Discerning Pictures: how we look at and understand pictures in comics
Upload
independentCategory
view
3download
0
Subtypes of anhedonia and facial electromyography response tonegative affective pictures in non-psychiatric adults
L.S. Kadison, K.A. Ragsdale, J.C. Mitchell, J.E. Cassisi and J.S. Bedwell*
Psychology Department, University of Central Florida, 4111 Pictor Lane, Orlando, FL, USA
(Received 23 May 2013; accepted 8 August 2014)
Introduction. Flat/constricted affect and anhedonia are symptoms found in severalpsychiatric disorders such as depression and schizophrenia. However, there are veryfew studies on the relationships between specific anhedonia subtypes and objectivelyassessed flat affect, and it appears that none of the existing studies examined potentialmoderation by sex.Methods. Forty-seven undergraduate students (60% male) completed self-report ques-tionnaires assessing three subtypes of anhedonia – non-social consummatory (CON)and anticipatory (ANT) anhedonia, and overall social anhedonia. Participants viewed15 pictures (5 neutral and 10 negative) from the International Affective Picture System,whereas facial muscle reaction was recorded using electromyography (EMG).Results. Male participants reporting a greater level of overall social or non-social CONanhedonia showed a greater EMG activity increase in the corrugator supercilii muscleto negative (vs. neutral) pictures. In females, the relationship was only found withsocial anhedonia and was opposite in direction, as increased social anhedonia related toless EMG activity change in the corrugator muscle.Conclusions. The relationship between anhedonia and flat affect varied as a function ofsex and anhedonia subtype. These findings may help explain discrepancies in thesparse existing literature examining this relationship in psychiatric populations andhave implications for assessment and treatment of these symptoms across psychiatricdisorders.
Keywords: anhedonia; facial; emotion; expression; electromyography
Anhedonia refers to a deficit in the experience of pleasure and is often broken down intotwo distinct subtypes: consummatory (CON) and anticipatory (ANT). CON anhedoniarefers to a decreased capacity for pleasure in the moment (e.g., the enjoyment of the smellof freshly cut grass), whereas ANT anhedonia specifies diminished pleasure when thinkingabout an upcoming event (e.g., deriving pleasure from the anticipation of a favouritemeal). Anhedonia can also be defined based on the type of stimulus, such as social or non-social. Social anhedonia is a lessened experience of pleasure from various types ofinterpersonal interactions (discernible from social anxiety; Brown, Silvia, Germeys, &Kwapil, 2007). Non-social anhedonia refers to a deficit in the experience of pleasure inresponse to a stimulus or situation that is not primarily related to interpersonal interactions.
Anhedonia is considered a core symptom of several psychiatric disorders includingschizophrenia-spectrum, depressive and bipolar disorders (American Psychiatric Association,
*Corresponding author. Email: [email protected]
Cognitive Neuropsychiatry, 2015Vol. 20, No. 1, 31–40, http://dx.doi.org/10.1080/13546805.2014.955172
© 2014 Taylor & Francis
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

2013); however, specific subtypes appear to be more prevalent within certain disorders.For example, several studies have shown that schizophrenia and depression are associatedwith intact CON pleasure but deficient ANT pleasure (Heerey & Gold, 2007; Horan,Blanchard, Clark, & Green, 2008; Horan, Wynn, Kring, Simons, & Green, 2010; althoughsee Strauss, Wilbur, Warren, August, & Gold, 2011; depression: see review by Dichter,2010). Further, social anhedonia is particularly predictive of later development ofschizophrenia (Gooding, Tallent, & Matts, 2005; Kwapil, 1998). Additionally, malestend to report more social and non-social anhedonia than females in both clinical andnon-clinical samples (Fonseca-Pedrero, Lemos-Giraldez, Muniz, Garcia-Cueto, &Campillo-Alvarez, 2008; Miettunen & Jaaskelainen, 2010).
