Significance and management of disability among urban elderly residents in Brazil
11
LUIZ R. RAMOS,MONICAPERRACINI, TEREZAE. ROSA, ALEX KALACHE SIGNIFICANCE AND MANAGEMENT OF DISABILITY AMONG URBAN ELDERLY RESIDENTS IN BRAZIL ABSTRACT. Brazil's population is aging very rapidly, and the care for the elderly is an emerging priority. The results of a multidimensional functional assessment of elderly residents in Sao Paulo showed extreme poverty and massive cohabitation in multigenera- tional households. The health profile showed a high prevalence of chronic illnesses, mental disorders, and disability. Using a Guttman scale, a set of activities of daily living was validated as an indicator of dependency. Attention was given to the dependency associated factors, and in particular to the association between chronic illness and loss of independence among the aged. Fortunately, for the existing health care system in Brazil, cultural values are still keeping the family in the front line of caregiving, but this situation is not likely to withstand the increasing burden of a growing elderly population with an ever higher rate of disability. Key Words: aging in Brazil, functional status, disability, family support, activities of daily living, hierarchical dependency INTRODUCTION Brazil's population is aging very rapidly. Since the 1950s life expectancy at birth has been growing steadily and is expected to reach 70 by the year 2025 - a 25 year gain in a 75 year period. There should be, in fact, an elderly 'boom' by the turn of the century as the baby 'boom' generation of the 1950s reaches old age. Those aged 60 or more currently represent the fastest growing age group in the country and wilt increase 105% from 1980 to the year 2000 and another 130% by the year 2025. In addition, marked declines in fertility rates since the 1970s will greatly increase the proportion of aged persons in the total population - from 5% in the 1980s to 14% in 2025 at which time Brazil will have 32 million people 60 years or older, comprising the sixth largest elderly population in the world (Ramos, Veras, and Kalache 1987). Indeed, the whole transition from a young to an old population has been occurring very fast - mortality rates started to fall in the 1940s and less than 30 years later birth rates dropped abruptly - and a stage of low mortality and low fertility should be reached in the first half of the next century. In other words, the demographic transition in Brazil will take less than a century, actually half the time that it took in Europe, for instance, where the transition started in the late 17th century (Figure 1) (Ramos 1993). THE NEW PUBLIC HEALTH SCENARIO It is important to realize that such a rapid aging of the population is occurring in a country in which the majority of the population lives under the poverty line. Journal o[' Cross-Cultural Gerontology 8: 313-323, 1993. 1993 Kluwer Academic Publishers. Printed in the Netherlands.
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Significance and management of disability among urban elderly residents in Brazil

LUIZ R. RAMOS, MONICA PERRACINI, TEREZA E. ROSA, ALEX KALACHE
SIGNIFICANCE AND MANAGEMENT OF DISABILITY
AMONG URBAN ELDERLY RESIDENTS IN BRAZIL
ABSTRACT. Brazil's population is aging very rapidly, and the care for the elderly is an emerging priority. The results of a multidimensional functional assessment of elderly residents in Sao Paulo showed extreme poverty and massive cohabitation in multigenera- tional households. The health profile showed a high prevalence of chronic illnesses, mental disorders, and disability. Using a Guttman scale, a set of activities of daily living was validated as an indicator of dependency. Attention was given to the dependency associated factors, and in particular to the association between chronic illness and loss of independence among the aged. Fortunately, for the existing health care system in Brazil, cultural values are still keeping the family in the front line of caregiving, but this situation is not likely to withstand the increasing burden of a growing elderly population with an ever higher rate of disability.
Key Words: aging in Brazil, functional status, disability, family support, activities of daily living, hierarchical dependency
INTRODUCTION
Brazil 's population is aging very rapidly. Since the 1950s life expectancy at birth has been growing steadily and is expected to reach 70 by the year 2025 - a 25 year gain in a 75 year period. There should be, in fact, an elderly 'boom' by the turn of the century as the baby 'boom' generation of the 1950s reaches old age. Those aged 60 or more currently represent the fastest growing age group in the country and wilt increase 105% from 1980 to the year 2000 and another 130% by the year 2025. In addition, marked declines in fertility rates since the 1970s will greatly increase the proportion of aged persons in the total population
- from 5% in the 1980s to 14% in 2025 at which time Brazil will have 32 million people 60 years or older, comprising the sixth largest elderly population in the world (Ramos, Veras, and Kalache 1987).
