
Subthalamic deep brain stimulation modulates small fiber–dependent sensory thresholds in...
7
Subthalamic deep brain stimulation modulates small fiber–dependent sensory thresholds in Parkinson’s disease Daniel Ciampi de Andrade a,b,c,⇑ , Jean-Pascal Lefaucheur d,e , Ricardo Galhardoni a,b , Karine S.L. Ferreira a,b , Anderson Rodrigues Brandão Paiva c , Edson Bor-Seng-Shu c , Luciana Alvarenga a , Martin L. Myczkowski a,f , Marco Antonio Marcolin a,f , Silvia R.D.T. de Siqueira a , Erich Fonoff a , Egberto Reis Barbosa c , Manoel Jacobsen Teixeira a,c a Pain Center, Department of Neurology, School of Medicine, University of São Paulo, São Paulo, Brazil b Pain Center, Instituto do Câncer do Estado de São Paulo, São Paulo, Brazil c Neurology Division, Hospital das Clínicas, School of Medicine, University of São Paulo, São Paulo, Brazil d EA 4391, Faculté de Médecine, Université Paris Est Créteil, Créteil, France e Service de Physiologie – Explorations Fonctionnelles, Hôpital Henri Mondor, Assistance Publique – Hôpitaux de Paris, Créteil, France f Transcranial Magnetic Stimulation Laboratories, Psychiatry Institute, University of São Paulo, São Paulo, Brazil Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article. article info Article history: Received 16 August 2011 Received in revised form 16 January 2012 Accepted 14 February 2012 Keywords: Chronic pain Parkinson’s disease Deep brain stimulation Sensory thresholds Subthalamic nucleus abstract The effects of deep brain stimulation of the subthalamic nucleus on nonmotor symptoms of Parkinson’s disease (PD) rarely have been investigated. Among these, sensory disturbances, including chronic pain (CP), are frequent in these patients. The aim of this study was to evaluate the changes induced by deep brain stimulation in the perception of sensory stimuli, either noxious or innocuous, mediated by small or large nerve fibers. Sensory detection and pain thresholds were assessed in 25 PD patients all in the off- medication condition with the stimulator turned on or off (on- and off-stimulation conditions, respec- tively). The relationship between the changes induced by surgery on quantitative sensory testing, spon- taneous CP, and motor abilities were studied. Quantitative sensory test results obtained in PD patients were compared with those of age-matched healthy subjects. Chronic pain was present in 72% of patients before vs 36% after surgery (P = .019). Compared with healthy subjects, PD patients had an increased sen- sitivity to innocuous thermal stimuli and mechanical pain, but a reduced sensitivity to innocuous mechanical stimuli. In addition, they had an increased pain rating when painful thermal stimuli were applied, particularly in the off-stimulation condition. In the on-stimulation condition, there was an increased sensitivity to innocuous thermal stimuli but a reduced sensitivity to mechanical or thermal pain. Pain provoked by thermal stimuli was reduced when the stimulator was turned on. Motor improve- ment positively correlated with changes in warm detection and heat pain thresholds. Subthalamic nucleus deep brain stimulation contributes to relieve pain associated with PD and specifically modulates small fiber–mediated sensations. Ó 2012 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved. 1. Introduction Parkinson’s disease (PD) classically has been viewed as a disease mainly affecting the motor system. However, nonmotor symptoms (NMS) such as depression, pain, sexual problems, bowel inconti- nence, and sleep disorders are present in a large majority of PD patients, and their importance has been increasingly recognized in recent years [3,15,33]. NMS are thought to be present from the early stages of the disease and may be related to extension of Lewy pathology to the nondopaminergic neuronal pathway [38]. Chronic pain (CP) is one of the most frequent NMS, and it was found that 62% of a cohort of 450 PD patients had CP [20,27]. Mechanisms involved in pain symptoms and their relation to nigrostriatal dopa- minergic insufficiency and motor impairment are still poorly understood [7,16]. Deep brain stimulation (DBS) has gained general use in the management of refractory dyskinesias and motor fluctuations in PD patients [8,18]. The subthalamic nucleus (STN) is one of the main targets of DBS, and its chronic stimulation can significantly 0304-3959/$36.00 Ó 2012 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.pain.2012.02.016 ⇑ Corresponding author. Address: Divisão de Clínica Neurológica do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, Secretaria de Neurologia, Instituto Central, Av. Dr. Enéas de Carvalho Aguiar, 255, 5.o andar, sala 5084, Cerqueira César 05403-900, São Paulo, SP, Brazil. Tel.: +55 11 97 75 35 38; fax: +55 11 36 70 27 12. E-mail address: [email protected] (D. Ciampi de Andrade). PAIN Ò 153 (2012) 1107–1113 www.elsevier.com/locate/pain
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Subthalamic deep brain stimulation modulates small fiber–dependent sensory thresholds in...

PAIN�
153 (2012) 1107–1113
w w w . e l s e v i e r . c o m / l o c a t e / p a i n
Subthalamic deep brain stimulation modulates small fiber–dependent sensorythresholds in Parkinson’s disease
Daniel Ciampi de Andrade a,b,c,⇑, Jean-Pascal Lefaucheur d,e, Ricardo Galhardoni a,b, Karine S.L. Ferreira a,b,Anderson Rodrigues Brandão Paiva c, Edson Bor-Seng-Shu c, Luciana Alvarenga a, Martin L. Myczkowski a,f,Marco Antonio Marcolin a,f, Silvia R.D.T. de Siqueira a, Erich Fonoff a, Egberto Reis Barbosa c,Manoel Jacobsen Teixeira a,c
a Pain Center, Department of Neurology, School of Medicine, University of São Paulo, São Paulo, Brazilb Pain Center, Instituto do Câncer do Estado de São Paulo, São Paulo, Brazilc Neurology Division, Hospital das Clínicas, School of Medicine, University of São Paulo, São Paulo, Brazild EA 4391, Faculté de Médecine, Université Paris Est Créteil, Créteil, Francee Service de Physiologie – Explorations Fonctionnelles, Hôpital Henri Mondor, Assistance Publique – Hôpitaux de Paris, Créteil, Francef Transcranial Magnetic Stimulation Laboratories, Psychiatry Institute, University of São Paulo, São Paulo, Brazil
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
a r t i c l e i n f o a b s t r a c t
Article history:Received 16 August 2011Received in revised form 16 January 2012Accepted 14 February 2012
Keywords:Chronic painParkinson’s diseaseDeep brain stimulationSensory thresholdsSubthalamic nucleus
0304-3959/$36.00 � 2012 International Associationhttp://dx.doi.org/10.1016/j.pain.2012.02.016
⇑ Corresponding author. Address: Divisão de ClínicaClínicas da Faculdade de Medicina da UniversidadeNeurologia, Instituto Central, Av. Dr. Enéas de Carvalh5084, Cerqueira César 05403-900, São Paulo, SP, Brazfax: +55 11 36 70 27 12.
