
Order and segmental mobility during polymer crystallization: Poly(butylene isophthalate)
Upload
independentCategory
view
0download
0
Segmental odontomaxillary dysplasia: report of a series of 5cases with long-term follow-up
Joseph C. Whitt, DDS, MS,a James W. Rokos, DDS, MS,b Charles L. Dunlap, DDS,c andBruce F. Barker, DDS,c Kansas City, MOUNIVERSITY OF MISSOURI
We report a series of 5 cases of segmental odontomaxillary dysplasia (SOMD) with follow-up periods rangingfrom 8 to 21 years, bringing the total number of reported cases to 45. SOMD is a sporadic, mesoectodermal dysplasiathat presents early in life, possibly as early as in utero and exhibits male gender predominance (1.7:1.0). Its featuresinclude enlargement of the soft tissue and/or bone of 1 hemimaxilla that may produce mild facial asymmetry.Subsequent growth of the affected area is proportional to that of the unaffected hemimaxilla. Sclerotic radiographicbone changes and dental developmental abnormalities are also present. The dense bone, which often exhibits aradiographic vertical orientation of the trabecular bone pattern, is typically associated with delayed eruption of theteeth. Congenitally missing premolar teeth (either or both) is a common feature of this condition that is of significantdiagnostic value. Although ipsilateral cutaneous findings have been reported in 23%, our cases exhibited none.Computed tomographic imaging demonstrated extensive involvement of the maxillary bone, including the lateral walland floor of the maxillary sinus and the hard palate. The affected bone presents no impediment to either orthodontictooth movement or to the successful osteointegration of dental implants. The cause of SOMD is unknown; the clues tothe cause of this unusual phenotypic expression are buried in the intricacies of developmental biology within the first
branchial arch. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:e29-e47)First described in 1987,1 segmental odontomaxillarydysplasia (SOMD) is a noninherited, sporadic, devel-opmental, mesoectodermal dysplasia that presents earlyin life and is characterized by asymptomatic enlarge-ment of 1 hemimaxilla that exhibits growth proportion-ate to the remainder of the maxillofacial complex. Itmay be accompanied by mild facial asymmetry second-ary to the hemimaxillary enlargement.2-4 A number ofvariable features may be seen in the affected region,including increased spacing and delayed eruption ofteeth, hypoplasia, malformation and abnormal resorp-tion of primary molars, hypodontia involving the per-manent premolar teeth, and fibrous hyperplasia of theoverlying soft tissues.3 Radiographically, the bone ofthe affected region exhibits localized, ill-defined in-creased bone density owing to coarse, irregular trabec-ulae with a variable vertical orientation.3,5 Encroach-
aProfessor, Oral and Maxillofacial Pathology, School of Dentistry,University of Missouri School of Dentistry.bAssistant Professor, Oral and Maxillofacial Pathology, School ofDentistry, University of Missouri School of Dentistry.cProfessor Emeritus, Oral and Maxillofacial Pathology, School ofDentistry, University of Missouri School of Dentistry.Received for publication Jan 11, 2011; returned for revision Mar 2,2011; accepted for publication Mar 7, 2011.1079-2104/$ - see front matter© 2011 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2011.03.013ment on the maxillary sinus may reduce its volume.The cause and pathogenesis of SOMD are unknown.
The original report of 2 cases was published ashemimaxillofacial dysplasia (HD).1 The authors of thesecond report of 8 cases suggested segmental odon-tomaxillary dysplasia as more descriptive.2 There havebeen 13 additional publications,3,4,6-16 bringing the to-tal number of reported cases to 40. Table I summarizesthe general clinical features of the 40 previously re-ported cases of SOMD and the 5 additional cases pre-sented here. We excluded 2 reports from inclusion inour review. One report17 provided insufficient clinical,historical, and radiographic information to substantiatethe diagnosis of SOMD; we were unable to exclude thepossibility that this case represents fibrous dysplasia onthe basis of the information provided. A second report18
was excluded because it fails to meet the establisheddiagnostic criteria for SOMD.1,2
The prevalence of SOMD is unknown, as only singlecases or series of cases have been reported. It is prob-ably more common than the literature indicates, be-cause it is likely that cases have been classified asfibrous dysplasia or atypical fibrous dysplasia.2 Sev-eral2,3,7 have cited an example of a case with featuresconsistent with SOMD as representing a portion of theradiographic spectrum of fibrous dysplasia.19,20
The purpose of this article is to review the literature
and present 5 additional cases of this rare developmen-e29

OOOOEe30 Whitt et al. August 2011
Table I. Demographic and general clinical features of previously reported cases of SOMD, including the present 5cases, in reverse chronologic order of publication
AuthorAge in years at
time of diagnosis GenderAffected
side Hypodontia Ipsilateral cutaneous findings Comments
Whitt et al. Case # 1 4 F R Both PM missing None present 21 years of follow-up,orthodontictreatment, 2 dentalimplantsosteointegrated with8 years of follow-up
Whitt et al. Case # 2 13 M R Both PM present None present 11 years of follow-up,orthodontic treatment
Whitt et al. Case # 3 11 F R 1st PM missing None present 8 years of follow-up,orthodontic treatment
Whitt et al. Case # 4 4 M R Both PM present None present 15 years of follow-up,orthodontic treatment
Whitt et al. Case # 5 9 M R 2nd PM missing None present 10 years of follow-up,orthodontic treatment
Bhatia et al. (2008)8 3 M L Both PM missing Ectopic eyelashes 4 years of follow-upKoenig et al. (2008)13 26 F R Both PM missing Hypertrichosis, commissural
lip cleft, hyperlinear palmsVertical alveolar defect
at distal of canineArmstrong et al. (2004)6
Case # 13.5 M L 1st PM missing Not stated TE primary canine
Armstrong et al. (2004)6
Case # 23.5 M L 2nd PM missing Not stated 7.5 years of follow-up,
TE primary canineand primary 1stmolar
Gavalda (2004)11 8 M R 2nd PM missing Not reported. Image exhibitsno lesions
Welsch and Stein(2004)16
5 M L One unspecified PMmissing
Becker’s nevus
Drake (2003)10 7 M L Both PM missing None presentBecktor et al. (2002)7
Case # 13 F L 1st PM missing Erythema Dental implant,
osteointegrated withshort-term follow-up
Becktor et al. (2002)7
Case # 28 M L 2nd PM missing None present 6 years of follow-up,
TE primary molarsBecktor et al. (2002)7
Case # 32 M L Both PM missing Erythema 10 years of follow-up,
TE permanent firstmolar
Becktor et al. (2002)7
Case # 43 M L 1st PM missing None present 3 years of follow-up
Velez et al. (2002)15
Case # 13.5 M R NR Hyperpigmentation and
hypertrichosisVelez et al. (2002)15
Case # 214 F L Both PM present None present
Prusack et al. (2000)4 9 F R Both PM missing, 3M missing,
None present
Jones and Ford (1999)12 7 M L Both PM missing, 3M missing,
Becker’s nevus Vertical alveolar defectat distal of canine
Paticoff et al. (1997)14
Case # 123 M R 2nd PM missing Hairy nevus Special education,
speech delays,mental illness,orthodontic treatment
Paticoff et al. (1997)14
Case # 27 M R 1st PM missing Hypertrichosis
DeSalvo et al. (1996)9 4 F L NR Upper lip hypopigmentationPackota et al. (1996)3
Case # 614 M L Both PM missing Discontinuity of vermillion
border with depression ofcheek commissural cleftand bilateral commissural
pits
oth ext
OOOOEVolume 112, Number 2 Whitt et al. e31
tal disorder. Extended follow-up periods from ranging8 to 21 years confirm the nonprogressive clinical be-
Fig. 1. Case 1. Clinical images depicting the patient’s appproduced no significant facial asymmetry beyond a mildimension of the maxillary alveolus extended from the mesof the primary molar teeth were hypoplastic and there wexposed in a mirror reflection).
