Subthalamic nucleus involvement in children: A neuroimaging pattern-recognition approach
8
Review article Subthalamic nucleus involvement in children: A neuroimaging pattern-recognition approach Thangamadhan Bosemani a , Cristina Anghelescu b , Eugen Boltshauser c , Alexander H. Hoon Jr. d,e , Phillip L. Pearl f , Dana Craiu b,g , Michael V. Johnston d,e,h , Thierry A.G.M. Huisman a , Andrea Poretti a,c, * a Section of Pediatric Neuroradiology, Division of Pediatric Radiology, Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins University School of Medicine, Baltimore, MD, USA b Pediatric Neurology Clinic, Alexandru Obregia Hospital, Bucharest, Romania c Department of Pediatric Neurology, University Children’s Hospital, Zurich, Switzerland d Kennedy Krieger Institute, Baltimore, MD, USA e Department of Pediatrics, The Johns Hopkins University School of Medicine, Baltimore, MD, USA f Division of Neurology, Children’s National Medical Center, Washington, DC, USA g Department of Neurology, Pediatric Neurology, Neurosurgery, Psychiatry, “Carol Davila” University of Medicine, Bucharest, Romania h Department of Neurology, The Johns Hopkins University School of Medicine, Baltimore, MD, USA article info Article history: Received 16 April 2013 Received in revised form 17 September 2013 Accepted 30 September 2013 Keywords: Magnetic resonance imaging Pattern-recognition approach Subthalamic nucleus Children abstract A neuroimaging-based pattern-recognition approach has been shown to be very helpful in the diagnosis of a wide range of pediatric central nervous system diseases. Few disorders may selectively affect the subthalamic nucleus in children including Leigh syndrome, succinic semialdehyde dehydrogenase deficiency, kernicterus, chronic end-stage liver failure and near total hypoxic-ischemic injury in the full-term neonates. The consideration of the constellation of clinical history and findings as well as additional neuroimaging findings should allow planning the appropriate diagnostic tests to make the correct diag- nosis in children with involvement of the subthalamic nucleus. ª 2013 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights reserved. Contents 1. Introduction ............................................................................................... 250 2. The subthalamic nucleus (STN) .............................................................................. 250 3. Leigh syndrome ............................................................................................ 251 * Corresponding author. Section of Pediatric Neuroradiology, Division of Pediatric Radiology, The Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins University School of Medicine, Charlotte R. Bloomberg Children’s Center, Sheikh Zayed Tower, Room 4174, 1800 Orleans Street, Baltimore, MD 21287-0842, USA. Tel.: þ1 4109556454; fax: þ1 4105023633. E-mail address: [email protected] (A. Poretti). Official Journal of the European Paediatric Neurology Society european journal of paediatric neurology 18 (2014) 249 e256 1090-3798/$ e see front matter ª 2013 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ejpn.2013.09.010
-
Upload
johnshopkins -
Category
Documents
-
view
3 -
download
0
Transcript of Subthalamic nucleus involvement in children: A neuroimaging pattern-recognition approach

e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6
Official Journal of the European Paediatric Neurology Society
Review article
Subthalamic nucleus involvement in children:A neuroimaging pattern-recognition approach
Thangamadhan Bosemani a, Cristina Anghelescu b, Eugen Boltshauser c,Alexander H. Hoon Jr.d,e, Phillip L. Pearl f, Dana Craiu b,g,Michael V. Johnston d,e,h, Thierry A.G.M. Huisman a, Andrea Poretti a,c,*a Section of Pediatric Neuroradiology, Division of Pediatric Radiology, Russell H. Morgan Department of Radiology
and Radiological Science, The Johns Hopkins University School of Medicine, Baltimore, MD, USAb Pediatric Neurology Clinic, Alexandru Obregia Hospital, Bucharest, RomaniacDepartment of Pediatric Neurology, University Children’s Hospital, Zurich, SwitzerlanddKennedy Krieger Institute, Baltimore, MD, USAeDepartment of Pediatrics, The Johns Hopkins University School of Medicine, Baltimore, MD, USAfDivision of Neurology, Children’s National Medical Center, Washington, DC, USAgDepartment of Neurology, Pediatric Neurology, Neurosurgery, Psychiatry, “Carol Davila” University of Medicine,
Bucharest, RomaniahDepartment of Neurology, The Johns Hopkins University School of Medicine, Baltimore, MD, USA
a r t i c l e i n f o
Article history:
Received 16 April 2013
Received in revised form
17 September 2013
Accepted 30 September 2013
Keywords:
Magnetic resonance imaging
Pattern-recognition approach
Subthalamic nucleus
Children
* Corresponding author. Section of PediatricRadiology and Radiological Science, The JohnZayed Tower, Room 4174, 1800 Orleans Stre
E-mail address: [email protected] (A. Po1090-3798/$ e see front matter ª 2013 Europhttp://dx.doi.org/10.1016/j.ejpn.2013.09.010
a b s t r a c t
A neuroimaging-based pattern-recognition approach has been shown to be very helpful in
the diagnosis of a wide range of pediatric central nervous system diseases. Few disorders
may selectively affect the subthalamic nucleus in children including Leigh syndrome,
succinic semialdehyde dehydrogenase deficiency, kernicterus, chronic end-stage liver
failure and near total hypoxic-ischemic injury in the full-term neonates. The consideration
of the constellation of clinical history and findings as well as additional neuroimaging
findings should allow planning the appropriate diagnostic tests to make the correct diag-
nosis in children with involvement of the subthalamic nucleus.
