
Normal versus abnormal genital findings in children: How well do examiners agree?
Upload
independentCategory
view
0download
0
European Journal of Cancer (2012) 48, 1842– 1852
A v a i l a b l e a t w w w . s c i e nc e d i r e c t . c o m
journa l homepage : www.e jcon l ine . com
Sinonasal, genital and acrolentiginous melanomas showdistinct characteristics of KIT expression and mutations
Nicola L. Schoenewolf a, Christian Bull a,f, Benedetta Belloni a,f, David Holzmann b,Sabina Tonolla a, Roland Lang c, Daniela Mihic-Probst d, Christian Andres e,Reinhard Dummer a,⇑
a Department of Dermatology, University Hospital Zurich, Gloriastr. 31, 8091 Zurich, Switzerlandb Department of Otorhinolaryngology, University Hospital Zurich, Frauenklinikstrasse 24, 8091 Zurich, Switzerlandc Department of Dermatology, Paracelsus Private Medical University Salzburg, Mullner-Hauptstr. 48, 5020 Salzburg, Austriad Department of Clinical Pathology, University Hospital Zurich, Schmelzbergstrasse 12, 8091 Zurich, Switzerlande Department of Dermatology, Technische Universitat of Munich, Biedersteiner Str. 29, 80802 Munchen, Germany
Available online 28 March 2012
09
do
⇑
KEYWORDS
KITMucosal melanomaAcrolentiginousmelanomaKIT expressionKIT-targeted therapy
59-8049/$ - see front matter
i:10.1016/j.ejca.2012.02.049
Corresponding author: Tel.:E-mail address: reinhard.du
f Contributed equally to the
� 2012 E
+41 44 2mmer@uwork.
Abstract KIT aberrations predict the outcome of targeted therapies in acrolentiginous(ALM) and mucosal (MM) melanoma patients.KIT immunoreactivity and mutation status was assessed in 41 ALM and 25 MM patients. Ofthese, 19 ALM and 15 MM patients had matched primary and metastatic lesions. P-ERK wasinvestigated in a subset of 9 ALM and 7 MM matched primary/metastatic pairs by immuno-histochemistry.Heterogeneous KIT immunoreactivity was observed in both primary and metastatic lesions.Mutations were present in four of 41 ALM (10%) and five of 25 MM (20%) patients. Onlyvulvar mucosal samples carried KIT mutations in contrast to sinonasal lesions (p = 0.0109).In KIT-mutated tumours, the mutations were present in KIT expressing as well as KITnegative cells, as shown by Laser Capture Microdissection (LCM). P-ERK expression waspreferentially found in metastases.KIT mutations predict treatment outcome with KIT inhibitors. Therefore, especially vulvarmelanoma patients should be screened for activating KIT mutations.� 2012 Elsevier Ltd. All rights reserved.
lsevier Ltd. All rights reserved.
55 1111; fax: +41 44 255 8988.sz.ch (R. Dummer).
1. Introduction
Today, melanoma is subdivided into moleculardefined groups as identified by Bastian and co-workers.1
One major subtype is characterised by an activatingmutation in the BRAF gene, a component of the MAPK

N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852 1843
(mitogen-activated protein kinase) signalling pathway.2
Increased MAPK activation is known to be a major dri-ver of cell growth and proliferation in more than 90% ofmelanomas – mostly occurring on non-chronically sun-damaged skin.2–4 BRAF is less commonly mutated inALM and MM when compared with melanomas arisingfrom non-chronically sun-damaged skin. Indeed, BRAFmutations were identified in 37% of acral melanomasamples tested in the phase II trial of imatinib byCarvajal et al.5 However, according to most recent stud-ies, these subtypes are predominantly showing aberra-tions in the KIT/CD117 gene. At least 31 mutationshave been described for KIT, these occur in exons 9,11, 13, 17 and 18.5–22 The receptor tyrosine kinaseKIT signals among others through the MAPK pathway.The presence of activating mutations in KIT may con-tribute to the activation of this pathway in ALM andMM.12,23,24
Even though several studies have investigated theexpression of KIT in ALM and MM, the particular roleof KIT expression in these melanoma subtypes remainscontroversial.6,8,18,22,25–27 In some studies KIT expres-sion is reported to be lost during melanoma progres-sion.16,28,29 For example, Rivera and co-workersobserved KIT immunoreactivity in epidermal compart-ments of oral mucosal melanomas, but not in the dermalcomponent.16 They suggested KIT expression beingessential mainly during early tumour growth. Otherstudies report increased KIT expression in metastasescompared to primary tumours.6,18,27
Phase II clinical trials using KIT targeting drugs suchas imatinib (GLEEVEC�, Novartis, Basel, Switzerland)failed in a patient population selected by KIT expressiononly.30 More recently, ALM and MM cases respondingto imatinib treatment have been reported.5,10,17,31,32
In these cases, activating KIT mutations weredetected.5,10,12,15,17,19,30–36
In order to explore the relationship between KITexpression, mutation, and tumour stages, we investi-gated immunohistochemical KIT expression and muta-tion status in primary ALM/MM lesions and theirmetastases. We also compared the frequency of KIT
mutations of MM in different anatomic locations asreported by Omholt et al.26
2. Material and methods
2.1. Patient tissue selection
Tumour tissues of 41 patients with ALM and 25 withMM were identified. 35 ALM and 21 MM primarytumours, 24 ALM and 15 MM lymphnode (stage III)metastases, as well as 9 ALM and 7 MM distant metas-tases (stage IV) were available. 19 ALM and 15 MMpatients had matched primary and metastatic lesions.Stages I, III and IV were applied according to AJCC
(American Joint Committee on Cancer)37 and theextended version for head and neck mucosal mela-noma.38 The study was approved by the local IRB(EK647 and EK800) at Kantonale Ethikkommission,Sonneggstr. 12, 8091 Zurich, Switzerland.
