Stem Cell Therapy for Arterial Restenosis: Potential Parameters Contributing to the Success of Bone...
21
After online publication, subscribers (personal/institutional) to this journal will have access to the complete article via the DOI using the URL: If you would like to know when your article has been published online, take advantage of our free alert service. For registration and further information, go to: http://www.springerlink.com. Due to the electronic nature of the procedure, the manuscript and the original figures will only be returned to you on special request. When you return your corrections, please inform us, if you would like to have these documents returned. Dear Author Here are the proofs of your article. • You can submit your corrections online, via e-mail or by fax. • For online submission please insert your corrections in the online correction form. Always indicate the line number to which the correction refers. • You can also insert your corrections in the proof PDF and email the annotated PDF. • For fax submission, please ensure that your corrections are clearly legible. Use a fine black pen and write the correction in the margin, not too close to the edge of the page. • Remember to note the journal title, article number, and your name when sending your response via e-mail or fax. • Check the metadata sheet to make sure that the header information, especially author names and the corresponding affiliations are correctly shown. • Check the questions that may have arisen during copy editing and insert your answers/corrections. • Check that the text is complete and that all figures, tables and their legends are included. Also check the accuracy of special characters, equations, and electronic supplementary material if applicable. If necessary refer to the Edited manuscript. • The publication of inaccurate data such as dosages and units can have serious consequences. Please take particular care that all such details are correct. • Please do not make changes that involve only matters of style. We have generally introduced forms that follow the journal’s style. • Substantial changes in content, e.g., new results, corrected values, title and authorship are not allowed without the approval of the responsible editor. In such a case, please contact the Editorial Office and return his/her consent together with the proof. • If we do not receive your corrections within 48 hours, we will send you a reminder. • Your article will be published Online First approximately one week after receipt of your corrected proofs. This is the official first publication citable with the DOI. Further changes are, therefore, not possible. • The printed version will follow in a forthcoming issue. Please note http://dx.doi.org/10.1007/s10557-011-6359-8
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Stem Cell Therapy for Arterial Restenosis: Potential Parameters Contributing to the Success of Bone...

After online publication, subscribers (personal/institutional) to this journal will haveaccess to the complete article via the DOI using the URL:
If you would like to know when your article has been published online, take advantageof our free alert service. For registration and further information, go to:http://www.springerlink.com.
Due to the electronic nature of the procedure, the manuscript and the original figureswill only be returned to you on special request. When you return your corrections,please inform us, if you would like to have these documents returned.
Dear Author
Here are the proofs of your article.
• You can submit your corrections online, via e-mail or by fax.
• For online submission please insert your corrections in the online correction form.
Always indicate the line number to which the correction refers.
• You can also insert your corrections in the proof PDF and email the annotated PDF.
• For fax submission, please ensure that your corrections are clearly legible. Use a fine
black pen and write the correction in the margin, not too close to the edge of the page.
• Remember to note the journal title, article number, and your name when sending your
response via e-mail or fax.
• Check the metadata sheet to make sure that the header information, especially author
names and the corresponding affiliations are correctly shown.
• Check the questions that may have arisen during copy editing and insert your
answers/corrections.
• Check that the text is complete and that all figures, tables and their legends are included.
Also check the accuracy of special characters, equations, and electronic supplementary
material if applicable. If necessary refer to the Edited manuscript.
• The publication of inaccurate data such as dosages and units can have serious
consequences. Please take particular care that all such details are correct.
• Please do not make changes that involve only matters of style. We have generally
introduced forms that follow the journal’s style.
• Substantial changes in content, e.g., new results, corrected values, title and authorship are
not allowed without the approval of the responsible editor. In such a case, please contact
the Editorial Office and return his/her consent together with the proof.
• If we do not receive your corrections within 48 hours, we will send you a reminder.
• Your article will be published Online First approximately one week after receipt of your
corrected proofs. This is the official first publication citable with the DOI. Further
changes are, therefore, not possible.
• The printed version will follow in a forthcoming issue.
Please note
http://dx.doi.org/10.1007/s10557-011-6359-8

AUTHOR'S PROOF
Metadata of the article that will be visualized in OnlineFirst
1 Article Title Stem Cell Therapy for Arterial Restenosis: Potential Parameters
Contributing to the Success of Bone Marrow-Deriv edMesenchymal Stromal Cells
2 Article Sub- Title
3 Article Copyright -Year
Springer Science+Business Media, LLC 2011(This will be the copyright line in the final PDF)
4 Journal Name Cardiov ascular Drugs and Therapy
5
Corresponding
Author
Family Name Umberto
6 Particle
7 Given Name Galderisi
8 Suffix
9 Organization Second University of Naples
10 Division Department of Experimental Medicine
11 Address Via L. De Crecchio, Naples 7-80138, Italy
12 Organization Department of Experimental Medicine
13 Division
14 Address Terni , Italy
15 Organization Second University of Naples
16 Division Excellence Research Center for CardiovascularDiseases
17 Address Naples , Italy
18 e-mail [email protected]
19
Author
Family Name Forte
20 Particle
21 Given Name Amalia
22 Suffix
23 Organization Department of Experimental Medicine
24 Division
25 Address Terni , Italy
26 Organization Second University of Naples
27 Division Excellence Research Center for CardiovascularDiseases
28 Address Naples , Italy

AUTHOR'S PROOF
29 e-mail
30
Author
Family Name Rinaldi
31 Particle
32 Given Name Barbara
33 Suffix
34 Organization Department of Experimental Medicine
35 Division
36 Address Terni , Italy
37 Organization Second University of Naples
38 Division Excellence Research Center for CardiovascularDiseases
39 Address Naples , Italy
40 e-mail
41
Author
Family Name Sodano
42 Particle
43 Given Name Loredana
44 Suffix
45 Organization Department of Experimental Medicine
46 Division
47 Address Terni , Italy
48 Organization Second University of Naples
49 Division Excellence Research Center for CardiovascularDiseases
50 Address Naples , Italy
51 e-mail
52
Author
Family Name Berrino
53 Particle
54 Given Name Liberato
55 Suffix
56 Organization Department of Experimental Medicine
57 Division
58 Address Terni , Italy
59 Organization Second University of Naples
60 Division Excellence Research Center for CardiovascularDiseases
61 Address Naples , Italy
62 e-mail
63 Author Family Name Rossi

AUTHOR'S PROOF
64 Particle
65 Given Name Francesco
66 Suffix
67 Organization Department of Experimental Medicine
68 Division
69 Address Terni , Italy
70 Organization Second University of Naples
71 Division Excellence Research Center for CardiovascularDiseases
72 Address Naples , Italy
73 e-mail
74
Author
Family Name Finicelli
75 Particle
76 Given Name Mauro
77 Suffix
78 Organization Department of Human Health Foundation
79 Division
80 Address Terni , Italy
81 Organization Second University of Naples
82 Division Excellence Research Center for CardiovascularDiseases
83 Address Naples , Italy
84 e-mail
85
Author
Family Name Grossi
86 Particle
87 Given Name Mario
88 Suffix
89 Organization Department of Experimental Medicine
90 Division
91 Address Terni , Italy
92 Organization Second University of Naples
93 Division Excellence Research Center for CardiovascularDiseases
94 Address Naples , Italy
95 e-mail
96
Author
Family Name Cobellis
97 Particle
98 Given Name Gilda

AUTHOR'S PROOF
99 Suffix
100 Organization Department of General Pathology
101 Division
102 Address Terni , Italy
103 Organization Second University of Naples
104 Division Excellence Research Center for CardiovascularDiseases
105 Address Naples , Italy
106 e-mail
107
Author
Family Name Botti
108 Particle
109 Given Name Chiara
110 Suffix
111 Organization Department of General Pathology
112 Division
113 Address Terni , Italy
114 Organization Second University of Naples
115 Division Excellence Research Center for CardiovascularDiseases
116 Address Naples , Italy
117 e-mail
118
Author
Family Name Feo
119 Particle De
120 Given Name Marisa
121 Suffix
122 Organization Department of Cardiothoracic and RespiratorySciences
123 Division
124 Address Terni , Italy
125 Organization Second University of Naples
126 Division Excellence Research Center for CardiovascularDiseases
127 Address Naples , Italy
128 e-mail
129
Author
Family Name Santè
130 Particle
131 Given Name Pasquale
132 Suffix

AUTHOR'S PROOF
133 Organization Department of Cardiothoracic and RespiratorySciences
134 Division
135 Address Terni , Italy
136 Organization Second University of Naples
137 Division Excellence Research Center for CardiovascularDiseases
138 Address Naples , Italy
139 e-mail
140
Author
Family Name Cipollaro
141 Particle
142 Given Name Marilena
143 Suffix
144 Organization Department of Experimental Medicine
145 Division
146 Address Terni , Italy
147 Organization Second University of Naples
148 Division Excellence Research Center for CardiovascularDiseases
149 Address Naples , Italy
150 e-mail
151
Schedule
Received
152 Revised
153 Accepted
154 Abstract Purpose: Restenosis is a complex and heterogeneous pathophy siologicalphenomenon occurring in patients submitted to rev ascularizationprocedures. Prev ious studies prov ed the antirestenotic properties ofinjected allogenic mesenchy mal stromal cells (MSCs) in an experimentalmodel of rat carotid (re)stenosis induced through arteriotomy . In this studywe describe some of the ef f ects subsequent to MSC treatment of ratssubmitted to carotid arteriotomy and possibly responsible f or theirantirestenotic ef f ect.Methods: Rat MSCs were isolated f rom bone marrow, expanded in vitroand characterized. Subsequently , we ev aluated the ef f ects of MSCadministration via tail v ein at 3 and 7 day s af ter carotid arteriotomy both inrat serum and in injured carotids, f ocusing on DNA oxidativ e damage(8-oxo-dG detection), cell prolif eration index (BrdU incorporation assay ),apoptotic index (TUNEL assay ), the expression of inf lammation- andprolif eration-related genes (RT-PCR), the release of growth f actors and ofinf lammation-related cy tokines (antibody array s and ELISA).Results: MSC administration induced a greater cell prolif eration in carotidsaf ter arteriotomy , together with an increased lev el of VEGF in the serumand with the higher expression of VEGF mRNA in injured carotids. Serumanaly sis also rev ealed a decreased lev el of the pro-inf lammatory

AUTHOR'S PROOF
cy tokines CXCL1, CXCL5, L-Selectin, ICAM-1 and LIX, and of TIMP1 andSDF-1alpha in MSC-treated rats. The MSC immunomodulatory activ ity wasconf irmed by the decreased expression of TLR2 and TLR4 in injuredcarotids.Conclusions: MSCs play an immunomodulatory paracrine role wheninjected in rats submitted to carotid arteriotomy , accompanied by therelease of VEGF, possibly contributing to the accelerated repair of theinjured v ascular wall.
