's ^ 'lb - Adelaide Research & Scholarship
235
TITLE THE DEVELOPMENT, VALIDATION AND ANALYSIS OF NEW ENDOSURGICAL PROCEDURES IN UPPER GASTROINTESTINAL SURGERY. Thesis submitted for the degree of Doctor of Medicine in the University of Adelaide Justin Raymond Bessell, M.B.,B.S. (Adelaide) July 1995 The work described was performed within the Department of Surgery of the University of Adelaide by C 7 .-'s ^ 'lb
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of 's ^ 'lb - Adelaide Research & Scholarship

TITLE
THE DEVELOPMENT, VALIDATION AND ANALYSIS OF NEW
ENDOSURGICAL PROCEDURES IN UPPER GASTROINTESTINAL
SURGERY.
Thesis submitted for the degree of Doctor of Medicine in the University of Adelaide
Justin Raymond Bessell, M.B.,B.S. (Adelaide)
July 1995
The work described was performed within the Department of Surgery of the University
of Adelaide
by
C7.-'s ^ 'lb

TABLE OF CONTENTS
TITLE
TABLE OF CONTENTS ....
TABLE OF FIGURES
ACKNOWLEDGEMENTS
PREFACE.
SUMMARY
DECLARATION......
1. AIMS
2.INTRODUCTION
I
ii
v
vlll
x
x11
XV
I
J
2.1 Evolution of the capability to perform advanced laparoscopic abdominal surgery3
2.I.1lmpact on surgical research in South Australia2.l.2Historical perspective of operative and technical advances
2.2 Complications of laparoscopic surgery ..
2.2.1 Complications related to needle and trocar insertion .................. 10
2.2.2 Complications related to the presence of a tension pneumoperitoneum ....... l52.2.3 Complications related to insertion and manipulation of instrumentation .....17
3. GENERAL PROBLEMS OF LAPAROSCOPY 18
3. I Temperature regulation.3.1 .I Introduction
Effect of warmed gas..............
Aims3.1.2 Methods3.1.3 Results..3. 1.4 Discussion...........
3.2 Thromboembolism ....
3.2. 1 Introduction ........
4
9
........18
........18
........2r
........2r
........22
........25
........28
........ 33
........ 33
........3s
........36
........38
........38
........39
3 .2.2 Thromboembolic risk induced by hypercoagulability..............Introduction...Aim................MethodsResultsDiscussion. 42
3.2.3 Thromboembolic risk induced by impaired blood flow in splanchnic visceral
vessels 44
Introduction. 45
Locoregional effect of pneumoperitoneum on splanchnic visceral vasculature45
Effect of systemic haemodynamics on splanchnic visceral vasculature ........ 48
Measurement of splanchnic visceral microcirculatory blood flow................' 50
Aims .53.54Methods
1l
Anaesthesia................Cannulation................Preparation of microspheres .
Standard sample......
Dose of microspheres .......
Baseline measurement of organ blood flows.............InsufflationPost-insufflation measurement of organ blood flowsSacrifice and organ harvest......Ethical implications ................
..........54
..........54
..........55
..........56
..........56
..56
..57
..57
.. 58
.. 58
Statistical analysis 59
Results. 60
Discussion... 63
3.2.4 Thromboembolic risk induced by impaired blood flow in lower limb vessels6T
3.2.5 Thromboembolic risk induced by vessel wall abnormalities ......723.2.6 Summary of net thromboembolic risk during laparoscopy...........................723.2.7 Tfuomoembolism prophylaxis for laparoscopy........ ...................73
4. DEVELOPMENT AND EVALUATION OF NEV/ APPLICATIONS IN
LAPAROSCOPIC GASTROINTESTINAL SURGERY 76
4.1 Oesophagectomy4.1.1 Introduction
Perivisceral oesophagectomyThoracoscopic oesophagectomy ..
Aim..........4.1.2 Methods ............
Anaesthesia................Operative details
Thoracoscopic oesophageal dissection...........Laparoscopic gastric mobilisation..................Thoracoscopic oesophagogastric anastomosis
4. 1.3 Results .............4. 1.4 Discussion.........
4.2 Highly selective vagotomy4.2.1 Introduction
History of open vagotomyDevelopment of minimal-access vagotomy .......
Aims4.1.2 Methods ............
Cervical tube oesophagostomyGastric acid output studies......Gastric emptying studiesAssessment of gastro-oesophageal reflux...Operative proceduresStatistical analysis
4.1.3 Results .............Clinical outcome....
767676809l9t929293
9495
101
102107
107
107
110
tt4rt4ll5118
119
122
122
124125125

Gastric acid outputGastric emptyingAssessment of oesophageal reflux
4.1.4 Discussion..4.3 Gastrostomy
5.1 Historical development of hernionhaphy5.1.1 Traditional methods of inguinal hernia repair
BassiniHalsted.....McVay (Coopers ligament repair)...ShouldiceLichtenstein ...............Preperitoneal repairs with and without mesh
5.I.2Laparoscopic methods of inguinal hernia repairLaparoscopic ligation of the neck of the sac ............
Laparoscopic plug (+ small mesh) repairLaparoscopic transabdominal intraperitoneal (onlay) patch..
Laparoscopic transabdominal preperitoneal patch
Laparoscopic extraperitoneal patch
Specific complications of laparoscopic hernia repair............5.2 Transabdominal preperitoneal herniorrhaphy..........
5.2. I Introduction .........
5.2.2 Methods ...........
5.2.3 Results .............5.2.4 Discussion.........
5.3 Extraperitoneal herniorrhaphy .. ................5.3. 1 Introduction ....
5.3.2 Methods ..........
5.3.3 Results5.3.4 Discussion.........
6. SUMMARY AND CONCLUSIONS..
6.1 General problems of laparoscopy.6. 1. 1 Temperature regulation.6.1.2 Thromboembolism
6.2.3 Gastrostomy...6.3 Assessment of routine laparoscopic procedures
...125
... 126
...r29
... 130
...1344.3.1 Introduction
Aim..........4.3.2 Methods ...........4.3.3 Results ............4.3.4 Discussion.......
5. ASSESSMENT OF ROUTINE LAPAROSCOPIC PROCEDURES ....143
t36t36140
140
t34
190
189
r43t43t43r43r44r4s146t47148
t49151
152155
159
161
t63r63r63t64170t74174174174r82188
189
6.2 Development and evaluation of new applications in laparoscopic gastrointestinal
surgery ..........I926.2.1 Oesophagectomy 192
6.2.2 Highly selective vagotomy 193194
1V
195

7. BIBLIOGRAPHY r97
V
TABLE OF FIGURES
TABLE I: INSUFFLATING GAS TEMPERATURE AT A FLOW RATE OF IO L/\4IN
(MANUFACTURERS TNFORMATTON) 23
FIGURE I: INTRAPERITONEAL TEMPERATURE 27
FIGURE 2: OESOPHAGEAL TEMPERATURE 28
TABLE 2: LEVELS OF COAGULATION INDICES IN VENOUS BLOOD IN PATIENTS
UNDERGOING OPEN ORLAPAROSCOPIC ABDOMINAL SURGERY. 40
FIGURE 3: LEVELS OF FIBRINOGEN IN G/L FOR OPEN AND LAPAROSCOPIC PROCEDURES.42
TABLE 3: MEAN MICROVASCULAR BLOOD FLOV/ RATES (MLS/MIN/100G TISSUE) FOR
VITAL INTRA-ABDOMINAL ORGANS BEFORE AND AFTER LAPAROSCOPIC
INSUFFLATION 63
FIGURE 4: (FROM LEFT TO RIGHT) 33MM CANNULA AND TROCAR, SPECIMEN
EXTRACTTON ADAPTOR, AND PORT EXCHANGE ROD (ENDOPATH-ETHTCON) 97
FIGURE 5: ENDOSURGICAL CIRCULAR STAPLER (STEALTH-ETHICON) WITH SPECIALLY
ADAPTED CONICAL ANVIL. 98
FIGURE 6: TEFLON STAPLERANVIL MODIFIED TO FACILITATE ENTRY INTO OPEN
PROXIMAL OESOPHAGEAL REMNANT. 99
FIGURE 7: STAPLERANVIL FIXED IN PROXIMAL OESOPHAGUS BY AN ENDOLOOP.
GASTRIC ANASTOMOTIC MARGIN IS INDICATED BY THE BROAD ARROW. THIN
ARROIù/ POINTS TO THE ENDOLOOP INTRODUCED THROUGH A CANNULA. lOO
FIGURE 8: PLASTIC T-TUBE OESOPHAGOSTOMY 117
TABLE 4: DIFFERENCE BETWEEN THE PRE AND POSTOPERATIVE GASTRIC ACID OUTPUT
VALUES 126
FIGURE 9: BASAL ACID OUPUT 126
FIGURE IO: PREOPERATIVE LIQUID GASTzuC EMPTYING 128
FIGURE I I: POSTOPERATIVE LIQUID GASTzuC EMPTYING 128
TABLE 5:DIFFERENCE BETWEEN PRE AND POSTOPERATIVE GASTRIC EMPTYING VALUES127
FIGURE 12: PRE AND POSTOPERATIVE REFLUX SCORES 129
TABLE6: DIFFERENCEBETWEENPREANDPOSTOPERATIVEREFLUX SCORES 129
FIGURE 13: THE ANTERIOR WALL OF THE BODY OF THE STOMACH GRASPED BY
BABCOCK FORCEPS, WITH TRANSABDOMINAL SUTURES PLACED BY AN
ENDOSCOPIC NEEDLE HOLDER. I38
FIGURE 14: FOLEY CATHETER MOUNTED ON AN ÍNTRODUCER PASSED INTO THE
PERITONEAL CAVITY, AND DIRECTED INTO THE STOMACH UNDER LAPAROSCOPIC
VISUALISATION. 139
TABLE 7:COMPARISON OF THE TWO PATIENT GROUPS 166
FIGURE 15: MEDIAN ACTIVITY LEVELS MEASURED ON AN ANALOGUE SCALE OF 0 - 10.167
vl

FIGURE 16: MEDIAN PAIN LEVELS MEASURED ON AN ANALOGUE SCALE OF 0 - 10. 167
FIGURE 17: MEAN NUMBER OF TOTAL ANALGESIC TABLETS TAKEN POST-OPERATIVELY
PERPATIENT. 168
TABLES:MORBIDITY 169
TABLE 9: PATIENTS' OPINION OF DAY CASE SURGERY 170
FIGURE 18: BREAKDOWN OF PATIENT GROUPS AFTER RANDOMISATION 176
TABLE l0: COMPARISON OF THE TWO PATIENT GROUPS 178
FIGURE 19: MEDIAN ACTIVITY LEVELS MEASURED ON AN ANALOGUE SCALE OF 0 - 10.180
FIGURE 20: MEDIAN PAIN LEVELS MEASURED ON AN ANALOGUE SCALE OF 0 - 10. 180
FIGURE 21: MEAN NUMBER OF TOTAL ANALGESIC TABLETS TAKEN POST-OPERATIVELY
PERPATIENT. I8I
TABLE 1l: POST-OPERATIVE MORBIDITY 182
vl1

ACKNOWLEDGEMENTS
The work which is reported in this thesis was made possible by a Medical Postgraduate
Research Scholarship awarded by the National Health and Medical Research Council of
Australia. Instruments and some specific project grant support were supplied by the
AutoSuture and Ethicon surgical instrument companies.
The studies described involved the Departments of Surgery within The Queen Elizabeth
Hospital, The Royal Adelaide Hospital and the University of Adelaide, and The Royal
Adelaide Centre for Endoscopic Surgery. Several studies involving animals were
conducted on the premises of the Institute of Medical and Veterinary Science.
The foremost acknowledgements must be for the important contributions of the two
supervisors, Professor G. J. Maddern and Professor G. G. Jamieson. Their innovative
concepts and suggestions were tempered by a clarity of insight that can only be aspired
to. Despite heavy workloads, their preparedness to become involved beyond the
scientific scope of the work was greatly appreciated. They provided continued personal
encouragement, and offered assistance with burdensome administrative and financial
matters. The fertile research environment they have provided to their Departments is
testimony to their dedication, and contributed to the completion of this work in no small
measure. Tribute must also be made to many others, by whose contributions this work
is honoured:
. Within The Queen Elizabeth Hospital Department of Surgery; Mr. A Slavotinek, Mr.
P. Byrne, Ms. S. Millard, Ms. S. Ireland, Ms L. Martin, Ms.O. Kapaniris, Mr. K.
Porter, Mr. A. Hines and Mr. P. Leppard.
vilt
o V/ithin The Royal Adelaide Hospital Department of Surgery and The Royal Adelaide
Centre for Endoscopic Surgeryl Dr. G. Pike, Mr. D. 'Watson, Mr. P. Devitt, Mr. P. G
Gill, Mr. N. DeYoung, Ms. N. Ascott, Ms. P. Baxter and Ms. E. Cunningham.
o Within the Institute of Medical and Veterinary Science; Dr. T. Kuchel, Dr. D
Noonan, Ms. K. Kaiser, Ms. T. Little and Ms. G. Summersides
o V/ithin the AutoSuture company; Mr. R. FazzalaÅ and Mr. A. Nicolo.
o V/ithin the Ethicon company; Ms. J. Prior, Mr. J. Meek, Dr. S. Straface.
o Within the Cook company; Mr. G. Taddeo, Mr. A. Ward.
o V/ithin the Kendall company; Ms. J. Richards
lx
PREFACE
Part of the work described in this thesis has been published or accepted for publication.
These publications are listed below in the order they were submitted.
1. Maddern GJ, Rudkin G, Bessell JR, Devitt P, Ponte L. A Comparison of
Laparoscopic and Open Inguinal Hernia Repairs as a Day Surgical Procedure.
Surgical Endoscopy 1994; 8: 1404-08.
2. Bessell JR, Maddern GJ, Manncke K, Ludbrook G, Jamieson GG. Combined
Thoracoscopic and Laparoscopic Oesophagectomy and Oesophagogastric
Reconstruction. Endoscopic Surgery and Allied Technologies 1994;2: 32-36
3. Bessell JR, Stanley B, Maddern GJ. The Emerging Role for Laparoscopic
Gastrostomy: A Case Report. Australian and New Zealand Journal of Surgery 1994;
64: 515-517.
4. Facchin M, Bessell JR, Maddern GJ. A Simplified Technique for Laparoscopic
Instrument Ties. Australian and New Zealand Journal of Surgery 1994; 64: 569-571
5. Bessell JR, Karatassas A, Patterson JR, Jamieson GG, Maddern GJ. Hypotherrnla
Induced by Laparoscopic Insufflation: A Randomised Study in a Pig Model. Surgical
Endos copy. 1995 : 9 : 7 9l -7 96
6. Bessell JR, Patkin M,Isabel L. Durability and Function of Disposable Vs Reusable
Laparoscopic Instrumentation. Endoscopic Surgery and Allied Technologies 1995;3
r43-146.
7. Maddern GJ, Bessell JR. [Editorial] Disposable vs. Reusable Laparoscopic
Instrumentation. Endoscopic Surgery and Allied Technologies 1995;3: 125-126.
X
8. Maddern GJ, Bessell JR. Disposable Vs Reusable Laparoscopic Instrumentation
[Glossary]. Endoscopic Surgery and Allied Technologies. 1995;3: 151-152.
9. Bessell JR, Devitt PG, Goyal S, Jamieson GG. Prolonged survival follows resection
of oesophageal SCC downstaged by prior chemoradiotherapy. Australian and New
Zealand Journal of Surgery. In press.
lO.Bessell JR, Pike G, Jamieson GG, Maddern GJ. Physiological outcome following
laparoscopic highly selective vagotomy: A controlled study in a pig model. Surgical
Endoscopy. In press
11.Pike GK, Mathew G, Bessell JR, Watson DI, Mitchell PC, Jamieson GG. The
assessment of hypercoagulability in patients undergoing open and laparoscopic
Nissen fundoplication. Australian and New Zealand Journql of Surgery.In press
xl
SUMMARY
This thesis develops, analyses, and validates the role of therapeutic laparoscopy in
situations where it is likely to be encountered in the practice of upper alimentary tract
surgery. This is achieved by an analysis of some general problems of laparoscopy,
particularly in relation to induced physiological disturbances; by development and
evaluation of new applications in laparoscopic gastrointestinal surgeryl and by assessing
the efficacy of laparoscopic procedures which have already entered routine practice.
The thesis commences with investigation into the hitherto relatively unexplored area of
the physiological sequelae of laparoscopic surgery. The impact of laparoscopy on
perioperative heat balance is documented in an animal study that quantifies changes in
core temperature over a three-hour period of high-flow carbon dioxide insufflatron.
Insufflation is shown to result in a significant fall in core temperature, and it is revealed
that currently available devices that provide warmed rather than cold insufflated gas
confer no protection against perioperative heat loss. The thromboembolic risk posed by
laparoscopic surgery is investigated by studying two of the three elements of Virchow's
triad; hypercoagulability and impaired blood flow. In a controlled human study,
changes in the level of blood coagulation markers before and after open and
laparoscopic Nissen fundoplication indicated that minimally-invasive procedures may
not protect against the risk of postoperative hypercoagulability. The potential for
laparoscopic insufflation to impair blood flow to vital intraabdominal organs was
considered in the light of reports detailing cases of fatal mesenteric thrombosis.
Radiolabelled microspheres were used to determine blood flow distributions in pigs, but
using this model decreased blood flow at the tissue level in the setting of laparoscopic
abdominal surgery could not be established.
xlt

The place of laparoscopy in upper gastrointestinal surgery is expanded and clarified by
the development and evaluation of three procedures hitherto unfamiliar in the
laparoscopic environment. In an animal model, a new 3-step totally endoscopic
operation for the surgical treatment of oesophageal carcinoma was devised. Another
controlled animal study demonstrated the physiological validity of laparoscopic highly
selective vagotomy. The outcome of laparoscopic highly selective vagotomy in terms of
gastric acid output, liquid gastric emptying and ambulatory pH monitoring suggested
that the use of laparoscopic highly selective vagotomy in clinical practice is appropriate
This section of the thesis concludes with a clinical study, in which a technique for
laparoscopic gastrostomy is reported which offers an alternative form of enteral access
after failed percutaneous endoscopic gastrostomy
Although inguinal hernias are not anatomically located in the upper gastrointestinal
tract, their treatment comprises a routine component of upper gastrointestinal surgical
practice. To resolve the current indications for laparoscopic herniorrhaphy, two
randomised-controlled clinical trials were conducted in a day surgery setting. These
determined that laparoscopic transabdominal preperitoneal herniorrhaphy should be
confined to the repair of recurrent, bilateral or undiagnosed hernias only, rather than
emerge as the standard operation. Similarly, laparoscopic extraperitoneal hernionhaphy
should not enter clinical practice until subjected to further study under trial conditions
with the aid of larger study populations and greater technical expertise, whilst the
results of long-term recurrence rates are awaited.
xltl
To my wife, Sara, whose love and support contributes immeasurably to the success of
my work.
To my parents Ray and Raylee, and my brother Kim, whose company throughout the
years has been the foundation of my fulfilling life
xlv
DECLARATION
I declare that this thesis contains no material which has been accepted for the award of
any other degree or diploma in any other University and that to the best of my
knowledge and belief, the thesis contains no material previously published or written by
another person, except where due reference is made in the text of the thesis. I further
consent to the thesis being made available for photocopying and loan if applicable if
accepted for the award of the degree.
sofr lrs
Justin Bessell
XV

1. AIMS
There were three specific objectives that guided the course of this thesis. These were
(i) To determine if particular physiological changes induced by the laparoscopic
environment predispose to increased patient risk.
(ii) To develop and evaluate new applications of laparoscopic upper
gastrointestinal surgery.
(iii) To assess the efficacy of routine laparoscopic procedures which had entered
clinical practice without prior validation.
Therefore, answers to the following questions were sought:
(i) Is there an increased risk of deleterious core temperature changes during
laparoscopic insuffl ation?
(ii) Is there an increased risk of thrombo-embolism induced by hypercoagulability
during laparoscopic surgery?
(iii) Is there an increased risk of thrombo-embolism induced by impaired visceral blood
fl ow during laparoscopic insuffl ation?
(iv) Is it possible to devise an endosurgical operative technique with the potential to
improve the outcome of patients undergoing oesophagectomy for oesophageal
carcinoma?
(v) Can the physiological validity of laparoscopic highly selective vagotomy be
demonstrated?
I

(vi) Can laparoscopic gastrostomy be developed to provide a feasible and desirable
altemative for enteral access?
(vii) Is laparoscopic transabdominal preperitoneal hernionhaphy more efficacious than
the conventional open approach?
(viii) Is laparoscopic extraperitoneal herniorrhaphy more effrcacious than the conven-
tional open approach?
a-L-
2. INTRODUCTION
2.1 Evolution of the capability to perform advanced laparoscopicabdominal surgery
2.1.1 lmpact on surgical research in South Australia
Laparoscopic cholecystectomy was introduced into major South Australian teaching
hospitals in 1990. The enduring success of this operation for routine removal of the
diseased gallbladder demonstrated first-hand to local surgeons the feasibility of
operative abdominal laparoscopy. The South Australian perception of laparoscopic
surgery soon followed the course of other international surgical communities; what was
previously obstinate resistance became an almost blind enthusiasm to adopt untested
and unproven laparoscopic procedures. Cuschieri has called this global phenomenon
"the biggest unaudited free-for-all in the history of surgery"(Cuschieri, 1995). At the
time of conceptualization of this thesis in late 1992, academic surgeons within the
Royal Adelaide Hospital and The Queen Elizabelh Hospital came to realizeihat
leadership in the field of laparoscopic surgery would not be sustained indefinitely by
involvement in the race to become the hrst to undertake a new laparoscopic operation.
A more enduring contribution could be made by subjecting the advantages of these new
techniques to the same rigorous analysis that had established the place of all prevrous
innovations. This became the principle underlying the structure of this thesis, and there
was no shortage of new procedures waiting to be validated! However, technical and
operative development was not abandoned, as oesophageal surgery in particular had
suffered from a relative paucity of the application of laparoscopic technology
Furthermore, because of the rapidly changing nature of this field of surgery, this
research had to be sufficiently flexible to cope with continual extensive refinements in
technology and procedure, and also be able to provide insight into new problems that
-J-

only became obvious as more complex surgery was attempted. Therefore the underlying
aims were more suitably addressed by proposing multiple hypotheses, rather than one
all-encompassing proj ect.
-4-

2.1.2 Historical perspective of operative and technical advancesThe evolution of laparoscopic surgery is inextricably linked to technological advances
which allow surgery to be conducted in anatomical locations that cannot be reached
except by the use of large incisions. The hrst published attempt to examine an internal
body cavity was published by Bozzini in 1806, who constructed a crude apparatus to
visualize the urethra for stones and tumours(Bozzini, 1806). However, it was 60 years
later before the first serviceable endoscope was developed by Desormeaux in 1865 to
inspect the bladder, cervix and uterus. This apparatus included a kerosene lamp, a
chimney vent, and a mirror(Desonneaux, 1865). Further developments in optical
technology and the invention of the Edison incandescent light bulb in 1880 allowed a
more contemporary-style cystoscope to be produced in Germany by Nitze in 1897. This
operating endoscope also included a working channel for the passage of customised
instruments. The Nitze cystoscope was used by Kelling in 1902 to examine the
abdominal cavity of a live dog following the creation of a pneumoperitoneum with
filtered air(Kelling,1902). Kelling later reported on his experience in humans, but it
was Jacobaeus who was the first surgeon to report a series of laparoscopies and
thoracoscopies in man in 1910, performed without pneumoperitoneum(Jacobaeus,
1e10).
These early techniques used filtered air as the insufflated gas, usually pumped in by a
syringe, until the development of a pneumoperitoneal needle by Goetze in 1918(Goetze,
1918). ln 1926 Zollikofer proposed the use of carbon dioxide as the insufflating gas as a
more rapidly absorbed substitute for air, and this was followed by the introduction of a
new insufflation needle by Veress in 1938(Veress, 1938). This needle, which still bears
his name, comprised a spring-loaded obturator contained within the outer stylet of the
-5-
needle. The obturator retracted during fascial penetration, and then emerged to cover the
sharp needle point after entering the body cavity. It was originally designed as a safe
means to create a pneumothorax, which was at the time a treatment for pulmonary
tuberculosis.
Operative laparoscopy had its beginnings in the 1930's when Kalk advocated the dual-
puncture technique to accommodate his specially-designed instruments, and he also
introduced the oblique 135o lens system laparoscope to allow a change in the viewing
direction by merely rotating the scope along its longitudinal axis. During this decade,
Fervers performed the first laparoscopic adhesiolysis(Fervers, 1933), Ruddock
described the biopsy of abdominal organs using monopolar electrocautery(Ruddock,
1934), and Boesch performed the first laparoscopic tubal sterilization(Boesch, 1936)
Laparoscope technology was further revolutionizedin 1952 when Fourestier eliminated
the risks of intemal electrical or thermal injury due to incandescent lighting by
developing a cold light system whereby an intense light was transmitted along a quartz
rod from the proximal to distal ends of the scope(Fourestier et al., 1952). Twelve
months later, Hopkins invented the rod-lens system(Hopkins, 1953), in which small air
lenses were combined with long glass rods (previously small glass lenses were
combined with long air spaces). This optical system doubled the light transmitting
capacity of endoscopes, and provided a significantly larger clear aperture
Kurt Semm of Kiel University in Germany is the patriarch of operative laparoscopy in
the modem era. His most often cited achievement is the development of an automatic
insufflation device. However, from the 1960's onward he contributed enormously by
many other innovative advances such as the suction-irrigator, hook scissors, the
-6-
laparoscopic morcellator, the endoloop applicator, needle-holders and laparoscopic
suturing, clip appliers, atraumatic forceps, and the endotrainer. Semm's technological
advances led to more complicated therapeutic laparoscopic procedures, predominantly
in the field of gynaecology. Operative innovations attributed to his team include
laparoscopic management of ectopic pregnancy, salpingostomy, oophorectomy,
salpingolysis, fimbriolysis, adhesiolysis, tumour biopsy, staging and debulking, and the
first laparoscopic appendicectomy in 1983(Semm, 1983)
Pioneering developments in the field of endoscopic surgery were also being advanced
during the early 1980's by another German Surgeon, Gerhard Buess, working from the
Johannes-Gutenberg University in Mainz. He used a technologically-advanced
stereoscopic magnifying optical system, insufflation, and endoscopic instruments for
the endoluminal resection of rectal and sigmoid colon tumours in an operation called
Transanal Endoscopic Microsurgery (TEM) that closely mimiced the subsequent
performance of laparoscopic intraabdominal surgery(Buess et al., 1988; Buess et al.,
1989). Although an important innovation in its own right, the importance of this
technique in terms of laparoscopic surgery was the pre-emptive development of a wide
range of endoscopic technology that later provided surgeons with immediate operative
capabilities once video technology arrived.
Despite other early protagonists such as George Berci(Berci et al., 1973), Alfred
Cuschieri(Cuschieri et al., I978), Paul Sugarbaker(Sugarbaker and Wilson, 1976), and
Andrew V/arshaw(V/arshaw et al., 1986) who advocated a role for laparoscopy in the
1970's and early 1980's, it failed to gain a foothold in General Surgical practice at that
time
-7 -

Acceptance of laparoscopy awaited the development of the computer chip video camera
in 1986. Although laparoscopy could never have developed without the substantial
aforementioned contributions, this breakthrough was surely the single most important
factor which sealed the influential place of laparoscopic surgery in modem surgical
practice. V/ithin one year, Mouret of Lyon had performed the first laparoscopic
cholecystectomy in a human, finally exciting momentous worldwide interest in
operative laparoscopy by General Surgeons. However several groups claim prior
independent development of laparoscopic cholecystectomy in an animal model, namely
Cuschieri and Nathanson in Dundee(Cuschieri and Buess, 1992), and Filipi(Filipi et al.,
1991). The first published report using a multipuncture technique in humans was by
Dubois in 1989(Dubois et al., 1989), and during that year the procedure was established
in Bordeaux by Perissat(Perissat et al., 1989), in Nashville by Reddick and
Olsen(Reddick and Olsen, 1990), in Dundee by Cuschieri and Nathanson(Cuschieri et
a1.,1990), and in Los Angeles by Berci(Berci, 1991). Since then, the practice of
laparoscopic cholecystectomy has snowballed internationally, and spawned the
development of the plethora of laparoscopic intraabdominal operations which are
currently performed
It is the reduced trauma of access offered by operative laparoscopy that has captured the
imagination of the General Surgical community. Several tiny incisions can replace a
long laparotomy or thoracotomy incision. The subsequent patient benefits that flow
from this include reduced total operative trauma, reduced incidence of major wound
complications, reduced adhesive complications, shorter hospital stay, and a quicker
return to work or normal activities(Cuschieri, 1995). However, laparoscopy is not
necessarily benehcial for every abdominal operation, and in some cases it may actually
-8-

be detrimental. The total operative trauma sustained by a patient undergoing a surgical
operation has 2 components;
. access trauma related to the exposure of the operative region (e.g. by laparoscopy or
laparotomy), and
o procedural trauma, which is the injury inflicted in executing the operative procedure.
The benefit of laparoscopic surgery over conventional open surgery is greatest when
access trauma constitutes a large component of the total operative insult(Cuschieri,
lees).
-9-

2.2 Complications of laparoscopic surgeryAs the capability to perform laparoscopic intraabdominal surgery evolved to to the
extent that it triggered a revolutionary change in the practice of gastro-intestinal
surgery, so did the capability for surgeons utilising this technology to create unfamiliar
complications. A generation of fully trained surgeons was required to re-enter the
learning-curve for operative surgery, resulting in a heightened awareness of potential
and observed complications unique to laparoscopy(Altman,1992). The complications
of laparoscopy can be broadly divided into two major groups; those inherent to
laparoscopy and those related to the specific operative procedure.
Complications related to specific operative procedures analysed in this work are
considered in the appropriate sections. Reference to complications related to other
specific operative procedures capable of being performed laparoscopically is beyond the
scope of this thesis. In contrast, investigation of complications universally inherent to
laparoscopy comprises a large part of this thesis, and an introductory overview is
conceptually useful as many can be avoided with knowledge of the pertinent technical
details. The complications inherent to laparoscopy include those related to needle and
trocar insertion; those related to the presence of a tension pneumoperitoneum; and those
related to the manipulation of laparoscopic instrumentation(Crist and Gadacz, 1993).
9
-10-
2.2.1 Complications related to needle and trocar insertion
The occurrence of injury to intraabdominal structures complicating insertion of
laparoscopic needles and trocars is well documented. The most serious injuries are
those inflicted on major vascular structures in the retroperitoneum and on splanchnic
viscera. The incidence of injury to major retroperitoneal vessels has been reported as
0.03% in two major studies; one analysing 100,000 laparoscopic gynaecologic
procedures(Mintz, 1977), and the other carefully followingup 3229laparoscopic
herniorrhaphies(Phillips et al., 1995). Between 9Yo and 13 o/o of patients sustaining such
an injury will die(Deziel etal.,1993 ; Baadsgaard et al., 1989). Vascular injury during
Veress needle insertion is usually obvious during aspiration manouevres as blood
appears in the syringe. Injury during trocar insertion may be concealed, and only
evidenced by intra-operative hypotension. Haemodynamic instability may be delayed
until the postoperative period if haemorrhage is contained in the retroperitoneum, or if
tamponaded by pneumoperitoneal pressure - especially in the case of venous injury
Immediate laparotomy and repair is mandatory as soon as major vascular injury is
suspected. Minor vascular injuries may also occrÍ during needle or trocar insertion, and
typically involve the epigastric vessels. These can usually be controlled by
electrocautery or suture ligation, and may be avoided by transillumination of the
anterior abdominal wall prior to trocar entry, and by visually controlled trocar egress at
the completion of the procedure.
Splanchnic viscera most commonly injured during initial laparoscopic abdominal access
are bowel and bladder, with a reported incidence of 0.1%o (Phillips et al., 1995 ; Deziel
et al., 1993). These may go unrecognised with potentially fatal consequences(McKernan
and Champion, 1995). Identification of such an injury can be made because of the odour
- 11-

produced, or visually by directly witnessing intestinal laceration, or indirectly by bilious
or faecal staining. Bladder injuries can be recognised by the appearance of blood or gas
in the urinary catheter bag. Most such injuries will require primary suture repair and
decompression of the viscus concemed until healing has been achieved. To avoid
splanchnic visceral injury, it is customary to position the patient in reverse
Trendelenburg tilt to displace viscera from the umbilicus, and nasogastric compression
of the stomach and urinary catheter drainage are also strongly recommended(Crist and
Gadacz,1993).
Techniques designed to minimize the complications of needle and initial blind trocar
access continue to evolve. The most popular is to perform "open laparoscopy" followed
by placement of a blunt{ipped Hasson trocar under direct vision(Hasson, 1971). Two
comparative studies have reported a lower complication than with the alternative Veress
needle technique(Ballem and Rudomanski, 1993 ; Sigman et al., 1993). Although the
Hasson approach is simple and requires no extra equipment, it does not provide the
definitive solution. It is technically more demanding if access to the umbilical
"window" is precluded by obesity or the consequences of previous surgery, and
conclusive data from large studies is still not evident(l.lathanson,1995). A newer
development designed to achieve safer access is the use of an "optical Veress needle"
that allows visual control of abdominal wall penetration prior to pneumoperitoneal
insufflation and trocar entry(Schaller et a1.,1995). Endoscopically-controlled trocar
insertion can also be achieved using a variety of other techniques, a selection of which
have been reviewed by Melzer(Melzer et al., 1995), including the "windo'wed trocar",
the "optical trocar", the "Visiport", arrd the "optical scalpel". An additional measure of
safety may be introduced to visually-guided endoscopic access by the use of suction to
-12-

anchor the peritoneum to the trocar, thereby preventing tenting and minimizing the
depth of penetration of the needle(Klemm and Salm, 1995).
Disposable trocars have a reputed safety advantage whereby a shield mechanism
protects the trocar point from damaging intra-abdominal organs. However the use of
shielded trocars does not completely eliminate the risk of visceral injury, and the
importance of the safety shield may be over-rated. First, the safety advantage of trocar
shields is proportional to the brevity of the interval between entry into the abdomen and
engagement of the shield(Oshinsky and Smith, 1992).If this interval is prolonged, for
example by excess penetration force or inadequate pneumoperitoneum, the trocar tip
will no longer be protected. Second, it may lull the unwary into a false sense of
security(Nathanson, 1995), which is perhaps the reason some surgeons report a
paradoxically lower rate of injury using trocars without a safety shield(Voyles et al.,
1992). Less tangible safety benefits have been attributed to the use of disposable
trocars, deriving from the guarantee that previously unused instruments are always
sharp, and can be utilised with greater precision in the knowledge that less force is
required to divide tissue. For example, one study has reported that disposable trocars
can be introduced with approximately half as much force (7.14 lb. or approximately 32
N) than is required for a similar reusable device (14.55 lb. or approximately 66 N). It
was suggested that the greater control imparted from a reduction in force could translate
to fewer trocar-related injuries(Corson et al., 1989).
Other potential problems associated with abdominal entry include complications at the
port site. Postoperative herniation at port sites has been well documented, and occurs in
about 1 in 1000 cases (Crist and Gadacz,1993; Phillips et al., 1995), with or without
-13-

strangulation or obstruction of the herniated viscus. Fascial closure of the umbilical
wound and all port sites lOmm or larger is now widely practiced in an attempt to reduce
the incidence of hernia formation. Use of cutting trocars may predispose to hernia
formation because of the capacious gap they create in transit through the abdominal
muscle layers by comparison with conical trocars.
Port sites may also become contaminated with micro-organisms or malignant cells.
'Wound infection at port sites is reported with an incidence of 0.l2Yo following
laparoscopic herniorrhaphy(Phillips et al., 1995),1% following laparoscopic
cholecystectomy and up to 3Yo following laparoscopic appendicectomy(Crist and
Gadacz,1993). As one would expect, these figures suggest that extraction of
contaminated specimens is more likely to precipitate wound infection than procedures
in which port sites are used only for instrument access
A more vexing problem is that of putative contamination of port sites with exfoliated
malignant cells following resection of intraabdominal tumours, resulting in port site
metastases. It is disturbing to read reports of subcutaneous metastases following
apparent curative laparoscopic resection of early stage tumours(Lauroy et a1., 1994;
Gleeson et al., 1993). This problem is of sufficient topical concern to have warranted a
leading review in the British Journal of Surgery(Vy'exner and Cohen, 1995). Wexner
and Cohen observe that at least 30 port site recurrences after laparoscopic operations
have been reported. By summarizing existing reports, they derive a 6.30/o incidence of
this complication after laparoscopic colorectal surgery for cure of malignancy. They
contrast the frequency with which this problem is reported against the paucity of
evidence for wound recuffence after colorectal surgery via a standard laparotomy. Only
-14-
one such series is available(Hughes et al., 1983), citing al%oincidence of wound
recurrence, considerably lower than the derived incidence for port site recurrence.
Although the aetiology of port site metastasis is unknown, it is associated with some
unusual features. Recurrence may occur at a port site distant from where the specimen
was retrieved(Wexner and Cohen,1995), recurrence is not limited to colorectal
malignancy(Gleeson et al., 1993), and preferential seeding of port sites compared with
the laparotomy wound has been observed when the operation has been converted to an
open approach(Jacobi et al., 1994).
Problems of port site contamination with micro-organisms may be minimized by
retrieving specimens in a sterile bag prior to extraction, and several commercial devices
designed to facilitate this process are now available. Unfortunately, for the reasons
outlined above, the same may not be true for port site contamination with malignant
cells, and there is presently no known way to avoid this complication besides restricting
the use of laparoscopy to the treatment of benign disease or palliative operations(Ramos
et al., 1994).
-15-

