Social relations: network, support and relational strain
13
Social relations: network, support and relational strain Pernille Due *, Bjørn Holstein, Rikke Lund, Jens Modvig, Kirsten Avlund Department of Social Medicine and Psychosocial Health, Institute of Public Health, University of Copenhagen, Blegdamsvej 3, 2200 Copenhagen, Denmark Abstract We introduce a conceptual framework with social relations as the main concept and the structure and the function of social relations as subconcepts. The structure of social relations covers aspects of formal relations and social network. The function of social relations covers social support, social anchorage and relational strain. We use this conceptual framework to describe social relations in the Danish population, with questionnaire data from the Danish Longitudinal Health Behaviour Study including a random sample of each of the age groups 25-, 50-, 60- and 70-year olds, N = 2,011. The postal questionnaires were answered by a random sample in each of the age groups. The results show marked age and gender dierences in both the structure and the function of social relations. The social network, measured as weekly contacts, weakens with age and so does instrumental support. Emotional support is unrelated to this decline in contact frequency and appears to be at the same level for younger and older individuals. Relational strain, measured as conflicts, declines with age for all kinds of social relations. The weakening of the social network with age does not seem to aect the level of emotional support and in turn seems to be partly compensated for by a simultaneous decline in relational strain. # 1999 Elsevier Science Ltd. All rights reserved. Keywords: Social relations; Social support; Relational strain; Social networks 1. Introduction Research on social relations has attracted much attention in the area of public health and social medi- cine. There is now documentation that people with strong social relations have a lower morbidity and mortality (Berkman and Syme, 1979; Orth-Gome´r and Johnson, 1987; Hanson, 1988; House et al., 1988; O ¨ stergren, 1991; Olsen, 1993; Kawachi et al., 1996). Further, they have a better possibility of recovery or survival after illness (Ruberman et al., 1984; Waxler- Morrisson et al., 1991; Glass and Maddox, 1992; Vogt et al., 1992). Several intervention studies show that it may increase patients’ recovery or survival to strengthen their social relations (Prince and Frasure- Smith, 1984; Spiegel et al., 1989; Nielsen, 1993). Despite the enormous interest in this area of research the conceptualisation still lacks a strong con- sensus. The main concepts which are used are social support and social network. However, the literature includes numerous related concepts, e.g. social re- lations, social integration, social participation and social anchorage. House and Kahn (in Cohen and Syme, 1985) intro- duced a conceptualisation, in which ‘‘the domain of social support’’ included three concepts. The first con- cept is social relationships. It included measures of the existence, number and frequency of social relations. Social network is seen as the structural element or the description of interactions within these social relations, including elements such as density, dispersion, dur- ation, homogeneity and reciprocity. According to House and Kahn social support is the functional aspect of the social relationships, and is further divided into four categories: informational, instrumental, emotional and appraisal support. This conceptualisation is clear Social Science & Medicine 48 (1999) 661–673 0277-9536/99/$ - see front matter # 1999 Elsevier Science Ltd. All rights reserved. PII: S0277-9536(98)00381-5 PERGAMON * Corresponding author. Tel.: +45-35-32-7962; fax: +45- 35-35-1181; e-mail: [email protected].
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Social relations: network, support and relational strain

Social relations: network, support and relational strain
Pernille Due *, Bjùrn Holstein, Rikke Lund, Jens Modvig, Kirsten Avlund
Department of Social Medicine and Psychosocial Health, Institute of Public Health, University of Copenhagen, Blegdamsvej 3, 2200
Copenhagen, Denmark
Abstract
We introduce a conceptual framework with social relations as the main concept and the structure and thefunction of social relations as subconcepts. The structure of social relations covers aspects of formal relations and
social network. The function of social relations covers social support, social anchorage and relational strain. We usethis conceptual framework to describe social relations in the Danish population, with questionnaire data from theDanish Longitudinal Health Behaviour Study including a random sample of each of the age groups 25-, 50-, 60-
and 70-year olds, N= 2,011. The postal questionnaires were answered by a random sample in each of the agegroups. The results show marked age and gender di�erences in both the structure and the function of socialrelations. The social network, measured as weekly contacts, weakens with age and so does instrumental support.
Emotional support is unrelated to this decline in contact frequency and appears to be at the same level for youngerand older individuals. Relational strain, measured as con¯icts, declines with age for all kinds of social relations. Theweakening of the social network with age does not seem to a�ect the level of emotional support and in turn seems
to be partly compensated for by a simultaneous decline in relational strain. # 1999 Elsevier Science Ltd. All rightsreserved.
Keywords: Social relations; Social support; Relational strain; Social networks
1. Introduction
Research on social relations has attracted much
attention in the area of public health and social medi-
cine. There is now documentation that people with
strong social relations have a lower morbidity and
mortality (Berkman and Syme, 1979; Orth-Gome r and
Johnson, 1987; Hanson, 1988; House et al., 1988;
OÈ stergren, 1991; Olsen, 1993; Kawachi et al., 1996).
Further, they have a better possibility of recovery or
survival after illness (Ruberman et al., 1984; Waxler-
Morrisson et al., 1991; Glass and Maddox, 1992; Vogt
et al., 1992). Several intervention studies show that it
may increase patients' recovery or survival to
strengthen their social relations (Prince and Frasure-
Smith, 1984; Spiegel et al., 1989; Nielsen, 1993).
Despite the enormous interest in this area of
research the conceptualisation still lacks a strong con-
sensus. The main concepts which are used are social
support and social network. However, the literature
includes numerous related concepts, e.g. social re-
lations, social integration, social participation and
social anchorage.
House and Kahn (in Cohen and Syme, 1985) intro-
duced a conceptualisation, in which ``the domain of
social support'' included three concepts. The ®rst con-
cept is social relationships. It included measures of the
existence, number and frequency of social relations.
Social network is seen as the structural element or the
description of interactions within these social relations,
including elements such as density, dispersion, dur-
ation, homogeneity and reciprocity. According to
House and Kahn social support is the functional aspect
of the social relationships, and is further divided into
four categories: informational, instrumental, emotional
and appraisal support. This conceptualisation is clear
Social Science & Medicine 48 (1999) 661±673
0277-9536/99/$ - see front matter # 1999 Elsevier Science Ltd. All rights reserved.
PII: S0277-9536(98 )00381-5
PERGAMON
* Corresponding author. Tel.: +45-35-32-7962; fax: +45-
35-35-1181; e-mail: [email protected].
and consistent in most respects, though it may cause
confusion that social support is seen both as a generalconcept and as the concept concerning the functionalaspects.
O'Reilly (1988) introduced the use of social networkas the main concept, de®ned as: ``An analytic concept,used to describe the structure of linkages between indi-
viduals or groups of individuals. Such networks have avariety of functions of which the provision of socialsupport is but one. Social support is provided through
the behaviours or actions of members of a networkand communicated through the network's structure''.In this de®nition the concept `social network' has two
dimensions, i.e. the structure and the function. Thetype of individuals in the social network and the fre-
quency of contacts between these individuals areexamples of factors which are included in the structureof the social network. The function of the social net-
work is equivalent to the social support concept andthus covers the qualitative and behavioural aspects ofthe social network.