155 Keywordsseparated by ' - '
Mesenchy mal stromal cells - Restenosis - Inf lammation - Vascularendothelial growth f actor
156 Foot noteinformation
The online v ersion of this article (doi:10.1007/s10557-011-6359-8) containssupplementary material, which is av ailable to authorized users.
Electronic supplementary material
Supplemental Figure 1Representativ e cross-sections of carotids f rom DiI-labeled MSC-treatedrats harv ested at 3 and 7 day s af ter arteriotomy . A, Uninjured carotid; B,rat carotid harv ested at 7 day s af ter arteriotomy and DiI-labeledMSCs-treatement. Representativ e DiI-labeled MSCs emitting redf luorescence are indicated by white arrows. Nuclei were counterstained withHoechst 33258, emitting blue f luorescence. 40x magnif ication. (JPEG 11kb)
Supplemental Table 1Summary of RT-PCR primer sequences, position, annealing temperatureand PCR product length of the target genes analy sed in rat carotids. (DOC38 kb)
Supplemental Table 2Summary of data concerning the characterization of bone marrow-deriv edMSCs expanded in vitro. TOP: RT-PCR analy sis of PPAR-g andosteopontin on mRNA samples extracted f rom undif f erentiated MSCs andf rom MSCs induced to dif f erentiate to adipocy tes and osteocy tes with
dif f erent media. Data are expressed as arbitrary densitometric units, mean ± SEM, n = 3 f or each group. BOTTOM: FACS analy sis of MSCs cultured f or15 day s f rom passage zero. (DOC 36 kb)

AUTHOR'S PROOF
UNCORRECTEDPROOF
1
23
4 Stem Cell Therapy for Arterial Restenosis: Potential5 Parameters Contributing to the Success of Bone6 Marrow-Derived Mesenchymal Stromal Cells
7 Amalia Forte & Barbara Rinaldi & Loredana Sodano & Liberato Berrino &
8 Francesco Rossi & Mauro Finicelli & Mario Grossi & Gilda Cobellis & Chiara Botti &9 Marisa De Feo & Pasquale Santè & Galderisi Umberto & Marilena Cipollaro
1011 # Springer Science+Business Media, LLC 2011
12
13 Abstract14 Purpose Restenosis is a complex and heterogeneous path-15 ophysiological phenomenon occurring in patients submitted16 to revascularization procedures. Previous studies proved the17 antirestenotic properties of injected allogenic mesenchymal
18stromal cells (MSCs) in an experimental model of rat19carotid (re)stenosis induced through arteriotomy. In this20study we describe some of the effects subsequent to MSC21treatment of rats submitted to carotid arteriotomy and22possibly responsible for their antirestenotic effect.23Methods Rat MSCs were isolated from bone marrow,24expanded in vitro and characterized. Subsequently, we25evaluated the effects of MSC administration via tail vein26at 3 and 7 days after carotid arteriotomy both in rat serum27and in injured carotids, focusing on DNA oxidative damage28(8-oxo-dG detection), cell proliferation index (BrdU incor-29poration assay), apoptotic index (TUNEL assay), the30expression of inflammation- and proliferation-related genes31(RT-PCR), the release of growth factors and of32inflammation-related cytokines (antibody arrays and33ELISA).34Results MSC administration induced a greater cell prolif-35eration in carotids after arteriotomy, together with an36increased level of VEGF in the serum and with the higher37expression of VEGF mRNA in injured carotids. Serum38analysis also revealed a decreased level of the pro-39inflammatory cytokines CXCL1, CXCL5, L-Selectin,40ICAM-1 and LIX, and of TIMP1 and SDF-1alpha in41MSC-treated rats. The MSC immunomodulatory activity42was confirmed by the decreased expression of TLR2 and43TLR4 in injured carotids.44Conclusions MSCs play an immunomodulatory paracrine45role when injected in rats submitted to carotid arterio-46tomy, accompanied by the release of VEGF, possibly47contributing to the accelerated repair of the injured48vascular wall.
49Key words Mesenchymal stromal cells . Restenosis .
50Inflammation . Vascular endothelial growth factor
Electronic supplementary material The online version of this article(doi:10.1007/s10557-011-6359-8) contains supplementary material,which is available to authorized users.
