Student Expectations About Mental Health and Aging
25
This article was downloaded by: [University of Toronto Libraries] On: 29 April 2015, At: 10:19 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Click for updates Gerontology & Geriatrics Education Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wgge20 Student Expectations About Mental Health and Aging Michelle Pannor Silver ab , Natalie Irene Warrick b & Alaina Cyr b a Anthropology/Health Studies, University of Toronto Scarborough Campus, Toronto, Ontario, Canada b Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Canada Accepted author version posted online: 26 Jan 2015.Published online: 26 Jan 2015. To cite this article: Michelle Pannor Silver, Natalie Irene Warrick & Alaina Cyr (2015): Student Expectations About Mental Health and Aging, Gerontology & Geriatrics Education, DOI: 10.1080/02701960.2015.1005288 To link to this article: http://dx.doi.org/10.1080/02701960.2015.1005288 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Transcript of Student Expectations About Mental Health and Aging

This article was downloaded by: [University of Toronto Libraries]On: 29 April 2015, At: 10:19Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Click for updates
Gerontology & Geriatrics EducationPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wgge20
Student Expectations About MentalHealth and AgingMichelle Pannor Silverab, Natalie Irene Warrickb & Alaina Cyrb
a Anthropology/Health Studies, University of Toronto ScarboroughCampus, Toronto, Ontario, Canadab Institute of Health Policy, Management and Evaluation, Universityof Toronto, Toronto, Ontario, CanadaAccepted author version posted online: 26 Jan 2015.Publishedonline: 26 Jan 2015.
To cite this article: Michelle Pannor Silver, Natalie Irene Warrick & Alaina Cyr (2015): StudentExpectations About Mental Health and Aging, Gerontology & Geriatrics Education, DOI:10.1080/02701960.2015.1005288
To link to this article: http://dx.doi.org/10.1080/02701960.2015.1005288
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Gerontology & Geriatrics Education, 00:1–23, 2015Copyright © Taylor & Francis Group, LLCISSN: 0270-1960 print/1545-3847 onlineDOI: 10.1080/02701960.2015.1005288
Student Expectations About Mental Healthand Aging
MICHELLE PANNOR SILVERAnthropology/Health Studies, University of Toronto Scarborough Campus and Institute of
Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Canada
NATALIE IRENE WARRICK and ALAINA CYRInstitute of Health Policy, Management and Evaluation, University of Toronto, Toronto,
Ontario, Canada
Drawing from stereotype embodiment theory this study contributesto existing literature by examining whether and how expecta-tions regarding mental health and aging changed for studentsenrolled in an undergraduate gerontology course at a Canadianresearch university (N = 51). At the beginning and end of thecourse, data from an open-ended word association exercise andthe Expectations Regarding Aging (ERA-12) survey was collectedand later analyzed. Investigators used content analysis and quan-tization to examine the word association data and statistical tests toanalyze the mental health subscale (ERA-MHS). Findings were inte-grated and presented in a convergence code matrix. Results showthat overall participants had more favorable expectations over time;in particular, ERA-MHS scores indicated less favorable expectationsat Time 1 (M = 48.86) than at Time 2 (M = 65.36) significant atp < .01, while terms like “successful aging” increased and termslike “depressed” decreased. Findings have implications for geriatricmental health competencies of students in the health professions.
KEYWORDS gerontology education, student perspectives, stereo-type embodiment theory, health care students, ageism
Address correspondence to Michelle Pannor Silver, Anthropology/Health Studies,University of Toronto Scarborough Campus, 1265 Military Trail, Toronto, Ontario M1C1A4,Canada. E-mail: [email protected]
1
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

2 M. Pannor Silver et al.
INTRODUCTION
Globally, the number of people who are age 60 years and over is expectedto more than double by 2050 (Lin, Bryant, & Boldero, 2010), yet societalattitudes toward aging have remained negative (Cuddy, Norton, & Fiske,2005; Lee, 2009). In particular, misconceptions, negative stereotypes, andbiases toward older adults are reportedly prevalent among students in thehealth sciences (Hayes et al., 2006; Nolan et al., 2008; L. Ross, Duigan, Boyle,& Williams, 2014). The increasing proportion of older adults will translateto increased demand for health services, including specialized mental andbehavioral health services (Lun, 2010). To this end, to handle the needs ofan aging population, health care professionals must be equipped to pro-vide age-specific and culturally competent geriatric care (Eshbaugh, Gross,& Satrom, 2010; Mackenzie, Gekoski, & Knox, 2006).
According to the Substance Abuse and Mental Health ServicesAdministration (SAMHSA; 2007) and Eden, Maslow, Le, and Blazer (2012),even where there is sufficient supply of health professionals, the avail-ability of practitioners who are trained to provide mental and behavioralhealth services to older adults is insufficient. In Canada alone, approximately100,000 students are enrolled in health-related university programs (CanadianInstitute for Health Information, 2007). As these students become health careprofessionals, their attitudes and expectations about aging will shape theways that they interact with aging individuals (Lovell, 2006) and affect thedelivery and quality of care they provide to older adults (Ferrario et al.,2007).
The World Health Organization defined mental health not only as theabsence of psychiatric disease, but
as a state of well-being in which every individual realizes his or her ownpotential, can cope with the normal stresses of life, can work productivelyand fruitfully, and is able to make a contribution to her or his community.(Herrman, Saxena, & Moodie, 2005, p. 2),
a definition that applies to people of all ages. The frequent conflation ofmental and cognitive health requires that we differentiate the two althoughour primary focus in this article is on the mental health dimension of expec-tations of aging. According to the National Institutes of Health (Hendrie et al.,2006), the definition of cognitive health broadly refers to fluid and crystal-lized intelligence, general memory, learning and retrieval ability, broad visualand auditory perception, and cognitive processing speed. Mental and cogni-tive health are multidimensional, likewise they must be viewed with a focuson successful aging instead of normative aging. Consistent with definitionsprovided by Sarkisian, Hays, Berry, and Mangione (2002), the difference
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 3
between the two constructs lies in the fact that studies of cognitive health typ-ically include aspects of cognitive processing and dementia (Hendrie et al.,2006), whereas mental health explores topics such as emotional intelligence,resiliency, mastery and self-efficacy (Baltes & Smith, 2003).
Stereotypes about older adults as mentally unwell—specifically thatolder adults are miserable, bored, lonely, and incompetent—are persistentin Western culture (Abramson & Silverstein, 2004; Bousfield & Hutchinson,2010). Although it may be true that older adults are at greater risk for depres-sion, social isolation, and suicide (Olson, 2007), these risks may be attributedto common life situations of older adults and not simply a “normal” part ofaging (Rothermund & Brandstädter, 2003).
Theoretical Framework
Expectations about aging can also influence the health behaviours of olderadults. Motivation for enhancing our understanding of student perceptionsregarding aging draws from theoretical work on ageism (Palmore, 2001) andstereotype embodiment theory that states that attitudes and expectations mayshape how stereotypes are manifest (Levy, 2009). Stereotype embodimentoccurs when cultural stereotypes become reified, altering the health andfunctioning of older adults (Levy, 2009). Age stereotypes exert their influencethrough three different pathways: psychological, behavioral, and physiolog-ical. The psychological pathway highlights the importance of older people’sown expectations, in that expectations may shape their health behaviors(Levy & Leifheit-Limson, 2009; Sarkisian et al., 2002). The behavioral path-way relates to healthy practices, because negative stereotypes often presumethat preventative health practices are futile because health problems are aninevitable result of aging (Levy & Myers, 2004). The physiological path-way involves the autonomic nervous system and the physiological impactof subliminal exposure to positive or negative stereotypes. Age stereotypesthus become expectations that develop into self-fulfilling prophecies (Levy& Leifheit-Limson, 2009).
