Supracarinal tracheal tear after atraumatic endotracheal intubation: anesthetic considerations for...
9
CASE CONFERENCE CASE 9 – 2014 Supracarinal Tracheal Tear After Atraumatic Endotracheal Intubation: Anesthetic Considerations for Surgical Repair Mary E. Arthur, MD,* Nadine Odo, BA,* William Parker, MD,† Paul M. Weinberger, MD,‡ and Vijay S. Patel, MD§ I ATROGENIC TRACHEAL TEARS are rare but very serious complications of tracheal intubation. Because an unknown fraction of postintubation tracheal injuries are undiag- nosed, misdiagnosed, or underreported, the actual incidence and outcomes of such injuries are unknown. The incidence of reported cases is approximately 1 in every 20,000 intubation attempts, 1 but postmortem studies suggest the actual incidence may be as high as 15% of emergency intubations. 2 When discovered, tracheal tears typically are managed conservatively, although larger tracheal tears generally require surgical inter- vention after diagnosis by fiberoptic bronchoscopy. The authors report on the anesthetic and surgical management of a large tracheal tear close to the carina in a young female patient and discuss airway management recommendations for such injuries. CASE PRESENTATION * A 27-year-old Caucasian female with a history of migraines and intractable seizure disorder presented for a left craniotomy and an implantation of subdural grid and depth electrodes to localize the site of her seizures. She and her husband had expressed a desire to have children, and this procedure was meant to facilitate weaning her off of potentially fetotoxic seizure medications. An uneventful anesthesia induction with 150 mg of propofol, 50 mg of lidocaine, and 50 μg fentanyl was followed by a single atraumatic attempt at direct laryngoscopy with a grade-1 view. The patient was intubated with a 7.0 endotracheal tube (ETT) that was taped at 22 cm at the lips before the surgeon attached the Mayfield frame to the head in the magnetic resonance imaging suite. After the required images were obtained, the intubated patient was transported to the operating room (OR) and sedated with propofol (100 μg/kg/min) for the second part of the procedure, a left craniotomy, implantation of subdural grid with the use of stealth navigation, and stereotactic implantation of right and left depth electrodes, to localize the epileptogenic focus. The patient was extubated and transported to the postanesthesia care unit after the uneventful procedure. On postoperative day 2, she was rushed to the OR for an emergency craniotomy to evacuate an epidural hematoma. Her reintubation with a styletted 7.0 ETT was atraumatic with a grade-1 view on laryngoscopy. Shortly after the procedure started, the patient spontaneously desaturated into the low 80s and was ventilated manually back to an SpO 2 of 100%. A second episode of desaturation occurred an hour and 25 minutes into the case, prompting an arterial blood gas (ABG) analysis, which revealed a PaO 2 of 49.3 mmHg. A repeat ABG 30 minutes after the desaturation episode was normal (PaO 2 of 370 mmHg). Thirty-two minutes after the second set of ABG results was obtained, a third episode of spontaneous desaturation (89%) reverted to 100% with little intervention. The authors observed that the ETT had migrated down into the right main bronchus and left breath sounds were diminished. The tube was readjusted and pulled back from 24 cm and retaped at 22 cm at the lip. Because of the unexplained desaturations in the OR, the anesthesia and surgical teams agreed that the patient should remain intubated. Axial and coronal views on computed tomography angiography, which were obtained to rule out a pulmonary embolus, instead revealed a small pneumomediastinum (Figs 1 and 2), prompting an urgent cardiothoracic consult and return to the OR for exploration. PaO 2 was 54.7 mmHg on arrival in the OR. Standard monitors were attached and adequate anesthesia was ensured. The surgeon then evaluated the entire trachea under fiberoptic guidance through the existing ETT and discovered a 6-cm tear that was 2 cm from the carina (Figs 3 and 4). The surgeon decided to approach the repair through a right thoracotomy. Because of the airway trauma and proximity of the injury to the carina, the authors isolated the left lung by advancing the ETT into the left main bronchus under bronchoscopic guidance. The patient was placed on ventilator support with a tidal volume of 400 mL. Peak and plateau airway pressures were 22 and 21 cmH 2 O, respec- tively, and SpO 2 was 100%. A desaturation episode (SpO 2 of 65%) an hour into the case could not be explained by the tube position because it was distal to the lesion. Fiberoptic bronchoscopy revealed further migration of the ETT past the left bronchial bifurcation. The ETT was, therefore, repositioned distal to the carina but proximal to the left bronchial bifurcation, also under fiberoptic guidance. Oxygenation improved significantly, and the patient was placed in a left lateral decubitus position for a 6-hour right open thoracotomy. The tracheal defect was found to be just beneath the ETT cuff (Fig 5), with only a thin membrane separating the cuff from the tracheal lumen. Once the defect was opened, the ETT and deflated cuff clearly could be seen just entering the left mainstem bronchus (Fig 6). The tube was advanced further to repair the site. Intraoperative management included intermittent manual ventilation for adequate oxygenation. From the Departments of *Anesthesiology and Perioperative Medicine, †Diagnostic, Therapeutic and Interventional Radiology, ‡Otolaryngology, and §Surgery, Medical College of Georgia, Georgia Regents University, Augusta, GA. Presented at the American Society of Anesthesiologists Annual Meet- ing, October 15-19, 2011, Chicago, IL as a medically challenging case. Address reprint requests to Mary E. Arthur, MD, 1120 15th Street, BIW-2144, Georgia Regents University, Augusta, GA 30912. E-mail: [email protected] Published by Elsevier Inc. 1053-0770/2602-0033$36.00/0 http://dx.doi.org/10.1053/j.jvca.2013.08.014 Key words: trachea, tracheal tear, endotracheal intubation, compli- cations, tracheal injury, anesthesia, otolaryngology, surgery *M. E. Arthur and N. Odo Journal of Cardiothoracic and Vascular Anesthesia, Vol 28, No 4 (August), 2014: pp 1149–1157 1149
Transcript of Supracarinal tracheal tear after atraumatic endotracheal intubation: anesthetic considerations for...

CASE CONFERENCE
CASE
9–2014Supracarinal Tracheal Tear After Atraumatic Endotracheal Intubation:Anesthetic Considerations for Surgical Repair
Mary E. Arthur, MD,* Nadine Odo, BA,* William Parker, MD,† Paul M. Weinberger, MD,‡ and Vijay S. Patel, MD§
IATROGENIC TRACHEAL TEARS are rare but veryserious complications of tracheal intubation. Because an
unknown fraction of postintubation tracheal injuries are undiag-nosed, misdiagnosed, or underreported, the actual incidence andoutcomes of such injuries are unknown. The incidence ofreported cases is approximately 1 in every 20,000 intubationattempts,1 but postmortem studies suggest the actual incidencemay be as high as 15% of emergency intubations.2 Whendiscovered, tracheal tears typically are managed conservatively,although larger tracheal tears generally require surgical inter-vention after diagnosis by fiberoptic bronchoscopy. The authorsreport on the anesthetic and surgical management of a largetracheal tear close to the carina in a young female patient anddiscuss airway management recommendations for such injuries.
