Single tooth replacement-expanded treatment options
13
Australian Dental Journal 1994;39(3):137-49 Single tooth replacement - Richard W. Chan, BDS, MDS, FRACDS Thomas N. Tseng, BDS, FRACDS Abstract The aim of any prosthesis is to restore function and aesthetics by replacing the missingtooth with minimal risks to adjacent tissues. The options presently avail- able to the patient for the replacement of a missing single tooth include the removable partial denture, partial and full coverage bridgework, resin-bonded bridgework and the single-tooth implant prosthesis. The relative merits and guidelinesfor successful appli- cation of these treatment modalities are presented. Key words: Bridge, implant, single tooth replacement. (Received for publication December 1992. Accepted July 1993.) Introduction With the development of treatment modalities during the last two decades, the options available for the replace- ment of the single missing tooth have expanded. Removable partial dentures, partial veneer and full coverage bridgework have been utilized for many years. In the 1950~~ the development of acrylic resin, which allowed the veneering of the metal full coverage bridge framework, offered an improved aesthetic result. The development of the porcelain-bonded-to-metal technique in the 1960s provided a more aesthetic and durable prosthesis. Advances in adhesion between enamel and synthetic resins led to the introduction of the resin-bonded bridge. Rochette,' and subsequently, the Maryland-type bonded bridgework,2-6 gained acceptance as a conservative alternative to conventional full coverage bridgework in selected cases. The latest addition to these treatment options is the single-tooth implant prosthesis. The aim of any prosthesis is to restore function and aesthetics by replacing the missing tooth with minimal risks to adjacent tissues. In this article the various options now available to the patient will be discussed. Removable partial dentures A removable partial denture (RPD) is a conservative treatment option. It is a reversible procedure that still allows the patient to proceed to the other treatment alter- natives in the future if desired. It is ideal in situations where potential abutment teeth have not fully erupted Australian Dental Journal 1994;39:3 expanded treatment options or when the alveolar processes have not yet fully grown as in early adolescent patients. Usually only minimal tooth preparation within enamel is required for a RPD. T o provide for better distribution of occlusal forces and to prevent rotation, occlusal rests are placed on the adjacent abutment teeth. Guide planes and enamel recontouring to improve clasp undercuts may also be used to increase retention of the RPD. In patients who have single-tooth edentulous spaces in more than one location within an arch, a RPD is capable of replacing more than one missing single tooth with the one appliance (Fig. la, b). If it is anticipated that addi- tional teeth will be lost sometime after the fabrication of the prosthesis, then a removable partial denture may be the treatment of choice. Where the patient has a diastema present adjacent to the missing tooth, a RPD will allow the preservation of the spacing if the patient so desires. In cases where there has been a reduction of the crestal height of the alveolar bone in the edentulous space, an acrylic flange can be added to the pontic allowing it to be the correct proportional length. In this circumstance, the RPD may offer an advantage compared with fixed bridgework, where ridge augmentation may be required to provide a more adequate ridge The creation of an aesthetic pontic can be difficult with fixed bridge- work, when alveolar bone loss is marked, due to the aesthetic limitations of currently available porcelain materials to simulate gingival tissues. A RPD can be used when the periodontal health of the adjacent abutment teeth is guarded, provided factors such as plaque, pocket depth, transmitted forces to the teeth and tissue coverage are controlled. Some patients consider the RPD to be a bulky appli- ance. Cross-arch stabilization is required in most cases. Where the RPD covers the anterior part of the palate, phonetic problems can arise. Plaque accumulation can occur between the appliance and supporting teeth with increased potential for caries and periodontal problems. The teeth that become involved are often in areas well away from the missing teeth. L e ~ h n e r , ~ in a two-year study on removable partial denture patients found greater plaque retention on the buccal surfaces of clasped teeth, on surfaces covered by the prosthesis, and on lingual surfaces where the major connector was closer than 2.0 mm to the gingival margin. 137
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Single tooth replacement-expanded treatment options
Australian Dental Journal 1994;39(3):137-49
Single tooth replacement - Richard W. Chan, BDS, MDS, FRACDS Thomas N. Tseng, BDS, FRACDS
Abstract The aim of any prosthesis is to restore function and aesthetics by replacing the missing tooth with minimal risks to adjacent tissues. The options presently avail- able to the patient for the replacement of a missing single tooth include the removable partial denture, partial and full coverage bridgework, resin-bonded bridgework and the single-tooth implant prosthesis. The relative merits and guidelines for successful appli- cation of these treatment modalities are presented.
Key words: Bridge, implant, single tooth replacement.
(Received for publication December 1992. Accepted July 1993.)
Introduction With the development of treatment modalities during
the last two decades, the options available for the replace- ment of the single missing tooth have expanded. Removable partial dentures, partial veneer and full coverage bridgework have been utilized for many years. In the 1 9 5 0 ~ ~ the development of acrylic resin, which allowed the veneering of the metal full coverage bridge framework, offered an improved aesthetic result. The development of the porcelain-bonded-to-metal technique in the 1960s provided a more aesthetic and durable prosthesis. Advances in adhesion between enamel and synthetic resins led to the introduction of the resin-bonded bridge. Rochette,' and subsequently, the Maryland-type bonded bridgework,2-6 gained acceptance as a conservative alternative to conventional full coverage bridgework in selected cases. The latest addition to these treatment options is the single-tooth implant prosthesis.
The aim of any prosthesis is to restore function and aesthetics by replacing the missing tooth with minimal risks to adjacent tissues. In this article the various options now available to the patient will be discussed.
Removable partial dentures A removable partial denture (RPD) is a conservative
treatment option. It is a reversible procedure that still allows the patient to proceed to the other treatment alter- natives in the future if desired. It is ideal in situations where potential abutment teeth have not fully erupted
Australian Dental Journal 1994;39:3
expanded treatment options
or when the alveolar processes have not yet fully grown as in early adolescent patients.
Usually only minimal tooth preparation within enamel is required for a RPD. T o provide for better distribution of occlusal forces and to prevent rotation, occlusal rests are placed on the adjacent abutment teeth. Guide planes and enamel recontouring to improve clasp undercuts may also be used to increase retention of the RPD.
In patients who have single-tooth edentulous spaces in more than one location within an arch, a RPD is capable of replacing more than one missing single tooth with the one appliance (Fig. la, b). If it is anticipated that addi- tional teeth will be lost sometime after the fabrication of the prosthesis, then a removable partial denture may be the treatment of choice. Where the patient has a diastema present adjacent to the missing tooth, a RPD will allow the preservation of the spacing if the patient so desires.
In cases where there has been a reduction of the crestal height of the alveolar bone in the edentulous space, an acrylic flange can be added to the pontic allowing it to be the correct proportional length. In this circumstance, the RPD may offer an advantage compared with fixed bridgework, where ridge augmentation may be required to provide a more adequate ridge The creation of an aesthetic pontic can be difficult with fixed bridge- work, when alveolar bone loss is marked, due to the aesthetic limitations of currently available porcelain materials to simulate gingival tissues.
A RPD can be used when the periodontal health of the adjacent abutment teeth is guarded, provided factors such as plaque, pocket depth, transmitted forces to the teeth and tissue coverage are controlled.
Some patients consider the RPD to be a bulky appli- ance. Cross-arch stabilization is required in most cases. Where the RPD covers the anterior part of the palate, phonetic problems can arise. Plaque accumulation can occur between the appliance and supporting teeth with increased potential for caries and periodontal problems. The teeth that become involved are often in areas well away from the missing teeth. Le~hner ,~ in a two-year study on removable partial denture patients found greater plaque retention on the buccal surfaces of clasped teeth, on surfaces covered by the prosthesis, and on lingual surfaces where the major connector was closer than 2.0 mm to the gingival margin.
