Strategic planning processes and financial performance among hospitals in Lebanon
12
Strategic planning processes and financial performance among hospitals in Lebanon Shadi Saleh 1 *, Amer Kaissi 2 , Adele Semaan 1 and Nabil Maher Natafgi 1 1 American University of Beirut, Department of Health Management & Policy, Beirut, Lebanon 2 Department of Health Care Administration, Trinity University, San Antonio, Texas United States ABSTRACT Background Strategic planning has been presented as a valuable management tool. How- ever, evidence of its deployment in healthcare and its effect on organizational performance is limited in low-income and middle-income countries (LMICs). The study aimed to explore the use of strategic planning processes in Lebanese hospitals and to investigate its association with financial performance. Methods The study comprised 79 hospitals and assessed occupancy rate (OR) and revenue- per-bed (RPB) as performance measures. The strategic planning process included six domains: having a plan, plan development, plan implementation, responsibility of planning activities, governing board involvement, and physicians’ involvement. Results Approximately 90% of hospitals have strategic plans that are moderately developed (mean score of 4.9 on a 1–7 scale) and implemented (score of 4.8). In 46% of the hospitals, the CEO has the responsibility for the plan. The level of governing board involvement in the pro- cess is moderate to high (score of 5.1), whereas physician involvement is lower (score of 4.1). The OR and RPB amounted to respectively 70% and 59 304 among hospitals with a strategic plan as compared with 62% and 33 564 for those lacking such a plan. No statistical association between having a strategic plan and either of the two measures was detected. However, the findings revealed that among hospitals that had a strategic plan, higher implementation levels were associated with lower OR (p < 0.05). Conclusions In an LMIC healthcare environment characterized by resource limitation, complex- ity, and political and economic volatility, flexibility rather than rigid plans allow organizations to better cope with environmental turbulence. Copyright © 2012 John Wiley & Sons, Ltd. KEY WORDS: strategic planning; hospital performance; low-income and middle-income countries BACKGROUND Strategic planning is the set of organizational processes that help an organization identify its desired future and develop its decision-making guidelines. When organi- zational decisions exhibit a logical consistency over time, the organization is said to have a “strategy,” which represents the means chosen to move from the current state *Correspondence to: S. Saleh, Department of Health Management & Policy, American University of Beirut, Riad El Solh, Beirut, Lebanon. E-mail: [email protected] Copyright © 2012 John Wiley & Sons, Ltd. THE INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT Int J Health Plann Mgmt 2013; 28: e34–e45. Published online 1 August 2012 in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/hpm.2128
Transcript of Strategic planning processes and financial performance among hospitals in Lebanon

THE INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT
Int J Health Plann Mgmt 2013; 28: e34–e45.Published online 1 August 2012 in Wiley Online Library(wileyonlinelibrary.com) DOI: 10.1002/hpm.2128
Strategic planning processes and financialperformance among hospitals in Lebanon
Shadi Saleh1*, Amer Kaissi2, Adele Semaan1 and Nabil Maher Natafgi11American University of Beirut, Department of Health Management & Policy, Beirut, Lebanon2Department of Health Care Administration, Trinity University, San Antonio, Texas United States
ABSTRACT
Background Strategic planning has been presented as a valuable management tool. How-ever, evidence of its deployment in healthcare and its effect on organizational performanceis limited in low-income and middle-income countries (LMICs). The study aimed to explorethe use of strategic planning processes in Lebanese hospitals and to investigate its associationwith financial performance.Methods The study comprised 79 hospitals and assessed occupancy rate (OR) and revenue-per-bed (RPB) as performance measures. The strategic planning process included sixdomains: having a plan, plan development, plan implementation, responsibility of planningactivities, governing board involvement, and physicians’ involvement.Results Approximately 90% of hospitals have strategic plans that are moderately developed(mean score of 4.9 on a 1–7 scale) and implemented (score of 4.8). In 46% of the hospitals, theCEO has the responsibility for the plan. The level of governing board involvement in the pro-cess is moderate to high (score of 5.1), whereas physician involvement is lower (score of 4.1).The OR and RPB amounted to respectively 70% and 59 304 among hospitals with a strategicplan as compared with 62% and 33 564 for those lacking such a plan. No statistical associationbetween having a strategic plan and either of the two measures was detected. However, thefindings revealed that among hospitals that had a strategic plan, higher implementation levelswere associated with lower OR (p< 0.05).Conclusions In an LMIC healthcare environment characterized by resource limitation, complex-ity, and political and economic volatility, flexibility rather than rigid plans allow organizations tobetter cope with environmental turbulence. Copyright © 2012 John Wiley & Sons, Ltd.
