uncontrolled growth.
Genetic Medicine
Describe the role of the medical student in moving or lifting a patient. Describe the principles and importance of safe manual handling. Describe occupational health and safety (OH&S) responsibilities in the medical workplace. Understand safe manual handling techniques in patient transfers. Demonstrate the ability to operate a standard hospital bed.
Medicine
• The determinants that lead to high prevalence of TB in certain areas • How the three levels of prevention are applied to tuberculosis • The barriers to accessing healthcare, particularly for immigrants and refugees • Some strategies for overcoming these barriers
Public Health
• Name and define the three levels of prevention • Give examples of prevention strategies • State where in the life cycle of a disease secondary prevention strategies should be
implemented • Define screening • Describe a framework for critically appraising articles on screening interventions
Medicine, Public Health
• Demonstrate an understanding of how the social determinants of health impact the healthcare management of individuals
• Describe the potential impact of culture as a social determinant on health outcomes • Recognise the patient and their experience in ‘patient-centred care’ • Demonstrate an understanding of the importance of being able to work sensitively
with people of diverse culture to achieve the best health outcomes possible for them, in line with codes of medical conduct in Australia and overseas.
Public Health, Interdisciplinary
1.07 – Is this serious // Carcinoma 21
1. Structure and function of breast General Objectives • To understand the gross anatomy of the breast and its location with respect to the structures of the chest
wall • To understand the structural changes to the breast during puberty, pregnancy and menopause • To understand the lymphatic drainage of the breast. The breasts are a secondary sexual feature in the female and a rudimentary structure in males and prepubescent females. Breast shape and size is dependent on age, genetic, racial, and dietary factors, parity and menopausal status. The mamma or breast is made up of mammary gland, the fatty superficial fascia in which it is embedded, and the overlying skin with nipple and surrounding pigmented skin, the areola. Although size and shape vary in the adult female, the base of the breast is relatively constant lying at the level of ribs 2 to 6, from the sternal edge almost to the midaxillary line. The upper lateral quadrant is prolonged along the lower margin of pectoralis major muscle, and may pass through the deep fascia and extend to the apex of the axilla (axillary tail). The breast lies in superficial fascia. It is separated from the deep (pectoral) fascia by a retromammary space which allows some degree of movement. The breast comprises15-20 lobes of glandular tissue radiating away from the nipple. Each lobe has a main lactiferous duct which opens onto the nipple, and a dilatation at the base of the nipple, the lactiferous sinus. Lobules are the parts of the lobe that are secretory (or potentially so). The glandular tissue is embedded in fat, which comprises the bulk of the non-lactating breast. Fibrous septa separate the lobes and bands of connective tissue connect the lobes to skin. They are better developed and more numerous in the upper half of the breast (suspensory ligaments of Cooper). The skin of the nipple is pigmented and hairless. The nipple is comprised of dense connective tissue, elastic fibres, and smooth muscle (in a predominantly circular orientation). Cold, tactile (e.g., suckling) or emotional stimulus induces erection of the nipple, wrinkling of the areola and compression of the lactiferous sinuses. The skin of the nipple and areola contain modified sweat and sebaceous glands, especially at the outer margin of the areola. The latter enlarge in early pregnancy. Their oily secretions act as a protective lubricant during lactation. In the second month of pregnancy the nipple and areola increase in pigmentation and do not return to their original colour. The male and immature female breast comprises a few ducts embedded in fibrous tissue. The nipple and areola are small and the ducts generally do not extend far beyond the areola. At puberty the nipple and areola enlarge, alveoli sprout from the ducts and considerable fatty infiltration of breast tissue takes place. During pregnancy, much of the fat in the gland is replaced by the proliferation of ducts and an increase in the numbers of secretory alveoli per lobule. When lactation ceases there is a progressive atrophy of ducts and lobules, and fatty replacement of breast tissue. Following menopause the glandular tissue atrophies. The breast also undergoes changes during each menstrual cycle. The lymphatic drainage of the breast is very variable. From a subareolar plexus, vessels drain predominantly (75%) to the axillary lymph nodes but also drain through the thoracic wall to parasternal and mediastinal nodes. Lymph vessels may drain to the contralateral breast, to deep cervical nodes and some may drain via the anterior abdominal wall to the groin. Living anatomy. The nipple lies a little below the centre of the breast in adult females. In males the nipple is relatively constant in position, lying at the level of the 4th intercostal space. The mnemonic 4+4=8 was useful for surface anatomy before the introduction of the metric system, indicating the 4th intercostal space, 4 inches (10 cm) from the midline at the level of the 8th thoracic vertebra. Occasionally supernumerary nipples, or breasts, may occur along the 'milk line', a line from axilla to groin.
References Use the textbooks in your Tutorial Room Optional references • Available in Medical Library: see Library Catalogue
o The Anatomy Coloring Book 3rd ed (2002), W. Kapit and L.M. Lawrence, Addison-Wesley Educational Publishers.
o Model of the trunk • Online

1.07 – Is this serious // Carcinoma 22
o Anatomy glossary - http://www.anatomy.usyd.edu.au/glossary o Online Wilson Museum of Anatomy - http://gmp.anatomy.usyd.edu.au/wilson_henle/ o Wilson bottles: 625 anterior & lateral (breast and lymphatics); 160 anterior (breast)
• Prosections, models, CDROMs o Prosections, skeleton, computer-based resources available in J. T. Wilson Museum of Anatomy -
room W401, Anderson Stuart Bldg, open 8.30 am - 5.30pm.
Author: Ms Deborah Bryce, Anatomy and Histology
1.07 – Is this serious // Carcinoma 23
2. Lumps in the breast Understanding the structure and function of the breast helps one to understand what causes breast lumps. The breast consists of glandular tissue arranged in lobules which contain the epithelial cells responsible for secretion. These secretory units empty into a network of epithelial-lined ducts which lead to the nipple. The rest of the breast is composed of fat and fibrous tissue which acts as a support structure and gives shape to the breast. The breast is subject to hormonal influences. It is the gonadotropins and sex hormones (oestrogen, progesterone) which exert the greatest effects. The changes may be quite varied amongst a population of women, and in an individual woman at any particular period of her life. The breast undergoes rapid growth during puberty, and subsequently undergoes cyclical changes during the menstrual cycle. During pregnancy the breast increases in volume and during lactation the breast cells secrete large volumes of milk. The glandular cells of the breast involute after the menopause, and breast volume shrinks with advancing age. Most breast lumps are transient aberrations of normal development and involution which occur during these times of physiological change throughout a woman's lifetime. However, some breast lumps are due to disease processes. The majority of these abnormal breast lumps are benign and will do little harm to the woman. It is important, however, to differentiate the benign breast lump from a cancer, for the earlier a cancer can be detected, the better the likely outcome from treatment for the patient. Some of the causes of breast lumps due to disease include: • Trauma which may cause destruction of the breast fat (this is not a disease). • A woman who is breast feeding may develop an infection in the breast which will lead to a painful lump. • Some lumps are derived from the supporting structure e.g. skin, fat, fibrous 'ligaments'. These lumps are not
hormonally influenced and cancer arising in these lumps is extremely rare. • By far the most common discrete lump found in young women, however, is the benign fibro adenoma
which is a localised overgrowth of glands and supporting tissue. • Cysts (enclosed sacs often lined by epithelium) are encountered with increasing frequency towards middle
age. They are almost always benign. Cysts are due to dilation of ducts. Microcysts are very common and are probably present in most women in the middle years of life. Large cysts, however, can cause palpable breast lumps.
Cysts may be part of a process which is called fibrocystic change. This is a broad term which covers a range of changes in the breast, from those that are physiological to those that can cause lumps. Some may be associated with an increased risk of developing cancer. Other components of fibrocystic change include fibrosis, and epithelial hyperplasia (an increase in the number of epithelial cells). As the hyperplasia becomes more pronounced and atypical cells increase, the greater the chance of the woman developing breast cancer. Breast cancer results when cells which have mutated grow in a haphazard and uncontrolled way. Breast cancer usually arises from ductal cells but can also originate in the lobules about 10% of the time.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Kumar, Abbas, Fausto and Aster. 2010. Robbins and Cotran: Pathologic Basis of Disease (8th Ed) pp.
1066-1073 • Kumar, Abbas, Fausto and Mitchell. 2007. Robbins: Basic Pathology (8th Ed) pp. 739-74. • Williamson RCN, Waxman BP, Scott. 1998. Scott, an aid to clinical surgery . (6th ed.) Churchill
Livingstone. • Browse NL.2005. Browse's introduction to the symptoms and signs of surgical disease . (4th ed.) Edward
Arnold. Multimedia (CD-Rom) • Anderson L.deB, Masters J. The Systematic Body 3.O. Systematic Software Limited, Sydney 1995.
Author: Associate Professor Brett Hambly, Pathology Author: Professor Martin Tattersall, Medicine
1.07 – Is this serious // Carcinoma 24
3. The nature of cancer Cancer is a form of neoplasm. A neoplasm is an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after cessation of the stimuli which evoked the change. It arises due to multiple genetic changes within one cell. A confusing array of terms are used to describe neoplasms. Some important examples include: cancer (a malignant neoplasm or tumour, probably from the Latin "crab", because of the stellate appearance of many neoplasms) and oncology (the study of neoplasms). The cancer may affect the patient in a number of different ways. For example, the cancer may lead to disfigurement, mechanical interference with normal function of an organ, destruction of part or all of an organ, ulceration of an epithelial surface, nutritional 'competition' leading to cachexia, para-neoplastic effects (for example, abnormal hormone production) and psychological effects. Depending on the severity of these affects the patient may die. A characteristic of neoplasms is the morphological changes that occur in the cells that are involved usually in response to some form of irritation (for example cigarette smoke). Two changes in the morphology of cells that may occur prior to neoplastic transformation are metaplasia and dysplasia. Metaplasia has occurred when a normal cell for that site changes into another normal morphology that is not normally seen at that site, for example, bronchial epithelium in the lungs changing to squamous epithelium in response to an irritant such as smoking. Dysplasia has occurred when there is a loss in the uniformity of the individual cells as well as a loss in their architectural orientation (the dysplastic cells start to look more like cancerous tissue). For example, cervical epithelium initially becomes dysplastic following infection with cancerous forms of human papilloma virus. Tissue will in theory return to normal upon removal of metaplastic and dysplastic stimuli. On the other hand, cells that have undergone neoplastic transformation differ from dysplastic cells by the changes being irreversible on removal of the stimulus. Neoplasms are made up of two types of cells: parenchymal cells that are the actual neoplastic cells and supportive stromal cells that are non-neoplastic, such as connective tissue and blood vessels, that have usually been induced to grow through the neoplasm by the neoplasm itself. Two other terms that you will frequently hear used about neoplasms, particularly malignant ones are differentiation and anaplasia. These terms refer to the extent to which parenchymal cells resemble comparable normal cells, both morphologically and functionally. The more anaplastic the cells look, the less they look like the original normal tissue. Anaplasia generally correlates with worse prognosis for the patient. Essentially, two types of neoplasms exist, benign and malignant. By definition, malignant cancers metastasise (spread to other parts of the body and start growing there), while benign tumours do not. Benign tumours are usually slow growing, innocuous and non-life threatening (except, for example, a benign meningioma, which presses on the brain in the indistensible cranium), while malignant cancers are often fast growing and life threatening, since they metastasise to and destroy other vital structures in the body, in addition to the primary site where they began growing. Benign tumours usually have the suffix 'oma', while malignant cancers are usually called a carcinoma (if of epithelial origin) or a sarcoma (if of mesenchymal origin). The way in which individual neoplasms are named varies considerably. Most neoplasms are named according to the histogenetic method, on the basis of their cell of origin; for example, an adenoma/adenocarcinoma arises from glandular cells, while a fibroma/fibro sarcoma arises from fibrous tissue. Neoplasms may also be named after individuals or according to the organ in which they are found.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Kumar, Abbas, Fausto and Aster. 2010. Robbins and Cotran: Pathologic Basis of Disease. (8th ed.) pp 260-
270. • Kumar, Abbas, Fausto and Mitchell. 2007. Robbins: Basic Pathology. (8th ed.) pp 171-181.
Author: Associate Professor Brett Hambly, Pathology
1.07 – Is this serious // Carcinoma 25
4. Lymphatic system and the spread of cancer Benign tumours do not metastasise, while malignant cancers usually eventually do. The treatment of cancer at present is directed towards removing the cancer itself (surgery, chemotherapy, radiotherapy) rather than treating the cause of the cancer (reversing the genetic changes in the neoplastic cells). Hence, 'successful' treatment necessitates the removal of the primary tumour and any secondary deposits (metastases). Cancer may spread by eight different mechanisms: locally, via the lymphatics, seeding in a body cavity, haematogenous spread, along tissue planes, implantation (usually at operation), spread from mucosa to mucosa and perineural spread. Of these, lymphatic spread is one of the most common and is usually the first. Lymph node metastasis is a marker of tumour behaviour and may indicate further spread. When a cancer reaches an appropriate stage of growth and suffers further genetic changes, the cancer cells are about to infiltrate into lymphatic ducts. The cells are then carried (by embolism or permeation) along the lymphatic ducts to the draining lymph nodes, where they will usually form a new cancer deposit. Some of the cells from this deposit may subsequently break away and spread further through the lymphatics. Lymphatic spread of a tumour is generally more common with carcinomas than with sarcomas. Notably, lymph nodes draining the region of a cancer may initially become enlarged due to the inflammatory response being generated by the cancer itself. This is termed reactive hyperplasia and may occur prior to spread of the tumour cells themselves. Often the macroscopically normal draining lymph nodes for a cancer will be surgically removed at the same time as the primary cancer, to reduce the risk of microscopic deposits being left in the nodes and to allow the pathologist to determine a prognosis (if the nodes show no tumour cells then the prognosis is substantially improved). Over a period of time cancers tend to become more aggressive and acquire greater malignant potential: tumour progression. This implies that individual subclones of a cancer progressively evolve; the phenotypic attributes of these subclones include a greater ability to metastasise successfully. For successful metastasis to occur the malignant cells must be able to complete a series of sequential steps, such as adhering to the basement membrane, breaking it down and moving across it.
References Use the textbooks in your Tutorial Room Optional References Available in Medical Library: see Library Catalogue • Kumar, Abbas, Fausto and Aster. 2010. Robbins and Cotran: Pathologic Basis of Disease. (8th ed.) pp 269-
270, 298-302. • Kumar, Abbas, Fausto and Mitchell. 2007. Robbins: Basic Pathology. (8th ed.) pp 179-181, 201-204.
