
Skin lightening, Whitening, Brightening
47
Skin lightening,Whitening, Brightening 1 By: Dr. Nooshin Tasharrofi Pharm D, PhD Assistant Professor, LUMS Email: [email protected]
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Skin lightening, Whitening, Brightening

Skin lightening, Whitening, Brightening
1
By: Dr. Nooshin Tasharrofi
Pharm D, PhD
Assistant Professor, LUMS
Email: [email protected]
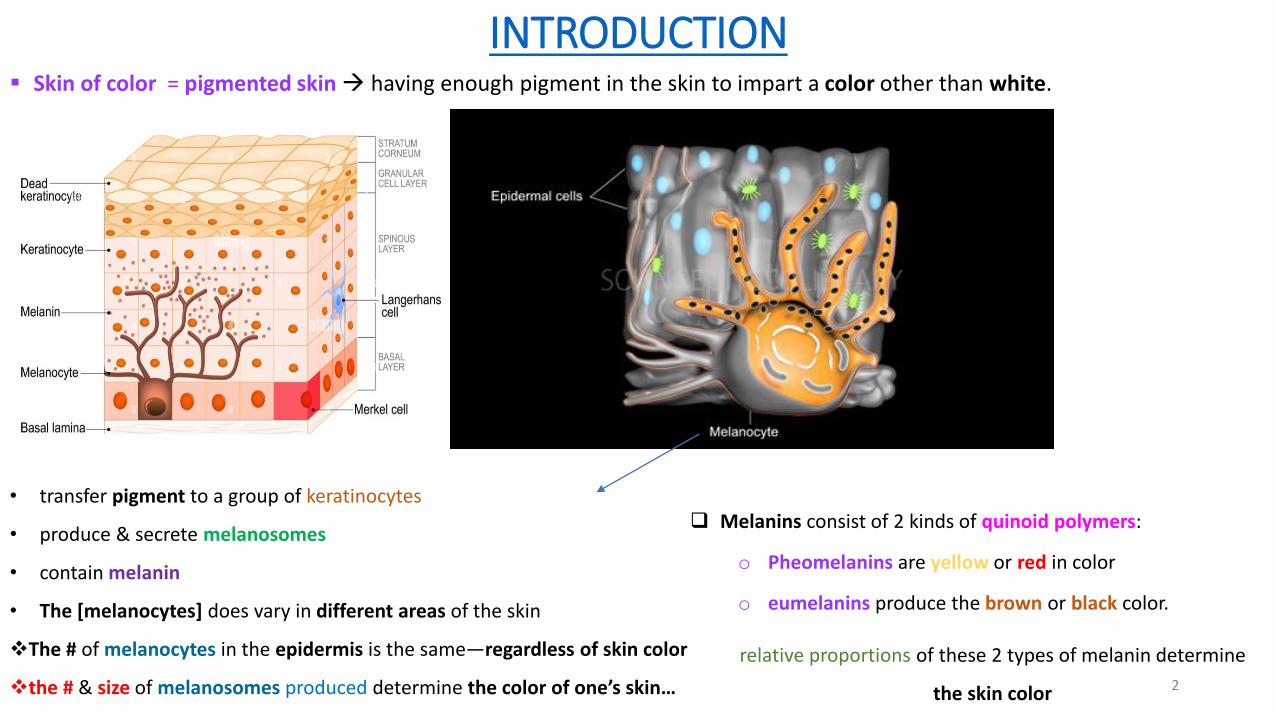
INTRODUCTION▪ Skin of color = pigmented skin → having enough pigment in the skin to impart a color other than white.
2
• transfer pigment to a group of keratinocytes
• produce & secrete melanosomes
• contain melanin
• The [melanocytes] does vary in different areas of the skin
❖The # of melanocytes in the epidermis is the same—regardless of skin color
❖the # & size of melanosomes produced determine the color of one’s skin…
❑ Melanins consist of 2 kinds of quinoid polymers:
o Pheomelanins are yellow or red in color
o eumelanins produce the brown or black color.
relative proportions of these 2 types of melanin determine
the skin color
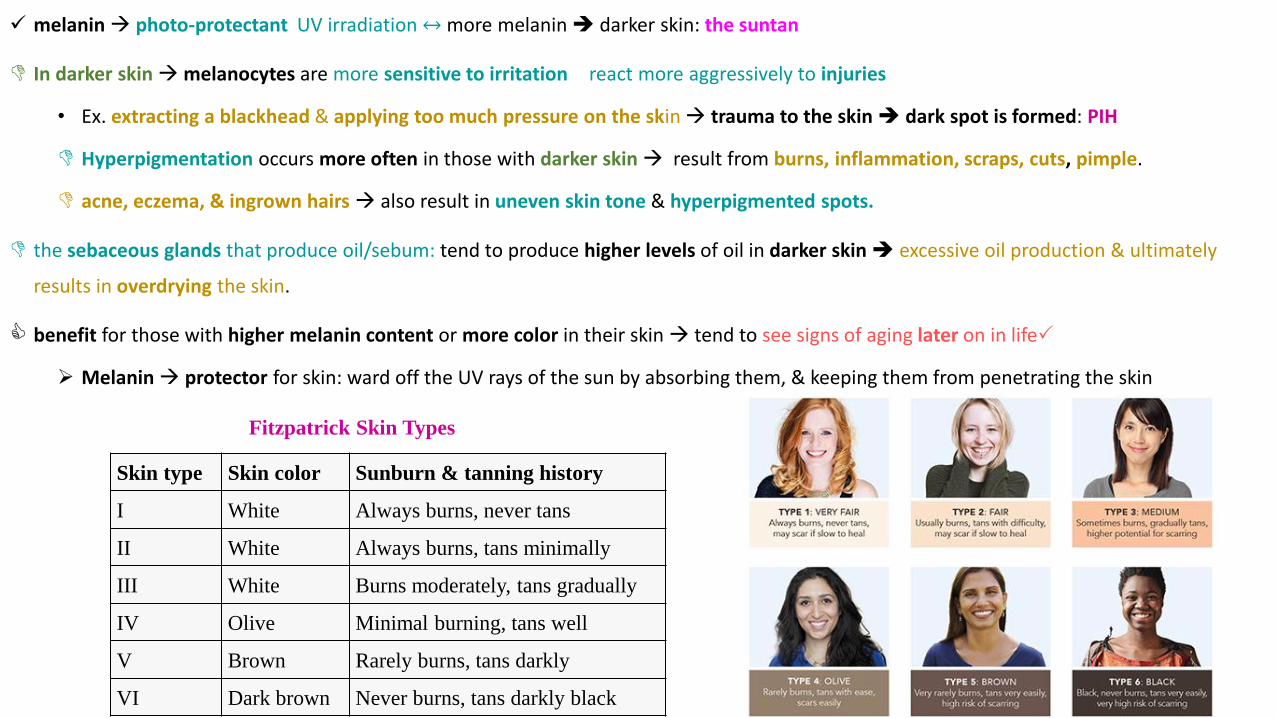
✓ melanin→ photo-protectant UV irradiation ↔more melanin ➔ darker skin: the suntan
In darker skin →melanocytes are more sensitive to irritation react more aggressively to injuries
• Ex. extracting a blackhead & applying too much pressure on the skin→ trauma to the skin ➔ dark spot is formed: PIH
Hyperpigmentation occurs more often in those with darker skin → result from burns, inflammation, scraps, cuts, pimple.
acne, eczema, & ingrown hairs → also result in uneven skin tone & hyperpigmented spots.
the sebaceous glands that produce oil/sebum: tend to produce higher levels of oil in darker skin ➔ excessive oil production & ultimately
results in overdrying the skin.
benefit for those with higher melanin content or more color in their skin → tend to see signs of aging later on in life
➢ Melanin→ protector for skin: ward off the UV rays of the sun by absorbing them, & keeping them from penetrating the skin
3
Skin type Skin color Sunburn & tanning history
I White Always burns, never tans
II White Always burns, tans minimally
III White Burns moderately, tans gradually
IV Olive Minimal burning, tans well
V Brown Rarely burns, tans darkly
VI Dark brown Never burns, tans darkly black
Fitzpatrick Skin Types

❑ copper & oxygen act as catalysts …
• Tyrosinase is a copper-containing enzyme:
o Ex. Kojic acid → chelating the copper
• Melanogenesis is a complex process of oxidative stages melanin formation depends on → the generation of free radical species
✓ ➔ topical antioxidants are useful in hyperpigmentation
✓ Many antioxidants have skin-brightening properties: scavenging free radicals that can be a precursor to hyperpigmentation4
❑ Melanosomes transferred into the keratinocytes → then continue on
their journey up through the epidermis where they eventually are bio-
converted to corneocytes & appear on the surface of the skin.
➢ accelerate the epidermal turnover: desquamation→ the melanin will
go away
➔ chemical exfoliators: lactic acid retinol derivative
retinol-like glucosamine derivatives
➢↑ the expression of the Pr of desquamation (a group of serine
proteases called kallikrein)
→ KLK5 (SC tryptic enzyme) or KLK7 (SC chymotryptic enzyme)
ocertain marine exo-polysaccharides ↑ enzyme expressions
5
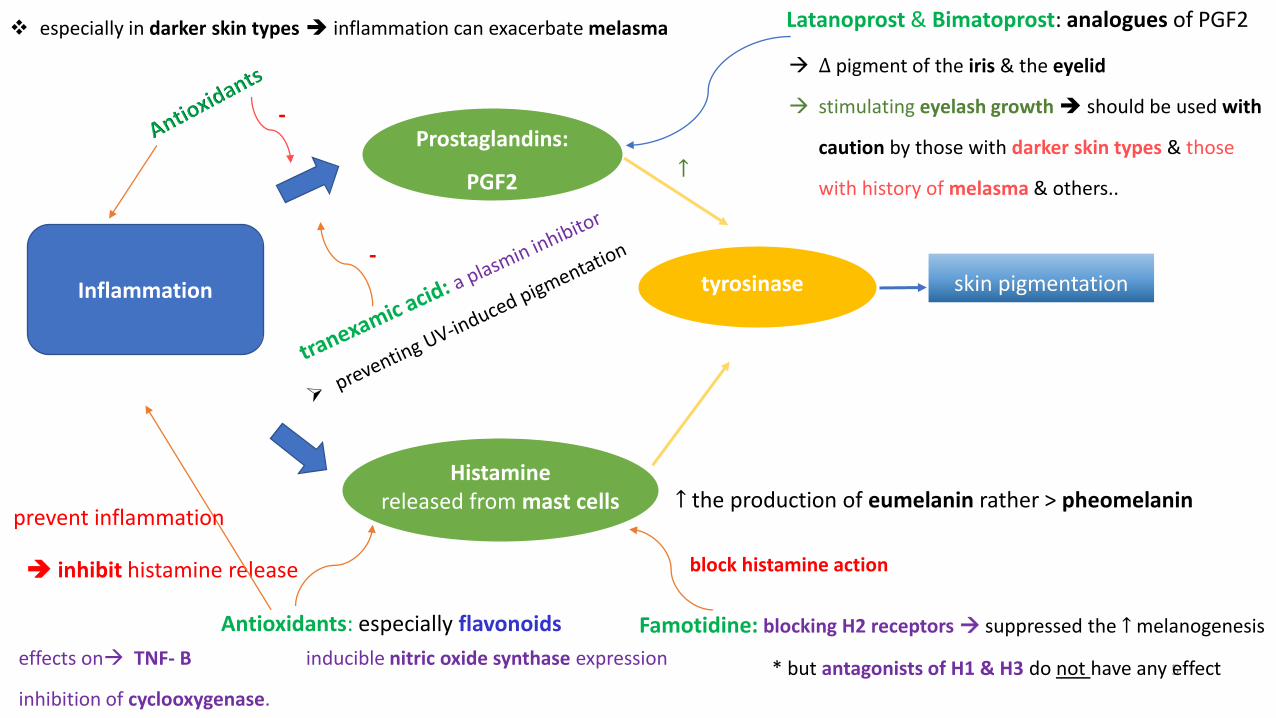
Inflammation
Prostaglandins:
PGF2
❖ especially in darker skin types ➔ inflammation can exacerbate melasma
skin pigmentation
-
tyrosinase
↑
-
→ ∆ pigment of the iris & the eyelid
→ stimulating eyelash growth ➔ should be used with
caution by those with darker skin types & those
with history of melasma & others..
Latanoprost & Bimatoprost: analogues of PGF2
Histaminereleased from mast cells ↑ the production of eumelanin rather > pheomelanin
effects on→ TNF- B inducible nitric oxide synthase expression
inhibition of cyclooxygenase.
Famotidine: blocking H2 receptors → suppressed the ↑ melanogenesis
* but antagonists of H1 & H3 do not have any effect
block histamine action
Antioxidants: especially flavonoids
➔ inhibit histamine release
prevent inflammation
❑ Sun Damage (photo damage or age spots or Photomelanosis):
• Sun→ the #1 trigger for hyperpigmentation causing sun spots from years of excessive exposure to the UV rays
• → commonly on the face, neck, & back the pigmentation may be patchy or a diffused darkening of the exposed skin
• UV stimulates keratinocytes & can break their DNA➔ keratinocytes look for protection→ “ask” the melanocyte to produce melanin
to be used as a “cap” for the next time keratinocytes are exposed to UV
➢ under UV: activated the cytokines→ alpha MSH (melanocyte stimulating hormone) & endothelin are released →Pro-opio melano
cortin (POMC) released by the keratinocytes
➢➔ The down-regulation of POMC will stop the communication between keratinocyte & melanocyte
o Undecylenoyl phenylalanine → act as alpha-MSH antagonist
o Ascophyllum nodosum extract is an algae extract → block endothelin adhesion to the membrane of the melanocyte.