E-mail address: [email protected] (D. Ciampi de Andr
The effects of deep brain stimulation of the subthalamic nucleus on nonmotor symptoms of Parkinson’sdisease (PD) rarely have been investigated. Among these, sensory disturbances, including chronic pain(CP), are frequent in these patients. The aim of this study was to evaluate the changes induced by deepbrain stimulation in the perception of sensory stimuli, either noxious or innocuous, mediated by small orlarge nerve fibers. Sensory detection and pain thresholds were assessed in 25 PD patients all in the off-medication condition with the stimulator turned on or off (on- and off-stimulation conditions, respec-tively). The relationship between the changes induced by surgery on quantitative sensory testing, spon-taneous CP, and motor abilities were studied. Quantitative sensory test results obtained in PD patientswere compared with those of age-matched healthy subjects. Chronic pain was present in 72% of patientsbefore vs 36% after surgery (P = .019). Compared with healthy subjects, PD patients had an increased sen-sitivity to innocuous thermal stimuli and mechanical pain, but a reduced sensitivity to innocuousmechanical stimuli. In addition, they had an increased pain rating when painful thermal stimuli wereapplied, particularly in the off-stimulation condition. In the on-stimulation condition, there was anincreased sensitivity to innocuous thermal stimuli but a reduced sensitivity to mechanical or thermalpain. Pain provoked by thermal stimuli was reduced when the stimulator was turned on. Motor improve-ment positively correlated with changes in warm detection and heat pain thresholds. Subthalamicnucleus deep brain stimulation contributes to relieve pain associated with PD and specifically modulatessmall fiber–mediated sensations.
� 2012 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
1. Introduction patients, and their importance has been increasingly recognized
Parkinson’s disease (PD) classically has been viewed as a diseasemainly affecting the motor system. However, nonmotor symptoms(NMS) such as depression, pain, sexual problems, bowel inconti-nence, and sleep disorders are present in a large majority of PD
for the Study of Pain. Published by
Neurológica do Hospital dasde São Paulo, Secretaria de
o Aguiar, 255, 5.o andar, salail. Tel.: +55 11 97 75 35 38;
ade).
in recent years [3,15,33]. NMS are thought to be present from theearly stages of the disease and may be related to extension of Lewypathology to the nondopaminergic neuronal pathway [38]. Chronicpain (CP) is one of the most frequent NMS, and it was found that62% of a cohort of 450 PD patients had CP [20,27]. Mechanismsinvolved in pain symptoms and their relation to nigrostriatal dopa-minergic insufficiency and motor impairment are still poorlyunderstood [7,16].
Deep brain stimulation (DBS) has gained general use in themanagement of refractory dyskinesias and motor fluctuations inPD patients [8,18]. The subthalamic nucleus (STN) is one of themain targets of DBS, and its chronic stimulation can significantly
Elsevier B.V. All rights reserved.

1108 D. Ciampi de Andrade et al. / PAIN�
153 (2012) 1107–1113
reduce motor symptoms. However, the impact of DBS on NMS hasbeen less often investigated. Two studies have shown that STN-DBS could produce significant pain relief in more than 80% of PDpatients, independently from motor effect [17,37]. Despite theseresults, the mechanisms implicated in the possible analgesic effectof STN-DBS remain speculative. The aim of our study was to eval-uate the changes in painful and nonpainful sensory thresholdsbrought about by STN-DBS in PD patients. We evaluated both largeand small fiber–mediated sensory thresholds using a comprehen-sive battery of quantitative sensory testing (QST) in on-stimulationvs off-stimulation conditions. In addition, we studied the relation-ship between sensory changes and the improvement in motorsymptoms and CP under STN-DBS.
2. Methods
Thirty patients with idiopathic PD according to the UKPD Soci-ety Brain Bank [6] treated by STN-DBS (Medtronic 3389 Minneap-olis, MN) due to refractory motor fluctuations were enrolled. Thestudy was approved by our institution ethic review board. All pa-tients signed an informed consent form. All patients were treatedby STN-DBS for more than 1 year before study entry, and STN-DBS stimulation parameters were considered to be optimized bythe time of the evaluation. Patients with cognitive decline (as as-sessed by Mini-Mental State Examination (MMSE) score <25), ma-jor depression according to Diagnostic and Statistical Manual ofMental Disorders IV criteria, or a previous history or risk factor forpolyneuropathy (e.g., diabetes mellitus, alcohol abuse, vitamindeficiency) were excluded. Patients who could not properly per-form the tests in the off medication–off stimulation conditiondue to PD severity were discarded from the analysis.
2.1. Clinical evaluation and CP assessment
Duration of the disease and STN-DBS treatment before evalua-tion, motor scores of the Unified Parkinson’s Disease Rating Score(UPDRS-III scores) in on- and off-medication conditions 3 monthsbefore surgery, daily L-dopa equivalent dose at the time of thestudy, and the presence of CP (before and after surgery under reg-ular treatment) were recorded. The presence of pain and its char-acteristics after surgery were assessed by the following tools:
1. Brazilian Portuguese version (B-PV) of the short McGill PainQuestionnaire, including sensory and affective subscores [22].
2. B-PV of the Brief Pain Inventory (BPI), including BPI–pain sever-ity index in the last 24 hours, current CP intensity (BPI–actualpain), and interference (BPI–interference) [12].
3. B-PV of the Douleur Neuropathique-4 and Neuropathic PainSymptom Inventory [4,30].
4. B-PV of the Hospital Anxiety and Depression Scale (HAD),including anxiety and depression subscores [36].
2.2. Experimental design
Dopaminergic medication was withdrawn overnight (at least12 hours) before the evaluation, which included 2 sessions. First,UPDRS-III and QST assessments were performed in on-stimulation,off-medication (on-stim) condition. Second, after the DBS systemwas switched off for 1 hour, UPDRS-III and QST assessments wereperformed in off-stimulation, off-medication (off-stim) condition.A neurologist experienced in PD and blinded to sensory symptomsand QST results performed all UPDRS-III scorings. The presence ofCP before and after surgery was assessed on the day of the exper-iment. Patients presenting CP at present were asked to fill in painquestionnaires and scales.