From the Departments of *Anesthesiology and PerioperativeMedicine, †Diagnostic, Therapeutic and Interventional Radiology,‡Otolaryngology, and §Surgery, Medical College of Georgia, GeorgiaRegents University, Augusta, GA.Presented at the American Society of Anesthesiologists Annual Meet-
ing, October 15-19, 2011, Chicago, IL as a medically challenging case.Address reprint requests to Mary E. Arthur, MD, 1120 15th Street,
BIW-2144, Georgia Regents University, Augusta, GA 30912. E-mail:[email protected] by Elsevier Inc.1053-0770/2602-0033$36.00/0
CASE PRESENTATION*
A 27-year-old Caucasian female with a history of migraines andintractable seizure disorder presented for a left craniotomy and animplantation of subdural grid and depth electrodes to localize the site ofher seizures. She and her husband had expressed a desire to havechildren, and this procedure was meant to facilitate weaning her off ofpotentially fetotoxic seizure medications.
An uneventful anesthesia induction with 150 mg of propofol, 50 mgof lidocaine, and 50 µg fentanyl was followed by a single atraumaticattempt at direct laryngoscopy with a grade-1 view. The patient wasintubated with a 7.0 endotracheal tube (ETT) that was taped at 22 cm atthe lips before the surgeon attached the Mayfield frame to the head inthe magnetic resonance imaging suite. After the required images wereobtained, the intubated patient was transported to the operating room(OR) and sedated with propofol (100 µg/kg/min) for the second part ofthe procedure, a left craniotomy, implantation of subdural grid with theuse of stealth navigation, and stereotactic implantation of right and leftdepth electrodes, to localize the epileptogenic focus. The patient wasextubated and transported to the postanesthesia care unit after theuneventful procedure. On postoperative day 2, she was rushed to theOR for an emergency craniotomy to evacuate an epidural hematoma.Her reintubation with a styletted 7.0 ETT was atraumatic with a grade-1view on laryngoscopy. Shortly after the procedure started, the patientspontaneously desaturated into the low 80s and was ventilatedmanually back to an SpO2 of 100%. A second episode of desaturationoccurred an hour and 25 minutes into the case, prompting an arterialblood gas (ABG) analysis, which revealed a PaO2 of 49.3 mmHg. Arepeat ABG 30 minutes after the desaturation episode was normal(PaO2 of 370 mmHg). Thirty-two minutes after the second set of ABGresults was obtained, a third episode of spontaneous desaturation (89%)
*M. E. Arthur and N. Odo
Journal of Cardiothoracic and Vascular Anesthesia, Vol 28, No 4 (August)
reverted to 100% with little intervention. The authors observed that theETT had migrated down into the right main bronchus and left breathsounds were diminished. The tube was readjusted and pulled back from24 cm and retaped at 22 cm at the lip.
Because of the unexplained desaturations in the OR, the anesthesiaand surgical teams agreed that the patient should remain intubated.Axial and coronal views on computed tomography angiography, whichwere obtained to rule out a pulmonary embolus, instead revealed asmall pneumomediastinum (Figs 1 and 2), prompting an urgentcardiothoracic consult and return to the OR for exploration.
PaO2 was 54.7 mmHg on arrival in the OR. Standard monitors wereattached and adequate anesthesia was ensured. The surgeon thenevaluated the entire trachea under fiberoptic guidance through theexisting ETT and discovered a 6-cm tear that was 2 cm from the carina(Figs 3 and 4). The surgeon decided to approach the repair through aright thoracotomy. Because of the airway trauma and proximity of theinjury to the carina, the authors isolated the left lung by advancing theETT into the left main bronchus under bronchoscopic guidance. Thepatient was placed on ventilator support with a tidal volume of 400 mL.Peak and plateau airway pressures were 22 and 21 cmH2O, respec-tively, and SpO2 was 100%. A desaturation episode (SpO2 of 65%) anhour into the case could not be explained by the tube position becauseit was distal to the lesion. Fiberoptic bronchoscopy revealed furthermigration of the ETT past the left bronchial bifurcation. The ETT was,therefore, repositioned distal to the carina but proximal to the leftbronchial bifurcation, also under fiberoptic guidance. Oxygenationimproved significantly, and the patient was placed in a left lateraldecubitus position for a 6-hour right open thoracotomy.
The tracheal defect was found to be just beneath the ETT cuff (Fig 5),with only a thin membrane separating the cuff from the tracheal lumen.Once the defect was opened, the ETT and deflated cuff clearly could beseen just entering the left mainstem bronchus (Fig 6). The tube wasadvanced further to repair the site. Intraoperative management includedintermittent manual ventilation for adequate oxygenation.