2.2. Immunohistochemical detection of KIT and p-ERK
Paraffin-embedded tissues of primary (35 ALM, 21MM) and metastatic (33 ALM, 22 MM) lesions weresectioned and stained with polyclonal rabbit anti-humanKIT/CD117 antibody (dilution1:500, DakoCytomation,Carpinteria, California, USA). For detection, the DakoREAL Detection System was used (Dako Cytomation)and counter-staining was performed with haematoxylin.Interstitial mast cell staining served as internal positivecontrol for KIT/CD117. Matched primary/metastaticlesion-pairs of nine ALM and seven MM patients werealso stained for anti-p-ERK (pP42/44) (dilution 1:100,Cellsignaling Technology, Danvers, Massachusetts,USA). Detection was conducted using the ABC complexsystem (Vector Laboratories, Burlingame, California,USA), and counter-staining was performed withhaematoxylin.
KIT and p-ERK immunoreactivity was assessedsemi-quantitatively by two independent investigatorsas follows: 0 (up to 5% of cells stained), 1 (5–25%), 2(25–50%), 3 (50–75%), 4 (75–100%). Staining intensitywas distinguished as weak (+), moderate (++) andstrong (+++) (Figs. 1 and 2).
2.3. Laser capture microdissection (LCM)
KIT/CD117-stained master slides of five patientswith known KIT mutations were chosen for laser cap-ture microdissection. Serial sections of 5 lm were cutand placed on membrane slides (Part-Nr: 50103, Molec-ular Machines & Industries, Glattbrugg, Switzerland)and deparaffinised shortly before LCM. These slideswere not stained for KIT (Fig. 3).
Three reference points were set on the master slideand subsequently assigned to the serial slides on themembrane. Areas with cells positively stained for KITas well as KIT negative cells were chosen according tothe master slide, marked and subsequently cut by thelaser (CellCutPlus-System, MMI - connected to aIX81-Olympus microscope, Hamburg, Germany).DNA was extracted by proteinase K digestion over48 h at 55 �C.
2.4. PCR and Sequencing
PCR was performed for KIT gene exons 9,11,13,17and 18 using the Expand High Fidelity PCR System(Roche, Basel, Switzerland). Primers (Microsynth, Balg-ach, Switzerland) and cycle conditions were chosen

Fig. 1. Primary and metastatic lesions of one ALM patient (case 7, Table 2). There is strong and widespread KIT (primary: 3++; stage IIImetastasis: 3++, stage IV metastasis: 2++) and p-ERK (primary: 3+++, stage III metastasis: 4+++, stage IV metastasis:2+++) expression in alllesions of this patient. Scale bar = 50, 31 lm.
1844 N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852
according to Curtin et al. and Tarn et al.9,39: KIT exon9: fwd 50-CCTAGAGTAAGCCAGGGCTTT-3’, bwd:50-GACAGAGCCTAAACATCCCCT-30, KIT exon11: fwd: 50-CTCTCCAGAGTGCTCTAATGA-30, bwd:50-AAGGAAGCCACTGGAGTTCCT-30, KIT exon13: fwd: 50-CTGCATGCGCTTGACATCAGT-30, bwd:50-AGGCAGCTTGGACACGGCTT-30, KIT exon 17:fwd: 50-GGTTTTCTTTTCTCCTCCAACC-30, bwd: 50-GCAGGACTGTCAAGCAGAGGA-30, KIT exon 18:fwd: 50-CATTTCAGCAACAGCAGCAT-30, bwd:50-CAAGGAAGCAGGACACCAAT-30.
Sequencing was performed by Microsynth (Balgach,Switzerland). Data were analysed using Chromas Lite(version 2.01, Technelysium Pty Ltd, Tewantin, Austra-lia) and BLAST (National Center for BiotechnologyInformation, National Library of Medicine, Bethesda,USA).
Amino acid changes were defined as mutationswhereas single nucleotide polymorphisms (SNPs) were
neglected as silent mutations (Table 1 (cases 13 and37) and Table 2 (case 31)).
2.5. Statistical methods
Fisher’s exact test was used to compare frequencies ofmutation in mucosal melanomas from different anatom-ical locations.
The correlation between KIT staining intensity anddistribution was performed according to Spearman. TheKruskall–Wallis-Test was applied in order to comparemelanoma groups and stages to the KIT expression levels.
3. Results
3.1. KIT expression in ALM and MM lesions
In ALM, heterogenous KIT immunoreactivity (>5%of melanoma cells) was detected in 21 of 35 (60%)

Fig. 2. KIT expression in the primary and metastatic tumour tissues of one vulvar melanoma patient. The primary mucosal melanoma lesion of thevulva and the corresponding metastases show strong KIT expression. Red coloured membranes correspond to KIT expression. The primary andthe stage IV metastasis (scapula) show intense (+++) and widespread (grade 3–4) distribution of KIT. The corresponding stage III metastasis(inguinal) shows less intense (++), but still widespread (grade 4) distribution of KIT. Scale bar = 50, 31 lm.
Fig. 3. Example for laser capture microdissected KIT negative (top left) versus KIT positive (right top) cell areas. Upon laser capturemicrodissection, KIT negative and KIT positive cell populations are subjected to PCR for particular KIT mutations (here shown as representativefor mutation L576P, exon 11). Sequencing of PCR products from both cell populations results in an amino acid exchange (bottom middle):CTT > CCT (L576P).
N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852 1845

Table 1Clinical, immunohistochemical and KIT mutation data of all sinonasal and genital melanoma patients.