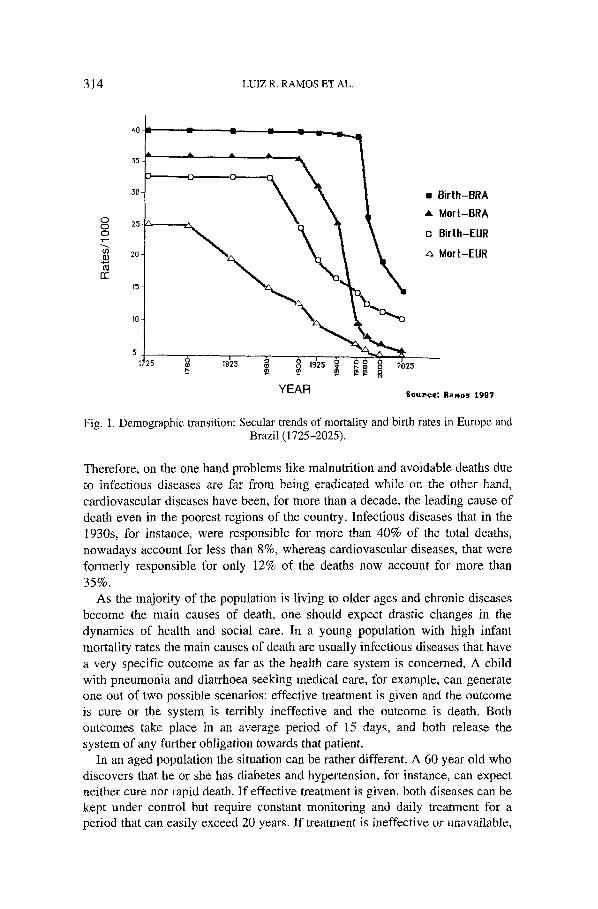
Indeed, the whole transition from a young to an old population has been occurring very fast - mortality rates started to fall in the 1940s and less than 30 years later birth rates dropped abruptly - and a stage of low mortality and low fertility should be reached in the first half of the next century. In other words, the demographic transition in Brazil will take less than a century, actually half the time that it took in Europe, for instance, where the transition started in the late 17th century (Figure 1) (Ramos 1993).
THE NEW PUBLIC HEALTH SCENARIO
It is important to realize that such a rapid aging of the population is occurring in a country in which the majority of the population lives under the poverty line.
Journal o[' Cross-Cultural Gerontology 8: 313-323, 1993. �9 1993 Kluwer Academic Publishers. Printed in the Netherlands.
314 LUIZ R, RAMOS ET AL.
0 0 0
o3
n "
4o L
o
30- �9 8irth-BRA
A Mort-BRA 25-
o BirIh-EUR
20- ,~ Mort-EUR
15-
)0-
7725 =~ ,8'2~ ~ ~ ' $ ~:~ ~ ' 1925 ~ 2025
Y E A R sou,c,: RaMos 1987
Fig. 1. Demographic transition: Secular trends of mortality and birth rates in Europe and Brazil (1725-2025).
Therefore, on the one hand problems like malnutrition and avoidable deaths due to infectious diseases are far from being eradicated while on the other hand, cardiovascular diseases have been, for more than a decade, the leading cause of death even in the poorest regions of the country. Infectious diseases that in the 1930s, for instance, were responsible for more than 40% of the total deaths, nowadays account for less than 8%, whereas cardiovascular diseases, that were formerly responsible for only 12% of the deaths now account for more than
35%. As the majority of the population is living to older ages and chronic diseases
become the main causes of death, one should expect drastic changes in the dynamics of health and social care. In a young population with high infant mortality rates the main causes of death are usually infectious diseases that have a very specific outcome as far as the health care system is concerned. A child with pneumonia and diarrhoea seeking medical care, for example, can generate one out of two possible scenarios: effective treatment is given and the outcome is cure or the system is terribly ineffective and the outcome is death. Both outcomes take place in an average period of 15 days, and both release the system of any further obligation towards that patient.
In an aged population the situation can be rather different. A 60 year old who discovers that he or she has diabetes and hypertension, for instance, can expect neither cure nor rapid death. If effective treatment is given, both diseases can be kept under control but require constant monitoring and daily treatment for a period that can easily exceed 20 years. If treatment is ineffective or unavailable,
DISABILITY AMONG URBAN ELDERLY IN BRAZIL 315
the patient will probably develop disabilities and, in such a case, will not live 20 years more but might live another 10 years, demanding, however, more intensive, sophisticated and, of course, expensive treatment.
