Short-term Results after Robot-assisted Laparoscopic Radical Prostatectomy Compared to Open Radical...
11
Platinum Priority – Prostate Cancer Editorial by Prokar Dasgupta on pp. 671–672 of this issue Short-term Results after Robot-assisted Laparoscopic Radical Prostatectomy Compared to Open Radical Prostatectomy Anna Wallerstedt a, *, Stavros I. Tyritzis a , Thordis Thorsteinsdottir b,c , Stefan Carlsson a , Johan Stranne d , Ove Gustafsson e , Jonas Hugosson d , Anders Bjartell f , Ulrica Wildera ¨ng b , N. Peter Wiklund a , Gunnar Steineck b,g , Eva Haglind h , on behalf of the LAPPRO steering committee a Department of Molecular Medicine and Surgery, Section of Urology, Karolinska Institutet, Solna, Stockholm, Sweden; b Division of Clinical Cancer Epidemiology, Department of Oncology, Institute of Clinical Sciences, Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden; c Faculty of Nursing, School of Health Sciences, University of Iceland, Reykjavik, Iceland; d Department of Urology, Institute of Clinical Sciences, Sahlgrenska Academy at the University of Gothenburg, Sahlgrenska University Hospital, Gothenburg, Sweden; e Department of Clinical Science, Intervention and Technology, Karolinska Institutet, Solna, Stockholm, Sweden; f Department of Urology, Ska ˚ne University Hospital, Lund University, Lund, Sweden; g Department of Oncology and Pathology, Division of Clinical Cancer Epidemiology, Karolinska Institutet, Solna, Stockholm, Sweden; h Department of Surgery, Institute of Clinical Sciences, Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden EUROPEAN UROLOGY 67 (2015) 660–670 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted September 23, 2014 Keywords: Radical prostatectomy Open Robot-assisted Complications Short-term results Abstract Background: Robot-assisted laparoscopic radical prostatectomy has become a wide- spread technique despite a lack of randomised trials showing its superiority over open radical prostatectomy. Objective: To compare in-hospital characteristics and patient-reported outcomes at 3 mo between robot-assisted laparoscopic and open retropubic radical prostatectomy. Design, setting, and participants: A prospective, controlled trial was performed of all men who underwent radical prostatectomy at 14 participating centres. Validated patient questionnaires were collected at baseline and after 3 mo by independent health-care researchers. Outcome measurements and statistical analysis: The difference in outcome between the two treatment groups were analysed using logistic regression analysis, with adjustment for identified confounders. Results and limitations: Questionnaires were received from 2506 (95%) patients. The robot-assisted surgery group had less perioperative bleeding (185 vs 683 ml, p <0.001) and shorter hospital stay (3.3 vs 4.1 d, p < 0.001) than the open surgery group. Operating time was shorter with the open technique (103 vs 175 min, p < 0.001) compared with the robot-assisted technique. Reoperation during initial hospital stay was more frequent after open surgery after adjusting for tumour characteristics and lymph node dissection (1.6% vs 0.7%, odds ratio [OR] 0.31, 95% confidence interval [CI 95%] 0.11–0.90). Men who underwent open surgery were more likely to seek healthcare (for one or more of 22 specified disorders identified prestudy) compared to men in the robot-assisted surgery group ( p = 0.03). It was more common to seek healthcare for cardiovascular reasons in the open surgery group than in the robot-assisted surgery group, after adjusting for nontumour and tumour-specific confounders, (7.9% vs 5.8%, OR 0.63, CI 95% 0.42–0.94). The readmittance rate was not statistically different between the * Corresponding author. Department of Molecular Medicine and Surgery, Section of Urology, Karolinska Institutet, Solna, Stockholm, Sweden. E-mail address: [email protected] (A. Wallerstedt). http://dx.doi.org/10.1016/j.eururo.2014.09.036 0302-2838/# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
-
Upload
karolinska -
Category
Documents
-
view
2 -
download
0
Transcript of Short-term Results after Robot-assisted Laparoscopic Radical Prostatectomy Compared to Open Radical...

E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0
avai lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Platinum Priority – Prostate CancerEditorial by Prokar Dasgupta on pp. 671–672 of this issue
Short-term Results after Robot-assisted Laparoscopic Radical
Prostatectomy Compared to Open Radical Prostatectomy
Anna Wallerstedt a,*, Stavros I. Tyritzis a, Thordis Thorsteinsdottir b,c, Stefan Carlsson a,Johan Stranne d, Ove Gustafsson e, Jonas Hugosson d, Anders Bjartell f, Ulrica Wilderang b,N. Peter Wiklund a, Gunnar Steineck b,g, Eva Haglind h,
on behalf of the LAPPRO steering committee
a Department of Molecular Medicine and Surgery, Section of Urology, Karolinska Institutet, Solna, Stockholm, Sweden; b Division of Clinical Cancer
Epidemiology, Department of Oncology, Institute of Clinical Sciences, Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden; c Faculty of
Nursing, School of Health Sciences, University of Iceland, Reykjavik, Iceland; d Department of Urology, Institute of Clinical Sciences, Sahlgrenska Academy at
the University of Gothenburg, Sahlgrenska University Hospital, Gothenburg, Sweden; e Department of Clinical Science, Intervention and Technology,
Karolinska Institutet, Solna, Stockholm, Sweden; f Department of Urology, Skane University Hospital, Lund University, Lund, Sweden; g Department of
Oncology and Pathology, Division of Clinical Cancer Epidemiology, Karolinska Institutet, Solna, Stockholm, Sweden; h Department of Surgery, Institute of
Clinical Sciences, Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden
Article info
Article history:Accepted September 23, 2014
Keywords:
Radical prostatectomy
Open
Robot-assisted
Complications
Short-term results
Abstract
Background: Robot-assisted laparoscopic radical prostatectomy has become a wide-spread technique despite a lack of randomised trials showing its superiority over openradical prostatectomy.Objective: To compare in-hospital characteristics and patient-reported outcomes at3 mo between robot-assisted laparoscopic and open retropubic radical prostatectomy.Design, setting, and participants: A prospective, controlled trial was performed of allmen who underwent radical prostatectomy at 14 participating centres. Validatedpatient questionnaires were collected at baseline and after 3 mo by independenthealth-care researchers.Outcome measurements and statistical analysis: The difference in outcome between thetwo treatment groups were analysed using logistic regression analysis, with adjustmentfor identified confounders.Results and limitations: Questionnaires were received from 2506 (95%) patients. Therobot-assisted surgery group had less perioperative bleeding (185 vs 683 ml, p <0.001)and shorter hospital stay (3.3 vs 4.1 d, p< 0.001) than the open surgery group. Operatingtime was shorter with the open technique (103 vs 175 min, p < 0.001) compared withthe robot-assisted technique. Reoperation during initial hospital stay was more frequentafter open surgery after adjusting for tumour characteristics and lymph node dissection(1.6% vs 0.7%, odds ratio [OR] 0.31, 95% confidence interval [CI 95%] 0.11–0.90). Men whounderwent open surgery were more likely to seek healthcare (for one or more of22 specified disorders identified prestudy) compared to men in the robot-assistedsurgery group ( p = 0.03). It was more common to seek healthcare for cardiovascularreasons in the open surgery group than in the robot-assisted surgery group, afteradjusting for nontumour and tumour-specific confounders, (7.9% vs 5.8%, OR 0.63, CI95% 0.42–0.94). The readmittance rate was not statistically different between the
r. Department of Molecular Medicine and Surgery, Section of Urology,lna, Stockholm, Sweden.