Casenumber
Melanomasubtype
Sex and ageat diagnosis
Targetedtherapy
KIT mutationstatus
Primary Metastasis III Metastasis IV
KIT p-ERK KIT p-ERK KIT p-ERK
1 Vulvovaginal Female (79) No x 0 x x x x x2 Vulvovaginal Female (57) No wt 0 x x x x x3 Vulvovaginal Female (75) Imatinib K642E 4+++ 0 2+++ 0 3+++ 0
4 Vulvovaginal Female (59) Imatinib L576P 0 0 0 0 x x
5 Vulvovaginal Female (60) No wt x x x x x x6 Vulvovaginal Female (78) No L576P 2+ 0 1+ 0 x x
7 Vulvovaginal Female (43) No x x x x x x x8 Vulvovaginal Female (50) No wt 0 x x x x x9 Vulvovaginal Female (76) No x x x x x x x
10 Vulvovaginal Female (63) No wt x x x x x x11 Vulvovaginal Female (x) x L641H 0 1+++ x x x x12 Vulvovaginal Female (x) x V560D 1++ x 3++ x x x13 Vulvovaginal Female (51) No L862L (SNP) 0 x x x 0 x14 Vulvovaginal Female (56) No x x x x x x x15 Vulvovaginal Female (48) No wt x x x x x x16 Vulvovaginal Female (72) No x x x x x x x17 Anal Male (59) Imatinib wt 0 0 0 3+++ 0 1+++
18 Anal Female (63) No wt x x x x x x19 Sinonasal Female (67) No wt 0 x 0 x x x20 Sinonasal Female (51) No wt 0 x 0 x x x21 Sinonasal Male (52) No wt x x 0 x 0 x22 Sinonasal Female (92) No wt 2+ 2++ 0 1++ 0 2+
23 Sinonasal Female (73) No x x x x x x x24 Sinonasal Female (81) No wt 0 x x x x x25 Sinonasal Female (68) No wt 0 x 0 x x x26 Sinonasal Male (73) No wt 0 x 0 x x x27 Sinonasal Female (76) No wt x x 0 x x x28 Sinonasal Male (50) No wt 0 x x x x x29 Sinonasal Male (72) No x x x x x x x30 Sinonasal Female (x) No x x x x x x x31 Sinonasal Male (48) No x x x x x x x32 Sinonasal Male (39) No x x x x x x x33 Sinonasal Male (78) No x 1++ 1+ x x 1+ 0
34 Sinonasal Female (77) No x 0 x 0 x x x35 Sinonasal Female (49) No wt 0 1+ x x 0 1+++
36 Sinonasal Female (71) No wt x x x x x x37 Sinonasal x x L862L (SNP) 1+++ x 0 x x x
x = Not available due to low/bad material quality/unknown clinical follow-up. wt = Wildtype.Bold: matching pairs with both, KIT and p-ERK expression.Staining intensity: + = weak, ++ = moderate, +++ = strong; <5% stained tumor cells = 0, 5–25% = 1, 25–50% = 2, 50–75% = 3, 75–100% = 4.
1846 N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852
primary lesions, 8 of 24 (33%) stage III metastases and 3of 9 (33%) stage IV metastases (Fig. 4, Table 3). Therewas a clear correlation between the percentage of KIT-positive cells and staining intensity (p < 0.001) (Table 3).KIT expression did not correlate with ALM stage(p = 0.08) (Table 3).
In MM, KIT was expressed in 6 of 21 (29%) primarylesions, 3 of 15 (20%) stage III metastases and 2 of 7(29%) stage IV metastases (Fig. 4, Table 3). Again, aclear correlation between the percentage of KIT-positivecells and staining intensity was observed (p < 0.01)(Table 3). KIT expression did not correlate with MMstage (p = 0.8593) (Table 3).
3 of 9 vulvovaginal MM (33%) expressed KIT in pri-mary lesions, 3 of 4 vulvovaginal MM (75%) in stage IIImetastases and 1 of 2 vulvovaginal MM (50%) in stage
IV metastases. Sinonasal/anal subgroup (MM) lesionsshowed KIT expression in 3 of 12 (25%) primary lesions,0 of 11 (0%) stage III metastases and 1 of 5 (20%) stageIV metastases. There were no significant differencesbetween these two mucosal melanoma subgroups withregard to the KIT expression levels (p = 0.5025)(Table 3).
In patients with matched primary/metastasistumour samples, 5 of 19 (26.3%) ALM and 4 of 15(27%) MM cases showed KIT immunoreactivity(>5% of melanoma cells) in both primary and meta-static lesions. 10 of 19 (52.6%) ALM and 9 of 15(60%) MM sample pairs were KIT negative for bothprimary and metastatic lesions. 90% of these KIT neg-ative MM pairs were derived from the sinonasal/analsubgroup (Tables 1 and 2).

Table 2Clinical, immunohistochemical and KIT mutation data of all acrolentiginous melanoma patients.