Diminished facial expressivity in response to emotional stimuli is another coresymptom of many psychiatric disorders and is a subtype of what is often referred to asconstricted or flattened affect. Whereas flat affect may appear to be a manifestation ofanhedonia, it is not the same construct. Anhedonia is an internal emotional experience,whereas flattened affect is outward expression. Further, anhedonia is defined asdiminished positive emotion, unlike flat affect, which is diminished positive and negativeemotion expression. Facial electromyography (EMG) is an objective measure of facialemotional expression with good psychometric properties (Fridlund & Cacioppo, 1986;Lee, Shackman, Jackson, & Davidson, 2009). EMG can differentiate negatively andpositively valenced emotional reactions by measuring activity in the corrugator superciliiand zygomatic major facial muscle groups, respectively (Cacioppo, Berntson, Larsen,Poehlmann, & Ito, 2000). Research using facial EMG has consistently reporteddiminished expressivity in response to emotional stimuli in a subset of individuals withschizophrenia (see review by Kring & Moran, 2008) and depression (Greden, Genero,Price, Feinberg, & Levine, 1986). Further, sex differences have been reported, as femalesdisplay greater facial EMG signals in response to unpleasant pictures than males(Dimberg & Lundquist, 1990; Huang & Hu, 2009; Lundqvist, 1995).
Research examining relationships between anhedonia and flattened affect in schizo-phrenia have produced mixed results. One study with individuals with schizophrenia foundthat increased clinician-rated anhedonia was related to reduced inflection in speech – oneform of flattened affect (Cohen, Alpert, Nienow, Dinzeo, & Docherty, 2008). However,another study found no relationship between clinician-rated anhedonia and the use ofpositive or negative emotional words in spoken narratives in a schizophrenia sample(Alpert, Rosenberg, Pouget, & Shaw, 2000). To gain further insight into the relationshipof flattened affect and anhedonia, it is important to study these constructs in non-psychiatric samples, which will allow the examination of the relationships without con-founds often present in psychiatric disorders (e.g., medication effects, complex symptominteractions). Leung, Couture, Blanchard, Lin, and Llerena (2010) found that higherlevels of social anhedonia were related to diminished facial expressivity in response toemotional film clips in a female non-psychiatric sample. However, an earlier study com-bining non-psychiatric males and females found that higher physical (i.e., primarily non-social) anhedonia was related to greater (rather than diminished) facial expressivityto both positive and negative stimuli (Fitzgibbons & Simons, 1992). Overall, thisrelationship has only been directly examined using objective markers of expressivity in ahandful of studies, which vary in the type of sample examined, anhedonia assessed,and emotional expression assessed. The potential moderation of sex also needs to beexamined in this relationship, as sex has been found to be a greater predictor of facialexpressivity than anhedonia (Berenbaum, Snowhite, & Oltmanns, 1987).
32 L.S. Kadison et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

To address this gap in research, the current study examined the relationshipbetween three self-reported anhedonia subtypes (i.e., overall social anhedonia, andnon-social ANT and CON anhedonia) and facial affective expressivity to negativelyvalenced pictures in non-psychiatric males and females. This study further contributesto the existing literature by examining the potential moderation of sex on theserelationships. A better understanding of this relationship informs assessment andtreatment across populations presenting with these symptoms. For example, examiningwhether sex moderates this relationship will inform clinicians who are assessing andtreating these symptoms to consider how the presentation and response to treatment mayvary by sex.
It was hypothesised that sex and social anhedonia will interact in relation to facialexpressivity to negatively valenced pictures; however, given the mixed existingliterature on this topic, examination of the simple effects will be exploratory. Weexpected moderation of sex based on findings of increased facial expressivity in females(Dimberg & Lundquist, 1990; Huang & Hu, 2009; Lundqvist, 1995) and greater self-reported anhedonia in males (Fonseca-Pedrero et al., 2008; Miettunen & Jaakelainen,2010). In terms of non-social anhedonia, CON, rather than ANT, anhedonia washypothesised to show a more robust relationship with EMG, as it reflects self-report oftypical “in-the-moment” emotion, similar to the in-the-moment EMG assessment. Inaddition, social, rather than non-social, anhedonia was hypothesised to have a strongerrelationship to the EMG response, as social anhedonia has shown stronger links toschizophrenia (Gooding et al., 2005; Kwapil, 1998) – a disorder that often includesflat affect.
