
Nanostructure, Morphology, and Properties of Fluorous Copolymers Bearing Ionic Grafts

DOI: 10.1126/scitranslmed.3003391, 128ra41 (2012);4 Sci Transl Med
et al.Marios PolitisParkinson's Patients Treated with Dopamine GraftsSerotonin Neuron Loss and Nonmotor Symptoms Continue in
Editor's Summary
to relieve nonmotor symptoms by restoring serotonin neurotransmission.be combined with other therapeutic approaches such as additional grafts of serotonin neurons in specific brain areas relief of both motor and nonmotor symptoms in PD, dopamine neuron replacement with fetal or stem cells will need toarousal, feeding, satiety, mood, and emotion. These findings indicate that for more complete, long-term symptomatic showed that there were far fewer serotonin neurons than usual in brain areas related to the regulation of sleep,with an agent that binds to the serotonin transporter and measures the integrity of serotonin-producing neurons synthesis of another key neurotransmitter, called norepinephrine, was unaffected in these patients. But another scanand receptors showed that dopamine neuronal function was restored by the fetal grafts. Also, the principal site of When these patients were imaged by positron emission tomography, radioactive tracers that tag dopamine neuronswith fetal grafts 13 to 16 years previously still exhibited nonmotor symptoms even as their motor symptoms improved.
. decided to use sophisticated brain imaging techniques to investigate why three PD patients transplantedet alPolitis PD,problems that have a significant negative impact on quality of life. Given the importance of nonmotor symptoms in
with dopamine loss but also nonmotor symptoms such as depression, fatigue, visual hallucinations, and sleepperformance but no improvement in nonmotor symptoms. PD causes not only severe motor symptoms associated inconsistent results among different trials, some PD patients showed encouraging clinical improvements in motornigrostriatal pathway that are selectively lost in PD and hence improve motor performance. Although there have been brains of patients with PD was initiated nearly 2 decades ago. The goal was to restore dopaminergic neurons in theevery 500 in the United States. A pioneering treatment involving transplantation of dopamine-rich fetal grafts in the
Parkinson's disease (PD) is the second most common neurodegenerative disorder affecting about 1 person in
Imaging Cell Therapy in Parkinson's Disease
http://stm.sciencemag.org/content/4/128/128ra41.full.htmlcan be found at:
and other services, including high-resolution figures,A complete electronic version of this article
http://www.sciencemag.org/about/permissions.dtl in whole or in part can be found at: article
permission to reproduce this of this article or about obtaining reprintsInformation about obtaining
is a registered trademark of AAAS. Science Translational Medicinerights reserved. The title NW, Washington, DC 20005. Copyright 2012 by the American Association for the Advancement of Science; alllast week in December, by the American Association for the Advancement of Science, 1200 New York Avenue
(print ISSN 1946-6234; online ISSN 1946-6242) is published weekly, except theScience Translational Medicine
on
Apr
il 5,
201
2st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om

R E S EARCH ART I C L E
PARK INSON ’S D I S EASE
Serotonin Neuron Loss and Nonmotor SymptomsContinue in Parkinson’s Patients Treatedwith Dopamine GraftsMarios Politis,1* Kit Wu,1 Clare Loane,1 Niall P. Quinn,2 David J. Brooks,1 Wolfgang H. Oertel,3
Anders Björklund,4 Olle Lindvall,5,6 Paola Piccini1
on
Apr
il 5,
201
2m
ag.o
rg
Cell therapy studies in patients with Parkinson’s disease (PD) have been confined to intrastriatal transplantation ofdopamine-rich fetal mesencephalic tissue in efforts to improve motor performance. Although some PD patientsreceiving the dopamine-rich grafts showed improvements in motor symptoms due to replacement of dopaminergicneurons, they still suffered from nonmotor symptoms including depression, fatigue, visual hallucinations, and sleepproblems. Using functional imaging and clinical evaluation of motor and nonmotor symptoms in three PD patientstransplanted with intrastriatal fetal grafts 13 to 16 years previously, we assessed whether reestablishment of do-paminergic neuronal networks is sufficient to improve a broad range of symptoms. At 13 to 16 years after trans-plantation, dopaminergic innervation was restored to normal levels in basal ganglia and preserved in a number ofextrabasal ganglia areas. These changes were associated with long-lasting relief of motor symptoms. Then, weassessed the integrity of their serotonergic and norepinephrine neuronal systems using [11C]DASB {[11C]3-amino-4-(2-dimethylaminomethylphenylthio) benzonitrile} positron emission tomography (PET) and 18F-dopa PET, respec-tively. 18F-Dopa uptake in the locus coeruleus was within the normal range. In contrast, [11C]DASB uptake in theraphe nuclei and regions receiving serotonergic projections was markedly reduced. These results indicate ongoingdegeneration of serotonergic raphe nuclei and their projections to regions involved in the regulation of sleep,arousal, feeding, satiety, mood, and emotion. Our findings indicate that future cell-based therapies using fetal tissueor stem cells in PD patients may require additional grafts of serotonergic neurons to relieve nonmotor symptoms byrestoring serotonergic neurotransmission in specific cerebral targets.
ienc
e
stm.s
cD
ownl
oade
d fr
om
INTRODUCTION
Cell therapies with fetal tissue or stem cells to treat patients with Par-kinson’s disease (PD) aim to provide long-lasting relief of disease symp-toms. It is now widely acknowledged that the clinical spectrum of PDinvolves not only the classic motor symptoms of rigidity, bradykinesiaand tremor, but also a number of nonmotor symptoms such as prob-lems with mood, sleep, and gastrointestinal tract function (1, 2). Thesenonmotor symptoms are a source of increasing complaints by PD pa-tients as the disease advances (2), have a significant negative impact onquality of life (3), and are difficult to treat (4).
On the basis of extensive pharmacological research and preclinicalgrafting experiments in animals, clinical trials using intrastriatal trans-plantation of fetal ventral mesencephalic (fVM) tissue in patients withPD have demonstrated that dopamine (DA)–rich grafts can reinnervatethe striatum, release DA, and, in some cases, produce long-lasting reliefof motor symptoms (5). Moreover, follow-up studies now suggest waysto avoid or treat the serious adverse effects of graft-induced dyskinesiasthat have hampered the further development of cell therapy for PD(6–8). So far, clinical cell therapy research in PD has been restricted
1Centre for Neuroscience, Division of Experimental Medicine, Faculty of Medicine,Hammersmith Hospital, Imperial College London, London W12 0NN, UK. 2Sobell De-partment of Motor Neuroscience and Movement Disorders, Institute of Neurology,University College London, Queen Square, London WC1N 3BG, UK. 3Department ofNeurology, Philipps-University, D 35033Marburg, Germany. 4Neurobiology Unit, WallenbergNeuroscience Center, 221 84 Lund, Sweden. 5Laboratory of Neurogenesis and Cell Therapy,Wallenberg Neuroscience Center, 221 84 Lund, Sweden. 6Lund Stem Cell Center, 221 84Lund, Sweden.*To whom correspondence should be addressed. E-mail: [email protected]
www.Sc
to the reestablishment of dopaminergic function in the striatum andthe improvement of motor symptoms.
Postmortem studies have shown that brain pathology in PD extendsbeyond the striatum (9) and the dopaminergic system, and studies inanimal models of PD have demonstrated that dysfunction of the nor-epinephrine (NE) and serotonergic neuronal systems could be implicatedin the occurrence of nonmotor symptoms (10–13). Furthermore, there isnow an established connection between extrastriatal serotonergic dys-function and the occurrence of nonmotor symptoms on the basis of invivo positron emission tomography (PET) studies in PD patients (14–18).
Here, using in vivo PET and a battery of clinical assessments inthree PD patients who had received neural transplants 13 to 16 yearspreviously (patients 7, 13, and 15 in the Lund series) (19, 20), wetested the hypothesis that intrastriatal transplantation of DA-richfVM tissue is insufficient to generate relief of nonmotor symptoms.Moreover, we assessed the integrity of extrastriatal dopaminergic,NE, and serotonergic systems and hypothesized that non-DA mono-aminergic dysfunction may be a major contributor to nonmotorsymptoms. The results of PD patients receiving grafts were comparedwith data from 24 PD control patients who had not received graftsand 24 normal healthy controls matched for age and sex (Table 1).