KEY WORDS: strategic planning; hospital performance; low-income and middle-income countries
BACKGROUND
Strategic planning is the set of organizational processes that help an organizationidentify its desired future and develop its decision-making guidelines. When organi-zational decisions exhibit a logical consistency over time, the organization is said tohave a “strategy,” which represents the means chosen to move from the current state
*Correspondence to: S. Saleh, Department of Health Management & Policy, American University ofBeirut, Riad El Solh, Beirut, Lebanon. E-mail: [email protected]
Copyright © 2012 John Wiley & Sons, Ltd.

e35STRATEGIC PLANNING PROCESSES AND FINANCIAL PERFORMANCE
to the desired future state. Using strategy, the organization can build on its strengths,address its weaknesses, exploit environmental opportunities, and avoid environmen-tal threats (Swayne et al., 2006). Therefore, strategic planning is commonly believedto be a key ingredient for high performance and organizational success.
The empirical relationship between strategic planning and organizational perfor-mance is, however, not that straightforward. In general industry, numerous studieshave reported a positive association between strategic planning and performance(Rhyne, 1986; Delmar and Shane, 2003; Glaister et al., 2008), whereas othersargued that such a relationship does not exist (Shrader et al., 1984; Pearceet al., 1987). In healthcare, most research on strategic planning is limited to casestudies and small samples and does not link strategic planning to organizationalperformance (Dubbs and Organization design consistency, 2002; Lemak andGoodrick, 2003; Wells et al., 2004). Still, there are few exceptions. A nationalstudy of the association between employing strategic initiatives and performanceof rural hospitals detected no association between the two (Mick et al., 1994).However, more recently, Kaissi and Begun (2008) examined the associationamong Texas hospitals and reported a favorable finding, whereas Delgado andLangabeer (2009) found that cancer centers that deploy strategic controlapproaches have better financial performance compared with their counterpartsthat do not.
Evidence of deployment of strategic planning in low-income and middle-income countries (LMICs) is rare (El-Jardali et al., 2007). This is noteworthybecause, relative to high-income countries, the healthcare environment in LMICis more complex, dynamic, and challenging (Mills et al., 2002), whereasresources are generally more limited. As such, the perceived need for strategicplanning should be high. Still, strategic planning in LMICs, if present, is set atthe national governmental level, with limited evidence of its employment anduse at the organizational level (Mostafa et al., 2004).
Lebanon is an LMIC located in the eastern Mediterranean region. TheLebanese healthcare system is pluralistic and fragmented because of the public–private mix involved in the financing and provision of health services as wellas the lack of coordination among the multiple financing and delivery systems.By the end of the 15-year civil war that started in 1975, the government startedstrengthening the public hospital sector to match the significant expansion ofthe private sector during war years. Since then, efforts have been dedicated toexpanding the number of public hospitals. As a result, the number of publichospitals increased from 12 in 1990 to 29 hospitals in 2011 (Ammar, 2009). Thismodified the public–private delivery mix that was predominantly private prior to1990. In addition, serious concerns related to financial performance due to majorinefficiencies, non-sustainable cost explosion (Lerberghe et al., 1997), and continuousmodifications of reimbursement schemes exist. More specifically, the financingmechanisms of hospital care are fragmented. There is a mix of healthcarefunding sources that include several public funds, as well as private insuranceschemes and out-of-pocket expenditures. Each of these sources has its ownbenefit packages, fee scales, and individual agreements with healthcare providers,tutelage authority, and financing intermediaries.
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

e36 S. SALEH ET AL.
Although the Lebanese healthcare system, with its complex and mixed setting ofprivate–public mix in delivery and financing, may share some similarities with theAmerican healthcare system, it is still a very unique system, especially when theconstant economic and political turmoil of the country is considered. Given thiscomplexity, hospitals in Lebanon can arguably benefit from strategic planning toalleviate the adverse impact of uncertainty in their environments and steer theiroperations towards improved performance (Begun and Kaissi, 2004). It is importantto note that as a requirement of the Lebanese national accreditation system whichstarted in 2002, hospitals are required to have a “five-year strategic plan [. . .] thatindicates future directions/initiatives for the hospital. . .” with advisory input fromthe Senior Management (MoPH, 2009).Although having a strategic plan is an overarching national health initiative, this
study went beyond the requirement of having a strategic plan to assessing the actualprocess and identifying the stakeholders involved in the strategic planning withinhospitals. The primary aims of this study are to explore the extent of use of thesestrategic planning processes in Lebanese hospitals and to investigate its associationwith financial performance. Although prior studies have examined this relationship,most were focused/based on industrialized countries.
