Use of surface electromyography to estimate neck muscle activity
22
Journal of Electromyography and Kinesiology 10 (2000) 377–398 www.elsevier.com/locate/jelekin Review Use of surface electromyography to estimate neck muscle activity Carolyn M. Sommerich a,* , Sharon M.B. Joines a , Veerle Hermans b , Samuel D. Moon c a Department of Industrial Engineering, North Carolina State University, Raleigh, NC 27695, USA b Faculty of Human Movement Sciences, Vrije Universiteit Amsterdam, Amsterdam, Netherlands c Department of Community and Family Medicine, Duke University Medical Center, Durham, NC, USA Accepted 27 August 2000 Abstract This paper reviews the literature concerning the use of surface electromyography (sEMG) for the study of the neck musculature in response to work and workplace design during light work and semi-static tasks. The paper also draws upon basic research and biomechanical modeling in order to provide methodological recommendations for the use of surface electromyography in this region of the body and to identify areas which require further investigation. The paper includes review and discussion of electrode site location, methods of normalization, data reliability, and factors that can affect sEMG signals from this region, including noise, physiologic artifact, stress, visual deficiencies, and pain. General guidance for maximum exertions with the neck musculature, for sEMG normalization or other purposes, is also included. 2000 Elsevier Science Ltd. All rights reserved. Contents 1. Introduction .................................................. 378 1.1. Relevance of neck muscle activity in ergonomics research .................... 378 2. Muscle selection ............................................... 379 2.1. Muscle selection in fundamental research on the cervical spine ................. 379 2.1.1. Physical modeling of neck muscle contributions ........................ 379 2.1.2. Biomechanical models of neck muscle contributions ..................... 380 2.1.3. Functional assessments of neck muscle activity ........................ 380 2.2. Effects of work and workplace design on muscle activity .................... 383 2.2.1. Light manual work .......................................... 383 2.2.2. VDT work ............................................... 387 2.2.3. Breaks ................................................. 387 3. Electrode placement ............................................. 388 3.1. Locating electrodes ........................................... 388 3.1.1. Anterior muscles ........................................... 388 3.1.2. Posterior muscles ........................................... 388 3.2. Crosstalk .................................................. 388 3.3. Innervation zones ............................................ 389 4. Normalization ................................................. 389 4.1. Level of exertion in reference contractions ............................. 389 4.2. Posture and direction of exertion in reference contractions .................... 390 * Corresponding author. Tel.: + 1-919-515-8614; fax: + 1-919-515- 5281. E-mail address: [email protected] (C.M. Sommerich). 1050-6411/00/$ - see front matter 2000 Elsevier Science Ltd. All rights reserved. PII:S1050-6411(00)00033-X
Transcript of Use of surface electromyography to estimate neck muscle activity
Journal of Electromyography and Kinesiology 10 (2000) 377–398www.elsevier.com/locate/jelekin
Review
Use of surface electromyography to estimate neck muscle activity
Carolyn M. Sommericha,*, Sharon M.B. Joinesa, Veerle Hermansb, Samuel D. Moonc
a Department of Industrial Engineering, North Carolina State University, Raleigh, NC 27695, USAb Faculty of Human Movement Sciences, Vrije Universiteit Amsterdam, Amsterdam, Netherlands
c Department of Community and Family Medicine, Duke University Medical Center, Durham, NC, USA
Accepted 27 August 2000
Abstract
This paper reviews the literature concerning the use of surface electromyography (sEMG) for the study of the neck musculaturein response to work and workplace design during light work and semi-static tasks. The paper also draws upon basic research andbiomechanical modeling in order to provide methodological recommendations for the use of surface electromyography in this regionof the body and to identify areas which require further investigation. The paper includes review and discussion of electrode sitelocation, methods of normalization, data reliability, and factors that can affect sEMG signals from this region, including noise,physiologic artifact, stress, visual deficiencies, and pain. General guidance for maximum exertions with the neck musculature, forsEMG normalization or other purposes, is also included. 2000 Elsevier Science Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3781.1. Relevance of neck muscle activity in ergonomics research . . . . . . . . . . . . . . . . . . . . 378
2. Muscle selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3792.1. Muscle selection in fundamental research on the cervical spine . . . . . . . . . . . . . . . . . 3792.1.1. Physical modeling of neck muscle contributions . . . . . . . . . . . . . . . . . . . . . . . . 3792.1.2. Biomechanical models of neck muscle contributions . . . . . . . . . . . . . . . . . . . . . 3802.1.3. Functional assessments of neck muscle activity . . . . . . . . . . . . . . . . . . . . . . . . 380
2.2. Effects of work and workplace design on muscle activity . . . . . . . . . . . . . . . . . . . . 3832.2.1. Light manual work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3832.2.2. VDT work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3872.2.3. Breaks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387
3. Electrode placement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3883.1. Locating electrodes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3883.1.1. Anterior muscles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3883.1.2. Posterior muscles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 388
3.2. Crosstalk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3883.3. Innervation zones . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 389
4. Normalization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3894.1. Level of exertion in reference contractions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3894.2. Posture and direction of exertion in reference contractions . . . . . . . . . . . . . . . . . . . . 390
* Corresponding author. Tel.:+1-919-515-8614; fax:+1-919-515-5281.
E-mail address:[email protected] (C.M. Sommerich).
1050-6411/00/$ - see front matter 2000 Elsevier Science Ltd. All rights reserved.PII: S1050-6411 (00)00033-X

378 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
5. Additional methodological issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3915.1. Relationship between sEMG and force or torque . . . . . . . . . . . . . . . . . . . . . . . . . 3915.2. sEMG as an estimator of muscle load . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3915.3. Reliability of data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3925.3.1. Reference exertions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3925.3.2. Exertions during performance of work tasks . . . . . . . . . . . . . . . . . . . . . . . . . . 392
6. Special concerns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3936.1. Swallowing and breathing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3936.2. Heartbeat (ECG) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3936.3. Visual stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3936.4. Muscular pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 394
7. Recommendations and questions for future research . . . . . . . . . . . . . . . . . . . . . . . . . 3947.1. Muscle selection and electrode placement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3947.1.1. Posterior muscles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3947.1.2. Anterior muscles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 394
7.2. Reliability, normalization, and data reduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3947.2.1. Precautions regarding maximum exertions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 395
7.3. Concluding remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 395
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 396
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 396
1. Introduction
The recognition of the need for a review of the useof surface electromyography (sEMG) in the study of theneck musculature was an outcome of the 1998 MarconiResearch Conference. One of the goals of the conferencewas to develop consensus papers on the use of sEMGin the study of the neck and upper extremity regionsduring precision tasks. The papers were to specificallyaddress circumstances under which sEMG amplitudecould be used to estimate loads of the neck and upperextremity muscles during static or semi-static occu-pational tasks. Limited consensus emerged during theconference regarding sEMG of the neck musculature,because relatively few studies have employed sEMGspecifically to the neck musculature, there are inconsist-encies among methods used in published studies, andthere have been few investigations of methodologicalconsiderations specific to application of sEMG in thatregion of the body, including reliability assessments. Assuch, the objectives of this paper are to review the lim-ited research in the area and identify questions for futureresearch. The paper addresses muscle selection, elec-trode placement, data normalization, and data reductionmethods for investigation of precision, static, or semi-static tasks where muscle fatigue is not the focal point ofinterest. Organization of the paper is depicted in Fig. 1.
1.1. Relevance of neck muscle activity in ergonomicsresearch
Musculoskeletal discomfort in the neck has been asso-ciated with a variety of occupations and types of work,from those categorized as physically demanding, such asfarm work [57,66] and patient care [7,33] to those thatare considered fairly static, such as dental work[17,47,51], work at video display terminals [5,36], andsewing machine operation [1,67]. In a group of DanishCAD operators, Jensen et al. [28] found a 70% 12-monthprevalence of musculoskeletal symptoms in the neck,higher than any other body region, including low back(54%), shoulders (54%), and hands/wrists (52%). Manytypes of tissue in the cervical region can be sites of pain,including the neck muscles, intervertebral discs, the pos-terior longitudinal ligament, and the facet joints [8].Whereas heavy or more physical work has been associa-ted with diagnoses of cervical spondylosis [22] anddegenerative changes [78], static work is more oftenassociated with tension neck syndrome (myofascial pain)or myalgia [20–22]. Static work concentrates the work-load on fewer, smaller muscle groups [71], which maybe selectively overloaded through prolonged activationof some of the fibers in those muscles.
Muscle activity in occupational tasks is often investi-gated using surface electromyographic recordings.Assessing activity in the muscles through electromyog-raphy provides insight into patterns of activation or ten-sion developed in the muscles, which may be of interest

379C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
Fig. 1. Organization of this review of the use of surface electromyography to study the neck musculature.
in and of itself, because sustained muscle activity isknown to cause ischemic muscular pain [8]. Even at jointloads as low as 5% of maximum capacity, localized mus-cle fatigue has been shown to develop during sustainedcontractions [68]. Thus the relevance of studying muscleactivity that is expected to be relatively low, such aswhen working with computers or performing lightassembly work. Additionally, muscle activation patternscan be used to test assumptions of biomechanical models[16,49], or can be used as input to models in order todevelop estimates of muscle tension and loads in othertissues that are specific to an individual [9]. In manystudies of semi-static work, often also entailing repetitivemovements of the upper extremities, attention has beenroutinely focused on the descending (or upper) trapeziusmuscle. This muscle is a prevalent site of pain. That painis sometimes referred to as chronic trapezius myalgia ortension-neck syndrome, and may be associated withwork [41]. It has been studied extensively and severalrecommendations have previously been made regardingnormalization of the EMG signal [42] and the placementof electrodes over this muscle [29]. As such, and sincethe actions of this muscle are directed mainly towardsthe scapula and clavicle [31,35,86], and it does notappear to function primarily as a head or neck stabilizer,the trapezius muscle is of secondary importance to thisreview. The primary goal of the paper is to focus onthose muscles whose main functions are stabilization ormovement of the head or neck.
2. Muscle selection
The goals of any particular electromyographic investi-gation will dictate which muscles are selected for study,but consideration may be given to muscles that are sensi-tive to changes in experimental conditions, muscles thatare relevant in a particular occupational setting (site ofpain; subject to loading), or muscles that will provideinput to a specific biomechanical model. Based on exten-sive anatomical dissections, Kamibayashi and Richmond[34] identified more than 20 pairs of muscles that stabil-ize and/or move the head and neck. Unfortunately, onlya few of those muscles are superficial enough to access
with surface electrodes. For example, the dorsal muscles,which include those that extend the neck and head, areorganized into at least four layers [73], with the semispi-nalis, considered by many to be the primary extensor,located behind the splenius, which is partially coveredby the trapezius. Muscle selection should, therefore, beguided not only by previous research related to work orworkplace design, but by knowledge gained from morebasic types of research, including physical and biomech-anical modeling and basic functional assessments of theneck musculature.
2.1. Muscle selection in fundamental research on thecervical spine
In this section, muscle selections are reviewed fromstudies that addressed questions of basic muscle controland coordination. The studies employed a variety oftools, including physical models, biomechanical models,and electromyography. Muscle nomenclature is that usedby the researchers, and therefore, is not consistentthroughout the review.
2.1.1. Physical modeling of neck muscle contributionsBernhardt et al. [6], and Nolan and Sherk [50]
developed physical models to determine the relativeimportance of the various neck muscles for axial rotationand extension, respectively. Based on dissection, Nolanand Sherk [50] “identified the transversospinalis muscles(multifidus, interspinalis, semispinalis capitis, and semis-pinalis cervicis) as those muscles directly attached to thebony elements of the cervical vertebrae and, therefore,were most likely to control vertebral position”. Theyconcluded that the splenius, iliocostalis, and longissimusmuscles were only secondary extensors, and primarilyfunctioned in rotation and lateral bending. Exercisingtheir physical model of the head and cervical spine ledthem to conclude that the semispinalis performed a vitalrole in dynamic stabilization of the cervical spine. Thephysical model of Bernhardt et al. [6], designed to vali-date an optimization-based biomechanical model,included representations of the splenius, sternocleidoma-stoid, longus colli, obliquus capitis inferior, and trapeziusmuscles, the muscles they judged to be the prime rotators