2.2.2 Complications related to the presence of a tension pneumoperitoneumComplications related to the physical presence of a tension pneumoperitoneum have
been amply reported in the anaesthetic and gynaecologic literature, but are less familiar
to alimentary tract surgeons, perhaps because their manifestations are isolated from the
site of the operative procedure. Systemic cardio-respiratory complications pursuant to
carbon-dioxide pneumoperitoneum are the best known (see Section3.2.3, Effect of
systemic haemodynamics on splanchnic visceral vasculature) and include alterations in
venous return and cardiac output, cardiac arrythmias, reduced lung compliance and
functional residual capacity, pneumothorax, and pneumomediastinum
Haemodynamic variations may also be induced by pneumoperitoneum at a loco-
regional rather than systemic level, adversely affecting the viability of splanchnic
viscera (see Section3.2.3, Locoregional effect of pneumoperitoneum on splanchnic
visceral vasculature) and haemodynamic changes at all levels combined with
haematologic alterations may accentuate the risk of thromboembolic sequelae (see
Section 3.2.6, Summary of net thromboembolic risk during laparoscopy).
Creation of a pneumoperitoneum with cold, and particularly non-humidified carbon-
dioxide can result in hypothermia with its attendant problems (see Section 3.1,
Temperature regulation). Misplacement or escape of gas into real or potential spaces
other than the peritoneal cavity results in surgical emphysema. This usually involves
subcutaneous or preperitoneal planes, and provided it is detected and corrected tends to
cause few clinical problems and resolves spontaneously. A rare but very dangerous
complication of gas under pressure is the opportunity for gas embolism. This may occur
directly if the insufflating needle or trocar enters a vessel, or indirectly if a large venous
channel is opened. Although small amounts of CO2 are rapidly absorbed from the
-16-
bloodstream and generally cause little problem(Gaff et al., 1959), entry of large
amounts of gas into the circulation can cause sudden cardiovascular collapse when
trapped in the right ventricle or pulmonary circulation. In addition to hypotension, the
clinical scenario includes tachycardia, a "mill-wheel" murmur, widened QRS interval
and increased P6CO2. Immediate treatment must consist of cessation of insufflation,
complete evacuation of the pneumoperitoneum, and positioning the patient in
Trendelenburg with left lateral tilt to prevent gas migrating to the outflow tract of the
right ventricle(McKernan and Champion, 1995). Artificial hyperventilation to blow-off
CO2 and aspiration of central venous gas should also be undertaken(Crist and Gadacz,
tee3).
2.2.3 Complications related to insertion and manipulation of instrumentationComplications directly attributable to deficiencies in instrument durability and function
include potential transmission of infection, visceral injury or leakage from malfunction,
electrical inj.try from insulation failure, and thermal injury from contact with light
sources. Furthermore, a legion of complications similar to those described for initial
trocar entry can also arise as a result of the surgeon's insertion of the instruments rather
than arising from the instrument per se
-17 -
3. GENERAL PROBLEMS OF LAPAROSCOPY
3.1 Temperature regulation
3.1.1 lntroductionClinical hypothermia has been defined as core temperature below 36o Centigrade (C)
(Morris and Kumar,1972). Perioperative hypothermia results from the effects of
anaesthesia, augmented by certain characteristics of the individual patient. General
anaesthesia influences the development of intraoperative hypothermia by disturbing
thermal regulatory mechanisms. This occurs in three phases(Sessler, 1993). In the first
instance anesthesia reduces the thermoregulatory threshold for vasoconstriction by 2.5"
C, resulting in a core-to-peripheral redistribution of body heat(Sessler,1993). A second
decrease in body temperature is a result of heat loss exceeding metabolic heat
production.
Heat production decreases only minimally during anaesthesia(Stevens et al., l97I), and
respiratory heat loss is relatively small(Bickler and Sessler, 1990), therefore the
predominant site of heat loss is cutaneous. For example, exposure of the unclad,
immobile patient to the cool theatre environment(Morris and Wilkey,1970; Morris and
Kumar, 1972 ; Clark et a1.,1954 ; Morris, l97I), evaporative water losses from surgical
incisions(Morris and Kumar, 1972), evaporation of surgical skin preparation solution,
and use of cold intravenous infusions or irrigating fluids(Imrie and Hall, 1991 ; Shanks
et al., 1988) can all cause heat loss through the skin. Certain types of surgery, such as
laparotomy, contribute to loss of heat from surgical incisions by increasing the surface
area of the patient available for heat exchange(Tollofsrud et al., 1984 ; Roe, 1971)
After 3-4 hours, core temperature finally reaches a plateau. Patients that are kept
relatively warrn require no active thermoregulation at this stage. If not kept warm,
-18-
thermoregulatory vasoconstriction decreases cutaneous heat loss(Sessler et al., 1992),
and sequesters metabolic heat to the core(Belani et al., 1993).
Patient characteristics such as age, size and associated medical conditions augment both
the degree of hypothermia and also the resultant effects. For example, in elderly patients
with limited cardiopulmonary reserves marked postoperative thermogenic shivering can
dramatically increase oxygen consumption, risking cardiac arrythmias, failure, or
myocardial infarction(Tollofsrud et al, 1984 ; Heymann, 1977).
The importance of perioperative hypothermia becomes apparent when the numerous
deleterious effects it may cause are considered. Conditions such increased susceptibility
to dermal infection(Sheffield et a1.,1994), induction of a hypokalaemic
state(Boelhou\À/er et al., 1987 ; Laszlo et al., 1990), impaired myocardial
function(Mattheussen et al., 1990), respiratory depression, negative nitrogen
balance(Carli et al., 1989), thrombocytopaenia, and depletion of clotting factors(Ellis et
aI.,1957) have been reported.
The net effect of these complications is reflected in the mortality rate of patients thus
affected. One study reported a24%o mortality in postoperative patients who remained
hypothermic after 2 hours compared with4yo of their normothermic
counterparts(Slotman et al., 1985). There is a financial penalty as well, because
hypothermic patients are reported to spend up to t hr longer in the Recovery
Ward(Conahan,1982).
In the past it had been assumed that the impact of laparoscopy would be to decrease the
risk of heat loss by comparison with the corresponding "open" procedure. This
assumption was based on the knowledge that the predominant thermal loss during
-19-
surgery is from exposed surfaces. During laparotomy the open abdomen exposes a
greater surface area, whereas during laparoscopy with the abdomen sealed there is less
potential heat loss from convection as well as conduction and radiation. Despite the
peritoneal cavity not being in contact with the ambient theatre environment, thermal
loss is at least comparable during open and laparoscopic cholecystectomy(V/allasvaara,
1992), and some factors unique to laparoscopy may actually increase the risk of heat
loss during this type of surgery(Ott,I99la; Monagle et al., 1993).
Laparoscopic procedures may take longer to perform than their open counterparts,
predisposing the patient to greater heat losses from prolonged exposure in the
anaesthetised state. In addition, during laparoscopy heat loss also occurs due to the use
of CO2 gas which is insufflated into the peritoneal cavity to provide surgical access
Some laparoscopic procedures require only modest CO2 flow rates, however other
advanced laparoscopic procedures such as colorectal and oesophageal operations
frequently result in large gas leaks due to the use of multiple large ports of up to 33mm
in diameter, insertion and removal of laparoscopic instruments, extraction of
electrocautery smoke which may obscure vision, aspiration of gas by the sucker as
intraperitoneal fluid is removed, and inadvertent removal of ports not fixed securely to
the abdominal wall. Insufflation may therefore be required at high-flow rates to
maintain adequate pneumoperitoneum over a sustained period. These factors of
prolonged laparoscopic surgery, flow rate greater than 3llmin, and frequent gas
extraction have previously been confirmed to result in thermal losses(Ott, l99la;
Seitzinger and Dudgeon, 1993)
The capability to perform advanced laparoscopic intra-abdominal surgery has resulted
in this mode of access currently accounting for a large proportion of operative
-20 -

procedures, yet controlled studies detailing the influence of laparoscopic surgery on
perioperative hypothermia are scarce. The existence of this problem in a clinical
practice setting, although widely recognised, is represented in the literature by a solitary
retrospective analysis published in 1993(Seitzinger and Dudgeon, 1993). Seitzinger
measured patients' temperatures during laparoscopic cases ranging between three and
six hours, and observed an average beginning temperature of 36.1o C fell to an average
of 33.3" C. Four to six hours rewarming was required in the recovery room to return the
patient to a normal temperature.
Effect of warmed gas
To counteract the cooling effect of CO2 some companies have provided insufflators
with built-in heating elements, despite the absence of controlled evidence that
laparoscopy contributes to perioperative hypothermia, or that gas warming devices are
protective against it. The only study to address this issue reported that postoperative
temperatures in 20 patients receiving warmed CO2 (35" -35.5" C) were within 0.lo C of
pre- and intra-operative findings(Ott, 1991b). This contrasted to a control group
receiving unwarmed CO2 (21" C) where a thermal loss of 0.3" C per 50L of consumed
CO2 was reported. Unfortunately, this valuable study was not randomised and different
operations were performed both between and within groups. Non-commercial warming
devices were used, and similar but not identical flow rates and volumes of CO2 were
used. These methodological factors could have introduced errors and the conclusion that
the use of physiologic temperature CO2 helps diminish thermal loss remains to be
proven.
-21 -
AimsThe aim of this study was to determine if there is an increased risk of deleterious core
temperature changes during laparoscopic insufflation. It was hypothesized:
1. That insufflation of CO2 gas contributes to hypothermia during laparoscopic surgery
if high-flow rates are required over a prolonged period of time
2. That insufflation of warmed rather than cold CO2 gas minimizes the extent of
hypothermia during laparoscopic surgery if high-flow rates are required over a
prolonged period of time.
3.1.2 MethodsEthical approval for this project was granted by the Animal Ethics Committees of The
Queen Elizabeth Hospital and the University of Adelaide. Six pigs of approximately 30
kg were studied. Each pig was anaesthetised and studied on 3 occasions, acting as its
own control. The order of these studies were randomised. Each of the studies were
performed one week apart to allow complete recovery of the animal from the
anaesthetic.
On one occasion the animal was anaesthetised for three-hours and temperature
measured without pneumoperitoneum being established. On another occasion, the
animal had cold CO2 insufflated at approximately 25" C (Table l) for three-hours. The
abdominal pressure was maintained at 10 mm Hg. The COr was delivered through a
modified LINS-1000 insufflator (Cook Medical Technology, QLD Australia) via a l0
mm port (Ethicon Australia) inserted into the peritoneal cavity through the umbilicus.
A second, supra-umbilical 10 mm port allowed a standardised "leak" of CO2 at l0
Llmin from the peritoneal cavity by fully opening the 3 way stopcock. This was
-22-
performed to simulate the repeated gas losses that are experienced clinically during
some advanced laparoscopic procedures.
On the remaining occasion, the animal had warmed CO2 insufflated at approximately
30' C (Table l) for three-hours, otherwise experimental parameters remained as for the
second occasion.
-23 -
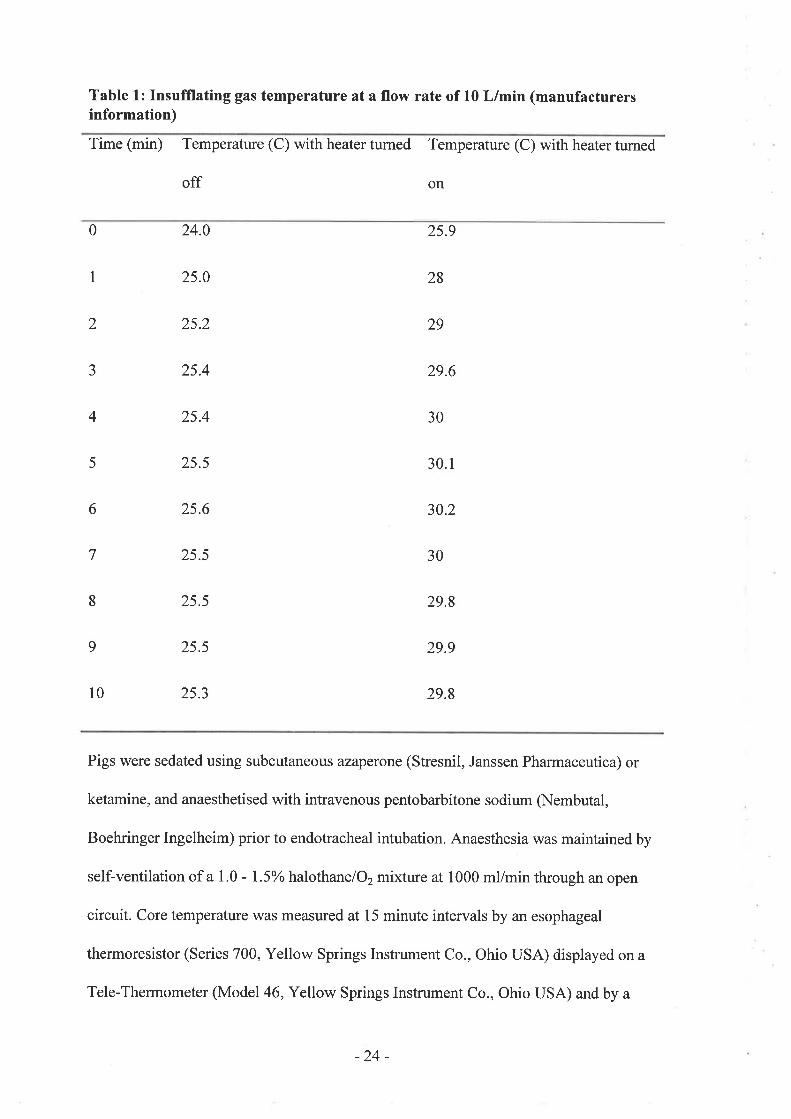
Table 1: Insufflating gas temperature at a flow rate of 10 L/min (manufacturersinformation)
Time (min) Temperature (C) with heater turned Temperature (C) with heater tumed
off on
0
I
2
J
4
5
l0
24.0
25.0
2s.2
25.4
2s.4
25.5
2s.6
25.5
25.5
25.5
25.3
29
25.9
28
29.6
30. r
30.2
30
29.8
29.9
29.8
30
6
7
8
9
Pigs were sedated using subcutaneous azaperone (Stresnil, Janssen Pharmaceutica) or
ketamine, and anaesthetised with intravenous pentobarbitone sodium (Nembutal,
Boehringer Ingelheim) prior to endotracheal intubation. Anaesthesia was maintained by
self-ventilation of a 1.0 - 1.5% halothanelO2mixture at 1000 ml/min through an open
circuit. Core temperature was measured at 15 minute intervals by atr esophageal
thermoresistor (Series 700, Yellow Springs Instrument Co., Ohio USA) displayed on a
Tele-Thermometer (Model46, Yellow Springs Instrument Co., Ohio USA) and by a
-24-

second similar thermoresistor placed into the peritoneal cavity through the umbilical
1Omm port to monitor intra-peritoneal temperature
Ambient temperature was also recorded at 15 minute intervals, and the temperature of
the theatre environment was maintained close to 24" C. A metallic reflective blanket
was wrapped around the animal to reduce thermal loss from cutaneous exposure.
All procedures were performed under aseptic conditions, and animals received a single
perioperative dose of intramuscular penicillirVstreptomycin. The animals were
anaesthetised before the placement of and during removal of laparoscopic ports. As only
two 1Omm diameter ports were required, postoperative analgesia was not required. As
no intra-abdominal procedure was carried out, post-operative ileus did not occur, and no
alteration to the animals eating pattem was observed. The one week interval between
studies allowed complete recovery from the effects of anaesthesia. Before reversal of
anaesthesia all ports were removed, and fascial and skin defects were closed with
sutures. At the completion of the final anaesthetic, the animals were killed by an
intravenous overdose of pentobarbitone.
The statistical method utilised was repeated measures analysis of variance, with
grouping factors of treatment (no gas, cold gas, warmed gas) and a within factor of
time. This method of analysis was the most appropriate for the described experimental
situation(Ludbrook, 1994). Analysis was performed using 5V, BMDP statistical
software UCLA (1991), with significance analyses performed at a probability level of
0.05.
-25 -

3.1.3 Resu/fs
Using repeated measures analysis of variance, regression lines representing the
predicted temperature effect over time were fitted to each of the three treatment groups.
The mean room temperature over all experiments was 23.7" C. Both intraperitoneal and
oesophageal temperature were significantly affected by the duration of the experiment
and the whether or not the animal received gas insufflation. It was found that the
regression lines summarizing changes over time for the cold gas and warm gas
treatment groups were statistically indistinguishable. Consequently, there was no
signihcant temperature difference between animals that received cold or warmed gas
over a 3 hour period, and these two groups can be considered to behave as one.
The intraperitoneal temperature at the commencement of anesthesia for control animals
that received no gas insufflation was 37.7" C, at 3 hours a significant rise in temperature
to 38o C was observed. The intraperitoneal temperature at the commencement of
anesthesia for animals that had cold or warmed gas insufflated was again3T.7" C,btú
fell to 36" C at 3 hours, a statistically significant difference of 1.7" C (p < 0.001). The
regression line that summarized temperatures recorded by control animals (no gas) was
significantly different from the pooled estimate of animals undergoing gas insufflation
O < 0.001), reaching almost 2o C after 3 hours (Figure 1).
-26 -
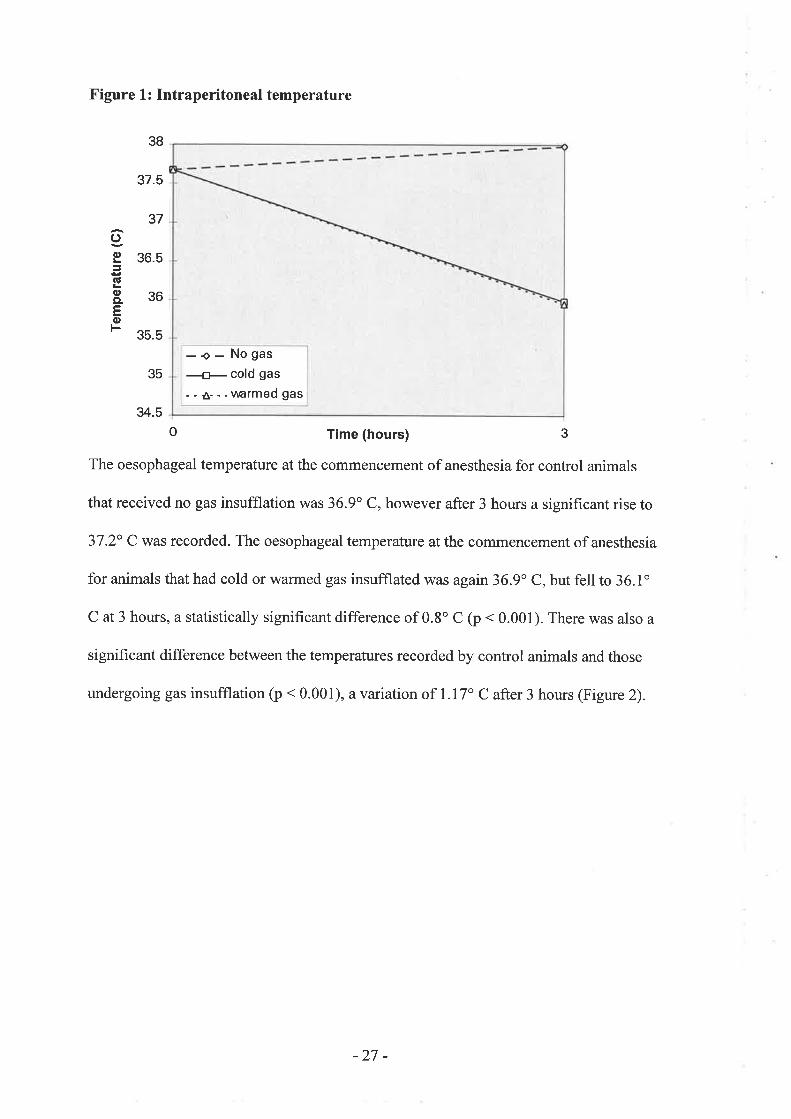
Figure L : Intraperitoneal temperature
37.5
35.5
34.5
o Time (hours) 3
The oesophageal temperature at the commencement of anesthesia for control animals
that received no gas insufflation was 36.9" C, however after 3 hours a significant rise to
37.2" C was recorded. The oesophageal temperature at the commencement of anesthesia
for animals that had cold or warmed gas insufflated was again36.9o C, but fell to 36.1o
C at 3 hours, a statistically significant difference of 0.8o C (p < 0.001). There was also a
significant difference between the temperatures recorded by control animals and those
undergoing gas insufflation (p < 0.001), a variation of 1.17" C after 3 hours (Figure 2).
3B
37
5
36
36.
oc,
a!
oCL
tso
35-. - No gas
a- cold gas
--A--.uarmedgas
-27 -
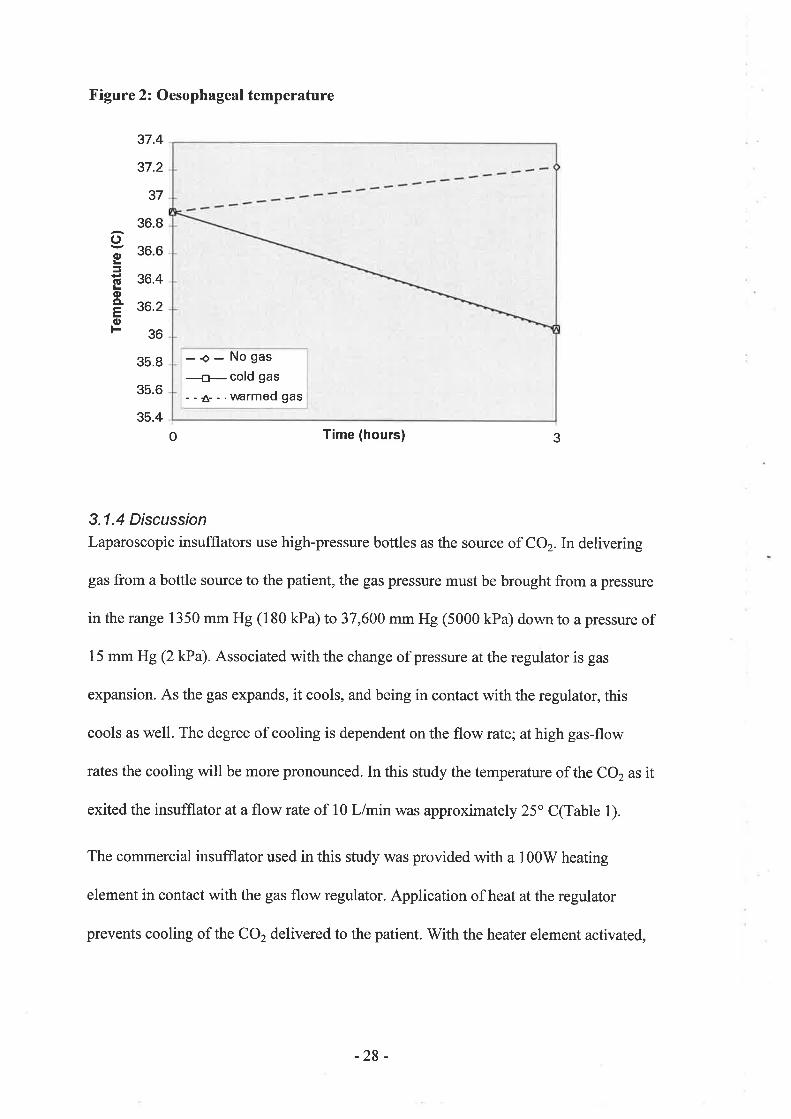
Figure 2: Oesophageal temperature
37.4
37.2
37
36.8
36.6
36.4
36.2
36
35.8
35.6
35.4
o Time (hours)
3.1.4 DiscussionLaparoscopic insufflators use high-pressure bottles as the source of CO2. In delivering
gas from a bottle source to the patient, the gas pressure must be brought from a pressure
in the range 1350 mm Hg (180 kPa) to 37,600 mm Hg (5000 kPa) down to a pressure of
15 mm Hg Q kPa). Associated with the change of pressure at the regulator is gas
expansion. As the gas expands, it cools, and being in contact with the regulator, this
cools as well. The degree of cooling is dependent on the flow rate; at high gas-flow
rates the cooling will be more pronounced. In this study the temperature of the CO, as it
exited the insufflator at a flow rate of l0 L/min was approximately 25" C(Table 1).
The commercial insufflator used in this study was provided with a 100V/ heating
element in contact with the gas flow regulator. Application of heat at the regulator
prevents cooling of the CO2 delivered to the patient. V/ith the heater element activated,
ooJ
(!oCL
(1,
F
3
-o- Nogas
#cold gas
- - Â- - .uarmed gas
-28 -

the regulator could be held at 45" C, and the temperature of the CO2 as it exited the
insufÍlator at a flow rate of 10 L/min was approximately 30o C (Table 1).
The methodology of this experiment controlled for the predominant confounding factors
which are known to cause intraoperative hypothermia; cutaneous heat losses from
exposure to an ambient theatre environment of less than24" C, evaporative water losses
from surgical incisions, and use of cold intravenous infusions or irrigating fluids.
Although inhaled gases were not warmed, the control arm of this experiment (no gas
insufflation) indicates that respiratory heat losses were not a contributing factor, and
this correlates with previous reports that respiratory heat losses are minimal(Bickler and
Sessler, 1990). Therefore the only factor acting to alter body temperature between the 3
arms of the experiment was the insufflation of cold or warmed gas.
Insufflation of CO2 gas at a flow rate of 10 L/min over a three-hour period resulted in a
statistically significant decrease in body temperature. The magnitude of this
hypothermic effect (up to 2" C) due solely to laparoscopy would exert a clinically
signif,rcant impact, especially when added to the numerous other factors tending to
reduce body temperature during general anaesthesia. The changes we observed concur
with two previous uncontrolled studies addressing the matter of laparoscopic
hypothermia in which it was reported that changes in core temperature as a result of
laparoscopy can be expected to fall by only 0.3o C for each 50L of CO2 delivered(Ott,
l99la; Ott, l99lb). Although it is true that an average leak of l0l/min is unlikely to be
tolerated for prolonged periods in most laparoscopic operations, this exaggerated
"worse-case" scenario was chosen as the model to unmask any effect which may be
potentially disguised by a more clinically modest situation. It is also perhaps trivial that
-29 -
the difference between the cold and warmed gas was only 5o C, but this represents the
limit of the capabilities of commercially-available insufflators. The design of the study
was intended to reflect the reality faced by surgeons in current clinical operating
conditions, therefore precluding the study of a potentially more useful warmed gas
temperature of 40o C, for example. Yet if laparoscopic gas warmers were to heat gas to
higher temperatures, this may introduce a deleterious drying effect on intra-abdominal
membranes and therefore the gas would also have to be humidified. Unfortunately, this
would cause condensation inside the insufflator and present an electrical safety hazard.
For the time being, the provision of humidified, physiological temperature gas is a
technological problem.
It is of interest that control pigs anaesthetised for three-hours at a mean temperature of
23.7" C recorded a rise in body temperature. A positive correlation between the rate of
body temperature rise and ambient room temperature has been reported in adult surgical
patients under general anaethesia(Clark et al., 1954), and this phenomenon has also
been shown to occur in dogs(Allen, 1986).
Our results have left one question unanswered - why was warrned gas no better,
although it exited the insufflator 5o warmer than the cold gas? A simple thermodynamic
calculation indicates that the heat required to raise the temperature of the CO2 gas
flowing at l0 L/min from 25 to 37" C is 0.9 W, and the heat required to raise the
temperature of the CO2 gas from 30 to 37" C is 0.48 W. Both of these are minuscule in
comparison to the basal metabolic rate of 80 W, and would reduce body temperature by
less than 0.lo over 3 hours. This confirms that the observed core temperature
differences cannot be explained by the difference in gas temperature used in this study.
-30-
So where did the heat go? A further thermodynamic calculation shows that the latent
heat required to evaporate body water in the pig to saturate the initially dry CO2 stream
of 10 L/minat37o C is l8 W. This indicates that the evaporation of body water to
saturate the CO2 is a much greater source of heat requirement and the corresponding
predicted temperature drop after 3 hours is 1.6o C for a 30 kg animal. V/ithin the errors
of measurement, this would account for the most of the observed intraperitoneal
temperature drop of 1.7o C.
In addition, a subsequent experiment prompted by these findings has shown that the
temperature of the gas, which was measured at the patient outlet of the insufflator,
rather than as it entered the abdomen, actually falls exponentially along the insufflator
tubing until it reaches room temperature. It was observed that the gas temperature will
fall roughly 63%o for every 1.5m length of insufflator tubing. Because standard
insufflator tubing is 3m long, the temperature of gas entering the abdomen in the
"\¡y'arm" and "cold" cases actually differed by only 0.7" C.
In summary, the results indicate that laparoscopic gas insufflation causes a significant
fall in core temperature, and the provision of warmed rather than cold gas using
currently available insufflators will confer no protection against a fall in perioperative
core temperature heat loss. However, it is suggested that humidification of the
insufflated CO2 would largely resolve the problem of laparoscopy-induced
hypothermia, but in addition, insufflator tubing should be equipped with an insulated
heating wire to prevent warmed gas equilibrating with room temperature as it flows to
the patient. However the provision of humidified, heated gas to minimize perioperative
hypothermia is a problem which remains to be overcome. Controlled studies will be
required to validate the clinical utility of future generations of insufflator apparatus,
- 31 -
with monitoring of gas saturation and temperature as it exits the device and as it enters
the patient's abdomen
-32-
3.2 Thromboembolism
3.2.1 lntroductionVenous thromboembolism following surgery is associated with significant morbidity
and mortality(Caprini and Natonson, 1989). The magnitude of the problem in the
United States alone has been cited at 630 000 cases annually, with 200 000
deaths(Dalen and Alpert, 1975). Most pulmonary emboli arise from thromboses in the
iliac and femoral veins. Such deep vein thrombosis (DVT) can be a source of
considerable morbidity, even if it does not precipitate pulmonary embolism. The
complications of chronic venous insufficiency, secondary varicose veins, and venous
gangrene consume large amounts of health care resources for their treatment.
Epidemiological studies have reported postphlebitic syndromes in up to 2o/o of the
population, and have projected that 800 000 Americans suffer from venous ulceration as
a result(Caprini et al., 1988).
Vascular thromboembolism occurs following both open and laparoscopic
procedures(Jamieson et al.,1994). The risk of fatal pulmonary embolism in patients
over 40 years of age undergoing open general surgical procedures is 0.65%(Caprini and
Arcelus, 1994). Although the incidence of postoperative thromboembolic disease
following minimally invasive procedures has not been objectively established, the risk
of pulmonary embolism must not be underestimated(Mitchell and Jamieson,1994;
Caprini and Arcelus, 1994). In a review of 77,604 patients undergoing laparoscopic
cholecystectomy at 4,292 American hospitals, 3 deaths were recorded as a result of
pulmonary embolism and2 from ischaemic bowel, giving a 0.006 0/o incidence of fatal
thromboembolic events(Deziel et al., 1993). A review of 12 000 patients undergoing
this procedure has reported l0 postoperative deaths (0.08%) (Scott et al., 1992). A
-JJ-

higher incidence of fatal postoperative pulmonary embolism of 0.14Yowas reported by
Dubois amongst 690 patients undergoing laparoscopic cholecystectomy(Dubois et al.,
1991). One particular series reported two clinically evident deep venous thromboses and
one fatal pulmonary embolism in 78 patients undergoing laparoscopic colorectal
surgery for malignant disease(Guillou et aL.,1993).
Death due to mesenteric thrombosis has been reported following uncomplicated
laparoscopic Nissen fundoplication(Mitchell and Jamieson, 1994) and laparoscopic
cholecystectomy(Paul et al., 1994) in otherwise healthy patients. Fatal portal vein
thrombosis following straightforward laparoscopic appendicectomy in a fit young
patient has also occurred (personal communication). These deaths secondary to
thromboembolism occurring after routine laparoscopic surgery have raised widespread
concern that some factor exacerbated by laparoscopy is acting to modify the danger to
patients that would previously have been considered low risk.
It has been estimated that clinically detectable non-fatal deep venous thrombosis
develops in 5Yo of patients undergoing open cholecystectomy who have not received
prophylaxis(Bergqvist et a1.,1990). There have not been any prospective series
objectively documenting the incidence of DVT after laparoscopic cholecystectomy, but
for comparison Caprini has recorded one DVT from amongst 74 patients prospectively
screened by duplex ultrasound (I.3%), after receiving graduated prophylaxis according
to risk(Caprini and Arcelus, 1994).It must be acknowledged that because most thrombi
remain silent, and discharge home occurs at an early stage following laparoscopic
procedures, it is likely that a considerable proportion of patients manifesting
thromboembolic complications are being missed.
-34-

Factors contributing to thromboembolism were originally described by Virchow, and
include hypercoagulability, impaired blood flow, and vessel wall abnormalities. During
laparoscopic surgery, changes in one or more of these factors may contribute to an
altered risk of postoperative thrombosis. These triad of factors are still considered the
most important influencing the pathogenesis of thromboembolism, but the hazard is
increased further in the presence ofadditional risk factors. Inherited risk factors consist
of antithrombin III deficiency, protein C or protein S deficiency, and
dysfibrinogenaemia. Acquired risk factors include advanced age, obesity, malignancy,
past history of thromboembolism. For the risk of thromboembolism to be accurately
assessed, the occurrence of any of the above predisposing factors must be recognised in
each patient.
This section investigates the thromboembolic risk during laparoscopic surgery by
experimental study of 2 of the 3 factors in Virchow's triad; hypercoagulability and
impaired blood flow in splanchnic visceral vessels. In order to formulate an
comprehensive analysis of the net risk of thromboembolic during laparoscopic surgery,
this section subsequently considers the available literature dealing with the remaining
elements of Virchow's triad; impaired blood flow in lower limb vessels, and vessel wall
abnormalities during laparoscopy. The section is completed by suggestions for
appropriate prophylaxis directed against this physiological complication of laparoscopy
based on sound theoretical principles and scientific evidence.
-35-
3.2.2 Thromboembolic risk induced by hypercoagulability
Introduction
The risk of venous thromboembolism following surgery has been demonstrated to
correlate with hypercoagulability which can be measured by a variety of tests. This is
the basis for using anticoagulants for the prevention of postoperative thromboembolism.
However, a direct relationship between any single test, hypercoagulability and the
incidence of thrombosis is not well established(Donaldson et al., 1990 ; V/alenga et al.,
1992).In addition, the specific process which initiates an increase in blood coagulation
following surgery has not been clearly identified.
Previously published work has documented hypercoagulability following open surgery
as in the past most operations were performed in this manner. A wide variety of
coagulation indices have been used to investigate this effect of open surgery, such as
protein C, protein S, antithrombin III, lupus-like anticoagulant(Donaldson et al., 1990),
heparin-induced platelet activation(Donaldson et al., 1990), factor VIII coagulant, Von
willebrand factor antigen, partial thromboplastin time(claes et al., 1992), and
plasminogen activator inhibitor-l (PAI-1) (Rosenfeld et al., 1993). Hypercoagulability
during the postoperative period has been documented thromboelastographically in
patients who do not receive prophylactic heparinization in a controlled study of 60
patients(Martinez et al., 1988). In a study of patients undergoing cholecystectomy
compared with healtþ controls, postoperative hypercoagulability could be traced in the
former group by a recalcification time system to determine first fibrin
formation(Lundquist and Sewdenborg, I 98 1).
Several of the above indicators remain unvalidated for routine use and are available
only as specific research tools. In contrast, D-dimer assays are generally available and
-36-
have been successfully used as markers for venous thrombosis following abdominal
surgery. Plasma D-dimer is a measurement of crosslinked fibrin degradation products
released as a result of fibrinolysis, and differs from earlier serum fibrin(ogen)
degradation product assays because of improved sensitivity and specificity for the lysis
of intravascular crosslinked f,rbrin(Rowbotham et al., 1992).In a study of 135 patients
undergoing major abdominal surgery, D-dimer levels preoperatively and on the first
postoperative day were significantly higher in the 3l patients who developed venous
thrombosis (by positive venography) than in the 104 patients who did not (by negative
Ir25 fibrinogen leg scanxRowbotham et al., Igg2).Another study assessing the
correlation between thrombotic tendency (as confirmed by venography) and D-dimer
levels in 185 postoperative patients determined an89Yo sensitivity for the
assay(Bounameaux et al., 1992).
Fibrinogen assays are also universally available and within the realm of the standard
battery of haematological investigations. Fibrinogen is a soluble plasma protein
involved in the fundamental reaction in blood clotting. The conversion of fibrinogen to
insoluble fibrin involves the release of polypeptides from the hbrinogen molecule
allowing the remaining fibrin monomer to polymerizeto form hbrin. The trend towards
hypercoagulability in the postoperative period can be demonstrated by elevation of
fibrinogen levels. Collins et al observed significant and predictable rises in fibrinogen
levels on the third and seventh day postoperatively in two groups of patients undergoing
major abdominal and major vascular surgery(Collins, Jr. et al., 1977). Other
investigators studying patients undergoing major abdominal surgery(Knight et al.,
1977), and extremity vascular surgery(Rosenfeld et al., 1993) have corroborated
-Jt-

elevated fibrinogen levels in the first72 hours postoperatively indicative of
hypercoagulability
V/ith the increasing use of laparoscopic methods for a variety of operations, further
investigation into the development of hypercoagulability and the accompanying
incidence of thrombosis has become necessary. To date, only one study, published in
abstract form, has addressed this matter(Caprini et al., 1991). Thirty-five consecutive
patients undergoing laparoscopic cholecystectomy taking a mean operative duration of
139 minutes were studied by this group in Illinois. Blood thromboelastography (TEG),
partial thromboplastin time (PTT), and prothrombin time (PT) were performed
preoperatively and on the first postoperative day. A significant increase in the TEG
index, and a significant reduction in the PTT were observed, suggesting that
laparoscopic cholecystectomy induces significant hypercoagulability on the first
postoperative day. Unfortunately this study was not controlled, and the results may
therefore not be unique to laparoscopic surgery but rather reflect other factors which
contribute to the well-established hypercoagulability that occurs after open surgery.
Aim
The aim of this clinical study was to assess fibrinogen, cross-linked fibrin degradation
products (D-dimer), prothrombin international normalised ratio (INR), activated partial
thromboplastin time (APTT) and platelets, during and following both open and
laparoscopic Nissen fundoplication to determine whether risk of thrombo-embolism
induced by hypercoagulability is increased by laparoscopic fundoplication.
-38-