137
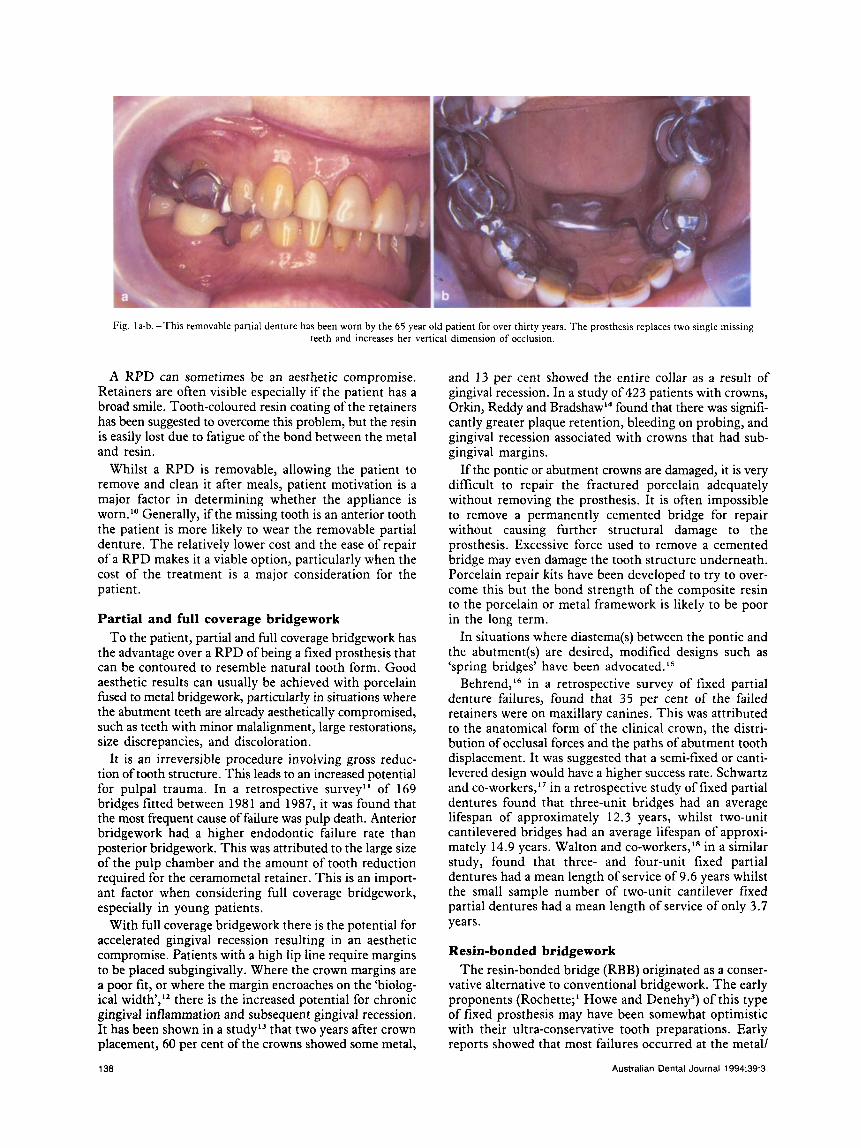
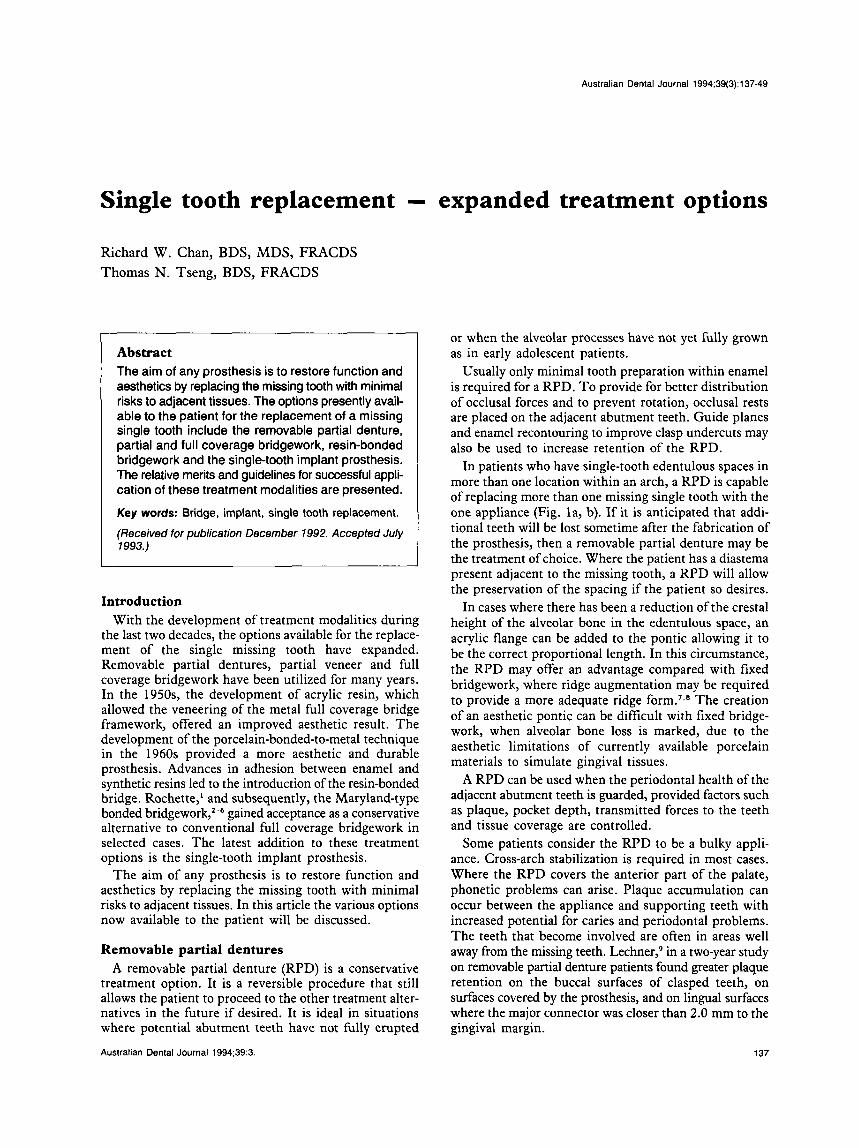
Fig. la-b.-This removable partial denture has been worn by the 65 year old patient for over thirty years. T h e prosthesis replaces two single missing teeth and increases her vertical dimension of occlusion.
A RPD can sometimes be an aesthetic compromise. Retainers are often visible especially if the patient has a broad smile. Tooth-coloured resin coating of the retainers has been suggested to overcome this problem, but the resin is easily lost due to fatigue of the bond between the metal and resin.
Whilst a RPD is removable, allowing the patient to remove and clean it after meals, patient motivation is a major factor in determining whether the appliance is worn.'O Generally, if the missing tooth is an anterior tooth the patient is more likely to wear the removable partial denture. The relatively lower cost and the ease of repair of a RPD makes it a viable option, particularly when the cost of the treatment is a major consideration for the patient.
Partial and full coverage bridgework T o the patient, partial and full coverage bridgework has
the advantage over a RPD of being a fixed prosthesis that can be contoured to resemble natural tooth form. Good aesthetic results can usually be achieved with porcelain fused to metal bridgework, particularly in situations where the abutment teeth are already aesthetically compromised, such as teeth with minor malalignment, large restorations, size discrepancies, and discoloration.
It is an irreversible procedure involving gross reduc- tion of tooth structure. This leads to an increased potential for pulpal trauma. In a retrospective survey" of 169 bridges fitted between 1981 and 1987, it was found that the most frequent cause of failure was pulp death. Anterior bridgework had a higher endodontic failure rate than posterior bridgework. This was attributed to the large size of the pulp chamber and the amount of tooth reduction required for the ceramometal retainer. This is an import- ant factor when considering full coverage bridgework, especially in young patients.
With full coverage bridgework there is the potential for accelerated gingival recession resulting in an aesthetic compromise. Patients with a high lip line require margins to be placed subgingivally. Where the crown margins are a poor fit, or where the margin encroaches on the 'biolog- ical width','' there is the increased potential for chronic gingival inflammation and subsequent gingival recession. It has been shown in a studyL3 that two years after crown placement, 60 per cent of the crowns showed some metal,
138
and 13 per cent showed the entire collar as a result of gingival recession. In a study of 423 patients with crowns, Orkin, Reddy and Brad~haw'~ found that there was signifi- cantly greater plaque retention, bleeding on probing, and gingival recession associated with crowns that had sub- gingival margins.
If the pontic or abutment crowns are damaged, it is very difficult to repair the fractured porcelain adequately without removing the prosthesis. It is often impossible to remove a permanently cemented bridge for repair without causing further structural damage to the prosthesis. Excessive force used to remove a cemented bridge may even damage the tooth structure underneath. Porcelain repair kits have been developed to try to over- come this but the bond strength of the composite resin to the porcelain or metal framework is likely to be poor in the long term.
In situations where diastema(s) between the pontic and the abutment(s) are desired, modified designs such as 'spring bridges' have been advocated."
Behrend,16 in a retrospective survey of fixed partial denture failures, found that 35 per cent of the failed retainers were on maxillary canines. This was attributed to the anatomical form of the clinical crown, the distri- bution of occlusal forces and the paths of abutment tooth displacement. It was suggested that a semi-fixed or canti- levered design would have a higher success rate. Schwartz and co-workers," in a retrospective study of fixed partial dentures found that three-unit bridges had an average lifespan of approximately 12.3 years, whilst two-unit cantilevered bridges had an average lifespan of approxi- mately 14.9 years. Walton and co-workers,'8 in a similar study, found that three- and four-unit fixed partial dentures had a mean length of service of 9.6 years whilst the small sample number of two-unit cantilever fixed partial dentures had a mean length of service of only 3.7 years.
Resin-bonded bridgework The resin-bonded bridge (RBB) originated as a conser-
vative alternative to conventional bridgework. The early proponents (Rochette;' Howe and Denehy3) of this type of fixed prosthesis may have been somewhat optimistic with their ultra-conservative tooth preparations. Early reports showed that most failures occurred at the metall
Australian Dental Journal 1994;39:3.