Table I. Continued
AuthorAge in years at time
of diagnosis Gender A
Packota et al. (1996)3
(11 remaining cases)5, 6, 9, 11, 16,
27 (NR for 5patients)
6 M, 5 F
Danforth et al. (1990)2
Case # 16 M
Danforth et al. (1990)2
Case # 24 F
Danforth et al. (1990)2
Case # 38 M
Danforth et al. (1990)2
Case # 46 F
Danforth et al. (1990)2
Case # 512 M
Danforth et al. (1990)2
Case # 68 M
Danforth et al. (1990)2
Case # 76 F
Danforth et al. (1990)2
Case # 828 F
Miles et al. (1987)1
Case # 115 M
Miles et al. (1987)1
Case # 23.5 F
F, female; L, left side; M, male; PM, premolar; R, right side; TE, to
havior. Most reports of SOMD have appeared in the
oral and maxillofacial surgery, pathology, and radiol-ogy literature, with only 3 reports in the pediatric
e at age 4 years. The lesion involved the right maxilla andess of the right upper lip. The increased buccolingual
the primary canine to the tuberosity. The occlusal surfacescing between the primary teeth (the intraoral image was
side HypodontiaIpsilateral cutaneous
findings Comments
4 9 cases missingboth PMs, 2cases missing 1PM
Not reported
2nd PM missing None present
Both PM missing None present
Both PM missing,primary caninemissing
None present
Both PM missing Not stated
2nd PM missing Not stated
2nd PM missing Not stated
1st PM missing Not stated
Both PM missing Not stated
Both PM missing Hypertrichosis
Both PM present Not stated
raction; NR, not reported.
earancd fullnial ofas spa
ffected
L7, R
R
R
L
R
R
R
L
R
R
L
dentistry literature8,9,13 and 1 in the orthodontic litera-

asymmetry. Both permanent premolar teeth were missing and the p
region. The permanent premolars were missing and there is retenti
gingival mucosa of the affected side.
OOOOEe32 Whitt et al. August 2011
ture.10 Wider recognition and reporting of this condi-tion will aid in elucidating its prevalence and manifes-tations.
CASE REPORTCase 1
This 4-year-old girl was seen in 1986, 1 year before theinitial recognition of this condition as a specific entity.1 Sheexhibited unilateral enlargement of the right maxilla thatproduced mild asymmetry of the right upper lip, characterizedby a taut appearance of the overlying vermillion, with morefullness compared with the contralateral side. Intraorally, theright maxilla exhibited enlargement extending from the me-sial of the primary canine to the tuberosity, accompanied byincreased spacing between the primary teeth (Fig. 1). Theocclusal surfaces of both primary molars exhibited hypopla-sia.
The lesion was investigated with multiple imaging meth-ods, including periapical radiographs, panoramic radiographs,
a moderate increase in buccolingual dimension that wasinvolve the incisor region. It caused no significant facial
ermanent canine tooth was positioned distally.
rged area extended from the tuberosity to the canine-incisoron of the second primary molar.
Fig. 2. Case 1. Clinical images at age 14. The lesion exhibitedproportionate to overall growth and extended further anteriorly to
Fig. 3. Case 1. The patient’s appearance at age 15 years. The enla
Fig. 4. Case 1. Clinical image depicting the appearance ofpatient’s dentition at age 15 years. The buccal aspect of theright maxilla is enlarged in comparison with the uninvolvedside. There is a sessile, white papule, accompanied by anerythematous, blanchable area of increased vascularity on
and computed tomographic (CT) scanning. Although these

etentio
OOOOEVolume 112, Number 2 Whitt et al. e33
materials could no longer be located for inclusion into thisarticle, the involved area was described as exhibiting anill-defined density of the right maxilla. Bone scintigraphy wasnegative. The patient’s medical history was noncontributoryand there were no associated cutaneous findings. The parents,as well as 2 siblings, were unaffected, although her fatherexhibited congenitally missing mandibular second premolars.Based on the clinical appearance, behavior (asymptomaticlesion with slow enlargement proportional to overall growth),and imaging findings, it was concluded that this lesion rep-resented a developmental process, possibly similar to fibrousdysplasia. It was decided to follow the patient closely. Abiopsy of the lesion was not performed as it was believed thatit was a non-neoplastic lesion with low potential for signifi-cant morbidity.
Over the next 10 years, the lesion exhibited moderateenlargement that was proportionate to overall growth. By theearly teenage years, her maxillary enlargement was slightlymore prominent and the expanded buccolingual dimension ofthe maxilla had advanced anteriorly beyond the canine toinvolve the incisor region (Figs. 2–4). The mild fullness ofthe right upper lip remained and there was no remarkablefacial asymmetry. Both permanent premolar teeth were miss-ing, the secondary primary molar was retained, and the per-manent canine tooth was incompletely erupted. A panoramicradiograph, exposed at the age of 15 years exhibited anill-defined density involving the area of the missing premolarteeth on the affected side (Fig. 5). The permanent secondmolar was unerupted and was extracted after unsuccessfulattempts to facilitate its eruption; the permanent third molarwas subsequently moved into its position.
Over the next 10 years, the lesion exhibited little change.Orthodontic treatment was initiated at age 15. At the age of 17years, 2 dental implants were placed in the area of dense boneto replace the missing premolar teeth. A panoramic radio-graph exposed at age 25 years exhibited a circumscribed areaof bone density involving the maxillary sinus floor that re-duced its size relative to the uninvolved side (Fig. 6). On
Fig. 5. Case 1. Panoramic radiograph at age 15 years, There ispermanent premolars on the affected side, accompanied by r
periapical radiographs, the bony trabeculae of the involved
right maxilla appeared coarse and vertically oriented, com-pared with the normal trabecular bone pattern of the unin-volved left maxilla (Fig. 7).
The patient described a number of small, white, sessilepapules involving the facial gingival mucosa of the affectedregion that had been incised in the past. One such lesioninvolving the buccal gingiva, clinically resembling a dentallamina inclusion cyst of the newborn, was observed in a clinicalimage exposed at the age of 14 years (Fig. 4) and was no longerpresent at clinical follow-up at age 25 years (see Discussionsection). There was a circumscribed, erythematous, blanchablezone of increased vascularity associated with this lesion thatpersisted through the most recent follow-up at age 25 years.