O'Reilly made an important contribution when hestated the importance of a clear conceptual de®nitionand recommended the use of social network as the
main concept. If social network is de®ned as ``thestructure of linkages between individuals or groups of
individuals'' the concept of social network will then
have two characteristics: (1) the overall concept whichcovers both structure and function of the relations and(2) the structural component of social network, i.e. one
of two key concepts, social support being the other.One important reason to clarify and separate the
concepts in this area of research is that theories and
empirical ®ndings indicate that di�erent mechanismsare responsible for the in¯uence of social relations onhealth.
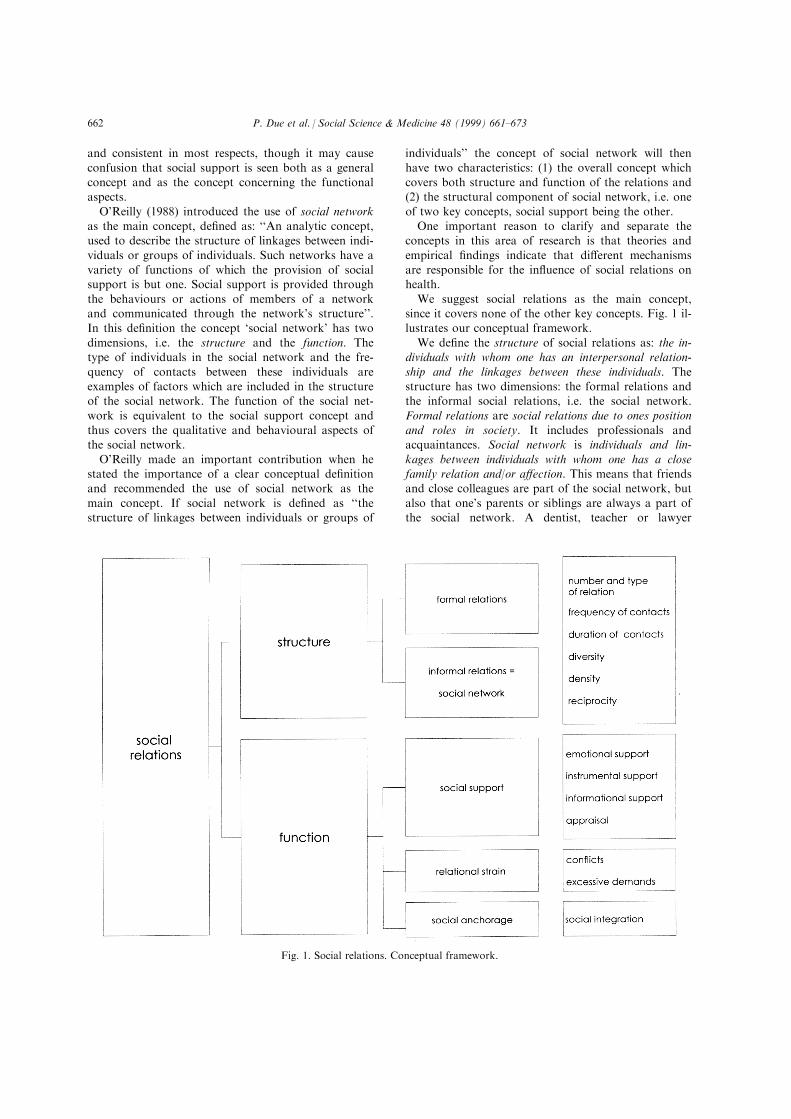
We suggest social relations as the main concept,since it covers none of the other key concepts. Fig. 1 il-lustrates our conceptual framework.
We de®ne the structure of social relations as: the in-dividuals with whom one has an interpersonal relation-
ship and the linkages between these individuals. Thestructure has two dimensions: the formal relations andthe informal social relations, i.e. the social network.
Formal relations are social relations due to ones positionand roles in society. It includes professionals andacquaintances. Social network is individuals and lin-
kages between individuals with whom one has a closefamily relation and/or a�ection. This means that friendsand close colleagues are part of the social network, but
also that one's parents or siblings are always a part ofthe social network. A dentist, teacher or lawyer
Fig. 1. Social relations. Conceptual framework.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673662

belongs to the formal relations, along with acquain-
tances like neighbours and the parents of one's best
friend. We consider terms like reciprocity, density, dur-
ation and social participation to be aspects of each of
the structural concepts.
The distinction between formal relations and social
network is important, as it is an interesting empirical
question as to what extent formal relations can replace
social network.
We de®ne the function of social relations as the inter-
personal interactions within the structure of the social
relations. The function covers the qualitative and beha-
vioural aspects of the social relations. The functional
dimension of social relations includes social support,
relational strain and social anchorage. Cohen and
Syme (1985) de®ne social support as the resources pro-
vided by other persons. We ®nd this de®nition useful.
Social support can be de®ned as having a negative
aspect, as used by Marmot et al. (1991) in the
Whitehall II study. This implies the following rede®ni-
tion of the social support concept: social support is the
level of resources provided by other persons.
Given this de®nition, social strain becomes another
important dimension of the function of social relations.
Most incidents of violence and sexual harassment take
place among people who know each other well, mainly
within families. Among older people it is found that
social relations may create severe strain at some point,
for example by obstructing an e�ort of the social- or
health service system towards an elderly patient (Due,
1990). Also, the role as a caregiver within the social
network can be so extensive and full of strain that the
health of the caregiver is a�ected (Parker, 1990; Twigg
et al., 1990; Due, 1993).
We argue that relational strain is di�erent from lack
of social support. We de®ne relational strain as the
extent to which functions of social relationships cause
emotional or instrumental strain. Relational strain is the
negative dimension of the functional aspect of social re-
lations. We have pointed out two important aspects of
relational strain: con¯icts and excessive demands. The
concept of relational strain may well have the same
essential aspects as job strain i.e. demand and control
(Karasek and Theorell, 1990). This will be an empirical
question for future studies.
Antonucci and Akiyama (1987) suggest that both
receiving and giving social support might enhance
health and wellbeing.
The term `social anchorage' is interesting, but the
importance of this concept in relation to health has
not yet been widely tested. According to Hanson:
``social anchorage describes to what degree the individual
belongs to and is anchored within formal and informal
groups, and in a more qualitative sense his feeling of
membership in these groups'' (Hanson, 1988). We
believe his qualitative dimension to be an important el-ement of the function of social relations.
The operationalisation of social network and socialsupport in this article considers everyday network andeveryday support and does not include an e�ort to
measure social network and support during episodes ofcrisis. However, since we study a randomly selectedpopulation, people who have currently experienced a
crisis will be represented in the study to the extent ofthe prevalence of crises in the population.Several studies have shown major age and gender
di�erences in limited areas of social relations.However, it has not been possible to ®nd a morethorough description of the structure and the functionof social relations among individuals in di�erent age
groups and among men and women. Such informationis important for future studies of associations between,for example, social relations and health.
The aim of this article is to present a conceptualframework for social relations and social support andto provide descriptive population-based survey data
for the structure and function of social relations formen and women in key life transition periods.