ª 2013 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights
reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2502. The subthalamic nucleus (STN) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2503. Leigh syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251
Neuroradiology, Division of Pediatric Radiology, The Russell H. Morgan Department ofs Hopkins University School of Medicine, Charlotte R. Bloomberg Children’s Center, Sheikhet, Baltimore, MD 21287-0842, USA. Tel.: þ1 4109556454; fax: þ1 4105023633.retti).ean Paediatric Neurology Society. Published by Elsevier Ltd. All rights reserved.

e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6250
3.1. Leigh syndrome due to COX deficiency with SURF1 mutation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2513.2. Leigh syndrome due to complex I deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251
4. Succinic semialdehyde dehydrogenase deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2535. Kernicterus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2536. Hepatic encephalopathy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2547. Hypoxic-ischemic injury in term neonates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2548. Other diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2559. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
1. Introduction 2. The subthalamic nucleus (STN)
Neuroimaging plays a key role in diagnostic investigations
and classification of diseases in pediatric neurology. The uti-
lization of a neuroimaging-based pattern-recognition
approach was first shown to be beneficial in the diagnosis of
white matter diseases by Marjo van der Knaap and Jaap Valk
in 1991.1 Subsequently, a neuroimaging-based pattern-recog-
nition approach was demonstrated to provide important in-
formation in assessing children with cerebellar atrophy,2
abnormalities of the dentate nucleus3 or intracranial calcifi-
cations.4 This approach enables us to create “neuroimaging
phenotypes”, which are helpful in identifying disease entities
or plan further targeted clinical, laboratory or genetic in-
vestigations to establish the correct diagnosis.
In this paper, we are focusing on the subthalamic nucleus
(STN). Involvement of the STN has been extensively described
in adults with movement disorders, particularly Parkinson
disease and neurosurgery using deep brain stimulation.5 The
role of the STN in children and its involvement in pediatric
neurological disorders, however, has been seldom reported.
After a short introduction about anatomy and function of the
STN in children, we will discuss the neuroimaging findings of
pediatric neurological disorders with involvement of the STN,
which have been selected on the basis of our experience and
with review of the literature using appropriate key words
(magnetic resonance imaging; pattern-recognition approach;
subthalamic nucleus; children).
Fig. 1 e Coronal T2-weighted images in a healthy (A) 9-month-o
located laterally to the hypointense red nucleus andmedially to
of the STN progressively decreases due to increasing iron depo
The STN is an almond shaped structure with a rostrocaudal
length of about 10 mm, situated in the most caudal part of the
diencephalon. The posterior limb of the internal capsule is on
its anterolateral border separating it from the globus pallidus
(GP) laterally; the fields of Forel (H1 andH2) and hypothalamus
(with which the borders are blurred) are on its medial border;
the substantia nigra (SN) is partially inferior andmedial to the
STN; the red nucleus posteromedially, and the zona incerta
and lenticular fasciculus are dorsally (superior and medial)
positioned.6,7
The STN is a key structure in the basal ganglia circuit and
serves as an important relay station within the cortico-
striothalamocortical circuit.7 It projects to both the external
and internal parts of the GP (tractus subthalamicus), to the
reticular part of the SN, striatum, cerebral cortex, substantia
innominata, pedunculopontine nucleus, and mesencephalic
and pontine reticular formation. Pallido-subthalamic con-
nections are well established. The STN receives its main
afferent inputs from the globus pallidus externus (GPe).
These afferents are GABAergic and have an inhibiting effect
on the STN. The efferent axons from the STN are gluta-
matergic and have an excitatory effect on the globus pallidus
internus (GPi).
On conventional MRI, the normal appearance of the STN
changes as myelination progresses in the first years of life. At
term, the normal STN on T1-weighted images is moderately
ld infant and (B) 12.5-year-old child show the STN (arrows)
the hypointense corticospinal tract. Over time, the T2 signal
sition.

Fig. 2 e 3-year-old child with Leigh disease due to COX I deficiency and SURF1 mutation: (A) axial, (B) coronal and (C)
parasagittal T2-weighted images shows T2-hyperintense signal abnormality in the STN (arrows), substantia nigra
(arrowhead in A), putamina (arrowhead in B), GP (asterisk in B) and periaqueductal gray matter (asterisk in A).
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6 251
hyperintense to the adjacent unmyelinated white matter.8
Hyperintensity on T1-weighted imaging is caused by various
factors, primarily the paramagnetic effect and immobilization
of water molecules. The former includes metal ions, melanin,
or free radicals; the latter includes concentrated solutions of
proteins, calcified tissue, and lipids. Additionally, glia forma-
tion or glial reaction may play a role in neonatal STN
hyperintensity.8
The T1-hyperintensity diminishes and disappears over
time and the STN becomes difficult to distinguish from the
surrounding white matter on T1-weighted images. On T2-
weighted images, the normal STN becomes progressively
hypointense due to increasing iron deposition.6 Hypointensity
on T2-weighted images is more prominent at high field
strength because of the increased susceptibility effect of iron
(Fig. 1).
