Eye-blink conditioning deficits indicate temporal processing abnormalities in schizophrenia
Upload
khangminh22Category
view
0download
0
62ournal ofNeurology, Neurosurgery, and Psychiatry 1995;58:692-698
Electromyography and recovery of the blink reflexin involuntary eyelid closure: a comparative study
M Aramideh, J L A Eekhof, L J Bour, J H T M Koelman, J D Speelman,B W Ongerboer de Visser
Graduate SchoolNeurosciencesAmsterdam, AZUA,Departnent ofNeurologyM AramidehJ D SpeelmanDivision of ClinicalNeurophysiology,Academic MedicalCentre, Amsterdam,The NetherlandsM AramidehJ L A EekhofL J BourJ H T M KoelmanB W Ongerboer de VisserCorrespondence to:DrM Aramideh,Department of Neurology(H2-214), AcademicMedical Centre,Meibergdreef 9, NL- 1 105AZ Amsterdam, TheNetherlands.Received 9 November 1994and in revised form1 February 1995Accepted 8 February 1995
AbstractElectromyographic (EMG) activity oforbicularis oculi and levator palpebraemuscles was recorded to study the originof involuntary eyelid closure in 33patients. The evoked blink reflex in allpatients and in 23 controls was also stud-ied. To examine the excitability of facialmotoneurons and bulbar interneurons inindividual patients and to compare theresults with EMG findings, Rl and R2recovery indices were calculated in all
subjects, as the average of recovery val-ues at 0 5, 0-3, and 0-21 second interstim-ulus intervals. Based on EMG patterns,the patients were divided into three sub-classes: EMG subclass 1, 10 patients withinvoluntary discharges solely in orbicu-laris oculi muscle; EMG subclass 2, 20patients with involuntary discharges inorbicularis oculi and either involuntarylevator palpebrae inhibition or a dis-turbed reciprocal innervation betweenorbicularis oculi and levator palpebrae;EMG subclass 3, three patients who didnot have blepharospasm, but had invol-untary levator palpebrae inhibition inassociation with a basal ganglia disease.The total patient group showed an
enhanced recovery of both RI and R2components compared with controls.Although 30 out of 33 patients had ble-pharospasm (EMG subclasses 1 and 2),RI recovery index was normal in 64% andR2 recovery index was normal in 54%.Patients with an abnormal R2 recovery
index had an abnormal Rl recovery indexsignificantly more often. All patientsfrom EMG subclass 1 had an abnormalR2 recovery index, whereas all patientsfrom EMG subclass 3 had normal recov-
ery indices for both Rl and R2 responses.Seventy five per cent of the patients fromEMG subclass 2 had normal recoveryindices. The results provide further evi-dence that physiologically blepharo-spasm is not a homogeneous diseaseentity, and indicate that different patho-physiological mechanisms at the supra-segmental, or segmental level, or bothare involved.
(7 Neurol Neurosurg Psychiatry 1995;58:692-698)
Keywords: dystonia; blepharospasm; blink reflexrecovery
Blepharospasm is a form of focal dystonia,with an aetiology and underlying pathophysi-ological mechanisms that are still obscure.Blepharospasm may occur in diseases of thebasal ganglia or in association with upperbrain stem abnormalities. 1-8 In most patients,however, it is idiopathic in origin.One investigation technique that has con-
tributed to our understanding of blepharo-spasm is the recorded blink reflex recovery,which indicates the state of excitability of thefacial motoneurons and bulbar interneurons.Electrical stimulation of the supraorbitalnerve elicits a blink reflex that consists of twocomponents; an early ipsilateral response, Rl,mediated through the pons by an oligosynapticpathway and a late bilateral response, R2,relayed through a polysynaptic medullarypathway.9-1" Motoneurons of the facial nerveconstitute the final common path for bothresponses. The recovery curve, also known asexcitability cycle, of Rl and R2 responses canbe obtained by applying two stimuli, condi-tioning and test, to the supraorbital nerve atdifferent interstimulus intervals. 14 Theexcitability of the blink reflex circuit may thenbe assessed by comparing the size of the testresponse with that of the conditioningresponse, which is partly dependent on thefunctional integrity of the suprasegmentalstructures. In healthy subjects, the R2 testresponse shows pronounced suppression atshorter interstimulus intervals,'0 whereaspatients with cortical lesions may exhibit anenhanced habituation and patients with basalganglia disorders a diminished habituation(enhanced recovery) of the response.'011Previous work has shown an enhanced recov-ery of the R2 response in patients with ble-pharospasm, which suggests hyperexcitabilityof the bulbar interneurons.'5'-8By simultaneous recording of the electro-