2. Methods
The data used are obtained from the baseline surveyin 1990 of the Danish Longitudinal Health BehaviourStudy (DLHBS). The study is designed to: (1) analyse
changes in health behaviour over time, (2) study socialbackground, living conditions and social relations aspredictors of health behaviour and (3) study interactions
and modi®cations between these background variablesand the in¯uences of health behaviours on health. The®rst follow-up was made in 1994 and the second follow-up will be in the year 2000. The focus of the present
work is thus one of the main determinants of the totalstudy: social relations in various life transition periods.The population is a random sample of the Danish
population selected from the national CentralPopulation Register. The study comprises ®ve cohorts:individuals born in 1975, 1965, 1940, 1930 and 1920.
These ®ve age groups were chosen speci®cally to rep-resent stages in the lifespan, where major changes insocial roles and social relations are expected to occurover a ten year period. The 15-year-olds develop from
adolescents to adults, a period of immense changes anda period known to ground later health behaviours. Thecohort of 25-year-olds was chosen to see the e�ect of
having children on health behaviours. The three oldestcohorts were chosen to represent other life transitions asmenopause/midlife, children leaving home, pension, the
loss of spouse and declining functional ability. The 15-year-olds who were born in 1975 are not included in thispaper, as their network data are not easy to compare
P. Due et al. / Social Science & Medicine 48 (1999) 661±673 663
with the data of the other cohorts. Table 1 shows the
study population and the response rate.
The study population were asked to enroll in a longi-
tudinal study. Data collection was made by postal ques-
tionnaires. The non-respondents were reminded twice.
The last reminder included a new questionnaire. Since
not all questions were relevant to all age groups, the
questionnaire di�ered among the ®ve cohorts. However,
we have made an attempt to include as many identical
questions in the questionnaires as possible, in order to
obtain the best comparability between the age groups.
The questionnaires were tested in a pilot survey which
included 100 randomly selected individuals in each age
group. This test was performed to check face validity,
i.e. to ensure willingness and ability to answer as well as
to check the appropriateness of the distribution. The
questionnaires were revised according to the experience
gained from this pilot testing. This paper includes data
on the 2,011 25±70-year-old individuals. A sample of
non-respondents from the four cohorts was brie¯y inter-
viewed by telephone. For economic reasons this was
only done among individuals who lived in the Eastern
area of the country. We asked the non-respondents
about their reasons for not answering the questionnaire.
We also asked nine questions from the relevant ques-
tionnaire in order to compare respondents and non-
respondents on central variables. Some results from this
study of non-respondents are shown in Table 2.
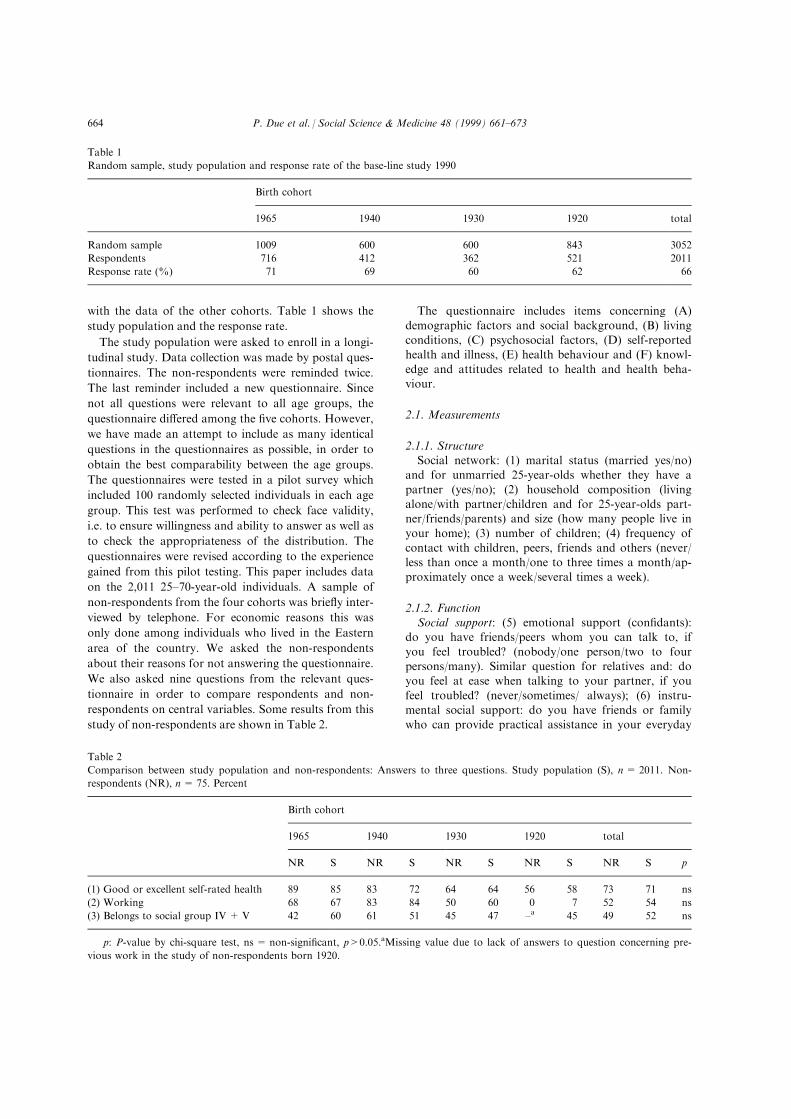
The questionnaire includes items concerning (A)
demographic factors and social background, (B) livingconditions, (C) psychosocial factors, (D) self-reportedhealth and illness, (E) health behaviour and (F) knowl-
edge and attitudes related to health and health beha-viour.
2.1. Measurements
2.1.1. StructureSocial network: (1) marital status (married yes/no)
and for unmarried 25-year-olds whether they have a
partner (yes/no); (2) household composition (livingalone/with partner/children and for 25-year-olds part-ner/friends/parents) and size (how many people live in
your home); (3) number of children; (4) frequency ofcontact with children, peers, friends and others (never/less than once a month/one to three times a month/ap-proximately once a week/several times a week).
2.1.2. FunctionSocial support: (5) emotional support (con®dants):
do you have friends/peers whom you can talk to, if
you feel troubled? (nobody/one person/two to fourpersons/many). Similar question for relatives and: doyou feel at ease when talking to your partner, if you
feel troubled? (never/sometimes/ always); (6) instru-mental social support: do you have friends or familywho can provide practical assistance in your everyday
Table 1
Random sample, study population and response rate of the base-line study 1990
Birth cohort
1965 1940 1930 1920 total
Random sample 1009 600 600 843 3052
Respondents 716 412 362 521 2011
Response rate (%) 71 69 60 62 66
Table 2
Comparison between study population and non-respondents: Answers to three questions. Study population (S), n= 2011. Non-
respondents (NR), n= 75. Percent
Birth cohort
1965 1940 1930 1920 total
NR S NR S NR S NR S NR S p
(1) Good or excellent self-rated health 89 85 83 72 64 64 56 58 73 71 ns
(2) Working 68 67 83 84 50 60 0 7 52 54 ns
(3) Belongs to social group IV + V 42 60 61 51 45 47 ±a 45 49 52 ns
p: P-value by chi-square test, ns = non-signi®cant, p>0.05.aMissing value due to lack of answers to question concerning pre-
vious work in the study of non-respondents born 1920.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673664
life? Do you have friends or family to help you econ-
omically, if one month expenses become too great?