RESULTS
Clinical status and nonmotor symptomsThe three transplanted PD patients studied here have been followed for13 to 16 years after surgery (patient 7 = 16th year after transplantation;
ienceTranslationalMedicine.org 4 April 2012 Vol 4 Issue 128 128ra41 1

R E S EARCH ART I C L E
patient 13 = 14th year; and patient 15 = 13th year). At their last as-sessment, they had significantly reduced unified PD rating scale(UPDRS) motor and total scores compared to ungrafted PD controlpatients in an “off ” medication state (P < 0.001), even though the du-ration of their PD averaged 20 years longer than that of the ungraftedPD control patients (Table 1). Their marked improvements in UPDRSmotor scores began during the first posttransplantation year forpatient 13, the second year for patient 7, and from the third year
www.Sc
for patient 15. By the end of the third posttransplantation year,their UPDRS motor scores were reduced from baseline by 40 to 56%(6, 8, 19, 20). As a consequence of improvements in motor perform-ance, patient 13 was able to stop L-dopa medication during the firstyear, patient 7 by the fourth, and patient 15 by the fifth year aftertransplantation.
The three grafted patients were rated for quality of life measuresand with a clinical battery of tests for screening nonmotor symptoms.
Table 1. Clinical characteristics of PD patients and healthy controls. M, male; F, female.
[11C]DASB PET study
ienceTranslationalMedici
18F-Dopa PET study
ne.org 4 April 2012 Vol 4 Issue
PD transplanted(n = 3)*
Normal control(n = 12)
PD control(n = 12)Normal control(n = 12)
PD control(n = 12)
Sex
10 M/2 F 10 M/2 F 10 M/2 F 10 M/2 F 3 MAge
63.3 ± 7.0† 62.9 ± 8.9 63.3 ± 5.9 62.6 ± 9.9 62.0 ± 6.1012
Parkinson’s disease duration
— 8.1 ± 1.1 — 8.0 ± 4.3 28.3 ± 1.2, 2
Unified Parkinson’s Disease Rating Scale (UPDRS) Motor Part III OFF — 43.2 ± 12.0 — 38.9 ± 10.2 12.3 ± 5.0il 5
UPDRS OFF (total)
— 72.3 ± 21.9 — 66.4 ± 22.1 29.7 ± 11.0Apr
Daily L-dopa equivalent dose — 795 ± 312 — 744 ± 433 0‡on
Mini-Mental State Examination
29.4 ± 0.7 27.8 ± 2.9 29.5 ± 0.5 28.9 ± 1.1 29.3 ± 0.6rg
Beck Depression Inventory Second Edition 3.1 ± 2.6 10.3 ± 4.4 2.9 ± 2.8 8.25 ± 5.0 7.3 ± 4.7g.o
Parkinson’s Disease Questionnaire–39§
— 63.2 ± 21.4 — 71.4 ± 25.0 24.0 ± 14.4ma
Nonmotor symptoms assessment scale for Parkinson’s disease
— 44.0 ± 33.1 — 45.3 ± 31.8 28.0 ± 18.0e
nc *Values at the time of their last PET imaging assessment. †Mean ± SD. ‡These subjects did not receive any dopaminergic medication. §Worst score = 156 (never = 0; always = 4).stm
.sci
e
Table 2. Nonmotor symptoms in transplanted PD patients.
rom
Patient 7
Patient 13 Patient 15ed f
PD nonmotor symptoms (NMS) questionnaire
9 yes/21 no 4 yes/26 no 11 yes/19 nooad
NMS assessment scale for PD
10 28 46nl
Parkinson’s Disease Sleep Scale (worst = 150) 38 13 29ow
Symptoms Urinary urgency Urinary urgency Urinary urgency DUrinary frequency
Urinary frequency Urinary frequencyNocturia
Loss of concentration Mood swingsConstipation
Back pain Anxiety/depression*Loss of concentration
Loss of libido ConstipationExcessive daytime sleepiness
Excessive sweating Loss of concentrationLeg
Hypersalivation Excessive daytime sleepinessParesthesias
Loss of smell ParesthesiasJoint pain
Weight loss Joint painLeg cramps
Urinary frequency Muscle cramps/spasmsHypersalivation
Loss of concentration Loss of libidoLoss of smell
Back pain Erectile dysfunctionBenign visual hallucinations
Hypersalivation
Loss of smell
*Hospital Anxiety and Depression Scale: (anxiety = 5/depression = 7).
128 128ra41 2

R E S EARCH ART I C L E
Their 39-item PD questionnaire (PDQ-39) scores were significantlyreduced compared to those of ungrafted PD control patients (P <0.001) (Table 1). The Mini-Mental State Examination (MMSE) scoresof the three transplanted PD patients, the PD control patients, and thenormal healthy controls were all within the normal range (Table 1).The Beck Depression Inventory Second Edition (BDI-II) mean scoreswere higher in the PD transplanted and PD control patients comparedto normal controls (P < 0.01) but were not raised above the discrim-inating threshold score for depression (>16) (21, 22) (Table 1).
The PD nonmotor symptoms questionnaire, the nonmotor symp-toms assessment scale for PD, the Hospital Anxiety and Depres-sion Scale (HADS), the PD Sleep Scale (PDSS), and body mass index(BMI) measures revealed the presence of a number of nonmotorsymptoms in patients 7, 13, and 15 (Table 2). All patients reported
www.Sc
on
Apr
il 5,
201
2st
m.s
cien
cem
ag.o
rgoa
ded
from
significant bowel and bladder dysfunction. Patients 7 and 15 exhibitedepisodes of excessive daytime sleepiness and reduced concentration.Patients 13 and 15 had problems with their libido. Patient 13 ex-perienced abnormal weight loss and excessive sweating, whereas pa-tient 15 was subject to episodes of anxiety and mood swings andexperienced visual hallucinations (Table 2).
Dopaminergic and extrastriatal monoaminergic innervationBy measuring the activity of aromatic amino acid decarboxylase, 18F-dopa PET provides an indirect measure of presynaptic dopaminergicneurons. We showed previously that there was a gradual increase inuptake of 18F-dopa (18F-dopa uptake is measured by the influx con-stant Ki) in the striatum that reached the normal range by the fourthposttransplantation year and has been sustained to date in the threegrafted PD patients (6, 8, 19, 20). Here, we assessed 18F-dopa uptake inthe basal ganglia (combined values for caudate, putamen, globus pallidus,subthalamic nucleus, and substantia nigra) 13 to 16 years after trans-plantation. We found that 18F-dopa uptake in the basal ganglia wasrestored to normal levels (mean ± 2 SD = 0.0078 to 0.0110): patient7 (0.0084), patient 13 (0.0084), and patient 15 (0.0086) (Fig. 1 andTable 3).
In line with dopaminergic neuron restoration in the striatum and ba-sal ganglia shown by longitudinal 18F-dopa PET studies, previous im-aging studies using [11C]raclopride PET have demonstrated restorationof DA release in the striatum (6, 8, 23, 24). [11C]Raclopride is a markerof postsynaptic DA D2 receptor availability (double [11C]raclopridePET scans with placebo and methamphetamine infusion challenges allowindirect measurements of DA release). In the current, more extended,analysis, we found restoration of DA release in the basal ganglia (8% re-duction of [11C]raclopride binding after methamphetamine; normalrange: 6 to 13%) in the three transplanted PD patients.
We further examined 18F-dopa uptake in a number of extrabasalganglia areas such as the hypothalamus, insula, prefrontal cortex (PFC),and thalamus in the 13 grafted PD patients 13 to 16 years after trans-plantation. We found that in the three grafted PD patients, 18F-dopauptake was within normal levels in virtually all areas (Fig. 2 andTable 3).
Fig. 1. 18F-Dopa influx constant (Ki) values for transplanted PD patientsversus controls. Scatter plot shows 18F-dopa influx constant (Ki) values for
the basal ganglia of three transplanted PD patients (7, 13, and 15), 12normal control (NC) individuals, and 12 PD patients matched for ageand sex who did not receive a fetal transplant. Scatter dot plot and errorbars represent mean ± 95% confidence interval. The scatter plot showsthat intrastriatal transplantation of fVM tissue in the three PD patients 13to 16 years earlier restored the dopaminergic innervation of the basalganglia.Dow
nl
Table 3. Regional 18F-dopa influx rate constant (Ki) values and between-group statistical comparisons (mean ± SD) for normal control (NC) indi-viduals, Parkinson’s disease (PD) patients, and Parkinson’s disease patients with intrastriatal grafts (PDG). All P values after analysis of variance(ANOVA) with Bonferroni post test. NS, nonsignificant.