3. Leigh syndrome
Leigh syndrome (LS, OMIM 256000) or subacute necrotizing
encephalomyelopathy represents a heterogeneous group of
neurodegenerative disorders. It is defined by characteristic
symmetric involvement of basal ganglia, midbrain, dentate
nuclei and, occasionally, cerebral white matter.9,10 The
affected infants and children typically present toward the end
of first year of life with muscular hypotonia, failure to thrive,
motor and cognitive regression, ataxia, dystonia, and oph-
thalmoplegia.9 LS is heterogeneous from a clinical, neuro-
imaging and genetic standpoint including mutations in both
mitochondrial and nuclear encoded genes, which code for
proteins of the respiratory chain complexes I, II, III, IV and V,
mitochondrial tRNA, pyruvate dehydrogenase complex and
coenzyme Q10.9,11
The neuroimaging phenotype in LS varies with the un-
derlying genotype. The involvement of the STN has been re-
ported in LS patients with 1) cytochrome c oxidase (COX)
deficiency with SURF1 mutation12,13 and 2) complex I
deficiency.14
3.1. Leigh syndrome due to COX deficiency with SURF1mutation
COX deficiency is the most common cause of LS.15 COX or
complex IV of the respiratory chain is composed of 13 struc-
tural subunits, 3 of which are encoded by mitochondrial DNA
(mtDNA) and the remainder by nuclear DNA (nDNA). Loss-of-
function mutation in one of these nuclear genes, SURF1, is the
most common cause of COX-deficient LS.16
Bilateral STN involvement as T2- and FLAIR-hyperintense
signal abnormality is a very common neuroimaging finding
in COX-deficient LS with underlying SURF1 mutations
(Fig. 2).12,13,17 The common additional neuroimaging findings
in children with COX-deficient LS due to SURF1 mutation
include T1-hypointense and T2- and FLAIR-hyperintense
signal abnormalities in the inferior olivary nuclei and nuclei
of the solitary tracts in the lower brain stem, inferior cere-
bellar peduncles, central tegmental tracts and reticular for-
mation in the dorsal pons and periaqueductal gray matter in
themidbrain.12,13,18,19 Involvement of the substantia nigra, red
nuclei, and dentate nuclei is less common, while the medial
thalami are uncommonly affected.12,13,18,19
3.2. Leigh syndrome due to complex I deficiency
Complex I (NADH: ubiquinone oxidoreductase) is the largest
component of the oxidative phosphorylation system and is
composed of at least 45 subunits, seven of which are encoded
by mtDNA.20 Isolated complex I deficiency is the most com-
mon etiology for respiratory chain defects in children and
accounts for various clinical phenotypes including not only
LS, but also Leber hereditary optic neuropathy (LHON), mito-
chondrial encephalomyopathy, lactic acidosis and stroke-like
episodes (MELAS), and numerous other clinical presentations
combining hypotonia, developmental delay, seizures, cardio-
myopathy, optic atrophy or retinopathy and other organ
involvement.21
Bilateral STN involvement as T2- and FLAIR-hyperintense
signal abnormality is a common finding in complex I
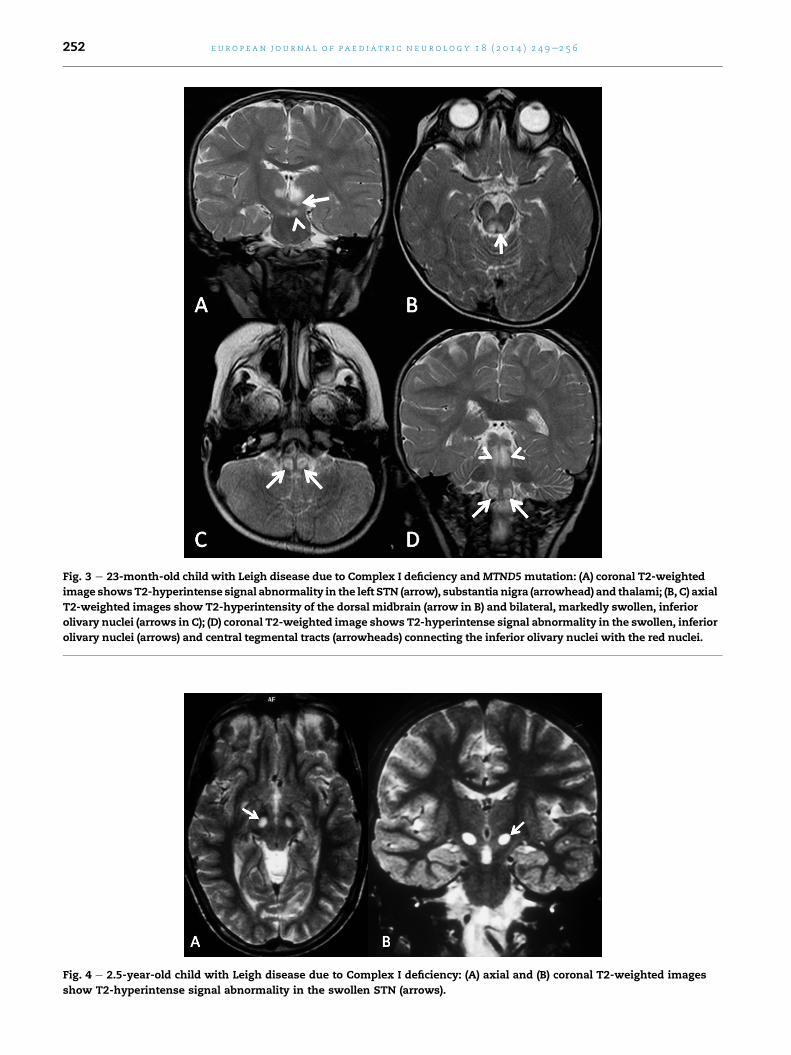
Fig. 3 e 23-month-old child with Leigh disease due to Complex I deficiency and MTND5 mutation: (A) coronal T2-weighted
image showsT2-hyperintense signal abnormality in the left STN (arrow), substantia nigra (arrowhead) and thalami; (B, C) axial
T2-weighted images show T2-hyperintensity of the dorsal midbrain (arrow in B) and bilateral, markedly swollen, inferior
olivary nuclei (arrows in C); (D) coronal T2-weighted image shows T2-hyperintense signal abnormality in the swollen, inferior
olivary nuclei (arrows) and central tegmental tracts (arrowheads) connecting the inferior olivary nuclei with the red nuclei.