LITERATURE REVIEW
Coursework in gerontology provides an opportunity to improve students’understanding of the normative changes of aging and the implications thosechanges have on individuals and society (Lin et al., 2010), but conflictingevidence exists as to whether and how a gerontology course may affectstudent attitudes and expectations (Aud, Bostick, Marek, & McDaniel, 2006;Cottle & Glover, 2007; Ferrario et al., 2007). Validated surveys such as theExpectations Regarding Aging (ERA; Sarkisian et al., 2002) or Facts on AgingQuiz (FAQ; Palmore, 1977, 1998) have been used in previous research
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

4 M. Pannor Silver et al.
to assess expectations, knowledge, and misconceptions about aging (i.e.,Bardach, Gayer, Clinkinbeard, Zanjani, & Watkins, 2010; Joshi, Malhotra, Lim,Ostbye, & Wong, 2010; O’Hanlon, Camp, & Osofsky, 2006; Roters, Logan,Meisner, & Baker, 2010; Stubblefield & Knapp, 2000). In purely quantitativestudies that have used the aforementioned surveys to evaluate the effectsof a gerontology course on student expectations, students’ knowledge andattitude scores toward older adults had improved in some (Bardach et al.,2010; Cottle & Glover, 2007; Runkawatt, Gustafsson, & Engström, 2013),whereas other research found no change in student attitudes (Snyder, 2006;Stuart-Hamilton & Mahoney, 2003). The challenge posed by using only quan-titative approaches is that they do not necessarily offer any explanationas to why this divergence may occur (Creswell & Clark, 2011). Likewise,researchers using qualitative approaches found that when the gerontologycourse included elements of narrative review about older persons there werenet positive effects on students’ knowledge, skills, attitudes, and personaldevelopment (Villar, Fabà, & Celdrán, 2013).
Changes in nursing students’ knowledge and attitudes of older adultsfollowing a gerontology course have been explored by Aud et al. (2006)and Lee (2009) through the use of methods which combined the FAQsurvey (Palmore, 1977, 1998) and Kogan Scales (Kogan, 1961) along withopen-ended comments and subjective writings. The use of these three mea-sures supported Lee (2009) and Aud et al. (2006) in capturing attitudes andbeliefs thought to be important to the social construction of aging but donot adequately address students’ future expectations of aging giving rise toour selection of the ERA-12 (Sarkisian et al., 2002) for this particular study.Although their findings suggest that students’ scores on the quantitative mea-sures remained negative indicating that attitudes toward aging did not changefollowing the course, some students did report more positive feelings towardolder adults in open-ended comments and subjective reports collected oncourse evaluations. Consequently, divergence between attitude scores andopen-ended comments within the same study suggest that underlying beliefstoward older adults and expectations are complex, necessitating an approachthat used a validated survey instrument and a means of allowing participantsto use their own words to best illuminate these complexities.
Although some studies to date have considered students’ expectationsand attitudes as they relate to older adults in general (Krout & McKernan,2007), to the physical aspect of aging (Henderson, Xiao, Siegloff, Kelton, &Paterson, 2008; Lee, 2009) and to cognitive changes (Chippendale, 2013),less attention has been paid to the mental health aspects of aging. The aimof this study was to examine whether participating in a gerontology courseembedded in a health studies program at a large research university changedstudents’ expectations regarding aging and mental health using a researchdesign that included an open-ended question and a survey questionnaire.In this study we put forward three research questions: (1) What words do
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 5
students associate with aging and mental health, and how do these changeover time? (2) How do student expectations regarding aging and mentalhealth change after participating in a gerontological health studies course, asmeasured by a validated survey? and (3) In what ways does the collection ofan open-ended question and a survey questionnaire contribute to a deeperunderstanding of the malleability of student expectations of mental healthand aging?
METHOD
Participants
Undergraduate students at a large research university in Ontario, Canada whowere enrolled in a one-semester course in gerontology during the winterterm of the 2014 school year were invited to participate in this researchstudy (N = 51). Participation in the study did not affect student grades.Of the 53 eligible students who provided written consent to participate in thisstudy, one did not finish the course and another student provided incompleteinformation on the questionnaire.
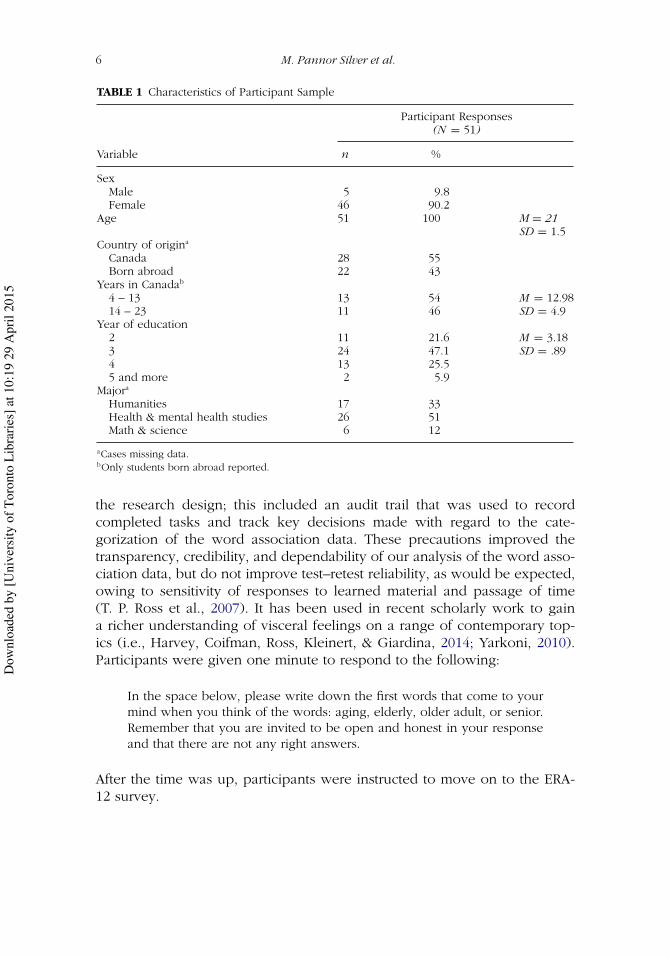
Participant demographics were relatively homogenous. More than onehalf (51%) of participants listed health and mental health studies as theirmajor program of study. The average age was 21 years (range 19–25),and 47% were in their third year of study. Most participants were female(90%). The proportion of Canadian-born participants in the study (55%) wassimilar to the proportion for the City of Toronto (47.8% Canadian-born citi-zens) (Statistics Canada, 2012). Among students who immigrated to Canada,the average time living in Canada was 12.98 years (SD = 4.9). Descriptivestatistics from these variables are presented in Table 1.