Brain regions
NC PD PDGien
NCversus PD
ceTranslationa
NCversus PDG
lMedicine.org 4
PDversus PDG
April 2012 Vol
ANOVA P andF values
Amygdala
0.0051 ± 0.0005 0.0031 ± 0.0005 0.0038 ± 0.0008 P < 0.0001 P < 0.01 NS P < 0.0001; F2,24 = 42.44Anterior cingulate
0.0033 ± 0.0004 0.0027 ± 0.0002 0.0030 ± 0.0001 P < 0.01 NS NS P < 0.01; F2,24 = 8.74Basal ganglia
0.0092 ± 0.0007 0.0057 ± 0.0009 0.0085 ± 0.0001 P < 0.0001 NS P < 0.0001 P < 0.0001; F2,24 = 65.39Hypothalamus
0.0065 ± 0.0007 0.0053 ± 0.0010 0.0055 ± 0.0007 P < 0.05 NS NS P < 0.05; F2,24 = 5.56Insula
0.0028 ± 0.0005 0.0022 ± 0.0002 0.0031 ± 0.0004 P < 0.01 NS P < 0.01 P = 0.0007; F2,24 = 9.95Locus coeruleus
0.0053 ± 0.0007 0.0042 ± 0.0010 0.0045 ± 0.0000 P < 0.05 NS NS P < 0.05; F2,24 = 5.19Posterior cingulate
0.0025 ± 0.0004 0.0017 ± 0.0002 0.0025 ± 0.0005 P < 0.0001 NS P < 0.01 P < 0.0001; F2,24 = 18.25Prefrontal cortex
0.0024 ± 0.0004 0.0015 ± 0.0003 0.0024 ± 0.0002 P < 0.0001 NS P < 0.001 P < 0.0001; F2,24 = 25.31Red nucleus
0.0059 ± 0.0006 0.0046 ± 0.0010 0.0053 ± 0.0001 P < 0.01 NS NS P < 0.01; F2,24 = 6.55Thalamus
0.0032 ± 0.0004 0.0026 ± 0.0005 0.0030 ± 0.0005 P < 0.05 NS NS P < 0.05; F2,24 = 4.674 Issue 128 128ra41 3

R E S EARCH ART I C L E
012
Noradrenergic innervationThe locus coeruleus is the principal origin of NE neurons and sendswidespread NE projections to cortical and brainstem areas (25, 26).We measured 18F-dopa uptake in locus coeruleus as a marker ofthe functional integrity of NE neurons (27) 13 to 16 years after trans-plantation. We found that 18F-dopa uptake in the locus coeruleus waswithin normal levels (normal mean ± 2 SD = 0.0040 to 0.0066) forpatient 7 (0.0045), patient 13 (0.0045), and patient 15 (0.0046) (Fig. 3and Table 3).
Serotonergic innervationThe PET marker [11C]3-amino-4-(2-dimethylaminomethylphenylthio)benzonitrile [11C]DASB binds to the serotonin transporter and servesas a functional marker of serotonergic neuronal integrity. The rapheregion contains a large population of serotonin neurons (28). Theserotonergic raphe nuclei showed major reductions in [11C]DASBbinding ([11C]DASB binding is measured by the binding potentialBPND) in patient 7 (1.27), patient 13 (1.37), and patient 15 (1.27).These reductions fell below the range for both normal healthy individ-
www.Sc
uals (mean 2.19 ± 2 SD 1.7 to 2.68) and ungrafted control PD patients(mean 1.77 ± 2 SD 1.38 to 2.16) (Fig. 4 and Table 4). Reductions in[11C]DASB binding in the raphe nuclei of transplanted PD patientsranged from 37.0 to 42.4% of that for normal control individualsand from 22.0 to 28.2% of that for ungrafted PD control patients(Fig. 4 and Table 4).
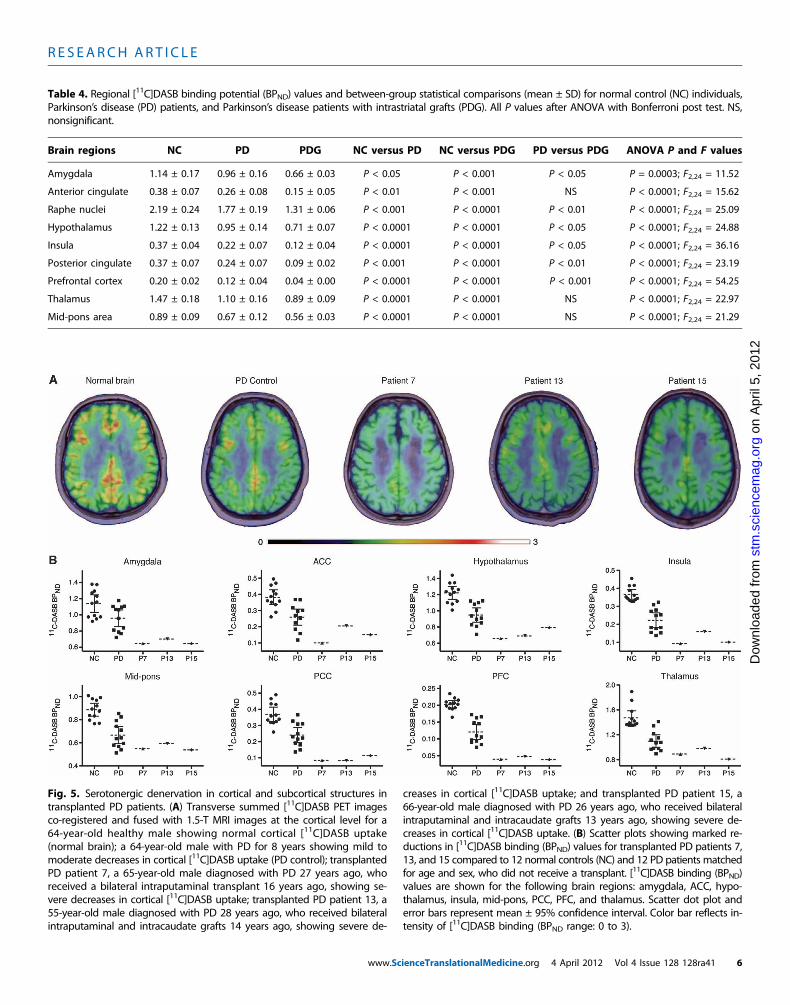
Patients 7, 13, and 15 also exhibited significant reductions in[11C]DASB binding relative to both normal healthy individualsand PD controls in a number of extrastriatal regions that receiveserotonergic innervation from raphe nuclei (Fig. 5). These reduc-tions in [11C]DASB binding relative to normal healthy individualsranged from 43.4% reduction in the amygdala (38.4% reduction rel-ative to PD control patients) to 44.9% in thalamus (26.1% compared toPD controls), 46.3% in hypothalamus (30.7% compared to PD con-trols), 73.7% in anterior cingulate cortex (ACC) (61.2% comparedto PD controls), 74.6% in the insula (60.2% compared to PD con-trols), 77.6% in posterior cingulate cortex (PCC) (65.5% comparedto PD controls), and 80.9% in PFC (67.9% compared to PD controls)(Fig. 5 and Table 4).
on
Apr
il 5,
2st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
Fig. 2. Dopaminergic innervation in cortical and subcortical structures oftransplanted PD patients several decades after diagnosis. (A) Transverse
showing normal cortical 18F-dopa uptake; and patient 15, a 66-year-old malediagnosed with PD 26 years ago, who received bilateral intraputaminal and
summed 18F-dopa PET images co-registered and fused with 1.5-T MRIimages at the cortical level for a 63-year-old healthy male showing normal18F-dopa uptake; a 62-year-old male with PD for 8 years showing significantdecreases in cortical 18F-dopa uptake (PD control); transplanted PD patient 7,a 65-year-old male diagnosed with PD 27 years ago, who received a bilateralintraputaminal transplant 16 years ago showing normal cortical 18F-dopauptake; PD patient 13, a 55-year-old male diagnosed with PD 28 years ago,who received bilateral intraputaminal and intracaudate grafts 14 years ago,
intracaudate grafts 13 years ago, showing normal cortical 18F-dopa uptake. (B)Scatter plots showing 18F-dopa influx constant (Ki) values for 12 normalhealthy control (NC) individuals, 12 PD patients, and three transplanted PDpatients (patients 7, 13, and 15). Ki values are shown for the following brainregions: amygdala, anterior cingulate cortex (ACC), hypothalamus, insula, pos-terior cingulate cortex (PCC), prefrontal cortex (PFC), red nucleus, and thala-mus. Scatter dot plot and error bars represent mean ± 95% confidenceinterval. Color bar reflects intensity of 18F-dopa uptake (Ki range: 0 to 0.014).