(nobody/friends/family/both friends and family). Social
strain: (7) con¯ict: do you experience con¯icts in your
everyday life with (separate items for) partner, family,
friends and colleagues (often/sometimes/no).
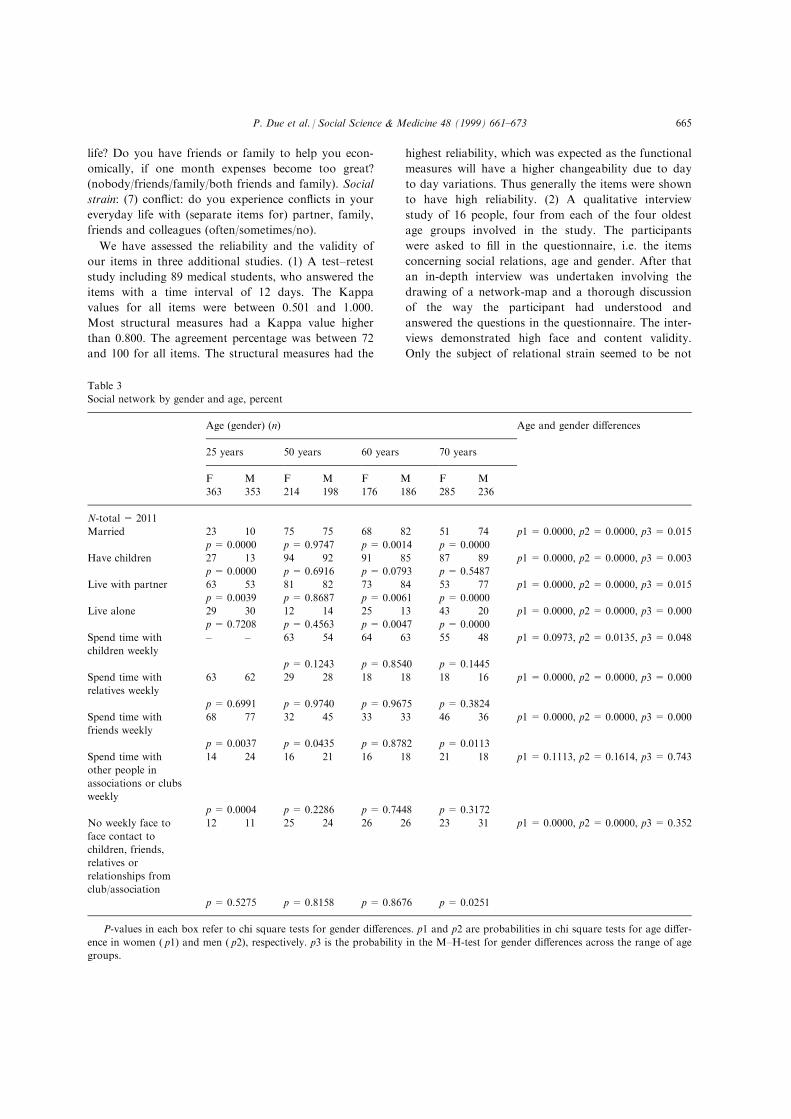
We have assessed the reliability and the validity of
our items in three additional studies. (1) A test±retest
study including 89 medical students, who answered the
items with a time interval of 12 days. The Kappa
values for all items were between 0.501 and 1.000.
Most structural measures had a Kappa value higher
than 0.800. The agreement percentage was between 72
and 100 for all items. The structural measures had the
highest reliability, which was expected as the functional
measures will have a higher changeability due to day
to day variations. Thus generally the items were shown
to have high reliability. (2) A qualitative interview
study of 16 people, four from each of the four oldest
age groups involved in the study. The participants
were asked to ®ll in the questionnaire, i.e. the items
concerning social relations, age and gender. After that
an in-depth interview was undertaken involving the
drawing of a network-map and a thorough discussion
of the way the participant had understood and
answered the questions in the questionnaire. The inter-
views demonstrated high face and content validity.
Only the subject of relational strain seemed to be not
Table 3
Social network by gender and age, percent
Age (gender) (n) Age and gender di�erences
25 years 50 years 60 years 70 years
F M F M F M F M
363 353 214 198 176 186 285 236
N-total = 2011
Married 23 10 75 75 68 82 51 74 p1 = 0.0000, p2 = 0.0000, p3 = 0.015
p= 0.0000 p = 0.9747 p= 0.0014 p= 0.0000
Have children 27 13 94 92 91 85 87 89 p1 = 0.0000, p2 = 0.0000, p3 = 0.003
p= 0.0000 p = 0.6916 p= 0.0793 p= 0.5487
Live with partner 63 53 81 82 73 84 53 77 p1 = 0.0000, p2 = 0.0000, p3 = 0.015
p= 0.0039 p = 0.8687 p= 0.0061 p= 0.0000
Live alone 29 30 12 14 25 13 43 20 p1 = 0.0000, p2 = 0.0000, p3 = 0.000
p= 0.7208 p = 0.4563 p= 0.0047 p= 0.0000
Spend time with
children weekly
± ± 63 54 64 63 55 48 p1 = 0.0973, p2 = 0.0135, p3 = 0.048
p = 0.1243 p= 0.8540 p= 0.1445
Spend time with
relatives weekly
63 62 29 28 18 18 18 16 p1 = 0.0000, p2 = 0.0000, p3 = 0.000
p= 0.6991 p = 0.9740 p= 0.9675 p= 0.3824
Spend time with
friends weekly
68 77 32 45 33 33 46 36 p1 = 0.0000, p2 = 0.0000, p3 = 0.000
p= 0.0037 p = 0.0435 p= 0.8782 p= 0.0113
Spend time with
other people in
associations or clubs
weekly
14 24 16 21 16 18 21 18 p1 = 0.1113, p2 = 0.1614, p3 = 0.743
p= 0.0004 p = 0.2286 p= 0.7448 p= 0.3172
No weekly face to
face contact to
children, friends,
relatives or
relationships from
club/association
12 11 25 24 26 26 23 31 p1 = 0.0000, p2 = 0.0000, p3 = 0.352
p= 0.5275 p = 0.8158 p= 0.8676 p= 0.0251
P-values in each box refer to chi square tests for gender di�erences. p1 and p2 are probabilities in chi square tests for age di�er-
ence in women ( p1) and men ( p2), respectively. p3 is the probability in the M±H-test for gender di�erences across the range of age
groups.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673 665

fully covered by the questionnaire. Feelings of dis-agreement or annoyance with relations were not
thought to be con¯icts, but were thought to be import-ant aspects of relational strain that were not coveredby the questionnaire. Another important aspect of
relational strain was the feeling of obligation towardother people. Finally, con¯icts were indicated lessoften in the questionnaire than the interviewer would
interpret from the interview. (3) A validity study wasmade among 42 after-AMI patients (age-range 35±75,10 women/22 men) (Mortensen et al., 1998). The
patients answered the questions on social relations andwere interviewed about their interpretation and assess-ment of the items. In general the items appeared to bevalid. However colleagues were shown as an important
network source for middle-aged men, mostly concern-ing the measure of weekly contacts. So for further usethis should be included as a separate item.