Fig. 4 e 2.5-year-old child with Leigh disease due to Complex I deficiency: (A) axial and (B) coronal T2-weighted images
show T2-hyperintense signal abnormality in the swollen STN (arrows).
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6252

Fig. 5 e 10 year-old child with SSADHD: (AeC) Coronal short tau inversion recovery images show bilateral symmetric
homogenous signal abnormalities in the lateral (white arrowheads in A, B) and medial (black arrowheads in A) parts of the
GP, STN (black arrows in B) and dentate nuclei (white arrows in C). (Reprinted with permission from Pearl et al., Neurology
2009; 73:423e9).
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6 253
deficient LS and is more frequently observed in children car-
rying mtDNA than in nuclear mutations (Figs. 3 and 4).12,13,17
In particular, STN involvement was reported in children
with complex I deficiency due to mutations in MTND1,22
MTND3,23 MTND524 and MTND6.25 Additional neuroimaging
findings in complex I deficiency include T1-hypointense and
T2- and FLAIR-hyperintense, symmetric signal abnormalities
in the brain stem affecting the substantia nigra, peri-
aqueductal gray matter, mamillothalamic and spinothalamic
tracts, medial lemniscus andmedial longitudinal fasciculus.14
Signal abnormalities of the putamen, caudate, pallidum, and
dentate nuclei are also frequent.14 A diffuse supratentorial
leukoencephalopathy involving the deep lobar white matter
has been observed only in patients with nDNA mutations,
while cerebellar atrophy and supratentorial stroke-like le-
sions were only observed in complex I deficient patients car-
rying mtDNA mutations.14
4. Succinic semialdehyde dehydrogenasedeficiency
Succinic semialdehyde dehydrogenase deficiency (SSADHD,
OMIM 271980) or 4-hydroxybutyric aciduria is a rare, auto-
somal recessive disease in the degradation pathway of
gamma-amino butyric acid (GABA) due to mutations in the
ALDH5A1 gene.26,27 Childrenwith SSADHD typically present in
the first years of life with mild-moderate intellectual
disability, disproportionate language impairment, hypotonia,
hyporeflexia, autistic behaviors, seizures, and
hallucinations.27
Bilateral, symmetric T2-hyperintense signal abnormality
of the STN is an occasional finding in SSADHD (Fig. 5).28
Neuroimaging findings in SSADHD typically include sym-
metric increased T2-signal in the globi pallidi and dentate
nuclei.27,29 Other occasional neuroimaging findings are T2-
hyperintense signal of the subcortical white matter and
diffuse cerebral and cerebellar atrophy.28
5. Kernicterus
Kernicterus is a pathological term that describes yellow
staining of the deep gray nuclei of the brain due to markedly
increased level and deposition of unconjugated bilirubin in
the neonatal period.30 Brain injury due to hyperbilirubinemia
selectively affects the STN, GP, substantia nigra, hippocam-
pus, and brain stem auditory, vestibular and oculomotor
nuclei.31 Red blood cell hemolysis is the most common etiol-
ogy of hyperbilirubinemia, but several other causes are also
well known.32 Additionally, in the presence of predisposing
factors (e.g. prematurity, sepsis, acidosis), kernicterus may
occur even at a lower level of bilirubin.32
Newborns with acute bilirubin encephalopathy typically
present with poor feeding, lethargy, high-pitched cry, irrita-
bility, seizures and abnormalities of muscular tone such as