Fig. 2 -This case illustrates the application of resin-bonded bridgework in the mandibular molar region where anatomical structures may restrict the use of single-tooth implants. Note the 'wraparound' design ofthe retamers to achieve increased resistance and retention form whilst maximizing the
amount of surface area for resin-bonding.
resin interface. Perforated retainers, first introduced at the University of Maryland,2 were found to have limit- ations. These bridges failed because of microleakage and the excessive wear of the exposed resin cement. These retainers need to be thicker for stiffness and fatigue resistance due to the weakening effect of the perforations. However, advances in electrolytic e t ~ h i n g , ~ , ~ chemical etching, sandblasting, and resin-metal bonding t e ~ h n o l o g y ~ ~ . ~ ~ have improved the strength of the residmetal bond. In addition, more definitive abutment tooth preparations and bridge design have made the resin- bonded bridge a more predictable form of single tooth replacement in selected cases.
In principle, resin-bonded retainers are very similar to the partial veneer retainers. Retentive features such as pins and contrabevels which are often missing in resin-bonded bridge retainers are compensated by the increased reten- tion provided by the resin-bonding to the tooth preparation. A study by Murakami and BarrackZi found that a linear relationship existed between the surface area of enamel bonded to the bridgework, and the force required to displace it.
As tooth preparation is kept to a minimum, the risk of pulpal involvement or irritation during full crown pre- paration is avoided. This is an important consideration in young patients.
Certain conditions may affect the quality of enamel avail- able for bonding. Concentrated peroxide-based vital bleaching agents may affect the enamel structure and hence the enamel/composite resin bond.22
Australian Dental Journal 1994;39:3
The design and the accuracy of the fit of the retainers are of utmost importance for the long-term stability of the The metal framework should be designed to resist any displacing forces. Occlusal rests and ledges provide resistance to occlusal forces along the long axis of the abutment tooth. Grooves and guide planes provide resistance to lateral displacement, and the majority of the retention required. Wherever possible, a wrap-around design should be used for the bridge retainers (Fig. 2).6.23-25 Since the tooth preparation is ideally kept supragingival, the resin-bonded bridge is less harmful to the periodontal tissues when compared with full coverage bridgework.6
Taking aesthetics into consideration, utilization of the maximum area of enamel available for bonding will enhance retention of the prosthesis. If there are large carious lesions or large restorations that will not allow adequate area for bonding, then the resin-tooth bond will be diminished. Teeth with short clinical crowns do not make good abutments for a resin-bonded bridge. Crown lengthening procedures should be employed to provide a greater area for mechanical retention. However, this usually provides very little additional enamel available for resin-bonding in the cervical region of the tooth.
In situations where there is a discrepancy in the align- ment of the abutment teeth, a successful result is difficult to achieve without excessive tooth reduction (which reduces significantly the amount of enamel available for resin-bonding). The use of a semi-fixed design may be necessary in these cases.
139
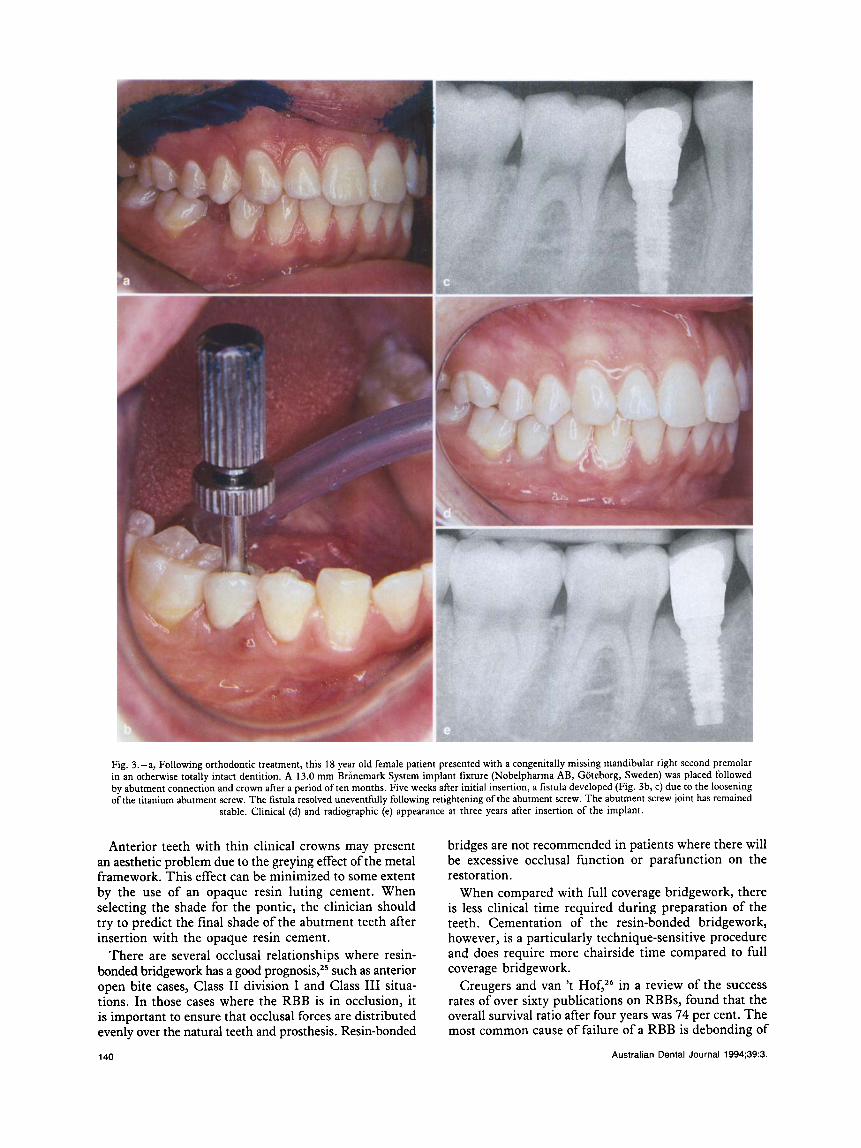
Fig. 3. -a, Following orthodontic treatment, this 18 year old female patient presented with a congenitally missing mandibular right second premolar in an otherwise totally intact dentition. A 13.0 mm Brinemark System implant fixture (Nobelpharma AB, Goteborg, Sweden) was placed followed by abutment connection and crown after a period of ten months. Five weeks after initial insertion, a fistula developed (Fig. 3b, c) due to the loosening of the titanium abutment screw. The fistula resolved uneventhlly following retightening of the abutment screw. The abutment screw joint has remained
stable. Clinical (d) and radiographic (e) appearance at three years after insertion of the implant.
Anterior teeth with thin clinical crowns may present an aesthetic problem due to the greying effect of the metal framework. This effect can be minimized to some extent by the use of an opaque resin luting cement. When selecting the shade for the pontic, the clinician should try to predict the final shade of the abutment teeth after insertion with the opaque resin cement.
There are several occlusal relationships where resin- bonded bridgework has a good prognosis,25 such as anterior open bite cases, Class I1 division I and Class I11 situa- tions. In those cases where the RBB is in occlusion, it is important to ensure that occlusal forces are distributed evenly over the natural teeth and prosthesis. Resin-bonded
140
bridges are not recommended in patients where there will be excessive occlusal function or parafunction on the restoration.
When compared with full coverage bridgework, there is less clinical time required during preparation of the teeth. Cementation of the resin-bonded bridgework, however, is a particularly technique-sensitive procedure and does require more chairside time compared to full coverage bridgework.
Creugers and van 't HofYZ6 in a review of the success rates of over sixty publications on RBBs, found that the overall survival ratio after four years was 74 per cent. The most common cause of failure of a RBB is debonding of
Australian Dental Journal 1994;39:3.
