Socioeconomic, environmental, demographic and behavioral factors associated with occurrence of...
10
Sot. Sci. Med. Vol. 36, No. 6, pp. 807-816, 1993 Printed in Great Britain 0277-9536/93 $6.00 + 0.00 Pergamon Press Ltd SOCIOECONOMIC, ENVIRONMENTAL, DEMOGRAPHIC AND BEHAVIORAL FACTORS ASSOCIATED WITH OCCURRENCE OF DIARRHEA IN YOUNG CHILDREN IN THE REPUBLIC OF CONGO NANCY B. MOCK,* THOMAS A. SELLERS, AHMED A. ABDOH and ROBERTR. FRANKLIN International Health Academic Program and Center for International Health and Development, School of Public Health and Tropical Medicine, Tulane University, New Orleans, LA 70112, U.S.A. Abstract-This study is the result of a cross-sectional survey undertaken in five regions of the Republic of Congo. A sample of 612 women having children under 3 years of age was interviewed to determine the socioeconomic, environmental, demographic and behavioral factors associated with the occurrence of diarrhea in young children. Logistic regression analysis was used to determine which variables predict the occurrence of diarrhea in a multivariable context. Most of the statistically significant variables were those suggesting behaviorally mediated modes of transmission. These include: type of weaning food fed to the child, maternal age, sex of the child, maternal sickness and method of refuse disposal. Male children had a more than two-fold odds of experiencing recent diarrhea than did female children among those greater than 1 year of age. Although breastfeeding status was not statistically significantly associated with diarrhea1 disease, children under 1 year of age who were already weaned had a greater odds of disease than those who were still breasted. Due to the pattern of extended breastfeeding in this population, this relationship was difficult to assess. Urban residence also was highly associated with diarrhea] disease occurrence. Urban residence is likely to reflect a host of socioeconomic, environmental and behavioral factors. These findings underscore the potential impact of educational interventions on the occurrence of diarrhea1 disease among young children. Key HordsAiarrhea, etiologic factors, developing countries, young children, Republic of Congo INTRODUCTION Diarrhea1 diseases represent a major cause of morbid- ity and mortality in all developing countries [I]. Children under the age of 5 are the most susceptible population group, and annual incidence rates ranging from 2 to 12 episodes have been reported [2, 31. For the more than 470 million children under 5 years of age residing in developing countries, an average of only three episodes of diarrhea per child per year would still mean 1.4 billion episodes annually [4, 51. Several studies have examined the relationship be- tween occurrence of diarrhea1 disease and family socio-economic and household environmental characteristics [6-131 although results were inconsist- ent where the significance of these variables is con- cerned. More recent studies have evaluated maternal child care behaviors as related predictors of diarrhea1 disease and as potentially mediating influences on resources and the environment [lo, 14-191. These studies, too, have not been consistent in their findings. The purpose of this study is to assess socio-economic, environmental, demographic and especially maternal behavioral variables as predictors of the occurrence of diarrhea1 disease among children *Address correspondence and reprint requests to: Nancy B. Mock, 1501 Canal Street. Suite 1305. New Orleans. LA 70112, U.S.A. in the Republic of Congo using survey data from a large-scale cross-sectional survey. METHODS AND MATERIALS The data reported here were collected during a cross-sectional survey conducted in the Republic of Congo between June and October 1981. A stratified cluster sample was selected from Brazzaville, Owando, Mossendjo, and Kinkala provinces, which are representative of the countrys major ecologic, economic, ethnic and urban and rural divisions. Brazzaville is the capital and largest city with an estimated 25% of the country’s population, while the other three zones are predominantly rural. Equal numbers of villages were selected in each strata and a systematic sample of mothers with children under 30 months of age was selected in each village. Details of the sampling scheme have been published elsewhere [20]. A questionnaire was designed to collect infor- mation on socio-economic and demographic factors, environmental sanitation, feeding practices, and health care services utilization. Health status vari- ables including nutritional status and recent morbid- ity experienced by the youngest child in the family also were assessed. Table 1 shows the list of variables examined in this analysis. A unique aspect of this data set for the region is that a large percentage of the 807
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Socioeconomic, environmental, demographic and behavioral factors associated with occurrence of...

Sot. Sci. Med. Vol. 36, No. 6, pp. 807-816, 1993 Printed in Great Britain
0277-9536/93 $6.00 + 0.00 Pergamon Press Ltd
SOCIOECONOMIC, ENVIRONMENTAL, DEMOGRAPHIC AND BEHAVIORAL FACTORS ASSOCIATED WITH
OCCURRENCE OF DIARRHEA IN YOUNG CHILDREN IN THE REPUBLIC OF CONGO
NANCY B. MOCK,* THOMAS A. SELLERS, AHMED A. ABDOH and ROBERT R. FRANKLIN
International Health Academic Program and Center for International Health and Development, School of Public Health and Tropical Medicine, Tulane University, New Orleans, LA 70112, U.S.A.
Abstract-This study is the result of a cross-sectional survey undertaken in five regions of the Republic of Congo. A sample of 612 women having children under 3 years of age was interviewed to determine the socioeconomic, environmental, demographic and behavioral factors associated with the occurrence of diarrhea in young children. Logistic regression analysis was used to determine which variables predict the occurrence of diarrhea in a multivariable context. Most of the statistically significant variables were those suggesting behaviorally mediated modes of transmission. These include: type of weaning food fed to the child, maternal age, sex of the child, maternal sickness and method of refuse disposal. Male children had a more than two-fold odds of experiencing recent diarrhea than did female children among those greater than 1 year of age. Although breastfeeding status was not statistically significantly associated with diarrhea1 disease, children under 1 year of age who were already weaned had a greater odds of disease than those who were still breasted. Due to the pattern of extended breastfeeding in this population, this relationship was difficult to assess. Urban residence also was highly associated with diarrhea] disease occurrence. Urban residence is likely to reflect a host of socioeconomic, environmental and behavioral factors. These findings underscore the potential impact of educational interventions on the occurrence of diarrhea1 disease among young children.
Key HordsAiarrhea, etiologic factors, developing countries, young children, Republic of Congo
INTRODUCTION
Diarrhea1 diseases represent a major cause of morbid- ity and mortality in all developing countries [I]. Children under the age of 5 are the most susceptible population group, and annual incidence rates ranging from 2 to 12 episodes have been reported [2, 31. For the more than 470 million children under 5 years of age residing in developing countries, an average of only three episodes of diarrhea per child per year would still mean 1.4 billion episodes annually [4, 51. Several studies have examined the relationship be- tween occurrence of diarrhea1 disease and family socio-economic and household environmental characteristics [6-131 although results were inconsist- ent where the significance of these variables is con- cerned. More recent studies have evaluated maternal child care behaviors as related predictors of diarrhea1 disease and as potentially mediating influences on resources and the environment [lo, 14-191. These studies, too, have not been consistent in their findings. The purpose of this study is to assess socio-economic, environmental, demographic and especially maternal behavioral variables as predictors of the occurrence of diarrhea1 disease among children
*Address correspondence and reprint requests to: Nancy B. Mock, 1501 Canal Street. Suite 1305. New Orleans. LA 70112, U.S.A.
in the Republic of Congo using survey data from a large-scale cross-sectional survey.
METHODS AND MATERIALS
The data reported here were collected during a cross-sectional survey conducted in the Republic of Congo between June and October 1981. A stratified cluster sample was selected from Brazzaville, Owando, Mossendjo, and Kinkala provinces, which are representative of the countrys major ecologic, economic, ethnic and urban and rural divisions. Brazzaville is the capital and largest city with an estimated 25% of the country’s population, while the other three zones are predominantly rural. Equal numbers of villages were selected in each strata and a systematic sample of mothers with children under 30 months of age was selected in each village. Details of the sampling scheme have been published elsewhere [20].