ienceTranslationalMedicine.org 4 April 2012 Vol 4 Issue 128 128ra41 4

R E S EARCH ART I C L E
DISCUSSION
Here, we show major loss of serotonergic neurons in raphe nuclei andwidespread serotonergic denervation in extrastriatal forebrain areas inthree PD patients who had received intrastriatal transplants of DA-rich fVM tissue 13 to 16 years earlier. In these patients, the storageand release of DA—measured by 18F-dopa and [11C]raclopride binding
www.Sc
on
Apr
il 5,
201
2nc
emag
.org
changes induced by methamphetamine—had been restored to nor-mal levels in grafted striatal areas. In addition, DA storage was pre-served at normal levels in basal ganglia and several limbic and corticalforebrain regions. These patients exhibited major motor symptom re-covery after transplantation, allowing withdrawal of their L-dopa med-ication for several years. However, clinical assessments demonstratedthe presence of a number of nonmotor symptoms diminishing qualityof life for these patients. These results are consistent with ongoingpathology in nondopaminergic systems indicated by loss of [11C]DASBbinding. This ongoing pathology affected serotonergic neurons in raphenuclei and their projections to cortical, subcortical, and deep nucleiareas. Although the evidence presented here is circumstantial, a caus-ative link is supported by data from biochemical (13), animal (11), andseveral in vivo PET studies demonstrating serotonergic system dys-function in PD patients suffering from nonmotor symptoms (14–18).
18F-Dopa PET measures the activity of the enzyme aromatic aminoacid decarboxylase and reflects NE neuron density in the locus coeru-leus (27). We found that 18F-dopa uptake in the locus coeruleus wasnormal in all three transplanted PD patients, indicating preservedfunction of this NE nucleus. Postmortem studies have demonstratedLewy body pathology in the locus coeruleus of brains from PD pa-tients (29–32), as well as marked reductions in tissue NE concentra-tions in forebrain regions innervated by the locus coeruleus (33, 34).Our finding of normal 18F-dopa uptake by the locus coeruleus in thetransplanted PD patients suggests that the cell bodies in the locuscoeruleus remain relatively intact, although their axonal projectionsmay be affected. Notably, the grafted PD patients had a significantlyyounger mean age of onset compared to the PD control patients, andthis could result in a different form or evolution of the disease. Indi-
Fig. 3. NE innervation in the locus coeruleus in transplanted PD patientsand controls. Scatter plot showing individual 18F-dopa influx constant (K )
ivalues for the locus coeruleus in transplanted PD patients 7, 13, and 15, in12 normal controls (NC), and in 12 PD patients matched for age and sex,who did not receive a transplant. Scatter dot plot and error bars representmean ± 95% confidence interval. NE innervation in the locus coeruleus oftransplanted PD patients is within the normal range (13 to 16 years) afterintrastriatal transplantation with fVM tissue.stm
.sci
eD
ownl
oade
d fr
om
Fig. 4. Loss of serotonergic innervation in the raphenuclei in transplanted PD patients. Scatter plot showsmarked reductions in [11C]DASB binding (BPND) valuesin individual raphe nuclei for transplanted PD patients7, 13, and 15 compared to 12 normal controls (NC) and12 PD patients matched for age and sex, who did notreceive a transplant. Corresponding sagittal summed[11C]DASB PET images co-registered and fused with1.5-T MRI images for the raphe nuclei of a 65-year-oldhealthy male showing normal raphe nuclei [11C]DASBbinding (BPND = 2.24) (circle); a 64-year-old male withPD for 8 years showing mild to moderate decreasesin raphe nuclei [11C]DASB binding (BPND = 1.80) (square);transplanted PD patient 7, a 65-year-old male diag-nosed with PD 27 years ago, who received a bilateralintraputaminal transplant 16 years ago, showing severedecreases in raphe nuclei [11C]DASB uptake (BPND =1.27) (triangle); transplanted PD patient 13, a 55-year-old male diagnosed with PD 28 years ago, whoreceived bilateral intraputaminal and intracaudategrafts 14 years ago, showing severe decreases in raphenuclei [11C]DASB binding (BPND = 1.38) (inverse triangle);and transplanted PD patient 15, a 66-year-old malediagnosed with PD 26 years ago, who received bilateralintraputaminal and intracaudate grafts 13 years ago,showing severe decreases in raphe nuclei [11C]DASBbinding (BPND = 1.27) (diamond). Scatter dot plotand error bars represent mean ± 95% confidence inter-val. Color bar reflects intensity of [11C]DASB uptake(BPND range: 0 to 3).
ienceTranslationalMedicine.org 4 April 2012 Vol 4 Issue 128 128ra41 5
R E S EARCH ART I C L E
Table 4. Regional [11C]DASB binding potential (BPND) values and between-group statistical comparisons (mean ± SD) for normal control (NC) individuals,Parkinson’s disease (PD) patients, and Parkinson’s disease patients with intrastriatal grafts (PDG). All P values after ANOVA with Bonferroni post test. NS,nonsignificant.
Brain regions
NC PD PDG NC versus PDwww.ScienceTra
NC versus PDG
nslationalMedicine.o
PD versus PDG
rg 4 April 2012 Vo
ANOVA P and F values
Amygdala
1.14 ± 0.17 0.96 ± 0.16 0.66 ± 0.03 P < 0.05 P < 0.001 P < 0.05 P = 0.0003; F2,24 = 11.52Anterior cingulate
0.38 ± 0.07 0.26 ± 0.08 0.15 ± 0.05 P < 0.01 P < 0.001 NS P < 0.0001; F2,24 = 15.62Raphe nuclei
2.19 ± 0.24 1.77 ± 0.19 1.31 ± 0.06 P < 0.001 P < 0.0001 P < 0.01 P < 0.0001; F2,24 = 25.09Hypothalamus
1.22 ± 0.13 0.95 ± 0.14 0.71 ± 0.07 P < 0.0001 P < 0.0001 P < 0.05 P < 0.0001; F2,24 = 24.88Insula
0.37 ± 0.04 0.22 ± 0.07 0.12 ± 0.04 P < 0.0001 P < 0.0001 P < 0.05 P < 0.0001; F2,24 = 36.16Posterior cingulate
0.37 ± 0.07 0.24 ± 0.07 0.09 ± 0.02 P < 0.001 P < 0.0001 P < 0.01 P < 0.0001; F2,24 = 23.19Prefrontal cortex
0.20 ± 0.02 0.12 ± 0.04 0.04 ± 0.00 P < 0.0001 P < 0.0001 P < 0.001 P < 0.0001; F2,24 = 54.25Thalamus
1.47 ± 0.18 1.10 ± 0.16 0.89 ± 0.09 P < 0.0001 P < 0.0001 NS P < 0.0001; F2,24 = 22.97Mid-pons area
0.89 ± 0.09 0.67 ± 0.12 0.56 ± 0.03 P < 0.0001 P < 0.0001 NS P < 0.0001; F2,24 = 21.29on
Apr
il 5,
201
2st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
Fig. 5. Serotonergic denervation in cortical and subcortical structures in11
creases in cortical [11C]DASB uptake; and transplanted PD patient 15, a
transplanted PD patients. (A) Transverse summed [ C]DASB PET imagesco-registered and fused with 1.5-T MRI images at the cortical level for a64-year-old healthy male showing normal cortical [11C]DASB uptake(normal brain); a 64-year-old male with PD for 8 years showing mild tomoderate decreases in cortical [11C]DASB uptake (PD control); transplantedPD patient 7, a 65-year-old male diagnosed with PD 27 years ago, whoreceived a bilateral intraputaminal transplant 16 years ago, showing se-vere decreases in cortical [11C]DASB uptake; transplanted PD patient 13, a55-year-old male diagnosed with PD 28 years ago, who received bilateralintraputaminal and intracaudate grafts 14 years ago, showing severe de-66-year-old male diagnosed with PD 26 years ago, who received bilateralintraputaminal and intracaudate grafts 13 years ago, showing severe de-creases in cortical [11C]DASB uptake. (B) Scatter plots showing marked re-ductions in [11C]DASB binding (BPND) values for transplanted PD patients 7,13, and 15 compared to 12 normal controls (NC) and 12 PD patients matchedfor age and sex, who did not receive a transplant. [11C]DASB binding (BPND)values are shown for the following brain regions: amygdala, ACC, hypo-thalamus, insula, mid-pons, PCC, PFC, and thalamus. Scatter dot plot anderror bars represent mean ± 95% confidence interval. Color bar reflects in-tensity of [11C]DASB binding (BPND range: 0 to 3).
l 4 Issue 128 128ra41 6

R E S EARCH ART I C L E
on
Apr
il 5,
201
2st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
viduals who develop PD at a younger age are more likely to have a ge-netic cause for their disease, and it is known that carriers of recessivemutations in the gene encoding parkin (PARK2) donot have Lewybodypathology. Such a genetic cause means that the disease would not nec-essarily follow Braak staging related to idiopathic PD (9). However, wehave not found any causative geneticmutations such as pointmutationsor exonic deletions/duplications in the coding region of thePARK2 geneinpatients 7 and15 (patient 13hasnot been checked for geneticmutations).