http://dx.doi.org/10.1053/j.jvca.2013.08.014Key words: trachea, tracheal tear, endotracheal intubation, compli-
cations, tracheal injury, anesthesia, otolaryngology, surgery
, 2014: pp 1149–1157 1149
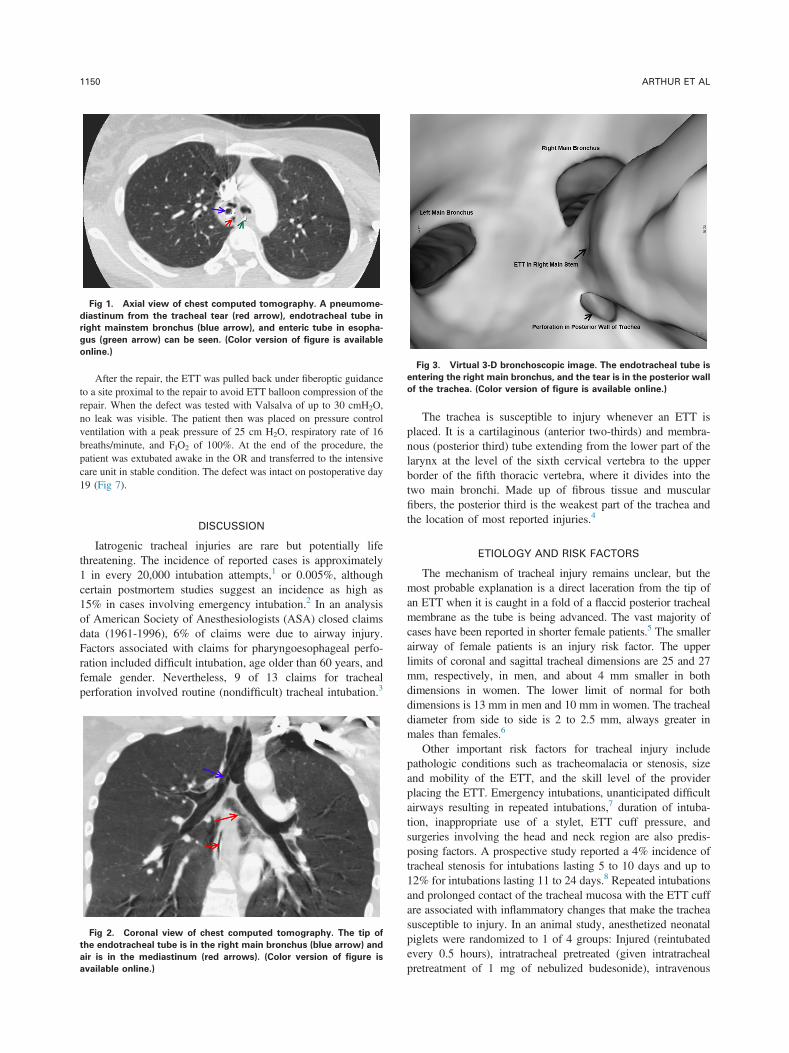
Fig 1. Axial view of chest computed tomography. A pneumome-
diastinum from the tracheal tear (red arrow), endotracheal tube in
right mainstem bronchus (blue arrow), and enteric tube in esopha-
gus (green arrow) can be seen. (Color version of figure is available
online.)
Fig 3. Virtual 3-D bronchoscopic image. The endotracheal tube is
entering the right main bronchus, and the tear is in the posterior wall
of the trachea. (Color version of figure is available online.)
ARTHUR ET AL1150
After the repair, the ETT was pulled back under fiberoptic guidanceto a site proximal to the repair to avoid ETT balloon compression of therepair. When the defect was tested with Valsalva of up to 30 cmH2O,no leak was visible. The patient then was placed on pressure controlventilation with a peak pressure of 25 cm H2O, respiratory rate of 16breaths/minute, and FIO2 of 100%. At the end of the procedure, thepatient was extubated awake in the OR and transferred to the intensivecare unit in stable condition. The defect was intact on postoperative day19 (Fig 7).
DISCUSSION
Iatrogenic tracheal injuries are rare but potentially lifethreatening. The incidence of reported cases is approximately1 in every 20,000 intubation attempts,1 or 0.005%, althoughcertain postmortem studies suggest an incidence as high as15% in cases involving emergency intubation.2 In an analysisof American Society of Anesthesiologists (ASA) closed claimsdata (1961-1996), 6% of claims were due to airway injury.Factors associated with claims for pharyngoesophageal perfo-ration included difficult intubation, age older than 60 years, andfemale gender. Nevertheless, 9 of 13 claims for trachealperforation involved routine (nondifficult) tracheal intubation.3
Fig 2. Coronal view of chest computed tomography. The tip of
the endotracheal tube is in the right main bronchus (blue arrow) and
air is in the mediastinum (red arrows). (Color version of figure is
available online.)
The trachea is susceptible to injury whenever an ETT isplaced. It is a cartilaginous (anterior two-thirds) and membra-nous (posterior third) tube extending from the lower part of thelarynx at the level of the sixth cervical vertebra to the upperborder of the fifth thoracic vertebra, where it divides into thetwo main bronchi. Made up of fibrous tissue and muscularfibers, the posterior third is the weakest part of the trachea andthe location of most reported injuries.4
ETIOLOGY AND RISK FACTORS
The mechanism of tracheal injury remains unclear, but themost probable explanation is a direct laceration from the tip ofan ETT when it is caught in a fold of a flaccid posterior trachealmembrane as the tube is being advanced. The vast majority ofcases have been reported in shorter female patients.5 The smallerairway of female patients is an injury risk factor. The upperlimits of coronal and sagittal tracheal dimensions are 25 and 27mm, respectively, in men, and about 4 mm smaller in bothdimensions in women. The lower limit of normal for bothdimensions is 13 mm in men and 10 mm in women. The trachealdiameter from side to side is 2 to 2.5 mm, always greater inmales than females.6
Other important risk factors for tracheal injury includepathologic conditions such as tracheomalacia or stenosis, sizeand mobility of the ETT, and the skill level of the providerplacing the ETT. Emergency intubations, unanticipated difficultairways resulting in repeated intubations,7 duration of intuba-tion, inappropriate use of a stylet, ETT cuff pressure, andsurgeries involving the head and neck region are also predis-posing factors. A prospective study reported a 4% incidence oftracheal stenosis for intubations lasting 5 to 10 days and up to12% for intubations lasting 11 to 24 days.8 Repeated intubationsand prolonged contact of the tracheal mucosa with the ETT cuffare associated with inflammatory changes that make the tracheasusceptible to injury. In an animal study, anesthetized neonatalpiglets were randomized to 1 of 4 groups: Injured (reintubatedevery 0.5 hours), intratracheal pretreated (given intratrachealpretreatment of 1 mg of nebulized budesonide), intravenous

Fig 4. Fiberoptic bronchoscopy of a 6 cm full thickness tracheal tear very close to the carina. (Color version of figure is available online.)
CASE 9–2014 1151
pretreated (given intravenous pretreatment of 0.3 mg/kg ofdexamethasone), or control (not intubated). Both expressionlevels of interleukin-6, an inflammatory cytokine, and degree oftracheal injury were significantly higher among “injured” and“intratracheal pretreated” subjects than controls. Systemicsteroids offered some protection against inflammation.9
Tracheal injury usually occurs at the tube cuff site.10
Hyperinflation of the ETT cuff is the most frequent risk factorfor tracheal ischemia and subsequent complications. In fact,just a few hours after intubation, the ETT cuff can causetracheal mucosal lesions, which may result in tracheal stenosisand rupture. Further, several reports described postoperativehoarseness and sore throat after general anesthesia, which wereattributed to high ETT cuff pressure.11,12 The prevalence ofpostintubation and post-tracheotomy stenosis varies from 10%to 19% in intensive care unit patients using a low-volume high-pressure endotracheal cuff.13 High-volume, low-pressure cuffsgreatly reduce the occurrence of cuff injury. An animal studythat compared manual with continuous control of endotrachealcuff pressure in a setting mimicking that of intubated criticallyill patients noted that all animals had hyperemia and hemor-rhage at the cuff contact area.14 The recommended mucosalpressure exerted by the cuff should, therefore, be below thecapillary mucosal pressure of approximately 26 mmHg.