Methods
Participants
Participants were enrolled in courses offered by a Psychology Department of a largeuniversity in the USA, using an online recruitment system that awarded course credit inreturn for participation. Participants were recruited as part of a larger study (Mitchell et al.,under review), which included an online administration of the Schizotypal PersonalityQuestionnaire (SPQ; Raine, 1991) and two validity scales. After excluding individualsbased on the validity scales or incomplete responses, participants falling in the topand bottom twentieth percentile on the SPQ total score were invited to participate in thelab-based portion of this study.
Forty-nine individuals participated in the lab-based study; however, two individualswere excluded from the data analysis due to invalid EMG data (as a result of artefact).Therefore, the final sample consisted of 47 participants (60% male). The average age ofthis sample was 20.37 (SD = 4.74), and the reported race was 66.1% Caucasian, 14.3%“Mixed/Other,” 10.7% Hispanic, 5.4% African American and 3.6% Asian. Althoughparticipants were initially recruited based on the online SPQ total scores beingrelatively high or low, the scores from a lab-based re-administration of the SPQreflected a relatively normal, but wide, distribution. As the relationships between theSPQ and the EMG data (without considering anhedonia) have been previously reportedfor this sample (Mitchell et al., under review), the present study will focus onrelationships between the self-reported anhedonia and the EMG, when covarying for theSPQ total score.
Cognitive Neuropsychiatry 33
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

Measures
Temporal Experience of Pleasure Scale (TEPS)
The TEPS is an 18-item self-report measure that provides subscales for CON and ANTpleasure and has been found to have good psychometric properties (Gard, Gard-Germans,Kring, & Oliver, 2006). The TEPS assesses CON and ANT pleasure in primarily non-social contexts. It is scored on a Likert scale ranging from very false for me (1) to verytrue for me (6), with lower scores indicating more anhedonia.
Anticipatory and Consummatory Interpersonal Pleasure Scale (ACIPS)
The ACIPS is a recently developed 17-item self-report measure designed to measuresocial and interpersonal pleasure (Gooding & Pflum, 2014a, 2014b). The ACIPS isscored on a 6-point Likert scale, with lower scores indicating more social anhedonia. Asfactor analysis on this measure does not support the use of separate ANT and CONsubscales (Gooding & Pflum, 2014b), we used the total score in our analyses. Twostudies have revealed that the ACIPS total score has high internal consistency along withgood convergent and discriminant validity (Gooding & Pflum, 2014a, 2014b).
Self-Assessment Manikin (SAM)
The SAM (Lang, Bradley, & Cuthbert, 2008) was used during the lab-based phase toassess arousal and affective valence in response to affective pictures using the numberkeys 1–9 on a keyboard. Arousal is measured on a range from calm (1) to excited (9) inresponse to a figure which illustrates arousal level. Similarly, valence is measured on ascale from unpleasant (1) to pleasant (9) in response to a figure which illustrates valence.
Affective Picture Electromyography Task (APET)
Based on the published normative ratings using the SAM affective rating system,5 neutral pictures and 10 negatively valenced pictures (containing images of threateningstimuli and others in distress) were selected from the International Affective PictureSystem (IAPS; Lang et al., 2008). Normative SAM ratings for the 15 pictures arepresented in Table 1. Using E-Prime 2.0 (Psychology Software Tools), each picture wasdisplayed for 8 seconds, immediately followed by the SAM ratings (unlimited time) andby an interstimulus interval that randomly varied between 30 and 40 seconds.
Procedure
The lab-based session consisted of informed consent, a re-administration of the SPQ(paper version) and administration of the TEPS, ACIPS and APET. During the APET,EMG signals over the corrugator supercilii and the zygomatic major muscle groups wererecorded using MindWare Technologies Inc. (Gahanna, OH) and BioLab Acquisitionsoftware (Version 3.0; MindWare Technologies, 2010). Five cup-style Ag–AgCl facialelectrodes (two measuring corrugator supercilii, two measuring zygomatic major and oneground electrode) were filled with saline conductive gel and placed on the participantusing 4-mm adhesive discs. EMG signals were amplified at a gain of 2,000.