THE ROLE OF DISABILITY
Williams (1979) has defined disability as a decline or loss of capacity to perform ordinary activities of daily living resulting from impaired functioning of an organ or limb (due to accident or disease). Disability usually generates depen- dency which should not be seen as synonymous with lack of autonomy. As pointed out by Grimley-Evans (1984) autonomy relates to self-determination regarding activies of everyday life, whereas dependency reflects the inability to perform them unaided.
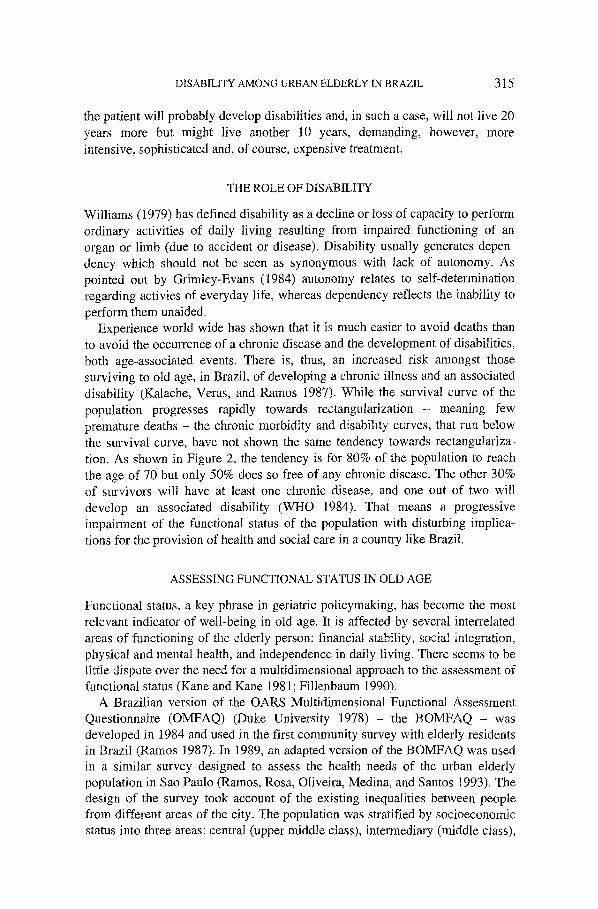
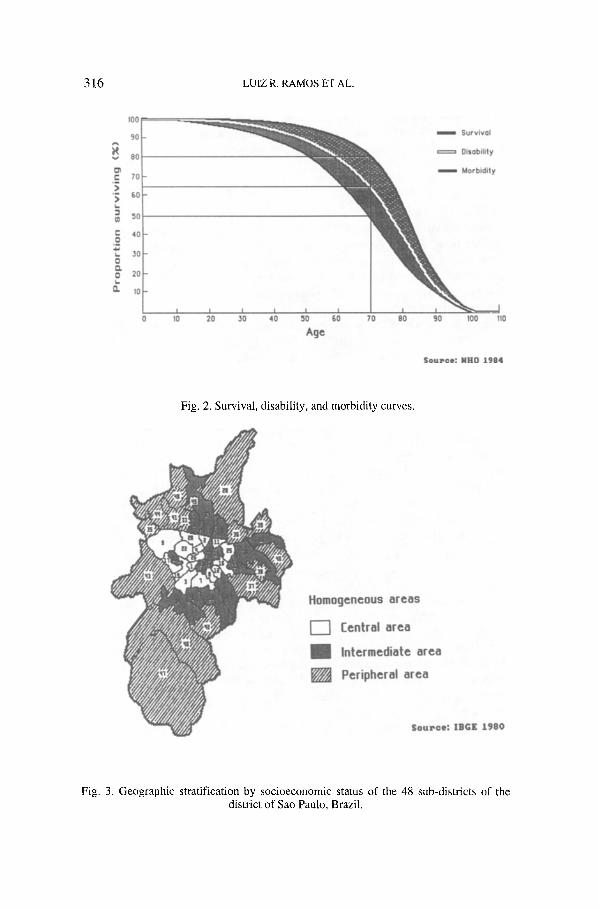
Experience world wide has shown that it is much easier to avoid deaths than to avoid the occurrence of a chronic disease and the development of disabilities, both age-associated events. There is, thus, an increased risk amongst those surviving to old age, in Brazil, of developing a chronic illness and an associated disability (Kalache, Veras, and Ramos 1987). While the survival curve of the population progresses rapidly towards rectangularization - meaning few premature deaths - the chronic morbidity and disability curves, that run below the survival curve, have not shown the same tendency towards rectangulariza- tion. As shown in Figure 2, the tendency is for 80% of the population to reach the age of 70 but only 50% does so free of any chronic disease. The other 30% of survivors will have at least one chronic disease, and one out of two will develop an associated disability (WHO 1984). That means a progressive impairment of the functional status of the population with disturbing implica- tions for the provision of health and social care in a country like Brazil.