Casenumber
Melanomasubtype
Sex and ageat diagnosis
Targetedtherapy
KITmutationstatus
Primary Metastasis III Metastasis IV
KIT p-ERK KIT p-ERK KIT p-ERK
1 Plantar right foot Female (52) No wt 3+++ 0 1+ 4+++ 2+ 3++
2 Plantar right foot Female (73) x wt 2+ x x x x x3 Plantar right foot Male (58) No wt x x x x x x4 Plantar right foot Male (64) x wt 0 x 0 x x x5 Plantar right foot Female (67) No x x x 0 x x x6 Plantar right foot Male (74) No x 2+++ x x x x x7 Plantar right foot heel Male (62) Imatinib wt 3++ 3+++ 3++ 4+++ 2++ 2+++
8 Plantar right foot heel Female (80) x x 0 x x x x x9 Plantar right foot heel Female (70) No L576P 2++ 0 0 0 x x
10 Plantar right foot heel Female (66) No wt x x x x x x11 Plantar right foot heel Female (82) No wt x x x x x x12 Plantar right foot heel Male (64) No wt 0 x 0 x x x13 Right foot Dig I Male (68) No wt 3+ x x x x x14 Right foot Dig I (nail) Female (55) No K642E x x 4++ x x x15 Right foot Dig I (nail) Male (49) No T632I 0 x 0 3+++ 0 2++
16 Right foot Dig I (nail) Male (46) No wt 1+++ x x x x x17 Right foot Dig I (nail) Male (59) x x x x x x 0 x18 Right foot Dig I (nail),
amelanotic
Male (63) Nilotinib wt 0 1++ 0 1+ x x
19 Any Dig right foot (IV) Male (67) No wt 1++ x 1+ x x x20 Right foot Dig II Female (40) No wt x x 0 x 0 x21 Right foot Dig II (nail) Female (73) Sorafenib(+DTIC) wt 1++ 0 0 x 0 x22 Interdigital III-IV right
footMale (50) No x 0 x x x x x
23 Any localisation rightfoot (back of the foot)
Male (25) CRAF 265A,sorafenib(+Taxol)
x x x x x x x
24 Border of right lateralfoot
Male (65) No wt x x x x x x
25 Right foot Female (65) x wt 2+++ x 3+++ x x x26 Forefoot right Female (37) No wt x x x x x x27 Plantar left foot Male (57) x wt 0 1+++ 0 1++ x x
28 Plantar left foot Female (61) No wt 0 x 0 x x x29 Left plantar foot Male (68) x wt x x x x x x30 Left plantar foot Male (55) No wt 3++ x 0 x x x31 Left plantar foot Female (65) x L862L (SNP) 2++ x x x x x32 Left plantar foot Male (78) No wt x x x x x x33 Left plantar foot, Dig IV Female (64) No L576P 1++ x x x x x34 Left foot Dig I Female (71) x wt 2+++ 0 0 3+++ 0 0
35 Left foot Dig I Male (51) No wt x x 1+ x x x36 Left foot Dig I Female (67) No wt 1+ x x x 0 x37 Dig II left foot Female (54) No wt x x 1+ x 1+ x38 Dig II left foot Male (42) No wt 0 x x x x x39 Left back of the foot,
distal btw II and Dig IVMale (30) x wt 2++ x x x x x
40 Left foot heel Male (64) No wt 0 0 0 0 x x
41 Left foot heel Female (29) No wt 3+ x x x x x42 Left foot ball Male (64) x wt 0 x x x x x43 Left hand Dig I Male (52) No wt 0 0 0 1++ x x
44 Left hand Dig I (nail) Male (46) No x 2++ x 1+ x x x45 Left hand Dig I Female (63) No wt 2++ x x x x x46 Left hand Dig I
(articulatio)Male (65) x x 0 x x x x x
47 Left hand Dig I (nail) Female (31) No wt x x 0 x x x48 Left hand Dig III (nail) Female (27) No wt 1+ x x x x x49 Left hand Dig II (nail) Male (61) No wt 0 x 0 x x x50 Left hand Dig II Female (59) No x 1+ x x x x x
x=Not available due to low/bad material quality/unknown clinical follow-up.wt=Wildtype.Bold: matching pairs with both, KIT and p-ERK expression.Staining intensity: +=weak, ++=moderate, +++=strong; <5% stained tumor cells=0, 5–25%=1, 25–50%=2, 50–75%=3, 75–100%=4.
N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852 1847
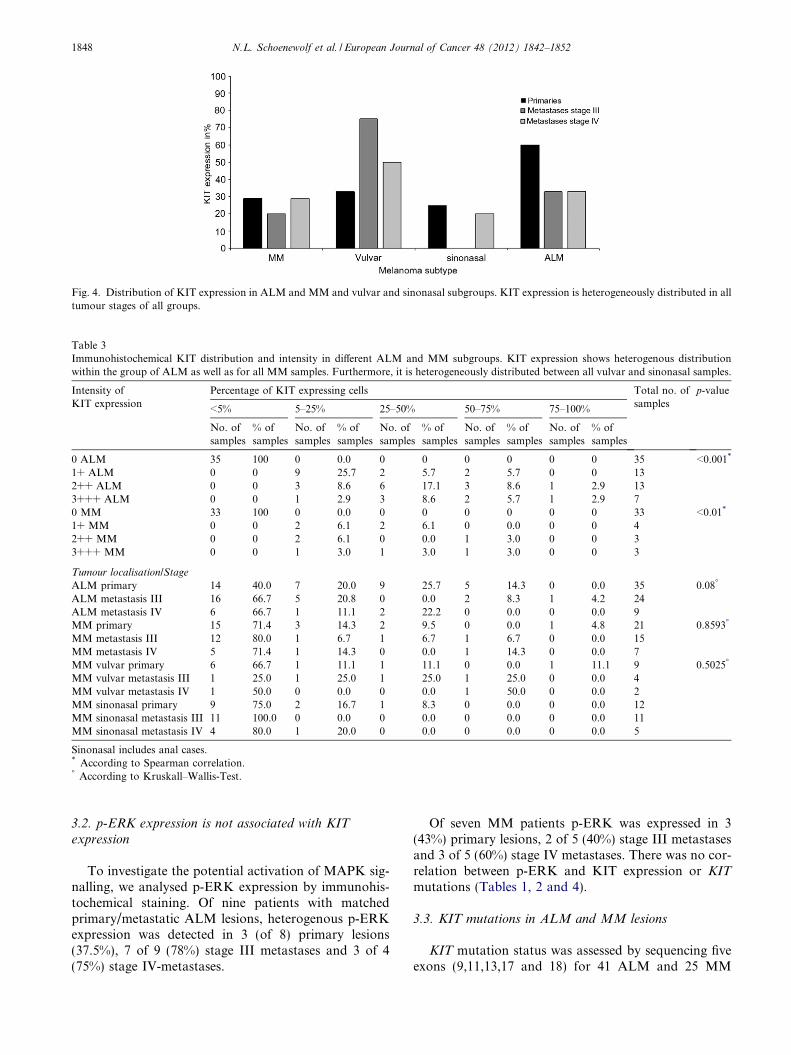
Fig. 4. Distribution of KIT expression in ALM and MM and vulvar and sinonasal subgroups. KIT expression is heterogeneously distributed in alltumour stages of all groups.