Author: Associate Professor Brett Hambly, Pathology
1.07 – Is this serious // Carcinoma 26
5. Responses to life-threatening illness "Breast cancer is one of the most feared and most publicly discussed diseases. Most women face its threat sooner or later, either personally in a close relative or friend, or in the form of breast symptoms". A surgeon wrote thus and went on to state that "its death rate has not fallen in 50 years and its treatment remains distressing". He believed that psychological needs tended to receive insufficient attention. Predisposition to Breast Cancer: Facts, Misconceptions and Myths Some Facts The prevalence of breast cancer is slowly increasing all over the Western world. Some factors associated with its onset include nulliparity, obesity (peak association), ionising radiation, being a late age primipara, and use of the contraceptive pill and heredity. These facts, being known to more informed women, may lead to much guilt and consequently anxiety and concern. Some Myths and Misconceptions Erroneous ideas abound with regard to the importance of breast trauma, cystitis, stressful events, divine retribution, lifestyle and smoking, as well its prevalence, the five year survival and frequency of benign versus malignant masses. Vogues for alternative cancer treatments (dietary change) and lifestyle changes are commonly employed even by educated women. Personality attributes Interesting psychophysiological research in Europe, North America and Australia has demonstrated an association between certain types of emotional expression and a tendency to develop malignant lesions. Neurohumoral and cytokine studies now showing some relationships. Importance of disseminating this data carefully and in context. Diagnosis Some epidemiological facts Women who delay treatment are generally older, of lower socio-economic class, less well educated and fearful of hospitals, surgery and cancer. Psychological Issues Alternatively, a belief of personal susceptibility for breast cancer affects health behaviours and leads to increased attendance for mammography. These desirable behaviours could be affected or nullified by unwillingness to for exposure (body image issues) or financial imperatives and/or work ethic issues slowing activation of positive health behaviours. The concept of threshold of awareness of need to act is important to consider. An apparent excess of knowledge by health professionals can lead to the 'it couldn't happen to me' syndrome even after discovery of a mass. Five identified coping styles include denial, fighting spirit, stoic acceptance, anxious and depressed acceptance and helpless/hopelessness. Treatment Mastectomy versus Lumpectomy In the past, significant proportion of women suffered great physical and psychiatric morbidity following mastectomy. Significant body image and sexuality issues. Radiotherapy Fear of risk of radiotherapy: stemming from knowledge of Chernobyl disaster and long-term risks now publicised after treatment of scalp ringworm. Fear of burns, fatigue & damage to 'normal structures'. Chemotherapy Nausea and vomiting and alopecia and fears of ill-defined long term sequelae. The body image implications of alopecia. Great sensitivity is needed to give the rationale for such treatment even if confidence exists in the oncologist's mind about the success of surgery. Counselling Issues
1.07 – Is this serious // Carcinoma 27
Importance of clinicians awareness of (often unspoken) issues regarding uncertainty of survival, changes in body image, 'becoming a burden', 'not fulfilling one's obligations' and becoming sexually less attractive to a partner. Studies show a 25-50% prevalence of clinical anxiety and depression in advanced disease. Appropriate counselling at all stages should involve a chance for ventilation and developing positive ways of restructuring the patients current and perceived situations. Initially directive, cathartic and supportive approaches may be appropriate. Counselling also has a place in pre and post-operative periods and during chemotherapy and radiotherapy. It may need subtle changes in approach. English research work describes a positive approach in advanced disease which involves adoption or 'fighting spirit'. Palliative care counselling is a unique and highly personal endeavour and, likewise, can be very supportive. Psychotropic Drugs Short-term courses of appropriate benzodiazepines (lorazepam) and use of tricyclic and new generation antidepressants can be adjuncts to counselling.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Morris T, Greer ST, Pettingale KW, Watson M. Patterns of expression of anger and their psychological
correlates in women with breast cancer. J Psychosom Res 1981; 25(2): 111-117 • Morris T, Pettingale K, Haybittle J. Psychological response to cancer diagnosis and disease outcome in
patients with breast cancer and lymphoma. Psycho-oncology 1992; 1(2): 105-114 • Fallowfield LJ, Hall A, Maguire GP, Baum M. Psychological outcomes of different treatment policies in
women with early breast cancer outside a clinical trial (see comments). BMJ 1990; 301(6752): 575-580. • Butow PN, Kazemi NJ, Beeney LJ, Griffin AM, Dunn SM, Tattersall MH. When the diagnosis is cancer:
patient communication experiences and preferences . Cancer 1996; 77(12): 2630-7. • Newell S, Sanson-Fisher RW, Girgis A, Bonaventura A. How well do medical oncologists' perceptions
reflect their patients' reported physical and psychosocial problems? Data from a survey of five oncologists. Cancer 1998; 83(8): 1640-51.
Author: Clinical Associate Professor Roger Whitworth Bartrop, Psychiatry
1.07 – Is this serious // Carcinoma 28
6. Team approaches to management of breast cancer Management options for 'early' (localized) breast cancer are complex. The options include surgery, radiotherapy and systemic treatment with hormones or chemotherapy. Before a patient commences treatment they may benefit from consultation with more than one breast specialist working in various interdisciplinary fields (a multidisciplinary approach). The surgeon will usually be the first specialist consulted and at the initial consultation will be responsible for a complete explanation of treatment options. If it is anticipated that other modalities of treatment will be required or indeed, even if the patient would like further clarification with respect to these treatments, then consultation with the appropriate radiation or medical oncologist is appropriate before surgicval treatment is undertaken. Consent is necessary, if the patient is to understand what may well be a prolonged course of multiple modality treatments. Other team members, such as breast care nurses can give valuable assistance to the newly diagnosed patient at this point. Surgical treatment includes excision of the tumour in the breast (wide local excision), removal of the whole breast (total mastectomy) and removal of the draining lymph nodes on the same side (axillary dissection). Both the breast and axilla may also be treated with radiotherapy (X-ray treatment) either in combination with surgery in the case of wide local excision or instead of surgery for management of the axilla. Adjuvant systemic treatments are indicated for most patients depending on their absolute risk of recurrence of their breast cancer. This will be in the form of chemotherapy or endocrine/hormonal therapies. Surgery is intended to completely remove the tumour with cosmesis being a secondary but important consideration. Fortunately, for most women with early breast cancer, there is a treatment option with similar survival outcome, namely breast conserving surgery and breast radiation or mastectomy. In breast conserving surgery only the tumour within the breast (with a margin of normal tissue) is removed ('lumpectomy'). This operation offers superior cosmesis and for many women maintaining body image is an important outcome. If a woman chooses treatment by breast conservation, subsequently radiotherapy is given to the remainder of the breast since this significantly reduces the risk of local recurrence. If a woman chooses to have a mastectomy, radiotherapy is usually not required. Regardless of how the breast is managed, the axilla in most instances will also be treated. Usually this takes the form of surgery to the axilla to remove some of the lymph glands but lymph glands in the axilla can be treated with radiotherapy with little discernible difference in treatment morbidity or outcome. The disadvantage of radiotherapy alone is that the nodes are not removed for pathological examination and prognostic information therefore is not obtained. Prognostic factors for survival in women with 'early' breast cancer include spread of cancer to axillary nodes, the number of nodes containing cancer, the dimensions and histological grade of the breast tumour. The presence of oestrogen and progesterone receptors in breast tumours is routine, and increasingly HER-2/neu (a trans membrane receptor tyrosine kinase that mediates growth, differentiation and survival of cells) is being measured. Depending on prognostic indicators, and on the tumour containing hormone receptors, either hormonal or chemotherapy will be recommended. Large clinical trials have shown that outcome is improved by systemic treatment to treat micrometastases which are not detectable on imaging tests. Trastuzumab (Herceptin) is now commonly given to women whose tumours contain HER-2/neu. Chemotherapy is given over a period of months, but hormonal treatments are commonly given for 5 or more years. Subsequent follow up includes physical examination and yearly mammography (partly to detect cancer development in the other breast). It is not possible to be prescriptive about treatment, as management will commonly be individualised. Generally however, specialist teams work within evidence-based best practice guidelines.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Clinical Practice Guidelines for the management of Early Breast Cancer. 2nd Edition 2001.
o A broad overview of early breast cancer that will provide a starting point for further reading. It is expected that you browse this reference.
Author: Professor Martin Tattersall, Medicine
1.07 – Is this serious // Carcinoma 29
7. Principles of screening non-communicable diseases Learning objectives: Students should be able to: • Name the three levels of prevention • Define the three levels of prevention • Give examples of prevention strategies • State where in the life cycle of a disease secondary prevention strategies should be implemented • Define screening • Describe a framework for critically appraising articles on screening interventions Levels of prevention of non-communicable disease Promoting, preserving and restoring health and minimizing suffering and distress are important goals of medicine and are embodied in the principles of disease 'prevention'. Strategies for disease prevention are traditionally considered as 'primary, secondary and tertiary'. There is sometimes debate about the exact boundaries between these three levels but the following definitions are generally accepted. • Primary prevention: aims at reducing the incidence of disease, illness and injury. It can be defined as the
'protection of health' at individual and community levels. Some examples are - maximising nutritional status and physical fitness and emotional well being, immunizing against infectious diseases and making the environment safe.
• Secondary prevention: aims at reducing the prevalence of disease, illness and injury by shortening the duration. It can be considered as measures to assist the early detection and prompt effective treatment of disease or illness in individuals and communities. Screening programs are a good example.
• Tertiary prevention: aims at reducing the number or impact of complications of disease, illness and injury. It includes measures to reduce or eliminate the long-term impairment, disability and suffering from disease and promotes adjustment to untreatable conditions.
Screening as a secondary prevention strategy for non-communicable disease Screening has been defined as:
"...the systematic application of a test or inquiry, to identify individuals at sufficient risk of a specific disorder to benefit from further investigation or directive preventive action, among persons who have not sought medical attention on account of symptoms of that disorder"
In the EBM part of your curriculum you will learn more about how to critically appraise articles about screening tests. In the Community & Doctor Theme we would like you to understand how screening might be used as a secondary prevention strategy for disease within populations. More opportunities to learn about screening will arise in later blocks but in this problem you should become familiar with the framework we would like you to use when considering the effectiveness or otherwise of screening tests.1 Mammography as a screening program for breast cancer The Australian and State Governments provide free breast cancer screening, actively offering screening to all Australian women aged 50-69 years. The US Preventive Services Task Force recommends:
"The USPSTF recommends biennial screening mammography for women aged 50 to 74 years. Grade: B recommendation
The decision to start regular, biennial screening mammography before the age of 50 years should be an individual one and take patient context into account, including the patient's values regarding specific benefits and harms. Grade: C recommendation "So, what does this mean if you are a woman in your 40s? You should talk to your doctor and make an informed decision about whether mammography is right for you based on your family history, general health, and personal values." Diana Petitti, MD, MPH Vice Chair, U.S. Preventive Services Task Force November 19, 2009
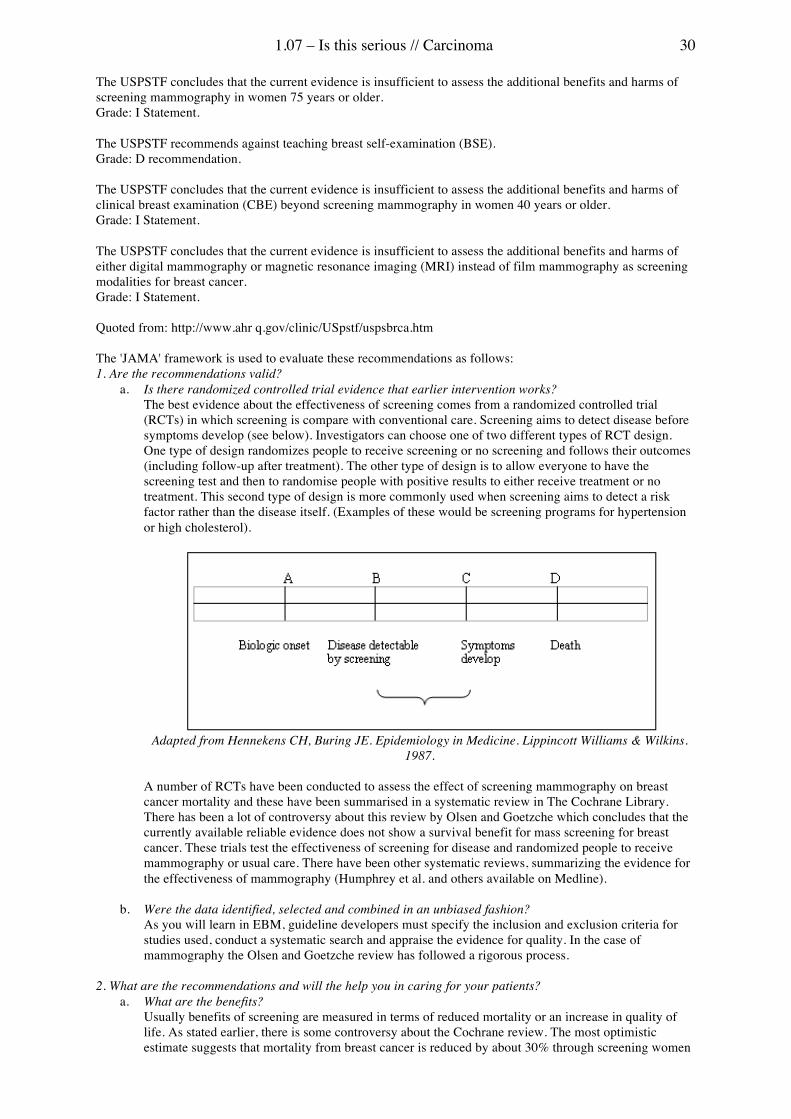
1.07 – Is this serious // Carcinoma 30
The USPSTF concludes that the current evidence is insufficient to assess the additional benefits and harms of screening mammography in women 75 years or older. Grade: I Statement. The USPSTF recommends against teaching breast self-examination (BSE). Grade: D recommendation. The USPSTF concludes that the current evidence is insufficient to assess the additional benefits and harms of clinical breast examination (CBE) beyond screening mammography in women 40 years or older. Grade: I Statement. The USPSTF concludes that the current evidence is insufficient to assess the additional benefits and harms of either digital mammography or magnetic resonance imaging (MRI) instead of film mammography as screening modalities for breast cancer. Grade: I Statement. Quoted from: http://www.ahr q.gov/clinic/USpstf/uspsbrca.htm The 'JAMA' framework is used to evaluate these recommendations as follows: 1. Are the recommendations valid?
a. Is there randomized controlled trial evidence that earlier intervention works? The best evidence about the effectiveness of screening comes from a randomized controlled trial (RCTs) in which screening is compare with conventional care. Screening aims to detect disease before symptoms develop (see below). Investigators can choose one of two different types of RCT design. One type of design randomizes people to receive screening or no screening and follows their outcomes (including follow-up after treatment). The other type of design is to allow everyone to have the screening test and then to randomise people with positive results to either receive treatment or no treatment. This second type of design is more commonly used when screening aims to detect a risk factor rather than the disease itself. (Examples of these would be screening programs for hypertension or high cholesterol).
Adapted from Hennekens CH, Buring JE. Epidemiology in Medicine. Lippincott Williams & Wilkins.
1987. A number of RCTs have been conducted to assess the effect of screening mammography on breast cancer mortality and these have been summarised in a systematic review in The Cochrane Library. There has been a lot of controversy about this review by Olsen and Goetzche which concludes that the currently available reliable evidence does not show a survival benefit for mass screening for breast cancer. These trials test the effectiveness of screening for disease and randomized people to receive mammography or usual care. There have been other systematic reviews, summarizing the evidence for the effectiveness of mammography (Humphrey et al. and others available on Medline).
b. Were the data identified, selected and combined in an unbiased fashion? As you will learn in EBM, guideline developers must specify the inclusion and exclusion criteria for studies used, conduct a systematic search and appraise the evidence for quality. In the case of mammography the Olsen and Goetzche review has followed a rigorous process.