* Corresponding authoKarolinska Institutet, So
E-mail address: anna.wallehttp://dx.doi.org/10.1016/j.eururo.2014.09.0360302-2838/# 2014 European Association of Urology. Published by Elsevier
[email protected] (A. Wallerstedt).
B.V. All rights reserved.

groups. A limitation of the study is the lack of a standardised tool for the assessment ofthe adverse events.Conclusions: This large prospective study confirms previous findings that robot-assistedlaparoscopic radical prostatectomy is a safe procedure with some short-term advantagescompared to open surgery. Whether these advantages also include long-term morbidityand are related to acceptable costs remain to be studied.Patient summary: We compare patient-reported outcomes between two commonlyused surgical techniques. Our results show that the choice of surgical technique mayinfluence short-term outcomes.
# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0 661
1. Introduction
Surgery-induced problems in the short term may cause
suffering for the patient and increased costs for the health
care system. Arguments for the introduction of laparoscopic
techniques include the contention that a smaller wound, as
compared to that produced by open surgery, would result in
less bleeding and fewer infections as well as a shorter length
of hospital stay. Evolving data supporting these assump-
tions and experiences suggest that the same pattern may
hold for robot-assisted laparoscopic radical prostatectomy
as compared with open surgery [1–3].
There are currently no large prospective studies com-
paring the short-term results of robot-assisted laparoscopic
prostatectomy and open radical prostatectomy. The mag-
nitude of the probable improvement in short-term outcomes
through use of the robot-assisted technique is, therefore, still
unknown, as is the effect on short-term outcomes other than
infections, bleeding, and length of hospital stay [4,5].
In order to assess potential differences between the two
types of procedure, we initiated a prospective controlled
trial at 14 centres in Sweden performing radical prostatec-
tomy, collecting information from both health-care profes-
sionals and patients. The aim of this study was to report the
frequency of certain prespecified short-term results and
adverse events after both robot-assisted laparoscopic
radical prostatectomy and open retropubic radical prosta-
tectomy, and to investigate potential differences between
the two procedures.
2. Patients and methods
2.1. Overview
This prospective controlled trial, LAPPRO (Laparoscopic Prostatectomy
Robot Open), recruited patients from seven centres using the robot-
assisted approach and seven centres performing open surgery. Patient-
reported data were collected before and 3 mo after surgery by a neutral
third-party trial secretariat. Health-care professionals completed clinical
record forms before, during, and 1.5–3 mo, 12 mo, and 24 mo after
surgery. The time point for measuring adverse events on patient reports
was set at 3 mo postoperatively. Further details can be found in the
publication describing the study [6] and in the protocol available
on www.ssorg.net. The Regional Ethical Review Board in Gothenburg
(No 277-07) approved the study. The trial is registered in the Current
Controlled Trials database (ISRCTN06393679).
LAPPRO is an external scientific review of the two surgical
techniques, as neither the principal investigator (E.H.) nor the deputy
principal investigator (G.S.) is a urologist and neither performs radical
prostatectomies. The prespecified statistical analysis plan is available as
supplementary material.
2.2. Patients
To avoid problems due to physician selection, we aimed to collect
data from all men diagnosed with prostate cancer and planned for
radical prostatectomy at the 14 participating centres from September 1,
2008 to November 7, 2011. For a majority of those participating,
geographical residency decided the technique used, not patient or
surgeon preferences. For this report, the inclusion criteria were age <75
yr, ability to read and write Swedish, informed consent, tumour stage
cT1, cT2, or cT3 (TNM Classification of Malignant Tumors) [7] with no
signs of distant metastases, and a prostate-specific antigen level of <20
ng/ml. To diminish the influence of the learning curve, we only included
men who were operated on by a surgeon with experience of at least
100 procedures as primary surgeon.
2.3. Data collection
The study-specific clinical record forms were tested face-to-face with
relevant health-care professionals. The study questionnaires reporting
patient outcomes have the same clinometric approach as a previous
randomised controlled trial, and more than 20 large data collections of
cancer survivors [8]. The basic idea was to categorise symptoms and
other phenomena by asking questions about them one by one [9]. The
validation of the questionnaires and the pilot study performed before the
start of the study has been described earlier [6]. During the trial, research
nurses and surgeons filled out the clinical record forms. The centres were
regularly asked to supply missing information and to check suspected
outliers. Two research nurses monitored the recruiting sites. The
preoperative questionnaire was given to the patient before surgery
and collected at the recruiting departments. The 3-mo questionnaires
were sent from the trial secretariat [6] (Table 1).
At 3 mo, we asked ‘‘Have you been readmitted to the hospital after the
surgery?’’ with answer categories ‘‘Yes’’ and ‘‘No’’. The patient could then
specify in free text the reason for readmittance. This information was
classified into different groups in a blinded fashion (Table 2). The question
‘‘Have you sought medical care because of any of the following disorders
after surgery?’’ had 22 specified disorders as answer categories, followed
by ‘‘Yes’’ and ‘‘No’’ options. From this question, we calculated the
probability of seeking health care by dichotomising between ‘‘never’’ and
‘‘once or more’’.
During the recruitment period, a number of quality assurance efforts
were made regarding the data. The information was entered manually
into electronic files. Approximately 1% of the records and questionnaires
were entered twice and compared.