Methods
Ten male and ten female patients were entered in the study. The patients' mean age \À/as
50 years (range 27 - 74 years). Seven patients underwent open Nissen fundoplication
and thirteen were performed by the laparoscopic technique.
Blood samples were drawn immediately prior to induction of anaesthesia þre-
induction), 15 minutes after skin incision (intraoperative), and on the first postoperative
day (day 1). All samples were analysed for levels of fibrinogen, cross-linked fibrinogen
degradation products (D-dimer), prothrombin international normalised ratio(INR),
activated partial thromboplastin time (APTT) and platelets. D-dimer values were
grouped within the following ranges: 0 - 0.25; 0.25-0.5; 0.25-0.5; 0.5-1.0; I - 2 mglL.
Data is expressed as mean + SEM and statistical differences were examined using
repeated measures analysis of variance (RM ANOVA) with contrasts using SAS PC
6.04 statistical software (SAS Institute lnc, Cary, North Carolina, USA). The protocol
for this study was approved by the Royal Adelaide Hospital Research Ethics
Committee.
-39-
Results
The results of blood coagulation indices are summarised in Table 2. Some sets of results
are incomplete due to sample clotting and this has been accounted for by the statistical
method used. The only coagulation marker to change significantly between the 3 time
periods was fibrinogen. Fibrinogen concentration changed to a similar degree in both
open and laparoscopic groups, decreasing after skin incision then increasing on day 1 to
a level above pre-induction values (Figure 3). For the open group, on day 1 pre-
induction and intraoperative levels were significantly different (p<0.05 and p<0.01
respectively). Likewise for the laparoscopic group, pre-induction and intraoperative
results were also significantly different on day I (p<0.005 in both cases).
No differences were evident between the open and laparoscopic groups, nor between
pre-induction, intraoperative and day I samples for any of the other coagulation indices.
No patient in this study developed a clinical deep vein thrombosis or pulmonary
embolism.
-40-
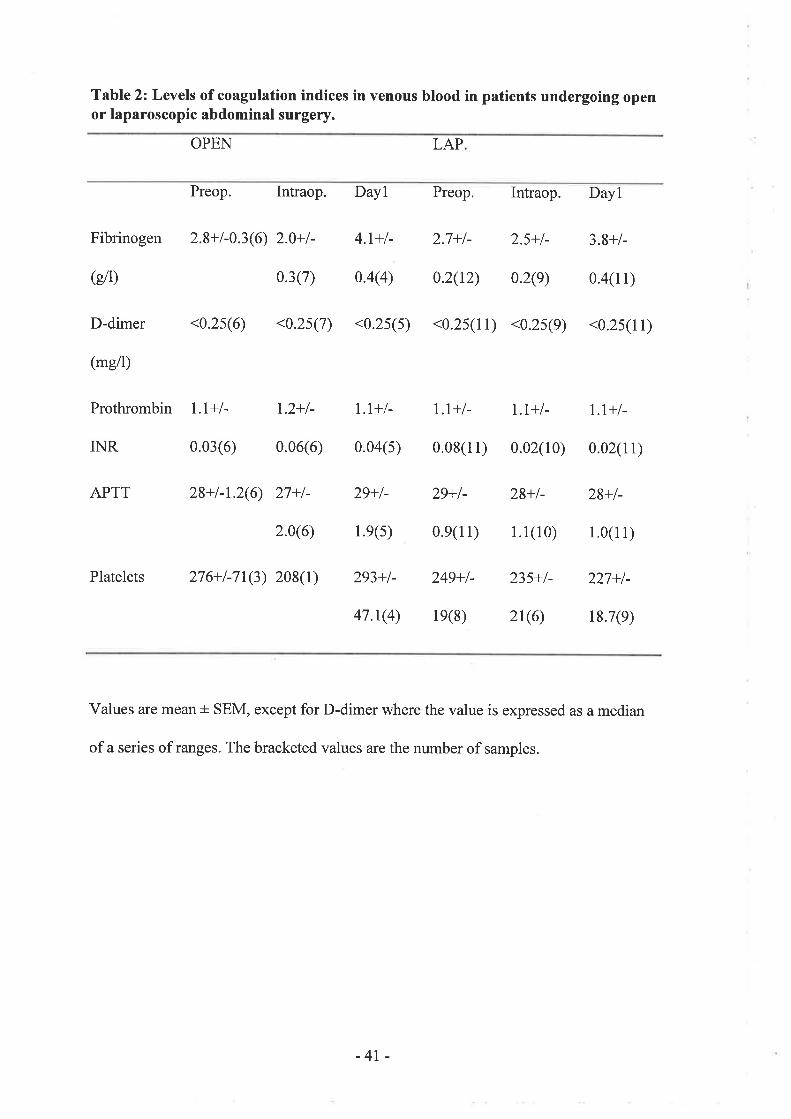
Table 2: Levels of coagulation indices in venous blood in patients undergoing openor laparoscopic abdominal surgery.
OPEN LAP
@fi)
Preop. Intraop. Dayl Preop. Intraop. Dayl
Fibrinogen 2.8+l-0.3(6) 2.0+l- 4.1+l- 2.7+l- 2.5+l- 3.8+/-
0.3(7) 0.4(4) 0.2(t2) 0.2(e) 0.4(11)
D-dimer <0.2s(6) <0.2s(7) <0.2s(s) <0.2s(11) <0.2s(9) <0.2s(11)
(mg/l)
Prothrombin l.I+l- 1.2+l- I.t+l- t.t+l- t.t+l- t.t+l-
INR 0.03(6) 0.06(6) 0.04(s) 0.08(11) 0.02(10) 0.02(11)
APTT 28+l-1.2(6) 27+l- 29+l- 29+L 28+t- 28+l-
2.0(6) 1.e(s) 0.e(11) 1.1(10) 1.0(l l)
Platelets 276+l-71(3) 208(l) 293+l- 249+l- 235+l- 227+/-
47.1(4) 1e(8) 2t(6) 18.7(e)
Values are mean + SEM, except for D-dimer where the value is expressed as a median
of a series of ranges. The bracketed values are the number of samples.
-4t-
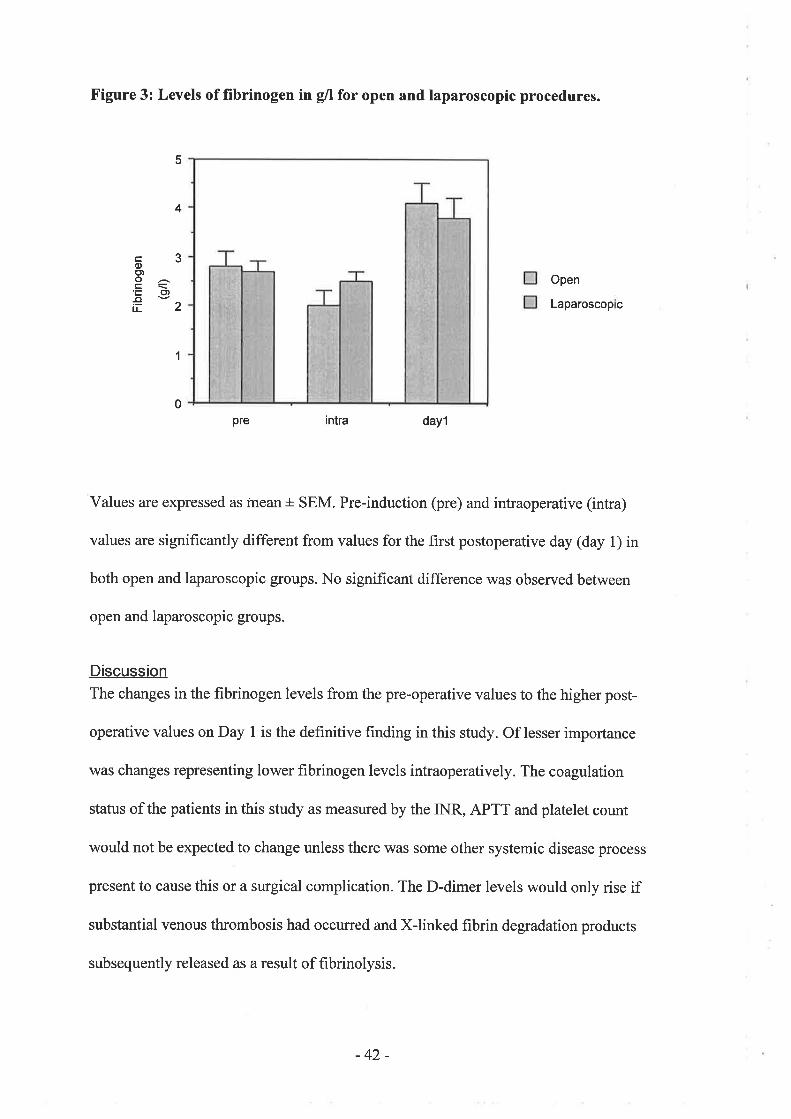
Figure 3: Levels of fïbrinogen in g/l for open and laparoscopic procedures.
intra dayl
Values are expressed as mean + SEM. Pre-induction (pre) and intraoperative (intra)
values are significantly different from values for the first postoperative day (day 1) in
both open and laparoscopic groups. No significant difference was observed between
open and laparoscopic groups.
Discussion
The changes in the fibrinogen levels from the pre-operative values to the higher post-
operative values on Day I is the definitive hnding in this study. Of lesser importance
was changes representing lower fibrinogen levels intraoperatively. The coagulation
status of the patients in this study as measured by the INR, APTT and platelet count
would not be expected to change unless there was some other systemic disease process
present to cause this or a surgical complication. The D-dimer levels would only rise if
substantial venous thrombosis had occurred and Xlinked fibrin degradation products
subsequently released as a result of fibrinolysis.
5
4
c3oo)o^L\'Ë o,€tL¿
1
0
Open
Laparoscop c
pre
-42-
Although significant changes in coagulability over time were demonstrated by
fibrinogen, it is important to emphasize that this measured factor is only one of many
other factors potentially involved in the balance between coagulation and
anticoagulation. Post-operative thrombosis may be associated with procoagulants or
defects such as resistance to activated Protein C or deficiencies ofProtein S,
antithrombin III and lupus-like anticoagulant. The possible importance of these other
indices is relevant, as has been mentioned in the introduction. However they are
frequently difficult to measure and many analyses of such indices remain unvalidated
for routine use and are limited to use only as specific research tools. Furthermore, to
gauge the relative importance of the plethora of interacting factors would require a
study in which each factor was measured and the results subjected to a multivaúate
analysis - a task of such magnitude and expense as to be unrealistic in practical terms.
For these reasons and with these provisos it is appropriate to consider the fibrinogen
results in isolation as markers of variability in coagulability.
Hypercoagulability demonstrated by elevated f,rbrinogen levels after open abdominal
surgery is the rule rather than the exception, and in this respect our results corroborate
available literature(Collins, Jr. et al., 1977 ; Knight et al., 1977 ; Caporale et al., l9S9).
The changes in fibrinogen levels we observed also suggest intraoperative
hypocoagulability during open fundoplication. Early reduction in fibrinogen
concentration has been similarly reported in cardiopulmonary bypass patients within
minutes of introduction of the bypass(Kern et al., 1992).
Fibrinogen alterations have not however, been used as markers for hypercoagulability
or to predict risk of postoperative thrombotic complications amongst patients
-43-
undergoing laparoscopic surgery. This study is the hrst to demonstrate that minimally-
invasive procedures do indeed precipitate elevated postoperative fibrinogen levels, and
corroborates likewise results that had been previously reported using different
coagulation indices following laparoscopic cholecystectomy(Caprini et al., I99l).
Surgical stress, as measured by attenuated metabolic and acute-phase reactants, has
recently been shown to be reduced in laparoscopic compared with open abdominal
surgery(Jakeways et aL,1994). The rise in fibrinogen on day I in both open and
laparoscopic patients in this study suggests that increase in coagulability occurs
regardless of the degree of access trauma. Laparoscopic surgery may therefore not offer
superior protection from the development of thrombosis. Until the incidence and
relative risk of thrombotic complications after laparoscopy is definitively established, it
is suggested that surgeons consider patients undergoing laparoscopic operations as of
equal or possibly higher risk than their open counterparts, and institute prophylaxis
appropriately.
-44-
3.2.3 Thromboembolic risk induced by impaired blood flow in splanchnicvisceralvesse/s
lntroductionReports of fatal small bowel necrosis following uncomplicated laparoscopic operations
on low-risk patients have suggested that insufflation of gas into a patient's abdomen to
provide access for laparoscopic surgery decreases the blood flow to the small bowel and
other vital intra-abdominal organs(Mitchell and Jamieson, 1994; Paul et al., 1994). The
mechanism whereby pneumoperitoneum may change splanchnic visceral blood flow is
not fully understood. Possible theories include some locoregional effect on visceral
vascular beds, alteration in systemic haemodynamic indices, or modification of the
other two factors in Virchow's triad such that thrombosis in visceral vessels is
precipitated
Locoregional effect of pneumoperitoneum on splanchnic visceral vasculature
An indication of the potential effect of laparoscopic insufflation on locoregional
splanchnic vasculature can be gained from analyses of visceral blood flows as a result
of elevated intraabdominal pressure (IAP) during the pre-laparoscopic era(Caldwell and
Ricotta, 1987 ; Diebel et al, 1992). Such studies were undertaken to determine the
sequelae of intraabdominal bleeding, tense ascites, or the application of military anti-
shock trousers to trauma patients. Caldwell and Ricotta studied the effect of elevated
IAP in nine anaesthetised dogs by means of an inflatable plastic bag inserted via a
laparotomy(Caldwell and Ricotta,1987). End-organ flows were determined by the
radioactive microsphere method. At an IAP of 20 mm Hg, there was a significant
decrease in absolute blood flow to the following organs: Oesophagus, stomach, gastric
mucosa, duodenum, jejunum, ileum, colon, pancreas, liver, spleen and renal cortex. In
addition, at an IAP of 40 mm Hg, a significant decrease in absolute blood flow to the
-45-
omentum, gallbladder, and adrenal was also seen. When absolute blood flows were
adjusted for changes in cardiac output, significant falls in blood flow to omentum,
oesophagus, stomach, gastric mucosa, duodenum, and jejunum were still observed at 20
mm Hg pressure. Similarly, pancreas, liver and spleen in addition showed a significant
diminutions of flow at 40 mm Hg pressure. The results of this study clearly
demonstrated that elevated IAP causes a marked decrease in visceral blood flow to most
organs, although at the time the mechanism responsible or clinical importance remained
in question. The advent of routine laparoscopic abdominal surgery has certainly
provided the hitherto quested clinical importance of these discoveries. Findings of
reduced renal tissue perfusion as a consequence of elevated IAP have recently been
independently confirmed in a study where laser Doppler flowmetry was measured
during laparoscopic insuffl ation(Chiu et al., 1994).
In1992, intraperitoneal Ringer's lactate solution was described as an alternative
technique to generated graded increases in IAP. Diebel et al used this method in
anaesthetised pigs to study the effect on hepatic blood flow measured by laser Doppler
flowmetry(Diebel et al., 1992). They showed that with constant normal mean arterial
pressure, hepatic microvascular blood flow fell significantly at 10 mm Hg, and at20
mm Hg wasTlYo of the control value. At 30 and 40 mm Hg pressure, hepatic blood
flow was reduced even more. The authors fail to explain why an apparently
cumbersome methodology was used despite the availability laparoscopic insufflators in
this era, although presumably crystalloid solution more closely mimicked the fluid
likely to be found in traumatised abdomens. The elegance of this methodology in
relation to laparoscopic physiology is that reduced hepatic blood flow with elevated IAP
was demonstrated on a purely mechanical basis as a consequence of increased
-46-

mesenteric vascular resistance, in the absence of the confounding metabolic effects of
CO2. Although not discussed in the manuscript, this is a valuable inference.
There is concern that any locoregional effect of pneumoperitoneum on the splanchnic
circulation may pose a particular risk because of the presence of two susceptible
capillary beds in sequence. Berggren et al have presented evidence to suggest that a
pneumoperitoneal pressure of 25 mm Hg causes the combined effect of increasing
gastrointestinal vascular resistanceby 2l8o/o and hepatic portal vascular resistance by
588%(Berggren et a1.,1993), calculated with the use of invasive mesenteric pressure
monitoring and ultrasound flow probes. The net effect of these changes was to reduce
portal blood flow resultant from vasoconstriction of the gastrointestinal vascular bed
and increased resistance to blood flow across the liver. Ishizaki et al likewise found
reductions in portal venous blood flow and superior mesenteric artery blood flow
measured by Doppler flow probes in dogs undergoing CO2 insufflation at a pressure of
16 mm Hg(Ishizaki et al., 1993b). Two points of interest emerge from this paper. First,
these parameters did not decrease at pneumoperitoneal pressures lower than l6 mm Hg.
Secondly, hepatic artery blood flow was not decreased at any level of IAP, in contrast to
the study by Diebel (Diebel et al., 1992) where increases in intraabdominal pressure
tended to have a more negative impact on hepatic arterial blood flow than on portal
venous flow. In a follow-up paper, the author proposed several locoregional
mechanisms to account for the decrease in splanchnic blood flow due to laparoscopic
insufflation(Ishizaki et al., 1993a). First, a pneumoperitoneal pressure of 16 mm Hg
mechanically compresses splanchnic veins, and according to Poiseuille's Law
-47 -

O _n(Pu - Pr)ra
gV/ where Q: flow and r: radius,
any reduction in the radius of the vessel will decrease blood flow and also increase
resistance in each vascular bed. Second, humorally-mediated vasoconstriction may
occur as a result of peritoneal distention and vasopressin release. Third, compression of
venous outflow and subsequent elevated intravascular pressures could trigger intrinsic
myogenic vasoconstriction of splanchnic vessels.
-48-
Effect of systemic haemodynamics on splanchnic visceral vasculature
Systemic haemodynamic changes have also been investigated in several of these studies
that assessed locoregional splanchnic blood flow. Reduced organ blood flow with
elevated IAP has been observed despite adjustment for changes in cardiac
output(Caldwell and Ricotta, 1987), and has also been documented in the presence of
constant cardiac output(Diebel et al., 1992), decreased cardiac output(Ishizaki et al.,
1993b; Ishizaki et al., 1993a), and increased cardiac output(Devitt et al., 1994 ;
Kashtan et al., 1981). Similar variability in central venous pressures have been recorded
in the face of consistently reduced visceral blood flow. Reduced splanchnic flow with
elevated IAP has been demonstrated in models devoid of the confounding effect of CO2
insufflation on primary cardiac mechanics(Diebel et al., 1992). These studies provide a
weight of evidence to suggest that diminished local splanchnic perfusion is a predictable
and reproducible event when intraabdominal pressure is raised, regardless of the
mechanism used, and irrespective of the variable concurrent systemic physiological
alterations encountered. On the basis of current data it would appear that impaired
visceral blood flow is predominantly affected by the locoregional environment, and
systemic haemodynamics play a minor role in moderated clinical situations. However, it
is acknowledged that the greater diversity of conditions that may be encountered in the
operating theatre as compared with controlled experimental situations may infrequently
yield extreme systemic haemodynamic fluctuations with the potential to influence
splanchnic blood flow more profoundly.
Because of the limited relevance of systemic haemodynamics to visceral
microvasculature in the presence of pneumoperitoneum, an extensive consideration of
the topic is beyond the scope of this work. The subject has been thoroughly
investigated, and sçveral good reviews have been published(Schauer and Schwesinger,
-49-

1995 ; Safran and Orlando,1994). These articles indicate that in contrast to the local
situation in splanchnic vasculature, elevated IAP and CO2 can be identified to
contribute independent effects to systemic haemodynamics. When they act in
combination, as with CO2 pneumoperitoneum, it can become very difficult to separate
the individual contribution of each to the net response. Reduced cardiac output has been
reported to result from the effects of hypercarbia following transperitoneal absorption of
Co2(Safran and orlando, 1994; v/illiams and Murr, 1993 ; Ho et ar., 1992). Although
moderate to severe hypercarbia causes arteriolar dilatation and reduced myocardial
contractility, the overall change in cardiac function is thought to be mediated by the
predominantly ß-adrenergic effect of catecholamine release(Safran and Orlando, 1994).
However mild hypercarbia appears to have little impact on haemodynamic function, and
moderate to severe increases in Pç62 are likely to be mitigated by the actions of the
anaesthetist and artificial ventilation. Cardiac output is also usually independently
reduced by elevated IAP. This results from decreased preload (decreased venous
return), and increased afterload (increased systemic vascular resistance)(Mclaughlin et
a1.,1995). These responses may be modified by the effect of heart rate and contractility
on cardiac output, as well as other secondary factors such as the patient's positioning
and volume status, and cardiac and pulmonary reserves. Obesity and the administration
of different types and doses of anaesthetic agents can also modulate the haemodynamic
response(Schauer and Schwesinger, 1 995).
-50-

Measurement of splanchnic visceral microcirculatory blood flow
Measurement of visceral microcirculatory blood flow has been performed by a number
of different methods. Current evidence suggests the radionuclide-labelled microsphere
technique is particularly suited for measurement of tissue blood flow and appears to be
superior to the "contact" measurements using laser Doppler or tissue implanted
electrical conductance probes(Heymann et al., 1977 ; Kvietys et al., 1998). The latter
method appears to indicate relative flows only. In addition, the indicator dilution
techniques, which are usually reliable, are limited because only one flow measurement
is possible. Using the radioisotope-labelled microsphere technique with appropriate
scintillation counting, it is possible to distinguish gamma emission energies of the
different nuclides such that up to l1 multiple flow measurements are possible under
different conditions during the same experiment.
Microspheres were developed in the late 1960's and consist of spherical particles made
from a biologically inert plastic or resin with a specific gravity slightly greater than
whole blood. The microsphere technique itself is based on the assumption that if the
microspheres are large enough (15 microns) they will mix with, flow with, and
distribute in the same manner as blood. All except those passing through any patent
arteriovenous shunts will be trapped in the tissue of interest during their first passage
through the microvasculature. Assuming that following intra-cardiac administration
such labelled microspheres are completely cleared from the circulation by being trapped
in the capillary bed, and that they are distributed in proportion to the cardiac output,
then the blood flow to any organ (ml min -l; can be calculated using the following
equation:
-51 -

Number of microspheres in target organ
f-)x
:oCtxdt
t.
'Where Ct represents the number of microspheres in a millilitre of arterial blood at time
Experimentally, this type of integration can be performed by mechanically withdrawing
blood at a predetermined rate from a distal point in the arterial system, thus creating an
artificial organ with known blood flow, which then can be compared with that of other
organ of interest.
The tissue flow (Q ) can then be calculated by determining the number of injected
microspheres in the withdrawal arterial sample (ia) the number of microspheres in the
tissue of interest (it) and relating these two values to the rate of withdrawal of arterial
blood (Fa).
itxFa
o: ia
This methodology was first described by Rudolph and Heymann(Rudolph and
Heymann, 1967) has been widely used in previous microvasculature investigations and
found reliable for the measurement of blood flow in all tissues except for portal
flow(Hales,1974). several excellent reviews of this methodology have been
published(Hales, 1994 ; Heymann et al., 1977 ; wagner et al., 1969 ; Hales, 1974), and
prominent in the field is Professor J.R.S. Hales of the University of N.S.W., formerly of
the C.S.I.R.O. in Adelaide.
-52-

In addition to tissue blood flow, the microsphere technique can be applied to the
regional distribution of blood flow in the same organ, total cardiac output, and for
measurement of total circulating blood passing through actual or potential arteriovenous
anastomoses(Hales, 1973 , 1994). The technique is relatively simple, has high degree of
reproducibility, and sources of error are well documented as are the appropriate
mechanisms for avoiding it(Hales,1973; Rudolph and Heymann,lg7l; Hales, 1994 ;
Buckberg et al., l97l).It is important to note that the effect of laparoscopic insufflation
on splanchnic blood flow has not been assessed by this method, despite being
successfully employed to assess the effect of elevated IAP on splanchnic blood flow in
the pre-laparoscopic era(Caldwell and Ricotta, 19S7). Most recent laparoscopic studies
have addressed the broader perspective of liver and mesenteric blood flow in preference
to determining the end-organ flow within the viscera (with the exception of
liver(Hashikura et al,1994) and kidney(Chiu et al., 1994)), and have used
methodologically inferior "contact" measurements.
AimsAn animal study was designed to address the specific question of whether there an
increased risk of thrombo-embolism induced by impaired visceral blood flow during
laparoscopic insufflation. The aim was to determine if there are any discernible
alterations in blood flow to vital intra-abdominal organs (stomach, small and large
bowel, kidneys, and liver) before and after a period of 2 hours of sustained
pneumoperitoneum.
Because this study was designed to be of a pilot nature, a second aim was to elucidate
whether the results supported a definitive investigation including greater numbers in the
study samples, and whether methodological improvements could be incorporated.
-53-

The long-term goal was to provide information to surgeons on any potential deleterious
effects of prolonged pneumoperitoneum, such that conditions which may precipitate
visceral ischaemia and organ dysfunction could be avoided.
The hypothesis (H1) was that a decrease in blood flows to vital visceral organs occurs
during laparoscopic insufflation, and the null hypothesis (H¡) was that there is no
change in organ blood flows during laparoscopic insufflation.
Methods
Domestic white pigs weighing approximately 25 kgwere used as the model for this
pilot study. Eleven animals were studied, the first of which was used for the purpose of
familiarisation with the methodology to be used, and whose results were not included in
the data analysis. The study sample proper comprised 5 experimental animals and 5
control animals, differentiated only by the presence or absence of a two hour period of
laparoscopic gas insufflation. The order of conducting control and experimental studies
was alternated for each pair.
Anaesthesia
Animals were initially sedated using subcutaneous ketamine hydrochloride (10 mg/ml)
given to effect. Anaesthesia was induced using approximately 8 mg of intravenous
pentobarbitone sodium (60 mg/ml) and maintained with an inhalational oxygen/nitrous
oxide mixture, administered by intermittent positive pressure ventilation with a tidal
volume of 15-20 ml/kg. Small top-up doses of approximately I - 2 mg of intravenous
pentobarbitone were additionally administered when necessary.
-54-

Cannulation
Through a left neck incision a polyetþlene catheter was placed into the internal carotid
artery and advanced into the left ventricle for injection of microspheres, and an identical
catheter was placed in the internal jugular vein and advanced into the right atrium for
withdrawal of blood that escaped first-pass capture in the circulation.
Peripheral arterial access was achieved through the right femoral artery for withdrawal
of blood as an artificial organ, and through the left femoral artery for monitoring of
intra-arterial blood pressure (IABP) and heart rate (HR). A Grass Instruments
polygraph, calibrated against a sphygmomanometer, was used primarily to confirm the
siting ofall cannulae by the characteristic changes in pressure transducer recordings.
The traces were subsequently used to continuously monitor IABP and HR to serve as a
visual guide to the haemodynamic stability of the animal throughout the duration of the
experiment.
Core temperature (CT) was measured before and after the period of insufflation by an
oesophageal thermoresistor (Series 700, Yellow Springs Instrument Co., Ohio USA)
displayed on a Tele-Thermometer (Model46, Yellow Springs Instrument Co., ohio
USA). Ambient room temperature (RT) was also recorded at each interval, and the
temperature of the theatre environment was maintained close to 24" C.
After cannulation was complete, the animal was allowed to stabilise for 30 minutes,
during which period the microspheres were prepared for injection.
-55-

Preparation of microspheres
Standard sampleA standard sample representing the number of radioactive counts per microsphere was
generated for each experiment as follows: A dilute suspension of microspheres was
prepared and placed on a hlter paper premarked with a grid pattem. The microspheres
were accurately counted using a microscope and placed in a sealed tube to be counted
with specimens from each experiment.
Dose of microspheresThe volume of the microspheres to be injected was calculated knowing the total activity
of the stock supplied, the activity per gram of the microspheres and the number of
microspheres per gram. The drawn up dose in the injection chamber was counted both
before and after the experiment and the resulting counts were compared with that of the
accurately counted spheres in the standard sample to obtain the exact number of spheres
in the injection dose. These measurements were done using an activated iodide crystal
coupled to a gamma spectrometer (biogamma TH Beckman Instruments).
lniectionBefore drawing up the injection dose, the stock supply was thoroughly mixed using a
vortex mixer and the required volume of the mixture was drawn up into the container
using a I ml syringe. This syringe was then replaced with one containing saline. The
spheres were then kept mixed by continual agitation of the injection chamber and the
infusion into the left ventricle began 15 seconds after the start of the withdrawal of the
reference sample. The dose of microspheres was given over 30 seconds and the
reference sample withdrawal continued for another 30 seconds after this.
-56-
Baseline measurement of organ blood flows
Approximately 0.5 x 106 15 micron sized microspheres kg-l of body weight (suspended
in l}Yo Dextran and 0.01% Tween) were then injected in the left ventricle using an
injection chamber. Strontiumss and Ceriumtot lab.ll"d microspheres with specific
activities in an approximate rutio of 2:1 or 3:l were used to measure baseline and post-
insufflation organ blood flows respectively, with the order of administration of the
differently-labelled nuclides alternated for each control/experimental pair.
It was only possible to determine cardiac output in the first two pairs of animals.
Because of the subsequent unavailability of a gamma counter that covered high KV's
and high doses due to equipment failure in another Department, it was necessary for the
counting of all subsequent samples to be undertaken using a particularly sensitive
gamma counter. As the methodology dictated cardiac output be calculated by relating
the total number of microspheres injected with the total number of microspheres in the
arterial withdrawal sample, energy yields in such samples simply overwhelmed the
g¿ìmma counter available.
lnsufflation
Insufflation of CO2 into the abdominal cavity was established in experimental animals
by means of a 5mm umbilical port using a LINS-1000 insufflator (Cook Medical
Technology, Qld) to maintain a sustained pneumoperitoneal pressure of 12 mm Hg over
a period of two hours. This step was omitted for control animals, which were
maintained under anaesthesia with no other intervention for this two hour period.
-57 -

Post-insufflation measurement of organ blood flows
After the two hour period had elapsed, blood flow estimations using the radiolabelled
microsphere method were repeated. Insufflation was then stopped, and intra-peritoneal
pressure was released completely.
Sacrifice and organ haruest
The experiment was then immediately concluded and the animal was killed by an
intravenous overdose of pentobarbitone. organ samples comprising 1.5 - 2.5 g of
abdominal viscera (small bowel, large bowel, liver, and kidneys) were placed in 3
preweighed vials which conformed with the counting equipment geometry. These were
sealed and reweighed, and their radioactivity determined using a Canberra multichannel
analyser adjusted to cover the main energy peaks of the various tracers, with the
assistance of a Maestro computer program. The blood from the femoral reference
sample was also placed into preweighed tubes and reweighed (to work out the
withdrawal rate) and then taken for counting of radioactivity with the other samples and
standards. The right atrial (pulmonary) blood withdrawn was also measured to provide
an approximation of microspheres that escaped first-pass capture in the circulation, with
the assumption that bronchial blood flow did not change significantly.
The intestinal mucosal blood flow as well as the renal cortical and medullary blood flow
were studied by separately counting of previously separated gut mucosa as well as
medullary and cortical elements of the kidney. Multiple specimens of each organ were
obtained in an attempt to reduce sampling elror, and the counts pooled for each organ
before statistical analysis.
-58-

Ethical implications
As the animals were anaesthetised before the placement of catheters and induction of
pneumoperitoneum, and killed before the completion of anaesthesia, the experiment
resulted in no pain to the animals. No special housing of the animals was required
preoperatively.
Approval was granted from the Radiation Safety Officer of The Queen Elizabeth
Hospital, from the Animal Ethics Committee of The Queen Elizabeth Hospital (N-15-
94), and from the Animal Ethics Committee of The University of Adelaide (M73194).
Sfafrsfica/ analysis
Statistical analysis was performed using repeated measures analysis of variance,
applying a between-subject factor according to group (control, or experimental animal)
and a within-subject factor of time (before, or after insufflation). Analysis was
performed using SPSS for Windows 6.1 statistical software (Chicago), with
significance defined as a probability level of 0.05.
As the null hypothesis was applied to each variable a priori, it was considered that each
variable represented an independent entity, and professional statistical advice indicated
that adjustments for multiple comparisons with a control were therefore unnecessary.
Repeated measures analysis of variance analyses were repeated applying a second
within-subject factor being the order in which Cerium or Strontium microspheres were
injected (i.e. Cerium for before insufflation measurements and Strontium for after
insufflation measurements, and vice-versa).
This study was designed to be of a pilot nature because of the time and expense incurred
by using radiolabelled microsphere methodology to measure microcirculature, and
-59-

ethical responsibilities to limit the number of animals to the minimum required to
answer the hypothesis. However it was possible to determine the number of pigs
required in each group for a subsequent definitive study of visceral blood flow using the
microsphere method by a statistical calculation using the following equation (for given
power against a specified difference(Armitage and Berry, 1994)):
2
n>2
Where n represents the number of experimental subjects required, and z2orepresents the
standardised normal deviate with probability 2a (for 2a: 0.05, z2o:1.96). p represents
Type II error, therefore at80Yo power I - Ê : 0.2 andz2p:0.842. o represents the
known standard deviation from observed results in the pilot study, and õ1 represents the
specified mean difference in blood flow between control and experimental animals.
-60-

Results
Table 3 shows the microvascular blood flow rates in control and experimental animals
before and after insufflation. Thep values are the results of the repeated measures
analysis of variance, and indicate that for all but one organ there were no significant
differences between the before and after flows in control compared with experimental
animals. The right lobe of the liver was the only organ in which a significant fall in
blood flow could be detected after laparoscopic insufflation.
There were no significant inequalities in variance between control and experimental
sample populations in all of the measured variables shown in Table 3.
Statistical results indicated there was a significantly lower ambient room temperature in
experimental pigs at the time post-insufflation blood flows were measured (p < 0.001).
However, the magnitude of the 0.6' C difference (24.20" C compared with 23.60" C)
was not considered clinically signif,rcant, and fuithermore did not influence the animals'
core temperatures, which were not significantly different at the time of before and after
flow measurements in control compared with experimental animals.
In the two pairs of pigs where cardiac output results were able to be incorporated in the
repeated measures analysis of variance, there was no significant difference between the
outputs before and after insufflation in control compared with experimental animals,
with an observed power of 50%o at the 0.05 level. IABP and HR remained stable under
experimental conditions in all animals. Mean blood pressure was 120196 for control
animals, and 118/86 for experimental animals, and this difference was not significant.
Creation and deflation of a 12 mm Hg tension pneumoperitoneum both caused
transitory elevations in systolic and diastolic blood pressure which reverted back to
normal levels very quickly. No sustained blood pressure alterations were induced by
-61 -

changes insufflation or desufflation, making analysis of these haemodynamic effects
meaningless.
There was also no significant difference between the total number of microspheres
injected before and after insufflation in control compared with experimental animals,
and good mixing with systemic cardiac outflow was confirmed by consistent clustering
of raw counts in kidney samples. The alternating order in which the two radionuclides
(Cerium or Strontium) were administered appeared to have no significant bearing on the
results of before and after organ flows in control compared with experimental animals
for the measured variables. Microspheres retrieved from venous withdrawal from the
right atrium represent those that have escaped first-pass capture in the circulation. The
number of microspheres withdrawn after f,rrst injections were on average 2.7 x l}-a of
the dose, and after second injections were only 3.5 x 10-s of the dose, eliminating this
potential source of error.
On the basis of observed results in this pilot study, and using the equation shown in the
Statistical analysis section of the Methods, it was determined that a minimum of 12 pigs
would be required in each of the control and experimental groups for a dehnitive study
of small bowel blood flow using the microsphere method. Mid-small-bowel (whole)
was chosen as the key variable to provide a standard deviation (o) of l3 mls/min. A
two-sided significance level (24) of 0.05 was used and a power of 80% was required
against a specified mean difference (õ1) of 15 mls/min. This specified mean difference
between mid-small-bowel blood flow in control and experimental pigs was chosen as it
represents roughly a 50Yo reduction in total flow (see Table 3).
-62-

Table 3: Mean microvascular blood flow rates (mls/min/100g tissue) for vital intra-abdominal organs before and after laparoscopic insufflation
CONTROL
VARIABLE
Caecum
Ileum mucosa
Ileum whole
Jejunum mucosa
Jejunum whole
Left kidney
Left kidney cortex
Left kidney medulla
Left lobe liver
Mid-small-bowelmucosa
Mid-small-bowelwhole
Right kidney
Right kidney cortex
Right kidney medulla
Right lobe liver
Rectum
Transverse colon
BEFORE AFTER
30.00 36.33
36.80 63.20
2t.13 41.13
35.00 41.60
26.40 32.20
166.00 229.80
236.80 3s3.60
24.80 16.40
49.80 82.00
32.20 37.00
p
0.66
0.25
0.17
0.38
0.84
0.s4
0.36
0.69
0.075
0.16
23.s3 29.93
154.60 217.60
220.00 324.80
33.20 28.40
59.60 93.80
9.75 12.75
24.00 11.00
0.64
0.s3
0.5
0.96
0.046
0.62
0.56
EXPERIMENTAL
BEFORE
34.46
30.97
24.4r
37.77
3r.52
208.1 8
217.74
44.25
56.0s
43.50
AFTER
48.96
30.39
24.39
34.50
35.34
247.00
272.90
33.26
45.7s
34.25
34.01 35.81
168.00
207.79
50.28
5t.54
2r.85
37.90
202.64
269.77
44.96
32.42
20.28
40.45
-63-
Discussion
Anecdotal reports of fatal small bowel necrosis following uncomplicated laparoscopic
operations on otherwise healthy patients have recently emerged(Mitchell and Jamieson,
1994 ; Paul et a1.,1994). There is concem that such complications may comprise part of
a spectrum of an increased thromboembolic risk posed by laparoscopic surgery, in
particular by affecting blood flow in splanchnic visceral vessels. However at present the
scientihc evidence to support such conjecture is limited to four published studies. Three
of these studies measured blood flow changes at the mesenteric level, rather than
microvascular flow in the specific organs at risk(Berggren et al., 1993 ; Ishizaki et al.,
I993b; Ishizaki et al., 1993a). Diminished splanchnic perfusion at high insufflation
presswes (> 16 mm Hg) appears to be a reproducible finding. The only study to assess
the effect of laparoscopic insufflation at an end-organ level focused only on perfusion
changes in renal tissue(Chiu et al., 1994). At moderate intraabdominal insufflation
pressures (I5 - 20 mm Hg) renal cortical blood flow was approximately doubled, and
renal medullary blood flow approximately halved.
The study herein contrasts with these existing works by concentrating investigation
predominantly on the end-organs responsible for the published episodes of fatal
intestinal ischaemia, namely the small and large bowel, and assessing respective blood
flow distribution at the tissue level. Furthermore, the microsphere methodology used is
well-established as a highly accurate and reproducible technique, and is superior to the
"contact" flow measurement methods (such as Doppler) employed in the few available
laparoscopic studies (see Introduction - Measurement of visceral microcirculatory blood
flow). The results of this study corroborate the reliability of the microsphere
methodology. At the two measurement intervals, no significant differences were
-64-

detected between control and experimental animals in terms of the statistical variance of
flows for each organ, the total number of microspheres injected, the order of
radionuclide injection, or the mixing ability of microspheres with the systemic
circulation. Unrelated to the microsphere technique, but also pertinent to the soundness
of the methodology used was absence of any observable difference in haemodynamic
parameters (cardiac output, IABP or HR) between study groups.
Scrutiny must also be directed towards circumstances that conspired to generate
methodological flaws, for two reasons. The scientific evidence subsequently produced
must therefore be considered conditional, and the identification of methodological
problems answered the second aim of this pilot study which was to allow for
improvements in a future definitive investigation.
Attempts to calculate the power of the study a priori werc rendered impossible by the
absence of biological standards for porcine organ flows, with the result that when the
observed po\¡/er at the 0.05 level for each measured variable was calculat ed, post hoc, it
\À/as generally below 50%. This indicated that there was only a low chance of registering
signif,rcant differences between measured variables from the control and experimental
populations due to inadequate sample sizes.
Furthermore, due to logistical problems it was not possible to control for changes in
cardiac output in the last 3 pairs of pigs, and endeavors to perform cardiac output
determinations using 7F thermodilution catheters were unfortunately also unsuccessful
due to the small size of the pigs and anatomic variation from humans.
Hales has shown using microsphere techniques that if an animal's ambient environment
is changed from being thermoneutral, cardiac output is redistributed while its absolute
-65-

level remained unchanged(Hales, 1994).It is for this reason that the observed mismatch
in room temperature over time between control and experimental groups is of concem,
and occurred despite airconditioned operating room facilities with ambient temperatures
thermostatically controlled close to 24 C. Fortunately the magnitude of the difference
was clinically insignificant, and did not effect the animals core temperature.
The only other recognised methodological shortcoming was the potential for
intermittent intravenous pentobarbitone anaesthesia to become inadequate, and the
requirement for repeated top-up doses could have made between-subject standardisation
difficult. This problem was fortunately not experienced, however it is acknowledged
that pentobarbitone administration by intravenous infusion would be superior.
Additionally, digital rather than analogue monitoring equipment would also have
facilitated more accurate data recording.
The evidence emanating from this pilot study implies that atwo hour period of
laparoscopic insufflation results in a significant decrease in blood flow to tissue in the
right lobe of the liver, even at the relatively modest pneumoperitoneal pressure of 12
mm Hg. However, fuither evidence suggests that a definitive study of this nature would
require at least l2 pigs in each group, assuming a clinically significant change would be
represented by a 50%o reduction in pre-insufflation blood flow rates to mid-small-bowel.
Because of statistical indications that there was a high likelihood our results were
confounded by Type II error, to accept the results of this pilot study that laparoscopic
insufflation does not diminish blood flow to the tissues of other vital intraabdominal
organs would be at the risk of falsely rejecting the hypothesis (H1). The results in Table
3 show a trend indicating that blood flow in many organs fell after the insufflation
-66-
period, and with a larger study population it is possible that these changes may become
signif,rcant.
In light of all the information assimilated from this study, it is impossible to make a
judgement on the validity of the hypothesis that laparoscopic insufflation may impair
visceral blood flow and contribute to thromboembolic events in the vessels of
intraabdominal organs. The weight of existing evidence (see Introduction, Impaired
blood flow in splanchnic visceral vessels) supports the theory that diminished
splanchnic perfusion is a reproducible event when IAP is raised from any cause -
laparoscopic or otherwise.
It is concluded that proof of decreased blood flow at the tissue level in the setting of
laparoscopic abdominal surgery remains to be established. A definitive investigation to
assimilate such evidence would be feasible using the microsphere technique, if at least
12 pigs were studied in each group. The methodology of such a project should
incorporate cardiac output determinations in all animals, an experimental environment
of controlled ambient temperature, maintenance anaesthesia by intravenous
pentobarbitone infusion, and continuous digital data recording.
-67 -