2.2. Statistics
The di�erences in social network by age and sex aretested for homogeneity by the chi square test and bythe Mantel±Haenszel test for the strati®ed analyses.
3. Results
Table 3 shows results on the social networkmeasures: household composition and contact fre-
quency. Table 4 shows results on emotional and instru-mental support measures and Table 5 shows relationalstrain measures for women and men in the four
cohorts.
3.1. Social network
3.1.1. Household composition and familyThe proportion of people living alone is greatest
among the 25-year-olds and lowest among the 50-year-
olds. Among the 70-year-olds more women than menlive alone ( p< 0.000) and among the 25-year-olds morewomen than men live with a partner ( p < 0.001). When
looking at 25-year-old parents we ®nd more womenthan men living with their children (98% versus 91%,p< 0.05). 7% of the 25-year-olds live with their friends,7% live with parents and more men than women
( p < 0.01). Approximately 90% of the three oldest agegroups have children. Among the 25-year-olds twice asmany women as men have children ( p< 0.000).
3.1.2. Contact frequencyWe ®nd no signi®cant age or gender di�erences when
looking at contact frequency with children. Contactwith other relatives are most frequent in the youngestage groups. We ®nd no gender di�erences in contact fre-
quency with relatives. Contact with friends is most fre-quent among the 25-year-olds, but at the age of 50
approximately half the men have weekly contact withtheir friends. This amount declines for the 60- and 70-year-old men to one third. Among women we ®nd a U-
shaped relationship with age. Among the 50- to 60-year-olds only one third of the women have weekly contactwith friends. Among 25-year-old women two out of
three and among 70-year-old women almost half haveweekly contact with friends. Also, network contactthrough involvement in organisations shows di�erent
patterns for men and women with age. A quarter of 25-year-old men have weekly contact through organis-ations, which is the highest frequency among men in theage groups we have studied. For women, we ®nd the
highest proportion among the 70-year-olds. Very fewDanes have no weekly contacts and less than 6% menand women in all age groups live alone and without
weekly contact to any of the measured relations.
3.2. Social support
3.2.1. Emotional supportMost people have at least one con®dant. Only very
few individuals do not ®nd a con®dant either in their
partner, family members or friends. We ®nd signi®-cantly more women who have a con®dant (odds ratio1.7 (95% CI: 2.2±1.2). More males than females reportcon®dant relationships with their partner and more
females than males report con®dant relationships withrelatives and friends.
3.2.2. Instrumental and economic supportMost young people have the possibility of ®nding
help for practical work in their everyday life. Only threeout of four 70-year-old woman think they have people
around who can give them instrumental support. Evenbigger age di�erences are found when we look at econ-omic support. Almost half of the 70-year-olds think
there is no possibility of having economic support.More men report lack of economic support, while asomewhat larger proportion of women feel a lack of
practical support.
3.3. Relational strain
3.3.1. Con¯icts
A relatively large proportion of the Danish popu-lation experience con¯ict in their everyday life, mostoften with their partner. We ®nd a strong age trend
toward fewer con¯icts with partner, family and friendswith increasing age.The age di�erences in social network, social support
and relational strain among men and women are shownbelow. We ®nd lower contact frequencies and increasinglack of instrumental support with age. Emotional
P. Due et al. / Social Science & Medicine 48 (1999) 661±673666
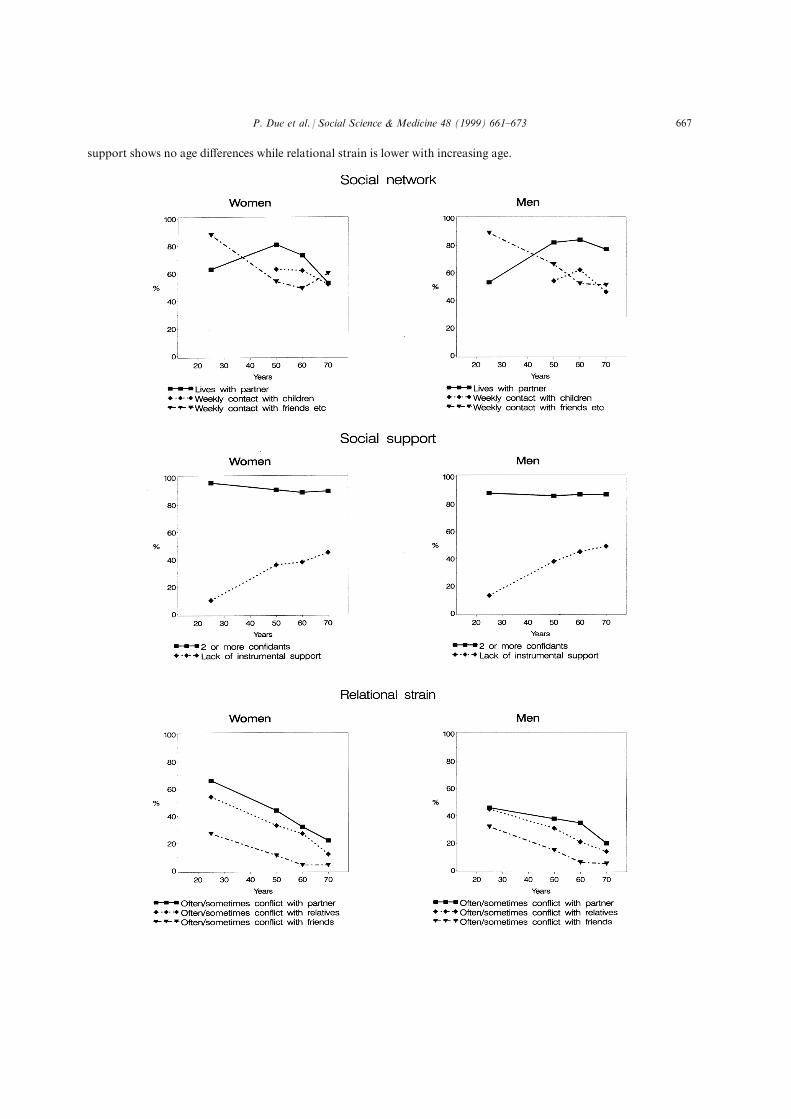
support shows no age di�erences while relational strain is lower with increasing age.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673 667

Table
4
Socialsupport
bygender
andage,
percent
Age(gender)(n)
Ageandgender
di�erences
25years
50years
60years
70years
FM
FM
FM
FM
363
353
214
198
176
186
285
236
Emotionalsupport
Alwayscon®dentrelationship
withpartner
a53
55
62
72
67
67
65
71
p1=
0.0148,p2=
0.0000,p3=
0.000
p=
0.7343
p=
0.0255
p=
0.8820
p=
0.2107
Atleast
onecon®dantamongrelatives
92
87
87
83
89
81
88
83
p1=
0.2963,p2=
0.4036,p3=
0.001
p=
0.0144
p=
ns
p=
ns
p=
0.0917
Atleast
onecon®dantamongfriends
96
87
87
82
89
81
89
83
p1=
0.0007,p2=
0.1667,p3=
0.000
p=
0.0000
p=
ns
p=
0.0459
p=
0.1038
Nocon®dentrelationship
atall
12
24
24
33
p1=
0.0883,p2=
0.6792,p3=
0.000
p=
0.1162
p=
0.8831
p=
0.1530
p=
0.8598
Lack
ofinstrumentalsupport
Nobodyto
provideinstrumentalsupport
75
16
15
22
20
25
20
p1=
0.0000,p2=
0.0000,p3=
0.111
p=
0.2877
p=
0.7951
p=
0.6502
p=
0.1788
Nobodyto
provideeconomic
support
10
13
36
38
38
45
45
49
p1=
0.0000,p2=
0.0000,p3=
0.070
p=
0.2905
p=
0.7441
p=
0.1339
p=
0.4087
aP-values
ineach
boxreferto
chisquare
testsforgender
di�erences.p1andp2are
probabilitiesin
chisquare
testsforage-di�erence
inwomen
(p1)andmen
(p2),respectively.