2.3. QST procedure
All participants went through a QST battery intended to assesslarge fiber (Ab) and small fiber (Ad and C)–mediated somatic sen-sory inputs, including experimental pain (EP) measurements usingsuprathreshold stimuli. Tests were performed at both hands, overthe thenar eminence for thermal testing, and over the dorsum ofthe hand for mechanical thresholds. Mechanical detection thresh-olds (MDT) and mechanical pain thresholds (MPT) were measuredusing calibrated von Frey hairs ranging from 0.008 to 300 g (NC17775, Bioseb, France) [10]. We defined MPT as the lowest pres-sure that was considered painful by the patient. Vibratory andthermal thresholds were measured using a VSA-3000/TSA-2001device (Medoc, Ramat Yshai, Israel). Vibration detection threshold(VDT) was measured at a constant frequency (100 Hz) and increas-ing amplitude (0.1 to 130 lm). The method of limits was used, thepatients being instructed to press a button when they perceivedthe beginning of vibratory sensation. For thermal detection thresh-olds (warm detection threshold [WDT], cold detection threshold[CDT]), the forced-choice method was used to avoid bias due toincreased motor reaction time related to PD. A contact thermode(20 � 35 mm) was applied to the thenar eminence at a neutraltemperature of 32�C. Temperature was increased or decreased ata rate of 1�C/s to 35�C (WDT) or 29�C (CDT). After each trial, pa-tients had 5 seconds to answer yes or no according to the perceivedsensation: ‘‘yes’’ answers caused the system to decrease the tem-perature difference to 1 �C, and then to 0.3 �C subsequently,whereas ‘‘no’’ answers meant for further increases in temperaturedifferences. This protocol also included dummy stimulations, con-sisting of trials during which there was no temperature changefrom baseline. The final threshold was considered after 3 consecu-tive correct answers. Heat and cold pain thresholds (HPT, CPT)were assessed by the methods of limits. Cooling and heating wereproduced at a linear rate of 1�C/s from a starting neutral tempera-ture of 32�C. Interstimulus intervals were 6 to 8 seconds for detec-tion thresholds, 15 to 20 seconds for heat pain thresholds, and 20to 30 seconds for cold pain thresholds. The thermode was gentlymoved around the test area after each stimulation. Temperaturesdid not exceed 50�C for heat and 0 �C for cold to avoid tissue dam-age. The average of 3 trials was computed. All thermal thresholdswere expressed as absolute temperature values. Suprathresholdheat stimulations (SuH) were also performed, with temperatureincreasing at a linear rate of 2�C/s from a starting neutral temper-ature of 32�C and kept constant for 2 seconds at 2 different targettemperatures (46�C and 48�C, in random order). EP intensity wasscored on a (0 to 100 mm) visual analogue scale (VAS). Infrathresh-old cold stimulations (InC) were performed by decreasing temper-ature from 32�C to 10�C and 5�C. The 2 VAS scores obtained duringSuH (46�C and 48�C) on the one hand, and during InC (10�C and5�C) on the other hand, were separately averaged to obtain a singlevalue of SuH and InC [26].
2.4. Healthy subjects and test-retest reproducibility
The QST results of PD patients were compared with those of 35age-matched healthy subjects. Healthy subjects also underwent 2consecutive QST batteries separated by 1 hour to assess test-retestchanges in QST measurements.
2.5. Statistical analyses
Descriptive statistics were used in the clinical characterizationof the sample. Because the Kolmogorov-Smirnov test revealed thatQST values did not have a normal distribution, we studied theeffect of STN-DBS (on-off vs off-off conditions) in PD patients andtest-retest in healthy subjects using the Wilcoxon signed rank test.
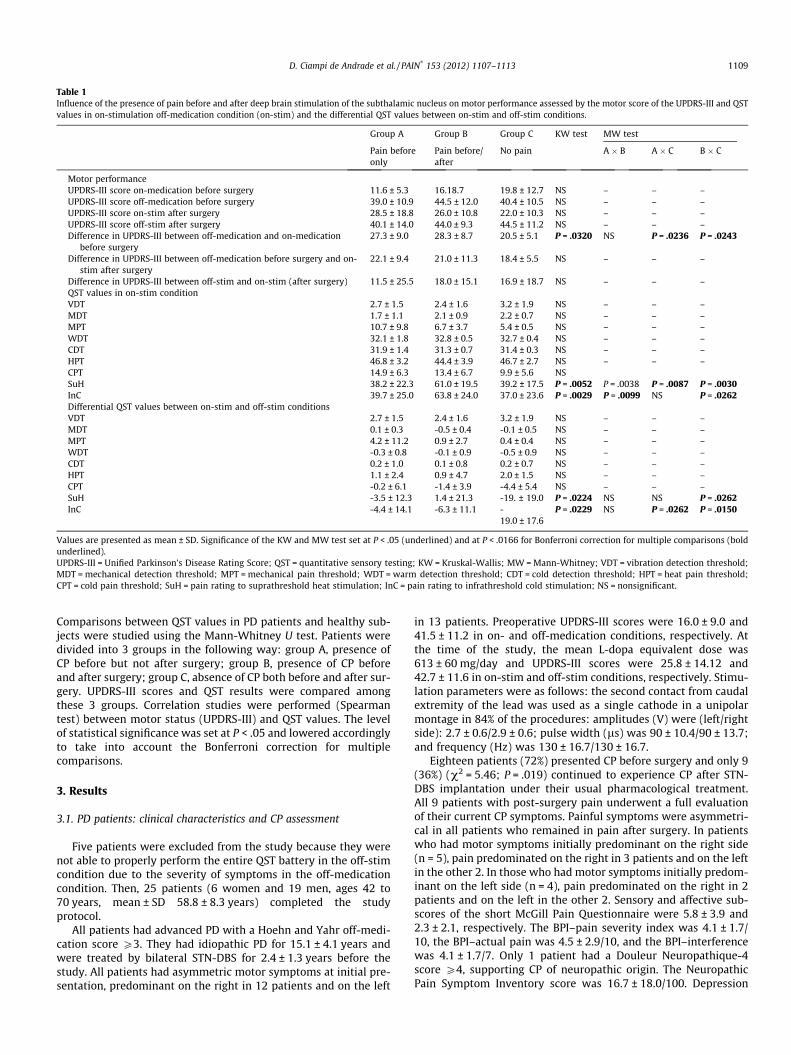
Table 1Influence of the presence of pain before and after deep brain stimulation of the subthalamic nucleus on motor performance assessed by the motor score of the UPDRS-III and QSTvalues in on-stimulation off-medication condition (on-stim) and the differential QST values between on-stim and off-stim conditions.