2.4. Statistical analysis
The statistical analysis plan defines the outcomes for this article, effect
measures, and possible confounders and mediators, as well as certain

Table 1 – Baseline characteristics of the patients a,d
Variable Open surgery b
(n = 778)Robot-assisted surgery c
(n = 1847)p value
Age at surgery (yr)
Median 63 (42–75) 63 (37–75) 0.03
Quartiles 59–67 58-66
Educational level, n (%)
University/college (>13 yr in school) 246 (35.5) 691 (42.4) 0.009
Technical training school (12–13 yr in school) 80 (11.5) 184 (11.3)
High school (10–12 yr in school) 208 (30.0) 462 (28.3)
Elementary school (�9 yr in school) 143 (20.6) 254 (15.6)
Other 14 (2.0) 30 (1.8)
Not stated 3 (0.4) 9 (0.6)
ASA e classification number, n (%)
I 508 (66.6) 1113 (60.4) 0.005
II 218 (28.6) 646 (35.0)
III 15 (2.0) 43 (2.3)
Not stated 22 (2.9) 42 (2.3)
Body mass index (kg/m2)
Median (range) 26.2 (18.2–38.2) 25.9 (18.8–54.3) 0.03
Quartiles 24.5–28.1 24.1–28.0
Not stated 12 32
Preoperative PSA (ng/ml)
Median (range) 6.2 (0.7–20.0) 6.1 (0.09–20.0) 0.73
Quartiles 4.5–9.0 4.5–8.9
Not stated (n) 19 8
Clinical tumour stage number, n (%)
T1 494 (64.7) 1099 (59.6) 0.006
T2 218 (28.6) 652 (35.4)
T3 27 (3.5) 57 (3.1)
Not stated 24 (3.2) 36 (2.0)
Gleason score biopsy
�7 716 (93.8) 1732 (93.9) 0.72
�8 45 (5.9) 102 (5.5)
Not stated 2 (0.3) 10 (0.5)
Total length of cancer in prostate biopsy (mm)
Median (interquartile range) 7.0 (3.2–14.9) 7.5 (4.0–16.0) 0.03
Not stated (n) 78 92
Postoperative prostate weight, n (%)
0–19 g 4 (0.5) 18 (1.0) 0.003
20–39 g 267 (35.5) 782 (42.9)
40–59 g 334 (44.4) 729 (40.0)
60–79 g 96 (12.8) 209 (11.5)
�80 g 51 (6.8) 86 (4.7)
Neurovascular bundle–preserving procedure, n (%)
Yes 516 (67.8) 1556 (84.4) <0.001
No 244 (32.1) 284 (15.4)
Not stated 1 (0.1) 3 (0.2)
Lymph node dissection, n (%)
Extended 48 (6.3) 162 (8.8) <0.001
Limited 155 (20.4) 63 (3.4)
Not done 554 (72.8) 1607 (87.2)
Not stated 4 (0.5) 11 (0.6)
Median time between surgery and answering of 3-mo questionnaire (mo)
Median (range) 3.1 (3.1–9.3) 3.1 (3.1–12.4) 0.74
Quartiles 3.1–3.1 3.1–3.1
Not stated (n) 88 194
PSA = prostate-specific antigen.a Total may not add up to 100 due to rounding of percentages.b Denotes retropubic radical prostatectomy.c Denotes robot-assisted laparoscopic radical prostatectomy.d No statistical difference was found between the occurrence of diabetes, cardiovascular disease, pulmonary disease, kidney disease, previous abdominal surgery,
and previous transurethral resection of the prostate (TURP).e ASA classification: I = normal healthy patient; II = mild systemic disease; III = severe systemic disease.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0662
sensitivity analyses. A power calculation was done to detect a difference on
the primary endpoint of the LAPPRO study; urinary leakage at 12 mo
(significance level p = 0.05, 80% power, two-sided test). All the outcomes
for the short-term results were defined before the start of the study, which
reduces the risk of differences that arise by chance. However, no
adjustment was made for multiple testing, which is a limitation of the
study.
Missing information on prostate weight was imputed by making a
linear regression model of postoperative prostate weight, as predicted by
preoperative prostate volume among men for whom information was

Table 2 – Possible associated factors for patient-reported readmission to hospital after open surgery and robot-assisted surgery a
Factor Group Readmissions, n (%) RR (95% CI) Age-adjusted RR (95% CI)
Age at surgery
37–59 yr 61 (8.0) 1.0 NA
60–69 yr 135 (9.1) 1.14 (0.85–1.52) NA
70–75 yr 24 (9.3) 1.16 (0.74–1.82) NA
Body mass index (kg/m2)
�30 172 (8.8) 1.0 1.0
>30 19 (8.0) 0.92 (0.58–1.44) 0.91 (0.58–1.44)
Preoperative PSA
<4.5 ng/ml 33 (5.6) 1.0 1.0
4.5–6.1 ng/ml 64 (9.8) 1.75 (1.17–2.62) 1.73 (1.15–2.60)
6.2–9.1 ng/ml 55 (8.4) 1.49 (0.98–2.26) 1.47 (0.96–2.23)
�9.2 ng/ml 63 (10.9) 1.95 (1.30–2.92) 1.89 (1.25–2.85)
Lymph node dissection
No 157 (7.6) 1.0 1.0
Yes 60 (14.2) 1.86 (1.41–2.45) 1.82 (1.38–2.41)
Prostate weight
0–19 g 1 (4.6) 0.66 (0.10–4.53) 0.68 (0.10–4.71)
20–39 g 68 (6.9) 1.0 1.0
40–59 g 100 (9.7) 1.41 (1.05–1.89) 1.38 (1.02–1.86)
60–79 g 26 (8.9) 1.29 (0.84–1.99) 1.25 (0.80–1.93)
�80 g 19 (14.4) 2.08 (1.30–3.35) 1.98 (1.21–3.22)
Clinical tumour stage
T1 115 (7.6) 1.0 1.0
T2 85 (10.2) 1.35 (1.03–1.76) 1.32 (1.01–1.73)
T3 14 (18.2) 2.40 (1.45–3.98) 2.36 (1.43–3.92)
Tumour stage of prostatectomy specimen
pT2 138 (7.9) 1.0 1.0
pT3 71 (10.5) 1.34 (1.02–1.76) 1.32 (1.00–1.74)
pT4 3 (23.1) 2.94 (1.08–8.04) 2.82 (1.02–7.75)
Gleason score for biopsy cores
�7 196 (8.4) 1.0 1.0
�8 18 (12.7) 1.51 (0.96–2.37) 1.44 (0.91–2.28)
Gleason score for pathologic specimen
�7 177 (8.1) 1.0 1.0
�8 25 (15.5) 1.92 (1.31–2.83) 1.88 (1.27–2.79)
IPSS irritative symptoms preoperatively
Mild (0–7) 90 (7.3) 1.0 1.0
Moderate (8–19) 78 (9.5) 1.29 (0.97–1.73) 1.25 (0.94–1.68)
Severe (20–35) 16 (11.2) 1.53 (0.92–2.53) 1.47 (0.89–2.44)
Mental disorder
No 178 (8.3) 1.0 1.0
Yes 15 (19.2) 2.32 (1.44–3.73) 2.48 (1.54–3.98)
RR = relative risk; CI = confidence interval; NA = not applicable; PSA = prostate-specific antigen; IPSS = International Prostate Symptom Score.a Postoperative irradiation, inguinal hernia, transurethral resection of the prostate (TURP), coronary bypass surgery, diabetes, cardiovascular disease, pulmonary
disease, neurologic disease, and kidney disease did not significantly affect the risk of readmission.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0 663
available for both variables. Imputation was performed in R utilizing
Multiple Imputations by Chained Equations (MICE) [10] from a data subset
which included the confounders, but listed as possible confounders only.
The required variables were added to each imputed dataset.
Possible confounders for each endpoint were selected from
20 probable risk factors as the variables statistically significantly
associated ( p <0.20) with each specific outcome in over half of the
imputed datasets. Relative risks were the percentage of patients with
that specific outcome in the robot-assisted laparoscopic group divided by
the percentage of patients with that outcome in the open surgery group.