p3istheprobabilityin
theM
±H-testforgender
di�erencesacross
therangeofagegroups.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673668

The decline in con¯ict by age shows a di�erent pat-
tern to the decline in contact frequency. The greatestdecline in contact frequency is seen between the 25-year-olds and the 50-year-olds, while con¯ict shows a
continuous decline from 25 to 70.
4. Discussion
The results of this survey point to three importantconclusions concerning social relations in a general
population: (1) remarkable age di�erences in the struc-ture and function of social relations are found. (2)There are signi®cant gender di�erences in the structureand function of social relations. (3) Social relations
seem to be less supportive for the elderly part of thepopulation, but elderly individuals also experiencefewer con¯icts with their social relations than younger
individuals.
4.1. Age di�erences
Several other studies con®rm that there are majorage di�erences in the structure of social relations.Generally speaking, young people have more social
contacts than older (Plovsing et al., 1983; Hansen,1986; Jensen et al., 1987; Rasmussen et al., 1988; Platz,1989; Hansen and Platz, 1995; Kjùller et al., 1995).
Key persons in the social network are found to bevery di�erent according to the age group concerned.Olsen et al. (1991) studied the social network in a
population of male shipyard workers and reportedmajor di�erences in the structure of the social networkas well as its impact on health in di�erent age groups
(Olsen et al., 1991). The article concluded that it might
introduce serious age-bias to the results, if several
social network variables were combined into one
index. These results lead to the hypothesis that parents,
children, relatives and friends have varying importance
for males' social network, when studied in a life per-
spective. Our results con®rm the ®ndings of Olsen et
al. in a representative population of both genders.
Household composition re¯ects the actual life phase
of people and re¯ects the fact that life phases are stag-
gered for men and women. Women establish with a
partner and children earlier than men and they also
loose their partners earlier.
Life phases are related to certain age levels, but the
content of social relations in each life phase may also
change from one birth cohort to another. Some of the
cohort e�ects are obvious: birth rates change from one
cohort to the next, the proportion of childless families
changes, the length of the time for which children live
with their parents changes, mortality pattern changes
through time, etc. The age di�erences reported here
will probably change over time and the social relations
of the future elderly population will re¯ect both age
and cohort e�ects.
We ®nd the greatest age di�erences in our contact
frequency data. Contacts with peers are the key con-
tacts among the 25-year-olds, while 70-year-olds have
more contacts with children, friends and people they
know from formal associations. Parents are included
in the group of peers in this survey, so we expect them
to account for a signi®cant part of the peer contact
among 25-year-olds. We expect that this di�erence in
contact pattern is mainly due to changes which most
Table 5
Exposure to con¯icts in everyday life by sex and age, percent
Sometimes or
always exposed to
con¯icts with...
Age (gender) (n) Age and gender di�erences
25 years 50 years 60 years 70 years
F M F M F M F M
363 353 214 198 176 186 285 236
Partner 66 46 44 38 32 35 22 20 p1 = 0.0000, p2 = 0.0000, p3 = 0.0000
p= 0.0102 p= 0.2147 p= 0.5132 p= 0.5859
Family 54 45 33 31 27 21 12 14 p1 = 0.0000, p2 = 0.0000, p3 = 0.0000
p= 0.0177 p= 0.5159 p= 0.7463 p= 0.4916
Friends 27 32 11 15 4 6 4 5 p1 = 0.0000, p2 = 0.0000, p3 = 0.0000
p= 0.2192 p= 0.2637 p= 0.2637 p= 0.3551
p1 and p2 are probabilities in chi square test across age groups for women and for men, p3 is the probability in the M±H-test
across sex and age groups.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673 669

people experience over a lifetime and we consider thechanges to be mainly age e�ects.
4.2. Gender di�erences
Gender di�erences in social relations are anotherfactor which has been considered in recent years.
Many studies report major gender di�erences in thestructure as well as the function of social relations.Generally, women have larger and closer social net-
works than men. Moreover, some studies show thatwomen do not always have the same health bene®tsfrom their social network as men (Antonucci andAkiyama, 1987; Due, 1991; Shumaker and Hill, 1991;
Tuomi, 1994; Shye et al., 1995).The total amount of contacts is more or less the
same for women and men but the contact pro®le dif-
fers: gender di�erences in social network are most evi-dent among 50-year-old individuals. 50-year-old maleshave the same amount of contact with friends as with
their children, while more 50-year-old women havecontact with their children and fewer have contactwith their friends. One possible explanation is thedi�erences in gender-roles, another is their di�erent life
situations. The study by Olsen et al. (1991) indicatedthat colleagues were important for male shipyardworkers. Men might have a greater overlap between
friends and colleagues, which might explain why menhave more frequent contacts with friends. Women'slarger diversity in their networks makes it more di�-
cult to ®t contact with friends into an everyday sche-dule, if most of the friends are from outside theworkplace.
It is yet to be studied whether this pattern willchange over time and appear to be a cohort e�ect. Weconclude, however, that it is important to measureboth contacts with children and contacts with friends
in order to cover the di�erent social network charac-teristics of men and women.Qualitative studies will be useful in studies of gender
di�erences in the role of colleagues as network mem-bers. A validity study was performed in a populationof AMI patients which con®rmed that colleagues are
important keypersons for men in mid-life, even if theyare not close enough to be considered friends.The patterns of formal relations are very di�erent
from the social network patterns. Formal relations
exist due to a mutual interest and make it possible tohave social contacts without any interpersonal commit-ment. A study among elderly Danish women who lived
alone showed that for some, it is very important to®nd social contacts which are characterised by uncom-mitment. These women have the lifelong experience
that social relationships lead to social demands. Inother words, they need to have some contacts that``give more than they take'' (Due, 1993). This fact can
be one possible explanation why social contactsthrough clubs and organisational work are most fre-
quent among the oldest women.