myographic (EMG) activities from the orbic-ularis oculi and levator palpebrae muscles, wehave shown that patients with blepharospasmare not a homogeneous group, becausediffering abnormalities of EMG pattems arefound among these patients. 19 20
In the present study, we examined therecovery of Rl and R2 responses and EMGactivity of orbicularis oculi and levator palpe-brae muscles in patients with involuntary eye-lid closure. The aim of the study was: (1) toevaluate the state of excitability of facialmotoneurons and bulbar interneurons in indi-vidual patients with a certain EMG abnormal-ity; (2) to see whether there is a correlation
692

Electromyography and recovery of the blink reflex in involuntary eyelid closure: a comparative study
Table 1 General characteristics of the patients examined
Number of patients (n) 33Women/men 22/11Mean age (y) (range) 67 (37-88)Mean age at onset (y) (range) 57 (25-77)Mean duration of illness (y) (range) 9 (1-20)Type of dystonia:
focal (n) 17segmental (n) 13
Treatment at time of study:Botulinum toxin type A (n) 7Medication (n) 3
between clinical data, EMG subclass, andrecovery values, and (3) to provide additionalinformation on possible underlying patho-physiological mechanisms of blepharospasm.
Materials and methodsThirty three patients, 22 women and 11 men
(mean age 67 (range 37-88) years) with invol-untary eyelid closure were studied. Table 1
summarises the clinical data of the patients.At the time of the study, seven patients were
already under treatmnent with botulinum Atoxin (Dysport) but in all patients voluntaryand reflex activity of the orbicularis oculicould easily be recorded. The control groupconsisted of 23 subjects (six women and 17men) with a mean age of 49 (range 18-73)years.The method ofEMG recording from orbic-
ularis oculi and levator palpebrae muscles hasbeen reported previously.'9 20 Blink reflexstudies were performed with the subject lyingsupine. Electrical stimuli were applied to thesupraorbital nerve at the supraorbital fora-men. Surface recording electrodes were
placed over the lower portion of orbicularisoculi ipsilateral to the stimulation site. AGrass stimulator was used to apply constantcurrent pulses with a duration of 0-2 ms. Theearly and late blink reflexes were evoked withstimulus intensity adjusted to three times thethreshold of the R2 response. Subjects were
requested to close their eyes gently duringstimulation, and responses with artefacts dueto involuntary movements were rejected.Paired stimuli (conditioning and test) weredelivered at interstimulus intervals of 0-5, 0-3,and 0-21 seconds and six trials were per-formed at each interval. Between successivetrials, a rest period of at least 30 seconds was
maintained to avoid habituation of theresponse. The low pass filter was set at 3 kHzand the high pass filter at 1 Hz (6 dB/oct).The sweep time was kept at 200 ms. Allresponses were stored digitally on a PDP11/73 computer. In an off line analysis proce-dure, performed fully automatically, reflexresponses were digitally band pass filteredwithin a range of more than 100 Hz to min-imise DC offsets and slow eye drifts andbelow 900 Hz to reduce the high frequencynoise. The responses were then full wave recti-fied and the average of six trials was computedfor each interstimulus interval. Peak ampli-tude of RI was calculated within a windowfrom 10 to 25 ms to avoid stimulation arte-fact, and that of R2 within a window from 32to 90 ms. The average rest activity level wasestablished within a window from 150 to 200ms and subtracted from the average response.For each subject, Rl and R2 recovery valueswere obtained by calculating the size of thetest response as a percentage of the condition-ing response at each interstimulus interval.Rl recovery index was calculated in each
subject as the mean value of peak amplituderecovery, obtained at interstimulus intervalsof 0-5, 0-3, and 0-21 seconds. The R2 recoveryindex was calculated in the same way. The
upper limit of normal for Rl and R2 was
defined as the mean + 2-5 SD.
STATISTICAL ANALYSISA correlative study was performed betweenthe clinical data, EMG subclasses, and blinkreflex recovery indices by means of Kruskall-Wallis and X2 tests, with the SPSS statisticalprogram. Differences and correlations were
considered significant at P values < 0-05.