Table 3Immunohistochemical KIT distribution and intensity in different ALM and MM subgroups. KIT expression shows heterogenous distributionwithin the group of ALM as well as for all MM samples. Furthermore, it is heterogeneously distributed between all vulvar and sinonasal samples.
Intensity ofKIT expression
Percentage of KIT expressing cells Total no. ofsamples
p-value
<5% 5–25% 25–50% 50–75% 75–100%
No. ofsamples
% ofsamples
No. ofsamples
% ofsamples
No. ofsamples
% ofsamples
No. ofsamples
% ofsamples
No. ofsamples
% ofsamples
0 ALM 35 100 0 0.0 0 0 0 0 0 0 35 <0.001*
1+ ALM 0 0 9 25.7 2 5.7 2 5.7 0 0 132++ ALM 0 0 3 8.6 6 17.1 3 8.6 1 2.9 133+++ ALM 0 0 1 2.9 3 8.6 2 5.7 1 2.9 70 MM 33 100 0 0.0 0 0 0 0 0 0 33 <0.01*
1+ MM 0 0 2 6.1 2 6.1 0 0.0 0 0 42++ MM 0 0 2 6.1 0 0.0 1 3.0 0 0 33+++ MM 0 0 1 3.0 1 3.0 1 3.0 0 0 3
Tumour localisation/Stage
ALM primary 14 40.0 7 20.0 9 25.7 5 14.3 0 0.0 35 0.08�
ALM metastasis III 16 66.7 5 20.8 0 0.0 2 8.3 1 4.2 24ALM metastasis IV 6 66.7 1 11.1 2 22.2 0 0.0 0 0.0 9MM primary 15 71.4 3 14.3 2 9.5 0 0.0 1 4.8 21 0.8593�
MM metastasis III 12 80.0 1 6.7 1 6.7 1 6.7 0 0.0 15MM metastasis IV 5 71.4 1 14.3 0 0.0 1 14.3 0 0.0 7MM vulvar primary 6 66.7 1 11.1 1 11.1 0 0.0 1 11.1 9 0.5025�
MM vulvar metastasis III 1 25.0 1 25.0 1 25.0 1 25.0 0 0.0 4MM vulvar metastasis IV 1 50.0 0 0.0 0 0.0 1 50.0 0 0.0 2MM sinonasal primary 9 75.0 2 16.7 1 8.3 0 0.0 0 0.0 12MM sinonasal metastasis III 11 100.0 0 0.0 0 0.0 0 0.0 0 0.0 11MM sinonasal metastasis IV 4 80.0 1 20.0 0 0.0 0 0.0 0 0.0 5
Sinonasal includes anal cases.* According to Spearman correlation.� According to Kruskall–Wallis-Test.
1848 N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852
3.2. p-ERK expression is not associated with KIT
expression
To investigate the potential activation of MAPK sig-nalling, we analysed p-ERK expression by immunohis-tochemical staining. Of nine patients with matchedprimary/metastatic ALM lesions, heterogenous p-ERKexpression was detected in 3 (of 8) primary lesions(37.5%), 7 of 9 (78%) stage III metastases and 3 of 4(75%) stage IV-metastases.
Of seven MM patients p-ERK was expressed in 3(43%) primary lesions, 2 of 5 (40%) stage III metastasesand 3 of 5 (60%) stage IV metastases. There was no cor-relation between p-ERK and KIT expression or KIT
mutations (Tables 1, 2 and 4).
3.3. KIT mutations in ALM and MM lesions
KIT mutation status was assessed by sequencing fiveexons (9,11,13,17 and 18) for 41 ALM and 25 MM

Table 4KIT and p-ERK expression for nine matching ALM and seven MM sample pairs.
Case number Melanoma subtype KIT mutationstatus
KIT expression primary tumor/metastasis III/metastasis IV
p-ERK expression primary tumor/metastasis III/metastasis IV
1 Plantar right foot wt 3+++;1+;2+ 0;4+++;3++7 Plantar right foot heel wt 3++;3++;2++ 3+++;4+++;2+++9 Plantar right foot heel L576P 2++;0;x 0;0;x
15 Right foot Dig I (nail) T632I 0;0;0 x;3+++; 2++18 Right foot Dig I (nail), amelanotic wt 0;0;x 1++;1+;x21 Right foot Dig II (nail) wt 1++;0;0 0;x;x27 Plantar left foot wt 0;0;x 1+++;1++;x34 Left foot Dig I wt 2+++;0;0 0;3+++;040 Left foot heel wt 0;0;x 0 ;0;x43 Left hand Dig I wt 0;0;x 0;1++;x3 Vulvovaginal K642E 4+++;2+++;3+++ 0;0;04 Vulvovaginal L576P 0;0;x 0;0;x6 Vulvovaginal L576P 2+;1+;x 0;0;x
17 Anal wt 0;0;0 0;3+++;1+++22 Sinonasal wt 2+;0;0 2++;1++;2+33 Sinonasal x 1++;x;1+ 1+;x;035 Sinonasal wt 0;x;0 1+;x;1+++
N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852 1849
patient samples. In thirteen cases, multiple lesions of onepatient were analysed. The mutations identified includedV560D (1 MM sample) and L576P (2 MM and 2 ALMsamples) in exon 11 and T632I (1 ALM sample), L641H(1 MM sample) and K642E (1 MM and 1 ALM sam-ples) in exon 13 (Tables 1 and 2). T632I and L641H havenot been previously reported in mucosal or acrolentigi-nous melanomas. Of 11 vulvovaginal lesions, five(45%) had KIT mutations in either exons 11 or 13.Twelve tested sinonasal lesions and two anal lesionsdid not show mutations in KIT. This results in a statis-tically different mutation frequency (p = 0.0109). Thegenetic KIT status was consistent in all matchedsamples.