CONCEPTUAL FRAMEWORK
Against this context, common strategic planning theories and hypothesis that arepromoted in the health administration literature and/or supported by particular orga-nizational concepts were studied. The first hypothesis relates to the organizationalenvironment impact on the strategic plan. Structural contingency theory argues thatorganizational structures need to be compatible with changes in the environment(Donaldson, 2001). A thorough and accurate assessment of environmental factorsis strongly enhanced by strategic planning. Institutional theory, on the other hand,posits that having a formal strategic plan is important because it allows the organiza-tion to gain legitimacy in the eyes of its important stakeholders, such as accreditingagencies and community organizations (Scott, 2000). Healthcare leaders seem toagree with these perspectives and argue that strategic planning is a key value-addedfunction of leadership in their organizations (Begun and Kaissi, 2005). Therefore, wehypothesize that the existence of a strategic plan is favorably associated with hospitalperformance (Hypothesis 1).The development of a strategic plan ideally involves a process that builds upon
assessments of external and internal environments as foundations. On the basis offindings from these assessments, a strategic map is drawn with goals, objectives,and strategic thrust. The Baldrige National Quality Program (2006) criteria for stra-tegic planning present a roadmap for ultimate strategic planning processes. Studieshave shown that not conforming to a well-defined comprehensive process may leadto negative performance (Veliyath and Shortell, 1993). In addition, the strategicplanning process should adapt an integrative approach, whereby the processes ofplanning and implementing strategies are combined in order to achieve long-termsuccess (Kohtamaki et al., 2010). As previously mentioned, this is a main assumption
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

e37STRATEGIC PLANNING PROCESSES AND FINANCIAL PERFORMANCE
in the structural contingency theory and has been highlighted by many (Bossidy et al.,2002; Begun and Kaissi, 2005). Implementation of strategic plans is obviously a keycomponent in its success, which mirrors that of the organization. Therefore, wehypothesize that a more developed strategic plan is positively associated with hospitalperformance (Hypothesis 2) and that implementation of the strategic plan is positivelyassociated with hospital performance (Hypothesis 3).
The responsibility of leading the strategic planning process and who should beinvolved in it vary by organization. It has been argued that strategic planning isprimarily the CEO’s job (Langely, 1988). Although in large organization, such afunction is delegated to a Deputy Director/Vice President for planning or to a strate-gic planning committee, recent evidence shows that maintaining this function in theCEO hands is associated with better performance (Kaissi and Begun, 2008). There-fore, we hypothesize that CEO control of the strategic planning process is positivelyassociated with hospital performance (Hypothesis 4).
The process of strategic planning would ideally involve all levels of managementand operations within organizations. Nevertheless, the board of trustees of an orga-nization has the primary responsibility of performing the strategic planning. Theboard should play an active role in this extensive planning process by establishingkey policy targets (Cleverley and Cameron, 2007). Studies have shown a positivecorrelation between governing board involvement and hospital performance (Kaissiand Begun, 2008). As such, we hypothesize that the level of governing boardinvolvement in the strategic planning process is positively associated with hospitalperformance (Hypothesis 5). In addition to the governing board, physicians arekey stakeholders in any healthcare organization. Involving physicians in the strategicplanning process from the early stages will engage them more as a group in itssuccess. Many have advocated for a partnership with physicians in the strategic plan-ning process to ensure success and enhanced performance (Alexander, 2006). There-fore, we hypothesize that the level of physician involvement in the strategic planningprocess is positively associated with hospital performance (Hypothesis 6).
METHODS
Study population
The study population comprised 119 private and 29 public acute care hospitals inLebanon. Eight public hospitals were not eligible to participate because these facil-ities were still not fully operational (recently built/renovated and in the process ofbeing equipped or governing structure has not been finalized). The total number ofrespondents was 79 hospitals (completing the strategic planning sections) represent-ing a response rate of 56.4%. This response rate compares very favorably with otherstudies employing voluntary surveying of senior healthcare organizations’ adminis-tration; the response rates of such studies ranged from 26% to 44% (Kaissi andBegun, 2008). Examining respondents and non-respondents revealed that bothgroups were similar on hospital characteristics examined with only one difference;
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

e38 S. SALEH ET AL.
all teaching hospitals in Lebanon (n = 5) responded to the survey and hence wereincluded. Ethical approval for the study was granted by the American Universityof Beirut Institutional Review Board.
Data sources
The study has two main data sources. The first comprised a survey conductedbetween October 2009 and September 2010 that collected data on strategic planningactivities and hospital performance measures and was completed by hospital admin-istration. For the hospital performance measures, the data reported by the hospitalswere validated (revenues-per-bed (RPBs)) by data from the Ministry of PublicHealth (MoPH). MoPH databases were also used to extract information on hospitalcharacteristics (ownership, teaching status, accreditation status, and bed size).The process of data collection was initiated by a letter faxed/e-mailed to the
hospital CEO outlining the purpose of the study and associated activities. In thefollowing 2 days, phone calls were made to the hospitals to ensure that the letterwas received and inquiring whether they are willing to complete the survey. If theresponse was positive, hospitals were asked about the best day/time to deliver thesurvey to the hospital CEO. Upon delivering the survey, hospitals were asked aboutthe time needed to complete the survey. On that pre-specified date, a call was placedto the CEO office to make sure that the survey was completed. Once informed of itscompletion, a private courier company was directed to pick up the survey. If theCEO indicated that she or he does not wish to complete the survey or 14 days passedwithout filling the survey (even after reminders), the hospital was considered as anon-respondent site.