A. Forte : B. Rinaldi : L. Sodano : L. Berrino : F. Rossi :M. Grossi :G. Umberto :M. CipollaroDepartment of Experimental Medicine,Terni, Italy
M. De Feo : P. SantèDepartment of Cardiothoracic and Respiratory Sciences,Terni, Italy
G. Cobellis : C. BottiDepartment of General Pathology,Terni, Italy
M. FinicelliDepartment of Human Health Foundation,Terni, Italy
G. Umberto (*)Department of Experimental Medicine,Second University of Naples,Via L. De Crecchio,7-80138 Naples, Italye-mail: [email protected]
A. Forte : B. Rinaldi : L. Sodano : L. Berrino : F. Rossi :M. Finicelli :M. Grossi :G. Cobellis :C. Botti :M. De Feo :P. Santè :G. Umberto :M. CipollaroExcellence Research Center for Cardiovascular Diseases,Second University of Naples,Naples, Italy
Cardiovasc Drugs TherDOI 10.1007/s10557-011-6359-8
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
51Q1 Introduction
52 Restenosis is considered as an excessive reparative reaction to53 vascular injury occurring during revascularization procedures.54 The current rate of this pathophysiological phenomenon is still55 high in the Western Countries [1], thus limiting the long-term56 success of revascularization procedures.57 Heterogeneity and complexity of the molecular phenom-58 ena contributing to restenosis often limited the efficacy of59 experimental therapies. On this basis, a more in depth60 analysis of the molecular mechanisms leading to restenosis61 and mediating the effects of the experimental therapeutic62 strategies is warranted.63 Mesenchymal stromal cells (MSCs) are non-64 hematopoietic multi-potent stem-like cells able to differen-65 tiate into both mesenchymal and non-mesenchymal line-66 ages. MSCs offer a series of advantages as a potential67 therapeutic tool: a) they can be isolated from a small68 aspirate of bone marrow; b) extensively proliferate in vitro69 while preserving a normal karyotype and telomerase70 activity on several passages [2]; c) express low71 immunogenicity [3], and hence their use in vivo should72 not require a pharmacological immunosuppression.73 MSCs have an intrinsic ability to differentiate into74 functional cell types able to repair the diseased or injured75 tissue in which they are localized. Nonetheless, MSC76 differentiation is not absolutely required for stem-cell77 mediated tissue repair and protection, as they can release78 a variety of factors which may protect the injured tissue79 through a paracrine mechanism [4–6].80 Experimental vascular surgical injury remains a major81 tool to dissect the molecular pathways involved in stenosis82 progression and to identify novel potential targets for (re)83 stenosis limitation. We set up and validated an arteriotomy84 model of surgical injury of rat common carotid [7]85 alternative to the model of balloon angioplasty and that86 mimics the injury affecting the arteries submitted to87 grafting or endarterectomy, since it is characterized by an88 interruption of both the internal and external elastic89 laminae, considered clinically relevant for the development90 of arterial stenosis. In a previous study we highlighted the91 positive antirestenotic role played by allogenic MSCs in the92 arteriotomy model of rat vascular injury [8], homing at the93 injury site up to 7 days after arteriotomy and limiting the94 lumen stenosis 30 days later. In this study we aimed to95 identify some of the factors possibly mediating the positive96 therapeutic effect of MSCs in experimentally induced (re)97 stenosis and analyzed the effects of MSC administration in98 rats at 3 and 7 days after carotid injury, focusing on DNA99 oxidative damage, the cell proliferation index, the expres-100 sion of selected genes involved in cell proliferation and in101 immune reaction and the apoptosis level in injured carotids,102 in conjunction with the analysis in serum samples of the
103differential levels of growth factors and of inflammation-104related cytokines.
105Methods
106Animals
107Studies were carried out on 12 week-old male Wistar rats108(230–250 g) (Charles Rivers, France). Rats were main-109tained in accordance with the guidelines of the NIH (Guide110for the Care and Use of Laboratory Animals, 1976). All111protocols were approved by the Animal Care and Use112Committee of the Second University of Naples. Rats were113acclimatized and quarantined for at least 1 week before114undergoing surgery.
115MSC cultures
116MSCs have been harvested from the bone marrow of the117femurs and tibias of adult Wistar rats. WKY rats have been118anaesthetized with an intraperitoneal injection of ketamine119hydrochloride and MSCs have been harvested from the120bone marrow by inserting a 21-gauge needle into the shaft121of the bone and flushing it with complete α-modified122Eagle’s medium (αMEM) containing 20% foetal bovine123serum (FBS), 2 mM L-glutamine, 100 U/ml penicillin,124100 μg/ml streptomycin. Cells from one rat have been125plated into two 100 mm dishes. After 24 h, non-adherent126cells have been discarded, and adherent cells have been127washed twice with PBS. The cells have been then incubated128for 5–7 days to reach confluence. In order to obtain the129sufficient amount of cells to be injected in rats at the time of130arteriotomy, MSCs were cultured for 23 days, including13115 days from passage zero (corresponding to passage 5)132and submitted to analysis of their differentiative ability and133stemness as well as senescence level, as described below.134All the cell culture reagents have been obtained from135Invitrogen (Milan, Italy).
136MSC differentiation
137Differentiation of isolated MSCs into the mesenchymal138osteogenic and adipogenic lineages was induced using139different protocols, as previously described [9].
140Senescence-associated β-galactosidase staining
141Cultured MSCs were fixed for 10 min with 2% formalde-142hyde/0.2% glutaraldehyde at room temperature (RT). Cells143were then washed twice with PBS and 2 ml of senescence-144associated β-galactosidase staining solution per 35 mm dish145were added. Cells were incubated at 37°C until blue
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
146 staining was clearly detectable under a light microscope.147 The percentage of senescent cells was calculated by the148 number of β-galactosidase-positive cells out of at least 500149 cells in different microscope fields. Just before using the150 senescence-associated β-galactosidase staining solution, we151 added 20 ml of citric acid/sodium phosphate in a volume of152 100 ml, pH 6.0, 150 mM NaCl, 2 mM MgCl2, 5 mM153 potassium ferricyanide, 5 mM potassium ferrocyanide and154 1 mg/ml X-Gal.
155 Cell cycle analysis
156 For each assay, 3×105 MSCs were collected and resus-157 pended in 500 μl of a hypotonic buffer (0.1% Triton X-100,158 0.1% sodium citrate and 50 μg/ml propidium iodide/159 RNAse A). Cells were incubated in the dark for 30 min160 and then analysed. Samples were acquired on a FACSCa-161 libur flow cytometer using the Cell Quest software (Becton162 Dickinson) and analysed using the Cell Quest software and163 the ModFitLT software version 3 (Becton Dickinson,164 Fanklin Lakes, NJ, USA).
165 Fluorescence immunocytochemistry
166 1.5×104 MSCs were used for immunofluorescence analysis167 of the expression of surface antigens CD73 (primary168 antibody mouse anti-rat CD73, BD Biosciences, San Jose,169 CA, USA, dil. 1:100), CD90 (primary antibody mouse anti-170 rat CD90, BD Biosciences, dil. 1:250) and CD105 (primary171 antibody goat anti-rat CD105, Santa Cruz, Santa Cruz, CA,172 USA, dil. 1:100), and of smooth muscle (SM) alpha-actin173 (primary antibody mouse anti-rat SM-alpha actin, Sigma-174 Aldrich, Milan, Italy, dil. 1:250). All the experiments were175 performed as previously described [8]. The nuclei were176 stained with Hoechst 33258 (Sigma-Aldrich) for 5 min and177 the samples examined under a fluorescence microscope178 (Leica, Wetzlar, Germany).
179 Vascular injury and MSC treatment
180 Arteriotomy of rat common carotid artery was performed as181 already published [7]. Briefly, a plastic Scanlom clamp for182 coronary artery grafting was placed for 10 s on the carotid183 causing a crushing lesion to the vessel. At the same point184 where the clamp was applied, a 0.5 mm longitudinal incision185 was done on the full thickness of the carotid. The incision186 did not cross to the other side of the vessel. Haemostasis was187 obtained with a single adventitial 8.0-gauge polypropylene188 stitch. Once bleeding stopped, the carotid artery was189 carefully examined and blood pulsation was checked distally190 to the incision. WKY rats submitted to arteriotomy were191 administered with 5×106 MSCs resuspended in 200 μl192 DMEM via tail vein injection (n=10), while control rats
193were administered with 200 μl DMEM (n=10) for all the194analyses we conducted. For homing analysis, 5×106 MSCs195were labelled with fluorescent Vybrant DiI (Molecular196Probes-Invitrogen, Milan, Italy) before injection in rats,197according to manufacturer’s instructions.
198Histological analysis
199For the analysis of the engraftment of DiI-labeled MSC, both200the injured and the contralateral uninjured carotids were201harvested at 7 days after arteriotomy from each rat (n=3),202included in paraffin and sectioned. Cross-sections at the203injury site were stained with the fluorescent dye Hoechst20433258 (Sigma-Aldrich, Milan, Italy) for nuclear identifica-205tion. Image screening and photography of serial cross-206sections were then performed using the Leica 4000 F207software.
2087,8-dihydro-8-oxo-2′-deoxyguanosine (8-oxo-dG)209immunohistochemical detection
210Immunohistochemistry was performed on cross-sections211from carotid arteries taken at 3 and 7 days after arteriotomy212and MSC or control DMEM injection and on control213carotids taken from uninjured rats immediately after214anesthesia (n=5 for each group). Experiments were215performed as already published [9]. After washing, DNA216was stained with fluorescent dye Hoechst 33258 for nuclear217identification. Specimen image screening and photography218were performed using a Leica F4000 System. Five cross-219sections localized at the injury site were analyzed for each220carotid. The percentages of 8-oxo-dG positive nuclei in the221tunicae intima and media were calculated by determining222the number of Hoechst-stained nuclei positive for 8-oxo-dG223staining. We considered for quantitative analysis after all224the immunohistochemistry experiments only positive cells225located in the endothelium and in the media, as the226adventitia was hardly distinguished from perivascular tissue227in injured carotids, especially at 7 days after arteriotomy,228and could have been partially damaged during carotid229harvesting or histological processing, thus leading to230unreliable results. A number of randomly selected cross-231sections were quantified for BrdU staining by two232independent observers blinded to the rat treatment to assess233inter-observer variation.