❑ In the nerves: nerves → stimulate the melanocytes ↑ the dendricity: via a peptide: Substance P → activate substance P
receptors→ ↑ the # of dendrites in the melanocytes➔ neuro-whitening…
o extract of Pancratum maritimum (white sea lily or sea daffodil): down-regulate POMC & ↓ the stimulation from
keratinocyte ↓ the # of Substance P receptors➔ prevents the stimulation of melanocytes from the nerves 6

❑ Melasma/Chloasma (pregnancy mask):
• A condition that is typically induced from hormones internally can also be induced from menopause even certain medications.
• MSH is a natural hormone in our bodies & is linked to pigmentation & hyperpigmentation development in Melasma/Chloasma
❑ Post-Inflammatory Hyperpigmentation (PIH)
• This condition can be seen in the skin after inflammation.
• Most commonly found in acneic skin conditions → includes “acne prone, reactive, oily skin type,” → experiences persistent breakouts & also post–aggressive
skin care treatments or medical procedures.
❑ Peri-Orbital Hypermelanosis (Undereye dark circles):
• very common disorder among the Asian population (especially the Indian population).
• Undereye circles (dark pigments around the peri-orbital area) →may be hereditary due to stress eye strain allergies ….
➢ Smoking drinking a lot of alcohol coffee soda or caffeine beverages will usually make dark circles worse.
➢ Diet & A lack of sleep also play a role → not having a healthy diet can affect it as well.
▪ Treatments of Peri-Orbital Hypermelanosis:
o Using a good eye cream twice a day:→ help prevent moisture loss hydrate the area assist the delicate skin in absorbing the moisture &
active ingredients while stimulating the blood supply.
o wearing sunglasses→ help prevent further pigmentation when exposed to the sun. 7
❑ Formation of melanin is influenced by →
• genetics certain medications diet environmental factors…
• TRIGGERS FOR HYPERPIGMENTATION
• 1. Sun (UVA/UVB rays, environmental damages, free radicals)
• 2. Hormones (internal unbalance, pregnancy, menopause)
• 3. Inflammation (blemishes, acne, injury, laser treatment, heat, medical & chemical procedures)
• 4. Oral Medications (diuretics, birth control pills, antibiotics, anti-depressants, ...)
• 5. Alcohol (aftershave, colognes, perfumes)
8
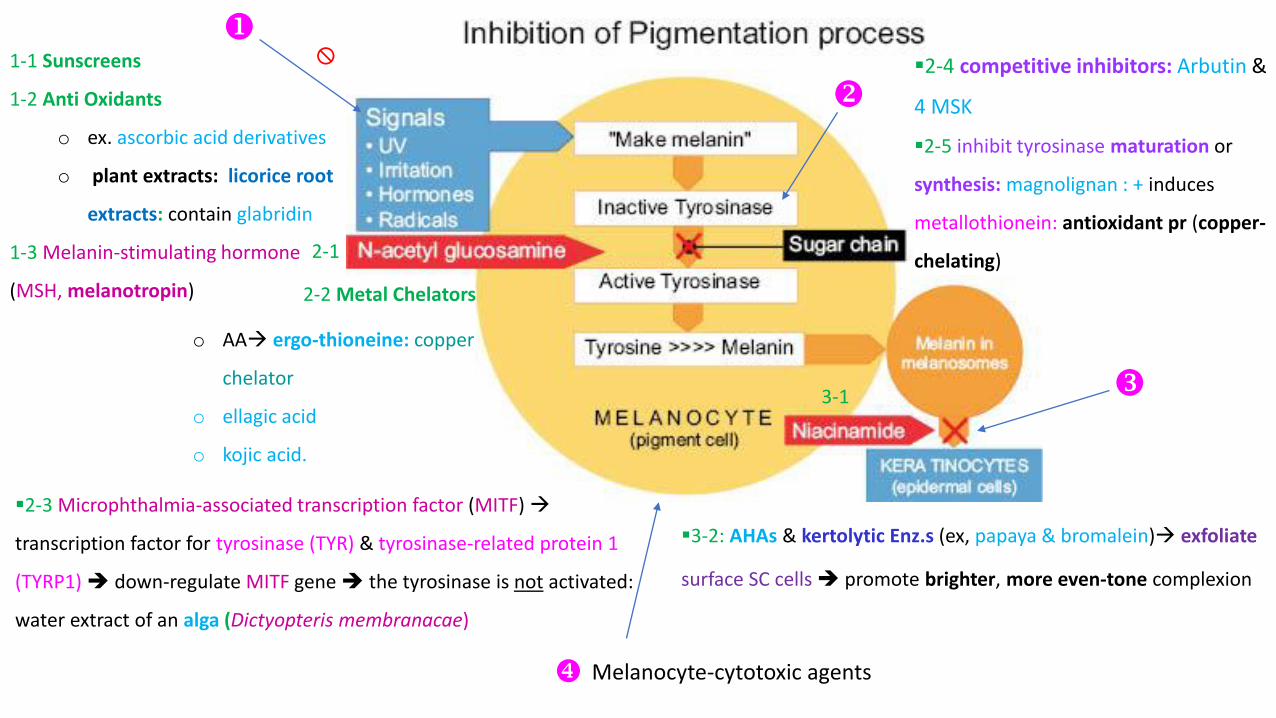
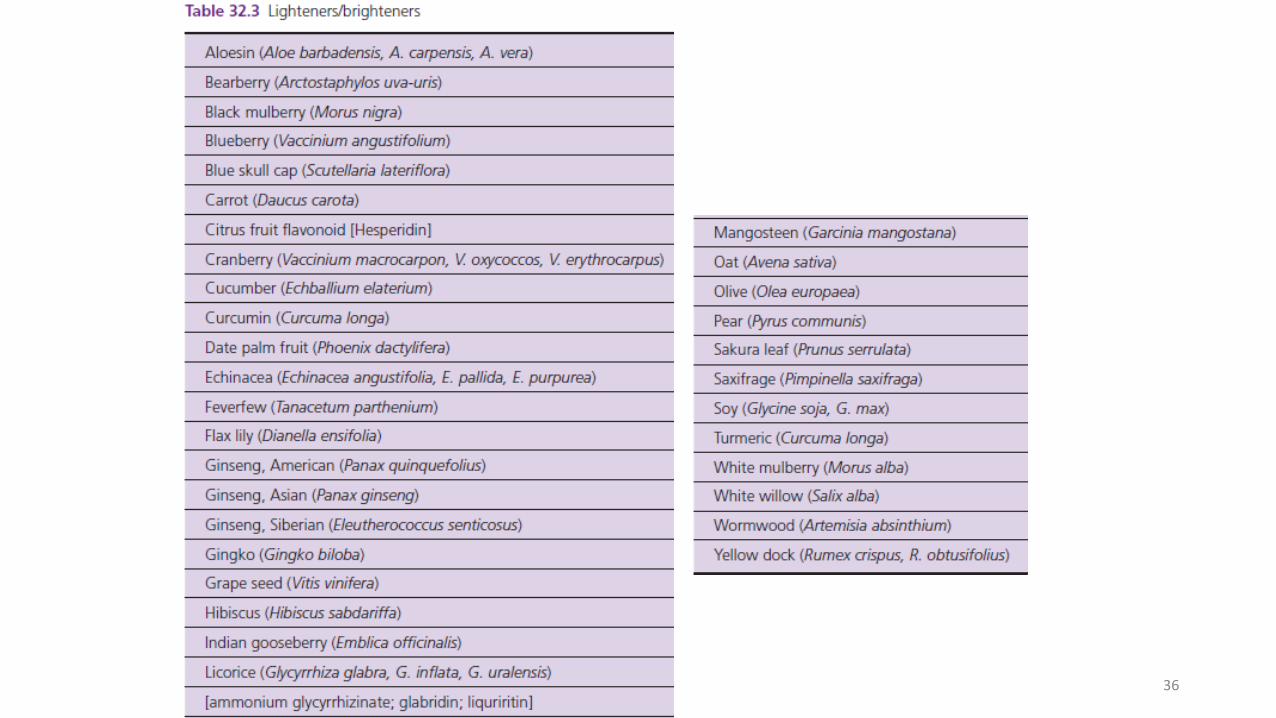
1-1 Sunscreens
1-2 Anti Oxidants
o ex. ascorbic acid derivatives
o plant extracts: licorice root
extracts: contain glabridin
1-3 Melanin-stimulating hormone
(MSH, melanotropin)
2-1
3-1
2-2 Metal Chelators
▪3-2: AHAs & kertolytic Enz.s (ex, papaya & bromalein)→ exfoliate
surface SC cells ➔ promote brighter, more even-tone complexion
o AA→ ergo-thioneine: copper
chelator
o ellagic acid
o kojic acid.
▪2-4 competitive inhibitors: Arbutin &
4 MSK
▪2-5 inhibit tyrosinase maturation or
synthesis: magnolignan : + induces
metallothionein: antioxidant pr (copper-
chelating)
▪2-3 Microphthalmia-associated transcription factor (MITF) →
transcription factor for tyrosinase (TYR) & tyrosinase-related protein 1
(TYRP1) ➔ down-regulate MITF gene ➔ the tyrosinase is not activated:
water extract of an alga (Dictyopteris membranacae)
Melanocyte-cytotoxic agents

10
❑ SunScreens/ UV absorber
• Even though sun protection does not directly interfere with the pigment formation process → it helps to block UV radiation
limit post-sun exposure erythema→ are key triggers for melanocytes to produce melanin
• is crucial to see results & maintain results from skin-lightening actives ➔
▪ In the keratinocyte →limit the communication between the keratinocytes & the melanocytes...
➢ applying a physical/chemical broad-spectrum photo-stable UVA/UVB sunscreen regularly when exposed to UV radiation
➢ protective clothing: woven UV absorbent fibers into protective clothing wide-brimmed hats long-sleeved shirts
pants the use of UV-protectant sunglasses
❖ take cover in the shade when the sun’s rays are strongest between 10 a.m. & 4 p.m➔ Seek cover indoors or at least in a shaded spot
11
❑ Skin Lightening & Whitening/Skin Bleaching: A common drug claim for OTC (1.5-2) &/RX (>2%) products containing Hydroquinone
➢ the only skin-lightening active ingredient that is recognized by the FDA.
➢ skin-bleaching active ingredient (according to FDA) → an agent designed to bleach or otherwise lighten limited areas of
hyperpigmented skin through the suppression of melanin pigment formation within skin cells → HQ
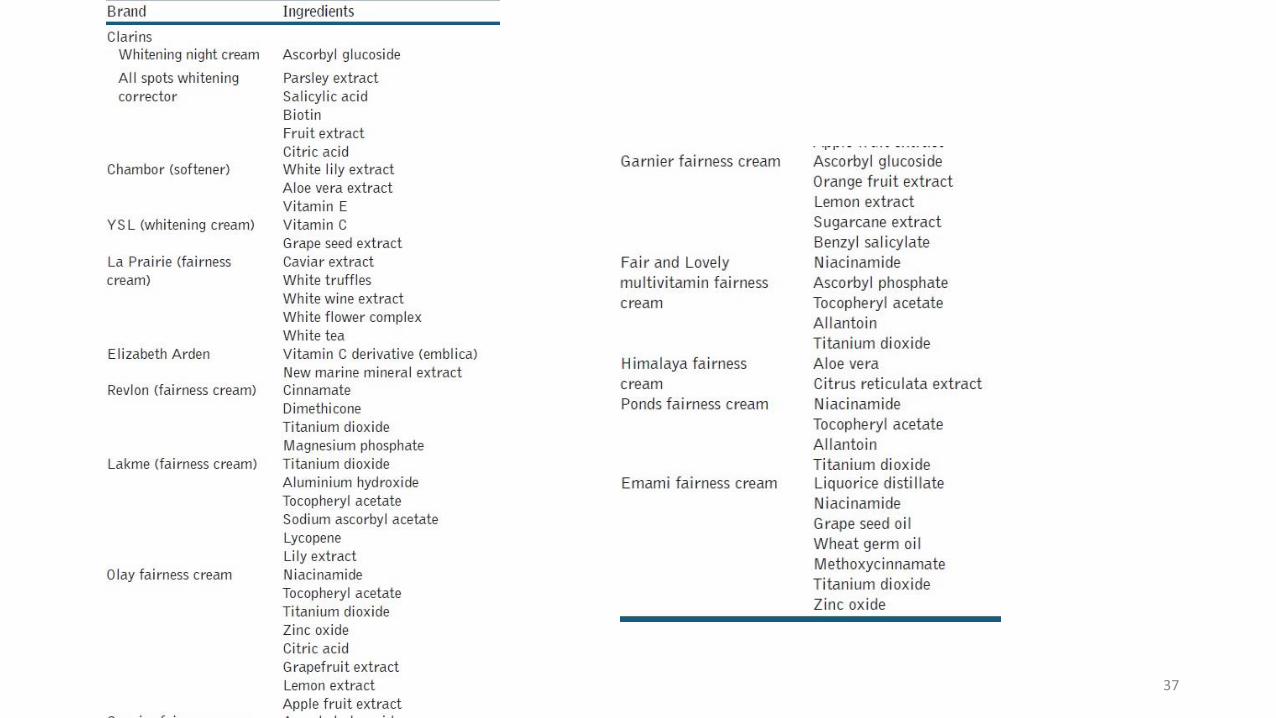
• Skin Brightening: formulations that brighten uneven skin tone & contain alternatives to HQ → botanicals, natural ingredients,
peptides & Vits
• The term “tyrosinase inhibitor” has been used widely in the market to define a skin-brightening active
❖ not all skin-brightening ingredients directly interfere with the catalyzing of the tyrosinase enzyme.