Data processing and statistical analyses
Offline data were subjected to a 30–200-Hz band pass filter to partially excludemovement and eye-blink artefact. The signal was then rectified to convert the
34 L.S. Kadison et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

negative-to-positive range of values to absolute values. The peak amplitude of theEMG signal (measured in microvolts) during the 8 seconds following each stimuluswas identified. We then calculated peak EMG amplitude change scores separately foreach of the two muscle groups by subtracting the average peak amplitude during theneutral pictures from the average peak amplitude during the negatively valencedpictures. This peak EMG amplitude change score was used for all analyses. Each of thethree scales of pleasure (ANT and CON TEPS and total ACIPS scores) was examinedin separate 2 × 2 mixed analyses of covariance that examined the influence of sex,anhedonia and interaction in relation to the peak EMG amplitude change score, whencovarying for the SPQ total score. In addition, 2 × 2 mixed multivariate analysesof covariances (MANCOVAs) were used to examine the relationship between each ofthe anhedonia subtypes and sex (and interaction) on the combination of the arousaland valence from the SAM ratings, when controlling for the SPQ score. Furtherexploratory analyses were conducted using partial correlations, which controlled forthe SPQ score.
Results
The descriptive statistics for all measures can be found in Table 2, and zero-ordercorrelations can be found in Table 3.
Anticipatory non-social pleasure (TEPS-ANT) and change incorrugator EMG response
There was no main effect of sex, F(1, 42) = 1.79, p = .19, ή = .04, or TEPS-ANT,F(1, 42) = .001, p = .97, ή < .001, and no interaction between sex and TEPS-ANT,F(1, 42) = 1.97, p = .17, ή = .05.
Table 1. Normative ratings of IAPS pictures using the SAM.
IAPS picture number/description Valence rating, M (SD) Arousal rating, M (SD)
Negative 9,413, men being hanged 1.76 (1.08) 6.81 (2.09)2,703, crying children 1.91 (1.26) 5.78 (2.25)9,075, starving child 1.29 (.64) 6.57 (2.39)6,500, knife to throat 2.73 (2.38) 7.09 (1.98)3,168, mutilated face 1.56 (1.06) 6.00 (2.46)1,114, open mouth edsnake 4.03 (2.16) 6.33 (2.17)1,525, attack dog 3.09 (1.72) 6.51 (2.25)2,120, close up of angry male face 3.34 (1.91) 5.18 (2.52)6,260, gun pointed at observer 2.44 (1.54) 6.93 (1.93)6,830, masked man with guns 2.82 (1.81) 6.21 (2.23)
Neutral 7,000, rolling pin 5.00 (.84) 2.42 (1.79)7,010, wicker basket 4.94 (1.07) 1.76 (1.48)7,175, lamp 4.87 (1.00) 1.72 (1.26)7,090, book 5.19 (1.46) 2.61 (2.03)7,080, fork 5.27 (1.09) 2.32 (1.84)
Cognitive Neuropsychiatry 35
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

Consummatory non-social pleasure (TEPS-CON) and change incorrugator EMG response
There was a significant main effect of sex, F(1, 42) = 8.93, p = .005, η2 = .17, as femalesshowed a greater change in corrugator EMG response. There was no main effect forTEPS-CON, F(1, 42) = .20, p = .66, η2 = .005. However, there was a significantinteraction between sex and TEPS-CON, F(1, 42) = 9.21, p = .004, η2 = .18. Aftercovarying for the SPQ total score, males showed a significant negative correlation
Table 2. Descriptive statistics by sex.