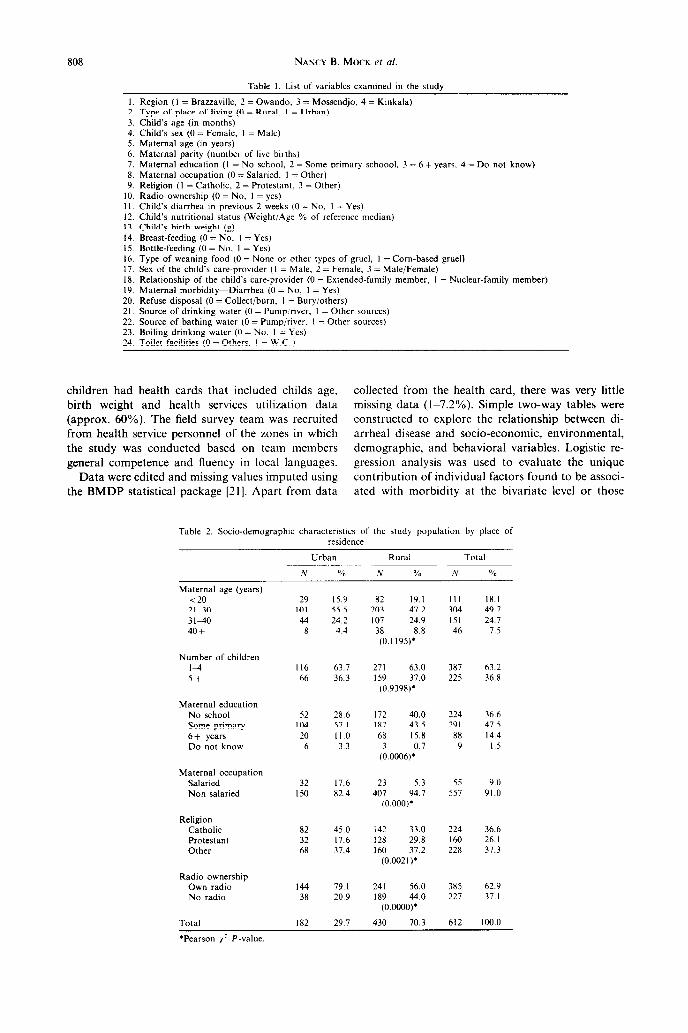
A questionnaire was designed to collect infor- mation on socio-economic and demographic factors, environmental sanitation, feeding practices, and health care services utilization. Health status vari- ables including nutritional status and recent morbid- ity experienced by the youngest child in the family also were assessed. Table 1 shows the list of variables examined in this analysis. A unique aspect of this data set for the region is that a large percentage of the
807
808 NANCY B. MOCK et al.
Table I. List of variables examined in the study
I. Region (1 = Brazzaville, 2 = Owando, 3 = Mossendjo, 4 = Kinkala) 2. Type of place of living (0 = Rural, I = Urban) 3. Child’s age (in months) 4. Child’s sex (0 = Female, I = Male) 5. Maternal age (in years) 6. Maternal parity (number of live births) 7. Maternal education (I = No school, 2 = Some primary schoool. 3 = 6 + years. 4 = Do not know) 8. Maternal occupation (0 = Salaried, I = Other) 9. Religion (I = Catholic, 2 = Protestant, 3 = Other)
IO. Radio ownership (0 = No, I = yes) I I. Child’s diarrhea in previous 2 weeks (0 = No, I = Yes) 12. Child’s nutritional status (Weight/Age % of reference median) 13. Child’s birth weight (g) 14. Breast-feeding (0 = No, I = Yes) 15. Bottle-feeding (0 = No, I = Yes) 16. Type of weaning food (0 = None or other types of gruel, I = Corn-based gruel) 17. Sex of the child’s care-provider (I = Male. 2 = Female, 3 = Male/Female) 18. RelatIonship of the child’s care-provider (0 = Extended-family member, I = Nuclear-family member) 19. Maternal morbidity-Diarrhea (0 = No, I = Yes) 20. Refuse disposal (0 = Collect/burn, I = Bury/others) 21. Source of drinking water (0 = Pump:river, I = Other sources) 22. Source of bathing water (0 = Pump/river, I = Other sources) 23. Boiling drinking water (0 = No, I = Yes) 24. Toilet facilities (0 = Others, I = W.C )
children had health cards that included childs age, collected from the health card, there was very little birth weight and health services utilization data missing data (l&7.2%). Simple two-way tables were (approx. 60%). The field survey team was recruited constructed to explore the relationship between di- from health service personnel of the zones in which arrheal disease and socio-economic, environmental,
the study was conducted based on team members demographic, and behavioral variables. Logistic re-
general competence and fluency in local languages. gression analysis was used to evaluate the unique Data were edited and missing values imputed using contribution of individual factors found to be associ-
the BMDP statistical package [2l]. Apart from data ated with morbidity at the bivariate level or those
Table 2. So&-demographlc charactenstu of the study population by place of residence
Urban Rural Total
N % N % N %
Maternal age (years) <20 21-30 3140 40+
Number of children I4 St
Maternal education No school Some primary 6+ years Do not know
Maternal occupation Salaried Non salaried
Religion Catholic Protestant Other
Radio ownership Own radio No radio
Total
29 15.9
IO1 55.5
44 24.2 8 4.4
II6 63.7
66 36.3
52 28.6
104 57 I
20 II.0
6 3.3
32 17.6
I50 82.4
82 45.0
32 17.6 6X 37.4
I44 79.1
38 20.9
182 29.7
82 19.1 203 47.2
107 24.9
38 8.8
(0.1195)'
271 63.0
I59 37.0
(0.9398)'
172 40.0 187 43.5
68 15.8
3 0.7
(0.0006)'
23 5.3
407 94.7 (o.ooo)*
142 33.0 128 29.8 160 37.2
(0.0021)'
241 56.0 I89 44.0
(0.0000)'
430 70.3
III 18.1
304 49.7
I51 24.7 4b 7.5
387 63.2
225 36.8
224 36.6
291 47 5
88 14.4 9 1.5
55
557
9.0
91.0
224 36.6
160 26.1
228 37.3
385 62.9 227 37.1
612 100.0
‘Pearson x2 P-value
Factors associated with diarrhea 809
Table 3. Child socio-demographic characteristics by place of residence
Urban Rural Total
N % N % N %
Child’s sex Male Female
Child’s age (months) o-6 7-12 13-24 25 +
Child’s diarrhea (previous 2 weeks) Yes NO
Ch;dllsnna;Ltritional status (Gomez)
Grade I Grade II/III
Total
91 50.0 91 50.0
32 17.6 40 22.0 72 39.6 38 20.8
38 20.9 I44 19. I
94 51.6 75 41.2 13 1.2
182 29.7
I95 43.3 235 54.7 (0.3343).
70 16.3 83 19.3
188 43.7 20.7
(804743).
76 17.7 354 82.3 (0.3515)’
208 48.4 176 40.9 46 10.7 (0.3759);
430 70.3
286 46.7 326 53.3
102 16.7 123 20. I 260 42.5 127 20.7
II4 18.6 498 81.4
302 49.4 251 41 .o
59 9.6
612 100.0
*Pearson x2 P-value.
commonly cited in the literature as being associated with the occurrence of diarrhea1 disease [22]. Finally, adjusted confidence intervals for the odds ratios were computed for comparative purposes that make a conservative correction for the sampling design effect.