hypotonia alternating with hypertonia and opisthotonus.
Clinical findings of chronic bilirubin encephalopathy consist
of dyskinetic movement disorders (athetosis and dystonia),
deafness or hearing loss due to auditory neuropathy, impair-
ments of upward gaze, and enamel hypoplasia of the decid-
uous teeth.30 Athetosis and dystonia most likely result from
disinhibition of the thalamus because destroying the output of
the GP reduces inhibitory input to the motor thalamus.33
In acute neonatal bilirubin encephalopathy, the STN ap-
pears symmetrically hyperintense on T1-weighted images.34
Another key neuroimaging finding is symmetric T1-
hyperintense signal abnormality in the GP.33,34 This may
reflect astroglial cell germinocystic reaction of the acute
event; additionally, edema and bilirubin itself may contribute
in the hyperacute stage.34 The signal intensity of the GP on T2-
weighted images is commonly normal, but may also be
hyperintense in rare cases.33e35 Additionally, T2-hyperintense
and T1-hypointense signal of periventricular and subcortical
white matter has been described.36 Loss of the T1-
hyperintense signal in the GP and STN occurs between the
first and third week after the acute event.34 In the chronic
phase, T2- and FLAIR-hyperintense signal abnormality of the
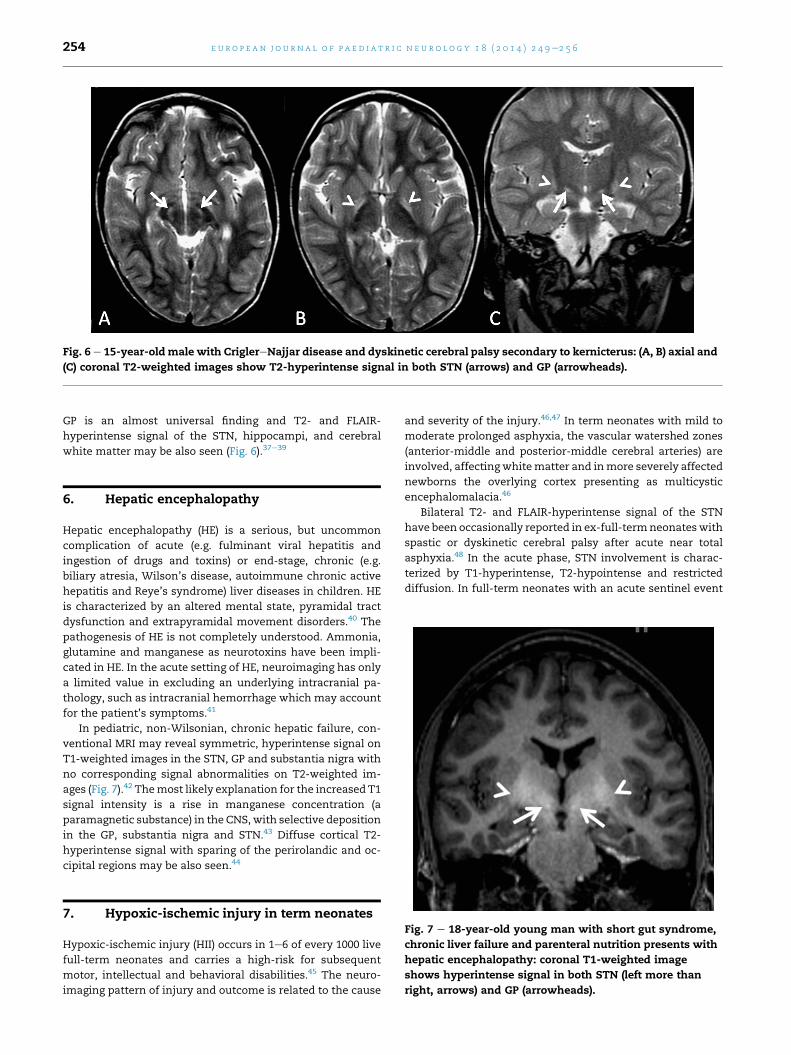
Fig. 6 e 15-year-oldmale with CriglereNajjar disease and dyskinetic cerebral palsy secondary to kernicterus: (A, B) axial and
(C) coronal T2-weighted images show T2-hyperintense signal in both STN (arrows) and GP (arrowheads).
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6254
GP is an almost universal finding and T2- and FLAIR-
hyperintense signal of the STN, hippocampi, and cerebral
white matter may be also seen (Fig. 6).37e39
6. Hepatic encephalopathy
Hepatic encephalopathy (HE) is a serious, but uncommon
complication of acute (e.g. fulminant viral hepatitis and
ingestion of drugs and toxins) or end-stage, chronic (e.g.
biliary atresia, Wilson’s disease, autoimmune chronic active
hepatitis and Reye’s syndrome) liver diseases in children. HE
is characterized by an altered mental state, pyramidal tract
dysfunction and extrapyramidal movement disorders.40 The
pathogenesis of HE is not completely understood. Ammonia,
glutamine and manganese as neurotoxins have been impli-
cated in HE. In the acute setting of HE, neuroimaging has only
a limited value in excluding an underlying intracranial pa-
thology, such as intracranial hemorrhage which may account
for the patient’s symptoms.41
In pediatric, non-Wilsonian, chronic hepatic failure, con-
ventional MRI may reveal symmetric, hyperintense signal on
T1-weighted images in the STN, GP and substantia nigra with
no corresponding signal abnormalities on T2-weighted im-
ages (Fig. 7).42 Themost likely explanation for the increased T1
signal intensity is a rise in manganese concentration (a
paramagnetic substance) in the CNS, with selective deposition
in the GP, substantia nigra and STN.43 Diffuse cortical T2-
hyperintense signal with sparing of the perirolandic and oc-
cipital regions may be also seen.44
Fig. 7 e 18-year-old young man with short gut syndrome,
chronic liver failure and parenteral nutrition presents with
hepatic encephalopathy: coronal T1-weighted image
shows hyperintense signal in both STN (left more than
right, arrows) and GP (arrowheads).