Group A Group B Group C KW test MW test
Pain beforeonly
Pain before/after
No pain A � B A � C B � C
Motor performanceUPDRS-III score on-medication before surgery 11.6 ± 5.3 16.18.7 19.8 ± 12.7 NS – – –UPDRS-III score off-medication before surgery 39.0 ± 10.9 44.5 ± 12.0 40.4 ± 10.5 NS – – –UPDRS-III score on-stim after surgery 28.5 ± 18.8 26.0 ± 10.8 22.0 ± 10.3 NS – – –UPDRS-III score off-stim after surgery 40.1 ± 14.0 44.0 ± 9.3 44.5 ± 11.2 NS – – –Difference in UPDRS-III between off-medication and on-medication
before surgery27.3 ± 9.0 28.3 ± 8.7 20.5 ± 5.1 P = .0320 NS P = .0236 P = .0243
Difference in UPDRS-III between off-medication before surgery and on-stim after surgery
22.1 ± 9.4 21.0 ± 11.3 18.4 ± 5.5 NS – – –
Difference in UPDRS-III between off-stim and on-stim (after surgery) 11.5 ± 25.5 18.0 ± 15.1 16.9 ± 18.7 NS – – –QST values in on-stim conditionVDT 2.7 ± 1.5 2.4 ± 1.6 3.2 ± 1.9 NS – – –MDT 1.7 ± 1.1 2.1 ± 0.9 2.2 ± 0.7 NS – – –MPT 10.7 ± 9.8 6.7 ± 3.7 5.4 ± 0.5 NS – – –WDT 32.1 ± 1.8 32.8 ± 0.5 32.7 ± 0.4 NS – – –CDT 31.9 ± 1.4 31.3 ± 0.7 31.4 ± 0.3 NS – – –HPT 46.8 ± 3.2 44.4 ± 3.9 46.7 ± 2.7 NS – – –CPT 14.9 ± 6.3 13.4 ± 6.7 9.9 ± 5.6 NSSuH 38.2 ± 22.3 61.0 ± 19.5 39.2 ± 17.5 P = .0052 P = .0038 P = .0087 P = .0030InC 39.7 ± 25.0 63.8 ± 24.0 37.0 ± 23.6 P = .0029 P = .0099 NS P = .0262Differential QST values between on-stim and off-stim conditionsVDT 2.7 ± 1.5 2.4 ± 1.6 3.2 ± 1.9 NS – – –MDT 0.1 ± 0.3 -0.5 ± 0.4 -0.1 ± 0.5 NS – – –MPT 4.2 ± 11.2 0.9 ± 2.7 0.4 ± 0.4 NS – – –WDT -0.3 ± 0.8 -0.1 ± 0.9 -0.5 ± 0.9 NS – – –CDT 0.2 ± 1.0 0.1 ± 0.8 0.2 ± 0.7 NS – – –HPT 1.1 ± 2.4 0.9 ± 4.7 2.0 ± 1.5 NS – – –CPT -0.2 ± 6.1 -1.4 ± 3.9 -4.4 ± 5.4 NS – – –SuH -3.5 ± 12.3 1.4 ± 21.3 -19. ± 19.0 P = .0224 NS NS P = .0262InC -4.4 ± 14.1 -6.3 ± 11.1 -
19.0 ± 17.6P = .0229 NS P = .0262 P = .0150
Values are presented as mean ± SD. Significance of the KW and MW test set at P < .05 (underlined) and at P < .0166 for Bonferroni correction for multiple comparisons (boldunderlined).UPDRS-III = Unified Parkinson’s Disease Rating Score; QST = quantitative sensory testing; KW = Kruskal-Wallis; MW = Mann-Whitney; VDT = vibration detection threshold;MDT = mechanical detection threshold; MPT = mechanical pain threshold; WDT = warm detection threshold; CDT = cold detection threshold; HPT = heat pain threshold;CPT = cold pain threshold; SuH = pain rating to suprathreshold heat stimulation; InC = pain rating to infrathreshold cold stimulation; NS = nonsignificant.
D. Ciampi de Andrade et al. / PAIN�
153 (2012) 1107–1113 1109
Comparisons between QST values in PD patients and healthy sub-jects were studied using the Mann-Whitney U test. Patients weredivided into 3 groups in the following way: group A, presence ofCP before but not after surgery; group B, presence of CP beforeand after surgery; group C, absence of CP both before and after sur-gery. UPDRS-III scores and QST results were compared amongthese 3 groups. Correlation studies were performed (Spearmantest) between motor status (UPDRS-III) and QST values. The levelof statistical significance was set at P < .05 and lowered accordinglyto take into account the Bonferroni correction for multiplecomparisons.
3. Results
3.1. PD patients: clinical characteristics and CP assessment
Five patients were excluded from the study because they werenot able to properly perform the entire QST battery in the off-stimcondition due to the severity of symptoms in the off-medicationcondition. Then, 25 patients (6 women and 19 men, ages 42 to70 years, mean ± SD 58.8 ± 8.3 years) completed the studyprotocol.
All patients had advanced PD with a Hoehn and Yahr off-medi-cation score P3. They had idiopathic PD for 15.1 ± 4.1 years andwere treated by bilateral STN-DBS for 2.4 ± 1.3 years before thestudy. All patients had asymmetric motor symptoms at initial pre-sentation, predominant on the right in 12 patients and on the left
in 13 patients. Preoperative UPDRS-III scores were 16.0 ± 9.0 and41.5 ± 11.2 in on- and off-medication conditions, respectively. Atthe time of the study, the mean L-dopa equivalent dose was613 ± 60 mg/day and UPDRS-III scores were 25.8 ± 14.12 and42.7 ± 11.6 in on-stim and off-stim conditions, respectively. Stimu-lation parameters were as follows: the second contact from caudalextremity of the lead was used as a single cathode in a unipolarmontage in 84% of the procedures: amplitudes (V) were (left/rightside): 2.7 ± 0.6/2.9 ± 0.6; pulse width (ls) was 90 ± 10.4/90 ± 13.7;and frequency (Hz) was 130 ± 16.7/130 ± 16.7.