RESULTS
Table 2 shows that the socio-demographic and economic characteristics of this sample are not atyp- ical of a central African population. Most of the sample is rural (approx. 70%), and most mothers are under 40 years of age (92.5%), with nearly two-thirds under 30 years of age. This sample is largely com- prised of multiparous women, each having an average of 5.9 children. More than one-third of the women interviewed had more than five living children.
The level of education among mothers in the sample is low but comparable to other central African countries. More than one-third have no formal education, and only 14.4% have had 6 or more years of schooling. As expected, the percentage of mothers with some formal education was greater in urban than in rural areas. Less than 10% of mothers held a salaried job, although the percentage was much higher in urban than in rural areas (17.6% vs 5.3%). In terms of religious affiliation, the sample was a mixture of Catholics, Protestants, and other religions that are indigenous derivatives of Christianity. Almost half of the urban women were Catholic compared to one-third of the rural women.
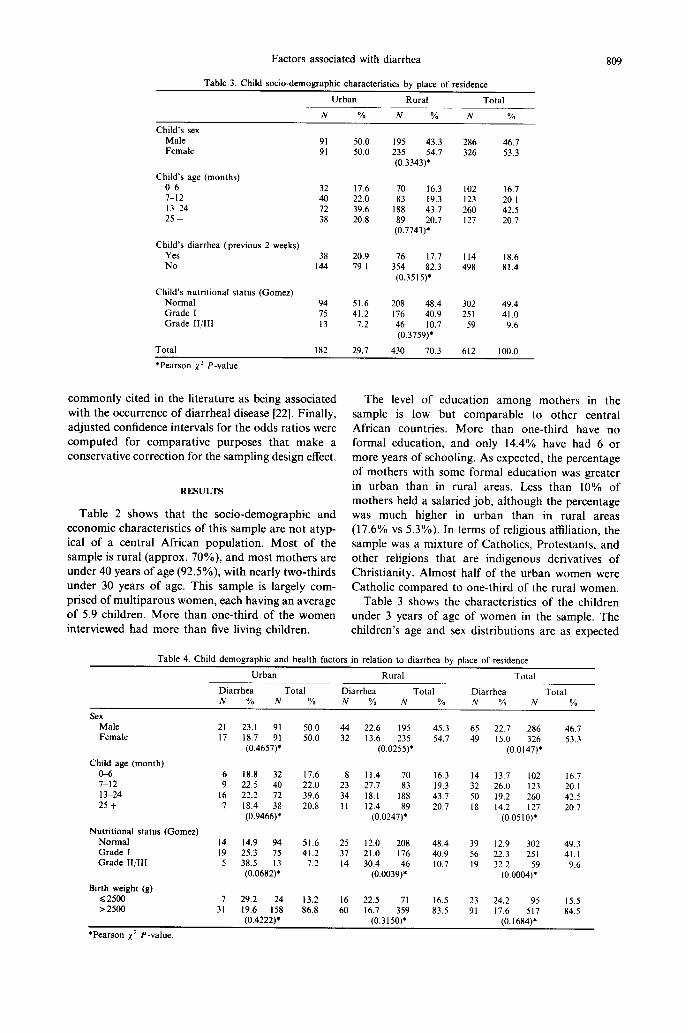
Table 3 shows the characteristics of the children under 3 years of age of women in the sample. The children’s age and sex distributions are as expected
Table 4. Child demographic and health factors in relation to diarrhea by place of residence
Urban Rural Total
sex
Diarrhea Total Diarrhea Total Diarrhea Total N % N % N % N % N % N %
Male 21
Female I7 23.1 91 18.7 91
(0.4657)'
50.0 44
50.0 32 22.6 I95
13.6 235
(0.0255)*
45.3 65 54.7 49
22.7 286 15.0 326
(0.0 147)’
46.1 53.3
Child age (month) 0+5 7-12 13-24 25 f
6 9
16 7
18.8 32 22.5 40
22.2 72
18.4 38
(0.9466)*
17.6 8 22.0 23
39.6 34
20.8 II
II.4 70
27.7 83
18.1 I88
12.4 89
(0.0247)'
16.3 14 19.3 32
43.7 50
20.7 18
13.7 102
26.0 123
19.2 260 14.2 127
(0.0510)*
16.7 20. I 42.5 20.7
Nutritional status (Gomez) Normal Grade I Grade II/III
14 I9 5
14.9 94 25.3 75
38.5 13 (0.0682)*
51.6 25 41.2 37
7.2 14
12.0 208
21.0 176
30.4 46
(0.0039)'
48.4 39
40.9 56 10.7 19
12.9 302 22.3 251 32.2 (o.ooo4;9
49.3 41.1
9.6
Birth weight (g) <2500 > 2500
29.2 24 13.2 16 22.5 71 16.5 23 24.2 95 19.6 I58 86.8 60 16.7 359 83.5 91 17.6 517
15.5 x4.5 3;
'Pearson x2 P-value.
(0.4222). (0.3150)* (0.1684).
NANCK B. Mote et al.
~I
All ages O-12 M 13.24 M >24 M
Age groups *
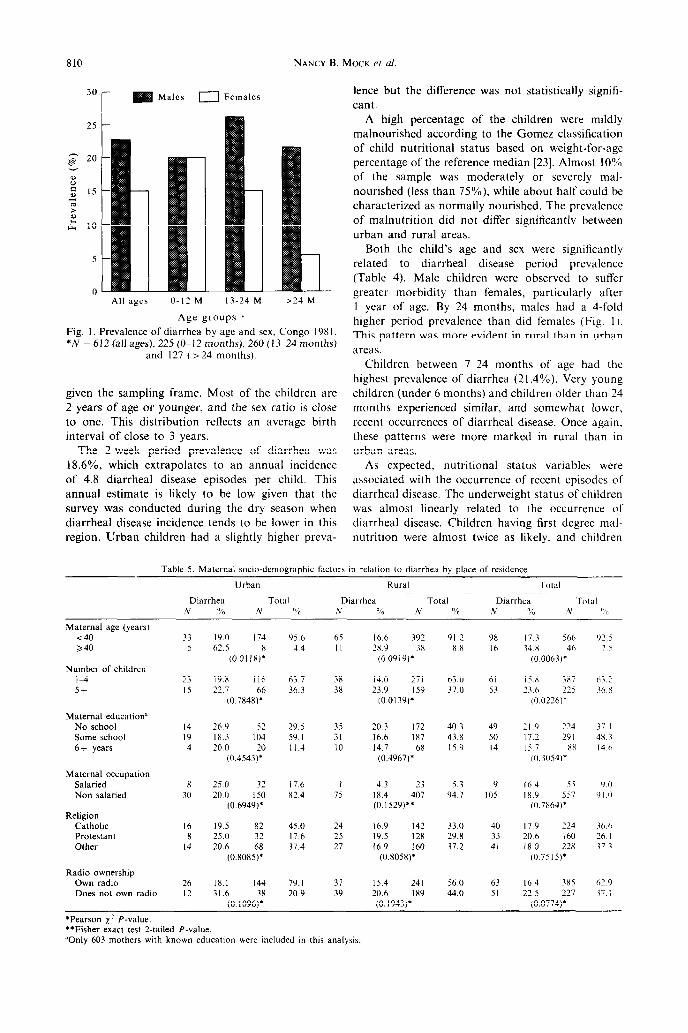
Fig. 1. Prevalence of diarrhea by age and sex, Congo 198 1. *N = 612 (all ages), 225 (O-12 months), 260 (13-24 months)
and 127 (> 24 months).
given the sampling frame. Most of the children are
2 years of age or younger, and the sex ratio is close to one. This distribution reflects an average birth interval of close to 3 years.