ASSESSING FUNCTIONAL STATUS IN OLD AGE
Functional status, a key phrase in geriatric policymaking, has become the most relevant indicator of well-being in old age. It is affected by several interrelated areas of functioning of the elderly person: financial stability, social integration, physical and mental health, and independence in daily living. There seems to be little dispute over the need for a multidimensional approach to the assessment of functional status (Kane and Kane 1981; Fillenbaum 1990).
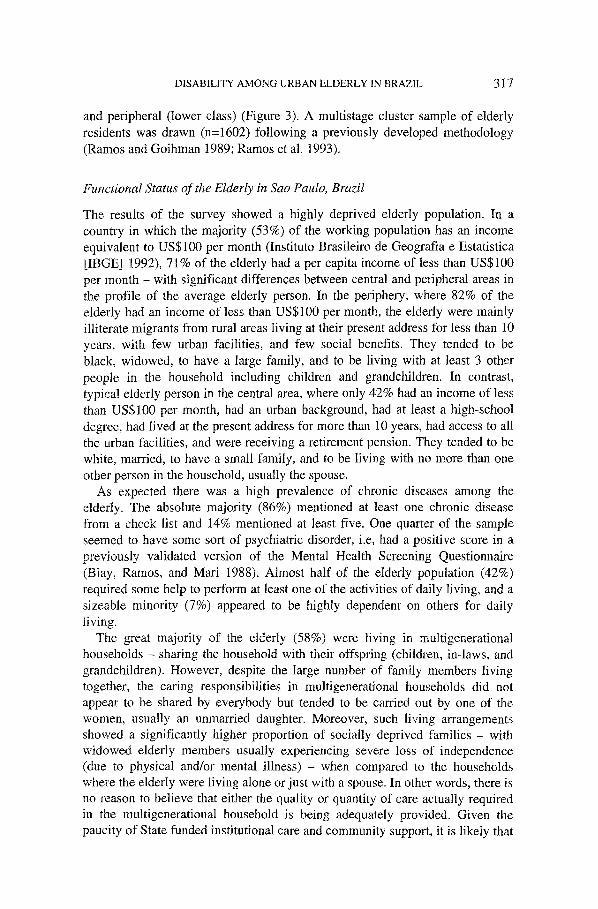
A Brazilian version of the OARS Multidimensional Functional Assessment Questionnaire (OMFAQ) (Duke University 1978) - the BOMFAQ - was developed in 1984 and used in the first community survey with elderly residents in Brazil (Ramos 1987). In 1989, an adapted version of the BOMFAQ was used in a similar survey designed to assess the health needs of the urban elderly population in Sao Paulo (Ramos, Rosa, Oliveira, Medina, and Santos 1993). The design of the survey took account of the existing inequalities between people from different areas of the city. The population was stratified by socioeconomic status into three areas: central (upper middle class), intermediary (middle class),
316 LUIZ R. RAMOS ET AL.
tO0
9O
80
r- 70 >
' ~ 60
O~ 50
e- 40 O
.io s0
20
t I I I / / ~ _ _ _ . _ _ . ~ . _ _ JO 20 30 40 50 60 70 80
Age
~ m Survival
Disability
~ m m Morbidi ty
90 100 110
S o u r c e : N H O 1 9 8 4
Fig. 2. Survival, disability, and morbidity curves.
Homogeneous areas
~ -~ Central area
Intermediate area
Peripheral area
S o u r c e : I B G E 1 9 8 0
Fig. 3. Geographic stratification by socioeconomic status of the 48 sub-districts of the district of Sao Paulo, Brazil.