Serotonergic neurons in the dorsal, medial, and ventral raphe nu-clei send axonal projections to widespread areas of the brain (35, 36).In the three transplanted PD patients, we observed a marked decreasein [11C]DASB binding in the raphe nuclei (more than 40%) and as-sociated extrastriatal target areas (up to 80%) including the amygdala,hypothalamus, insula, cingulate, and prefrontal cortices. The loss ofextrastriatal serotonergic innervation is most likely due to degenera-tion of raphe nuclei projections, consistent with previous findings thatboth Lewy bodies and cell loss have been observed in these nuclei atearly stages of PD (9, 37–39). We have previously shown in patients 7,13, and 15 that in parallel with this degeneration, fVM tissue graftsgave rise to serotonergic hyperinnervation locally in the striatum(increased striatal [11C]DASB binding), which was associated with graft-induced dyskinesias (6, 8). The new data show that the serotonergicneurons within striatal grafts were not able to restore serotonergic in-nervation or compensate for its loss outside of the striatum.
According to Braak staging, early Lewy body pathology targets thecaudal nuclei of raphe (raphe magnus; stage 2), which predominantlyproject to the brainstem and spinal cord and later targets the rostral nu-clei (raphe dorsalis and medialis; stage 3), which project to the thalamus,limbic, and cortical regions (9, 40). Previous in vivo PET data on pa-tients with early, established, and advanced PD (average of 14 years afterthe appearance of symptoms) have demonstrated marked serotonergicdenervation starting in striatal and extrastriatal regions, whereas medio-dorsal and medio-ventral raphe nuclei are affected only in the ad-vanced stages of the disease (41). The unique [11C]DASB PET datawe present here from transplanted PD patients with 27 to 29 years ofdisease duration indicate a progressive and continuous degeneration ofserotonergic raphe neurons affecting widespread areas of the forebrain.
Grafted PD patients were not receiving dopaminergic medica-tion, whereas PD control patients were receiving both DA agonistsand L-dopa. An influence of DA agonists and L-dopa on serotonergictransmission could be a confounding factor in the PET analysis. How-ever, a recent study indicated that chronic exposure to dopaminergictherapy did not alter [11C]DASB binding in a set of brain regions similarto those investigated here (41).
The nonmotor symptoms in the grafted PD patients included ex-cessive daytime sleepiness, constipation, reduced concentration, weightloss, anxiety and depression, and visual hallucinations. Several lines ofevidence indicate that some of these symptoms are associated with themarked widespread decrease in brain serotonergic innervation. Theserotonergic system is involved in the regulation of both basic andcomplex physiological functions such as sleep, arousal, feeding, satiety,mood, and emotion (42). Accordingly, several in vivo PET studies havedemonstrated serotonergic system dysfunction in PD patients sufferingfrom nonmotor symptoms such as depression (14, 17), fatigue (16),abnormal changes in BMI (18), and visual hallucinations (15).
We demonstrate here in three PD patients the occurrence of non-motor symptoms associated with a widespread loss of serotonergic in-nervation despite successful intrastriatal dopaminergic grafts and
www.Sc
major recovery ofmotor function. Our findings show that implantationinto striatum of dopaminergic neuroblasts or precursors from fetalbrain tissue or derived from stem cells will not be able to ameliorate theentire clinical spectrum of PD symptoms. For more complete, long-termsymptomatic relief in PDpatients, intrastriatal DA cell replacement willneed to be combined with other therapeutic approaches targeting ex-trastriatal nondopaminergic systems. Our findings raise the possibilitythat in the future, suitably targeted implantation of serotonergic neu-roblasts or precursors in raphe nuclei or forebrain areasmay counteractnonmotor symptoms in PD. However, as a first step, before clinicalapplication is considered, the ability of serotonin grafts to reversenonmotor deficits in PD must be demonstrated in appropriate ani-mal models.
MATERIALS AND METHODS
Ethical permission to perform this study was obtained from theHammersmith and Queen Charlotte’s and Chelsea Hospitals ResearchEthics Committee. Permission to administer [11C]DASB, 18F-dopa, and[11C]raclopride was obtained from the Administration of RadioactiveSubstances Advisory Committee, UK. Written consent was obtainedfrom all subjects in accordance with the Declaration of Helsinki.
SubjectsWe studied three PD patients with bilateral intrastriatal transplantationof fVM tissue (patients 7, 13, and 15 in the Lund series) with PET im-aging and a battery of clinical assessments. Their results were com-pared with a group of 24 nondemented, nondepressed patients withidiopathic PD fulfilling the UK Brain Bank clinical criteria for PD (43)with no other history of neurological or psychiatric disorder, and a groupof 24 normal controls, all in good health with no past medical history(Table 1).
Transplantation proceduresDetails for the tissue preparation and neurosurgical procedures havebeen described previously (6, 8, 19, 20, 44–46). In brief, dissociatedfVM tissue was implanted with computed tomography (CT)– andmagnetic resonance imaging (MRI)–guided stereotactic neurosurgeryalong five trajectories bilaterally in the putamen (all patients) and twotrajectories in the head of the caudate nucleus (patients 13 and 15). Thetissue was procured from dead human fetuses aged 6 to 8 weeks afterconception and was obtained from routine suction abortions. All pa-tients received immunosuppressive treatment starting 2 days beforetransplantation and continuing for a mean of 29 months (44).
Clinical assessmentsAll subjects underwent a detailed clinical interview. General clinicalassessments included the UPDRS and the 32-item Wearing-off Ques-tionnaire (WOQ-32). UPDRS motor scores from previous assess-ments were retrospectively analyzed. The battery of nonmotor clinicalassessments included the PD nonmotor symptoms questionnaire, thenonmotor symptom assessment scale for PD, and the MMSE. Anxietyand depression levels were evaluated with BDI-II, the Hamilton RatingScale for Depression (HRSD), and HADS. Sleep was evaluated withthe PDSS and quality of life with PDQ-39. Changes in BMI were eval-uated as shown elsewhere (18). L-Dopa equivalent dose (LED) wascalculated with a formula previously described (41).
ienceTranslationalMedicine.org 4 April 2012 Vol 4 Issue 128 128ra41 7

R E S EARCH ART I C L E
on
Apr
il 5,
201
2st
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
Scanning proceduresAll PD patients and healthy volunteers were scanned at the CyclotronBuilding, Hammersmith Hospital (London, UK). All patients had theirL-dopa medication stopped for at least 18 hours before PET, and DAagonists were stopped 3 days before scanning. Subjects were scannedafter fasting and in a resting state with low light and no noise in theroom. Smoking and consumption of alcohol, coffee, and other caffein-ated beverages were not allowed at least 12 hours before scanning. Allsubjects had a volumetric 1.5-T MRI (Picker Eclipse) for the purposes ofimage registration to facilitate localization of the regions of interest(ROIs) and for volume analysis. Subjects were placed in the scannerswith transaxial planes oriented parallel to the orbitomeatal line, and headpositioning was monitored throughout the scan.
18F-Dopa18F-Dopa PET scans were performed with an ECATHR+ (CTI/Siemens962) PET tomography scanner that has 15.5-cm total axial field ofview (FOV) and provides 63 transaxial planes. This camera has amean reconstructed image transaxial resolution over a 10-cm radiusFOV (from the center) of 6.0 + 0.5 mm and an axial resolutionof 5.0 + 0.8 mm (47). To improve 18F-dopa availability to the brain,we pretreated subjects with 150 mg of carbidopa 1 hour before radio-isotope injection (48). A mean dose of 185 MBq of 18F-dopa in 10 ml ofnormal saline was infused intravenously over 30 s. Scanning began at thestart of tracer infusion generating 26 time frames over 94 min and30 s.