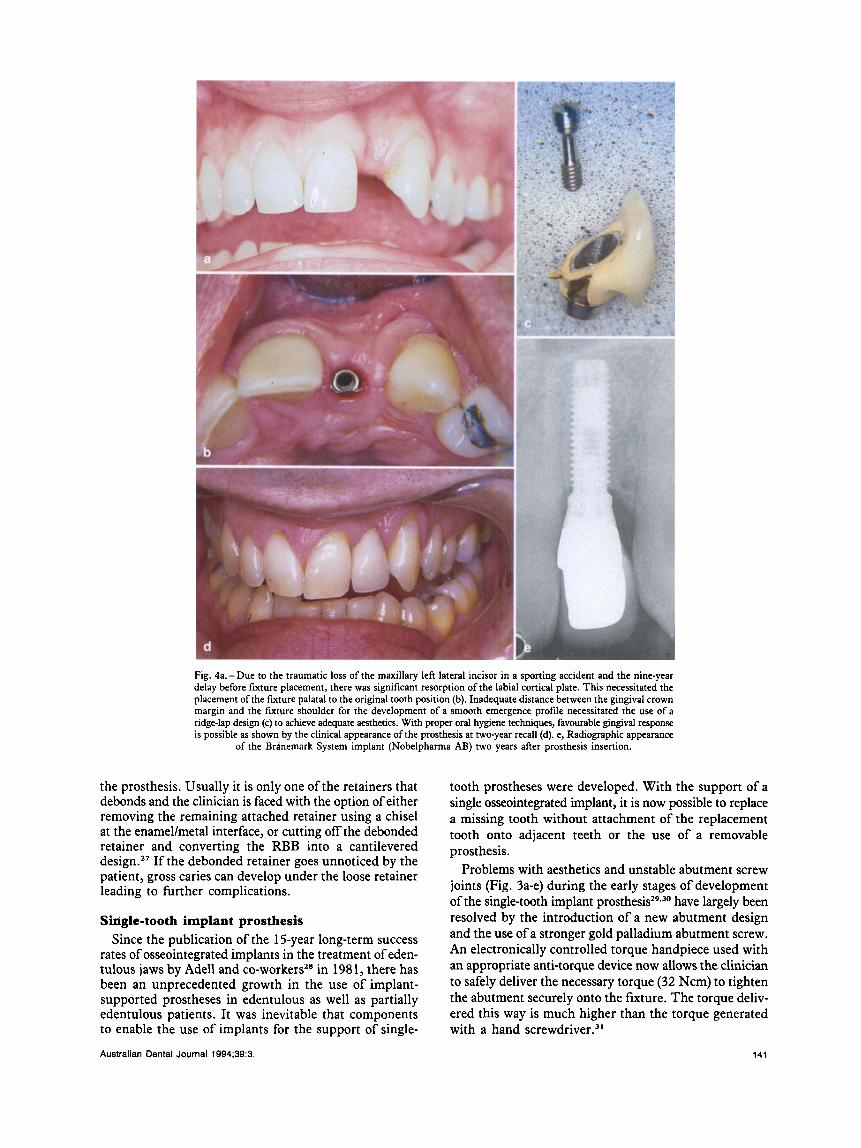
Fig. 4a.-Due to the traumatic loss of the maxillary left lateral incisor in a sporting accident and the nine-year delay before fixture placement, there was significant resorption of the labial cortical plate. This necessitated the placement ofthe fixture palatal to the original tooth position (b). Inadequate distance between the gingival crown margin and the fixture shoulder for the development of a smooth emergence profile necessitated the use of a ridge-lap design (c) to achieve adequate aesthetics. With proper oral hygiene techniques, favourable gingival response is possible as shown by the clinical appearance of the prosthesis at two-year recall (d). e, Radiographic appearance
of the Brinemark System implant (Nobelpharma AB) two years after prosthesis insertion.
the prosthesis. Usually it is only one of the retainers that debonds and the clinician is faced with the option of either removing the remaining attached retainer using a chisel at the enamellmetal interface, or cutting off the debonded retainer and converting the RBB into a cantilevered de~ign.~’ If the debonded retainer goes unnoticed by the patient, gross caries can develop under the loose retainer leading to further complications.
Single-tooth implant prosthesis Since the publication of the 15-year long-term success
rates of osseointegrated implants in the treatment of eden- tulous jaws by Adell and co-workersz8 in 1981, there has been an unprecedented growth in the use of implant- supported prostheses in edentulous as well as partially edentulous patients. It was inevitable that components to enable the use of implants for the support of single-
Australian Dental Journal 1994;39:3.
tooth prostheses were developed. With the support of a single osseointegrated implant, it is now possible to replace a missing tooth without attachment of the replacement tooth onto adjacent teeth or the use of a removable prosthesis.
Problems with aesthetics and unstable abutment screw joints (Fig. 3a-e) during the early stages of development of the single-tooth implant p r o s t h e ~ i s ~ ~ ~ ~ ~ have largely been resolved by the introduction of a new abutment design and the use of a stronger gold palladium abutment screw. An electronically controlled torque handpiece used with an appropriate anti-torque device now allows the clinician to safely deliver the necessary torque (32 Ncm) to tighten the abutment securely onto the fixture. The torque deliv- ered this way is much higher than the torque generated with a hand crewd driver.^^
141
142
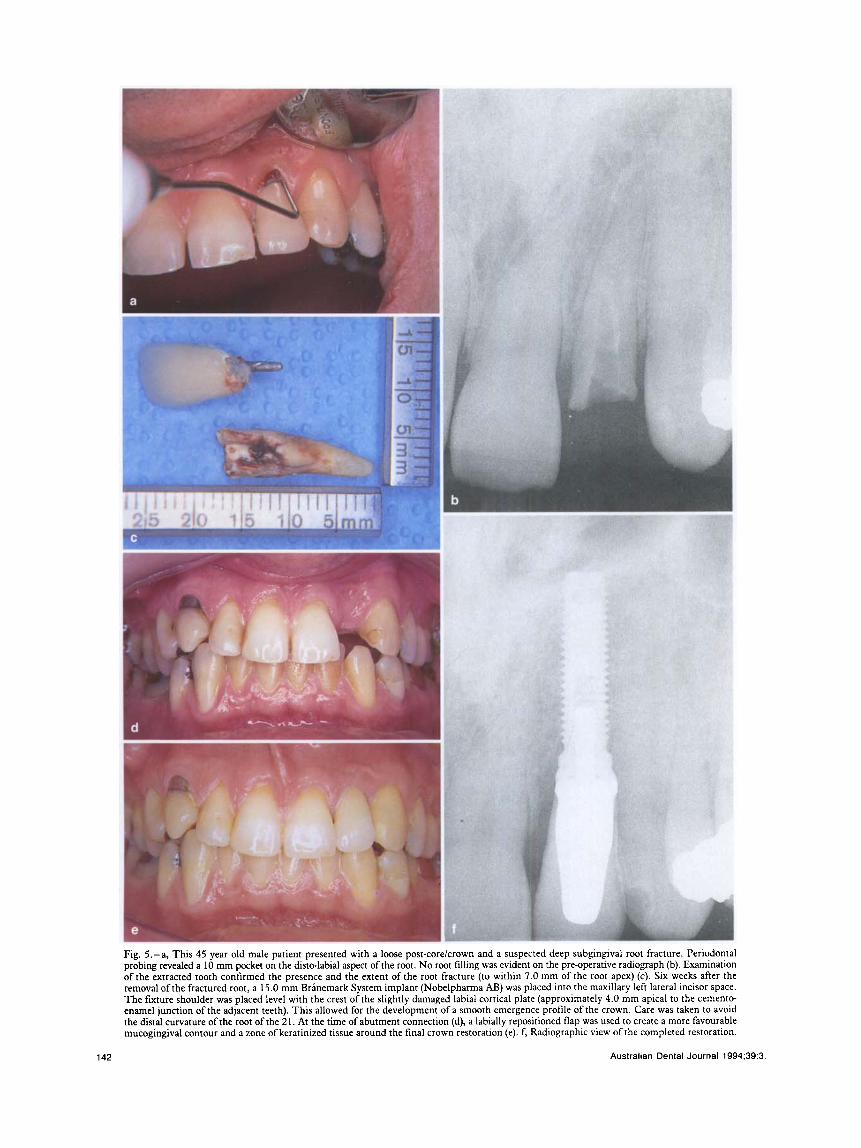
Fig. 5.-a, This 45 year old male patient presented with a loose post-corelcrown and a suspected deep subgingival root fracture. Periodontal probing revealed a 10 mm pocket on the disto-labial aspect ofthe root. No root filling was evident on the pre-operative radiograph (b). Examination of the extracted tooth confirmed the presence and the extent of the root fracture (to within 7.0 rnm of the root apex) (c). Six weeks after the removal ofthe fractured root, a 15.0 mm Brinemark System implant (Nobelpharma AB) was placed into the maxillary left lateral incisor space. The fixture shoulder was placed level with the crest of the slightly damaged labial cortical plate (approximately 4.0 mm apical to the cemento- enamel junction of the adjacent teeth). This allowed for the development of a smooth emergence profile of the crown. Care was taken to avoid the distal curvature of the root of the 2 1. At the time of abutment connection (d), a labially repositioned flap was used to create a more favourable mucogingival contour and a zone of keratinized tissue around the final crown restoration (e). f, Radiographic view of the completed restoration.
Australian Dental Journal 1994 ;39:3
The process of osseointegration is dependent on a gentle surgical technique carried out in a sterile environment, the use of a biocompatible implant material (such as commercially pure titanium), and a period of healing in which the implant is not subjected to occlusal force^.^' Profuse irrigation and the use of sterile, disposable rotary instruments ensure that the implant is placed into vital bone. With careful handling of soft tissue, postoperative pain and oedema are generally mild and of a short duration. Tissue response to the transmucosal titanium abutment has been found to resemble both clinically and histologically that of the soft tissues around natural teeth.33
With careful planning, and meticulous attention to furture angulation, soft tissue management and the crown emergence profile, a more superior aesthetic result can be achieved with a single-tooth implant compared with fmed bridgework. Should excessive gingival recession occur subsequent to crown insertion, provided adequate soft tissue thickness exists, and the fixture shoulder has been placed far enough apically at the time of fixture insertion, a shorter abutment can be inserted in order to maintain a subgingival crown margin for optimum aesthetics.
Australian Dental Journal 1994;39:3.
