SAPERCONAZOLE IN THE TREATMENT OF SYSTEMIC AND SUBCUTANEOUS MYCOSES
6
PHARMACOLOGY AND THERAPEUTICS SAPERCONAZOLE IN THE TREATMENT OE SYSTEMIC AND SUBCUTANEOUS MYCOSES LILIANA FRANCO, M.D,, IVAN GOMEZ, M.D., AND ANGELA RESTREPO, PH.D. Abstract In a 2-year period, 30 patients with culture-proven mycoses (chromoblastomycosis, sporotrichosis, and paracoccid- ioidomycosis) were treated with the new orally administered triazole, saperconazole (spz) (R66905), The daily dose varied from 100 to 200 mg. All patients responded to treatment; the mean time required to heal the lesions and convert the cul- tures to negative was 3,5 months for sporotrichosis, 4,6 for paracoccidioidomycosis, and 9,0 for chromoblastomycosis. Evaluation by a scoring system indicated that 36,6% of the patients achieved complete resolution of the pretherapy ab- normalities, while the remaining (63,3%) experienced major improvement. No colateral effects were reported; there were no bone-marrow or liver toxicities, SPZ is an effective drug for the treatment of the above-mentioned mycoses and appears to be suitable for the control of chromoblastomycosis, Int J Dermatol 1992; 31:725-729 The imidazole derivatives have facilitated the treat- ment and improved the prognosis of patients with sub- cutaneous and systemic mycoses.''^ The newer triazoles such as fluconazole and itraconazole have a broader antifungal spectrum and are less toxic than the parent compound, ketoconazole.' Furthermore, they are more active and have a longer half-life.^'^ One of the newest triazoles, presently undergoing clinical trials, is saperconazole (R66905) (SPZ), a lipo- phylic compound that possesses a wide spectrum of ac- tivity and can be administered by the oral route.''•^ We have had the opportunity to use this triazole in the treatment of a series of patients with subcutaneous and deep-seated mycoses. The results of the clinical trials have been encouraging and are presented here. Materials and Methods In a period of 2 years (September, 1988, to September, 1990), 30 patients with subcutaneous or systemic mycoses entered the spz study group. Thirteen of these patients had sporotrichosis, eight had chromoblastomycoses, and nine had paracoccidioidomycosis. Twenty-six of the patients were men and four were women; there were seven chil- From the Corporacion para Investigaciones Biologicas (cm). Hospital Pablo Tobon Uribe, Medellin, Colombia. Address for correspondence: Angela Restrepo, Seccion de Mi- cologia, Corporacion para Investigaciones Biologicas (CIB), Apartado Aereo #73-78, Medellin, Colombia. dren, ages 10 to 14 years (mean 13 years). Mean age for the whole group was 41,0 years (range 10-70), The diagnosis was established in all cases by the isola- tion of the causative agent in culture. In the case of chro- moblastomycosis the only etiologic agent isolated was Fonsecaea pedrosoi. Where pertinent, direct microscopic ex- amination (KOH preparation) served as the initial parameter for inclusion in the study. Such an examination was positive in 96% of the patients under study. At time of the initial con- sultation in our service, signs and symptoms of the mycotic problem had been present for a mean period of 84,1 months, with large variations according to the mycosis, as follows: sporotrichosis 6,5 months, chromoblastomycosis 220,5 months, and paracoccidioidomycosis 6,8 months. Six patients (5 with chromoblastomycosis and 1 with sporotri- chosis) were failures from previous antimycotic therapies. Upon the establishment of the etiologic diagnosis, in- formed consent was obtained from each patient (or guar- dian) after the experimental nature of the drug under study had been fully explained, Saperconazole (SPZ) was administered in doses of 100 to 200 mg/day depending on the mycosis and its severity; capsules were taken once a day with breakfast. The drug's toxicity was monitored monthly by means of clinical and lab- oratory examinations; the latter included hematology (hemo- globin, hematocrit, white blood cell count, platelet count, sedimentation rate) and liver function tests (total bilirubin, alkaline phosphatases, prothrombin time, serum aspartate aminotransferase, and serum alanine aminotransferase). Treatment was considered complete and the medication .withdrawn when all lesions had resolved clinically and cul- tures had converted to negative and had remained so for two consecutive monthly appointments. The outcome of therapy was evaluated according to a scoring system reported previously,^ in which each of the clinical abnormalities present before therapy, and any posi- tive mycologie finding, received an arbitrary score. The sum of the resultant scores constituted the denominator of a fraction. At the end of therapy the same signs were evalu- ated and their scores aggregated to form the numerator. The resultant equation was calculated and the results ex- pressed as follows: a negative numerator indicated a deteri- orating clinical condition; a numerator of 0, no change; a positive numerator, minor ot major improvement; and a numerator equal to 1,0, complete resolution of all prethera- py abnormalities. RESULTS SFZ Dose. The 13 sporotrichosis patients received 100 mg/day; seven of those with paracoccidioidomyco- sis were also treated with this dose; due to the severity 725
Transcript of SAPERCONAZOLE IN THE TREATMENT OF SYSTEMIC AND SUBCUTANEOUS MYCOSES

PHARMACOLOGY AND THERAPEUTICS
SAPERCONAZOLE IN THE TREATMENT OE SYSTEMICAND SUBCUTANEOUS MYCOSES
LILIANA FRANCO, M.D,, IVAN GOMEZ, M.D., AND ANGELA RESTREPO, PH.D.