2. What are the recommendations and will the help you in caring for your patients?
a. What are the benefits? Usually benefits of screening are measured in terms of reduced mortality or an increase in quality of life. As stated earlier, there is some controversy about the Cochrane review. The most optimistic estimate suggests that mortality from breast cancer is reduced by about 30% through screening women
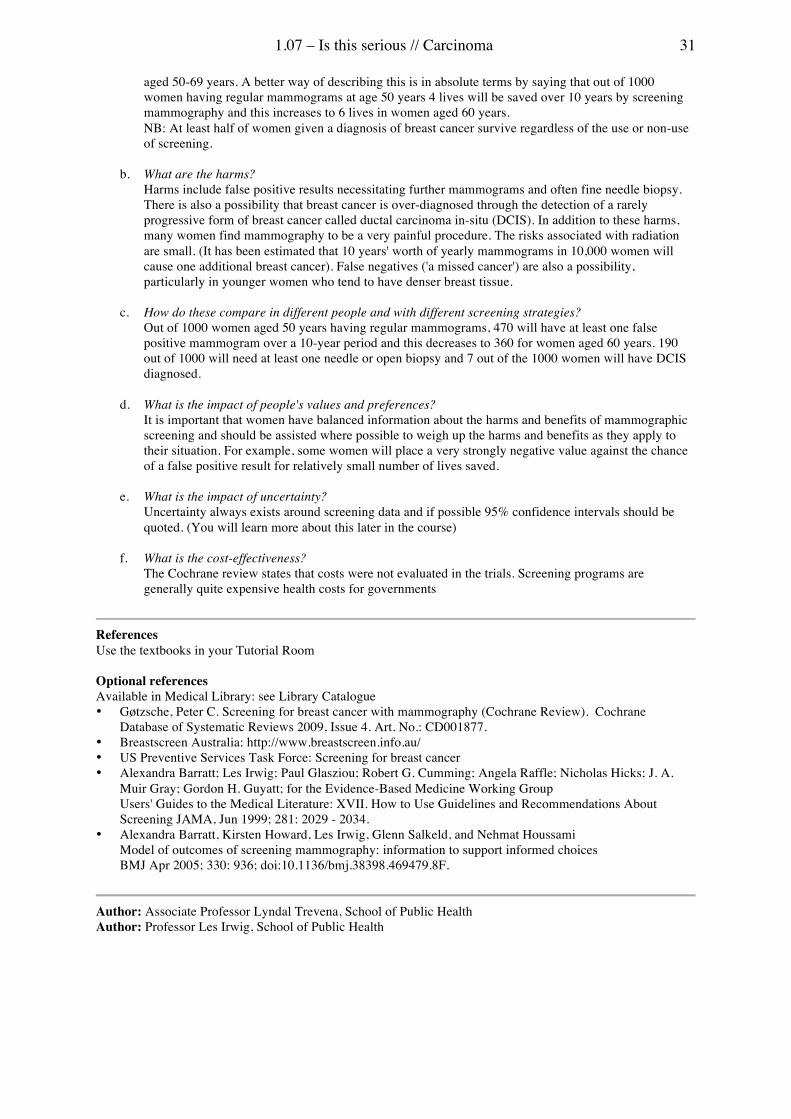
1.07 – Is this serious // Carcinoma 31
aged 50-69 years. A better way of describing this is in absolute terms by saying that out of 1000 women having regular mammograms at age 50 years 4 lives will be saved over 10 years by screening mammography and this increases to 6 lives in women aged 60 years. NB: At least half of women given a diagnosis of breast cancer survive regardless of the use or non-use of screening.
b. What are the harms? Harms include false positive results necessitating further mammograms and often fine needle biopsy. There is also a possibility that breast cancer is over-diagnosed through the detection of a rarely progressive form of breast cancer called ductal carcinoma in-situ (DCIS). In addition to these harms, many women find mammography to be a very painful procedure. The risks associated with radiation are small. (It has been estimated that 10 years' worth of yearly mammograms in 10,000 women will cause one additional breast cancer). False negatives ('a missed cancer') are also a possibility, particularly in younger women who tend to have denser breast tissue.
c. How do these compare in different people and with different screening strategies? Out of 1000 women aged 50 years having regular mammograms, 470 will have at least one false positive mammogram over a 10-year period and this decreases to 360 for women aged 60 years. 190 out of 1000 will need at least one needle or open biopsy and 7 out of the 1000 women will have DCIS diagnosed.
d. What is the impact of people's values and preferences? It is important that women have balanced information about the harms and benefits of mammographic screening and should be assisted where possible to weigh up the harms and benefits as they apply to their situation. For example, some women will place a very strongly negative value against the chance of a false positive result for relatively small number of lives saved.
e. What is the impact of uncertainty? Uncertainty always exists around screening data and if possible 95% confidence intervals should be quoted. (You will learn more about this later in the course)
f. What is the cost-effectiveness?
The Cochrane review states that costs were not evaluated in the trials. Screening programs are generally quite expensive health costs for governments
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Gøtzsche, Peter C. Screening for breast cancer with mammography (Cochrane Review). Cochrane
Database of Systematic Reviews 2009, Issue 4. Art. No.: CD001877. • Breastscreen Australia: http://www.breastscreen.info.au/ • US Preventive Services Task Force: Screening for breast cancer • Alexandra Barratt; Les Irwig; Paul Glasziou; Robert G. Cumming; Angela Raffle; Nicholas Hicks; J. A.
Muir Gray; Gordon H. Guyatt; for the Evidence-Based Medicine Working Group Users' Guides to the Medical Literature: XVII. How to Use Guidelines and Recommendations About Screening JAMA, Jun 1999; 281: 2029 - 2034.
• Alexandra Barratt, Kirsten Howard, Les Irwig, Glenn Salkeld, and Nehmat Houssami Model of outcomes of screening mammography: information to support informed choices BMJ Apr 2005; 330: 936; doi:10.1136/bmj.38398.469479.8F.
Author: Associate Professor Lyndal Trevena, School of Public Health Author: Professor Les Irwig, School of Public Health
32
1.08 – A QUESTION OF COMMUNICATION // TUBERCULOSIS Learning objectives Detailed anatomical organisation of the blood vessels of the upper limb, their major course and innervations.
Anatomy
Two different aspects of manipulation in the human host. The relationship between organ, tissue and cell transplantation and the host immune response. How vaccination improves host immunity.
Immunology
The mechanisms involved in the process of infection and immunity in response to microbacterium.
Immunology
Mechanisms of: Central T and B cell tolerance, peripheral T and B cell tolerance, genetic factors in autoimmunity, the role of infections in autoimmunity, and finally, some selected autoimmune disease.
Immunology
Mechanisms of hypersensitivities (Type I-IV reactions) and congenital and acquired immune deficiencies.
Immunology
Means by which viruses spread through the host, the genetic determinants of viral virulence, and the mechanisms of disease production. The mechanisms of viral damage to tissues and organs, virus-induced immunopathology, persistent and latent infections and viral oncogenesis.
Infectious Diseases
Factors promoting colonisation, adherence, motility and Fe acquisition. The mechanisms involved in evading host defences; capsules, inhibition of phagocytosis, protein A. The factors that damage the host; exotoxins, endotoxin, hydrolytic enzymes.
Infectious Diseases
Chronic infection from the viewpoint of the organism and the host. How this affects diagnosis, management and control. The different elements of the specific immune response and how they are regulated.
Pathology
• To appreciate the possible outcomes of acute inflammation • To understand the aetiologies of chronic inflammation • To be cognisant of the similarities and differences between the different forms of
chronic inflammation at the cellular level
Pathology
The patient-doctor interaction and formulate a series of questions that may be answered using the best available research evidence.
Epidemiology
• Define a communicable disease • Explain what is required for the development, implementation and evaluation of health
policies • Describe the legislative underpinnings of public health policy • Describe the priorities and strategies for public health policy in Australia • Understand the principles of disease surveillance and the investigation of a disease
outbreak
Public Health
How to take a drug and alcholol medical history from a patient, together with how to undertake a physical examination on these patients.
Medicine
Describe Standard Precautions and Transmission Based Precautions. Demonstrate surgical scrub techniques. Demonstrate gowning and gloving (no touch technique). Demonstrate change of gloves while maintaining a sterile field.
Medicine
• Name the three levels of prevention • Define the three levels of prevention • Give examples of prevention strategies • State where in the life cycle of a disease secondary prevention strategies should be
implemented • Define screening • Describe a framework for critically appraising articles on screening interventions
Medicine, Public Health
1.08 – A question of communication // Tuberculosis 33
1. Systemic responses to infection One effect of infections is to cause generalised or systemic symptoms such as a raised temperature, tiredness and weight loss. These effects may be similar regardless of the type of organism or site of infection. Such symptoms are caused by the release of small messenger proteins or cytokines from infected cells or from leucoctyes recruited to the site of infection. These molecules have important local effects in promoting an inflammatory response to contain the infection. When they enter the circulation, however they can have effects at distant sites. Cytokines are produced as part of an initial host response and are not dependent on antigen-specific recognition of the pathogen causing the infection. Cytokines with generalised actions Macrophages are the major source of pro-inflammatory cytokines. These include: • Tumour necrosis factor (TNF), • Interleukin-1 (IL-1) • Interleukin-6 These are often secreted sequentially in response to bacterial infections. One product of gram-negative bacteria, called lipo-polysaccharide (LPS) is a very potent stimulus for TNF. Components of mycobacterial cell walls also stimulate TNF synthesis. Viral infections, such as the 'common cold' or influenza, stimulate the rapid release of a different cytokine Interferon-alpha (IFN-a) which has a local 'anti-viral' effect, but also causes the fever and malaise typical of influenza. Effects of cytokines Acute changes • Fever. Temperature is normally tightly regulated through a 'thermo-regulatory' centre in the hypothalamus
(details in year 2). A fall in the temperature produces shivering which generates local heat, while a rise causes sweating in order to lose heat through evaporation. The effect of TNF, IL-1 and viral-induced IFN-a is to reset the thermostat so the metabolic activity of the body produces excess heat. This effect is mediated by prostaglandins and can be inhibited by aspirin or other drugs which inhibit prostaglandin synthesis.
• Acute Phase Response (APR). The liver is the major source of serum proteins. TNF, IL-1 and IL-6 cause rapid changes to the pattern of proteins produced. Albumin, the major transport protein, is switched off while the synthesis of other proteins which contribute to the inflammatory response is increased. These include: complement proteins and other opsonins (such as C-reactive protein) which aid the phagocytosis of bacteria; anti-proteolytic enzymes which limit tissue destruction; and fibrinogen, an important clotting protein. This APR pattern is a marker of infection and inflammation. This is often associated with a rise in the Erythrocyte Sedimentation Rate (ESR).
• Bone marrow. Another cytokine, Granulocyte Colony Stimulating Factor (G-CSF) which is released by macrophages, endothelium and fibroblasts at the site of the infection, stimulates the bone marrow to produce and release more neutrophils to help resist the infection.
Chronic changes Within days of infection cytokines such as TNF have metabolic effects, promoting the breakdown of proteins and fat to provide energy. TNF also suppresses the appetite causing anorexia. Over weeks this results in wasting of muscles and weight loss leading to cachexia. Suppression of bone marrow function may cause a normochromic, normocytic anaemia of chronic infection. Catastrophic effects In acute severe infections such as septicaemia or severe malaria, massive amounts of TNF and other cytokines are released. This can cause: • Inhibition of mycocardial contractility and dilatation of blood vessels resulting in shock • Suppression of the bone marrow and a fall in circulating lymphocyte numbers (lymphopenia) • Activation of the coagulation system and intravascular thrombosis
References Use the textbooks in your Tutorial Room

1.08 – A question of communication // Tuberculosis 34
Optional references Available in Medical Library: see Library Catalogue • An overview of non-specific immunity:
o Roitt I, Brostoff J, Male D, eds. Adaptive and non-specific immunity. In: Immunology. (4th ed.) London: Mosby, 1996; chapter 1. (Current edition: Male D et al, 7th Ed, 2006, Chap 1 and 6)
• A description of the cytokines responsible for the systemic response to infection: • Abbas AK, Lichtman AH, Porter JS. Cytokines. In: Cellular and Molecular Immunology. (5th ed.)
Philadelphia: WB Saunders, 2003; chapter 11. Also Chap 12, Innate Immunity.
Author: Professor Warwick Britton, Medicine
1.08 – A question of communication // Tuberculosis 35
2. Structure of the respiratory tract General Objectives • To understand the general functions, and name the parts, of the respiratory tract. • To describe the location and extent of parts of the respiratory system. The respiratory tract is divided into upper and lower parts. The upper respiratory tract comprises nasal cavity, pharynx and larynx. The lower respiratory tract comprises trachea, lungs and pleura. The respiratory system can also be divided into a conducting part that warms, moistens and filters air, and conducts it to the lungs, and a respiratory portion for gaseous exchange. In addition to its respiratory function, the larynx functions in phonation. Air passes through the external nares or nostrils into the nasal cavity, which is divided into two halves by the nasal septum. On the lateral walls, shelves of thin bone covered with mucous membrane called conchae project into the nasal cavity. They create air turbulence to increase contact between air and mucosa and increase the surface area to warm, moisten and humidify air. Structures draining into the nasal cavity include the nasolacrimal ducts draining tears from the eyes and the air-filled paranasal sinuses. Olfactory mucosa is located in the upper third of the nasal cavity. Inspired air flows from the nasal cavity to pharynx then larynx. The auditory tubes open into the nasopharynx on either side allowing drainage and air pressure equilibration of the middle ear. The pharyngeal tonsils are located in the roof and posterior wall of the nasopharynx and when inflamed and swollen (adenoids) may obstruct the nasopharynx. The larynx connects pharynx to trachea and comprises a cartilaginous framework that prevents the airway from collapsing. It acts as a guardian of the air passages (especially during swallowing) and is important in vocalisation. The vocal folds move widely apart in deep inspiration, vibrate together in phonation and are held tightly together when the breathe is held e.g., prior to coughing or sneezing or when lifting. When swallowing, the larynx rises and the flexible epiglottis buckles over the laryngeal inlet like a lid. This routes food into the laryngopharynx and oesophagus. The trachea is a long, flexible fibromuscular tube (10-12 cm) supported by cartilage. It lies in the lower neck and mediastinum and is kept patent by C-shaped hyaline cartilage rings. The gap in the cartilage posteriorly allows for expansion of the oesophagus when swallowing. Fibroelastic tissue between the cartilaginous rings allows the trachea to stretch and recoil with movements of the diaphragm. Below the level of the sternal angle, the trachea divides into two primary (principle, main) bronchi, which pass to each lung. The right is shorter, wider and more vertical, consequently inhaled objects are more prone to lodge in the right side of the bronchial tree. Repeated branching of the bronchi and associated vessels of the lungs forms the substance of each lung. Primary bronchi divide into secondary or lobar bronchi (3 on the right, 2 on the left), then to tertiary or segmental bronchi. Bronchi continue to divide until no cartilage remains in the walls, now called bronchioles (<1-1.5 mm diameter). The terminal air sacs of the bronchial tree are named alveoli; each is surrounded by a network of capillaries. Gaseous exchange occurs between the thin walls of the alveoli and capillaries. Alveoli first appear in the walls of respiratory bronchioles; the respiratory portion of bronchial tree is therefore defined as commencing at this level. The two lungs, each with its pleural sac, occupy all but the central area (mediastinum) of the thoracic cavity. The right lung is larger. It is shorter, because of the liver below, but wider because the heart and pericardium bulge more to the left. The left lung is divided into 2 lobes by an oblique fissure and is characterised by a cardiac notch and lingula on the upper lobe. An oblique and horizontal fissure divide the right lung into 3 lobes (upper, middle, lower). Structures enter and exit each lung through the hilum. These include the bronchi, pulmonary and bronchial vessels, lymphatics and nerves (autonomic and afferent). Parietal pleura lines the thoracic walls, diaphragm and mediastinum. From the mediastinum it reflects onto the lung surface where it is renamed visceral pleura. A small volume of pleural fluid in the pleural cavity facilitates movement of each lung, and ensures that the surfaces cling together, a condition that is essential for normal breathing. Note that respiratory mucosa (ciliated, pseudostratified, columnar epithelium) has an important cleansing action on the respiratory tract. It is found in the nasal cavity, sinuses, nasopharynx, larynx, trachea and bronchi. A mucous layer traps dust and microorganisms, and the 'mucous blanket' is moved by ciliary action toward the throat (pharynx) to be swallowed. Smoking affects the ciliary action in the lower respiratory tract and reduces

1.08 – A question of communication // Tuberculosis 36
mucous elimination from the lungs. Also note that the lung tissue has a rich lymphatic supply for removal of excess fluid and particulate matter.
References Use the textbooks in your Tutorial Room Online • Anatomy glossary - http://www.anatomy.usyd.edu.au/glossary • Online Wilson Museum of Anatomy - http://gmp.anatomy.usyd.edu.au/wilson_henle/museum/ • Wilson bottles: 374 (right lung), 380 (left lung), 226 and 379 (lungs in situ)
Author: Ms Deborah Bryce, Anatomy and Histology
1.08 – A question of communication // Tuberculosis 37
3. Chronic inflammation Sequelae of acute inflammation There are a number of possible sequelae of an acute inflammatory response. • If the initial injury was minor, leading to a modest exudative response, and if any associated contamination
with microorganisms was rapidly controlled by phagocytes, then the lesion may resolve. Fibrin is degraded and exudate fluid reabsorbed via the lymphatics, leaving the affected tissue in its original state.
• If injury was minor, but a substantial amount of fibrin was deposited, then the exudate may be subjected to organization, or acute healing by fibrous repair. Here, macrophages degrade the fibrin and fibroblasts produce collagen, giving rise to fibrous tissue acutely.
• Where a greater degree of damage was sustained, then there will be healing, which consists of tissue regeneration, longer-term fibrous repair, or (most commonly) a combination of these two processes.