Males (N = 28) Females (N = 19)
Mean SD Range Mean SD Range
1. ACIPS total 82.11 10.79 44–97 87.05 7.01 72–992. TEPS-CON 37.46 5.59 28–47 38.86 5.75 23–473. TEPS-ANT* 44.00 6.79 33–58 48.00 4.4 41–594. ZYGO –.85 2.51 –8.1 to 3.92 –.19 1.21 –3.87 to 2.055. CORR .96 2.38 –5.06 to 7.4 1.20 3.90 –6.96 to 106. Arousal 2.77 1.29 –.30 to 4.90 3.54 1.69 –.30 to 5.607. Valence –2.06 1.11 –4.3 to –.300 –2.62 1.15 –4.6 to –.608. SPQ total score 25.07 17.03 3–63 21.95 16.18 2–589. Constrict Affect 2.46 1.97 0–7 1.63 1.67 0–6
ACIPS total = total score on the Anticipatory and Consummatory Interpersonal Pleasure Scale; TEPS-CON =total Consummatory score on the Temporal Experience of Pleasure Scale; TEPS-ANT = total Anticipatory scoreon the Temporal Experience of Pleasure Scale; ZYGO = peak amplitude of the zygomatic major EMG tonegative minus neutral pictures; CORR = peak amplitude of the corrugator supercilii EMG to negative minusneutral pictures; Arousal = average SAM arousal rating to negative minus neutral pictures; Valence = averageSAM valence rating to negative minus neutral pictures; SPQ = Schizotypal Personality Questionnaire; ConstrictAffect = total score on Constricted Affect Subscale of the SPQ.*p < .05 between sexes.
Table 3. Zero-order correlations by sex; males (N = 28) are shown below the diagonal, andfemales (N = 19) are shown above the diagonal.
1. 2. 3. 4. 5. 6. 7. 8. 9.
1. ACIPS total — .38 .38 –.01 .45* .38 –.31 –.13 –.302. TEPS-CON .53** — –.15 .04 .40 .57* –.50* .14 –.0033. TEPS-ANT .60** .49** — .29 .12 .22 –.04 .36 .154. ZYGO –.07 –.15 –.11 — .17 .06 .15 .29 .165. CORR –.56** –.47* –.38* .19 — .29 –.43 .08 –.096. Arousal .17 .13 .36 .24 –.08 — –.76** –.08 –.227. Valence .05 –.30 –.18 .13 .07 –.48** — .19 .378. SPQ total –.06 .13 –.05 .06 –.22 –.16 –.11 — .86**9. Constrict Affect –.34 –.14 –.22 –.08 .11 –.20 –.08 .59** —
ACIPS total = total score on the Anticipatory and Consummatory Interpersonal Pleasure Scale; TEPS-CON =total Consummatory score on the Temporal Experience of Pleasure Scale; TEPS-ANT = total Anticipatory scoreon the Temporal Experience of Pleasure Scale; ZYGO = peak amplitude of the zygomatic major EMG tonegative minus neutral pictures; CORR = peak amplitude of the corrugator supercilii EMG to negative minusneutral pictures; Arousal = average SAM arousal rating to negative minus neutral pictures; Valence = averageSAM valence rating to negative minus neutral pictures; SPQ total = total score from Schizotypal PersonalityQuestionnaire; and Constrict Affect = Constricted Affect Subscale of the SPQ.*p < .05; **p < .01.
36 L.S. Kadison et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

between TEPS-CON and the corrugator EMG change (i.e., a greater level of CONnon-social anhedonia related to a greater EMG change), r(25) = –.46, p = .02, whereasfemales showed no relationship, r(16) = .39, p = .11.
ACIPS total score and change in corrugator EMG response
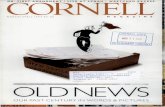
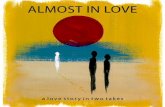
There was a significant main effect of sex, F(1, 42) = 11.88, p = .001, η2 = .22, as femalesshowed a greater change in corrugator EMG response. There was no main effect forACIPS total score, F(1, 42) = 1.35, p = .25, η2 = .03. However, there was a significantinteraction between sex and ACIPS total score, F(1, 42) = 12.30, p = .001, η2 = .23. Aftercovarying for the SPQ total score, males showed a significant negative correlationbetween the ACIPS total score and the corrugator EMG change (i.e., a greater level ofsocial anhedonia related to a greater EMG change), r(25) = –.59, p = .001 (see Figure 1),whereas females showed a significant positive relationship (i.e., a greater level of socialanhedonia related to a weaker EMG change), r(16) = .47, p = .05 (see Figure 2).