Abstract
In a 2-year period, 30 patients with culture-proven mycoses(chromoblastomycosis, sporotrichosis, and paracoccid-ioidomycosis) were treated with the new orally administeredtriazole, saperconazole (spz) (R66905), The daily dose variedfrom 100 to 200 mg. All patients responded to treatment; themean time required to heal the lesions and convert the cul-tures to negative was 3,5 months for sporotrichosis, 4,6 forparacoccidioidomycosis, and 9,0 for chromoblastomycosis.Evaluation by a scoring system indicated that 36,6% of thepatients achieved complete resolution of the pretherapy ab-normalities, while the remaining (63,3%) experienced majorimprovement. No colateral effects were reported; there wereno bone-marrow or liver toxicities, SPZ is an effective drug forthe treatment of the above-mentioned mycoses and appearsto be suitable for the control of chromoblastomycosis,
Int J Dermatol 1992; 31:725-729
The imidazole derivatives have facilitated the treat-ment and improved the prognosis of patients with sub-cutaneous and systemic mycoses.''^ The newer triazolessuch as fluconazole and itraconazole have a broaderantifungal spectrum and are less toxic than the parentcompound, ketoconazole.' Furthermore, they are moreactive and have a longer half-life. '̂̂
One of the newest triazoles, presently undergoingclinical trials, is saperconazole (R66905) (SPZ), a lipo-phylic compound that possesses a wide spectrum of ac-tivity and can be administered by the oral route.''•^ Wehave had the opportunity to use this triazole in thetreatment of a series of patients with subcutaneous anddeep-seated mycoses. The results of the clinical trialshave been encouraging and are presented here.
Materials and MethodsIn a period of 2 years (September, 1988, to September,1990), 30 patients with subcutaneous or systemic mycosesentered the spz study group. Thirteen of these patients hadsporotrichosis, eight had chromoblastomycoses, and ninehad paracoccidioidomycosis. Twenty-six of the patientswere men and four were women; there were seven chil-
From the Corporacion para Investigaciones Biologicas (cm).Hospital Pablo Tobon Uribe, Medellin, Colombia.
Address for correspondence: Angela Restrepo, Seccion de Mi-cologia, Corporacion para Investigaciones Biologicas (CIB),Apartado Aereo #73-78, Medellin, Colombia.
dren, ages 10 to 14 years (mean 13 years). Mean age for thewhole group was 41,0 years (range 10-70),
The diagnosis was established in all cases by the isola-tion of the causative agent in culture. In the case of chro-moblastomycosis the only etiologic agent isolated wasFonsecaea pedrosoi. Where pertinent, direct microscopic ex-amination (KOH preparation) served as the initial parameterfor inclusion in the study. Such an examination was positivein 96% of the patients under study. At time of the initial con-sultation in our service, signs and symptoms of the mycoticproblem had been present for a mean period of 84,1months, with large variations according to the mycosis, asfollows: sporotrichosis 6,5 months, chromoblastomycosis220,5 months, and paracoccidioidomycosis 6,8 months. Sixpatients (5 with chromoblastomycosis and 1 with sporotri-chosis) were failures from previous antimycotic therapies.
Upon the establishment of the etiologic diagnosis, in-formed consent was obtained from each patient (or guar-dian) after the experimental nature of the drug under studyhad been fully explained,
Saperconazole (SPZ) was administered in doses of 100 to200 mg/day depending on the mycosis and its severity;capsules were taken once a day with breakfast. The drug'stoxicity was monitored monthly by means of clinical and lab-oratory examinations; the latter included hematology (hemo-globin, hematocrit, white blood cell count, platelet count,sedimentation rate) and liver function tests (total bilirubin,alkaline phosphatases, prothrombin time, serum aspartateaminotransferase, and serum alanine aminotransferase).