3.2.4 Thromboembolic risk induced by impaired blood flow in lower /imb yesse/s
Femoral venous stasis during laparoscopic surgery occurs as a result of several separate
but cumulative mechanisms; diminished blood clearance rate from the legs by reduced
femoral venous velocity resultant from the loss of the normal calf muscle pump from
immobility and neuromuscular blockade, calf dilatation during induction of general
anaesthesia(Coleridge Smith et al., 1990), reverse Trendelenburg positioning(Arcelus et
a1.,1993), and the creation of a tension pneumoperitoneum(Jorgensen et al., 1994).
Operative venodilation yielding diminished capacitance has been confirmed to occur in
at least two separate studies during open surgery. Coleridge-Smith studied changes in
calf vein diameter using high resolution ultrasound in 62 patients undergoing a range of
General Surgical procedures(Coleridge Smith et al., 1990). Significant venous
distention of between 22% - 28Yo was observed by the end of the procedure,
accentuated by dependent positioning (37%) and intravenous fluid administration
(48%), as would be the case during laparoscopic operations. Their data was interpreted
to show that as venous diameter increases during the operation, the ability to further
increase in response to a rise in venous pressure is reduced. Venous distention during
anaesthesia has been shown to occur in the upper limbs during the course of surgical
procedures(Comerota et a1.,1989). Dilatation in excess of 20%o was shown to correlate
with the risk of postoperative radiofibrinogen-detectable DVT. Venodilation has also
been demonstrated during laparoscopic cholecystectomy(Jorgenson et al., 1 994). Six
patients were studied by Jorgenson et al using Doppler ultrasound after creation of a
l2mmHg pneumoperitoneum. A significant increase in mean common femoral vein
diameter of 30%o was observed.
-68-
Reverse Trendeleburg positioning of 30" - 45" head up not only accentuates
intraoperative increases in venous diameter and cross-sectional area(Coleridge Smith et
a1.,1990; Arcelus et al., 1993) but also diminishes blood clearance rate from the legs
by reducing femoral venous velocity. In a study on 5 pigs undergoing laparoscopic
Nissen Fundoplication, an ultrasound flow probe applied to the femoral vein
demonstrated a reduction in femoral venous outflow during reverse Trendelenburg
position for any given intraabdominal pressure(Jorgensen et al., 1994).
Reduced linear blood flow velocity from lower limb veins during open surgery has been
confirmed using thermodilution probes, radioisotopic NaCl2a measurement,
phlebography, and Doppler ultrasonography(Millard et al.,1993). This occurs as a
result of the abolition of the soleal calf muscle pump during the immobility and muscle
relaxation inherent in general anaesthesia. In the anaesthetised patient, venous return
from the legs therefore depends predominantly on the pressrre gradient between the
venules (12-18 mm Hg) and the right atrium (4-5 mm Hg). The introduction of an
additional pressure barrier between these sites such as a15-20 mm Hg
pneumoperitoneum could be expected to further reduce venous retum. This has been
conf,rrmed by a number of studies assessing femoral venous pressure, peak blood
velocity, venous pulsatility, and venous flow measurements.
Beebe et al examined the common femoral veins of 8 patients undergoing laparoscopic
cholecystectomy using duplex ultrasound and invasive venous pressure
monitoring(Beebe et al., 1993). Compared with preoperative measurements, a 14 mm
Hg pneumoperitoneum resulted in a significant increase in femoral venous pressure and
a significant reduction in peak blood flow velocity, as well as reducing or eliminating
-69-

pulsatility in75Yo of patients indicating partial proximal venous obstruction. These
changes were maintained during the entire period of insufflation, but were restored to
preoperative levels upon deflation. It was concluded that abdominal insufflation causes
venous stasis during laparoscopic cholecystectomy.
Millard et al studied the combination of pneumoperitoneal insufflation at 13- l5 mm Hg
and 30o reverse Trendelenburg tilt during laparoscopic cholecystectomy in 20
patients(Millard et al., 1993). They measured peak femoral blood flow velocity using
ultrasound, and also investigated the effect of intermittent pneumatic compression. A
significant 42Yo decrease in peak blood flow velocity was observed, and intermittent
pneumatic compression reversed that effect, returning blood flow velocity to normal.
Jorgensen et al also studied the effects of insufflation during laparoscopic
cholecystectomy(Jorgenson et a1.,1994). They measured femoral blood flow velocity
using ultrasound, however at a pneumoperitoneal pressure of 12 mm Hg. The effects of
intermittent pneumatic compression and intermittent electric calf stimulators were also
investigated. Their study againconfirmed that intraoperative venous stasis was
significantly increased by the presence of a pneumoperitoneum, additional to any
decrease resulting from general anaesthesia. Although both intermittent pneumatic
compression and intermittent electric calf stimulation increased peak venous blood flow
velocity during general anaesthesia, with a pneumoperitoneum in place neither device
was able to retum the depressed blood flow velocity to the values recorded without a
pneumoperitoneum, in contrast to the f,rndings by Millard et al(Millard et al., 1993).
The influence of a third intraoperative prophylactic modality against venous stasis;
graduated compression stockings (TED, Kendall), was investigated by V/ilson et al in a
-70-
randomised study of 40 patients undergoing laparoscopic cholecystectomy at
pneumoperitoneal pressures of 15 mm Hg with 20" of reverse Trendelenburg
tilt(Wilson et al., 1994). Venous occlusion plethysmography was used to monitor
venous outflow. In the 20 patients not wearing stockings, venous outflow fell in 65Yo of
patients, returning to normal once pneumoperitoneum was released. In the group
wearing stockings, these changes were abolished in90o/o of patients. The only
significant result was the observation that at mid-operation median venous outflow was
significant less in the group not wearing stockings.
These studies provide strong evidence to suggest that independent of all other risk
factors, creation of a laparoscopic pneumoperitoneum leads to an increased chance of
thromboembolism by impairing lower limb venous flow beyond that resultant from the
loss of the normal calf muscle pump during general anaesthesia. This has prompted
investigation into the most appropriate thromboprophylactic measures to meet this new
challenge.
It must be stated that in all of these studies the pneumoperitoneal stimulus was not
controlled for by an equivalent non-insufflated group. In the studies by Millard(Millard
et al., 1993) and V/ilson(Wilson et al., 1994) it is impossible to isolate the individual
contribution of the coincident pneumoperitoneum and reverse Trendelenburg tilt.
In the study by V/ilson(Wilson et al., 1994) median venous outflow during surgery was
significantly better in patients wearing TED stockings that those who were not, but
whether this flow benefit in the stockinged group is significantly better than pre-
insufflation levels remains unresolved. Jorgensen(Jorgenson et al., 1994) has shown that
intermittent electric calf stimulators do not appear to be an effective deterrent against
-71 -

venous stasis during laparoscopy, and the evidence determining the benefit of
intermittent pneumatic compression is conflicting.
Furthermore blood velocity, not flow was the parameter measured in the studies
utilising ultrasound, and many vascular surgeons believe that the objectivity of venous
Doppler is compromised by the inherent interobserver variation and error, and propose
that thermodilution flow measurements should remain as the gold standard
investigation.
3.2.5 Thromboembolic risk induced by yesse/ wall abnormalitiesEndothelial damage during laparoscopic surgery is an unresolved issue, but it has been
suggested that venous dilatation may cause endothelial cracking that is followed by
exposure of subendothelial collagen, platelet adhesion, and activation of the coagulation
cascade(Schaub et a1.,1978; Comerota et a1.,1989). The site of endothelial damage
then acts as a nidus for thrombosis formation in the veins.
3.2.6 Summary of net thromboembolic risk during laparoscopyIn light of the introductory and experimental evidence presented, it is appropriate to
now review the net thromboembolic risk posed by laparoscopic surgery. There is
currently no definitive clinical evidence of the absolute degree of risk, but anecdotal
reports of disastrous thromboembolic complications have caused great concem and
awareness of the problem. Experimentally, postoperative hypercoagulability has been
proven, impaired blood flow in lower limb vessels has also been proven, and impaired
blood flow in visceral vessels appears likely on previous evidence in spite of the failure
of the study herein to ascribe a significant to the effect of CO2 insufflation. The final
element in Virchow's triad, vessel wall abnormalities, ¿ìre unproven during laparoscopic
surgery, but theories of endothelial damage are plausible.
-72-
In summary, laparoscopy is certainly not minimally-invasive in terms of the
development of postoperative thrombosis. In fact, laparoscopy may well negatively
influence all 3 elements of Virchow's triad, sometimes beyond that of open surgery, and
possibly result in a cumulatively greater risk for the development of venous
thromboembolism.
3.2.7 Thromoembolism prophylaxis for laparoscopyThis risk can be minimized by addressing each component of Virchow's triad in turn.
Hypercoagulability can be safely prevented by unfractionated low-dose subcutaneous
heparin or low-molecular weight heparin(Collins et al., 1988 ; Lassen et a1.,1991),
whereas dextran and oral anti-coagulants are now rarely used as prophylactic measures
in General Surgical patients. Venous stasis in lower limbs can be overcome using
physical methods such as graduated compression stockings (TED@, Kendall), or the
sequential pneumatic compression device (Kendall). Both have been shown to be
effective in significantly improving femoral venous blood flow (see Section 3.2.4
Thromboembolic risk induced by impaired blood flow in lower limb vessels). It is
important to note that electrical calf stimulators have not been proven to be an effective
deterrent against venous stasis during laparoscopy. Impaired blood flow in visceral
vessels and venodilation are both caused by elevated IAP, and can be prevented by
keeping insufflation pressures to < 16 mm Hg. The problem of elevated IAP can be
completely abolished by the use of gasless laparoscopy, and this may become ultimately
the safest option.
On present evidence, the recommendation is to tailor these prophylactic options
according to the patient's disease and degree of risk. This is facilitated by including a
risk factor assessment sheet in the preoperative workup of all laparoscopy patients. A
-73 -
prototype form has been designed by Caprini, whereby patients are stratified into low,
moderate, or high risk on a number of designated criteria(Caprini and Arcelus, 1994).
For low risk patients, early ambulation is encouraged and graduated compression
stockings are reconìmended. For moderate risk patients, either conventional low-dose
heparin, or a combination of graduated compression stockings with a sequential
pneumatic compression device should be used. For high risk patients, a combination of
heparin, a sequential pneumatic compression device as well as graduated compression
stockings are recommended.
Caprini also makes the point that because laparoscopic patients get discharged early, it
is advisable that patients wear their graduated compression stockings at home for at
least four weeks(Caprini and Arcelus, 1994). Regardless of risk, all patients should have
insufflation pressures kept below 16 mm Hg, and for very-high risk patients the use of
gasless laparoscopy should be considered.
Gasless laparoscopy is simply the use of retractor systems that permit laparoscopic
exposure without the creation of a pneumoperitoneum. Many technological devices
have been invented, most of which are attached to a winch and 'Goligher'-type
framework above the patient's chest.
The simplest systems use T-bar or U-shaped retractors inserted into the peritoneal
cavity, usually around the falciform ligament, to provide an isolated area of lift which
enhances the exposure provided by pneumoperitoneum(Gazayetli, I99l ; Kitano et al.,
1992).Insufflation pressures can therefore be kept very low in these cases. Other
authors have described a technique that uses long surgical wires placed into the
subcutaneous tissue of the anterior abdominal wall(Nagai et al., 1991). An Australian-
-74-
developed system now offers what look like intraperitoneal coathangers to elevate the
anterior abdominal wall. However the most advanced system is the planar lift
device(Smith et al., 1993). V/ith this system an expandable fan-shaped retractor is
positioned in the peritoneal cavity via a 2 - 3 cm periumbilical incision, and attached to
an electrically-powered 'lift' fixed to the side rail of the table. In obese patients further
exposure can be provided by the use of a second retractor.
The major advantage of gasless laparoscopy is that it abolishes the requirement for
elevated IAP and by so doing diminishes the risk of thromboembolism. Other
advantages are also apparent. Because there is no need to maintain an airtight seal,
incisions or valveless ports can be used instead of conventional sealed trocars. This type
of access permits considerably more degrees of freedom for instrument
maneuverability, which is ergonomically desirable, and allows a wider range of
instruments to be used, even conventional needle-holders and the like.
The disadvantages of gasless laparoscopy are that some of these devices require
additional small incisions and may potentiate more pain. Device assembly can
sometimes be complicated, and the operative exposure is somewhat different to that
provided by CO2 insufflation. Whereas the distention provided by pneumoperitoneum is
dome-shaped, the exposure provided by a retractor is like a truncated pyramid, and is
generally limited to a specific quadrant of the abdomen.
-75 -
4. DEVELOPMENT AND EVALUATION OF NEW APPLICATIONS IN
LAPAROSCOPIC GASTROINTESTINAL SURGERY
4.1 Oesophagectomy
4.1.1 lntroductionThe invasiveness of conventional techniques of oesophagectomy entail a significant
morbidity and mortality rate in oesophageal cancer patients who have an increased
operative risk because of their age, depressed pulmonary function, portal hypertension,
and nutritional deficiencies(Earlam and Cunha-Melo, 19S0). Open oesophagectomy
without thoracotomy (blunt transhiatal oesophagectomy) has been advocated to reduce
the morbidity associated with an abdomino-thoracic approach to
oesophagectomy(orringer and Sloan, 1978). However, the proposed theoretical
advantages have not been demonstrated(Goldminc et al., 1993 ; Siewert et al., 1986).
Disadvantages to blunt transhiatal oesophagectomy have been reported however, and
include significant intraoperative blood loss, trauma to the azygos vein, trauma to the
bronchial tree, lesions of the recurrent laryngeal nerves, and cardiac arrythmias. In
addition, curative resection (if feasible) is impaired because nodal dissection is
impossible, and there is a significarfi (4%to 9%) conversion rate to thoracotomy
because of adherence to mediastinal structures(Goldminc et al., 1993 ; Orringer, 1984).
A minimally-invasive approach to the intrathoracic oesophagus is considered to be an
evolving solution by overcoming the disadvantages of blunt transhiatal oesophagectomy
whilst retaining the advantages conferred by avoidance of a thoracotomy. The ability to
perform radical node dissections and curative en-bloc resections under direct vision
without thoracotomy is a major advantage of this technique, and could lead to improved
survival(Goldminc et al., 1993 ; Akiyama et al., 19S4).
-76-

Perivisceral oesoohaoectomvA spectrum of endosurgical techniques for oesophagectomy have been reported over the
last six years, however no one method has become standard(Buess, l99l ; Leahy et al.,
1990 ; Gossot et al., 1992; Buess, 1992; Dallemagne et al., 1923 ; Cuschieri, 1993).
The first published technique for minimally-invasive oesophagectomy was described in
1989 by Kipfmuller et al(Kipfmuller et al., 1989), and described as "Endoscopic
Microsurgical Dissection of the Oesophagus (EMDE)". Subsequently this procedure has
become known as "Perivisceral (Endoscopic) oesophagectomy". The oesophagus is
approached with a bulbous-tipped operating mediastinoscope inserted via a cervical
incision anterior to the left sternomastoid muscle, taking care not to damage the vagus
or recurrent laryngeal nerves. The perioesophageal tissues are exposed for dissection by
mechanical dilatation of the space in front of the instrument, and this avoids the
requirement for pneumatic dilatation of the posterior mediastinum (as would be
required for a thoracoscopic dissection).
An operating mediastinoscope was specifically-designed to enable this novel surgical
technique to be performed. A rigid cold-light fiberoptic endoscope fits inside an outer
sheath which has an integrated aspiration and inigation system. The distal end of the
outer sheath is bell-shaped and enlarged, and has been more recently modified to
incorporate an indentation to centre the instrument over the oesophagus(Becker et al.,
1993). The top of the distal end of the outer sheath with aspiration openings is flattened
to reduce the risk of damage to the membranous trachea. The outer sheath has an 8mm
working channel down which can be passed instruments enabling dissection,
coagulation, irrigation and aspiration. To reduce the rate of instrument changes, an 8mm
continuous suction probe has been developed. The tip of the probe allows monopolar
-77 -

electrocautery, and another central channel permits the passage of 5mm endoscopic
scissors. If the scissors are withdrawn slightly back into the central channel, the suction
that has been applied is allowed to take effect and aspirate any fluid in front of the probe
without a change of instruments. The internal rigid endoscope has a 10" obliquely offset
eyepiece which can be connected to a laparoscopic video camera, thereby allowing
circumferential dissection of the thoracic oesophagus under two to four times magnified
vision. This allows a close up view of the wall of the oesophagus and blood vessels
entering the oesophagus which can then be safely coagulated or clipped, and then
divided under direct vision. This is in contrast to the blunt transhiatal oesophagectomy
technique which frequently results in uncontrolled rupture of these vessels and is
associated with bleeding into the mediastinum which in many cases leads to respiratory
morbidity and mortality.
The oesopheageal dissection is carried downwards to the hiatus in a circumferential
fashion using the longitudinal muscle fibres of the oesophagus as a guide. When the
abdominal cavity is reached, a laparotomy is performed and the stomach is prepared as
the neo-oesophagus (a second abdominal team can perform this concurrently if desired).
A nasogastric tube is passed up through the hiatus, grasped by forceps passed down
through the operating mediastinoscope, and retracted out of the cervical incision. The
cervical oesophagus is then divided by a linear stapler, after which the cranial end of the
nasogastric tube is attached to distal margin of division. Traction then extracts the
oesophagus downwards into the abdomen, followed by operating mediastinoscope to
divide any remaining attachments. The gastric tube to be used for the oesophageal
replacement is brought upward to the neck under endoscopic control, and a two layer
hand-sewn cervical anastomosis completes the reconstruction. The operative technique
-78-
has undergone minor revisions since initially described, and has been reported in some
detail in a recent publication(Manncke et al., I994b).
This work was initially described in an animal model. Cardiopulmonary parameters
(heart rate, arterial blood pressure and PaO2) were reported to be significantly less
depressed during and after EMDE in comparison with abdominothoracic and blunt
transhiatal oesophagectomy(Kipfmuller et al., 1990). The first report of use of this
technique in humans appeared in 1990, published by Buess and Becker from Tübingen
in Germany(Buess and Becker, 1990). The first patient was operated on in September
1989, and by May 1990 six men and one woman with Tl to T3 tumours had been
operated on. Blood loss was under 100 mls for all patients, and the operation time was
between three and four hours. No intra- or post-operative problems were reported. By
october of the same year their experience had increased to 17 unselected
patients(Buess, 1991). The mean operation time in this series was 205 minutes and the
mortality was 5.9o/o. Average intra-operative blood loss was less than 200 mls and the
respiratory morbidity rate was low. The most recent results from the Tübingen group
were documented in 1993(Becker et aI,1993). The authors had performed the
procedure in 31 patients by that time. The majority of the patients had middle third
tumours, and T3 lesions predominated. Mediastinal blood loss was still less than 200
mls, but mean total duration of the operation had decreased to 186 minutes, with a mean
time for the mediastinoscopic procedure of 61 minutes. The conversion rate to
thoracotomy was 6%io, and the post-operative mortality rate was 6.4%. The only
complication attributable to the to the mediastinoscopic technique was recurrent
laryngeal nerve palsy in one patient. Thirteen of the 29 surviving patients experienced
-79-
minor pulmonary complications. Postoperative radiographic contrast studies showed
minor anastomotic insufficiency in 6 patients, 4 of which were subclinical.
Two subsequent studies have been published by Siewert's group in Munich describing
uncontrolled prospective series(Bumm et a1.,1993; Bumm and Siewert,l994).In their
experience with 57 patients where the perivisceral endoscopic oesophagectomy
technique was applied, a 30-day mortality rate of 5.3o/owas observed, with no fatalities
related to the perivisceral dissection. A steep learning curye for the procedure was of
some note, operation time decreasing sharply during the study period, and 3
oesophageal injuries occurring during perivisceral dissection in the initial phase(Bumm
and Siewert,1994).In a separately published study including a subset of 30 of the same
patients, perivisceral oesophagectomy was compared with transhiatal oesophagectomy
in a matched case-control study(Bumm et aI.,1993). Mortality was similar in both
groups (6.6%vs.I3.3Yo respectively), but importantly pulmonary complications were
significantly less severe in the perivisceral group. The risk of injury to the recurrent
laryngeal nerve with the open technique was reportedly reduced by the perivisceral
oesophagectomy technique, and in the opinion of the authors, this played an important
role in postoperative pulmonary rehabilitation by preventing "silent" aspiration.
Although further evaluation of this method is required, these initial reports suggest that
the perivisceral technique is associated with reduced blood loss and a more controlled
dissection of the oesophagus, with especially good results achieved with small distal
tumours, particularly adenocarcinomas. It is possible that a significant reduction in the
pulmonary morbidity and corresponding mortality of oesophagectomy will be
forthcoming.
-80-
Thoracoscopic oesophagectomyAlthough unproven, it can reasonably be anticipated that thoracoscopic oesophageal
resection will offer similar benefits of improved postoperative respiratory function,
early discharge from the Intensive Care Unit, reduced postoperative pain, and
diminished risk to intrathoracic structures. In addition, thoracoscopic dissection has the
advantage of improved access to the lower oesophagus by comparison with perivisceral
oesophagectomy. In the event of a potential curative resection radical lymphadenectomy
may also be performed and enlarged nodes removed separately or en-bloc with the
oesophagus.
The first report of thoracoscopic oesophagectomy appeared in 1990(Leahy et al., 1990),
but all techniques have three common elements:
o A thoracoscopic oesophageal dissection,
o formation of a gastric tube as the oesophageal substitute, and
o arr o€sophagogastric anastomosis.
Thoracoscopic oesophageal dissection is a relatively straightforward procedure, and
became quickly established in many groups. However, it is usually combined with an
open abdominal procedure for mobilisation of the stomach. It is conceivable that some
of the gains achieved by thoracoscopy may be nullified by the presence of a laparotomy
incision. However laparoscopic gastric mobilisation is much more technically
demanding, and reports of combined minimally-invasive oesophagogastric procedures
are less frequent. Perhaps the greatest technological hurdle to the completion of a totally
endosurgical oesophagectomy is the construction of a safe oesophagogastric
anastomosis. When total oesophagectomy has been performed with the proximal
resection margin situated in the upper third, this is not so much of a problem, as a low-
-81 -
morbidity cervical incision can be employed to fashion a traditional hand-sewn
anastomosis. However, if a subtotal oesophagectomy has been undertaken, the
anastomosis is more problematic, and some form of stapled anastomosis is necessary if
open access is to be avoided. Suitable endoscopic stapling instruments making the
anastomosis practically feasible only became available in 1993 (e.g. Stealth stapler -
Ethicon Australia, North Ryde, NSW), and even then were not specifically designed for
this application and were often modified. Customised endoscopic staplers for
intrathoracic anastomosis are still not commercially available in Australia because of
the small market and lack of standardisation for this operation. Until now, no studies
have successfully demonstrated all three components (a thoracoscopic oesophageal
dissection, laparoscopic formation of a gastric tube, and a circular intrathoracic stapled
oesophagogastric anastomosis) in the same procedure.
In 1990 Leahy et al first described oesophagectomy in the pig(Leahy et al., 1990). A left
thoracoscopic approach was used without insufÍlation, ambient pressure being adequate.
Four puncture access was required, and due to deficiencies in laparoscopic instruments
available at the time, conventional sponge holders and retractors were required.
Although Leahy reported that the stomach could be easily mobilised from above, and a
stapled side-to-side oesophagogastric anastomosis constructed after division of the
diaphragm(Leahy et al., 1990), this technique has not been duplicated because of
theoretical concems with staple closure of the large diaphragmatic defect created.
Experimental thoracoscopic dissection of the oesophagus in swine was next described
by Gossot in 1992(Gossot et al., 1992), but no attempt was made to mobilise the
stomach or construct an anastomosis. Later that year, Dallemagne et al published a case
-82-

report of the first successful human oesophagectomy in an 80 year old man with a
squamous cell carcinoma of the middle third(Dallemagne et al., 1923). A thoracoscopic
dissection was combined with a laparoscopic gastroplasty and an open cervical
anastomosis. The procedure lasted nine and a half hours, and tubalisation of the
stomach required eleven cartridges of an EndoGIA stapler, and the technique appeared
awkward. Although the cost in operative time and consumables appeared dramatic, the
elderly patient made an equally dramatic postoperative recovery and was discharged on
day 9.In 1992 Peracchia et al also reported using thoracoscopic mobilisation in 10
patients with oesophageal cancer, recording no intraoperative or postoperative
complications(Peracchia et al.,l992a). No further detail was given, and it is
unfortunately impossible to judge the importance of this contribution. Lointier et al,
1993, performed a study of thoracoscopic dissection in two human cadavers to
determine the optimum operating room setup and sites for trocar placement(Lointier et
al.,l993a). The feasibility of thoracoscopic dissection that had been described in
existing reports was confirmed. They advocated the advantages of supine patient
positioning for the dissection, thereby obviating the need to turn the patient for
subsequent stages of the operation, and allowing two surgical teams to operate
simultaneously. Perhaps the most important contribution of this paper was to highlight
the anatomical differences that limit the practical value of animal models in the
development of minimally-invasive oesophagectomy. The oesophagus of the pig lies
much more exposed, and the vessels are clearly visible, facilitating dissection. In
contrast, the human mediastinum contains much more compactfat and connective
tissue, and dissection is somewhat more difficult.
-83-

Thoracoscopic oesophagectomy through a right-sided posterolateral approach was also
clinically applied by Cuschieri in five patients with the only complication being one
vocal cord palsy(Cuschieri et al., 1992). However these patients required open
synchronous abdominal and cervical procedures for mobilisation of the stomach and for
the oesophagogastric anastomosis respectively. Insertion of a flexible gastroscope was
used to facilitate the procedure, as the lighted tip aids identification of the oesophagus,
but more importantly by flexing the instrument the organ can be lifted out of the
vertebral gutter. The time taken for the thoracoscopic procedure ranged from 3 - 4
hours, and the total duration of operation from 4.5 - 7.5 hours. Remarkably,
postoperative opiate analgesia was not required after the second day, and patients were
discharged after a median of 11 days. Cuschieri makes the point in this paper that
mediastinal node dissection is much easier with thoracoscopy than with the limited
view provided by the mediastinoscopic approach developed by Buess. This series was
expanded to 27 consecutive patients in a subsequent paper by the same author in
1993(Cuschieri, 1993). Seven patients had to be excluded because of inoperabrlity (74%
resectability rate). Thoracotomy was required in one of the remaining 20 patients
because of massive aortic bleeding encountered during the separation of a large tumour
from the aorta. Of the 19 successful thoracoscopic dissections there was no measurable
blood loss with a median duration of 5.5 hours. There \ /as no mortality in this series,
and apart from the previously mentioned vocal cord palsy, one further patient developed
a significant anastomotic leak, and three additional patients developed respiratory
complications. This author made the important observation that the incidence of
postoperative pulmonary complications does not appear to be reduced solely by the
avoidance of thoracotomy. He concluded that thoracoscopic oesophagectomy required a
-84-

considerably longer operating time, was technically demanding beyond the already
arduous open operation, and the investment in the required technology rendered it a
more expensive surgical option. At the time he was a pre-eminent world leader in this
operation, and his results and calls for the justification of this procedure in terms of
patient outcome had a significant moderating influence on global enthusiasm. This
opinion would seem to be mirrored by a Surgical Workshop published by Azagra in the
British Journal of Surgery(AzagraJ. 1993). They reported eight patients who underwent
oesophagectomy for cancer in which thoracotomy was replaced by thoracoscopy during
their standard three-stage resection. Although they reported the oesophageal dissection
to be technically easy, pulmonary complications were notable by their prominence.
Intraoperatively, intermittent pulmonary re-expansion was requested by the anaesthetic
team in one patient, another developed a pulmonary infection postoperatively, and six
others showed radiological evidence of oedematous lesions on the right side resulting
from poor pulmonary re-expansion.
By this time it was becoming clearly apparent that CO2 capnothorax had significant
implications for the anaesthetist, and the corresponding lung collapse was likely to be
the major factor precipitating the failure to demonstrate reduced pulmonary
complications following thoracoscopy. Peden and Prys-Roberts explored these
physiological changes in more detail during ten thoracoscopic oesophageal dissections
where the right lung was collapsed by the use of a double-lumen endotracheal tube and
insuffflation of CO2 into the thoracic cavity(Peden and Prysroberts,1993). The mean
period of one-lung anaesthesia lasted up to 3 hours (mean 2 hours) but the majority of
the changes in physiological variables occurred within the first few minutes, coinciding
with rapid insufflation of CO2 and deflation of the lung. The commonest problems were
-85-

an increase in P¡CO2 requiring increased fresh gas flow and minute ventilation. A more
alarming problem was the sudden decrease in blood pressure during insufflation of CO2
whereby the systolic pressure decreased in five of the ten patients by between 15 and 35
mm Hg from a previously stable level of 90 to 120 mm Hg. cessation of co2
insufflation, and escape of the CO2 from the thorax rapidly retumed the respiratory and
haemodynamic variables to their previous level. In one patient thoracoscopy had to be
abandoned because of dangerous fluctuations in these physiological parameters.
Extensive patient monitoring was considered mandatory. The authors stated that the
haemodynamic instability and hypoxia resulting from rapid or excessive insufflation of
CO2, or failure to of the lung to adequately deflate in response to compression by CO2
was likened to a tension pneumothorax. If this occurs the capnothorax should be
immediately released and the patient stabilised before cautious reintroduction of slow
insufflation. Postoperatively, residual pneumothorax can create problems if undetected,
and can result from residual pockets of CO2 especially if the lung is not fully re-inflated,
or from pneumothorax of the opposite lung caused by excessive intrathoracic pressures.
Recurrent laryngeal nerve damage was also thought to be a factor contributing to
postoperative pulmonary morbidity by provoking aspiration.
Subsequent series of thoracoscopic mobilisation of the oesophagus as part of a multi-
stage procedure (Collard et al., 1993), (Gossot et al., 1993) have similarly reported
unfavourably high pulmonary complication rates. McAnena et al(McAnena et al., 1994)
reported some degree of right lung consolidation in all nine patients in their series.
Three required bronchoscopy to assist removal of bronchial secretions, and all but one
required assisted ventilation for at leastT2 hours. The authors recommended that
thoracoscopic oesophagectomy not be routinely adopted until measures to overcome the
-86-
postoperative respiratory problems are resolved. Intraoperative difficulties were
responsible for conversion rates to thoracotomy in the order of 15%(Collard et al.,
1993)to2ÙYo(Gossot et a1.,1993). Difficulties in exposure of the posterior mediastinum
by a right lateral thoracoscopy were reported to be contributory, and were considered to
impair the surgeon's ability to manage any untoward intraoperative injuries to
mediastinal structures.
Fortunately, an elegantly simple solution to the problems of acute capnothorax and poor
exposure of the mediastinum has been developed by Cuschieri(Cuschieri, 1994), who
had previously voiced reservations about thoracoscopic oesophagectomy. The patient is
positioned in the prone jack-knife position. This results in lateral displacement of the
scapula and excellent access to the mediastinum and the entire intrathoracic
oesophagus. As the right lung falls away form the operative field by gravity, good
visualisation is achieved without the need for one-lung anaesthesia or CO2 insufflation.
The renewed enthusiasm of this prominent surgeon in the procedure was shared by
many, and a consensus developed that one of the major impediments to the further
development of this promising new operation had been overcome.
The laparoscopic mobilisation and tubalisation of the stomach is not a major technical
obstacle to complete endosurgical oesophagectomy. Apart from the few instances in
which it has been reported as part of a three-stage oesophagectomy, partial gastrectomy
has been reported as an individual procedure for treatment of ulcer disease and benign
or malignant neoplasms. Laparoscopic local excisions of benign or submucosal tumours
have been reported on several occasions(Abercrombie et al., 1993 ;Fowler and White,
I99l ;Lttkaszcyzyk and Preletz,1992). A totally-intraabdominal laparoscopic Billroth-
-87 -
II gastrectomy was performed by Goh in 1992(Goh et al., 1992). Although the
procedure required 4 hours and 17 applications of the EndoGIA stapler, the patient's
intraoperative course was uneventful, and postoperative recovery was remarkable.
Another similar case was reported by Lointier in 1993(Lointier et al., 1993b). Anvari
has recently reported a series of three laparoscopic-assisted vagotomies and distal
gastrectomies, with continuity re-established by Billroth I or II anastomoses(Anvari and
Park,1994). Operation time ranged from2 hours 35 minutes to 4 hour 40 minutes,
blood loss was minimal, and patients recovered well. A 5cm muscle-splitting incision
was used to construct the anastomosis, despite which a considerable number of
laparoscopic staplers were still required. Most authors comment that laparoscopic
gastric resections can be performed safely and within a reasonable length of time by
surgeons with experience in this area. The majority of the technical descriptions to date
probably reflect reports ofthe respective surgeons' learning curves, and considerable
reductions in operating duration and consumables can be reasonably expected with
further experience.
The problematic oesophagogastric anastomosis has been addressed by two other studies
concurrent to my own, and subsequently published after completion of my
study(Manncke et al.,I994a; Lloyd et al., 1994). An important point of differentiation
is that the stapled intrathoracic anastomotic techniques described in these animal and
human studies required at least a minilaparotomy for insertion of the circular staple gun.
Manncke et al described a non-survival porcine study in which a stapled intrathoracic
anastomosis was performed transgastrically in eleven animals, and transorally in a
further eight(Manncke et al,l994a). Extensive modifications \¡/ere required to the
available stapling devices for these techniques to be performed. In the transgastric
-88-

approach the detached stapler anvil is inserted into the proximal oesophageal stump
under thoracoscopic guidance, and fixed with two PDS endoloops. The staple gun is
inserted into the abdomen via a laparotomy and then into the stomach via an
antrostomy. The hand-piece of the stapler is used to push the tubalised stomach
transhiatally into the thorax. Thereafter the stomach wall is perforated by the spike, the
two parts of the stapler are reconnected, and the anastomosis is completed. In the
transoral approach the stapler is wound open after being inserted into the oesophagus
from a cranial direction. The oesophagus is ligated in continuity with two ligatures
positioned at the side of the gun and at the anvil. The oesophagus is transected between
these ligatures, and the stapler disconnected. This allows a separate stapler spike with
an attached trailing wire to be inserted into the anvil/oesophageal specimen complex.
As the oesophageal specimen is extracted into the abdomen via alaparotomy, the anvil
and trailing wire follow. After the stomach has been prepared, the anvil is re-inserted
into the stomach via an antrostomy and fixed with a purse-string suture. By traction on
the wire, the stomach can be pulled into the thorax, after which the wire is removed.
The anastomosis is then performed by reconnecting and approximating both parts of the
stapler. This procedure was found to be complicated by the insufficient length and
rigidity of the staplers, makingperorum insertion difficult, and this technically
descriptive manuscript reported no outcome parameters. The transoral approach,
although ingenious, has many steps liable to increase the chance of technical error or
malfunction, and is unlikely to be practically feasible until long, flexible circular
staplers become commercially available(Rossi, 1994). The transgastric approach has the
fundamental limitation of requiring a laparotomy, and as a totally endosurgical
procedure was not entertained, the necessity or superiority of an intrathoracic
-89-

anastomosis beyond the easier and perhaps safer hand-sewn cervical anastomosis is
questionable.
Transgastric circular stapled oesophagogastric anastomosis under thoracoscopic control
has been attempted in eight patients by Lloyd et al, and was successful in five(Lloyd et
a1.,1994). A slightly simpler technique for manouevring the anvil into the.oesophageal
remnant is described, by means of a clear plastic suction tube passed perorum. This tube
is passed out of a thoracic oesophagotomy above the tumour and delivered through the
hiatus into the abdomen. Again the minimally-invasive value of the operation is
diminished by the need for a laparotomy to guide the tube outside the abdomen. This is
required to allow the stapler anvil with spike to be pushed firmly onto the tubing. By
cranial traction on the tube, the anvil is drawn back into the oesophagus. After
thoracoscopic transection of the oesophagus by a linear stapler and orthodox formation
of a gastric tube has been completed, the staple gun/stomach assembly is delivered
transhiatally to approximate the oesophageal remnant. It is stated that by pushing on the
plastic tube from above, the anvil spike may be driven through the proximal
oesophageal staple line, but no details are given on how this works in practice. It would
be natural to assume that the exit point of the spike would be imprecise, and that it
would be difficult to deliver enough force to achieve penetration given the flexible
nature of the suction tubing. Once the anvil and staple gun are re-engaged and fired, the
entire assembly, with the suction tubing still attached to the anvil, is withdrawn out of
the abdominal incision. Importantly, the integrity of all double-stapled anastomoses in
this series v/as proven by barium swallow at day ten postoperatively. These
investigators are not only the sole group to have demonstrated the practicability of a
thoracoscopic circular stapled anastomosis, but have demonstrated its safety as well.
-90-
Unfortunately the novelty of the suction tube technique to place the anvil may well
become a liability if and when this approach is used during laparoscopic gastric
mobilisation, as it unlikely this large bore tube could be successfully manouevred out of
currently available laparoscopic ports. Theoretical concerns also exist about
dissemination of malignant cells by the passage of intraluminal instruments prior to
construction of anastomoses, which could potentially be accentuated by
laparoscopy(Gertsch et al., 1992; Berends et al., 1994 ;Norgrenj and Svensson, 19g5).
To date all described stapled anastomotic techniques require a laparotomy, àtê
technically complex, and would translate poorly to a laparoscopic approach. In the final
analysis, as will be shown by -y results, they are unnecessary.
AimThe aim of this study was to investigate whether existing techniques of minimally-
invasive oesophageal and gastric mobilization could be advanced sufficiently in
combination with a thoracoscopic oesophagogastric anastomosis to allow complete
endosurgical oesophagectomy to be safely performed.
-91 -

4.1.2 Methods
AnaesthesiaTen 70 kg domestic pigs were used as the animal model. General anaesthesia was
induced with ketamine 10 mg/kg administered subcutaneously followed by 2%
halothane in oxygen via a face-mask. A Robert-Shaw type 42F left-sided double-lumen
endotracheal tube was introduced into the trachea via a tracheostomy and then the
endobronchial lumen, and correctly positioned by ausculatation of the chest. The
animals were paralysed using pancuronium administered intravenously 0.1 mg/kg and
ventilated using a Bird Mark 8 ventilator. Anaesthesia was maintained using 1 - 2 %
halothane in oxygen and muscle paralysis maintained with intravenous pancuronium
0.05 mg/kg/hr. Single lung ventilation with collapse of the right lung was used during
thoracoscopy. A large bore orogastric tube was used to empty the stomach before
surgery commenced.
The first two animals died during thoracoscopy. In the next eight animals arterial
saturation was continuously monitored using a pulse oximeter with a probe on the left
ear, and arterial pressure measured using a20G cannula inserted into an artery in the
left hindlimb and connected to a Deseret transducer with systolic and diastolic pressure
continuously displayed on a liquid crystal display. In these animals, four to six litres of
normal saline was administered via a cannula into an ear vein during the course of
surgery to minimise the cardiovascular effects of reverse Trendelenburg positioning,
positive intraperitoneal pressure during laparoscopy and mediastinal pressure during
thoracoscopy. In the last eight animals, there were no episodes of significant
hypotension.
-92 -
Operative detailsThe surgical team consisted of the surgeon, an assistant to hold the camera & retractors,
and a second assistant to assist with retraction and to manipulate a gastroscope. A 3
stage operation was performed, commencing with a thoracoscopic dissection of the
oesophagus with the animal in the left lateral position.
Thoracoscopic oesophageal dissection
Carbon dioxide was insufflated into the right thoracic cavity to a maximum pressure of
6 mmHg. A 30 degree telescopelcamerc assembly was inserted to provide a view of the
operative field through the trocar in the 9th intercostal space in the mid-axillary line. The
remaining four trocars were inserted under videoendoscopic control in the following
locations; one 1Omm trocar for the fan-shaped lung retractor was placed in the 7th
intercostal space in the mid-clavicular line, one 1Omm trocar was placed in the 7th
intercostal space in a paravertebral position , one 1Omm trocar was placed in the 5th
intercostal space in the mid-axillary line for dissection or Babcock forceps, and one
5mm trocar was inserted in the 5th intercostal space in a paravertebral position for
insertion of Endoloops. A good view of the upper and lower limits of dissection was
obtained by moving the telescopelcamera assembly between the upper and lower ports
in the mid-axillary line. A flexible oesophagoscope insertedper orLtm, as described by
Cuschieri(Cuschieri et al., 1992), assisted dissection by manipulating the position of the
oesophagus with the endoscope's flexible tip. The oesophagus was initially approached
in its lower third, commencing with division of the mediastinal pleura to expose the
oesophagus, and dissection was then undertaken caudally to fully mobilise the
oesophagus within the hiatus and divide the inferior pulmonary ligament. The
oesophagus was elevated by Babcock forceps and dissected free from its posterior
attachments to the aorta, which were cauterised or clipped, and divided. It was
-93 -

necessary to divide both vagal trunks to achieve full mobilizationof the thoracic
oesophagus. The middle third of the oesophagus was then separated from its
attachments. Depending on the level of resection the upper third of the oesophagus was
then mobilised.
After oesophageal dissection was complete an extra-corporeally tied ligature was
snugged at the upper limit of resection in order to minimize the potential spillage of
"tumour" cells, and the oesophagus was divided just above this point, leaving an open
proximal oesophageal remnant. Subsequent laparoscopic mobilisation of the intra-
abdominal oesophagus was considerably facilitated by guiding the lighted tip of the
endoscope through the hiatus from above before concluding the thoracoscopy.
Laparoscopic gastric mobilisation
The second stage was performed with the animal in the supine position and standard
abdominal laparoscopy was commenced with insufflation of carbon dioxide through the
umbilicus to a maximum pressure of 12 mmHg. Five trocars were inserted into the
abdominal cavity (four lOmm and one 12mm). The oesophageal hiatus was rapidly
identified by the light of the endoscope. It was dissected free which then allowed the
operative specimen to be pulled into the abdomen. The subsequent ability to retract the
gastroesophageal junction in any direction made exposure and dissection of the stomach
much easier. The gastrophrenic ligament was transected and dissection continued with
ligation and division of the short gastric vessels. Following this the lesser curvature of
the stomach was mobilised by dividing the vessels in the cephalad portion of the lesser
omentum between clips. When suffrcient gastric mobility to enable the stomach to reach
into the left hemithorax had been achieved, the left upper quadrant 10mm port was
exchanged for an 18mm port through which a linear endostapler was passed to divide
-94-
the oesophagus at the gastroesophageal junction. The l8 mm port was then exchanged
for a 33mm port. The specimen extraction adaptor for the 33mm Endopath port (Figure
4) was a safe and simple way to deliver the resected oesophagus intact. A longitudinal
gastrotomy was performed by elevating the pylorus between 2 Babcock forceps. The
laparoscopic circular endoluminal stapler (Stealth - Ethicon) (Figure 5) was inserted
through the 33mm port and manoeuvred into the stomach so the spike could be made to
perforate the fundus. The stapler anvil was connected to the spike using the anvil
docking instrument (Ethicon) and was wound down to hold the stomach in position. A
Babcock forcep was used to hold the gastrotomy edges apposed to avoid spillage of
gastric contents. The stapler assembly was then passed through the hiatus. The hiatus
was usually able to admit the stomach without constricting it, but was the hiatus
enlarged by anterior division if necessary.
Th oracoscop i c oe so p h ag og astric anasfomosls
The final step of the operation involved construction of a circular 25 mmdiameter
stapled intrathoracic oesophagogastric anastomosis. Under direct thoracoscopic
visualisation the anvil of the stapler was extended and inserted into the open proximal
oesophageal remnant. This manouevre was facilitated by a modification to the anvil
such that it was longer and more conical in shape (Figure 6). The anvil was then fixed in
position with an Endoloop ligature (Figure 7). Excess tissue was trimmed, the device
was adjusted to provide the correct degree of tension, and the staples were fired. The
instrument was removed and the anastomosis and doughnuts were inspected for any
break in continuity. The anastomosis was further checked to be watertight by
installation of saline through the orogastric tube after gently occluding the fundus with
an endoscopic bowel clamp. The gastrotomy was closed as a pyloroplasty by firing a
-95-

linear endostapler transversely across the defect. The trocars were removed and the
animals were then killed with pentobarbitone without reversal of anaesthesia.
All procedures on the animals were recorded on videotape to allow review of the
operative performance. This allowed enors to be identified and refinements to surgical
technique to be planned before the next procedure, maximising the experience gained
from each animal, and ensuring progress in experimentation. Paired data was analysed
by a V/illcoxon matched-pairs signed-ranks test and unpaired data by a Willcoxon
analysis.
-96-

Figure 4: (From left to right) 33mm cannula and trocar- specimen extractionadaptcr, ænd parÉ exchange rod (Endopath-Ethican)
-97 -

