Electrophysiological effects of guanosine and MK-801 in a quinolinic acid-induced seizure model

Nephrol Dial Transplant (2013) 28: 1751–1761doi: 10.1093/ndt/gfs391Advance Access publication 29 November 2012
Selective phosphodiesterase-5 (PDE-5) inhibitor vardenafilameliorates renal damage in type 1 diabetic rats by restoringcyclic 30,50 guanosine monophosphate (cGMP) level inpodocytes
Lilla Fang1,
Tamás Radovits2,3,
Gábor Szabó2,
Miklós M. Mózes1,
László Rosivall1,4
and Gábor Kökény1
1Institute of Pathophysiology, Semmelweis University, Budapest,
Hungary,2Department of Cardiac Surgery, University of Heidelberg,
Heidelberg, Germany,3Heart Center, Semmelweis University, Budapest, Hungary and4Hungarian Academy of Sciences and Semmelweis University
Research Group for Pediatrics and Nephrology, Budapest, Hungary
Correspondence and offprint requests to: Gábor Kökény;E-mail: [email protected]
Keywords: cyclic GMP, phoshopdiesterase-5, podocyte, TGF-β1, type 1 diabetes
ABSTRACT
Background. Diabetic nephropathy (DN) is characterized bypodocyte damage and increased phosphodiesterase-5 (PDE-5)activity-exacerbating nitric oxide (NO)-cyclic 30,50 guanosinemonophosphate (cGMP) pathway dysfunction. It has beenshown that PDE-5 inhibition ameliorates DN. The role of po-docytes in this mechanism remains unclear. We investigatedhow selective PDE-5 inhibition influences podocyte damage instreptozotocin (STZ) diabetic rats.Methods. Male Sprague–Dawley rats (250–300 g) were in-jected with STZ and divided into two groups: (i) STZ control(non-treated, STZ, n = 6) and (ii) STZ + vardenafil treatment(10 mg/kg/day, STZ-Vard, n = 8). Non-diabetic rats served asnegative controls (Control, n = 7). Following 8 weeks of treat-ment, immunohistochemical and molecular analysis of thekidneys were performed.Results. Diabetic rats had proteinuria, increased renal trans-forming growth factor (TGF)-β1 expression and podocytedamage when compared with controls. Vardenafil treatmentresulted in preserved podocyte cGMP levels, less proteinuria,reduced renal TGF-β1 expression, desmin immunostaining inpodocytes and restored both nephrin and podocin mRNAexpression. Diabetes led to increased glomerular nitrotyrosineformation and renal neuronal nitric oxide synthase and endo-thelial nitric oxide synthase mRNA expression, but vardenafildid not influence these parameters.
Conclusions. Our data suggest that a dysfunctional NO-cGMP pathway exacerbates podocyte damage in diabetes. Inconclusion, vardenafil treatment preserves podocyte functionand reduces glomerular damage, which indicates therapeuticpotential in patients with DN.
INTRODUCTION
The incidence of diabetes mellitus and diabetic nephropathy(DN) is increasing exponentially worldwide [1, 2]. DN ischaracterized by oxidative stress [3], podocyte damage [4] andglomerulosclerosis [5]. Decreasing bioavailability of nitricoxide (NO) in diabetes might play a crucial role in theprogression, but the detailed pathomechanism is not fullyunderstood.
NO-cyclic 30,50 guanosine monophosphate (cGMP) axis isessential in the maintenance of renal perfusion and glomerularfiltration [6]. NO is synthesized in the vascular endothelialcells by endothelial nitric oxide synthase (eNOS) from L-argi-nine. NO exerts many of its biological actions by cGMP, whichis degraded rapidly by phosphodiesterases (PDE). In thekidney, the cGMP hydrolysing enzyme phosphodiesterase-5(PDE-5) is expressed in proximal tubules, collecting ducts andthe glomerulus [7]. Among haemodynamic actions [6, 8],NO-driven cGMP regulates glomerular filtration by modulat-ing the slit membrane and cytoskeletal reorganization in
ORIG
INALARTIC
LE
© The Author 2012. Published by Oxford University Press onbehalf of ERA-EDTA. All rights reserved.
1751
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

podocytes [9, 10]. In diabetes, cGMP production was shownto decrease in the glomeruli [11]. Causes of NO-cGMP dys-function in DN include scavenging of NO by reactive oxygenspecies (ROS) [12] and increased PDE-5 activity [13] whichwas reported to be the main cGMP hydrolysing enzyme in ratglomeruli [14].
The beneficial effect of elevating cGMP levels by selectivePDE-5 inhibition has been proven in several renal diseasemodels [15–18], including animal models of both type 1 andtype 2 diabetes where reduced glomerulosclerosis and protei-nuria was shown [19–21]. Although podocytes are postulatedto play a pivotal role in the progression of DN [22, 23], andcGMP presumably plays an important role in the regulation ofpodocyte function [9, 10], the effect of PDE-5 inhibition onpodocyte function in diabetes is still unknown.
In our study, we investigated whether the elevation ofcGMP levels by pharmacological treatment with vardenafil, ahighly selective PDE-5 inhibitor, could preserve podocytefunction and reduce podocyte damage in the rat model ofstreptozotocin (STZ)-induced type 1 diabetes mellitus. Wefound that vardenafil treatment raised serum cGMP levels andintracellular cGMP levels in podocytes, decreased proteinuria,attenuated podocyte damage and restored nephrin andpodocin expression.
MATERIALS AND METHODS
Animals
Male Sprague–Dawley rats (250–300 g, Charles River, Sulz-feld, Germany) were housed at a constant temperature of22 ± 2°C with 12 h light/dark cycles, had access to standardrodent chow and water ad libitum.