380 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
of the head and neck. Four of the ten muscles investi-gated by these two teams of researchers are accessiblethrough sEMG, at least at some level along the cervicalspine: semispinalis capitis, splenius capitis, sternocleido-mastoid, and trapezius. However, access to the semispin-alis capitis is quite limited, as described by Queisser etal. [54].
2.1.2. Biomechanical models of neck musclecontributions
In addition to physical models, mathematical modelshave been developed to advance the understanding ofthe function of the cervical spine and musculature.Moroney et al. [49] developed an optimization-basedbiomechanical model of the neck, which included 14pairs of muscles, and was fashioned on the lumbar spinecutting plane model of Schultz and Andersson [65]. Choiand Vanderby Jr. [9] extended their efforts by applyingtwo additional solution techniques: an EMG-basedapproach and an EMG assisted optimization approach.The double optimization scheme was designed to minim-ize maximum muscle contraction intensity, and then ver-tebral compression. Platysma, infrahyoid, sternocleido-mastoid, longus colli and cervicis, scalene anterior,scalene medius, longissimus cervicis, levator scapulae,multifidus, semispinalis cervicis and capitis, spleniuscervicis and capitis, and trapezius were included in themodel.
In an effort to validate the model, Moroney et al. [49]collected sEMG data from 14 subjects who performeda series of isometric, voluntary maximum exertions inattempted flexion, extension, lateral bending, and twist-ing of the head and neck. Subjects then performed a ser-ies of exertions in which they resisted moments appliedthrough a helmet, in each of the same directions as thefirst task. Electrodes were all placed at the level of C4,and locations were specified as “anterior, anterolateral,posterolateral, and posterior, with approximate azimuthangles of 35, 70, 105, and 150 deg, respectively” (originat center of vertebral body; midsagittal plane marked 0°,anterior, and 180°, posterior) and later in the text wereassociated with specific muscles as follows: anterior withplatysma and infrahyoid, anterolateral with sternocleido-mastoid, posterolateral with scalene anterior and levatorscapulae, and posterior with splenius capitis and trapez-ius. However, these designations do not appear to com-pletely correspond to the cross-sectional anatomical ref-erence the authors cited. Moroney et al. [49] foundcorrelations from 0.29 to 0.85 between model predic-tions of activity in the muscles matched to electrode sitesand activity recorded from those sites. Correlations werepoorest for trapezius and levator scapulae, all below0.50. Correspondence of muscles and electrode sites wassomewhat different in Choi and Vanderby Jr. [9]. Theyexplained that muscles in the model were grouped tocorrespond with electrode locations, based on the
assumption that muscles of the same group were func-tionally similar and would display similar activity levels.Their groupings were as follows: anterior with platysmaand infrahyoid; anterolateral with sternocleidomastoid,longus colli and cervicis, scalene anterior; posterolateralwith scalene medius, longissimus cervicis, levator scapu-lae, splenius cervicis; and posterior with splenius capitis,trapezius, semispinalis cervicis and capitis.
One inherent limitation of the optimization approachis an output that does not predict antagonistic activity.The approach “forces” some muscles to be inactive,which can result in underestimation of muscle and jointloads. EMG-driven models have no such restrictions,and as such can provide more accurate informationregarding muscles that are likely to contribute to variousexertions. Muscles that were predicted to develop themost tension during peak isometric exertions, based onthe EMG-driven approaches of Choi and Vanderby Jr.[9], were: extension — levator scapulae, semispinaliscapitis and cervicis, trapezius, splenius capitis, multi-fidus; flexion — sternocleidomastoid, infrahyoid; lateralbending — sternocleidomastoid, levator scapulae, semis-pinalis capitis. Muscles included in the model ofMoroney et al. [49], that are accessible to sEMG at thelevel of C4 include sternocleidomastoid, trapezius, lev-ator scapulae, splenius capitis, platysma, and infrahyoid.However, the latter two muscles are generally not con-sidered to be stabilizers or movers of the head or neck,but are rather considered muscles of facial expressionand mouth and tongue stabilizers, respectively.
Based partly on the dissection work of Kamibayashiand Richmond [34], Vasavada et al. [75] developed a19-muscle biomechanical model of the neck, in order toexplore moment generating capacities of the muscleswith the head and neck in various postures. For a neutralposture, they determined that semispinalis had the great-est extension moment-generating capacity, followedclosely by splenius. Sternocleidomastoid had the greatestmoment-generating capacity in both flexion and lateralbending. Trapezius had the greatest moment-generatingcapacity in axial rotation, which was actually exceededby its lateral bending capacity. Each of these muscles isaccessible with surface electrodes, at least to someextent.
2.1.3. Functional assessments of neck muscle activityMost of the studies just reviewed relied solely on anat-
omy to predict the functions of the neck muscles. Elec-tromyography is seen by many as a way to verify musclefunction. The challenges of applying it in the cervicalregion are the main topic of this review. Studiesreviewed in this and the next subsection show whatresearchers have learned about the activity of the cervi-cal musculature through use of electromyography. Tak-ebe et al. [73] used bipolar fine wire electrodes to studyactivity in the splenius capitis and semispinalis capitis

381C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
in 15 subjects during movements of the head in variousdirections. Both muscles were found to be very active inextension movements and rotation movements combinedwith extension. In many subjects, maximum semispinalisactivity occurred in extension against resistance in a neu-tral sitting posture. Maximum splenius activity alsooccurred in that posture or in rotation against resistance.Neither muscle was active in quiet upright sitting. Onlythe semispinalis was even slightly active in maintainingthe head in a prone position. (Refer to Table 1 for asummary of each of the studies included in thissubsection.)
Schuldt and Harms-Ringdahl [64] studied the relation-ship between neck extension torque and activity in vari-ous neck muscles (see Table 1), as well as effects onthose relationships due to neck posture and individualdifferences between subjects. The cervical erector spinae(ES) electrode site displayed the greatest activation level(normalized to maximum); splenius and levator scapulaewere “intermediate in activation”. Activity levels in thecervical ES were higher in a mid-flexed posture (midwaybetween the head and neck being fully flexed and beingin a neutral, upright position) compared with a neutralposture, for the same “relative submaximal… moment”.The trapezius was found to be only minimally activeduring neck extension.
Keshner et al. [35] studied activation patterns in theneck musculature during upright sitting with the head ina neutral posture throughout the experiment. Theysought to identify preferred directions of activation offour cervical muscles which they assumed would beimportant for isometric head stabilization against anexternally applied destabilizing load, and that were cap-able of being studied with surface electrodes. They choseto study sternocleidomastoid, trapezius, splenius capitis,and semispinalis capitis. The authors were able to verifysurface electrode locations and muscle activation pat-terns with data from indwelling electrodes in a subset ofsubjects. From this research, the authors determined that:(1) muscle activation patterns varied somewhat betweensubjects, but especially in the resistance provided bysplenius to off-plane lateral bending; (2) splenius prim-arily responded to lateral bending, rather than extension;(3) semispinalis capitis was consistently active in exten-sion and posterolateral bending; and (4) trapezius con-tributed little to head stabilization. With regard to splen-ius activity, in half the subjects splenius was primarilyactive in lateral and anterolateral stabilization, and in theremaining subjects was primarily active in lateral andposterolateral stabilization. Findings with regard to thesplenius are somewhat at odds with those of Takebe etal. [73], who found little or no activation of that musclein lateral bending against resistance.
Queisser et al. [54] studied the relationship betweenactivity from various muscles (see Table 1) and iso-metric neck extension torque, as well as effects on those
relationships due to neck flexion posture, electrodelocation, and individual differences between subjects.They found that each of the muscles they studied wasactive during isometric neck extension, though someonly at higher levels of torque. The only muscle that wasactive at all exertion levels was the semispinalis capitis.Although posture had an impact on the relationshipbetween sEMG and torque within individuals, there wasno systematic effect across subjects.
Some of the interpretations and conclusions ofKeshner et al. [35] were challenged by MayouxBenhamou et al. [44], regarding the function of thesplenius capitis and the use of surface EMG to studythat muscle. Mayoux Benhamou et al. [44] used surfaceand fine wire electrodes to study splenius activity, andlooked for correspondence between the two signals.Computerized tomography was used to aid placement ofboth surface and intramuscular electrodes. Subjects per-formed a series of slow head movements in variousdirections (against gravitational resistance), as well as aset of maximum isometric exertions. Signals from bothtypes of electrodes showed activity in lateral bending(movement and isometric tasks), similar to Keshner etal. [35]. However, differences were found for some ofthe other exertions. The authors believed that crosstalkfrom adjacent muscles (primarily sternocleidomastoid;they monitored that muscle, as well as the trapezius andlevator) provided an explanation for their findings andthose of Keshner et al. [35] (who had found results splitamong subjects between anterolateral and posterolateralstabilization from the splenius). Mayoux Benhamou etal. [44] identified tasks during which the surface spleniuselectrodes detected activity and the wire electrodesdetected no signal: flexion from an extended position toneutral, extension from neutral to an extended position,contralateral rotation, and isometric flexion. Consistentwith Mayoux Benhamou et al. [44], the splenius wasalso shown, through use of MRI, to be active in exten-sion and ipsilateral rotation, and inactive in flexion andin contralateral rotation and flexion [11]. MayouxBenhamou et al. [44] suggested that surface electrodesonly be used on large neck muscles, such as the sterno-cleidomastoid, or when activity from the “dorsal group”would be sufficient.
Concerns raised by Mayoux Benhamou et al. [44]regarding the splenius led to examination of a study byMathiassen and Winkel [43], for similar concernsregarding use of surface electrodes to study the semispi-nalis capitis. Mathiassen and Winkel [43] chose toexplore the potential for differential activation of areaswithin the upper trapezius related to humerus positionand torque at the glenohumeral joint. What makes thisstudy relevant to the current discussion is the locationof one of the pairs of surface electrodes, at the level ofC1/C2 and 25 mm from the spinal column, a positiononly 5 mm lateral to the spot used by Keshner et al. [35]

382 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
Table 1Muscle selection and electrode location descriptions from functional assessments of the neck musculature
Study/task Muscles of interest Electrode locations Primary muscle activation
Takebe et al. [73]Various head movements and Splenius capitis 3 cm below mastoid process and 3 Head extension and ipsilateral headpostures; free and against resistance cm lateral from midline rotation
Semispinalis capitis 2 cm below occipital bone and 2 cm Head extensionlateral from midlineNote: used only fine wire electrodes
Schuldt and Harms-Ringdahl [64]Produced neck extension at several Cervical ES/covered by Cranial electrode at level of C2(C3)levels; upright and mid-flexed neck trapezius pars descendspostures
Splenius Caudal electrode at C2(C3) betweenuppermost parts of trapezius andsternocleidomastoid
Levator scapulae Both electrodes between posteriormargin of sternocleidomastoid andanterior margin of trapezius parsdescendensNote: center distances 30–35 mm;also examined trapezius and thoracicerector spinae
Keshner et al. [35]Upright head posture, sagittally Sternocleidomastoid Over muscle belly, about 1/3 of Anterolateral flexion, flexion, lateralsymmetric; isometric; resist external length rostral to sternal attachment bendloads applied through helmet
Trapezius Over muscle belly, about C6–C7 Isolated shoulder joint movementlevel and dorsal to insertion onlateral third of clavicle
Splenius capitis Palpated for muscle belly a location Lateral bend, and for 1/2 subjectsthat measured 6 cm rostral to C7 anterolateral bend and for other 1/2(about C4 level) and 6–8 cm lateral subjects posterolateral bend
Semispinalis capitis Over palpated muscle belly at Extension and posterolateral bendlocation 2 cm below occipital boneat about C1–C2 level, and 2 cmlateral to midline
Mayoux Benhamou et al. [44]Upright head posture; slow head Splenius capitis Wire at C4, 2 cm from midline Slow movements with no resistance:movements without resistance and ipsilateral rotation, extension,isometric maximums controlled flexion (eccentric); also
ipsilateral bendingIsometric maximums: ipsilateralrotation; also extension (ipsilateralbend not performed)
Splenius capitis Surface electrodes: upper surface at Slow movements with no resistance:C2, with 5 mm separation extension; also ipsilateral rotation
and bendingIsometric maximums: similaractivation levels in extension,flexion, ipsilateral and contralateralrotation
Sternocleidomastoid C2 (surface) Slow movements with no resistance:contralateral rotation; also extensionbeyond neutral, flexion fromextended posture, ipsilateral tilt fromtilted to neutral postureIsometric maximums: contralateralrotation; also flexion
Trapezius C2 (surface)Levator C4 (wire) Isometric maximums: shoulder shrug
Queisser et al. [54]Supine posture, sagittally symmetric; Levator scapulae Between posterior margin offour flexion angles; eight levels of sternocleidomastoid and anteriorrelative isometric extension exertions margin of trapezius, pars descendens
Trapezius C5/C6 about 2 cm laterally ofmedian line
(continued on next page)