The 2-week period prevalence of diarrhea was 18.6%. which extrapolates to an annual incidence of 4.8 diarrhea1 disease episodes per child. This annual estimate is likely to be low given that the survey was conducted during the dry season when diarrhea1 disease incidence tends to be lower in this region. Urban children had a slightly higher preva-
lence but the difference was not statistically signifi- cant.
A high percentage of the children were mildly malnourished according to the Gomez classification of child nutritional status based on weight-for-age percentage of the reference median [23]. Almost 10% of the sample was moderately or severely mal- nourished (less than 75%), while about half could be characterized as normally nourished. The prevalence of malnutrition did not differ significantly between urban and rural areas.
Both the child’s age and sex were significantly related to diarrhea1 disease period prevalence (Table 4). Male children were observed to suffer greater morbidity than females, particularly after I year of age. By 24 months, males had a 4-fold higher period prevalence than did females (Fig. I ). This pattern was more evident in rural than in urban areas.
Children between 7-24 months of age had the highest prevalence of diarrhea (21.4%). Very young children (under 6 months) and children older than 24 months experienced similar, and somewhat lower. recent occurrences of diarrhea1 disease. Once again, these patterns were more marked in rural than in urban areas.
As expected, nutritional status variables were associated with the occurrence of recent episodes of diarrhea1 disease. The underweight status of children was almost linearly related to the occurrence of diarrhea1 disease. Children having first degree mal- nutrition were almost twice as likely. and children
Table 5. Maternal socio-demographtc factors in relation to diarrhea by place of residence
Urban RWCdl Total
Diarrhea TOWI Diarrhea Total Dwrhea Total N a,$ .Y “j” N % hi % N % N 1’ ”
Maternal age (years) <40 a40
Number of children l-4 5+
Maternal education” No school Some school 6f years
Maternal occupation Salaried Non salaried
Religmn Catholic Protestant Other
Radio ownership Own radio Does not own radio
33 5
23 15
14 I9 4
x 30
I6 8
L4
26 I2
19.0 174 62.5 x
CO.01 IX)’
19.x I I6 22.7 66
(0.7X48)’
26.9 52 18.3 104 20.0 20
(0.4543)’
25.0 32 20.0 150
(0.b949)’
19.5 82 25.0 32 20.6
(0.8085:~
IX.1 144 79.1 37 15.4 241
95.6 65 44 II
b3.7 38 36.3 3x
29.5 35 59. I 31 II.4 IO
17.6 I x2 4 7s
45.0 24 17.6 25 37.4 27
16.6 392 2X 9 3x
(0.0919)’
14.0 271 23.9 I59
(0.0139)’
20.3 I72 Ihb I87 14.7 68
(0.4967)’
4.3 23
IS.4 407 (0.1529)”
16.9 142 19.5 I28 16.9 160
(0.X058)*
31.6 (0. IO,,:.”
20.9 39 20.6 I89 (0.1943)’
91.2 98 xx I6
I7 3 5bb 34 x 46
(0.0063~’
y2.q
7
63.0 37.0
61 15.X 3X7 53 23.b 225
(O.OZ?b)*
b3.7
36.X
40.3 43.x 15.9
49 ?I.‘) ‘24 50 17.2 291 I4 15.7 xx
~0.3054)*
37.1 1X.3 14.6
53 94 7
9 IO5
I64 55 IX.9 557 (0.7Xb4)*
Y 0 ‘)I n
33.0 29.X 37.2
40 17.9 224 33 20.6 I60 41 18.0 228
(0 7515)’
3b.b 76 I 17 3
56.0 63 16.4 385 62 Y 44.0 51 22 5 227 37 I
(0.0774)1
*Pearson x2 P-value. **Fisher exact test 2-tailed P-value. *Only 603 mothers with known education were included in this analysis.
Factors associated with diarrhea 811
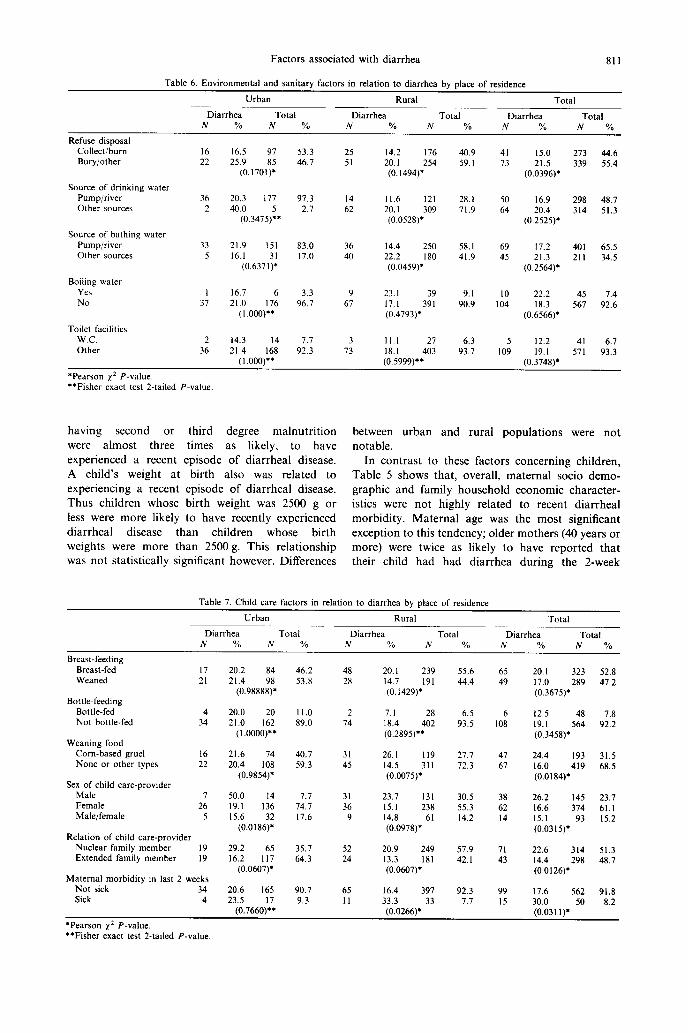
Table 6. Environmental and sanitary factors in relation to diarrhea by place of residence
Urban Rural Total
Diarrhea Total Diarrhea Total Diarrhea Total N % N % N % N % N % N %
Refuse disposal Collect/burn Bury/other
I6 22
16.5 97 25.9 85
(0.1701)*
20.3 177 40.0
(0.3475):*
21.9 151 16.1
(0.637 I::
16.7 6 21.0 176
(l.ooo)**
14.3 I4 21.4 I68
(I .ooo)**
53.3 25 46.7 51
14.2 176 20. I 254 (0.1494)’
40.9 59. I
41 13
28.1 50 71.9 64
58.1 69 41.9 45
9.1 90.9
IO 104
6.3 93.7
5 12.2 41 6.1 109 19.1 571 93.3
(0.3748)’
15.0 21.5
(0.0396)*
213 44.6 339 55.4
Source of drinking water Pump/river Other sources
36 2
97.3 14 2.1 62
Il.6 I21 20. I 309 (0.0528)*
16.9 20.4
(0.2525).
298 48.7 314 51.3
Source of bathing water Pump/river Other sources
33 5
83.0 36 17.0 40
14.4 250 22.2 I80 (0.0459)8
Il.2 21.3
(0.2564);
401 65.5 211 34.5
Boiling water Yes NO
3.3 9 96.7 67
23.1 39 17.1 391 (0.4793)*
II.1 27 18.1 403 (0.5999)**
22.2 18.3
(0.6566)’
45 7.4 567 92.6 37
Toilet facilities W.C. Other
2 36
7.7 3 92.3 73
*Pearson x2 P-value. **Fisher exact test 2-tailed P-value
having second or third degree malnutrition were almost three times as likely, to have experienced a recent episode of diarrhea1 disease. A child’s weight at birth also was related to experiencing a recent episode of diarrhea1 disease. Thus children whose birth weight was 2500 g or less were more likely to have recently experienced diarrhea1 disease than children whose birth weights were more than 2500 g. This relationship was not statistically significant however. Differences
between urban and rural populations were not notable.