❑ The labeling of the product contains→
• a statement of the indications : “For the gradual fading or lightening of dark discolorations/spots/areas/freckles/age spots.”
• + contain the appropriate warnings identified by the FDA.
❖ term used to describe alternatives is “skin brightening,” or you can say it helps to promote a more even skin tone
12
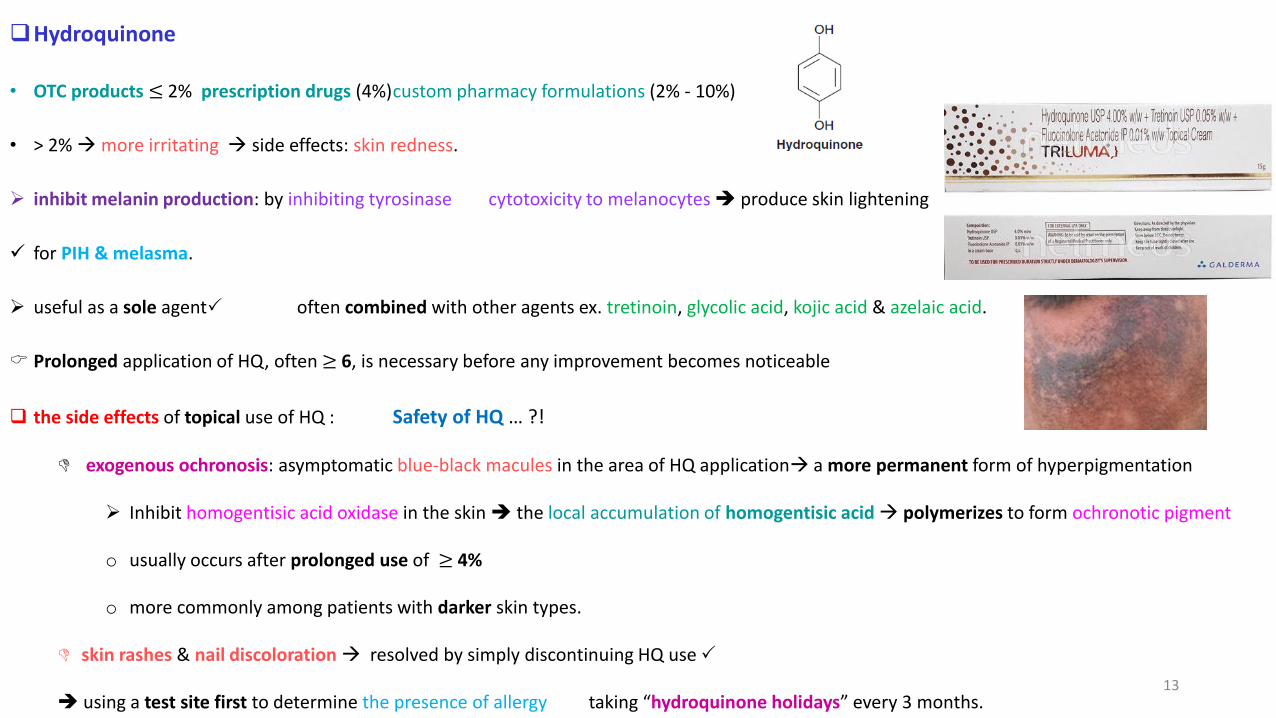
❑Hydroquinone
• OTC products ≤ 2% prescription drugs (4%)custom pharmacy formulations (2% - 10%)
• > 2% →more irritating → side effects: skin redness.
➢ inhibit melanin production: by inhibiting tyrosinase cytotoxicity to melanocytes ➔ produce skin lightening
✓ for PIH & melasma.
➢ useful as a sole agent often combined with other agents ex. tretinoin, glycolic acid, kojic acid & azelaic acid.
Prolonged application of HQ, often ≥ 6, is necessary before any improvement becomes noticeable
❑ the side effects of topical use of HQ : Safety of HQ … ?!
exogenous ochronosis: asymptomatic blue-black macules in the area of HQ application→ a more permanent form of hyperpigmentation
➢ Inhibit homogentisic acid oxidase in the skin ➔ the local accumulation of homogentisic acid → polymerizes to form ochronotic pigment
o usually occurs after prolonged use of ≥ 4%
o more commonly among patients with darker skin types.
skin rashes & nail discoloration → resolved by simply discontinuing HQ use
➔ using a test site first to determine the presence of allergy taking “hydroquinone holidays” every 3 months.13
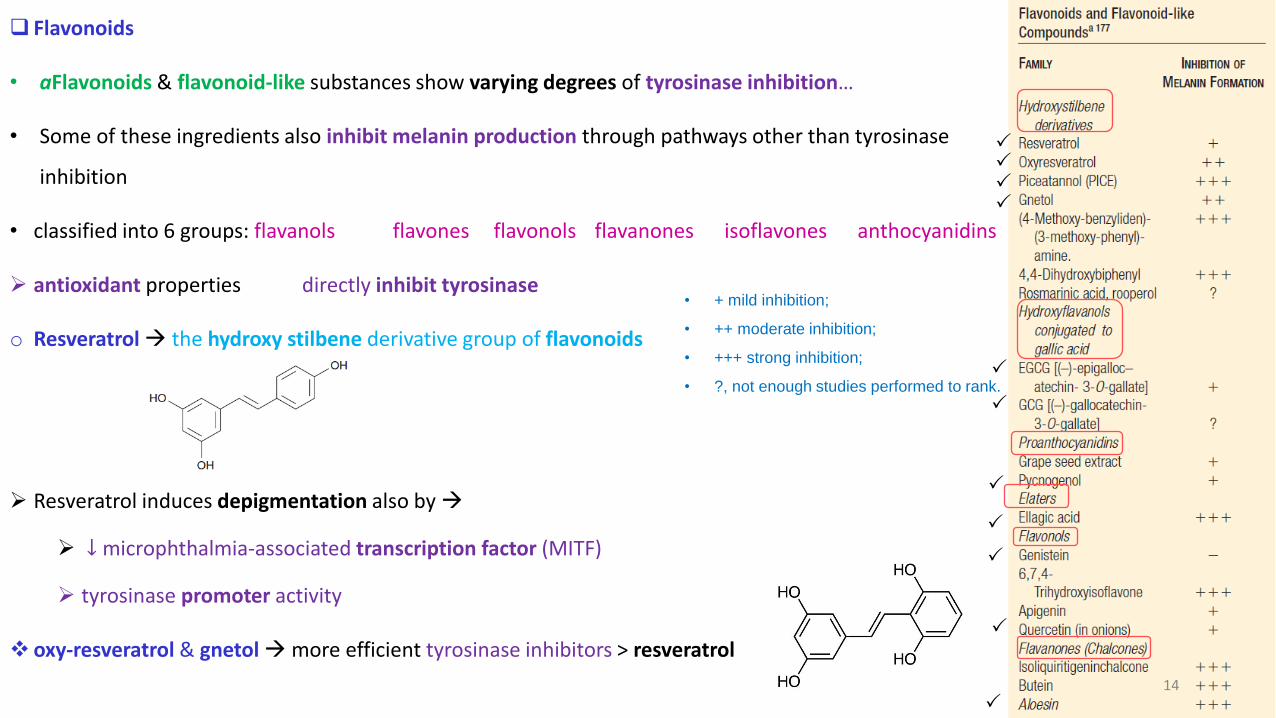
❑ Flavonoids
• aFlavonoids & flavonoid-like substances show varying degrees of tyrosinase inhibition…
• Some of these ingredients also inhibit melanin production through pathways other than tyrosinase
inhibition
• classified into 6 groups: flavanols flavones flavonols flavanones isoflavones anthocyanidins
➢ antioxidant properties directly inhibit tyrosinase
o Resveratrol→ the hydroxy stilbene derivative group of flavonoids
➢ Resveratrol induces depigmentation also by →
➢ ↓ microphthalmia-associated transcription factor (MITF)
➢ tyrosinase promoter activity
❖ oxy-resveratrol & gnetol→more efficient tyrosinase inhibitors > resveratrol
14
• + mild inhibition;
• ++ moderate inhibition;
• +++ strong inhibition;
• ?, not enough studies performed to rank.
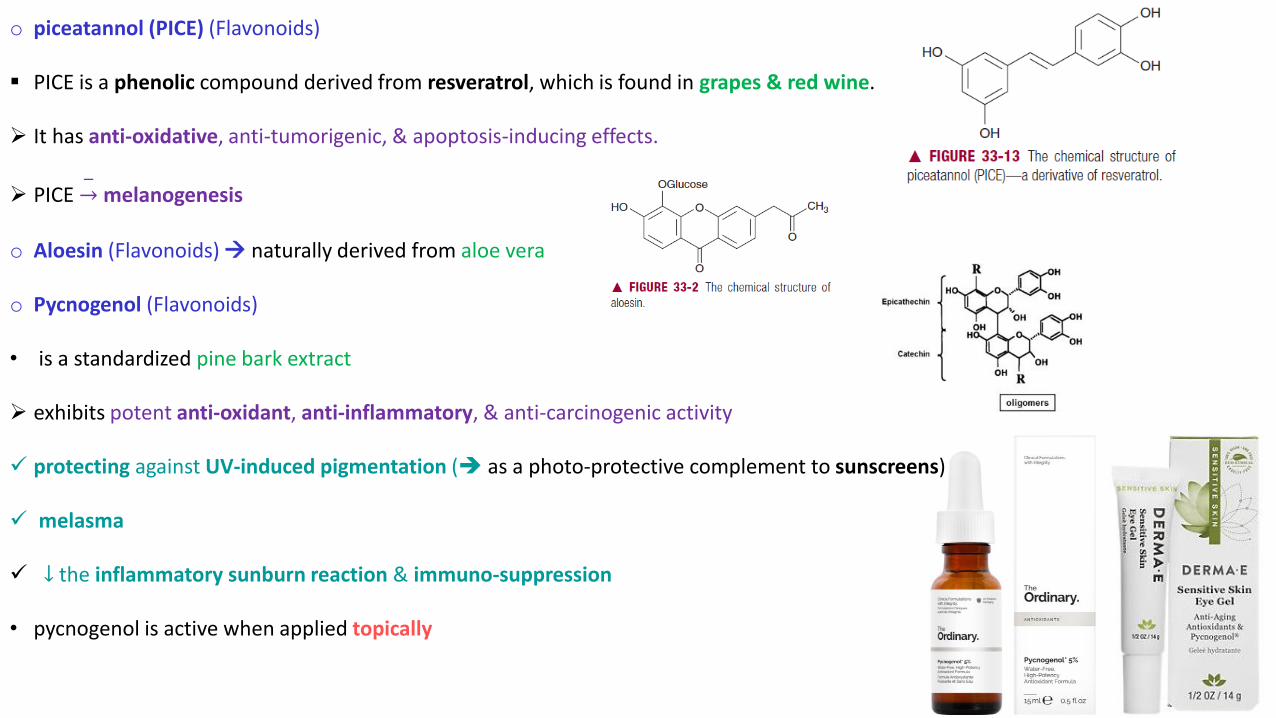
o piceatannol (PICE) (Flavonoids)
▪ PICE is a phenolic compound derived from resveratrol, which is found in grapes & red wine.
➢ It has anti-oxidative, anti-tumorigenic, & apoptosis-inducing effects.
➢ PICE ՜−
melanogenesis
o Aloesin (Flavonoids) → naturally derived from aloe vera
o Pycnogenol (Flavonoids)
• is a standardized pine bark extract
➢ exhibits potent anti-oxidant, anti-inflammatory, & anti-carcinogenic activity
✓ protecting against UV-induced pigmentation (➔ as a photo-protective complement to sunscreens)
✓ melasma
✓ ↓ the inflammatory sunburn reaction & immuno-suppression
• pycnogenol is active when applied topically
15
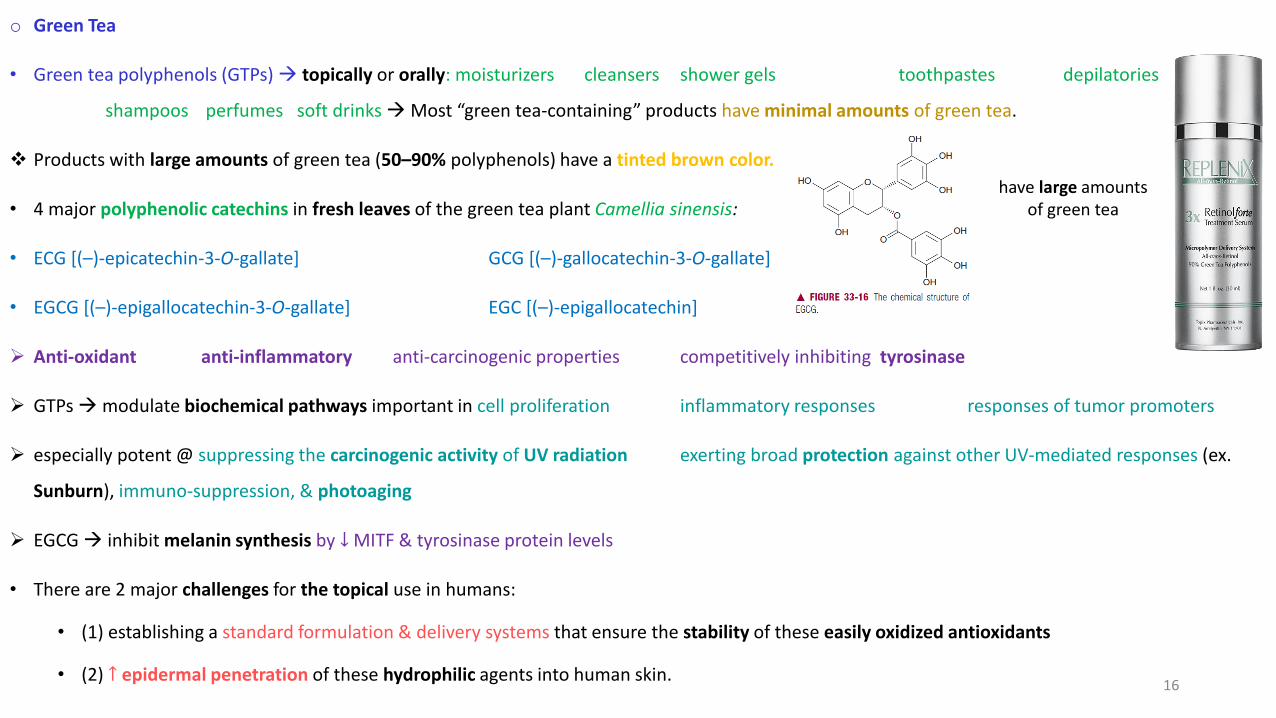
o Green Tea
• Green tea polyphenols (GTPs) → topically or orally: moisturizers cleansers shower gels toothpastes depilatories
shampoos perfumes soft drinks →Most “green tea-containing” products have minimal amounts of green tea.