383C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
Table 1 (continued)
Study/task Muscles of interest Electrode locations Primary muscle activation
Splenius capitis 6–8 cm lateral of median line atlevel of C4
Semispinalis capitis About 2 cm below occipital bone at Only muscle of the four tested thatC1/C2, and 2 cm lateral to median exhibited linear EMG activity-to-line torque relationship
Mathiassen and Winkel [43]Glenohumeral joint torque with Upper trapezius At level of C1/C2, 25 mm fromvarious positions of the arm spinal column
And three other locations morelateral and caudal
and Queisser et al. [54] for detecting semispinalis capitisactivity. Muscle activity from the electrode pair at thatlocation was sensitive to arm position, particularlyrelated to vertical arm position, particularly in womenand under the higher torque condition (30 Nm), and wasalso affected when subjects performed exertions with thecontralateral shoulder. Mathiassen and Winkel [43] com-mented on the uncertainty regarding the recordings fromthat location, remarking that they “may be considerablyinfluenced by activity from muscles other than” theupper trapezius, meaning muscles adjacent to the trapez-ius. Because other cervical muscles were not studied, thereason for the activity (contribution to shoulder stabiliz-ation or contribution to neck stabilization) cannot bedetermined.
Taken together, these fundamental studies indicatethat at least a few of the muscles important for neckmovement and stabilization are accessible with surfaceelectrodes. They are semispinalis capitis (extension,posterolateral bending), splenius capitis (extension, lat-eral bending, rotation), levator (lateral bending,rotation), sternocleidomastoid (flexion, rotation, lateralbending), and trapezius (most studies found it did notcontribute to head or neck motion or stabilization, butresearchers may need to monitor for crosstalk from it ifarms are active). However, as just discussed, concernshave been raised regarding the specificity of signals fromsurface electrodes over the splenius and semispinalis.
2.2. Effects of work and workplace design on muscleactivity
In contrast to the previous subsection, which exploredbasic function of the neck musculature with the use ofsEMG, this subsection reviews studies of various semi-static occupational tasks and effects of various modifi-cations or tasks on the sEMG. Many studies of lightwork are concerned with postures adopted by workersin response to the design of the workstation. Posturesare most often characterized simply by joint angle, butoccasionally external moments are estimated to expressthe burden on the active and passive tissues within the
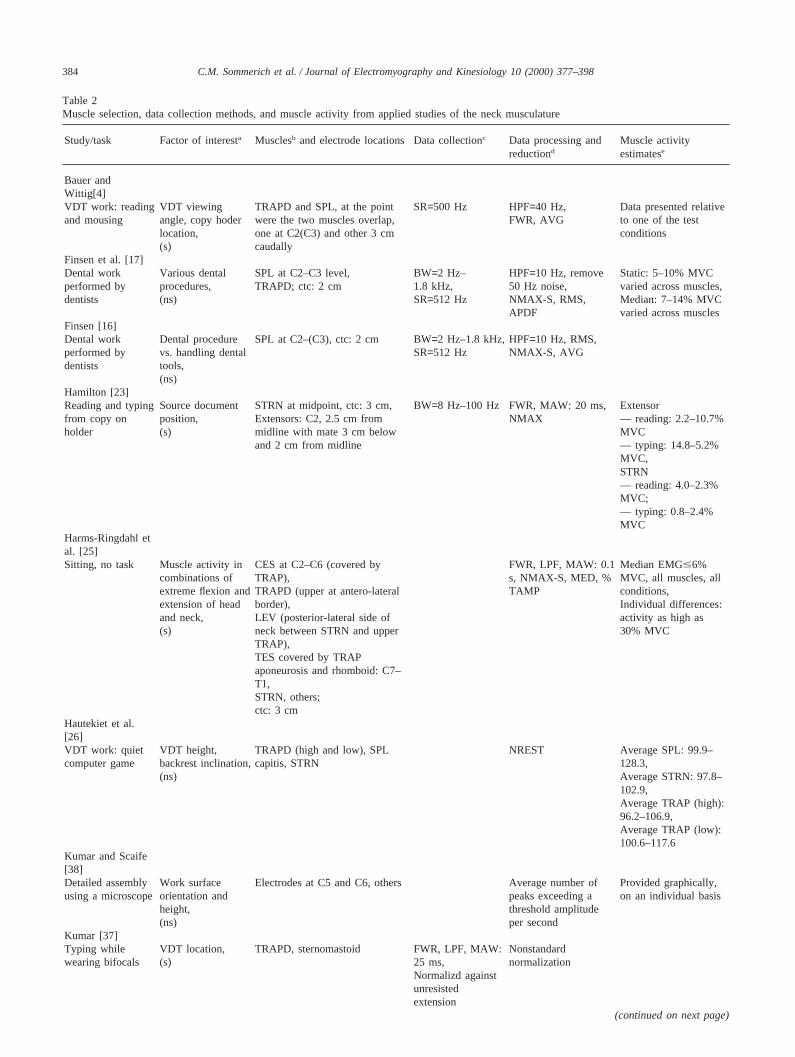
body associated with maintaining those postures [16,25].Muscle is the active tissue that provides part of thecounteracting moment, and sEMG is thought to reflectthe activity level of the muscle. Most ergonomicsresearch studies that have examined sEMG activity fromcervical musculature present results in terms of muscleactivity level, normalized or not, but do not attempt toestimate from that activity the tension in the muscle orthe muscle’s contribution to the restorative moment.Summary information on muscle selection, electrodeplacement, and data collection and processing from thestudies reviewed in this section is presented in Table 2.
2.2.1. Light manual workIn addition to the basic functional studies described
elsewhere in this review, Schu¨ldt and colleagues perfor-med several applied studies of the impact of workstationdesign and posture on muscle activity. Harms-Ringdahlet al. [25] described a study that focused exclusively onmuscle activity associated with five head and neck work-ing postures (four combinations of extremes of flexionand extension, and an upright neutral posture). For thesubjects as a group, muscle activity was quite low(maximum median activity at 6% MVC, but most were2% MVC or below, though some individuals displayedactivity as high as 10–30% MVC). There were generallyno significant differences in muscle activity across theconditions. However, cervical ES (covered by trapezius)was activated to 6% MVC in the head forward posture(neck flexion with head extension), in comparison to 0%MVC in other postures. Schu¨ldt et al. [60] reported aver-age muscle activity requirements in various seated pos-tures during a simulated circuit board assembly task. Ingeneral they found that neck flexion was accompaniedby increased activation of the trapezius-covered cervicalerector spinae (Tu-ESc), almost regardless of trunk pos-ture. Slumped forward trunk posture increased activityin Tu-ESc, levator scapulae, and other thoracic andshoulder muscles compared to a vertical trunk orien-tation, and a slightly reclined trunk resulted in evenfurther reduction of activity in most of those muscles,though not the already minimally activated levator scap-
384 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
Table 2Muscle selection, data collection methods, and muscle activity from applied studies of the neck musculature
Study/task Factor of interesta Musclesb and electrode locations Data collectionc Data processing and Muscle activityreductiond estimatese
Bauer andWittig[4]VDT work: reading VDT viewing TRAPD and SPL, at the point SR=500 Hz HPF=40 Hz, Data presented relativeand mousing angle, copy hoder were the two muscles overlap, FWR, AVG to one of the test
location, one at C2(C3) and other 3 cm conditions(s) caudally
Finsen et al. [17]Dental work Various dental SPL at C2–C3 level, BW=2 Hz– HPF=10 Hz, remove Static: 5–10% MVCperformed by procedures, TRAPD; ctc: 2 cm 1.8 kHz, 50 Hz noise, varied across muscles,dentists (ns) SR=512 Hz NMAX-S, RMS, Median: 7–14% MVC
APDF varied across musclesFinsen [16]Dental work Dental procedure SPL at C2–(C3), ctc: 2 cm BW=2 Hz–1.8 kHz, HPF=10 Hz, RMS,performed by vs. handling dental SR=512 Hz NMAX-S, AVGdentists tools,
(ns)Hamilton [23]Reading and typing Source document STRN at midpoint, ctc: 3 cm, BW=8 Hz–100 Hz FWR, MAW: 20 ms, Extensorfrom copy on position, Extensors: C2, 2.5 cm from NMAX — reading: 2.2–10.7%holder (s) midline with mate 3 cm below MVC
and 2 cm from midline — typing: 14.8–5.2%MVC,STRN— reading: 4.0–2.3%MVC;— typing: 0.8–2.4%MVC
Harms-Ringdahl etal. [25]Sitting, no task Muscle activity in CES at C2–C6 (covered by FWR, LPF, MAW: 0.1 Median EMG#6%
combinations of TRAP), s, NMAX-S, MED, % MVC, all muscles, allextreme flexion and TRAPD (upper at antero-lateral TAMP conditions,extension of head border), Individual differences:and neck, LEV (posterior-lateral side of activity as high as(s) neck between STRN and upper 30% MVC
TRAP),TES covered by TRAPaponeurosis and rhomboid: C7–T1,STRN, others;ctc: 3 cm
Hautekiet et al.[26]VDT work: quiet VDT height, TRAPD (high and low), SPL NREST Average SPL: 99.9–computer game backrest inclination, capitis, STRN 128.3,
(ns) Average STRN: 97.8–102.9,Average TRAP (high):96.2–106.9,Average TRAP (low):100.6–117.6
Kumar and Scaife[38]Detailed assembly Work surface Electrodes at C5 and C6, others Average number of Provided graphically,using a microscope orientation and peaks exceeding a on an individual basis
height, threshold amplitude(ns) per second
Kumar [37]Typing while VDT location, TRAPD, sternomastoid FWR, LPF, MAW: Nonstandardwearing bifocals (s) 25 ms, normalization
Normalizd againstunresistedextension
(continued on next page)
385C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
Table 2 (continued)
Study/task Factor of interesta Musclesb and electrode locations Data collectionc Data processing and Muscle activityreductiond estimatese
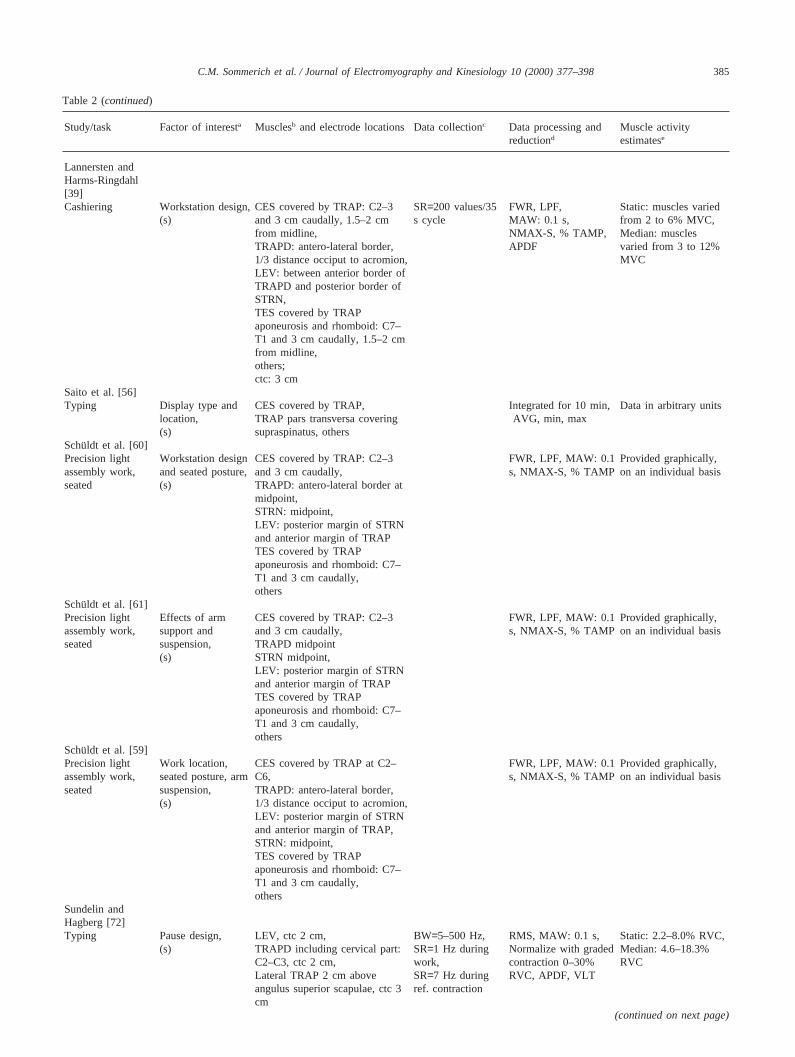
Lannersten andHarms-Ringdahl[39]Cashiering Workstation design, CES covered by TRAP: C2–3 SR=200 values/35 FWR, LPF, Static: muscles varied
(s) and 3 cm caudally, 1.5–2 cm s cycle MAW: 0.1 s, from 2 to 6% MVC,from midline, NMAX-S, % TAMP, Median: musclesTRAPD: antero-lateral border, APDF varied from 3 to 12%1/3 distance occiput to acromion, MVCLEV: between anterior border ofTRAPD and posterior border ofSTRN,TES covered by TRAPaponeurosis and rhomboid: C7–T1 and 3 cm caudally, 1.5–2 cmfrom midline,others;ctc: 3 cm
Saito et al. [56]Typing Display type and CES covered by TRAP, Integrated for 10 min, Data in arbitrary units
location, TRAP pars transversa covering AVG, min, max(s) supraspinatus, others
Schuldt et al. [60]Precision light Workstation design CES covered by TRAP: C2–3 FWR, LPF, MAW: 0.1 Provided graphically,assembly work, and seated posture, and 3 cm caudally, s, NMAX-S, % TAMP on an individual basisseated (s) TRAPD: antero-lateral border at
midpoint,STRN: midpoint,LEV: posterior margin of STRNand anterior margin of TRAPTES covered by TRAPaponeurosis and rhomboid: C7–T1 and 3 cm caudally,others
Schuldt et al. [61]Precision light Effects of arm CES covered by TRAP: C2–3 FWR, LPF, MAW: 0.1 Provided graphically,assembly work, support and and 3 cm caudally, s, NMAX-S, % TAMP on an individual basisseated suspension, TRAPD midpoint
(s) STRN midpoint,LEV: posterior margin of STRNand anterior margin of TRAPTES covered by TRAPaponeurosis and rhomboid: C7–T1 and 3 cm caudally,others
Schuldt et al. [59]Precision light Work location, CES covered by TRAP at C2– FWR, LPF, MAW: 0.1 Provided graphically,assembly work, seated posture, arm C6, s, NMAX-S, % TAMP on an individual basisseated suspension, TRAPD: antero-lateral border,
(s) 1/3 distance occiput to acromion,LEV: posterior margin of STRNand anterior margin of TRAP,STRN: midpoint,TES covered by TRAPaponeurosis and rhomboid: C7–T1 and 3 cm caudally,others
Sundelin andHagberg [72]Typing Pause design, LEV, ctc 2 cm, BW=5–500 Hz, RMS, MAW: 0.1 s, Static: 2.2–8.0% RVC,
(s) TRAPD including cervical part: SR=1 Hz during Normalize with graded Median: 4.6–18.3%C2–C3, ctc 2 cm, work, contraction 0–30% RVCLateral TRAP 2 cm above SR=7 Hz during RVC, APDF, VLTangulus superior scapulae, ctc 3 ref. contractioncm
(continued on next page)
386 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
Table 2 (continued)
Study/task Factor of interesta Musclesb and electrode locations Data collectionc Data processing and Muscle activityreductiond estimatese
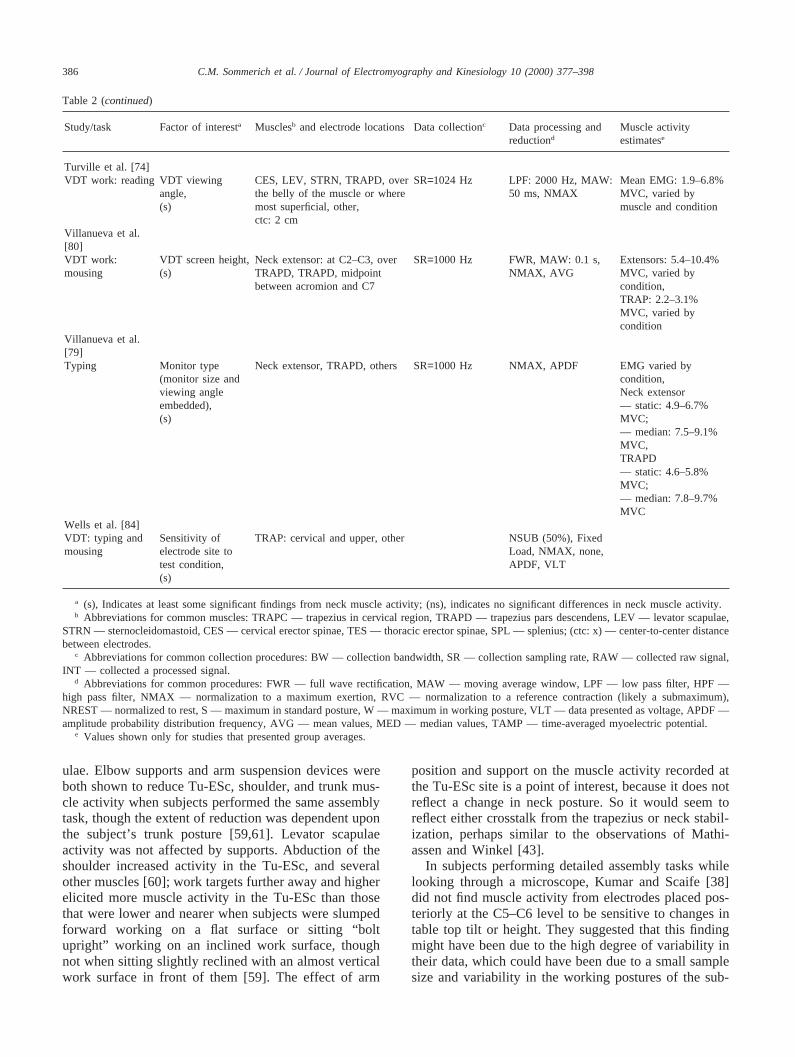
Turville et al. [74]VDT work: reading VDT viewing CES, LEV, STRN, TRAPD, over SR=1024 Hz LPF: 2000 Hz, MAW: Mean EMG: 1.9–6.8%
angle, the belly of the muscle or where 50 ms, NMAX MVC, varied by(s) most superficial, other, muscle and condition
ctc: 2 cmVillanueva et al.[80]VDT work: VDT screen height, Neck extensor: at C2–C3, over SR=1000 Hz FWR, MAW: 0.1 s, Extensors: 5.4–10.4%mousing (s) TRAPD, TRAPD, midpoint NMAX, AVG MVC, varied by
between acromion and C7 condition,TRAP: 2.2–3.1%MVC, varied bycondition
Villanueva et al.[79]Typing Monitor type Neck extensor, TRAPD, others SR=1000 Hz NMAX, APDF EMG varied by
(monitor size and condition,viewing angle Neck extensorembedded), — static: 4.9–6.7%(s) MVC;
— median: 7.5–9.1%MVC,TRAPD— static: 4.6–5.8%MVC;— median: 7.8–9.7%MVC
Wells et al. [84]VDT: typing and Sensitivity of TRAP: cervical and upper, other NSUB (50%), Fixedmousing electrode site to Load, NMAX, none,
test condition, APDF, VLT(s)
a (s), Indicates at least some significant findings from neck muscle activity; (ns), indicates no significant differences in neck muscle activity.b Abbreviations for common muscles: TRAPC — trapezius in cervical region, TRAPD — trapezius pars descendens, LEV — levator scapulae,
STRN — sternocleidomastoid, CES — cervical erector spinae, TES — thoracic erector spinae, SPL — splenius; (ctc: x) — center-to-center distancebetween electrodes.
c Abbreviations for common collection procedures: BW — collection bandwidth, SR — collection sampling rate, RAW — collected raw signal,INT — collected a processed signal.
d Abbreviations for common procedures: FWR — full wave rectification, MAW — moving average window, LPF — low pass filter, HPF —high pass filter, NMAX — normalization to a maximum exertion, RVC — normalization to a reference contraction (likely a submaximum),NREST — normalized to rest, S — maximum in standard posture, W — maximum in working posture, VLT — data presented as voltage, APDF —amplitude probability distribution frequency, AVG — mean values, MED — median values, TAMP — time-averaged myoelectric potential.
e Values shown only for studies that presented group averages.
ulae. Elbow supports and arm suspension devices wereboth shown to reduce Tu-ESc, shoulder, and trunk mus-cle activity when subjects performed the same assemblytask, though the extent of reduction was dependent uponthe subject’s trunk posture [59,61]. Levator scapulaeactivity was not affected by supports. Abduction of theshoulder increased activity in the Tu-ESc, and severalother muscles [60]; work targets further away and higherelicited more muscle activity in the Tu-ESc than thosethat were lower and nearer when subjects were slumpedforward working on a flat surface or sitting “boltupright” working on an inclined work surface, thoughnot when sitting slightly reclined with an almost verticalwork surface in front of them [59]. The effect of arm
position and support on the muscle activity recorded atthe Tu-ESc site is a point of interest, because it does notreflect a change in neck posture. So it would seem toreflect either crosstalk from the trapezius or neck stabil-ization, perhaps similar to the observations of Mathi-assen and Winkel [43].
In subjects performing detailed assembly tasks whilelooking through a microscope, Kumar and Scaife [38]did not find muscle activity from electrodes placed pos-teriorly at the C5–C6 level to be sensitive to changes intable top tilt or height. They suggested that this findingmight have been due to the high degree of variability intheir data, which could have been due to a small samplesize and variability in the working postures of the sub-