In contrast to these factors concerning children, Table 5 shows that, overall, maternal socio demo- graphic and family household economic character- istics were not highly related to recent diarrhea1 morbidity. Maternal age was the most significant exception to this tendency; older mothers (40 years or more) were twice as likely to have reported that their child had had diarrhea during the 2-week
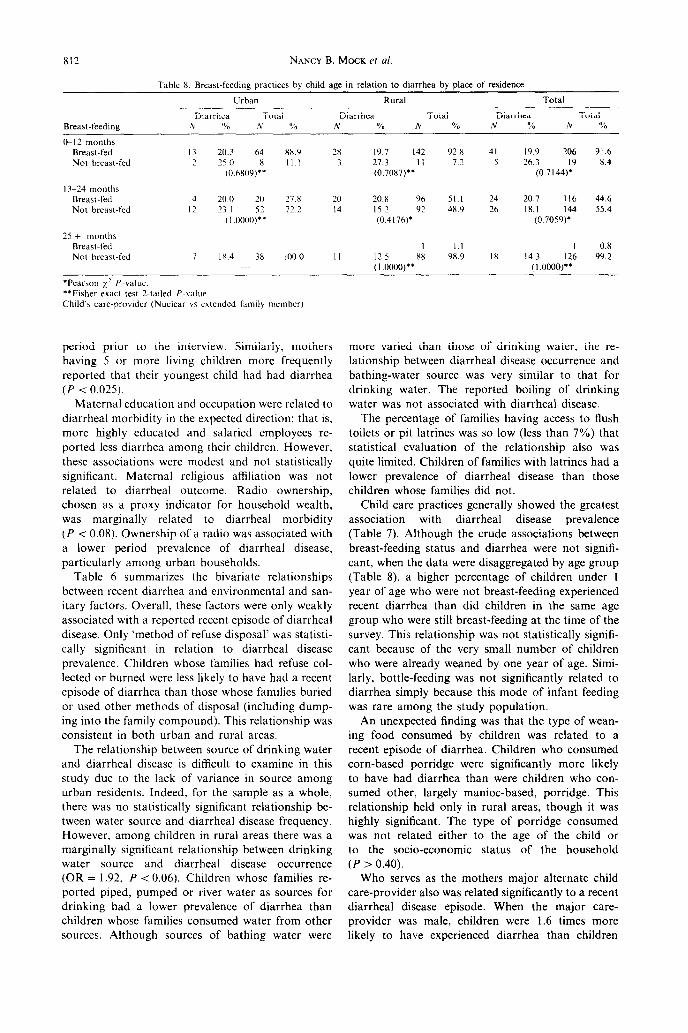
Table 7. Child care factors in relation to diarrhea by place of residence
Urban Rural Total
Diarrhea Total Diarrhea Total Diarrhea Total N % N % N 0% N % N % N %
Breast-feeding Breast-fed I7 Weaned 21
Bottle-feeding Bottle-fed 4 Not bottle-fed 34
Weaning food Corn-based gruel 16 None or other types 22
Sex of child care-provider Male 7 Female 26 Male/female 5
Relation of child care-provider Nuclear family member 19 Extended family member I9
Maternal morbidity in last 2 weeks Not sick 34 Sick 4
20.2 84 21.4 98
(0.98888)*
20.0 20 21.0 162
(I .oooo)**
21.6 74 20.4 I08
(0.9854)*
50.0 14 19.1 136 15.6 32
(0.0186)’
29.2 65 16.2 II7
(0.0607)’
20.6 I65 23.5
(0.7660:~
46.2 48 53.8 28
20.1 239 14.7 I91 (0.1429)’
II.0 2 89.0 74
7.1 28 18.4 402 (0.2895)**
40.7 31 59.3 45
26. I II9 14.5 311 (0.0075)’
7.7 31 74.7 36 17.6 9
23.7 I31 15.1 238 14.8 61 (0.0978)’
35.7 52 64.3 24
20.9 249 13.3 I81 (0.0607)*
90.7 65 16.4 397
55.6 65 44.4 49
6.5 6 93.5 I08
27.7 47 72.3 67
30.5 38 55.3 62 14.2 I4
57.9 42.1
92.3 7.7
71 43
99 I5
20. I 323 52.8 17.0 289 47.2 (0.3675)’
12.5 48 7.8 19.1 564 92.2 (0.3458)*
24.4 193 31.5 16.0 419 68.5 (0.0184)’
26.2 I45 23.7 16.6 374 61.1 15.1 93 15.2 (0.0315).
22.6 314 51.3 14.4 298 48.1 (0.0 I26)*
17.6 562 91.8 30.0 50 8.2 9.3 II 33.3 33
(0.0266)’ (0.0311)*
‘Pearson x2 P-value. **Fisher exact test 2-tailed P-value.
812
Breast-feedme
NANCY B. MOCK et al.
Table 8. Breast-feeding practices by child age in relation to diarrhea by place of residence
Urban Rllral Total
Diarrhea Total Diarrhea Total Diarrhea Total ,A % N % N % N % N % N %
&I2 months Breast-fed Not breast-fed
13-24 month5 Breast-fed Not breast-fed
25 + months Breast-fed Not breast-fed
I3 20.3 64 8X.9 2x 19.7 142 1 L 25.0 (“.6x09)*: II I 3 27.3 II
(0.7087)”
4 20 0 20 27.8 20 20.8 96 51.1 24 20.7 II6 44.6 I2 23. I 52 72.2 14 I52 92 4x 9 26 18.1 144 55.4
( I .oooo)** (0.4176)’ (0.7059)’
7 I x.4 38 100.0 II 12.5 xx (I .0000)”
92.x 41 19.9 206 91.6 72 5 26 3 I9 x.4
(0 7144)’
I.1 I 0.8 9x.9 IX 14.3 126 99.2
(I 0000Y
*Pearson 1: **Fisher test P-value. Child‘s care-provider (Nuclear YS extended family member)
period to interview. mothers 5 more children frequently
that youngest had diarrhea <
Maternal and were to morbidity the direction; is,
highly and employees ported diarrhea their However,
associations modest not significant. religious was related diarrhea1 Radio chosen a indicator household was related diarrhea1 (P 0.08). of radio associated a period of disease,
among households. 6 the relationships
recent and and itary Overall, factors only associated a recent of disease. ‘method refuse was cally in to disease
Children families refuse lected burned less to had recent
of than whose buried used methods disposal dump- into family This was
in urban rural The between of water
diarrhea1 is to in study to lack variance source urban Indeed, the as whole,
was statistically relationship tween source diarrhea1 frequency.
among in areas was marginally relationship drinking
source diarrhea1 occurrence = P 0.06). whose re-
piped, or water sources drinking a prevalence diarrhea children families water other
Although of water
more than of water, re- between disease and
source very to for water. reported of
water not with disease. percentage families access flush or latrines so (less 7%)
statistical of relationship was limited. of with had
lower of disease those whose did
Child practices showed greatest with disease
(Table Although crude between status diarrhea not
cant, the were by group 8). higher of under
year age were breast-feeding recent than children the age
who still at time the This was statistically
cant of very number children were weaned one of Simi-
bottle-feeding not related diarrhea because mode infant was among study
An finding that type wean- food by was to
recent of Children consumed porridge significantly likely
have diarrhea were who sumed largely porridge. relationship only rural though was
significant. type porridge was related to age the or
the status the (P 0.40).
serves the major child also related to recent
disease When major provider male, were times likely have diarrhea children
Tab
le
9.