The unadjusted relative risks were completed using log binomial
regression models, which also provided the 95% confidence intervals
(CI 95%). In addition, we provided odds ratios (OR), modelled by logistic
regression, with the adjusted ratios calculated as a pooled estimate from
the 50 imputed datasets. The calculations were performed using the
GENMOD procedure in SAS 9.3 for Windows (SAS Institute Incorporated,
Cary, NC, USA). To compare the occurrence of possible confounders in
the robot-assisted laparoscopic group with the open-surgery group, we
calculated p values by chi-square test or Wilcoxon rank-sum test, where
appropriate.
In the present study, we report the results unadjusted and after
three different adjustments (A, B, and C), where adjustment A is the
use of stringent confounders which are not likely to affect the surgical
technique differently in the two groups, thus only affecting the
outcome as true confounders (Tables 3, 4 and 5). Adjustment B refers
to all factors in A with the addition of tumour-related factors that are
confounders, but may also be mediating factors, since they may affect
the surgery differently in the respective surgical groups. Adjustment
C refers to A and B with the addition of lymph node dissection, which
should also be considered a confounder, but may also be a mediating
factor due to differences in technique in the respective surgical
groups.
3. Results
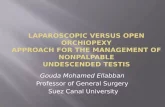
We collected data from 4003 men; 980 were excluded
because their surgeon had performed <100 operations, and
398 were excluded for not meeting inclusion criteria and for
other causes, as stated in the flow chart (Fig. 1). Of

Table 3 – Comparison between open surgery and robot-assisted surgery concerning parameters during hospital stay a
Variable Open surgery b
Mean (range)Median (IQR)
Robot-assisted surgery c
Mean (range)Median (IQR)
p value
Perioperative bleeding (ml) 683 (50–8000)
550 (350–800)
185 (0–5200)
100 (50–200)
<0.001
OR d time (min) 103 (40–428)
89 (74–125)
175 (45–575)
168 (144–201)
<0.001
Time in recovery unit (h) 6.7 (1–90)
4.0 (2.8–7.0)
4.5 (0–45)
4.0 (3.0–5.0)
0.054
Length of hospital stay (d) 4.1 (1–17)
4 (3–5)
3.3 (2–53)
3 (2–4)
<0.001
Open surgery, b
n (%)Robot-assisted
surgery, c
n (%)
Unadjusted RR(CI 95%)
UnadjustedOR (CI 95%)
Adjusted for nontumourconfounders d,e
OR (CI 95%)
Adjusted forA + tumour-specific
confounders f
OR (CI 95%)
Adjusted forA + B + lymph
node dissection g
OR (CI 95%)
Reoperation during
initial hospital stay
8 (1.6) 13 (0.7) 0.47 (0.20–1.13)
0.47 (0.19–1.13) 0.46 (0.19–1.14) 0.32 (0.12–0.90) 0.31 (0.11–0.90)
Mortality during
hospital stay
0 (0) 0 (0) NA NA NA NA
OR time = operating room time ‘‘skin to skin’’; IQR = interquartile range; RR = relative risk; CI = confidence interval; NA = not applicable.a Total may not add up to 100 due to rounding of percentages.b Denotes retropubic radical prostatectomy.c Denotes robot-assisted laparoscopic radical prostatectomy.d Possible confounders to be used in adjustments for each outcome were selected as variables significantly associated (p value <0.20) with the specific outcome.e Adjustment A: employment status preoperatively, postoperative irradiation, previous operation for inguinal hernia, previous transurethral resection of the
prostate (TURP), pulmonary disease, mental disorder, or kidney disease.f Adjustment B: Adjustment A + tumour factors (preoperative prostate-specific antigen level, clinical tumour stage, tumour stage of prostatectomy specimen,
Gleason score on biopsy cores, Gleason score pathology on specimen).g Adjustment C: Adjustment A + B + lymph node dissection.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0664
2625 eligible men, 778 were operated on by open surgery
and 1847 by robot-assisted surgery. Altogether, 2506 (95%)
men were evaluated for short-term results and adverse
events. Table 1 shows the baseline characteristics of the
participants. Men operated on by the robot-assisted
procedure more often had university or college education,
a higher American Society of Anesthesiology Classification
score, higher clinical tumour stages and longer total length
of cancer in the prostate biopsies. Nerve-sparing surgery
was more often done during robot-assisted procedures,
even after adjustment for tumour characteristics. Limited
lymph node dissection was significantly more common
during open procedures, whereas extended lymph node
dissection was more common in the robot-assisted group.
The occurrence of diabetes, cardiovascular disease, pulmo-
nary disease, kidney disease, previous abdominal surgery,
previous transurethral resection of the prostate (TURP), and
mental disorder was not statistically different between the
two groups.
As shown in Table 2, we investigated predictors of
patient-reported readmission to hospital. Factors that
significantly increased the risk of readmission included
preoperative prostate-specific antigen level, lymph node
dissection, prostate weight, clinical tumour stage, tumour
stage of prostatectomy specimen, Gleason score on
pathology specimen, and a history of mental disorder.
No deaths occurred during the hospital stay (Table 3).
Three patients died within 3 mo of surgery in the robot-
assisted laparoscopic group, and no one died in the open
radical prostatectomy group, which resulted in no statisti-
cally significant difference ( p = 0.56). A statistically signifi-
cant difference between the groups was found for the amount
of perioperative bleeding (185 vs 683 ml, p < 0.001) and
length of hospital stay (3.3 vs 4.1 days, p < 0.001), in
favour of the robot-assisted technique. Operating time was
longer in the robot-assisted group compared to the open
technique (103 vs 175 min, p < 0.001). Reoperation during
initial hospital stay was significantly more frequent after
open surgery (1.6%) versus the robot-assisted technique
(0.7%) when adjusting for tumour factors and lymph node
dissection, with OR 0.31 (CI 95% 0.11–0.90) (Table 3).
The adverse events that occurred within 3 mo after the
surgery are presented in five groups: infection, cardiovascu-
lar, surgical, gastrointestinal, and psychological (Table 4).
During the study period, men operated on by the open
technique were more likely to seek healthcare compared to
men operated on by the robot-assisted technique, p = 0.03. It
was significantly more common to seek healthcare for
cardiovascular reasons in the open group after adjusting for
nontumour and tumour-specific confounders (OR 0.63, CI
95% 0.42–0.94). Gastrointestinal and psychological reasons
for seeking health care were significantly more frequent in
the open group (OR 0.77, CI 95% 0.62–0.97 vs OR 0.76, CI 95%
0.60–0.96). The significance was sustained for psychological
reasons after adjusting for nontumour and tumour-specific
confounders (Table 4).
Readmittance within 3 mo was not statistically different
between the techniques (Table 5).