The investigation conforms with the Guide for the Care andUse of Laboratory Animals published by the US National Insti-tutes of Health (NIH Publication No. 85-23, revised 1996). Allprocedures and handling of animals during the investigationswere reviewed and approved by the local Ethical Committeefor Animal Experimentation.
Induction of diabetes mellitus
Type 1 diabetes mellitus was induced in rats with a singleintraperitoneal (i.p.) dose of STZ (60 mg/kg) in citrate buffer(0.1 mol/L). Control animals received buffer only. After 72 h,blood glucose level was determined (Accu-Chek®, Roche, Man-nheim, Germany). Animals with a random blood glucose level>15 mmol/L were considered as diabetic and were includedinto the study.
Experimental groups, treatment protocol
Diabetic rats were randomized to diabetic control (STZ,n = 6) and vardenafil treatment (STZ-Vard, n = 8) groups.Rats injected with citrate buffer served as non-diabetic con-trols (Control, n = 7). Diabetic animals were treated for 8weeks with the selective PDE-5 inhibitor, vardenafil (STZ-Vard group, 10 mg/kg/day dissolved in 0.01 mol/L citratebuffer) or with vehicle (Control and STZ groups) per os in
drinking water. The daily water intake was registered and thedose of vardenafil was repeatedly adjusted.
Body and kidney weights were measured at harvest.
Blood pressure measurements, blood and urinechemistries
At the end of the treatment period, rats were anaesthetizedwith ketamine (100 mg/kg) and xylazine (3 mg/kg) i.p. andwere placed on controlled heating pads. Arterial bloodpressure was recorded by 2 F microtip pressure–volume cath-eter (SPR-838, Millar Instruments, Houston, TX), and themean arterial pressure (MAP) was computed.
Blood samples were taken from the inferior caval vein.Urine samples were obtained by sterile punction of the urinarybladder. Serum glucose and urea levels as well as urine creati-nine concentration were determined on a Reflotron analyser(Roche). Urine protein concentration was measured usingBCA Protein Assay (Pierce Thermo Scientific, Rockford), andurinary protein/creatinine ratios were calculated.
Serum cGMP levels were determined by enzyme immu-noassay (EIA) using a commercial kit (Amersham cGMP EIABiotrak System, GE Healthcare, Buckinghamshire, UK).
Serum thiobarbituric acid reactive substances (TBARS) asmarkers of lipid peroxidation were determined by fluorometricassay using a commercial kit (OXItek TBARS Assay Kit, Zep-tometrix Inc., Buffalo, NY).
Renal histology and immunohistochemistry
Periodic-acid Schiff (PAS) staining was performed on for-malin fixed, paraffin-embedded kidney samples. Glomerulardamage was assessed according to el Nahas et al. [24]. The glo-merular score of each animal was derived as the arithmeticmean of 60 glomeruli (×400 magnification). The tubulardamage (dilatation, atrophy, hyalin in tubular lumen, infiltra-tion of mononuclear cells and interstitial fibrosis) was assessedas previously described [25].
Immunohistochemistry was performed on paraffin sec-tions, using the avidin–biotin method, as previously described[25]. After antigen retrieval with citric buffer, slides were incu-bated with primary antibodies [rabbit polyclonal anti-fibro-nectin, 1:1000, Sigma-Aldrich, Budapest, Hungary; rabbitpolyclonal anti-transforming growth factor (TGF)-β1, 1:100;Santa Cruz Biotechnology, Santa Cruz, CA; mouse mono-clonal anti-desmin, 1:50, Dako, Frank Diagnosztika, Budapest,Hungary; rabbit polyclonal anti-nephrin, Abcam, USA; rabbitpolyclonal anti-nitrotyrosine, 1:200, Chemicon/Millipore, Bill-erica, MA; rabbit polyclonal anti-cGMP 1:2000, AbD Serotec,Düsseldorf, Germany] then with appropriate secondary anti-bodies (BioGenex, San Ramon, CA) and developed using FastRed (Dako). Immunohistochemical reactivity (×400 magnifi-cation) was evaluated in a blinded manner as described else-where [25]: 0, no staining; 1, weak; 2, mild; 3, strong.Fibronectin staining and glomerular cGMP content werequantified as follows: intensity score (1, weak staining; 2, inter-mediate staining; 3, extensive staining) and area score (1, up to10% positive cells; 2, 11–50% positive cells; 3, 51–80% positivecells; 4, >80% positive cells) were assessed, and an average
ORIG
INALARTIC
LE
L. Fang et al.
1752
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

score was calculated for each field of view (intensity score mul-tiplied by area score) [26].
Nephrin and cGMP double immunostaining was per-formed on frozen kidney sections. Briefly, acetone-fixed sec-tions were rehydrated with phosphate-buffered saline, blockedwith 5% serum, incubated with primary antibodies (anti-cGMP, 1:4000, AbD Serotec, and guinea pig polyclonal anti-nephrin, 1:500, Fitzgerald Industries, Acton, MA), then withsecondary antibodies (Dylight-488 conjugated donkey anti-guinea pig and Cy3 conjugated donkey anti-rabbit, both at1:500, Jackson Immunoresearch, West Grove, PA), thenwashed, mounted and analysed under a fluorescent micro-scope.
Immunoblot
Kidney samples (20 mg) were homogenized in RIPA lysisbuffer containing complete protease inhibitor cocktail(Roche). Protein concentration was determined by the BCAassay. Samples were mixed with 2× Laemmli buffer and boiled.Equal amounts of protein (40 µg) were separated on 10%sodium dodecyl sulphate–polyacrylamide gel, transferred tonitrocellulose membranes and blocked with 5% skim milk inTris-buffered saline, containing 0.1% Tween-20. Membraneswere incubated overnight at 4°C with either rabbit polyclonalanti-PDE5a antibody (1:1000, Enzo, Plymouth Meeting, PA)or mouse monoclonal anti-glyceraldehyde-3-phosphate dehy-drogenase (GAPDH) antibody (1:2000, Millipore, Billerica,MA), washed and incubated with peroxidase-conjugated sec-ondary antibody (anti-mouse IgG or anti-rabbit IgG, 1:2000,Cell Signaling, Danvers, MA). Blots were visualized by ECLdetection kit (Pierce Thermo).