[11C]RacloprideAll [11C]raclopride scans were performed with the ECAT EXACT HR++
PET tomography scanner (49) as previously described (23, 24). Briefly,each subject received two [11C]raclopride PET scans, 2 to 3 days apart,and was assigned randomly to have an intravenous dose of normal sa-line before one scan and methamphetamine (0.3 mg/kg) before theother scan. Saline or methamphetamine was administered as a bolusover 30 s, 7 min before the injection of 140-MBq intravenous bolusdose of [11C]raclopride. Subjects did not know whether they wouldreceive saline or methamphetamine. Scanning began 30 s before tracerinfusion, generating 20 time frames over 60 min.
[11C]DASBThe [11C]DASB scans were performed with the ECAT EXACT HR+
PET tomography scanner as previously described (17, 41). A mean[11C]DASB dose of 450 MBq was administered as a bolus intravenousinjection 30 s after the initiation of scanning.
PET data analysisThe investigators analyzing the scans were blinded to the clinical char-acteristics of the participants. ROI image analysis was used.
18F-Dopa data analysis18F-Dopa is taken up by monoaminergic neurons that contain aromaticaminoaciddecarboxylase. Thismakes 18F-dopaPETamarker of thepatternof monoaminergic neuron innervation in areas in which such innervationpredominates—the dopaminergic neurons in the striatum and the NE neu-rons of the locus coeruleus (25). Here, we used a centralized analysis tech-nique to implement quality control as has been described elsewhere (50).
18F-Dopa influx rate constant (Ki) values for each ROI were com-puted with the multiple-time linear graphical analysis method (51)
www.Sc
with occipital cortex activity providing a reference input function rep-resenting nonspecific tissue tracer uptake (52). Summed images of the26 frames of the dynamic 18F-dopa time series reflecting both tracerdelivery and specific uptake of 18F-dopa collected over 30 to 90 min af-ter intravenous infusion were created for spatial normalization pur-poses (52). The summed images were spatially normalized to a smoothed18F-dopa template in Montreal Neurological Institute (MNI) stereo-tactic space (created in-house from healthy control subjects) withSPM5 (http://www.fil.ion.ucl.ac.uk/spm) implemented in MATLAB7(The Mathworks Inc.). Then, the transformation parameters were ap-plied to the respective 18F-dopa Ki maps. This technique standardizesbrain position and shape, allowing the use of standard object maps inMNI space to quantify tracer uptake in preselected ROIs. To optimizeimage quality, we audited the quality of the reference region input func-tion time-activity curves, the alignment of Ki maps, and the corre-sponding summed images. The ROIs sampled included amygdala,ACC, basal ganglia (caudate, putamen, globus pallidus, subthalamicnucleus, and substantia nigra), hypothalamus, insula, locus coeruleus,PCC, PFC, red nucleus, and thalamus. Their anatomical definition hasbeen previously described (27, 53) and was crosschecked with theTalairach and Tournoux (54) stereotactic atlas in combination withthe Duvernoy (55) three-dimensional sectional atlas. The final objectmap was applied to the spatially normalized Ki maps, and the valuesfor specific 18F-dopa uptake of individual regions were extracted withANALYZE8.1 medical imaging software (Mayo Foundation). To en-sure correct placement of the ROIs, we inspected each plane of thenormalized Ki maps and summed images.
[11C]Raclopride data analysisThe [11C]raclopride ROI analytical approach has been described pre-viously (23, 24). Briefly, parametric images of [11C]raclopride bindingpotential (BPND) were generated from the dynamic [11C]raclopridePET scans with a basis function implementation of the simplifiedreference region compartmental model with the cerebellum providingthe reference nonspecific tissue input function (56). The ROI analysiswas performed with ANALYZE8.1, and ROIs sampled included cau-date, putamen, total striatum, and basal ganglia. For each subject, theright to left averaged ROI binding potentials were calculated.
[11C]DASB data analysisThe [11C]DASB ROI analysis has been previously described (17, 41).Briefly, the input function was derived from the activity in the poste-rior cerebellar gray matter cortex, avoiding inclusion of the vermis(57). After reconstruction of the dynamic [11C]DASB image volume,a summed image volume was created from the entire dynamic dataset. The MRIs of subjects were co-registered to the summed PET vol-ume with the Mutual Information Registration algorithm in theSPM5. After co-registration, the definition of ROIs was performed onthe co-registered MRIs with ANALYZE8.1. ROIs were manually de-fined on both hemispheres for amygdala, ACC, hypothalamus, insula,mid-pons area, PCC, PFC, raphe nuclei, and thalamus.
The transformation characteristics generated from the co-registrationwere applied to the dynamic PET data set and the ROIs projected ontothe image volume. By obtaining the regional concentrations of radioac-tivity (kBq/ml) from the full dynamic scan, the decay-corrected time-activity curves were computed and movement during the scan wasassessed. Any movement detected was corrected with a frame-by-frame realignment procedure as previously described (58). Volume of
ienceTranslationalMedicine.org 4 April 2012 Vol 4 Issue 128 128ra41 8

R E S EARCH ART I C L E
distribution ratios (VDRs) were computed for ROI time-activity curveswith the graphical analysismethodof Logan et al. (59), and theBPNDwascalculated as VDR − 1 (60, 61). Right to left averaged BPND values werecomputed for all ROIs.
Statistical analysis (for Tables 3 and 4)Statistical analysis was performed with GraphPad Prism (version 5.0dfor Macintosh, GraphPad Software Inc.). For all comparisons, variancehomogeneity and Gaussianity were tested with Bartlett and Kolmogorov-Smirnov tests. Depending on the success of the normality tests and thedifferences on SDs between samples, parametric or nonparametric testswith or without corrections were used as appropriate.
Percentage decreases of regional [11C]raclopride BPND reflectingincreases of DA release after a methamphetamine challenge comparedto the practically defined OFF medication condition were calculatedaccording to the following formula:
n A
pril
5, 2
012
%D½11C�Raclopride ¼½11C�Raclopride BPNDðOFF‐MethamphetamineÞ½11C�Raclopride BPNDOFF � 100
REFERENCES AND NOTES
ost
m.s
cien
cem
ag.o
rgD
ownl
oade
d fr
om
1. K. R. Chaudhuri, D. G. Healy, A. H. Schapira; National Institute for Clinical Excellence, Non-motor symptoms of Parkinson’s disease: Diagnosis and management. Lancet Neurol. 5,235–245 (2006).
2. M. Politis, K. Wu, S. Molloy, P. G. Bain, K. R. Chaudhuri, P. Piccini, Parkinson’s disease symp-toms: The patient’s perspective. Mov. Disord. 25, 1646–1651 (2010).
3. P. Martinez-Martin, C. Rodriguez-Blazquez, M. M. Kurtis, K. R. Chaudhuri; NMSS ValidationGroup, The impact of non-motor symptoms on health-related quality of life of patientswith Parkinson’s disease. Mov. Disord. 26, 399–406 (2011).
4. L. D. Wood, J. J. Neumiller, S. M. Setter, E. K. Dobbins, Clinical review of treatment optionsfor select nonmotor symptoms of Parkinson’s disease. Am. J. Geriatr. Pharmacother. 8, 294–315(2010).
5. O. Lindvall, A. Björklund, Cell therapy in Parkinson’s disease. NeuroRx 1, 382–393(2004).
6. M. Politis, K. Wu, C. Loane, N. P. Quinn, D. J. Brooks, S. Rehncrona, A. Bjorklund, O. Lindvall,P. Piccini, Serotonergic neurons mediate dyskinesia side effects in Parkinson’s patientswith neural transplants. Sci. Transl. Med. 2, 38ra46 (2010).
7. M. Politis, Dyskinesias after neural transplantation in Parkinson’s disease: What do weknow and what is next? BMC Med. 8, 80 (2010).
8. M. Politis, W. H. Oertel, K. Wu, N. P. Quinn, O. Pogarell, D. J. Brooks, A. Bjorklund, O. Lindvall,P. Piccini, Graft-induced dyskinesias in Parkinson’s disease: High striatal serotonin/dopaminetransporter ratio. Mov. Disord. 26, 1997–2003 (2011).
9. H. Braak, K. Del Tredici, U. Rüb, R. A. de Vos, E. N. Jansen Steur, E. Braak, Staging ofbrain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 24, 197–211(2003).
10. S. J. Kish, Biochemistry of Parkinson’s disease: Is a brain serotonergic deficiency acharacteristic of idiopathic Parkinson’s disease? Adv. Neurol. 91, 39–49 (2003).