Treatment was considered complete and the medication.withdrawn when all lesions had resolved clinically and cul-tures had converted to negative and had remained so fortwo consecutive monthly appointments.
The outcome of therapy was evaluated according to ascoring system reported previously,^ in which each of theclinical abnormalities present before therapy, and any posi-tive mycologie finding, received an arbitrary score. Thesum of the resultant scores constituted the denominator ofa fraction. At the end of therapy the same signs were evalu-ated and their scores aggregated to form the numerator.The resultant equation was calculated and the results ex-pressed as follows: a negative numerator indicated a deteri-orating clinical condition; a numerator of 0, no change; apositive numerator, minor ot major improvement; and anumerator equal to 1,0, complete resolution of all prethera-py abnormalities.
RESULTS
SFZ Dose. The 13 sporotrichosis patients received100 mg/day; seven of those with paracoccidioidomyco-sis were also treated with this dose; due to the severity
725

International Journal of DermatologyVol, 31, No, 10, October 1992
of the disease process the remaining two with the juve-nile form of the latter mycosis, received 200 mg/day.This higher dose was also employed in the eight patientswith chromoblastomycosis.
Duration of Therapy. The mean duration of thera-py varied according to the patient's response and typeof mycosis. In the sporotrichosis group, mean durationwas 3.5 months (range 2-6 months). For paracoccid-ioidomycosis, 4.6 months (range 3-6 months) were re-quired, and for patients with chromoblastomycosis 9months of therapy were needed (range 5-12 months).
Clinical Response
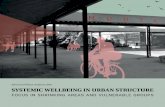
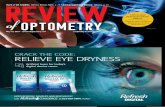
Sporotrichosis. At the time of the initial consultation,60 percent or more of the patients exhibited ulcera-tion, suppuration, nodular lesions, and tissue infiltration(Fig. 1). The former three alterations decreased sub-stantially during the first 2 months of SPZ therapy. Theinfiltration took longer to disappear, but resolved com-plete after 5 to 6 months of therapy. The pre and post-therapy aspects of two patients with sporotrichosis areillustrated in Figures 2-5.
Paracoccidioidomycosis. In these patients, im-provement was promptly noticed (Table 1). Constitu-tional symptoms (anorexia, fever, asthenia, adynamia)disappeared during the first month of therapy. Skinand mucosal lesions healed in 1 to 2 months (Figs.6-9). The various pulmonary alterations began to im-prove after 1 montb and after 3 to 6 months of SPZmost of them had disappeared.
Chromoblastomycosis. As shown in Table 2, the ul-cerative and exudative lesions, as well as the desquama-tion observed pretherapy, disappeared 3 to 6 monthsafter the initiation of SPZ treatment. Nodular (or verru-cous) formations required a longer time to resolve (6-9
% PATIENTS WITH LESIONS
100
90 '
80 "
70 "
60 '
50 1
40 "
30 "
20 1
10 "
0
— - = ^ ^
\ \ \\ \
\ Vk
\ ^1 1
Pre - treatment 1-2(n = 13) (n = 13)
- • — NODULES
# INFILTRATION
—*— SUPPUHATION
—•— ULCERATION
\
3-4 5-6
(n = 12) (n = 13)
Figure 2. Patient 1. Lymphangitic sporotrichosis of 2months duration before therapy. Note large lesion at site ofinoculation and involvement of draining lymph nodes.
PERIOD OF OBSERVATION (MONTHS)
Figure 1. Clinical response in patients with sporotrichosis
treated with saperconazole.
Figure 3. Patient 1. Healing with residual scarring after 3months of saperconazole therapy (100 mg/day)(cf. Fig. 2).
months). As shown in Figures 10 and 11 the appearanceof the lesions improved substantially during treatment.
Cultures
The mycologie evaluation by means of cultures re-vealed that all patients with paracoccidioidomycosis,as well as 92% of those with sporotrichosis, becamenegative after 1 to 2 months of therapy. At the sametime 87% of the cultures from chromoblastomycosispatients were still positive. F. pedrosoi required 5 to 6months of SPZ treatment to be eradicated.
Toxicity
No collateral effects were reported by the patients.Furthermore, there were no changes in the hematologictests. As shown in Table 3 the hepatic function studiesexhibited no significant variations during the course ofSPZ therapy.
The levels of alkaline phosphatases in the sevenchildren in the study should be considered separately
726

Treatment of MycosesFranco, Gomez, and Restrepo
as tbey are normally higher (82-250 U) than in theadult population. In the six sporotrichosis cases, valuesvaried from 269 units pretherapy to 274 units after 3months of SPZ. The only child with paracoccidioidomy-cosis had hepatosplenomegaly and exhibited bigbly ab-normal values (1695 U); however, the figures droppedduring therapy to 1177 and 776 after 3 and 6 monthsof SPZ, respectively.