Table 4 – Comparison between open and robot-assisted surgery concerning patient-reported adverse events 3 mo after surgery a
Adverse event Opensurgery, b
n (%)
Robot-assistedsurgery, c
n (%)
UnadjustedRR
(CI 95%)Unadjusted OR
(CI 95%)
Adjusted fornontumour
confounders d,e
OR (CI 95%)
Adjusted forA + tumour-specific
confounders f
OR (CI 95%)
Adjusted forA + B + lymph
node dissection g
OR (CI 95%)
Infection 121 (16.4) 309 (17.6) 1.08 (0.89–1.31)
1.09 (0.87–1.38) 1.03 (0.81–1.32) 0.91 (0.70–1.18) 0.90 (0.69–1.18)
Infection in the
operation wound
42 (5.6) 59 (3.3) – – – –
Pneumonia 5 (0.7) 8 (0.5) – – – –
Urinary tract infection 89 (11.9) 262 (14.8) – – – –
Cardiovascular 58 (7.9) 101 (5.8) 0.74 (0.54–1.01)
0.72 (0.52–1.01) 0.69 (0.47–1.00) 0.63 (0.42–0.94) 0.65 (0.43–1.00)
Pulmonary embolism 6 (0.8) 5 (0.3) – – – –
Hypertension 34 (4.6) 70 (4.0) – – – –
Acute myocardial
infarction
1 (0.1) 2 (0.1) – – – –
Arrhythmia or other
heart diseases
12 (1.6) 24 (1.4) – – – –
Deep venous thrombosis 14 (1.9) 4 (0.2) – – – –
Stroke 0 (0.0) 0 (0.0) – – – –
Surgical 187 (25.2) 392 (22.3) 0.88 (0.76–1.03)
0.85 (0.70–1.04) 0.84 (0.67–1.04) 0.81 (0.64–1.03) 0.85 (0.66–1.08)
Pain in the operation
wound
49 (6.6) 42 (2.4) – – – –
Pain in the lower
abdomen
58 (7.8) 149 (8.4) – – – –
Pain in the upper
abdomen
20 (2.7) 57 (3.2) – – – –
Bleeding from the
operation wound
37 (5.0) 46 (2.6) – – – –
Bleeding from the
urinary tract
66 (8.8) 162 (9.2) – – – –
Inguinal hernia 14 (1.9) 33 (1.9) – – – –
Catheter blockage 58 (7.8) 100 (5.7) – – – –
Gastrointestinal 138 (18.7) 264 (15.1) 0.81 (0.67–0.97)
0.77 (0.62–0.97) 0.78 (0.61–1.01) 0.76 (0.60–1.01) 0.77 (0.58–1.03)
Nausea 17 (2.3) 35 (2.0) – – – –
Impaired appetite 37 (5.0) 64 (3.6) – – – –
Loose or frequent stools 48 (6.4) 99 (5.6) – – – –
Constipation 84 (11.2) 138 (7.8) – – – –
Psychological 122 (16.6) 228 (13.1) 0.79 (0.64–0.97)
0.76 (0.60–0.96) 0.81 (0.62–1.06) 0.72 (0.53–0.96) 0.78 (0.58–1.06)
Depressed mood 92 (12.3) 156 (8.8) – – – –
Worry 94 (12.6) 187 (10.6) – – – –
OR = odds ratio; RR = relative risk; CI = confidence interval.a Total may not add up to 100 due to rounding of percentages.b Denotes retropubic radical prostatectomy.c Denotes robot-assisted laparoscopic radical prostatectomy.d Possible confounders to be used in adjustments for each outcome were selected as variables significantly associated ( p value <0.20) with the specific outcome.e Adjustment A. Readmission adjusted for: employment status preoperatively, International Prostate Symptom Score (IPSS), neurologic disease, mental disorder,
kidney disease, and prostate weight. Infection adjusted for: previous transurethral resection of the prostate (TURP), IPSS, cardiovascular disease, pulmonary disease,
neurologic disease, mental disorder, and prostate weight. Cardiovascular adjusted for: age at surgery, educational level, employment status preoperatively, body
mass index (BMI), IPSS, diabetes, cardiovascular disease, pulmonary disease, mental disorder, prostate weight. Surgical adjusted for: employment status
preoperatively, BMI, IPSS score, IPSS, cardiovascular disease, pulmonary disease, mental disorder, kidney disease, and prostate weight. Gastrointestinal adjusted for:
age at surgery, educational level, employment status preoperatively, BMI, postoperative irradiation, coronary bypass surgery, smoking, IPSS, diabetes,
cardiovascular disease, pulmonary disease, mental disorder, and prostate weight. Psychological adjusted for: age at surgery, educational level, employment status
preoperatively, physical exercise, postoperative irradiation, coronary bypass surgery, smoking, IPSS, mental disorder, and prostate weight.f Adjustment B: Adjustment A + tumour factors (preoperative prostate-specific antigen level, clinical tumour stage, tumour stage of prostatectomy specimen,
Gleason score on biopsy cores, and Gleason score pathology on specimen).g Adjustment C: Adjustment A + B + lymph node dissection.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0 665
4. Discussion
In this prospective controlled trial comparing robot-
assisted laparoscopic and open retropubic radical prosta-
tectomy, we studied short-term results and adverse events
as secondary endpoints defined by patient reports, thus
avoiding any bias that may arise when health-care
personnel with technique preferences assess outcome
[11,12]. The results show that men were more likely to
seek health care within 3 mo after open surgery compared
to robot-assisted surgery. Reoperation during initial hospi-
tal stay was statistically significantly more frequent after

Table 5 – Comparison between open and robot-assisted surgery concerning patient-reported readmissions 3 mo after surgery a
Readmission andreadmission causes
Open surgery, b
n (%)Robot-assisted
surgery, c
n (%)
Unadjusted RR(CI 95%)
Unadjusted OR(CI 95%)
Adjusted fornontumour
confounders d,e
OR (CI 95%)
Adjusted forA + tumour-specific
confounders f
OR (CI 95%)
Adjusted forA + B + lymph
node dissection g
OR (CI 95%)
Readmission 57 (7.7) 163 (9.3) 1.21 (0.91–1.62)
1.23 (0.90–1.69) 1.26 (0.89–1.78) 1.21 (0.83–1.77) 1.39 (0.94–2.06)
Infection 10 (1.3) 37 (2.0) 1.56 (0.78–3.12)
1.57 (0.78–3.17) 1.61 (0.75–3.43) 1.44 (0.64–3.21) 1.68 (0.73–3.85)
UTI 7 (0.9) 21 (1.1) – – – –
Deep infections 2 (0.3) 7 (0.4) – – – –
Sepsis 0 (0.0) 7 (0.4) – – – –
Wound infection 1 (0.1) 2 (0.1) – – – –
Cardiovascular 9 (1.2) 5 (0.3) 0.23 (0.08–0.70)
0.23 (0.08–0.69) 0.32 (0.09–1.16) 0.28 (0.07–1.09) 0.32 (0.08–1.27)
Pulmonary embolism 5 (0.6) 3 (0.2) – – – –
DVT 2 (0.3) 0 (0.0) – – – –
Chest pain 1 (0.1) 1 (0.1) – – – –
AMI 1 (0.1) 1 (0.1) – – – –
Surgical 15 (1.9) 55 (3.0) 1.54 (0.88–2.72)
1.56 (0.88–2.78) 1.54 (0.82–2.87) 1.48 (0.75–2.92) 1.77 (0.87–3.60)
Catheter blockage and
retention after catheter
removal
7 (0.9) 19 (1.0) – – – –
Anastomotic leakage 1 (0.1) 14 (0.8) – – – –
Bleeding 1 (0.1) 9 (0.5) – – – –
Lymphocele 4 (0.5) 3 (0.2) – – – –
Abdominal pain 2 (0.3) 10 (0.5) – – – –
Miscellaneous 4 (0.5) 25 (1.4) 2.63 (0.92–7.54)
2.66 (0.92–7.65) 2.34 (0.78–6.99) 1.63 (0.54–4.96) 1.44 (0.47–4.45)
Operation hernia 0 (0.0) 4 (0.2) – – – –
Other likely related to
procedure
1 (0.1) 13 (0.7) – – – –
Other not likely related
to procedure
2 (0.3) 6 (0.3) – – – –
Psychological 1 (0.1) 2 (0.1) – – – –
Readmission leading to
reoperation
13 (1.7) 29 (1.6) 0.94 (0.49–1.80)