Measures
WORD ASSOCIATION EXERCISE
A word association exercise was used to elicit responses that reflect underly-ing associations and relationships between concepts to explore the personalunconscious (Spiteri, 2005). Word association protocols are widely usedwithin psychological and linguistic disciplines as a measure of a participant’sgrowing lexicon (Strauss, Sherman, & Spreen, 2006). According to Fitzpatrick,Playfoot, Wray, and Wright (2013), use of a principled method for collect-ing, scoring (categorizing), and analyzing word association responses—as inthe case of the protocols used in this research—aid in evaluating reliabil-ity and validity in behavioral responses over time. To ensure replicability ofour protocols, strategies aimed at increasing rigor were embedded within
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15
6 M. Pannor Silver et al.
TABLE 1 Characteristics of Participant Sample
Participant Responses(N = 51)
Variable n %
SexMale 5 9.8Female 46 90.2
Age 51 100 M = 21SD = 1.5
Country of origina
Canada 28 55Born abroad 22 43
Years in Canadab
4 – 13 13 54 M = 12.9814 – 23 11 46 SD = 4.9
Year of education2 11 21.6 M = 3.183 24 47.1 SD = .894 13 25.55 and more 2 5.9
Majora
Humanities 17 33Health & mental health studies 26 51Math & science 6 12
aCases missing data.bOnly students born abroad reported.
the research design; this included an audit trail that was used to recordcompleted tasks and track key decisions made with regard to the cate-gorization of the word association data. These precautions improved thetransparency, credibility, and dependability of our analysis of the word asso-ciation data, but do not improve test–retest reliability, as would be expected,owing to sensitivity of responses to learned material and passage of time(T. P. Ross et al., 2007). It has been used in recent scholarly work to gaina richer understanding of visceral feelings on a range of contemporary top-ics (i.e., Harvey, Coifman, Ross, Kleinert, & Giardina, 2014; Yarkoni, 2010).Participants were given one minute to respond to the following:
In the space below, please write down the first words that come to yourmind when you think of the words: aging, elderly, older adult, or senior.Remember that you are invited to be open and honest in your responseand that there are not any right answers.
After the time was up, participants were instructed to move on to the ERA-12 survey.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 7
EXPECTATIONS REGARDING AGING (ERA-12) SURVEY
The ERA-12 is a shortened version of the 38-item survey that measures expec-tations regarding aging in older adults (Joshi et al., 2010; Sarkisian, Steers,Hays, & Mangione, 2005) validated in a number of studies (i.e., Sarkisian,Shunkwiler, Aguilar, & Moore, 2006; Sarkisian et al., 2005). It includes threefour-item scales that address expectations about physical health (Questions1–4), mental health (Questions 5–8), and cognitive function (Questions9–12), as well as an overall expectations regarding aging scale when combin-ing all 12 items. Higher scores on the ERA-12 are associated with expectationsof achievement and maintenance of high physical, mental and cognitive func-tioning for self and others while aging, whereas lower scores are indicativeof expected declines. The observed interitem reliability for the overall scoreand mental health portions in this sample is as follows: Cronbach’s alphawas α = –0.60 for Time 1 mental health and exceeded α = .33 for the Time2 mental heath portion of the scale, and, for the overall ERA-12 itself, α =.351 and α = .521. As demonstrated by Sarkisian et al. (2005) acceptable lev-els of reliability and construct validity for the ERA-12 scales were establishedin two different samples of community-dwelling older adults (n = 429 andn = 643) with Cronbach’s alpha, α = .75 for the mental health subscale andα = .88 overall. Within this study, construct validity for the ERA-38 was estab-lished based upon correlations with other validated measures of self-reportedhealth (i.e., Geriatric Depression Scale by Hoyl et al., 1999) and indicatorsof successful aging (Mental Component Survey–12; Ware, Kosinski, & Keller,1995). The shortened ERA-12 (Sarkisian et al., 2005) has also been shownto capture 88% of the variation in the ERA-38 overall score (Sarkisian et al.,2002). Although initially intended for older adults, the ERA-12 has been val-idated in three other samples of similar size in younger adults (i.e, Davis,Bond, Howard, & Sarkisian, 2011; Galambos & Curl, 2013; Roters et al.,2010). The Cronbach’s alpha reported by these studies ranged from 0.75 to0.82, indicating that for larger samples it is generally a strong and reliablemeasure with good internal validity.
Procedures
INTERVENTION: GERONTOLOGY COURSE
Between data collection time points, students participated in a geronto-logical health studies course. The course focused on presenting studentswith a substantial range of disciplinary perspectives on the phenomena ofaging including anthropology, sociology, psychology, and economics. Theobjectives of participating in the course were to critically examine researchon health and aging in Canada, contrast successful aging and age-related
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

8 M. Pannor Silver et al.
decline, reflect on worldwide demographic trends in aging and public poli-cies related to health and aging, and produce a research paper relevant tohealth and aging. Theoretical frameworks were introduced to students in amanner that was integrated into substantive topics. For example, in a mod-ule about financial well-being, work, and retirement basic principles frommicroeconomic theory were introduced as well as discussions about the lifecourse perspective (i.e., Elder & Rockwell, 1979) and the resource perspec-tive (Wang, Henkens, & van Solinge, 2011). In addition to this, students wereasked to consider the continued relevance of role theory, continuity theory,and activity theory (i.e., Alley, Putney, Rice, & Bengtson, 2010; Bengtson,Rice, & Johnson, 1999) and to question the implications of theoretical frame-works on their own understanding of different facets of mental health andaging (Clarke, Marshall, House, & Lantz, 2011).
Topics covered during the course included a module on health care,aging, and social structures in Canada as they compare to other comparablydeveloped countries; cognitive function and decline; financial well-being,work, and retirement; physical mobility and adapted environments; familyand social support; and a module on death, dying, and longevity. The read-ings assigned for the course were designed to help students contextualizeand question different understandings of mental health at later points inthe life course. For example, some readings featured ethnographic accountswhile others relied predominantly on quantitative methodology to assessmental health through psychometric scales. Guest speakers from the Ministryof Health and Long-Term Care provided students with examples of the impli-cations of mental health issues among older adults on the health care systemand discussed specific policies that aim to address mental health needs forolder adults.
An independent research assistant with no association to thegerontology course presented students with written and oral informationabout the study, administered written consent forms prior to participation,and assigned a unique ID number to each student participant. After provid-ing written consent, participants completed a questionnaire package duringthe second week (Time 1) and again during the 12th week (Time 2) ofa 13-week course. At Time 1, the questionnaire package contained threeparts: a demographic survey, a word association exercise, and the ERA -12-item survey. At Time 2, the questionnaire contained identical versions of theword association exercise and the ERA-12. The demographic survey collectedbasic demographic information on each participant including age, sex, yearof study, major, country of birth, and number of years living in Canada. Thecourse instructor, also the study’s principle investigator, did not participate indata collection and did not access any collected data until all student gradeshad been submitted at the end of the course. Ethical approval for the studywas obtained from the lead author’s Office of Research Ethics.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 9
Design & Analysis
A pre–post study design was used to examine changes in students’ expec-tations of aging and mental health over time as illustrated in Figure 1.Researchers used content analysis to interpret the word association data(Mayring, 2004) with the aim of uncovering meaning in context, interpretingthe terms from a realist perspective and interpreting the data (Vaismoradi,Turunen, & Bondas, 2013). Members of the research team each conductedan independent review of word association data sets to identify terms relatedto mental health guided by the categories identified by Sarkisian et al. (2002):life satisfaction, loneliness, happiness, depression, anxiety, emotional well-being, and grief. This was followed by two authors (AC & NW) extractingdata independently via content analysis coding of the word association data,which allowed for cross-referenced coding and discussion of judgment-baseddecisions. The principal investigator (MS) was consulted during the anal-ysis to ensure that interpretations were consistent in the context of thesubject matter. All mental health terms identified in the word associationdata set were assigned a negative, neutral, or positive valence. Examplesof positive terms included enjoy life, relaxed, fun, fulfillment, and helpful.Examples of negative terms included dependence, lonely, and sad. The onlyterm attributed a neutral valence was mental health. The identified men-tal health terms were quantized by assigning a negative, neutral, or positivevalence (Sandelowski, Voils, & Knafl, 2009) and given a score of –1, 0, or +1,respectively, labeled words as positive (indicated an affirmative or encourag-ing adjective/adverb/ noun), neutral (held no judgment value for adjective/adverb/noun), or negative (indicated a declining or deleterious adjective/
Word Association
Task
ERA-12Survey
Data Collection
Content Analysis
Gerontology Course
(13 weeks)
Time 2
Word Association
Task
ERA-12Survey
Time 1
Quantization and content analysis
of words for convergence or divergence with
ERA-MHS
Integration
Descriptive Statistics & t test
Analysis
FIGURE 1 The pre–post study design.