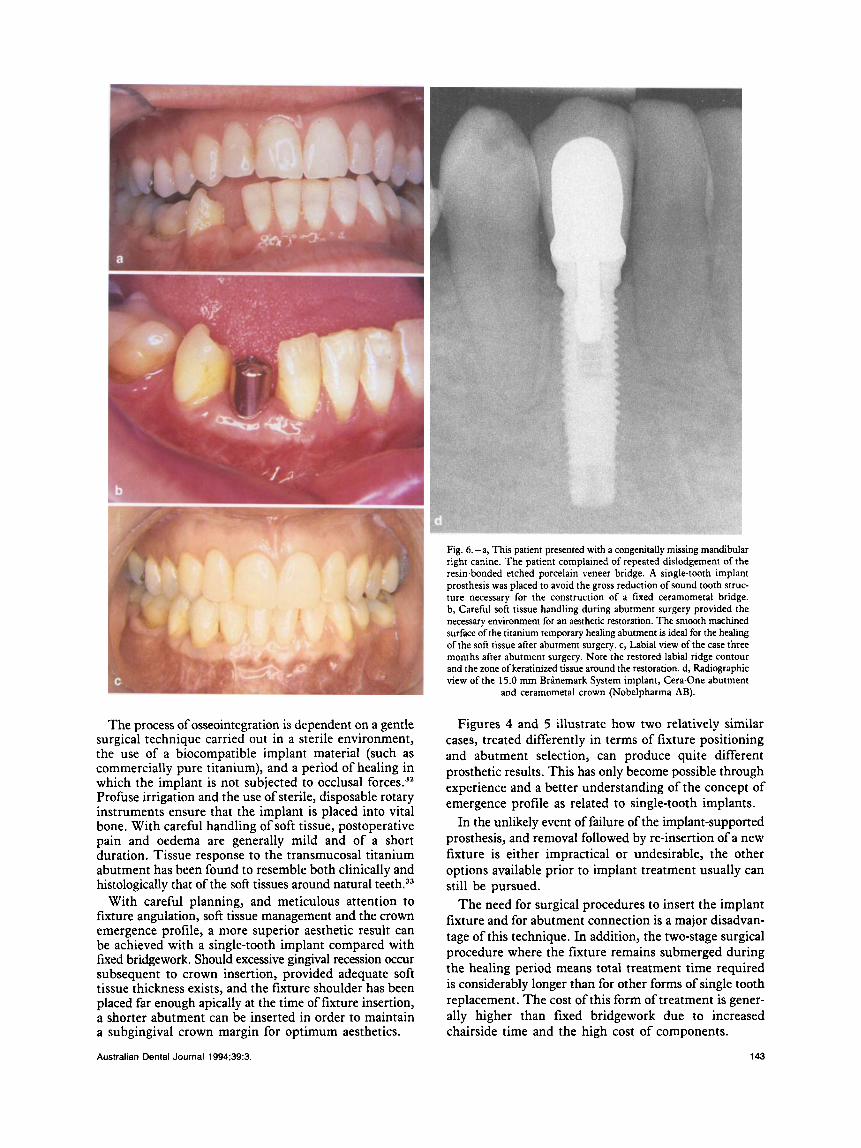
Fig. 6.-a, This patient presented with a congenitally missing mandibular right canine. The patient complained of repeated dislodgement of the resin-bonded etched porcelain veneer bridge. A single-tooth implant prosthesis was placed to avoid the gross reduction of sound tooth struc- ture necessary for the construction of a fixed ceramometal bridge. b, Carehl soft tissue handling during abutment surgery provided the necessary environment for an aesthetic restoration. The smooth macluned surface ofthe titanium temporary healing abutment is ideal for the healing of the soft tissue after abutment surgery. c, Labial view of the case three months after abutment surgery. Note the restored labial ridge contour and the zone ofkeratinized tissue around the restoration. d, Radiographic view of the 15.0 mm Brinemark System implant, Cera-One abutment
and ceramometal crown (Nobelpharma AB).
Figures 4 and 5 illustrate how two relatively similar cases, treated differently in terms of fixture positioning and abutment selection, can produce quite different prosthetic results. This has only become possible through experience and a better understanding of the concept of emergence profile as related to single-tooth implants.
In the unlikely event of failure of the implant-supported prosthesis, and removal followed by re-insertion of a new fixture is either impractical or undesirable, the other options available prior to implant treatment usually can still be pursued.
The need for surgical procedures to insert the implant fixture and for abutment connection is a major disadvan- tage of this technique. In addition, the two-stage surgical procedure where the fixture remains submerged during the healing period means total treatment time required is considerably longer than for other forms of single tooth replacement. The cost of this form of treatment is gener- ally higher than fixed bridgework due to increased chairside time and the high cost of components.
143
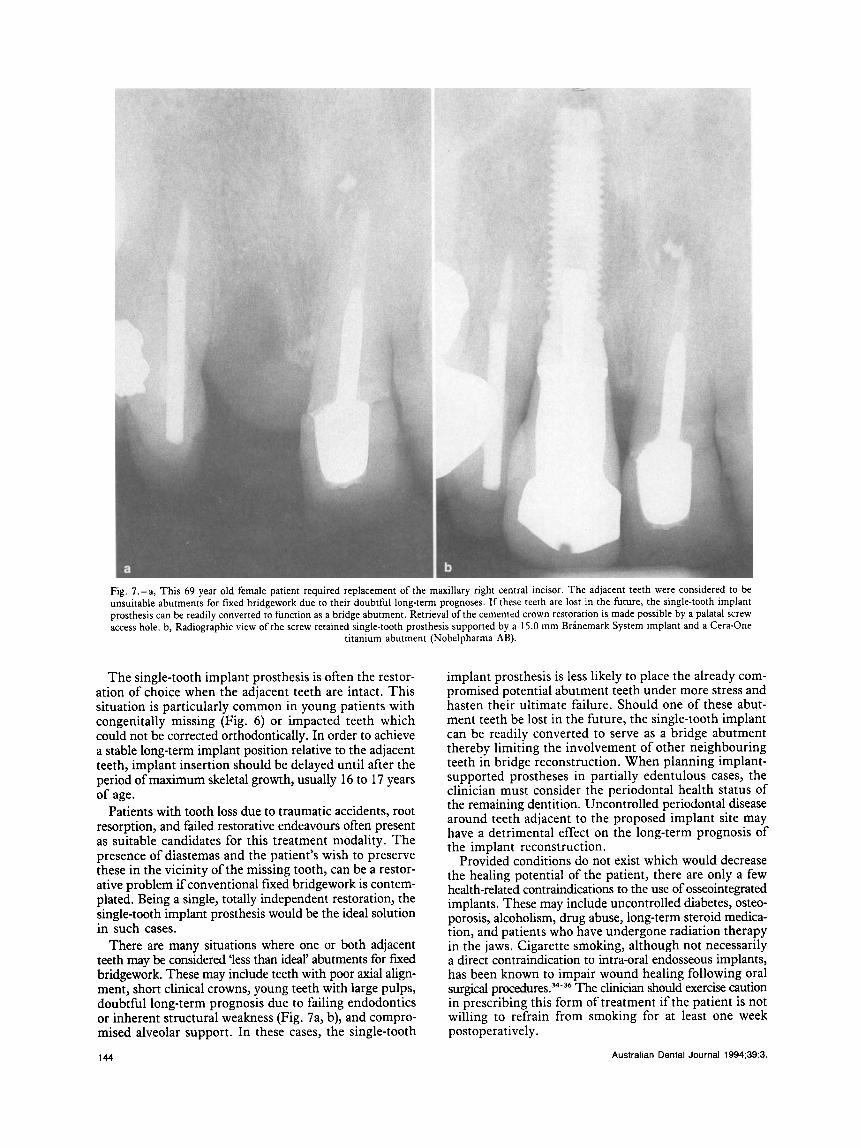
Fig. 7.-a, This 69 year old female patient required replacement of the maxillary right central incisor. The adjacent teeth were considered to be unsuitable abutments for fixed bridgework due to their doubtful long-term prognoses. If these teeth are lost in the future, the single-tooth implant prosthesis can be readily converted to function as a bridge abutment. Retrieval of the cemented crown restoration is made possible by a palatal screw access hole. b, Radiographic view of the screw retained single-tooth prosthesis supported by a 15.0 mm Branemark System implant and a Cera-One
titanium abutment (Nobelpharma AB).
The single-tooth implant prosthesis is often the restor- ation of choice when the adjacent teeth are intact. This situation is particularly common in young patients with congenitally missing (Fig. 6 ) or impacted teeth which could not be corrected orthodontically. In order to achieve a stable long-term implant position relative to the adjacent teeth, implant insertion should be delayed until after the period of maximum skeletal growth, usually 16 to 17 years of age.
Patients with tooth loss due to traumatic accidents, root resorption, and failed restorative endeavours often present as suitable candidates for this treatment modality. The presence of diastemas and the patient’s wish to preserve these in the vicinity of the missing tooth, can be a restor- ative problem if conventional fixed bridgework is contem- plated. Being a single, totally independent restoration, the single-tooth implant prosthesis would be the ideal solution in such cases.
There are many situations where one or both adjacent teeth may be considered ‘less than ideal’ abutments for fured bridgework. These may include teeth with poor axial align- ment, short clinical crowns, young teeth with large pulps, doubtful long-term prognosis due to failing endodontics or inherent structural weakness (Fig. 7a, b), and compro- mised alveolar support. In these cases, the single-tooth
implant prosthesis is less likely to place the already com- promised potential abutment teeth under more stress and hasten their ultimate failure. Should one of these abut- ment teeth be lost in the future, the single-tooth implant can be readily converted to serve as a bridge abutment thereby limiting the involvement of other neighbouring teeth in bridge reconstruction. When planning implant- supported prostheses in partially edentulous cases, the clinician must consider the periodontal health status of the remaining dentition. Uncontrolled periodontal disease around teeth adjacent to the proposed implant site may have a detrimental effect on the long-term prognosis of the implant reconstruction.