Eighteen patients (72%) presented CP before surgery and only 9(36%) (v2 = 5.46; P = .019) continued to experience CP after STN-DBS implantation under their usual pharmacological treatment.All 9 patients with post-surgery pain underwent a full evaluationof their current CP symptoms. Painful symptoms were asymmetri-cal in all patients who remained in pain after surgery. In patientswho had motor symptoms initially predominant on the right side(n = 5), pain predominated on the right in 3 patients and on the leftin the other 2. In those who had motor symptoms initially predom-inant on the left side (n = 4), pain predominated on the right in 2patients and on the left in the other 2. Sensory and affective sub-scores of the short McGill Pain Questionnaire were 5.8 ± 3.9 and2.3 ± 2.1, respectively. The BPI–pain severity index was 4.1 ± 1.7/10, the BPI–actual pain was 4.5 ± 2.9/10, and the BPI–interferencewas 4.1 ± 1.7/7. Only 1 patient had a Douleur Neuropathique-4score P4, supporting CP of neuropathic origin. The NeuropathicPain Symptom Inventory score was 16.7 ± 18.0/100. Depression

Table 2Quantitative sensory testing in patients with PD in off-medication condition with subthalamic nucleus stimulation switched on (on-off) or off (off-off).
PD patients off-off PD patients on-off Healthy subjects off-off vs controls, P values* on-off vs controls, P values* off-off vs on-off, P values�
VDT (lm) 2.7 ± 1.7 2.7 ± 1.6 1.4 ± 0.6 <.0001 <.0001 .9049
MDT (g) 2.0 ± 1.1 2.0 ± 0.9 0.9 ± 1.1 <.0001 <.0001 .9261
MPT (g) 5.8 ± 3.2 7.8 ± 6.6 13.3 ± 7.0 <.0001 .0002 <.0001WDT (�C) 32.8 ± 1.2 32.5 ± 1.1 35.3 ± 3.2 .001 <.0001 .0065CDT (�C) 31.3 ± 1.0 31.5 ± 1.0 27.9 ± 4.2 <.0001 <.0001 .0290HPT (�C) 44.6 ± 3.7 45.9 ± 3.5 45.7 ± 2.9 .0719 .4258 .0070CPT (�C) 14.8 ± 5.6 13.0 ± 6.4 11.5 ± 7.2 .0067 .4565 .0063SuH (/100) 53.0 ± 24.4 46.7 ± 22.4 35.7 ± 26.4 .0014 .0328 .0233InC (/100) 56.8 ± 29.8 47.6 ± 26.8 32.9 ± 25.4 .0002 .0058 .0001
Significance set at P < .05 (underlined) and at P < .0055 for Bonferroni correction for multiple comparisons (bold underlined).PD = Parkinson’s disease; VDT = vibration detection threshold; MDT = mechanical detection threshold; MPT = mechanical pain threshold; WDT = warm detection threshold;CDT = cold detection threshold; HPT = heat pain threshold; CPT = cold pain threshold; SuH = pain rating to suprathreshold heat stimulation; InC = pain rating to infrathresholdcold stimulation.* Mann-Whitney U test.� Wilcoxon Signed Rank Test.
Table 3Literature data on the influence of subthalamic nucleus stimulation on quantitative sensory testing in patients with Parkinson’s disease under deep brain stimulation of thesubthalamic nucleus and comparisons with healthy subjects.
Sensitivity to:
Innocuous mechanicalstimuli
Mechanicalpain
Electricalpain
Innocuous warmstimuli
Heat pain Innocuous coldstimuli
Cold pain
In on-stim conditionGierthmühlen et al. Unchanged Unchanged Increased Unchanged Increased IncreasedSpielberger et al. Unchanged Unchanged Unchanged UnchangedMaruo et al. Increased Unchanged Increased UnchangedThis study Unchanged Decreased Increased Decreased Increased Decreased
Compared with healthy subjectsDjaldetti et al. Unchanged Unchanged Increased Unchanged IncreasedSchestatsky et al. Unchanged IncreasedMylius et al. [25] Increased IncreasedZambito Marsala
et al.Increased
Nolano et al. Decreased Decreased Decreased Decreased Decreased UnchangedVela et al. UnchangedMylius et al. [25] Increased DecreasedThis study Decreased Increased Increased Unchanged or
increasedIncreased Increased
1110 D. Ciampi de Andrade et al. / PAIN�
153 (2012) 1107–1113
and anxiety subscores of the HAD were 6.5 ± 3.6 and 7.2 ± 4.1,respectively. CP was diffuse in 1 patient, located in the upper limbsin 2 and in the lower limbs in 3, and was axial in 3 patients.According to the usual classification of PD-associated pain syn-dromes [1], we found musculoskeletal CP in 6 patients (osteoar-thritis n = 2; low back pain n = 4) and dystonic CP in 3 patients.None had radicular or central neuropathic. Duration of diseasewas not significantly different in the 3 groups of patients. Interest-ingly, patients without CP before or after surgery (group C) pre-sented lower motor improvement in the preoperative L-dopacharge test (on-medication–off-medication UPDRS-III score differ-ence before surgery) than patients with CP (A and B) (Table 1).
3.2. QST results
3.2.1. On-stim vs off-stimBecause no threshold significantly differed between the right
and left hands or between the most or least symptomatic side inPD patients or in healthy subjects (all P > .20, Wilcoxon test),results obtained from both hands were pooled before analysis.
All QST values are presented in Table 2. The detection of largefiber–mediated sensations (MDT, VDT) did not change in PDpatients between on-stim and off-stim conditions. In contrast, PDpatients had a reduced sensitivity to mechanical pain (MPT
increase) and to thermal pain (HPT increase and CPT decrease) inthe on-stim condition, but they showed a higher sensitivity todetect innocuous thermal sensations (WDT decrease and CDTincrease). Finally, VAS scores rating EP in SuH and InC were re-duced when the stimulator was turned on. Only MPT increaseand the reduced EP ratings in InC were significant after Bonferronicorrection. Interestingly, patients who still had CP after surgery(group B) showed higher EP ratings for noxious thermal stimula-tion than patients without CP after surgery (groups A and C). Onthe other hand, patients without CP before or after surgery (groupC) presented the greatest modulation of thermal EP in the on-stimvs off-stim condition (Table 1).