ERA-12 = expectations regarding aging survey (12-item); ERA-MHS = expectations regardingaging survey-mental health subscale.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

10 M. Pannor Silver et al.
adverb/noun) (Sandelowski, 1993). Valence scores were calculated for eachcategory at Time 1 and Time 2 by adding up the scores of correspondingterms.
Using a repeated-measures cross-sectional design (Campbell & Stanley,1966) data collected from the ERA-12 survey was analyzed by assessingresponses for each item on a 4-point Likert-type scale ranging from 1 (def-initely true) to 4 (definitely false). The summative overall score for theERA-12 ranged from 12 to 48 (with each domain ranging from 4 – 16). OverallERA-12 scores and mental health subscale (ERA-MHS) scores were calculatedfrom participant responses and were transformed to scores ranging from 0 to100, as per the algorithm provided by Sarkisian et al. (2005). Responses tothe ERA-MHS were recoded into dichotomous responses of “true” or “false”by collapsing “definitely” and “somewhat” true and false into their respec-tive categories; frequencies of true and false responses were tallied for eachquestion at both time points. Paired samples t tests were used to determineif there were statistically significant differences between participants’ over-all ERA-12 and ERA-MHS scores at Time 1 and Time 2. SPSS v21 softwarewas used to conduct statistical analyses on these scores (IBM Corp, 2012).The results of these inferential tests are reported, as are effect sizes (Cohen’sd) and confidence intervals. A reliability analysis was conducted to validatethe Cronbach’s alpha (measure of internal consistency reliability) obtainedfrom these data and validate these results against Sarkisian et al. (2005). Thesignificance level used for all tests is p = .05.
Subsequent to separate analyses, data from the open-ended word exer-cise and the survey questionnaire were analyzed with the intent of observingwhether there was any mutual illumination of findings (Woolley, 2009).Results from the survey questionnaire at Time 1 and Time 2 are presented inTable 4. Open-ended word exercise data are presented in Table 4. Changesin the frequency and valence of terms related to mental health on the wordassociation and frequency of true and false responses on questions from theERA-MHS were used to determine points of concordance or disagreementand overall change from Time 1 to Time 2.
RESULTS
Nine categories related to mental health were present in the content analy-ses of the word association exercise. The categories dependence on others,relaxation, social involvement, loneliness, sadness, mental health, socialinclusion, and overall well-being appeared in Time 1 and Time 2 data sets,whereas life enjoyment appeared only at Time 2. Most categories identifiedmatched those mentioned by Sarkisian et al. (2002) with the addition ofdependence on others, mental health, and social inclusion. These categorieswere added to ensure that we were exhaustive in our coding and inclusive
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15
Student Expectations About Mental Health and Aging 11
TABLE 2 Themes Identified From Word Association Exercise and Corresponding ExamplesWith Valence Assignment
Themes Examples of Words (valence)
Dependence on others Dependent/dependence (–), need help (–), reliance (–),independence (+)
Relaxation Relaxed (+), free from stress (+), not stressed out (+)Social involvement Active (+), helpful (+), sharing (+), generous (+)Loneliness Lonely (–), alone (–), less social (–), isolated (–)Sadness/happiness Sad (–), unhappy (–), depressed (–), happy (+), happy after
retirement (+)Mental health Mental health (N), emotional (–), mental health problem (–)Social inclusion Kind (+), compassionate (+), social (+), friends, good
company, friendly (+)Life enjoyment Enjoy life (+), finding pleasure in hobbies (+), fun (+),Overall well-being Fulfillment (+), Increased quality of life (+), Successful aging
(+), Regretful (–), Bored (–)
of all mental health words generated by students. Examples of terms withineach category are provided in Table 2.
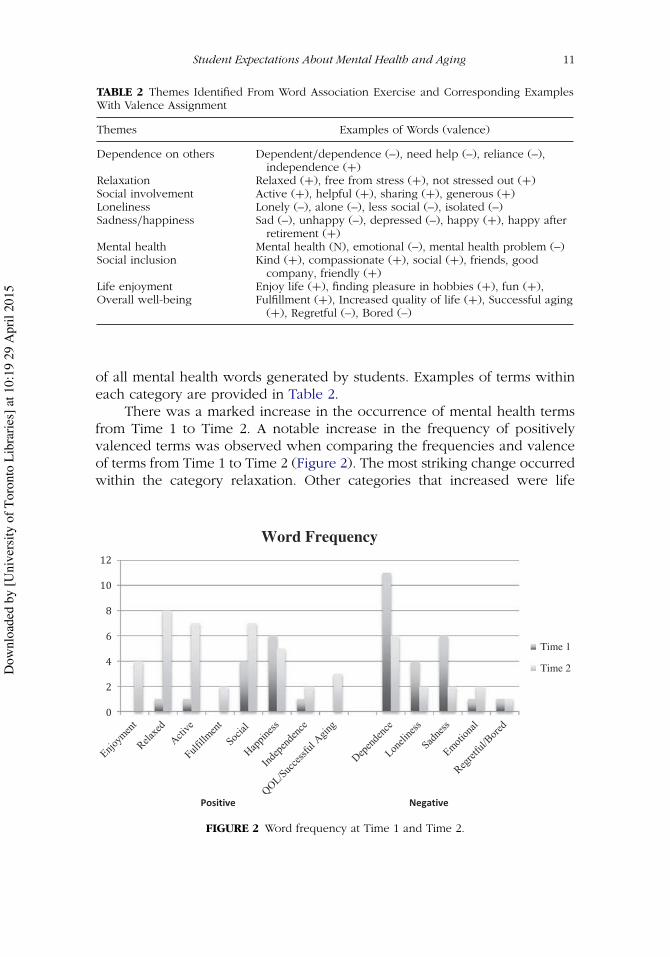
There was a marked increase in the occurrence of mental health termsfrom Time 1 to Time 2. A notable increase in the frequency of positivelyvalenced terms was observed when comparing the frequencies and valenceof terms from Time 1 to Time 2 (Figure 2). The most striking change occurredwithin the category relaxation. Other categories that increased were life
Positive
Word Frequency
Time 1
Time 2
Negative
FIGURE 2 Word frequency at Time 1 and Time 2.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

12 M. Pannor Silver et al.
TABLE 3 Comparison of Mean ERA-12 and ERA-MHS Scores From Time 1 to Time 2
Time 1 Time 2(N = 51) (N = 51)
Domain M SD CI M SD CIMean Difference
[95% CI] Test Statistic, p Value
Aging(overall)
45.86 9.05 42.5, 51.46 53.49 10.47 48.22, 57.82 −7.63 [–10.89, –4.36] t(50) = –4.68, p < .01
MentalHealth
48.86 12.02 41.02, 52.46 65.36 16.19 57.72, 72.72 −16.50 [–22.16, –10.85] t(50) = –5.86, p < .01
ERA-12 = expectations regarding aging survey (12-item); ERA-MHS = expectations regarding agingsurvey-mental health subscale; CI = confidence interval.
enjoyment, social involvement, and overall well-being. Similarly, the occur-rence of negatively valenced categories decreased, particularly the categoriesdependence on others and sadness.