Although double-lumen endotracheal tubes (DLT) are cur-rently the most widely used tubes to achieve lung isolation, they
Fig 5. Tracheal defect just beneath the endotracheal tube cuff. A thin m
available online.)
are stiff, bulky, and notorious for causing severe tracheal damage.Risk factors for DLT-related tracheal injury include direct trauma,cuff overinflation and pre-existing airway pathology.15 It is morelikely that a tracheobronchial injury will be caused by a single-lumen tube than a DLT, but this is because more patients areintubated with single-lumen tubes. DLTs account for less than 1%of all tracheal ruptures.16 Nevertheless, an inappropriately sizedDLT can cause airway trauma, interfere with oxygenation, andhinder lung separation during one-lung ventilation.17,18 Selectingthe appropriate size is problematic, because the tracheal internaldiameter does not closely correlate with sex, age, height, orweight. Suggested criteria for sizing left-sided DLT have includedmeasuring tracheal diameter by chest radiograph,19 left mainbronchus diameter by CT scan,20 or left main bronchus by directmeasurement using a posterior-anterior chest x-ray and estimatingthe bronchial diameter to be 10% smaller than measured.17,18
The authors combined a meta-analysis of articles publishedfrom 1966 to 2007 with a more recent single-center observa-tional study (2003-2008) and found that being female and olderappeared to be risk factors for injury, as did emergencyintubation, difficult intubation, and use of a DLT. Shorterstature and overweight may also be factors (Table 1).
SYMPTOMS
Because the signs and symptoms can be nonspecific,diagnosis of tracheobronchial injury requires a high index of
embrane separates the defect from the cuff. (Color version of figure is

Fig 6. Repaired site immediately after surgery. There was no visible leak when the repaired defect was tested with valsalva to 30 cmH2O.
(Color version of figure is available online.)
ARTHUR ET AL1152
suspicion and should be considered in patients who developsubcutaneous emphysema after intubation, with or withoutrespiratory symptoms. Tracheobronchial injury also couldpresent with pneumothorax, hemoptysis, respiratory insuffi-ciency, tracheal shift, cyanosis, airway obstruction, and pneu-momediastinum. Some patients may be asymptomatic.18 Ifthere have been repeated intubations, the differential diagnosisfor hypoxemia should include tracheal injury. The recurrenthypoxemic episodes in this patient mandated a chest x-ray andCT scan. The pneumomediastinum noted on CT prompted animmediate cardiothoracic consult and fiberoptic bronchoscopy,which led to a definitive diagnosis.
DIAGNOSIS
The severity and urgency of airway compromise often dictatethe modality used for diagnosis. A chest x-ray and CT scan ofthe thorax are warranted in a patient with suspected post-intubation tracheobronchial injury. The diagnostic sensitivity ofCT is 85% in tracheobronchial injury. CT angiography imagescan be processed by maximum intensity projection and mini-mum intensity projection (MinIP), which are volume renderingtechniques that define the volume of interest. Either the entireimage data set or the region of interest may be used. Organsfilled with air, eg, airways and sinuses, are shown using MinIP.
Fig 7. Intact defect on postoperative day 19. (
Three-dimensional surface shaded display (3-DSSD) recognizestissue either by its density (similar to CT) or manually bydrawing the contour of the organ and showing the surface of theorgans as an opaque object. When the cursor is placed within theairway of an image, the contours of the airway will be indicated.MinIP and 3-DSSD were used to reconstruct the trachealperforation in this case (Fig 3). Fiberoptic bronchoscopy is thegold standard for diagnosis confirmation and revealing the sizeand extent of a lesion.21 Because this patient arrived in the ORalready intubated, it was important to pull the ETT back toensure that the whole length of the trachea was evaluated.
OVERALL MANAGEMENT
Depending on the presenting signs and symptoms, as wellas the extent of the injury, treatment may consist of eitherconservative management or urgent surgical repair. A post-operative mortality as high as 40% has been reported afteriatrogenic rupture of the tracheobronchial tree.22 A studycomparing conservatively managed and surgical groupsreported a mortality rate of 29% and 2.8%, respectively. Thereis little consensus on management of postintubation trachealtears. Factors to consider include size, location, and depthof tear; associated esophageal injury; mediastinitis; andneed for ventilator support.23 Recent evidence suggests that
Color version of figure is available online.)

Table 1. Risk Factors for Tracheal Injury Based on Minambres
and Cardillo
Risk Factor
Minambres 1966–
2007 (n ¼ 182)
Cardillo 2003–
2008 (n ¼ 30)
Percent with
Risk Factor
Female gender 156 28 87%
Short stature
(o165 cm)*22 73%
Age 450 years* 16 53%
BMI Z25* 16 53%
Use of double-
lumen tube
85 4 42%
Emergency
intubation
50† 8 27%
Difficult
intubation
26 ‡ 14%
Abbreviation: BMI, body mass index.
*Analyzable data not available from Minambres study; mean age
was 61 years.
†Information not available for 12 patients in Minambres study.
‡Data not available from Cardillo study.
CASE 9–2014 1153
conservative management produces more favorable outcomesfor small lesions once the patient is clinically stable.21,24–27 Onthe other hand, immediate surgical repair is required when alesion is large enough to be life-threatening. Cardillo et alstaged tracheal lesions based on the tracheal wall involvement,from level I (mucosal or submucosal tracheal involvementwithout mediastinal emphysema and without esophagealinvolvement) to level IIIB (any laceration of the tracheal wallwith esophageal injury or mediatinitis).23 Primary signs ofmediastinitis, such as localized mediastinal fluid or pneumo-mediastinum or both, can be used to identify patients withmediastinitis. The site of the lesion determines the surgicalapproach as well as the surgical service to be called upon torepair it. High and mid-tracheal injuries usually are repaired byan otolaryngologist, and low tracheal and bronchial injuries, bya thoracic surgeon. A right-sided approach is recommended toavoid the large thoracic vessels. The authors propose analgorithm to help guide diagnosis and treatment of suspectedtracheal injuries based on experience at this institution andCardillo’s classification of tracheal injury (Fig 8).