3.2.2. Test-retest reproducibility in healthy subjectsNo thresholds significantly differed between the first and the
second examinations in healthy subjects, except the CDT, whichwas higher at the first measurement (first vs second measurement31.6 ± 0.2 and 31.5 ± 0.4, respectively; P = .0030). This result showsthat the QST results obtained in PD patients were not biased be-cause of an unbalanced order of examination between on-stimand off-stim conditions. Regarding the CDT increase at the secondtest in PD patients, it cannot also be explained by a test-retest ef-fect, because in contrast to PD patients, it decreased at the secondtest in healthy subjects.

D. Ciampi de Andrade et al. / PAIN�
153 (2012) 1107–1113 1111
3.2.3. Comparisons between PD patients and healthy subjectsIn both on-stim and off-stim conditions, PD patients had higher
MDT, VDT, and CDT and lower MPT and WDT compared withhealthy subjects. These differences were significant after Bonfer-roni correction. HPT did not differ in any condition. CPT was higherin PD patients than in healthy subjects only in the off-stim condi-tion, but this difference did not persist after Bonferroni correction.Finally, VAS scores rating under EP in both SuH and InC were high-er in PD patients than in healthy subjects, but the difference onlypersisted in the off-stim condition after Bonferroni correction(Table 2).
3.3. Correlation analyses
The changes induced by STN-DBS in UPDRS-III scores and QSTvalues correlated to WDT and HPT. The decrease in UPDRS-III scorecorrelated positively with HPT (increased sensitivity to heat pain;rho = 0.504, P = .0012) and negatively to WDT (reduced sensitivityto warm stimuli; rho = 0.370, P = .0152). All other correlations be-tween motor changes in the on-stim condition and QST data, CP,pain questionnaires, and scale scores were negative.
4. Discussion
The primary objective of this study was to investigate the im-pact of STN-DBS on large and small fiber–dependent sensorythresholds in off-medication PD patients. We found that DBS mod-ulated exclusively small fiber–dependent sensory inputs byincreasing the sensitivity to innocuous thermal stimuli and byreducing the sensitivity to mechanical and thermal painful stimuli.Moreover, EP ratings decreased when painful thermal stimuli wereapplied in on-stim vs off-stim condition. Thus, STN-DBS reduced CPin parallel with the improvement of the discrimination of thermalsensation.
Compared with healthy subjects, PD patients had an increasedsensitivity to mechanical pain and innocuous thermal stimuli,but a reduced sensitivity to innocuous mechanical stimuli in bothon-stim and off-stim conditions. In addition, they had an increasedEP to painful thermal stimuli, particularly in the off-stim condition.The fact that PD patients had a better detection of innocuous ther-mal sensation than healthy subjects was an original result and maybe related to improvement in the methodological sensory detec-tion techniques (forced choice) used in this study. These changescould be translated by a net increase in the sensory limen (differ-ence between detection and pain thresholds), indicating that underSTN-DBS only, there was a wider range of stimuli intensities per-ceived as nonpainful when compared with the off-stim condition.In the on-stim condition, sensory thresholds tended to normalizeaccording to the reference values measured in healthy subjects.
4.1. Literature data
The impact of STN-DBS on QST thresholds has been previouslyinvestigated in 3 very recent reports (Table 3) [14,21,34]. Gier-thmühlen et al. [14] found that STN-DBS increased the sensitivityto innocuous thermal stimuli and also to cold pain. In contrast,Spielberger et al. [34] did not observe any influence of STN-DBSon thermal detection or pain thresholds. Finally, Maruo et al. [21]found that STN-DBS increased the sensitivity to innocuous thermalstimuli but not to painful thermal stimuli. In this latter study, com-parisons with healthy subjects were also made: the sensitivity toinnocuous thermal stimuli was reduced in PD patients only inthe off-stim condition, whereas the sensitivity to thermal paindid not differ between subjects and patients. Literature dataregarding QST results in PD compared with healthy subjects are
also summarized in Table 3 [9,10,24,28,31,36,39]. In general, thesestudies were restricted to a few sensory modalities, mostly con-cerning A-o and C conveyed sensory inputs. Detection thresholdsto cold stimuli and pain thresholds to either heat or cold stimuliwere seldom assessed, as well as EP rating to supra-thresholdstimulations.
4.2. Methodological limitations
In the present study, patients underwent a complete chronicpain assessment exclusively in the postoperative period. Thus,information on pain symptoms before surgery was obtained frommedical records and patient information, which could be subjectto assessment and recall bias.
Concerning the comparison of QST results between studies, itshould take into account the heterogeneity in the clinical presenta-tion of PD patients among the studies or in the methods used toperform the test, such as the size of the thermode probe or theway to measure detection thresholds. For instance, a smaller ther-mode surface was used in a previous study [21], which was likelyto yield different results from ours. More importantly, the methodof limits was the one used in virtually all previous studies. It meansthat increased thresholds may be related, at least partially, to anincreased motor reaction time, especially in PD patients in theoff-stim condition. Because patients are asked to press a buttonas soon as they perceive the change in temperature, a delay in mo-tor reaction will cause an increase in the measured threshold unre-lated to sensory detection. Our study was the first to assessthermal detection thresholds by using the method of forced choicein PD patients. In this paradigm, different temperatures are pre-sented to the participant, who has the time to answer and to decidewhether or not the stimuli were perceived, so that motor reactiontime has no influence on the final result. Moreover, dummy stim-ulations, during which no stimulus is presented, were randomlyapplied. This trick is supposed to improve attention paid by pa-tients for the successful completion of the task.
Cognitive dysfunction was not assessed in this study, based onthe third part of the UPDRS, which includes only motor evaluationsand not cognitive ones. The possible influence of cognitive disorderon QST results was limited by the method we used to perform QST,independent of reaction time as aforementioned. However, onecould argue that some PD patients, especially those with persistentCP after surgery, would be more prone to present altered resultscaused by pain-related attention deficit [2] and effects of analgesicdrugs, for example. This is a potential limitation of our study, andfurther studies evaluating the influence of cognitive factors on thedevelopment of pain in PD patients, treated or not by DBS, will de-serve attention.