387C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
jects (sometimes resting heads on the microscope; some-times resting arms on the table top). The processingmethod may also have been a factor, because the authorscharacterized the signal as the “average number of peaksthat exceeded a given amplitude in one second”. Elec-trode sites were chosen by the authors “because (thosesites) were most frequently affected by pain in the oper-atives seeking medical help”.
In a study of different types of cash register systems,Lannersten and Harms-Ringdahl [39] reported static,median, and peak activity loads in the cervical ES(splenius at the location sampled, according to commentsof the authors), levator scapulae, and several shoulderand thoracic spine muscles. All activity was normalizedto maximum reference contractions, per the method ofSchuldt and Harms-Ringdahl [62], which is similar toSchuldt et al. [59], reported in Table 2. The cervical ESand levator scapulae displayed less activity than theother muscles the authors studied (only 1/4 to 1/2 asactive), and they were generally not sensitive to changesin the checkout procedures. The levator scapulae wassensitive to differences between keyboard and scanningmodes of entry.
Finsen et al. [17] performed an observational study ofeight female dentists, collecting both posture and sEMGdata while the dentists performed five common dentalprocedures. Dentists assumed relatively static postures,with cervical spines in pronounced flexion, sometimesalso with lateral flexion or rotation, and with somedegree of arm abduction. Muscle activity was nor-malized to a maximum exertion performed in a neutralseated posture. In each of the tasks, static EMG levelsin the splenius, sampled at C2–C3, exceeded the 5% ofmaximum voluntary contraction (% MVC) recommen-dation of Jonsson [32]. No differences in sEMG wereobserved between tasks, thus failing to confirm anyhypothetical beneficial muscle relaxation effect fromvariation among the various dental procedures.
2.2.2. VDT workSeveral studies of computer monitor and copy holder
placement have employed sEMG to characterize effectsof different placement locations. Height from the floorand viewing angle are the two common ways placementis characterized. Several studies have been performedusing each location convention. Almost without excep-tion, sEMG from electrodes located in the posteriorupper cervical region reflected differences in monitorlocation, at least between extremes in location.
Hamilton [23] found that normalized, mean sEMGsignals from electrodes located over the sternocleidoma-stoid and “extensor muscles of the neck” were sensitiveto changes in copy holder location for reading tasks(both muscles) and typing tasks (extensors only). Bauerand Wittig [4] chose to study activity from a single pairof electrodes located over the “trapezius pars descendens
and splenius cervicis”, because they regarded muscles atthat site to be “substantially responsible for the flexion ofthe cervical spine and its fixation in the median plane”.Subjects read and performed a pointing task. sEMG,presented as a percentage of the sEMG in the eye levelcondition, reflected differences between that location andlower locations when subjects were seated upright. How-ever, with a reclined seat back, eye level activity wasnot different from other locations. Only extreme differ-ences in copy holder location were reflected in differ-ences in sEMG. Turville et al. [74] found differencesin monitor viewing angle reflected in mean, maximum-normalized data from electrodes over the sternocleidom-astoid, levator scapulae, and cervical ES muscles, col-lected during an extended reading task.
Similar to Bauer and Wittig [4], Hautekiet et al. [26]found no significant differences in sEMG, as a percent-age of resting sEMG, from splenius capitis, trapeziuspars descends (high), or sternocleidomastoid in responseto changes in monitor location when subjects wereseated in a chair with a reclined backrest. They found anon-significant trend towards greater muscle activitywith a lower monitor position with subjects seatedupright, though results were not statistically significant.Villanueva and colleagues did find significant differ-ences in muscle activity recorded from electrodes at C2–C3 “to record the activity of the neck extensor muscle”and over the lateral portion of the trapezius [80]. In everysubject, extensor activity, normalized to maximum,showed a significant increase with decreasing height ofthe monitor (p,0.001 for each subject). Villanueva etal. [79] also found normalized static and median neckextensor activity to be sensitive to differences betweencomputer monitors — a complex mix of change in typeof screen, size of screen, and location of center of screen.Work on all flat panel screens elicited more muscleactivity than work on a standard desktop monitor. Saitoet al. [56], who compared a standard monitor to a single,smaller flat panel screen, found only one significant dif-ference among neck, shoulder, and upper backmuscles — the average value of the non-normalizedactivity from the cervical ES (covered by the trapezius)was greater with the flat panel screen. Viewing anglesfor the standard monitor and flat panel were 0.3° and235°, respectively.
To the question of appropriate monitor placement,Kumar [37] added the imposition of wearing simulatedbifocals. Electrodes were described as located on“descending trapezius and sternomastoid muscles”, andvoltage values were “normalized against unresistedextension values for the subject”. Both locations werefound to be sensitive to monitor placement.
2.2.3. BreaksSundelin and Hagberg [72] assessed the effects of dif-
ferent types of rest breaks, passive pauses (sitting with