Post-^therapy Evaluation
At the time of this report we have followed 27 of the 30SPZ-treated patients, among these are 12 with sporotri-chosis who have been observed for a mean period of12.6 months (range 3-24), nine with paracoccidioidomy-cosis followed for 14 months (range 6-36), and six withchromoblastomycosis with 20 months of follow-up(range 7-33 months). There bave been no relapses.
Scoring system
As sbown in Table 4, none of the patients undergoingSPZ therapy became worse, remained unaltered, or ex-
Table 1. Clinical Response in Paracoccidioidomyosis
Patients Treated with Saperconazole
Figure 4. Patient 2. Spoioinchosis, laige infiltrated crusty
lesions of the knee of 3.5 years duration. Before therapy.
Abnormality
Constitutionalsymptoms
Weight loss
Cough
Expectoration
Dyspnea
Hypoventilation
Auscultatoryalterations
Dysphonia
Mucosae and/orskin lesions
Lymph nodehypertrophy
No.
Before
Therapy(n=9)
8
4
8
8
5
5
5
4
5
7
of Patients with Lesions
During Therapy
1(n=9)
0
0
4
3
4
5
1
1
2
2
3(n=9)
0
0
1
1
2
2
0
0
0
0
(months)
6(n=3)
0
0
0
0
1
1
0
0
0
0
Table 2. Clinical Response in ChromoblastomycosisPatients Treated with Saperconazole
Alterations
Ulcerative lesions
Exudative lesions
Desquamationand/or scaleformation
Nodular and/orverroucousformation
No
BeforeTherapy(n=S)
4
5
8
8
, of Patients
During '
1 3(n=8) (n=8)
1 0
4 1
8 4
8 5
with Lesions
Therapy (months)
6(,1=8)
0
0
0
4
9(n=S)
0
0
0
2
12(,t=S)
0
0
0
0
Table 3. Hepatic Function Tests in Patients with
Mycotic Disorders Treated with Saperconazole
Mean Values During Indicated
Before Period of Therapy (fnonths)
Therapy 1 3 6 9 12
Alterations (n=30) (,i=30)(n=30)(n=30)(,i=24) (,i=2)
Total bilirubin 2,3 1.0 0,7 0,6 0.6 0,9(up to 1,0 mg)
Serum asparate 32.0 29.0 20.0 18.0 17.6 20,0aminotransferase(10-30U)
Serum alanine 26 17.3 15.3 12.0 11.0 10.0aminotransferase(6-37 U)
Alkaline
Figure 5. Patient 2, after 5 months of saperconazole (100
mg/day). Healed skin with hyperpigmentation (cf. Fig. 4).
120phosphatases(adult 36-92 U)-'
Prothrombin time 0,89(0,8-1.2)
107 100 84 102 71.5
0,88 0,91 0,91 0,91 0,94
* 11=23, the 7 children were not included in this tabulation.
727

International Journal of DermatologyVol, 31, No, 10, October 1992
Table 4. Point System Evaluation of the Results of Saperconazole Therapy in Various Mycoses
Categories
Negative numberator
Zero numerator
Positive numerator<0,49>0.50
Numerator equalsdenominator
Interpretation
Deterioration
No change
Minor improvementMajor improvementComplete resolution
Sporotrichosis(n=13)
0
0
023,077,0
No, of Patients per Category
Chromoblastomycosis(n=8)
0
Q
087.512.5
(5)
Paracoccidioidomycosis(,i=9)
0
0
0100.00
0
Figure 6. Patient 3. Skin and mucosal lesions in paraco-coccidioidomycosis. Note ulceration, infiltration, and crustformation.
Figure 7. Patient 3, after 1 month of 100 mg/day sapercona-zole. Although exulceration of the lower eye-lid is still present,the previously observed pathology has disappeared (cf. Fig. 6).
perienced only minor improvement during therapy.Depending on the mycoses, 23 to 100% of the casesimproved markedly, and 12.5 to 7 7 % achieved com-plete resolution of the pretherapy abnormalities.
DISCUSSION
The discovery of the orally absorbable azole deriva-tives radically changed the approach to the treatmentof systemic and subcutaneous mycoses.'-^-^ Tbe mod-ern trend is towards the development of new com-pounds with increased potency, wider spectrum ofactivity, and diminished toxicity.' In this context, SPZrepresents an advance in the control of severe andchronic mycoses.