3.4. KIT mutations occur in KIT negative and KIT
positive melanoma cells
Among tumours with activating KIT mutations,lesions from three ALM patients and three MMpatients showed positive KIT expression (Tables 1and 2).
LCM revealed the presence of KIT mutations in bothKIT expressing and KIT negative tumour cells in fivepatient lesions with KIT mutations (Fig. 3).
4. Discussion
KIT/CD117 is a 148kD surface molecule involved inthe melanocytic development, migration and prolifera-tion. There are no large studies on KIT expression inpatient-matched primary/metastasis pairs in MM andALM. Our results show that KIT immunoreactivity israndomly present in early and late phases of disease.However, a KIT negative primary lesion results inKIT negative metastases.
In order to illuminate the potential impact of KITexpression on p-ERK expression,26,40 we studied ERKphosphorylation in seven MM and nine ALM patient-matched pairs of primary and metastatic lesions. Therewas no correlation between KIT and p-ERK expressionsuggesting the involvement of other KIT independentpathways such as the PI3K kinase pathway. Interest-ingly, KIT-wildtype tumours predominantly were lack-ing KIT expression, but presenting positive p-ERKstaining.
Despite the low sample number, this finding impliesalternative pathways to achieve p-ERK activation,especially in the advanced stages. This was also sug-gested by Hofman et al.25 They analysed the mutationstatus and expression intensity of KIT in uveal mela-noma patients. Eventually, they detected and increasedfrequency of p-ERK expression in advanced stages.Thus they suggested alternative activation of theMAPK pathway to be involved during tumorprogression.25
Careful investigations of KIT immunoreactivity inKIT mutated cases failed to show a convincing associa-tion between KIT expression intensity and KIT muta-tion status.22,26 We performed laser capturemicrodissection of distinct KIT positive versus KIT neg-ative tumour areas. The mutation analysis revealed thepresence of mutations in all areas confirming for the firsttime the clear independence of KIT mutations and KITexpression. Since KIT immunoreactivity is independentof KIT mutation in our study, we conclude that immu-nohistochemistry is not a reliable screening tool formutations in ALM/MM patients.
Five out of 11 vulvovaginal lesions, had KIT muta-tions in either exons 11 or 13. Twelve tested sinonasallesions and two anal lesions did not show mutations inKIT. This resulted in a statistically significant mutationfrequency (p = 0.0109).

Table 5Systematic investigation of the mutation frequency in ALM and MM at specified locations.
Published by Acrolentiginous melanoma Vulvovaginal melanoma Sinonasal melanoma Anal melanoma
Beadling et al., 20088
Carvajal et al., 20115
Omholt et al., 201126
8.33% (3/36*)43% (3/7)7% (1/14)
Satzger et al., 200818
Handolias et al., 201031
Abysheva et al., 201141
Omholt et al., 201126
Carvajal et al., 20115
33% (3/9)29% (2/7)7% (1/15)35% (8/23)62% (8/13)
Antonescu et al., 20076
Beadling et al., 20088
Satzger et al., 200818
Handolias et al., 201031
Abysheva et al., 201141
Omholt et al., 201126
Carvajal et al., 20115
15% (3/20)44% (4/9�)13% (1/8)67% (4/6)25% (6/24)9% (2/22)50% (6/12)
Curtin et al., 20069
Kong et al., 201122
Carvajal et al., 20115
30% (3/10)11.9% (23/193)21.4% (18/84)
This study 10% (4/41) 45% (5/11) 0% (0/ 12) 0% (0/2)
Total mutation frequency 15% (48/328) 35% (27/78) 10% (7/69) 25% (26/103)
* This collective consisted of 29 sinonasally and 7 orally located tumours. The mutation frequency was not directly shown for the anatomiclocation.� Including vulvovaginal cases.
1850 N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852
In light of the recent data of Omholt et al., supportedby data of Abysheva et al.41 the KIT mutation frequencyin mucosal melanoma depends on the anatomic locationof the primary tumour.26 While genital melanomas showa mutation rate of approximately 30%, sinonasal lesionspresent a very low mutation rate. It is important to notethat data are especially rare for sinonasal melanoma (seeTable 5 for an overview). To our knowledge, only onereport exists on sinonasal melanoma.36 According toour findings, the frequency of KIT mutations variesdepending on the location of mucosal melanomas.10,17,31
The melanocyte population in the genital area and thesinus might derive from different neural crestcompartments.
Melanocyte classification distinguishes between non-classical and classical melanocyte subtypes (LionelLarue, personal communication). However, while allmelanocytes residing in mucosal membranes are gener-ally considered non-classical, there may yet be anotherlayer of sub classification which could explain the differ-ences observed between specific groups of mucosalmelanomas.