388 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
hands in lap), active pauses (sitting while performingexercises), and diverting pauses (walking away from theworkstation), on subjective discomfort and muscleactivity of the levator scapulae and the trapezius,sampled at the C2–C3 level and at a lateral location. Thereference contraction (RC) for normalization purposeswas a maximum shoulder shrug. This exertion has beenfound to be effective in eliciting maximum activity inthe levator and upper trapezius in some subjects, but isunlikely to elicit maximum activity in the neck exten-sors. sEMG was collected during exertions from 0 to30% RC. A power function was used to describe therelationship between muscle activity as voltage and forceexertion level. Pauses lasted 10–12 s, and occurred every6 min for a 30-min test period. Data were presented asamplitude probability distribution frequency (APDF).For all electrode sites, only the peak activity (99thpercentile) was found to differ between pause conditions.
These applied studies show that there is variation inthe reported degree of precision between experi-mentalists with respect to placement of electrodes, speci-ficity of muscles sampled, as well as combinations ofmuscles sampled. Consistent with the basic researchstudies discussed previously, workplace researchersoften sampled from some combination of splenius, ster-nocleidomastoid, levator, and trapezius muscles. Semis-pinalis capitis was not specifically mentioned in theseapplied studies. Instead, several researchers opted for asite a bit lower on the neck (C2–3 rather than C1–2),acknowledging that they were sampling from upper trap-ezius fibers in addition to the muscle of interest —referred to as the cervical erector spinae. Most likelywhat is sampled is the trapezius and the semispinaliscapitis if electrodes are high enough, or the trapezius,splenius capitis, and semispinalis capitis if sampled a bitlower still or further from the midline.
3. Electrode placement
3.1. Locating electrodes
It may be clear by now that there are basically twoapproaches which researchers seem to take in locatingsurface electrodes to study the neck musculature: mus-cle-specific sites (such as in Keshner et al. [35] andQueisser et al. [54]) and location-specific sites (such asin Choi and Vanderby Jr. [9] and Moroney et al. [49]).Data from location-specific sites may be appropriatewhen interest is in levels of activity in a muscle group,such as the dorsal muscle group (also referred to as thecervical paraspinal group). However, problems ininterpretation of results can arise when data are thoughtto come from muscle-specific sites, but contain crosstalkfrom adjacent muscles — essentially making the sitelocation-specific, instead. This is the problem about
which Mayoux Benhamou et al. [44] was concerned.Additional information about both types of electrodesites is presented in this section, along with further dis-cussion about crosstalk, and another important place-ment-related issue: muscle innervation zones.
3.1.1. Anterior musclesZipp [89], a classic source of recommendations for
electrode locations based on work by that author and aUS Air Force technical report [13], only provides infor-mation on one cervical muscle — the sternocleidomas-toid. He recommended a location one-third the length ofa line from the mastoid process to the suprasternal notch,consistent with Davis [13]. This location differs from the“1/2 the distance” recommendation of Cram et al. [12],who also suggested the site be “slightly posterior to thecenter of the muscle belly” with 2 cm electrode separ-ation, based on their experience.
3.1.2. Posterior musclesCram et al. [12] also provided a recommendation for
a “quasi-specific” site for sampling the “midcervical par-aspinal” muscles (trapezius, capitis and cervicis groups),with electrodes centered 2 cm apart about a spot 2 cmfrom the midline at C4. As mentioned previously, morespecific locations were provided by Keshner et al. [35],who described access to the splenius capitis, which liesbeneath the trapezius and the sternocleidomastoid, as “arectangular area on the lateral portion of the neck wherethe (splenius) is the most superficial muscle. This musclecan be palpated between the (sternocleidomastoid) and(trapezius) when resistive extension and lateral rotationare performed in the same direction as the muscle”. Theydescribed access to the semispinalis as follows: “…mostof (semispinalis) lies close to midline and can be pal-pated by resisting head extension. The muscle is coveredby either (splenius) or (trapezius) except for a small areaextending from its insertion to about the level of thesecond cervical vertebrae”. The electrode locations theychose are listed in Table 1.
3.2. Crosstalk
Crosstalk is the detection of signals from more thanone muscle through a pair of electrodes. Several of thestudies reviewed to this point, though not specificallyusing the term crosstalk, acknowledged that their elec-trode sites collected signals from multiple muscles. Forexample, Bauer and Wittig [4] reported measuring mus-cle activity “at the point where the cervical m. erectorspinae and the m. trapezius pars descendens overlap eachother” because they considered those muscles to be “sub-stantially responsible for the flexion of the cervical spineand its fixation in the median plane”. However, few stud-ies have specifically investigated crosstalk in the neckmusculature. In order to assess the amount of crosstalk

389C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
in sEMG from the semispinalis, splenius, and trapeziusmuscles, Keshner et al. [35] compared responses fromsurface and indwelling electrodes at the same locations(though intramuscular trapezius electrodes were located“closer to midline, but at the same cervical levels, to becertain of recording from the upper fibers”). Data fromthe semispinalis and splenius were comparable betweenmethods, based on visual inspection of polar plots ofactivity from the two types of electrodes. However, pat-terns for trapezius activity were quite different betweenthe two methods. For both subjects tested, indwellingelectrodes indicated that the muscle responded mostactively to a destabilizing contralateral pulling load inthe posterolateral direction for one subject and the ante-rolateral for the other subject; these directions were notshown to be preferred when examining data from thesurface electrodes. The authors added that the trapeziuswas most active, based on data from both types of elec-trodes, when subjects performed isolated shoulder move-ments, rather than during head stabilization efforts.These results suggested to the authors that the muscleprimarily functioned as a scapular stabilizer, instead ofa mover or stabilizer of the head. This may also indicatethat activity from the surface trapezius location containscrosstalk from underlying head stabilizers, as alluded toby Mathiassen and Winkel [43]. As previously dis-cussed, Mayoux Benhamou et al. [44] provided contra-dictory conclusions to those of Keshner et al. [35],regarding the nature of the electrode site for the splenius.
Crosstalk is an issue in the use of surface electromy-ography in many parts of the body — wherever small orthin muscles are closely packed. Methods for detectingcrosstalk include the double differential technique andfrequency spectrum analysis. Readers are referred to areview paper by De Luca [14] for a more thorough dis-cussion of the topic of crosstalk.
3.3. Innervation zones
Even if electrodes are properly located over a parti-cular muscle of interest, and crosstalk is determined notto be a problem, there can still be another location-related problem if the electrodes are placed such thatthey straddle the muscle’s innervation point (innervationzone). The electromyographic signal is less reactive andgenerally unreliable from electrodes located over a mus-cle’s innervation zone (IZ) [3]. Queisser et al. [54] wereconcerned with determining whether the electrodelocation sites they had selected were over muscle inner-vation zones. As such, they located an extra electrodeon either side of each primary pair of electrodes, andcompared signals from the three pairs of electrodes thatcould be formed by adjacent electrodes at each musclesite. Based on pronounced reduction in sEMG ampli-tudes, they determined that their standardized electrodesites were located over the semispinalis IZ in three of
12 subjects, over the splenius capitis IZ in five subjects,and over the levator scapulae IZ in one subject. Suchhigh percentages for the semispinalis and spleniusappear to raise the level of concern regarding the abilityto detect activity with surface electrodes, both specifi-cally and reliably, from these two muscles.
It should be mentioned that many of the researcherscited in this review found the opportunity to dissecthuman cadavers prior to their use of surface electromy-ography substantially improved their abilities to specifi-cally locate particular muscles in the neck. However, thepresence of IZ below electrode sites, particularly for thesplenius [54] signifies that proper location of a muscledoes not guarantee obtaining data that are representativeof the activation of the muscle. Additional researchshould be conducted in order to determine robust esti-mates for the likelihood of IZ presence at sites that arecommonly used for surface electromyography of theneck muscles. Consideration should be given towardsincorporating, as standard practice, testing for the pres-ence of IZ when studying the neck muscles with sEMG.
4. Normalization
Normalization of EMG data has been proposed toaddress variation introduced in the measurement processby differences in electrode spacing, anatomical factors,and variation in electrode placement in multi-day experi-ments in order to facilitate comparisons between differ-ent muscles and individual subjects. According to Bas-majian and De Luca [3], “The absence of normalizationoften constitutes a deficiency in many reported investi-gations which have compared or averaged groups of sub-jects”. Normalization may be used so that EMG ampli-tude can be reported as a percentage of amplitudedisplayed during a maximum voluntary exertion, or maybe taken further to provide an estimate of muscle force.The relationship between sEMG and force or torque istypically described by either a linear or a power function.Basmajian and De Luca [3] suggested several reasonsfor muscle-dependent differences in the EMG–forcerelationship, including motor unit recruitment and firingrate properties, location of fast twitch fibers within themuscle and relative to electrodes, crosstalk from othermuscles, activity in antagonist muscles, as well as pro-cessing methods and choice of amplitude descriptor (rootmean square, integrated, etc.).
4.1. Level of exertion in reference contractions
There is a lack of consensus regarding terminologyand methods in the normalization procedure. Mathiassenet al. [42] suggested expressing the normalization of theEMG amplitude either in percentage of a reference vol-untary electrical activation (% RVE) during a submaxi-
390 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
mal contraction, or in percentage of the maximal volun-tary electrical activation (% MVE). Several advantagesand disadvantages can be argued for both these tasks,submaximal or maximal. In summary, when a maximalcontraction is used, questions can be asked regarding thevalidity of the performance when the subject is unmot-ivated or unaccustomed to the task [42]. Jensen et al.[30] concluded that when estimating maximal ampli-tudes, one maximal contraction does not produce areliable estimate. This is particularly true for exertionsmade with the head, as most people are unaccustomedto performing forceful exertions with their heads, andtherefore require practice to produce true and consistentmaximums. Jensen et al. [30] recommended that as manycontractions as possible should be performed to estimatethe maximal amplitude, without fatiguing the subject.However, Veiersted [76] raised a concern that maximalcontractions might cause discomfort, potential injury,and the risk of delayed muscle soreness. Especially inthe neck region, a maximal exertion without appropriateprecautions can be questionable in terms of the sensi-tivity of the neck during manipulation, forceful exer-tions, or rapid increases in force. In order to overcomethese problems, a reference submaximal contractionmight be considered. Bauer and Wittig [4] simply nor-malized data from the various conditions they tested todata from one particular condition. Veiersted [76] men-tioned the possibility of using an external load todecrease the sensitivity of a test contraction and improvestandardization. The negative points of using a submaxi-mal reference contraction are that no answer can begiven regarding the percentage of the maximal capacityat which the muscles are performing, or regarding rela-tive contributions among different muscles, and thatdirect comparisons with other studies are precluded.
In a series of reports, Wells and colleagues [83,84]explored within- and between-day repeatability of sEMGfrom a number of locations, including “cervical trapeziusfibers”, in order to identify a set of recording sites thatwere both sensitive to differences between test con-ditions and consistent in the estimates of activity theyproduced. Reliability of the APDF data was charac-terized by the intraclass correlation coefficient (ICC).Between-day ICCs were affected by choice of normaliz-ation method, though not consistently for the variouselectrode locations. Wells et al. [83] used several nor-malization schemes to explore the impact of normaliz-ation method on ICC. Methods included normalizationto a maximum, to a fixed value, to 50% of maximum, aswell as without normalization. APDF from the cervicallocation was found less sensitive to normalizationmethod than some of the other locations (sites overshoulder or forearm muscles), but was also found to beless reliable than several of those sites.
4.2. Posture and direction of exertion in referencecontractions
Since light work tasks are characterized by fairly staticsubmaximal contractions during which no fast or force-ful neck or shoulder movements are present, dynamicreference contractions do not seem warranted. Rather, areproducible, stable position should be chosen. However,when several head and neck postures or movements arepresent during the work task, Finsen [15] raised the issueof the use of a slow dynamic reference contraction forthe normalization of the EMG amplitude, based on theresults of Christensen et al. [10]. For the biceps muscle,the average muscle length was similar during a slowconcentric and eccentric phase of a dynamic contractionand the amplitude of the surface and the intramuscularEMG was not different. However, this has to be investi-gated for the neck region, since some muscles displayan increase in amplitude at any non-zero velocity.
The focus of a report by Schu¨ldt and Harms-Ringdahl[62] was identification of single, static reference contrac-tions that consistently produced maximum exertions insubjects seated in an upright, neutral posture: isometricneck extension against resistance at the occiput for thecervical ES/trapezius; isometric lateral flexion withresistance against the temple for splenius and levatorscapulae. Keshner et al. [35] found linear EMG–forcerelationships for each of the neck stabilizers they studiedwhen the muscles acted in their preferred directions,though exertions were at submaximum levels (from 0.9to 3.6 kg of destabilizing weights were applied in thatpart of the experiment).
On the other hand, posture-specific normalization hasalso been recommended [48]. There are two primaryreasons to account for posture in normalization. One rea-son is that the portion of the muscle “seen” by the elec-trodes changes as the muscle lengthens or shortens inresponse to changes in joint orientation. The other reasonis that the length and moment arm of the muscle changewith changes in posture, which means a change inmoment generating capacity about the joint. In order torelate EMG to force, the change in moment generatingcapacity should be considered. Schu¨ldt and Harms-Ring-dahl [63] showed that “upper cervical spine” position(head fore–aft rotation) did not impact maximum EMGlevels in the cervical ES/trapezius, levator scapulae, orsplenius, though lower cervical spine position did havean effect in subjects sitting upright and producing exten-sion exertions (electrode locations were those reportedin Schuldt and Harms-Ringdahl [64], and listed in Table1). In their examination of the semispinalis muscle wher-ein subjects performed isometric extensions whilesupine, Queisser et al. [54] found the EMG–torquerelationship to be linear in each of the four neck posturesthey examined (from 0 to 30° of flexion), in 10 of 12subjects. They did not, however, examine the effect of