Figure 5: EndosurgicaË cireular sÉaptrer (SÉealÉh-Ethican) rvith speciatlv adepiedconieal anvil.
-98-
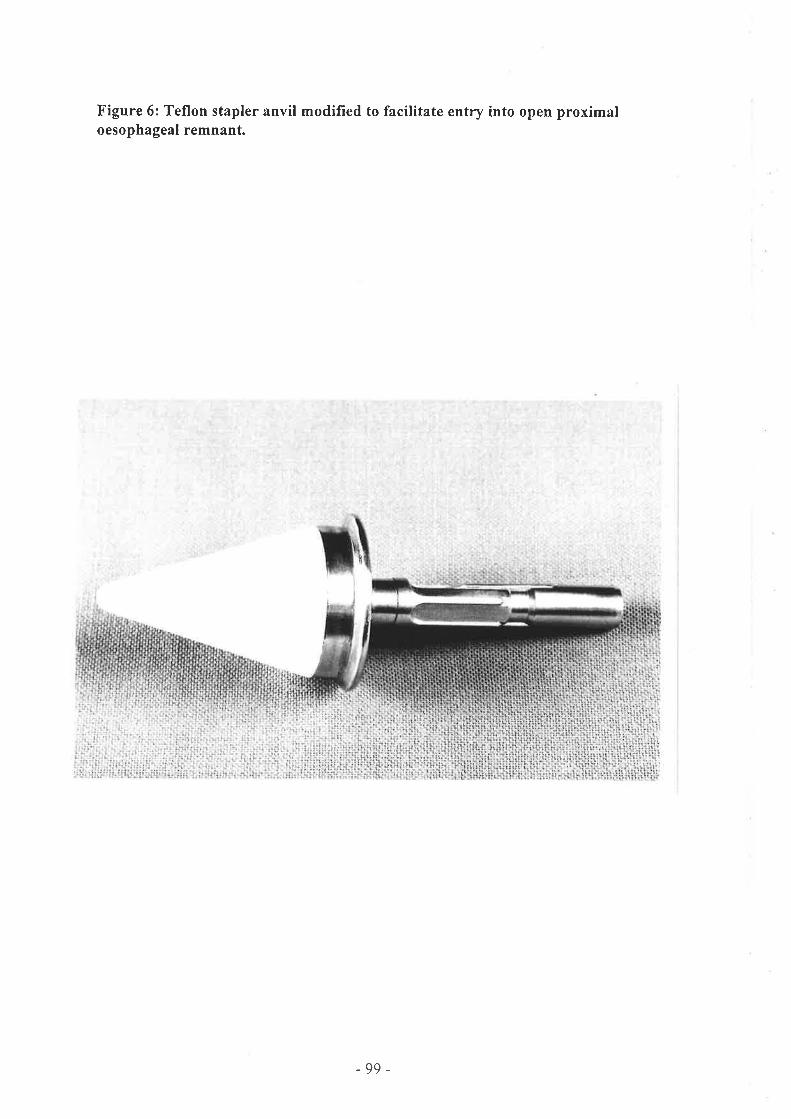
Figure 6: Teflon stapler anvil modified to facilitate entry into open proximaloesophageal remnant.
-99-
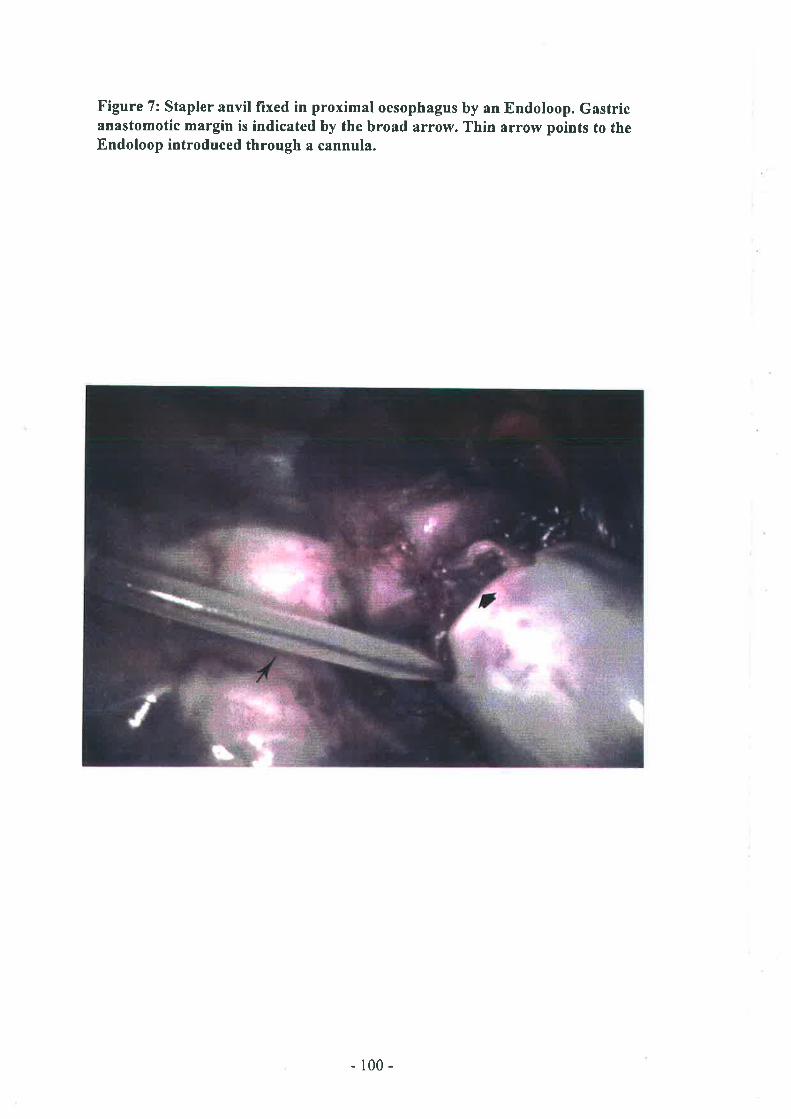
Figure 7: Stapler anvil lixed in proximal oesophagus by an Endoloop. Gastricanastomotíc margin is indicated by the broad arrow. Thin arrow points to theEndoloop introduced through a cannula.
-100-
4.1.3 Resu/fs
Successful thoracoscopic dissection of the oesophagus was achieved in all 10 plgs.
proximal resection margin was situated in the middle third in three cases, and in the
lower third in seven cases. The median length of oesophagus resected was 8.5 cm
(range 6.5 - 13.5 cm). Bleeding was minimal in each oesophageal dissection, and no
other major complications were recorded for this stage. Extensive pleural adhesions
were divided in three animals. For each oesophageal dissection 5 trocars , I endoloop,
and one fan-shaped retractor were used. A clip applier was used twice to control arterial
branches passing directly from the aorta to the oesophagus. The median operative
duration for this stage was 49 minutes (range 30 - 110 minutes).
Laparoscopic mobilisation of the stomach was performed successfully in all but one
animal. This pig had not been adequately fasted, and the large volume of feed present in
the stomach was unable to be removed laparoscopically and prevented adequate
mobilization. This was the longest part of the procedure with a median duration of 60
minutes (range 60 - 135 minutes). For each gastric dissection, the following
consumables were used: Three 1Omm trocars, one 12mm trocar, one 18mm trocar and
one 33 mm trocar. In addition, one clip applier/divider, one Stealth device, and one
linear stapler with a reloaded cartridge were required.
On one occasion after the dissection was complete, a disposable fan-retractor breached
the capsule of the liver and entered an hepatic vein resulting in afatalhaemorrhage.
Bleeding complications during this stage were otherwise minimal.
In the first animal there was some spillage of gastric contents from the gastrotomy as
the Stealth device was inserted.
-101 -
Thoracoscopic oesophagogastric anastomosis was the quickest stage of the procedure
with a median duration of 40 minutes (range l5 - 60 minutes ). A mean of 1.4
endoloops was required. Anastomoses were situated in the middle third of the
oesophagus in three pigs, and in the lower third of the oesophagus in six pigs. An
anastomosis was not performed in the animal who died from hepatic bleeding. Seven of
the ten anastomoses \À/ere watertight. However leakage was detected on three occasions
and was repaired with intemrpted Vicryl sutures. The donuts of tissue within the stapler
were intact in eight cases. The median duration for the procedures was 171 minutes
(range 134 - 2I0 minutes ).
4.1 .4 DrscussionIn the past, most methods of endosurgical oesophagectomy have relied on conventional
open oesophagogastric anastomosis via a cervical incision(Buess, 1991 ; Dallemagne et
al., 1923 ; cuschieri , 1993). The only two previous studies to have attempted a
minimally-invasive stapled anastomosis have required at least a
minilaparotomy(Manncke et al,I994a; Lloyd et al., Lgg4),notwithstanding such
additional requirements as extensively modified instrumentation and technically
complicated operative manouevres. This study has developed a potential solution to the
problematic stapled intrathoracic anastomosis, which is the limiting step in the
completion of total endosurgical oesophagectomy. Fully laparoscopic oesophagectomy
was successfully performed in six animals without the necessity for division of the
diaphragm. Even in the animals where extensive pleural and peritoneal adhesions were
encountered, it was possible to successfully complete the operation without conversion
to open surgery.
-102-
The duration of surgery was relatively short, with the median duration being a little
under three hours. The fact that the operations were performed on normal pigs without
bulky oesophageal tumours may be thought to mitigate this achievement. However if
preoperative synchronous chemoradiotherapy is administered to human subjects, the
tumour is not macroscopically apparent at the time of surgery 1n 46Vo of patients(Gill
and Jamieson,1992). With the greater precision demanded and their larger size, it is
likely that the operating time would be considerably longer in human subjects.
However, the duration of surgery for minimally-invasive oesophagectomy is likely to
compare favourably with open oesophagectomy because of the considerable time
savings achieved from the rapid ingress and egress from the operative sites. Other
factors which are likely to make the application of this technique to humans more
difficult compared to the pig include the greater f,rxity and adiposity of the human
oesophagus, the larger and more constant human azygos vein, the more substantial
greater omentum and short gastric vessels and the difficulty of directing the stapler in an
orientation which will allow insertion of the head into the proximal oesophagus.
The technical advantages of a laparoscopic gastric mobilisation over laparotomy include
the excellent view of the hiatus and the ease of its dissection. Once the intra-abdominal
portion of the oesophagus is mobilised it can be extracted from the thorax into the
peritoneal cavity without difficulty. This provides the surgeon with the unique ability to
retract on the gastroesophageal junction in any direction which considerably facilities
gastric mobilisation. However this manouevre also allows the escape of insufÍlated
intra-abdominal gas into the thorax under pressure, and leakage of gas may occur from
the mouth if the open proximal oesophageal remnant is not sealed. As with
conventional open gastric surgery, the surgeon must be a\¡/are of the position of the
-103-

common bile duct during mobilisation of the distal stomach, as it is at risk should the
mobilisation be carried too far distally. It was always possible to obtain sufhcient
gastric mobility in the pig without performing a Kocher manouevre.
The circular endoluminal stapler used was an Ethicon ILS redesigned for laparoscopic
bowel anastomoses. However it was well adapted to oesophagogastric anastomosis by
virtue of the additional length provided and particularly by the degree of distal
curvature. These features are so particularly suited to intra-thoracic anastomosis that we
advocate the use of this instrument with open gastric mobilisation when orientation of
the instrument is less of a problem. The length of oesophagus resected and site of
anastomosis are constrained only by the length of the shaft, and this factor could be
corrected in future generations of the instrument. The flat anvil provided, however, was
unsuitable because it was difficult to insert into the lumen of the proximal oesophageal
remnant, and had to be inserted almost sideways. The modified Teflon conical anvil
was demonstrably easier to insert, but required greater vigilance during passage through
the hiatus as surrounding structures were at risk of trauma from its pointed tip.
Insertion of the circular stapler through a longitudinal gastrotomy sited at the pylorus
was necessary to prevent the gastrotomy being pulled up into the chest with the
proximal stomach, and had the advantage of being easily closed transversely by alinear
stapler thereby conveniently accomplishing a pyloroplasty as a drainage
procedure(Snyders, 1993).
It is of vital importance for the stomach to be emptied before the operation is
commenced otherwise gastric mobilisation is very diffrcult, and insertion of the circular
stapler may lead to a flood of gastric juice into the peritoneal cavity. A Babcock forcep
-to4-
applied to the two sides of the gastrotomy beneath the stapler helps to seal any potential
leak, and allows retrograde traction to be exerted on the fundus as the stapler spike is
extended. Perforation ofthe spike through the gastroesophagealjunction had been seen
to cause the linear staple line to open in a previous trial animal. Therefore puncture of
the anterior fundus is considered safer and it also provides greater gastric length.
Oesophagogastric anastomosis performed with the circular stapler has been documented
to have a very low leakage rate (0%oto 3.5%) (Wong et al., 1987 ; Ajani et al., 1993).
The endoscopic method described is very similar to the open technique, and an
equivalent degree of safety can be expected. As with the open procedure, the surgeon
must be aware of the inherent problems with stapled oesophageal anastomoses.
Anastomotic insufficiency from insecure fixation of the proximal margin to the anvil by
the endloop, excess tension on the gastric fundus, or too much intervening tissue
between the ends to be joined will contribute to anastomotic leakage. Seven of ten of
our anastomoses were watertight, and those that leaked were able to be repaired by
laparoscopically-placed sutures. Although the doughnuts were not intact in two animals,
their respective anatomoses \À/ere watertight and they appeared intact to visual
inspection. No difhculty was encountered in constructing anastomoses of 25mm
diameter in pigs, however 25mm circular stapled anastomoses in humans have been
associated with postoperative stricture rates of up to 29Yo(Wong et al., 1987 ; Chassin,
ree3).
The major complications \ /ere the intraoperative deaths of three animals. As a response
to the deaths of the first two pigs in our series, invasive intra-arterial pressure
monitoring and pulse oximetry was undertaken and no further diffrculties were
-105-

encountered. It appears great caution must be taken to prevent the hypotensive effects of
gas insufflated into the abdomen and thorax. The third animal death was a result of
traumatic laceration of a hepatic vein by a disposable fan-shaped liver retractor, caused
by unexpected movement of the animal. Videotape review revealed that if the blade of
this style of retractor is turned side-on, it can act as a knife on the structure it is
supporting. Subsequent use of an alternate retractor removed any risk of this occurring.
Total endosurgical oesophagectomy is feasible, and it is likely that a stapled
intrathoracic anastomosis can be constructed without exposing patients to risks beyond
those of the equivalent open technique. The method developed appears to be a viable
option for palliation or cure of oesophageal tumors. In the context of existing literature,
it seems likely that thoracoscopic oesophagectomy can be performed safely in the
majority of selected patients, although it should not be seen as a panacea to all the
problems that have dogged orthodox oesophagectomy for so long. Rather, the likely
benefits of reduced postoperative pain, quicker recovery time, and reduced
intraoperative blood loss should be considered in light of other requirements of the
individual patient. Thoracoscopic oesophagectomy is now a useful surgical option that
can be added to the armamentarium of treatments for oesophageal cancer. Pulmonary
complications may or may not be reduced using this approach, and the merits of
thoracoscopic resection must await confirmation by controlled trials.
-106-
4.2 Highly selective vagotomy
4.2.1 lntroduction
Historv of ooen vaootomvThe vagus nerves were first described by Galen in about 200 AD, but it was not until
1814 that Brodie first demonstrated that vagotomy in dogs reduced gastric
secretion(Brodie, 1814). However the first human vagotomy (apparently performed by
Jaboulay in 1901) was not for peptic ulcer disease but rather to relieve abdominal pain
in a patient with tabes dorsalis(Woodward, l9S7).
It was Latarjet in 1920 who first used truncal vagotomy therapeutically on patients with
duodenal ulcers(Skandalakis et al., 1986). He recognised delayed gastric emptying and
later added a gastroenterostomy to the procedure. In spite of his success, it took another
20 years before Dragstedt's work convinced Americans that vagotomy was a viable
alternative to partial gastrectomy, which up until then had been the preferred treatment
for duodenal ulcer disease(Dragstedt, 1945).
Truncal vagotomy combined with antrectomy was introduced by Farmer & Smithwick
in 1952(Farmer and Smithwick,7952). The combined operation became very popular
when it became apparent that peptic ulcer recurrence rate was less than 1%. The
physiological success of this operation stems from the fact that the removal of the
gastric antrum renders the parietal cell mass less sensitive, and since a small amount of
parietal cell innervation probably persists in most patients after vagotomy, this
innervation is nullified because of the diminished presence of gastrin.
Selective vagotomy was the next development, in an attempt to decrease postvagotomy
diarrhoea. The hepatic and coeliacvagal divisions to the gallbladder and small intestine
were spared, intemrpting only the anterior and posterior descending gastric divisions
-t07-
(the nerves of Laterjet). However this operation still caused gastric stasis, and it did not
achieve widespread acceptance until Griffith & Harkins combined it with a drainage
procedure in l957(Griffith and Harkins, 1957).
In 1969 Johnston & V/ilkinson from Leeds demonstrated that it was possible to divide
only the vagal branches to the parietal cells, preserving the nerves of Latarjet and motor
innervation to the pylorus and antrum(Johnston and Wilkinson, 1969). This highly
selective vagotomy reduces acid secretion as effectively as truncal vagotomy, and is
very safe with an operative mortality rate well under IYo. The innervated antrum
provides undisturbed solid emptying, and preservation of the pylorus reduces the
tendency for duodeno-gastric reflux. There is a low incidence of unwanted side-effects
such as dumping and post-vagotomy diarrhoea(Taylor, I982a). Many surgeons believe
that HSV is the optimal surgical treatment for chronic duodenal ulcer refractory to
medical therapy.
However, there are inherent disadvantages to HSV that have prevented it from gaining
widespread acceptance. The ulcer recurrence rate tends to be higher than for truncal
vagotomy and pyloroplasty(Taylor et al., 1990). There is a risk of damaging the the
nerve of Latarjet which may delay gastric emptying, and a risk of ischaemic necrosis of
the lesser curve which although rare, can be fatal. The operation can also be protracted
and technically diffrcult. In 1978 Hill and Barker developed a technically simpler
modification(Hill and Barker,1978). They combined an anterior HSV with a posterior
truncal vagotomy. This operation achieved a reduction in acid output reportedly similar
in magnitude to highly selective vagotomy without any increase in gastric emptying
difficulties.
-108-

In the early 1980's Thomas Taylor published the details of another operation as an
alternative to HSV(Taylor, 1982b). The technique denervates the parietal cell mass in a
more expedient manner without the risk of ischaemic necrosis of the lesser curve nor
damage to the the nerve of Latarjet(Taylor, 1982a). Followup studies have shown this
procedure to relatively simple, quick, and easy to perform(Taylor, 19S5). Delayed
gastric emptying has been reported in L7o/o of patients. Post-vagotomy diarrhoea has
been troublesome in only O.33%(Taylor et al., 1990). Ulcer recuffence rates have been
reported in the range of 6Yo - 8%(Taylor et al., 1990 ; Oostvogel and van Vroonhoven,
1988). By comparison with truncal vagotomy and pyloroplasty the Taylor operation has
a lower incidence of dumping and diarrhoea and achieves better overall Visick grading,
with no reported difference in ulcer recurrence rates at this stage(Taylor et al., 1990).
Comparison with HSV has shown similarly good clinical outcomes and low ulcer
recurrence rates, but HSV takes considerably longer to perform than the Taylor
procedure(Oostvogel and van Vroonhoven, 1988). Sharp dissection of the seromyotomy
may cause occasional mucosal perforation, and Taylor has modified the operation to
include an "overlap repair" with lateral displacement to reinforce the stomach(Taylor,
1982b; Taylor, 1982a).
Gomez-Ferrer subsequently further modified the Taylor procedure, whereby the
seromyotomy is performed by a linear stapler rather than sharp dissection. The stapler
accomplishes simultaneous division and reanastomosis along the lesser curye of the
stomach, and then a posterior truncal vagotomy is performed. Results in an open
environment showed recurrent ulceration in I2Yo of patients, good reductions in
postoperative basal and peak acid outputs, but residually innervated strips of mucosa on
-109-

the lesser curve were observed following Endoscopic Congo Red Testing(Monis et al.,
lee3).
Development of minimal-access vagotomyIn open abdominal procedures, the duration of hospitalisation and time required to
retum to normal activities are often related to the trauma of laparotomy(Neugebauer et
al., 1991). Following the introduction of laparoscopic access for abdominal surgery, it
was quickly realised that laparoscopic vagotomy might offer the same physiological
eflrcacy as established anti-ulcer procedures(Cuschieri,1992), but with the additional
benefits conferred by minimally-invasive access. The entire spectrum of open vagotomy
procedures have since been duplicated in the laparoscopic environment.
A thoracoscopic approach to the vagal trunks was popularizedby Wittmoser in the
1950's using a single-puncture technique(Schurr and Buess, 1993), but never gained
wide acceptance for the treatment of peptic ulcer disease. Since 1989, elective truncal
vagotomy for chronic duodenal ulcer has been described by Dubois using the
thoracoscopic route(Dubois, 1992), with selective simultaneous or subsequent
endoscopic balloon dilatation of the pylorus if pylorospasm is a problem. He contends
that if patients with a history of diarrhoea are excluded, serious post-vagotomy
diarrhoea is uncommon, and routine pyloroplasty is unnecessary. The advantages of this
procedure are portrayed to be a lower rate of recurrent ulceration than HSV, and the
technical simplicity and speed of the thoracoscopic operation. In a series of 21 patients
all ulcers were healed after short follow-up, and minimal morbidity was
encountered(Dubois, 1994).In particular no long-term gastric stasis was observed,
despite two patients requiring pyloric dilatation. Larger series of this procedure have not
been forthcoming, and it is now considered to be reserved for use in patients with
- 110-
evidence of incomplete vagotomy, where a redo laparoscopic procedure may be
diffrcult due to scarring and adhesion formation(Branicki and Nathanson, 1994 ;
Corbelle, Jr and Corbelle, 1993). Truncal vagotomy and pyloromyotomy can also be
performed via the laparoscopic route(Pietrafitta et al., l99l ; Dubois, 1992), but this
would appear to have little advantage over the more straightforward thoracoscopic
approach.
Laparoscopic posterior truncal vagotomy and anterior seromyotomy has become a
popular procedure, as evidenced by the numerous literature reports(Voeller et al.,l99l ;
Shapiro et al., l99I ; Mouiel and Katkhouda,1992; Katkhouda and Mouiel, l99l :
Croce et al., 1994). This operation was introduced by Katkhouda and Mouiel in
1990(Katkhouda and Mouiel, l99l), and to date Katkhouda has reported the largest
experience in a series of 90 patients(Katkhouda et a1.,1994). There was no mortality or
conversions to an open procedure. Postoperatively, mild diamhoea was observed in
three patients, and mild symptomatic gastric stasis in a further three, but all settled with
conservative treatment. An ulcer recuffence rate of 4.2Yo after follow-up of 2 - 4I
months was reported, and basal and maximal acid outputs were reduced by 79Yo and
83olo respectively. These early results suggest laparoscopic posterior truncal vagotomy
and anterior seromyotomy is safe, and may produce a clinical outcome similar to that
obtained in open surgery. However this procedure is unlikely to be adopted by the many
surgeons who retain misgivings about the corresponding open operation because of the
theoretical risk of leaving a strip residually innervated mucosa on the lesser curve, and
who prefer HSV because of its anatomic and pathophysiological elegance.
- 111 -
Laparoscopic HSV was first reported by Bailey in 1991, combined with a laparoscopic
cholecystectomy in a patient with intractable duodenal ulcer disease and symptomatic
biliary colic(Bailey et al., 1991). The tedious dissection associated with the open
procedure was reportedly made easier by videoscopic magnification. The largest
published series was conducted by Dallemagne, who reported the results of 35 patients,
25 of whom also underwent an anti-reflux procedure(Dallemagne et al., 1994). Gastric
acid studies were performed in only 12 patients, and the mean follow-up after operation
was 7.3 (range 3 - 22) months. The mean operating time was 110 (range 85 - 205)
minutes for HSV alone. There was no 30 day mortality or morbidity, and the mean
length of hospital stay was 3.6 (range 2 - 6) days. All ulcers were seen to be healed on
postoperative endoscopy, and only two patients remained symptomatic on follow-up;
one with epigastric discomfort and the other with diarrhoea. Apparent reductions in
basal and maximal acid outputs were reported but not subjected to statistical analysis.
Despite a lack of controlled data, these basic clinical results suggest that laparoscopic
HSV may be as safe and possibly as effective as the open operation, but with the
advantages of a70o/o reduction in hospital stay, and 50%o reduction in the overall
recovery period. Furthermore, a cost-benefit analysis of medical therapy compared to
conventional as well as laparoscopic vagotomy has reported that surgery is more cost-
effective than medicine at 2 years, and safer than medicine at 4 years as a result of
complications from failed medical therapy. It was suggested that the impact of
laparoscopic surgery will be to widen the margin of benefit for surgery(Fletcher, 1993).
The first reported case of anterior HSV and posterior truncal vagotomy was performed
by Nottle, an Australian surgeon, in July 1991(Nottle, 1991). Kum and Goh described
their technique in a another case report in 1992 (Kum and Goh, 1992), and have
-rt2-
subsequently reported their fuither experience in 6 patients in 1993(Kum and Goh,
1993). There is little data on which a judgement can be made on the clinical outcome,
utility, or efftcacy of this procedure however. It is currently recommended that this
procedure remain an altemative in the armamentarium of laparoscopic vagotomy
procedures, to be used dependant on the suitable configuration ofthe anterior vagus
nerve and its branches(Branicki and Nathanson, 1994).
In 1992 Hannon reported his adaptation of the Gomez-Ferrer vagotomy, describing a
technique of laparoscopic linear stapled anterior seromyotomy and posterior truncal
vagotomy used in two patients(Hannon et al., 1993). Although no clinical outcome data
is available for this operation, the authors promote the ease and speed of use it provides.
Truncal vagotomy and distal gastrectomy has been the last established anti-ulcer
procedure to make the transition to the laparoscopic environment. In 1994 Anvari and
Park(Anvari and Park, 1994) reported the cases of three patients whose vagal trunks
were divided in the abdomen by laparoscopy, followed by stapled distal gastric
resections and single-layer hand-sewn extracorporeal anastomoses via a 5-6 cm
subcostal muscle-splitting incision. Although the procedures lasted up to 4 h 40 min in
duration, and required a wide array of expensive instruments, the patients were
discharged on days 4,5, and 6. No follow-up or comparative outcome data were
presented, mortality and morbidity were absent, and hospital stay was clearly shorter
than is the general experience for the corresponding open operation.
Unfortunately this multiplicity of minimally-invasive vagotomy techniques, combined
with low refer¡al rates for surgery has meant that the experience of each group has been
limited to relatively small series. No long-term clinical results are available by which
the efficacy of laparoscopic vagotomy can be definitively judged.
-113-

AimsThe aim of this study was to demonstrate the physiological validity of laparoscopic
highly selective vagotomy. Specific hypotheses tested can be summarized as follows.
l. To assess whether laparoscopic HSV is as effective in reducing the acid output of the
stomach as its open counterpart.
2. Thatthe laparoscopic HSV causes no greater disturbance of non-nutrient liquid
gastric emptying than its open counte{part.
3. That the laparoscopic HSV procedure causes no disturbance of gastro-oesophageal
competence and does not facilitate the development of acid gastro-oesophageal
reflux.
4.1.2 MethodsTwenty-five kg domestic white pigs were chosen as a suitable model due to their gastro-
oesophageal anatomic similarity to humans, and to allow a controlled series which
would eliminate confounding variables from the analysis. Animals were treated in
accordance with the Australian Code of Practice for the Care and Use of Animals for
Scientific Purposes, and ethical approval was granted by the Animal Ethics Committees
of the University of Adelaide and the Institute for Medical and Veterinary Science.
Twenty-two animals were studied in 4 groups. The first group did not have any
operative procedure. Because the pigs doubled in size over the 8 week study period,
these pigs controlled for the effect of growth on the physiological tests that were
performed at the beginning and end of the study. The second group of pigs underwent
laparoscopy and mobilisation of the stomach, but did not have a vagotomy performed.
This group controlled for any effect that may be attributable to the laparoscopic
environment alone. The third group of pigs underwent a traditional open HSV to act as
-rt4-

controls for the operative technique under investigation, and the fourth group underwent
the experimental procedure, the laparoscopic HSV.
The study period was broken up into 3 discrete stages, a 2 week preoperative period, a
one week perioperative period, and a 5 week postoperative period. To enable gastric
access, the animals underwent insertion of a cervical oesophagostomy on week one.
Preoperative gastric physiological studies were performed on week two, and the
operative procedure was performed on week three. Animals were then housed for 5
weeks postoperatively with regular review of their clinical progress. Four weeks after
their operative procedure, the gastric physiological studies were repeated. on
completion of the tests the animals were killed, and if any complication had supervened
a post-mortem was performed.
Cervical tube oesophagostomyOperations were performed after a 12hour fast. General anaesthesia was induced with
ketamine 10 mg/kg (10Omg/ml) administered subcutaneously followed by 2%halothane
in oxygen via a face-mask. An endotracheal tube was introduced into the trachea per
orum, and correctly positioned by auscultation of the chest. The animals were ventilated
using a Bird Mark 8 ventilator. Anaesthesia was maintained using I - 2 % halothane in
oxygen. A large bore orogastric tube was used to localise the oesophagus.
Animals received 2.5-3.0 mls (250mglml) of penstrep preoperatively and on days I to 3
postoperatively in a single intramuscular dose. The neck was shaved immediately
preoperatively, cleaned with chlorhexidine and prepared with aqueous Betadine.
Using full aseptic technique a transverse incision was made in the left hand side of the
neck just below the cricoid cartilage. Using a combination of sharp and blunt dissection
- 115 -

the oesophagus was exposed, aided by palpation of the orogastric tube. using
coagulation diathermy a2 mm hole was made into the lumen of the oesophagus, and
gently stretched open. 2/0 Surgipro (USSC) running pursestring suture maintained
approximation of the mucosa to the muscular wall of the oesophagus.
A t-tube plastic oesphagostomy was placed into the lumen (Figure 8), and the
pursestring suture tightened and tied. The oesophagostomy was brought out onto the
skin through a separate caudal stab incision. The skin was closed with 3/0 nylon.
Postoperatively animals received water only on the first day, milk only on the second
day, after which a soft diet was gradually re-introduced. Analgesia was achieved by use
of finadyne (flunixin meglumine - Herriet Agvet) 2mlsl45kg. Pigs were thereafter able
to maintain normal nutrition and body weight.
-116-
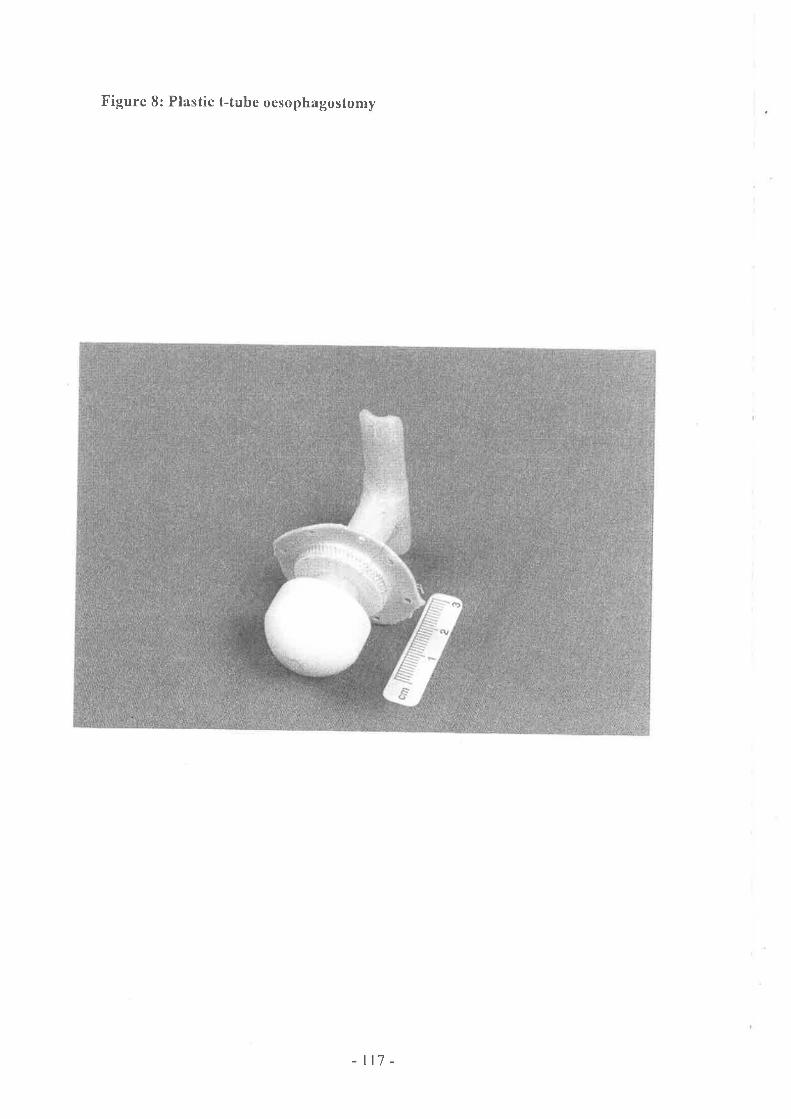
Figure 8: Plastic t-tube oesophagostomy
-rr7 -
Gastric acid output studiesThe pigs were allowed one week to recover from oesophagostomy insertion before the
preoperative baseline physiological tests were commenced. Gastric acid output
measurements were made after a 12 hour fast. Pigs were trained to stand quietly in a
metabolic crate while the position of the lower oesophageal sphincter was determined
by pull-through manometry. A 14 F Ryle's tube was then able to be accurately placed in
the stomach through the oesophagostomy. The length of the orogastric tube was
measured and a mark was made at the level of the lower oesophageal sphincter. Correct
positioning of the tip of the tube in the stomach was confirmed by a water-recovery test
(Hassan and Hobsley,1970) i.e. aspiration was attempted, and if unsuccessful the
position of the tube was readjusted until some aspirate was obtained. Twenty ml of
water was then instilled through the tube and aspiration attempted. If 16-20 ml of water
was recovered the tube was said to have passed the water-recovery test and the tip was
assumed to be in the stomach). The tube was then withdrav¡n2.5 cm at a time, the
water-recovery test being repeated. The tube was fixed in the shortest possible position
at which it passed the water-recovery test. Low intermittent suction was applied to the
tube to empty any resting juice and air. If any residual debris was detected the stomach
was lavaged with isotonic saline until the return was clear.
Gastric juice was collected under resting conditions by four 15 minute aspirates. Basal
secretion is used conventionally to describe the fasting gastric secretion. It represents
the secretion of the parietal cell mass being excited under the resting conditions of the
test. Transpyloric loss of secreted acid was assumed to be minimal because of
continuous suction. Polyethylene glycol was not used as an indicator of gastric
emptying, to maintain parity with the majority of described methods in the literature,
- 118 -

and because of previously documented minimal transpyloric loss of this marker during
acid secretery studies(Hunter et al., 1989). Secretion during the first half hour of a basal
hour's collection is greater than in the second half hour, presumably due to the
stimulatory effect of swallowing the nasogastric tube, so only the second half hour
results were used, and these have been reported to show good
reproducibility(Hallenbeck et al., 197 6).
To elicit the peak acid output of the stomach, parietal cells were artifrcially stimulated
by intramuscular pentagastrin (Peptavlon ICI, 6 ¡tglkg). The drug was allowed to take
effect for 15 minutes, then four fifteen minutely specimens of gastric juices were again
collected by aspiration for one hour under maximally-stimulated conditions. The
samples were immediately filtered through gaulze into specimen containers. Peak acid
output (mmol/hr) was dehned as the sum of the 2 highest consecutive 15 minute
samples multiplied by 2.Inthis study, maximal acid output (defined as highest
observed acid output), or maximum acid output (MAO, defined as the output in the
whole hour after a stimulant) are not reported. For each 15 minute specimen the volume
(ml), pH and titratable acidity (mlWL) were measured:
. pH was measured using a pH meter.
o Titratable acidity was the number of mmol of 0.lN NaOH(Lavigne et a1.,1979)
added per litre of stomach content needed to raise the pH to 7.O(Baron, 1978).
. Acid output (mmol) was calculated as volume (mL) x titratable acidity (mmol/L).
- 119-

Gastric emotvinq studiesGastric emptying studies were performed on a separate occasion. The pigs were fasted,
and a l4 F tube was placed in the stomach through the oesophagostomy with the
animals awake and upright. Correct positioning of the tip of the tube in the stomach was
confirmed by a recovery test(Hassan and Hobsley, 1970). Low intermittent suction was
applied to the tube to empty any residual debris and the stomach lavaged with isotonic
saline until the return was clear. Mixing was performed by aspirating and re-injecting
the stomach contents with a 50 mL syringe for one minute, with a pumping action
performed at least 12 times.
The analytic method used was based on the double sampling technique of
George(George, 1968), extended with Beckers calculation procedure to correct for
gastric secretion and net test meal outflow(Beckers et al., 1988). This method shows a
high degree of correlation with Hunt's chloride technique(Hunt, 1974), which is used
for estimating gastric secretion. Non-nutrient isotonic test meals were used because
hyperosmolar and nutrient liquids can slow gastric emptying by feedback from
duodenal osmoreceptors(V/ilbur and Kelly,1973). Solid emptying was not addressed
because proximal gastric vagotomy is associated with near noÍnal levels of solid
emptying(Lavigne et al., 1979).
Samples of the dilute test meal and concentrated dye solutions were taken for
quantitative analysis. Liquid test meals consisting of 600m1 of isotonic saline containing
15 mglL of phenol red (20 mls of concentrated solution + 670 mls distilled water) was
administered through the tube, mixed with gastric contents, and an initial sample
immediately taken. High volume liquid test meals were used because larger volumes
provide more reproducible results by avoiding the small individual differences in
-t20-

emptying associated with recovery of small volumes(Gleysteen et al., 1976). 5 ml
samples were taken at2,5,10, 15, 20,30, and 40 minutes. on each occasion a sample
was taken, l0 ml of dye (500 mgll-) was added and mixed, and then a second 5 ml
sample was taken. To obtain the phenol red concentration an aliquot of every sample
was diluted 20-fold with a 0.25-0.5mol/L concentration NaOH/lr{aHCO3 buffer, and
measured on a spectrophotometer at 560 nm(Schedl,1966).
where:
Vsnb : volume of gastric contents before adding dye (ml)
Vtrru : volume of gastric contents after adding dye (ml)
Vir, : volume of dye added (ml)
Vtn : volume of test meal (ml)
CSnb : dye concentration in gastric contents before adding dye (mglml)
Ctrru : dye concentration in gastric contents after adding dye (mglml)
Cir, : dye concentration in volume of added dye (mg/ml)
Anb : amount of dye in gastric contents before adding dye (mg)
: Vsnb x Csnb
Ana : amount of dye in gastric contents before adding dye (mg)
: VSna x CSna
-t2t-

calculation of gastric volume: calculation of test meal volume:
, Ct" - Ct*VSnb: Vln xÇsm - Çs"r
Vt, Anu
A1n_r¡u
Ain-r¡r
A1n-z¡ux vtlAro
XAto
By measuring the phenol red concentration of every sample the test meal volumes at
each time point could be calculated, and gastric emptying could then be derived by the
change in test meal volume.
Assessment of gastro-oesophageal refluxOesophageal reflux was measured using static 8 hour ambulatory pH monitoring; longer
recording periods were not practically feasible. The lower oesophageal high pressure
zone was first localised by pull-through manometry. The pH probe (Monocrystant) was
then positioned 5cm proximal to this level, and pH recorded for 8 hours using a
datalogger (Digitrapper Mk II, Synectics Medical, Sweden). The pigs were partially
restrained in a metabolic crate throughout the study but were allowed to feed normally.
The pH data was analysed using Esophagram software (Synectics Medical, Sweden),
and a reflux score was derived representing the percentage of time that pH was below
4.O(Heij et al., l99l).
-122-
Operative procedures
On week 3 the operative procedures were performed, excepting the control group which
had no surgery. General anaesthesia was induced by animal house staff using
subcutaneous ketamine and inhalational halothane. Open HSV was performed by the
well-established technique(Goligher J.C. 1974) under supervision by a specialist upper
gastrointestinal surgeon.
The laparoscopic HSV was performed with a zero degree telescope inserted via a lQmm
umbilical cannula. Two additional 10mm working ports were inserted just above the
umbilicus in paramedian positions. A 5mm trocar was placed in the right subcostal
region to retract the liver, and a left flank trocar was used to apply tension to the
stomach. The avascular portion of the lesser omentum was divided to gain access to the
oesophageal hiatus. The peritoneum overlying the right crus and oesophagus was
dissected, allowing both vagal trunks to be identified. The anterior and posterior leaves
of the lesser omentum were then serially separated from the lesser curve of the stomach
to the left of the crow's foot in a manner similar to the open procedure. The
neurovascular structures were diathermied, or clipped and divided if sufficiently large.
The lowermost 5-7cm of oesophagus was then bared of any remaining nerve fibers
running onto the stomach. During laparoscopic HSV, an Endoscopic Congo Red Test
was used to show total denervation of the parietal cell mass(Donahue et al., 1987). An
endoscope was prepared by securing a I4F or l6F nasogastric tube by means of 3
rubber bands placed 5 cm apart connected to a 50cc Tooumi syringe. Three 500m1
basins were prepared containing:
l. Normal saline
2. 0.5% NaHCO3 (30cc of 8.4%o NaHCO3 diluted to 5O0cc(Schneider and Andrus,
-123-