0.94 (0.49–1.82) 1.07 (0.54–2.13) 1.22 (0.54–2.73) 1.44 (0.62–2.34)
Readmission not leading
to reoperation
36 (4.6) 116 (6.3) 1.36 (0.94–1.95)
1.38 (0.94–2.03) 1.45 (0.95–2.22) 1.34 (0.85–2.11) 1.56 (0.97–2.50)
OR = odds ratio; RR = relative risk; CI = confidence interval.a Total may not add up to 100 due to rounding of percentages.b Denotes retropubic radical prostatectomy.c Denotes robot-assisted laparoscopic radical prostatectomy.d Possible confounders to be used in adjustments for each outcome were selected as variables significantly associated ( p value < 0.20) with the specific
outcome.e Adjustment A. Infection adjusted for: age at surgery, employment status preoperatively, physical exercise, previously operated for inguinal hernia, previous
transurethral resection of the prostate (TURP), International Prostate Symptom Score (IPSS), cardiovascular disease, mental disorder, kidney disease, and
prostate weight. Cardiovascular adjusted for: IPSS, pulmonary disease, neurologic disease, and prostate weight. Surgical adjusted for: age at surgery,
employment status preoperatively, coronary bypass surgery, IPSS, mental disorder, and prostate weight. Miscellaneous adjusted for: age at surgery,
postoperative irradiation, previously operated for inguinal hernia, IPSS, kidney disease, and prostate weight. Readmission leading to reoperation adjusted for:
age at surgery, postoperative irradiation, and prostate weight. Readmission not leading to reoperation adjusted for: employment status preoperatively,
previously operated for inguinal hernia, previous TURP, IPSS, mental disorder, and prostate weight.f Adjustment B: Adjustment A + tumour factors (preoperative prostate-specific antigen level, clinical tumour stage, tumour stage of prostatectomy specimen,
Gleason score on biopsy cores, and Gleason score pathology on specimen).g Adjustment C: Adjustment A + B + lymph node dissection.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0666
open surgery when adjusting for tumour factors and
lymph node dissection. The robot-assisted technique also
improved short-term outcomes such as perioperative
bleeding and length of hospital stay, but resulted in
longer operating time compared to open surgery. Howev-
er, there was no statistically significant difference in
readmittance rate between the groups within 3 mo after
the operation.
It was more common to seek health care after open
surgery compared to robot-assisted surgery. The data
specifically show that it was more common to seek health
care for cardiovascular reasons in the open group. The
difference was statistically significant after adjusting for
nontumour and tumour-specific confounders. Patient-
reported outcomes showed higher absolute percentages
of thromboembolic events, deep venous thrombosis and
pulmonary embolism in the open radical prostatectomy
group compared to the robot-assisted surgery group
(Table 4). Similar results have been presented by van
Hemelrijck et al [13] in a large retrospective case-control

[(Fig._1)TD$FIG]
(n = 4003)
No informed consent (n = 21)
Robot-assisted laparoscopic radical prostatectomy (n = 1847)
Evaluable (n = 2625)
Reported to the study register Start date: September 1, 2008 End date: November 7, 2011
>75 yr ≥20 ng/ml prostate-specific antigen (PSA) >T3 tumor stage Metastatic disease
Withdrawn consent; not understanding Swedish; physical, psychosocial and practical reasons (n = 281)
Open radical prostatectomy (n = 778)
Surgeon having performed <100 operations (n = 980) No cancer in surgical specimen (n = 2) No operation performed (n = 26)
Analysed (n = 745)
Preoperative clinical report form 98%
Surgical clinical report form 98%
Postoperative care clinical report form 98%
6–12-wk clinical report form 98%
Preoperative patient questionnaire 89%
3-mo patient questionnaire 96%
Analysed (n = 1761)
Response rates
Preoperative clinical report form 100%
Surgical clinical report form 100%
Postoperative care clinical report form 100%
6–12-week clinical report form 99%
Preoperative patient questionnaire 88%
3-mo patient questionnaire 96%
Fig. 1 – Flow chart for the analysis of short-term results of the LAPPRO trial. Numbers may not total correctly, because the same individual may havefulfilled more than one exclusion criteria.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0 667
study. A theory for the reason for more thromboembolic
events in the open group is that the extraperitoneal
approach leaves a smaller space than the robot-assisted
approach if haematomas or lymphoceles occur, and this
could result in high pressure on the femoral veins and lead
to deep venous thrombosis, which also is a common cause of
pulmonary embolism. However, Gandaglia et al [14] recently
reported in a study of 5915 men that patients treated with
open and robot-assisted techniques had similar risk of overall
postoperative complications, and that robot-assisted surgery
led to a higher risk of genitourinary and miscellaneous
medical complications.
Patients operated on by open surgery reported some-
what more contact with the health-care system for
gastrointestinal symptoms compared to those operated
on by robot-assisted surgery, although this was not
statistically significantly different (Table 4). Most trials
of laparoscopic versus open abdominal surgery have found
that gastrointestinal symptoms (ie, nausea, impaired
appetite, or changes in stools) occur for a longer period
of time after open surgery [15,16]. However, Schroeck et al
[17] reported no difference concerning bowel function
between a robot-assisted laparoscopic group and an open
retropubic radical prostatectomy group. Results also show

E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0668
that more men sought care due to psychological symptoms
after open surgery compared to the robot-assisted ap-
proach (Table 4). In Sweden and the USA, men have an
increased risk of suicide in the year after a prostate cancer
diagnosis [18–20]. Men with newly diagnosed prostate
cancer seek psychiatric health care more often than cancer-
free men [21]. Our study, finding a difference in the
prevalence of psychological symptoms between surgical
techniques, indicates that predictors other than the
existential challenge of the cancer diagnosis need to be
explored in relation to psychiatric morbidity among
prostate cancer patients.