Quantitative RT–PCR
One hundred milligrams of whole kidneys were homogen-ized and total RNA was isolated according to the manufac-turer’s protocol (SV Total RNA kit, Promega, Madison, WI).Two micrograms of RNA were reverse transcribed (HighCapacity cDNA Reverse Transcription kit, Applied Biosys-tems, Forster City, CA) using random primers. PCR reactionswere performed on a BioRad CFX thermal cycler (BioRad,Hercules, CA) using the Power SYBR Green PCR Master Mix(Applied Biosystems). The specificity and efficiency of thePCR reaction was confirmed with the melting curve and stan-dard curve analysis, respectively. Duplicate samples were nor-malized to GAPDH expression. The mean values areexpressed with the formula 2−ΔΔCt. Primer sequences were asfollows: TGF-β1 forward: 5-CACCATCCATGACATGAACC-3; TGF-β1 reverse: 5-TCATGTTGGACAACTGCTCC-3;eNOS forward: 5-TGACCCTCACCGATA-CAACA-3; eNOSreverse: 5-CTGGCCTTCTGCTCATTTTC-3; neuronal nitricoxide synthase (nNOS) forward: 5-GACAAC-GTTCCTGTGGTCCT-3; nNOS reverse: 5-TCCAGTGTGCTCTTCAGGTG-3;nephrin forward: 5-GCCTCTTGACCATCGCTAATG-3; nephrinreverse: 5-GACAACCTTCAGTCCCAGTG-3; podocin forward:5-TCCCTTTTCCATCTGGTTCTG-3; podocin reverse: 5-CTTGTGATAGGT-GTCCAGGC-3; GAPDH forward: 5-CAAT-GACCCCTTCATTGACC-3; GAPDH reverse: 5-CGCCAGTA-GACTCCACAACA-3.
Statistics
All the data are presented as mean ± SD. In the case of thefunctional measurements and blood chemistries, differencesbetween the groups were eveluated using one-way analysis ofvariance (ANOVA) followed by Tukey’s post hoc test. His-tology, immunohistochemistry and PCR data were analysedusing the Kruskal–Wallis test followed by Dunn’s test. Thelevel of significance was set to P < 0.05.
RESULTS
Vardenafil increased serum cGMP levels in diabetic rats
Effectiveness of vardenafil treatment was evaluated byserum cGMP levels at harvest. Diabetes tended to reduceserum cGMP levels in non-treated STZ rats when comparedwith non-diabetic controls, but vardenafil treatment signifi-cantly restored, and actually elevated, serum cGMP levelsabove the range of non-diabetic controls (Table 1).
Vardenafil did not affect metabolic changes, renalhypertrophy or blood pressure in diabetic rats
Serum glucose levels and daily water intake rose, while bodyweight decreased in diabetic rats, regardless of treatment.Kidneys of both vardenafil-treated and non-treated diabetic ratsdeveloped significant hypertrophy as shown by increased kidneyweight/body weight ratio at the time of harvest (Table 1).
STZ rats tended to have slightly elevated serum urea levels,but the difference was statistically not significant. There wasno difference in the MAP values among the groups at harvest(Table 1).
Vardenafil decreased the extent of glomerularremodelling, proteinuria, fibronectin and TGF-β1expression in diabetic rats
When compared with controls, glomerular hypertrophy,mild mesangial expansion and adhesions to Bowman’s capsulewere observed in diabetic rats, which were ameliorated by var-denafil treatment (Figure 1A–E). The tubulointerstitial lesionsof STZ rats were characterized by tubular dilatation andatrophy, which was significantly ameliorated by vardenafiltreatment. Mononuclear cell infiltration was not seen incontrol kidneys, and only to a minimal extent in diabetickidneys regardless of treatment protocol (data not shown).
Diabetes led to significantly elevated urine protein/creati-nine ratio in STZ rats when compared with healthy controls.Vardenafil-treated rats, however, had lower urinary protein/creatinine ratio when compared with STZ rats (Figure 1F).
Fibronectin expression, evaluated by immunohistochemis-try, was augmented in STZ rats, but significantly reduced byvardenafil treatment (Figure 2A–C, G and H).
Both glomeruli and tubulointerstitium of STZ kidneysshowed strong TGF-β1 immunostaining (Figure 3A–C), whichwas significantly reduced after vardenafil treatment (Figure 3Gand H).
According to immunostaining results, TGF-β1 mRNAexpression in whole kidney homogenates was significantly
ORIG
INALARTIC
LE
V a r d e n a fi l p r o t e c t s p o d o c y t e s i n d i a b e t e s
1753
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

higher in non-treated STZ rats when compared with non-dia-betic controls. Vardenafil treatment normalized the mRNAexpression to similar levels as seen in non-diabetic controls(Figure 4A).
Vardenafil restored cGMP content in podocytes anddecreased podocyte damage in diabetic kidneys
Immunoblot analysis revealed renal PDE-5 overexpressionin both non-treated and treated diabetic rats when comparedwith controls (P < 0.05, Figure 5).