During the 21-year follow-up period, from ages 4 yearsthrough 25 years, enlargement of the lesion was proportionate tothe growth of the uninvolved side. The reduced buccolingualdimension of the affected area (Fig. 8) is the result of surgicalreduction performed to establish physiological tissue contours.This was accomplished about the time of orthodontic therapy.
Case 2This 13-year-old boy presented with delayed eruption of the
teeth of the right maxilla, accompanied by enlargement thatextended from the tuberosity to the incisor area, increased spac-ing between the teeth, and hypoplasia of the second primarymolar (Fig. 9). His chief complaint was fullness of the rightupper lip secondary to the maxillary enlargement (Fig. 10). Thepatient’s medical history was noncontributory. A sibling exhib-ited normal oral findings. There were no associated cutaneousfindings and biopsy of the lesion was not performed.
A panoramic radiograph at age 14 years exhibited a ra-diodensity of the right posterior maxilla that involved thefloor of the maxillary sinus, reducing its size in relation to theuninvolved left side (Fig. 11). Both premolars in the affectedhemimaxilla were present. The second premolar erupted with-out assistance, but the first premolar required surgical expo-sure to assist eruption and, when erupted, exhibited a gray
defined area of bone density involving the area of the missingn of the primary second molar.
an ill-
discoloration and was determined to be nonvital (Fig. 12),

ird mo
appear
OOOOEe34 Whitt et al. August 2011
possibly as a result of the assisted eruption procedure per-formed between the ages of 14 and 18 years.
In a panoramic radiograph exposed at the age of 18 years (Fig.13), the vertically oriented appearance of the involved trabecularbone could be seen clearly and the lesion exhibited a sharplydemarcated anterior margin that was also apparent in periapical(Fig. 14) and oblique radiographs (Fig. 15) exposed at the age of 24years.
Orthodontic treatment was complicated by the soft tissueenlargement that interfered with bracket placement and requiredgingivoplasty to provide access for orthodontic appliances. Clo-sure of the spacing between the teeth of the involved hemimax-illa was not completed because treatment was discontinued whenthe patient entered military service.
A photograph taken at age 18 years exhibited a number of small,
Fig. 6. Case 1. Panoramic radiograph at 25 years. On thecircumscribed area of bone density involving the maxillary sunerupted second permanent molar was extracted and the th
Fig. 7. Case 1. Periapical radiographs at age 25 years. The preosteointegration. The bony trabeculae of the involved right mnormal trabecular bone pattern of the uninvolved left maxillwith the uninvolved side. The anterior margin of the lesion
white, sessile papules, clinically resembling dental lamina inclusion
cysts of the newborn, involving the facial gingival mucosa of theaffected region. These lesions regressed and were not observed atclinical follow-up at age 24 years (see Discussion section).
The photograph of the maxillary arch taken at age 24 years(Fig. 12), gives the impression that the enlarged contour ofthe maxillary anterior alveolus has regressed; however, thisappearance is the result of surgical reduction of the area thatwas performed between the ages of 14 and 18 years to addressthe patient’s chief complaint of fullness of the upper lip. Thepermanent second premolar partially erupted without assis-tance, although chronologically late.
Over the 11-year period of follow-up, between the ages of 13years and 24 years, the lesion did not progress clinically beyondenlargement that was proportional to the growth of the unin-volved side and it exhibited no detectable change in radiographic
t’s right side in the area of the dental implants, there wasoor that reduced its size relative to the uninvolved side. Thelar was moved into its position.
implants were placed at age 17 and underwent uncomplicatedappeared coarse and vertically oriented, compared with the
size of the right maxillary sinus was reduced in comparisoned sharply defined.
patieninus fl
molaraxilla
a. The
appearance.

prem
OOOOEVolume 112, Number 2 Whitt et al. e35
Case 3This 11-year-old girl presented with unilateral expansion
of the right hemimaxilla that produced mild asymmetry of theright upper lip and cheek. The enlarged area extended fromthe tuberosity to the incisor area (Fig. 16) and was accompa-nied by delayed eruption of teeth on the affected side withoutan increase in space between the teeth. The first premolar onthe affected side was missing and the first primary molarexhibited hypoplasia. Radiographically, the affected area ex-hibited an ill-defined radiodensity with a coarse, granulartrabecular pattern (Fig. 17).
At the age of 19 years, a panoramic radiograph exhibited a
Fig. 8. Case 1. Clinical images depicting the patient’s appeareflection). The affected hemimaxilla appears reduced in sizcontours. Dental implants occupy the position of the missing
Fig. 9. Case 2. The appearance of the involved and unin-volved sides of the patient’s maxilla at age 13 years. Therewas an increased buccolingual dimension of the right maxil-lary alveolar process, extending from the incisor area to thetuberosity. The primary second molar was hypoplastic andthere was increased spacing between the teeth of the involvedhemimaxilla.
radiodensity with a coarse, granular pattern and a well-de-
fined anterior margin in the canine-premolar area that hadreduced the size of the maxillary sinus in comparison with theuninvolved side (Fig. 18). Periapical radiographs exhibitedcoarse, granular bone trabeculae with a vertical orientation(Fig. 19). The remaining first premolars in the uninvolvedquadrants were extracted to gain space to facilitate orthodon-tic treatment, during which it was noted that the teeth on theaffected side moved more slowly because of the dense bone.
During the 8-year period of clinical follow-up between theages of 11 years and 19 years, the lesion was stable and didnot exhibit enlargement that was disproportionate to thegrowth of the uninvolved side. At the age of 19 years, theenlargement of the maxillary alveolus appeared to have re-gressed somewhat (Fig. 20); however, this appearance is theresult of surgical reduction of the area that was performed atthe age of 15 years to address the patient’s concerns offullness of the midface on the affected side. Microscopicexamination of the excised mucosa revealed fibrous and fi-bromyxoid hyperplasia, containing thick collagen bundlescommingled with zones of hematoxylinophilic myxoidground substance (Fig. 21). The patient’s medical history wasnoncontributory and there were no associated cutaneous find-ings. A bone biopsy was not performed.
Case 4This 4-year-old boy presented with increased buccolingual
dimension of the right posterior maxilla extending from thetuberosity to the mesial of the primary canine. This wasaccompanied by delayed eruption of the primary first molarand increased spacing between the teeth of the affected side(Fig. 22). Panoramic radiographs exposed at the ages of 4 and5 years (not shown) exhibited an ill-defined radiodensity witha coarse trabecular pattern involving the premolar area of theright maxilla. This was accompanied by marked hypoplasia ofthe unerupted primary first molar. CT imaging of the patient’smaxilla performed at the age of 6 years exhibited a moder-
at age 25 years (the intraoral image was exposed in a mirrorndary to surgical reduction to establish physiological tissueolar teeth.
rancee seco
ately increased buccolingual dimension of the alveolar pro-

olar to
molar
OOOOEe36 Whitt et al. August 2011
cess of the right posterior maxilla. There was a coarse, gran-ular pattern of the trabecular bone in the expanded area andprominent thickening of the anterior and lateral walls of themaxillary sinus that reduced its size in comparison with theunaffected side (Fig. 23).