4.3. General overview on QST changes induced by STN-DBS
STN-DBS is thought to modulate dopaminergic circuitry into thebrain [31]. Its motor effect positively correlates to preoperative L-dopa response, which can predict a good outcome of DBS treat-ment [11]. In the present study, we found that changes in WDTand HPT correlated to motor improvement when the stimulatorwas turned on. Experimental studies showed that dopaminergicpathways are implicated in pain integration and modulation toheat noxious stimulation [5,32,40]. Genetic factors also supportthe association between low dopaminergic activity and high painsensitivity [35].
Other neurotransmitters are involved in PD pathophysiology,such as substance P (SP) in the direct striato-pallidal pathway,enkephalin (Enk) in the indirect striato-pallidal pathway, or GABAin both pathways [19]. Because DBS acts on basal ganglia circuitry,there is a possible role played by these nondopaminergic transmit-

1112 D. Ciampi de Andrade et al. / PAIN�
153 (2012) 1107–1113
ters in the modulation of NMS, such as pain in PD. We showed thatpatients with persisting CP after DBS (group B) had higher VASscores to painful stimuli (EP), whereas patients without pain beforeor after surgery (group C) showed greater reduction of EP intensityin the on-stim condition. One may hypothesize that patients ofgroup B may have a relatively less affected direct pathway, withhigher levels of SP (hyperalgesia), whereas patients of group Ccould have a greater hyperactivity of the indirect pathway, associ-ated with a more intense Enk action (analgesia). This would ac-count for their different motor response to L-dopa and differentEP and CP profiles after DBS. Also, it would explain why patientswithout CP before or after surgery (i.e., high Enk) showed the high-est EP modulation under DBS [23]. This is further corroborated bythe fact that experimental studies showed that DBS reverses somechanges related to nigro-striatal denervation, such as GABA over-expression, whereas it had no effects on other phenomena suchas overexpression of Enk in the indirect or under expression ofSP in the direct pathways [13,29]. This hypothesis needs to betested formally by experimental studies, but could provide new in-sights on the relationship between pain, motor symptoms, andtheir relief after treatment in PD patients.
4.4. Conclusion
This study showed that STN-DBS was associated with asignificant relief of ongoing CP and changes in cutaneous sensorythresholds, mostly thermal innocuous and noxious ones. In partic-ular, the modulation of heat and warm detection was related toDBS-induced motor improvement. These data will add to thegrowing knowledge on the mechanisms of action of STN-DBS onNMS in PD.
Conflict of interest statement
The authors report no conflict of interest.
Acknowledgements
This study was funded by FAPESP (Fundação de Amparo à Pes-quisa do Estado de São Paulo) #2010/19392, and Pain Center Re-search Fund from the Department of Neurology, University of SãoPaulo, São Paulo, Brazil. The authors thank the patients, who haveendured the discomforts of off-medication periods so that wecould better understand their disease condition and treatmentsmade to correct it. The authors also thank Professor Wilson Brottofor logistic help.
References
[1] Beiske AG, Loge JH, Ronningen A, Svensson E. Pain in Parkinson’s disease:prevalence and characteristics. Pain 2009;141:173–7.
[2] Borkum JM. Maladaptive cognitions and chronic pain: epidemiology,neurobiology, and treatment. J Rat-Emo Cognitive-Behav Ther 2010;28:4–24.
[3] Chaudhuri KR, Odin P. The challenge of non-motor symptoms in Parkinson’sdisease. Progr Brain Res 2010;184:325–41.
[4] Ciampi de Andrade D, Ferreira KA, Nishimura CM, Yeng LT, Batista AF, de Sa K,Araujo J, Stump PR, Kaziyama HH, Galhardoni R, Fonoff ET, Ballester G, Zakka T,Bouhassira D, Teixeira MJ. Psychometric validation of the Portuguese versionof the Neuropathic Pain Symptoms Inventory. Health Qual Life Outcomes2011;30:107.
[5] Coffeen U, Lopez-Avila A, Ortega-Legaspi JM, del Angel R, Lopez-Munoz FJ,Pellicer F. Dopamine receptors in the anterior insular cortex modulate long-term nociception in the rat. Eur J Pain 2008;12:535–43.
[6] Daniel SE, Lees AJ. Parkinson’s disease society brain bank, London: overviewand research. J Neural Transm Suppl 1993;39:165–72.
[7] Dellapina E, Gerdelat-Mas A, Ory-Magne F, Pourcel L, Galitzky M, Calvas F,Simonetta-Moreau M, Thalamas C, Payoux P, Brefel-Courbon C. Apomorphineeffect on pain threshold in Parkinson’s disease: a clinical and positron emissiontomography study. Mov Disord 2011;26:153–7.
[8] Deuschl G, Schade-Brittinger C, Krack P, Volkmann J, Schafer H, Botzel K,Daniels C, Deutschlander A, Dillmann U, Eisner W, Gruber D, Hamel W, Herzog
J, Hilker R, Klebe S, Kloss M, Koy J, Krause M, Kupsch A, Lorenz D, Lorenzl S,Mehdorn HM, Moringlane JR, Oertel W, Pinsker MO, Reichmann H, Reuss A,Schneider GH, Schnitzler A, Steude U, Sturm V, Timmermann L, Tronnier V,Trottenberg T, Wojtecki L, Wolf E, Poewe W, Voges J. A randomized trial ofdeep-brain stimulation for Parkinson’s disease. N Engl J Med2006;355:896–908.
[9] Djaldetti R, Shifrin A, Rogowski Z, Sprecher E, Melamed E, Yarnitsky D.Quantitative measurement of pain sensation in patients with Parkinsondisease. Neurology 2004;62:2171–5.
[10] Ducreux D, Attal N, Parker F, Bouhassira D. Mechanisms of central neuropathicpain: a combined psychophysical and fMRI study in syringomyelia. Brain2006;129:963–76.
[11] Feng T, Li W, Lu L, Wang Y, Shi W, Zhang J, Chan P. Acute stepwise challengetest with levodopa in treated patients with parkinsonism. Parkinsonism RelDisord 2009;15:354–8.
[12] Ferreira KA, Teixeira MJ, Mendonza TR, Cleeland CS. Validation of brief paininventory to Brazilian patients with pain. Support Care Cancer2011;19:505–11.