Study variables
The main dependent variables measured hospital performance. The measures usedincluded occupancy rate (OR) and revenue per bed (RPB). OR presents as an industry-specific measure, commonly employed in health services research as an indicatorof hospital performance. High hospital OR, usually implying a high market demand,has been cited to increase prospects of profitability (Burns et al., 2000). Furthermore,a study by Younis et al. (2006), on hospital financial performance in the USA,reveals that OR is a factor influencing efficiency, profitability, and liquidity, withinthe hospital industry, and, thus, a key predictor of financial performance. Specificallyin Lebanon, OR has been a focus of many hospitals in the past 10 years since theLebanese MoPH has aggressively pursued the opening of public hospitals resultingin additional supplies of beds across high-demand regions of the country. Thisgovernmental intervention decreased the MoPH subsidized admission from 86% to73%, causing alarm for the hospitals concerning efficiency and achieving economiesof scale (Ammar, 2009). From that perspective, hospitals became concerned aboutthe effect of strategic policy decisions on OR within the hospitals.Net patient RPB, which is calculated by dividing the net patient revenue for a
hospital by the number of beds, has been cited as indicative of an institution’scompetitive power in attracting patients and staffing its beds (Smith et al., 2006).In relation to OR concern (see preceding discussions) and the fact that most hospitals
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

e39STRATEGIC PLANNING PROCESSES AND FINANCIAL PERFORMANCE
have a present revenue ceiling from the MoPH (the predominant payer of hospitalservices in Lebanon) (Kronfol, 2006), RPB became a key financial performanceindicator for the financial wellbeing and survival of many hospitals especially inlight of the decrease in number of contracts of hospitals with MoPH and limits onthe yearly ceiling (Ammar, 2009). It is worth noting that outlier values on both finan-cial performance measures were removed from the analysis. The other alternativeexplored was log transformation; however, this did not result in the normalizationof the measures.
The strategic planning process characteristics were derived from those employedby Kaissi and Begun (2008). These included six domains, each measured with asingle variable. They included (i) having a strategic plan; (ii) extent of strategic plandevelopment (scale of 1–7, based on Baldrige criteria); (iii) extent of strategic planimplementation (scale of 1–7, based on Baldrige criteria); (iv) responsibility of stra-tegic planning activities (CEO vs Other); (v) extent of governing board involvementin strategic planning activities (scale of 1–7) and; (vi) extent of physicians’ involve-ment in strategic planning activities (scale of 1–7). Other study variables includedhospital characteristics. These were ownership (public, private not-for-profit, andprivate for-profit), teaching status, bed size, and accreditation status. The latter is aclassification employed by the MoPH, and it is indicative of the service and qualitysophistication of the facility with classification A as the highest designation.
Data analysis
Univariate analysis was used to describe hospital characteristics and performance.The association between the independent variables and between these and the depen-dent variables was examined using Student t-tests and chi-square testing. Multivari-ate modeling was also employed to examine the effect of independent and controlvariables on hospital performance. Separate models were constructed for each ofthe two performance measures. The models were two levels. The first level includedthe availability of a strategic plan as the main independent variable whereas thesecond-level models included strategic planning characteristics and processes asmain independent variables among hospital that had a strategic plan. Before conduct-ing each of the models, tests examined the collinearity among all covariates in themodel. If correlation among covariates was significant and higher than 0.40, adecision was made on which of the correlated variables are kept in the model.Collinearity was detected among the four variables: extent of strategic plan imple-mentation, extent of strategic plan development, level of governing board involve-ment in strategic plan development, and level of physician involvement instrategic plan development. The authors decided to include extent of implementationin the model for three reasons: (i) the relation between extent of implementation andoccupancy was significant in the bivariate analysis, and we wanted to investigatewhether such a strong association would persist after controlling for other variables;(ii) including the variable on whether the CEO was solely responsible for strategicplan development versus with others can be considered as a proxy of level of govern-ing board and physician involvement in strategic plan development, that is, if she orhe is solely responsible, which may indicate a smaller role for the governing board
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

e40 S. SALEH ET AL.
and physicians; and (iii) we would have liked to include extent of strategic plandevelopment variable to measure its independent effect on occupancy. However,the variable was the most correlated with extent of implementation at 0.69. Hence,the authors decided to include extent of implementation because of its relevanceand the support of the literature of its critical role. It is also worth noting that almostall public hospitals had no accreditation classification, so public ownership wasdropped from the regression models.