We found consistent KIT mutation status betweenpatient-matched primary and metastatic lesions. How-ever there is evidence to suggest that if KIT mutationsare not found, amplification analysis of the KIT geneshould be considered.6,9,22,42 Jiang and co-workers haveconfirmed the relevance of KIT amplification in additionto mutant KIT in this context.12 They suggested a posi-tive selection for mutant KIT in case of KIT amplifica-tion and thus allowing higher sensitivity towardstargeted therapy. The outcome of a phase II study by
Guo et al. showed that particularly KIT mutations inexons 11 and 13, not necessarily in conjunction withamplifications, show a high sensitivity towards imatinibtreatment.32 The recent study published by Carvajalet al. did not show a significant difference between imati-nib responding patients that showed KIT mutations andaberrations and those only carrying KIT mutations5
Similar to several reported cases, our patientsresponding to imatinib treatment carried activatingKIT mutations.6,17,27,43 It is convincing that the presenceof KIT activating mutations is essential for treatmentresponse to KIT-targeting therapies. Despite an abstractby Zhu et al., reporting on KIT mutated sinonasal mel-anoma, only few KIT mutations occur in sinonasal/analmelanomas in contrast to vulvar melanomas26 and(Table 5). The search for patients in ongoing trialsshould thus focus on vulvar melanomas.
In conclusion, KIT expression is heterogeneous andshows no relationship with disease progression. There-fore KIT immunoreactivity is not a valuable markerfor treatment decisions. In mucosal melanoma patients,KIT mutation frequency is significantly associated withanatomic location. Vulvar melanoma patients are proneto carry activating KIT mutations and thus may be morelikely to benefit from KIT-targeted therapy than othersubtypes.
Conflict of interest statement
There is a possible conflict of interest for the follow-ing authors: Nicola Schoenewolf and Reinhard Dum-mer, as this project was partly financially supported by

N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852 1851
Novartis Pharmaceuticals. All other authors declare noconflict of interest.
Acknowledgements
This work was supported by Novartis Pharmaceuti-cals and in part by the Gottfried und Julia Bangerter-Rhyner-Stiftung and the G+B Schwyzer Stiftung. B.Belloni was supported by the MSD scholarship grantfor oncologic research.
Many thanks for lab support from Marie-ThereseAbdou, Ines Kleiber, Martina Storz, Christa Dudliand team. Ludmila Merker and Antje Schlutter fromMMI were very dedicated to train us for laser capturemicrodissection. With regard to contents, we thankKeith Hoek and Prof. Helmut Kerl for their critical pa-per revision. Daniel Widmer was a big help sharing hisstatistical knowledge.
References
1. Curtin JA, Fridlyand J, Kageshita T, et al. Distinct sets of geneticalterations in melanoma. The New England journal of medicine
2005;353(20):2135–47.2. Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene
in human cancer. Nature 2002;417(6892):949–54.3. Cohen C, Zavala-Pompa A, Sequeira JH, et al. Mitogen-actived
protein kinase activation is an early event in melanoma progres-sion. Clin Cancer Res. 2002;8(12):3728–33.
4. Gray-Schopfer V, Wellbrock C, Marais R. Melanoma biology andnew targeted therapy. Nature. 2007;445(7130):851–7.
5. Carvajal RD, Antonescu CR, Wolchok JD, et al. KIT as aTherapeutic Target in Metastatic Melanoma. JAMA
2011;305(22):2327–34.6. Antonescu CR, Busam KJ, Francone TD, et al. L576P KIT
mutation in anal melanomas correlates with KIT protein expres-sion and is sensitive to specific kinase inhibition. Int J Cancer.
2007;121(2):257–64.7. Ashida A, Takata M, Murata H, et al. Pathological activation of
KIT in metastatic tumors of acral and mucosal melanomas. Int J
Cancer. 2009;124(4):862–8.8. Beadling C, Jacobson-Dunlop E, Hodi FS, et al. KIT gene
mutations and copy number in melanoma subtypes. Clin Cancer
Res. 2008;14(21):6821–8.9. Curtin JA, Busam K, Pinkel D, Bastian BC. Somatic activation of
KIT in distinct subtypes of melanoma. J Clin Oncol.
2006;24(26):4340–6.10. Hodi FS, Friedlander P, Corless CL, Heinrich MC. Mac Rae S,
Kruse A, et al. Major response to imatinib mesylate in KIT-mutated melanoma. J Clin Oncol. 2008;26(12):2046–51.
11. Holden JA, Willmore-Payne C, Layfield LJ. Tyrosine kinaseactivating mutations in human malignancies: implications fordiagnostic pathology. Experimental and molecular pathology.
2008;85(1):68–75.12. Jiang X, Zhou J, Yuen NK, et al. Imatinib targeting of KIT-
mutant oncoprotein in melanoma. Clin Cancer Res. 2008;14(23):7726–32.
13. Lutzky J, Bauer J, Bastian BC. Dose-dependent, completeresponse to imatinib of a metastatic mucosal melanoma with aK642E KIT mutation. Pigment cell & melanoma research.
2008;21(4):492–3.14. McLean SR, Gana-Weisz M, Hartzoulakis B, et al. Imatinib
binding and cKIT inhibition is abrogated by the cKIT kinase
domain I missense mutation Val654Ala. Mol Cancer Ther.
2005;4(12):2008–15.15. Quintas-Cardama A, Lazar AJ, Woodman SE, et al. Complete
response of stage IV anal mucosal melanoma expressing KITVal560Asp to the multikinase inhibitor sorafenib. Nat Clin Pract
Oncol. 2008;5(12):737–40.16. Rivera RS, Nagatsuka H, Gunduz M, et al. C-kit protein
expression correlated with activating mutations in KIT gene inoral mucosal melanoma. Virchows Archiv : an international journal
of pathology. 2008;452(1):27–32.17. Satzger I, Kuttler U, Volker B, et al. Anal mucosal melanoma with
KIT-activating mutation and response to imatinib therapy–casereport and review of the literature. Dermatology. 2010;220(1):77–81.
18. Satzger I, Schaefer T, Kuettler U, et al. Analysis of c-KITexpression and KIT gene mutation in human mucosal melanomas.Br J Cancer. 2008;99(12):2065–9.