The mean of the overall ERA-12 scores was smaller at Time 1, indicatingmore negative expectations (M = 45.86) than at Time 2 (M = 53.48); thisresult was statistically significant at p < .001 (Table 3). Similarly, the meanof the ERA-MHS scores showed a statistically significant (p < .001) increasein favorable expectations of aging and mental health from Time 1 (M =48.86) to Time 2 (M = 65.36). The effect size for the overall ERA-12 scores(Cohen’s d = –.779) indicates a large effect and the ERA-MHS scores (Cohen’sd = –1.16) a very large effect between Time 1 and Time 2. The 95% confi-dence interval for the mean difference in overall ERA-12 scores was –10.89 to–4.36 and for the ERA-MHS score was –22.16 to –10.85 (Table 3).
Integrated Results
Table 4 illustrates the total count of themes that emerged from the wordassociation exercise at Time 1 and Time 2. The collection of open-endedword associations and ERA scores with a specific focus on mental health(Table 5) provided greater clarity about the malleability of expectations ofaging by uncovering areas of divergence and convergence. We discoveredthat findings converged in three and diverged on one of these constructs.
CONVERGENCE BETWEEN CATEGORIES SOCIAL INVOLVEMENT AND
DEPENDENCE ON OTHERS AND ERA-12 QUESTION “I EXPECT THAT AS IGET OLDER I WILL SPEND LESS TIME WITH FAMILY AND FRIENDS.”
At Time 1, the categories social involvement and dependence on others hadvalences of +1 and –11, respectively (Table 4), whereas 61% of participantsindicated true on Question 5 of the ERA-12 (Table 5). At Time 2, theseexpectations were virtually reversed. The categories social involvement hada valence of +7 and dependence on others had a valence of –4, whereasonly 24% of participants indicated Question 5 of the ERA-12 was true. Thesefindings suggest that at by the end of the course participants came to betterunderstand how older adults contribute to society.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 13
TABLE 4 Total Count of Themes Appearing in Word Association Data at Time 1 and Time 2
Occurrences
Theme (Valence) Time 1 Time 2
Dependent/need help (–) 11 6Independence (+) 1 2Active/social involvement (+) 1 7Lonely/alone/less social (–) 4 2Social inclusion (+) 4 7Relaxed/free from stress (+) 1 8Life enjoyment (+) 0 4Sadness/depressed (–) 6 2Happiness (+) 6 5Mental health (N) 1 0Emotional/mental health problem (–) 1 2Fulfillment (+) 0 2Increased quality of life (+) 0 1Successful aging (+) 0 2Regretful/bored (–) 1 1Total
Positive 13 38Neutral 1 0Negative 23 13
Number of terms used 37 51
TABLE 5 Dichotomized Results From the ERA-12 Mental Health Subscale Questions at Time1 and Time 2
Time 1 Time 2(N = 51) (N = 51)
True False True FalseERA-12 Questions n (%) n (%) n (%) n (%)
5. Spending less time with friends andfamily as one ages.
31 (60.8) 20 (39.2) 12 (23.5) 39 (76.5)
6. Being lonely is just something thathappens when people get old.
20 (39.2) 31 (60.8) 10 (19.6) 41 (80.4)
7. As people get older they worrymore.
13 (25.5) 38 (74.5) 21 (41.2) 30 (58.8)
8. It’s normal to be depressed whenyou are old
38 (74.5) 13 (25.5) 12 (23.5) 39 (76.5)
Overall ERA-MHS scores M = 48. 85 M = 65.36SD = 12.02 SD = 16.19
ERA-MHS = expectations regarding aging survey-mental health subscale.
CONVERGENCE BETWEEN CATEGORIES LONELINESS AND SOCIAL INCLUSION
AND ERA-12 QUESTION “BEING LONELY IS JUST SOMETHING THAT HAPPENS
WHEN PEOPLE GET OLD”
At Time 1, the categories loneliness and social inclusion had valences of–4 and + 4, respectively, whereas 39% of participants indicated Question
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

14 M. Pannor Silver et al.
6 of the ERA-12 was true. At Time 2, these expectations were slightly morepositive. These findings suggest that exposure to concepts such as the natureof the family in late life may have given students greater perspective on thesocial aspects that contribute to mental health.
DIVERGENCE BETWEEN CATEGORIES RELAXATION AND LIFE ENJOYMENT AND
ERA-12 QUESTION “AS PEOPLE GET OLDER THEY WORRY MORE”
At Time 1, the category relaxation had a valence of +1, whereas 26% ofparticipants indicated true to older adults worrying more. At Time 2, therewas a substantial positive change in the word association data, but more par-ticipants (41%) indicated that they agreed with the statement “As people getolder they worry more.” Although these findings seem to diverge, it is possi-ble that, together, they capture how participants’ expectations of aging andmental health became more nuanced. Participants’ may have become moreaware of the challenges older adults face (i.e., chronic illness, reduced pen-sions), while also understanding that enjoying life and being more worriedare both representative of aging and mental health.
CONVERGENCE BETWEEN CATEGORIES “SADNESS” AND “MENTAL HEALTH” AND
ERA-12 QUESTION “IT’S NORMAL TO BE DEPRESSED WHEN YOU ARE OLD”
At Time 1, the categories sadness and mental health had valences of –6 and0, respectively, whereas 75% of participants indicated “true” on Question8 of the ERA-12. At Time 2, valences remained fairly consistent, whereas theERA-12 scores had changed. By the end of the course, participants betterunderstood that depression and sadness are not normal experiences of theaged. Participants’ greater awareness of this fact may better equip them indetecting mental health issues in older adults, leading to more appropriatecourses of treatment for patients.
DISCUSSION AND IMPLICATIONS
This is the first study we are aware of that used word association with theERA-12 to investigate whether and how undergraduate students’ expecta-tions regarding aging and mental health changed following exposure toa gerontology course. At the start of the course, participants’ expectationsregarding aging and mental health were in line with existing literatureon aging stereotypes among young adults (Abramson & Silverstein, 2004;Bousfield & Hutchison, 2010). In reassessing expectations at the end ofthe course, we discovered that exposure to coursework in gerontologypositively influenced participants’ expectations of aging and mental health.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 15
These expectations were found to be more reflective of the variation in lifesituations that exists among older adults.
Identification of depression and other mental health related symptoms,such as grief, anxiety and emotional well-being are made more difficult byother age-related complicating factors such as cognitive decline commonto patients with dementia, the presence of other mental health disorders(i.e., secondary substance abuse), and comorbidity of medical problems lim-iting physical function (Thorpe, 2009). Providers must be aware of theirown perceived bias concerning expectations of aging as well as knowledgeof interventions that are age-specific and culturally competent to provideappropriate and effective treatment of mental health disorders (Mackenzieet al., 2006). The existing literature has shown considerable variation whenreporting on the impact gerontology courses have on student attitudes (Audet al., 2006; Bardach et al., 2010; Cottle & Glover, 2007; Ferrario et al., 2007),however variations in study results may be attributed to course differences orreliance on a single method as opposed to an approach that draws from andintegrates findings from a survey questionnaire and an open-ended wordexercise. Examining the integrated findings from each time point presentstwo very different ideas about the participants’ expectations regarding agingand mental health. The findings at Time 1 may be an indication of youngerpeople’s expectations of the older adult who is a worry-free dependent thatis less fulfilled in their social relationships. The findings at Time 2 paint aportrait of the older adult as an emotionally balanced, active communitymember who enjoys life despite the challenges they face.
We identified that the mental health-related terms used by participantsat Time 1 were largely negative, primarily focusing on dependence and sad-ness, whereas ERA-12 and ERA-MHS scores indicated expected declines withaging. The mental health-related terms used by participants at Time 2 weremore positive, with a stronger presence of terms related to social involve-ment, enjoying life, relaxation, and overall well-being. Additionally, themarked increase in and wider variety of mental health related terms includedin the Time 2 word association dataset suggests that participants were moreaware of the varying aspects of mental health and aging as the course nearedcompletion. Likewise, overall ERA-12 and ERA-MHS scores increased overtime, indicating that expectations of aging improved. Therefore, this studyhas shown that student expectations of aging and mental health are mal-leable, and that it is possible to positively influence students’ expectations ofaging and mental health through a gerontology course.