Anhedonia ratings and change in zygomatic EMG response(negative minus neutral pictures)
Results revealed that there was no main effect of anhedonia or sex, and no interactionbetween sex and anhedonia for any of the three anhedonia subtypes (all ps > .50).
Anhedonia ratings and subjective SAM ratings of pictures
MANCOVAs revealed that, of the three anhedonia subtypes, only TEPS-CON showed asignificant relationship with the two SAM ratings (arousal and valence), F(2, 41) = 5.12,p = .01, ή = .20, but there was no interaction between the TEPS-CON and sex in thisrelationship, F(2, 41) = 1.83, p = .17, ή = .08. Partial correlations of this main effect(controlling for SPQ) showed a positive relationship between the TEPS-CON and thearousal change, r(44) = .37, p = .01, and a negative relationship between the TEPS-CON
Figure 1. Scatterplot of EGM peak amplitude change in corrugator muscle in relation to theACIPS total score in male participants.
Cognitive Neuropsychiatry 37
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

and the valence change, r(44) = –.40, p = .01. Individuals with more CON non-socialanhedonia (i.e., lower TEPS-CON score) showed less of an increase in arousal, but agreater decrease in valence (i.e., more unpleasant), to negative, compared with neutral,pictures.
Conclusions
The hypothesis that sex and anhedonia would interact in relation to facial expressivitywas supported. With regard to CON non-social anhedonia, increased anhedonia related to agreater EMG change in males, but no relationship was found for females. This resultwas consistent with a study with a non-psychiatric sample that also found an increasedEMG change to negative pictures in relation to physical anhedonia, although that studydid not explore moderation of sex (Fitzgibbons & Simons, 1992). The heightened negativeresponse to negatively valenced stimuli in our male participants could relate to a poten-tiation of negative emotion seen in anhedonic conditions (e.g., depression), or suggest thatnegative expression is less blunted than positive, which has been reported in depression(Bylsma, Morris, & Rottenberg, 2008). Consistent with the EMG results, individuals withmore CON non-social anhedonia showed a greater increase in self-reported negativevalence to the negative pictures. Whereas this finding was limited to males with the EMG,the relationship with behavioural ratings was found across both sexes.
Overall social anhedonia, as expected, showed the strongest relationships with theEMG response. Consistent with CON non-social anhedonia, greater social anhedoniarelated to a greater EMG response in males (see Figure 1). However, females showed asignificant, albeit weaker, relationship in the opposite direction; more social anhedoniarelated to a weaker EMG change in females (see Figure 2). This is consistent with one studythat examined non-psychiatric females, which also found that greater social anhedoniarelated to a weaker facial expressivity change (Leung et al., 2010). Social anhedonia did notrelate to the behavioural ratings of the pictures within either sex.
Figure 2. Scatterplot of EGM peak amplitude change in corrugator muscle in relation to theACIPS total score in female participants.
38 L.S. Kadison et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

The current results inform both assessment and treatment of flat affect and anhedoniain psychiatric disorders, as the results highlight the importance of considering sex. Forexample, males presenting with high levels of negative affective facial expression maystill be experiencing anhedonia, whereas this is less likely for females. These relation-ships appear to be particularly strong with social anhedonia. In terms of treatment,patients presenting with either extreme of facial expressivity may benefit from clinicianfeedback and self-monitoring. The findings of this study highlight the importance ofconsidering sex in such a treatment, given the differential relationship with the experienceof anhedonia. Further research is needed to clarify why the sexes differed in theserelationships, as the current study cannot address the particular mechanisms involved.
A limitation of this study was not including positively valenced stimuli, as the largerstudy was focused on reactions to negative stimuli. Thus, as expected, no relationshipswere found in the zygomatic EMG response (which measures positive expressions) forsex or anhedonia subtypes. Future research should examine these relationships inresponse to positively valenced stimuli to determine whether the zygomatic muscle groupshows a similar pattern of relationships found in the present study.