An incisional biopsy of alveolar bone at age 4 exhibitedcoarse, thickened trabeculae composed of both woven andmature lamellar bone with a pagetoid appearance (Fig. 24).There was no evidence of appositional osteoblastic activity orof active osteoclastic resorption. The marrow spaces con-tained predominately fatty marrow. At the periosteal surface,the cortex was irregular and ill defined and transitionedabruptly to cellular fibrous connective tissue (Fig. 25). Thepatient’s medical history was noncontributory; there were noassociated cutaneous findings and no clinically significant
Fig. 10. Case 2. The patient’s appearance at 14 years (the intrwas fullness of the right upper lip secondary to enlargementaffected side that required surgical exposure of the first prem
Fig. 11. Case 2. Panoramic radiograph at age 14 years. The ithe right maxillary sinus in relation to the uninvolved left sidethe second premolar erupted without assistance, the first pre
facial asymmetry.
A panoramic radiograph taken at age 17 exhibited anill-defined density of the right maxilla that reduced the size ofthe right maxillary sinus in comparison with the uninvolvedside (Fig. 26). Management of unerupted teeth was a partic-ular challenge in this case. The first permanent molar had notfully erupted by the age of 8 years and required 2 years ofactive intervention, including surgical exposure and elastictraction to bring it into occlusion. The permanent canine toothon the affected side was impacted and also required surgicalexposure and traction to bring it into occlusion. Both premo-lars in the affected hemimaxilla were present and eruptedwithout active intervention, although both were delayedchronologically. The first premolar crown was markedly hy-poplastic. We were unable to reconstruct the sequence ofevents to determine whether this represented developmental
mage was exposed in a mirror reflection). His chief complaintalveolar process. There was delayed eruption of teeth on the
assist eruption.
d right maxilla shows a radiodensity that reduced the size ofpremolars in the affected hemimaxilla were present. Althoughrequired surgical exposure to assist eruption.
aoral iof the
nvolve. Both
hypoplasia or environmental hypoplasia, secondary to pulpal

OOOOEVolume 112, Number 2 Whitt et al. e37
disease involving the overlying hypoplastic primary molar(Turner tooth). Both maxillary first premolars were extractedas part of the orthodontic treatment plan. The permanentsecond molar erupted late and did not require intervention tobring it into occlusion.
During the 15-year interval of follow-up, between the agesof 4 years and 19 years, the lesion exhibited clinical enlarge-ment that remained in proportion to the growth of the unin-volved hemimaxilla.
Case 5This 9-year-old boy presented with delayed eruption of teeth
Fig. 12. Case 2. Occlusal images depicting the appearance ofexposed in a mirror reflection. At the age of 18 years, the fira gray discoloration after surgical exposure to assist eruptiobuccolingual dimension of the anterior alveolar process apppatient’s chief complaint of right upper lip asymmetry. The peassistance, although chronologically late.
Fig. 13. Case 2. Panoramic radiograph at the age of 18 yeaincreased bone density involving the alveolar process that redThe bony trabeculae of the affected hemimaxilla exhibit a canterior border.
and increased buccolingual dimension of the right posterior
maxilla (Fig. 27). The right hemimaxilla exhibited an increasedcontour of the facial surface that was more prominent comparedwith the uninvolved side (Fig. 28). A panoramic radiographexhibited an ill-defined radiodensity involving the right maxilla,associated with a missing second premolar in the affected region(Fig. 28). A periapical radiograph of the enlarged posteriormaxilla exhibited diffuse density of the alveolar bone accompa-nied by a coarse, vertically oriented trabecular pattern and irreg-ular root resorption of the second primary molar (Fig. 29). Therewas no increased spacing between the teeth of the involvedhemimaxilla. A CT scan performed at the age of 13 yearsexhibited extensive involvement of the maxillary bone with
ient’s maxilla at ages 18 years (left) and 24 years (right), botholar in the involved hemimaxilla had partially erupted withwas determined to be nonvital. At the age of 24 years thedecreased as the result of surgical reduction to address thent second molar on the affected side partially erupted without
the patient’s right side, there was a circumscribed area ofhe size of the maxillary sinus relative to the uninvolved side.vertically oriented pattern with a sharp demarcation of the
the patst premn andearedrmane
rs. Onuced toarse,
thickening of the lateral wall and floor of the maxillary sinus,

milita
OOOOEe38 Whitt et al. August 2011
reducing its volume compared with the uninvolved side. Thelesion also involved the hard palate (Fig. 30).
Surgical reduction of soft tissue in the involved area wasrequired to place orthodontic appliances. The retained secondprimary molar was extracted and the space was adjusted for theplacement of a dental implant to replace the missing permanentsecond premolar.
During the 10-year follow-up period, from ages 9 years to19 years, the lesion exhibited mild enlargement that wasproportional to the growth of the uninvolved hemimaxilla. Abiopsy was not performed. There was no clinically significantfacial asymmetry, no associated cutaneous findings, and thepatient’s medical history was noncontributory.
REVIEW OF THE LITERATUREThe general clinical features of the 40 previously re-
Fig. 14. Case 2. Periapical radiographs of the affected and uof the involved right maxilla appeared coarse and verticallyuninvolved left maxilla. Orthodontic closure of the spacingbecause treatment was discontinued when the patient entered
Fig. 15. Case 2. Oblique radiographic projection of the rightmaxilla at age 24 years. The affected bone exhibits verticalorientation of coarse, thickened trabeculae with a sharplydefined anterior margin.
ported cases of SOMD and the additional 5 cases de-
scribed here are summarized in Table I with comments ontreatment performed. The mean age at diagnosis was 9years with a range of 2 years to 28 years. A number ofreports disclosed that maxillary enlargement had beenrecognized earlier than the age at which the diagnosis wasestablished and was observed at birth in 4 instances.1,2,14
There was a male gender predilection with a male-to-female ratio of 1.7 to 1.0. Race was stated for only 70% ofthe reports and recorded as Caucasian1-4,8-10,13 for 63%(25 cases), including all of our cases, and as AfricanAmerican15,16 for 8% (3 cases).
There was no predominance for location in one hemi-maxilla over the other, with essentially equal distributionbetween the left (23 cases) and the right (22 cases). Facialasymmetry was reported in 42%1,2,4,6,8,9,11,13-16 and was
ed sides of the maxilla at age 24 years. The bony trabeculaeed compared with the normal trabecular bone pattern of then the teeth of the involved hemimaxilla was not completedry service.