Immunostaining revealed significant glomerular cGMPcontent in non-diabetic kidneys, mostly localized to podocytes(Figure 2D, see arrows and inset picture) and to a less extentto endothelial cells. Decreased glomerular cGMP staining inSTZ rats was almost restored by vardenafil treatment(Figure 2E–F, and I). Tubular cGMP staining showed similarresults, which indicates that vardenafil could preserve intra-cellular cGMP levels in diabetic kidneys (Figure 2J). Doubleimmunostaining depicted remarkable glomerular co-localiz-ation of cGMP and nephrin in controls and STZ-Vard
Table 1. Serum cGMP levels, metabolic parameters, kidney weights, serum urea levels and MAPwere measured at the time of harvest
Serum cGMP(pmol/mL)
Serum glucose(mmol/L)
Bodyweight (g)
Kidney weight/body weight (g/g)
Serum urea(mg/dL)
MAP(mmHg)
Control 14.3 ± 9.5 12.3 ± 4.0 349 ± 27 0.46 ± 0.05 53.1 ± 9.8 77.2 ± 8.1
STZ 7.5 ± 1.4 33.6 ± 5.3* 332 ± 35* 0.64 ± 0.04* 73.2 ± 16.7 72.8 ± 5.1
STZ-Vard 26.9 ± 13.3# 35.5 ± 8.5* 317 ± 71* 0.66 ± 0.13* 64.1 ± 13.9 77.6 ± 12.8
Data are presented as mean ± SD.MAP, mean arterial pressure.*P < 0.05 versus Control.#P < 0.05 versus STZ (ANOVA).
F IGURE 1 : Kidney histology and urinary protein/creatinine ratio at harvest. Representative photomicrographs of PAS-stained kidneys (×400magnification) show normal glomerular structure in the control (A), mild mesangial expansion and attachment to Bowman’s capsule in the STZ(B) and normal structure in the STZ-Vard (C) groups (bar represents 50 μm). (D–E) Glomerular and tubulointerstitial damage index scoresfrom each group are shown. (F) Urinary protein/creatinine ratio (mg protein/mg creatinine) is shown. Data are presented as mean ± SD.*P < 0.05 versus control; #P < 0.05 versus STZ (Kruskal–Wallis).
ORIG
INALARTIC
LE
L. Fang et al.
1754
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

F IGURE 2 : Immunostaining for fibronectin and intracellular cGMP was performed. Representative photomicrographs of fibronectin-stainedglomeruli and tubulointerstitium (×400 magnification) show mild staining in the control (A), increased glomerular and tubulointerstitial fibro-nectin staining in the STZ (B) and mild fibronectin staining in the STZ-Vard (C) groups (bar represents 50 μm). Glomerular (G) and tubuloin-terstitial (H) fibronectin immunoreactivity scores from each group are shown. (D–F) Representative photomicrographs of glomerular cGMPstaining (×630 magnification) where arrows point on podocytes (inset: podocytes are further magnified to ×1000). The intensive immunoreactiv-ity in control, presumably localized to podocytes (arrows) and endothelial cells (D), was almost absent in the STZ (E) but restored in the STZ-Vard (F) groups (bar represents 50 μm). Evaluation of cGMP staining in glomeruli (I) and tubular cells (J). Data are presented as mean ± SD.*P < 0.05 versus Control; #P < 0.05 versus STZ (Kruskal–Wallis).
ORIG
INALARTIC
LE
V a r d e n a fi l p r o t e c t s p o d o c y t e s i n d i a b e t e s
1755
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

F IGURE 3 : Immunostaining for TGF-β1, desmin and nephrin were performed in paraffin-embedded kidney sections. Representative photo-micrographs of TGF-β1-stained glomeruli and tubulointerstitium (×400 magnification) show no staining in control (A), strong glomerular andmild tubulointerstitial TGF-β1 expression in the STZ (B) but only weak TGF-β1 expression in the STZ-Vard (C) groups (bar represents 50 μm).Glomerular (G) and tubulointerstitial (H) TGF-β1 staining scores from each group are shown. Desmin and nephrin immunostaining were per-formed to evaluate podocyte damage. Representative photomicrographs of desmin-stained glomeruli (×630 magnification) show no desminstaining in the control (D), strong desmin expression in podocytes of the STZ (E) and only mild desmin expression in podocytes of the STZ-Vard (F) groups (bar represents 50 μm). Desmin (I) and nephrin (J) staining scores from each group are shown. Data are presented as mean ±SD. *P < 0.05 versus control; #P < 0.05 versus STZ (Kruskal–Wallis).
ORIG
INALARTIC
LE
L. Fang et al.
1756
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

kidneys. Compared with non-diabetic controls, cGMP stainingintensity of STZ rats was reduced, and cGMP was practicallyabsent in nephrin-positive podocytes. In contrast, podocytesof vardenafil-treated rats depicted apparently elevated cGMPcontent when compared with non-treated STZ rats (Figure 6).In addition, 2–5% of cGMP-positive glomerular area was notco-localized with nephrin in the capillary loops, representingpresumably endothelial cGMP staining (Supplementary data,Figure S1A–D).
Desmin and nephrin immunostaining were performed toevaluate the extent of podocyte damage [27]. Desmin stainingwas stronger in the STZ group than in non-diabetic controls.
Vardenafil significantly reduced desmin expression to anintermediate level between the STZ and the control levels(Figure 3D, E and I). In contrast, nephrin staining was reducedin STZ rats when compared with non-diabetic controls, but re-stored after chronic vardenafil treatment (Figure 3J). Duringprogression, podocin and nephrin expressions usually becomereduced in podocytes, and that is accompanied by increasedproteinuria. In our study, both nephrin and podocin mRNAexpression levels in diabetic rats were reduced by ∼50% whencompared with non-diabetic controls, but vardenafil treatmentrestored nephrin and podocin mRNA expression to normallevels (Figure 4B and C).