11. T. N. Taylor, W. M. Caudle, K. R. Shepherd, A. Noorian, C. R. Jackson, P.M. Iuvone, D.Weinshenker,J. G. Greene, G. W. Miller, Nonmotor symptoms of Parkinson’s disease revealed in an animalmodel with reduced monoamine storage capacity. J. Neurosci. 29, 8103–8113 (2009).
12. C. Delaville, P. D. Deurwaerdère, A. Benazzouz, Noradrenaline and Parkinson’s disease.Front. Syst. Neurosci. 5, 31 (2011).
13. D. M. Kuhn, C. E. Sykes, T. J. Geddes, K. L. Jaunarajs, C. Bishop, Tryptophan hydroxylase 2aggregates through disulfide cross-linking upon oxidation: Possible link to serotonin deficitsand non-motor symptoms in Parkinson’s disease. J. Neurochem. 116, 426–437 (2011).
14. I. Boileau, J. J. Warsh, M. Guttman, J. A. Saint-Cyr, T. McCluskey, P. Rusjan, S. Houle, A. A. Wilson,J. H. Meyer, S. J. Kish, Elevated serotonin transporter binding in depressed patients withParkinson’s disease: A preliminary PET study with [11C]DASB. Mov. Disord. 23, 1776–1780(2008).
15. B. Ballanger, A. P. Strafella, T. van Eimeren, M. Zurowski, P. M. Rusjan, S. Houle, S. H. Fox,Serotonin 2A receptors and visual hallucinations in Parkinson disease. Arch. Neurol. 67,416–421 (2010).
www.Sc
16. N. Pavese, V. Metta, S. K. Bose, K. R. Chaudhuri, D. J. Brooks, Fatigue in Parkinson’s disease islinked to striatal and limbic serotonergic dysfunction. Brain 133, 3434–3443 (2010).
17. M. Politis, K. Wu, C. Loane, F. E. Turkheimer, S. Molloy, D. J. Brooks, P. Piccini, Depressivesymptoms in PD correlate with higher 5-HTT binding in raphe and limbic structures. Neurology75, 1920–1927 (2010).
18. M. Politis, C. Loane, K. Wu, D. J. Brooks, P. Piccini, Serotonergic mediated body mass indexchanges in Parkinson’s disease. Neurobiol. Dis. 43, 609–615 (2011).
19. P. Hagell, A. Schrag, P. Piccini, M. Jahanshahi, R. Brown, S. Rehncrona, H. Widner, P. Brundin,J. C. Rothwell, P. Odin, G. K. Wenning, P. Morrish, B. Gustavii, A. Björklund, D. J. Brooks,C. D. Marsden, N. P. Quinn, O. Lindvall, Sequential bilateral transplantation in Parkinson’s dis-ease: Effects of the second graft. Brain 122, 1121–1132 (1999).
20. P. Brundin, O. Pogarell, P. Hagell, P. Piccini, H. Widner, A. Schrag, A. Kupsch, L. Crabb, P. Odin,B. Gustavii, A. Björklund, D. J. Brooks, C. D. Marsden, W. H. Oertel, N. P. Quinn, S. Rehncrona,O. Lindvall, Bilateral caudate and putamen grafts of embryonic mesencephalic tissue treatedwith lazaroids in Parkinson’s disease. Brain 123, 1380–1390 (2000).
21. A. F. Leentjens, F. R. Verhey, G. J. Luijckx, J. Troost, The validity of the Beck DepressionInventory as a screening and diagnostic instrument for depression in patients with Parkinson’sdisease. Mov. Disord. 15, 1221–1224 (2000).
22. C. D. Silberman, J. Laks, C. F. Capitão, C. S. Rodrigues, I. Moreira, E. Engelhardt, Recognizingdepression in patients with Parkinson’s disease: Accuracy and specificity of two depressionrating scale. Arq. Neuropsiquiatr. 64, 407–411 (2006).
23. P. Piccini, D. J. Brooks, A. Björklund, R. N. Gunn, P. M. Grasby, O. Rimoldi, P. Brundin, P. Hagell,S. Rehncrona, H. Widner, O. Lindvall, Dopamine release from nigral transplants visualized invivo in a Parkinson’s patient. Nat. Neurosci. 2, 1137–1140 (1999).
24. P. Piccini, N. Pavese, P. Hagell, J. Reimer, A. Björklund, W. H. Oertel, N. P. Quinn, D. J. Brooks,O. Lindvall, Factors affecting the clinical outcome after neural transplantation in Parkinson’sdisease. Brain 128, 2977–2986 (2005).
25. R. Y. Moore, J. P. Card, in Handbook of Chemical Neuroanatomy: Classical Transmitters in theCNS, Part I, A. Bjorklund, T. Hokfelt, Eds. (Elsevier, Amsterdam, 1984), vol. 2, pp. 123–156.
26. A. Björklund, O. Lindvall, in Handbook of Physiology—The Nervous System: Intrinsic RegulatorySystems of the Brain, Catecholaminergic Brain Stem Regulatory Systems, F. E. Bloom, Ed.(American Physiological Society, Bethesda, MD, 1986), vol. 4, pp. 155–235.
27. R. Y. Moore, A. L. Whone, S. McGowan, D. J. Brooks, Monoamine neuron innervation of thenormal human brain: An 18F-DOPA PET study. Brain Res. 982, 137–145 (2003).
28. H. W. Steinbusch, Distribution of serotonin-immunoreactivity in the central nervous system ofthe rat-cell bodies and terminals. Neuroscience 6, 557–618 (1981).
29. V. Chan-Palay, E. Asan, Alterations in catecholamine neurons of the locus coeruleus insenile dementia of the Alzheimer type and in Parkinson’s disease with and without de-mentia and depression. J. Comp. Neurol. 287, 373–392 (1989).
30. M. Gesi, P. Soldani, F. S. Giorgi, A. Santinami, I. Bonaccorsi, F. Fornai, The role of the locuscoeruleus in the development of Parkinson’s disease. Neurosci. Biobehav. Rev. 24, 655–668(2000).
31. H. Braak, K. Del Tredici, H. Bratzke, J. Hamm-Clement, D. Sandmann-Keil, U. Rüb, Staging ofthe intracerebral inclusion body pathology associated with idiopathic Parkinson’s disease(preclinical and clinical stages). J. Neurol. 249 (Suppl. 3), 1–5 (2002).
32. H. Braak, E. Ghebremedhin, U. Rüb, H. Bratzke, K. Del Tredici, Stages in the development ofParkinson’s disease-related pathology. Cell Tissue Res. 318, 121–134 (2004).
33. P. Jenner, M. Sheehy, C. D. Marsden, Noradrenaline and 5-hydroxytryptamine modulationof brain dopamine function: Implications for the treatment of Parkinson’s disease. Br. J.Clin. Pharmacol. 15 (Suppl. 2), 277S–289S (1983).
34. P. Gaspar, C. Duyckaerts, C. Alvarez, F. Javoy-Agid, B. Berger, Alterations of dopaminergicand noradrenergic innervations in motor cortex in Parkinson’s disease. Ann. Neurol. 30,365–374 (1991).
35. D. van der Kooy, T. Hattori, Dorsal raphe cells with collateral projections to the caudate-putamen and substantia nigra: A fluorescent retrograde double labeling study in the rat.Brain Res. 186, 1–7 (1980).
36. B. Lavoie, A. Parent, Immunohistochemical study of the serotoninergic innervation of thebasal ganglia in the squirrel monkey. J. Comp. Neurol. 299, 1–16 (1990).
37. R. J. D’Amato, R. M. Zweig, P. J. Whitehouse, G. L. Wenk, H. S. Singer, R. Mayeux, D. L. Price,S. H. Snyder, Aminergic systems in Alzheimer’s disease and Parkinson’s disease. Ann. Neurol.22, 229–236 (1987).
38. G. M. Halliday, Y. W. Li, P. C. Blumbergs, T. H. Joh, R. G. Cotton, P. R. Howe, W. W. Blessing,L. B. Geffen, Neuropathology of immunohistochemically identified brainstem neurons inParkinson’s disease. Ann. Neurol. 27, 373–385 (1990).
39. W. Paulus, K. Jellinger, The neuropathologic basis of different clinical subgroups of Parkinson’sdisease. J. Neuropathol. Exp. Neurol. 50, 743–755 (1991).
40. H. Braak, K. Del Tredici, Invited Article: Nervous system pathology in sporadic Parkinsondisease. Neurology 70, 1916–1925 (2008).