Fig. 16. Case 3. The appearance of the patient’s maxilla atage 11 years (exposed in a mirror reflection). The righthemimaxilla exhibited an increase in buccolingual dimensionextending from the incisor area to the tuberosity, accompa-nied by delayed eruption of teeth, hypoplasia of the firstprimary molar, and palatal eruption of the permanent canine.
naffectorientbetwee
frequently described as appearing as a prominence of the

e is an
is redu
OOOOEVolume 112, Number 2 Whitt et al. e39
upper lip. Absence of facial asymmetry was reported in12%,10,12,15 including 2 of our cases and was not recordedfor the remainder of the cases. Ipsilateral cutaneous find-ings over the affected area were associated with 28%3,7-
9,12-16 and included hypertrichosis, hyperpigmentation,hypopigmentation, ectopic eyelashes, commissural cleft-ing, hairy nevus and Becker nevus. The absence of cuta-neous findings was reported in 33%, including all of ourcases. The remainder of the authors did not comment onthis feature. Both hyperlinear palms and commissural
Fig. 17. Case 3. Panoramic radiograph at age 11 years thaaccompanied by an ill-defined radiodensity with a coarse appmissing, the first primary molar exhibited root resorption,pyramidal area obliterating a portion of the anterior mandibl
Fig. 18. Case 3. Panoramic radiograph at age 19 years. The reas part of the orthodontic treatment plan. The coarse, granulara well-defined anterior margin and the right maxillary sinus
clefting were associated with 1 case.13 Two reports12,13
described a marked lucency distal to the canine that wassuspicious for a bony cleft radiographically.
The radiographic appearance of the margin of theaffected bone, when commented on, was described aspoorly defined. Adjectives used to describe the radio-graphic appearance of the altered pattern of the cancel-lous bone of the affected region included coarse, sclerotic,thickened, granular, irregular, mottled, and vertically ori-ented trabeculae. Vertically oriented trabeculae were de-scribed in 37%,3,4,12,15 including 3 of our cases, where this
bited delayed tooth eruption in the right posterior maxilla,e of the trabecular bone pattern. The first premolar tooth wasere was no increased spacing of teeth. The opaque, whiteartifact produced by a lead-lined thyroid shield.
g 3 first premolars in the unaffected quadrants were extractedrance of the trabecular bone in the affected quadrant exhibitsced in size in comparison with the left.
t exhiearancand th
maininappea
pattern was observed in both periapical and CT images for

prove
OOOOEe40 Whitt et al. August 2011
1 case. We observed a well-defined, distinct, anteriorradiographic margin of the bony lesion at the canine-premolar region in 3 of our cases, as others have ob-served.7 A radiographic reduction in the size of the max-illary sinus was reported in 49%,2-4,7,9,12 including all ofour cases. An absence of radiographic encroachment onthe maxillary sinus was specifically reported by 5%,7,11,15
and the remainder of the authors did not comment on thisissue.
Approximately one-half of the reported cases in-cluded a biopsy as part of the diagnostic workup. Theenlarged gingival mucosa exhibited nonspecificchanges, consisting of collagenous fibrous connective
Fig. 19. Case 3. Periapical radiographs at age 19 years exaffected area (left image) compared with the typical trabeorthodontic treatment, it was noted that the teeth moved moreunaffected areas.
Fig. 20. Case 3. The patient’s facial appearance at age 19 ye3 years after the completion of orthodontic treatment. The bucsecondary to surgical recontouring of the affected area to im
tissue (Fig. 21), with variable areas of myxoid
change,2,9 reminiscent of the appearance of perifollic-ular connective tissue as others have observed.2 Thehistopathology of the affected bone was also nonspe-cific and generally consisted of thickened, irregularlyshaped trabeculae of immature woven bone withnumerous resting and reversal lines. There was a lackof osteoblastic rimming and, in most instances, noevidence of ongoing osteoclastic resorption,2,7,9 withthe exception of focal areas of active resorption andosteoblastic rimming in a 2-year-old patient.7 Themarrow spaces were variably described as containingloose, paucicellular, fibrous tissue,9 containing onlya few fat cells.7 One report described the marrow as
coarse trabeculae with a vertical orientation involving thebone pattern of the unaffected side (right image). During
through the denser bone of the affected area compared with
ft) and the appearance of her maxilla at the same age (right),ual dimension of the affected hemimaxilla appears decreasedfacial contours.
hibitedcularslowly
ars (lecoling
hypervascular.7

n stain
OOOOEVolume 112, Number 2 Whitt et al. e41
Some combination of missing premolars in the af-fected area was a common finding reported in 91%(Table I), and involved the absence of both premolars
Fig. 21. Case 3. Photomicrographs of soft tissue from the invtissue exhibited fibrous and fibromyxoid hyperplasia with buof pale blue myxoid ground substance (hematoxylin and eosi
Fig. 22. Case 4. Study casts of the patient’s maxilla obtainederuption of both primary and permanent teeth, accompaniedextending from the tuberosity to the canine area.
Fig. 23. Case 4. Axial CT images of the patient’s maxilla at aof the alveolar process of the right posterior maxilla, a coarsthickening of the anterior and lateral walls of the maxillary sinpanel).
in 53% and of 1 premolar in 40%. When 1 premolar
was absent, the missing premolar was distributed es-sentially equally between the first premolar (6 cases)and the second premolar (8 cases). The identity of the
area, excised at age 15 years, to improve facial contour. Thef thick, eosinophilic collagen fibers commingled with zones, original magnification, left panel �200, right panel �400).
ages of 4, 15, and 18 years, respectively, exhibited delayedreased buccolingual dimension of the right posterior maxilla
ars exhibited a moderately increased buccolingual dimensionular pattern of the expanded area (left panel) and prominentreduced its size in comparison with the unaffected side (right
olvedndles o
at theby inc
ge 6 yee, granus that
missing premolar was unspecified in 3 cases. In only

OOOOEe42 Whitt et al. August 2011
9% were both premolars present, including 2 of ourcases; the status of the complement of premolars wasnot reported in 2 cases.
Delayed eruption of teeth in the involved segmentwas observed in 70%,2,3,6-12,14,15 including all of ourcases. The remainder did not comment. Increased spac-ing between teeth in the involved segment was a com-mon finding reported in 76%,1,3,6-8,10-12,15,16 including3 of our cases. No increased spacing was specifically
Fig. 24. Case 4. Photomicrograph of an incisional biopsy ofalveolar bone from the involved area obtained at the age of 4years that exhibited thickened trabeculae containing bothwoven (W) and mature lamellar bone (L) with numerousreversal lines. There was no evidence of appositional osteo-blastic activity or of active osteoclastic resorption. The mar-row spaces contained predominately fatty marrow (hematox-ylin and eosin stain, original magnification �200).