• The presence of pyogenic microorganisms will provoke the formation of pus. • Finally, in a small minority of lesions, the stimulus may be persistent and of a sort that leads to a chronic
inflammatory reaction. Chronic inflammation is a delayed, prolonged response taking two major forms: one characterised by the presence of substantial numbers of macrophages and lymphocytes in the affected tissue (chronic granulomatous inflammation), and a second characterised by large numbers of polymorphonuclear leukocytes (chronic suppurative inflammation). It is less uniform than acute inflammation. However, continuing destruction and repair of normal tissue are always seen in chronic inflammation. Chronic inflammation The four invariable characteristics of chronic inflammation are: • Persistence (chronicity) • Cellular infiltration • Destruction of normal tissue • Formation of fibrous tissue In some circumstances, chronic inflammatory reactions may seriously impair organ function and be life-threatening. Chronic suppurative inflammation This pattern occurs when the persistence of certain micro-organisms, or some types of foreign material, or modified host tissue, lead to the continuing recruitment of neutrophils to the area of the lesion. The usual patterns are chronic ulcer or abscess. The latter consists characteristically of a central area of purulent necrosis surrounded by a capsule of fibrous tissue. Typically the lesion expands until it ruptures, collapses and is repaired with fibrous tissue. Chronic granulomatous inflammation Macrophages (often in differentiated forms), lymphocytes, fibroblasts and new blood vessels are characteristic of this type of destructive reaction. Cytokines are important in the maintenance and growth of such lesions. There are 3 major sub-forms of this reaction. The first is caused by certain types of foreign body, e.g. indigestible sutures that have been left in place. Several unusual forms of macrophage are characteristically seen, for example 'epithelioid cells', and multinucleate 'giant cells' which are formed by the fusion of epithelioid cells. The fibrotic reaction is diffuse throughout the lesion. The second (often called the 'immune type' granuloma) is a reaction to the presence of certain types of micro-organism, particularly those that can live within cells such as macrophages. Epithelioid and giant cells also are seen in this type of lesion. The fibrotic reaction is often capsular, leading to a 'walling off' of the lesion. This pattern may be seen in tuberculosis or leprosy. The third form has some similarities to the immune type, but the aetiological agents are as yet unknown. An example is sarcoidosis.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue

1.08 – A question of communication // Tuberculosis 38
• Kumar V, Abbas, AK, Fausto, N. Pathological basis of disease. (7th ed.) Philadelphia: WB Saunders Co, 2005.
o Most relevant: part of Chapter 2 (pp 78-85). ���Related: Chapters 1 (pp 4-32), and 3 (pp 87-118). • Kumar V, Abbas AK, Fausto N, Aster JC. Pathological basis of disease. (8th ed.) Philadelphia: Saunders
Elsevier, 2010. o Most relevant: part of Chapter 2 (pp 70-75). ���Related: Chapters 1 (pp 5-38), and 3 (pp 79-108).
Museum • Preserved specimens. ���It is suggested that students examine and discuss these specimens in groups. They
have been chosen to illustrate the different patterns of chronic inflammation. Photographic images of the specimens are available on line. However, it is preferable to examine the actual specimens in the Pathology Museum.
o Chronic gastric ulcer - specimen 34.2573.3 (13462B) o Osteomyelitis in femur - specimen 9.527.1 (13226) o Pulmonary tuberculosis - specimen 24.573.1 (15118) o Sarcoidosis in spleen - specimen 43.579.1 (2379) o Foreign body reaction in peritoneum - specimen 36.94.1 (1035)
• Microscopic specimens. ���The following images are available on-line: o Foreign body granuloma (peritoneum) - slide A8-2 o Tuberculous granuloma (lung) - slide H14-1 o Sarcoid granuloma (lymph node) - slide A49/1
Some specimens will be discussed in a Theme Session.
Author: Professor Nicholas Hunt, Bosch Institute
1.08 – A question of communication // Tuberculosis 39
4. Immune response to mycobacterium Macrophages and T cells respond to primary infection Mycobacterium tuberculosis is spread by aerosol droplets and the bacilli are deposited in the terminal alveoli. There are then three stages in the host response. Mycobacteria resist killing Mycobacteria have a number of methods of resisting killing. This has two consequences: • Persisting antigen stimulates the release of cytokines, particularly tumour necrosis factor which promotes
granuloma formation and chronic inflammation. Chronic infection may lead to a mild normocytic, normochromic anaemia.
• Small numbers of viable mycobacteria persist in a 'dormant' phase, and continuing lifelong 'surveillance' by competent CD4 T cells is required to prevent their growth.
Reactivation of infection Later in life the dormant infection may be reactivated if the T cell immunity wanes. You should identify some of the factors which can cause this. The release of macrophage products, including cytokines such as TNF, leads to tissue death, caseous necrosis typical of TB, and cavities in the lungs. Detection of immunity to TB The detection of mycobacteria-specific T cells can be used as indirect evidence of past TB infection. This is traditionally done by a Tuberculin (Mantoux) skin test which detects a delayed type hypersensitivity (DTH) response to mycobacterial proteins. You should understand how this is done and what it means. More recently the presence of M. tuberculosis-specific T cells secreting Interferon-gamma has also been used to determine past infection. Human Immunodeficiency Virus (HIV) and Tuberculosis HIV infection is the greatest single risk factor for TB. Patients with HIV are more liable to both primary M. tuberculosis infection and reactivation of TB infection. Why is the CD4 T cell susceptible to infection with HIV and how does this predispose to TB? Are there differences in the patterns of TB in HIV infected subjects? 1. The mycobacteria are phagocytosed by alveolar macrophages which are organ-specific scavenger cells.
Other macrophages are attracted to the site to form a collection of cells in which the mycobacteria mutiply slowly. In addition mycobacteria are phagocytosed by lung dendritic cells (DCs) (the sentinels which are activated by mycobacterial products to undergo maturation and express costimulatory molecules and secrete cytokines to become functional antigen presenting cells.
2. After 1-2 weeks the DCs containing mycobacteria migrate to the draining lymph nodes in the hilum of the lung. The bacteria are partially degraded in the phago-lysosome and short peptides from digested proteins bind to HLA Class II molecules which are expressed on the cell surface. Naive T lymphocytes circulate through lymph nodes and are exposed to the mycobacterial peptides on antigen presenting cells. Antigen-specific CD4 T cells are stimulated to proliferate and form clones of T cells which can recognise mycobacteria-infected cells. The macrophages secrete cytokines such as IL-12 which direct the CD4 T cell to produce pro-inflammatory cytokines, including Interferon-gamma.
3. The mycobacteria-specific T cells then migrate through the efferent lymphatics and then the blood stream to the site of infection in the alveolus. The T cells migrate across the capillary and through their T cell receptor recognise the peptide/HLA complex on infected macrophages. Activated T cells secrete cytokines such as Interferon-gamma to stimulate bacterial killing mechanisms in the macrophages. Some infected cells are killed in the process and the mycobacteria released are engulfed by fresh activated macrophages which kill the organisms. The collection of macrophages and T cells forms a granuloma which over 6-8 weeks limits the infection.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • A general introduction to the processes of cell mediated immunity.
o Abbas AK, Lichtman AH. Basic Immunology, Chap 5 & 6. (2n ed) 2005. Philadelphia: WB Saunders
• A detailed account of cells and cytokines responsible for protective immunity. o Abbas AK, Lichtman AH. Immunity to microbes. In: Cellular and Molecular Immunology. (5th
ed.) Philadelphia: WB Saunders, 2003; Chapter 15.

1.08 – A question of communication // Tuberculosis 40
o Abbas AK, Lichtman AH. Effector mechanisms of Cell-mediated Immunity. In: Cellular and Molecular Immunology. (5th ed.) Philadelphia: WB Saunders, 2003; Chapter 13.
• A clear description of delayed type hypersensitivity and its clinical significance. o Warwick Britton. Hypersensitivity-Type IV. In: Male DI, Brostoff J, Roth DB, Roitt I, , eds.
Immunology. (7th ed.) London: Mosby, 2006; Chapter 26
Author: Professor Warwick Britton, Medicine
1.08 – A question of communication // Tuberculosis 41
5. TB: the global perspective TB as a global health problem TB is a devastating disease that has long been part of human history. It currently infects about 30% of the world's population, most of whom live in low or middle income countries. In fact, 95% of TB cases occur in developing countries. The current global prevalence of TB is 20 million cases which amounts to 350 cases per 100,000 population. Every second someone is newly infected with TB and someone dies of TB every 15 seconds. TB is the second biggest infectious disease killer worldwide, second only to HIV/AIDS. If control of TB is not strengthened, it is estimated that by the year 2020 nearly 1 billion people will become newly infected with TB, 150 million people will become unwell, and 36 million people will die. TB is also the leading killer of women aged 15 to 44, surpassing all causes of maternal mortality. There are 22 countries that account for 80% of the world's TB and which are designated to be 'high burden countries'. These countries, listed in order of global rank by estimated number of cases are: India, China, Indonesia, Bangladesh, Nigeria, Pakistan, South Africa, Philippines, Russian Federation, Ethiopia, Kenya, Democratic Republic of Congo, Viet Nam, United Republic of Tanzania, Brazil, Thailand, Zimbabwe, Cambodia, Myanmar, Uganda, Afghanistan, and Mozambique. Refer to the maps in the WHO report, 2002: http://www.who.int/tb/publications/global-report/2004/en/annex5.pdf Why has this happened? TB is a treatable disease, but despite this fact, disease rates have been continuing to increase globally. As a result of this trend, TB was declared a global emergency in 1993 by the World Health Organization. Major reasons for the global increase in the TB burden are: • Lack of attention to the disease resulting in decreased funding to TB programs and decreased TB services • HIV: for HIV + people the risk of reactivation of TB is 10% per year compared to 10% per lifetime for
HIV- people. Therefore, increasing rates of HIV infection throughout the world have a great effect on the TB epidemic.
• Breakdown in public health infrastructure e.g. due to war, political upheaval • Demographic changes: in developing countries disease rates are highest in the adolescent and young adult
population. This age group has increased in size recently because the decline in childhood mortality rates has been more rapid than the decline in birth rates over the last few years.
• Poverty: the number of less developed countries has doubled in the last 10 years • Population movement: due to armed conflict, labour migration and increased travel and trade. It is
estimated that up to 50% of the world's refugee population is infected with TB. • MDR-TB: multi-drug resistant TB requires longer and more expensive treatment - this is especially difficult
in developing countries TB close to home The Western Pacific region, of which Australia is part, contains 30% of the world's TB sufferers. In addition, southeast Asia carries the biggest burden of TB in terms of numbers with about 3 million cases of TB occurring per year. These statistics emphasise the importance for Australia to have a global vision for TB control. With frequent international travel and trade, combined with immigration to Australia, poor tuberculosis control in other countries has the potential to adversely affect TB control in Australia. TB in Australia TB is currently well controlled in Australia and we are fortunate to have one of the lowest rates of TB in the world. In addition, rates of MDR-TB are low as is HIV/TB co-infection. Rates of TB began to fall in Australia at the end of the 19th century with improving living standards. Rates fell further after the success of the post-World War II National TB Campaign and the low rate has since been maintained. However, specific subgroups of the Australian population such as Indigenous Australians and persons born overseas have rates much higher than the rest of the population. Over 80% of cases of tuberculosis seen in Australia are in foreign born people, with the highest rates in people born in Asia. In 2001, the overall incidence rate for the Australian population was 5.1 cases per 100,000. However the rate for people born overseas was 19.3 cases per 100,000, for Indigenous Australians 9.8 cases per 100,000, and for non-indigenous Australian born persons 1 case per 100,000.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue
1.08 – A question of communication // Tuberculosis 42
Sources of Global Health Data • The WHO website:
o www.who.int/health_topics/tuberculosis/en/ (tuberculosis) o www.who.int/health_topics/idindex.htm (infectious diseases) o www.who.int/csr/don/en (disease outbreaks) o globalatlas.who.int/ (global atlas of disease)
• The Stop TB Partnership (hosted by WHO): o www.stoptb.org/
• Worldbank: o devdata.worldbank.org/hnpstats/
• UNICEF - Monitoring and statistics o www.unicef.org/statis
Additional References Communicable Diseases Network Australia. National Strategic Plan for TB Control in Australia Beyond 2000. www.health.gov.au/internet/wcms/Publishing.nsf/Content/cda-pubs-other-tb_plan.htm
1.08 – A question of communication // Tuberculosis 43
6. Outbreak: surveillance & control What is surveillance? Surveillance is an essential part of disease control and has been defined by the WHO as the 'ongoing systematic collection, collation, analysis and interpretation of data, and the dissemination of information to those who need to know in order that action may be taken'. The objectives of surveillance systems are listed below: • Measure occurrence or burden of disease • Describe the natural history of disease • Detect trends • Identify outbreaks • Identify at risk populations • Evaluate and guide control measures • Stimulate and guide research priorities • Guide policy decisions Surveillance can be described as passive or active. Passive surveillance involves notification of cases of disease in symptomatic individuals who present to heath services. Active surveillance on the other hand, involves actively looking for disease cases. Surveillance systems most commonly use passive surveillance as it is less expensive and easier to perform. However, it has the disadvantage of underestimating the total disease burden. This is because only a small proportion of people with disease will go on to have a confirmed diagnosis that will be notified to the relevant authorities. This concept is demonstrated in Figure 1 "The communicable disease surveillance pyramid" shown here - www.health.gov.au/internet/wcms/publishing.nsf/Content/cda-pubs-cdi-2003-cdi2701-htm-cdi2701a6.htm Active surveillance, although more expensive, has the advantage of being able to provide a more complete picture of disease burden and is often used during epidemics. Sentinel surveillance is another method that can be used to collect information about diseases. It involves the selection of certain health providers/locations that will report detailed information about certain conditions. The information from this small sample can then be used to estimate disease burden and trends for a larger population. There are a variety of surveillance systems in Australia that are listed below. The National Notifiable Diseases Surveillance System (NNDSS) has a list of 55 diseases that are notifiable by law to the relevant State or Territory health authorities. The States and Territories then report this data to the Commonwealth every 2 weeks. Surveillance of clinical cases • National Notifiable Diseases Surveillance System (NNDSS) • HIV/AIDS surveillance • Australian Paediatric Surveillance Unit (APSU) • OzFoodNet Laboratory surveillance • HIV/AIDS surveillance • National Influenza Surveillance Scheme • Australian Gonococcal Surveillance Programme • LabVISE - Virology and Serology Laboratory Reporting Scheme • National Enteric Pathogens Surveillance System • Australian Meningococcal Surveillance Programme • Australian Rotavirus Surveillance Programme • OzFoodNet • National Mycobacterial Surveillance System • Australian Mycobacterium Reference Laboratory Network Sentinel surveillance • Australian Sentinel Practice Research Network (ASPREN) • Sentinel Chicken Surveillance Programme • National Influenza Surveillance Programme Vaccine preventable diseases • National Notifiable Diseases Surveillance System (NNDSS) • Australian Childhood Immunisation Register (ACIR)
1.08 – A question of communication // Tuberculosis 44
Tuberculosis Surveillance Tuberculosis is a notifiable disease in Australia under the National Notifiable Diseases Surveillance System (NNDSS). In addition to the mandatory reporting of clinical cases, laboratories that isolate the tubercle bacillus from specimens are also required to report this by law along with the presence of any antibiotic resistance. Much of the screening, investigation and management of TB is carried out in NSW through its network of 29 chest clinics. These chest clinics are required to provide free investigation and treatment of TB regardless of Medicare or residency status. An understanding of the natural history of TB is important for surveillance of this disease. Following infection with the TB bacillus, 90% of individuals will develop what is known as latent TB or asymptomatic infection. Such individuals are not unwell, nor are they infectious to others. They have about a 10% chance of developing active TB in their lifetime. Early detection of people with asymptomatic TB infection enables them to receive prophylactic anti-TB chemotherapy that will decrease their chances of later developing disease. The other 10% of those infected with TB will go on to develop active disease. Such individuals are symptomatic and if they have active pulmonary TB, are capable of spreading the disease to others. Both passive and active surveillance are used in TB control. Passive surveillance is used for individuals with active TB that present to health services. Active surveillance, using the Mantoux skin test, is used in the situations below and often identifies individuals with asymptomatic infection. a. Contact tracing - of any persons in close contact with an active case of TB. b. Immigrants - are referred to a chest clinic immediately on arrival if they have had previous TB treatment or
an abnormality suspicious for active TB on the pre-migration chest X-ray. Other immigrants are referred for assessment within 6 months.
c. Persons who are HIV positive - should be screened for TB with the Mantoux test before immunosuppression develops (preferably at diagnosis) as immunosuppression increases the chances of a false negative result.