1992)) + 0.3o/o Congo Red (3g in 500m1).
3. 2.0% NaHCO3 + 0.3% Congo Red
Because general anaesthesia depresses acid secretion, pentagastrin ("peptavlon" ICI)
íVglkgwas injected subcutaneously 15-20 minutes before the test(Donahue et al.,
1986). A preliminary gastric lavage was performed with saline if the first view of the
stomach shows food debris or particulate matter. The gastroesophageal junction was
tethered with a catheter to minimize the risk of acid reflux into the oesophagus, and the
duodenum was obturated by a laparoscopic bowel clamp. Two hundred ml of the 0.5%
NaHCO3 solution was injected into the stomach via the attached nasogastric tube. The
stomach was manipulated to ensure coating of the entire surface. The stomach was
aspirated via the tube and the tube bunged. If the entire gastric mucosa was coated the
time was noted and the test proceeded. If any of the surface remained uncoated, the
inigation/aspiration sequence was repeated.
Positive findings were defined as blackened areas seen within 2 minutes (indicating a
pH of < 3.0). In contrast successfully denervated areas secrete acid slowly enough to
delay the colour change for 8 to 10 minutes. If the entire stomach was black within 2
minutes, lavage was repeated with a 2Yo solution, to show a differenti al rate of secretion
between innervated and denervated mucosa.
In the sham laparoscopic group the stomach was mobilised by division of the lesser
omentum in an identical manner to the laparoscopic HSV, except no neurovascular
structures were divided.
-r24-
Statistical analvsisThe statistical method utilised was repeated measures analysis of variance, with
grouping factors of treatment (control, open HSV, laparoscopic gastric mobilisation and
laparoscopic HSV) and a within factor of time. Significant results were defined as p
values of 0.05 or less. Analysis was performed using SAS PC 6.04 statistical software
(SAS Institute Inc., Cary, N.C.).
4.1.3 Resu/fs
Clinical outcomeDuring the postoperative period 5 pigs died of gas bloat; 4had undergone open HSV
and one a laparoscopic gastric mobilisation. This is a well known veterinary condition
whereby the stomach became massively distended with air, and was refractory to
repeated attempts at decompression. One animal died from an adhesional small bowel
obstruction following an open HSV, and another died when a laparoscopically
mobilised stomach became strangulated in the thorax. No postoperative complications
were observed in animals that underwent laparoscopic HSV. Clinically, animals in the
laparoscopic HSV group recovered more quickly than those in the open HSV group,
and most of the former were back to a near normal diet by day 3.
Gastric acid outputTable 4 shows the statistical differences between the pre and postoperative gastric acid
output values for each of the 4 groups. Because the pigs grew vigorously over the 8
week study period, postoperative values were corrected by a factor corresponding to the
mean weight gain observed in the control group. Basal acid output results were analysed
on a logarithmic scale to achieve a normal distribution of the values, thereby increasing
the power of the statistical test. Basal acid output was significantly reduced after both
open and laparoscopic HSV (p : 0.005 and p :0.02 respectively), but was statistically
-t2s-

unchanged in the control and sham laparoscopic gastric mobilisation groups, as
illustrated by Figure 9. None of the groups showed a significant reduction in
postoperative peak acid output
Table 4: Difference between the pre and postoperative gastric acid output values
GROUP BASAL ACID OUTPUT (log) PEAK ACID OUTPUT
CTRL p:0.67 p: 1.0
SHAM p:0.19 p:0.71
OPEN p:0.005 p:0.62
LAP p:0.02 p:0.94
Figure 9: Basal acid ouput
D Preop
¡ Postop.
IEE
ê
!
3.5
3.0
2.5
2.O
1.5
1.0
0.5
0.0
CTRL SHAM OPEN LAP
-126-

Gastric emotvinoPre and postoperative gastric volume changes over time are represented in Figures 10
and 11 respectively, and Table 5 indicates the statistical difference between these pre
and postoperative values, however only significant results are reported. Following open
HSV, postoperative liquid gastric emptying was significantly impaired at 1 and 30
minutes (p: 0.04). The open HSV also caused significant interference with gastric
emptying at 10 minutes when compared with controls. Laparoscopic HSV was not
observed to significantly interfere with liquid gastric emptying. Control animals showed
a significantly delayed "postoperative" gastric emptying at 2 minutes, limiting the
inferences that can be drawn from the remaining 2 minute results listed in Table 5.
Table 5: Difference between pre and postoperative gastric emptying values
GROUP TIME p
OPEN t: 1 min p:0.04
OPEN t:30 min p:0.04
OPEN vs CTRL t: l0 min p:0.04
CRTL t:2min p:0.03
SHAM vs CTRL t:2min p:0.03
OPENvs CTRL t:2min p:0.02
-127-

Figure 10: Preoperative liquid gastric emptying
JE
E
ã,9
üño
1
Et
.E
o
800
7(X)
600
500
400
300
200
100
llME (min!)
TIME (n¡ns)
15
t5
+SHAM.. + -.OPEN
- :---LAP+CTRL
+SHAM..G- OPEN- o. LAP
+CTRL
0
2 't0
l0
20 30
30
40
40
Figure 11: Postoperative liquid gastric emptying
800
700
600
500
400
300
200
100
a
0
2
-128-
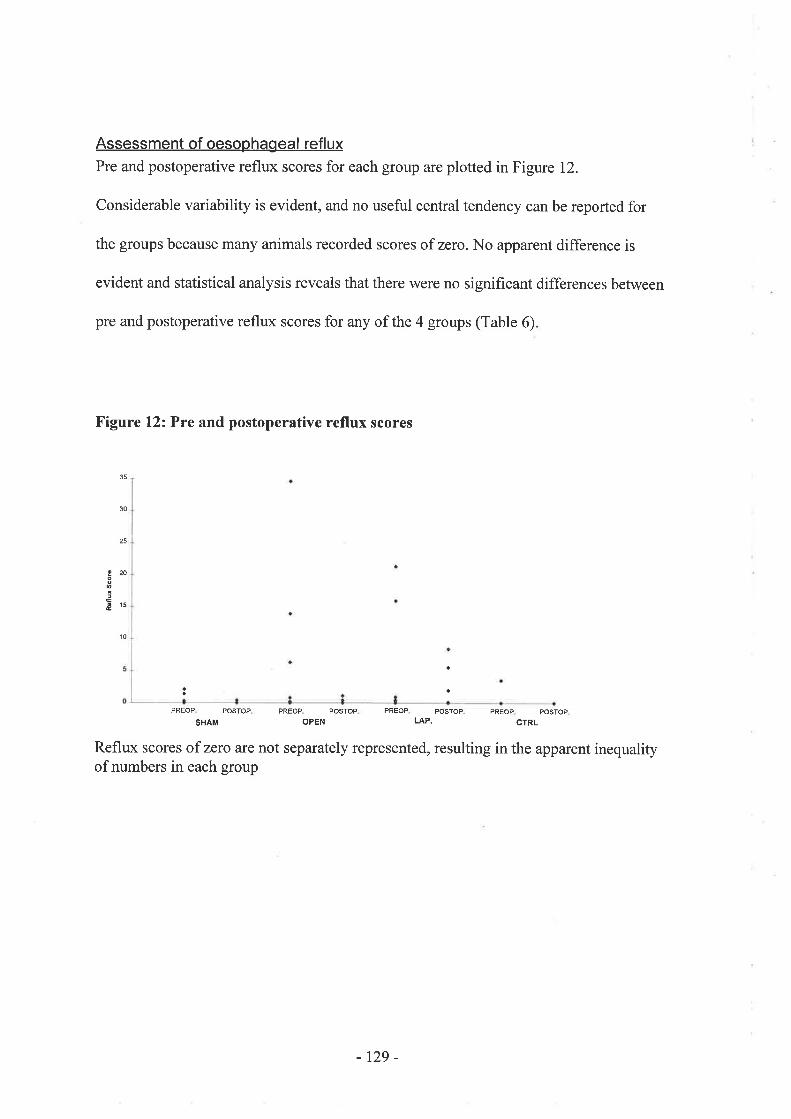
Assessment of oesophageal refluxPre and postoperative reflux scores for each group are plotted in Figure 12.
Considerable variability is evident, and no useful central tendency can be reported for
the groups because many animals recorded scores of zero. No apparent difference is
evident and statistical analysis reveals that there were no significant differences between
pre and postoperative reflux scores for any of the 4 groups (Table 6)
Figure l2z Pre and postoperative reflux scores
30
25
E20o
&15
10
PREOP POSTOP PREOP POSTOP PREOP POSTOP PREOP POSTOP
SHAM OPEN LAP. CTRL
Reflux scores of zero are not separately represented, resulting in the apparent inequalityof numbers in each group
-129-

Table 6: Difference between pre and postoperative reflux scores
GROUP p
CTRL p:0.91
SHAM p :0.8
OPEN p: 0.22
LAP p:0.34
4.1 .4 Drscussion
Gastric physiological studies endure as the only objective criteria by which the new
laparoscopic vagotomy techniques can be validated to be as good as the existing
procedures. Because laparoscopic vagotomy has only been technologically feasible for
5 years, the follow-up of operated patients is necessarily too short to allow comparison
of the clinical efficacy of the procedure with the documented long-term outcome of
open HSV. In addition, the impact of medical therapy on peptic ulcer disease, notably
the development of successful regimens for the eradication of Helicobacter pylori and
proton pump inhibitor drugs, have resulted in a considerable diminution in the numbers
of patients referred for surgery. Furthermore, the collective experience of laparoscopic
vagotomy within specialist centres has been diluted by the plethora of alternative
techniques competing to become the procedure of choice. For example, selected reports
from current literature reveal Dubois promoting thoracoscopic truncal vagotomy in a
series of 2l patients(Dubois,1994), Katkhouda supporting laparoscopic posterior
truncal vagotomy and anterior seromyotomy in a series of 90 patients(Katkhouda et al.,
1994), Dallemagne advocating laparoscopic HSV in a series of 35 patients(Dallemagne
-130-

et al., 1994), Kum and Goh reporting the use of anterior HSV and posterior truncal
vagotomy in 6 patients(Kum and Goh, 1992), and Hannon describing his technique of
linear stapled laparoscopic anterior seromyotomy and posterior truncal
vagotomy(Hannon et al., 1993).
The use of gastric secretory studies for the physiological assessment of vagotomy is a
well-established technique, despite ongoing criticism. When performed routinely after
vagotomy they serve as a functional measure of the degree of parietal cell denervation
which represents the technical efficacy of the surgery. After open highly selective
vagotomy, the reduction in acid output is about 80 - 90% for basal, and 50 - 60%o for
pentagastrin-stimulated acid secretion, influenced however by a leaming curve effect
attributable to the technical difficulty of the operation whereby substantially lower acid
outputs have been reported following vagotomies by specialist compared with novice or
general surgeons(Baron, 1978). Basal acid output may be a more relevant determinant
of the quality of vagotomy than stimulated acid output, as it reflects the period of
gastric secretion when acid may act on the stomach unbuffered by food. Historically, an
80o/o reduction in basal acid output has been considered proof of adequate
vagotomy(Nylamo, 1987). More recently, a reduction in basal acid output of < 80% has
been reported to accurately predict recurrent ulceration after open highly selective
vagotomy(Cohen et al., 1993).
The two largest published reports(Cadiere et al., 1994; Dallemagne et al., 1994) of
laparoscopic HSV have observed the procedure to be very safe with no postoperative
morbidity or mortality amongst a total of 68 patients, and complete ulcer healing was
observed on endoscopy for all but 3 patients. However gastric secretory studies were
-131 -

performed in only 16 of the 68 patients, and no attempt was made to statistically
analyse whether a significant decrease in acid secretory response had been achieved. No
human controlled trials have compared the efficacy of laparoscopic HSV against the
open operation. One controlled animal study assessed the completeness of vagotomy at
2 weeks by killing the animals and mapping innervated gastric mucosa with Congo
Red, a non-standard technique which is unlikely to be applicable to future human
comparisons(Schneider et al., 1992).In this study, both open and laparoscopic HSV
resulted in a signif,rcant reduction in basal acid output, but such changes were not
evident in the 2 control groups. Although signihcant reductions in peak acid outputs
were not observed in any of the groups, other investigators have reported that pigs
commonly have a paradoxical response to agents that cause hypersecretion in humans,
such as pentagastrin(Fitzgibbons, 1994).
Gastric emptying of liquids is controlled by the fundus of the stomach. After vagotomy,
receptive relaxation of the fundus is abolished resulting in higher intragastric pressures
and faster liquid emptying(V/ilbur and Kelly, 1973). The situation with solids is
different. Solid gastric emptying is regulated by the antrum and pylorus rather than the
fundus. Parietal cell vagotomy is associated with near normal levels of solid emptying
because the vagal innervation to the pylorus and antrum is preserved(Lavigne et al,
1979). To date, no other studies have quantitated the effect of laparoscopic HSV on
gastric emptying. In this study open HSV caused significant interference with gastric
emptying at 1 and 30 minutes, and also at 10 minutes when compared with controls, but
no impairment of gastric emptying was evident following laparoscopic HSV.
-t32-

It remains controversial whether or not HSV precipitates gastro-oesophageal reflux. A
number of theories have been proposed to explain why this might occur. It now seems
clear that HSV causes no signihcant changes in resting sphincter pressure, but that there
may be a loss of the adaptive response of the sphincter when intra-abdominal pressure
rises(Martinoli, 1982). Mobilisation of the stomach during HSV also results in a degree
of gravitational dependence which may alter the angle of His(Temple and McFarland,
I975). No significant differences between pre and postoperative acid reflux scores for
any of the 4 groups were observed in this study. Given the limitation of the pH
recording duration, these results suggest that laparoscopic HSV is unlikely to precipitate
gastro-oesophageal reflux.
In conclusion, this study observed that domestic white pigs were prone to gas bloat after
laparotomy, but in contrast laparoscopic procedures were well tolerated. Laparoscopic
HSV was as effective as its open counterpart in reducing basal acid output, and
laparoscopic HSV was superior to open HSV because it did not interfere with liquid
gastric emptying. Neither open nor laparoscopic HSV were observed to precipitate
gastro-oesophageal reflux. This data suggests that the continued use of laparoscopic
HSV in clinical practice is appropriate. In the future, the methodological protocol
described for gastric secretory studies should be routinely applied to assess the
physiological outcome of laparoscopic vagotomy in human patients.
-133-

4.3 Gastrostomy
4.3.1 lntroductionFollowing the advent of percutaneous endoscopic gastrostomy (PEG) for patients
requiring long-term enteral access or gastric decompression, it has replaced surgical
open gastrostomy (OG) as the preferred technique. Retrospective comparisons have
reported a significantly lower mortality and morbidity with PEG compared with open
gastrostomy(Sali et al., 1993 ; Ponsky and Gauderer, 1989). However a randomised
prospective trial of the two methods reported equivalent morbidity and mortality
providing both are performed under local anaesthesia(Stiegmann et al., 1990), but this is
less often possible with OG than PEG and the results may not reflect the clinical
experience of other centres. Percutaneous gastrostomy can also be performed using a
Seldinger technique under radiological guidance, and although less popular it has
achieved similar results to endoscopic gastrostomy(Halkier et al., 19S9).
Under certain circumstances percutaneous gastrostomy is contraindicated or may fail.
These situations occur with a reported incidence of 3o/o and 5Yo respectively(Stiegmann
et al., 1990), and until recently OG has been the only alternative. The documented
complications of OG, and the knowledge that most patients excluded from percutaneous
gastrostomy are poor surgical candidates combine to make OG an unattractive
proposition. Two recent developments have changed this situation.
In 1990 Mansberger described a technique of combined endoscopic and surgical
placement of a gastrostomy under local anaesthesia when PEG is
contraindicated(Mansberger and Kavouklis, 1990). General anaesthesia nor a
laparotomy is required. The gastrostomy is placed under direct vision through a2cm
abdominal incision using endoscopic guidance, and secured by a gastric purse-string
-r34-

and suture fixation to the abdominal wall. This technique reportedly eliminates
unsatisfactory adhesion between the gastric serosa and anterior abdominal wall, a
complication which is frequently fatal(Ditesheim et al., 19S9).
With the rapid acceptance of laparoscopic upper gastrointestinal surgery a second
minimally invasive alternative to percutaneous gastrostomy has emerged. Laparoscopic
gastrostomy was first described in 1991(Edelman and Unger, I99l ; Shallman, l99l),
and several recent variations to the technique have been reported(Cossa et al., 1992;
Haggie, 1992; Mr.phy et al., 1992; Duh and V/ay, 1993b). These methods use an
adaptation of the Russell PEG technique(Russell et al., 1984) by direct puncture of the
stomach either immediately by a laparoscopic port or by a peel away sheath following
progressive dilatation of a needle tract. All describe suture fixation of the stomach to the
anterior abdominal wall under direct vision with the sutures tied over skin bolsters.
Accurate fixation of the stomach to the anterior abdominal wall under direct vision is a
major advantage of laparoscopic gastrostomy. This makes it safer than radiologically-
placed percutaneous tubes in patients with upper aero-digestive obstruction preventing
PEG. Although combined endoscopic and surgical placement of a gastrostomy can also
overcome conditions which hinder satisfactory adhesion of an endoscopically placed
tube, the use of laparoscopy is within the realm of the majority of General Surgeons and
does not rely on the availability of an endoscope or a trained endoscopist. Evidence is
accumulating to indicate that gastroesophageal reflux is precipitated or worsened by
gastrostomy tube feeding(Jarnagin et a1^, 1992; Grunow et al., 1989). In the recent
Australian study, two patients died following continued aspiration after placement of
PEG tubes(Sali et a1.,1993). This has lead to the suggestion that jejunostomy feeding
may be preferable for patients at risk of aspiration pneumonia(Gottfried and Plumser,
-r35-
1984), or that prophylactic fundoplication be combined with gastrostomy tube
placement(Bui et al., 1989). If a laparoscopic approach is used, the surgeon can choose
between either of these measures which can be employed quickly and easily during the
procedure. Laparoscopic jejunostomy may well evolve as the preferred measure in
patients at high risk for aspiration of gastrostomy feeds, and a recent report detailed
excellent results using this technique(Duh and W'ay, I993a).
AimIt was hypothesized that laparoscopic gastrostomy could offer a viable alternative to
enteral access after failed percutaneous endoscopic gastrostomy (PEG). When enteral
access by PEG is contra-indicated, it was proposed that laparoscopic gastrostomy could
present a less invasive alternative than open gastrostomy (OG), and could be easily
performed by General Surgeons with basic laparoscopic skills without the assistance of
an endoscopist.
4.3.2 MethodsThe procedure was performed on a previously healthy l5 year old female cyclist who
sustained severe head injuries after being struck by a car. Over the succeeding
hospitalisation pharyngeal inco-ordination required prolonged nasoenteric feeding. pEG
was attempted but was unsuccessful as the stomach was situated entirely above costal
margin and was unable to be apposed to the anterior abdominal wall.
The operation was performed under general anaesthesia four days after the failed pEG.
The procedure commenced with the insertion of a 10-12mm umbilical port into the
peritoneal cavity using an open technique, followed by CO2 insufflation to a pressure of
5mm Hg. The telescope-camera assembly was inserted through the umbilical port and
under direct vision a second 10-l2mm and a third 5mm port were placed in left and
-136-

right paramedian positions respectively. A fourth 5mm port was placed in the right
upper quadrant. The anterior wall of the body of the stomach was grasped with
Babcock forceps and approximated to a convenient position beneath the left anterior
abdominal wall, above which a2mm incision was made in the skin of the left upper
quadrant and a subcutaneous pouch fashioned. Four 2/0 Vicryl sutures on 36mm
curved atraumatic needles were passed through the anterior abdominal wall into the
peritoneal cavity where they were grasped with endoscopic needle holding forceps
(Figure 13). These sutures were were then placed at four appropriate anchor points
through the gastric wall and passed back out through the anterior abdominal wall. A
lcm gastrotomy was made between the sutures using the coagulating diathermy hook.
A24F silastic Foley catheter was passed through the anterior abdominal wall into the
peritoneal cavity mounted on a catheter introducer and directed into gastric lumen under
laparoscopic visualisation (Figure 14). The balloon was inflated with 3Omls of normal
saline and traction on the catheter brought the stomach into close apposition with
anterior abdominal wall. The Vicryl sutwes were then hand tied extra-corporeally with
the knots situated in the subcutaneous pouch. At completion of the operation the
pneumoperitoneum was released while the gastrostomy was under direct vision. The
camera and all ports were removed, and the left upper quadrant skin incision closed
with subcuticular 3/0 Prolene. The catheter was fixed to the skin with a temporary 210
silk suture. The fascial port sites were closed with 3/0 Vicryl and the overlying skin
with steri-strips
-137 -

Figure 13: The anterior wall of the body of the stomach grasped by Babcockforceps, with transabdominal sutures placed by an endoscopic needle holder.
-138-
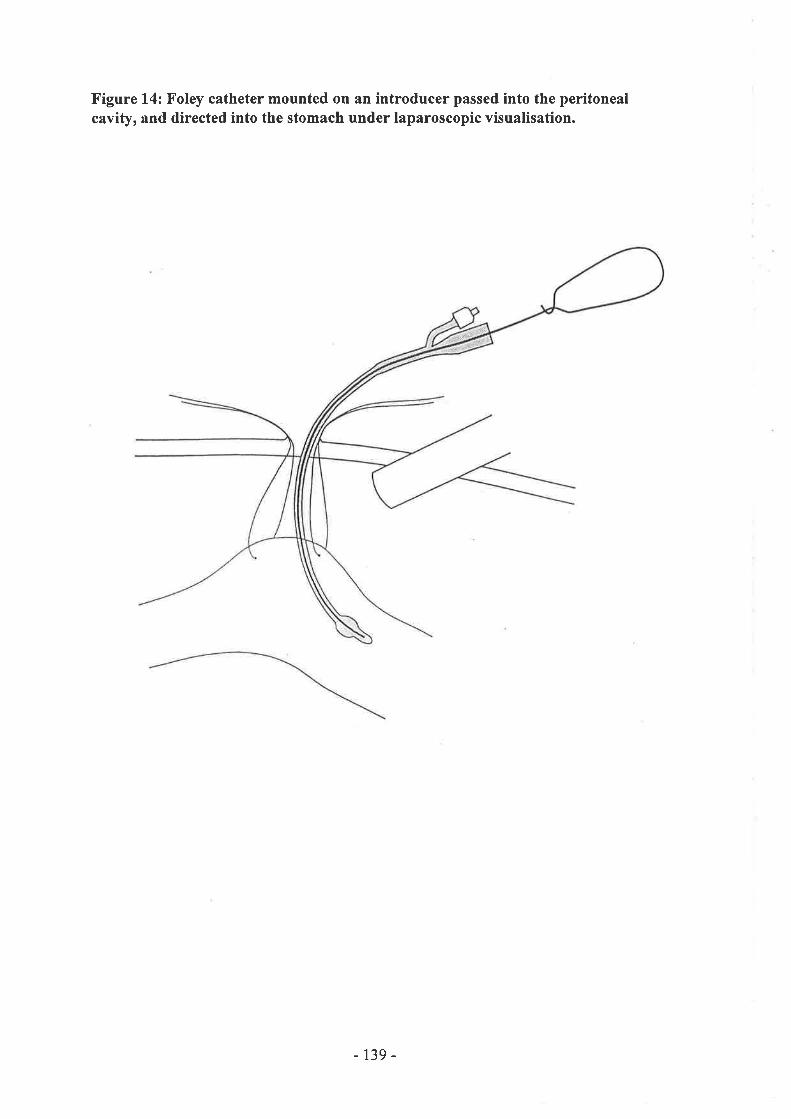
Figure 14: Foley catheter mounted on an introducer passed into the peritonealcavity, and directed into the stomach under laparoscopic visualisation.
-139-
4.3.3 Resu/ús
Post-operatively the gastrostomy remained patent when flushed with 20mls of normal
saline four times a day. By day four the patient's bowel sounds were present and
gastrostomy feeding was commenced. The patient's post-operative progress was
uncomplicated, and the gastrostomy continued to function well following discharge
from hospital to a rehabilitation institution.
4.3.4 Drscussion
Gastrostomy for enteral feeding or gastric decompression has traditionally been
performed by open surgery. Recent reports indicating a lower morbidity and mortality
rate for PEG compared with OG(Sali et al., 1993 ; Ponsky and Gauderer, 1989) have
justif,red the more minimally-invasive approach that percutaneous techniques provide.
PEG is not immune from complications, in particular as a result of insecure fixation of
the stomach to the anterior abdominal wall(Ditesheim et al., 1989), and post-procedural
reflux and aspiration pneumonia(Jamagin et al., 1992 ; Grunow et al., 1989). In
situations where PEG is contraindicated or has failed, laparoscopic gastrostomy can
offer a minimally-invasive alternative.
Curved needles were used to place fixation sutures in the case reported. These were not
ideal as some difficulty was encoutered passing them accurately out through the anterior
abdominal wall. However the normal straight needles as would be used for subcuticular
sutures are also not useful as they are too long to easily manipulate laparoscopically,
and dedicated laparoscopic needles are too short to pass through the anterior abdominal
wall in all but slim individuals. The use of T-Fasteners (Ross Laboratories, Columbus,
Ohio) to retract and anchor the stomach is an innovative solution to this unique
diffrculty(Duh and V/ay, 1993a ; Duh and Way, 1993b). These devices consist of a
-r40-
metal T-bar lcm long, lmm in diameter with a nylon suture attatched to its centre. They
are introduced percutaneously into the enteric lumen by a slotted needle and dislodged
by a stylet, after which both needle and stylet are removed. Until such equipment
becomes locally available, the choice of the appropriate suture needle will have to be
made on a case-by-case basis.
In this patient it was technically easier to to approximate the stomach to the anterior
abdominal wall under laparoscopic control than at PEG, perhaps related to the more
comprehensive view of intra-abdominal landmarks offered by the laparoscope making it
easier to choose an appropriate location beneath the costal margin. Four-point suture
fixation and balloon traction ensured firm apposition of the gastric mucosa and anterior
abdominal wall, but the addition of a gastric purse-string could add a further measure of
safety. The use of a skin incision and subcutaneous pouch into which the extra-
corporeal knots were snugged is a minor technical improvement over previous
descriptions where skin bolsters \ilere used, risking pressure necrosis should the sutures
be tied under excess tension. A further technical modification employed in the reported
case was to minimize the potential for damage to adjacent structures by not puncturing
the stomach by a direct percutaneous route, but rather via a small gastrotomy made with
the coagulating hook.
It is concluded that laparoscopic gastrostomy is a viable option when PEG is
contraindicated or has failed. In some respects it provides benefits surpassing PEG,
because poor apposition between the stomach and anterior abdominal wall can be
prevented, and prophylaxis against reflux and aspiration pneumonia can be easily
incorporated into the procedure. However, whether it is better than OG remains to be
proven in randomised controlled trials, because laparoscopic gastrostomy has to be
-t4t-

carried out under general anaesthesia while OG can be performed under local
anaesthesia.
-t42-
5. ASSESSMENT OF ROUTINE LAPAROSCOPIC PROCEDURES
5.1 Historical development of herniorrhaphy
5.1.1 Traditional methods of inguinal hernia repairAn extensive review of traditional methods of inguinal hernia repair is beyond the scope
of this work, however an introduction to some differentiating concepts in the
management of the posterior inguinal wall is relevant to place the development of
laparoscopic hernia repair in perspective.
Bassini
From the time of his original description in 1887, Bassini's operation has become a
standard for inguinal hernia repairs. Perhaps his greatest contribution was to be the first
to suggest opening the neck of the inguinal canal to deal with the neck of the sac at the
deep inguinal ring. Relatively recently, new English translations of the original
operation of Bassini were published from his original Italian manuscript and subsequent
treatise in German 3 years later in 1890(Brown et al., 1966). These indicate that Bassini
stitched the triple layer of internal oblique, the transversus abdominis muscle, and the
transversalis fascia to the isolated posterior border of the inguinal (Poupart's) ligament
between the pubic tubercle medially and the spermatic cord laterally. It is this stage of
the operation that is most commonly associated with the name of Bassini.
Since then, there have been many modifications to this repair, predominant being the
descriptions by Halsted(Halsted, 1893 ; Halsted, 1903), McVay(McVay and Anson,
1942; McVay, 1989), and from the Shouldice Hospital(Shearbum and Myers, 1969).
These techniques share the same time-honoured principles of isolation and excision of
the hernial sac with reconstruction and reinforcement of the posterior wall of the
inguinal canal.
-143-
Halsted
In 1893, Halsted himself admitted that his operation and that of Bassini were nearly
identical, but elucidated some minor differences(Halsted, 1S93). Bassini always brought
the cord out through the deep inguinal ring, but the position that Halsted selected was
determined by the condition of the muscles. In contrast to Bassini, Halsted advocated
reducing the bulk of the cord by excising superfluous veins. Furthermore, he initially
described allowing the cord to remain in the subcutaneous plane, preferring not to
reapproximate the external oblique aponeurosis by sutures as Bassini described,
however by 1903 he had incorporated this step in his repair(Halsted, 1903).
McVav lCoooers lioament reoeir)An excellent description of the technique and results of the McVay operation (Cooper's
ligament repair) was published by Rutledge in 1988(Rutledge, 1988). Over a 25 year
period he performed this operation on942 patients and had personally followed up 906
repairs in 7 47 patients for an aveÍage of 9 years. For primary repairs he observe d a I .9Yo
recurrence rate. He concluded that a Cooper's ligament repair provides a strong
posterior inguinal wall and repairs all of the defects that can occur in the groin.
McVay's basic anatomical concept is that for all practical pu{poses, groin hernias are
concemed only with the transversus abdominus layer (muscle, aponeurosis, and
fascia)(McVay, 1989). The normal insertion of these elements of the posterior inguinal
wall is Cooper's ligament, and hence the rationale for using this as the anchoring
structure in the repair of groin hernias in which the posterior wall has been damaged
(direct, large indirect, or femoral). Proponents of techniques that reconstruct this
specific area argue that Bassini's repair and variants thereof are unanatomical because
all layers of the posterior wall are brought down (often under tension) to the inguinal
-t44-

ligament, which many believe to be solely the site of insertion of the extemal oblique
aponeurosis(Glassow, 1986). These points are considered critical to minimising the
recuffence rate, and are ignored by Bassini-type repairs.
The essential differentiating features of the operation are that the posterior wall of the
inguinal canal is incised and Cooper's ligament is dissected free. Obturator and external
spermatic tributeries of the inferior epigastric artery are divided, and any attenuated
conjoint tendon is resected. All preperitoneal tissues are imbricated, and the femoral
canal is closed with sutures. The repair is constructed with intemrpted sutures being
placed between the transversus abdominis arch and Cooper's ligament as far laterally as
the femoral vein. The repair is continued laterally between the transversus abdominis
arch and the inguinal (Poupart's) ligament until the cord exits laterally and obliquely
out the internal ring.
ShouldiceThe Shouldice hernioplasty originated from the Surgeon and Hospital of the same name
in Toronto, Canada, and had evolved to its present form by 1950. Although it has been
called the modern equivalent of the original Bassini operation(Wantz,1989), it owes
perhaps greater similarity to the McVay technique because it shares the same
recognition of the basic importance of reconstructing the defective transversalis fascia.
Vital to the understanding of this operation is that when the posterior inguinal wall is
divided, two flaps of transversalis fascia result, an upper and lower(Glassow, l936). A
total of four lines of continuous nonabsorbable sutures are then used in the repair of the
posterior inguinal wall. The f,trst suture line begins at the pubic tubercle and ends
medial to the internal ring, approximating the free upper edge of the lower transversalis
flap underneath the upper flap, which then overlaps it. The second suture line is a
-145-
continuation of the first, reversed at the internal ring, attaching the free edge of the
upper transversalis flap to the shelving surface of the inguinal (Poupart's) ligament. The
third suture line commences with a new thread at the internal ring and brings the
internal oblique and transversus abdominis muscles down to the inguinal ligament. The
fourth suture line is a continuation of the third, reversed at the pubic bone, to reinforce
these same structures to one another at a slightly more superficial level.
Glassow reported on 12 548 repairs conducted at the Shouldice Hospital between 1954
and 1974, and cited a recurrence rate of only l.l % for primary repairs(Glassow, l9S6)
The same publication included a summary of seven other series all using the same
technique with at least 10 year follow-up, and reported a mean recuffence rate of 1.5 %
from 1l 809 patients
LichtensteinLichtenstein and colleagues from Cedars-Sinai Medical Centre in Los Angeles contend
that all of the abovementioned repairs share the common disadvantage of tension on the
suture line(Lichenstein et al., 1989). They believe that this is the eventual cause of
postoperative disruption, and is the prime aetiology of hernia recrrrrence. In 1989, they
described a technique of tension-free hernionhaphy(Lichenstein et aL.,1989). In this
repair, the posterior inguinal wall is dealt with by overlaying a suitable size of
polypropelene mesh. The lower edge is sutured to the lacunar ligament proceeding
laterally along the inguinal ligament beyond the intemal ring. A slit in the mesh at this
site allows the emergence of the cord. The superior edge of the mesh is sutured to the
rectus sheath and conjoint tendon. The lateral tails of the mesh are fixed to the inguinal
ligament by a single suture.
-146-

Using this approach, the usual approximation of aponeurotic tissue under tension is
avoided. Furthermore, the technique is simple, quick, and requires less dissection
making it less painful and suitable for local anaesthesia. In a subsequent paper,
Lichtenstein's group reported a recuffence rate of only 0.13 % in a series of 1552
consecutive, unselected, primary hernia repairs(Schulman et a1.,1992). These excellent
results were coffoborated by four other series cited in the same paper, where an overall
recuffence rate of 0.22 o/o and infection rate of 0.03 %o was observed from amongst 3019
operations
Preoeritoneal repairs with and without mesh
The definitive technique for preperitoneal herniorrhaphy was first described by Cheatle
in 192O(Cheatle,1920), and despite significant contributions by Henry and McEvedy, it
was not popularised until the work of Nyhus and Condon in the 1960's(Read, 1989)
This approach can be utilised for a variety of repairs, including suture, fascial graft,
iliopubic tract, or Cooper's ligament techniques. It has gained wide acceptance for its
particular suitability to the management of recurrent or strangulated hernias.
In the classic description by Nyhus(1.{yhus et al., 1960), after entering the preperitoneal
space through a transverse incision, a complete view is obtained of the posterior
inguinal wall from behind. The peritoneal sac can be dissected, or simply divided and
left in-situ. Sutures are then placed between the transversus arch superiorly and the
iliopubic tract inferiorly depending on the location of the defect. Using an identical
technique for the repair of 248 consecutive first-time recurrent hernias, Greenberg
reported a I.7 Yo recurrence rate within 5 years(Greenberg, 1987)
More recently, the use of polypropelene prostheses to buttress the posterior wall of the
inguinal canal has been reported using a preperitoneal approach. Nyhus placed a tai-
-147 -
lored piece of mesh as part of a preperitoneal repair of recurrent defects, reporting a 1 .7
o/o re-recurrence rate in 115 hernias over a 10 year period(Nyhus et al., 1988). Stoppa
and'Warlaumont also described a technique of preperitoneally placed polyester mesh
prostheses which are tacked to the posterior wall of the inguinal canal(Stoppa and
Warlaumont, 1993). This approach has the advantage of covering the hernial defect as
well as adjacent normal tissue beyond the limits of the defect, with intra-abdominal
pressure creating an effrcient means of fixing of the mesh over the site of the hernia,
rather than by the apposition of tissues.
5.1.2 Laparoscopic methods of inguinal hernia repairThe first human laparoscopic herniorrhaphy was performed by Ger (Ger, 1982) by intra-
abdominal stapling of the neck of the hernial sac. Laparoscopic herniorrhaphy tech-
niques subsequently evolved into two main groups; plug or patch repairs. Many
surgeons have since abandoned the plugging techniques because ofthe high recurrence
rate. Patch repairs remain popular, and three different types have been described; trans-
abdominal intraperitoneal, transabdominal prepreperitoneal, and extraperitoneal.
A plethora of publications considering the merits of laparoscopic hernionhaphy are now
available, however at the time of conception of this work reports of laparoscopic
herniorrhaphies in humans had been few with the number of patients undergoing
surgery and the follow up period usually being quite limited. Enough evidence had
accumulated to substantiate the alleged advantages of reduced post-operative
pain(Salerna et al., l99l ; Corbitt, l99I), shorter hospital stay and a more rapid return
to work(Dion and Morin, 1992; Salerna et al., I99I ; McKeman and Laws, 1993 ; Dion
and Morin, 1992), however there had not been any published randomised controlled
trials comparing the laparoscopic technique with a conventional open repair. There still
-148-
remains no published randomised controlled trial investigating the increasingly popular
laparoscopic extraperitoneal hernia repair. Furthermore, while open hernia repair as a
day surgical procedure was well established in many centres, the place of day surgery in
laparoscopic hernia repair had not been critically assessed.
Laparoscopic liqation of the neck of the sacIn 1982, Ger developed a technique whereby incidental groin hemiae found at the time
of laparotomy for other intraabdominal conditions could be dealt with by closing the
peritoneal opening with clips(Ger, 1982). He treated 14 patients in this manner, and
followed them up for periods ranging between 26 to 44 months. Only one recunence
was noted. The success of this method led to an experimental study designed to test the
feasibility of this technique in the laparoscopic environment. Fifteen beagle dogs with
congenital indirect inguinal hernias were operated on, 12 laparoscopically(Ger et al.,
1990). In addition to the usual video-laparoscopy setup, a customised combination
l2mm stapler with extendable forceps was developed by the author to facilitate the
procedure (Herniastat, Innovative Surgical Devices,Westbury, NY). This is used to pick
up the edges of the hernial opening, approximate them, and apply 14mm titanium
staples of 0.5mm in diameter. Peritoneum, subperitoneal tissue, and transversalis fascia
are approximated; the number of staples placed depends on the size of the hernial
orifrce. In all 12 dogs operated on the hernia was cured. Examination of en-bloc
inguinal specimens showed that if the staples were properly applied, they sank below
the peritoneum and disappeared from view, whereas superficial application resulted in
staple migration and loss of effective closure.
Ger and colleagues believe this technique is effective for small indirect hernias,
particularly in young adult and paediatric patients. For larger indirect hernias, and other
-r49-

types, they advocate supplementing the repair by mesh insertion into the sac. They
caution that if too much mesh is placed in the sac, problems of discomfort and an
externally palpable mass are manifested. If the mesh protrudes into the abdominal
cavity, it may cause intestinal perforation or adhesional obstruction. In their most recent
paper, Ger had closed 31 hernias with satisfactory results in27 instances(Ger et al.,
1993). On the basis of these results, the authors believe laparoscopic hemia repair offers
a rapid recovery and earlier retum to work with far less discomfort, and the highest
possible ligation of the sac, although no objective comparative data is provided to
support these assertions. By not dissecting the inguinal canal, they also suggest the risk
of ischaemic orchitis and entrapment neuropathy is diminished. However, they qualify
their assertions by highlighting the potential disadvantages incurred by the inherent
dangers of laparoscopy, and the unknown long-term recurrence rate.
A novel technique for cure of indirect hernias by laparoscopic closure of the internal
ring has been described by Geraghty (Geraghty et al., 1994). They use a hollow J-needle
inserted percutaneously, which is directed through the superior and inferior margins of
the deep ring under laparoscopic guidance. An 0 nylon suture is passed through the
needle, which is subsequently withdrawn, and the thread is tied extemally. Three
sutures are usually sufficient to close the deep ring completely. This technique was used
successfully in25 consecutive patients, with no recurrences over 8.5 months follow-up
and one instance of urinary retention. The authors laud the technique because it is
simple, inexpensive, and does not require clips or prosthetic material.
Techniques of ring closure have been critcised for the requirement that patients restrict
activities for 6 weeks to allow the scar to strengthen, obviously nulliÛring return to
work advantages conferred by laparoscopy(Anegui et al., 1993). Furthermore, other
-150-

defects in the posterior wall may be missed because the inguinal floor has not been
completely inspected. It seems the wheel may turn full circle, and this technique will
find a place to close incidentally found small indirect hernias during other laparoscopic
procedures.
Laparoscopic plug (t small mesh) repairThe laparoscopic mesh plug repair was developed by Schultz, who was also the first to
report a series of laparoscopic hernionhaphies in 1990(Schultz et al., 1990). The
peritoneum adjacent to the indirect hernial sac was incised, and the sac dissected by a
laser fibre. The indirect defect was plugged with rolls of polypropylene mesh covered
by two or three fuither small flat pieces of mesh until the defect was filled. The
peritoneum was re-approximated with clips. In the initial series, 20 hernia repairs were
followed for 3 - 11 months, with one recuffence attributed to an unrecognised direct
component. In a subsequent presentation of their results, six direct recurïences were
detected in the first 50 patients(Cheslyn-Curtis and Russell, 1993), leading the authors
to revise their technique by including additional placement of a large flat mesh
fashioned to cover the entire inguinal area.
Corbitt was another early adopter of laparoscopic mesh plugging techniques, publishing
a series in 1991 of 20 inguinal hernia repairs performed as day cases(Corbitt, 1991). He
used a modified mushroom-shaped mesh plug with an attached square patch laid across
the intemal ring to act as a stopper to prevent plug migration. Although initially
enthusiastic because patients were pain-free and returned to normal activity the first
post-operative day, after following these patients for up to two years there was a greater
than l5 o/o recurrence rate(Cheslyn-Curtis and Russell,1993).
-151 -