❖ Products with large amounts of green tea (50–90% polyphenols) have a tinted brown color.
• 4 major polyphenolic catechins in fresh leaves of the green tea plant Camellia sinensis:
• ECG [(–)-epicatechin-3-O-gallate] GCG [(–)-gallocatechin-3-O-gallate]
• EGCG [(–)-epigallocatechin-3-O-gallate] EGC [(–)-epigallocatechin]
➢ Anti-oxidant anti-inflammatory anti-carcinogenic properties competitively inhibiting tyrosinase
➢ GTPs →modulate biochemical pathways important in cell proliferation inflammatory responses responses of tumor promoters
➢ especially potent @ suppressing the carcinogenic activity of UV radiation exerting broad protection against other UV-mediated responses (ex.
Sunburn), immuno-suppression, & photoaging
➢ EGCG → inhibit melanin synthesis by ↓ MITF & tyrosinase protein levels
• There are 2 major challenges for the topical use in humans:
• (1) establishing a standard formulation & delivery systems that ensure the stability of these easily oxidized antioxidants
• (2) ↑ epidermal penetration of these hydrophilic agents into human skin.
have large amounts of green tea
16

o Silymarin
• a naturally-occurring polyphenolic flavonoid or flavonolignans compound derived from the seeds of the
milk thistle plant Silybum marianum.
• The main component of silymarin is silybin (silibinin) → its most biologically active constituent for anti-
oxidant anti-inflammatory anti-carcinogenic properties.
• Topical application of silybin prior to, or immediately after, UV irradiation → strong protection against
UV-induced damage in the epidermis
• silybin enhances UVB-induced apoptosis & acts as a UVB damage sensor to confer its biologic action.
• Chemoprotective activity against skin cancer inhibit UV-induced NF-B activation in keratinocytes
➢→ free radical scavenging & a modulation of intracellular GSH content.
• ➔ silymarin may favorably supplement sunscreen protection & provide additional anti photo-
carcinogenic protection
• oral supplements .
17
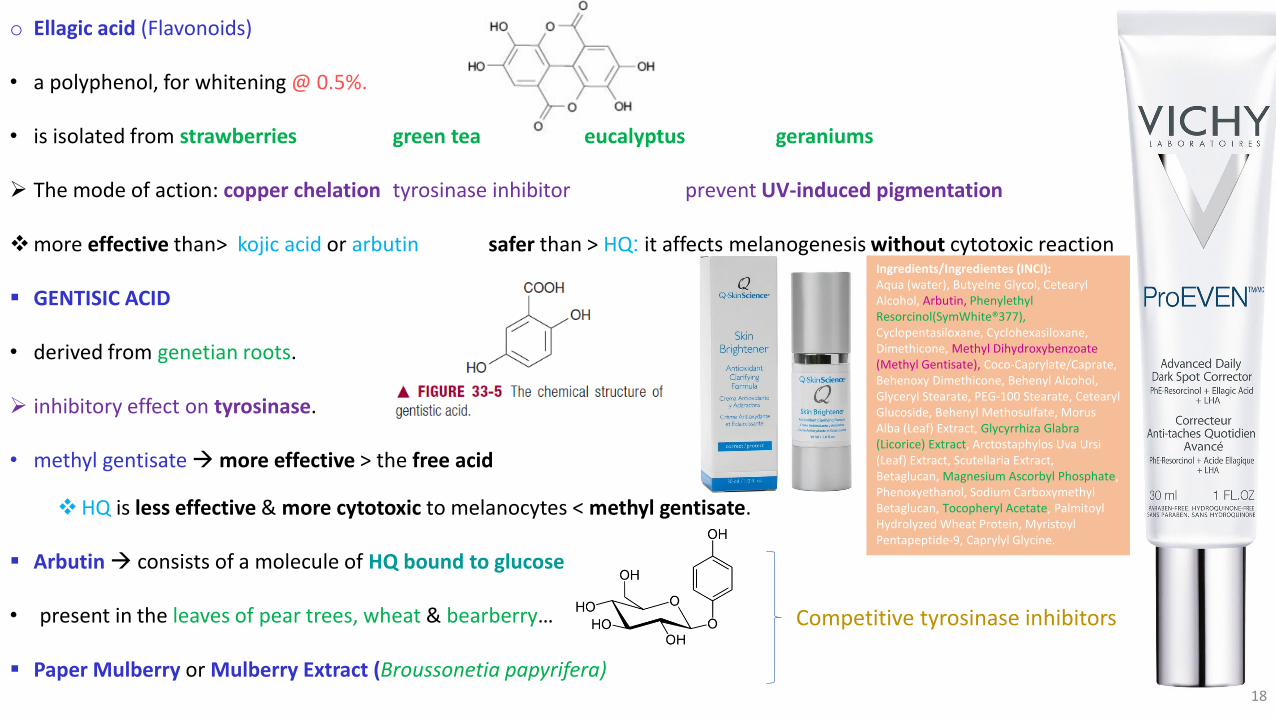
o Ellagic acid (Flavonoids)
• a polyphenol, for whitening @ 0.5%.
• is isolated from strawberries green tea eucalyptus geraniums
➢ The mode of action: copper chelation tyrosinase inhibitor prevent UV-induced pigmentation
❖more effective than> kojic acid or arbutin safer than > HQ: it affects melanogenesis without cytotoxic reaction
▪ GENTISIC ACID
• derived from genetian roots.
➢ inhibitory effect on tyrosinase.
• methyl gentisate →more effective > the free acid
❖HQ is less effective & more cytotoxic to melanocytes < methyl gentisate.
▪ Arbutin → consists of a molecule of HQ bound to glucose
• present in the leaves of pear trees, wheat & bearberry…
▪ Paper Mulberry or Mulberry Extract (Broussonetia papyrifera)18
Competitive tyrosinase inhibitors
Ingredients/Ingredientes (INCI):Aqua (water), Butyelne Glycol, CetearylAlcohol, Arbutin, Phenylethyl Resorcinol(SymWhite®377), Cyclopentasiloxane, Cyclohexasiloxane, Dimethicone, Methyl Dihydroxybenzoate (Methyl Gentisate), Coco-Caprylate/Caprate, Behenoxy Dimethicone, Behenyl Alcohol, Glyceryl Stearate, PEG-100 Stearate, CetearylGlucoside, Behenyl Methosulfate, Morus Alba (Leaf) Extract, Glycyrrhiza Glabra (Licorice) Extract, Arctostaphylos Uva Ursi(Leaf) Extract, Scutellaria Extract, Betaglucan, Magnesium Ascorbyl Phosphate, Phenoxyethanol, Sodium Carboxymethyl Betaglucan, Tocopheryl Acetate, Palmitoyl Hydrolyzed Wheat Protein, MyristoylPentapeptide-9, Caprylyl Glycine.
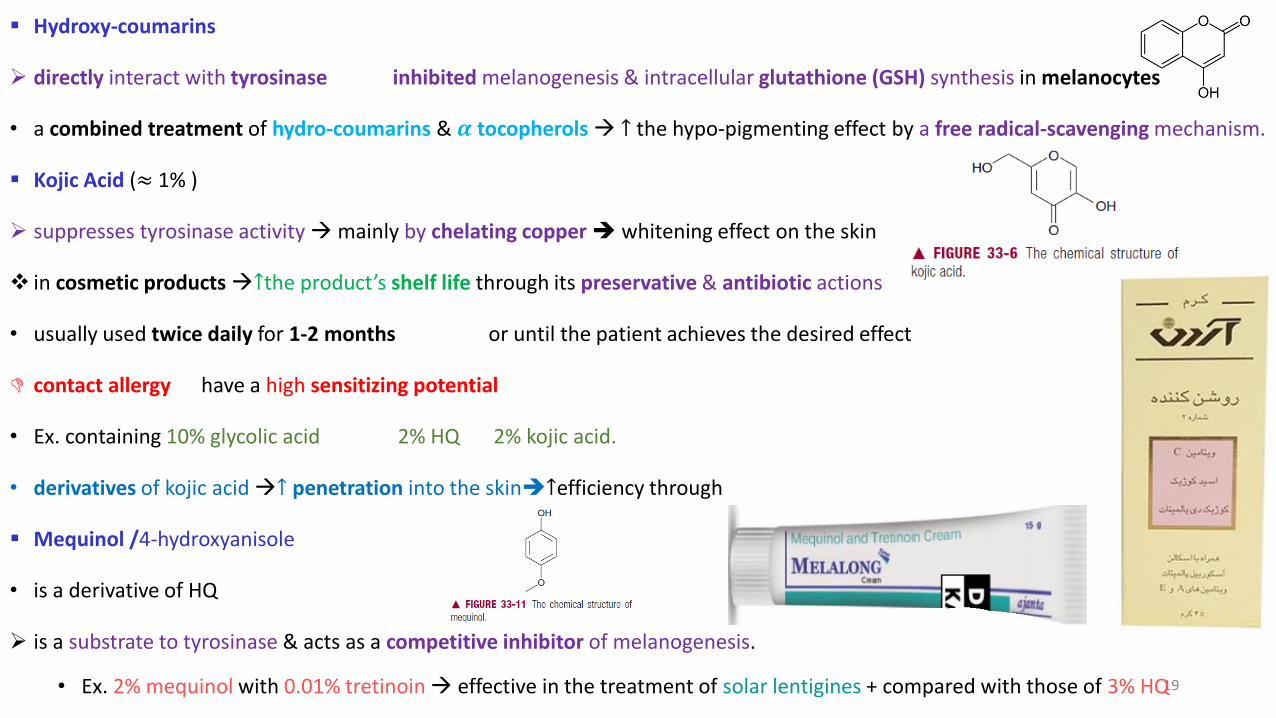
▪ Hydroxy-coumarins
➢ directly interact with tyrosinase inhibited melanogenesis & intracellular glutathione (GSH) synthesis in melanocytes
• a combined treatment of hydro-coumarins & 𝜶 tocopherols → ↑ the hypo-pigmenting effect by a free radical-scavenging mechanism.
▪ Kojic Acid (≈ 1% )
➢ suppresses tyrosinase activity →mainly by chelating copper ➔ whitening effect on the skin
❖ in cosmetic products→↑the product’s shelf life through its preservative & antibiotic actions
• usually used twice daily for 1-2 months or until the patient achieves the desired effect
contact allergy have a high sensitizing potential
• Ex. containing 10% glycolic acid 2% HQ 2% kojic acid.
• derivatives of kojic acid →↑ penetration into the skin➔↑efficiency through
▪ Mequinol /4-hydroxyanisole
• is a derivative of HQ
➢ is a substrate to tyrosinase & acts as a competitive inhibitor of melanogenesis.