d. Health Care workers and health care students - should be screened on commencement of employment and on exit by the Mantoux test. For those working in high risk areas, 12 to 24 monthly routine screening is recommended.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Information about NNDSS:
http://www.health.gov.au/internet/wcms/publishing.nsf/Content/Nationally+notifiable+diseases+%28NNDSS%29-1
• CDC. Public Health Surveillance Slide Set: www.cdc.gov/epo/dphsi/phs/overview.htm • Communicable Diseases Australia Website: http://www9.health.gov.au/cda/Source/CDA-index.cfm • Australia's Notifiable Diseases Status 2001: www.health.gov.au/internet/wcms/publishing.nsf/Content/cda-
pubs-cdi-2003-cdi2701-htm-cdi2701a6.htm • Surveillance systems reported in CDI, 2003: www.health.gov.au/internet/wcms/publishing.nsf/Content/cda-
pubs-cdi-2003-cdi2701-htm-cdi2701l.htm
Author: Heather Gidding, Paediatrics and Child Health
1.08 – A question of communication // Tuberculosis 45
7. Health System Structure: Access for Immigrants Access to public health care in Australia (Medicare) People who reside in Australia (except Norfolk Island) are eligible for Medicare if they hold Australian or New Zealand citizenship, they have permanent residency or have applied for permanent residency (restrictions apply to persons who have applied for a parent visa). Migration programs and Australian policy Applications for permanent residency to Australia can be made under the 'Migration Program' (business people, special skills, employer-sponsored, family etc) or via the 'Humanitarian Program' (off-shore and on-shore). Temporary visas to live and work in Australia for a limited period of time can be granted for students, professionals and retirees. Temporary residents are not entitled to public health care (Medicare) but Australia does have reciprocal health agreements with a number of countries (Finland, Italy, Malta, the Netherlands, New Zealand, Sweden, the United Kingdom and the Republic of Ireland). Health requirements for visitors and overseas students in Australia All visitors to Australia are required to declare their health status on their visa application form. A medical report may be required in the case of people over 70 years, a parent of an Australian staying more than 6 months, a person likely to enter a healthcare or classroom environment, someone known or suspected to be suffering from a medical condition or someone intending to stay more than 3 months and who has recently visited a country with a very high risk rate of tuberculosis (TB). (Very high risk countries include Argentina, Bangladesh, Brazil, Chile, China, Federal Republic of Yugoslavia, Hong Kong, India, Indonesia, Korea, Malaysia, Pakistan, Papua New Guinea, Philippines, Portugal, Russia, Singapore, Sri Lanka, South Africa, Vietnam, Zimbabwe). Health requirements on application for Australian temporary or permanent residency When applying to immigrate to Australia a health examination is required. Before being given a permanent or temporary visa, individuals must satisfy the 'Health Requirement'. All applicants are asked to undergo a medical examination, a chest X-ray if 11 years and older and an HIV/AIDS test. Tuberculosis and the health requirement Tuberculosis is the only medical condition specifically mentioned in migration legislation as precluding the issue of a visa. Opportunity is given to enable an applicant to undergo treatment in most cases. The World Health Organisation has declared TB to be a global epidemic and the current Australian Health Requirements are one strategy to reduce the public health risk of this communicable disease. Applicants with a chest X-ray showing possible evidence of TB are asked to undergo further testing. If found to have untreated or active TB they are asked to complete a course of treatment and undergo further testing on completion. Non-active TB cases are asked to sign an undertaking to present for monitoring within their state or territory health service. Health services for culturally diverse Australian residents There are a number of services that cater specifically for people from culturally diverse backgrounds. Publicly funded programs and services within the NSW Health System are well described in the booklet " Multicultural Health Services and Programs in NSW (NSW Health) " - PDF. As this document describes, these programs have been developed to promote equal access to healthcare regardless of ethnicity and to provide healthcare that recognizes the cultural diversity of the Australian community. The Primary Health and Community Care Branch of the NSW Health Department is responsible for multicultural health. Of the seventeen area health service authorities in NSW, ten of these employ dedicated coordinators or directors of multicultural health. In addition to this there are six Health Care Interpreter Services (Central Sydney, Northern Sydney, South Western Sydney, Western Sydney, Illawara and Hunter). They provide professional interpreter services free of charge in over 50 languages to people using public health services around the state. They will also do translations of up to 50 words at no cost. Other publicly funded multicultural workers in some areas include: • Multicultural health workers - they help people from culturally and linguistically diverse backgrounds to
access health services. This may include referral, group work, health education and community development.
• Multicultural staff development officers - these officers train staff in cross cultural skills • Bilingual counselors - mainly work at community health centres and provide mental health assessment,
counseling, consulting and referral. • Multicultural health promotion officers - develop and evaluate health promotion programs for people of
culturally and linguistically diverse (CALD) backgrounds
1.08 – A question of communication // Tuberculosis 46
• Multicultural aged care workers - advise on and improve quality of care for older people from CALD backgrounds and help them to access the right services and facilities
• Ethnic obstetric liaison officers - provide antenatal and postnatal education and support for women from CALD backgrounds
• Multicultural Health Liaison Officers - liaise with consumers from CALD backgrounds and health services. They also provide cultural awareness education and support for health professionals and provide information and education to consumers.
• Bilingual Community Educators - recruit people from their own communities to provide education and support
• Sessional Bilingual Health Workers - provide education and information on topics such as Drug and Alcohol, Womens Health and Child Protection.
NB: Not all of these positions will be available in each area health service. Other health programs that you may wish to read more about include: • NSW Multicultural Health Communication Service • Transcultural Mental Health Centre • Transcultural Aged Care Service • NSW Refugee Health Service • Multicultural HIV/AIDS and Hepatitis C Service • Service for the Treatment and Rehabilitation of Torture and Trauma Survivors (STARTTS) • NSW Education Program on female Genital Mutilation • Drug and Alcohol Multicultural Education Centre • Thalassemia Society of NSW • FPA Health Multicultural Services • Immigrant Women's Health Service • Sydney Indo-Chinese Community Refugee Youth Support Group
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Department of Immigration and Multicultural and Indigenous Affairs: Frequently Asked Questions: Health
Examinations http://www.immi.gov.au/allforms/health-requirements/index.htm • Australian Government: Health Insurance Commission: About Medicare
http://www.medicareaustralia.gov.au/ • NSW Multicultural Health Communication Service http://www.mhcs.health.nsw.gov.au/ • Multicultural Health Services and Programs in NSW (NSW Health)
Author: Associate Professor Lyndal Trevena, School of Public Health
1.08 – A question of communication // Tuberculosis 47
8. Health and its determinants: Ethnicity Ethnicity and culture Thinking back to the earlier Learning Topic "Health & its determinants: Nutrition" you will recall that we discussed nutrition as an example of a health determinant. Similarly, 'ethnicity' and 'culture' can play an important part in determining the health of a population. Ethnicity generally refers to the racial background of an individual and could be considered a genetic factor determining health. Ethnic groups obviously share a common culture, which may also affect lifestyle and behavioural factors through diet, attitudes, beliefs, religious practices and customs. Measuring ethnicity There are a number of ways that ethnicity can be measured. Each measure has its own limitations and relevance. For example, language spoken at home may be the most relevant measure if considering access to services. The 2001 Census attempted to get a better understanding of a person's ethnic background by asking about ancestry. This included the person's birthplace as well as their parents' place of birth. It showed that the number of people indicating Australian ancestry increased from 3.4 million in 1986 (20% population) to 6.7 million (35.5% population) in 2001. 22.1% of the population recorded multiple ancestries in 2001 which was an increase from 12.6% in 1986. As described in "Health System Structure: Access for immigrants" learning topic, Australia has quite stringent immigrant health requirements and results in most migrants having better than average health, known as 'the healthy migrant effect'. On the other hand, some migrant groups, minorities and refugees can become socially isolated and therefore susceptible to ill health. On average, Australian immigrants have a lower mortality than their Australian-born counterparts but this difference decreases the longer they have lived within Australia. It is important therefore, not only to consider country of birth but also the duration of Australian residency in determining health effects. Overseas-born Australians and their health In the 2001 Census of Population and Housing the majority of people counted in Australia were Australian-born (71.8% or 13,629,685 people). This was slightly less than the 73.9% in 1996 Census. People born in the United Kingdom represented 5.5% (1,036,245 people) of the population, a decrease from 6.0% in 1996. English was the only language spoken at home by 79.1% of the population, a decrease from 81.4% in 1996. Of those people who spoke a language other than English at home, the highest proportion (1.9% or 353,605 people) spoke Italian, a decrease from 2.1% in 1996.1 In other words about 29% of Australians were born overseas. Mortality patterns vary substantially between different overseas-born groups. For example, most migrants have a lower rate of death from cardiovascular disease than those who are Australian-born. This difference, however, tends to level off the longer people live in Australia. Death from lung cancer and a greater level of physical inactivity are more commonly seen in those born in the UK and other European countries. Cervical cancer death rates are higher in Asian-born women and Australian-born men have the highest prostate cancer mortality rate. Skin cancers are more common in those born in Australia than any other country in the world.2 A special note on finding information about how common a characteristic or condition is within the community You may notice that in this and other learning topics within this block we have been considering how common a characteristic or condition is within a specified population group (eg children, elderly Australians etc). When looking for good quality estimates of the frequency (ie prevalence or incidence) of a characteristic or condition you should try to access information that fulfills the following criteria: • Includes a representative sample of the population of interest (eg a Census which counts 'everyone', or a
large, randomly-selected survey sample). • Uses accurate measurement tools (eg validated questionnaires or standardized measures) • Has been conducted by a reputable and independently reviewed source (eg Australian Institute of Health &
Welfare, Australian Bureau of Statistics, World Health Organisation, NSW Health Department Disease Surveillance reports, State Cancer Registry Reports etc)
• Reports on 95% confidence intervals for prevalence and incidence estimates • Uses a cross-sectional design for prevalence estimates and a cohort design for incidence
References
1.08 – A question of communication // Tuberculosis 48
1. Australian Bureau of Statistics - Census of Population and Housing: Selected Social and Housing Characteristics Publication 2015.0
2. Australia's Health 2004. www.aihw.gov.au/publications/index.cfm/title/10014
Author: Associate Professor Lyndal Trevena, School of Public Health
49
1.09 – MRS. NEWMAN’S INDIGESTION // ACUTE CARDIAC PRESENTATION Learning objectives Detailed organisation of the brachial plexus and its major branches and innervations. The signs and symptoms after lesion to different parts of the plexuses (e.g. roots) and the major nerves of the upper limb (e.g. median, ulna, radial).
Anatomy
The appearance of a normal artery and vein, the appearance of an atherosclerotic plaque in a medium sized vessel, some of the complications of atherosclerosis and finally, the appearance of a myocardial infarction at ~1 week.
Pathology
• To appreciate the possible outcomes of acute inflammation • To understand the aetiologies of chronic inflammation • To be cognisant of the similarities and differences between the different forms of
chronic inflammation at the cellular level
Pathology
The applications of antibodies in clinical immunology. Infectious Diseases Measures taken to prevent infection, including: quarantine, hygiene and sanitation, vector control and prevention of exposure to vectors, immunisation and the eradication of infectious diseases.
Infectious Diseases
Bacterial culture methods, virus isolation by cell culture, rapid antigenic detection methods, molecular diagnosis and finally, serology.
Infectious Diseases
Antimicrobial therapy and the emergence of resistance, sterilisation and disinfection, immunisation, surveillance and vector control, public health engineering and finally, prevention of zoonotic infections and overall food safety.
Infectious Diseases
The use and abuse of legal and illicit drugs for non-medical purposes. What is known about the associated dependency and psycho-active properties of these drugs.
Pharmacology
The rationale for the use of biochemical tests, especially troponin, in the diagnosis of acute myocardial infarction.
Biochemistry
The rationale, purposes and data sources for disease surveillance and apply them to the investigation of outbreaks.
Public Health
List key health indicators (mortality, morbidity, population distribution) in Indigenous health in Australia. Explain strengths and weaknesses of data State the number of Australians who identify as Indigenous and their distribution across Australia (urban, rural, remote and very remote).
Indigenous Health, Public Health
At the end of the Medical Program (on graduation), students should be able to recognise the strengths and limitations of available data used as key indicators of Indigenous health.
Indigenous Health
At the end of the Medical Program (on graduation), students should be able to list key health indicators, including characteristics of mortality and morbidity, and population distributions specific to Indigenous Australians.
Indigenous Health
On graduation students should be able to state the approximate number of Australians who currently identify as Aboriginal/Indigenous, their distribution throughout Australia and the percentages of this population that live in urban, rural and remote areas.
Indigenous Health
The new and highly practical approach to human ageing; that is, the distinction between successful and unsuccessful ageing and how this is brought about.
Geriatric Medicine
The epidemiology of genetic disorders, the levels of treatment and the significance of triplet mutations. The ethical dilemmas in treatment of genetic disorders, and finally, the basic prenatal genetic diagnostic strategies.
Genetic Medicine
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 50
1. Structures of the chest Introduction The thorax lodges the heart, lungs, major vessels and nerves and the trachea and oesophagus. Its skeletal framework is resilient and expandable and encloses and protects upper abdominal organs as well as thoracic organs. It comprises the sternum, ribs and costal cartilages and thoracic vertebrae. Thoracic Cavity and Mediastinum The thoracic cavity communicates with the neck and abdominal cavity, through the thoracic inlet and outlet respectively. The diaphragm closes the thoracic outlet and forms the boundary between the thoracic and abdominal cavities. Movements of the diaphragm and thoracic wall create pressure changes in the thoracic cavity that cause air to move into and out of the lungs and assist venous return to the heart. The thoracic cavity is divided into 2 lateral parts, which contain the lungs and pleura and a median part called the mediastinum. The mediastinum contains the heart, major vessels (pulmonary and systemic), the trachea and oesophagus, and the vagus and phrenic nerves. Pericardium The heart is surrounded by pericardium. The tough, outer fibrous pericardium retains the heart in position and limits acute over-distension of its chambers. It attaches to the roots of the great vessels above and behind and to the diaphragm below. As the diaphragm descends (inspiration), the heart is pulled down and elongated, and as it relaxes and ascends with expiration, the heart becomes more horizontal and bulges laterally. The serous pericardium lies deep to the fibrous pericardium and surrounds the pericardial cavity. The parietal layer lines the inner surface of the fibrous pericardium and the visceral layer invests the heart. The two layers are continuous at the roots of the great vessels. A thin film of fluid in the pericardial cavity facilitates friction-free movement of the heart. Heart The heart is a four-chambered double pump that occupies the middle mediastinum. An obliquely placed septum divides the heart into right and left parts. The right side of the heart receives deoxygenated blood and pumps it to the lungs. The left side receives oxygenated blood from the lungs and ejects it into the aorta. The ventricles are the heart's pumps; the left generates higher pressures and its walls are consequently much thicker than those of the right. Note that atria receive blood from veins and ventricles propel blood from the heart into arteries. The right atrium receives venous blood from: the superior vena cava, which drains head, neck, upper limbs and thoracic cavity; the inferior vena cava, which drains the lower limbs, pelvis and abdomen; and the coronary sinus, which drains the heart itself. The left ventricle pumps blood into the ascending aorta, which gives off left and right coronary arteries that supply the heart. The arch of the aorta gives off arteries that supply the head, neck and upper limbs and the descending thoracic aorta and its continuation supply the thoracic walls and cavity and all structures below the diaphragm. Heart valves allow blood to flow in only one direction. The atrioventricular (AV) valves prevent backflow into the atria during ventricular contraction. The tricuspid (right AV) valve has three cusps and the mitral (left AV) valve has two. The pulmonary and aortic semilunar valves are situated at the base of the pulmonary trunk and aorta respectively. Each possesses three cusps that fill with blood when the ventricles relax and prevent arterial blood from re-entering the heart. Innervation of Heart The heart receives efferent (motor) supply from autonomic nerves. The effect is somewhat akin to an accelerator and brake. Sympathetic fibers arise from T1-4(5) regions of the spinal cord and cause an increase in rate and force of contraction. Parasympathetic fibers arise from the vagus (cranial nerve 10) and primarily slow the heart rate. Visceral afferents (sensory nerves from viscera) are involved in cardiac reflexes. Those subserving pain are stimulated by ischaemia and accumulation of metabolic products. They travel with the sympathetic nerves and enter the spinal cord at T1-4(5) levels. Cardiac referred pain is therefore perceived as arising from the area of skin supplied by spinal cord segments T1-4(5).
References Use the textbooks in your Tutorial Room

1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 51
• Moore KL, Dalley AF, Agur AMR. Clinically oriented anatomy. 6th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006.