Fig. 25. Case 4. Photomicrograph of an incisional biopsy ofalveolar bone at the periosteal surface of the affected area(inferior portion of image), obtained at the age of 4 years, thatexhibited an irregular and ill-defined cortical zone that tran-sitioned abruptly to cellular fibrous connective tissue (hema-toxylin and eosin stain, original magnification �200).
reported in 12%,2 including 2 of our cases. The remain-
der did not comment on the issue. Root resorption ofprimary molars was reported in 42%,2,3,7,12,13 including2 of our cases and was specifically reported as not beingpresent in 21%,2,3,7 including 1 of our cases. The re-mainder of the reports made no comment on this find-ing. Dysplasia of primary molar crowns was reported aspresent in 51%,1-3,6-11,13-15 including 4 of our cases,and not present in 12%,2 including 1 of our cases. Theremainder of the reports did not comment on this fea-ture. A wide range of additional morphologic anoma-lies of the primary teeth in the affected area weredescribed by Packota et al.3 in a radiographic series of12 cases. An additional report examined the histopa-thology of the deciduous teeth from the affected areaand found that most of the dentin was histologicallynormal with the exception of localized areas of dys-plastic dentin.6
Long-term clinical follow-up, ranging from 2 to 21years was recorded for 10 cases,2,6-8 including all of ourcases. For cases with follow-up, progressive enlarge-ment that was proportionate to overall growth wasreported in 27%,2,4,8,9,12 including all of our cases andwas described as slight by those who commented on thedegree. In 30%,1,2,7,14,15 the authors specifically statedthat they observed no enlargement and the remaindermade no comment. During the follow-up period, thealtered trabecular bone pattern remained stable, as wewere able to observe in 2 of our cases and as othershave reported.2
DISCUSSIONThe cause of SOMD is unknown. The preponderance
of evidence suggests that it is a noninherited develop-mental disorder, as cases appear sporadically. Reportsdescribing jaw enlargement at birth1,2,14 imply that theprocess may begin as early as in utero. Consistentinvolvement of a unilateral maxillary segment2,4 andhypodontia involving premolar teeth3,4,14 suggest thatthe process involves a field defect involving the anlagenof the first branchial arch.14 Somatic mutation occur-ring in a specific progenitor cell influencing the devel-opment of the involved hemimaxilla3,6 may account forthe mesoectodermal changes4 in a manner similar tothat described for fibrous dysplasia.21,22 Why such aneffect would be limited to only 1 side of the maxilla isa mystery.
Long-term follow-up indicates that SOMD is a non-progressive condition that persists and although it mayexhibit progressive enlargement, the increase in size isproportionate to the overall growth of the individual;the affected segment does not grow out of proportion tounaffected areas.2,16 This behavior is in distinct con-trast with fibrous dysplasia in which the enlargement of
the affected bone exhibits disproportionate growth. The
his im
OOOOEVolume 112, Number 2 Whitt et al. e43
negative findings reported on bone scintigraphy7 and inone of our cases support the concept of a lesion withlow metabolic activity and low growth potential. Al-though SOMD exhibits definite male gender predomi-nance (1.7:1.0), there is insufficient evidence to drawconclusions regarding possible racial predilection.
The differential diagnosis has been extensively dis-cussed by others2,4,6,9,14,23 and is limited to entities that
Fig. 26. Case 4. Panoramic radiograph at age 17 years. Therin this image) and an ill-defined density of the right maxilpermanent molar required active intervention over 2 yearswithout intervention, although chronologically late. The permsurgical exposure and traction to bring it into occlusion. Bwithout assistance. The first premolar exhibited marked enamof the orthodontic treatment plan.
Fig. 27. Case 5. The patient’s facial appearance and maxillainvolved the right hemimaxilla, produced very mild facial asythe affected side. The right hemimaxilla exhibited a moderatto the canine region that is partly obscured by the cheek in t
may cause unilateral enlargement of 1 hemimaxilla,
including gingival fibromatosis, segmental hemifacialhyperplasia, regional odontodysplasia, craniofacial fi-brous dysplasia, and neurofibromatosis. Clinical, radio-graphic and when required, histopathologic findingshelp to narrow the differential diagnosis. We believethat, in most cases, the clinical and radiographic ap-pearance of SOMD is sufficiently distinctive to estab-lish the diagnosis on those grounds alone. Biopsy of the
delayed eruption of teeth on the affected side (second molar,reduced the size of the involved maxillary sinus. The firsteve eruption, whereas the second molar eventually eruptedcanine tooth on the affected side was impacted and requiredmolars were present and both erupted chronologically late
oplasia. Both maxillary first premolars were extracted as part
h (exposed in a mirror reflection) at age 9 years. The lesionry, and was accompanied by delayed eruption of the teeth onase in buccolingual dimension extending from the tuberosityage and is better appreciated in the following figure.
e wasla thatto achianent
oth preel hyp
ry arcmmet
e incre
involved bone is not essential for diagnosis. In unusual

OOOOEe44 Whitt et al. August 2011
presentations, bone biopsy may be helpful, particularlyto exclude other lesions, such as fibrous dysplasia. In
Fig. 28. Case 5. Images depicting the clinical and radiographicappearance of the affected hemimaxilla. Clinically, the buccal con-tour of the right maxilla (top image) was moderately enlargedcompared with the uninvolved left side. The panoramic radiographexhibited a missing second premolar tooth, accompanied by anill-defined radiodensity involving the right maxilla. The clinicalimage was exposed at the age of 9 years and the panoramic radio-graph was exposed at the age of 11 years.
Fig. 29. Case 5. A periapical radiograph of the area of the affectedhemimaxilla exhibited a diffuse density of the bone with a coarse,vertically oriented trabecular pattern, a missing second premolar,and irregular root resorption of the second primary molar. Therewas no increased spacing between the teeth of the involved hemi-maxilla.
questionable situations, soft tissue biopsy may also be
helpful in narrowing the differential diagnosis, for ex-ample, by eliminating neurofibromatosis from consid-eration.
In discussing the cause of the clinical enlargement,Danforth et al.2 observed that in some cases the max-illary enlargement could be caused by excessive gin-giva rather than excessive bone, an observation thatwas confirmed by Packota et al.,3 who concluded thatthere was no radiographic evidence of bone enlarge-ment in 6 of their 12 cases. In reports in which theauthors attempted to determine the source the maxillaryenlargement, they concluded that in 35%1,2,4,6,7,9,14,15 itwas caused by a combination of both bone and softtissue. The data required to assess the proportion ofcases in which the enlargement is caused by boneand/or soft tissue are incomplete, as the remainder ofthe reports contain only partial information. For ourcases, we were able to demonstrate both hard and softtissue enlargement in Case 5, hard tissue enlargementin Case 4, and soft tissue enlargement in Cases 1, 2, and3. We were unable to draw further conclusions becauseof the incomplete and fragmentary nature of the recordsavailable. Regardless of the source of the enlargement,the radiographic alterations appear to be present in allpatients.2 The vertical orientation of coarse trabecularbone in the affected region is a distinctive featurereported in close to 40% of cases. We fancifully likenedit to the appearance of falling water in a waterfall.