In closing, this study shows that sex and anhedonia interact in relation to facialexpressivity. Social anhedonia in particular shows a strong relationship with facialexpressivity and shows the most robust interaction with sex. These findings may helpexplain many discrepancies in the current research examining anhedonia and flat affectand have clinical implications for assessment and treatment of these symptoms acrosspsychiatric disorders.
AcknowledgementsThe authors would like to thank Ms Daniella S. Schlander and Mr Christopher Spencer forassistance with data collection and entry. In addition, the authors thank Drs Valerie Sims andDeborah C. Beidel for contributions with the design and interpretation of the data.
ReferencesAlpert, M., Rosenberg, S. D., Pouget, E. R., & Shaw, R. J. (2000). Prosody and lexical accuracy in
flat affect schizophrenia. Psychiatry Research, 97, 107–118. doi:10.1016/S0165-1781(00)00231-6
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders(5th ed.). Washington, DC, WA: American Psychiatric Publishing.
Berenbaum, H., Snowhite, R., & Oltmanns, T. F. (1987). Anhedonia and emotional responses toaffect evoking stimuli. Psychological Medicine, 17, 677–684. doi:10.1017/S0033291700025915
Brown, L. H., Silvia, P. J., Myin-Germeys, I., & Kwapil, T. R. (2007). When the need to belonggoes wrong: The expression of social anhedonia and social anxiety in daily life. PsychologicalScience, 18, 778–782. doi:10.1111/j.1467-9280.2007.01978.x
Bylsma, L. M., Morris, B. H., & Rottenberg, J. (2008). A meta-analysis of emotional reactivity inmajor depressive disorder. Clinical Psychology Review, 28, 676–691.
Cacioppo, J. T., Berntson, G. G., Larsen, J. T., Poehlmann, K. M., & Ito, T. A. (2000). Thepsychophysiology of emotion. In R. Lewis & J. M. Haviland-Jones (Eds.), The handbook ofemotion (2nd ed., pp. 173–191). New York, NY: Guilford Press.
Cohen, A. S., Alpert, M., Nienow, T. M., Dinzeo, T. J., & Docherty, N. M. (2008). Computerizedmeasurement of negative symptoms in schizophrenia. Journal of Psychiatric Research, 42, 827–836. doi:10.1016/j.jpsychires.2007.08.008
Dichter, G. (2010). Anhedonia in unipolar major depressive disorder: A review. The OpenPsychiatry Journal, 4, 1–9. doi:10.2174/1874354401004010001
Dimberg, U., & Lundquist, L. (1990). Gender differences in facial reactions to facial expressions.Biological Psychology, 30, 151–159. doi:10.1016/0301-0511(90)90024-Q
Cognitive Neuropsychiatry 39
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14

Fitzgibbons, L., & Simons, R. F. (1992). Affective response to color-slide stimuli in subjects withphysical anhedonia: A three systems analysis. Psychophysiology, 29, 613–620. doi:10.1111/j.1469-8986.1992.tb02036.x
Fonseca-Pedrero, E., Lemos-Giraldez, S., Muniz, J., Garcia-Cueto, E., & Campillo-Alvarez, A.(2008). Schizotypy in adolescence: The role of gender and age. Journal of Nervous and MentalDisorders, 196, 161–165. doi:10.1097/NMD.0b013e318162aa79
Fridlund, A. J., & Cacioppo, J. T. (1986). Guidelines for human electromyographic research.Psychophysiology, 30, 261–273.