Reoperation during hospital stay was significantly more
frequent after open surgery compared to robot-assisted
surgery when adjusting for tumour factors and lymph node
dissection (Table 3). Similarly, in a meta-analysis by Tewari
et al [1], reoperation rates were significantly higher in the
open surgery group compared to the robot-assisted surgery
group; however, after propensity adjustments, there was no
significant difference. The reduced risk for reoperation with
the robot-assisted technique might be explained by less
tissue trauma and/or less perioperative bleeding, which has
previously been shown in other types of surgery to lead to a
lower degree of inflammatory response [22].
As others have previously shown, our results indicate that
robot-assisted laparoscopic radical prostatectomy seems to
be advantageous over open surgery in terms of perioperative
bleeding and length of hospital stay (Table 3). These results
are similar to data in a newly conducted meta-analysis and in
a registry-based study [1,23,24]. The reason for less bleeding
in the robot-assisted technique is usually explained by the
pneumoperitoneum, which gives a high pressure in the
abdomen during surgery and minimises perioperative
bleeding. The positioning of the patient in the Trendelen-
bourg position, which reduces venous blood pressure, is
another explanation which may have a positive effect on
perioperative bleeding. The shorter operating time associat-
ed with the open technique, as reported in this study, was
also confirmed by other authors [25,26].
There was no statistically significant difference in the
overall readmission rate within 3 mo after surgery; however,
the overall readmission rate was slightly more common after
robot-assisted surgery compared to open surgery (9.3% vs
7.7%; Table 5). These data confirm the report of Gandaglia
et al [14], who reported in 2014 that patients undergoing
open and robot-assisted surgery had similar odds of
readmission within 90 d after surgery. Although there was
no statistically significant difference between the groups
concerning causes for patient-reported readmissions in our
study, the data show that it was more common to be
readmitted for cardiovascular reasons after open surgery, but
this significance disappeared after adjustments. In a national
registry-based study, Chung et al [27] found higher rates of
readmission after open retropubic radical prostatectomy
compared to the robot-assisted approach.
The strengths of our study include the prospective,
controlled design, size, short inclusion period, high
response rate, use of validated measures, and the neutral
third-party approach. We made sure to obtain accurate
information of known and suspected risk factors for
adjustment. The modest changes after adjustments indi-
cate that the residual confounding is small, if any. Since
health-care professionals in the respective centres were
not blinded, either as assessors or as reporters of surgery-
induced problems, the reports could be influenced by their
enthusiasm for the surgical technique used in their centre.
The ‘‘I want to please my surgeon’’ attitude among
patients, on the other hand, is possibly related more to
the surgeon than the surgical technique [28,29]. A
limitation of the study, apart from the nonrandomised
design, is the lack of a standardised tool for the assessment
of the adverse events. At the time when the study was
designed and initiated, the Clavien-Dindo system of
systematic grading of adverse events after surgical
procedures, which requires data on the management of
the complications, was not generally recognised and,
therefore, was not included in the clinical report forms
[30]. Another limitation is the lack of a standardised
postoperative clinical pathway in the study. Each of the
14 centres used their own best practice, and this might
influence the hospital stay data.
5. Conclusions
Our study shows that short-term outcomes may be
influenced by the surgical technique used for radical
prostatectomy. However, evaluating the pros and cons of
robot-assisted laparoscopic radical prostatectomy as com-
pared with open surgery involves weighing together a large
number of incommensurable short- and long-term out-
comes, including economic consequences and cure rates.
Author contributions: Anna Wallerstedt had full access to all the data in the
study and takes responsibility for the integrity of the data and the accuracy
of the data analysis.
Study concept and design: Wallerstedt, Tyritzis, Carlsson, Hugosson,
Bjartell, Wilderang, Wiklund, Steineck, Haglind.
Acquisition of data: Wallerstedt, Tyritzis, Thorsteinsdottir, Carlsson,
Stranne, Gustafsson, Hugosson, Bjartell, Wilderang, Wiklund, Steineck,
Haglind.
Analysis and interpretation of data: Wallerstedt, Tyritzis, Thorsteinsdottir,
Carlsson, Stranne, Gustafsson, Hugosson, Bjartell, Wilderang, Wiklund,
Steineck, Haglind
Drafting of the manuscript: Wallerstedt, Hugosson, Bjartell, Wiklund,
Steineck, Haglind.
Critical revision of the manuscript for important intellectual content:
Wallerstedt, Tyritzis, Thorsteinsdottir, Carlsson, Stranne, Gustafsson,
Hugosson, Bjartell, Wilderang, Wiklund, Steineck, Haglind.
Statistical analysis: Wallerstedt, Wilderang
Obtaining funding: Wiklund, Steineck, Haglind
Administrative, technical, or material support: Wiklund, Steineck, Haglind.
Supervision: Wiklund, Steineck, Haglind.
Other (specify): None.
Financial disclosures: Anna Wallerstedt certifies that all conflicts of
interest, including specific financial interests and relationships and
affiliations relevant to the subject matter or materials discussed in the
manuscript (eg, employment/affiliation, grants or funding, consultan-
cies, honoraria, stock ownership or options, expert testimony, royalties,
or patents filed, received, or pending), are the following: None.

E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0 669
Funding/Support and role of the sponsor: None.
Acknowledgment statement: The HRQL study was supported by research
grants from the Swedish Cancer Foundation (2010/593), Region Vastra
Gotaland, Sahlgrenska University Hospital (ALF grants 138751 and
146201, agreement concerning research and education of doctors),
Swedish Research Council, Mrs. Mary von Sydow Foundation, Anna and
Edvin Berger foundation, and EUSP fellowship grant to Dr. Stavros I.
Tyritzis. We thank Dr. Sven Grundtman for including patients.
Appendix A. Members of the LAPPRO steering
committee
Bo Anderberg, Department of Surgery, St Gorans Hospi-
tal, Stockholm, Sweden; Ingela Bjorholt, Nordic Health
Economics, Goteborg, Sweden; Thomas Jiborn, Department
of Urology, Skane University Hospital, Lund University,
Lund, Sweden; Jan-Erik Damber, Department of Urology,
Institute of Clinical Sciences, Sahlgrenska Academy at the
University of Gothenburg, Goteborg, Sweden; Ali Khatami,
Department of Urology, Institute of Clinical Sciences,
Sahlgrenska Academy at the University of Gothenburg,
Goteborg, Sweden; Mikael Wulkner-Sylme, Department of
Urology, Varberg Hospital, Varberg, Sweden; Christer
Edlund, Department of Surgery, Kungsbacka Hospital,
Kungsbacka, Sweden; Erik Pileblad, Capio Lundby Hospital,
Gothenburg, Sweden; Hans Boman, Department of Surgery,
Alingsas Hospital, Alingsas, Sweden; Ola Bratt, Department
of Urology, Helsingborg Hospital, Helsingborg, Sweden;
Ulrika Westlund, Department of Urology, Sodersjukhuset,
Stockholm, Sweden
References
[1] Tewari A, Sooriakumaran P, Bloch DA, Seshadri-Kreaden U, Hebert AE,
Wiklund P. Positive surgical margin and perioperative complication
rates of primary surgical treatments for prostate cancer: a systematic
review and meta-analysis comparing retropubic, laparoscopic, and
robotic prostatectomy. Eur Urol 2012;62:1–15.