FINDINGS
Hospital characteristics and strategic planning processes
More than three-fifths of hospital respondents (62.3%) were private-for-profit withfive hospitals (6.3%) classified as teaching hospitals (academic medical centers)(Table 1). The average number of beds was 106.5. The majority of hospitals wereclassified as C (44.6%)—classification is dependent on accreditation guidelines bythe MoPH; “A” classification is for large general hospitals that have a clinicaleducation component whereas “D” is for small hospitals with limited specialties.In terms of hospital performance, the average OR was 69.8% with average RPB of$56 200/year.Approximately 90% of Lebanese hospitals have a strategic plan. Strategic plans
are moderately developed (mean score of 4.9 on a 1–7 scale) and moderately imple-mented (mean score of 4.8 on a similar scale). In 46% of the hospitals, the CEO hasthe responsibility for the strategic plan. The level of involvement of the governingboard in the strategic planning process is moderate to high (mean score of 5.1 on a1–7 scale), whereas not surprisingly the level of physician involvement is lower(mean score of 4.1 on a similar scale).
Association between strategic planning processes and hospital performance
The bivariate association between strategic planning process and hospital perfor-mance revealed that extent of strategic plan implementation was adversely relatedto OR, that is, the more a hospital implemented its strategic plan, the lower its OR(p< 0.05) (Table 2). A similar trend was observed with level of governing boardinvolvement in strategic plan development. The multivariate modeling revealed noassociation between having a strategic plan and either of the two performance mea-sures (Table 3). However, the findings revealed that, among hospitals that had a stra-tegic plan, higher implementation levels were associated with lower ORs (p< 0.05).
DISCUSSION AND CONCLUSION
The goal of the study was to assess the association between strategic planning andhospital financial performance. However, the findings did not lend support to thehypotheses that argued for a favorable association between existence of strategicplanning and its processes and financial performance. On the contrary, there was
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm
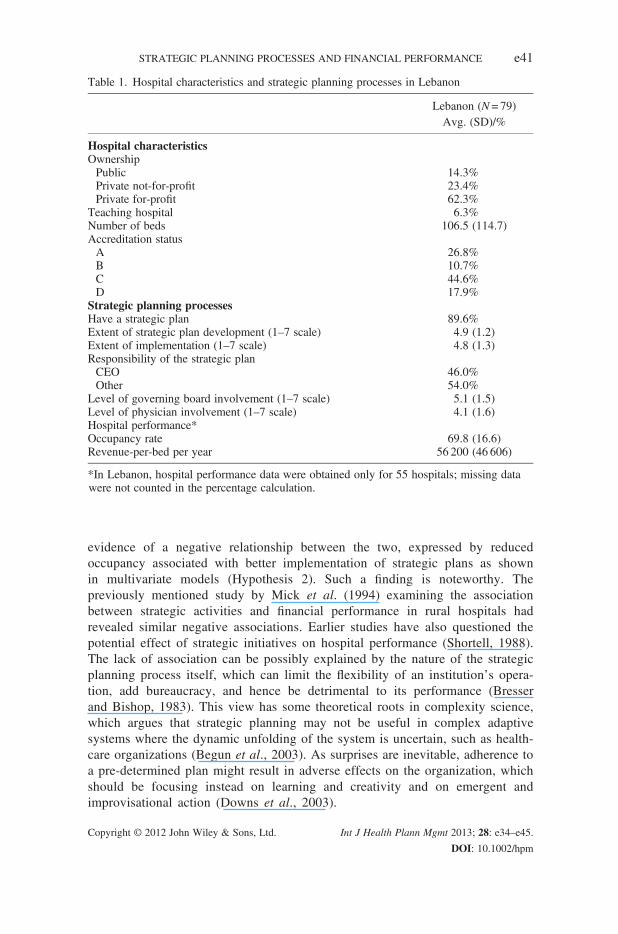
Table 1. Hospital characteristics and strategic planning processes in Lebanon
Lebanon (N= 79)Avg. (SD)/%
Hospital characteristicsOwnershipPublic 14.3%Private not-for-profit 23.4%Private for-profit 62.3%
Teaching hospital 6.3%Number of beds 106.5 (114.7)Accreditation statusA 26.8%B 10.7%C 44.6%D 17.9%
Strategic planning processesHave a strategic plan 89.6%Extent of strategic plan development (1–7 scale) 4.9 (1.2)Extent of implementation (1–7 scale) 4.8 (1.3)Responsibility of the strategic planCEO 46.0%Other 54.0%
Level of governing board involvement (1–7 scale) 5.1 (1.5)Level of physician involvement (1–7 scale) 4.1 (1.6)Hospital performance*Occupancy rate 69.8 (16.6)Revenue-per-bed per year 56 200 (46 606)
*In Lebanon, hospital performance data were obtained only for 55 hospitals; missing datawere not counted in the percentage calculation.
e41STRATEGIC PLANNING PROCESSES AND FINANCIAL PERFORMANCE
evidence of a negative relationship between the two, expressed by reducedoccupancy associated with better implementation of strategic plans as shownin multivariate models (Hypothesis 2). Such a finding is noteworthy. Thepreviously mentioned study by Mick et al. (1994) examining the associationbetween strategic activities and financial performance in rural hospitals hadrevealed similar negative associations. Earlier studies have also questioned thepotential effect of strategic initiatives on hospital performance (Shortell, 1988).The lack of association can be possibly explained by the nature of the strategicplanning process itself, which can limit the flexibility of an institution’s opera-tion, add bureaucracy, and hence be detrimental to its performance (Bresserand Bishop, 1983). This view has some theoretical roots in complexity science,which argues that strategic planning may not be useful in complex adaptivesystems where the dynamic unfolding of the system is uncertain, such as health-care organizations (Begun et al., 2003). As surprises are inevitable, adherence toa pre-determined plan might result in adverse effects on the organization, whichshould be focusing instead on learning and creativity and on emergent andimprovisational action (Downs et al., 2003).