Provided conditions do not exist which would decrease the healing potential of the patient, there are only a few health-related contraindications to the use of osseointegrated implants. These may include uncontrolled diabetes, osteo- porosis, alcoholism, drug abuse, long-term steroid medica- tion, and patients who have undergone radiation therapy in the jaws. Cigarette smoking, although not necessarily a direct contraindication to intra-oral endosseous implants, has been known to impair wound healing following oral surgical procedures.”-36 The clinician should exercise caution in prescribing this form of treatment if the patient is not willing to refrain from smoking for at least one week postoperatively.
Australian Dental Journal 1994;39:3. 144
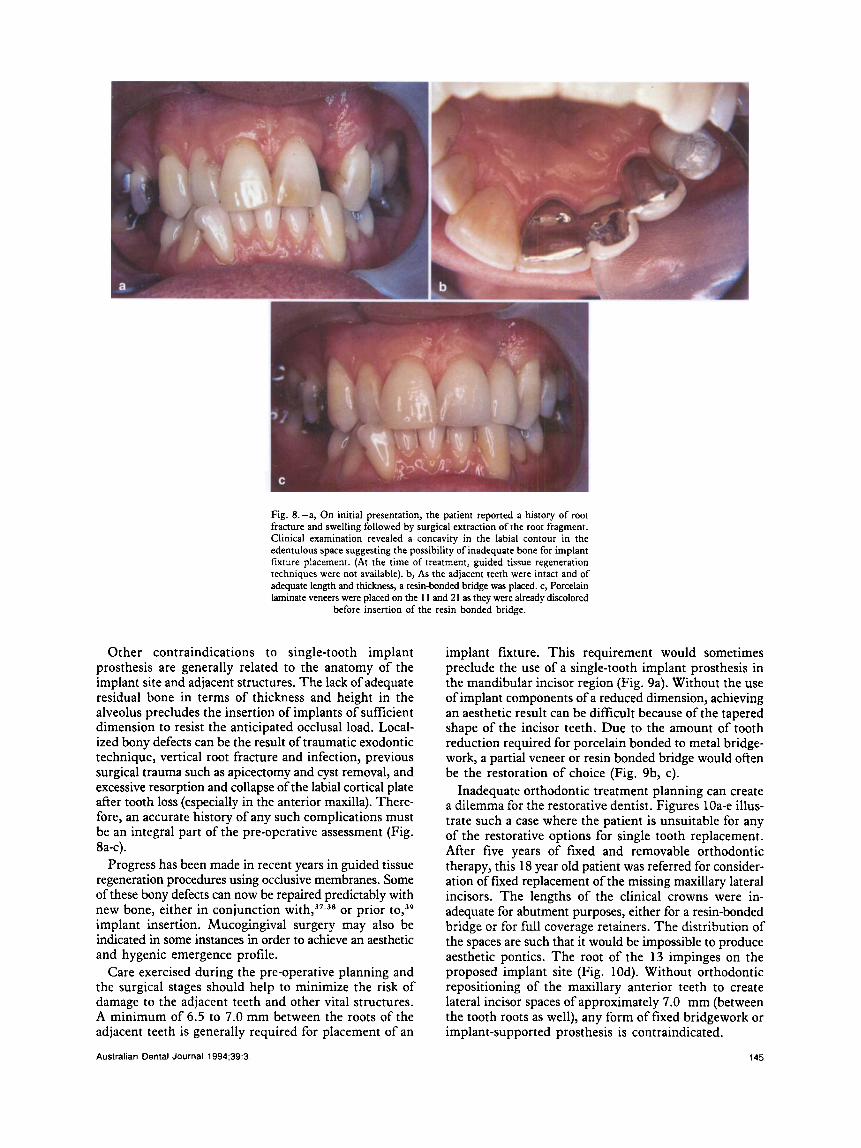
Fig. 8.-a, On initial presentation, the patient reported a history of root fracture and swelling followed by surgical extraction of the root fragment. Clinical examination revealed a concavity in the labial contour in the edentulous space suggesting the possibility of inadequate bone for implant fixture placement. (At the time of treatment, guided tissue regeneration techniques were not available). b, As the adjacent teeth were intact and of adequate length and thickness, a resin-bonded bridge was placed. c, Porcelain laminate veneers were placed on the 1 1 and 21 as they were already discolored
before insertion of the resin bonded bridge.
Other contraindications to single-tooth implant prosthesis are generally related to the anatomy of the implant site and adjacent structures. The lack of adequate residual bone in terms of thickness and height in the alveolus precludes the insertion of implants of sufficient dimension to resist the anticipated occlusal load. Local- ized bony defects can be the result of traumatic exodontic technique, vertical root fracture and infection, previous surgical trauma such as apicectomy and cyst removal, and excessive resorption and collapse of the labial cortical plate after tooth loss (especially in the anterior maxilla). There- fore, an accurate history of any such complications must be an integral part of the pre-operative assessment (Fig. 8a-c).
Progress has been made in recent years in guided tissue regeneration procedures using occlusive membranes. Some of these bony defects can now be repaired predictably with new bone, either in conjunction ~ i t h , ~ ' . ~ ~ or prior implant insertion. Mucogingival surgery may also be indicated in some instances in order to achieve an aesthetic and hygenic emergence profile.
Care exercised during the pre-operative planning and the surgical stages should help to minimize the risk of damage to the adjacent teeth and other vital structures. A minimum of 6.5 to 7.0 mm between the roots of the adjacent teeth is generally required for placement of an
Australian Dental Journal 1994;39:3.
implant fixture. This requirement would sometimes preclude the use of a single-tooth implant prosthesis in the mandibular incisor region (Fig. 9a). Without the use of implant components of a reduced dimension, achieving an aesthetic result can be difficult because of the tapered shape of the incisor teeth. Due to the amount of tooth reduction required for porcelain bonded to metal bridge- work, a partial veneer or resin bonded bridge would often be the restoration of choice (Fig. 9b, c).
Inadequate orthodontic treatment planning can create a dilemma for the restorative dentist. Figures 10a-e illus- trate such a case where the patient is unsuitable for any of the restorative options for single tooth replacement. After five years of fixed and removable orthodontic therapy, this 18 year old patient was referred for consider- ation of fixed replacement of the missing maxillary lateral incisors. The lengths of the clinical crowns were in- adequate for abutment purposes, either for a resin-bonded bridge or for full coverage retainers. The distribution of the spaces are such that it would be impossible to produce aesthetic pontics. The root of the 13 impinges on the proposed implant site (Fig. 10d). Without orthodontic repositioning of the maxillary anterior teeth to create lateral incisor spaces of approximately 7.0 mm (between the tooth roots as well), any form of fixed bridgework or implant-supported prosthesis is contraindicated.
145
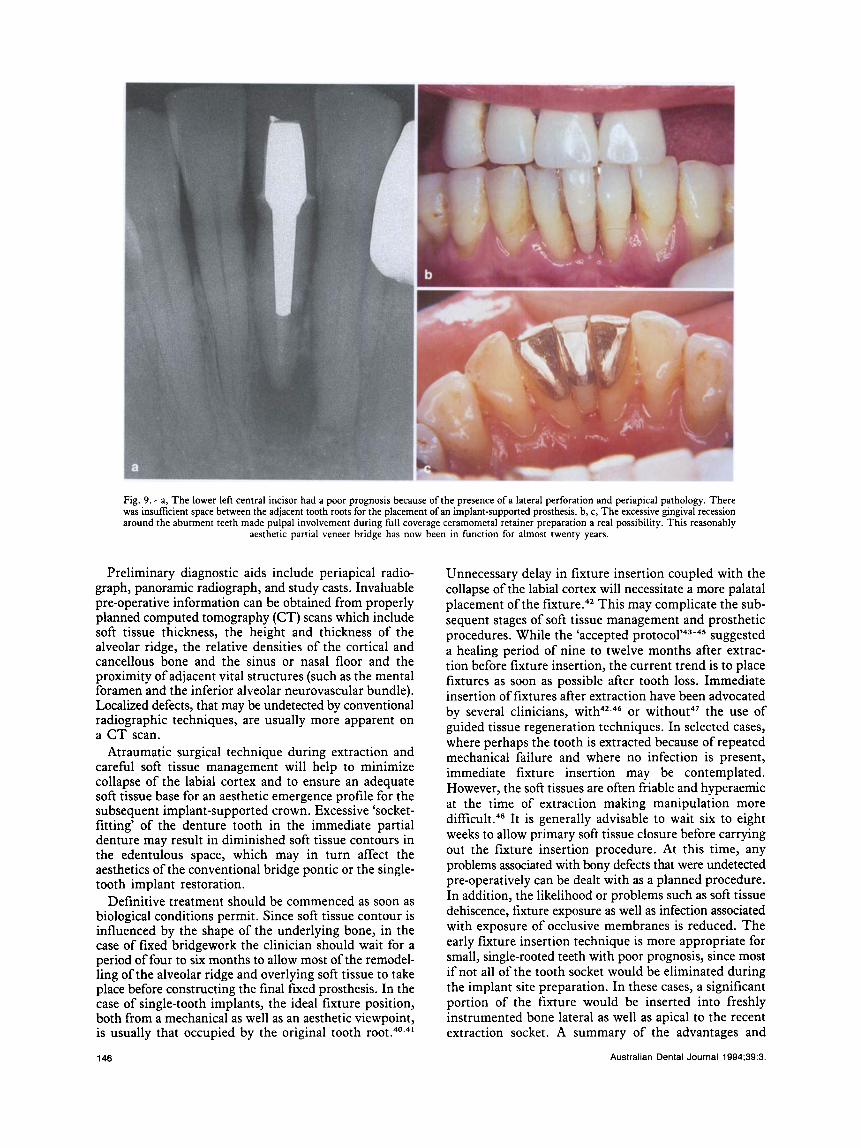
Fig. 9.-a, The lower left central incisor had a poor prognosis because of the presence of a lateral perforation and periapical pathology. There was insufficient space between the adjacent tooth roots for the placement of an implant-supported prosthesis. b, c, The excessive gingival recession around the abutment teeth made pulpal involvement during full coverage ceramometal retainer preparation a real possibility. This reasonably
aesthetic partial veneer bridge has now been in function for almost twenty years.