4.3. Social support and relational strain
Our results show that the decline in social contactwith age does not a�ect the ability of the network to
create con®dent relations. It is an interesting issuewhether the changes in structure of social relationsover time and especially over the life course are
re¯ected in the function of social relations.A decline is found in economic and practical sup-
port. This may indicate that fewer contacts give fewerresources with regard to help. However, it could also
partly be due to di�erences in measurement: whenthere is no need for help, the answers to our questionmay describe support availability. For individuals who
need help, the answers may describe actual support, asdiscussed below. Finally, it may re¯ect resourcesamong individuals in the network at di�erent periods
of time. Younger people have younger networks withpossibly more available resources.The most interesting result is that we ®nd signi®-
cantly less con¯icts in the social network of elderly in-dividuals compared to younger. The con¯icts do notseem to be fewer because of fewer contacts. Thedecline is the same for all kinds of contact resources,
and it follows a di�erent and quite consistent pattern.Consequently we believe that two di�erent expla-nations are relevant. First, elderly people have had the
chance over time to develop a more carefully selectedsocial network, i.e. they may have divorced the partnerwith whom there was con¯ict, and they may have cut
contacts with friends and relatives who were toodemanding. Second, all of us may become more prag-matic as we grow older, and as Tornstam (1996)describes in his Theory of Gerotranscendence we may
be more reluctant to engage in con¯icts, because every-day life questions seem to be of less importance.
5. The study and the measurement
It is important to consider how the study design andmeasurements may a�ect the reported results. Thestrength of this study is, ®rst of all, that it is based on
a real random and consequently representative sampleof the Danish population in the chosen age groups.The response rate was acceptable, except for the two
oldest cohorts in which the 38±40% non-response mayhave a�ected representativeness.We made a thorough study of non-responders.
However, there might be an over representation of iso-lated and handicapped people among the non-respon-ders that could compromise our results especially on
P. Due et al. / Social Science & Medicine 48 (1999) 661±673670

con®dent relations. Other comparable Danish studies
have had an overrepresentation of divorced and
unmarried among the non-respondents (Kjùller et al.,
1995). Hansen (1986) found 10% women and 14%
men, age 30±69, who did not have a friend to discuss
personal problems with. Both of these studies have
results that resemble our ®ndings.
Our measurements of the structure of the social net-
work correspond with known standards which are
usually thought to have acceptable validity.
Measurements of function are much more varied in
the literature (Orth-Gome r and Unde n, 1987; O'Reilly,
1988). Our studies of reliability and validity revealed
satisfactory results for both structural and functional
measures.
Research on social support and health has often
indicated the importance of having con®dent relations
(OÈ stergren, 1991). We ®nd a large prevalence of con®-
dent relations in all strata, which leads us to conclude
that our measure is not e�cient to stratify the popu-
lation. Nevertheless, it is important to include this
variable as part of the dimension of emotional support.
Our measure is, however, used in a representative
sample of the Danish population and thereby as a gen-
eral measure of the perception of having con®dants in
everyday life situations. Con®dent relations might be
of smaller prevalence and of greater relevance when
studying other groups, e.g. seriously ill patients. This
could also be the case among our non-respondents,
leading to an overestimation of the prevalence of con®-
dants. Measuring social support among seriously ill
people would illustrate, how the social network func-
tions in crisis, while the present study concentrates on
everyday support. As O'Reilly, we expect these two
aspects of the function of social relations to be very
di�erent (O'Reilly, 1988).
Instrumental social support, in this survey measured
as the perceived possibility of getting practical and
economic support, shows marked age di�erences. A
major consideration is whether the need for support in-
¯uences the experience of what support is available.
There is a possibility that individuals in need of sup-
port will consider the actual support to a greater
extent, than individuals with no need of support. This
indicates that questions about perceived social support
measure two di�erent elements. For those in need of
help we measure the actual received support and for
those with no actual need of support we measure the
perceived availability of support.
Among elderly people a greater proportion of indi-
viduals need practical support. Several Danish studies
have shown that those who have the greatest decline in
functional ability get the most practical support
(Holstein et al., 1991, 1997) or in other words: those
who need help, get help.
This leads us to suggest that the reported age di�er-ences in social support may partly be due to di�erences
in need for support for the di�erent age groups, lead-ing to the measurement of perceived availability ofsupport in the younger cohorts and actual, experienced
support in the older cohorts. Winemiller points thatmost studies measure people's perception of supportavailable, rather than the support that they are likely
to utilise (Winemiller et al., 1993). We would arguethat the same item could measure availability or actualsupport depending on the person's actual need of sup-
port.If this is the case, then we need ®rstly to distinguish
whether perceived availability of social support is thekey factor which in¯uences health over time or
whether the actual available support is the importantfactor. Secondly we need to create an instrument todistinguish these.
There are however indications that perceived socialsupport is the most important concept in relation tohealth. Wethington and Kessler (1986) found perceived
support to be more important in predicting adjustmentto stressful life events than the received support. Blazer(1982) and many other studies have shown perceived
support as a predictor of mortality.Like Orth-Gome r and Unde n (1987) we state that
all four types of social relations i.e. children, relatives,friends and contacts from involvement in formal as-
sociations should be included in measures of the struc-ture of social network in population based surveys.Our results show that an age- and gender-related bias
will be introduced if one of these groups is excluded.This is especially true if these dimensions are combinedinto an index of social network. This might give
entirely di�erent pictures of the social network struc-ture depending on which factor is left out.One key issue in psychosocial health research is to
illuminate which factors within the structure and func-
tion of social relationships are the most important indetermining health, morbidity and mortality. Amongother things the e�ect of the various components of
social network remains to be demonstrated in a longi-tudinal study. Future analyses of our material intendto help answer this question.
Therefore studies including social relations as adeterminant should still ensure a broad and multi-facetted measure of social relations.
Acknowledgements
The study was ®nanced by The Danish CancerSociety (No. 93-504) and the Danish Research Council
(No. 9600251). We thank Birgit Pallesen for help withthe manuscript and Allen Sawitz for help with dataprocessing. We also thank the reviewers and the editor
P. Due et al. / Social Science & Medicine 48 (1999) 661±673 671
for constructive comments to an earlier draft of thispaper.
References
Antonucci, T.C., Akiyama, H., 1987. An examination of sex
di�erences in social support among older men and women.
Sex Roles 17, 737±749.
Berkman, L.F., Syme, S.L., 1979. Social networks, host resist-
ance, and mortality: a nine-year follow-up study of
Alameda County residents. American Journal of
Epidemiology 109, 186±204.
Blazer, D.G., 1982. Social support and mortality in an elderly
community population. American Journal of Epidemiology
115, 684±694.
Cohen, S., Syme, S.L. (Eds.), 1985. Social Support and
Health. Academic Press, New York.
Due, P., 1990. Det sociale netvñrk paÊ prùve: stùtte eller
belastning? (Challenging the social network: support or
strain?). Gerontologi og samfund 6, 12±14.
Due, P., 1991. Enlige kvinder: Et proletariat med et stñrkt
socialt netvñrk (Single women: a proletariat with a strong
social network). In: Helset, A. (Ed.), Gamle kvinner i
Norden: deres liv i tekst og tall (Old Women in the Nordic
Countries: Their Lives in Text and Figures). Norsk
Gerontologisk Institut, Oslo, pp. 259±271.
Due, P., 1993. Livslùb og helbred hos gamle, enlige, fattige
kvinder i Danmark (Life course and health among elderly,
poor, Danish women living alone). In: Helset, A. (Ed.), I
lyst og nùd: livssituasjonen for gamle kvinner med minste-
pensjon i Danmark, Norge og Sverige. Norsk
Gerontologisk Institut, Oslo, pp. 21±120.