7. Hypoxic-ischemic injury in term neonates
Hypoxic-ischemic injury (HII) occurs in 1e6 of every 1000 live
full-term neonates and carries a high-risk for subsequent
motor, intellectual and behavioral disabilities.45 The neuro-
imaging pattern of injury and outcome is related to the cause
and severity of the injury.46,47 In term neonates with mild to
moderate prolonged asphyxia, the vascular watershed zones
(anterior-middle and posterior-middle cerebral arteries) are
involved, affecting whitematter and inmore severely affected
newborns the overlying cortex presenting as multicystic
encephalomalacia.46
Bilateral T2- and FLAIR-hyperintense signal of the STN
have been occasionally reported in ex-full-termneonateswith
spastic or dyskinetic cerebral palsy after acute near total
asphyxia.48 In the acute phase, STN involvement is charac-
terized by T1-hyperintense, T2-hypointense and restricted
diffusion. In full-term neonates with an acute sentinel event
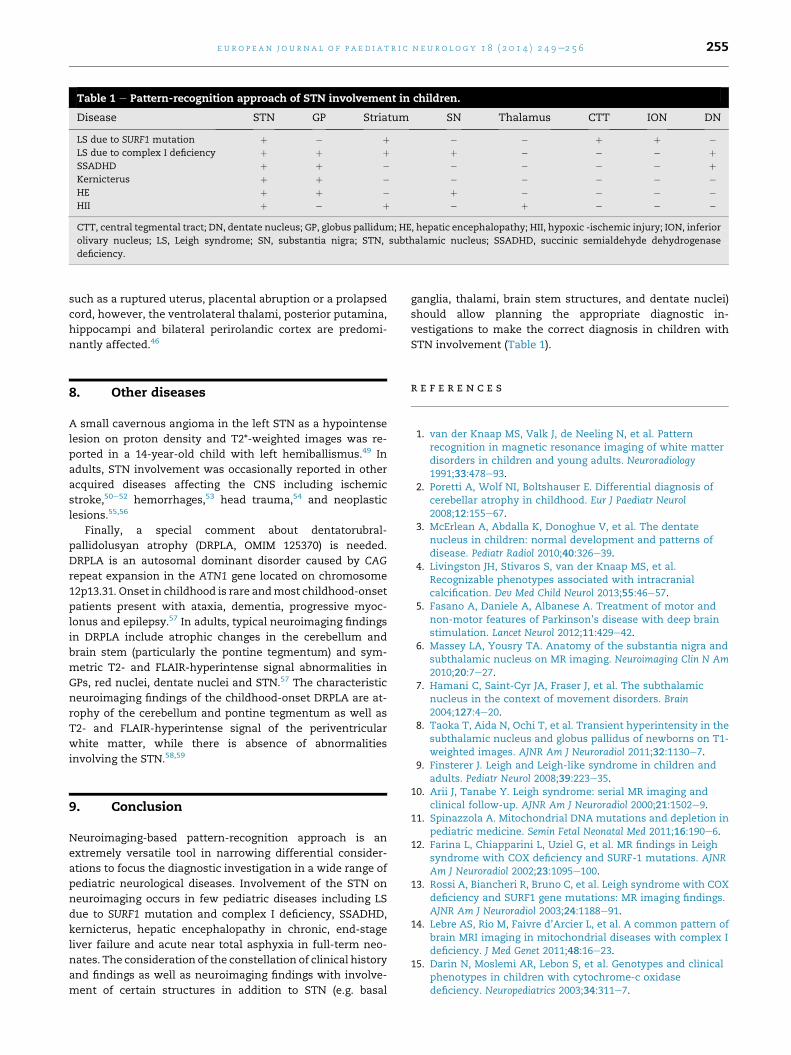
Table 1 e Pattern-recognition approach of STN involvement in children.
Disease STN GP Striatum SN Thalamus CTT ION DN
LS due to SURF1 mutation þ � þ � � þ þ �LS due to complex I deficiency þ þ þ þ � � � þSSADHD þ þ � � � � � þKernicterus þ þ � � � � � �HE þ þ � þ � � � �HII þ � þ � þ � � �
CTT, central tegmental tract; DN, dentate nucleus; GP, globus pallidum; HE, hepatic encephalopathy; HII, hypoxic -ischemic injury; ION, inferior
olivary nucleus; LS, Leigh syndrome; SN, substantia nigra; STN, subthalamic nucleus; SSADHD, succinic semialdehyde dehydrogenase
deficiency.
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6 255
such as a ruptured uterus, placental abruption or a prolapsed
cord, however, the ventrolateral thalami, posterior putamina,
hippocampi and bilateral perirolandic cortex are predomi-
nantly affected.46
8. Other diseases
A small cavernous angioma in the left STN as a hypointense
lesion on proton density and T2*-weighted images was re-
ported in a 14-year-old child with left hemiballismus.49 In
adults, STN involvement was occasionally reported in other
acquired diseases affecting the CNS including ischemic
stroke,50e52 hemorrhages,53 head trauma,54 and neoplastic
lesions.55,56
Finally, a special comment about dentatorubral-
pallidolusyan atrophy (DRPLA, OMIM 125370) is needed.
DRPLA is an autosomal dominant disorder caused by CAG
repeat expansion in the ATN1 gene located on chromosome
12p13.31. Onset in childhood is rare andmost childhood-onset
patients present with ataxia, dementia, progressive myoc-
lonus and epilepsy.57 In adults, typical neuroimaging findings
in DRPLA include atrophic changes in the cerebellum and
brain stem (particularly the pontine tegmentum) and sym-
metric T2- and FLAIR-hyperintense signal abnormalities in
GPs, red nuclei, dentate nuclei and STN.57 The characteristic
neuroimaging findings of the childhood-onset DRPLA are at-
rophy of the cerebellum and pontine tegmentum as well as
T2- and FLAIR-hyperintense signal of the periventricular
white matter, while there is absence of abnormalities
involving the STN.58,59
9. Conclusion
Neuroimaging-based pattern-recognition approach is an
extremely versatile tool in narrowing differential consider-
ations to focus the diagnostic investigation in a wide range of
pediatric neurological diseases. Involvement of the STN on
neuroimaging occurs in few pediatric diseases including LS
due to SURF1 mutation and complex I deficiency, SSADHD,
kernicterus, hepatic encephalopathy in chronic, end-stage
liver failure and acute near total asphyxia in full-term neo-
nates. The consideration of the constellation of clinical history
and findings as well as neuroimaging findings with involve-
ment of certain structures in addition to STN (e.g. basal
ganglia, thalami, brain stem structures, and dentate nuclei)
should allow planning the appropriate diagnostic in-
vestigations to make the correct diagnosis in children with
STN involvement (Table 1).
r e f e r e n c e s
1. van der Knaap MS, Valk J, de Neeling N, et al. Patternrecognition in magnetic resonance imaging of white matterdisorders in children and young adults. Neuroradiology1991;33:478e93.
2. Poretti A, Wolf NI, Boltshauser E. Differential diagnosis ofcerebellar atrophy in childhood. Eur J Paediatr Neurol2008;12:155e67.