Online • Anatomy glossary - http://www.anatomy.usyd.edu.au/glossary • Online Wilson Museum of Anatomy - http://gmp.anatomy.usyd.edu.au/wilson_henle/ (Medical Program
password) • Wilson bottles: 378 anterior (heart and great vessels); 228 anterior (surface markings of the heart). • Prosections are available in the J. T. Wilson Museum of Anatomy - room W401, Anderson Stuart Bldg,
open 8.30 am - 5.30pm. • Netter, Frank. The interactive Atlas of Clinical Anatomy. Summit, N.J.: Novartis, c1997. CDROM is
available in the Medical library (611.00222 32) and Wilson Museum.
Author: Ms Deborah Bryce, Anatomy and Histology

1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 52
2. Mechanisms of pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or an experience described in terms of such damage. Pain is usually associated with the activation of peripheral nerves by a stimulus that damages tissue or has the potential to do so, but the term 'pain' describes both the perception of the nociceptive event and the person’s psychological response to it. Pain is highly subjective, and a person’s experience of and response to pain is strongly influenced by previous experiences, cultural and genetic background, gender and psychological state. The context in which the pain is experienced and the intensity of the noxious stimulus are also important. This can make determining the severity of pain difficult, but untreated pain has significant adverse consequences for the physiological and psychological status of the patient, particularly if pain becomes chronic. Chronic pain represents an enormous personal and social burden with substantial economic implications, and some pain specialists consider pain relief to be a basic human right. Sensory nerves that detect noxious stimuli are nociceptors, and their nerve endings are found in almost all regions of the body. However, there are many more sensory nerves supplying the skin than deeper tissues such as muscle and viscera, which is one reason why pain from events such as heart attacks is relatively poorly localized, and why damage to organs such as the liver can be relatively painless. Nociceptive fibers in the heart project with the sympathetic nerves to the thoracic spinal cord and also via the vagus to the brainstem. Sensory neurons that detect noxious events usually have small diameter axons with little or no (C-/Group IV fibers) myelination and thus they transmit information relatively slowly compared with touch or position sensitive sensory afferents. Activation of nociceptors is often associated with a variety of reflexes such as increased local blood flow, spasm of nearby muscles, changes in blood pressure and dilation of the pupil. Many nociceptors are specialized to detect only noxious events, but some sensory nerves can detect both normal and potentially damaging stimuli. Nociceptors can be activated by a wide range of stimuli including heat, cold, stretching, pressure and chemicals produced by damaged or dying tissue. Mediators present in damaged or inflamed tissue can either directly activate sensory nerve endings or sensitize them to activation by other stimuli. Such mediators include prostaglandins, bradykinin, leukotrienes, serotonin, histamine, adenosine triphosphate (ATP), substance P, protons, and lactate-there are a multitude. Mediators are released from epithelial cells, mast cells, muscle and blood vessels in response to tissue damage or insult (such as ischaemia) and even sensory nerve endings themselves release substance P and CGRP, both of which contribute to ongoing 'neurogenic' inflammation. It is important to realize that each of these molecules is acting at specific receptors on nerve cells, and these receptors are potential targets for analgesics. Inhibition of prostaglandin synthesis is the major analgesic mechanism of drugs such as aspirin. Information from peripheral nerve endings is carried to the spinal cord electrically, so anything that activates nociceptors produces a depolarisation of the nerve ending large enough to generate an action potential which propagates via the sensory nerve to the spinal cord, where it stimulates the release of neurotransmitter onto neurons of the dorsal horn. The membrane potential at which nerve cells begin to fire action potentials is called threshold. Some sensory mediators directly open ion channels to depolarize sensory nerve endings (e.g. protons or ATP) while others change the function of sensory ion channels so that they open more readily. For example, bradykinin and prostaglandins cause an ion channel that detects noxious heat (TRPV1) to open at a lower temperature than normal, so that skin temperature activates nociceptors and thus the inflamed tissue feels tender or painful. Such an exaggerated response to a noxious stimulus is called hyperalgesia. The specific central pathways for nociception and interactions in brain and spinal cord will be considered in later weeks but it is important to remember that a distinction is made between the activation of nociceptors and the experience of the complex sensation, pain. You should also realize that not all painful sensations arise from stimulation of peripheral nociceptors, and pain arising from nerve damage in the central nervous system can be amoung the most intense and refractory to treatment. Patients with visceral pain, such as that associated with a heart attack, often find it difficult to precisely localize the source of the pain. Several factors contribute to such uncertainties including relatively sparse innervation of visceral tissue, the innervation of a relatively large region by branches of a single nociceptive sensory neuron and relatively widespread diffusion of nociceptive mediators into surrounding regions.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue

1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 53
• Up to date definitions of terms related to nociception, pain and analgesia can be found on the web site of the International Association for the Study of Pain (IASP). The IASP website also has a series of short Clinical Updates covering many aspects of pain, from sociological to basic mechanisms.
o http://www.iasp-pain.org/terms-p.html • The initial few sections of the two chapters listed below provide different but complementary introductions
to the subject. Refer also to your medical dictionary or the index of other texts for further definitions of unfamiliar terms.
o Kandel ER, Schwartz JH. Principles of neural science. 4th ed. New York: McGraw-Hill; 2000. Chapter 24. (The perception of pain) [Available as an E-book]
o Thews G, Schmidt RF. Human physiology. 2nd completely rev. ed. Berlin ; New York: Springer-Verlag; 1989. Chapter 10.
• The main reference book describing the underlying science of pain and its treatment is “Wall and Melzacks Textbook of Pain” 5th Edition, Edited by Steve McMahon and Martin Koltzenberg, Elsevier, 2005. Definitely worth a look if you are at interested in the area.
• The activation of nociceptors represents one example of a much broader topic of cell signalling and interactions. The introductory few pages of the chapter below offer a more general account.
o Alberts B. Molecular biology of the cell. 4th ed. New York: Garland Science; 2002. Chapter 15. (Cell Communication) [Available as an E-book]
• An account of the role in inflammation of the mediators referred to above is provided in: o Kumar V, Abbas AK, et al. Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia:
Elsevier Saunders; 2005. [Available as an E-book]
Author: Dr Christopher Vaughan, Kolling Institute of Medical Research
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 54
3. Pathogenesis of arterial disease The heart depends on an adequate supply of oxygenated blood via the coronary artery system. This system must be capable of providing an increased supply to meet the greater demands of the myocardium, for example, during physical exertion. The ability to increase the supply on demand depends greatly upon this arterial system having a uniformly generous lumen free of significant (>50%) narrowing. The most important disorder which impairs the ability of the coronary artery system to supply the heart with adequate blood is atherosclerosis. This is a disease in which the intima and media of arteries undergo progressive focal thickening. The basic abnormality in atherosclerosis is the fibro-fatty plaque. Such plaques contain lipid, fibrous tissue, smooth muscle cells and inflammatory cells such as macrophages. As the plaques grow, they lead to narrowing of the lumen of the artery with reduction in blood flow and a change in flow from laminar to turbulent. One or more coronary arteries with luminal reduction of about 50% or more of their original size may be able to supply the muscle with adequate blood at rest but flow may be insufficient during exercise. The reduced blood flow (ischaemia) may produce angina at this stage without permanent injury to the cardiac muscle. In advanced atherosclerosis, a large plaque may progress rapidly as a result of erosion of its superficial portion (fibrous cap) or a deep oblique crack (fissure). When blood flow changes to turbulent as a result of the local narrowing, the blood cells are displaced from the central or axial part of the stream toward the periphery. Platelets can now come into contact with and adhere to the collagen of the plaque exposed by the ulcer or fissure. Coagulation is initiated and can culminate in total obstruction of the affected artery, the process being referred to as thrombosis or atherothrombosis. Blood flow in that artery ceases totally. A limited amount of blood may still reach the area usually supplied by the obstructed vessel via small branches of neighbouring patent 'collateral' vessels. Nevertheless, the target tissue is undersupplied (ischaemic) and becomes hypoxic. Ischaemia leads to death of myocytes. Necrosis or structural evidence of death follows and within 1-2 days the myocytes exhibit obvious microscopic abnormalities such as loss of nuclei and of cytoplasmic striations. Tissue necrosis due to ischaemia is referred to as infarction. The presence of necrotic tissue stimulates an acute inflammatory reaction, the major aim of which is to remove the infarcted tissue and prepare for its replacement by fibrous scar tissue. This occurs because myocytes are permanent cells and probably cannot regenerate to replace necrotic myocytes. The fibrous scar which replaces the infarct will allow the ventricular wall to retain its integrity but there may be long-term problems for the patient relating to the presence of this scar. Fibrous tissue lacks the contractility of heart muscle and a large scar may lead to reduced ventricular contractile properties. In spite of the ability of the surviving myocytes to undergo compensatory enlargement or hypertrophy in an attempt to retain adequate ventricular function, the replacement of a mass of myocytes by scar tissue is likely to lead to reduced ventricular contractility and decreased efficiency of that ventricle as a pump. Scar may also be a focus for electrical instability, which may result in arrhythmias.
References Use the textbooks in your Tutorial Room Optional references • The textbook by Kumar et al provides coverage of fundamental concepts in Pathology. Cotran et al is
similar in its provision of fundamentals but is a more comprehensive text. The text by Rubin and Farber is comparable with Cotran et al. The text by Stevens and Lowe, while more superficial in its presentation is nevertheless adequate in the coverage of basic concepts. All these texts provide basic correlation of fundamental disease processes and the clinical abnormalities with which they are associated.
• Kumar V, et al. Robbins basic pathology. 8th ed. Philadelphia P.A.: Saunders/Elsevier; 2007. • Kumar V, et al. Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia: Elsevier Saunders;
2005. [Available as an E-book] • Stevens A, Lowe JS. Pathology. 2nd ed. Edinburgh ; New York: Mosby; 2000. • Rubin E, Gorstein F. Rubin's pathology: clinicopathologic foundations of medicine. 4th ed. Philadelphia:
Lippincott Williams & Wilkins; 2005.
Author: Professor David Celermajer, Medicine

1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 55
4. Overview of management Acute myocardial infarction (AMI) remains the commonest cause of death in Australia. The majority of these deaths is secondary to ventricular arrhythmias and occurs within the first few hours of symptoms. People with chest pain should be educated that this pain may be due to a 'heart attack' and that they should present to the closest hospital preferably with ambulance transport. The diagnosis of AMI is made in the hospital emergency department by history, examination and electrocardiogram (ECG). The pain is typically retrosternal, lasts longer than 20 minutes and is unrelieved by sublingual nitrate medications, but an AMI can also present with less typical symptoms. The ECG often shows characteristic abnormalities. Patients are placed on continuous ECG monitoring and an intravenous cannula is inserted to allow rapid delivery of drugs or fluids is inserted. Patients are given oxygen by mask and intravenous narcotics for analgesia. Aspirin is provided as early as possible for inhibition of platelet activity. The usual cause of AMI is an acute thrombotic occlusion of an atheromatous coronary artery. In the absence of an adequate collateral blood supply the myocardium downstream of the coronary thrombosis will infarct unless blood flow can be restored. Infarction occurs over hours and myocardium is potentially salvageable by prompt treatment. The aim is to restore coronary blood flow as quickly as possible. In centres with access to cardiac catheterisation facilities, this can be achieved by emergency (primary) angioplasty and stenting (percutaneous coronary intervention, or PCI) of the affected artery. Alternatively, restoration of coronary blood flow can be attempted by intravenous administration of thrombolytic therapy in the emergency department as soon as the diagnosis is established and any contraindications are excluded. Contraindications include a high risk of bleeding, eg recent surgery, trauma or cerebrovascular accident. Results are best when therapy (either thrombolytic therapy or PCI) is initiated within the first few hours from the onset of chest pain, although some benefits may occur up to 12 hr from onset of symptoms. Commonly used thrombolytic drugs include streptokinase, recombinant human tissue plasminogen activator, and tenecteplase. Patients are routinely prescribed aspirin for the antiplatelet effects. The decision whether to treat with thrombolysis or PCI depends on the patient circumstances and availability of a cardiac catheter laboratory. Most importantly, therapy directed towards restoring coronary flow must be initiated as soon as possible. Following the emergency management of AMI the diagnosis is confirmed by serial estimation of venous blood markers of myocardial injury (troponins or creatine kinase) and serial ECGs. The patient is monitored in a coronary care unit (CCU) for 24-48 hr. During this period there is a particularly high risk of life-threatening arrhythmias, and continuous ECG monitoring by trained staff maximises the chances of successful defibrillation and cardiac resuscitation, if required. Ongoing chest pain may indicate continuing ischaemia and is treated with intravenous narcotics, nitrates and but may require urgent coronary angiography and revascularisation. Myocardial oxygen demand is reduced by bed rest and by drugs such as beta blockers which lower heart rate and these are given to most patients. Left ventricular failure may occur following large or recurrent myocardial infarctions and is managed by inotropic drugs, diuretics and sometimes intraortic balloon pump. Angiotensin converting enzyme inhibitors are useful in the prevention and management of heart failure and can help in ventricular healing or remodeling. Statins are started to lower LDL cholesterol and anti-platelet drugs are continued; all these measures aimed at long-term prevention of recurrent episodes are best initiated early during hospitalisation. During the time in CCU, education and counseling for the patient and their family is initiated. After CCU the patient is ambulated. Any recurrent chest pain is reported. Patients receive dietary advice and counseling to stop smoking. Prior to discharge patients may be stratified into low or high risk groups depending on exercise tolerance, evidence for ongoing ischaemia, left ventricular function and propensity for ventricular arrhythmias. Usual length of hospital stay is 3-5 days and prior to discharge an exercise test may be performed. In selected patients further investigations such as coronary angiography and/or electrophysiology study are indicated. After hospital discharge patients would ideally attend cardiac rehabilitation, with further education and a graduated exercise programme. Risk factors for atherosclerosis, eg blood pressure, lipids, smoking status and metabolic status (e.g. presence of impaired glucose tolerance or diabetes), are assessed and treated. An individual who has had an AMI is at high risk of having a further event, therefore secondary prevention is critical. Long-term treatment with aspirin, statins (LDL cholesterol lowering), ACE inhibitors and beta-blockers are of proven effectiveness, and should be considered for use in all patients.
References Use the textbooks in your Tutorial Room
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 56
Optional references Available in Medical Library: see Library Catalogue • ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction—
Executive Summary. Circulation, 2004 110: 588-636. • AHA/ACC Guidelines for Secondary Prevention for Patients With Coronary and Other Atherosclerotic
Vascular Disease: 2006 Update. Circulation, 2006 113:2363-2372. • Heart and Stroke Facts. A report by the National Heart Foundation of Australia, 2003.