234BrdU proliferation assay
235Rats were submitted to carotid arteriotomy and to MSC236or control DMEM injection. Eighteen hrs prior to237sacrifice at 3 and 7 days after injury (n=5 for each238group) they were administered i.p. with 50 mg/kg239Bromodeoxyuridine (BrdU) (Roche) for detection and
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
240 quantification of cells that entered into the cell cycle241 within 24 h of sacrifice. The 4% formaldehyde-fixed242 sections (5 μm) were deparaffinized and rehydrated.243 Immunohistochemical detection of incorporated BrdU244 was performed as previously published [9]. Image screen-245 ing and photography of serial cross-sections submitted to246 colorimetric immunohistochemical analysis were per-247 formed using a Leica IM1000 System. Five cross-248 sections localized at the injury site were analyzed for each249 carotid. The percentages of BrdU-positive nuclei in the250 tunicae intima and media were calculated by determining251 the number of hematoxylin-stained nuclei that were252 positive for immunohistochemical staining of BrdU. A253 number of randomly selected cross-sections were quanti-254 fied for BrdU staining by two independent observers255 blinded to the rat treatment to assess inter-observer256 variation.
257 TUNEL assay
258 Assays were performed on carotid arteries taken at 3 and259 7 days after arteriotomy and MSC or control DMEM260 injection and on control carotids taken from uninjured rats261 after anesthesia (n=5 for each group). The 4%262 formaldehyde-fixed sections (5 μm) were deparaffinized263 and rehydrated. Immunohistochemical detection of frag-264 mented DNA in apoptotic cells was performed as previ-265 ously published [9]. Specimen image screening and266 photography were performed using a Leica F4000 System.267 Five cross-sections localized at the injury site were268 analyzed for each carotid. The percentages of apoptotic269 nuclei in the tunicae intima and media were calculated by270 determining the number of Hoechst-stained nuclei positive271 for TUNEL staining. When observed with 40-100x objec-272 tives, cells showing morphological features typically273 associated with apoptosis, as well as positive to TUNEL274 reaction, were considered to be apoptotic. A number of275 randomly selected cross-sections were quantified for276 TUNEL staining by two independent observers blinded to277 rat treatment to assess inter-observer variation.
278 Enzyme-linked immunoadsorbent assay (ELISA)
279 The concentrations of Stromal cell-derived factor 1α (SDF-280 1α), Vascular endothelial growth factor (VEGF) and281 chemokine (C-X-C motif) ligand 1 (CXCL1) in serum282 samples harvested at 3 and 7 days after arteriotomy from283 rats submitted to MSC or DMEM treatment (n=5 for each284 group) and from uninjured rats (n=3) were measured using285 commercial ELISA kits (R&D Systems for VEGF, code286 RRV00, and SDF-1alpha, code DSA00; PeproTech for287 CXCL1, code 900-K57) following the manufacturer’s288 instructions. Optical density was measured at 450 nm using
289an ELISA plate reader (TECAN). All assays were repeated290twice.
291Cytokine antibody array hybridization
292The profile of the relative levels of 29 cytokines in the293serum samples harvested at 3 and 7 days after arteriotomy294from rats submitted to MSC or DMEM treatment (n=5 for295each group) and from uninjured rats (n=3) was determined296using the Rat Cytokine Array Panel A membranes (R&D297Systems, code ARY008). The nitrocellulose membranes298provided by the manufacturer contained 29 capture anti-299bodies spotted in duplicate on the surface. Each membrane300also included three pairs of positive control spots in the301corners of each array, except for the corner at the right302bottom, which contained negative control spots. Serum303samples for each of the 5 experimental groups were pooled304before hybridizations (150 μl of each serum sample).305Hybridizations and signal measurements were done follow-306ing the manufacturer’s instructions, after incubation of the 5307membranes with the chemiluminescent HRP substrate308Immobilon Western (Millipore). Array signals were ac-309quired using the Chemidoc system (Bio-Rad) and the310associate software QuantityOne. Array images used for311signal quantification (expressed as pixel density) are from3121 min exposure to the camera. All the 5 membranes were313processed simultaneously. All hybridizations were repeated314twice.
315RNA extraction and RT-PCR analysis
316Total RNAwas extracted from cultured MSCs, from injured317rat carotids at 3 and 7 days after arteriotomy (n=5 MSC-318treated rats and n=5 DMEM-treated rats, for each time319point) and from uninjured rat carotids (n=3) using the320RNAeasy minikit (Qiagen) according to manufacturer’s321instructions. RT-PCR experiments were performed as322already published [9]. GeneBank sequences for rat mRNAs323and the Primer Express software (Applied Biosystem) were324used to design primer pairs for the genes osteopontin,325peroxisome proliferator-activated receptor-γ (PPAR-γ),326VEGF-A, Toll-like receptor 2 (TLR2), TLR4 and for the327house keeping gene glyceraldehyde-3-phosphate dehydro-328genase (GAPDH). Primer sequences and PCR conditions329are reported in Supplemental Table 1.
330Statistical analysis
331All statistical analysis was performed usingGraphPad software332(Prism 4.0). Data are presented as the mean±SEM. Statistical333significance was determined using two-way analysis of334variance followed by Bonferroni’s multiple comparison test.335Values of p<0.05 were considered significant.
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
336 Results
337 Bone marrow-derived rat MSCs retain multipotent338 potentiality, high proliferative activity and low senescence339 after expansion in vitro
340 Before MSC administration in rats submitted to arterio-341 tomy, we verified that the MSCs we extracted from rat bone342 marrow and expanded in vitro for 15 days from passage343 zero retained their biological characteristics. Moreover, we344 applied the minimal criteria for defining multipotent MSCs,345 as suggested by the International Society for Cellular346 Therapy (ISCT) [10]. In agreement with these criteria, we347 isolated MSCs on the basis of their adherence to plastics348 and we confirmed through Alizarin Red and Oil Red O349 staining and through RT-PCR analysis for the markers350 osteopontin and PPAR-γ that rat bone marrow-derived351 MSCs were able to differentiate to osteocytes and adipo-352 cytes, respectively, using our standard in vitro culture-353 differentiating conditions (Supplemental Table 2). More-354 over, MSCs were immunophenotyped, revealing the ex-355 pression of the surface markers CD73 (ecto 5 ′356 nucleotidase), CD90 (Thy-1) and CD105 (endoglin). We357 also verified that MSCs expressed SM-alpha actin, another358 feature of MSCs that provides them with contractile ability359 (data not shown).360 The FACS analysis revealed that during the in vitro361 expansion the MSCs maintained their proliferative capacity362 as they were mainly in the G1 and S phase of cell cycle (50363 and 49%, respectively) (Supplemental Table 2).364 Finally, since senescence can hamper cell differentiation365 ability and stemness, we performed a time-dependent366 follow-up of cellular senescence through the in situ β-367 galactosidase assay, based on the increased expression of β-368 galactosidase in the lysosomal compartment of senescent369 cells, detected as a blue perinuclear staining specifically at370 acid pH. The assay demonstrated that MSCs showed a371 limited 23±3.4% of senescent cells (n=3) at the time of372 injection in vivo.
373 MSCs engraft at the injury site in arteriotomy-injured374 carotids
375 Carotids were harvested from WKY rats at 7 days after376 arteriotomy and DiI-MSC injection to verify the homing of377 MSCs at the injury site. Histological analysis conducted on378 carotid cross-sections at level of injury site revealed an379 accumulation of DiI-MSCs mainly in the adventitia and in380 perivascular tissue, with some MSCs present also in the381 media (Supplemental Fig. 1B). No DiI-labeled MSCs were382 detectable in contralateral uninjured carotids, thus revealing383 the specificity of MSC engraftment at the injury site384 (Supplemental Fig. 1A).
385MSC treatment affects the expression of target genes386in arteriotomy-injured rat carotids
387We evaluated the capacity of MSCs to modulate the388expression of VEGF, TLR2 and TLR4 in arteriotomy-389injured carotids, as these genes are known to be involved in390vascular cell proliferation and in innate immunity, respective-391ly. Total RNA has been extracted from carotids at 3 and 7 days392after arteriotomy and from uninjured carotids to verify by RT-393PCR the differential expression of target mRNAs.394VEGF mRNA showed an increase at 3 days after395arteriotomy in carotids from MSC-treated rats in compar-396ison to carotids from DMEM-treated rats (p<0.05) (Fig. 1),397followed by an inversion of this trend at 7 days after398arteriotomy. mRNAs coding for TLR2 and 4 showed a399significant decrease both at 3 and 7 days after arteriotomy400in carotids from MSC-treated rats in comparison to carotids401from DMEM-treated rats (p<0.05) (Fig. 1). Overall RT-402PCR data suggest that modulation of VEGF, TLR2 and403TLR4 is feature of MSC-treated rats.