391C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
normalizing task data in one posture with maximumscollected in another posture.
As only a few studies have specifically addressedmethodological questions surrounding normalizationprocedures for the neck musculature, this would seem tobe an area ripe for investigation. Those researchers whodo normalize their data seem to do so with respect to asingle posture — the importance of the change in musclelength does not seem to have been fully explored.Additionally, restrictions on lateral bending and rotationhave not been addressed. Also, in light of the crosstalkidentified by Mayoux Benhamou et al. [44], which wasparticularly noticeable during isometric maximum exer-tions, when assuming muscle-specific electrode sites thepractice of using a maximum value from any maximumexertion may not be valid; consideration should be givento restricting identification of maximum values to thoseexertions known to be in the primary direction of actionfor the specific muscle.
5. Additional methodological issues
Once sEMG data are collected, the primary interestof ergonomics researchers seems to be amplitude of thesignal (mean, median, or static values). Only a few haveattempted to make a connection between muscle forceand muscle activity determined from sEMG, a connec-tion that would seem to require an understanding of therelationship between sEMG level and external loads onthe head and neck, as well as a biomechanical modelingcomponent. An additional methodological issue that isrelated to interpretation of EMG data, and one that israrely addressed by researchers, is the reliability of theirmethods, and consequently their data and results.Reliability will also be addressed in this section.
5.1. Relationship between sEMG and force or torque
Sundelin and Hagberg [72] developed a power func-tion to relate muscle activity to levels of exertionbetween 0 and 30% of maximum, though the relation-ship was not presented in the paper, and the selectedreference exertion was not appropriate for elicitingmaximum activity from at least one of the locationssampled (posterior neck at level of C2–C3).
In studying the response of several neck muscles to0.9 kg (2 lb) incremental increases in isometric loadingin a small subset of their subjects, Keshner et al. [35]found a linear relationship in the primary loading direc-tions of the muscles. Semispinalis displayed linearresponses to increased loads presented in pure flexion(requiring pure extension resistance) and in counteringa pure lateral load on the contralateral side (requiringpure ipsilateral resistance). Splenius displayed linearresponses to flexion and extension loads, and to a contra-
lateral load. Sternocleidomastoid displayed a linearresponse to loads in extension and contralateral bending.A variety of non-linear relationships were also displayed.For some subjects and muscles, the muscle remainedinactive until an apparent load threshold was exceeded,after which point the muscle became very active. Insome subjects, a muscle which was active when loadedin a non-preferred direction would suddenly becomesilent beyond a certain load level. Additionally, somemuscles displayed a non-linear increase in response toloading in a non-preferred direction.
One of the specific goals of the research of Queisseret al. [54] was the examination of the sEMG–torquerelationship in the neck extensors. In pooling their dataacross subjects, only semispinalis sEMG activity (µV)showed a linear relationship with extension torque (Nm).These findings were consistent across the four postures.The other muscles displayed non-linear increases insEMG with increasing torque. They also looked at theseassociations for individual subjects, and concluded thatthere were some significant differences between individ-uals. One of the reasons for the differences was thelocation of electrodes over innervation zones for somesubjects. Other reasons included examining the sEMG–torque relationship in absolute, rather than normalized,terms. Queisser et al. [54] examined the impact of sev-eral normalization schemes on the sEMG–torquerelationship. Normalization of either torque or sEMGsubstantially reduced intersubject variation, with nor-malization of both being most effective. In spite of theimpact, however, the authors cautioned that “individu-ally predictions vary by up to 15% of the MVC”, whichthey suggested would cause problems in trying to predictan individual’s response from the mean results of agroup. They concluded with a warning against usinggroup results to predict individual responses.
In contrast to the linear relationship identified byQueisser et al. [54], Schu¨ldt and Harms-Ringdahl [64]found a non-linear relationship between cervical ESactivity and extension moment, both of which were nor-malized to maximum values. Splenius also displayed anon-linear relationship to neck extension. Although, forboth muscles a few individuals displayed linear relation-ships.
5.2. sEMG as an estimator of muscle load
Harms-Ringdahl et al. [25] studied the associationbetween neutral and extreme combinations of head andneck postures and activity in the cervical ES, sternoclei-domastoid, and levator scapulae muscles. sEMG datawere normalized to maximum contractions collected ina neutral posture. Although calculated moments aboutthe centers of rotation for the head and neck varied withhead and neck posture, normalized sEMG amplitude didnot, and as such amplitudes were not reflective of the

392 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
internal forces which were supporting the head and neckin those various postures. This may accurately reflect theactivity of the muscles, that is the flexion-relaxationphenomenon observed by Meyer et al. [46] in extremeflexion, or may reflect a methodological problem withthe normalization procedure (no accounting for pos-tural differences).
Finsen [16] presented similar findings in a study ofdentists’ working postures. Dentists tended to adopt twoneck postures, one moderately flexed and the other moresevere (and more common). The flexion angle of theatlanto-occipital (AO) joint was essentially constant.Activity in the splenius, normalized to a neutralmaximum, did not correspond to the moments due to theweight of the head and neck calculated for the two pos-tures. The author also pointed out the difference betweenthe mechanical load and the muscle activity when eachwas normalized to maximum. Her estimate of the mech-anical load was 40% of maximum while the activity inthe splenius was 10% of maximum. As the authorpointed out, however, only one muscle was monitoredin this study while there are several that are positionedto provide extensor moments to the neck. She noted thatpassive structures are also likely to provide resistancemoments.
5.3. Reliability of data
In order to characterize the response of a muscle ormuscle group to a particular condition (such as amaximum exertion; one keyboard vs. another; one hand-tool vs. another), the degree of variability in the EMGsignal must be assessed. This can help to determine thenumber of samples needed to provide stable estimatesof the various statistical values used to describe theEMG signal, and can be useful in weighing advantagesand disadvantages of various experimental designs (forexample, exposing subjects to all test conditions in a sin-gle day vs. exposing them to different conditions on dif-ferent days in order to reduce carryover effects). Repro-ducibility in individual subjects is important inlongitudinal studies of muscle load as a risk factor formuscle pain or in assessing interventions [76]. Few ofthe authors who have used sEMG to study the neckmusculature have addressed reliability or repeatabilityissues in their work. Therefore, discussion of this topicwill extend beyond sEMG applied to the neck muscu-lature.
5.3.1. Reference exertionsVeiersted [76] reviewed the main factors that affect
the EMG signal associated with a given level of exer-tion: interelectrode resistance, muscle temperature, localmuscle fatigue, electrode spacing, and electrode positionrelative to the muscle. Normalization of the EMG signalto a reference exertion recorded in the same time period
is meant to account for these factors which differbetween subjects and can differ within subjects overtime.
The reliability of EMG data from maximum referenceexertions was questioned by Yang and Winter [87]. Theycompared the consistency of sEMG data from maximumvoluntary contractions (MVCs) to that of submaximumexertions controlled by feedback, using the triceps mus-cle. They found within days CVs of 9–10%, and betweendays CVs of 12–16%. ICCs were found to be greater forsubmaximum exertions (ranging from 0.78 to 0.95) thanfor maximums (ranging from 0.52 to 0.81), with vari-ation due to number of repetitions within and betweendays. Based on assessment of their data, the authors sug-gested that the best method for collecting EMG data wasto collect all data in a single day, and perform test(normalization) contractions at the beginning and end ofthe test session. If multiple testing days are necessary,they suggested averaging test contraction data acrossdays, in order to increase reliability. They suggested aminimum of three repetitions within a day, if multipledays are required, but only one experimental conditionoccurs in a day.
In a series of reports, Wells and colleagues [83,84](Table 2) explored within- and between-day reliability ofsEMG from a number of locations, including “cervicaltrapezius fibers”, in order to identify a set of recordingsites that were both sensitive to differences between testconditions and consistent in the estimates of activity theyproduced. Cervical trapezius location produced ICCvalues of 0.43–0.56, values below those of several othermuscles [83]. Between-day ICCs were found to be affec-ted by the normalization method, though the effectvaried among the different recording sites. Veiersted[76] determined the main sources of variation, inattempts to reproduce test contractions for the trapezius,to be in repositioning electrodes (CV=16.8%) and repo-sitioning subjects (CV=15.9%). Lengths taken to minim-ize variation from those two sources included use of trac-ing paper to mark electrode and landmark locations, anduse of several spatial markers to position subjects.
5.3.2. Exertions during performance of work tasksWhen employing EMG to quantify a work task the
signal will vary due to the basic stochastic nature of thesignal and in response to muscle activation and length,as well as in response to changes in the factors men-tioned above. Veiersted [77] evaluated the reliability ofrepeated measures of static sEMG activity (10th percen-tile APDF) in the upper trapezius during light work.Across 4 days, two measures each day, the authorreported a within-subject CV of 20%, and an estimatedreliability coefficient of 0.59, for EMG data that rangedfrom 0.05 to 4% MVC. Wells et al. [83,84] determinedthat a 20-min time period containing several repeatedsamplings of the sEMG signal was necessary to achieve

393C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
their desired level of measurement precision, a CV of10%, for 10th, 50th, and 90th percentile sEMG statisticsfor wrist extensor and trapezius muscles for subjects per-forming tasks on a computer. Within- and between-dayICCs for 10th percentile sEMG data ranged between0.43–0.96 and 0.0–0.92, respectively, depending onmuscle and normalization method. Kumar and Scaife[38] (Table 2), the only other neck musculature studyto consider variation in their data, reported finding nosimilarity in neck muscle activity sampled during differ-ent days between the same subjects. This, however, mayhave been due to the wide variety of postures their smallnumber of subjects assumed during the course of thestudy.
Given the limited number of reports of reliability ofneck muscle sEMG data, it may be premature to con-clude that neck muscle sEMG responses are inconsistent,which would bring research results into question andmake comparisons between studies difficult. However,the limited number of reports of data reliability indicatesa void in the research knowledge base which needs tobe addressed. Conflicting explanations of results of stud-ies of basic muscle function, such as those offered byKeshner et al. [35], and Mayoux Benhamou et al. [44],demonstrate that reliability of data should be a funda-mental concern of all researchers.
6. Special concerns
When using electromyography, it is important to beaware that factors in addition to those of interest to aspecific experimental hypothesis may affect muscleactivity. For example, muscle tension may reflect non-muscular sources of pain or dysfunction, such as the“splinting” mechanism which is commonly observed intransitory straightening of the cervical curvature follow-ing significant cervical extension injury. Other factorsthat may alter muscle activity include anxiety or stress[19], task-related cognitive/attentional demands [82,85],task-related pain [24], or impaired vision [40]. Environ-mental noise (60 Hz) and other types of artifact are alsoparticularly problematic in studying sEMG from theneck musculature during quiet work. Since the signal ofinterest is very low, the signal-to-noise ratio is easilyreduced when noise is present. Additionally, neck mus-cle sEMG signals are subject to some types of artifactto which signals from muscles located elsewhere in thebody are not. These special concerns for extraneousinfluences on sEMG from the neck musculature arereviewed in this section.
6.1. Swallowing and breathing
Utilizing indwelling electrodes in 10 subjects, Vitti etal. [81] found no activity in the sternocleidomastoid
muscles of any subjects during dry or wet swallowingand moderate activity in 18 of 20 (left and right) musclesduring deep breathing. However, Ormeno et al. [52]specifically chose to study the activity of the sternoclei-domastoid in their research on patients with myogeniccranio-cervical-mandibular dysfunction undergoingocclusal splint therapy, in order to learn whether postureaffected EMG activity during swallowing and otheractivities. In a study of the effects of computer monitorplacement, Sommerich et al. [69] found forceful swal-lowing and sniffling introduced artifacts in the sternocle-idomastoid sEMG signal for subjects working quietly ata VDT. Portions of data that contain such artifactsshould be removed prior to analysis.
6.2. Heartbeat (ECG)
Few authors mentioned the presence or absence ofECG in their sEMG data. Bansevicius et al. [2], whosampled the frontalis, temporalis, splenius, and trapeziusmuscles, judged heartbeat contamination to be minimal,and therefore considered it part of the noise in their sys-tem. By contrast, Queisser et al. [54] reported ECG inter-ference in all four neck muscles they studied. It was mostpronounced in the levator scapulae, and less though stilldistinct in the trapezius and semispinalis capitis. It wasonly slightly evident in the recording of the restingsplenius capitis. Their solution was to subtract theresting rms value from rms values during contractions.Bauer and Wittig [4] reported high pass filtering theirdata at 40 Hz to eliminate heartbeat. Because the ECGappears as such a defined artifact, another way to treatan EMG signal that contains it would be to remove thoseparts of the data that contain the artifact. In essence, onlyconsider the data in between heartbeat registrations.
6.3. Visual stress
Lie and Watten [40] found activity from the “upperneck including splenius”, “levator and upper trapezius”,and other assorted facial and shoulder muscles wassensitive to visual stress experienced by seated subjectsreading at eye level under different visual stress con-ditions. In a group of subjects without musculoskeletalsymptoms in the cervical region, neck muscle activityincreased with a decrease in viewing distance (from 6m to 40 cm, reading material subtending a visual angleof 1° in both cases), and activity increased in the neckand levator locations in conditions that induced vergencestress and accommodation stress. In a group of subjectswith long-standing occupational cervicobrachial disorder(OCD) symptoms, optimal correction of visualdeficiencies resulted in a decrease in activity in the neckand levator muscles during reading at 40 cm. Theauthors suggested that sustained stress of the visual sys-tem, induced by a combination of the nature of some