Log
istic
re
gres
sion
an
alys
is
mod
el
95%
C
onfi
denc
e in
terv
al
Tel
Tll
Coe
ffic
ient
SE
_
Coe
ffic
ient
/SE
O
dds
ratio
(U
nadj
uste
d)
(Def
f A
djus
ted)
Inte
rcep
t B
reas
t-fe
edin
g (b
reas
t-fe
d vs
no
t)
Bot
tle-f
eedi
ng
(bot
tle-f
ed
vs
not)
W
eani
ng
food
(C
orn-
base
d gr
uel
vs
not)
C
hild
’s
(>lZ
M
vs
<l2
M)
age
Chi
ld’s
se
x (M
ale
vs
fem
ale)
Bir
th
wei
ght
(LB
W
vs
norm
al)
Mat
erna
l ag
e (2
40
year
s vs
~4
0)
Mat
erna
l si
ckne
ss
(Sic
k vs
no
t)
Mat
erna
l ed
ucat
ion
(Som
e sc
hool
Y
S no
ne)
Mat
erna
l oc
cupa
tion
(Sal
arie
d vs
ot
her)
N
umbe
r of
ch
ildre
n (5
+
vs
~5)
Chi
ld’s
ca
re-p
rovi
der
(Nuc
lear
vs
ex
tend
ed
fam
ily
mem
ber)
R
adio
ow
ners
hip
(ow
n vs
no
t)
Sou
rce
of
drin
king
w
ater
(O
ther
vs
pu
mp/
rive
r)
Ref
use
disp
osal
(O
ther
vs
bu
m/c
olle
ct)
Toi
let
faci
litie
s (O
ther
vs
W
C)
Pla
ce
of
resi
denc
e (U
rban
vs
ru
ral)
B
reas
t fe
edin
g x
Age
in
tera
ctio
n Se
x x
Age
in
tera
ctio
n W
eani
ng
food
x
Res
iden
ce
inte
ract
ion
*Goo
dnes
s of
fit
x2
= 4
61.0
0 w
ith
P-va
lue
>0.
7.
“See
Tab
le
9 fo
r ef
fect
m
odif
icat
ion
adju
sted
od
ds
ratio
. ‘P
<
0.02
5.
ZP
<
0.05
.
- I .7
9200
0.
9588
-
1.86
9 -0
.843
68
0.60
52
- 1.
394
a
-0.6
2845
0.
4902
-
1.28
2 0.
533
(0.2
04,
1.39
4)
(0.1
37,
2.07
6)
0.73
455
0.29
49
2.49
1’
a -
I .57
420
0.63
23
-2.4
90’
0.20
7 (0
.060
,0.7
15)
(0.0
36,
1.19
5)
0.03
607
0.35
36
0.10
2 a
0.36
805
0.29
75
I.23
7 I .4
45
(0.8
07,2
.589
) (0
.633
,3.2
96)
0.84
176
0.39
09
2.15
3’
2.32
0 (I
.07
9,4.
992)
(0
.785
,6.8
57)
0.77
502
0.35
63
2. I7
52
2.17
1 (I
.08
0,4.
364)
(0
.808
, 5.
828)
0.
0199
7 0.
2694
0.
074
1.02
0 (0
.602
, I .7
30)
(0.4
83,2
.153
) -0
.093
29
0.42
22
-0.2
21
0.91
I
(0.3
98.2
.084
) (0
.283
,2.9
36)
0.15
062
0.26
82
0.56
2 I.
163
(0.6
87,
1.96
7)
(0.5
53.2
.445
) 0.
5462
9 0.
2549
2.
1432
1.
727
(1.0
48,2
.846
) (0
.852
,3.5
00)
-0.3
7696
0.
2380
-
1.58
4 0.
686
(0.4
30,
1.09
4)
(0.3
55,
1.32
7)
0.51
546
0.32
27
1.59
7 1.
674
(0.8
90,
3.15
2)
(0.6
85,4
.096
) 0.
6242
9 0.
2316
2.
696’
1.
867
(1.1
86,2
.939
) (0
.982
. 3.
548)
0.
4810
4 0.
5308
0.
906
I.61
8 (0
.572
.4.5
79)
(0.3
71,
7.04
5)
I .24
060
0.39
90
3.1
IO’
3.45
8 (1
.582
,7.5
58)
(1.1
44,1
0.45
0)
I .25
630
0.67
78
1.85
3 1
0.87
877
0.45
97
I.91
2 a
-0.8
4653
0.
4987
-
1.69
8 a
814 NANCY B. MOCK et al
looked after primarily by women or when the respon- sibility was evenly shared between men and women. Children who were cared for primarily by extended- family members were healthier than those cared for mainly by nuclear-family members. Another unusual relationship examined in this study was the associ- ation between maternal and child diarrhea1 disease during the same 2-week period prior to the survey. Rural children whose mothers had experienced a diarrhea1 episode were twice as likely to have had diarrhea as children whose mothers did not report diarrhea] morbidity.
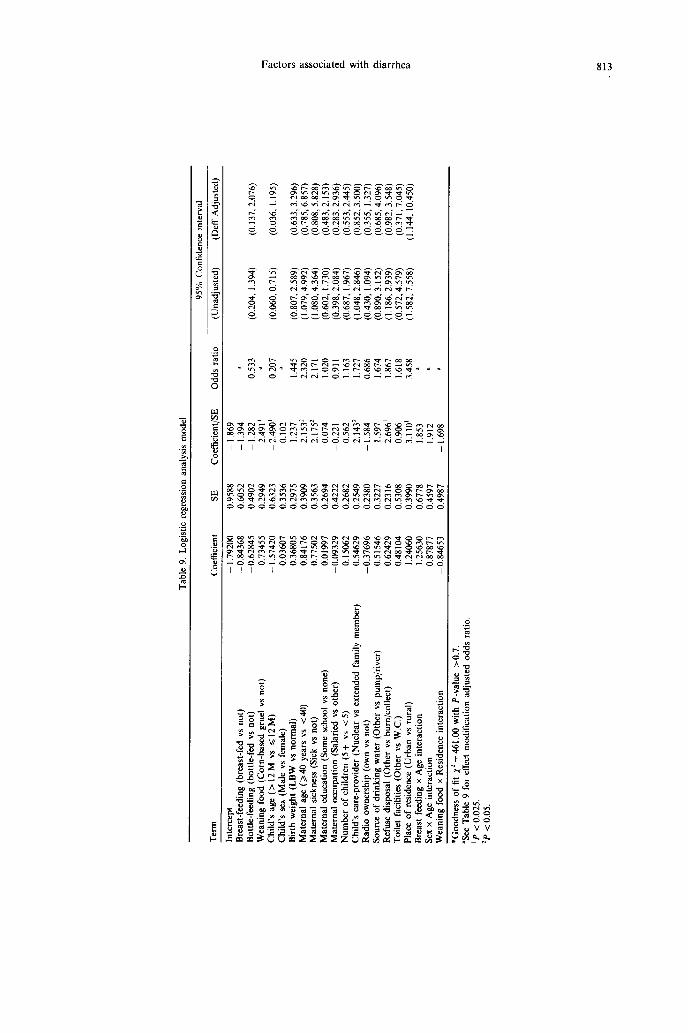
Table 9 summarizes the results of logistic re- gression analysis. including all major socio-economic, demographic, environmental and child-feeding and child-care variables found to be associated with the diarrhea outcome variable in the bivariate analysis, or commonly cited in the literature as being associ- ated with this outcome. The most significant was that the odds were 3.5 times greater for urban than for rural children. Maternal age greater than 40 and maternal sickness both were associated with more than a 2-fold increase in the odds for diarrhea] disease. In the final analysis, which family member supported the mother in providing care also was significantly related to diarrhea] outcome. Children cared for by members of a nuclear family had a I.7 times greater odds of experiencing diarrhea than children who were cared for by members of an extended family. After controlling for other vari- ables. improper refuse disposal remained a significant factor.