Schultz and Corbitt have since abandoned this technique in favour of transabdominal
preperitoneal mesh placement. The unacceptably high incidence of recurrence was
explained by limited dissection of the inguinal floor so missing concomitant hernias. A
recent review of the place for plug repairs suggested that it should be confined to use in
recurrent direct or indirect hernias up to 3.5 cm in diameter, primary femoral hernias,
and recurrent femoral hemias(Schulman et al., 1994).
Laparoscopic transabdominal intraperitoneal (onlay) patchThe next development in laparoscopic hemiorrhaphy was in retrospect a retrograde step
Once it had become apparent that preperitoneal plug repairs must be supplemented or
superseded by preperitoneal mesh patches, some groups questioned the need for
extensive preperitoneal dissection and suggested it could be eliminated and the same
result achieved by simply affixing an onlayed prosthesis directly on the peritoneum.
This was expected to result in a simpler and quicker operation, less morbidity and
consequently improved functional outcome for the patient. However some significant
disadvantages have become evident. Because the mesh is anchored mainly to the
peritoneum, the entire complex can slip into the hemia defect. Another well-recognised
problem caused by intraperitoneal polypropylene or Marlex mesh is erosions of, and
adhesions to the bowel, or infection of the prosthesis, with complications related to
these occurrences.
To test this hypothesis, Fitzgibbons, Salerno, Filipi and others conducted an animal
study in which polypropylene mesh, with and without an oxidised regenerated cellulose
adhesion barrier, was used to repair indirect hernias by the intraperitoneal onlay
technique(Fitzgibbons et al., 1994). Groups of male pigs were followed for both short-
term (6 weeks) and long-term (7.1 month) time frames. All herniorrhaphies were
-152-
successful with no recurrences. After short-term follow-up, 8l%o of 26laparoscopically-
placed prostheses adhered to the bladder or small bowel. After long-term follow-up,
48% of 42 laparoscopically-placed prostheses adhered to the bladder, small bowel, or
seminal vesicles. No complications related to mesh placement were obseryed, nor did
mesh stapled over cord structures appear to affect fertility by constricting the vas
deferens or spermatic vessels. The oxidised regenerated cellulose adhesion barrier
appeared to have no value decreasing the rate ofadhesions for laparoscopically-placed
prostheses. This study has quantified the degree of visceral adhesion formation to
intraperitoneal mesh, which would appear to occur in at least half of all laparoscopic
cases. No complications were observed as a consequence of this in pigs, but clinically
significant complications are well-recognised in humans. The success of the repairs in
this study is of minor consequence, as the dynamic forces in quadripeds would not be
expected to reflect the situation in the human groin. Therefore this study did not resolve
the problems of mesh slippage or uffecognised preperitoneal hernias. The most
reassuring result was the absence of fertility complications. Although this study was
only published in 1994, encouraging results emanating from this study (as early as
1990) have been cited on several different occasions in varying stages of completeness
to support the use of this technique. Literature reviews on the subject of laparoscopic
herniorrhaphy therefore tend to over-represent the importance of this approach, giving a
misleading impression that this technique is more widely advocated that it is. One of
these reviews \ /as written by the authors of the study, citing the manuscript in I992had
been submitted to an anonymous journal(Filipi et al., 1992), another review cites the
former review written by the authors of the study(Anegui et ar.,1993) and other
reviews cite two different book chapters also written by the authors of the
-153-

study(cheslyn-curtis and Russell,1993; Hanaff, 1993). This seems to be a good
example of how easily untested laparoscopic procedures can be disseminated into
surgical practice by enthusiastic advocates.
The benefits of polytetrafluoroethylene (PFTE) or Gore-Tex mesh in comparison to
other synthetic materials are based on the possibility of its use as an onlay mesh without
re-peritonealisation, and its characteristic of providing frbroblast proliferation without a
severe foreign body reaction. Toy and Smoot have described a laparoscopic
herniorrhaphy technique using an expanded PFTE Gore-Tex patch peritoneal onlay with
staple fixation(Toy and Smoot, 1992). Eighty-three hemioplasties were done under
general anaesthesia on 7 5 patients in an outpatient surgical facility, and followed for a
maximum of 20 months. There were2 recurrences (2.4%). The first occurred due to
staple disruption along the border of the Gore-Tex patch, and the authors now advocate
longer-leg staples. The second recurrence was attributed to inadequate fixation to
Cooper's ligament, and their technique was subsequently modified to incorporate
peritoneal dissection to enable direct visualisation of this structure. Toy and Smoot
considered laparoscopic hernioplasty to be at an investigational stage, and concluded
that its use should be confined to prospective studies. The authors noted that it was
gratifuing that awell-organised, multicentre trial, with defined outcome measures had
been commenced, and more recently publicised(Go, 1995).
The preliminary results of a prospective randomised trial of laparoscopic onlay
herniorrhaphy using expanded PFTE versus conventional inguinal hernia repair have
recently been published(Vogt et al., 1995). Thirty patients were randomised to the
laparoscopic group, 3l to the open group, and followed for a mean of g months.
Unfortunately, although the laparoscopic arm was standardised, in the open arm neither
-r54-
the operative technique nor the anaesthetic was controlled, instead relying on the
surgeons' or patients' preference. Apparently the Bassini and McVay repairs were the
most popular methods, and one could argue that these do not represent the state-of-the-
art in tension-free or anatomical open inguinal hernia repair. The authors' laparoscopic
onlay technique also incorporated the peritoneal dissection to enable direct visualisation
of Cooper's ligament, as described by Toy and Smoot. Full peritoneal dissection was
carried out if the hernia was unable to be visualised endoscopically. This would appear
to make this technique only minimally different to preperitoneal patch repairs, but with
the disadvantages entailed by exposed intraperitoneal mesh. Nevertheless, the authors
observed that in the laparoscopic group, mean operative time was shorter, post-
operative pain was significantly less, and return to normal activity was significantly
shorter. Two recurrences were witnessed in the open group and one in the laparoscopic
group, and overall complications and morbidity was low. If the methodological flaws in
this study are ignored, the results indicate that in all parameters besides the unassessable
recurrence rate, laparoscopic hemiorrhaphy is an efficacious procedure.
-15s-
Laparoscopic transabdominal preperitoneal patchThe basis of this method is the open preperitoneal technique of Stoppa (Stoppa and
warlaumont, 1993). The laparoscopic adaptation was devised by Arregui, who
description was published in l992(Anegui et a1., 1992). Since that time, articles
detailing the results of transabdominal preperitoneal patch repairs (TAPP) have
increasingly proliferated(Dion and Morin,1992; Voeller et al., 1993 ; Corbitt, 1993 ;
Himpens, 1993 ; Katkhouda and Mouiel,1993; 'Wheler, 1993 : Geis et a1.,1993 ;
Newman et al., 1993 ; wheeler, 1993 ; Seid et al., 1992; Morrison, 1993 ; polglase and
McMunick, 1994; Catts et al., 1994 : Paget, 1994 ; Winchester et al., 1993 ; panton
and Panton,1994; Kavic, 1995 ; Dion, 1993 ; Stoker et al., 1994 ; Millikan et a1.,1994
; Milkins et al., 1993 ; Cornell and Kerlakian,lgg4) and are indicative of the wide
popularity of this approach. Therefore only some of the most important papers will be
considered in this review(Arregui et a1.,1992; Brooks, 1994 ; Payne et al., 1994).
Arregui describes that the peritoneal cavity is entered laparoscopically in the usual
manner, after which the hemia sac is excised at its neck facilitating entry into the
preperitoneal space. This whole area is bluntly dissected to expose predominantly the
transversalis fascia and surrounding structures. In indirect hernias, the internal ring is
tightened with an interrupted suture, and in direct hernias the transversalis fascia is
loosely closed with a running suture. Polypropylene mesh (approximately 2.5 x 4.5
inches) is then fashioned to fit as a complete sheet over the internal ring, the testicular
vessels, the spermatic cord laterally, Hesselbach's triangle medially, and Cooper's
ligament inferiorly. The authors observe that the inferior epigastric vessels do not need
to be divided nor passed over the mesh. The mesh is anchored with 3-0 Vicryl sutures to
the transversalis fascia and the transversus abdominis arch superomedially, to the
-156-
iliopubic tract or Cooper's ligament inferiorly, and to the transversalis fascia and
transversus abdominis lateral to the internal ring. Lastly, the peritoneum is closed over
the mesh with a continuous absorbable suture. Sixty-one repairs were performed on 52
patients followed for a mean of 2.3 months. Patients were discharged on the same or
next day, and were allowed free activity. Only three minor complications ensued, and
no recurrences were evident in this very brief follow-up. The technique is admittedly
time-consuming, but this has been redressed in subsequent studies where staples rather
than sutures were used.
Comparative trials between laparoscopic TAPP herniorrhaphy and traditional open
inguinal hernia repair began appearing in print in April 1994. Six studies have been
published, of which three are prospective case control studies(Millikan et a1.,1994 ;
Brooks, 1994 ; Cornell and Kerlakian,lgg4) and three are randomised controlled trials;
one from the UK(Stoker et al, L994), one from the USA(payne et a1.,1994), and one
from Australia(Maddern et al., 1994).
Stoker et al published the first randomised controlled trial of laparoscopic
herniorrhaphy(Stoker et a1.,1994). The laparoscopic repair was performed as described
by Arregui, but using staples to fìx the Prolene mesh. The tension-free open repair was
performed in an identical manner to that at our institution (see Section 5.2.2 Methods,
Transabdominal preperitoneal herniorrhaphy), except that all repairs were conducted
under general anaesthesia. Following a learning-curve of 35 laparoscopic patients,
excluded from the analysis, 150 patients were randomised in equal numbers to each
group, and followed for a mean of 7 months during which no recuffences were observed
in either group. Their results showed the laparoscopic operation took on average l5
-t57-
minutes longer for unilateral repairs, but was only 30 minutes total for the last 20 cases
in the trial. Mean analogues pain scores were recorded on eight separate occasions until
day 7 post-operatively, and were significantly lower on each occasion in the
laparoscopic group. The median time taken to return to normal activity was
significantly shorter in the laparoscopic group (3 days cf 7 days), as was median time
taken to return to work (14 days cf 28 days). The complication rate was also lower in
the laparoscopic group (8 % cf 2r %). The extra expense of materials for the
laparoscopic procedure was f 168 per case, but such costs were expected to be recouped
by the community with fewer days lost from work. This trial represented a significant
advance in the management of hemiae, convincingly proving that in all parameters
besides recurrence (not assessed), the laparoscopic operation was better.
The work conducted at our institution was the second randomised controlled trial,
published in August 1994(Maddern et a1.,1994), and is discussed in Section 5.2,
Transabdominal preperitoneal herniorrhaphy. The only other randomised controlled
trial was published in September 1994 by Payne and others from the University of
Honolulu(Payne et a1.,1994). Fifty-two patients were randomised to the Lichenstein
tension-free open hemioplasty performed under local anaesthesia, and 48 to a
laparoscopic TAPP hernioplasty as described by Arregui, except mesh was stapled in
place. Unilateral laparoscopic repairs lasted an average of 68 minutes, which was not
significantly different to the open operation. Patients were discharged after a mean of
4.8 hours following laparoscopic repairs, againthis was not signihcantly different to
patients who underwent the open operation. Patients having primary open repair of
unilateral hernias returned to work after amean of l7 days. Following laparoscopy, the
mean time to return to work on objective measures was 8.9 days, and multiple
-158-

regression analysis controlling for the intensity of the job found this difference to be
significant. Eighteen percent of patients in the open group , and 12 Yo inthe laparoscopic
group sustained minor, transient complications. No recuffences were detected after a
median follow-up period of 10 months. The mean total hospital cost was almost
US$600 more for the laparoscopic operation. From these results it can be concluded that
in terms of operative and hospitalisation times, and short-term outcome, these two
modern operations are equally good. The balance between cost savings generated by an
earlier retum to work or a less expensive procedure cannot be appropriately generalised,
and is really a matter for resolution between the surgeon and the individual patient.
The studies by Stoker(stoker et al., 1994) and Payne(Payne et al., 1994) were
methodologically sound, and compared a standardised laparoscopic operation against
well-established, currently favoured open hemiorrhaphies. Until long-term data is
available, these studies justifu the continued use of laparoscopic TAPP repairs in a trial
setting.
Laparoscopic extraperitoneal patchA totally extraperitoneal approach to inguinal hemiorrhaphy had been advocated by
McKeman as early as 1993(McKernan and Laws, 1993), and has as its main advantage
the potential to eliminate all early and late complications related to violation of the
peritoneal cavity associated with other transabdominal laparoscopic hernia repairs.
Although prosthetic mesh is introduced by a different access route, the final
preperitoneal destination of the mesh makes it principally another laparoscopic variant
of the Stoppa and Warlaumont open hernioplasty.
-159-

In his most recent article McKernan describes his technique(McKernan,1993). A20
mm umbilical skin incision is deepened to the rectus sheath, which is opened in the
midline and the rectus muscle bluntly separated. A tunnel is then created by blunt
dissection in the plane between rectus and the peritoneum, and dissection towards the
pubis is continued with the aid of low-pressure insufflation. Care must be taken at all
times not to perforate the peritoneum. Dissection of the groin commences initially at
Cooper's ligament cephalad to the iliac vein and in the region of a direct hernia.
Peritoneal dissection is extended cephalad to expose the internal ring and indirect sac,
which can be dissected from the cord if small, or severed and ligated proximally if
large. A 3 x 5 inch piece of polypropylene mesh is then introduced into the
preperitoneal space and positioned to cover the hernia defect. The mesh is split to allow
passage of the cord and secured in position with a hernia stapler.
McKernan has successfully performed 100 herniorrhapies in 68 patients using this
technique. Minor complications included an Il Yo incidence of seroma formation at
sites of large direct hernias. Operative time averaged just over one hour, and all patients
were discharged by the first post-operative day. All had returned to normal activities
within one week. No recurrences were detected after mean follow-up of 10 months.
A larger series of 200 repairs in 155 patients was detailed by the French surgeon Begin
in 1993(Begin, 1993). The technique was as previously described, but expanded PFTE
(GoreTex) mesh was used in 5 cases. The average duration of the procedure for
unilateral hernias was 45 minutes, however in I I patients there was significant
breaching of the peritoneum. The mean duration of stay was 44 hours; essentially
patients were discharged the day after surgery, at which time their mean analogue pain
-160-
score was 2.5 on a scale of 0 to 10. Only 25 Yo of patients needed analgesia following
discharge. Begin also makes mention of early postoperative groin effusions requiring
aspiration on 3 instances, and noted one scrotal haematoma. Persistent postoperative
pain was a feature in 6 patients, requiring operative intervention to free a trapped lateral
cutaneous nerve in one patient. Ninety-six percent of patients regarded the results as
good or excellent. The mean duration for return to normal activity was 17 days,
although the reader gains the impression that results were not normally distributed, and
perhaps if non-parametric descriptive statistics were more appropriately used, the
median return to work would have been closer to 7 days. In the maximum follow-up
period of 22 months, one recuffence was seen, and re-operation revealed prosthetic
slippage due to inadequate f,rxation. No comment was made on efforts to redress the
potential for this to occur in the future.
These studies indicate the extraperitoneal approach is safe and not prohibitively
difficult, the early results show some promise, and the procedure seems destined for
increasing popularity. Unfortunately even short-term outcome parameters have not yet
been subjected to the rigourous evaluation of a randomised controlled trial, and it is
therefore difficult to identifu a place for the procedure in current surgical practice
besides that of an experimental technique.
Specific complications of laparoscopic hernia repairMacFayden was the first to assimilate the data from multiple series such that some
general impression of the incidence of complications following laparoscopic
herniorrhaphy could be gauged(MacFayden et al., 1993). Subsequently a
comprehensive collective series of outcome data from multiple institutions has been
published, and includes some of the same patients(Phillips et al., 1995). There is little
-161 -

one could add to this excellent treatise which represents the current state of knowledge
on this topic, and although all of its results are worthy of mention, only some will be
considered.
The study reports on the complications of 322g laparoscopic hernia repairs in2559
patients. Sixty percent of patients underwent the TAPP repair, 18 % the intraperitoneal
onlay mesh technique, 9 %othe plug and patch repair, and2 o/o simple closure of the
neck of the sac. Major complications, defined as requiring intervention or readmission
occurred in 0.5 o/o of patients, and minor complications in 8 %. With a mean follow-up
of 22 months there were 1 .6 Yo recunences. No technique seemed to be associated with
any specific complications though simple closure of the neck of the sac had a3 %o
recurrence rate and a moderate incidence of haematomas and testicular pain, surprising
given the simple nature of the procedure. The authors placed laparoscopic
complications in perspective with those observed after open herniorrhaphy, and reported
that the incidence of ischaemic orchitis/testicular pain, seromas, hydrocoeles, and
neuralgia was similar to that seen following traditional anterior approaches.
The authors identified two complications unique to the laparoscopic approach. Small
bowel obstruction occurred in 0.2 o/o of patients. Four of the five obstructions occurred
in the TAPP group due to hemiation through inadequately closed peritoneum,
highlighting the concems about contact of prosthetic mesh with intraperitoneal viscera.
One obstruction resulted from a port-site hernia. Lateral cutaneous nerve injury or
entrapment was the other complication unique to laparoscopy. The authors concluded
that ifpatients are properly selected and surgeons are adequately trained, laparoscopic
herniorrhaphy can be performed with an acceptably low incidence of complications.
-162-
5.2 Transabdominal preperitoneal herniorrhaphy
5.2.1 lntroductionThe aim of this study was to compare the efficacy of laparoscopic transabdominal
preperitoneal inguinal hernia repair to a conventional open approach in a day surgical
unit. with assessment of post operative pain, activity levels, clinical outcome and cost.
5.2.2 MethodsEighty six patients scheduled for elective inguinal hernia repair at the Royal Adelaide
Hospital were investigated in a randomised controlled study. The patients were
randomised to receive either the laparoscopic or standard open hernia repair, and a
preoperative assessment was made regarding the presumed nature of the hernia (direct
or indirect).
The laparoscopic repair was performed under general anaesthesia via a transabdominal
preperitoneal approach. Access was via two 1Omm and one 5mm cannulae, the
umbilical port for the camera assembly, and bilateral iliac fossa ports for grasping,
dissection and stapling instruments. The peritoneum was incised above the hemial
defect from within the abdomen and the hemial sac was invaginated. A polypropylene
mesh (Prolene, Ethicon, North Ryde, NSW) was individually sized for each patient,
introduced into the preperitoneal space, and stapled to the posterior wall of the inguinal
canal using an Ethicon Endoscopic Multifeed Stapler (EMS). The peritoneum was then
reapproximated with staples. The port holes were closed with 1 Ethibond and infiltrated
with0.25%o Marcaine with l:400 000 adrenaline.
The open repair was performed under local anaesthesia. A total of 50 ml of l%o
Lignocaine with l:100 000 adrenaline was infiltrated using a22 gauge short bevel
needle to find the correct tissue plane for the ilioinguinal, iliohypogastric, and
-163-

genitofemoral nerves and the peritoneal sac. The proposed incision was infiltrated with
a22 gauge spinal needle. Additional analgesia was provided by further injection into
the spermatic cord and pubic tubercle during the procedure with sedation when
necessa"ry. Excess hernial sac was dealt with by high ligation and excision in the case of
indirect hernias and by invagination in direct hernias. The posterior inguinal wall was
repaired by a variant of the Shouldice technique whereby a continuous 0 Prolene suture
approximated the transversalis fascia to the iliopubic tract. This was overlayed by a
tension-free double darn of 0 Prolene between the conjoint tendon and inguinal
(Poupart's) ligament. The wound was closed in layers and20 ml of 0.25Yo Marcaine
with 1:400 000 adrenaline was infiltrated.
For both operations records were kept of operation time (skin incision to skin closure),
consumables used, complications, and type of hernia found.
Patients were also contacted 30 days after surgery by a third party to gain their
impression of the Day Surgery experience. They were asked to classiff their experience
as "very satisfied", "satisfied", "not satisfied" or "would not agree again".
Comparative results for 2 independent samples were analysed on SPSS for Windows
6.1 statistical software (Chicago) using the Mann-Whitney U test with a2-tailed,a level
of 0.05.
5.2.3 Resu/fs
There were 86 patients in the study, of which 44 underwent conventional open hernia
repair and 42 underwent laparoscopic hernia repair. Seventeen patients had bilateral
hernias. Fifteen of these patients were randomised to have the laparoscopic repair with
both hernias repaired simultaneously. Two patients with bilateral hernias were
randomised to have the open repair and included as separate attendances because each
-164-
hernia was repaired on a different occasion. One hundred and one hernia repairs were
performed in total. The median follow up period to date is 179 days with a range of 97
to 289 days. All of the patients in the study were male with the exception of 5 females
in the open group and2 in the laparoscopic group.
The measured parameters for the two groups of patients are given in Table 7. From the
42 patients who had an open repair only 3 required conversion to a general anaesthetic.
All patients undergoing the laparoscopic repair had general anaesthesia. Table 7 also
indicates the type of hernias found at operation. The preoperative examination predicted
the operative hernia type in 79%o of cases excluding the pantaloon hernias, as none of
the pantaloon hernias were confidently diagnosed prior to surgery.
The median operation time for the bilateral operations performed laparoscopically was
60 minutes (range 30 - 100). When bilateral hernia repairs were excluded, the median
operation time was not significantly different between the open and laparoscopic
repairs. In contrast, in patients who were day cases and did not require admission the
median post-operative discharge time was signihcantly shorter for the open group þ <
0.05) (Table 7). The median number of days required to return back to work or normal
activity was not significantly different between the open and laparoscopic groups, even
when only unilateral hernias were considered, however a trend towards an earlier return
to work in the laparoscopic group was present.
-l6s-
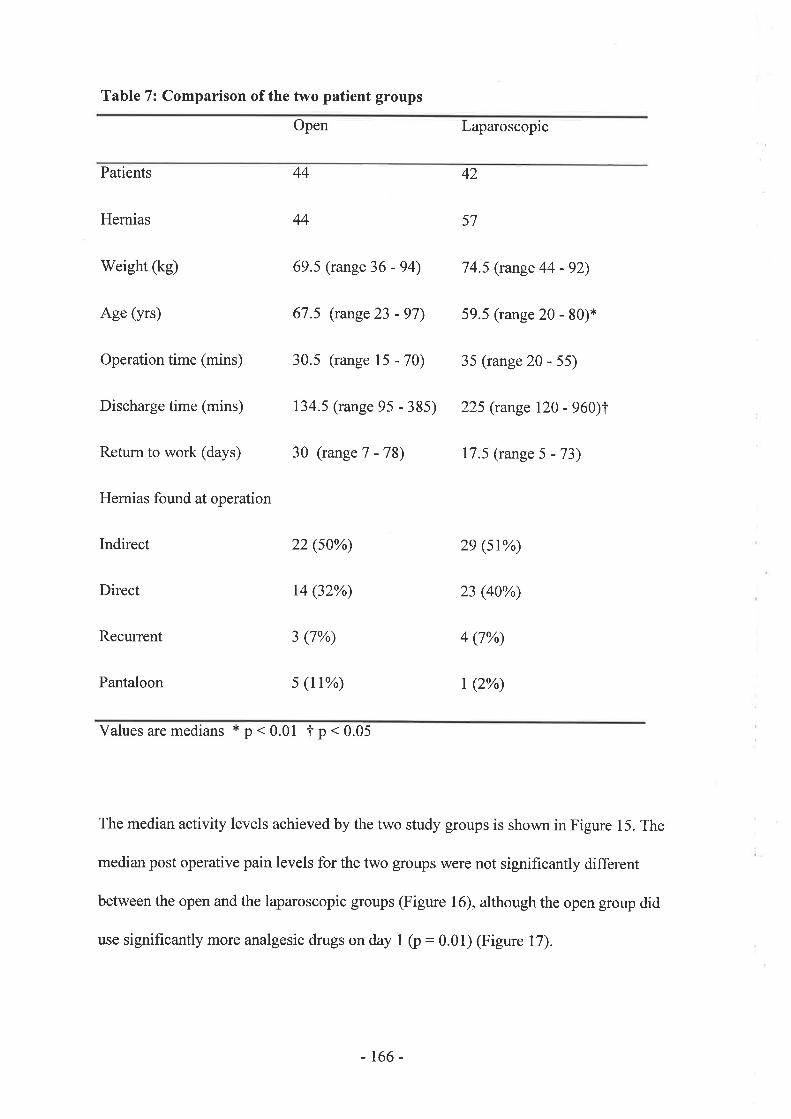
Table 7: Comparison of the two patient groups
Open Laparoscopic
Patients 42
Hernias 57
Weight (kg) 69.5 (range 36 - 94) 74.5 (range 44 - 92)
Age (yrs) 67 .5 (range23 - 97) 59.5 (range 20 - 80¡*
Operationtime (mins) 30.5 (range 15 - 70) 35 (range 20 - 55)
Discharge time (mins) 134.5 (range 95 - 385) 225 (range 120 - 960)I
Retum to work (days) 30 (range 7 - l8) 17.5 (range 5 - 73)
Hernias found at operation
Indirect 22 (s0%) 2e (st%)
Direct 14 (32%) 23 (40%)
Recurrent 3 (7%) 4 (7%)
Pantaloon s (tr%) t (2%)
44
44
Valuesaremedians *p<0.01 f p<0.05
The median activity levels achieved by the two study groups is shown in Figure 15. The
median post operative pain levels for the two groups were not significantly different
between the open and the laparoscopic groups (Figure l6), although the open group did
use significantly more analgesic drugs on day I (p: 0.01) (Figure 17).
-t66-

Figure 15: Median activity levels measured on an analogue scale of 0 - 10.
10 101010
9
I
7
b
5
4
3
2
1
o
9.25
7.75 7.75
55 ! open
lap
Preop Day 1 Day 3 Day 10 Day 30 Day'180
Figure 16: Median pain levels measured on an analogue scale of 0 - 10.
44
35
3
25
4
o
3
-9(!oat
.=oo-
2 lj open
I lap2
5
1
11
o5
oo ooDay 1 Day 3 Day 10 Day 30 Day 180
Values for Day 30 and Day 180 were zero.
-t67 -
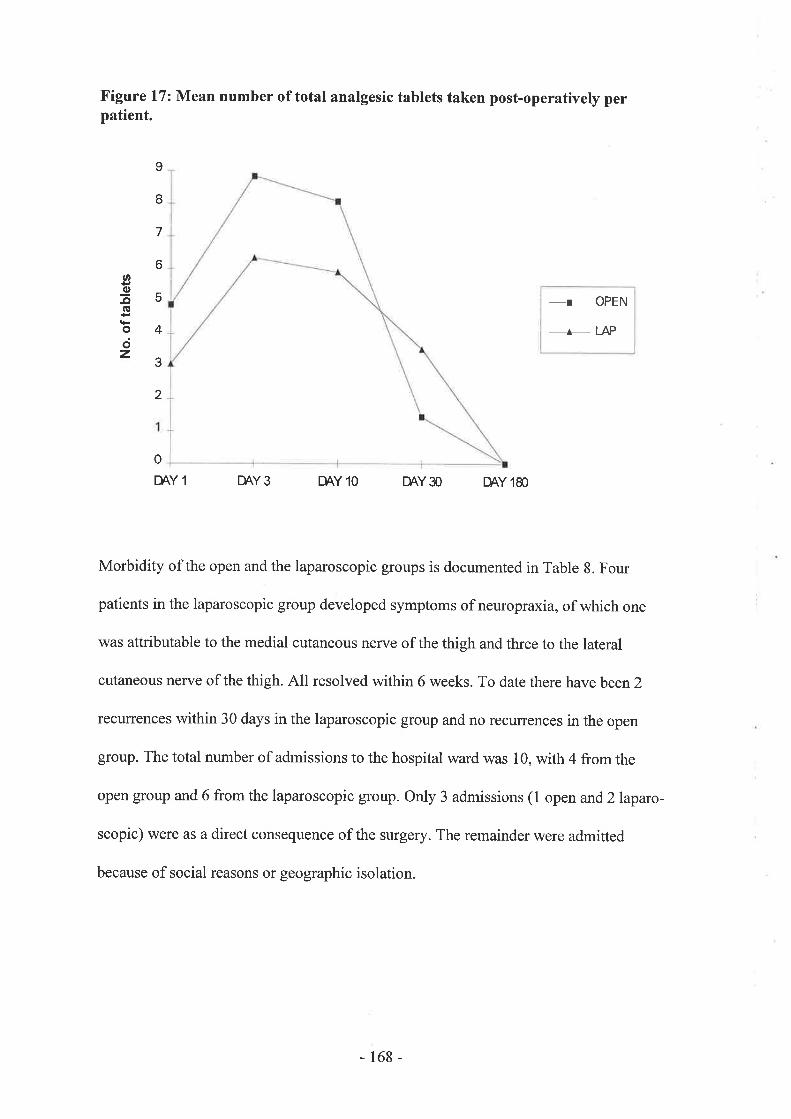
Figure 17: Mean number of total analgesic tablets taken post-operatively perpatient.
-T OPEN
_^_ LAP
o
DAY 1 DAY3 DAY 10 DAY3O DAYI8O
Morbidity of the open and the laparoscopic groups is documented in Table 8. Four
patients in the laparoscopic group developed symptoms of neuropraxia, of which one
was attributable to the medial cutaneous nerve of the thigh and three to the lateral
cutaneous nerve of the thigh. All resolved within 6 weeks. To date there have been2
recunences within 30 days in the laparoscopic group and no recuffences in the open
group. The total number of admissions to the hospital ward was 10, with 4 from the
open group and 6 from the laparoscopic group. Only 3 admissions (1 open and2laparo-
scopic) were as a direct consequence of the surgery. The remainder were admitted
because ofsocial reasons or geographic isolation.
U,
-glt(!octz
9
I
7
6
5
4
3
2
-168-

Table 8 : Morbidity
Complication Open Laparoscopic
Bruising/swelling t4
Seroma./traematoma 2
Neuropraxia
Scrotal(bruising/swelling) 3
Porthole complication
Intra-abdominal bleed
Small bowel obstruction
Vasovagal collapse
Total 2r (47%) 17 (40%)
All but 3 patients were contacted to obtain their opinion of day case surgery. Eighty five
percent of these patients were satisfied with day surgery and l5Yo were not satisfied
(Table 9).
5
2
2
4
4
1
I
0
0
0
I
01
-169-

Table 9: Patients'Opinion of Day Case Surgery
Opinion Open Laparoscopic Total
Very satisfied t9 16 3s (48%)
Satisfied 15 t2 27 (37%)
Not satisfied 6 (8%)24
Would not agree again 3 2 s (7%)
Total 39 34 73 (r00%)
With respect to the added costs associated with laparoscopic hernia repair, there was a
mean of 1.1 staplers used for every hernia repaired, and each patient required 3 trocars.
In2 patients a disposable surgical clip applier was required to control bleeding from the
inferior epigastric vessels, additionally all laparoscopic patients required general
anaesthesia rather than local anaesthetic infiltration.
5.2.4 DiscussionAt the time of conception of this work in early 1992, no other randomised controlled
study had been conducted to compare laparoscopic hernia repair with a conventional
open technique. The number of laparoscopic hemia repairs performed in this study and
the follow up period, although short, are similar to other published series(Popp,1993 ;
McKernan and Laws, 1993 ; Corbitt, l99I ; Halverson and McVay,1970).
In order to compare the optimal operative techniques for the repair of hernias, local
anaesthetic with sedation as necessary was used for the open inguinal hernia repairs and
general anaesthetic for the laparoscopic hernia repairs. Only 3 patients under local
-170-

anaesthesia needed conversion to general anaesthesia during the operation, usually due
to inadequate block in obese patients. Although many surgeons continue to repair
hemias under general anaesthesia, local anaesthesia has the advantages of being more
cost-effective and eliminating the risks associated with general anaesthesia.
The relationship between the surgeon's classification of inguinal hemias on
examination and the type of hernia found at operation has been previously
documented(Ralphs et al., 1980). This study suggests that correct identification of the
type of hernia before operation is possible in79Yo of cases when pantaloon hernias are
not present.
The results indicate that laparoscopic transabdominal preperitoneal inguinal hernia
repair is comparable to the conventional open repair with respect to operation time,
post-operative pain and activity levels, as well as the number of days required for return
to work. This is in contrast to previous uncontrolled studies (Dion and Morin, 1992 ;
Salerna et al., l99l ; McKernan and Laws, 1993 ; Corbitt, 1991) reporting reduced post-
operative pain and a more rapid return to work for patients with hernias repaired laparo-
scopically. Although the number of patients studied was small, a trend to earlier return
to work for the laparoscopic group did exist. Post-operative pain was low after laparo-
scopic inguinal hernia repair, but the results of this study show that post operative pain
was equally low following the open repair. This could be attributed to gentler handling
of the tissues and greater precision during open hernia repair because the patient had
only local anaesthetic infiltration. While recorded pain levels were not significantly
different, there were greater analgesic requirements in the open group to achieve this
result (Figure 17). The shorter discharge time for the open group was not surprising
-t7I-
considering the majority were performed under local anaesthesia and were able to
recover sooner and avoided the side effects ofgeneral anaesthesia.
Because of the remote location of several of our patients or the inability to locate a
responsible family member for the first postoperative night, 7 patients required "hotel"
admissions. If one considers the true medical admissions, 3 patients (l open and2
laparoscopic) required admission. An 8l year old female in the open group required
admission for observation due to a vasovagal attack just prior to discharge. In the
laparoscopic group, one admission was due to a signihcant intra-abdominal bleed and
the other because of a porthole haemorrhage which required re-operation. The patient
who developed an intra-abdominal bleed suffered from a known bleeding disorder, and
recovered spontaneously with fluid and blood transfusion.
The small bowel obstruction diagnosed on day 10 in a patient of the laparoscopic group
resulted from adherence of bowel to the prosthetic mesh because of a disrupted lateral
peritoneal closure post-operatively. The bowel obstruction and peritoneal defect were
subsequently dealt with by a laparotomy.
Although the follow up period was suitable for the assessment of post-operative pain
and activity levels, it was not sufficient to draw any definite conclusions regarding
recurrence rates. The two recurrences reported in this study were in asthmatic patients,
both with a history of severe coughing during the post-operative period. One of these
patients was also on high dose steroids, and the other was later found to have an occult
sigmoid colon carcinoma. These factors may have contributed to early recuffence.
The implications of this study for day case inguinal hernia surgery are promising.
Hernia repair as a day case surgical procedure has not adversely affected the patients in
-172-

terms of post-operative pain and activity levels. In addition, there was a high degree of
satisfaction with the procedure from patients in both the laparoscopic and open groups.
The results indicate that both types of surgery can be successfully performed as day
case procedures, with the corresponding hnancial benefits(Flanagan and Bascom,
r e8 1).
In summary, laparoscopic transabdominal preperitoneal hemiorrhaphy has not been
shown to be superior to a conventional open inguinal hemia repair with respect to
reducing post-operative pain and increasing post-operative activity levels. Similarly, it
has not been demonstrated by this study that laparoscopic transabdominal preperitoneal
herniorrhaphy leads to a quicker return to work. In terms of major complications
requiring re-operation or admission, the laparoscopic operation appears inferior. These
results, in combination with the added cost, suggest that this laparoscopic approach
currently does not warrant widespread use in unilateral hernia repairs. Laparoscopic
transabdominal preperitoneal herniorrhaphy does have a clear place for a patients with
bilateral hemias, recurrent hernias or clinically doubtful hernias. The bilateral hernias
can be repaired simultaneously, and yet the patient can still be discharged on the same
day, avoiding the need for two separate admissions or hospitalisations. In the case of
recurrent hernias, the laparoscopic approach permits access through previously
undisturbed tissue. In the obese patient or small symptomatic hernias a laparoscopic
examination can also accurately clarifu the nature of any hernial defect.
-173-

5.3 Extraperitoneal herniorrhaphy
5.3.1 IntroductionThe aim of this study was to compare the efficacy of laparoscopic extraperitoneal ingui-
nal hernia repair to a conventional open approach in a day surgical unit, with
assessment of post operative pain and activity levels, and clinical outcome.
5.3.2 Methods
One hundred and four patients scheduled for elective inguinal hernia repair at the Royal
Adelaide Hospital and the Queen Elizabeth Hospital were investigated in a randomised
controlled study. After being judged suitable for Day Surgery, patients were randomised
to receive either an extraperitoneal laparoscopic or standard open hernia repair, and all
operations were performed by or under the immediate guidance of four Consultant
Surgeons experienced in the appropriate techniques.
The laparoscopic repair was performed under general anaesthesia via an extraperitoneal
approach. Access was via two 1Omm and one 5mm cannulae, the umbilical port for the
camera assembly, and bilateral iliac fossa ports for grasping, dissection and stapling
instruments. The peritoneum was dissected from the abdominal wall and the hernial sac
was reduced. A polypropylene mesh (Prolene) was individually sized for each patient,
introduced into the preperitoneal space, and stapled to the posterior wall of the inguinal
canal using an Ethicon Endoscopic Multifeed Stapler (EMS). The port holes were
closed with I Ethibond and infiltrated with 0.25% Marcaine with l:400 000 adrenaline.
The open repair was performed as described in Section 5.2.2, Methods, Transabdominal
preperitoneal herni orrhaphy.
For both operations records were kept of operation time (skin incision to skin closure),
complications, and type of hernia found.
Comparative results for 2 independent samples were analysed on SPSS for'Windows
6.1 statistical software (Chicago) using the Mann-Whitney U test with a2-tailedc¿ level
of 0.05.
-174-

5.3.3 Resu/ús
There were 104 patients in the study, of whom 72 underwent conventional open hernia
repair and32 underwent laparoscopic extraperitoneal hernia repair.
After being judged suitable for day surgery, 50 patients were randomised to have the
laparoscopic repair, and 54 the open repair. The final disparity in group sizes occurred
because 18 laparoscopic patients crossed-over to the open group for the following
reasons, which are represented graphically in Figure 18: One patient was subsequently
deemed unsuitable for day surgery general anaesthesia and therefore required an open
procedure under local anaesthesia. Three patients were unsuitable for laparoscopic
repairs because of large inguinoscrotal hernias. Four patients had previous abdominal
scars precluding laparoscopic access or extraperitoneal dissection. Two patients refused
laparoscopic operations, and two patients with bilateral hernias were randomised to
have the laparoscopic repair under general anaesthesia but elected to have open surgery
on both sides performed during the same operation. Six patients were converted from
laparoscopic to open herniorrhaphy because of intraoperative difficulties. These have
been included in analysis of the open group. However retained in the analysis of the
laparoscopic group were three patients who had a failed extraperitoneal herniorrhaphy
and were converted to the transperitoneal technique.
-175-

Figure 18: Breakdown of petient groups after randomisation
Suitable for Day Surgery104
Open54
Laparoscopic50
Anaesthetic r¡sk1
Unsuitable3
Scars4
Refused2
Bilateral2
Failed6
Laparoscopic32
Open72
Transperitoneal3
Extraperitoneal29
-t76-