ResultsTable 2 summarises the results of therecorded EMG and blink reflex recovery.
EMG FINDINGSAccording to the EMG patterns, patientswere divided into three subclasses. Tenpatients belonged to EMG subclass 1, inwhom EMG recording showed involuntarydischarges in the orbicularis oculi alone, withnormal tonic activity of levator palpebrae andnormal reciprocal innervation of orbicularisoculi and levator palpebrae. EMG subclass 2consisted of 20 patients. Besides involuntary
Table 2 Mean values ofRl and R2 recovery indices in patients and controls
Focal Mean Rl No of Mean R2 No ofNo of segmental index abnormal index abnormal
Group subjects dystonia (range) Rl indices (range) R2 indices
Controls 23 - 78 (36-120) - 22 (11-42) -
Patients:Whole group 33 17/13 125 (35-227)*** lot 42 (6-108)*** 15EMG subclass:
1 10 3/7 161 (73-278)*** 5 60 (45-79)*** 102 20 14/6 118 (35-215)* 5 32 (6-108) NS 53 3 - 96 (74-107) NS 0 60 (28-37) NS 0
The recovery indices are given in percentages. * p < 0-05; *** p < 0-001 v controls.tRl could not be recorded in five patients, two from EMG subclass 1 and three from EMG subclass 2.
693

Aramideh, Eekhof, Bour, Koelman, Speelman, Ongerboer de Visser
discharges in orbicularis oculi, EMG record-ing in these patients disclosed either episodesof involuntary inhibition of tonic activity oflevator palpebrae or a disturbed reciprocalinnervation of orbicularis oculi and levatorpalpebrae. EMG subclass 3 consisted of threepatients. Abnormality in these patients wascharacterised by solely involuntary inhibitionof levator palpebrae, with normal activity oforbicularis oculi and normal reciprocal inner-vation of orbicularis oculi and levator palpe-brae muscles. These three patients had,therefore, no blepharospasm.
BLINK REFLEX FINDINGSControlsThere was pronounced variability in Rlrecovery from one subject to another at differ-ent interstimulus intervals. The mean recov-ery of Rl at the 05 second interval was 69%and this increased to 78% at 021 seconds.Table 2 shows RI and R2 recovery indices.The mean value of the Rl recovery index was78% (range, 36%-120%), and the upper limitof normal was 135%. The R2 recovery curveshowed less variability. By contrast with Rl,recovery of R2 gradually decreased from 29%at the 0 5 second interval to 15% at 0-21 sec-onds. The R2 recovery index had a meanvalue of 22% (range 11 %-42%), and theupper limit of normal was 43%.
PatientsIn five patients, the RI recovery index couldnot be calculated because the amplitude of Rlwas too low with respect to the noise.Recovery of Rl gradually increased from117% at the 0 5 second interval to 137% at0-21 seconds. Table 2 shows Rl and R2recovery indices for the total patient groupand for the three EMG subclasses. The Rlrecovery index in the patient group differedsignificantly from that in the control group (P< 0-001). Recovery of R2 gradually decreasedfrom 50% at the 0 5 second interval to 31% at0-21 seconds. R2 recovery index in the patientgroup was significantly higher than that in thecontrol group (P < 0.001).
Considering the individual data, 18 of 28patients (64%) had a normal Rl recoveryindex, and 18 of 33 patients (54%) had a nor-mal R2 recovery index (table 2). A significantnumber of patients with an abnormal Rlrecovery index also had an abnormal R2recovery index (P = 0.01, Yates correctedtest).
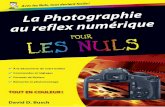
Considering the data from different EMGsubclasses, the Rl recovery index differed sta-tistically from control subjects in EMG sub-class 1 (P < 0 001, table 2) and less so inEMG subclass 2 (P < 0.05). The R2 recoveryindex differed statistically from control sub-jects only in EMG subclass 1 (P < 0001). Allthe patients from EMG subclass 1 had anabnormal R2 recovery index, and 50% ofthem also had an abnormal Rl recoveryindex. Dystonia of other cranial or cervicalmuscles was found significantly more often inEMG subclass 1 (P < 0.01, table 2). Figure 1shows an example of abnormal Rl and R2
recovery curves in one of the patients fromthis group. All three patients from EMG sub-class 3 had normal Rl and R2 recoveryindices, whereas all had associated basal gan-glia disease; one had progressive supranuclearpalsy, and two had multiple system atrophy.Interestingly, 15 patients (75%) from EMGsubclass 2 had a normal R2 recovery index.Figure 2 shows normal Rl and R2 recoverycurves in one of the patients from this group.