394 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
work (VDT) and uncorrected visual deficiencies inworkers, could lead to increased activity in posturalmuscles. What is not clear is whether the increase is dueto an increased need for stabilization of the head andneck, a forward positioning of the head, or, as theauthors suggested, is due to a connection between theextraoccular and smooth eye muscles and the posturalmuscles through synapses in the midbrain and brainstem.
6.4. Muscular pain
Harms-Ringdahl and Ekholm [24] studied EMGactivity in the splenius, thoracic ES, and trapeziusmuscles during sustained extreme neck flexion. sEMGwas low for all muscles throughout the test. Whileactivity of the splenius was not found to correlate withintensity of pain that developed during the test, EMGactivity was greater at the end of the test than at thebeginning, as was pain experienced by the subjects.There were no changes in posture to which sEMGincreases could have been attributed. The authors sug-gested that increases might have been due to the pain,“indicating that tonic (sustained) reflex mechanismsmight have been elicited”. By contrast, Bansevicius etal. [2] found no increase in splenius activity during a 1-h long, two-choice reaction time task, though ratings ofdiscomfort increased steadily during the task. Subjectsin the latter study were seated in office chairs andworked on VDTs during the task, so, unlike the formerstudy, no overtly awkward or uncomfortable postureswere involved.
To summarize this section, even if electrodes areproperly placed and data are collected and normalizedin an appropriate manner, artifacts can be introduced intothe data from a number of sources. Pilot studies can beutilized to screen data for these types of artifacts, toensure that they are either eliminated or properlyaccounted for.
7. Recommendations and questions for futureresearch
7.1. Muscle selection and electrode placement
Electrode location is particularly critical in the cervi-cal region because of the overlapping organization of themusculature. This should be explicitly described in themethods section of any paper in which electromyogra-phy is used, regardless of the muscles studied, though ina few of the papers examined for this review locationdescriptions were quite vague. Given that limited accesssites seem to exist for sampling deeper muscles,additional studies are needed to more fully explore inner-vation zones and crosstalk in those and other muscles ofthe neck. Such studies will help to determine whether
electrode sites, particularly in the posterior region, canbe considered muscle-specific, or must be consideredonly location-specific.
7.1.1. Posterior musclesResearch has shown that semispinalis capitis is a pri-
mary head/neck extensor and that splenius capitis con-tributes to extension, and ipsilateral rotation and bend-ing. As such, both are important to study. However,access to both is limited, based on small areas that maybe accessible via surface electrodes in some subjects, thepotential presence of innervation zones in those samesmall areas in some subjects, and the presence ofimmediately adjacent muscles which may have differentfunctions from semispinalis or splenius and may intro-duce misleading crosstalk into the signal. Therefore, ourrecommendation is to place electrodes over the sitesspecified in either Keshner et al. [35], MayouxBenhamou et al. [44], or Queisser et al. [54], but to con-sider those location-specific sites, rather than muscle-specific. Additionally, those sites may not be appropriateif head/neck postures are non-neutral. Activity from theupper trapezius should also be sampled, since it is sensi-tive to shoulder load, and may affect activity from otherposterior cervical sites; sternocleidomastoid should alsobe sampled for crosstalk influence.
7.1.2. Anterior musclesSternocleidomastoid and levator scapulae are both
accessible with surface electrodes. Levator scapulae isactive during extension and ipsilateral rotation, and alsoreflects differences in some head/neck/trunk postures.Electrodes should be located based on careful palpation,as surface access to the muscle is limited. Sternocleido-mastoid contributes to flexion, rotation, and lateral bend,and has been shown to be responsive to changes inhead/neck posture, at least during quiet tasks. Electrodelocations from muscle midpoint to as high as C2 havebeen proposed. Higher placement of the electrodes isadvisable if head movement is to occur, due to less rela-tive movement between skin (and therefore surfaceelectrodes) and muscles. Research is needed to definethe limits of head rotation and lateral bend within whichelectrodes will still cover the muscles. Both muscles aresusceptible to artifact from ECG, hard swallowing, andsniffling, so data should be screened prior to analysis.
7.2. Reliability, normalization, and data reduction
Few researchers have published results regardingreliability of their data. There would seem to be muchto be gained from exploring this area, including improv-ing the understanding of costs to collecting data on mul-tiple days, and methods for reducing those costs, includ-ing various normalization procedures.
Only a few studies have specifically addressed metho-

395C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
dological questions surrounding normalization pro-cedures for the neck musculature, which also involvesexploring the EMG–torque/force relationship. Whendata are normalized in applied studies, it is with respectto a single posture — the importance of the change inmuscle length does not seem to have been fully charac-terized. Restrictions on lateral bending and rotation havenot been addressed. In most studies, normalization hasbeen demonstrated to improve reliability, and is rec-ommended by experts in the use of electromyography.Normalization is recommended in order to discuss datafrom a group of subjects. Otherwise, the degree of varia-bility in the data is likely to mask condition effects. Themethod of normalization, from exertion description todata processing, should be explicitly described in themethods section of any paper in which electromyogra-phy is used. Although head/neck posture has been shownto have some effect on sEMG and moment capability,no normalization method which accounts for varioushead/neck postures has come into wide-spread accept-ance. Until this occurs, our recommendation is for nor-malization based on the widely-used method of Schu¨ldt[58], assuming subjects will work in a fairly neutral pos-ture. If subjects are to work in a non-neutral posture, thatposture should be used for collecting maximums. Formultiple working postures, revert to the method ofSchuldt [58], unless the study will be able to account forvariation introduced by maximums in multiple postures.Maximum exertions should be practiced prior to datacollection, and three maximums should be collected,with at least 2 min of rest in between. Subjects shouldbe restrained and should exert against fixed objectsrather than manual resistance, to ensure their safety andthat exertions are isometric.
7.2.1. Precautions regarding maximum exertionsAlthough none of the studies in this review reported
adverse events or quantified specific risks associatedwith performance of maximum exertions with the headand neck, the potential would seem to exist, particularlyif subjects and equipment are not properly secured, or ifsubjects have certain medical conditions. The risk poten-tial deserves consideration in subject exclusion criteriaand design of studies involving maximal, near maximal,or prolonged isometric cervical muscle contractions. Atleast three broad categories of theoretical risk with pro-longed maximal muscular exertions of the trunk, andperhaps of the cervical muscles, would seem to be: (1)musculoskeletal strain injuries, or perhaps aggravationof underlying conditions such as cervical spondylosis;(2) unfavorable cardiac or circulatory occurrences [53],such as extreme blood pressure elevation or disturbancein cranial blood flow; and (3) other conditions that couldbe aggravated by postural changes or strain, such as sev-ere, recurrent vertigo or cephalgia.
Studies of cervical muscle strength in healthy popu-
lations were not found to contain information thatexplicitly addressed risk or precautionary measures[45,88], with the exception of Staudte and Du¨hr [70].Subjects between 14 and 84 years performed maximumisometric neck extensions in a neutral prone position,and prone with head rotated 45° in either direction.Exclusion criteria were “trauma, previous surgery of(cervical spine), major impairment of the range ofmotion, neural segmental signs, cephalgia and/or vertigo,pain” [70].
Safety was a primary issue for Highland et al. [27],in evaluating a program to improve strength and rangeof motion in the cervical spines of patients with non-spinal cord injuries to that region. No patients (70 —cervical strain, 14 — herniated disc, 6 — degenerateddisc) were injured during the 8-week program, eventhough they were asked to move through full ranges offlexion and extension, and were asked to producedflexion and extension exertions at 100% MVC. Theauthors attributed their ability to do this safely by con-ducting four orientation sessions with each subject priorto the start of the program, and to the testing devicewhich allowed the researchers to restrain patients andfully support the weight of their heads in extension.Fatigue testing of patients with osteoarthritis (OA) of thecervical spine, was conducted by Gogia and Sabbahi[18]. Patients performed isometric flexion and extensionexertions at 100% MVC while restrained in a neutralupright posture. Safety was not explicitly discussed, butexclusion criteria included patients who had had “OA ofthe cervical spine for more than 6 months, … cervicalspine surgery, neurologic symptoms, acute painful epi-sodes, or second diagnosis of rheumatoid arthritis”.
In conclusion, the literature suggests that maximalcervical exertions can be performed safely, provided theprotocol includes appropriate precautions that addresssubjects, equipment, and methods. Depending on theduration and intensity of cervical muscle contraction,certain prudent exclusionary considerations for subjectsmay include, but may not be limited to: (1) existence ofcurrent cervically-related diagnoses or symptoms unlessthey are elements of the experimental hypothesis; (2)history of dizziness, fainting, symptomatic irregularheartbeat, or severe headache aggravated by straining;(3) diagnosis, symptoms, or very high risk of carotid orcoronary artery disease; (4) current diagnosis of poorlyor marginally-controlled high blood pressure; or (5) sev-ere limitations in pulmonary function capacity. Regard-ing performance of exertions, subjects and equipmentshould be restrained in such a way as to preclude anyunexpected or unintended motion, and a limited numberof maximum exertions should be performed in order toreduce the risk of severe muscle fatigue. Additionally,standard precautionary principles should be followed,including advising subjects to discontinue testing at anypoint, such as for unusual severe pain or discomfort.