Vardenafil had no effect on oxidative stress markers ofdiabetic rats
Diabetic kidneys presented strong nitrotyrosine immunor-eactivity both in glomeruli and in tubulointerstitium as amarker of local nitrosoxidative stress [28]. Vardenafil had nosignificant influence on the amount of renal nitrotyrosine for-mation (Table 2). Serum TBARS levels (which reflect theamount of systemic lipid peroxidation) did not show signifi-cant difference among the groups (Control: 1.18 ± 0.12; STZ:1.00 ± 0.15; STZ-Vard: 0.89 ± 0.10 MDA unit/mL; n.s.,ANOVA).
Expression of nNOS mRNA was significantly increased indiabetic groups regardless of treatment protocol (Table 2).Although non-treated diabetic kidneys expressed slightlyhigher levels of eNOS mRNA than non-diabetic controls, thedifferences were not statistically significant and vardenafil didnot alter eNOS expression (Table 2). The mRNA expression ofiNOS was similar in all groups (Table 2).
DISCUSSION
DN is characterized by oxidative stress, podocyte damage andglomerulosclerosis, accompanied by increased PDE-5 activitywhich exacerbates NO-cGMP pathway dysfunction. PDE-5inhibition has been shown to ameliorate experimental DN, yetthe role of podocytes in this mechanism remains unclear. The
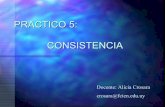
F IGURE 4 : Expression levels of TGF-β1 (A), nephrin (B) and podocin (C) mRNA from kidneys of each group are shown. Data are presentedas mean ± SD. *P < 0.05 versus control; #P < 0.05 versus STZ (Kruskal–Wallis).
F IGURE 5 : Immunoblot analysis of renal PDE-5 expression. Repre-sentative blots for PDE-5 (132 kDa) and GAPDH (38 kDa) areshown (n = 2/group). PDE-5 expression in each group was calculatedas a mean of three separate gels (n = 2/group/gel). PDE-5 was nor-malized to GAPDH and expressed as fold expression relative tocontrol sample. *P < 0.05 versus control, Kruskal–Wallis test.
ORIG
INALARTIC
LE
V a r d e n a fi l p r o t e c t s p o d o c y t e s i n d i a b e t e s
1757
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

present study provides the first in vivo evidence that pharma-cological treatment with selective PDE-5 inhibitor vardenafilattenuates renal damage in type 1 diabetic rats by raising intra-cellular cGMP content of podocytes, and restoring nephrinand podocin expression. Based on the results, we suggest thatdisturbances of NO-cGMP pathway due to PDE-5 overactivityin diabetes might significantly account for pathologicalchanges in podocytes.
Vardenafil is a highly selective inhibitor of PDE-5 thatcauses accumulation of NO-driven cGMP. Vardenafil has beensuccessfully used in the treatment of erectile dysfunction ofdiabetic patients [29], yet its effects on podocytes have notbeen evaluated.
An increasing number of studies suggest that reduced NOproduction in diabetes results in glomerular damage, yet the
molecular mechanisms remain unclear [30]. TGF-β1 plays acrucial role in the progression of glomerulosclerosis [31, 32],characterized by the accumulation of extracellular matrix(ECM) components such as fibronectin [25, 33]. In mesangialcells, hyperglycaemia induces the production of latent TGF-β1[34] and thrombospondin-1 (TSP-1), an activator of latentTGF-β1 [35]. In our study, vardenafil attenuated mesangial ex-pansion, tubular damage, TGF-β1 and fibronectin expression,corroborating the recent report of Kuno et al. [21] on sildena-fil-treated type 2 diabetic rats.
Accumulating evidence suggests a major role for podocytesin the pathogenesis of DN [4, 36]. Podocytes stimulated byhigh glucose and proteinuria may induce AngII-dependentTGF-β1 expression of mesangial cells [4, 37]. Albumin directlystimulates TGF-β1 production in podocytes [38], while high
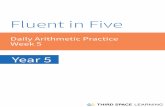
F IGURE 6 : Localization of nephrin and cGMP on podocytes with dual immunofluorescent labelling. Nephrin staining depicts podocytes inglomeruli of control, STZ and STZ-Vard rats (green colour, left pane). Glomerular cGMP is abundantly detected in control and STZ-Vardkidneys, while it is almost absent in glomeruli of non-treated STZ rats (red colour, middle pane). The dual-labelling (yellow colour, right pane)shows co-localization of cGMP and nephrin and indicates that diabetes and vardenafil treatment influence cGMP content of podocytes (×630magnification, bar represents 50 μm).
Table 2. Results of renal immunohistochemistry and quantitative RT–PCR (qPCR) studies
Nitrotyrosine qPCR of NO synthase isoforms
Glomerular Tubular eNOS nNOS iNOS
Control 0.19 ± 0.08 0.18 ± 0.15 0.66 ± 0.12 0.81 ± 0.39 0.63 ± 0.17
STZ 0.64 ± 0.07* 0.56 ± 0.11* 0.96 ± 0.16 9.68 ± 3.28* 0.65 ± 0.24
STZ-Vard 0.56 ± 0.14* 0.59 ± 0.07* 0.93 ± 0.28 5.29 ± 2.09*,# 0.47 ± 0.19
Light microscopy was used at magnification of ×400 for semiquantitative scoring of immunostaining. qPCR results were normalized toGAPDH and expressed using the formula 2−ΔΔCt. All data are presented as mean ± SD.*P < 0.05 versus control.#P < 0.05 versus STZ (Kruskal–Wallis).
ORIG
INALARTIC
LE
L. Fang et al.
1758
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

glucose increases podocyte sensitivity to ambient TGF-β1 [39]and induces TSP-1 production in podocytes [40]. Thus, podo-cytes may contribute to the activation of latent TGF-β1secreted by mesangial cells in diabetes. Finally, mesangialTGF-β1 overproduction in diabetes [34, 39, 41] may, in return,promote podocyte damage, effacement [42] and apoptosis[43].