ANESTHETIC MANAGEMENT
The fact that the surgeon and anesthesiologist share theairway presents a challenge in tracheal surgery. The surgeonneeds airway access and a surgical field unobstructed by theETT, and the anesthesiologist must provide adequate ventilationand oxygenation in the presence of an open airway. Ventilationcan be achieved by manual oxygen jet ventilation, high-frequency jet ventilation, distal tracheal intubation, or lungisolation using a bronchial blocker. In some instances, cardio-pulmonary bypass may be needed. Surgical repair of trachealinjuries requires general anesthesia with endotracheal intuba-tion. In this case, the surgeon approached the repair through aright thoracotomy to avoid the large vessels on the left side. Aright radial arterial catheter was inserted before induction ofanesthesia. Stable hemodynamics and adequate cerebral perfu-sion pressure were maintained. An intracranial pressure (ICP)monitor was placed soon after induction and opioids and beta-
blockers were given to prevent increases in ICP and worseningof the tracheal injury. Lidocaine was administered to preventpain, hypertension, tachycardia, and “bucking” on the tube.Because the surgery was planned for the region of the greatvessels, two 16-G intravenous catheters were placed to ensureadequate intravenous access in the event of a catastrophic bleed.
The lung isolation technique depends on the proximity ofthe lesion to the carina. The authors chose a left mainstemintubation with a single-lumen tube as the lesion was very closeto the carina. Left-sided DLT routinely are used for lungisolation but are bulky and cannot be used in an airway withpre-existing trauma. Bronchial blockers are another option. In asimilar case,28 the inner lumen of a 7F Arndt endobronchialblocker was used to ventilate the right lung with manual jetventilation at a jet frequency of 1 Hz, aiming for an inspiration-to-expiration ratio of 1:2. Although oxygenation was adequate,the patient retained CO2. If the authors had used this techniquein this patient, there would have been a massive air leak fromthe injury site. Further, CO2 retention in a patient with pre-existing brain injury would have led to an increase in ICP and aworse neurologic outcome. Dreyfuss et al recommended high-frequency ventilation for management of tracheobronchialtrauma, because it allows good ventilation without increasedpositive airway pressures even in the presence of pulmonarycontusion and avoids the need for a cuffed ETT, which coulddamage the tracheal suture line.29 Iwasaki reported that aUnivent tube, an ETT with a movable blocker capable ofexcluding one lung, facilitated perioperative and intraoperativerespiratory management by preventing aspiration of blood intothe healthy lung while maintaining adequate ventilation.30 Theauthors chose ventilator settings that ensured adequate ventila-tion while at the same time avoiding airway pressureincreases, which could further worsen the injury or compro-mise the repair after the case. It is advisable to maintain apeak airway pressure of 25 cmH2O or below. In this patient,ventilatory support and oxygenation were facilitated byendobronchial intubation by advancing the single-lumenETT into the left main bronchus but making sure the authorsdid not block the bifurcation of the left lung. Mechanicalventilation via the ETT was supplemented by intermittentmanual ventilation throughout the case. Clearly, the patientwith a possible tracheal injury should not be intubated orallyin a “blind” manner, even with direct visualization of thecords, to avoid distal tracheal injury. Most thoracic surgeonsand cardiothoracic anesthesiologists recommend endotrachealintubation under direct fiberoptic visualization to confirmpositioning distal to the damaged area. Both surgeon andanesthesiologist must be familiar with airway anatomy toensure correct placement of the ETT; otherwise, a falsepassage could be created into soft tissue through the trachealdefect. There also must be excellent communication andcoordination between the providers to ensure patient safetywith well-planned and executed airway management strat-egies. Inotropic or vasopressor support may be necessary,especially in patients with depressed ventricular function, tomaintain cerebral and coronary perfusion pressures. In theabsence of depressed ventricular function, a pure alpha-agonist such as phenylephrine infusion can be used tomaintain cerebral perfusion pressure without elevating
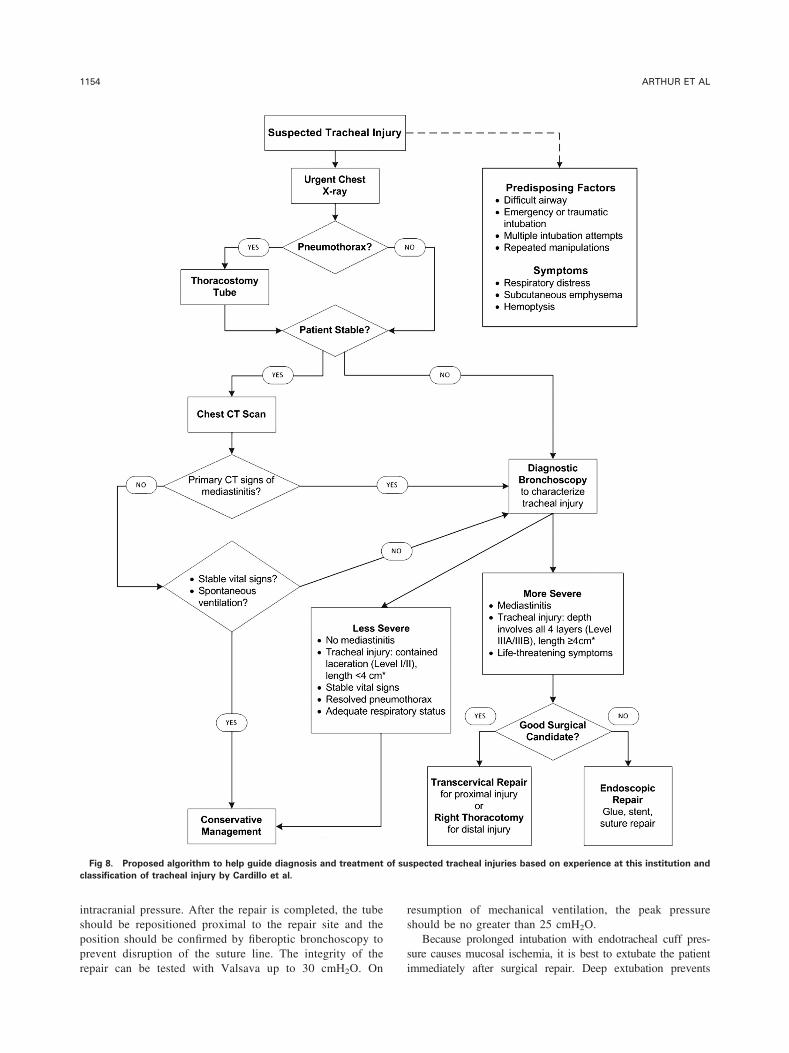
Fig 8. Proposed algorithm to help guide diagnosis and treatment of suspected tracheal injuries based on experience at this institution and
classification of tracheal injury by Cardillo et al.