DiscussionWe investigated the recovery of Rl and R2components of the blink reflex in patientswith involuntary eyelid closure, as one singlegroup or divided into three subclasses accord-ing to the EMG patterns of orbicularis oculiand levator palpebrae muscles. Patients withEMG subclass 1 had involuntary dischargessolely in orbicularis oculi muscle.20 EMG sub-class 2 consisted of patients with involuntarydischarges in orbicularis oculi, accompaniedby either involuntary inhibition of levatorpalpebrae motor activity, or a disturbed recip-rocal innervation of orbicularis oculi and leva-tor palpebrae. In an earlier report,20 weproposed the term "blepharospasm-plus" todesignate those patients with this type ofEMG abnormality. The patients from EMGsubclass 3 had solely involuntary inhibition oflevator palpebrae,2' 22 also known as apraxia ofeyelid opening,2' with no clinical or EMGsigns of blepharospasm.'9 20 We included thesepatients in the present study because the dif-ferentiation between blepharospasm andinvoluntary levator palpebrae inhibition is notalways easy to make clinically and synchro-nous EMG recording from orbicularis oculiand levator palpebrae is often required.20
In controls, RI recovery showed some vari-ability between subjects at all three interstimu-lus intervals. From 0-5 to 0-21 secondintervals, Rl recovery showed a gradualenhancement, with relatively less suppressionat 0-3 seconds. By contrast, R2 recoveryshowed almost no interindividual variabilityand from 0 5 to 0'21 second intervals therewas a gradual increase in suppression. Also, inthe total patient group the recovery of Rl dif-fered from that of R2. There was often anabsolute increase of Rl test response whenthe interval was shortened from 0 5 to 0-21seconds, whereas the R2 test response dimin-ished at shorter intervals. Such a difference inthe properties of Rl and R2 responses hasalso been found in other studies.2426 The samefacial nerve motoneurons generate bothresponses and the final efferent pathway iscommon. Therefore, the difference in therecovery behaviours of Rl and R2 responses,in both the controls and patients, should becaused by the bulbar interneurons. Yet it can-not entirely be explained by the difference inthe number of bulbar interneurons throughwhich these responses are relayed, and isprobably also dependent on the individualproperties of the interneurons, their relationto one another, and the suprasegmentaldrives on them. A difference in presynaptic
694

695Electromyography and recovery of the blink reflex in involuntary eyelid closure: a comparative study
Figure 1 (A) Rectifiedand averaged (6 x)EMG responses atintervals 0-5, 0 3, and0 21 seconds between theconditioning and teststimuli in a patientfromEMG subclass 1. Recoverycurve for Rl (B) and R2(C) in the same patient.The recovery ofRl and R2responses are enhanced atall three intervals. ISI =interstimulus interval; tlcratio = testresponselconditioningresponse.
Conditioning
10 ms/div
Test
I
10 ms/div
65 _
C95
00-
L-o.~_r
cNcr
35 -
0.21 0.3ISI (s)
0.5
inhibition at the primary cutaneous afferentterminals27 28 also cannot be excluded.The enhanced recovery of the R2 response
found in the total patient group confirms theresults of previous authors.'5-'8 We also foundan increased recovery of the Rl response,
whereas Tolosa et all'5 noted a normal Rlrecovery and the other authors did not reporton the features of Rl recovery in patients withblepharospasm.'1'8 Although these conflictingresults and the lack of information on thisissue may require further investigation, some
features of the recorded blink reflex are infavour of an enhanced excitability of theoligosynaptic pathway through which the Rlresponse is transmitted. Willer et al29 reportedon the existence of a crossed trigeminofacialconnection, and showed that a contralateralRl response can easily be obtained in healthysubjects when the test stimulus was preceded
0 0.21 0.3ISI (s)
0.5
by an adequate conditioning stimulus. Yetafter single stimulation of the supraorbitalnerve, Berardelli et al16 recorded a contralat-eral Rl response in six of 16 patients with ble-pharospasm. Based on these data, it seems
that at least the crossed oligosynaptic route
mediating the contralateral Rl response ishyperactive in some patients with blepharo-spasm. Therefore, we agree with the conclu-sion of Tolosa et al 5 that the facialmotoneurons themselves are not hyperactivein patients with blepharospasm. We presumeinstead that the interneurons involved in thegeneration of both the Rl and R2 responses
may be hyperexcitable.The pathways through which the basal gan-
glia can modulate the blink reflex are
unknown. It seems, however, that the basalganglia exert an inhibitory influence on thebulbar intemeurons, even if it occurs
A
0-21
en
0.3
05
B
300 -
0C.-6._
250 F
200

Aramideh, Eekhof, Bour, Koelman, Speelman, Ongerboer de Visser
Figure 2 (A) Rectifiedand averaged (6 x)EMG responses atintervals 05, 0 3, and0 21 seconds between theconditioning and teststimuli, in a patientfromEMG subclass 2. Recoverycurve for RI (B) and R2(C) in the same patient.The recovery ofRl and R2responses are normal at allthree intervals. ISI =interstimulus interval; tlcratio = testresponselconditioningresponse.