• Ex. 2% mequinol with 0.01% tretinoin → effective in the treatment of solar lentigines + compared with those of 3% HQ 19
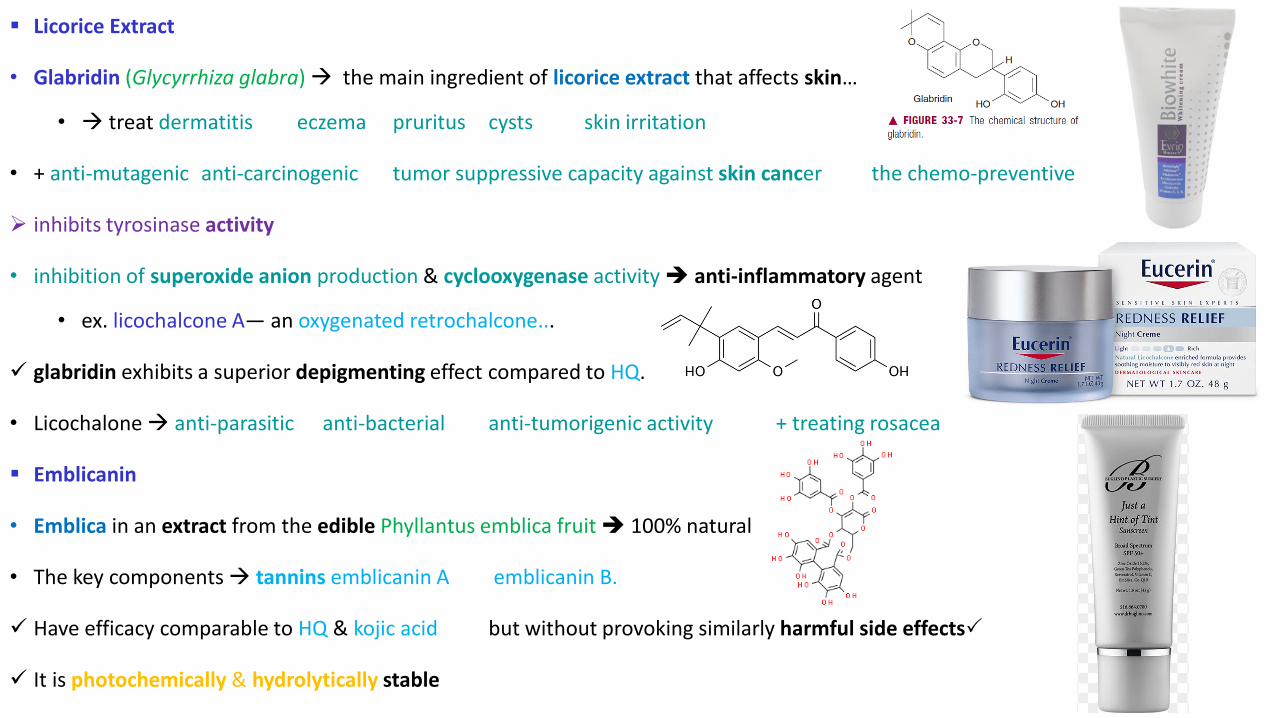
▪ Licorice Extract
• Glabridin (Glycyrrhiza glabra) → the main ingredient of licorice extract that affects skin…
• → treat dermatitis eczema pruritus cysts skin irritation
• + anti-mutagenic anti-carcinogenic tumor suppressive capacity against skin cancer the chemo-preventive
➢ inhibits tyrosinase activity
• inhibition of superoxide anion production & cyclooxygenase activity ➔ anti-inflammatory agent
• ex. licochalcone A— an oxygenated retrochalcone...
✓ glabridin exhibits a superior depigmenting effect compared to HQ.
• Licochalone→ anti-parasitic anti-bacterial anti-tumorigenic activity + treating rosacea
▪ Emblicanin
• Emblica in an extract from the edible Phyllantus emblica fruit ➔ 100% natural
• The key components → tannins emblicanin A emblicanin B.
✓ Have efficacy comparable to HQ & kojic acid but without provoking similarly harmful side effects
✓ It is photochemically & hydrolytically stable 20
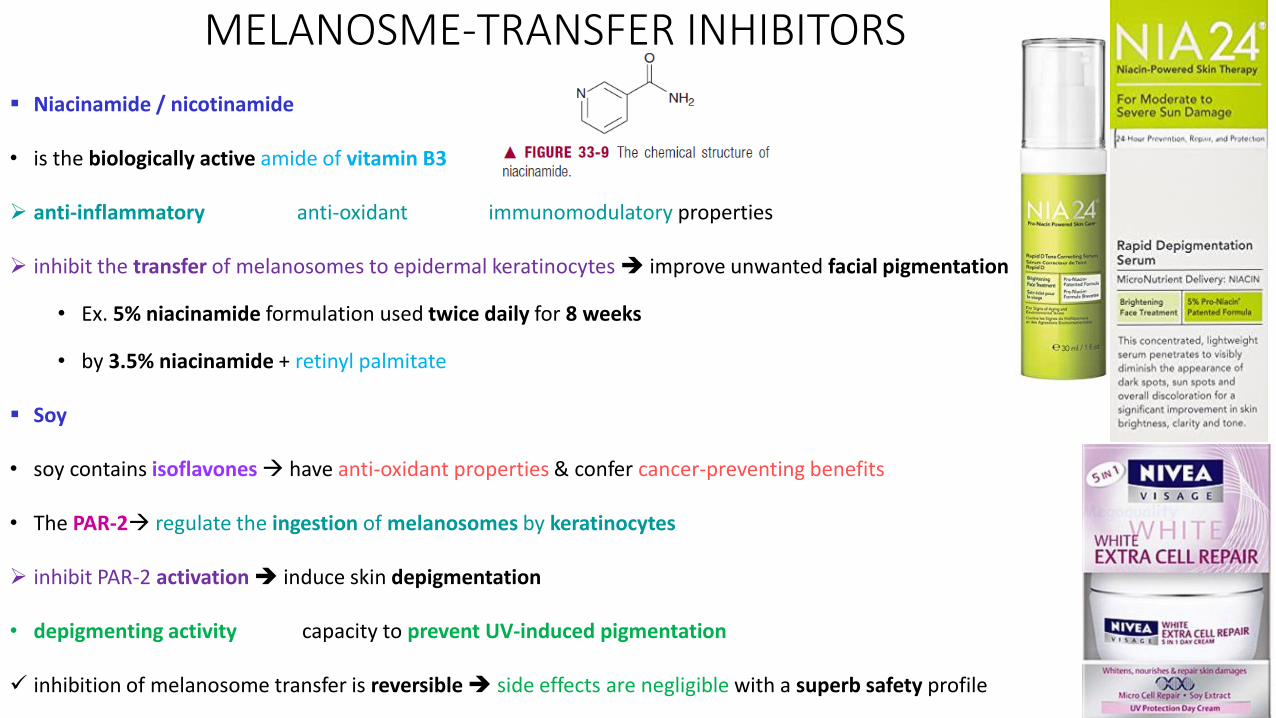
MELANOSME-TRANSFER INHIBITORS
▪ Niacinamide / nicotinamide
• is the biologically active amide of vitamin B3
➢ anti-inflammatory anti-oxidant immunomodulatory properties
➢ inhibit the transfer of melanosomes to epidermal keratinocytes ➔ improve unwanted facial pigmentation
• Ex. 5% niacinamide formulation used twice daily for 8 weeks
• by 3.5% niacinamide + retinyl palmitate
▪ Soy
• soy contains isoflavones→ have anti-oxidant properties & confer cancer-preventing benefits
• The PAR-2→ regulate the ingestion of melanosomes by keratinocytes
➢ inhibit PAR-2 activation➔ induce skin depigmentation
• depigmenting activity capacity to prevent UV-induced pigmentation
✓ inhibition of melanosome transfer is reversible➔ side effects are negligible with a superb safety profile 21

Melanocyte-cytotoxic agents▪ Azelaic Acid
• Azelaic acid (Azelex™, FinaceaR) → a naturally-occurring saturated di-carboxylic acid
• a useful adjunct in the treatment of post-inflammatory pigment alteration (PIPA).
➢ ՜−
the energy production &/or DNA synthesis of hyperactive melanocytes
➢ partially antit-tyrosinase activity (competitive inhibitor)
➢ in part inhibitory action on neutrophil-generated ROS: is a scavenger of OH° & inhibits oxyradical toxicity ➔ ↓
oxidative tissue injury @ sites of inflammation & in melanin formation.
✓ AA is even more effective > topical HQ for patients with melasma, without the latter’s side effects
• ex. (azelaic acid 20% cream + glycolic acid 15% or 20% lotion) is as effective as 4% HQ cream
• In the US, topical azelaic acid is available by prescription → 15% gel (rosacea) 20% cream (acne)
The use for hyperpigmentation is off-label
• is well tolerated → adverse effects generally limited to mild local cutaneous irritation.
▪ N-Acetyl-4-S-cysteaminyl phenol (NACP)
➢ is a melano cytotoxic agent consisting of phenolic & catecholic compounds with potent depigmenting properties 22
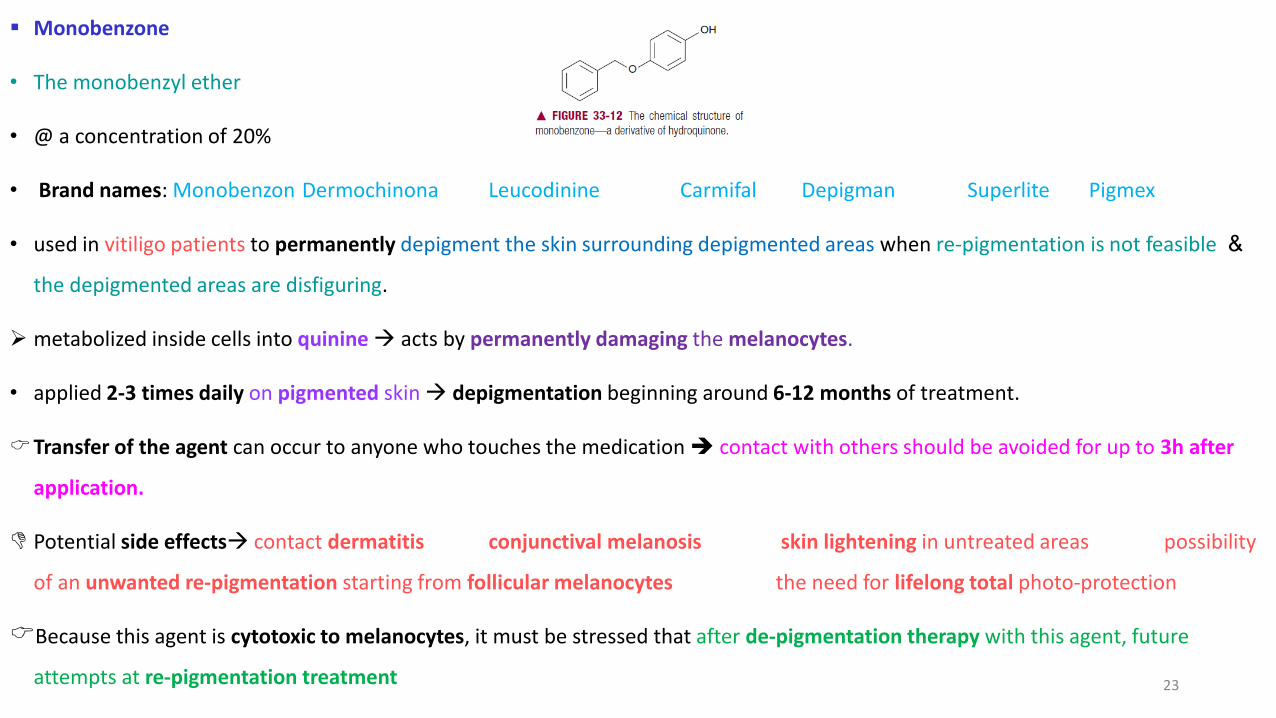
▪ Monobenzone
• The monobenzyl ether
• @ a concentration of 20%
• Brand names: Monobenzon Dermochinona Leucodinine Carmifal Depigman Superlite Pigmex
• used in vitiligo patients to permanently depigment the skin surrounding depigmented areas when re-pigmentation is not feasible &
the depigmented areas are disfiguring.
➢ metabolized inside cells into quinine→ acts by permanently damaging the melanocytes.
• applied 2-3 times daily on pigmented skin→ depigmentation beginning around 6-12 months of treatment.
Transfer of the agent can occur to anyone who touches the medication ➔ contact with others should be avoided for up to 3h after
application.
Potential side effects→ contact dermatitis conjunctival melanosis skin lightening in untreated areas possibility
of an unwanted re-pigmentation starting from follicular melanocytes the need for lifelong total photo-protection
Because this agent is cytotoxic to melanocytes, it must be stressed that after de-pigmentation therapy with this agent, future
attempts at re-pigmentation treatment 23
ANTIOXIDANTS➢ Antioxidants→ anti-aging anti-carcinogenic anti-inflammatory activities ↓ pigmentation that occurs after exposure to UV light
(➔ treatment of melasma, In vitiligo: anti-oxidants may affect melanin production)
➢ Anti-oxidants (ex, GSH, a naturally-occurring anti-oxidant involved in regulating melanin synthesis) → inhibit or delay
hyperpigmentation
• comparison of normal melanocytes ↔melanocytes from vitiligo patients: levels in the vitiligo patients: lower catalase activity &
higher vitamin E & ubiquinone (CoQ10) ➔ an imbalance in the anti-oxidant status & ↑ the intracellular peroxide levels
❖ some anti-oxidants ↑ skin pigmentation ➔ the individual properties of each anti-oxidant should be considered before using them to ↓
skin pigmentation ➔ the indiscriminate use of these compounds should be weighed with caution.
Each anti-oxidant & its effects should be considered separately & it should not be assumed that all anti-oxidants will inhibit
melanogenesis → an opposite effect seems to be possible in some cases & unexpected hyper-pigmentation can occur.
• ex, quercetin, an extract of onion, is a tyrosinase inhibitor in vitro; however, this flavonol is a strong inductor of melanogenesis in
normal & malignant human melanocytes, & in reconstituted 3D human epidermis models.