In contrast to other reports that described the in-volved bony trabeculae as exhibiting immature wovenbone,2,4,7,9 the histopathology of our Case 4, a biopsyfrom a 4-year-old, exhibited a combination of bothlamellar and woven trabecular bone (Figs. 24 and 25).Apparently, bone biopsies of other cases have exhibitedsome degree of mature lamellar bone formation, asothers have alluded to it by stating that mature lamellarbone was usually not present.2 The marrow spaces ofthe biopsy from our Case 4 exhibited unremarkablefatty marrow, in contrast to fibrous marrow2,7 or afibrous connective tissue stroma4,9 surrounding the tra-beculae of affected bone as reported by others.2,4,7,9
Histologically, we, and others,2 observed a lack of awell-defined bony cortex and an irregular transitionfrom pagetoid bony trabeculae to the cellular fibrousconnective tissue that composed the soft tissue portion ofthe enlargement (Fig. 25). This correlates well with oper-ative reports that described the lack of typical buccalcortical plate and described that the fibrous tissue ap-peared to grow into the bone and blend with it.4 Thisfinding that has also been correlated with the ill-definednature of the cortex observed on CT imaging.4
As we noted in our review of the literature section,the lesional bone was reported to have encroached upon
the maxillary sinus in close to half of the reported
thosis
OOOOEVolume 112, Number 2 Whitt et al. e45
cases. We suspect that maxillary sinus involvement hasbeen underreported, as this determination is highly de-pendent on the type and quality of the imaging studiesperformed. CT imaging of a limited number of cases4,11
and 2 of our cases exhibit extension of the affectedbone beyond the alveolar process to involve the lateralwall and floor of the maxillary sinus. The lesional bonemay extend superiorly to the zygoma and orbital floorto surround the infraorbital canal.4 Although othershave reported that the horizontal palatal shelf does notappear to be involved,2,4,11 our Case 5 does exhibitinvolvement of the horizontal palatal shelf. Interest-ingly, 3 of our cases exhibited a distinct, well-definedanterior radiographic margin on plain films. We suspectthat the ability to observe this feature may be dependenton the type and quality of the imaging studies per-formed.
Hypodontia involving the premolars is a variablefeature in SOMD. The approximately equal distributionbetween the first and second premolars when 1 premo-lar is missing is quite unusual because, in the generalpopulation, the second premolar is much more com-monly missing than the first premolar. Indeed, the find-ing of congenitally missing first premolars is so unusualthat this finding alone should prompt closer scrutiny ofthe patient. Excessive tooth spacing in the involvedsegment is a frequent, but variable, finding and is likelyrelated not only to enlargement of the alveolar process3
but also to more mundane causes, such as tooth andarch size discrepancies. Indeed, some patients exhibitedno increased spacing,2 and even crowding, as seen inone of our cases.
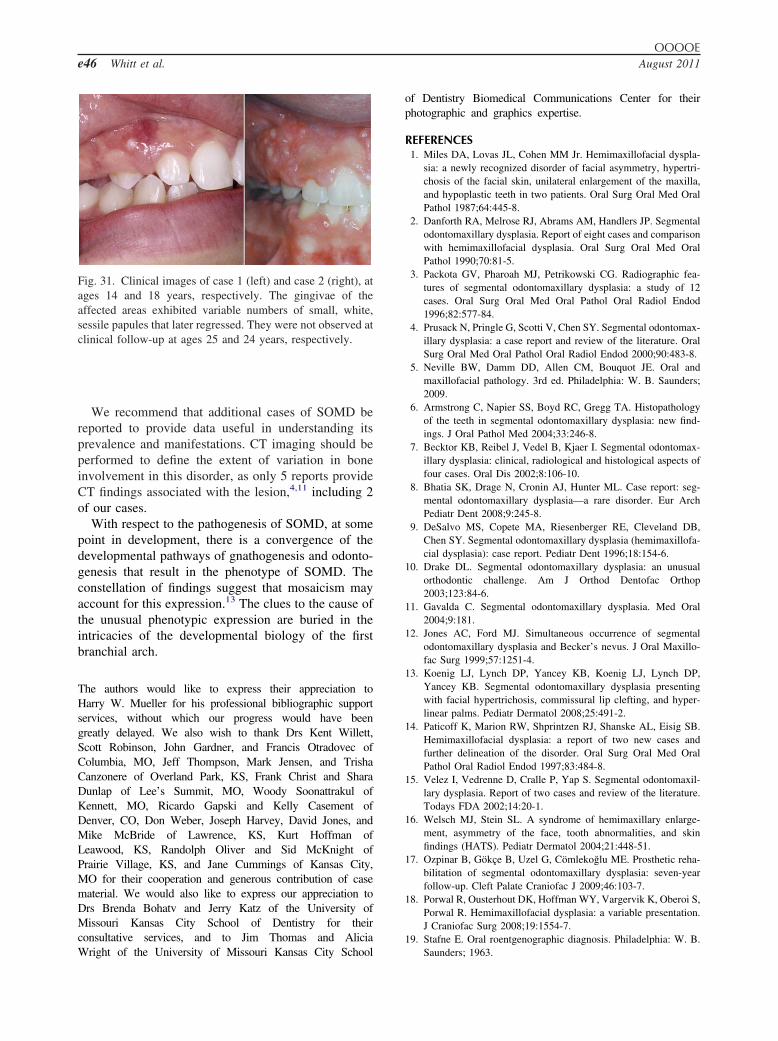
Two of our cases exhibited a variable number ofsmall, white, sessile papules, resembling dental lamina
Fig. 30. Case 5. Contiguous, 3.0-mm slices of a CT scan (bonto anterior (right image). The lesion involves the lateral wall anto the uninvolved side. The involved trabecular bone exhiincreased thickness of the palatal shelf (third panel). The mexhibited multiple polypoid lesions that represented sinus pa
cysts of the newborn, involving the facial gingival
mucosa at ages 14 and 18 years (Fig. 31) that regressedby ages 25 and 24 years, respectively. One patientreported that one of these lesions had been “incised”and that no tissue had been submitted for histopatho-logic examination.
The acronym HATS (Hemimaxillofacial enlarge-ment, Asymmetry of the face, Tooth abnormalities, andSkin findings) has been proposed for this condition.16
Although this is a handy mnemonic device that empha-sizes the occurrence of cutaneous findings (23%), itmay overemphasize both the degree of the asymmetrythat is clinically observed in affected individuals andpossibly the extent of bone involvement.
Patients with SOMD present a wide variety of man-agement considerations, including concerns for possi-ble progressive facial deformity and hereditary trans-mission, management of delayed eruption, enlargementof soft tissue, excessive spacing, missing teeth, andsupraeruption of opposing teeth.10 Reports of treatmentand outcomes for patients with SOMD are limited. Softtissue and/or bone removal to facilitate tooth eruptionhas been required,9,10 as well as in 2 of our cases. Inaddition to the successful osteointegration of dentalimplants in the affected bone of one of our cases (Figs.3 and 4), there is one additional report of successful ofdental implant placement in the affected bone.7 Surgi-cal recontouring of the enlarged area was performed inall of our cases for a variety of reasons, includingproviding access for placement of orthodontic appli-ances, to improve access for personal oral hygiene, andto address patients’ cosmetic concerns with respect tolip and cheek enlargement. In one of our cases, orth-odontic tooth movement through the affected bone was
ow) performed at age 13, oriented from posterior (left image)r of the right maxillary sinus, decreasing its volume in relationcoarse, vague vertical orientation (second panel). There islining of the uninvolved maxillary sinus was thickened andunrelated to SOMD.
e windd floo
bits aucosal
described being slower that in the unaffected quadrants.