3. McErlean A, Abdalla K, Donoghue V, et al. The dentatenucleus in children: normal development and patterns ofdisease. Pediatr Radiol 2010;40:326e39.
4. Livingston JH, Stivaros S, van der Knaap MS, et al.Recognizable phenotypes associated with intracranialcalcification. Dev Med Child Neurol 2013;55:46e57.
5. Fasano A, Daniele A, Albanese A. Treatment of motor andnon-motor features of Parkinson’s disease with deep brainstimulation. Lancet Neurol 2012;11:429e42.
6. Massey LA, Yousry TA. Anatomy of the substantia nigra andsubthalamic nucleus on MR imaging. Neuroimaging Clin N Am2010;20:7e27.
7. Hamani C, Saint-Cyr JA, Fraser J, et al. The subthalamicnucleus in the context of movement disorders. Brain2004;127:4e20.
8. Taoka T, Aida N, Ochi T, et al. Transient hyperintensity in thesubthalamic nucleus and globus pallidus of newborns on T1-weighted images. AJNR Am J Neuroradiol 2011;32:1130e7.
9. Finsterer J. Leigh and Leigh-like syndrome in children andadults. Pediatr Neurol 2008;39:223e35.
10. Arii J, Tanabe Y. Leigh syndrome: serial MR imaging andclinical follow-up. AJNR Am J Neuroradiol 2000;21:1502e9.
11. Spinazzola A. Mitochondrial DNA mutations and depletion inpediatric medicine. Semin Fetal Neonatal Med 2011;16:190e6.
12. Farina L, Chiapparini L, Uziel G, et al. MR findings in Leighsyndrome with COX deficiency and SURF-1 mutations. AJNRAm J Neuroradiol 2002;23:1095e100.
13. Rossi A, Biancheri R, Bruno C, et al. Leigh syndrome with COXdeficiency and SURF1 gene mutations: MR imaging findings.AJNR Am J Neuroradiol 2003;24:1188e91.
14. Lebre AS, Rio M, Faivre d’Arcier L, et al. A common pattern ofbrain MRI imaging in mitochondrial diseases with complex Ideficiency. J Med Genet 2011;48:16e23.
15. Darin N, Moslemi AR, Lebon S, et al. Genotypes and clinicalphenotypes in children with cytochrome-c oxidasedeficiency. Neuropediatrics 2003;34:311e7.

e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 8 ( 2 0 1 4 ) 2 4 9e2 5 6256
16. Tiranti V, Jaksch M, Hofmann S, et al. Loss-of-functionmutations of SURF-1 are specifically associated with Leighsyndrome with cytochrome c oxidase deficiency. Ann Neurol1999;46:161e6.
17. Bruno C, Biancheri R, Garavaglia B, et al. A novel mutation inthe SURF1 gene in a child with Leigh disease, peripheralneuropathy, and cytochrome-c oxidase deficiency. J ChildNeurol 2002;17:233e6.
18. Canafoglia L, Franceschetti S, Antozzi C, et al. Epilepticphenotypes associated with mitochondrial disorders.Neurology 2001;56:1340e6.
19. Salviati L, Freehauf C, Sacconi S, et al. Novel SURF1 mutationin a child with subacute encephalopathy and without theradiological features of Leigh syndrome. Am J Med Genet A2004;128A:195e8.
20. Hoefs SJ, Rodenburg RJ, Smeitink JA, et al. Molecular base ofbiochemical complex Ideficiency.Mitochondrion2012;12:520e32.
21. Fassone E, Rahman S. Complex I deficiency: clinical features,biochemistry and molecular genetics. J Med Genet2012;49:578e90.
22. Moslemi AR, Darin N, Tulinius M, et al. Progressiveencephalopathy and complex I deficiency associated withmutations in MTND1. Neuropediatrics 2008;39:24e8.
23. McFarland R, Kirby DM, Fowler KJ, et al. De novo mutations inthe mitochondrial ND3 gene as a cause of infantilemitochondrial encephalopathy and complex I deficiency. AnnNeurol 2004;55:58e64.
24. Crimi M, Galbiati S, Moroni I, et al. A missense mutation inthe mitochondrial ND5 gene associated with a Leigh-MELASoverlap syndrome. Neurology 2003;60:1857e61.
25. Malfatti E, Bugiani M, Invernizzi F, et al. Novel mutations ofND genes in complex I deficiency associated withmitochondrial encephalopathy. Brain 2007;130:1894e904.
26. Pearl PL, Gibson KM, Quezado Z, et al. Decreased GABA-Abinding on FMZ-PET in succinic semialdehyde dehydrogenasedeficiency. Neurology 2009;73:423e9.
27. Pearl PL, Novotny EJ, Acosta MT, et al. Succinic semialdehydedehydrogenase deficiency in children and adults. Ann Neurol2003;54(Suppl. 6):S73e80.
28. Acosta MT, Munasinghe J, Pearl PL, et al. Cerebellar atrophy inhuman and murine succinic semialdehyde dehydrogenasedeficiency. J Child Neurol 2010;25:1457e61.
29. Ziyeh S, Berlis A, Korinthenberg R, et al. Selectiveinvolvement of the globus pallidus and dentate nucleus insuccinic semialdehyde dehydrogenase deficiency. PediatrRadiol 2002;32:598e600.
30. Shapiro SM, Bhutani VK, Johnson L. Hyperbilirubinemia andkernicterus. Clin Perinatol 2006;33:387e410.
31. Hayashi M, Satoh J, Sakamoto K, et al. Clinical andneuropathological findings in severe athetoid cerebral palsy:a comparative study of globo-Luysian and thalamo-putaminal groups. Brain Dev 1991;13:47e51.