ARTHUR ET AL1154
intracranial pressure. After the repair is completed, the tubeshould be repositioned proximal to the repair site and theposition should be confirmed by fiberoptic bronchoscopy toprevent disruption of the suture line. The integrity of therepair can be tested with Valsava up to 30 cmH2O. On
resumption of mechanical ventilation, the peak pressureshould be no greater than 25 cmH2O.
Because prolonged intubation with endotracheal cuff pres-sure causes mucosal ischemia, it is best to extubate the patientimmediately after surgical repair. Deep extubation prevents

CASE 9–2014 1155
coughing and bucking on the tube, which could disrupt thesuture lines. In patients with marginal respiratory status, thepatient should remain intubated and adequate sedation providedto prevent coughing and bucking. In a hemodynamically stablepatient, dexmedetomidine, an alpha-2 centrally acting agent, is agood choice for sedation because it allows for smooth extuba-tion; the patient remains calm and comfortable yet is easilyarousable and able to follow commands. In a hemodynamicallyvulnerable patient, continued intubation with mechanical ven-tilation may be needed until the patient is ready for extubation.Midazolam and fentanyl infusion are useful agents in such cases.Administration of systemic steroid injections may decrease theseverity of the inflammatory response and should be consideredin patients who are reintubated or intubated for prolongedperiods to decrease the incidence of tracheal damage.9,31
PROGNOSIS
Better diagnostic techniques and clinical judgment have ledto much earlier recognition and intervention. Tracheal injuryalways should be considered after endotracheal intubation iscompromised by hypoxemia, pneumomediastinum or pneumo-thorax, or subcutaneous emphysema without a known cause.Despite its rarity, tracheobronchial rupture always should beconsidered after blunt chest and neck trauma, and traumatic andemergent intubations, and should be recognized and treatedearly to restore lung function and prevent associatedcomplications.
SUMMARY
Tracheal tears are rare and potentially life-threateninginjuries that require a high index of suspicion to diagnose.Animal studies have shown that atraumatic intubations, multi-ple intubations, and prolonged contact with the cuff canincrease the likelihood for injury and that steroids may decreasethe inflammatory cascade, providing a protective effect.Because differences in tracheal anatomy also can affectincidence of injury, it is advisable to use a much smallerETT when intubating female or shorter patients.
Selection criteria for conservative or surgical managementof postintubation tracheal lacerations are a matter of debate. Ifthere are life-threatening symptoms, however, surgical closureis the obvious answer to restore effective ventilation andprevent short- and long-term complications such as medias-tinitis and tracheal stenosis.
COMMENTARY: CARDIOTHORACIC SURGEON’S
PERSPECTIVE†
Although rare, iatrogenic tracheobronchial injuries arecaused most commonly by endotracheal intubation, particularlyunder emergency or other stressful conditions. Similar injuriesalso have been associated with percutaneous tracheostomyinsertion.32 A high degree of suspicion is important for promptdiagnosis and management.
The most common clinical findings after these injuries issubcutaneous emphysema involving the upper chest and neck,
†V. S. Patel
mediastinal emphysema, hemoptysis, and pneumothorax. Theinitial evaluation often involves radiographic imaging, includ-ing a chest CT scan;33 however, the study of choice is adiagnostic fiberoptic bronchoscopy.34,35 The latter providesdirect visualization of the entire tracheobronchial anatomy toconfirm and define the lesion, including its location, length, anddepth. This information directs subsequent management of theinjury. In addition, fiberoptic bronchoscopy can facilitateairway management in nonoperative patients who requirecontinued mechanical ventilation. In surgical patients, intra-operative fiberoptic bronchoscopy is indispensable in facilitat-ing controlled endotracheal intubation and endotracheal tubeexchange, preventing worsening of the tracheal injury, andpositioning of the ETT.
The preferred treatment traditionally has been early surgicalintervention; however, the role for nonoperative managementhas grown.36,37 Despite the lack of universally acceptedmanagement guidelines, conservative management is favoredin patients with spontaneous ventilation with small lacerationsmeasuring less than 2 to 4 cm; the clinically stable withminimal and nonprogressive manifestations of subcutaneousand mediastinal emphysema, drained pneumothorax, absenceof mediastinitis and esophageal injury; and the critically ill whoare poor surgical candidates.23,38,39 Surgical intervention isfavored in patients with progressively worsening clinicalmanifestations, ventilator support instability, pneumothoraxwith large air leak and persistently collapsed lung, and largetears. Early surgical intervention provides reliable healing andavoids immediate and long-term complications includingabnormal scarring and stenosis, particularly in patients withdistal injuries involving the carina and subcarinal lacera-tions.40,41 Regardless of the treatment strategy selected, allpatients diagnosed with a tracheal laceration, including thosemanaged nonoperatively, should receive a broad spectrumantibiotic for at least 7 days.38
The surgical approach is based on the location of theinjury.41 Lacerations in the proximal two-thirds of the posteriormembranous wall can be repaired safely through atranscervical-transtracheal approach.40 The surgical procedureinvolves a cervical low-collar incision exposing the midlinetrachea. An anterior longitudinal tracheotomy allows access tothe posterior membranous injury. The field should be preparedfor a possible partial or full sternotomy. A previously posi-tioned small single-lumen ETT ensures adequate space forrepair of the injury. If necessary, the orotracheal tube can bewithdrawn and a new distal tracheal tube positioned throughthe tracheotomy to facilitate unhindered exposure and repair ofthe full extent of the injury. The latter would require intra-operative planning and preparation, including coordinationwith the anesthesia team for successful airway management.This approach preserves the vascular supply to the trachea andavoids injury to the recurrent laryngeal nerve during excessivetracheal dissection.