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm
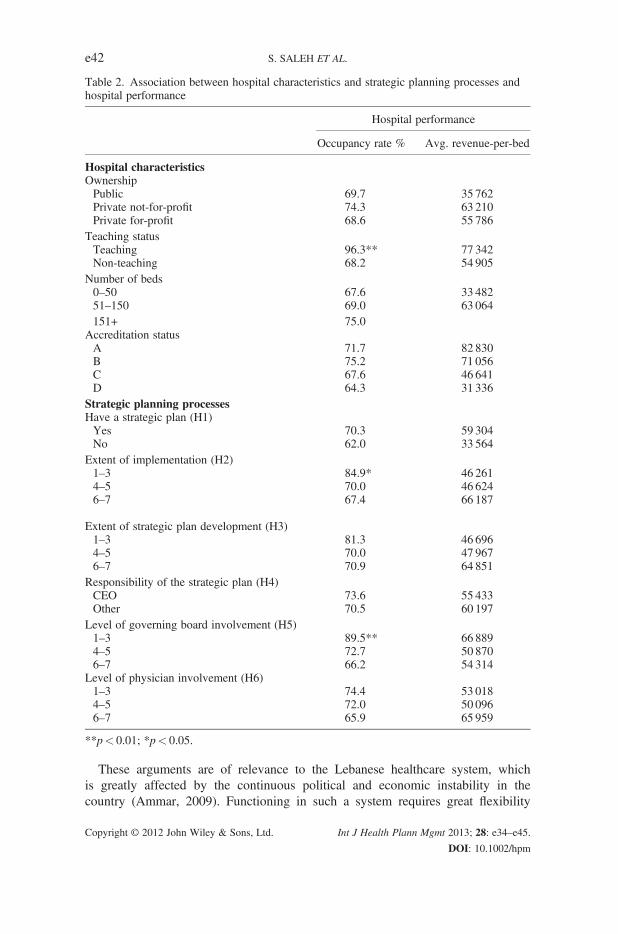
Table 2. Association between hospital characteristics and strategic planning processes andhospital performance
Hospital performance
Occupancy rate % Avg. revenue-per-bed
Hospital characteristicsOwnershipPublic 69.7 35 762Private not-for-profit 74.3 63 210Private for-profit 68.6 55 786
Teaching statusTeaching 96.3** 77 342Non-teaching 68.2 54 905
Number of beds0–50 67.6 33 48251–150 69.0 63 064151+ 75.0
Accreditation statusA 71.7 82 830B 75.2 71 056C 67.6 46 641D 64.3 31 336
Strategic planning processesHave a strategic plan (H1)Yes 70.3 59 304No 62.0 33 564
Extent of implementation (H2)1–3 84.9* 46 2614–5 70.0 46 6246–7 67.4 66 187
Extent of strategic plan development (H3)1–3 81.3 46 6964–5 70.0 47 9676–7 70.9 64 851
Responsibility of the strategic plan (H4)CEO 73.6 55 433Other 70.5 60 197
Level of governing board involvement (H5)1–3 89.5** 66 8894–5 72.7 50 8706–7 66.2 54 314
Level of physician involvement (H6)1–3 74.4 53 0184–5 72.0 50 0966–7 65.9 65 959
**p< 0.01; *p< 0.05.
e42 S. SALEH ET AL.
These arguments are of relevance to the Lebanese healthcare system, whichis greatly affected by the continuous political and economic instability in thecountry (Ammar, 2009). Functioning in such a system requires great flexibility
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

Table 3. Multivariate models
Model 1occupancy rate
Model 2revenue-per-bed
Unstandardizedcoefficient
Standarderror
Unstandardizedcoefficient
Standarderror
Level 1Hospital characteristicsOwnershipPublic Reference ReferencePrivate for-profit �5.8 9.0 5309 14 021
Number of beds 0.0 0.1 �58 90Accreditation statusA 0.0 13.0 62 063 20 301**B 9.1 12.5 43 108 19 414*C 3.4 9.9 6043 15 731D Reference Reference
Have a strategic plan 12.7 13.4 12 912 20 979R2 0.08 0.46
Level 2 (have a strategic plan)Hospital characteristicsOwnershipPublic Reference — ReferencePrivate for-profit 10.1 8.1 �4561 13 441
Number of beds �0.05 0.07 �135 110Accreditation statusA �19.1 13.8 65 955* 23 113B �14.5 13.6 39 432 22 612C �32.2 12.3* �9645 20 878D Reference Reference
Strategic planning processesResponsibility of thestrategic planCEO 0.3 5.8 �7858 10 450Other Reference Reference
Extent ofimplementation1–3 Reference Reference4–5 �27.2 9.7* �11 304 18 5916–7 �22.0 9.9* 9403 18 179
R2 0.40 0.70
*p< 0.05; **p< 0.01.