32. Shapiro SM. Chronic bilirubin encephalopathy: diagnosis andoutcome. Semin Fetal Neonatal Med 2010;15:157e63.
33. Johnston MV, Hoon Jr AH. Possible mechanisms in infants forselective basal ganglia damage from asphyxia, kernicterus, ormitochondrial encephalopathies. J Child Neurol 2000;15:588e91.
34. Govaert P, Lequin M, Swarte R, et al. Changes in globuspallidus with (pre)term kernicterus. Pediatrics2003;112:1256e63.
35. Martich-Kriss V, Kollias SS, Ball Jr WS. MR findings inkernicterus. AJNR Am J Neuroradiol 1995;16:819e21.
36. Counsell SJ, Tranter SL, Rutherford MA. Magnetic resonanceimaging of brain injury in the high-risk term infant. SeminPerinatol 2010;34:67e78.
37. Coskun A, Yikilmaz A, Kumandas S, et al. Hyperintenseglobus pallidus on T1-weighted MR imaging in acutekernicterus: is it common or rare? Eur Radiol 2005;15:1263e7.
38. Katar S, Akay HO, Taskesen M, et al. Clinical and cranialmagnetic resonance imaging (MRI) findings of 21 patientswith serious hyperbilirubinemia. J Child Neurol 2008;23:415e7.
39. Gkoltsiou K, Tzoufi M, Counsell S, et al. Serial brain MRI andultrasound findings: relation to gestational age, bilirubinlevel, neonatal neurologic status and neurodevelopmentaloutcome in infants at risk of kernicterus. Early Hum Dev2008;84:829e38.
40. Butterworth RF. The neurobiology of hepatic encephalopathy.Semin Liver Dis 1996;16:235e44.
41. Rovira A, Alonso J, Cordoba J. MR imaging findings in hepaticencephalopathy. AJNR Am J Neuroradiol 2008;29:1612e21.
42. Genovese E, Maghnie M, Maggiore G, et al. MR imaging of CNSinvolvement in children affected by chronic liver disease.AJNR Am J Neuroradiol 2000;21:845e51.
43. Butterworth RF, Spahr L, Fontaine S, et al. Manganesetoxicity, dopaminergic dysfunction and hepaticencephalopathy. Metab Brain Dis 1995;10:259e67.
44. Sharma P, Eesa M, Scott JN. Toxic and acquired metabolicencephalopathies: MRI appearance. AJR Am J Roentgenol2009;193:879e86.
45. de Vries LS, Jongmans MJ. Long-term outcome after neonatalhypoxic-ischaemic encephalopathy. Arch Dis Child FetalNeonatal Ed 2010;95:F220e4.
46. de Vries LS, Groenendaal F. Patterns of neonatal hypoxic-ischaemic brain injury. Neuroradiology 2010;52:555e66.
47. Miller SP, Ramaswamy V, Michelson D, et al. Patterns of braininjury in term neonatal encephalopathy. J Pediatr2005;146:453e60.
48. Griffiths PD, Radon MR, Crossman AR, et al. Anatomiclocalization of dyskinesia in children with “profound”perinatal hypoxic-ischemic injury. AJNR Am J Neuroradiol2010;31:436e41.
49. Linn J, Seelos KC, Botzel K. Hemiballism caused by a smallcavernoma in the subthalamic nucleus. Mov Disord2006;21:2266e7.
50. Etemadifar M, Abtahi SH, Abtahi SM, et al. Hemiballismus,hyperphagia, and behavioral changes following subthalamicinfarct. Case Report Med 2012;2012:768580.
51. Park HK, Kim HJ, Kim SJ, et al. From Jekyll to Hyde after limbicsubthalamic nucleus infarction. Neurology 2011;77:82e4.
52. Renard D, Le Floch A, Castelnovo G, et al. Hemiballism due toan ipsilateral subthalamic nucleus lesion. J Neurol2011;258:507e9.
53. Provenzale JM, Glass JP. MRI in hemiballismus due tosubthalamic nucleus hemorrhage: an unusual complication ofliver transplantation. Neuroradiology 1996;38(Suppl. 1):S75e7.
54. Kim HJ, Lee DH, Park JH. Posttraumatic hemiballism withfocal discrete hemorrhage in contralateral subthalamicnucleus. Parkinsonism Relat Disord 2008;14:259e61.
55. Barutca S, Turgut M, Meydan N, et al. Subthalamic nucleustumor causing hyperphagiaecase report. Neurol Med Chir(Tokyo) 2003;43:457e60.
56. Karampelas I, Podgorsak MB, Plunkett RJ, et al. Subthalamicnucleus metastasis causing hemichorea-hemiballism treatedby gamma knife stereotactic radiosurgery. Acta Neurochir(Wien) 2008;150:395e6 discussion 7.
57. Sunami Y, Koide R, Arai N, et al. Radiologic andneuropathologic findings in patients in a family withdentatorubral-pallidoluysian atrophy. AJNR Am J Neuroradiol2011;32:109e14.
58. Brunetti-Pierri N, Wilfong AA, Hunter JV, et al. A severe caseof dentatorubro-pallidoluysian atrophy (DRPLA) withmicrocephaly, very early onset of seizures, and cerebral whitematter involvement. Neuropediatrics 2006;37:308e11.
59. Shimojo Y, Osawa Y, Fukumizu M, et al. Severe infantiledentatorubral pallidoluysian atrophy with extremeexpansion of CAG repeats. Neurology 2001;56:277e8.