OOOOEe46 Whitt et al. August 2011
We recommend that additional cases of SOMD bereported to provide data useful in understanding itsprevalence and manifestations. CT imaging should beperformed to define the extent of variation in boneinvolvement in this disorder, as only 5 reports provideCT findings associated with the lesion,4,11 including 2of our cases.
With respect to the pathogenesis of SOMD, at somepoint in development, there is a convergence of thedevelopmental pathways of gnathogenesis and odonto-genesis that result in the phenotype of SOMD. Theconstellation of findings suggest that mosaicism mayaccount for this expression.13 The clues to the cause ofthe unusual phenotypic expression are buried in theintricacies of the developmental biology of the firstbranchial arch.
The authors would like to express their appreciation toHarry W. Mueller for his professional bibliographic supportservices, without which our progress would have beengreatly delayed. We also wish to thank Drs Kent Willett,Scott Robinson, John Gardner, and Francis Otradovec ofColumbia, MO, Jeff Thompson, Mark Jensen, and TrishaCanzonere of Overland Park, KS, Frank Christ and SharaDunlap of Lee’s Summit, MO, Woody Soonattrakul ofKennett, MO, Ricardo Gapski and Kelly Casement ofDenver, CO, Don Weber, Joseph Harvey, David Jones, andMike McBride of Lawrence, KS, Kurt Hoffman ofLeawood, KS, Randolph Oliver and Sid McKnight ofPrairie Village, KS, and Jane Cummings of Kansas City,MO for their cooperation and generous contribution of casematerial. We would also like to express our appreciation toDrs Brenda Bohatv and Jerry Katz of the University ofMissouri Kansas City School of Dentistry for theirconsultative services, and to Jim Thomas and Alicia
Fig. 31. Clinical images of case 1 (left) and case 2 (right), atages 14 and 18 years, respectively. The gingivae of theaffected areas exhibited variable numbers of small, white,sessile papules that later regressed. They were not observed atclinical follow-up at ages 25 and 24 years, respectively.
Wright of the University of Missouri Kansas City School
of Dentistry Biomedical Communications Center for theirphotographic and graphics expertise.
REFERENCES1. Miles DA, Lovas JL, Cohen MM Jr. Hemimaxillofacial dyspla-
sia: a newly recognized disorder of facial asymmetry, hypertri-chosis of the facial skin, unilateral enlargement of the maxilla,and hypoplastic teeth in two patients. Oral Surg Oral Med OralPathol 1987;64:445-8.
2. Danforth RA, Melrose RJ, Abrams AM, Handlers JP. Segmentalodontomaxillary dysplasia. Report of eight cases and comparisonwith hemimaxillofacial dysplasia. Oral Surg Oral Med OralPathol 1990;70:81-5.
3. Packota GV, Pharoah MJ, Petrikowski CG. Radiographic fea-tures of segmental odontomaxillary dysplasia: a study of 12cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1996;82:577-84.
4. Prusack N, Pringle G, Scotti V, Chen SY. Segmental odontomax-illary dysplasia: a case report and review of the literature. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2000;90:483-8.
5. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral andmaxillofacial pathology. 3rd ed. Philadelphia: W. B. Saunders;2009.
6. Armstrong C, Napier SS, Boyd RC, Gregg TA. Histopathologyof the teeth in segmental odontomaxillary dysplasia: new find-ings. J Oral Pathol Med 2004;33:246-8.
7. Becktor KB, Reibel J, Vedel B, Kjaer I. Segmental odontomax-illary dysplasia: clinical, radiological and histological aspects offour cases. Oral Dis 2002;8:106-10.
8. Bhatia SK, Drage N, Cronin AJ, Hunter ML. Case report: seg-mental odontomaxillary dysplasia—a rare disorder. Eur ArchPediatr Dent 2008;9:245-8.
9. DeSalvo MS, Copete MA, Riesenberger RE, Cleveland DB,Chen SY. Segmental odontomaxillary dysplasia (hemimaxillofa-cial dysplasia): case report. Pediatr Dent 1996;18:154-6.
10. Drake DL. Segmental odontomaxillary dysplasia: an unusualorthodontic challenge. Am J Orthod Dentofac Orthop2003;123:84-6.
11. Gavalda C. Segmental odontomaxillary dysplasia. Med Oral2004;9:181.
12. Jones AC, Ford MJ. Simultaneous occurrence of segmentalodontomaxillary dysplasia and Becker’s nevus. J Oral Maxillo-fac Surg 1999;57:1251-4.
13. Koenig LJ, Lynch DP, Yancey KB, Koenig LJ, Lynch DP,Yancey KB. Segmental odontomaxillary dysplasia presentingwith facial hypertrichosis, commissural lip clefting, and hyper-linear palms. Pediatr Dermatol 2008;25:491-2.
14. Paticoff K, Marion RW, Shprintzen RJ, Shanske AL, Eisig SB.Hemimaxillofacial dysplasia: a report of two new cases andfurther delineation of the disorder. Oral Surg Oral Med OralPathol Oral Radiol Endod 1997;83:484-8.
15. Velez I, Vedrenne D, Cralle P, Yap S. Segmental odontomaxil-lary dysplasia. Report of two cases and review of the literature.Todays FDA 2002;14:20-1.
16. Welsch MJ, Stein SL. A syndrome of hemimaxillary enlarge-ment, asymmetry of the face, tooth abnormalities, and skinfindings (HATS). Pediatr Dermatol 2004;21:448-51.
17. Ozpinar B, Gökçe B, Uzel G, Cömlekoglu ME. Prosthetic reha-bilitation of segmental odontomaxillary dysplasia: seven-yearfollow-up. Cleft Palate Craniofac J 2009;46:103-7.
18. Porwal R, Ousterhout DK, Hoffman WY, Vargervik K, Oberoi S,Porwal R. Hemimaxillofacial dysplasia: a variable presentation.J Craniofac Surg 2008;19:1554-7.
19. Stafne E. Oral roentgenographic diagnosis. Philadelphia: W. B.
Saunders; 1963.
OOOOEVolume 112, Number 2 Whitt et al. e47
20. Zimmerman D, Dahlin D, Stafne E. Fibrous dysplasia of themaxilla and mandible. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1958;11:55-68.
21. Rosenberg A. Bones, joints and soft tissue tumors. In: Kumar V,Abbas AK, Fausto N, editors. Robbins and Cotran pathologicbasis of disease. 7th ed. Philadelphia: Elsevier Saunders; 2005. p.1300.
22. Weinstein LS, Shenker A, Gejman PV, Merino MJ, Friedman E,Spiegel AM, et al. Activating mutations of the stimulatory Gprotein in the McCune–Albright syndrome. N Engl J Med
1991;325:1688-95.23. Gorlin R, Pindborg J, Cohen M Jr. Syndromes of the head andneck. 2nd ed. New York: McGraw-Hill; 1976.
Reprint requests:Joseph C. Whitt, DDS, MSUniversity of Missouri Kansas CitySchool of Dentistry650 E. 25th StreetKansas City, MO 64108
[email protected]Copyright © 2022 FDOKUMEN




