e43STRATEGIC PLANNING PROCESSES AND FINANCIAL PERFORMANCE
and may penalize institutions that develop and adopt long-term strategic initia-tives. Therefore, hospital administrators are advised to adopt a short-term flexibleplanning process with limited resource investments (and immediate returns), as itmay be more suitable in such an environment and arguably associated with betterperformance. This is echoed in a recent study that showed that flexibility is animportant mediator in the relationship between strategic planning and performance(Rudd et al., 2008).
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

e44 S. SALEH ET AL.
Moreover, as previously discussed, hospitals in Lebanon are required to have astrategic plan in order to qualify for accreditation by the MOPH. Therefore, havinga strategic plan may be more of an action to fulfill accreditation requirements than toactually improve hospital performance. This is highlighted by the fact that althoughthe majority of the hospitals report having a strategic plan, the levels of developmentand implementation of the plan are moderate at best, which is critical for success andfavorable outcomes.Another possible explanation of the findings relates to the cross-sectional nature
of the data. Given that the dependent variable (financial performance) and indepen-dent variables (strategic planning processes) were reported by the same respondentsat the same time, it is possible that hospitals that are concerned about their negativefinancial performance have decided to develop a strategic plan in order to improvetheir performance and to obtain accreditation from the MOPH (with its addedbenefits of access to financial contracts). Therefore, a more longitudinal assessmentof the relationship may be more appropriate in the future.Two limitations for this study warrant consideration. The first lies in the fact that
our results are based on the perception of hospital administrators. Although there isno reason to assume inaccuracy, underreporting of revenues remains a potentialconcern. Second, several private hospitals are family owned. A number of governingboard members and medical administrators would be family members and concur-rently involved in all aspects of the organization’s operation. In these institutions,it would have been challenging to respond to survey items related to the levelof involvement.In conclusion, it remains true that organizations with the most environmentally
adequate strategies usually perform best, both financially and operationally (Goldsteinet al., 2002). This study has argued that the fixed element is sensitivity to the environmen-tal context and the variable element is planning characteristics and processes. In an LMIChealthcare environment characterized by resource limitation, complexity, and politicaland economic volatility, flexibility rather than rigid plans seem to better allow organiza-tions to cope with environmental turbulence. By staying flexible, organizations can antic-ipate changes in real time and allocate resources accordingly.
ACKNOWLEDGEMENTS
The authors have no competing interests, financial or non-financial, in relation to thepublication of the manuscript. Funding was obtained through an American Universityof Beirut University Research Board grant.
REFERENCES
Alexander K. 2006. Advancing strategic planning. Front
Health Serv Manage 23: 39–41.
Ammar W. 2009. Health beyond Politics. WHO Eastern
Mediterranean Regional Office: Beirut, Lebanon.
Copyright © 2012 John Wiley & Sons, Ltd.
Baldrige National Quality Program. 2006. Health
Care Criteria for Performance Excellence.
National Institute of Standards and Technology:
Gaithersburg, MD.
Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm

e45STRATEGIC PLANNING PROCESSES AND FINANCIAL PERFORMANCE
Begun JW, Kaissi AA. 2004. Uncertainty in health care
environments: myths or reality. Health Care Manage Rev
29: 31–39.
Begun JW, Kaissi AA. 2005. An exploratory study of health-
care strategic planning in twometropolitan areas. JHealthc
Manag 50: 264–275.
Begun JW, Zimmerman B, Dooley KJ. 2003. Health care
organizations as complex adaptive systems. In
Advances in Health Care Organization Theory, Mick SS,
WyttenbackME (eds). Jossey-Bass: San Francisco; 253–88.
BossidyL, CharanR, BurckC. 2002.Execution: TheDiscipline
of Getting Things Done. Crown Business: New York.
Bresser RK,BishopRC. 1983. Dysfunctional effects of formal
planning: two theoretical explanations. Acad Manage Rev
8: 588–99.
Burns L, Bazzoli G, Dyan L, Wholey D. 2000. Physician–
hospital strategic alliances. Health Serv Res 35: 101–132.
Cleverley WO, Cameron AE. 2007. Essentials of Healthcare
Finance. Jones & Bartlett Learning: Sudbury, Massachusetts.
Delgado RI, Langabeer JR. 2009. Strategic performance eval-
uation in cancer centers. J Healthc Manag 54: 369–381.