• Glycyrrhizin → popular anti-oxidant frequently used to inhibit tyrosinase → stimulate melanogenesis in B16 melanoma cells.24
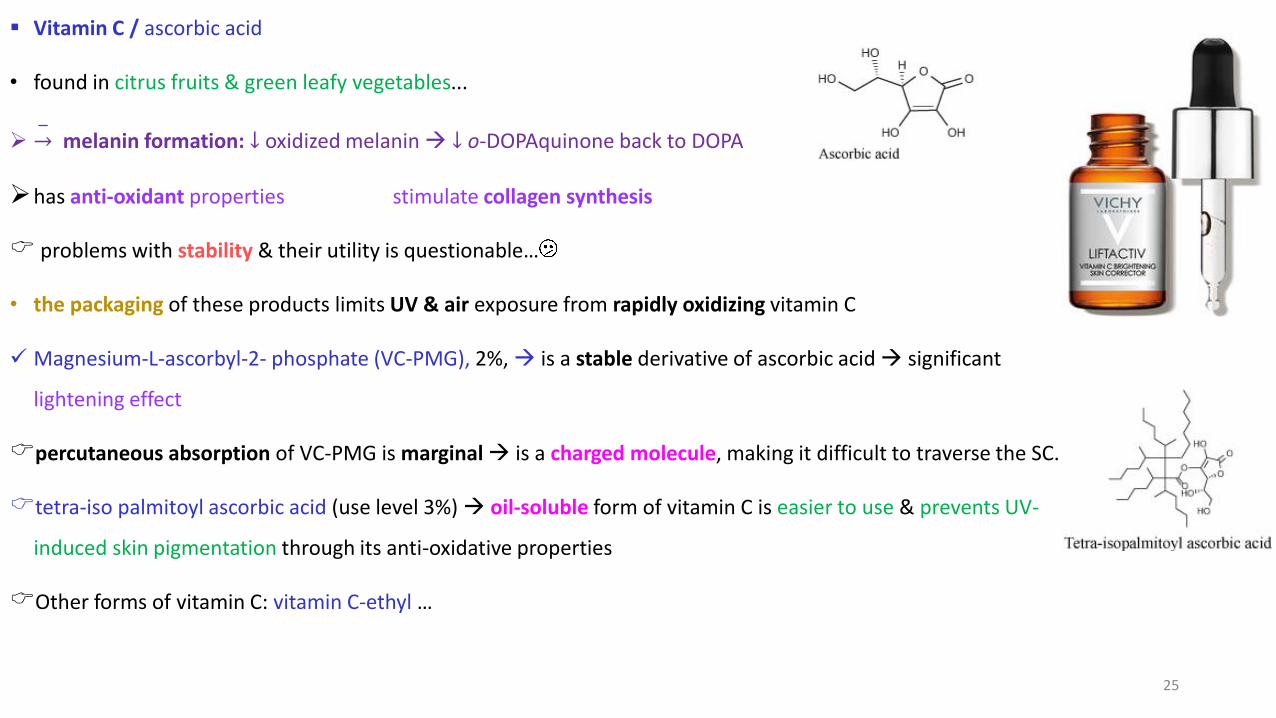
▪ Vitamin C / ascorbic acid
• found in citrus fruits & green leafy vegetables...
➢ ՜−
melanin formation: ↓ oxidized melanin → ↓ o-DOPAquinone back to DOPA
➢has anti-oxidant properties stimulate collagen synthesis
problems with stability & their utility is questionable…
• the packaging of these products limits UV & air exposure from rapidly oxidizing vitamin C
✓ Magnesium-L-ascorbyl-2- phosphate (VC-PMG), 2%,→ is a stable derivative of ascorbic acid → significant
lightening effect
percutaneous absorption of VC-PMG is marginal → is a charged molecule, making it difficult to traverse the SC.
tetra-iso palmitoyl ascorbic acid (use level 3%) → oil-soluble form of vitamin C is easier to use & prevents UV-
induced skin pigmentation through its anti-oxidative properties
Other forms of vitamin C: vitamin C-ethyl …
25
▪ Vitamin E
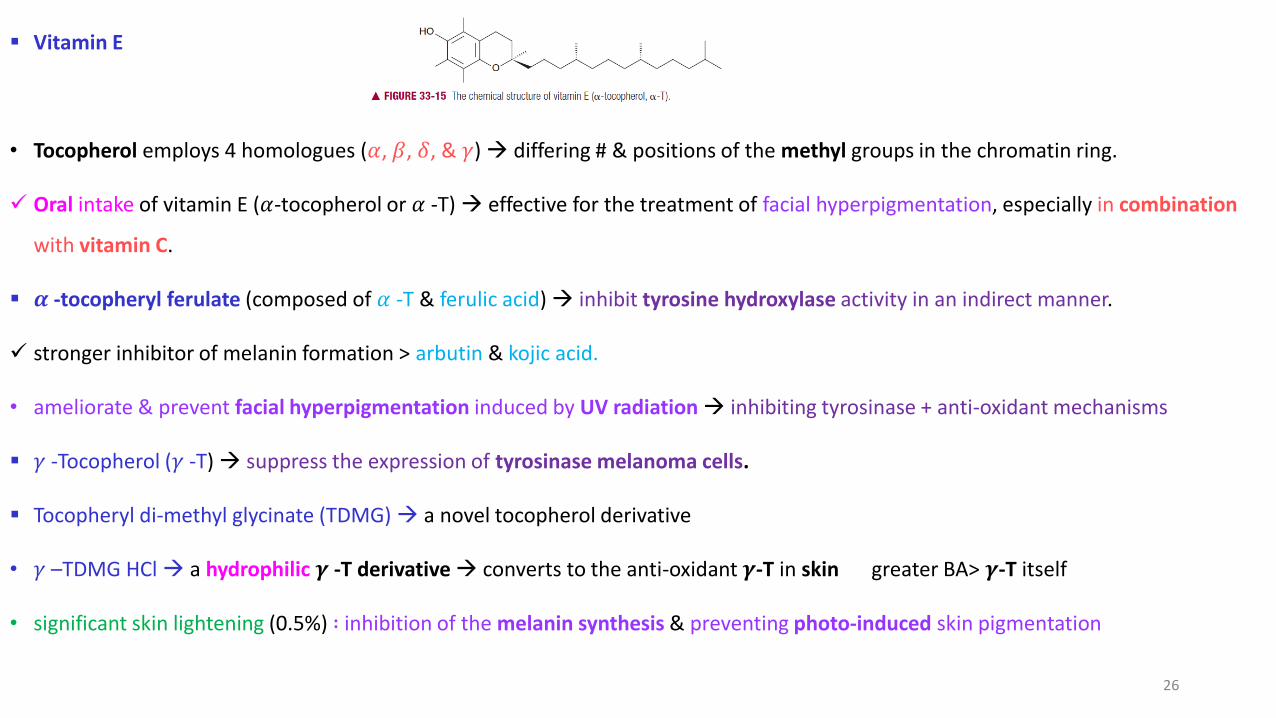
• Tocopherol employs 4 homologues (𝛼, 𝛽, 𝛿, & 𝛾) → differing # & positions of the methyl groups in the chromatin ring.
✓ Oral intake of vitamin E (𝛼-tocopherol or 𝛼 -T) → effective for the treatment of facial hyperpigmentation, especially in combination
with vitamin C.
▪ 𝜶 -tocopheryl ferulate (composed of 𝛼 -T & ferulic acid) → inhibit tyrosine hydroxylase activity in an indirect manner.
✓ stronger inhibitor of melanin formation > arbutin & kojic acid.
• ameliorate & prevent facial hyperpigmentation induced by UV radiation → inhibiting tyrosinase + anti-oxidant mechanisms
▪ 𝛾 -Tocopherol (𝛾 -T) → suppress the expression of tyrosinase melanoma cells.
▪ Tocopheryl di-methyl glycinate (TDMG) → a novel tocopherol derivative
• 𝛾 –TDMG HCl → a hydrophilic 𝜸 -T derivative → converts to the anti-oxidant 𝜸-T in skin greater BA> 𝜸-T itself
• significant skin lightening (0.5%) ∶ inhibition of the melanin synthesis & preventing photo-induced skin pigmentation
26
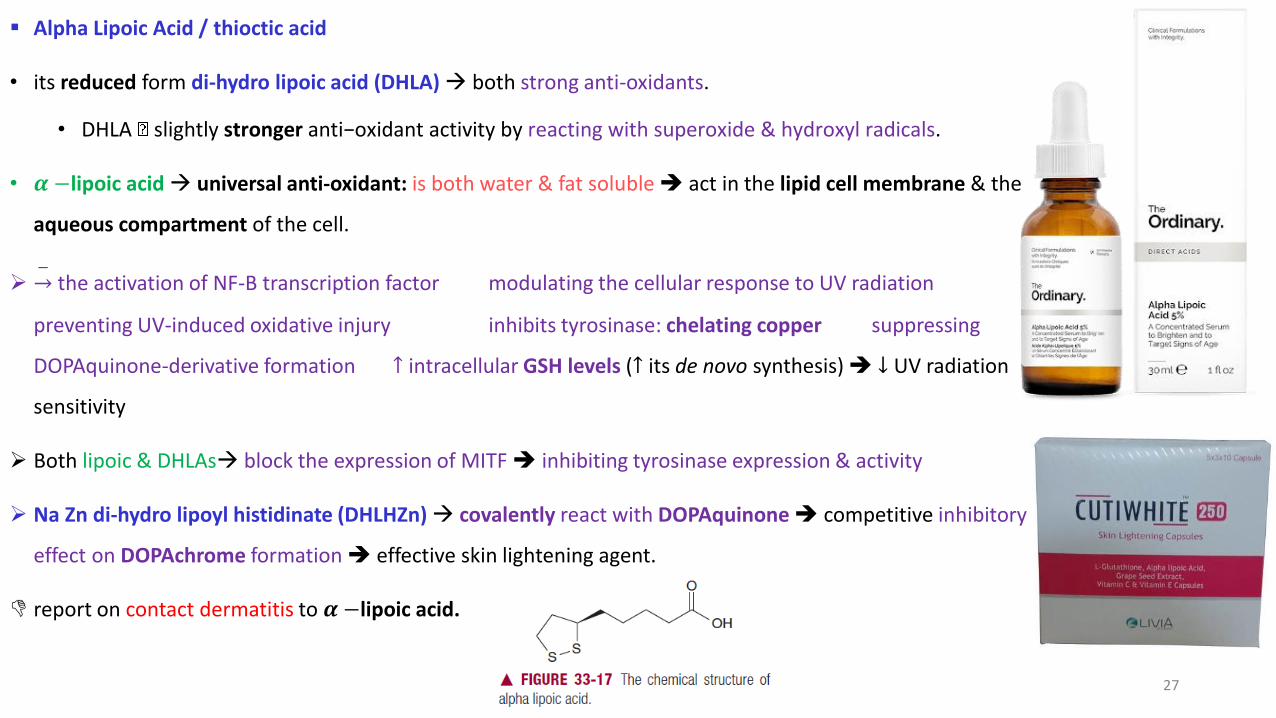
▪ Alpha Lipoic Acid / thioctic acid
• its reduced form di-hydro lipoic acid (DHLA) → both strong anti-oxidants.
• DHLA slightly stronger anti−oxidant activity by reacting with superoxide & hydroxyl radicals.
• 𝜶 −lipoic acid → universal anti-oxidant: is both water & fat soluble ➔ act in the lipid cell membrane & the
aqueous compartment of the cell.
➢ ՜−
the activation of NF-B transcription factor modulating the cellular response to UV radiation
preventing UV-induced oxidative injury inhibits tyrosinase: chelating copper suppressing
DOPAquinone-derivative formation ↑ intracellular GSH levels (↑ its de novo synthesis) ➔ ↓ UV radiation
sensitivity
➢ Both lipoic & DHLAs→ block the expression of MITF ➔ inhibiting tyrosinase expression & activity
➢ Na Zn di-hydro lipoyl histidinate (DHLHZn)→ covalently react with DOPAquinone➔ competitive inhibitory
effect on DOPAchrome formation ➔ effective skin lightening agent.
report on contact dermatitis to 𝜶 −lipoic acid.
27

❑ 𝜶- Hydroxy Acids (AHA) & 𝜷- Hydroxy Acid (BHA)
• Ex. Glycolic Acid → very versatile peeling agent minimal complications used in 20-70%
• lactic Acid
✓ People with virtually any skin type can be candidates for AHA & BHA peels
• they exert different effects on the epidermis & the dermis...
• In the epidermis: diminished corneocyte cohesion➔more rapid desquamation of the pigmented keratinocytes → the newly formed
keratinocytes will contain less pigment ↑ the keratinocyte turnover rate ➔ shortening the cell cycle.
• In melanoma cells AHAs also directly inhibit tyrosinase activity.
✓ glycolic acid peels →minimal adverse effects for the treatment of PIH
• lactic acid → treat melasma + ↓ pigmentation
When treating PIPA with peels, it is initially important to use lower concentrations of AHA
& slowly ↑ the strength to avoid irritating the skin, causing even more hyperpigmentation.
✓ The use of topical HQ preparations pre-& post-peel ↓ the chances of aggravating PIPA.
OTHER AGENTS
28
❑Retinoids
✓ lipophilic vitamin A derivatives → easily penetrate the epidermis.
➢ directly influencing melanocytes indirectly modulating melanogenesis
➢ Topical retinoids directly affect melanogenesis via tyrosinase, TRP-1 & -2 expression.
➢
𝒊𝒏𝒉𝒊𝒃𝒊𝒕detoxification of toxic species➔ ↑ the melano-cytotoxic effect of depigmenting agents.
➢ By accelerating the cell turnover of epidermal keratinocytes→ promote ↓ melanosome transfer to the keratinocytes
➔ induces desquamation ➔ accelerated loss of melanin in the SC.
➢ induce dispersion of keratinocyte pigment granules➔ a uniform distribution of melanin content in the epidermis + ↓ the
cohesiveness of corneocytes
✓ Indirectly: changes in the SC may facilitate the penetration of other/additional depigmenting agents into the epidermis & ↑ their B.A
➔ ↑ depigmentation
• Tretinoin (Retin-A™, Renova™, Avita™) (0.05- 0.1%) → used to treat PIPA & melasma
• It is frequently employed as an adjuvant in the treatment of pigmentation disorders29

• The topical retinoid tazarotene (Avage™, Tazorac™)→ improve irregular hyper-pigmentation associated with photoaging
✓ Adapalene (Differin Gel™ 0.1% and 0.3%) is a potent synthetic retinoid → had significantly fewer side effects.