A
0.21
-aFn
03
0.5
B
60
0r-
0
a: 50
40_0
Conditioning
10 ms/divC
Test
10 ms/div
15 F
00
INet
5
0.21 0.3ISI (s)
0.5
indirectly via cortical pathways becauselesions of these pathways can suppress theblink reflex." 3031 Evinger et al32 showed thatapomorphine, a dopamine receptor agonist,and nicotine, which releases dopamine in thestriatum, increase the latency of the R2response without altering the latency of theRl response. In their recent paper, Basso etal 26 showed that partial or even completelesions of the substantia nigra and ventraltegmental area in rats do not modify the Rlrecovery at all, whereas R2 recovery showspronounced excitability. Accordingly, inpatients with Parkinson's disease Rl recoveryis normal,'4"3 R2 recovery is enhanced,'4'334and R2 latency is shortened.'4 Furthermore,patients with Huntington's disease exhibit a
decrease in blink reflex excitability34 35 and an
increase in the latency of the R2 response,34-'6
0 0.21 0.3ISI (s)
0.5
comparable with those findings in patientswith hemispheric lesions. By contrast, Rlrecovery was enhanced in our patients and theprevious studies showed that the latency ofR2is normal in patients with blepharospasm.'5-'7Based on these findings, two important con-clusions can be drawn. Firstly, it is conceiv-able that dopaminergic activity of at least thesubstantia nigra may not control the state ofactivity of facial motoneurons directly or indi-rectly, through the oligosynaptic reflex path-way, and that the enhanced Rl recovery inour patients as a group should have someother origin. Secondly, it is possible that alter-ations in basal ganglia activity influence thebulbar interneurons somehow differently inpatients with idiopathic blepharospasm fromthose patients with known diseases of thebasal ganglia such as Parkinson's disease.
696

Electromyography and recovery of the blink reflex in involuntary eyelid closure: a comparative study
A causal relation between hyperexcitabilityof interneurons and the occurrence of invol-untary discharges in orbicularis oculi becomesless evident when we consider the data of Rland R2 recovery indices in individual patientsor in patients from different EMG subclasses.Our results showed a normal Rl recoveryindex in 64% and a normal R2 recovery indexin 54% of the total patient group, despite thefact that 30 out of 33 patients had involuntarydischarges in orbicularis oculi, whether or notin combination with involuntary levatorpalpebrae inhibition (EMG subclasses 1 and2). An abnormal Rl recovery index occurredsignificantly more often in patients with anabnormal R2 recovery index. An interestingfinding was that all patients with blepharo-spasm alone (EMG subclass 1), had anabnormal R2 recovery index and 50% alsohad an abnormal Rl recovery index. On theother hand, those patients with involuntarydischarges in orbicularis oculi with eitherinvoluntary levator palpebrae inhibition or adisturbed reciprocal innervation of orbicularisoculi and levator palpebrae (EMG subclass2), often had normal RI and R2 recoveryindices. At the time of this study, seven out of20 patients from EMG subclass 2 werealready under treatment with botulinum Atoxin. It is unlikely that this influenced therecovery values in these patients, because pre-vious studies1837 showed no difference in theblink reflex excitability in patients with ble-pharospasm before and after such treatment.Furthermore, it is also unlikely that patientswith blepharospasm alone may have had asevere form of orbicularis oculi muscle dysto-nia, because as noted by Pauletti et al,'7 there isno correlation between the severity of dysto-nia and the excitability of the blink reflex. Themost probable explanation is a difference inunderlying pathophysiological mechanisms.There may be a dissociation of the supra-segmental controls resulting in involuntaryorbicularis oculi contraction, whether or notaccompanied by disturbed