In diabetic kidneys, podocytes show cytoskeletal redistribu-tion and widening of foot processes along with reducednephrin and podocin expression [4, 36]. Nephrin and podocinare major components of the slit diaphragm between foot pro-cesses, and their loss contributes to pathological filtration,leading to proteinuria [44, 45]. We found reduced nephrinand podocin expression and significant proteinuria in kidneysof non-treated diabetic rats, while vardenafil treatment re-stored nephrin and podocin expression and reduced protei-nuria almost to the normal level.
We suggest that these beneficial effects of vardenafil on po-docytes in vivo were due to an increase in intracellular cGMPlevel, as shown by immunostaining. Compared with podo-cytes, the minor changes in glomerular endothelial cGMP im-munoreactivity suggest that it contributed marginally to theglomerular effects of vardenafil. In podocytes, cGMP regulatesthe filtration barrier by modulating the slit membrane andcytoskeletal protein reorganization [9, 10]. In mesangial cells,cGMP-dependent protein kinase (PKG) inhibits glucose-induced TSP-1 expression [46] and vardenafil was reported todecrease TSP-1 expression in anti-Thy1 nephritic rats [47].Therefore, decreased cGMP levels in diabetes might accountfor podocyte damage, reduced nephrin and podocinexpression and proteinuria. We suggest that the preservationof podocyte cGMP content significantly accounts for restorednephrin and podocin expression. In addition, restoring podo-cyte and circulating cGMP levels might reduce the glomerularactivation of latent TGF-β1, as supported by reduced glomeru-lar TGF-β1 immunostaining.
PDE-5 inhibition might also improve diabetic kidneydisease by its potential anti-inflammatory, anti-oxidative orhaemodynamic effects. Experimental renal mass reductionstudies have shown that sildenafil, another selective PDE-5inhibitor, may reduce inflammatory infiltration and oxidativestress [15]. In our study, however, vardenafil had no effect onrenal mononuclear cell infiltration. One explanation may bethat in our model, tubulointerstitial infiltration was not signifi-cant in non-treated diabetic animals when compared withnon-diabetic controls. Secondly, different PDE-5 inhibitorsmay exert different effects on inflammation [48]. In fact, Ho-henstein et al. [47] have recently reported that vardenafiladministration did not affect renal inflammatory cell influx inexperimental glomerulonephritis.
In diabetes, not only high glucose but also the increasedgeneration of ROS may contribute to augmented AngII pro-duction in podocytes [4], leading to mesangial TGF-β1 over-production. It has been reported that intracellular cGMPaccumulation reduce oxidative injury of the tissues in diabetes[49] and sildenafil reduces superoxide generation [50]. Wehave therefore postulated that vardenafil would decrease oxi-dative stress in the kidneys. In contrast to our expectations, we
could not confirm the potential antioxidative effect of varde-nafil in our model. Neither serum TBARS concentration norrenal nitrotyrosine immunostaining showed significant differ-ences in any diabetic groups studied.
Potential renal haemodynamic changes would also be ex-pected due to PDE-5 inhibition. The elevated serum cGMPlevel presumably covered the biological effects of NO; never-theless, the NO production remained unchanged. This mayraise the question whether changes in cGMP levels could in-terfere with blood pressure and, consecutively, with renaldamage. As the MAP did not differ considerably amongtreated and non-treated rats, the beneficial effects of vardenafilon renal pathology were independent of blood pressure.
Nitric oxide causes vasodilatation in the afferent arterioles[8] which leads to glomerular hypertension and hyperfiltra-tion. Elevating the levels of cGMP, the effector of NO, by var-denafil administration would be therefore expected toaggravate glomerular hyperfiltration. Recent studies, however,do not confirm this hypothesis. In the study of Lau et al. [19],vardenafil administration did not induce hyperfiltration in dia-betic rabbits, and sildenafil treatment of type 2 diabetic ratswas reported to attenuate hyperfiltration [21] instead of aggra-vating it. In our study, relative kidney weights were not differ-ent in diabetic groups regardless of vardenafil treatment,suggesting that PDE-5 inhibition with vardenafil did not influ-ence renal hyperfiltration.
These findings suggest that the observed beneficial effectsof vardenafil on podocytes in vivo were mostly due to an in-crease in intracellular cGMP content.
We conclude that in the STZ model of diabetes, pharmaco-logical inhibition of PDE-5 by vardenafil raised serum cGMPlevels, preserved intracellular cGMP levels of podocytes andpodocyte function by restoring nephrin and podocinexpression. The beneficial effects of selective PDE-5 inhibitionon the progression of DN were independent of blood pressureor the extent of nitrosoxidative stress. Our findings pinpointthe podocytes as target cells that suffer NO-cGMP signallingdisturbances in diabetes. The observation of the beneficialeffect of restoring cGMP levels on podocyte and renal damagein type 1 diabetes might suggest the possible use of vardenafilas a new regimen in the treatment of DN.
SUPPLEMENTARY DATA
Supplementary data are available online at http://ndt.oxfordjournals.org.
ACKNOWLEDGEMENTS
The technical assistance of Krisztina Fazekas, Magdolna Pekárand Heike Ziebart is gratefully acknowledged. This work waspartly supported by a grant from the Hungarian Society forHypertension.