[13] Gerfen CR, McGinty JF, Young 3rd WS. Dopamine differentially regulatesdynorphin, substance P, and enkephalin expression in striatal neurons: in situhybridization histochemical analysis. J Neurosci 1991;11:1016–31.
[14] Gierthmühlen J, Arning P, Binder A, Herzog J, Deuschl G, Wasner G, Baron R.Influence of deep brain stimulation and levodopa on sensory signs inParkinson’s disease. Mov Disord 2010;25:1195–202.
[15] Hanagasi HA, Akat S, Gurvit H, Yazici J, Emre M. Pain is common in Parkinson’sdisease. Clin Neurol Neurosurg 2011;113:11–3.
[16] Juri C, Rodriguez-Oroz M, Obeso JA. The pathophysiological basis of sensorydisturbances in Parkinson’s disease. J Neurol Sci 2010;289:60–5.
[17] Kim HJ, Paek SH, Kim JY, Lee JY, Lim YH, Kim MR, Kim DG, Jeon BS. Chronicsubthalamic deep brain stimulation improves pain in Parkinson disease. JNeurol 2008;255:1889–94.
[18] Krack P, Batir A, Van Blercom N, Chabardes S, Fraix V, Ardouin C, Koudsie A,Limousin PD, Benazzouz A, LeBas JF, Benabid AL, Pollak P. Five-year follow-upof bilateral stimulation of the subthalamic nucleus in advanced Parkinson’sdisease. N Engl J Med 2003;349:1925–34.
[19] Lang AE, Lozano AM. Parkinson’s disease, second of two parts. N Engl J Med1998;15:1130–43.
[20] Letro GH, Quagliato EM, Viana MA. Pain in Parkinson’s disease. ArqNeuropsiquiatr 2009;67:591–4.
[21] Maruo T, Saitoh Y, Hosomi K, Kishima H, Shimokawa T, Hirata M, Goto T,Morris S, Harada Y, Yanagisawa T, Aly MM, Yoshimine T. Deep brainstimulation of the subthalamic nucleus improves temperature sensation inpatients with Parkinson’s disease. Pain 2011;152:860–5.
[22] Melzack R. The McGill Pain Questionnaire: major properties and scoringmethods. Pain 1975;1:277–99.
[23] Millan MJ. Descending control of pain. Progr Neurobiol 2002;66:355–474.[24] Mylius V, Engau I, Teepker M, Stiasny-Kolster K, Schepelmann K, Oertel WH,
Lautenbacher S, Moller JC. Pain sensitivity and descending inhibition of pain inParkinson’s disease. J Neurol Neurosur Psychiatr 2009;80:24–8.
[25] Mylius V, Brebbermann J, Dohmann H, Engau I, Oertel WH, Möller JC. Painsensitivity and clinical progression in Parkinson’s disease. Mov Disord2011;26:2220–5.
[26] Nahmias F, Debes C, de Andrade DC, Mhalla A, Bouhassira D. Diffuse analgesiceffects of unilateral repetitive transcranial magnetic stimulation (rTMS) inhealthy volunteers. Pain 2009;147:224–32.
[27] Negre-Pages L, Regragui W, Bouhassira D, Grandjean H, Rascol O. Chronic painin Parkinson’s disease: the cross-sectional French DoPaMiP survey. Mov Disord2008;23:1361–9.
[28] Nolano M, Provitera V, Estraneo A, Selim MM, Caporaso G, Stancanelli A,Saltalamacchia AM, Lanzillo B, Santoro L. Sensory deficit in Parkinson’sdisease: evidence of a cutaneous denervation. Brain 2008;131:1903–11.
[29] Salin P, Manrique C, Forni C, Kerkerian-Le Goff L. High-frequency stimulationof the subthalamic nucleus selectively reverses dopamine denervation-induced cellular defects in the output structures of the basal ganglia in therat. J Neurosci 2002;22:5137–48.
[30] Santos JG, Brito JO, de Andrade DC, Kaziyama VM, Ferreira KA, Souza I, TeixeiraMJ, Bouhassira D, Baptista AF. Translation to Portuguese and validation of theDouleur Neuropathique 4 questionnaire. J Pain 2010;11:484–90.
[31] Schestatsky P, Kumru H, Valls-Sole J, Valldeoriola F, Marti MJ, Tolosa E, ChavesML. Neurophysiologic study of central pain in patients with Parkinson disease.Neurology 2007;69:2162–9.
[32] Sheng HY, Qu CL, Huo FQ, Du JQ, Tang JS. D2-like but not D1-like dopaminereceptors are involved in the ventrolateral orbital cortex-inducedantinociception: a GABAergic modulation mechanism. Exp Neurol2009;215:128–34.
[33] Simuni T, Sethi K. Nonmotor manifestations of Parkinson’s disease. Ann Neurol2008;64:65–80.
[34] Spielberger S, Wolf E, Kress M, Seppi K, Poewe W. The influence of deep brainstimulation on pain perception in Parkinson’s disease. Mov Disord2011;26:1367–8.
[35] Treister R, Pud D, Ebstein RP, Laiba E, Gershon E, Haddad M, Eisenberg E.Associations between polymorphisms in dopamine neurotransmitter pathwaygenes and pain response in healthy humans. Pain 2009;147:187–93.
[36] Vela L, Lyons KE, Singer C, Lieberman AN. Pain-pressure threshold in patientswith Parkinson’s disease with and without dyskinesia. Parkinsonism RelDisord 2007;13:189–92.

D. Ciampi de Andrade et al. / PAIN�
153 (2012) 1107–1113 1113
[37] Witjas T, Kaphan E, Azulay JP. Non-motor fluctuations in Parkinson’s disease.Rev Neurol 2007;163:846–50.
[38] Wolters E, Braak H. Parkinson’s disease: premotor clinico-pathologicalcorrelations. J Neural Transm Suppl 2006;70:309–19.
[39] Zambito Marsala S, Tinazzi M, Vitaliani R, Recchia S, Fabris F, Marchini C,Fiaschi A, Moretto G, Giometto B, Macerollo A, Defazio G. Spontaneous pain,
pain threshold, and pain tolerance in Parkinson’s disease. J Neurol2011;258:627–33.
[40] Zhu J, Chen Y, Lai J, Dang Y, Yan C, Xu M, Chen T. Dopamine D3 receptorregulates basal but not amphetamine-induced changes in pain sensitivity inmice. Neurosci Lett 2010;477:134–7.




