levator palpebraemuscle activity, which cannot be examinedby simply eliciting the blink reflex.Dissociation between innervation of emo-tional and voluntary movements of the facialmusculature is well recognised in patientswith central facial paresis, and with thalamicor pallidal lesions.3839 Symptomatic blepharo-spasm may occur in disorders of the basalganglia but never, to our knowledge, as an iso-lated abnormality. Conversely, no study hasyet provided clear evidence for any pathologyof the basal ganglia and their involvement inthe generation of involuntary contractions ofthe eyelids in patients with idiopathic ble-pharospasm. On the other hand, Siegel et a140reported on cells, located within a portion ofthe medial reticular formation, which showeddischarges in relation to the closing move-ments of eyelids. The authors mentioned thatsome of these cells probably project directly tothe facial cells and some may relay their out-puts over multisynaptic pathways. In anotherreport, Siegel et af4' also proposed that localinteraction of these medial reticular formation
cell populations may allow synthesis of thesimple reflex movements generated in thebrain stem. We suggest that besides theabnormal drives exerted by the basal ganglia,disorders of the segmental structures may alsocontribute to the enhanced excitability of theblink reflex responses and to the generation ofblepharospasm. This assumption may explainwhy the recovery of Rl and R2 responses wasoften enhanced in patients with blepharo-spasm alone, who also often had dystonia ofother cranial muscles without additional clini-cal features pointing to abnormal basal gan-glia activity.
All three patients from EMG subclass 3,with involuntary levator palpebrae inhibition,had normal Rl and R2 recovery indices.These patients also had abnormalities of,among others, the basal ganglia. Therefore,certain disorders of the basal ganglia mayinfluence the tonic activity of levator palpe-brae muscle without altering the excitability ofthe blink reflex. We are unaware of any previ-ous reports on this issue.
In conclusion, the results of the presentpaper are in agreement with our earlier find-ings, 92042 and provide further evidence that,physiologically, blepharospasm is not a homo-geneous disease entity. They indicate that var-ious pathophysiological mechanisms at thesuprasegmental, or segmental, level, or both,are involved.
We thank Drs L Volger and A Hilgevoord for their help instatistical analysis.
1 Marsden CD. Blepharospasm-oromandibular dystoniasyndrome (Brueghel's syndrome): a variant of adult-onset torsion dystonia? J7 Neurol Neurosurg Psychiatry1976;39:1204-9.
2 Jankovic J, Ford J. Blepharospasm and orofacial-cervicaldystonia: clinical and pharmacological findings in 100patients. Ann Neurol 1983;13:402-1 1.
3 Fahn S, Marsden CD, Calne B. Classification and investi-gation of dystonia. In: Marsden CD, Fahn S, eds.Movement disorders 2. London: Butterworths, 1988:332-58.
4 Grandas F, Elston J, Quinn N, Marsden CD. Blepharo-spasm: a review of 264 patients. 7 Neurol NeurosurgPsychiatry 1988;51:767-2.
5 Jankovic J. Etiology and differential diagnosis of blepharo-spasm and oromandibular dystonia. Adv Neurol 1988;49:103-16.
6 Fahn S. Blepharospasm: A form of focal dystonia. AdvNeurol 1988;49: 125-35.
7 Jankovic J, Patel SC. Blepharospasm associated withbrainstem lesions. Neurology 1983;33:1237-40.
8 Leenders KL, Frackowiak RSJ, Quinn N, Brooks D,Sumner D, Marsden CD. Unilateral blepharospasm andcontralateral hemidystonia and parkinsonism in a patientwith a unilateral rostral brainstem-thalamic lesion:structural and functional abnormalities studied with CT,MRI and PET scanning. Mov Disord 1986;1:51-8.
9 Ongerboer de Visser BW, Kuypers HGJM. Late blinkreflex changes in lateral medullary lesions. Anelectrophysiological and neuroanatomical study ofWallenberg's syndrome. Brain 1978;101:285-94.