ORIG
INALARTIC
LE
V a r d e n a fi l p r o t e c t s p o d o c y t e s i n d i a b e t e s
1759
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
1. ERA-EDTA. ERA-EDTA Registry Annual Report 2008. Amster-dam, The Netherlands: Academic Medical Center, Departmentof Medical Informatics, 2010
2. USRDS. Atlas of Chronic Kidney Disease and End-Stage RenalDisease in the United States. MD: National Institutes of HealthBethesda, U.S. Renal Data System, 2010
3. Suzuki D, Miyata T, Saotome N et al. Immunohistochemical evi-dence for an increased oxidative stress and carbonyl modificationof proteins in diabetic glomerular lesions. J Am Soc Nephrol1999; 10: 822–832
4. Wolf G, Chen S, Ziyadeh FN. From the periphery of the glomeru-lar capillary wall toward the center of disease: podocyte injurycomes of age in diabetic nephropathy. Diabetes 2005; 54:1626–1634
5. Mauer SM. Structural–functional correlations of diabetic nephro-pathy. Kidney Int 1994; 45: 612–622
6. Ballermann BJ, Marsden PA. Endothelium-derived vasoactivemediators and renal glomerular function. Clin Invest Med 1991;14: 508–517
7. Knight S, Snellen H, Humphreys M et al. Increased renal phos-phodiesterase-5 activity mediates the blunted natriuretic responseto ANP in the pregnant rat. Am J Physiol Renal Physiol 2007;292: F655–F659
8. Raij L, Baylis C. Glomerular actions of nitric oxide. Kidney Int1995; 48: 20–32
9. Pavenstadt H. Roles of the podocyte in glomerular function. AmJ Physiol Renal Physiol 2000; 278: F173–F179
10. Sharma R, Lovell HB, Wiegmann TB et al. Vasoactive substancesinduce cytoskeletal changes in cultured rat glomerular epithelialcells. J Am Soc Nephrol 1992; 3: 1131–1138
11. Craven PA, Studer RK, DeRubertis FR. Impaired nitric oxide-de-pendent cyclic guanosine monophosphate generation in glomer-uli from diabetic rats. Evidence for protein kinase C-mediatedsuppression of the cholinergic response. J Clin Invest 1994; 93:311–320
12. Pacher P, Obrosova IG, Mabley JG et al. Role of nitrosative stressand peroxynitrite in the pathogenesis of diabetic complications.Emerging new therapeutical strategies. Curr Med Chem 2005; 12:267–275
13. Dousa TP. Cyclic-30,50-nucleotide phosphodiesterase isozymes incell biology and pathophysiology of the kidney. Kidney Int 1999;55: 29–62
14. Matousovic K, Tsuboi Y, Walker H et al. Inhibitors of cyclicnucleotide phosphodiesterase isozymes block renal tubular cellproliferation induced by folic acid. J Lab Clin Med 1997; 130:487–495
15. Rodriguez-Iturbe B, Ferrebuz A, Vanegas V et al. Early treatmentwith cGMP phosphodiesterase inhibitor ameliorates progressionof renal damage. Kidney Int 2005; 68: 2131–2142
16. Dousa TP. Signaling role of PDE isozymes in pathobiology of glo-merular mesangial cells. Studies in vitro and in vivo. CellBiochem Biophys 1998; 29: 19–34
17. Ghali-Ghoul R, Tahseldar-Roumieh R, Sabra R. Effect of chronicadministration of sildenafil on sodium retention and on the he-modynamic complications associated with liver cirrhosis in therat. Eur J Pharmacol 2007; 572: 49–56
18. Lledo-Garcia E, Rodriguez-Martinez D, Cabello-Benavente Ret al. Sildenafil improves immediate posttransplant parameters inwarm-ischemic kidney transplants: experimental study. Trans-plant Proc 2007; 39: 1354–1356
19. Lau DH, Mikhailidis DP, Thompson CS. The effect of vardenafil(a PDE type 5 inhibitor) on renal function in the diabetic rabbit:a pilot study. In Vivo 2007; 21: 851–854
20. Jeong KH, Lee TW, Ihm CG et al. Effects of sildenafil onoxidative and inflammatory injuries of the kidney instreptozotocin-induced diabetic rats. Am J Nephrol 2009; 29:274–282
21. Kuno Y, Iyoda M, Shibata T et al. Sildenafil, a phosphodiesterasetype 5 inhibitor, attenuates diabetic nephropathy in non-insulin-dependent Otsuka Long-Evans Tokushima Fatty rats. Br J Phar-macol 2011; 162: 1389–1400
22. Lee HS. Pathogenic role of TGF-beta in the progression of podo-cyte diseases. Histol Histopathol 2011; 26: 107–116
23. Wolf G, Ritz E. Combination therapy with ACE inhibitors andangiotensin II receptor blockers to halt progression of chronicrenal disease: pathophysiology and indications. Kidney Int 2005;67: 799–812
24. el Nahas AM, Zoob SN, Evans DJ et al. Chronic renal failure afternephrotoxic nephritis in rats: contributions to progression.Kidney Int 1987; 32: 173–180
25. Piecha G, Kokeny G, Nakagawa K et al. Calcimimetic R-568 orcalcitriol: equally beneficial on progression of renal damage insubtotally nephrectomized rats. Am J Physiol Renal Physiol 2008;294: F748–F757
26. Hirschberg K, Radovits T, Loganathan S et al. Selective phospho-diesterase-5 inhibition reduces neointimal hyperplasia in ratcarotid arteries after surgical endarterectomy. J Thorac Cardio-vasc Surg 2009; 137: 1508–1514
27. Floege J, Kriz W, Schulze M et al. Basic fibroblast growth factoraugments podocyte injury and induces glomerulosclerosis in ratswith experimental membranous nephropathy. J Clin Invest 1995;96: 2809–2819
28. Vaziri ND, Ni Z, Oveisi F et al. Enhanced nitric oxide inacti-vation and protein nitration by reactive oxygen species in renalinsufficiency. Hypertension 2002; 39: 135–141
29. Goldstein I, Young JM, Fischer J et al. Vardenafil, a new phos-phodiesterase type 5 inhibitor, in the treatment of erectile dys-function in men with diabetes: a multicenter double-blindplacebo-controlled fixed-dose study. Diabetes Care 2003; 26:777–783
30. Zhao HJ, Wang S, Cheng H et al. Endothelial nitric oxidesynthase deficiency produces accelerated nephropathy in diabeticmice. J Am Soc Nephrol 2006; 17: 2664–2669
31. Han DC, Hoffman BB, Hong SW et al. Therapy with antisenseTGF-beta1 oligodeoxynucleotides reduces kidney weight andmatrix mRNAs in diabetic mice. Am J Physiol Renal Physiol2000; 278: F628–F634