404MSC treatment affects cell proliferation index405after arteriotomy
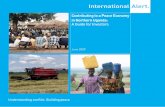
406We then evaluated the effect of MSC treatment on cell407proliferation stimulated by arteriotomy giving a pulse of BrdU408to the injured rats. Carotids have been harvested at 3 and 7 days409after arteriotomy and from uninjured rats and the cross-sections410at the injury site were submitted to BrdU immunohistochemical411detection for assessment of the cell proliferation index.412The intravenous administration of MSCs in rats after413carotid arteriotomy induced a significant increase of414proliferating cells up to 25% and to 14.4% at 3 and 7 days415after arteriotomy, respectively (p<0.05) (Fig. 2, lower416panel). Conversely, we revealed a 4.4% of BrdU-positive417cells at 3 days after arteriotomy, followed by an increase to4187% of BrdU-positive cells at 7 days after arteriotomy in419DMEM-treated animals (Fig. 2, lower panel). No BrdU-420positive cells were detectable in carotids from uninjured421rats (Fig. 2a and lower panel). These data suggest that MSC422treatment increases cell proliferation in injured carotids.423BrdU-positive cells were located in the endothelium and424in the tunica media, as well as in focal neointima, when425present (Fig. 2b, c). We highlighted BrdU-positive cells426also in the adventitia and in perivascular tissue, particularly427in actively forming vasa vasorum at 7 days after arterio-428tomy (data not shown).
429MSC treatment does not affect the oxidative DNA damage430and the apoptosis level after arteriotomy
431We evaluated the effect of MSC intravenous administration432on oxidative stress induced by arteriotomy in carotids
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
433 harvested at 3 and 7 days after injury and MSC or control434 DMEM treatment and from uninjured rats. The carotid435 cross-sections at the injury site were submitted to immu-436 nohistochemistry for 8-oxo-dG, one of the most frequent437 base lesions accumulating after oxidative damage to DNA,438 due to the low redox potential of guanine, that makes this439 base particularly vulnerable [11]. The oxidized guanine
440pairs with adenine during DNA replication, inducing G:C441to T:A transversions. Since the ROS can induce also RNA442oxidative damage in cells, the carotid cross-sections were443treated with ribonuclease during the experimental proce-444dure. Consequently, the hybridization signal we detected445for 8-oxo-dG was specific for the nuclear DNA.446The 17.5% and 20% of nuclei in the endothelium and in447the tunica media of carotids from MSC-treated rats were448positive for 8-oxo-dG staining at 3 and 7 days after449arteriotomy, respectively (p<0.05) (Fig. 3e). A similar450percentage of cells positive for 8-oxo-dG staining has been451measured in DMEM-treated rats. The nuclei positive for452oxidative DNA damage were homogeneously distributed in453all the three tunica layers and in the perivascular tissue,454around the injury site and the polypropylene stitch applied455as suture of the arteriotomy (Fig. 3a, b). A basal level of456about 1.5% cells positive to 8-oxo-dG has been detected in457carotids from uninjured rats (Fig. 3e).458We also evaluated the effect of MSC intravenous459infusion on cell apoptosis induced by arteriotomy in460carotids harvested at 3 and 7 days after arteriotomy and461MSC or control DMEM treatment and from uninjured462rats. The carotid cross-sections at the injury site were463submitted to TUNEL assay for apoptosis detection. The464percentage of cells positive to TUNEL assay in injured465carotids from MSC-treated rats was similar to the values466measured in DMEM-treated rats (Fig. 3f), with a 13.3%467of TUNEL-positive cells at 3 days after arteriotomy (p<4680.05), followed by a decrease to 8.9% of TUNEL-positive469cells at 7 days after arteriotomy (p<0.05). Apoptotic cells470were located mainly in the endothelium and in the471adventitia, around the injury site (Fig. 3c, d). Carotids472from uninjured rats showed a basal level of 0.7% of473TUNEL-positive cells (Fig. 3f). Overall data indicate that474the arteriotomy alone affects the oxidative DNA damage475and apoptosis and that MSC treatment does not modulate476these phenomena.
477MSC treatment affects serum concentration of different478factors after arteriotomy
479On the basis of the above reported observations and of the480current literature, we hypothesized that the intravenous481administration of MSCs could modulate the serum levels of482some cytokines. To verify this hypothesis, serum samples483harvested at 3 and 7 days after arteriotomy from rats treated484with MSCs or with control DMEM and from uninjured rats485have been analyzed through the hybridization with nitro-486cellulose membrane arrays spotted in duplicate with 29487antibodies specific for rat cytokines. The complete list of488the 29 detectable cytokines is available on the manufacturer489site (www.rndsystems.com/product_detail_objectname_rat490cytokinearray.aspx).
Q2 Fig. 1 RT-PCR analysis of the expression of mRNAs coding forVEGF, TLR2 AND TLR4 and MSC or control DMEM treatment inrat carotids at 3 (n=5 for each group) and 7 (n=5 for each group) daysafter arteriotomy and in carotids from uninjured rats (n=3). Allmeasurements were normalized with respect to endogenous GAPDHlevels. The values are expressed in arbitrary units as relative changesover the normalized uninjured control. Data are presented as the mean±SEM. *:p<0.05 vs. DMEM-treated carotids
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
491 The hybridization of the antibody arrays with serum492 from uninjured rats revealed the basal constitutive493 expression of 5 proteins (ICAM-1/CD54, CCL5/494 RANTES, CXCL5/LIX, L-Selectin and TIMP-1), in495 agreement with the reference hybridization data provid-496 ed by the manufacturer (Fig. 4). The expression of all497 these 5 proteins was increased at 3 days after arteriotomy,498 but to a significantly lesser extent in MSC-treated rats (p<499 0.05) (Fig. 4). Nonetheless, the modulatory effect played500 by MSCs was greater for chemokine (C-C motif) ligand 5501 (CCL5/RANTES), Tissue inhibitor of metalloproteases-1502 (TIMP-1) and chemokine (C-X-C motif) ligand 5503 (CXCL5/LIX) (Fig. 4). Interestingly, at 7 days after504 arteriotomy, the hybridization signals corresponding to505 CXCL5/LIX, intercellular adhesion molecule 1 (ICAM-1)506 and L-Selectin were lower than basal levels observed in507 uninjured rats, while the hybridization signals508 corresponding to TIMP-1 and CCL5/RANTES were509 undetectable (Fig. 4), suggesting that the increase of pro-510 inflammatory factors is early and transient in rats511 submitted to vascular injury and that a possible negative512 feedback mechanism of regulation occurs for these factors513 at later time points after arteriotomy.
514The antibody array data were integrated with the ELISA515analysis of the same serum samples for three targets, VEGF,516SDF-1α and CXCL1, selected on the basis of the relevant517role played in vascular cell proliferation, in homing of518progenitor cells and in inflammation, respectively, and519hence of interest in our experimental model of disease. Data520analysis revealed a significant increase of VEGF concen-521tration in the serum of injured DMEM-treated rats at 3 and5227 days after arteriotomy (p<0.05 vs. uninjured rats)523(Fig. 5). Of interest, VEGF increase was significantly524higher in the serum of rats treated with MSCs after carotid525arteriotomy and harvested at 7 days after injury (p=0.014526vs. DMEM-treated rats) (Fig. 5).527The ELISA analysis also revealed a significant 2.2-fold528increase of the chemokine CXCL1 at both 3 and 7 days529after arteriotomy in the serum of DMEM-treated rats. The530intravenous administration of MSCs significantly reduced531the concentration of CXCL1 at 3 days after arteriotomy (p=5320.022 vs. DMEM-treated rats) (Fig. 5), with a not533statistically significant trend for a decreased concentration534also at 7 days after arteriotomy.535The serum concentration of the factor SDF-1α signifi-536cantly increased at 7 days after arteriotomy in the serum of
Fig. 2 Immunohistochemical analysis of the proliferation index at 3and 7 days after carotid arteriotomy and MSC or control DMEMtreatment (n=5 for each group). Upper panel: Representativeimmunohistochemical staining of BrdU in uninjured carotids (a) andin injured rat carotids at 3 days after arteriotomy and MSC (b) or
DMEM (c) treatment. Black arrows in B and C indicate thearteriotomy site. BrdU-positive cells are stained in brown. Hematox-ylin nuclei counterstaining in blue (40x magnification). Lower panel:percentage in the tunicae media and intima of cells positive to BrdU
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
537 DMEM-treated rats (p=0.009 vs. uninjured rats), with a538 significant reduction after MSC treatment below the basal539 concentration measured in serum from uninjured rats (p=540 0.002 vs. DMEM-treated rats) (Fig. 5).