Gard, D. E., Gard-Germans, M., Kring, A. M., & Oliver, J. P. (2006). Anticipatory andconsummatory components of the experience of pleasure: A scale development study. Journalof Research in Personality, 40, 1086–1102. doi:10.1016/j.jrp.2005.11.001
Gooding, D. C., & Pflum, M. J. (2014a). The assessment of interpersonal pleasure: Introduction ofthe anticipatory and consummatory interpersonal pleasure scale (ACIPS) and preliminaryfindings. Psychiatry Research, 215, 237–243. doi:10.1016/j.psychres.2013.10.012
Gooding, D. C., & Pflum, M. J. (2014b). Further validation of the ACIPS as a measure of socialhedonic response. Psychiatry Research, 215, 771–777. doi:10.1016/j.psychres.2013.11.009
Gooding, D. C., Tallent, K. A., & Matts, C. W. (2005). Clinical status of at-risk individuals 5 yearslater: Further validation of the psychometric high-risk strategy. Journal of Abnormal Psychology,114, 170–175. doi:10.1037/0021-843X.114.1.170
Greden, J. F., Genero, N., Price, L., Feinberg, M., & Levine, S. (1986). Facial electromyography indepression. Archives of General Psychiatry, 43, 269–274. doi:10.1001/archpsyc.1986.01800030087009
Heerey, E., & Gold, J. (2007). Patients with schizophrenia demonstrate dissociation betweenaffective experience and motivated behavior. Journal of Abnormal Psychology, 116, 268–278.doi:10.1037/0021-843X.116.2.268
Horan, W., Blanchard, J., Clark, L., & Green, M. (2008). Affective traits in schizophrenia andschizotypy. Schizophrenia Bulletin, 34, 856–874. doi:10.1093/schbul/sbn083
Horan, W., Wynn, J., Kring, A., Simons, R., & Green, M. (2010). Electrophysiological correlates ofemotional responding in schizophrenia. Journal of Abnormal Psychology, 119, 18–30.doi:10.1037/a0017510
Huang, H., & Hu, S. (2009). Sex differences found in facial EMG activity provoked by viewingpleasant and unpleasant photographs. Perceptual and Motor Skills, 109, 371–381. doi:10.2466/pms.109.2.371-381
Kring, A., & Moran, E. (2008). Emotional response deficits in schizophrenia: Insights fromaffective science. Schizophrenia Bulletin, 34, 819–834. doi:10.1093/schbul/sbn071
Kwapil, T. R. (1998). Social anhedonia as a predictor of the development of schizophrenia-spectrum disorders. Journal of Abnormal Psychology, 107, 558–565. doi:10.1037/0021-843X.107.4.558
Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (2008). International affective picture system (IAPS):Affective ratings of pictures and instruction manual (Technical Report No. A-8). Gainesville:University of Florida.
Lee, H., Shackman, A. J., Jackson, D. C., & Davidson, R. J. (2009). Test-retest reliability ofvoluntary emotion regulation. Psychophysiology, 46, 874–879. doi:10.1111/j.1469-8986.2009.00830.x
Leung, W., Couture, S., Blanchard, J., Lin, S., & Llerena, K. (2010). Is social anhedonia related toemotional responsivity and expressivity? A laboratory study in women. Schizophrenia Research,124, 66–73. doi:10.1016/j.schres.2010.06.012
Lundqvist, L. (1995). Facial EMG reactions to facial expressions: A case of facial emotionalcontagion? Scandinavian Journal of Psychology, 36, 130–141. doi:10.1111/j.1467-9450.1995.tb00974.x
Miettunen, J., & Jaakelainen, E. (2010). Sex differences in Wisconsin schizotypy scales—A metaanalysis. Schizophrenia Bulletin, 36, 347–358. doi:10.1093/schbul/sbn075
Raine, A. (1991). The SPQ: A scale for the assessment of schizotypal personality based on DSM-III-R criteria. Schizophrenia Bulletin, 17, 555–564. doi:10.1093/schbul/17.4.555
Strauss, G. P., Wilbur, R. C., Warren, K. R., August, S. M., & Gold, J. M. (2011). Anticipatory vs.consummatory pleasure: What is the nature of hedonic deficits in schizophrenia? PsychiatryResearch, 187, 36–41. doi:10.1016/j.psychres.2011.01.012
40 L.S. Kadison et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
entr
al F
lori
da]
at 0
8:35
12
Nov
embe
r 20
14
Copyright © 2022 FDOKUMEN