Researchers have argued that the pervasiveness of ageist attitudes andnegative views toward old age have resulted from personal apprehensionsand expectations about future selves (Dorfman, Murty, Ingram, Evans, &Power, 2004; Oakes & Sheehan, 2014). Henderson et al.’s (2008) worksuggests that quality of life courses improve expectations of aging, where
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

16 M. Pannor Silver et al.
biomedical courses may not. McLafferty and Morrison’s (2004) research sug-gest that coursework in gerontology may “over-rely [on] teaching negativeaspects of aging” (p. 446), thus inculcating the next wave of practitionerswith skewed expectations of aging for themselves and the persons for whomthey provide care. In accordance with stereotype embodiment theory, whichsuggests that expectations about aging are malleable (Levy, 2009), this studydemonstrated that the presentation of the positive aspects as part of thecourse in gerontology helped to improve students’ expectations of agingand mental health.
Our findings offer numerous practical implications for health care edu-cators, researchers and policy makers. Improving care and support to olderadults with mental illness requires that specialized educational and trainingopportunities be made available to meet the increasing demand for mentaland behavioral health services (SAMHSA, 2007). Results from this study showthat shifting expectations of aging may be achieved by increasing awarenessof the practical and emotional intelligence that comes with aging (Cowen,1985), by emphasizing the problem-solving skills that accumulate over thelife span (Baltes & Smith, 2003) and by sharing the commonalities that existbetween younger and older adults (Gonzales, Morrow-Howell, & Gilbert,2010). Educators of health professionals may be especially concerned withcore competencies for training in certain areas, particularly in regards tosuccessful models of aging.
Limitations and Suggestions for Future Research
Although this study uniquely examines student expectations about aging andmental health by integrating findings from an open-ended word exercise anda validated survey questionnaire, there were some limitations. Participantresponses may have changed over time due to factors other than the course(i.e., not enough time between ERA-12 measurements, practicing, fatigue,natural development). The timing and presentation of course material mayhave shaped the frequency of terms appearing in the Time 2 word associ-ation data, possibly due to a recency effect, where material learned morerecently is better recalled than older material (Neath & Knoedler, 1994).Researchers attributed a positive, neutral or negative valence to wordsbased on single word responses from word association data. Given thatthis may have introduced some minor interpretive latitude on behalf of theresearchers, it is important to consider what effect this process may havehad on our results. Fortunately, though some terms included in the wordassociation data sets could be interpreted as ambiguous (e.g., slow could beinterpreted as cognitive or physical slowing), we did not find any ambiguousterms relating to mental health. The factor loadings in the principal com-ponents analysis (PCA) for the expectations regarding aging survey-mental
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 17
health subscale (ERA-MHS) at Time 1 did not align as theoretically conceptu-alized by Sarkisian et al. (2005). As a general rule of thumb a bare minimumof 10 observations per variable are necessary to avoid computational dif-ficulties and produce stable estimates with the PCA (Tabachnick & Fidell,2007). Our relatively small sample size may have contributed to the lowerthan expected Cronbach’s alpha for the Time 1 and Time 2 measures on theERA-MHS subscale and as a consequence the α = .70 reliability standardfor group comparisons as put forth by Nunnally and Bernstein (1994) waslikely not met. The low Cronbach’s alpha could indicate that some itemsdid not correlate positively with one another. What is interesting is that theCronbach’s alpha improved significantly from the Time 1 mental health tothe Time 2 mental health subscale. At Time 1, it was assumed that therewas no prior exposure to coursework in mental health and aging.What thissuggests is that the ERA-12 may not perform as predicted by Sarkisian et al.(2002) with respect to small samples of young adults without prior exposureto concepts and principles of mental health and aging. Because the origi-nal ERA-12 was intended to capture older adults’ expectations of their ownexperiences with aging they could rely upon personal experience whereasa young adult without such insight may not know enough about the experi-ence of mental health in old age to make informed opinions to respond tothe true/false categories in a manner consistent with theory. Consequently,their report on a relatively small number of items for the mental healthsubscale did not conform to the predicted manner at Time 1.
This study further motivates the need for future studies, which inves-tigate the validity of ERA-12 in samples of younger adults. Notably, Roterset al. (2010) maintained internal validity (i.e., Cronbach alpha greater than0.8) of the ERA-12 among a demographically similar sample (upper-yearundergraduate students at a large, Canadian metropolitan university with anaverage age of 21.5); however this was with a much larger sample size (N =145), which may explain the inconsistency of our results. In future studies,researchers may also choose to perform member checking with participantsto clarify any instances of ambiguity in the word association task. Use ofother methods such as individual interviews and focus groups, in conjunc-tion with validated survey instruments, may also provide a more in depthexplanation of expectations about aging among this population. To furtheradvance knowledge in this area, further research is required to examine howchanged expectations of aging and mental health impacts delivery of care toolder adults.
CONCLUSIONS
The purpose of this study was to explore how students’ expectations ofmental health and aging changed after participating in a gerontology health
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15
18 M. Pannor Silver et al.
studies course. In this study, the case was made for ongoing usage of mul-tiple methods strategies for investigating future research on mental healthin aging by demonstrating how integrated findings contribute to a deeperunderstanding of the malleability of student expectations of mental healthand aging. Ultimately, our research suggests that providing better quality ofcare for the growing population of older adults will require students of healthand aging to have more positive, albeit realistic perspectives about aging andmental health issues.
ACKNOWLEDGMENTS
The authors would like to thank the 51 undergraduate students who partici-pated in this study as well as Sasithra Kanageswaran and Connie Phung fortheir work as research assistants on this project. The authors would also liketo acknowledge the support of Dr. Katie Dainty, Dr. Robin Hayeems, and allof the graduate students who participated in the Health Services Researchcourse.
FUNDING
Natalie Warrick, MSc, PhD Student, would like to gratefully acknowledge thefunding support provided by the Ontario Graduate Scholarship, the TorontoRehab Kirshenblatt Memorial Scholarship and the Saint Elizabeth HealthcareMichael Decter Health Leadership and Policy Studies Scholarship.
ORCID
Michelle Pannor Silver http://orcid.org/0000-0003-3870-7434
REFERENCES
Abramson, A., & Silverstein, M. (2006). Images of aging in America 2004.Washington, DC: AARP and the University of Southern California.
Alley, D. E., Putney, N. M., Rice, M., & Bengtson, V. L. (2010). The increasing useof theory in social gerontology: 1990–2004. Journals of Gerontology Series B:Psychological Sciences and Social Sciences, 65(5), 583–590.
Aud, M. A., Bostick, J. E., Marek, K. D., & McDaniel, R. W. (2006). Introducingbaccalaureate student nurses to gerontological nursing. Journal of ProfessionalNursing, 22(2), 73–78.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 19
Baltes, P. B., & Smith, J. (2003). New frontiers in the future of aging: From successfulaging of the young old to the dilemmas of the fourth age. Gerontology, 49(2),123–135.
Bardach, S. H., Gayer, C. C., Clinkinbeard, T., Zanjani, F., & Watkins, J. F. (2010). Themalleability of possible selves and expectations regarding aging. EducationalGerontology, 36(5), 407–424.
Bengtson, V. L., Rice, C. J., & Johnson, M. L. (1999). Are theories of aging important?Models and explanations in gerontology at the turn of the century. In V. L.Bengston & K. W. Schaie (Eds.), Handbook of theories of aging (pp. 3–20). NewYork, NY: Springer Publishing.