Injuries involving the distal trachea and subcarinal bronchusgenerally are approached through a right posterolateral thor-acotomy through the fourth or fifth intercostal space to provideexcellent exposure of the distal trachea, the bifurcation, andboth mainstem bronchi.42 In rare cases of distal left bronchialinjuries, the left thoracotomy approach is preferable. Single-

ARTHUR ET AL1156
lung isolation and stable airway management are vital andaccomplished using fiberoptic bronchoscopy and activeengagement of the anesthesia team. The importance of planningthe intraoperative airway management with the anesthesia teamcannot be overemphasized for a successful outcome. Therepaired injury typically is buttressed with an intercostal muscleor pleural flap.43 Surgical intervention provides a definitive andrelatively safe treatment for these complex injuries.41,44 Thepostoperative prognosis generally is dictated by preoperativerisk factors, including patient age, emergency intubation, malegender, underlying medical comorbidities that necessitatemechanical ventilation, delayed diagnosis, and mediastini-tis.21,45 Recent reports of endoscopic repair techniques includeapplications of glue, suture repair, and placement of stent tocover the injury. Their role in future management of theseinjuries is yet to be defined.46,47
COMMENTARY: OTOLARYNGOLOGIST’S PERSPECTIVE‡
The trachea extends proximally from the larynx through theneck to enter the mediastinum and intrathoracic segment distally.Thus, surgical evaluation and intervention for serious trachealairway issues such as stenosis, cancer, or trauma often involveboth otolaryngology and cardiothoracic surgery. Because thisparticular injury was confined to the distal trachea at the level ofthe carina, surgical intervention was appropriately led by thecardiothoracic surgery team. It should be noted that in anemergency situation involving a suspected airway injury, theanesthesiologist (or intensivist) should consider consulting bothservices if they are available. Otolaryngologists often are wellversed in emergency airway management and positioned toprovide a rapid initial endoscopic evaluation of the trachea. Incenters with a focus on airway reconstruction, it is common forthe two services to share cases and complement each other’sexpertise. Proximal injuries are better managed through a cervicalapproach by the otolaryngology team, whereas distal lesionsusually require a thoracotomy or sternotomy approach. Often ajoint approach is indicated, and even cervical tracheal repair cannecessitate thoracic maneuvers to release tension on the trachea.48
In nonoperative situations, such as when the patient is in theintensive care unit with a suspected tracheal injury, a high-resolution CT greatly can impact surgical planning if thepatient’s condition allows.49
The surgical approach will be dictated by the nature of theinjury and the patient’s clinical presentation. Often if the injury isproximal (as opposed to near the carina), less than 3 cm in size,and one that does not involve the esophagus, conservative
‡P. M. Weinberger
management can be successful.50 The disrupted tracheal mucosais allowed to repair without surgical closure by either clinicalobservation alone or by advancing the ETT cuff distal to theinjury. Placement of the ETT without further expanding theinjury is critical. This is best accomplished by passing anendoscope distal to the injury and advancing the ETT over theendoscope (a modified Seldinger technique using the endoscopeas the guidewire). The patient is left on mechanical ventilationfor several days to a week, and the area of injury examinedendoscopically, usually in the OR. If this approach fails or if theinjury is large or involves the esophagus, an open approach isnecessary.48 Occasionally, the site of injury can be accessed viaan anterior tracheostomy, with endoscopic visualization fromabove (transglottic) although suturing can be quite problematicthrough this limited access. For patients with suspected esoph-ageal disruption, an esophagoscopy at the time of repair ismandated. The cervical operative site is flooded with saline, andair is insufflated into the esophagus while observing theoperative site for air bubbles. If an injury are noted, it shouldbe repaired directly and a muscle flap or acellular skin graftinterposed between the tracheal repair and the esophageal repair.Most often a circumferential tracheal transection and reanasto-mosis are required to obtain adequate access to the esophagealinjury in these cases.48
The otolaryngologist is uniquely equipped to evaluate vocalfold motion after the repair. Injury to the recurrent laryngealnerve during tracheal surgery, although uncommon, is certainlywithin the realm of possibility and should be ruled out.Additionally, multiple and emergency intubations increase thelikelihood of arytenoid dislocation, which usually can becorrected if identified early. It has been suggested that clinicalmonitoring for hoarseness or stridor is inadequate for detectingvocal fold immobility, so endoscopic evaluation of vocal foldmotion is recommended.49
The prognosis varies according to the degree of injury.Patients with proximal tracheal injuries without esophagealinvolvement have an excellent prognosis barring other fac-tors.50 For patients with distal injuries (such as the present case)or esophageal involvement, outcomes tend to be less favorablebut can still be quite good if managed appropriately.
ACKNOWLEDGMENTS
The authors thank William Bates, MD at the Medical College ofGeorgia at Georgia Regents University for his help in the 3Dreconstruction of the trachea showing the tear.
REFERENCES
1. Lampl L: Tracheobronchial injuries. Conservative treatment.Interact Cardiovasc Thorac Surg 3:401-405, 20042. Maxeiner H: Weichteilverletzungen am Kehlkopf bei notfallmä-
ßiger Intubation. Anästh Intensivmed 29:42-49, 19883. Domino KB, Posner KL, Caplan RA, et al: Airway injury during
anesthesia: A closed claims analysis. Anesthesiology 91:1703-1711, 1999
4. Marty-Ane CH, Picard E, Jonquet O, et al: Membranous trachealrupture after endotracheal intubation. Ann Thorac Surg 60:1367-1371, 19955. Kaloud H, Smolle-Juettner FM, Prause G, et al: Iatrogenic
ruptures of the tracheobronchial tree. Chest 112:774-778, 19976. Tewfik TL: Trachea anatomy. Medscape Reference Web site.