Glass, T.A., Maddox, G.L., 1992. The quality and quantity of
social support: stroke recovery as psycho-social transition.
Social Science and Medicine 34, 1249±1261.
Hansen, E.B., Platz, M., 1995. 80±100-aÊ riges levekaÊ r (The
Living Conditions of 80±100-years old People). The Danish
National Institute of Social Research, Copenhagen.
Hansen, E.J., 1986. Danskernes levekaÊ r: 1986 sammenholdt
med 1976 (The Living Conditions of the Danes:
Comparisons between 1986 and 1976). Hans Reitzels
Forlag, Copenhagen.
Hanson, B.S., 1988. Social network, social support and health
in elderly men. Doctoral dissertation. Lund University,
MalmoÈ .
Holstein, B.E., Avlund, K., Heikkinen, R.-L., 1997. Home
help and informal social support for elderly people in three
Nordic localities. Facts, Research and Intervention in
Geriatrics, 41±54.
Holstein, B.E., Due, P., Almind, G., Holst, E., 1991. The
home-help service in Denmark. In: A. Jamieson (Ed.),
Home Care for Older People in Europe. Oxford University
Press, Oxford, pp. 38±62.
House, J.S., Landis, K.R., Umberson, D., 1988. Social re-
lationships and health. Science 241, 540±545.
Jensen, M.K., Andersen, D., Fridberg, T., Nielsen, K.A.,
1987. Socialt netvñrk og socialpolitik. En undersùgelse i 2
lokalomraÊ der (Social Network and Social Policy. A Study
in Two Local Communities). The Danish National Institute
of Social Research, Copenhagen.
Karasek, R., Theorell, T., 1990. Healthy Work. Basic Books,
New York.
Kawachi, I., Colditz, G.A., Ascherio, A., Rimm, E.B.,
Giovannucci, E., Stampfer, M.J., Willett, W.C., 1996. A
prospective study on social networks in relation to total
mortality and cardiovascular disease in men in the USA.
Journal of Epidemiology and Community Health 50, 245±
251.
Kjùller, M., Rasmussen, N.K., Keiding, L., Petersen, H.C.,
Nielsen, G.A., 1995. Sundhed og sygelighed i Danmark
1994 (Health and Disease in Denmark 1994). Danish
Institute of Clinical Epidemiology, Copenhagen.
Marmot, M.G., Smith, G.D., Stans®els, S., Patel, C., North,
F., Head, J., White, I., Brunner, E., Feeney, A., 1991.
Health inequalities among British civil servants: the
Whitehall II study. Lancet 337, 1387±1393.
Mortensen, O.S., Hansen, L.G., Fromholt, L., Hansen, H.H.,
1998. Health related quality of life after primary coronary
angioplasty or thrombolytic therapy for acute myocardial
infarction. Paper presented at the Fifth International
Congress of Behavioral Medicine. Copenhagen, Denmark.
Nielsen, H., 1993. Akut myokadieinfarkt hos ñldre (Acute
myocardial infarction among elderly people). Doctoral dis-
sertation. Design Management, Copenhagen.
Olsen, O., 1993. Impact of social network on cardiovascular
mortality in middle aged Danish men. Journal of
Epidemiology and Community Health 47, 176±180.
Olsen, O., Iversen, L., Sabroe, S., 1991. Age and the operatio-
nalization of social support. Social Science and Medicine
32, 767±771.
O'Reilly, P., 1988. Methodological issues in social support
and social network research. Social Science and Medicine
26, 863±873.
Orth-Gome r, K., Johnson, J.V., 1987. Social network inter-
action and mortality. A six year follow-up study of a ran-
dom sample of the Swedish population. Journal of Chronic
Diseases 40, 949±957.
Orth-Gome r, K., Unde n, A.-L., 1987. The measurement of
social support in population surveys. Social Science and
Medicine 24, 83±94.
OÈ stergren, P.-O., 1991. Psychosocial resources and health.
With special reference to social network, social support and
cardiovascular disease. Doctoral dissertation. Lund
University, MalmoÈ .
Parker, G., 1990. With Due Care and Attention: a Review of
Research on Informal Care, 2nd ed. Family Policy Studies
Centre, London.
Platz, M., 1989. Gamle i eget hjem. Bind 1: LevekaÊ r (Old
Non-institutionalized People, vol. 1: Living conditions).
The Danish National Institute of Social Research,
Copenhagen.
Plovsing, J., Pruzan, V., Majlund, J.E., 1983. Sociale netvñrk
og holdninger til sociale ydelser (Social Network and
Attitudes toward Social Bene®ts). The Danish National
Institute of Social Research, Copenhagen.
Prince, R., Frasure-Smith, N., 1984. Comforting the after-cor-
onary patients. Canadian Family Physician 30, 1095±1099.
Rasmussen, N.K., Groth, M.V., Bredkjaer, S.R., Madsen,
M., Kamper-Jùrgensen, F., 1988. Sundhed og sygelighed i
Danmark 1987 (Health and Disease in Denmark 1987).
Danish Institute of Clinical Epidemiology, Copenhagen.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673672

Ruberman, W., Weinblatt, E., Goldberg, J.D., Chaudhary,
B.S., 1984. Psychosocial in¯uences on mortality after myo-
cardial infarction. New England Journal of Medicine 311,
552±559.
Shumaker, S.A., Hill, D.R., 1991. Gender di�erences in social
support and physical health. Health Psychology 10, 102±
111.
Shye, D., Mullooly, J.P., Freeborn, D.K., Pope, C.R., 1995.
Gender di�erences in the relationship between social net-
work support and mortality: a longitudinal study of an
elderly cohort. Social Science and Medicine 41, 935±947.
Spiegel, D., Bloom, J.R., Kraemer, H.C., Gottheil, E., 1989.
E�ect of psychosocial treatment on survival of patients
with metastatic breast cancer. Lancet II, 888±891.
Tornstam, L., 1996. Gerotranscendence: a theory about
maturing into old age. Journal of Ageing and Identity 1,
37±50.
Tuomi, K., 1994. Characteristics of work and life predicting
coronary heart disease. Finnish research project on aging
workers. Social Science and Medicine 38, 1509±1519.
Twigg, J., Atkin, K., Perring, C., 1990. Carers and Services: a
Review of Research. HMSO, London.
Vogt, T.M., Mullooly, J.P., Ernst, D., Pope, C.R., Hollis,
J.F., 1992. Social networks as predictors of ischemic heart
disease, cancer, stroke and hypertension: incidence, survival
and mortality. Journal of Clinical Epidemiology 45, 659±
666.
Waxler-Morrisson, N., Hislop, T.G., Mears, B., Kan, L.,
1991. E�ects of social relationships on survival for women
with breast cancer: a prospective study. Social Science and
Medicine 33, 177±183.
Wethington, E., Kessler, R.C., 1986. Perceived support,
received support and adjustment to stressful life events.
Journal of Health and Social Behavior 27, 78±89.
Winemiller, D., Mitchell, E., Sutcli�, J., Cline, D., 1993.
Measurement strategies in social support: a descriptive
review of the literature. Journal of Clinical Psychology 49,
638±648.
P. Due et al. / Social Science & Medicine 48 (1999) 661±673 673