41. M. Politis, K. Wu, C. Loane, L. Kiferle, S. Molloy, D. J. Brooks, P. Piccini, Staging of serotonergicdysfunction in Parkinson’s disease: an in vivo 11C-DASB PET study. Neurobiol. Dis. 40, 216–221(2010).
ienceTranslationalMedicine.org 4 April 2012 Vol 4 Issue 128 128ra41 9

R E S EARCH ART I C L E
on
Apr
il 5,
201
2st
m.s
cien
cem
ag.o
rgde
d fr
om
42. S. H. Fox, R. Chuang, J. M. Brotchie, Serotonin and Parkinson’s disease: On movement,mood, and madness. Mov. Disord. 24, 1255–1266 (2009).
43. A. J. Hughes, S. E. Daniel, L. Kilford, A. J. Lees, Accuracy of clinical diagnosis of idiopathicParkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry55, 181–184 (1992).
44. O. Lindvall, S. Rehncrona, P. Brundin, B. Gustavii, B. Astedt, H. Widner, T. Lindholm, A. Björklund,K. L. Leenders, J. C. Rothwell, R. Frackowiak, C. D. Marsden, B. Johnels, G. Steg, R. Freedman,B. J. Hoffer, Å. Seiger, M. Bygdeman, I. Strömberg, L. Olson, Human fetal dopamine neuronsgrafted into the striatum in two patients with severe Parkinson’s disease. A detailed accountof methodology and a 6-month follow-up. Arch. Neurol. 46, 615–631 (1989).
45. G. K. Wenning, P. Odin, P. Morrish, S. Rehncrona, H. Widner, P. Brundin, J. C. Rothwell, R. Brown,B. Gustavii, P. Hagell, M. Jahanshahi, G. Sawle, A. Björklund, D. J. Brooks, C. D. Marsden,N. P. Quinn, O. Lindvall, Short- and long-term survival and function of unilateral intrastriataldopaminergic grafts in Parkinson’s disease. Ann. Neurol. 42, 95–107 (1997).
46. S. Rehncrona, A critical review of the current status and possible developments in braintransplantation. Adv. Tech. Stand. Neurosurg. 23, 3–46 (1997).
47. G. Brix, J. Zaers, L. E. Adam, M. E. Bellemann, H. Ostertag, H. Trojan, U. Haberkorn, J. Doll,F. Oberdorfer, W. J. Lorenz, Performance evaluation of a whole-body PET scanner using theNEMA protocol. National Electrical Manufacturers Association. J. Nucl. Med. 38, 1614–1623(1997).
48. J. M. Hoffman, W. P. Melega, T. C. Hawk, S. C. Grafton, A. Luxen, D. K. Mahoney, J. R. Barrio,S. C. Huang, J. C. Mazziotta, M. E. Phelps, The effects of carbidopa administration on 6-[18F]fluoro-L-DOPA kinetics in positron emission tomography. J. Nucl. Med. 33, 1472–1477 (1992).
49. T. J. Spinks, T. Jones, P. M. Bloomfield, D. L. Bailey, M. Miller, D. Hogg, W. F. Jones, K. Vaigneur,J. Reed, J. Young, D. Newport, C. Moyers, M. E. Casey, R. Nutt, Physical characteristics of theECAT EXACT3D positron tomograph. Phys. Med. Biol. 45, 2601–2618 (2000).
50. A. L. Whone, D. L. Bailey, P. Remy, N. Pavese, D. J. Brooks, A technique for standardizedcentral analysis of 6-18F-fluoro-L-DOPA PET data from a multicenter study. J. Nucl. Med. 45,1135–1145 (2004).
51. C. S. Patlak, R. G. Blasberg, J. D. Fenstermacher, Graphical evaluation of blood-to-brain transferconstants from multiple-time uptake data. J. Cereb. Blood Flow Metab. 3, 1–7 (1983).
52. J. S. Rakshi, T. Uema, K. Ito, D. L. Bailey, P. K. Morrish, J. Ashburner, A. Dagher, I. H. Jenkins,K. J. Friston, D. J. Brooks, Frontal, midbrain and striatal dopaminergic function in earlyand advanced Parkinson’s disease A 3D [18F]dopa-PET study. Brain 122, 1637–1650(1999).
53. R. Y. Moore, A. L. Whone, D. J. Brooks, Extrastriatal monoamine neuron function in Parkinson’sdisease: An 18F-dopa PET study. Neurobiol. Dis. 29, 381–390 (2008).
54. J. Talairach, P. Tournoux, Co-planar Stereotaxic Atlas of the Human Brain (Thieme, New York,1988).
55. H. M. Duvernoy, The Human Brain: Surface, Blood Supply, and Three-Dimensional SectionalAnatomy (Springer-Verlag Wien, New York, ed. 2, 1999).
56. R. N. Gunn, A. A. Lammertsma, S. P. Hume, V. J. Cunningham, Parametric imaging of ligand-receptor binding in PET using a simplified reference region model. Neuroimage 6, 279–287(1997).
www.Scie
57. S. J. Kish, Y. Furukawa, L. J. Chang, J. Tong, N. Ginovart, A. Wilson, S. Houle, J. H. Meyer,Regional distribution of serotonin transporter protein in postmortem human brain: Is thecerebellum a SERT-free brain region? Nucl. Med. Biol. 32, 123–128 (2005).
58. A. J. Montgomery, K. Thielemans, M. A. Mehta, F. Turkheimer, S. Mustafovic, P. M. Grasby,Correction of head movement on PET studies: Comparison of methods. J. Nucl. Med. 47,1936–1944 (2006).
59. J. Logan, J. S. Fowler, N. D. Volkow, G. J. Wang, Y. S. Ding, D. L. Alexoff, Distribution volumeratios without blood sampling from graphical analysis of PET data. J. Cereb. Blood FlowMetab. 16, 834–840 (1996).
60. N. Ginovart, A. A. Wilson, J. H. Meyer, D. Hussey, S. Houle, Positron emission tomographyquantification of [11C]-DASB binding to the human serotonin transporter: Modeling strategies.J. Cereb. Blood Flow Metab. 21, 1342–1353 (2001).
61. R. B. Innis, V. J. Cunningham, J. Delforge, M. Fujita, A. Gjedde, R. N. Gunn, J. Holden, S. Houle,S. C. Huang, M. Ichise, H. Iida, H. Ito, Y. Kimura, R. A. Koeppe, G. M. Knudsen, J. Knuuti,A. A. Lammertsma, M. Laruelle, J. Logan, R. P. Maguire, M. A. Mintun, E. D. Morris, R. Parsey,J. C. Price, M. Slifstein, V. Sossi, T. Suhara, J. R. Votaw, D. F. Wong, R. E. Carson, Consensusnomenclature for in vivo imaging of reversibly binding radioligands. J. Cereb. Blood FlowMetab. 27, 1533–1539 (2007).
Acknowledgments: We thank all participants and their families, and we gratefully acknowl-edge the contributions of other members of the Lund-London-Marburg neurotransplantationteam. Funding: Supported by the Medical Research Council, UK and Swedish Research Coun-cil and Michael J. Fox Foundation for Parkinson’s Research. Author contributions: M.P. con-ceived the study and conceptualized the experimental design. P.P., O.L., and A.B. gave input toexperimental design. M.P. organized the study, and N.P.Q., W.H.O., P.P., and K.W. aided in theorganization and study investigation. M.P. and K.W. performed the scans and the clinical assess-ments. C.L. and M.P. performed the analysis of the imaging data. M.P. supervised the analysisof the imaging data and analyzed the clinical data. M.P., O.L., A.B., D.J.B., and P.P. interpretedthe data. M.P. wrote the first draft and prepared the manuscript. O.L. edited the manuscript. Allauthors gave input to the manuscript. M.P. generated the figures. N.P.Q. has the clinical su-pervision and follow-ups of patients 7 and 15 and W.H.O. of patient 13. O.L. headed the clinicaltransplantation program. P.P., O.L., and A.B. are the senior authors. Competing interests: Theauthors declare that they have no competing interests.
Submitted 27 October 2011Accepted 8 March 2012Published 4 April 201210.1126/scitranslmed.3003391
Citation: M. Politis, K. Wu, C. Loane, N. P. Quinn, D. J. Brooks, W. H. Oertel, A. Björklund,O. Lindvall, P. Piccini, Serotonin neuron loss and nonmotor symptoms continue in Parkinson’spatients treated with dopamine grafts. Sci. Transl. Med. 4, 128ra41 (2012).
oa
nceTranslationalMedicine.org 4 April 2012 Vol 4 Issue 128 128ra41 10
Dow
nl
Copyright © 2022 FDOKUMEN




