Author: Professor Anushka Patel, The George Institute for International Health
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 57
5. Treatment adherence Controversy exists about whether to use the term treatment 'compliance', or 'adherence', or a completely different term such as 'therapeutic cooperation. 'Compliance' is used more widely although it has an implication of subservience to a health professional who 'knows best'; 'adherence' implies a behavioural response rather than a personal trait. Neither adequately describes the mutual cooperation that characterises optimum interactions between patient and health care professional, especially during the management of chronic illness. Whichever term is used, the concept is defined as "the extent to which a person's behaviour, in terms of taking medication, following diets or executing lifestyle changes, coincides with medical, dental or health advice". Compliance is not the necessarily the end goal and indeed may not always be desirable - for example, when a patient continues to take medication that has serious side effects. Therefore, 'success' of treatment compliance needs to be measured by actual improvements in health ('health gain'), which is a more important outcome measure than just changes in medicine taking or other lifestyle alterations. In order to understand treatment adherence, familiarity with a number of important psychological concepts is essential. The medical or dental practitioner needs to understand how people learn to respond in a certain way and how that behaviour can be changed, how attitudes develop (for example, attitudes towards taking medication), and how attitudes can be changed, and the significance of self-efficacy and learned helplessness in patient behaviour. Each person has a unique set of beliefs, attitudes, motives, experiences, knowledge and expectations that affect their health behaviour. Learning Theory Most human behaviour is learned, learning being defined as a change in behaviour based on experience. There are several types of learning: Associative learning - where the pairing of events is an essential part of the learning process. Classical conditioning - reflexive behaviour is elicited in response to a stimulus that precedes it. This is best exemplified by the "Pavlov's dog" experiment where a dog salivates (unconditioned response - UCR) when presented with food (unconditioned stimulus - UCS). Then when a bell (conditioned stimulus - CS) is paired with the food, the dog salivates in response to the food, and eventually the dog salivates (conditioned response - CR) to the sound of the bell alone. If the food is never again paired with the bell, the CR will be extinguished and disappear. Similarly, people can learn to be 'hungry' (UCR) when an unconditioned stimulus (food) is presented with a conditioned stimulus such as a dinner bell, or a set time on their watch. Patients receiving anti-cancer treatment that makes them nauseous may become conditioned to feel nauseous by other components of the hospital environment such as the smell of the hospital or the sight of the room where treatment is administered. Operant or instrumental conditioning - behaviour is emitted in anticipation of an event (a reinforcer). Types of operant conditioning include reinforcement (where a particular behaviour is strengthened, making it more likely that the behaviour will occur - reinforcement can be positive or negative), aversive conditioning and stimulus control. Positive reinforcement - when something that is valued (a reinforcer, a reward) is presented following the desired behaviour, e.g. paediatricians giving children lollies, GPs giving patients praise for adhering to treatment regimes. Negative reinforcement - contrary to popular usage of this term, negative reinforcement refers to removal of an unpleasant stimulus as the result of a particular behaviour, and not a negative or angry response to behaviour, which is defined as punishment. Thus, removal of a patient's anxiety about their illness through compliance with treatment is more likely to strengthen the compliant behaviour. Aversive conditioning and punishment - rather than trying to increase behaviours, the aim is to decrease them by use of an unpleasant, aversive stimulus, or removal of a pleasant stimulus. Parents who attempt to stop their children from smoking by having them smoke a whole packet of cigarettes are delivering an aversive conditioning strategy (albeit not the best choice of strategy!). Stimulus control - an environmental cue reinforces a given behaviour in a certain way. Thus in smoking cessation programs, smokers are advised to sit in non-smoking sections of hotels, so that there is an environmental restriction on their smoking. Clearly, the type of reinforcement is an important factor, and may have different values for different patients. A patient whose parent died of cancer may respond more to programs that remove anxiety about cancer, such as

1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 58
screening for bowel cancer. Social reinforcers such as praise, attention and affection are powerful reinforcers - but in adolescents such social reinforcers from peer groups may run counter to health objectives. Reinforcers tend to work better than punishments in changing behaviour, a major reason being that punishment does not teach a desirable alternative behaviour to replace the one which is being extinguished. Non-associative learning - pairing of events is not required for behaviour change. Habituation - decline in responsiveness to the repeated presentation of a stimulus. This form of learning can be used in treatment of phobias, where exposure to the feared stimulus can reduce its potency. Sensitisation - repeated presentation or awareness of a stimulus intensifies the response. Observational learning and modelling - this occurs when another person's behaviour is observed, the consequences are noted, and then the behaviour is imitated. Thus, medical or dental students may model their interpersonal behaviours by watching experienced practitioners. Modelling in the form of educational films can be used to lessen children's anxiety about future hospitalisations. Learned Helplessness Learned helplessness occurs when the patient has been taught to believe through a history of past failures, that they are unable to control aspects of their environment, to improve their performance or situation. The concept arose from experiments on animals, where a state of apathy and depression-like symptomatology was induced by administering inescapable electric shocks. This state in humans affects their willingness to try to master new skills and learn new material. Thus, patients who feel that they have failed in previous diets will be less likely to try new weight loss techniques. Those who feel that their illness is an indication of their own failure will become discouraged and give up without trying to improve their situation. Self-efficacy The opposite of learned helplessness is self-efficacy, the belief a person holds that they can succeed at something that they want to do. Patients decide whether to engage in health promoting behaviour by considering whether it will achieve the desired effect, and whether they are capable of carrying it out. A patient may know that exercise will assist in fitness, but not feel capable of doing it. This concept is closely linked to self-esteem, the general feeling that a person has about himself or herself. Condiotte and Lichenstein (1982) found that self-efficacy predicted which smokers would relapse, how soon they would relapse, and in what situations relapse would be likely to occur. If they started smoking again, those with high self-efficacy were more likely to attempt to quit again than those with low self-efficacy. Other research has shown that self-efficacy affects health behaviour and outcomes over a wide range of diseases. Lorig et al (2001) found that improvement in perceived self-efficacy was accompanied by reduction on health care utilisation as measured by attendance at emergency departments and outpatient clinics. (Lorig and colleagues' body of publications is well worth accessing.) Locus of control Individuals with strong internal locus of control believe that they are responsible for and control their own bodies, whereas those who tend towards external locus of control believe that they cannot influence their own bodies, and that disease is a result of events from outside that are beyond their control, random fate. They tend to see themselves as victims of circumstance. In between is the idea of locus of control resting with 'powerful others'; these individuals do not accept responsibility for their own body and welfare, but neither do they attribute their welfare to fate. They see the health practitioner as responsible for their health care, their partner as responsible for their nutrition, their employer as responsible for their safety at work, and so on (Christensen et al, 1997). The concept of locus of control is clearly related to self-efficacy; if a patient believes that have control they are more likely to believe that they can succeed at a task. Whilst patients with strong internal locus of control take responsibility, they may take too much responsibility and make independent decisions about medication, dosage, and other regimes (Hartmann, 2000). External locus patients make compliant in-patients, but have difficulty managing their ongoing treatment compliance once released from hospital. This aspect of the patient's belief system is an important predictor of treatment compliance and health outcomes. Attitudes and attitude change Patients' beliefs about themselves, their illness, their treatment, and the significance of the roles of others, are related to the general area of attitudes and attitude change. Whilst it is essential to identify factors such as locus of control and self-efficacy that can play an important role in treatment compliance, it is also important to understand how such attitudes are formed and how they might be changed. (See also Health Belief Model learning topics.)

1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 59
An attitude can be defined as a relatively enduring cluster of feelings, emotions and behaviours pertaining to person, objects and issues, which constitute a mental "state of readiness", and which are learned (not inborn) and related to experience. Thus, attitudes have cognitive, emotional and behavioural components. Attitudes can be acquired through classical conditioning, modelling, and other forms of social learning, and their purpose is to assist in helping individuals to organise information and new experiences. Attitudes may be changed in a number of ways - repetition, persuasive messages, and use of credible sources are some ways in which pharmaceutical companies attempt to alter medical and dental practitioners' attitudes towards new products, for example. Cognitive dissonance is another way in which attitude change can be provoked. This refers to two separate beliefs or attitudes which are inconsistent with each other. The dissonance or contradiction is unpleasant, and so the individual attempts to reduce the tension by (a) changing one or more cognitions to bring the two attitudes into line, (b) adding new cognitions which strengthen one side or the other, or (c) decreasing the subjective importance of the matter. Smoking beliefs provide examples of all of these techniques. Whitehead (2001) points out that the tension emanating from cognitive dissonance can be used as a motivating state "because the client is most likely to be seeking out ways to minimalise or eliminate the tensions and discomfort they feel within their existing behaviour." Further reading Further reading about these basic psychological concepts can be undertaken by referring to the textbook in your tutorial room, or any of the behavioural sciences in medicine and health psychology text books in the Medical or Fisher Libraries. The references supplied below are only a small sample of recent research into these areas, and further OVID searches will prove productive in increasing understanding of the relevance of learning theory, self efficacy and attitudes to patients' treatment compliance and health outcomes.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • Christensen AJ, Wiebe JS, Lawton WJ. (1997) Cynical hostility, powerful others control expectancies, and
patient adherence in hemodialysis. Psychosomatic Medicine, 59(3):307-312. • Condiotte MM, Lichenstein E (1982) Self efficacy and relapse in smoking cessation programs. Journal of
Consulting and Clinical Psychology, 49(5): 648-658. • Hartmann, DJ (2000) Locus of control and program completion for state funded alcohol clients. Alcoholism
Treatment Quarterly, 18(2): 27-35. • Lorig, KR. Ritter P, Stewart AL, Sobel, DS, William Brown B, Bandura, A, Gonzalez VM, Laurent DD,
Holman HR (2001) Chronic Disease Self-Management Program: 2-Year Health Status and Health Care Utilization Outcomes. Medical Care, 39(11):1217-1223.
• Wainwright, SP, Gould D (1997) Non-adherence with medications in organ transplant patients: a literature review. Journal of Advanced Nursing, 26(5): 968-977.
• Whitehead D (2001) Health education, behavioural change and social psychology: nursing's contribution to health promotion? Journal of Advanced Nursing. 34(6): 822-832.
Author: Professor Susan Hayes, Medicine
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 60
6. Hypoxia ischaemia and cell death Although heart and skeletal muscle are biochemically similar, the two tissues differ metabolically. Under normal conditions, metabolism in heart muscle (myocardium) is aerobic; fatty acids, ketone bodies, lactate and pyruvate are oxidised to carbon dioxide and water with release of energy which is transferred to adenosine 5'-triphosphate (ATP). In cardiac and skeletal muscle, energy is stored as creatine phosphate formed from the ATP by the enzyme creatine kinase (CK). The creatine phosphate is used to maintain the level of cellular ATP to drive the contractile process of the myocardium, involving interaction of the proteins, actin and myosin. When under a heavy workload, the heart can also oxidise glucose to form ATP but the resting heart preferentially oxidises fatty acids. The heart stores some glucose in the form of glycogen which may be used under anaerobic conditions. Myocardial ischaemia may occur when the blood supply of nutrients and oxygen becomes insufficient due either to a decrease in supply or an increase in demand. Blood flow to a portion of the heart may be interrupted by blockage of a coronary artery; platelets from the blood may adhere to the broken edges of an atherosclerotic plaque resulting in formation of a thrombus which occludes the vessel. A portion of the myocardium is deprived of nutrients and oxygen and levels of ATP to drive the contractile process can only be maintained by breakdown of the myocardial glycogen to glucose units which can be used to produce small amounts of ATP via glycolysis. Glucose is converted to pyruvate in a series of 10 enzyme-catalysed reactions. Under aerobic conditions, the pyruvate is completely oxidised to carbon dioxide and water with the production of ATP. In ischaemic myocardium, the pyruvate is converted to lactate in a reaction catalysed by the enzyme, lactate dehydrogenase (LDH) and the net yield of ATP is much lower. However, the cardiac pain and fatigue associated with ischaemia is attributed to glycolytically generated acid rather than lactic acid. The intramuscular pH may decrease from 7.0 to 6.4, levels of ATP and creatine phosphate in cardiac muscle decrease due perhaps to a reduced activity of the glycolytic enzyme, phosphofructokinase, at the lower cellular pH. To maintain the function and viability of the myocardium a little longer, levels of ATP are maintained using the enzyme, myokinase (adenylate kinase), which converts two molecules of ADP to ATP and AMP. Subsequent deamination of one of the products of the myokinase reaction, AMP, by the enzyme, adenylate deaminase, increases this production of ATP. However in the continuing absence of an oxygen supply, these temporary metabolic strategies also become depleted and lactate and hydrogen ions (H+) accumulate. The H+ ions are cleared from the cytosol by the Na+-H+ exchanger leading to accumulation of intracellular Na+ that exchanges with extracellular Ca2+; increased intracellular Ca2+ can induce death of myoblasts with release of their contents into the circulation. Over the next few weeks the infarct in the heart is replaced by fibroblasts leaving a nonfunctional fibrotic lesion. Three cardiac markers that appear in the blood stream after a myocardial infarction are lactate dehydrogenase (LDH), creatine kinase (CK) and troponin, which exist as cardiac isoforms whose presence in the peripheral circulation confirms the occurrence of myocardial infarction and may indicate its extent. Diagnostic tests have been developed to measure levels of LDH, CK and troponin in blood.
References Use the textbooks in your Tutorial Room Optional references Available in Medical Library: see Library Catalogue • The textbook by Voet provides a current view of Biochemistry at a detailed and fundamental level, Stryer is
also a valuable and detailed text. The book by Bhagavan provides the fundamentals of a variety of clinical disorders.
o Voet D, Voet JG. Biochemistry. 3rd ed. New York: J. Wiley & Sons; 2004. • Berg JM, Tymoczko JL, Stryer L. Biochemistry. 6th ed. New York: W.H. Freeman; 2007. • Bhagavan NV. Medical biochemistry. 4th ed. San Diego: Harcourt/Academic Press; 2002. [Available as an
E-Book]
Author: Professor Richard Christopherson, Molecular and Microbial Biosciences
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 61
7. Coronary artery disease in Australian Aborigines and Torres Strait Islanders Learning objectives: Students should be able to: • Describe the difference between the prevalence of coronary artery disease in Indigenous and non-
Indigenous populations in Australia • Describe the comparative trends in mortality in coronary artery disease in Indigenous and non-Indigenous
populations in Australia • Describe the major risk factors for coronary artery disease in Aborigines and Torres Strait Islanders Please note: references are given throughout for acknowledgment and interest. The content of these citations will not be examinable. “Aboriginal and Torres Strait Islander peoples continue to suffer a substantially greater burden of ill health than other Australians. This health disadvantage begins at an early age and continues throughout adult life. It reflects the broader social and economic disadvantages faced by Indigenous Australians.”1 Cardiovascular disease (CVD), particularly coronary heart disease (CHD), is the leading cause of death among Indigenous people.2 The leading cardiovascular conditions contributing to increased mortality are coronary heart disease, stroke and hypertensive disease. Rheumatic heart disease is not a common contributor to mortality from CVD in the non-Indigenous population. However “Indigenous Australians have one of the highest rates of acute rheumatic fever and chronic rheumatic heart disease in the world.”3 The number of Indigenous deaths from CVD (1996-2000) was more than three times the number expected from rates for the non-Indigenous population. The leading specific cause of death for both Indigenous males and females for this period was coronary heart disease, for which cause there were around three times more deaths than expected. Rheumatic heart disease (RHD) was responsible for relatively few deaths, but the standardised mortality ratio4 was 27.0 for males and 23.3 for females. (See Figure 1) During 1998-01 there were 8% fewer coronary artery bypass graft (CABG) operations for Indigenous males than for other Australian men. For Indigenous women the rates of CABG were 31% higher. In the same period there were 55% fewer coronary angioplasty procedures for Indigenous males compared with other Australian males. Among Indigenous women there were 16% more coronary angioplasty procedures, compared with other Australian females.5 Indigenous CVD mortality occurs amongst young and middle aged Indigenous people. The very high rate of mortality (compared with non-Indigenous Australians) from coronary heart disease is similar to age-specific death rates for non-Indigenous people at least twenty years older. (See Figure 2) Amongst young Aboriginal sportsmen the estimated incidence of IHD-related sudden cardiac death in the NT between 1982 and 1996 was 19-24 per 100,000 player-years, compared with 0.54 per 100,000 player-years among Australian rules footballers of similar ages in Victoria.6 The available evidence suggests that the disparity between Indigenous and non-Indigenous people is widening, mainly because Indigenous people do not appear to have benefited from the substantial declines in coronary heart disease and stroke mortality that have occurred in Australia over the past thirty years. Whilst death from cardiovascular disease in the total Australian population has declined since the late 1960s, 7, 8 these improvements in mortality have not been shared by Indigenous people.9 The declines for the total population have been attributed to a combination of reductions in the levels of various risk factors (including smoking, high blood pressure, and dietary saturated fats) and improvements in management of coronary heart disease and stroke events and established disease.10, 11 The major CVD risk factors for the Indigenous population are the same as those for the total population, but the prevalence of these risk factors is often much higher among Indigenous people.12 There is a higher rate of low birth-weight in Aborigines and Torres Strait Islanders. This has been linked with increased aortic wall thickening, suggesting that intrauterine growth restriction may predispose to later cardiovascular risk.13 As is true for many health issues, the high prevalence of risk factors found among the Indigenous population reflects the broader social and economic disadvantages faced by Indigenous Australians: “people in lower socioeconomic groups are more likely to die from cardiovascular disease compared with people in higher socioeconomic groups.”14
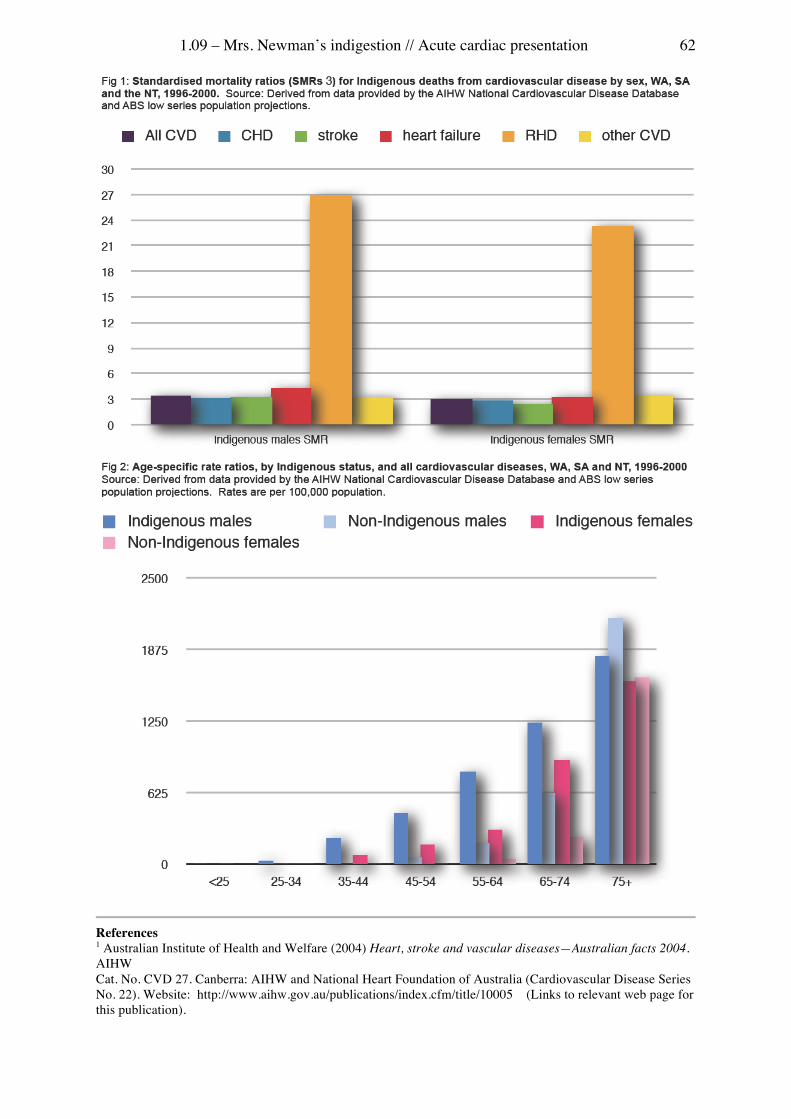
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 62
References 1 Australian Institute of Health and Welfare (2004) Heart, stroke and vascular diseases—Australian facts 2004. AIHW Cat. No. CVD 27. Canberra: AIHW and National Heart Foundation of Australia (Cardiovascular Disease Series No. 22). Website: http://www.aihw.gov.au/publications/index.cfm/title/10005 (Links to relevant web page for this publication).