The results of the present study indicate that thistriazole can be used successfully for the treatment ofsporotrichosis, paracoccidioidomycosis, and with pro-longed courses of therapy, also for chromoblastomyco-sis. As shown by the scoring system, all patientstreated with SPZ improved markedly or achieved com-plete resolution of their abnormalities.
In sporotrichosis and paracoccidioidomycosis, SPZ isas effective as itraconazole,*^ as it produces remarkable
improvement in about the same time and with a similardose. In this respect SPZ becomes an alternative to itra-conazole therapy. Cultures became negative soonerwith the newer azole; in 92% of the cases Sporothrixschenckii was no longer recovered after 1 to 2 monthsof SPZ therapy. A similar period of itraconazole thera-py, left 31% of the patients with positive cultures.' Inparacoccidioidomycosis, the effect of SPZ is even moresuperior as no culture remained positive after 1 monthof treatment with 100 mg/day of the drug; Itracona-zole, on the other hand, required 3 months to eradicatethe fungus.''
We consider that the greatest advantage of SPZ lies inits potency against F. pedrosoi; chromoblastomycosiscaused by this fungus is an extremely difficult disease tocure,** and among the azoles only itraconazole used forprolonged periods (12-24 months), produces 20% ofcures.** The eight chromoblastomycosis patients in thepresent series, including five who were failures of previ-ous chemotherapy, were cured and required an averageof 9 months to heal, in contrast with the 12 to 24month period indicated for itraconazole." Cultures be-came negative in all patients treated with SPZ after 5 to6 months of uninterrupted, 200 mg/day treatment. Onthe other hand, prolonged (up to 24 months) itracona-
728

Treatment of MycosesFranco, Gomez, and Restrepo
Figure 8. Patient 4. Paracoccidioidomycosis, before thera-py. Ulcerative lesion with raised borders. Note hemorrhagicspots and exudation.
Figure 9. Patient 4, after 1 month of 100 mg/day saper-conazole. Lesion has healed, there is hypochromic scarringwith no infiltration or ulceration {cf. Fig. 8).
zole therapy failed to eradicate F. pedrosoi from the le-sions.** At the end of therapy, 20% of the patients hadno residual lesions. In the remaining cases, scarring,pigmentation defects, and in the case of paracoccid-ioidomycosis, ventilatory alterations, remained as se-quelae of the mycotic processes. This is no different tothe experience with other therapies.''-^
Saperconazole therapy was well tolerated andproved safe. The hematopoietic system and the livershowed no signs of toxicity, even after prolonged (12months) therapy for chromoblastomycosis.
Although no relapses have been observed in the pa-tients from this series, prolonged post-therapy observa-tions are required to define the real value of this newmedication.
Acknowledgments: The saperconazole was donated byJanssen Pharmaceutica, Beerse, Belgium, The cooperation ofDr. Jose A, Daunas, Medical Director of Janssen Pharmaceu-tica Colombia, is appreciated.
Figure 10. Patient 5. Chromoblastomycosis of 25 yearsduration before therapy. Note infiltration, raised borders,and crusts.
Figure 11. Patient 5, after 5 months of sapcrconazole 200mg/day. Lesions are now healed; hypochromic scarring re-mains (cf. Fig. 10).
REFERENCES
1, Jacobs PH, Nail L, Discovering antimycotic drugs:today and tomorrow, Cutis 1990; 45:245-249,
"2. Graybill JR, Azole therapy of systemic fungal infec-tions. In: Holmberg K, Meyer R, eds. Diagnosis andtherapy of systemic fungal infections. New York: RavenPress, Ltd, 1989:133,
3. Bailey EM, Krakovsky DJ, Ryback MJ, The triazole an-tifungal agents: A review of itraconazole and flucona-zole, Pharmacotherapy 1990; 10:146-153,
4. Van Cutsem J, Van Gerven F, Janssen PAJ. Sapercona-zole, a new potent antifungal triazole: In vitro activityspectrum and therapeutic efficacy. Drugs of the Future1989; 14:1187-1209.
5, Odds FC, Antifungal activity of saperconazole (R66905)in vitro, J Antimicrob Chemother 1989; 24:533-537.
6, Restrepo A, Robledo J, Gomez I, et al, Itraconazoletherapy in lymphangitic and cutaneous sporotrichosis.Arch Dermatol 1986; 122:413-417.
7. Naranjo MS, Trujillo M, Munera Ml, et al. Treatmentof paracoccidioidomycosis with itraconazole. J MedVet Mycol 1990; 28:67-76,
8, Restrepo A, Gonzalez A, Gomez I, et al. Treatment ofchronioblastomycosis with itraconazole. AntifungalDrugs 1988; 54:504-516.
729