Preliminary diagnostic aids include periapical radio- graph, panoramic radiograph, and study casts. Invaluable pre-operative information can be obtained from properly planned computed tomography (CT) scans which include soft tissue thickness, the height and thickness of the alveolar ridge, the relative densities of the cortical and cancellous bone and the sinus or nasal floor and the proximity of adjacent vital structures (such as the mental foramen and the inferior alveolar neurovascular bundle). Localized defects, that may be undetected by conventional radiographic techniques, are usually more apparent on a C T scan.
Atraumatic surgical technique during extraction and careful soft tissue management will help to minimize collapse of the labial cortex and to ensure an adequate soft tissue base for an aesthetic emergence profile for the subsequent implant-supported crown. Excessive ‘socket- fitting’ of the denture tooth in the immediate partial denture may result in diminished soft tissue contours in the edentulous space, which may in turn affect the aesthetics of the conventional bridge pontic or the single- tooth implant restoration.
Definitive treatment should be commenced as soon as biological conditions permit. Since soft tissue contour is influenced by the shape of the underlying bone, in the case of fixed bridgework the clinician should wait for a period of four to six months to allow most of the remodel- ling of the alveolar ridge and overlying soft tissue to take place before constructing the final fixed prosthesis. In the case of single-tooth implants, the ideal fixture position, both from a mechanical as well as an aesthetic viewpoint, is usually that occupied by the original tooth r ~ ~ t . ~ ~ . ~ ~
146
Unnecessary delay in fixture insertion coupled with the collapse of the labial cortex will necessitate a more palatal placement of the This may complicate the sub- sequent stages of soft tissue management and prosthetic procedures. While the ‘accepted p ro toc01’~~-~~ suggested a healing period of nine to twelve months after extrac- tion before fixture insertion, the current trend is to place fixtures as soon as possible after tooth loss. Immediate insertion of fixtures after extraction have been advocated by several clinicians, it"'.^‘' or without4’ the use of guided tissue regeneration techniques. In selected cases, where perhaps the tooth is extracted because of repeated mechanical failure and where no infection is present, immediate fixture insertion may be contemplated. However, the soft tissues are often friable and hyperaemic at the time of extraction making manipulation more d i f f i c ~ l t . ~ ~ It is generally advisable to wait six to eight weeks to allow primary soft tissue closure before carrying out the fixture insertion procedure. At this time, any problems associated with bony defects that were undetected pre-operatively can be dealt with as a planned procedure. In addition, the likelihood or problems such as soft tissue dehiscence, fixture exposure as well as infection associated with exposure of occlusive membranes is reduced. The early fixture insertion technique is more appropriate for small, single-rooted teeth with poor prognosis, since most if not all of the tooth socket would be eliminated during the implant site preparation. In these cases, a significant portion of the fixture would be inserted into freshly instrumented bone lateral as well as apical to the recent extraction socket. A summary of the advantages and
Australian Dental Journal 1994;39:3.

Fig. 10.-a-e. This 18 year old patient was unsuitable for any of the restorative options for single tooth replacement. After five years of fixed and removable orthodontic therapy, she had been referred for consideration of a fixed replacement for the missing maxillary lateral incisors. (See text.)
Australian Dental Journal 1994;39:3. 147

Table 1. Immediate implant fixture insertion Table 4. Removable partial denture Advantages
Eliminates one surgical procedure(?) Shortens overall treatment time Reducelprevent collapse of buccal cortex and palatal resorption Placement of implant in original tooth position
Increased potential of infection Difficulty in achieving primary closure resulting in exposure of implant
The use of pedicle flaps to achieve soft tissue closure often result in
Disadvantages
andlor ridge augmentation material to oral cavity
untoward mucogingival alterations which may require surgical correction later
surgery
Keller, 1991)48
Augmentation material often requires removal before abutment connection
Tissues are often too friable and hyperaemic to manipulate (Tolman and
Lack of long-term clinical data
Table 2. Early (6 to 8 weeks) implant fixture insertion Advantages
Primary soft tissue healing Absence of residual infection Provides full mucosal coverage of fucture (and ridge augmentation material) Preservation of soft tissue height Little change in bony anatomy since extraction Placement of fixture in original tooth position A planned procedure Augmentation material can be removed during abutment surgery
Slight increase in treatment time Lack of long-term clinical data
Disadvantages
Table 3. Standard (9 to 12 months) implant fixture insertion Advantages
Complete soft tissue healing ‘Filling in’ of socket with matured bone Absence of residual infection Long-term clinical data (from edentulous cases only)
Collapse of buccal cortical plate Loss of alveolar ridge height Prolonged treatment time
Disadvantages
disadvantages of the different implant insertion times can be found in Tables 1 to 3.
The clinician is advised to exercise caution in prescribing single-tooth implant prosthesis for the replace- ment of molar teeth. Apart from the potential problems of access during instrumentation, the increased dimen- sion of the occlusal table may result in the restoration being subjected to more torque and possibly a higher chance of loosening of the abutment screw.” Similarly, replace- ment of canines in patients with cuspid-protected occlusion and deep overbite requires special consideration. Either anterior or posterior group disclusion may help to reduce the anticipated functional and parafunctional stresses on the implant prosthesis. Consideration may be given to the use of a nocturnal acrylic resin occlusal splint in patients suspected of a bruxing habit. Due to the difference in the degree of mobility of the natural teeth and the single-tooth implant prosthesis, the occlusal scheme should provide
‘Henry PJ. Thirty consecutive single-tooth restorations. The truth. Lecture, Nobel- pharma Team Days Conference, Sydney, 2 December 1990.
148
Advantages Conservative (minimal tooth preparation) Reversible procedure Can replace multiple missing teeth Useful in cases where diastema is to be preserved Can incorporate pink acrylic flange to compensate for loss of soft tissue Ease of repair Low cost
Disadvantages Removable appliance Bulky appliance Aesthetic compromise Phonetic problems Increased potential for caries and periodontal problems
Table 5. Full coverage bridgework Advantages
Fixed prosthesis Aesthetic restoration Natural contour Short treatment time Structurally or aesthetically compromised adjacent abutment teeth can
Moderate cost
Irreversible procedure Increased potential of pulpal trauma and gingival irritation (especially
young patients) Accelerated gingival recession Difficult to repair Non-retrievable Difficult to use in cases where diastema is to be preserved Requires flossing under pontic
be restored at the same time
Disadvantages
Table 6. Resin-bonded bridgework Advantages
Conservative preparation Fixed prosthesis Can be an aesthetic restoration Natural contour Short treatment time Moderate cost
Must adhere to strict case selection criteria in terms of alignment, clinical
Can be an aesthetic compromise with thin, fairly translucent abutment
Technique sensitive - meticulous attention during tooth preparation
Disadvantages
crown length and structural integrity of abutment teeth
teeth
and insertion
Table 7. Single-tooth implant prosthesis Advantages
Free-standing, fixed restoration No preparation of neighbouring teeth Superior aesthetics (emergence profile) Natural contour Same hygiene procedure as natural tooth Interchangeable precision engineered components Retrievability Other replacement options still available in event of failure Can be used easily in ‘diastema’ cases ‘Unsuitable’ abutment teeth - poor axial alignment, short clinical crown,
young thin teeth with large pulps, teeth with doubtful long-term prognosis
Disadvantages Need for surgery Duration of treatment High cost of components Must have adequate bone in the edentulous space for fixture placement Use in molar region with caution Technically demanding - precise surgical placement
Australian Dental Journal 1994;39:3.
for light, even, centric contacts on clenching. Lateral and protrusive contacts should be kept to a minimum.