541Of note, despite the antibodies spotted on the arrays542included also those for VEGF, this factor resulted to be543undetectable after serum hybridization at any of the time544points we analyzed (general minimum detectable dose of the
Fig. 3 Immunohistochemical analysis of the DNA oxidative damageindex (a, b, e) and of the apoptosis index (c, d, f) at 3 and 7 days aftercarotid arteriotomy and MSC or control DMEM treatment and incarotids from uninjured rats (n=5 for each group). a, b: representativeimmunohistochemical staining of 8-oxo-dG in injured rat carotids at7 days after arteriotomy and MSC (a) or DMEM (b) treatment (40xmagnification). e: percentage in the tunicae media and intima of cellspositive to 8-oxo-dG. c, d: representative immunohistochemical
staining of apoptotic cells in injured rat carotids at 3 days afterarteriotomy and MSC (c) or DMEM (d) treatment (40x magnifica-tion). f: percentage in the tunicae media and intima of cells positive toTUNEL assay. Green fluorescence in A and B: 8-oxo-dG-positivecells. Red fluorescence in C and D: TUNEL-positive cells. Hoechst33258 (blue) nuclei counterstaining. Arrows indicate representativepositive nuclei to 8-oxo-dG and to TUNEL assay
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
545 arrays is about 80 pg/mL). Conversely, the ELISA analysis546 (minimum detectable dose of VEGF <0.09 pg/mL) allowed547 the quantitative analysis of VEGF concentration in all the548 serum samples, showing its gradual increase at 3 and 7 days549 after arteriotomy, boosted by MSC administration. This550 discrepancy is probably related to the different sensitivity of551 the two techniques we used to analyze the rat serum samples.
552 Discussion
553 This study has been conducted in a murine pre-clinical554 model of vascular stenosis induced by arteriotomy, rather
555then by the classically applied balloon angioplasty. The556arteriotomy model we set up mimics the damage that557affects the arteries submitted to endarterectomy or to by-558pass interposition, as it is based on a longitudinal incision559of the vascular wall through the full thickness, included the560internal and the external elastic laminae, sutured with a561polypropilene stitch.562Qualitative morphological analysis of arteriotomy-injured563rat carotids revealed that the surgical injury induced in the564chronic phase a marked neoadventitia along with extracellular565matrix and elastic lamina accumulation in both groups of rats,566with only limited focal neointima in a few cases [7, 8]. In567addition, internal and external elastic lamina and media
Fig. 4 Rat cytokine antibody array analysis of rat serum samplesharvested at 3 and 7 days after arteriotomy and MSC or controlDMEM treatment (n=5 for each group) and of serum from uninjuredrats (n=3). The values in the histogram are expressed in arbitrary
densitometric units and refer to quantification of spots at 3 days afterarteriotomy. Data are presented as the mean±SEM. *:p<0.05 vs.DMEM-treated carotids
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
568 disruptions at the injury site were evident, often with media569 substitution by fibrotic tissue. Our previous gene expression570 microarray data obtained in this model [12] revealed the571 early and marked up-regulation of inflammation-related572 genes, thus supporting the expected picture of inflammatory573 cell infiltration in the acute phase after arteriotomy (mainly at574 4 h and 3 days after arteriotomy).
575In this study we described some of the events occurring576in the early phase following rat carotid arteriotomy, as the577effect of intravenously infused MSCs is presumably more578evident in the acute and sub-acute phase after injury, with579long-term effects reflected by the reduced stenosis at58030 days after injury [8].
581MSC treatment affects the expression of target genes582in arteriotomy-injured rat carotids
583VEGF is known to stimulate the proliferation of endothelial584cells (ECs) and the migration and proliferation of smooth585muscle cells (SMCs) [13]. The MSC treatment in586arteriotomy-injured rats increases the VEGF production in587terms of mRNA and protein, both in the carotids and in the588serum, respectively (Figs. 1 and 5). The increase of VEGF589mRNA observed in injured carotids from MSC-treated rats590could be related to the paracrine activity of MSCs homed at591the injury site (Supplemental Figure 1). TLRs are known to592link innate and adaptive immunity. The activation and the593role of TLR2 and TLR4 in inflammation and neointima594proliferation associated to stenosis progression after vascu-595lar injury has already been highlighted by other studies596[12–14]. The decrease of mRNAs coding for TLR2 and597TLR4 in injured carotids from MSC-treated rats in598comparison to DMEM-treated rats (Fig. 1) suggests an599immunomodulatory action of MSCs in injured carotids600through a paracrine mechanism, in agreement with previous601data [8]. These results suggest that MSCs are able to602establish a favorable regenerative microenvironment in603injured tissue, also through a local down-modulation of604the immune reaction, as also hypothesized by Caplan [15].
605MSC treatment affects cell proliferation index606but not oxidative stress and apoptosis in arteriotomy-injured607rat carotids
608The increased cell proliferation observed at the arteriotomy609site in injured rats after MSC treatment in comparison to610DMEM-treated rats (Fig. 2), possibly contributes to limit611the long-term (re)stenosis through an early repair of the612injured vascular wall. Our hypothesis of a possible para-613crine action of MSCs in enhancing tissue repair would be in614agreement with other observations obtained in a model of615wound healing [16]. Moreover, MSCs could positively616affect the endothelial differentiation and function, as617suggested by others [17]. Nonetheless, additional experi-618ments would be necessary to address this point.619We previously highlighted in our model of carotid620arteriotomy a relevant and persistent oxidative stress621induced, either directly and indirectly, by arteriotomy,622together with extensive cell apoptosis [9]. Our new data623unexpectedly indicate that the intravenous infusion of
Fig. 5 ELISA analysis of rat serum samples harvested at 3 and 7 daysafter arteriotomy and MSC or control DMEM treatment (n=5 for eachgroup) and of serum from uninjured rats (n=3). Data are presented asthe mean±SEM. *:p<0.05 vs. DMEM-treated carotids
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
624 MSCs does not affect the progression of these phenom-625 ena in arteriotomy-injured carotids, at least at the time626 points we analysed. Intracellular generation of ROS627 could be a critical event for the directional migration of628 MSCs, as already demonstrated elsewhere [18]. None-629 theless, it has been also demonstrated that ROS inhibit630 MSC adhesion in ischemic myocardium [19]. Consequent-631 ly, the role of oxidative stress on MSC recruitment should632 be further addressed, with particular reference to the633 vasculature. In addition, the antioxidant role of MSCs in634 vivo has been highlighted mainly in models of neurode-635 generative diseases [20, 21], with some evidence also in636 myocardial ischemia [22].