10 Ongerboer de Visser BW, Cruccu G. Neurophysiologicexamination of the trigeminal, facial, hypoglossal, andspinal accessory nerves in cranial neuropathies and brainstem disorders. In: Brown WF, Bolton CF, eds. Clinicalelectromyography. Pennsylvania: Butterworths, 1993:61-92.
11 Ongerboer de Visser BW. Comparative study of cornealand blink reflex latencies in patients with segmental orwith central lesions. In: Desmedt JE, ed. Motor controlmechanisms in health and disease. New York: Raven Press,1983:757-72.
12 Kimura J, Lyon LW. Orbicularis oculi reflex in Wallenbergsyndrome: alteration of the late reflex by lesion of thespinal tract and nucleus of the trigeminal nerve. Jf NeurolNeurosurg Psychiatry 1972;35:228-33.
13 Kimura J. Alteration of the orbicularis oculi reflex by pon-tine lesions: study in multiple sclerosis. Arch Neurol1970;22:156-61.
14 Kimura J. Disorders of intemeurons in parkinsonism. Theorbicularis oculi reflex to paired stimuli. Brain 1973;96:87-96.
697

Aramideh, Eekhof, Bour, Koelman, Speelman, Ongerboer de Visser
15 Tolosa E, Montserrat L, Bayes A. Blink reflex studies infocal dystonias: enhanced excitability of brainsteminterneurons in cranial dystonia and spasmodic torticollis.Mov Disord 1988;3:61-9.
16 Berardelli A, Rothwell JC, Day BL, Marsden CD.Pathophysiology of blepharospasm and oromandibulardystonia. Brain 1985;108:593-608.
17 Pauletti G, Berardelli A, Cruccu G, Agostino R, ManfrediM. Blink reflex and the masseter inhibitory reflex inpatients with dystonia. Mov Disord 1993;8:495-500.
18 Cohen LG, Hallett M, Warden M, Dambrosia J.Excitability of blink reflexes in patients with blepharo-spasm after successful treatment with botulinum toxin.Ann Neurol 1987;22:172.
19 Aramideh M, Ongerboer de Visser BW, Devriese PP, BourU, Speelman JD. Electromyographic features of levatorpalpebrae superioris and orbicularis oculi muscles in ble-pharospasm. Brain 1994;117:27-38.
20 Aramideh M, Ongerboer de Visser BW, Koelman JHTM,Bour U, Devriese PP, Speelman JD. Clinical andelectromyographic features of levator palpebrae superi-oris muscle dysfunction in involuntary eyelid closure.Mov Disord 1994;9:395-402.
21 Lepore FE, Duvoisin RC. Apraxia of eyelid opening: aninvoluntary levator inhibition. Neurology 1985;35:423-7.
22 Lepore FE. So-called apraxias of lid movement. AdvNeurol 1988;49:85-90.
23 Goldstein JE, Cogan DG. Apraxia of lid opening. ArchOphthalmol 1965;73: 155-9.
24 Shahani B. Effects of sleep on human reflexes with a doublecomponent. J Neurol Neurosurg Psychiatry 1968;31:574-9.
25 Sunohara N, Tomi H, Satoyoshi E, Tachibana S. Glabellatap sign. Is it due to a lack of R2-habituation? J7 NeurolSci 1985;70:257-67.
26 Basso MA, Strecker RE, Evinger C. Midbrain 6-hydroxy-dopamine lesions modulate blink reflex excitability. ExpBrain Res 1993;94:88-96.
27 Darian-Smith I. Presynaptic component in the afferentinhibition observed within trigeminal brain-stem nucleiof the cat. J Neurophysiol 1965;28:695-709.
28 Stewart DH Jr, Scibetta CJ, King RB. Presynaptic inhibi-tion in the trigeminal relay nuclei. J7 Neurophysiol1967;30: 135-53.
29 Willer JC, Boulu P, Bratzlavsky M. Electrophysiologicalevidence for crossed oligosynaptic trigemino-facial con-nections in normal man. J7 Neurol Neurosurg Psychiatry1984;47:87-90.
30 Kimura J, Wilkinson JT, Damasio H, Adams HR,Shivapour E, Yamada T. Blink reflex in patients withhemispheric cerebrovascular accident (CVA). Blinkreflex in CVA. J Neurol Sci 1985;67: 15-28.