DISABILITY AMONG URBAN ELDERLY IN BRAZIL 317
and peripheral (lower class) (Figure 3). A multistage cluster sample of elderly residents was drawn (n=1602) following a previously developed methodology (Ramos and Goihman 1989; Ramos et al. 1993).
Functional Status of the Elderly in Sao Paulo, Brazil
The results of the survey showed a highly deprived elderly population. In a country in which the majority (53%) of the working population has an income equivalent to US$100 per month (Instituto Brasileiro de Geografia e Estatistica [IBGE] 1992), 71% of the elderly had a per capita income of less than US$100 per month - with significant differences between central and peripheral areas in the profile of the average elderly person. In the periphery, where 82% of the elderly had an income of less than US$100 per month, the elderly were mainly illiterate migrants from rural areas living at their present address for less than 10 years, with few urban facilities, and few social benefits. They tended to be black, widowed, to have a large family, and to be living with at least 3 other people in the household including children and grandchildren. In contrast, typical elderly person in the central area, where only 42% had an income of less than US$100 per month, had an urban background, had at least a high-school degree, had lived at the present address for more than 10 years, had access to all the urban facilities, and were receiving a retirement pension. They tended to be white, married, to have a small family, and to be living with no more than one other person in the household, usually the spouse.
As expected there was a high prevalence of chronic diseases among the elderly. The absolute majority (86%) mentioned at least one chronic disease from a check list and 14% mentioned at least five. One quarter of the sample seemed to have some sort of psychiatric disorder, i.e, had a positive score in a previously validated version of the Mental Health Screening Questionnaire (Blay, Ramos, and Mari 1988). Almost half of the elderly population (42%) required some help to perform at least one of the activities of daily living, and a sizeable minority (7%) appeared to be highly dependent on others for daily living.
The great majority of the elderly (58%) were living in multigenerational households - sharing the household with their offspring (children, in-laws, and grandchildren). However, despite the large number of family members living together, the caring responsibilities in multigenerational households did not appear to be shared by everybody but tended to be carried out by one of the women, usually an unmarried daughter. Moreover, such living arrangements showed a significantly higher proportion of socially deprived families - with widowed elderly members usually experiencing severe loss of independence (due to physical and/or mental illness) - when compared to the households where the elderly were living alone or just with a spouse. In other words, there is no reason to believe that either the quality or quantity of care actually required in the multigenerational household is being adequately provided. Given the paucity of State funded institutional care and community support, it is likely that
318 LUIZ R. RAMOS ET AL.
those living in multigenerational households are doing so less because of cultural and emotional preferences than because there are no alternatives (Ramos 1992).
MEASURING DEPENDENCY IN OLD AGE
Of all the variables affecting the personal functioning of the elderly, dependency is perhaps the single most important. Researchers and administrators have been concerned with determining the degree of dependency in order to assess whether it is feasible for the individual to live in the community. This concern has contributed to the development of numerous scales (Lawton and Brody 1969; Katz 1983; Fillenbaum 1985) that measure independence in three domains: mobility, personal care, and house care capacities. As suggested by Katz, Ford, Moskowitz, Jackson, and Jaffe (1963) in a pioneer study, the activities of daily living are hierarchically related and reflect the developmental patterns found in children and possibly in reverse order, the regression during the natural process of aging.