Bousfield, C., & Hutchison, P. (2010). Contact, anxiety, and young people’s attitudesand behavioral intentions towards the elderly. Educational Gerontology, 36(6),451–466. doi:http://dx.doi.org/10.1080/03601270903324362
Campbell, D., & Stanley, J. (1966). Experimental and quasi-experimental designs forresearch. Chicago, IL: Rand McNally & Company.
Canadian Institute for Health Information. (2007). Canada’s health care providers,2007. Ottawa, Canada: Author.
Chippendale, T. (2013). Elders’ life stories: Impact on the next generation ofhealth professionals. Current Gerontology and Geriatrics Research, 2013, 1–7.doi:http://dx.doi.org/10.1155/2013/493728.
Clarke, P., Marshall, V., House, J., & Lantz, P. (2011). The social structuring of mentalhealth over the adult life course: advancing theory in the sociology of aging.Social Forces, 89(4), 1287–1313.
Cottle, N. R., & Glover, R. J. (2007). Combating ageism: Change in student knowl-edge and attitudes regarding aging. Educational Gerontology, 33(6), 501–512.doi:http://dx.doi.org/10.1080/03601270701328318
Cowen, E. L. (1985). Person-centred approaches to primary prevention in mentalhealth: Situation-focused and competence-enhancement. American Journal ofCommunity Psychology, 13(1), 31–48.
Creswell, J. W., & Clark, V. L. P. (Eds.). (2011). Designing and conducting mixedmethods research (2nd ed.). Thousand Oaks, CA: Sage.
Cuddy, A. J., Norton, M. I., & Fiske, S. T. (2005). This old stereotype: The pervasive-ness and persistence of the elderly stereotype. Journal of Social Issues, 61(2),267–285. doi:http://dx.doi.org/10.1111/j.1540-4560.2005.00405.x
Davis, M. M., Bond, L. A., Howard, A., & Sarkisian, C. A. (2011). Primary careclinician expectations regarding aging. The Gerontologist, 51(6), 856–866.
Dorfman, L. T., Murty, S. A., Ingram, J. G., Evans, R. J., & Power, J. R. (2004).Intergenerational service-learning in five cohorts of students: Is attitude changerobust? Educational Gerontology, 30(1), 39–55. doi:10.1080/03601270490248446
Eden, J., Maslow, K., Le, M., & Blazer, D. (Eds.). (2012). The mental health andsubstance use workforce for older adults: in whose hands? Washington, DC:National Academies Press. Retrieved from http://www.iom.edu/Reports/2012/The-Mental-Health-and-Substance-Use-Workforce-for-Older-Adults.aspx
Elder, G. H., & Rockwell, R. C. (1979). The life-course and human development: Anecological perspective. International Journal of Behavioral Development, 2(1),1–21.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

20 M. Pannor Silver et al.
Eshbaugh, E. M., Gross, P. E., & Satrom, T. (2010). Predictors of self-reported like-lihood of working with older adults. Educational Gerontology, 36(4), 312–329.doi:http://dx.doi.org/10.1080/03601270903058481
Ferrario, C. G., Freeman, F. J., Nellett, G., & Scheel, J. (2007). Changing nursingstudents’ attitudes about aging: An argument for the successful aging paradigm.Educational Gerontology, 34(1), 51–66. doi:10.1080/03601270701763969
Fitzpatrick, T., Playfoot, D., Wray, A., & Wright, M. J. (2013). Establishing the reliabil-ity of word association data for investigating individual and group differences.Applied Linguistics, 2013, 1–29. doi:10.1093/applin/amt020
Galambos, C., & Curl, A. (2013). Developing gerontological competency: A curricu-lum approach. Gerontology & Geriatrics Education, 34(3), 309–321.
Gonzales, E., Morrow-Howell, N., & Gilbert, P. (2010). Changing medical stu-dents’ attitudes toward older adults. Gerontology & Geriatrics Education, 31(3),220–234.
Harvey, M. M., Coifman, K. G., Ross, G., Kleinert, D., & Giardina, P. (2014).Contextually appropriate emotional word use predicts adaptive health behav-ior: Emotion context sensitivity and treatment adherence. Journal of HealthPsychology, 19(5), 1–11. doi:http://dx.doi.org/10.1177/1359105314532152.
Hayes, L. J., Orchard, C. A., McGillis Hall, L., Nincic, V., O’Brien-Pallas, L., &Andrews, G. (2006). Career intentions of nursing students and new nurse grad-uates: A review of the literature. International Journal of Nursing EducationScholarship, 3(1), 1–15. doi:http://dx.doi.org/10.2202/1548-923x.1281
Henderson, J., Xiao, L., Siegloff, L., Kelton, M., & Paterson, J. (2008). ‘Older peoplehave lived their lives’: First year nursing students’ attitudes towards older people.Contemporary Nurse, 30(1), 32–45.
Hendrie, H. C., Albert, M. S., Butters, M. A., Gao, S., Knopman, D. S., Launer, L.J., . . . Wagster, M. V. (2006). The NIH Cognitive and Emotional Health Project:Report of the Critical Evaluation Study Committee. Alzheimer’s & Dementia,2(1), 12–32.
Herrman, H., Saxena, S., & Moodie, R. (2005). Promoting mental health: con-cepts, emerging evidence, practice: A report of the World Health Organization,Department of Mental Health and Substance Abuse in collaboration withthe Victorian Health Promotion Foundation and the University of Melbourne.Geneva, Switzerland: World Health Organization.
Hoyl, M. T., Alessi, C. A., Harker, J. O., Josephson, K. R., Pietruszka, F. M., Koelfgen,M., . . . Rubenstein, L. Z. (1999). Development and testing of a five-item versionof the Geriatric Depression Scale. Journal of the American Geriatrics Society,47 , 873–878.
IBM Corp. (2012). IBM SPSS Statistics for Mac, V. 21.0. Armonk, NY: Author.Joshi, V. D., Malhotra, R., Lim, J., Ostbye, T., & Wong, M. (2010). Validity
and reliability of the Expectations Regarding Aging (ERA-12) instrumentamong middle-aged Singaporeans. Annals of Academic Medicine Singapore, 39,394–398.
Kogan, N. (1961). Attitudes toward old people: The development of a scale and anexamination of correlates. Journal of Abnormal and Social Psychology, 62(1),44–54. doi:http://dx.doi.org/10.1037/h0048053
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 21
Krout, J. A., & McKernan, P. (2007). The impact of gerontology inclusion on 12thgrade student perceptions of aging, older adults and working with elders.Gerontology & Geriatrics Education, 27(4), 23–40.
Lee, Y. S. (2009). Measures of student attitudes on aging. Educational Gerontology,35(2), 121–134. doi:10.1080/03601270802523577
Levy, B. R. (2009), Stereotype embodiment: A psychosocial approach to aging.Current Directions in Psychological Science, 18, 332–336.
Levy, B. R., & Leifheit-Limson, E. (2009). The stereotype-matching effect: greaterinfluence on functioning when age stereotypes correspond to outcomes.Psychology and Aging, 24(1), 230–233. doi:http://dx.doi.org/10.1037/a0014563.
Levy, B. R., & Myers, L. M. (2004). Preventive health behaviors influenced by self-perceptions of aging. Preventive Medicine, 39(3), 625–629.