• Oral 0.05% isotretinoin → not statistically significant results in treating Thai patients with melasma.
The side effects of retinoids: dryness irritation scaling: signs of a damaged skin barrier ➔ This condition allows for other agents to
more readily penetrate into the skin & ↑efficacy (ex., with HQ)
➢ It is advisable to add a corticosteroid to retinoid therapy to mitigate irritation.
• the combination consisting of 0.1% tretinoin+ 5% HQ+ 0.1% dexamethasone → the Kligman formula → treat melasma.
30
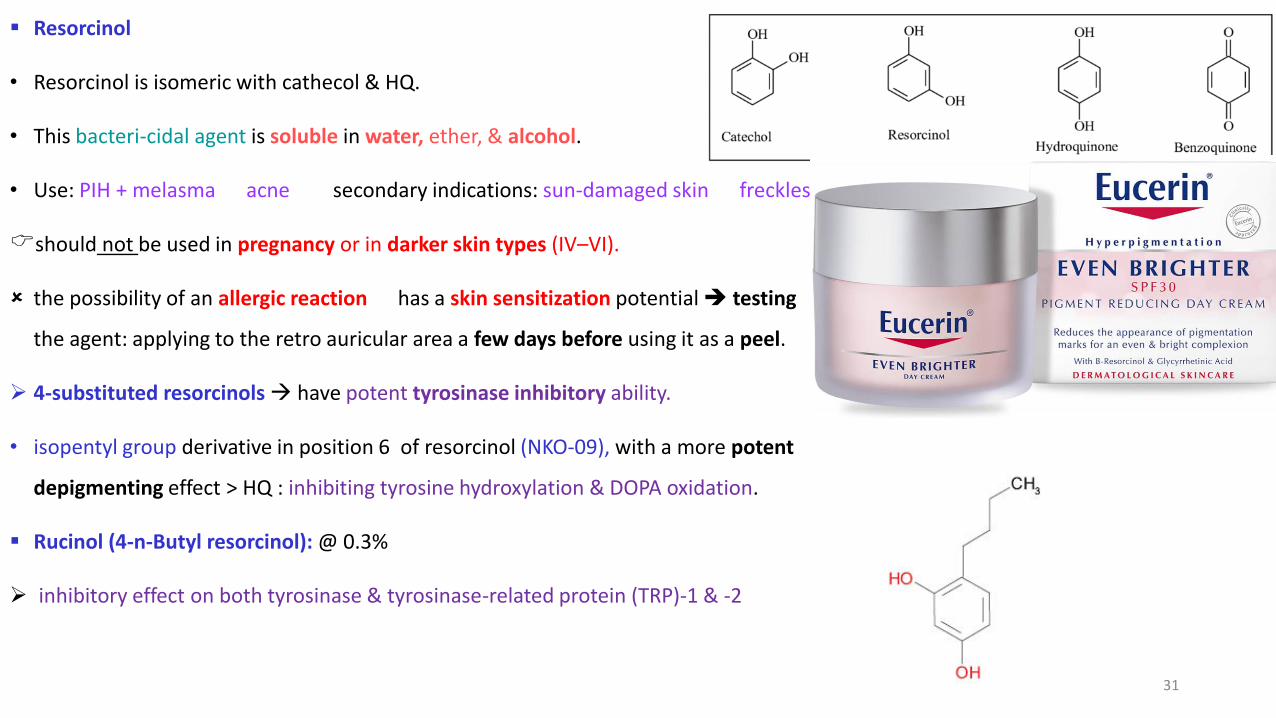
▪ Resorcinol
• Resorcinol is isomeric with cathecol & HQ.
• This bacteri-cidal agent is soluble in water, ether, & alcohol.
• Use: PIH + melasma acne secondary indications: sun-damaged skin freckles
should not be used in pregnancy or in darker skin types (IV–VI).
the possibility of an allergic reaction has a skin sensitization potential ➔ testing
the agent: applying to the retro auricular area a few days before using it as a peel.
➢ 4-substituted resorcinols→ have potent tyrosinase inhibitory ability.
• isopentyl group derivative in position 6 of resorcinol (NKO-09), with a more potent
depigmenting effect > HQ : inhibiting tyrosine hydroxylation & DOPA oxidation.
▪ Rucinol (4-n-Butyl resorcinol): @ 0.3%
➢ inhibitory effect on both tyrosinase & tyrosinase-related protein (TRP)-1 & -2
31
▪ Octa-decene dioic Acid (ODA)
• is a skin-whitening agent with a similar structure to azelaic acid.
➢ is a PPAR-𝛾 (peroxisome proliferator-activating receptor ) agonist→ the stimulate PPAR
• PPARs are members of the nuclear receptor superfamily, regulating important cellular functions: cell proliferation &
differentiation, + inflammatory responses.
• 3 subtypes of PPAR (designated 𝛼, 𝛽 & 𝛾 ) are expressed in human melanocytes.
➢ The binding to PPAR leads to reduced melanin production through ↓ synthesis of tyrosinase mRNA.
▪ Linoleic acid:
• Linoleic acid (LA) is an unsaturated omega-6 fatty acid called 18:2 (n-6).
• can be obtained from hydrolysis of vegetals (ex. Safflowe evening primrose kukui seed oils).
• Linoleic acid (omega-6) is located in the cell membranes
➢ can ↓ the tyrosinase level accelerate tyrosinase degradation➔ less melanin being produced➔whitening
• @ 0.1% 32
▪ Pyruvic Acid
• is an alpha-keto-acid with keratolytic anti-microbial sebo-static properties
• + stimulate new collagen production & elastic fiber formation.
• treatment of acne effectively ↓ the pigmentation in melasma ↑ skin elasticity ↓ skin wrinkling
✓ No side effects, such as persistent erythema or PIH, were observed.
▪ Tranexamic acid:
• Tranexamic acid is a drug used to treat melasma
➢
inhibitUV-induced hyperpigmentation & melanocyte activity (lightening skin)
• In people with melasma, or dark spots→ the pigment-suppressing abilities of tranxemic acid works best on localized areas of
irregular melanin distribution.
➢ Tranexamic acid prevents the binding of plasminogen (originating from endothelial cells) to keratinocytes→ a possible mechanism
for melasma treatment.
▪ Tranexamic acid cetyl ester HCl → The mode of action is similar to the tranexamic acid used by Shiseido33
▪ 4-Methoxy potassium salicylate (4 MSK):
➢ tyrosinase inhibition
▪ Adenosine mono-phosphate (AMP) di-Na salt: @ 3%
➢ This AMP salt acts as a fuel to the cells ➔ produce more energy ➔ ↑ epidermal turnover & the cells containing melanin will exfoliate
faster ➔ ↓ the melanin content in the skin.
▪ Magnolignan (Di-propyl bi-phenyl-2,2’-di-ol): @ 0.5%
• belongs to the family of poly phenols looks like the magnolol of magnolia.
• Magnolignan retards or slows down the maturation of tyrosinase.
• rhododendrol/ 4-(4-Hydroxy phenyl)-2-butanol (4-HPB) :
➢ a competitive inhibitor of tyrosinase. 34
▪ Chamomilla extract:@ 0.5%
• anti-inflammatory
• the mechanism does not involve tyrosinase
➢ cells communicate with each other & once activated by UVB, the keratinocytes produce alpha-MSH & endotheline→ bind to specific
receptors in the SC & activate the melanocytes
➢→ Chamomille extract acts as an antagonist of this receptor ➔ ↓ the “call” for melanin production.
• Bovine placenta:
• long used along with the use of vitamin C & its derivatives.
• The main source of placental extract was bovine
• it could also come from porcine origin→ recently used to replace the bovine due to the BSE issue (The form of this disease in
humans is the Creutzfeldt Jakob Disease)
➢ the mode of action of placental extract → ↑ cell turnover to remove the melanin from the upper layers of the skin or the role
of high concentrations of minerals & amino acids, to ↓ melanin synthesis 35
36
37
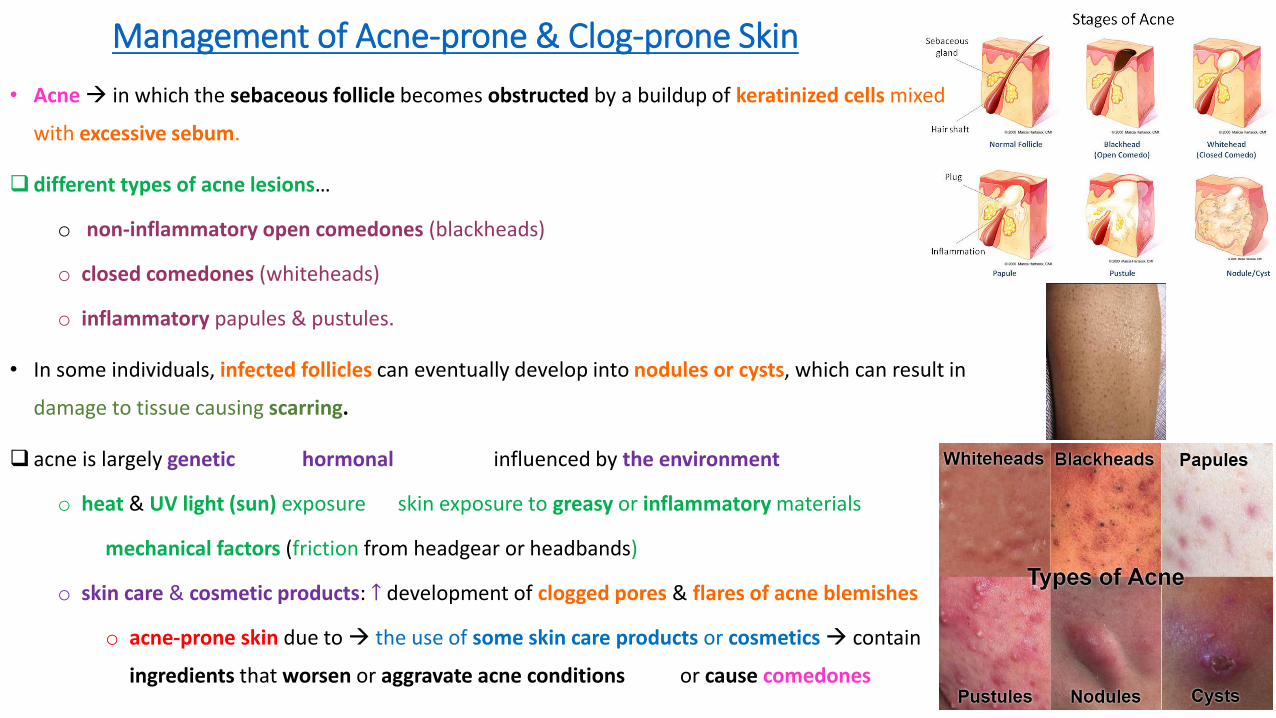
Management of Acne-prone & Clog-prone Skin
• Acne→ in which the sebaceous follicle becomes obstructed by a buildup of keratinized cells mixed
with excessive sebum.
❑ different types of acne lesions…
o non-inflammatory open comedones (blackheads)
o closed comedones (whiteheads)
o inflammatory papules & pustules.
• In some individuals, infected follicles can eventually develop into nodules or cysts, which can result in
damage to tissue causing scarring.
❑ acne is largely genetic hormonal influenced by the environment
o heat & UV light (sun) exposure skin exposure to greasy or inflammatory materials
mechanical factors (friction from headgear or headbands)
o skin care & cosmetic products: ↑ development of clogged pores & flares of acne blemishes
o acne-prone skin due to → the use of some skin care products or cosmetics→ contain
ingredients that worsen or aggravate acne conditions or cause comedones
o Comedogenic ingredients → agents that can cause or exacerbate follicular hyperkeratosis: thickening of the walls of the follicle due
to retention of keratinocytes➔ comedon formation.
• Comedogenicity→ the tendency of cosmetic products or ingredients to cause or worsen the development of comedones, which can
lead to inflammatory acne lesions→ “acne cosmetica,”.
o other ingredients → causing irritation or inflammation in the follicles➔ sudden flares of papules or pustules → acnegenic reactions.
❖Acnegenic →may not necessarily cause comedones to form
• some surfactants/emulsifiers some fragrances or essential oils extreme pH levels physical/mechanical contact
• Acnegenic reactions occur within a few days of beginning to use a new product.
❑management of acne-prone & clog-prone skin:
• proper management of excess sebum & follicular exfoliation to loosen plugged follicles & prevent further plugging of the
follicles
• the use of products with no non-comedogenic & non-acnegenic ingredients

❑Acne-prone & clog-prone skin can also be affected by aging skin conditions…
• The onset of wrinkles, discolorations, & elastosis associated with aging or photo-aging
▪ Many skin care products intended to help diminish the appearance of aging are also designed for helping dry skin (needs additional
emollient to protect against dehydration & TEWL) → Such materials also ↓ the appearance of wrinkles & the rougher skin texture
associated with dehydrated skin.
However, because of their high emollient content, they can potentially cause problems for those with oily & acne-prone aging skin ➔
should be carefully formulated—avoiding ingredients known to cause clogged follicles & flares of acne blemishes.