Hierarchical Dependency
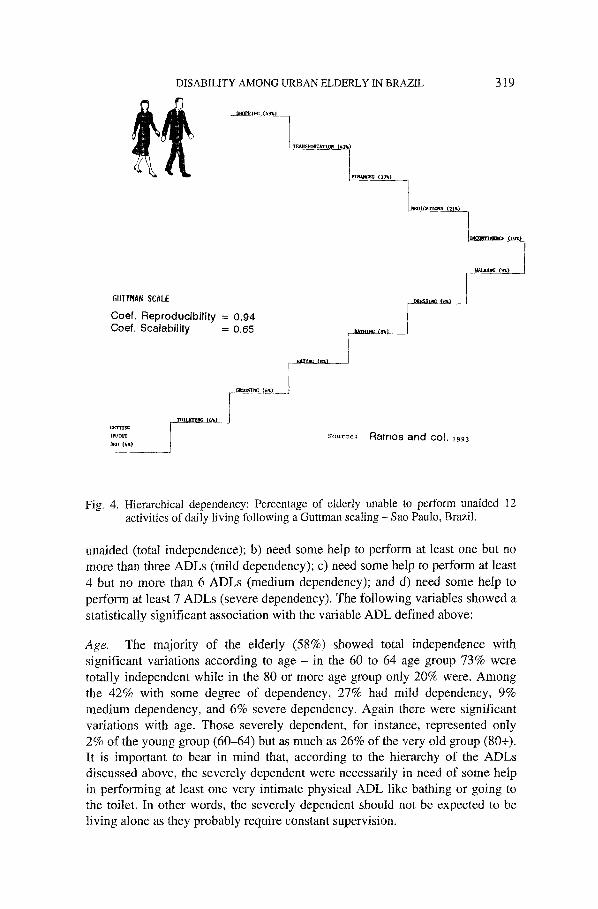
The results of the survey in Sao Paulo have confirmed this hierarchical loss of independence among the aged. A dependency ladder was constructed based on the scaling technique developed by Guttman (1950) (Figure 4). The scale shows that the person first loses the ability to perform instrumental activities of daily living - shopping, getting a bus, caring for finances, and taking medicines properly, in this order. A sizeable proportion of the elderly population requires some help to perform at least one of these activities, namely shopping (49%).
Only after the instrumental activities have been affected are the physical activities of daily living supposed to be affected. At this stage, the person loses the ability to be continent, walk on a flat surface, dress, bathe, eat, groom, go to the toilet, and get in and out of bed, in this order. Although only less than 10% of the elderly actually required some help to perform these activities, they represent a high risk group, as they usually cannot live alone anymore and probably have associated physical and mental diseases.
It is worth mentioning that there are some sex differences in the way people go down the ladder of dependency. Men lose early the ability to dress and groom themselves without help but tend to remain continent and able to walk, whereas women become incontinent and unable to walk much earlier, but grooming is the last activity that they actually require help to perform.
Dependency Associated Factors
In order to understand the factors associated with dependency in daily life the elderly were divided into four categories regarding the ability to perform the 12 activities of daily living (ADL) discussed above: a) able to perform all the ADLs
DISABILITY AMONG URBAN ELDERLY IN BRAZIL 319
6UHMAN SCALE
Coef. Reproducibi l i ty = 0 ,g4 Coef. Scalabil ity = 0.65
I./r~rl" Source; R a m o s a n d co l . 1993
V-
Fig. 4. Hierarchical dependency: Percentage of elderly unable to perform unaided 12 activities of daily living following a Guttman scaling - Sao Paulo, Brazil.
unaided (total independence); b) need some help to perform at least one but no more than three ADLs (mild dependency); c) need some help to perform at least 4 but no more than 6 ADLs (medium dependency); and d) need some help to perform at least 7 ADLs (severe dependency). The following variables showed a statistically significant association with the variable ADL defined above:
Age. The majority of the elderly (58%) showed total independence with significant variations according to age - in the 60 to 64 age group 73% were totally independent while in the 80 or more age group only 20% were. Among the 42% with some degree of dependency, 27% had mild dependency, 9% medium dependency, and 6% severe dependency. Again there were significant variations with age. Those severely dependent, for instance, represented only 2% of the young group (60-64) but as much as 26% of the very old group (80+). It is important to bear in mind that, according to the hierarchy of the ADLs discussed above, the severely dependent were necessarily in need of some help in performing at least one very intimate physical ADL like bathing or going to the toilet. In other words, the severely dependent should not be expected to be living alone as they probably require constant supervision.
320 LUIZ R. RAMOS ET AL.
Sex. Women showed more dependence in daily living than men - 52% of the women showed some degree of dependency against only 25% of the men. This higher dependency of women is more obvious in the mild and medium depen- dency groups - 33% against 15% and 12% against 5% respectively. In the severely dependent group the difference is smaller - 7% against 5%. This relative overrepresentation of men in the last group in comparison to the others might suggest that the transition from total independence to total dependence is more abrupt among men.
Household Structure. With regard to the household structure, the elderly living in three-generational households were consistently more dependent than those living in other arrangements - only 49% of those living in three-generational households were totally independent whereas this proportion increased to 58% among those in two-generational households, to 60% among those living alone, and to 64% among those in one-generational households. Although the one- generational households seemed to contain the more independent elderly people, those living alone showed the lowest proportion of severely dependent - 4.5% compared to 5% among those in one, 6% among those in two, and 9% among those in three-generational households.