ORIG
INALARTIC
LE
L. Fang et al.
1760
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from

32. Ziyadeh FN, Hoffman BB, Han DC et al. Long-term preventionof renal insufficiency, excess matrix gene expression, and glomer-ular mesangial matrix expansion by treatment with monoclonalantitransforming growth factor-beta antibody in db/db diabeticmice. Proc Natl Acad Sci USA 2000; 97: 8015–8020
33. Floege J, Alpers CE, Burns MW et al. Glomerular cells, extracellu-lar matrix accumulation, and the development of glomerulo-sclerosis in the remnant kidney model. Lab Invest 1992; 66:485–497
34. Wolf G, Schroeder R, Zahner G et al. High glucose-induced hy-pertrophy of mesangial cells requires p27(Kip1), an inhibitor ofcyclin-dependent kinases. Am J Pathol 2001; 158: 1091–1100
35. Yevdokimova N, Wahab NA, Mason RM. Thrombospondin-1 isthe key activator of TGF-beta1 in human mesangial cells exposedto high glucose. J Am Soc Nephrol 2001; 12: 703–712
36. Jefferson JA, Shankland SJ, Pichler RH. Proteinuria in diabetickidney disease: a mechanistic viewpoint. Kidney Int 2008; 74:22–36
37. Wolf G, Butzmann U, Wenzel UO. The renin–angiotensinsystem and progression of renal disease: from hemodynamics tocell biology. Nephron Physiol 2003; 93: P3–P13
38. Abbate M, Zoja C, Morigi M et al. Transforming growth factor-beta1 is up-regulated by podocytes in response to excess intraglo-merular passage of proteins: a central pathway in progressive glo-merulosclerosis. Am J Pathol 2002; 161: 2179–2193
39. Iglesias-de la Cruz MC, Ziyadeh FN, Isono M et al. Effects ofhigh glucose and TGF-beta1 on the expression of collagen IV andvascular endothelial growth factor in mouse podocytes. KidneyInt 2002; 62: 901–913
40. Han SH, Yang S, Jung DS et al. Gene expression patterns inglucose-stimulated podocytes. Biochem Biophys Res Commun2008; 370: 514–518
41. Chen S, Jim B, Ziyadeh FN. Diabetic nephropathy and transform-ing growth factor-beta: transforming our view of glomerulo-sclerosis and fibrosis build-up. Semin Nephrol 2003; 23:532–543
42. Dessapt C, Baradez MO, Hayward A et al. Mechanical forces andTGFbeta1 reduce podocyte adhesion through alpha3beta1
integrin downregulation. Nephrol Dial Transplant 2009; 24:2645–2655
43. Wu DT, Bitzer M, Ju W et al. TGF-beta concentrationspecifies differential signaling profiles of growth arrest/differen-tiation and apoptosis in podocytes. J Am Soc Nephrol 2005; 16:3211–3221
44. Putaala H, Soininen R, Kilpelainen P et al. The murine nephringene is specifically expressed in kidney, brain and pancreas: inac-tivation of the gene leads to massive proteinuria and neonataldeath. HumMol Genet 2001; 10: 1–8
45. Roselli S, Heidet L, Sich M et al. Early glomerular filtration defectand severe renal disease in podocin-deficient mice. Mol Cell Biol2004; 24: 550–560
46. Wang S, Skorczewski J, Feng X et al. Glucose up-regulates throm-bospondin 1 gene transcription and transforming growth factor-beta activity through antagonism of cGMP-dependent proteinkinase repression via upstream stimulatory factor 2. J Biol Chem2004; 279: 34311–34322
47. Hohenstein B, Daniel C, Wittmann S et al. PDE-5 inhibitionimpedes TSP-1 expression, TGF-beta activation and matrixaccumulation in experimental glomerulonephritis. Nephrol DialTransplant 2008; 23: 3427–3436
48. Roumeguere T, Zouaoui Boudjeltia K, Babar S et al. Effects ofphosphodiesterase inhibitors on the inflammatory response ofendothelial cells stimulated by myeloperoxidase-modified low-density lipoprotein or tumor necrosis factor alpha. Eur Urol2010; 57: 522–528
49. Milani E, Nikfar S, Khorasani R et al. Reduction of diabetes-induced oxidative stress by phosphodiesterase inhibitors in rats.Comp Biochem Physiol C Toxicol Pharmacol 2005; 140: 251–255
50. Koupparis AJ, Jeremy JY, Muzaffar S et al. Sildenafil inhibits theformation of superoxide and the expression of gp47 NAD[P]Hoxidase induced by the thromboxane A2 mimetic, U46619, incorpus cavernosal smooth muscle cells. BJU Int 2005; 96:423–427
Received for publication: 30.9.2011; Accepted in revised form: 18.7.2012
ORIG
INALARTIC
LE
V a r d e n a fi l p r o t e c t s p o d o c y t e s i n d i a b e t e s
1761
by guest on February 26, 2016http://ndt.oxfordjournals.org/
Dow
nloaded from
Copyright © 2022 FDOKUMEN