http://emedicine.medscape.com/article/1949391-overview#showall.Updated June 19, 2013. Accessed November 5, 2013.7. Borasio P, Ardissone F, Chiampo G: Post-intubation tracheal
rupture. A report on ten cases. Eur J Cardiothorac Surg 12:98-100,
1997
CASE 9–2014 1157
8. Jaeger K, Ruschulte H, Osthaus A, et al: Tracheal injury as asequence of multiple attempts of endotracheal intubation in the courseof a preclinical cardiopulmonary resuscitation. Resuscitation 43:147-150, 20009. Oshodi A, Dysart K, Cook A, et al: Airway injury resulting from
repeated endotracheal intubation: Possible prevention strategies. PediatrCrit Care Med 12:e34-e39, 201110. Sarper A, et al: Tracheal stenosis after tracheostomy or intuba-
tion: review with special regard to cause and management. Tex HeartInst J 32:154-158, 200511. Liu J, Zhang X, Gong W, et al: Correlations between controlled
endotracheal tube cuff pressure and postprocedural complications: Amulticenter study. Anesth Analg 111:1133-1137, 201012. Joe HB, Kim DH, Chae YJ, et al: The effect of cuff pressure on
postoperative sore throat after Cobra perilaryngeal airway. J Anesth 26:225-229, 201213. Kastanos N, Estopá Miró R, Marín Perez A, et al: Laryngo-
tracheal injury due to endotracheal intubation: Incidence, evolution, andpredisposing factors. A prospective long-term study. Crit Care Med 11:362-367, 198314. Nseir S, Duguet A, Copin MC, et al: Continuous control of
endotracheal cuff pressure and tracheal wall damage: A randomizedcontrolled animal study. Crit Care 11:R109, 200715. Fitzmaurice BG, Brodsky JB: Airway rupture from double-lumen
tubes. J Cardiothorac Vasc Anesth 13:322-329, 199916. Liu H, Jahr JS, Sullivan E, et al: Tracheobronchial rupture after
double-lumen endotracheal intubation. J Cardiothorac Vasc Anesth 18:228-233, 200417. Hannallah MS, Benumof JL, Ruttimann UE: The relationship
between left mainstem bronchial diameter and patient size. J Cardio-thorac Vasc Anesth 9:119-121, 199518. Russell WJ, Strong TS: Dimensions of double-lumen tracheo-
bronchial tubes. Anaesth Intensive Care 31:50-53, 200319. Brodsky JB, Lemmens HJ: Tracheal width and left double-lumen
tube size: A formula to estimate left-bronchial width. J Clin Anesth 17:267-270, 200520. Chow MY, Liam BL, Thng CH, et al: Predicting the size of a
double-lumen endobronchial tube using computed tomographic scanmeasurements of the left main bronchus diameter. Anesth Analg 88:302-305, 199921. Minambres E, Burón J, Ballesteros MA, et al: Tracheal rupture
after endotracheal intubation: A literature systematic review. Eur JCardiothorac Surg 35:1056-1062, 200922. Hofmann HS, Rettig G, Radke J, et al: Iatrogenic ruptures of the
tracheobronchial tree. Eur J Cardiothroac Surg 21:649-652, 200223. Cardillo G, Carbone L, Carleo F, et al: Tracheal lacerations after
endotracheal intubation: A proposed morphological classification to guidenon-surgical treatment. Eur J Cardiothorac Surg 37:581-587, 201024. Beiderlinden M, Adamzik M, Peters J: Conservative treatment of
tracheal injuries. Anesth Analg 100:210-214, 200525. Chen EH, Logman ZM, Glass PS, et al: A case of tracheal injury
after emergent endotracheal intubation: A review of the literature andcausalities. Anesth Analg 93:1270-1271, table of contents, 200126. Mullan GP, Georgalas C, Arora A, et al: Conservative manage-
ment of a major post-intubation tracheal injury and review of currentmanagement. Eur Arch Otorhinolaryngol 264:685-688, 200727. Prunet B, Lacroix G, Asencio Y, et al: Iatrogenic post-intubation
tracheal rupture treated conservatively without intubation: A casereport. Cases J 1:259, 200828. Luyet C, Boudah R, McCartney CJ, et al: Low-frequency jet
ventilation through a bronchial blocker for tracheal repair after a rarecomplication of percutaneous dilatational tracheostomy. J CardiothoracVasc Anesth 27:108-110, 2013
29. Dreyfuss D, Jackson RS, Coffin LH, et al: High-frequency ventila-tion in the management of tracheal trauma. J Trauma 26:287-289, 198630. Iwasaki M, Kaga K, Ogawa J, et al: Bronchoscopy findings and
early treatment of patients with blunt tracheo-bronchial trauma.J Cardiovasc Surg 35:269-271, 199431. Othersen HB Jr: Intubation injuries of the trachea in children.
Management and prevention. Ann Surg 189:601-606, 197932. Walz MK, Peitgen K, Thürauf N, et al: Percutaneous dilatational
tracheostomy–Early results and long-term outcome of 326 critically illpatients. Intensive Care Med 24:685-690, 199833. Scaglione M, Romano S, Pinto A, et al: Acute tracheobronchial
injuries: Impact of imaging on diagnosis and management implications.Eur J Radiol 59:336-343, 200634. Baumgartner FJ, Ayres B, Theuer C: Danger of false intubation
after traumatic tracheal transection. Ann Thorac Surg 63:227-228,199735. Rossbach MM, Johnson SB, Gomez MA, et al: Management of
major tracheobronchial injuries: A 28-year experience. Ann ThoracSurg 65:182-186, 199836. Conti M, Pougeoise M, Wurtz A, et al: Management
of postintubation tracheobronchial ruptures. Chest 130:412-418, 200637. Schneider T, Storz K, Dienemann H, et al: Management of
iatrogenic tracheobronchial injuries: A retrospective analysis of 29cases. Ann Thorac Surg 83:1960-1964, 200738. Jougon J, Ballester M, Choukroun E, et al: Conservative treat-
ment for postintubation tracheobronchial rupture. Ann Thorac Surg 69:216-220, 200039. Gomez-Caro Andres A, Moradiellos Díez FJ, Ausín Herrero P,
et al: Successful conservative management in iatrogenic tracheobron-chial injury. Ann Thorac Surg 79:1872-1878, 200540. Angelillo-Mackinlay T: Transcervical repair of distal membra-
nous tracheal laceration. Ann Thorac Surg 59:531-532, 199541. Mussi A, Ambrogi MC, Menconi G, et al: Surgical approaches to
membranous tracheal wall lacerations. J Thorac Cardiovasc Surg 120:115-118, 200042. Gabor S, Renner H, Pinter H, et al: Indications for surgery in
tracheobronchial ruptures. Eur J Cardiothorac Surg 20:399-404,200143. Anderson TM, Miller JI Jr: Use of pleura, azygos vein,
pericardium, and muscle flaps in tracheobronchial surgery. Ann ThoracSurg 60:729-733, 199544. Carbognani P, Bobbio A, Cattelani L, et al: Management of
postintubation membranous tracheal rupture. Ann Thorac Surg 77:406-409, 200445. Leinung S, Möbius C, Hofmann HS, et al: Iatrogenic tracheo-
bronchial ruptures - treatment and outcomes. Interact CardiovascThorac Surg 5:303-306, 200646. Marchese R, Mercadante S, Paglino G, et al: Tracheal stent to
repair tracheal laceration after a double-lumen intubation. Ann ThoracSurg 94:1001-1003, 201247. Welter S, Jacobs J, Krbek T, et al: A new endoscopic technique
for intraluminal repair of posterior tracheal laceration. Ann Thorac Surg90:686-688, 201048. Grillo HC: Reconstruction of the trachea. Experience in 100
consecutive cases. Thorax 28:667-679, 197349. Sulica L: Hoarseness misattributed to reflux: sources and patterns
of error. Transactions of the 2010 Meeting of the American Laryngo-logic Association, Las Vegas, Nevada, April 2010, p. 42. Available athttp://www.alahns.org/i4a/pages/index.cfm?pageid=3502. AccessedNovember 4, 2013.50. Carretta A, Melloni G, Bandiera A, et al: Conservative and
surgical treatment of acute posttraumatic tracheobronchial injuries.World J Surg 35:2568-2574, 2011