In a country with virtually no formal home help and community services for the elderly and with only private long term care institutions, those living alone have to be relatively fit. Should their degree of dependency increase the tendency is to cohabit with married children. In a sense, the three-generational household might be seen as the community institution for the deprived elderly.
Chronic Diseases. Dependency in daily living in old age was strongly as- sociated with poor mental and physical health. Of those with a mental health problem (27%), almost two-thirds had some degree of dependency (65%) and more than one in ten showed severe dependency (11%). Among the healthy minority free of any physical chronic diesease (14%), the absolute majority (83%) showed total independence and only 2% had a severe dependency. Conversely, among the particularly unhealthy minority mentioning at least 5 chronic diseases (14%), the majority showed some degree of dependency (64%) and one out of ten had severe dependency.
Although the majority of the elderly had at least one chronic illness, they did not necessarily have an associated disability. In fact, in 46% of the cases there was at least one chronic disease but no associated disability. In all, only 12% of the elderly were free of disability and free of chronic illness. Interestingly enough, however, there was a very small minority (2%) that despite not having any chronic illness did show a degree of dependency. This proportion of 'healthy disabled' increased significantly with age - it varied from 0.8% among the 60 to 64 age group to 12% among the 80+ age group. Even controlling for mental illness, hearing and visual impairments, there was still a number of 'healthy disabled' among the very old, suggesting that, despite the possible lack of diagnosis opportunities, something other than disease can actually determine
DISABILITY AMONG URBAN ELDERLY tN BR AZIL 32 t
some degree of dependency. A possible explanation for this finding would be increased age-determined frailty, affecting the ability of a naturally selected cohort of healthy aged to perform daily activities. Health care in these cases ought to be mainly physical therapy.
Falls. Among those who have had at least one fall in the previous year (31%), more than half (54%) were in need of some help to perform at least one ADL - 33% of the mild, 13% of the medium, and 8% of severely dependent.
Hospital Care. The results of the survey in Sao Paulo reveal, for instance, that those with some degree of dependence have demanded significantly more hospital care. While only 8% of the elderly in the total sample had been in hospital at least once in the previous 12 months, among those with medium or severe dependency this proportion goes up to 18%.
DISCUSSION
Care for the elderly is an emerging priority for Brazil. A growing number of people will be reaching old age and, therefore, be at an increased risk of moving from a good functional status to a poor functional status. The consequences of that move can be devastating both to the elderly person and to the health and social care systems.
Several factors, apart from age itself, can cause the deterioration of the functional status of an aging person: accidents, physical illness and mental illness. As the survey data indicate, all these factors tend to be highly prevalent in old age. Not surprisingly a sizeable proportion of the elderly population was in need of rehabilitation and care. Care includes health education, various treatments and therapies, prostheses, as well as formal and informal care in the community. If at all available, these procedures and services might well promote a full recovery, but such is not the usual outcome. More often than not, an aged person has a partial recovery and a chronic demand for services and care. The main problem, however, concerns the cases in which no recovery is obtained and one out three possible outcomes has to be faced: death (a relatively easy way out); institutionalization (often not available or not affordable in countries like Brazil); or a community ordeal. The last tend to be the most common outcome in cases in which functional status deteriorates in a country that still relies heavily on the family for the care of the elderly. Very little has been invested so far in preventive measures and in long term surveillance of chronic conditions affecting the aged.
The promotion of well-being in old age is a function of the preservation of a good functional status that depends on the availability of a full range of services prepared to provide home care, community support, specialized outpatient care, and hospital and institutional beds. The availability of such services very much depends on economic resources, cultural values, social consciousness, political awareness, and the type of health system. Brazil's national health system is still,
322 LUIZ R. RAMOS ET AL.
however, very much geared towards the care of children. There are few resources, no social consciousness, and only palliative policies regarding the well-being of the elderly population. Fortunately, cultural values are still keeping the family on the front line of caregiving, but this situation is not likely to withstand the increasing burden generated by the growing proportion of elderly with increasing life expectancy and ever higher rates of dependency.
ACKNOWLEDGEMENTS
The researchers are thankful to the Panamerican Health Organization (PAHO), the World Banks' Metropolitan Health Program of Sao Paulo, the National Research Council (CNPQ), and the Research Funding Agency of the State of Sao Paulo (FAPESP) for the funding.