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 63
2 Reference: Australian Indigenous Healthinfonet: http://www.healthinfonet.ecu.edu.au/ Note: This learning topic has largely been drawn from this reference site. Further details are available on the site, but are not examinable. 3 Australian Institute of Health and Welfare (2004) Heart, stroke and vascular diseases—Australian facts 2004. AIHW Cat. No. CVD 27. Canberra: AIHW and National Heart Foundation of Australia (Cardiovascular Disease Series No. 22). Website: http://www.aihw.gov.au/publications/index.cfm/title/10005 (Links to relevant web page for this publication). 4 Standardised mortality ratio (SMR) is the ratio of the actual number of deaths identified as Indigenous and the number expected from the age-specific rates of the same-sex non-Indigenous population. It is important to recognise that the data used in this Learning Topic has not been adjusted for the likely under-identification of Indigenous people in deaths registrations. 5 Australian Institute of Health and Welfare (2004). Heart, stroke and vascular diseases—Australian facts 2004. AIHW Cat. No. CVD 27. Canberra: AIHW and National Heart Foundation of Australia (Cardiovascular Disease Series No. 22). Website: http://www.aihw.gov.au/publications/index.cfm/title/10005 (Links to relevant web page for this publication). 6 Young MC, Fricker PA, Thomson NJ and Lee AP (1999) Sudden death due to ischaemic heart disease in young Aboriginal sportsmen in the Northern Territory, 1982-1996 . Medical Journal of Australia, 1999 170: 425-428 7 Mathur S (2002) Epidemic of coronary heart disease and its treatment in Australia . Canberra: Australian Institute of Health and Welfare, 2002 8 Mathur S and Gajanayake I 1998. Surveillance of cardiovascular mortality in Australia 1985–1996. AIHW cat. no. CVD 3. Canberra: Australian Institute of Health and Welfare (Cardiovascular disease series no. 6) Website; http://www.aihw.gov.au/publications/index.cfm/title/3421 (links to relevant web page for this publication) 9 Kunitz SJ (1994) Health of populations of Northern Queensland Aboriginal communities: change and continuity Human Biology, 1994 66(5): 917-943 10 Australian Institute of Health and Welfare (2001) Heart, stroke and vascular diseases: Australian facts 2001 . Canberra: Australian Institute of Health and Welfare. Website: http://www.aihw.gov.au/publications/cvd/hsvd01/ (Links to relevant web page for this publication). 11 Mathur S (2002) Epidemic of coronary heart disease and its treatment in Australia Canberra: Australian Institute of Health and Welfare 12 Australian Institute of Health and Welfare (2001) Heart, stroke and vascular diseases: Australian facts 2001. Canberra: Australian Institute of Health and Welfare. Website: http://www.aihw.gov.au/publications/cvd/hsvd01/ (Links to relevant web page for this publication). 13 Skilton M, Evans N, Griffiths K Harmer JA and Celemajer DS (2005) Aortic wall thickness in newborns with intrauterine growth restriction Lancet 2005 365(9469): 1484-1486
Author: Dr Lilon Bandler, Office of Medical Education (OME)
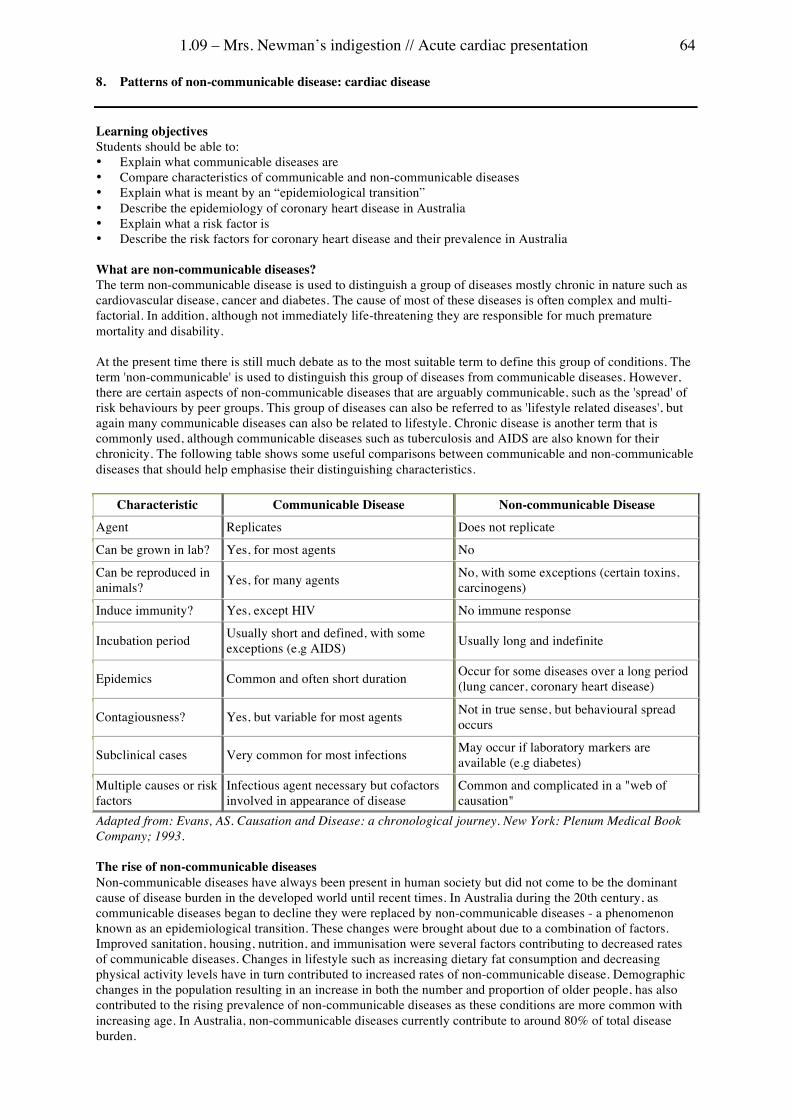
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 64
8. Patterns of non-communicable disease: cardiac disease Learning objectives Students should be able to: • Explain what communicable diseases are • Compare characteristics of communicable and non-communicable diseases • Explain what is meant by an “epidemiological transition” • Describe the epidemiology of coronary heart disease in Australia • Explain what a risk factor is • Describe the risk factors for coronary heart disease and their prevalence in Australia What are non-communicable diseases? The term non-communicable disease is used to distinguish a group of diseases mostly chronic in nature such as cardiovascular disease, cancer and diabetes. The cause of most of these diseases is often complex and multi-factorial. In addition, although not immediately life-threatening they are responsible for much premature mortality and disability. At the present time there is still much debate as to the most suitable term to define this group of conditions. The term 'non-communicable' is used to distinguish this group of diseases from communicable diseases. However, there are certain aspects of non-communicable diseases that are arguably communicable, such as the 'spread' of risk behaviours by peer groups. This group of diseases can also be referred to as 'lifestyle related diseases', but again many communicable diseases can also be related to lifestyle. Chronic disease is another term that is commonly used, although communicable diseases such as tuberculosis and AIDS are also known for their chronicity. The following table shows some useful comparisons between communicable and non-communicable diseases that should help emphasise their distinguishing characteristics.
Characteristic Communicable Disease Non-communicable Disease
Agent Replicates Does not replicate
Can be grown in lab? Yes, for most agents No
Can be reproduced in animals? Yes, for many agents No, with some exceptions (certain toxins,
carcinogens)
Induce immunity? Yes, except HIV No immune response
Incubation period Usually short and defined, with some exceptions (e.g AIDS) Usually long and indefinite
Epidemics Common and often short duration Occur for some diseases over a long period (lung cancer, coronary heart disease)
Contagiousness? Yes, but variable for most agents Not in true sense, but behavioural spread occurs
Subclinical cases Very common for most infections May occur if laboratory markers are available (e.g diabetes)
Multiple causes or risk factors
Infectious agent necessary but cofactors involved in appearance of disease
Common and complicated in a "web of causation"
Adapted from: Evans, AS. Causation and Disease: a chronological journey. New York: Plenum Medical Book Company; 1993. The rise of non-communicable diseases Non-communicable diseases have always been present in human society but did not come to be the dominant cause of disease burden in the developed world until recent times. In Australia during the 20th century, as communicable diseases began to decline they were replaced by non-communicable diseases - a phenomenon known as an epidemiological transition. These changes were brought about due to a combination of factors. Improved sanitation, housing, nutrition, and immunisation were several factors contributing to decreased rates of communicable diseases. Changes in lifestyle such as increasing dietary fat consumption and decreasing physical activity levels have in turn contributed to increased rates of non-communicable disease. Demographic changes in the population resulting in an increase in both the number and proportion of older people, has also contributed to the rising prevalence of non-communicable diseases as these conditions are more common with increasing age. In Australia, non-communicable diseases currently contribute to around 80% of total disease burden.
1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 65
What is the burden and distribution of coronary heart disease in Australia? Coronary heart disease continues to be the leading cause of mortality in Australia, even despite a decline in mortality rates of more than 60% since the late 1960s. In addition to mortality, coronary heart disease is also an important cause of ill health, disability, and reduced quality of life. The distribution of CHD varies within different subgroups of the Australian population. Men are twice as likely to have a coronary event as women and CHD incidence rates and mortality increase with age. Mortality rates from CHD also differ according to socioeconomic status with people in the lowest socioeconomic group having mortality rates double that of those in the highest socioeconomic category. Indigenous Australians also have death rates from CHD that are much higher than the rest of the population. What are risk factors? Risk factors are 'determinants, characteristics or exposures that are associated with a greater risk of ill health'. They can be non-modifiable or modifiable. Non-modifiable risk factors are certain characteristics such as age or genetic inheritance that cannot be changed. Modifiable risk factors can be biomedical parameters such as obesity or high blood pressure. They also include behavioural factors such as smoking and level of physical activity. Risk factors are characteristics that are more common in people with disease than in people without disease and are therefore said to be associated with an increased probability of disease occurrence. However, risk factors do not always 'cause' a disease. As a result, the presence of a risk factor does not mean an individual will definitely develop a disease, rather it indicates that their chances of doing so are increased. In addition, not all people with a disease will have a risk factor. Risk of disease increases progressively as the number of risk factors increases. Therefore, people with multiple risk factors have a much higher chance of developing disease than people with one risk factor alone. In addition, many risk factors have a continuous association with the disease, such that defining a threshold for normality is somewhat arbitrary. Examples include the associations between blood pressure and cholesterol with coronary heart disease. The higher the blood pressure, the greater the risk of developing coronary heart disease. However, most individuals who develop disease have moderate elevations of a number of risk factors, rather than an extreme elevation of a single risk factor. As well as the group of characteristics commonly referred to as risk factors, there are many underlying features of an individual's environment or socio-economic circumstances that also increase their 'risk' of disease. Such factors, however, are normally referred to as 'health determinants' as opposed to risk factors. These 'determinants' often interact with each other - for example peer pressure as a social environmental factor can increase tobacco smoking behaviour. (Consider Learning Topic 8 in 1.01) What are the risk factors for coronary heart disease? • Age • Male sex • Family history Non-modifiable Modifiable Biomedical • High blood cholesterol • High blood pressure • Overweight and obesity • Diabetes mellitus
Behavioural • Tobacco smoking • Insufficient physical activity • Excessive alcohol consumption • Nutrition How common are modifiable risk factors for CHD? In the 2001 National Health Survey, respondents were asked about their health and health behaviours. The results indicate that nine in ten adult Australians surveyed report having at least one modifiable risk factor. This corresponds to an estimated 13.1 million Australians affected. In 2001, based on self reported information, more women (35.3%) than men (26.2%) aged 18 years and over had just one risk factor, whereas more men (26.1%) than women (20.9%) had three or more risk factors. The prevalence of three or more risk factors, as expected, is more common among older people (about one in three aged 65 years and over). The prevalence of risk factors varies with socioeconomic status. Men in the lowest socioeconomic group are two times as likely to have 3 or

1.09 – Mrs. Newman’s indigestion // Acute cardiac presentation 66
more risk factors than men in the highest socioeconomic group. Indigenous Australians have high prevalence rates of many risk factors compared to the rest of the Australian population. Indigenous Australians are more likely to smoke, have diabetes, and be obese and are less likely to be physically active. Risk factors are more common (80%) in Australians reporting heart disease than those without heart disease (68%). However, it is difficult to determine how much heart disease is due to the presence of risk factors. Recently it has been suggested that as much as 75% of CHD in the population can be explained by high blood cholesterol, high blood pressure and cigarette smoking. In addition, it has been estimated that 24% of CHD deaths can be attributed to high blood pressure, 21% to physical inactivity, 20% to high blood cholesterol, 8% to tobacco smoking and 7% to excess body weight. As a result, the prevalence of risk factors in the population have an important impact on CHD disease burden in Australia. See table 4.1 "Risk factor prevalence rates by age and sex 1999-2001 From: Epidemic of Coronary Heart Disease and its Treatment in Australia AIHW 2002 - http://www.aihw.gov.au/publications/cvd/echdta/echdta-c04.pdf
References Use the textbooks in your Tutorial Room • Evans AS. Causation and disease: a chronological journey. New York: Plenum Medical Book Co.; 1993. • Waters. A.M., Bennett, S., 1995, Risk factors for cardiovascular disease: a summary of Australian data,
Australian Institute of Health and Welfare (AIHW), Canberra. • Australian Institute of Health and Welfare, 2004. Australia's Health 2004. AIHW Cat. No AUS 44. AIHW:
Canberra. • Australian Institute of Health and Welfare. Living Dangerously: Australians with Multiple Risk Factors for
Cardiovascular Disease. AIHW Cat. No AUS 57. Canberra: AIHW; 2005 • Australian Institute of Health and Welfare, 2004. Heart, Stroke and Vascular Diseases, Australian Facts
2004, AIHW Cat. No CVD 27. Canberra: AIHW; 2004 • Australian Institute of Health and Welfare. Chronic diseases and associated risk factors in Australia, 2001.
AIHW Cat. No PHE 33. Canberra: AIHW; 2001.