637 MSC treatment affects serum levels of different factors638 after arteriotomy
639 It is well known that cell trapping in the pulmonary640 microvasculature can significantly reduce the number of641 MSCs that can access injured organs; as a matter of fact, the642 majority of MSCs, whose diameter is about 15–19 micron,643 are trapped in lung capillaries within few seconds after644 intravenous injection [23]. Despite the number of allogenic645 MSCs that were able to escape pulmonary trapping and to646 home at the injury site at 3 and 7 days after arteriotomy was647 not high, they were sufficient to limit the negative648 remodeling in arteriotomy-injured rat carotids at 30 days649 after injury, with a lumen area 36% greater than in control650 carotids [8]. These findings support the concept that the651 number of MSCs necessary in regenerative medicine652 protocols do not necessarily need to be high, as MSCs are653 presumed to play their reparative and anti-inflammatory654 action mainly through soluble factors, playing a paracrine655 action [24, 25]. In agreement with these observations, our656 data revealed that the number of MSCs in the serum of rats657 at 3 and 7 days after intravenous administration was658 sufficient to induce a significant increase of the concentra-659 tion of VEGF (Fig. 4), a growth factor secreted not only by660 vascular cells but also by MSCs [26]. The increase of661 VEGF in the serum (Fig. 5) and the slight transient increase662 of VEGF mRNA in injured carotids of rats administered663 with MSCs (Fig. 1) could be directly or indirectly related to664 the increased proliferation highlighted in MSC-treated rats,665 possibly leading to an accelerated repair of the vascular666 wall after arteriotomy, that in turn can lead to a limitation of667 the long-term hyperplasia and negative remodelling. Our668 hypothesis is in agreement with other data obtained in669 murine models of endothelial denudation injury injected670 with recombinant adenovirus expressing VEGF, demon-671 strating that the VEGF systemic [27] or local overexpres-672 sion [28] accelerated the endothelial repair and inhibited673 neointima formation. Other studies also revealed the674 beneficial role of VEGF overexpression both in models of
675disease and in patients [29, 30]. Despite our past and676present data support the idea of a positive role played by677VEGF secreted in the serum of rats injected with MSCs and678in the injured carotids where MSCs homed, additional679experiments will be necessary to confirm the role of VEGF680as a main mediator of the MSC therapeutic antirestenotic681effect. Moreover, as MSCs have been efficaciously defined682as “multidrug dispensers” [15], additional studies will be683necessary to identify potentially synergic molecules.684It has been recently highlighted that SDF-1α can be685produced and secreted by MSCs [31, 32]. Nonetheless, it686has also been reported that MSCs do not produce SDF-1α687but they consume it in vitro [33]. Most importantly, SDF-1α688constitutive expression is upregulated in injured arteries [12,68934, 35], playing a role in the recruitment of stem cells for690tissue repair and in inflammation. In agreement with this691observation, the ELISA assay revealed a significant increase692of SDF-1α in the serum of rats at 7 days after carotid693arteriotomy. On the basis of our data and of the current694literature, we can speculate that the decreased concentration695of SDF-1α under the basal levels observed at 7 days after696arteriotomy in the serum of rats treated with MSCs could be697mainly related to a reduced secretion by the injured vascular698wall, thanks to the early paracrine reparative and immuno-699modulatory action played by injected MSCs, in synergy with700a sequestering activity played by the CXCR4 receptors701expressed by MSCs and by vascular cells at the injury site.702Moreover, it could be speculated a role also for VEGF,703whose concentration increased in MSC-treated rats (Fig. 5),704as it has been demonstrated that relative dynamic changes of705VEGF and SDF-1α occur after tissue injury [36] or706disruption of the CXCR4/SDF-1α axis [37], in turn related707to the mobilization and homing of the stem cells.708The differential analysis of serum samples through their709hybridization with antibody arrays revealed an influence of710allogenic MSCs on the levels of the soluble form of TIMP-1, a711protein able to inhibit the matrix metalloproteinases 2 and 9712and actively involved in the degradation and remodeling of713the extracellular matrix. Of interest, increasing evidence714indicates also a much more complex role for TIMPs, and in715particular for TIMP-1, as growth factors and growth inhibitors716and in cell signal transduction pathways and apoptosis717inhibition [38]. In particular, it has been highlighted a growth718inhibitory effect of TIMP-1 on non-malignant cells [39]. On719this basis, the decrease of the soluble form of TIMP-1 we720observed in the serum of MSC-treated rats could at least in721part be responsible for the reduced carotid remodeling in722MSC-treated rats [8], but could also affect other pathophys-723iological phenomena triggered by carotid arteriotomy,724including cell proliferation.725Antibody array and ELISA data provided also informa-726tion about the immunomodulatory properties of MSCs727injected after rat carotid arteriotomy, supported by the
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
728 reduction of the serum levels of CXCL1, ICAM-1, L-729 Selectin, LIX/CXCL5 and CCL5/RANTES (Figs. 4 and 5).730 The soluble inflammation-related molecules emerged731 during the analysis of rat serum may play a role as732 biomarkers reflecting the reparative and anti-inflammatory733 role of MSCs in the injury site and/or in the activation state734 of circulating cells, but they could also contribute to inter-735 cellular signalling at systemic level and provide new736 insights into MSC potential therapeutic action. The737 inflammation-related molecules emerged in our analysis738 are associated with different pathogenic steps in restenosis739 progression: endothelium activation and leukocyte adhesion740 (ICAM-1, L-Selectin) [41, 42], neutrophil recruitment741 (LIX/CXCL5, CXCL1) [40, 41], chemoattraction of T cells742 and monocytes (CCL5/RANTES) [43]. The decreased743 concentration of these molecules in MSC-treated rats744 support their capacity to interfere with the above mentioned745 steps. These considerations integrate our previous data [8]746 indicating that the engraftment of MSCs in arteriotomy-747 injured carotids reduced the expression of the monocyte748 chemoattractant protein-1 (MCP-1) and of the interleukin-749 1β (IL-1β), known to act as proinflammatory cytokines,750 and increased the expression of transforming growth factor-751 β (TGF−β), endowed with immunosuppressive properties.
752 Conclusions
753 MSCs are multipotent self-renewing cells also endowed with754 immunomodulatory properties. Most importantly, MSCs have755 relevant secretory properties, producing growth factors and756 cytokines with a paracrine, trophic activity. In this study we757 described some of the effects of MSC treatment on the758 pathophysiological phenomena triggered by rat carotid arte-759 riotomy. Overall results suggest that intravenously infused760 MSCs in rats after carotid arteriotomy play a paracrine action,761 inducing a decrease of pro-inflammatory molecules and a762 release of VEGF, possibly leading to a rapid repair of the763 injured vascular wall. Additional experiments will be neces-764 sary to address the mechanisms and identify the mediators at765 the basis of the MSC paracrine action.766767 Acknowledgements We are grateful to Dr. Karen English for768 support with ELISA serum analysis, to Dr. Monica Mattia for769 excellent care of animal welfare and to Ms. M.R. Cipollaro for770 administrative assistance.
771 Grants This work has been partially funded by a SHRO grant to U.G.
772 References773
774 1. Lal BK. Recurrent carotid stenosis after CEA and CAS: diagnosis775 and management. Semin Vasc Surg. 2007;20:259–66.
7762. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R,777Mosca JD, et al. Multilineage potential of adult human mesen-778chymal stem cells. Science. 1999;284:143–7.7793. Beggs KJ, Lyubimov A, Borneman JN, Bartholomew A, Moseley780A, Dodds R, et al. Immunologic consequences of multiple, high-781dose administration of allogeneic mesenchymal stem cells to782baboons. Cell Transplant. 2006;15:711–21.7834. Yokokawa M, Ohnishi S, Ishibashi-Ueda H, Obata H, Otani K,784Miyahara Y, et al. Transplantation of mesenchymal stem cells785improves atrioventricular conduction in a rat model of complete786atrioventricular block. Cell Transplant. 2008;17:1145–55.7875. Shabbir A, Zisa D, Lin H, Mastri M, Roloff G, Suzuki G, et al.788Activation of host tissue trophic factors through JAK-STAT3789signaling: a mechanism of mesenchymal stem cell-mediated790cardiac repair. Am J Physiol Heart Circ Physiol. 2010;299:791H1428–38.7926. Caplan AI, Dennis JE. Mesenchymal stem cells as trophic793mediators. J Cell Biochem. 2006;98:1076–84.7947. Forte A, Di Micco G, Galderisi U, Guarino FM, Cipollaro M, De795Feo M, et al. Molecular analysis of arterial stenosis in rat carotids.796J Cell Physiol. 2001;186:307–13.7978. Forte A, Finicelli M, Mattia M, Berrino L, Rossi F, De Feo M, et798al. Mesenchymal stem cells effectively reduce surgically induced799stenosis in rat carotids. J Cell Physiol. 2008;217:789–99.8009. Forte A, Finicelli M, Grossi M, Vicchio M, Alessio N, Sante P, et801al. DNA damage and repair in a model of rat vascular injury. Clin802Sci (Lond). 2009;80310. Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini804F, Krause D, et al. Minimal criteria for defining multipotent805mesenchymal stromal cells. The International Society for Cellular806Therapy position statement. Cytotherapy. 2006;8:315–7.80711. Neeley WL, Essigmann JM. Mechanisms of formation, genotox-808icity, and mutation of guanine oxidation products. Chem Res809Toxicol. 2006;19:491–505.81012. Forte A, Finicelli M, De Luca P, Quarto C, Onorati F, Sante P, et811al. Expression profiles in surgically-induced carotid stenosis: a812combined transcriptomic and proteomic investigation. J Cell Mol813Med. 2008;12:1956–73.81413. Li D, Zhang C, Song F, Lubenec I, Tian Y, Song QH. VEGF815regulates FGF-2 and TGF-beta1 expression in injury endothelial816cells and mediates smooth muscle cells proliferation and migra-817tion. Microvasc Res. 2009;77:134–42.81814. Hollestelle SC, De Vries MR, Van Keulen JK, Schoneveld AH,819Vink A, Strijder CF, et al. Toll-like receptor 4 is involved in820outward arterial remodeling. Circulation. 2004;109:393–8.82115. Caplan AI. Why are MSCs therapeutic? New data: new insight. J822Pathol. 2009;217:318–24.82316. Chen L, Tredget EE, Wu PY, Wu Y. Paracrine factors of824mesenchymal stem cells recruit macrophages and endothelial825lineage cells and enhance wound healing. PLoS One. 2008;3:826e1886.82717. Salvolini E, Orciani M, Vignini A, Mattioli-Belmonte M,828Mazzanti L, Di Primio R. Skin-derived mesenchymal stem cells829(S-MSCs) induce endothelial cell activation by paracrine mech-830anisms. Exp Dermatol. 19:848–50.83118. Novo E, Busletta C, Bonzo LV, Povero D, Paternostro C,832Mareschi K, et al. Intracellular reactive oxygen species are833required for directional migration of resident and bone marrow-834derived hepatic pro-fibrogenic cells. J Hepatol. 54:964–74.83519. Song H, Cha MJ, Song BW, Kim IK, Chang W, Lim S, et al.836Reactive oxygen species inhibit adhesion of mesenchymal stem837cells implanted into ischemic myocardium via interference of838focal adhesion complex. Stem Cells. 28:555–63.83920. Lanza C, Morando S, Voci A, Canesi L, Principato MC, Serpero LD,840et al. Neuroprotective mesenchymal stem cells are endowed with a841potent antioxidant effect in vivo. J Neurochem. 2009;110:1674–84.