❑ Skin creams, foundations, & … formulated with fatty materials: certain oils, FAs, or fatty esters can cause problems in acne-prone &
clog-prone clients
• fatty materials → ↑ hyperkeratosis & plugging of the follicles & non-inflammatory comedones
• →may evolve into flares of inflammatory acne lesions
Oils waxes emollient fatty materials are primarily used in the formulation of a product vehicle➔ used in larger concentrations
& significant portion of the product ➔ comedogenic
✓ Performance-enhancing actives such as peptides, AHAs, sunscreen actives, & antioxidants are rarely comedogenic.

Common Comedogenic Ingredients
HighlyComedogenic(4-5/5 or 5/3)
ModeratelyComedogenic(3-4/5 or 2/3)
MildlyComedogenic(2-3/5 or 1/3)
Non-comedogenic
Acetylated LanolinCoal TarCocoa ButterCoconut OilIsopropyl IsostearateIsopropyl LinoleateIsopropyl MyristateIsopropyl PalmitateIsostearic AcidLanolic AcidLinseed OilMyreth 3MyristateMyristyl MyristateOleic AcidOleth-3Oleyl AlcoholSqualene
Butyl StearateDecyl OleateGrape Seed OilIsostearyl NeopentanoateLauric AcidMink OilMost D & C Red PigmentsMyristyl LactateOctyl PalmitateOctyldodecanolSorbitan OleateSoybean OilTocopherol
Avocado OilCaprylic/Capric TriglyceridesCorn OilEvening Primrose OilGlyceryl StearateHexylene GlycolLanolinLanolin AlcoholLauryl AlcoholMineral OilOlive OilPeanut OilSesame OilSafflower OilStearic AcidSunflower Oil(Please note that mildlycomedogenic
AllantoinBehenic AcidButylene GlycolCarbomerCastor OilCetyl PalmitateCholesterolCyclomethiconeCyclopentasiloxaneDimethiconeGlycerinIron OxidesIsopropyl AlcoholJojoba OilKaolinLecithinOctyldodecyl StearateOctyldodecyl Stearoyl StearateOctinoxateOctisalateOxybenzonePanthenol
ingredients are generally not a problem when used in diluted concentrations.Check to see their ranking of concentration on the ingredientlabel.)
PetrolatumPhenyl TrimethiconePolysorbatesPropylene GlycolPropylene GlycolDicaprate/DicaprylateSD AlcoholSodium HyaluronateSodium PCASorbitolSoya SterolSqualaneTridecyl StearateTridecyl TrimellitateWaterZinc OxideZinc Stearate
• MANAGEMENT OF ACNE-PRONE SKIN
• 1. Sebum/Oiliness Management
• appropriate cleansers to rid the skin of excessive sebum, & help control oiliness & shininess
• surfactant cleansers help to remove excess oil
• Surfactant cleansers are user-friendly & should be developed to rinse easily.
• cleansers with the appropriate amount of surfactant ➔ effectively cleanse the skin without over-drying, or causing irritation from barrier
function disruption.
• Cleansing milks: used for makeup removal, but should be designed to not leave residues of potentially comedogenic fats on the skin.
• Toners: Their main functions: remove residue from the cleanser, & to adjust the pH of the skin surface to 5.5–6.2
• → for acne-prone skin sometimes contain alcohols
➢ but overuse of these can cause dryness & potential irritation that consumers find objectionable, especially when they may be using
drying agents or keratolytics to clear the acne.
• Consumers with oily, clogged, or acne-prone skin generally prefer extremely lightweight moisturizers & sunscreens, foundation, or serums...
➢ Avoidance of oily materials in all wearable products helps to ↓ physical oiliness ՜ ↓ potential comedogenicity.

• 2. Follicular Keratolytics
▪ Follicular keratolytic non-prescription products such as those containing AHAs, salicylic acid, or benzoyl peroxide → help to flush
follicles of debris drying up acne lesions breaking loose existing comedones chemically sloughing the follicles ➔ help
prevent development of new comedones.
• Choice of active agent/ingredients & product type (such as gel, liquid, or lotion) → the severity of the acne condition Aging
changes sensitive skin conditions...
➢ Stronger concentrations of keratolytics & anti-bacterials (such as benzoyl peroxide or salicylic acid) may be needed for more severe
cases.
➢ a vehicle containing a significant amount of SD alcohol may be helpful for → a younger oily skin
➢ a silicone vehicle → would be a better choice for an older, aging, acne-prone skin because it is less likely to dehydrate skin &
accentuate wrinkles or other aging distortions.
➢ 𝛼 & 𝛽 hydroxy acids are a great choice for acne-prone aging skin →help to clear follicles + exfoliate the surface & can
significantly improve the appearance of wrinkles, hyperpigmentation, & texture issues associated with photoaging.
➢ Benzoyl peroxide gel → in teenagers & clients of any age with more inflamed & pustular acne due to its keratolytic & antibacterial -
properties
• 3. Avoidance of Acnegenic & Comedogenic Products
• Vehicle & emollient ingredients are the most likely to cause comedogenicity issues & must be carefully selected.
• The concentration of these ingredients should also be carefully determined since the skin type is already oily.
✓ Most wearable products for this skin type are in lotion or fluid form due to their low emollient or fatty material content.
• Products must be efficacious & meet the beauty needs of the client → They must be practical & of high quality & cosmetic elegance.
• ex, a moisturizer that is documented non-comedogenic is of no value if it is sticky, hard to apply, or pills under makeup → A
product that is easy to use will result in better compliance with the skin care program.
• This will include feel & practicality, ease of application, rinsability of cleansers, & the proper selection of a container that
facilitates easy application of the product.
❖ Compliance with the program will result in better results & consistency in product use.
❖ “program approach” is the best way to successfully improve the skin’s condition → includes using the step-by-step program as
designed by esthetician, avoiding the use of potentially comedogenic products outside the program, & complying with the system
instructions.
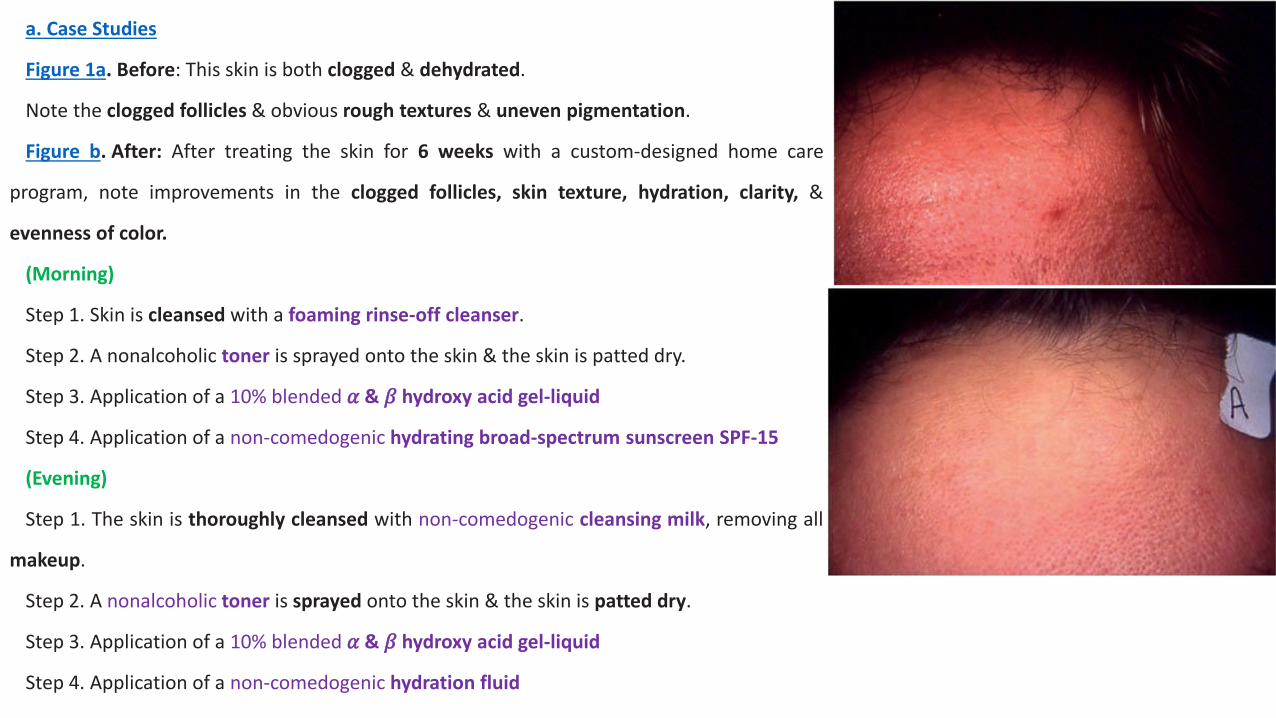
a. Case Studies
Figure 1a. Before: This skin is both clogged & dehydrated.
Note the clogged follicles & obvious rough textures & uneven pigmentation.
Figure b. After: After treating the skin for 6 weeks with a custom-designed home care
program, note improvements in the clogged follicles, skin texture, hydration, clarity, &
evenness of color.
(Morning)
Step 1. Skin is cleansed with a foaming rinse-off cleanser.
Step 2. A nonalcoholic toner is sprayed onto the skin & the skin is patted dry.
Step 3. Application of a 10% blended 𝛼 & 𝛽 hydroxy acid gel-liquid
Step 4. Application of a non-comedogenic hydrating broad-spectrum sunscreen SPF-15
(Evening)
Step 1. The skin is thoroughly cleansed with non-comedogenic cleansing milk, removing all
makeup.
Step 2. A nonalcoholic toner is sprayed onto the skin & the skin is patted dry.
Step 3. Application of a 10% blended 𝛼 & 𝛽 hydroxy acid gel-liquid
Step 4. Application of a non-comedogenic hydration fluid
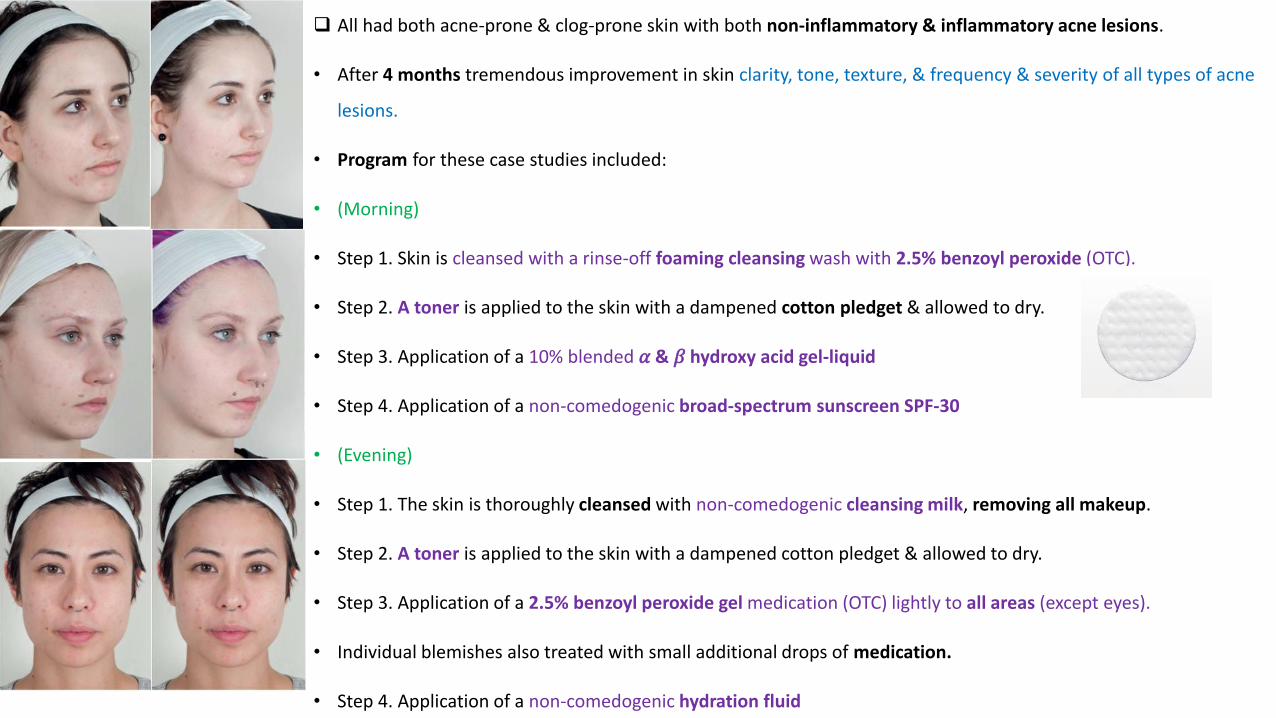
❑ All had both acne-prone & clog-prone skin with both non-inflammatory & inflammatory acne lesions.
• After 4 months tremendous improvement in skin clarity, tone, texture, & frequency & severity of all types of acne
lesions.
• Program for these case studies included:
• (Morning)
• Step 1. Skin is cleansed with a rinse-off foaming cleansing wash with 2.5% benzoyl peroxide (OTC).
• Step 2. A toner is applied to the skin with a dampened cotton pledget & allowed to dry.
• Step 3. Application of a 10% blended 𝛼 & 𝛽 hydroxy acid gel-liquid
• Step 4. Application of a non-comedogenic broad-spectrum sunscreen SPF-30
• (Evening)
• Step 1. The skin is thoroughly cleansed with non-comedogenic cleansing milk, removing all makeup.
• Step 2. A toner is applied to the skin with a dampened cotton pledget & allowed to dry.
• Step 3. Application of a 2.5% benzoyl peroxide gel medication (OTC) lightly to all areas (except eyes).
• Individual blemishes also treated with small additional drops of medication.
• Step 4. Application of a non-comedogenic hydration fluid




