Lin, X., Bryant, C., & Boldero, J. (2010). Measures for assessing student attitudestoward older people. Educational Gerontology, 37(1), 12–26. doi:http://dx.doi.org/10.1080/03601270903534796
Lovell, M. (2006). Caring for the elderly: Changing perceptions and attitudes. Journalof Vascular Nursing, 24(1), 22–26. doi:http://dx.doi.org/10.1016/j.jvn.2005.11.001
Lun, M. W. A. (2010). Student knowledge and attitudes toward older people andtheir impact on pursuing aging careers. Educational Gerontology, 37(1), 1–11.doi:10.1080/03601270903534770
Mackenzie, C. S., Gekoski, W. L., & Knox, V. J. (2006). Age, gender, and the under-utilization of mental health services: The influence of help-seeking attitudes.Aging and Mental Health, 10(6), 574–582.
Mayring, P. (2004). Qualitative content analysis. In U. Flick, E. von Kardoff, & I.Steinke (Eds.), A companion to qualitative research (pp. 266–269). London,England: Sage.
McLafferty, I., & Morrison, F. (2004). Attitudes towards hospitalized older adults.Journal of Advanced Nursing, 47(4), 446–453. doi:http://dx.doi.org/10.1111/j.1365-2648.2004.03122.x
Neath, I., & Knoedler, A. J. (1994). Distinctiveness and serial position effects inrecognition and sentence processing. Journal of Memory and Language, 33(6),776–795.
Nolan, M., Davies, S., Brown, J., Wilkinson, A., Warnes, T., McKee, K., . . . Stasi, K.(2008). The role of education and training in achieving change in care homes:A literature review. Journal of Research in Nursing, 13(5), 411–433. doi:http://dx.doi.org/10.1177/1744987108095162
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory (3rd ed.). New York,NY: McGraw-Hill.
Oakes, C. E., & Sheehan, N. W. (2014). Students’ perceptions of a community-based service-learning project related to aging in place. Gerontology & GeriatricsEducation, 35(3), 285–296.
O’Hanlon, A. M., Camp, C. J., & Osofsky, H. J. (1993). Knowledge of and atti-tudes toward aging in young, middle-aged, and older college students: Acomparison of two measures of knowledge of aging. Educational Gerontology:An International Quarterly, 19(8), 753–766. doi:http://dx.doi.org/10.1080/0360127930190806
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

22 M. Pannor Silver et al.
Olson, M. D. (2007). Gerontology content in MSW curricula and student attitudestoward older adults. Educational Gerontology, 33(11), 981–994.
Palmore, E. B. (1977). Facts on aging: A short quiz. The Gerontologist, 17(4),315–320.
Palmore, E. B. (1998). The facts on aging quiz. New York, NY: Springer y.Palmore, E. B. (2001). The ageism survey first findings. The Gerontologist, 41(5),
572–575. doi:http://dx.doi.org/10.1093/geront/41.5.572Ross, L., Duigan, T., Boyle, M., & Williams, B. (2014). Student paramedic atti-
tudes towards the elderly: A cross-sectional study. Australasian Journal ofParamedicine, 11(3), 1–7.
Ross, T. P., Calhoun, E., Cox, T., Wenner, C., Kono, W., & Pleasant, M. (2007).The reliability and validity of qualitative scores for the Controlled Oral WordAssociation Test. Archives of Clinical Neuropsychology, 22(4), 475–488.
Roters, J., Logan, A. J., Meisner, B. A., & Baker, J. (2010). A preliminary study of per-ceptions of aging in athletes and non-athletes. Psychology of Sport and Exercise,11(1), 67–70.
Rothermund, K., & Brandstädter, J. (2003). Coping with deficits and losses in laterlife: from compensatory action to accommodation. Psychology and Aging, 18(4),896–905.
Runkawatt, V., Gustafsson, C., & Engström, G. (2013). Different cultures but similarpositive attitudes: A comparison between Thai and Swedish nursing stu-dents’ attitudes toward older people. Educational Gerontology, 39(2), 92–102.doi:http://dx.doi.org/10.1080/03601277.2012.689934
Sandelowski, M. (1993). Theory unmasked: The uses and guises of theory inqualitative research. Research in Nursing & Health, 16(3), 213–218.
Sandelowski, M., Voils, C. I., & Knafl, G. (2009). On quantitizing. Journal of MixedMethods Research, 3(3), 208–222. doi:10.1177/1558689809334210
Sarkisian, C. A., Hays, R. D., Berry, S., & Mangione, C. M. (2002). Development,reliability, and validity of the Expectations Regarding Aging (ERA-38) survey.The Gerontologist, 42(4), 534–542.
Sarkisian, C. A., Shunkwiler, S. M., Aguilar, I., & Moore, A. A. (2006). Ethnic differ-ences in expectations for aging among older adults. Journal of the AmericanGeriatrics Society, 54(8), 1277–1282.
Sarkisian, C. A., Steers, W. N., Hays, R. D., & Mangione, C. M. (2005). Developmentof the 12-item Expectations Regarding Aging survey. The Gerontologist, 45(2),240–248. doi:http://dx.doi.org/10.1093/geront/45.2.240
Snyder, J. R. (2006). The influence of instruction on college students’ atti-tudes toward older adults. Gerontology & Geriatrics Education, 26(2), 69–79.doi:10.1300/J021v26n02_05
Spiteri, L. F. (2005). Word association testing and thesaurus construction: A pilotstudy. Cataloging & Classification Quarterly, 40(1), 55–78.
Statistics Canada. (2012). The Canadian population in 2011: Population counts andgrowth. Retrieved from http://www12.statcan.ca/census-recensement/2011/as-sa/98-310-x/98-310-x2011001-eng.cfm
Strauss, E., Sherman, E. M., & Spreen, O. (2006). A compendium of neuropsycho-logical tests: Administration, norms, and commentary (3rd ed.). New York, NY:Oxford University Press.
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15

Student Expectations About Mental Health and Aging 23
Stuart-Hamilton, I., & Mahoney, B. (2003). The effect of aging awareness trainingon knowledge of, and attitudes towards, older adults. Educational Gerontology,29(3), 251–260.
Stubblefield, J. L., & Knapp, P. (2000). Changing students’ perceptions of aging:The impact of an intergenerational service learning course. EducationalGerontology, 26(7), 611–621.
Substance Abuse and Mental Health Services Administration. (2007). An actionplan for behavioral health workforce development. Retrieved from http://www.samhsa.gov/Workforce/Annapolis/WorkforceActionPlan.pdf
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics. Boston, MA:Pearson/Allyn & Bacon.
Thorpe, L. (2009). Depression vs. dementia: How do we assess? Canadian Reviewof Alzheimer’s Disease and Other Dementias, 28(1), 17–21.
Vaismoradi, M., Turunen, H., & Bondas, T. (2013). Content analysis and thematicanalysis: Implications for conducting a qualitative descriptive study. Nursing &Health Sciences, 15(3), 398–405.
Villar, F., Fabà, J., & Celdrán, M. (2013). Using older people’s life stories to teachdevelopmental psychology and aging: Benefits and difficulties. EducationalGerontology, 39(12), 867–877. doi:10.1080/03601277.2013.767076
Wang, M., Henkens, K., & van Solinge, H. (2011). Retirement adjustment: A review oftheoretical and empirical advancements. American Psychologist, 66(3), 204–213.
Ware, J. E., Kosinski, M., & Keller, S. D. (1995). SF-12: How to score the SF-12 physicaland mental health summary scales. Second edition. Boston, MA: The HealthInstitute, New England Medical Center.
Woolley, C. M. (2009). Meeting the mixed methods challenge of integration in asociological study of structure and agency. Journal of Mixed Methods Research,3(1), 7–25.
Yarkoni, T. (2010). Personality in 100,000 words: A large-scale analysis of person-ality and word use among bloggers. Journal of Research in Personality, 44(3),363–373. doi:http://dx.doi.org/10.1016/j.jrp.2010.04.001
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 1
0:19
29
Apr
il 20
15