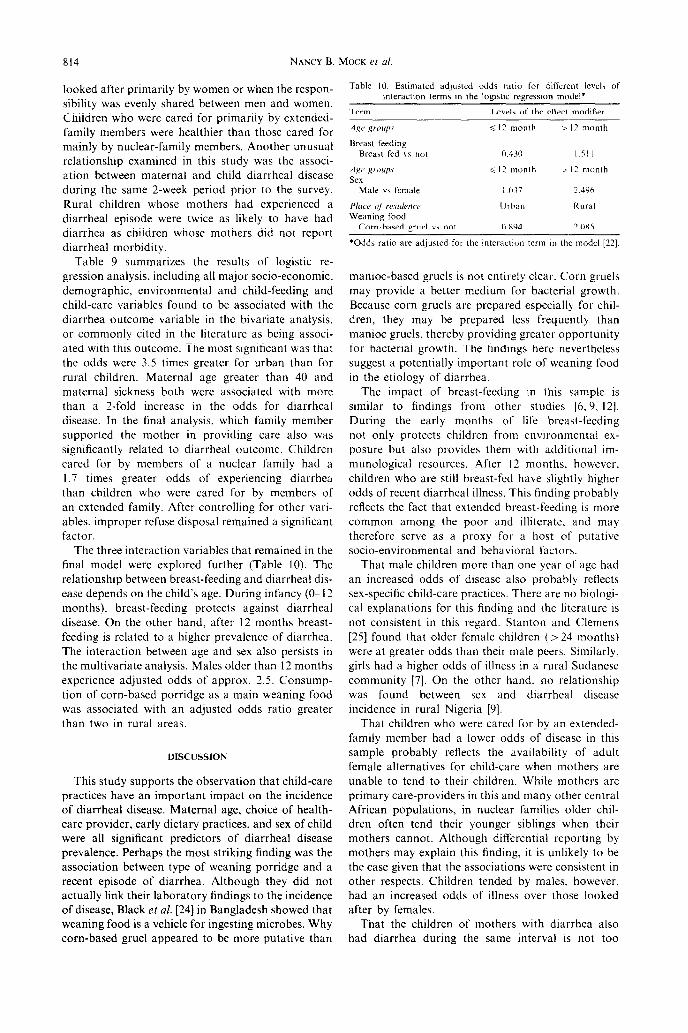
The three interaction variables that remained in the final model were explored further (Table 10). The relationship between breast-feeding and diarrhea1 dis- ease depends on the child’s age. During infancy (O-l 2 months), breast-feeding protects against diarrhea] disease. On the other hand, after I2 months breast- feeding is related to a higher prevalence of diarrhea. The interaction between age and sex also persists in the multivariate analysis. Males older than 12 months experience adjusted odds of approx. 2.5. Consump- tion of corn-based porridge as a main weaning food was associated with an adjusted odds ratio greater than two in rural areas.
DISCUSSION
This study supports the observation that child-care practices have an important impact on the incidence of diarrhea] disease. Maternal age, choice of health- care provider, early dietary practices, and sex of child were all significant predictors of diarrhea1 disease prevalence. Perhaps the most striking finding was the association between type of weaning porridge and a recent episode of diarrhea. Although they did not actually link their laboratory findings to the incidence of disease, Black et ul. [24] in Bangladesh showed that weaning food is a vehicle for ingesting microbes. Why corn-based gruel appeared to be more putative than
Table IO. Estimated adjusted odds ratio for different levela of
interactIon terms in the logistic regrewon model*
Term Levels of the effect modifier
Age groups <I? month > I? month
Breast feedmg
Male vs female
Place of residmcr
Weaning food
Corn-based gruel YS not 0.894 2.0115
‘Odds ratio are ad,justed for the interaction term jr1 the model [22].
maniac-based gruels is not entirely clear. Corn gruels may provide a better medium for bacterial growth. Because corn gruels are prepared especially for chil- dren, they may be prepared less frequently than maniac gruels, thereby providing greater opportunity for bacterial growth. The findings here nevertheless suggest a potentially important role of weaning food in the etiology of diarrhea.
The impact of breast-feeding in this sample is similar to findings from other studies [6.9, 121. During the early months of life breast-feeding not only protects children from environmental ex- posure but also provides them with additional im- munological resources. After I2 months. however, children who are still breast-fed have slightly higher odds of recent diarrhea] illness. This finding probably reflects the fact that extended breast-feeding is more common among the poor and illiterate. and may therefore serve as a proxy for a host of putative socio-environmental and behavioral factors.
That male children more than one year of age had an increased odds of disease also probably reflects sex-specific child-care practices. There are no biologi- cal explanations for this finding and the literature is not consistent in this regard. Stanton and Clemens [25] found that older female children (>24 months) were at greater odds than their male peers. Similarly. girls had a higher odds of illness in a rural Sudanese community [7]. On the other hand. no relationship was found between sex and diarrhea] disease incidence in rural Nigeria [9].
That children who were cared for by an extended- family member had a lower odds of disease in this sample probably reflects the availability of adult female alternatives for child-care when mothers are unable to tend to their children. While mothers are primary care-providers in this and many other central African populations, in nuclear families older chil- dren often tend their younger siblings when their mothers cannot. Although differential reporting by mothers may explain this finding, it is unlikely to be the case given that the associations were consistent in other respects. Children tended by males. however, had an increased odds of illness over those looked after by females.
That the children of mothers with diarrhea also had diarrhea during the same interval is not too
Factors associated with diarrhea 815
surprising. Maternal morbidity may be considered a general index of disease exposure in the family because the mother is both food handler and usual child-care provider. Moreover, care of the infant is undoubtedly compromised when the mother herself is ill.
Maternal age also is likely to be a proxy in this sample for child-care practices related to the trans- mission of diarrhea1 disease. Again, there is no consist- ent finding in the literature with respect to maternal age [9, 12, 131, which is a proxy for a host of factors including family size, educational level, modernity, and energy level for child care. In analyzing these data the first two factors were taken into account; it is therefore likely that older mothers hold more tena- ciously to certain putative traditional practices or are just physically not up to providing quality child-care.
Among the water and sanitation variables measured in this study, only one was significantly related to diarrhea1 disease. In the Congolese house- holds investigated, proper disposal of refuse was protective of child health. Refuse disposal also was found to be a significant determinant in Urban Bangladesh [16, 171. On the other hand, source of drinking-water and latrine availability were not re- lated to recent diarrhea. This is not surprising in the central African context where very few families have access to truly safe water. In this case, type of water source provides little information about water quality. In addition, water quantity is not measured. Access to proper latrines was rare in this sample, but was nevertheless not significantly related to the prevalence of diarrhea1 disease.
Three basic explanations of the relative lack of association between the measured environmental vari- ables and diarrhea1 disease: (1) the survey measured only indirectly the quantity and quality of water consumed by children, (2) little variability appears to exist in this sample with respect to water quality, quantity and latrine use, (3) the general level of environmental hygiene in this area may be so poor that marginal improvements in water and latrine access may produce negligible health impacts. The last interpretation is consistent with the fact that refuse disposal in this sample is associated with diarrhea because refuse disposal is usually correlated with overall environmental hygiene so it is a better differ- entiating factor. The finding that urban children had more than three times odds of diarrhea than their rural counterparts is also consistent with this explanation.