19. Terheyden P, Houben R, Pajouh P, et al. Response to imatinibmesylate depends on the presence of the V559A-mutated KIToncogene. J Invest Dermatol. 2010;130(1):314–6.
20. Willmore-Payne C, Holden JA, Hirschowitz S, Layfield LJ. BRAFand c-kit gene copy number in mutation-positive malignantmelanoma. Human pathology. 2006;37(5):520–7.
21. Willmore-Payne C, Holden JA, Tripp S, Layfield LJ. Humanmalignant melanoma: detection of BRAF- and c-kit-activatingmutations by high-resolution amplicon melting analysis. Human
pathology. 2005;36(5):486–93.22. Kong Y, Si L, Zhu Y, et al. Large-scale analysis of KIT
aberrations in Chinese patients with melanoma. Clin Cancer Res.
2011;17(7):1684–91.23. Lennartsson J, Jelacic T, Linnekin D, Shivakrupa R. Normal and
oncogenic forms of the receptor tyrosine kinase kit. Stem Cells.
2005;23(1):16–43.24. Thommes K, Lennartsson J, Carlberg M, Ronnstrand L. Identi-
fication of Tyr-703 and Tyr-936 as the primary association sites forGrb2 and Grb7 in the c-Kit/stem cell factor receptor. The
Biochemical journal. 1999;341(Pt 1):211–6.25. Hofmann UB, Kauczok-Vetter CS, Houben R, Becker JC.
Overexpression of the KIT/SCF in uveal melanoma does nottranslate into clinical efficacy of imatinib mesylate. Clin Cancer
Res. 2009;15(1):324–9.26. Omholt K, Grafstrom E, Kanter-Lewensohn L, Hansson J,
Ragnarsson-Olding BK. KIT Pathway Alterations in MucosalMelanomas of the Vulva and Other Sites. Clin Cancer Res.
2011;17(12):3933–42.27. Torres-Cabala CA, Wang WL, Trent J, et al. Correlation between
KIT expression and KIT mutation in melanoma: a study of 173cases with emphasis on the acral-lentiginous/mucosal type. Mod-
ern pathology : an official journal of the United States and Canadian
Academy of Pathology, Inc. 2009;22(11):1446–56.28. Montone KT, van Belle P, Elenitsas R, Elder DE. Proto-oncogene c-
kit expression in malignant melanoma: protein loss with tumorprogression. Modern pathology : an official journal of the United
States and Canadian Academy of Pathology, Inc. 1997;10(9):939–44.29. Shen SS, Zhang PS, Eton O, Prieto VG. Analysis of protein
tyrosine kinase expression in melanocytic lesions by tissue array.Journal of cutaneous pathology. 2003;30(9):539–47.
30. Kim KB, Eton O, Davis DW, et al. Phase II trial of imatinibmesylate in patients with metastatic melanoma. Br J Cancer.
2008;99(5):734–40.31. Handolias D, Hamilton AL, Salemi R, et al. Clinical responses
observed with imatinib or sorafenib in melanoma patientsexpressing mutations in KIT. Br J Cancer. 2010;102(8):1219–23.
32. Guo J, Si L, Kong Y, et al. Phase II, open-label, single-arm trial ofimatinib mesylate in patients with metastatic melanoma harboring c-Kit mutation or amplification. J Clin Oncol. 2011;29(21):2904–9.
33. Kluger HM, Dudek A, McCann C, Rink L, Ritacco J, Adrada C,et al. A phase II trial of dasatinib in advanced melanoma. J ClinOncol. 2009;27(suppl):abstract 9010.

1852 N.L. Schoenewolf et al. / European Journal of Cancer 48 (2012) 1842–1852
34. Woodman SE, Trent JC, Stemke-Hale K, et al. Activity ofdasatinib against L576P KIT mutant melanoma: molecular,cellular, and clinical correlates. Mol Cancer Ther.
2009;8(8):2079–85.35. Yamaguchi M, Harada K, Ando N, Kawamura T, Shibagaki N,
Shimada S. Marked response to imatinib mesylate in metastaticacral lentiginous melanoma on the thumb. Clin Exp Dermatol.2010.
36. Zhu Y SL, Kong Y, Chi Z, Yuan X CC, Sheng X GJ, L S.Response to sunitinib in Chinese KIT -mutated metastaticmucosal melanoma. J Clin Oncol. 2009;27 ((suppl):abstracte20017).
37. Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009AJCC melanoma staging and classification. J Clin Oncol.
2009;27(36):6199–206.38. Edge SB, Compton CC. The American Joint Committee on
Cancer: the 7th edition of the AJCC cancer staging manual andthe future of TNM. Annals of surgical oncology.
2010;17(6):1471–4.
39. Tarn C, Merkel E, Canutescu AA, et al. Analysis of KITmutations in sporadic and familial gastrointestinal stromaltumors: therapeutic implications through protein modeling. Clin
Cancer Res. 2005;11(10):3668–77.40. Houben R, Vetter-Kauczok CS, Ortmann S, et al. Phospho-ERK
staining is a poor indicator of the mutational status of BRAF andNRAS in human melanoma. J Invest Dermatol. 2008;128(8):2003–12.
41. Abysheva SN, Iyevleva AG, Efimova NV, et al. KIT mutations inRussian patients with mucosal melanoma. Melanoma research.
2011;21(6):555–9.42. Bastian BC, LeBoit PE, Hamm H, Brocker EB, Pinkel D.
Chromosomal gains and losses in primary cutaneous melanomasdetected by comparative genomic hybridization. Cancer Res.
1998;58(10):2170–5.43. Schoenewolf NL, Urosevic-Maiwald M, Dummer R. Tumor
heterogeneity of mucosal melanomas during treatment withimatinib. Br J Dermatol. 2011.
Copyright © 2022 FDOKUMEN




