Delmar F, Shane S. 2003. Does business planning facili-
tate the development of new ventures? Strateg Manag
J 24: 1165–1185.
Donaldson L. 2001. The Contingency Theory of Organi-
zations. Sage: Thousand Oaks, CA.
Downs A, Durant R, Carr AN. 2003. Emergent strategy
development for organizations. Emergence 5: 5–28.
Dubbs NL, Organization design consistency. 2002. The
PennCARE and Henry Ford health system experi-
ences. J Healthc Manag 47: 307–318.
El-Jardali F, Jamal D, Abdallah A, Kassak K. 2007. Human
resources for health planning and management in the
Eastern Mediterranean Region: facts, gaps and forward
thinking for research and policy.HumResourHeal 5: 9–20.
Glaister KW, Dincer O, Tatoglu E, Demirbag M, Zaim S.
2008. A causal analysis of formal strategic planning and
firm performance: evidence from an emerging country.
Manag Decis 46: 365–391.
Goldstein S, Ward P, Leong G, Butler T. 2002. The effect of
location, strategy, and operations technology on hospital
performance. J Oper Manag 20: 63–75.
Kaissi AA, Begun JW. 2008. Strategic planning processes
and hospital financial performance. J Healthc Manag
53: 197–208.
KronfolN. 2006. Rebuilding of the Lebanese healthcare system:
health sector reforms. East Mediterr Health J 12: 459–472.
Kohtamaki M, Kautonen T, Kraus S. 2010. Strategic plan-
ning and small business performance. Entrepreneurship
and Innovation 11: 221–229.
Langely A. 1988. The roles of formal strategic planning.
Long Range Plann 21: 40–50.
Lemak CH, Goodrick E. 2003 Strategy as simple rules:
understanding success in a rural clinic. Health Care
Manage Rev 28: 179–188.
Copyright © 2012 John Wiley & Sons, Ltd.
Lerberghe WV, Ammar W, Rashidi RE, Sales A, Mechbal
A. 1997. Reform follows failure: unregulated private care
in Lebanon. Health Policy Plan 12: 296–311.
Mick SS, Morlock LL, Salkever DG, Malitz F, Wise CG,
Jones A. 1994. Strategic activity and financial perfor-
mance of U.S. rural hospitals: a national study, 1983 to
1988. J Rural Health 10: 150–167.
Mills A, Brugha R, Hanson K, McPake B. 2002. What can
be done about the private health sector in low-income
countries. Bull World Health Organ 80:325–330.
Ministry of Public Health (MoPH). 2009. Lebanese
National Hospital Accreditation System Standards.
Standard GB1—Governing Body & Management.
Haute Autorité De Sante (France) and Ministry of Public
Health (Lebanon). http://www.moph.gov.lb/Hospital-
Accreditation/Old/Pages/LesGrillesdeDiagnostic.aspx
Accessed on 28 June 2012.
Mostafa MM, Sheaff R, Morris M, Ingham V. 2004. Strate-
gic preparation for crisis management in hospitals:
empirical evidence from Egypt. Disaster Prevention
and Manag 13: 399–408.
Pearce JAI, Freeman EB, Robinson JRB. 1987. The tenuous
link between formalized strategic planning and financial
performance. Acad Manage Rev 12: 658–75.
Rhyne LC. 1986. The relationship of strategic planning to
financial performance. Strategic Manage J 7: 423–36.
Rudd JM, Greenley GE, Beatson AT, Lings IN. 2008.
Strategic planning and performance: extending the
debate. J Bus Res 61: 99–108.
Scott WR. 2000. Institutions and Organizations. Sage:
Thousand Oaks, CA.
Shortell SM. 1988. The evolution of hospital systems:
unfulfilled promises and self-fulfilling prophesies.
Medical Care Review 45: 177–214.
Shrader CB, Taylor L, Dalton DR. 1984. Strategic
planning and organizational performance: a critical
appraisal. J Manag 10: 149–171.
Smith A, Houghton S, Hood J, Ryman J. 2006. Power rela-
tionships among top managers: does top management
team power distribution matter for organizational perfor-
mance? J Bus Res 59: 622–629.
Swayne LE, Duncan JE, Ginter PM. 2006. Strategic
Management of Health Care Organizations. Blackwell
Publishing: Malden, MA.
Veliyath R, Shortell S. 1993. Strategic orientation, strategic
planning system characteristics and performance. J Manag
Stud 30: 359–381.
Wells R, Lee SD, McClure J, Baronner L, Davis L. 2004.
Strategy development in small hospitals: stakeholder
management in constrained circumstances. Health Care
Manage Rev 29: 218–228.
Younis MZ, Younies HZ, Okojie F. 2006. Hospital financial
performance in the United States of America: a follow-
up study. La Revue de Sante de laMediterranee Orientale
12: 670–678.
Int J Health Plann Mgmt 2013; 28: e34–e45.
DOI: 10.1002/hpm