396 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
7.3. Concluding remarks
Surface electromyography from muscle-specific(sternocleidomastoid) and location-specific sites (oversplenius capitis and semispinalis capitis) in the cervicalregion has been shown to be sensitive to changes insemi-static occupational tasks and workstation design(most often in well-controlled studies and in which EMGsignals were normalized to maximum exertions). How-ever, several methodological issues should be developedfurther in order to improve interpretation of muscleactivity from this area of the body. Those issues includecrosstalk (for example: which electrode locations aresusceptible and under what circumstances; what specificsteps can be taken to reduce or account for crosstalk inthis region), location of innervation zones (for example:for the commonly used sites in the cervical region, inwhat percentage of subjects do electrode sites coincidewith innervation zones; development of specific methodsthat can be generally adopted to screen for presence ofinnervation zones), normalization (for example: whenshould multiple postures be tested; should reference con-tractions be maximum or submaximum), and reliability(applies to all previous questions). These questions arenot necessarily unique to sEMG applied at the neck [14].Improved understanding of these issues could lead tomethodological standardization, which would improveconfidence in use of sEMG to estimate neck muscleloads, and facilitate comparisons of results between stud-ies. An additional area that requires further work isdeveloping the relationship between sEMG and esti-mates of muscle tension or joint torque, which appearsweak at this point, particularly, it seems, where very sim-ple biomechanical models have been used. This may bean indication that simple models will not suffice for thecervical region. EMG-driven models that link muscleactivity with high fidelity biomechanical models may berequired to explain muscle activation patterns and pro-duce plausible estimates of muscle tension, when work-ing in a complex, multi-joint, multi-muscle region suchas the neck.
Looking into the future, electromyography may cometo be commonly augmented by the use of imaging tech-niques to aid in the placement of surface electrodes[44,55]. In addition, because of their capability to show(evidence of) activity in surface and deep muscles non-invasively and without crosstalk, electromyographymight eventually be replaced, in at least some instances,by the use of imaging techniques (MRI [11] or ultra-sound [55]).
Acknowledgements
The authors wish to thank Dr Chris Jensen of theNational Institute of Occupational Health in Copenhagen
Denmark, for his thoughtful review of the manuscript.Many of his suggestions were incorporated into the finalversion of the document. Thanks are also extended toDr David Rempel and Dr Moshe Solomonow for provid-ing the opportunity for a formal examination of the useof surface electromyography in the neck and upperextremities in workplace design research.
References
[1] Andersen JH, Gaardboe O. Prevalence of persistent neck andupper limb pain in a historical cohort of sewing machine oper-ators. Am J Ind Med 1993;24:677–87.
[2] Bansevicius D, Westgaard RH, Jensen C. Mental stress of longduration: EMG activity, perceived tension, fatigue, and paindevelopment in pain-free subjects. Headache 1997;37:499–510.
[3] Basmajian JV, De Luca CJ. Muscles alive, their functionsrevealed by electromyography. 5th ed. Baltimore: Williams &Wilkins, 1985.
[4] Bauer W, Wittig T. Influence of screen and copy holder positionson head posture, muscle activity and user judgement. Appl Ergon1998;29:185–92.
[5] Bernard B, Sauter S, Fine L, Petersen M, Hales T. Job task andpsychosocial risk factors for work-related musculoskeletal dis-orders among newspaper employees. Scand J Work EnvironHealth 1994;20:417–26.
[6] Bernhardt P, Wilke H-J, Wenger KH, Jungkunz B, Bo¨hm A,Claes LE. Multiple muscle force simulation in axial rotation ofthe cervical spine. Clin Biomech 1999;14:32–40.
[7] Bork BE, Cook TM, Rosecrance JC, Engelhardt KA, ThomasonME, Wauford IJ, Worley RK. Work-related musculoskeletal dis-orders among physical therapists. Phys Ther 1996;76:827–35.
[8] Cailliet R. Neck and arm pain. 3rd ed. Philadelphia: F.A. DavisCompany, 1991.
[9] Choi H, Vanderby R Jr.. Comparison of biomechanical humanneck models: muscle forces and spinal loads at C4/5 level. J ApplBiomech 1999;15:120–38.
[10] Christensen H, Søgaard K, Jensen BR, Finsen L, Sjøgaard G.Intramuscular and surface EMG power spectrum from dynamicand static contractions. J Electromyogr Kinesiol 1995;5:27–36.
[11] Conley MS, Meyer RA, Bloomberg JJ, Feeback DL, Dudley GA.Noninvasive analysis of human neck muscle function. Spine1995;20:2505–12.
[12] Cram JR, Kasman GS, Holtz J. Introduction to surface electromy-ography. Gaithersburg, MD: Aspen Publishers, Inc., 1998.
[13] Davis J. Manual of surface electromyography. Dayton, OH:Wright Air Development Center, Wright Patterson Air ForceBase, TR 59–184, 1959.
[14] De Luca C. The use of surface electromyography in biomechan-ics. J Appl Biomech 1997;13:135–63.
[15] Finsen L. Biomechanical analyses of occupational work loads inthe neck and shoulder. PhD thesis, National Institute of Occu-pational Health, Copenhagen, 1995.
[16] Finsen L. Biomechanical aspects of occupational neck posturesduring dental work. IJIE 1999;23:397–406.
[17] Finsen L, Christensen H, Bakke M. Musculoskeletal disordersamong dentists and variation in dental work. Appl Ergon1998;29:119–25.
[18] Gogia P, Sabbahi M. Electromyographic analysis of neck musclefatigue in patients with osteoarthritis of the cervical spine. Spine1994;19:502–6.
[19] Goldstein IB. Role of muscle tension in personality theory. Psy-chol Bull 1964;61:413–25.
[20] Grieco A, Molteni G, De Vito G, Sias N. Epidemiology of mus-
397C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
culoskeletal disorders due to biomechanical overload. Ergonom-ics 1998;41:1253–60.
[21] Hagberg M, Silverstein B, Wells R, Smith MJ, Hendrick HW,Carayon P, Perusse M. In: Kourinka I, Forcier L, editors. Workrelated musculoskeletal disorders (WMSDs): a reference book forprevention. London: Taylor & Francis, 1995.
[22] Hagberg M, Wegman DH. Prevalence rates and odds ratios ofshoulder–neck diseases in different occupational groups. Br J IndMed 1987;44:602–10.
[23] Hamilton N. Source document position as it affects head positionand neck muscle tension. Ergonomics 1996;39:593–610.
[24] Harms-Ringdahl K, Ekholm J. Intensity and character of pain andmuscular activity levels elicited by maintained extreme flexionposition of the lower-cervical-upper-thoracic spine. Scand JRehabil Med 1986;18:117–26.
[25] Harms-Ringdahl K, Ekholm J, Schu¨ldt K, Nemeth G, ArboreliusUP. Load moments and myoelectric activity when the cervicalspine is held in full flexion and extension. Ergonomics1986;29:1539–52.
[26] Hautekiet M, Hermans V, Spaepen A, Snijders K. The influencesof the height of the VDU screen, and the position of the backrest on the neck muscle load and the position of the head. In:Proc. IEA; Tampere, Finland, 1997.
[27] Highland T, Dreisinger T, Vie L, Russell G. Changes in isometricstrength and range of motion of the idolated cervical spine aftereight weeks of clinical rehabiliation. Spine 1992;17:S77–82.
[28] Jensen C, Borg V, Finsen L, Hansen K, Juul-Kristensen B, Chris-tensen H. Job demands, muscle acitivity and musculoskeletalsymptoms in relation to work with the computer mouse. ScandJ Work Environ Health 1998;24:418–24.
[29] Jensen C, Vasseljen O, Westgaard RH. The influence of electrodeposition on bipolar surface electromyogram recordings of theupper trapezius muscle. Eur J Appl Physiol 1993;67:266–73.
[30] Jensen C, Vasseljen O, Westgaard RH. Estimating maximal EMGamplitude for the trapezius muscle: on the optimization of experi-mental procedure and electrode placement for improvedreliability and increased signal amplitude. J Electromyogr Kine-siol 1996;6:51–8.
[31] Johnson G, Bogduk N, Nowitzke A, House D. Anatomy andactions of the trapezius muscle. Clin Biomech 1994;9:44–50.
[32] Jonsson B. Kinesiology, with special reference to electromyo-graphic kinesiology. In: Cobb WA, Van Duijn H, editors. Con-temporary clinical neurophysiology. Amsterdam: Elsevier Scien-tific Publishing Co., 1978:417–28.
[33] Josephson M, Lagerstrom M, Hagberg M, Wigaeus Hjelm E.Musculoskeletal symptoms and job strain among nursing person-nel: a study over a three year period. Occup Environ Med1997;54:681–5.
[34] Kamibayashi L, Richmond F. Morphometry of human neckmuscles. Spine 1998;23:1314–23.
[35] Keshner E, Campbell D, Katz R, Peterson B. Neck muscle acti-vation patterns in humans during isometric stabilization. ExpBrain Res 1989;75:335–44.
[36] Knave BG, Wibom RI, Voss M, Hedstrom LD, Bergqvist UO.Work with video display terminals among office employees. I.Subjective symptoms and discomfort. Scand J Work EnvironHealth 1985;11:457–66.
[37] Kumar S. A computer desk for bifocal lens wearers, with specialemphasis on selected telecommunication tasks. Ergonomics1994;37:1669–78.
[38] Kumar S, Scaife WGS. A precision task, posture, and strain. JSafety Res 1979;11:28–36.
[39] Lannersten L, Harms-Ringdahl K. Neck and shoulder muscleactivity during work with different cash register systems. Ergo-nomics 1990;33:49–65.
[40] Lie I, Watten RG. Oculomotor factors in the aetiology of occu-
pational cervicobrachial diseases (OCD). Eur J Appl Physiol1987;56:151–6.
[41] Lindman R, Hagberg M, Angqvist K, Soderlund K, Hultman E,Thornell L. Changes in muscle morphology in chronic trapeziusmyalgia. Scand J Work Environ Health 1991;17:347–55.
[42] Mathiassen S, Winkel J, Ha¨gg G. Normalization of surface EMGamplitude from the upper trapezius muscle in ergonomic stud-ies — a review. J Electromyogr Kinesiol 1995;5:197–226.
[43] Mathiassen SE, Winkel J. Electromyographic activity in theshoulder–neck region according to arm position and glenohu-meral torque. Eur J Appl Physiol 1990;61:370–9.
[44] Mayoux Benhamou MA, Revel M, Vallee C. Surface electrodesare not appropriate to record selective myoelectric activity ofsplenius capitis muscle in humans. Exp Brain Res1995;105:432–8.
[45] Mayoux-Benhamou MA, Revel M. Influence of head position ondorsal neck muscle efficiency. Electromyogr Clin Neurophysiol1993;33:161–6.
[46] Meyer JJ, Berk RJ, Anderson AV. Recruitment patterns in thecervical paraspinal muscles during cervical forward flexion: evi-dence of cervical flexion-relaxation. Electromyogr Clin Neuro-physiol 1993;33:217–23.
[47] Milerad E, Ekenvall L. Symptoms of the neck and upperextremities in dentists. Scand J Work Environ Health1990;16:129–34.
[48] Mirka GA. The quantification of EMG normalization error. Ergo-nomics 1991;34:343–52.
[49] Moroney SP, Schultz AB, Miller JAA. Analysis and measure-ment of neck loads. J Orthop Res 1988;6:713–20.
[50] Nolan JP, Sherk HH. Biomechanical evaluation of the extensormusculature of the cervical spine. Spine 1988;13:9–11.
[51] Oberg T, Oberg U. Musculoskeletal complaints in dental hygiene:a survey study from a Swedish county. J Dent Hyg1993;67:257–61.
[52] Ormeno G, Miralles R, Santander H, Casassus R, Ferrer P, Pal-azzi C, Moya H. Body position effects on sternocleidomastoidand masseter EMG pattern activity in patients undergoingocclusal splint therapy. Cranio 1997;15:300–9.
[53] Phillips CA, Petrofsky JS. Cardiovascular responses to isometricneck muscle contractions: results after dynamic exercise withvarious headgear loading configurations. Aviat Space EnvironMed 1984;55:740–5.
[54] Queisser F, Blu¨thner R, Bra¨uer D, Seidel H. The relationshipbetween the electromyogram-amplitude and isometric extensiontorques of neck muscles at different positions of the cervicalspine. Eur J Appl Physiol 1994;68:92–101.
[55] Rezasoltani A, Kallinen M, Malkia E, Vihko V. Neck semispin-alis capitis muscle size in sitting and prone positions measuredby real-time ultrasonography. Clin Rehabil 1998;12:36–44.
[56] Saito S, Miyao M, Kondo T, Sakakibara H, Toyoshima H.Ergonomic evaluation of working posture of VDT operationusing personal computer with flat panel display. Ind Health1997;35:264–70.
[57] Sakakibara H, Miyao M, Kondo T, Yamada S. Overhead workand shoulder–neck pain in orchard farmers harvesting pears andapples. Ergonomics 1995;38:700–6.
[58] Schuldt K. On neck muscle activity and load reduction in sittingpostures. An electromyographic and biomechanical study withapplications in ergonomics and rehabilitation. Scand J RehabilMed Suppl 1988;19:1–49.
[59] Schuldt K, Ekholm J, Harms-Ringdahl K, Arborelius UP, Ne´methG. Influence of sitting postures on neck and shoulder e.m.g. dur-ing arm–hand work movements. Clin Biomech 1987;2:126–39.
[60] Schuldt K, Ekholm J, Harms-Ringdahl K, Nemeth G, ArboreliusUP. Effects of changes in sitting work posture on static neck andshoulder muscle activity. Ergonomics 1986;29:1525–37.
[61] Schuldt K, Ekholm J, Harms-Ringdahl K, Ne´meth G, Arborelius
398 C.M. Sommerich et al. / Journal of Electromyography and Kinesiology 10 (2000) 377–398
UP. Effects of arm support or suspension on neck and shouldermuscle activity during sedentary work. Scand J Rehabil Med1987;19:77–84.
[62] Schuldt K, Harms-Ringdahl K. Activity levels during isometrictest contractions of neck and shoulder muscles. Scand J RehabilMed 1988;20:117–27.
[63] Schuldt K, Harms-Ringdahl K. Cervical spine position versuse.m.g activity in neck muscles during maximum isometric neckextension. Clin Biomech 1988;3:129–36.
[64] Schuldt K, Harms-Ringdahl K. E.m.g./moment relationships inneck muscles during isometric cervical spine extension. ClinBiomech 1988;3:58–65.
[65] Schultz AB, Andersson GBJ. Analysis of loads on the lumbarspine. Spine 1981;6:76–82.
[66] Scutter S, Turker KS, Hall R. Headaches and neck pain in far-mers. Aust J Rural Health 1997;5:2–5.
[67] Serratos-Perez JN, Mendiola-Anda C. Musculoskeletal disordersamong male sewing machine operators in shoemaking. Ergonom-ics 1993;36:793–800.
[68] Sjøgaard G, Kiens B, Jo¨rgensen K, Saltin B. Intramuscular press-ure. EMG and blood flow during low-level prolonged static con-traction in man. Acta Physiol Scand 1986;128:475–84.
[69] Sommerich CM, Joines SMB, Psihogios JP. Effects of VDTviewing angle on user biomechanics, comfort, and preference. In:Proc. The Human Factors and Ergonomics Society 42nd AnnualMeeting; Chicago, 1998:861–5.
[70] Staudte H-W, Du¨hr N. Age- and sex-dependent force-relatedfunction of the cervical spine. Eur Spine J 1994;3:155–61.
[71] Stock SR. Workplace ergonomic factors and the development ofmusculoskeletal disorders of the neck and upper limbs: a meta-analysis. Am J Ind Med 1991;19:87–107.
[72] Sundelin G, Hagberg M. The effects of different pause types onneck and shoulder EMG activity during VDU work. Ergonomics1989;32:527–37.
[73] Takebe K, Vitti M, Basmajian J. The functions of semispinaliscapitis and splenius capitis muscles: an electromyographic study.Anat Rec 1974;179:477–80.
[74] Turville KL, Psihogios JP, Ulmer TR, Mirka GA. The effects ofvideo display terminal height on the operator: a comparison ofthe 15 degree and 40 degree recommendations. Appl Ergon1998;29:239–46.
[75] Vasavada A, Li S, Delp S. Influence of muscle morphometry andmoment arms on the moment-generating capacity of human neckmuscles. Spine 1998;23:412–21.
[76] Veiersted KB. The reproducibility of test contractions for cali-bration of electromyographic measurements. Eur J Appl Physiol1991;62:91–8.
[77] Veiersted KB. Reliability of myoelectric trapezius muscle activityin repetitive light work. Ergonomics 1996;39:797–807.
[78] Viikari-Juntura ER. The scientific basis for making guidelinesand standards to prevent work-related musculoskeletal disorders.Ergonomics 1997;40:1097–117.
[79] Villanueva MB, Jonai H, Saito S. Ergonomic aspects of portablepersonal computers with flat panel displays (PC-FPDs): evalu-ation of posture, muscle activities, discomfort and performance.Ind Health 1998;36:282–9.
[80] Villanueva MB, Jonai H, Sotoyama M, Hisanaga N, Takeuchi Y,Saito S. Sitting posture and neck and shoulder muscle activitiesat different screen height settings of the visual display terminal.Ind Health 1997;35:330–6.
[81] Vitti M, Fujiwara M, Basmajian JV, Iida M. The integrated rolesof longus colli and sternocleidomastoid muscles: an electromyo-graphic study. Anat Rec 1973;177:471–84.
[82] Wærsted M, Westgaard RH. Attention-related muscle activity indifferent body regions during VDU work with minimal physicalactivity. Ergonomics 1996;39:661–76.
[83] Wells R, Norman R, Shannon H, Cole D, Woo H, Bao S.Exposure measurement in the upper limbs of VDT operatorsusing electromyography: reliability within and between days. In:Proc. PREMUS, 1998.
[84] Wells R, Norman R, Shannon H, Cole D, Woo H, Bao S.Exposure measurement in the upper limbs of VDT operatorsusing electromyography: responsiveness to different tasks. In:Proc. PREMUS, 1998.
[85] Westgaard RH, Bjorklund R. Generation of muscle tensionadditional to postural muscle load. Ergonomics 1987;30:911–23.
[86] Yamshon LJ, Bierman W. Kinesiologic electromyography II. Thetrapezius. Arch Phys Med Rehabil 1948;29:647–51.
[87] Yang JF, Winter DA. Electromyography reliability in maximaland submaximal isometric contractions. Arch Phys Med Rehabil1983;64:417–20.
[88] Ylinen JJ, Rezasoltani A, Julin MV, Virtapohjz HA, Ma¨lkia EA.Reproducibility of isometric strength: measurement of neckmuscles. Clin Biomech 1999;14:217–9.
[89] Zipp P. Recommendations for the standardization of lead pos-itions in surface electromyography. Eur J Appl Physiol1982;50:41–54.