[2] Ficarra V, Novara G, Rosen RC, et al. Systematic review and meta-
analysis of studies reporting urinary continence recovery after
robot-assisted radical prostatectomy. Eur Urol 2012;62:405–17.
[3] Montorsi F, Wilson TG, Rosen RC, et al. Best practices in robot-
assisted radical prostatectomy: recommendations of the Pasadena
Consensus Panel. Eur Urol 2012;62:368–81.
[4] Alemozaffar M, Sanda M, Yecies D, Mucci LA, Stampfer MJ, Kenfield
SA. Benchmarks for operative outcomes of robotic and open radical
prostatectomy: results from the Health Professionals Follow-up
Study. Eur Urol 2015;67:432–8.
[5] Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and
robot-assisted radical prostatectomy: a systematic review and
cumulative analysis of comparative studies. Eur Urol 2009;55:
1037–63.
[6] Thorsteinsdottir T, Stranne J, Carlsson S, et al. LAPPRO: a prospective
multicentre comparative study of robot-assisted laparoscopic and
retropubic radical prostatectomy for prostate cancer. Scand J Urol
Nephrol 2011;45:102–12.
[7] Sobin LH, Compton CC. TNM seventh edition: what’s new, what’s
changed: communication from the International Union Against
Cancer and the American Joint Committee on Cancer. Cancer
2010;116:5336–9.
[8] Steineck G, Helgesen F, Adolfsson J, et al. Quality of life after radical
prostatectomy or watchful waiting. N Engl J Med 2002;347:790–6.
[9] Steineck G, Bergmark K, Henningsohn L, al-Abany M, Dickman PW,
Helgason A. Symptom documentation in cancer survivors as a basis
for therapy modifications. Acta Oncol 2002;41:244–52.
[10] R Development Core Team. A language and environment for statis-
tical computing. Vienna, Austria: R Foundation for Statistical Com-
puting; 2005.
[11] Steinsvik EA, Fossa SD, Axcrona K, Fransson P, Widmark A, Dahl AA.
Do perceptions of adverse events differ between patients and
physicians? Findings from a randomized, controlled trial of radical
treatment for prostate cancer. J Urol 2010;184:525–31.
[12] Sonn GA, Sadetsky N, Presti JC, Litwin MS. Differing perceptions of
quality of life in patients with prostate cancer and their doctors.
J Urol 2013;189(1 Suppl):S59–65.
[13] Van Hemelrijck M, Garmo H, Holmberg L, Stattin P, Adolfsson J.
Multiple events of fractures and cardiovascular and thromboem-
bolic disease following prostate cancer diagnosis: results
from the population-based PCBaSe Sweden. Eur Urol 2012;61:
690–700.
[14] Gandaglia G, Sammon JD, Chang SL, et al. Comparative effectiveness
of robot-assisted and open radical prostatectomy in the postdisse-
mination era. J Clin Oncol 2014;32:1419–26.
[15] Veldkamp R, Kuhry E, Hop WC, et al. Laparoscopic surgery versus
open surgery for colon cancer: short-term outcomes of a random-
ised trial. Lancet Oncol 2005;6:477–84.
[16] van der Pas MH, Haglind E, Cuesta MA, et al. Laparoscopic versus
open surgery for rectal cancer (COLOR II): short-term outcomes of a
randomised, phase 3 trial. Lancet Oncol 2013;14:210–8.
[17] Schroeck FR, Krupski TL, Sun L, et al. Satisfaction and regret after
open retropubic or robot-assisted laparoscopic radical prostatec-
tomy. Eur Urol 2008;54:785–93.
[18] Bill-Axelson A, Garmo H, Lambe M, et al. Suicide risk in men with
prostate-specific antigen-detected early prostate cancer: a nation-
wide population-based cohort study from PCBaSe Sweden. Eur Urol
2010;57:390–5.
[19] Fang F, Fall K, Mittleman MA, et al. Suicide and cardiovascular death
after a cancer diagnosis. N Engl J Med 2012;366:1310–8.
[20] Carlsson S, Sandin F, Fall K, et al. Risk of suicide in men with low-
risk prostate cancer. Eur J Cancer 2013;49:1588–99.
[21] Bill-Axelson A, Garmo H, Nyberg U, et al. Psychiatric treatment in
men with prostate cancer–results from a Nation-wide, population-
based cohort study from PCBaSe Sweden. Eur J Cancer 2011;47:
2195–201.
[22] Okholm C, Goetze JP, Svendsen LB, Achiam MP. Inflammatory
response in laparoscopic vs. open surgery for gastric cancer. Scand
J Gastroenterol 2014;1–8.
[23] Trinh QD, Sammon J, Sun M, et al. Perioperative outcomes of robot-
assisted radical prostatectomy compared with open radical pros-
tatectomy: results from the nationwide inpatient sample. Eur Urol
2012;61:679–85.
[24] Carlsson S, Nilsson AE, Schumacher MC, et al. Surgery-related
complications in 1253 robot-assisted and 485 open retropubic
radical prostatectomies at the Karolinska University Hospital.
Sweden Urology 2010;75:1092–7.
[25] Krambeck AE, DiMarco DS, Rangel LJ, et al. Radical prostatectomy
for prostatic adenocarcinoma: a matched comparison of open
retropubic and robot-assisted techniques. BJU international 2009;
103:448–53.
[26] Tewari A, Srivasatava A, Menon M. A prospective comparison of
radical retropubic and robot-assisted prostatectomy: experience in
one institution. BJU Int 2003;92:205–10.
[27] Chung SD, Kelle JJ, Huang CY, Chen YH, Lin HC. Comparison
of 90-day re-admission rates between open retropubic radical

E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 6 0 – 6 7 0670
prostatectomy (RRP), laparoscopic RP (LRP) and robot-assisted lap-
aroscopic prostatectomy (RALP). BJU Int 2012;110:E966–71.
[28] Litwin MS, Lubeck DP, Henning JM, Carroll PR. Differences in
urologist and patient assessments of health related quality of life
in men with prostate cancer: results of the CaPSURE database. J Urol
1998;159:1988–92.
[29] Mansson A, Henningsohn L, Steineck G, Mansson W. Neutral third
party versus treating institution for evaluating quality of life after
radical cystectomy. Eur Urol 2004;46:195–9.
[30] Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo
classification of surgical complications: five-year experience. Ann
Surg 2009;250:187–96.