Summary Replacement of the missing single tooth is one of the
most common prosthodontic problems encountered by the clinician. The currently available options and their select- ion criterias have been presented. The advantages and disadvantages of each option are summarized in Tables 4 to 7.
Acknowledgements The expertise of the following in the implant treatment
provided is duly acknowledged. Surgery: Dr B. Edelman (Fig. 3,4); Ceramics: B. Walters, P. Wagner and G. Roth. The authors sincerely thank Professor W. R. Hume for his constructive comments on the original manuscript. They are grateful to Dr Mark Spencer for his assistance in the reproduction of the slide materials and Mrs Christine Chan for assistance in the preparation of the manuscript. The contribution of Nobelpharma Australia Pty Limited towards the cost of production of the colour illustrations is greatly appreciated.
References 1. Rochette AL. Attachment of a splint to enamel of lower anterior teeth.
J Prosthet Dent 1973;30:418-23. 2. Kuhlke KL, Drennon DG. An alternative to the anterior single tooth
removable partial denture. J Int Assoc Dental Child 1977;8:11-4. 3. Howe DF, Denehy GE. Anterior fixed partial dentures utilizing the
acid etch technique and a cast metal framework. J Prosthet Dent
4. Thompson VP, Livaditis GJ, Del-Castillo E. Resin-bond to electrolyt- ically etched non precious alloys for resin-bonded prostheses. J Dent Res 1981;Sp Iss A:377:Abstr 265.
5. Livaditis GJ, Thompson VP. Etched castings: An improved retentive mechanism for resin-bonded retainers. J Prosthet Dent 1982;47:52-8.
6. Simonsen R, Thompson VP, Barrack G. Etched cast restorations: Clin- ical and laboratory techniques. Chicago: Quintessence, 1983.
7. Bahat 0, Deeb C, Golden T, Komarnyckyi 0. Preservation of ridges using hydroxyapatite. Int J Periodont Restor Dent 1987;6:35-41.
8. Gray JL, Quattlebaum JB. Correction of localized alveolar ridge defects utilizing hydroxyapatite and a ‘tunnelling’ approach: a case report. Int J Periodont Restor Dent 1988;3:73-7.
9. Lechner SK. A longitudinal survey of removable partial dentures. 111. Tissue reactions to various denture components. Aust Dent J
10. Bates JF. 1. Patient motivation, personality and successful dentures. Dent Update 1986;13:90-5.
11. Cheung GSP, Dimmer A, Mellor R, Gale M. A clinical evaluation of conventional bridgework. J Oral Rehabil 1990; 17: 131-6.
12. Ingber JS, Rose LF, Coslet JG. The biological width - a concept in periodontics and restorative dentistry. Alpha Omegan 1977;10:62-5.
13. Weir D, Stoffer W, Irvin D, er al. The stability of crown margin place- ment vs time. J Dent Res 1986;65:Abstr 1154:297.
14. Orkin DA, Reddy J, Bradshaw D. The relationship of the position of crown margins to gingival health. J Prosthet Dent 1987;57:421.
15. Kantorowicz GF. Inlays, crowns and bridges. 2nd edn. Baltimore: Williams Wilkins, 1970.
16. Behrend DA. Failure of maxillary canine retainers for fixed prostheses. Int J Prosthod 1989;2:429-37.
17. Schwartz NL, Whitsett LD, Berry TG, Stewart JL. Unserviceable crowns and fixed partial dentures: lifespan and causes for loss of serv- iceability. J Am Dent Assoc 1970;81:1395-401.
18. Walton JN, Gardner F, Agar J. A survey of crown and fixed partial denture failure: length of service and reasons for replacement. J Prosthet Dent 1986;56:4 16-21.
19. Musil R, Tiller HJ. The adhesion of dental resins to metal surfaces. The Kulzer silicoater technique. 1st edn. Wehrheim: Kulzer, 1984.
20. Ishjkima T, Caputo AA, Mito R. Adhesion of resin to casting alloys. J Prosthet Dent 1992;67:445-9.
1977;37:28-3 1.
1985;30:29 1-5.
Australian Dental Journal 1994;39:3
21. Murakami I, Barrack G. Relationship ofsurface area and design to the bond strength of etched cast restorations: an in virro study, J Prosthet Dent 1986;56:539-45.
22. Titley KC, Torneck CD, Smith DC, er al. Adhesion of composite resin to bleached and unbleached bovine enamel. J Dent Res 1988;67:1523-8.
23. Flood AM. Resin bonded prostheses: clinical guidelines. Aust Dent
24. Creugers NHJ, Snoek PA, van ’t Hof MA, Kayser AF. Clinical perfor- mance of resin-bonded bridges: a 5-year prospective study. 11. The influence of patient-dependent variables. J Oral Rehabil 1989;16:521-7.
25. Sykes DG, Walton TR. Resin bonded fixed partial dentures. A Review. Aust SOC Prosth Bull 1983;25-30.
26. Creugers NHJ, van ’t Hof MA. An analysis of clinical studies on resin- bonded bridges. J Dent Res 1991;70:146-9.
27. Ali A, Cassidy M, Gilmour A. Resin-bonded bridges: 2. Treatment planning, clinical cases and failures. Dent Update 1992; 1932-7.
28. Adell R, Eriksson B, Lekholm U, Brinemark P-I, Jemt T . A long- term follow up study of osseointegrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants 1990;5:347-59.
29. Jemt T, Lekholm U, Griindahl K. A 3-year follow up study of early single implant restorations ad modum Branemark. Int J Periodont Restor Dent 1990;10:341-9.
30. Jemt T, Laney WR, Harris D, Henry PJ, er al. Osseointegrated implants for single tooth replacement: a 1-year report from a multicenter prospec- tive study. Int J Oral Maxillofac Implants 1991;6:29-36.
31. Jorneus L, Jemt T, Carlsson L. Loads and designs of screw joints for single crowns supported by osseointegrated implants. Int J Oral Max- illofac Implants 1992;7:353-9.
32. Brinemark P-I, Zarb GA, Albrektsson T, eds. Tissue-integrated pros- theses. Osseointegration in clinical dentistry. Chicago: Quintessence, 1985.
33. Bower RC. Periodontal considerations of endosseous implants: A philosophy for understanding the tissue-implant interface. Aust Prosthod
34. Jones JK, Triplett RG. The relationship ofcigarette smoking to impaired intraoral wound healing: A review of evidence and implications for patient care. J Oral Maxillofac Surg 1992;50:237-9.
35. Preber H, Bergstrom J. Effect of cigarette smoking on periodontal healing following surgical therapy. J Clin Periodontol 1990;17:324-8.
36. Sweet JB, Butler DP. The relationship of smoking to localized oste- itis. J Oral Surg 1979;37:732.
37. Nyman S, Lang NP, Buser D, Bragger U. Bone regeneration adjacent to titanium dental implants using guided tissue regeneration: a report of two cases. Int J Oral Maxillofac Implants 1990;5:9-14.
38. Dahlin C, Lekholm U, Linde A. Membrane-induced bone augmenta- tion at titanium implants. A report of ten fixtures followed from 1 to 3 years after loading. Int J Periodont Restor Dent 1991;11:273-82.
39. Buser D, Bragger U, Lang NP, Nyman S. Regeneration and enlarge- ment of jaw bone using guided tissue regeneration. Clin Oral Imp1 Res
40. Parel SM, Sullivan DY. Guidelines for optimal fixture placement. In: Parel SM, Sullivan DY, eds. Esthetics and osseointegration. Dallas: Taylor, 1989: 19-28.
41. Sherwood RL, Sullivan DY. Concepts and techniques of single-tooth implant restorations. Esthetic Dent Update 1991;2: 16-22.
42. Lazzara RJ. Immediate implant placement into extraction sites: Surgical and restorative advantages. Int J Periodont Restor Dent 1989;9:333-43.
43. Johansson C, Albrektsson T. Integration ofscrew implants in the rabbit: A 1-year follow-up of removal torque of titanium implants. Int J Oral Maxillofac Implants 1987;2:69-75.
44. Ohrnell LO, Palmquist J, Brinemark P-I. Single tooth replacement. In: Worthington P, Brinemark P-I, eds. Advanced osseointegration surgery. Applications in the maxillofacial region. Chicago: Quintessence,
45. Nilson H, Lindh T . The treatment of the edentulous jaw. In: Restora- tive dentist’s manual. Gothenburg: Nobelpharma, 1991:Al-A7.
46. Becker W, Becker BE. Guided tissue regeneration for implants placed into extraction sockets and for implant dehiscences: surgical techniques and case reports. Int J Periodont Restor Dent 1990;10:377-91.
47. Barzilay I, Gaser GN, Caton J, Shenkle G. Immediate implantation of pure titanium threaded implants into extraction sockets. J Dent Res
48. Tolman DE, Keller EE. Endosseous implant placement immediately following dental extraction and alveoloplasty: preliminary report with 6-year follow-up. Int J Oral Maxillofac Implants 1991;6:24-8.
J 1989;34:209-18.
J 1987;1:25-8.
1990;1:22-32.
1992:211-32.
1988;67:234-40.
Address for correspondenceheprints: 14th Floor, Park House,
187 Macquarie Street, Sydney, New South Wales 2000.
149