REFERENCES
Blay, S., L.R. Ramos, and J.J. Mari 1988 Validity of a Brazilian Version of the Older American Resources and Services (OARS) Mental Health Screening Questionnaire. Journal of the American Geriatric Society 36:687-692.
Duke University Center for the Study of Aging and Human Development 1978 Multi- dimensional Functional Assessment: The OARS Methodology. Durham, N.C.: Duke University.
Fillenbaum, G.G. 1985 Screening the Elderly: A Brief Instrumental ADL Measure. Journal of the American Geriatric Society 33:698-706.
Fillenbaum, G.G. 1990 Assessment of Health and Functional Status; An International Comparison. In: Improving the Health of Older People: A World View. R.L. Kane, J. Grimley-Evans, and D. Macfadyen, eds. Pp. 69-90. Oxford: Oxford University Press.
Grimley-Evans, J. 1982 Prevention of Age Associated Loss of Autonomy: Epidemiologi- cal Approaches. Journal of Chronic Diseases 37(5):353-363.
Guttman, A. 1950 The Basis of Scalogram Analysis. In: Measurement and Prediction. S.A. Stouffer, ed. Princeton University Press, New York.
IBGE - Fundacao Instituto Brasileiro de Geografia e Estatistica 1993 Anuario Estatistico do Brasil: 1992. Rio de Janeiro: IBGE
IBGE - Fundacao Instituto Brasileiro de Geografia e Estatistica 1980 Censo Demografico de Sao Paulo. Recenseamento Geral do Brasil IX Tomo I No. 19, Rio de Janeiro.
Kalache, A. R., Veras, and L.R. Ramos 1987 Ageing of the World Population: A New Challenge. Revista de Saude Publica 21 (3):200--210.
Kane, R.A., and R.L. Kane 1981 Assessing the Elderly: A Practical Guide to Measure- ment. Toronto: Lexington Books.
Katz, S. 1983 Assessing Self-Maintenance: Activities of Daily Living, Mobility, and Instrumental Activities of Daily Living. Journal of the American Geriatric Society 31:721-727.
Katz, S., A.B. Ford, R.W. Moskowitz, B.A. Jackson, M.W. Jaffe 1963 Studies of Illness in the Aged - the Index of ADL: A Standardized Measure of Biological and Psychoso- cial Function, Journal of the American Medical Association 185 (12):914-919.
Lawton, M.P., and E.M. Brody 1969 Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. The Gerontologist 9:179-186.
Ramos, L.R. 1987 Growing Old in Sao Paulo, Brazil: Assessment of Health Status and Family Support of the Elderly of Different Socioeconomic Strata Living in the

DISABILITY AMONG URBAN ELDERLY IN BRAZIL 323
Community. Ph.D. Thesis, University of London. Ramos, L.R. 1992 Family Support for the Elderly in Sao Paulo, Brazil. In Family Support
for the Elderly: The International Experience. H. Kendig, A, Hashimoto, and L. Coppard, eds. Pp. 224-232. Oxford: Oxford University Press.
Ramos, L.R. 1993 Brazil. In Developments and Research on Aging: An International Handbook. E. Palmore, ed. Pp. 2540. Westport: Greenwood Publishing Group.
Ramos, L.R., R. Veras, and A. Kalache 1987 Populational Ageing: A Brazilian Reality. Revista de Saude Publica 21(3):211-224.
Ramos, L.R., and S. Goihman 1989 Geographic Stratification by Socioeconomic Status: Methodology from a Household Survey with Elderly People in San Paulo, Brazil. Revista de Sande Publica 23(6):478492.
Ramos, L.R., T.E.C. Rosa, Z.M. Oliveira, M.C.G. Medina, F.R.G. Santos 1993 Multi- dimensional Profile of the Resident Elderly in the District of San Paulo: Results from a Household Survey and its Implications for Health Planning. Revista de Sande Publica 27(2):87-94.
Williams, R,G.A. 1979 Theories and Measurement of Disability. Journal of Epidemiologi- cal Community Health 33:32-47.
World Health Organization 1984 The Uses of Epidemiology in the Study of the Elderly. Technical Report Series 706, WHO, Geneva.
Center for the Study of Aging Escola Paulista de Medicina Rua dos Ottonis 731 04025-002 - Sao Paulo, Brazil