Financial and other resource limitations with which to combat disease call for prudence in selecting strategies to mitigate the effects of diarrhea in children. Studies such as this one that employ ad- vanced statistical analysis to consider simultaneously multiple contributing factors may help to provide important insights as to how resources should be allocated. At the same time, however, several caveats are in order.
Because the data presented here are cross-sectional in nature, it is not possible to assign a cause-and-effect
relationship between variables. Of particular concern, also, is the valid classification of diarrhea1 disease status. Maternal reporting of childhood diarrhea1 disease is known to be potentially biased [13]. In the analysis of cross-sectional data from Zaire, Tsui et al. found that the level of maternal education differen- tially affects maternal reporting of child morbidity including diarrhea. Their findings were based on a stratified analysis of the correlates of child morbidity by level of maternal education. A similar analysis performed on this data from Congo did not show the same effect on the relationship between diarrhea and the covariates of interest in the form and magnitude across the education-specific models. In addition, unlike the Zaire data, a higher prevalence of diarrhea was reported by mothers having no formal education than those who had had some education (21.9% vs 16.8%).
Regardless of the shortcomings of the data, how- ever, several observations can be made that have important implications for intervention. Environmen- tal indices, were not highly predictive of diarrhea1 disease occurrence. This finding contrasts with the commonly held assumption that control of diarrhea1 diseases in poor communities is dependent on the introduction of clean water and safe disposal of human excreta. While drinking-water and sanitation projects should remain long-term goals, the data in this study support Chen’s contention [26] that the introduction of potable water and sanitation technol- ogies are not the only necessary condition for reducing diarrhea1 diseases prevalence in poor societies.
Rather, these data suggest that maternal practices related to hygiene, breast-feeding, sanitary food prep- aration, appropriate weaning practices, and health care are potentially all important determinants of diarrhea1 disease incidence. These factors may hold enormous promise for the low-cost, culturally acceptable, effective prevention of diarrhea1 disease. Indeed, one recent study from Bangladesh suggests that appropriate behavioral interventions can have a moderate impact on diarrhea1 disease incidence.
1.
2.
3.
4.
5.
REFERENCES
Synder J. D. and Merson M. H. The magnitude of the global problem of acute diarrhea1 disease: a review of active surveillance data. Bull. WHO 60, 605613, 1982. Mata L. J. The Children of Santa Maria Caupaque: A Prospective Field Study of Health and Growth. MIT Press, Cambridge, MA, 1978. Rohde J. E. and Northruu R. E. Taking science where the diarrhea is. In Acute ‘Diarrhea in Ckldhood. CIBA Foundation Symposium 42, p. 339. Elsevier/Excerpta Medica, Amsterdam, 1976. Rohde J. E. Preparing for the next round: convalescent care after acute infection. Am. J. clin. Nurr. 31, 2258-2268, 1978. Fox J. P., Hail C. E., Cooney M. K., Lute R. E. and Kronmal R. A. The Seattle virus watch. II. Objectives, study population and its observation, data processing and summary of illnesses. Am. J. Epidemiol. 96, 270-285, 1972.
816 NANCY B. MOCK et nl.
6.
I.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
Esrey S. and Habicht .I. P. Epidemiologic evidence for health benefits from improved water and sanitation in developme. countries. Eaidemiol. Rev. 8, 117-128, 1986. El Samam F. Z., Willett W. C. and Ware J. H. Predictors of simple diarrhea in children under 5 years-A study of a Sudanese rural community. Sot. Sri. Med. 29, IO65%1070, 1989. Pickering H. Social and environmental factors associ- ated with diarrhea and growth in young children: child health in urban Africa. Ser. Scl. Med. 25 121 127. 1985. Hulty S. R. A., Blum D., Kirkwood B. R.. Emeh R. and Feachem R. G. The epidemiology of acute diarrhea in rural community in Imo State. Nigeria. Trans. R. Sot. Med. Hyg. 81, 865-870, 1987. - Tavlor S. M.. Frank J.. White N. F. and Mvers J. Modeling the incidence of childhood diarrhea. .S&. Sci. Med. 23, 995~-1002, 1986. Henry F. J. Environmental sanitation infection and nutritional status of infants in rural St. Lucia, West Indies. Trans. R. Sot. Trap. Med. Hyg. 75, 507-513, 1981. Freij L. and Wall S. Quantity and variation in morbid- ity: THAID-analysis of the occurrence of gastroenteritis among Ethiopian children. Inr. J. Epidemic/. 8,3 13 -325, 1979. Tsui A. O., DeClerque J. and Mangani N. Maternal and sociodemographic correlates of child morbidity in Bas Zaire: the effects of maternal reporting. Sot. Sci. Med. 26, 701-713. 1988. Bertrand W. E. and Walmus B. F. Maternal knowledge, attitudes and practices as predictors of diarrhea1 disease in young children. Inr. J. Epidemiol. 12,205--210, 1983. King J. and Bratt D. Soci-economic. dietary and cultural factors associated with diarrhea1 disease in Trinidad and Tobago. J. Trap. Ped. 34, 104-107, 1988. Alam N.. Wojtyniak B., Henry F. J. and Bahaman M. M. Mothers personal and domestic hygiene and diarrhea incidence in young children in rural Bangladesh. Int. J. Epidemiol. 18, 242-247. 1989. Baltazar J. C. and Solon F. S. Disposal of feces of children under two years old and diarrhea incidence:
18.
19.
20.
21.
22.
23.
24
25
26
a case-control study. Inr. J. Epidemiol. 18, S16-S19, 1989. Clemens J. D. and Stanton B. F. An educational intervention for altering water-sanitation behaviors to reduce childhood diarrhea in urban Bangladesh. I. Application of the case-control method for the develop- ment of an intervention. Am. J. Epidemlol. 125, 284.~291. 1987. Stanton B. F. and Clemens J. D. An educational intervention for altering water-sanitation behaviors to reduce childhood diarrhea in urban Bangladesh. II. A randomized trail to assess the impact of the intervention on hygienic behaviors and rates of diarrhea. Am. J. Epidemiol. 125, 292-30 I, 1987. Huntington D. E., Tchicayat Cr., Sellers T. A. and Franklin R. R. Findings from the health and nutrition survey in four regions of the Peoples Republic of the Congo. Cen. Afr. J. Med. 32, 1888195, 1986. Dixon W. J., Brown M. B.. Engelman L., Frane J. W., Hill M. A., Jennrich R. 1. and Toporek J. D. (Eds) BMDP Statistical Sofrwarr. pp. 217 243. University of California Press, Los Angeles, 1985. Kleinbaum D. G., Kupper L. L. and Morgenstern H. (Eds) Epidemiologic research. Principles und Quanfitar- iw Methods. Lifetime Learning Publications, Belmont, CA, 1982. Gomez F.. Galvan R. R., Frenk S.. Munoz J. C.. Chavez R. and Vazquez J. Mortality in second and third degree malnutrition. J. Trap. Ped. 2, 77~-83. 1956. Black R. E.. Brown K. H., Becker S., Abdul Alim A. R. M. and Merson M. H. Contamination of weaning foods and transmission of enterotoxigenic Escherichia coli diarrhea in children in rural Bangladesh. Trans. R. Sot. trap. Med. Hyg. 76, 2599264. 1982. Stanton B. F. and Clemens J. D. Socioeconomic vari- ables and rates of diarrhea1 disease in Urban Bangladesh. Trans. R. Sot. trap. Med. Hyg. 81, 278-282, 1987. Chen L. C. Interactions of diarrhea and malnutrition: mechanisms and interventions. In Diarrhea and Malnutrition (Edited by Chen L. and Scrimshaw N.). pp. 3319. Plenum Press, New York, 1983.