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
842 21. Witherick J, Wilkins A, Scolding N, Kemp K. Mechanisms of843 oxidative damage in multiple sclerosis and a cell therapy approach844 to treatment. Autoimmune Dis. 2011:164608.845 22. Tsubokawa T, Yagi K, Nakanishi C, Zuka M, Nohara A, Ino H, et846 al. Impact of anti-apoptotic and anti-oxidative effects of bone847 marrow mesenchymal stem cells with transient overexpression of848 heme oxygenase-1 on myocardial ischemia. Am J Physiol Heart849 Circ Physiol. 298:H1320-9.850 23. Schrepfer S, Deuse T, Reichenspurner H, Fischbein MP, Robbins851 RC, Pelletier MP. Stem cell transplantation: the lung barrier.852 Transplant Proc. 2007;39:573–6.853 24. Psaltis PJ, Zannettino AC, Worthley SG, Gronthos S. Concise854 review: mesenchymal stromal cells: potential for cardiovascular855 repair. Stem Cells. 2008;26:2201–10.856 25. Lange C, Brunswig-Spickenheier B, Cappallo-Obermann H,857 Eggert K, Gehling UM, Rudolph C, et al. Radiation rescue:858 mesenchymal stromal cells protect from lethal irradiation. PLoS859 One. 6:e14486.860 26. Sadat S, Gehmert S, Song YH, Yen Y, Bai X, Gaiser S, et al. The861 cardioprotective effect of mesenchymal stem cells is mediated by862 IGF-I and VEGF. Biochem Biophys Res Commun.863 2007;363:674–9.864 27. Hutter R, Carrick FE, Valdiviezo C, Wolinsky C, Rudge JS,865 Wiegand SJ, et al. Vascular endothelial growth factor regulates866 reendothelialization and neointima formation in a mouse model of867 arterial injury. Circulation. 2004;110:2430–5.868 28. Asahara T, Bauters C, Pastore C, Kearney M, Rossow S, Bunting869 S, et al. Local delivery of vascular endothelial growth factor870 accelerates reendothelialization and attenuates intimal hyperplasia871 in balloon-injured rat carotid artery. Circulation. 1995;91:2793–872 801.873 29. Markel TA, Wang Y, Herrmann JL, Crisostomo PR, Wang M,874 Novotny NM, et al. VEGF is critical for stem cell-mediated875 cardioprotection and a crucial paracrine factor for defining the age876 threshold in adult and neonatal stem cell function. Am J Physiol877 Heart Circ Physiol. 2008;295:H2308–14.878 30. Cobellis G, Maione C, Botti C, Coppola A, Silvestroni A, Lillo S,879 et al. Beneficial effects of VEGF secreted from stromal cells in880 supporting endothelial cell functions: therapeutic implications for881 critical limb ischemia. Cell Transplant. 2010;19:1425–37.882 31. Bakondi B, Shimada IS, Peterson BM, Spees JL. SDF-1alpha883 secreted by human CD133-derived multipotent stromal cells
884promotes neural progenitor cell survival through CXCR7. Stem885Cells Dev. 2011;20:1021–9.88632. Wang F, Yasuhara T, Shingo T, Kameda M, Tajiri N, Yuan WJ, et887al. Intravenous administration of mesenchymal stem cells exerts888therapeutic effects on parkinsonian model of rats: focusing on889neuroprotective effects of stromal cell-derived factor-1alpha.890BMC Neurosci. 2010;11:52.89133. Schinkothe T, Bloch W, Schmidt A. In vitro secreting profile of892human mesenchymal stem cells. Stem Cells Dev. 2008;17:199–893206.89434. Yin Y, Zhao X, Fang Y, Yu S, Zhao J, Song M, et al. SDF-1alpha895involved in mobilization and recruitment of endothelial progenitor896cells after arterial injury in mice. Cardiovasc Pathol. 2010;19:218–27.89735. Li JM, Zhang X, Nelson PR, Odgren PR, Nelson JD, Vasiliu C, et898al. Temporal evolution of gene expression in rat carotid artery899following balloon angioplasty. J Cell Biochem. 2007;101:399–900410.90136. Deng ZR, Yang C, Ma AQ, Chen XY, Geng T. Dynamic changes902of plasma VEGF, SDF-1 and peripheral CD34+ cells in patients903with acute myocardial infarction. Nan Fang Yi Ke Da Xue Xue904Bao. 2006;26:1637–40.90537. Pitchford SC, Furze RC, Jones CP, Wengner AM, Rankin SM.906Differential mobilization of subsets of progenitor cells from the907bone marrow. Cell Stem Cell. 2009;4:62–72.90838. Chirco R, Liu XW, Jung KK, Kim HR. Novel functions of TIMPs909in cell signaling. Cancer Metastasis Rev. 2006;25:99–113.91039. Taube ME, Liu XW, Fridman R, Kim HR. TIMP-1 regulation of911cell cycle in human breast epithelial cells via stabilization of p27912(KIP1) protein. Oncogene. 2006;25:3041–8.91340. Huo Y, Weber C, Forlow SB, Sperandio M, Thatte J, Mack M, et914al. The chemokine KC, but not monocyte chemoattractant protein-9151, triggers monocyte arrest on early atherosclerotic endothelium. J916Clin Invest. 2001;108:1307–14.91741. Choong ML, Yong YP, Tan AC, Luo B, Lodish HF. LIX: a918chemokine with a role in hematopoietic stem cells maintenance.919Cytokine. 2004;25:239–45.92042. Zarbock A, Ley K, McEver RP, Hidalgo A. Leukocyte ligands for921endothelial selectins: specialized glycoconjugates that mediate922rolling and signaling under flow. Blood. 2011;92343. Halwani R, Al-Abri J, Beland M, Al-Jahdali H, Halayko AJ, Lee924TH, et al. CC and CXC chemokines induce airway smooth muscle925proliferation and survival. J Immunol. 2011;186:4156–63.
926
Cardiovasc Drugs Ther
JrnlID 10557_ArtID 6359_Proof# 1 - 18/11/2011

AUTHOR'S PROOF
UNCORRECTEDPROOF
AUTHOR QUERIES
AUTHOR PLEASE ANSWER ALL QUERIES.
Q1. Please check if the section headings are assigned to appropriate levels.Q2. Figure 1, 3 and 5 - contain poor quality text and text below 6pts. Please provide replacement
otherwise, please advise if we can proceed with the figure/s as is.