31 Berardelli A, Accomero N, Cruccu G, Fabiano F, GuerrisiV, Manfredi M. The orbicularis oculi response afterhemispheral damage. J Neurol Neurosurg Psychiatry1983;46:837-43.
32 Evinger C, Basso MA, Manning KA, Sibony PA,Pellegrini JJ, Hom AKE. A role for the basal ganglia innicotinic modulation of the blink reflex. Exp Brain Res1993;92:507-15.
33 Agostino R, Berardelli A, Cruccu G, Stocchi F, ManfrediM. The corneal and blink reflexes in Parkinson's diseasewith on-off fluctuations. Mov Disord 1987;4:227-35.
34 Esteban A, Gimenez-Roldan S. Blink reflex inHuntington's chorea and Parkinson's disease. ActaNeurol Scand 1975;52:145-57.
35 Agostino R, Berardelli A, Cruccu G, Pauletti G, Stocchi F,Manfredi M. Correlation between facial involuntarymovements and abnormalities of blink and cornealreflexes in Huntington's chorea. Mov Disord 1988;3:281-9.
36 Bollen E, Arts RJHM, Roos RAC, Van Der Velde EA,Buruma OJS. Brainstem reflexes and brainstem auditoryevoked responses in Huntington's chorea. Jf NeurolNeurosurg Psychiatry 1986;49:313-5.
37 Valls-Sole J, Tolosa ES, Ribera G. Neurophysiologicalobservations on the effect of botulinum toxin treatmentin patients with dystonic blepharospasm. J NeurolNeurosurg Psychiatry 1991;54:310-3.
38 Monrad-Krohn GH. On facial dissociation. ActaPsychiatrica et Neurologica 1939;14:557-66.
39 Monrad-Krohn GH. On the dissociation of voluntary andemotional innervation in facial paresis of central origin.Brain 1924;47:22-35.
40 Siegel JM, Tomaszewski KS, Wheeler RL. Behavioralorganization of reticular formation: studies in theunrestrained cat. II. Cells related to facial movements.J Neurophysiol 1983;3:717-23.
41 Siegel JM, Nienhuis R, Wheeler RL, McGinty DJ, HarperRM. Discharge pattern of reticular formation unit pairsin walking and REM sleep. Exp Neurol 1981;74:875-91.
42 Aramideh M, Bour U, Koelman JHTM, Speelman JD,Ongerboer de Visser BW. Abnornal eye movements inblepharospasm and involuntary levator palpebrae inhibi-tion: clinical and pathophysiological considerations.Brain 1994;177:1457-74.
Cervicogenic headache: an early description
Despite the controversies surrounding the clinicalsources and pathological basis for cervicogenicheadache, this term was used by, and often is attrib-uted to Otto Sjaastad,'52although Barre and Riff hadearlier described headache and vertigo, related to cervi-cal arthritis, ascribed to stimulation of the vertebralnerve.3 However, an impressive, but little knowndescription is found in the fourth of 18 lectures givenbetween 1860 and 1862 on Rest and Pain, in JohnHilton's classical text4:
"Suppose a person to complain of pain upon thescalp, is it not very essential to know whether thatpain is expressed by the fifth nerve or by the great orsmall occipital? Thus pain in the anterior and lateralpart of the head, which are supplied by the fifthnerve, would suggest that the cause must be some-
where in the area of distribution of the other por-tions of the fifth nerve. So if the pain be expressed,the cause must assuredly be connected with thegreat or small occipital nerve, and in all probabilitydepends on disease of the spine between the firstand second cervical vertebrae."
JM S PEARCE305 Beverley Road,
Anlaby, Hull H10 7BG, UK
1 Sjaastad 0. Headache and the influence of stress. A per-sonal view. Ann Clin Res 1987;19:122-8.
2 Sjaastad 0. Cervicogenic headache: the controversialheadache. Clin Neurol Neurosurg 1992;94(suppl):S 147-9.
3 Barre JA, Riff P. Le vertige qui fait entendre de Lermoyez:etude des fonctions vestibulaires a propos d'un castypique; role possible de l'irritation du nerf vertebralpar arthrite cervicale. Revue Oto-neuro-ophthalmology1926; 4:498-501.
4 Hilton J. Rest and pain. Walls EW, Phillips EE, eds.London: Bell, 1950:77.
698
Copyright © 2022 FDOKUMEN