Eleven patients had bilateral hernias. Seven of these patients were randomised to have
the laparoscopic repair with both hernias repaired simultaneously. Two of these patients
were randomised to have the open repair and were recorded as separate attendances
because each hernia was repaired on a different occasion. As stated above, the
remaining two patients with bilateral hernias were randomised to have the laparoscopic
repair but elected to have open surgery on both sides performed during the same
operation. One hundred and thirteen hernia repairs were performed in total.
From the 72 patients who had an open repair, 14 underwent general anaesthesia and 56
underwent local anaesthesia, of whom I required conversion to a general anaesthetic.
All patients undergoing the laparoscopic repair had general anaesthesia.
Table 10 indicates the type of hernias found at operation. The median follow up period
to date is 220 days with a range of 9 to 568 days. All of the patients in the study were
male with the exception of 2 females in the open group and 4 in the laparoscopic group.
The measured parameters for the two groups of patients are also listed in Table 10.
-177 -
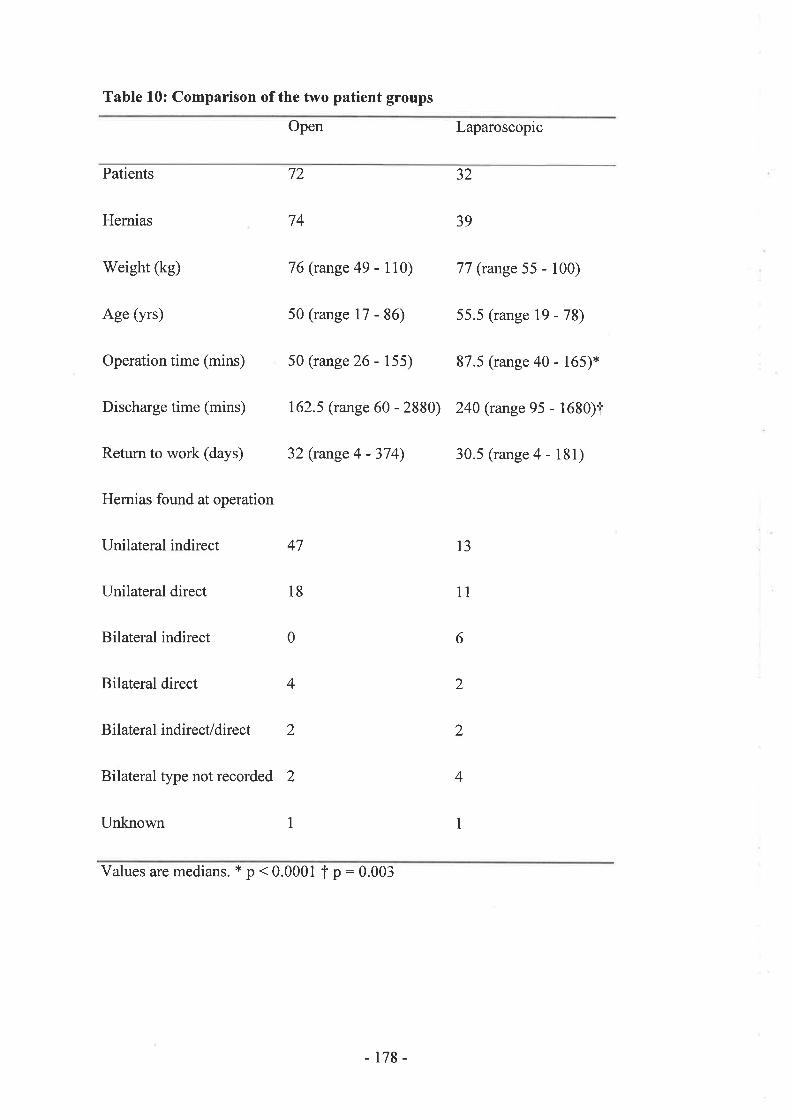
Table 10: Comparison of the two patient groups
Open Laparoscopic
Patients 72 32
Hernias 74 39
Weight (kg) 76 (range 49 - 110) 77 (range 55 - 100)
Age (yrs) 50 (range 17 - 86) 55.5 (range 19 - 78)
Operation time (mins) 50 (range 26 - 155) 87.5 (range 40 - 165)*
Discharge time (mins) 162.5 (range 60 - 2880) 240 (range 95 - 1630)T
Return to work (days) 32 (range 4 - 374) 30.5 (range 4 - 181)
Hernias found at operation
Unilateral indirect 47 l3
Unilateral direct 18
Bilateral indirect
Bilateral direct
Bilateral indirect/direct 2
Bilateral type not recorded 2
Unknown
1l
60
4 2
2
4
1I
Values are medians. * p < 0.0001 t p : 0.003
-178-
The median operation time for the bilateral operations performed laparoscopically was
115 minutes (range 90 - 160). When bilateral hernia repairs were excluded in both
groups, the median operation time was still signifrcantly greater for laparoscopic repairs
(37 mins for open, 69 mins for laparoscopic, p < 0.0001). For patients who were
successfully performed as day cases and did not require admission, the median time
until post-operative discharge remained significantly shorter for the open group (39
mins for open, 62 mins for laparoscopic, p : 0.0001). The median number of days
required to return back to work or normal activity was not significantly different
between the open and laparoscopic groups, even when only unilateral hernias were
considered, however a trend towards an earlier retum to work in the laparoscopic group
was present.
The median activity levels achieved by the two study groups is shown in Figure 19. The
median post-operative pain levels between the open and the laparoscopic groups were
not significantly different (Figure 20), except on day 3 when patients in the open group
recorded significantly greater discomfort (p:0.02). Figure 21 indicates the open group
did use significantly more analgesic drugs on days I and 3 (p: 0.0045 and p: 0.001
respectively).
-179-

Figure 19: Median activity levels measured on an analogue scale of 0 - 10.l0 10 10 10 10 10 10 10
0
10
9
I
7
b
5
4
3
I
00
7
I6oø
:to
55
1'l
o Lap
¡ Open
¡ Lap
¡ Open
25
2
0
Preop Day 1 Day 3 Day 10 Day 30 Day 180 Day 360
Figure 20: Median pain levels measured on an analogue scale of 0 - 10.
5
45
4
5
0
3535
3
25
2
I6oo
ao-
1.515
05 05
00 00
Day 1 Day 3 Day 10 Day 30 Day 180 Day 360 Day 540
Values for Day 30, Day 180, Day 360, and Day 540 (for the open group) were zero
- 180 -

Figure 21: Mean number of total analgesic tablets taken post-operatively perpatient.
E LAp
g Open
Day I Day 3 Day 10 Day 30
Surgical morbidity is detailed in Table I 1. Major complications, defined as requiring re-
intervention or admission, were evident in 5 of the 72 patients in the open group (7 %),
and 4 of the 32 patients in the laparoscopic group (I2.5 %). Two patients in the open
group developed significant postoperative haematomas. One patient in the laparoscopic
group suffered bleeding as a result of a port-site complication, and one other patient was
re-admitted 2 days postoperatively with wound pain which resolved spontaneously
within 24 hours. There have been 2 recurrences in the laparoscopic group, one at 30
days and the other at2I0 days, and no recurrences in the open group. The total number
of admissions to the hospital ward was I 1, with 9 admissions (5 open and 4laparo-
scopic) as a direct consequence of the surgery, and a fuither 2 admissions in the open
group because ofsocial reasons.
øs¡G
odz
2
-181 -

Table 11: Post-operative morbidity
Open Laparoscopic
Admissions (maj or complications) Admissions (maj or complications)
- 2 haematomas - 1 assisted ventilation after
GA
- 1 prophylaxis against resp. - I portsite bleed
complications
- I for observation after GA - I for observation after GA
(unspecified) (unspecified)
- 1 for wound pain (no - 1 for wound pain (no
abnormality detected) abnormality detected)
Minor complications
- t haematomaday 7
- I haematoma day 10
Total 7 (9.7 %) Total 4 (12.5 %)
-182-

5.3.4 Drscussion
In considering data detailing the outcome of hernia repair, the statistics collated by
Lichtenstein(Lichenstein et al., 1989) are particularly salient to deficiencies in the
current knowledge regarding the status of laparoscopic hernionhaphy. He noted that a
1983 study by the Rand Corporation indicated that at least 10 %o of all primary repairs
will fail(Rand Corporation, 1983). Of these, 50 % first appear five or more years after
the initial operation, and75 0/o of those hernias that recur become apparent within ten
years of the original operation(Lichtenstein and Shore, I976). Furthermore,20 Yo of
recurrences will not become apparent until 15 to 25 years postoperatively(Ravitch,
1969).In addition, he stated that many reports are flawed because of inappropriate
comparison of different surgical methods, or differences in individual techniques with
the same method, and also because significant numbers of patients are lost to follow-up,
amongst which are likely to be the highest number of recurrences. In light of such
information, it will be some time yet before any reliable data about recurrence following
laparoscopic hemiorrhaphy is available. It is clearly too early to make a f,rnal decision
on the place of laparoscopy in the spectrum of hernia surgery, and all currently available
information, including that herein must be regarded as somewhat shrouded by the
preliminary nature of the findings. It is easy to lose cognisance of this basic tenet if one
becomes absorbed in the atmosphere of didactic argument put forward by both
proponents and opponents of laparoscopic herniorrhaphy operations.
However, as laparoscopic hernia surgery has progressed from elementary to anatomical
techniques, a need has emerged to assess specific operative approaches and determine
which provides optimal results. In this respect, the information from this study fills the
- 183 -

curent void of randomised controlled trials investigating the effrcacy of laparoscopic
extraperitoneal hernionhaphy.
The potential advantages of laparoscopic extraperitoneal hernionhaphy have been
welcomed by surgeons. A totally extraperitoneal approach avoids the inherent technical
dangers of intraperitoneal laparoscopy (see Section 2.2, Complications of laparoscopy).
These general complications may be more imagined than real insofar as herniorrhaphy
is concerned, as a large multi-institutional series of 3229 laparoscopic hernia repairs
failed to document any such general complications not specifically related to technical
aspects of the repair(Phillips et a1.,1995).
The extraperitoneal approach should also avoid any risk of intraperitoneal migration of
prosthetic mesh and the complications associated with adherence of mesh to visceral
structures. Extraperitoneally-placed mesh is not immune from slippage however, and
laparoscopic hemia reculrence has been attributed to this process(Begin, 1993).
Not so welcome for laparoscopic surgeons is the technically demanding nature of
extraperitoneal hernionhaphy beyond that of TAPP or intraperitoneal repairs. A high
degree ofskill and concentration is required for the dissection to stay in the correct
plane during progress from umbilicus to groin. The extraperitoneal operations in this
study took a median of 52 minutes longer than the TAPP repairs cited previously (see
Section 5.2, Transabdominal preperitoneal herniorrhaphy), and a median of almost 40
minutes longer than patients randomised to the open repair. Peritoneal breaches
mandated conversion from extraperitoneal to TAPP repairs in 2 of the 32 laparoscopic
patients in this study (6.25 %), and peritoneal breaching was observed in 1l of 155
patients (7 %) in the series reported by Begin(Begin, 1993). This is not an insignificant
- 184 -
problem, and the 16 o/o overall conversion rate from extraperitoneal to other operative
approaches in this study reached almost unacceptable levels. More recently this
dissection has been facilitated by the use of a balloon trocar dissector which obviates
the need for CO2 insufflation(Ferzli and Dysarz,1994; Kieturakis et al., 1994). This
innovation, first described by Ferzli and Dysart in mid-1994 makes progress in the
extraperitoneal plane much easier, and had it been used in this series may have
considerably minimised the conversion rate.
Despite the added technical challenge presented by the extraperitoneal repair, surgical
morbidity was low (I2.5 %), and comparable to patients randomised to the open repair
(9.7 %).It is of note that the overall complication rate in both open and laparoscopic
groups was considerably lower than detected in the previous TAPP study, and can only
be attributed to greater familiarity with both laparoscopic hemiorrhaphy and the use of
local anaesthesia during open repairs, given that diligence of follow-up was equivalent
in both studies. The high rate of post-operative seroma formation after laparoscopic
extraperitoneal repairs witnessed in previous series(McKernan, 1993 ; Begin, 1993) was
not in evidence amongst the patients in this study. However, the two early recurrences
amongst only 32 patients is a cause for concern, as it likely more will become evident
with the progression of time, but as explained earlier this parameter will be withheld
from consideration of the outcome of laparoscopic hernionhaphy until longer follow-up
periods have elapsed.
The results indicate that laparoscopic extraperitoneal inguinal hernia repair is
comparable to the conventional open repair with respect to post-operative activity levels
and the number of days required for return to work. A median of 30.5 days was required
- 185 -

for patients to return to work after the laparoscopic operation, considerably longer than
reported in previous uncontrolled studies(McKernan, 1993 ; Begin, 1993 ; Cable et al.,
1994), although correlating well with the patients' median activity levels, which did not
uniformly return to normal until day 30 (Figure l9). Patients' pain levels were near to
pre-operative levels by day 10, so it appears unlikely that activity and return to work
were delayed by the pain of the procedure. It is postulated that demographic differences
account for the disparity between the time taken to retum to work in this and other
studies. For viable inter-study comparisons to be made about post-operative activity and
functional recovery, subjective tools such as the analogue scales commonly used can be
dehcient. An objective measurement tool for these variables has been applied to
laparoscopic transabdominal preperitoneal herniorrhaphy by Payne(Payne et al., 1994),
and would facilitate assimilation of this body of literature if adopted in future studies.
Laparoscopic extraperitoneal inguinal hernia repair is inferior to the conventional open
repair in terms of operation time and time to hospital discharge. The technical
challenges posed by the extraperitoneal approach have been discussed above, and the
shorter discharge time for the open group can be attributed to the more rapid recovery
after local anaesthesia.
The laparoscopic herniorrhaphy is superior to the open repair with respect to post-
operative pain levels and analgesic requirements. Although during conventional repairs
under local anaesthesia patient's tissues were handled gently, patients in this group still
suffered more pain on day 3, despite the intake of a significantly greater analgesic load
at this time (Figure2l).
- 186 -

A methodological shortcoming of this study must be acknowledged. There were
considerably fewer patients in the laparoscopic group, introducing the risk of errors in
statistical inference. The groups were otherwise well matched for age, sex and weight. It
could be argued that the statistical differences that did occur amongst measured
variables in laparoscopic patients were highly significant to a degree of magnitude that
suggests errors of Type I or Type II would have not influenced the result to a large
extent. Although approximately equal numbers of patients were randomised initially, a
greater proportion of laparoscopic patients at the Royal Adelaide Hospital crossed-over
to the open group. This may indicate inconstancies in surgeons' technical abilities.
In conclusion, laparoscopic extraperitoneal herniorrhaphy has features comparable to,
inferior to and superior to conventional open repair. At present, the individual surgeon
must balance the disadvantages and potential costs of the prolonged operation and the
longer period spent in hospital against the benefits to the patient of less pain and
analgesia requirements. Other factors in the assessment of this operation include the
technical difflrculty and higher conversion rate, the low incidence of post-operative
complications, and the unknown long-term recurrence rate. There will also be certain
patients for whom this operation may be unsuitable, such as those with abdominal scars
from previous surgery. Laparoscopic extraperitoneal herniorrhaphy is a promising
operation, and can no longer be regarded as a Phase I experimental procedure. However
on current evidence it is unlikely to become the dominant form of groin hernia repairs.
It should be subjected to further study under trial conditions such that its position can be
clarified with the aid of larger study populations and greater technical expertise, whilst
awaiting the results of long-term follow-up on recuffence rates.
-t87 -
6. SUMMARY AND CONCLUSIONS
The capability for laparoscopic abdominal surgery has had unprecedented impact on the
technical implementation of clinical surgery. The success of laparoscopic
cholecystectomy in demonstrating that minimally-invasive procedures can result in
significantly shorter hospitalisation, disability, and pain for the patient ensured enduring
enthusiasm for this type of access. However the subsequent ardour to adopt other
untested laparoscopic procedures challenged, and perhaps even threatened academic
swgery to keep pace with contemporary practice yet establish the place of these new
innovations by rigorous analysis. It was this atmosphere that was the genesis for the
research contained herein.
A historical perspective of operative and technical advances that allowed laparoscopic
surgery to reach this state of development is outlined in the introductory chapter. The
evolution of surgery in previously inaccessible locations is followed from 1806, when
Bozzini constructed a crude apparatus to visualize the urethra, to the contributions of
Kurt Semm who is the father of operative laparoscopy in the modern era. Widespread
adoption of laparoscopy ensued once computer-chip video-cameras became available in
1986. It was this breakthrough which sealed the influential place of laparoscopic
surgery in modern surgical practice.
The new information provided by this thesis contributes to a better understanding and a
clearer definition for the role of therapeutic laparoscopy in the practice of upper
alimentary tract surgery. This was achieved by determining the risks to patients from
the physiological effects of laparoscopy, by the development and evaluation of new
applications for minimally-invasive surgery, and by assessing the efhcacy of routine
laparoscopic procedures which had entered the clinical arena without prior validation.
- 188 -
In order to marshall the evidence required to address these issues, several separate
studies were required to answer relevant questions, and the contribution of each can
now be summarized.
6.1 General problems of laparoscopy
6.1 .1 Temperature regulationHypothermia is a common postsurgical problem more marked in patients at the
extremes of age. Maintenance of perianaesthetic normothermia is of great importance to
counteract the numerous deleterious consequences of hypothermia, yet information
documenting the impact of laparoscopy on perioperative heat balance is scarce.
The impact of laparoscopy on perioperative heat balance was documented in a study
that quantified changes in core temperature over a three-hour period of high-flow
carbon-dioxide insufflation in a randomised, controlled trial of six pigs. Each animal
was anaesthetised and studied on three occasions under standardised conditions, acting
as its own control by insufflation with no gas compared with insufflation by cold gas
and warmed gas. Insufflation of carbon-dioxide at high flow rates over a prolonged
period of time was shown to result in a significant fall in core temperature. Yet the
provision of warmed rather than cold insufflated gas conferred no protection against
changes in core temperature, due to the small amount of heat required to warm the gas
to body temperature. A much greater effect can be attributed to the latent heat required
to saturate the insufflated gas, and most of the hypothermic effect is due to this cause.
It is concluded that humidification of the insufflated carbon-dioxide would largely
resolve the problem of laparoscopy-induced hypothermia, but in addition, insufflator
tubing should be equipped with an insulated heating wire to prevent warmed gas
equilibrating with room temperature as it flows to the patient. However technical
-189-
problems remain to be overcome before insufflators can provide humidified, heated gas
to minimize perioperative hypothermia, and it is recommended that controlled studies
validate the clinical utility of future generations of insufflator apparatus before they
enter the marketplace.
6.1.2 Thromboembolism
Minimally-invasive access for abdominal operations has been proven to reduce the risk
of some postoperative complications. However thromboembolism is not amongst them,
by virtue of the absence of any definitive clinical data detailing the incidence of
thromboembolism after laparoscopic surgery. Uncontrolled clinical audits suggest the
incidence of fatal thromboembolic events may be low, but because most thrombi remain
silent, and discharge home often occurs early following laparoscopic procedures, it is
likely thal a considerable number of patients are being missed. Further evidence of the
problem can be found in case reports which have been published documenting death
due to mesenteric thrombosis and infarction.
The factors comprising Virchow's triad are still considered the most important in the
pathogenesis of thromboembolism, and include hypercoagulability, impaired blood
flow, and vessel wall abnormalities. In the absence of definitive clinical data,
experimental evidence documenting changes in one or more of these factors during
laparoscopic surgery may be usefully employed to extrapolate the risk of postoperative
thrombosis to patients in current clinical practice.
The experimental evidence associating hypercoagulability and laparoscopic surgery was
collected in a controlled human study which measured fibrinogen, D-dimer,
prothrombin, APTT and platelet levels before, during and after open and laparoscopic
-190-
Nissen fundoplication. Hypercoagulability was demonstrated to be present on the first
postoperative day compared to preoperative values, irrespective of whether the
operation was performed open or laparoscopically. It was concluded that minimally-
invasive procedures do not protect against the risk of postoperative hypercoagulability
Impaired femoral venous blood flow during general abdominal sugery occurs as a
result of several separate but cumulative mechanisms; loss of the normal calf muscle
pump, calf venodilatation during general anaesthesia, and reverse Trendelenburg
positioning. Recent evidence suggest that in addition, creation of a tension
pneumoperitoneum independently impairs lower limb venous flow. When a
pneumoperitoneum is combined with existing factors tending to cause venous stasis
during open surgery, their net effect may be greatly magnified.
The potential for laparoscopic insufflation to impair blood flow is not limited to femoral
vessels, but may also affect vessels supplying vital intraabdominal organs. This
hypothesis was investigated by the use of radiolabelled microspheres to determine
blood flow distributions in a pig model. Proof of decreased blood flow at the tissue
level in the setting of laparoscopic abdominal surgery was not established. It was
concluded that a definitive investigation to assimilate such evidence would be feasible
using the microsphere technique, if the study incorporated larger sample populations
and methodolo gical refi nements
There is currently no experimental evidence to suggest that laparoscopic surgery causes
endothelial damage. However, a widely held theory postulates that operative
venodilatation resultant from insufflation and general anaesthesia may cause endothelial
cracking, followed by exposure of subendothelial collagen, platelet adhesion, and
-l9t-

activation of the coagulation cascade. The site of endothelial damage may then act as a
nidus for thrombosis formation during laparoscopy
In summary, laparoscopy can not be said to be minimally-invasive in terms of the
development of postoperative thrombosis. Laparoscopy appears to negatively influence
all three elements of Virchow's triad, sometimes beyond that of open surgery, and may
result in a cumulatively greater risk for the development of venous thromboembolism
Until definitive clinical studies become available, it is recommended that patients
undergoing laparoscopic operations be considered to be of equal or possibly higher risk
than their open counterparts, and that appropriate prophylaxis be instituted.
6.2 Development and evaluation of new applications ¡n laparoscopicgastro¡ ntest¡nal su rgery
6.2.1 OesophagectomySubtotal oesophagectomy and immediate oesophagogastric reconstruction is a favoured
option for cure or palliation of oesophageal carcinoma. The conventional approach
involves a thoracotomy and laparotomy exposing the patient to the attendant pulmonary
and intrathoracic complications. Alternative approaches to oesophagectomy without
thoracotomy have failed to diminish the complication rate and may compromise the
chance of cure. An endoscopic approach to the surgical management of oesophageal
carcinoma is considered to be an evolving solution because it rernoves the need for
thoracotomy and laparotomy but adheres to established oncologic principles.
A 3-step minimally-invasive operation was devised consisting of thoracoscopic
oesophageal dissection, laparoscopic gastric mobilisation and thoracoscopic end-to-end
oesophago-gastric anastomosis using a circular endoluminal stapler. This total
endosurgical oesophagectomy was shown to be technically feasible in an animal model,
-192-
and the stapled oesophagogastric anastomosis was capable of being safely performed in
a manner comparable to the conventional procedure.
It is concluded that endosurgical treatment of oesophageal carcinoma has potential to
reduce the number of postoperative complications or deaths. However, it will need to
demonstrate clear superiority over existing specific treatment modalities before it could
be advocated to enter clinical practice.
6.2.2 Highly selective vagotomySince Latarjetin 1920 and Dragstedt in 1943 demonstrated the therapeutic utility of
vagotomy for the treatment of patients with peptic ulcer disease, the operation has
undergone continuous development and refinement in an effort to eradicate troublesome
side-effects such as disturbed gastric emptying, dumping and diarrhoea. In 1969
Johnston & Wilkinson demonstrated that it was possible to divide only the vagal
branches to the parietal cells, preserving the nerves of Latarjet and motor innervation to
the pylorus and antrum. This highly selective vagotomy reduces acid secretion as
effectively as truncal vagotomy, and is very safe with an operative mortality rate well
under lYo.The innervated antrum provides undisturbed solid emptying, and
preservation of the pylorus reduces the tendency for duodeno-gastric reflux.
Open highly selective vagotomy has withstood the rigours of objective evaluation to
become the optimal surgical treatment for chronic duodenal ulcer refractory to medical
therapy in many centres. Laparoscopic highly selective vagotomy has not been
subjected to the same scrutiny before entering clinical practice. A variety of
laparoscopic vagotomy procedures have been developed but unfortunately the
multiplicity of techniques combined with low referral rates for surgery has meant that
-193-
the experience of each group has been limited to relatively small series. No long-term
clinical results are available by which the effrcacy of laparoscopic vagotomy can be
definitively judged. To address this deficiency in the present state of knowledge, a
controlled animal study was conducted to demonstrate the physiological validity of
laparoscopic vagotomy.
Gastric acid output was measured by an aspiration technique, liquid gastric emptying
was calculated by the double sampling technique of George, and gastro-oesophageal
reflux was assessed by 8 hour ambulatory pH monitoring. Laparoscopic highly selective
vagotomy was shown to be as effective as its open counterpart in reducing basal acid
output, and did not interfere with liquid gastric emptying in contrast to the open
operation. Neither open nor laparoscopic highly selective vagotomy were observed to
precipitate gastro-oesophageal reflux. It is concluded that the continued use of
laparoscopic highly selective vagotomy in clinical practice is appropriate.
6.2.3 GastrostomyGastrostomy for enteral feeding or gastric decompression has traditionally been
performed by open surgery. Recent reports indicating a lower morbidity and mortality
rate for percutaneous endoscopic gastrostomy compared with open gastrostomy have
justified the more minimally invasive approach that percutaneous techniques provide.
Percutaneous endoscopic gastrostomy is not immune from complications, in particular
as a result of insecure fixation of the stomach to the anterior abdominal wall, and post-
procedural reflux and aspiration pneumonia.
Following a review of the available literature on the feasibility of laparoscopic
gastrostomy, a viable technique was developed to offer an alternative form of enteral
access, and successfully performed in the case reported. The procedure incorporates a
-194-
modification to existing laparoscopic techniques whereby the anchoring sutures are
hand-tied and buried in a subcutaneous pouch. Laparoscopic gastrostomy is less
invasive than open gastrostomy, and can be easily performed by General Surgeons with
basic laparoscopic skills without the assistance of an endoscopist. In some respects it
provides benefits surpassing percutaneous endoscopic gastrostomy, because the poor
apposition between the stomach and anterior abdominal wall can be prevented, and
prophylaxis against reflux and aspiration pneumonia can be easily incorporated into the
procedure. It is concluded that laparoscopic enteral access has emerged as the preferred
approach when percutaneous endoscopic gastrostomy is contraindicated or has failed.
6.3 Assessment of routine laparoscopic proceduresAlthough inguinal hernias are not anatomically located in the upper gastrointestinal
tract, their treatment comprises a significant and controversial component of the
practice of upper gastrointestinal surgery. A wide variety of eponymous traditional
methods of inguinal hernia repair have been developed from the time of Bassini's
original description in 1887, differentiated primarily in their management of the
posterior inguinal wall
Laparoscopic herniorrhaphy was first performedin 1979, and operative techniques have
evolved into two main groups; plug or patch repairs. Many surgeons have abandoned
the plugging techniques because of the high recurrence rate, but patch repairs remain
popular, and three different types have been described; transabdominal intraperitoneal,
transabdominal preperitoneal, and extraperitoneal. However, as laparoscopic hernia
surgery has progressed from elementary to anatomical techniques, a need has emerged
to resolve the indications for laparoscopic herniorrhaphy, and to assess which operative
approach provides optimal results.
-195-
Two randomised-controlled trials were conducted in a day surgery setting. A standard
conventional open hemioplasty was compared with transabdominal preperitoneal
laparoscopic hemiorrhaphy, and extraperitoneal laparoscopic herniorrhaphy
respectively. The laparoscopic transabdominal preperitoneal approach provided no
advantages in duration of operation, postoperative pain or time taken to return to work.
It was concluded that this operation should be confined to recurrent, bilateral or
undiagnosed hernias only, rather than emerge as the routine operation. In contrast, some
features of laparoscopic extraperitoneal hemiorrhaphy were superior to the open repair,
indicating it should no longer be regarded only as a Phase I experimental procedure
However it was concluded that laparoscopic extraperitoneal hernionhaphy should not
enter clinical practice until subjected to fuither study under trial conditions with the aid
of larger study populations and greater technical expertise, whilst the results of long-
term recurrence rates are awaited.
-196-

7. BIBLIOGRAPHY
Abercrombie JF, McAnena OJ, Rogers J, and V/illiams NS. (1993) LaparoscopicResection of a Bleeding Gastric Tumour-Surgical Workshop. Br. J. Surg. 80:373
Ajani JA, Roth JA, Ryan MB et al. (1993) Intensive preoperative chemotherapy withcolony-stimulating factor for resectable adenocarcinoma of the esophagus orgastroesophageal junction. J. Clin. Oncol. I|:22-28.
Akiyama H, Tsurumaru M, Kawamura T, and Ono Y. (1981) Principles of surgicaltreatment for carcinoma of the esophagus: Analysis of lymph node involvement. Ann.Surg. 194:438-446.
Akiyama H, Tsurumaru M, and Wanatabe G. (1984) Development of surgery forcarcinoma of the oesophagus. Am. J. Surg. 147:9-16.
Alkatori NK, Girardi L, and Skinner DB. (1994) Squamous Cell Carcinoma of theEsophagus: Therapeutic Dilemma. World J. Surg. 18:308-3 I 1.
Allen DP. (1986) Effect of anaesthesia upon temperature and blood pressure. Tr. Am.Soc. Anesth.14:367
Altman LK. (1992) Surgical injuries lead to new rule. New York Times 14 June:1
Anvari M and Park A. (1994) Laparoscopic-assisted vagotomy and distal gastrectomySurg. Endosc. 8: I 3 12-1315.
Arcelus JI, Caprini JA, Traverso CI, Size G, and Hasty JH. (1993) The role of elasticcompression stockings to prevent venous dilatation induced by a reverse trendelenburgposition.
Armitage P, and Berry G. (1994) In: Statistical methods in medical research. 3rd ed. pp.197 -I98. Oxford: Blackwell Scientific Publications
Arregui ME, Davis CJ, Yucel O, and Nagan RF. (1992) Laparoscopic mesh repair ofinguinal hernia using a preperitoneal approach: A preliminary report. Surg. Laparosc.Endosc. 2(1):53-58.
Arregui ME, Navarrete J, Davis CJ, Castro D, and Nagan RF. (1993) Laparoscopicinguinal hernoirrhaphy. techniques and controveries. Surg. Clin. North Am. 73:513-527.
AzagraJ. S. (1993) Thoracoscopy in oesophagectomy for oesophageal cancer. Br. JSurg. 80:320-321.
-t97 -
Baadsgaard Starr-Edwards, Bille S, Egebald K. (1989) Major vascular injury duringgynecologic laparoscopy: A report of a case and review of published cases. Acta Obstet.Gynecol. Scand. 68:283 -285.
Bailey RW, Flowers JL, Graham SM, and Zucker KA. (1991) Combined laparoscopiccholecystectomy and selective vagotomy. Surg. Laparosc. Endos c. I :45 -49 .
Ballem RV and Rudomanski J. (1993) Techniques of pneumoperitoneum. SurgLaparosc. Endosc. 3 :42-43.
Baron JH. Selective surgery for duodenal ulcer. 1978;I(23):153-178
Becker HD, Buess GF, Mentges BR, and Naruhn MB. (1993) Endoscopicesophagectomy. Adv. Surg. 26:397 -410.
Beckers EJ, Rehrer NJ, Brouns F, Ten Hoor F, and Saris WHM. (1988) Determinationof total gastric volume, gastric secretion and residual meal using the double sampletechnique of George. Gut. 29 :1725 -1729.
Beebe DS, McNevin MP, Crain JM et al. (1993) Evidence of venous stasis afterabdominal insufflation for laparoscopic cholecystectomy. Surg Gynecol. Obstet.176:443-447.
Begin G-F. (1993) Laparoscopic extraperitoneal treatment of inguinal hemias in adultsA series of 200 cases. End. Surg. l:204-206.
Belani KG, Sessler DI, Larson MD et al. (1993) The pupillary light reflex: Effects ofanestheti c s and hyperthermia. Anesthe siolo gy . 7 9 :23 -27 .
Berci G, Shore JM, Panish J et al. (1973) The evaluation of a new peritoneoscope as a
diagnostic aid to the surgeon. Ann. Surg. 178:37.
Berci G. (1991) Laparoscopic cholecystectomy viewed from the USA. Aust. N. Z. JSurg. 6l:249-250.
Berends FJ, Kazemier G, Bonjer JH, and Lange JF. (1994) Subcutaneous metastases
after laparoscopic colectomy. Lancet. 3 44:89 | 4
Berggren U, Rasmussen I, and Arvidsson D. (1993) Effects on systemic and splanchniccirculation induced by pneumoperitoneum.
Bergqvist D, Matzsch T, Jendteg S, Lindgren B, and Persson U. (1990) The cost-effectiveness of prevention of post-operative thromboembolism. Acta Chir. Scand.156:36-41.
Bickler P and Sessler DL (1990) Efficiency of airway heat and moisture exchangers inanesthitized humans. Anesth. Analg. 7 I :41 5 -418.
-198-

Boelhouwer R, Bruining H, and Ong G. (1987) Correlations of serum potassiumfluctuations with body temperature after major surgery. Crit. Care Med. 15:310-312
Boesch PF. (1936) Laparoskopie. Schweiz Z Krankenhaus Anstaltsw.6:62
Bounameaux H, Khabiri E, Hubre O, Schneider PA, Didier D, and de Moerloose P.
(1992) Value of liquid crystal contact thermography and plasma lecel of D-Dimer forscreening of deep venous thrombosis following general abdominal surgery. Thromb.Haemost. 67:603-606.
Bozzini P. (1806) Lichtleiter, eine Erfingdung Zur Anshung Innerer Theile undKrankheit Nebst Abbildung. J Pract Arzeyhunde.24:107
Branicki FJ and Nathanson LK. (1994) Minimal access gastroduodenal surgery. Aust.N. Z. J. Surg. 64:589-598.
Brodie B. (1814) Experiments and observations on the influence of the nerves of theeighth pair on the secretions of the stomach. Phil. Trans. R. Soc. (London). 104:102-106.
Brooks DC. (1994) A Prospective Comparison of Laparoscopic and Tension-Free OpenHemiorrhaphy. Arch. Surg. 129:3 6I-366.
Brown RK, Galletti G, and Tumm KS. (1966) New technique for the cure of inguinalhemia: By Edoardo Bassini in 1 187 and 1890. J. Hist. Med.40I-407 .
Buckberg GD, Luck JC, Payne DB, Hoffman JIE, Archie JP, and Fixler DE. (1971)Some sources of error in measuring regional blood flow with radioactive microspheres.J. Appl. Physiol. 3 1 :598-605.
Buess, G., Kipfmüller, K., Hack, D., Grüßner, R., Heintz, A., Junginger, Th. (1988)Technique of transanal endoscopic microsurgery. Surg. Endosc. 2:71-75
Buess, G., Kipfmüller, K., Ibald, R., Hack, D., Heintz, A. (1989) Clinical results oftransanal endoscopic microsurgery. Surg. Endosc. 2:245 -250
Buess G and Becker HD. (1990) Minimally invasive surgery in tumors of theesophagus. Langenbecks Arch. Chir. Suppl. Ii. Verh. Dtsch. Ges. Forsch. Chir.1355-1 360.
Buess G. (1991) Endoscopic esophagectomy without thoracotomy. Prob. Gen. Surg.8:478-486.
Buess G. (1992) Thoracoscopic dissection of the esophagus. Surg. Endosc. 6:150-151
Buess GF and Maddern GJ. (1994) Endoscopic oesophagectomy. In: Jamieson GG anddeBas H (Eds.) Robb & Smith Operative Surgery. Surgery of the Upper Gastro-intestinal Tract, 5th edn. pp. 535-541.
-r99-
Bui HD, Dang CV, Chaney RH, and Vergara LM. (1989) Does gastrostomy andfundoplication prevent aspiration pneumonia in mentally retarded persons? Am. J.
Ment. Retard. 9416-19.
Bumm R, Holscher AH, Feussner H, Tachibana M, Bartels H, and Siewert JR. (1993)Endodissection of the Thoracic Esophagus. Technique and Clinical Results inTranshiatal Esophagectomy. Ann. Surg. 218 :97 -I04.
Bumm R and Siewert JR. (1994) Results of transmediastinal endoscopic oesophagealdissection. End. Surg. 2:16-20.
Cable RL, Gilling PJ, and Jones V/O. (1994) Laparoscopic extraperitoneal inguinalhernia repair using a balloon dissection technique. Aust. N. Z. J. Surg. 64:431-433.
Cadiere GB, Himpens J, and Bruyns J. (1994) Laparoscopic proximal gastric vagotomyEnd. Surg.2:105-108.
Caldwell CB and Ricotta JJ. (1987) Changes in visceral blood flow with elevatedintraabdominal pressure. J. Surg. Res. 43:14-20.
Caporale A, Tirindelli MC, Aurello P et al. (1989) Evaluation of postoperative bloodcoagulation changes in elderly patients undergoing major surgery. Ital. J. Surg. Sci.19:51-56.
Caprini JA, Scurr JH, and Hasty JH. (1988) Role of compression modalities in aprophylactic program for deep vein thrombosis. Semin. Thromb. Hemost. 14(Suppl.):77-87.
Caprini JA, Arcelus JI, Traverso CI, and Vittum D. (1991) Hypercoagulability afterlaparoscopic cholecystectomy. Thromb. Haemost. 65 :13 47
Caprini JA and Arcelus JI. (1994) Prevention of postoperative venousthromboembolism following laparoscopic cholecystectomy. Surg. Endosc. S:747-747
Caprini JA and Natonson RA. (1989) Postoperative deep vein thrombosis: currentclinical considerations. Semin. Thromb. Hemost. | 5 :244-249 .
Carli F, Emery PW, and Freemantle CAJ. (1989) Effect of peroperative normothermiaon postoperative protein metabolism in elderly patients undergoing hip arthroplasty. Br.J Anaesth. 63:276-282.
Catts PF, Aroney M, and Indyk JS. (1994) Laparoscopic repair of inguinal hernia. Med.J. Aust. 161:243-248
Chassin, J.L. (1993) Stapled oesophageal anastomoses. In: Jamieson, G.G. (Ed.)Surgery of the Oesophagu s, pp. 7 13 -720. Churchill Livingstone (London).
-200-

Cheatle GL. (1920) An operation for the radical cure of inguinal and femoral hemia.Brit. Med. J.2:168
Cheslyn-Curtis S and Russell RCG. (1993) Laparoscopic herniorrhaphy. Literaturereview. End. Surg. 1:188-192.
Chiu AV/, Azadzoi KM, Hatzichristou DG, Siroky MB, Krane RJ, and Babayan RK.(1994) Effects of intra-abdominal pressure on renal tissue perfusion during laparoscopyJ. Endourol. 8:99-103.
Claes Y, Hemelrijck JV, and Gerven MV. (1992) Influence of hydroxyethyl starch oncoagulation in patients during the perioperative period. Anesth. Analg. 75:24-30.
Clark RE, Orkin LR, and Rovenstine EA. (1954) Body temperature studies inanesthetized man-effect of environmental temperature, humidity and anesthesia system.JAMA. 154:3ll-319.
Cohen F, Valleur P, Serra J, Brissett D, Chiche L, and Hautefeuille P. (1993)Relationship between gastric acid secretion and the rate of recurrent ulcer after parietalcell vagotomy. Ann. Surg. 217 :253 -259.
Coleridge Smith PD, Hasty JH, and Scurr JH. (1990) Venous stasis and vein lumenchanges during surgery. Br. J. Surg.77:1055-1059.
Collard J, Lengele B, Otte J, and Kestens P. (1993) En bloc and standardesophagectomies by thoracoscopy. Ann. Thorac. Surg. 56:675-679.
Collins GJ, Jr., Barber JA,ZajtchtrkR, Vanek D, and Malogne LA. (1977) The effectsof operative stress on the coagulation profile. Am. J. Surg. 133:612-616.
Collins R, Scrimgeur A, Yusuf S, and Peto R. (1988) Reduction in fatal pulmonaryembolism and venous thrombosis by perioperative administration of subcutaneousheparin. N. Engl. J. Med. 318:1162-1172.
Comerota AJ, Stewart GJ, Alburger PD, Smalley K, and White JV. (1989) Operativevenodilation: a previously unsuspected factor in the cause of postoperative deep veinthrombosis. Surgery. I 06:301 -8.
Conahan TJ. (1982) Heating reduces recovery time (cost) in outpatients.Anesthesiology. 67 :128- I 3 0.
Corbelle JL, Jr and Corbelle JL. (1993) Indication for thoracoscopic vagotomy. SurgLaparosc. Endosc. 3 :39 5 -397 .
Corbitt JD. (1991) Laparoscopic hernoirrhaphy. Surg. Laparosc. Endosc. l:23-25
Corbitt JD. (1993) Transabdominal preperitoneal herniorrhaphy. Surg. Laparosc.Endosc. 3:328-332.
-20t -
Cornell RB and Kerlakian GM. (1994) Early complications and outcomes of the currenttechnique of transperitoneal laparoscopic herniorrhaphy and a comparison to thetraditional open approach. Am. J. Surg. 168:275-279.
Corson SL, Batzer FR, Gocial B, and Maislin G. (1989) Measurement of the forcenecessary for laparoscopic trocar entry. J. Reprod. Med. 34:282-284.
Cossa JP, Marmuse JP, Lecomte P, Le Goff JY, Johanet H, and Benhamou G. (1992)Tubular gastrostomy using celioscopy. Presse Med. 21:1519-1521.
Crist DW and Gadacz TR. (1993) Complications of laparoscopic surgery. Surg. Clin.North Am.73:265-289
Croce E, Azzola M, Golia M et al. (1994) Laparoscopic posterior truncal vagotomy andanterior proximal gastric vagotomy. End. Surg. 2:113-116.
Cuschieri A, Hall AW, Clark J. (1978) Value of laparoscopy in diagnosis andmanagement of pancreatic carcinoma. Gut. 19:672.
Cuschieri A, Berci G, and McSherry CK. (1990) Laparoscopic cholecystectomy. Am. J.
Surg. 159:273
Cuschieri A. (1992) Laparoscopic vagotomy. Gimmick or reality? Surg. Clin. NorthA:m.72:357-367.
Cuschieri, A. and Buess, G. (1992) Introduction and Historical aspects. In: Buess, G.,Cuschieri, A. and Perissat, J. (Eds.) Operative manual for endoscopic surgery, pp. 1-5Springer Verlag.
Cuschieri A, Shimi S, and Banting S. (1992) Endoscopic oesophagectomy through aright thoracoscopic approach. J. R. Coll. Surg. Edinb . 37:7 -ll .
Cuschieri A. (1993) Endoscopic subtotal oesophagectomy for cancer using a rightthoracoscopic approach. Surgical Oncology. 2(Suppl 1):3-1 1.
Cuschieri A. (1994) Thoracoscopic subtotal oesophagectomy. End. Surg. 2:2I-25.
Cuschieri A. (1995) Whither minimal access surgery: Tribulations and expectationsAm. J. Surg. 169:9-19.
Dalen JE and Alpert J. (1975) Natural history of pulmonary embolism. Prog.Cardiovasc . Dis. 57 :259
Dallemagne B,'Weerts JM, Jehaes C et al. (1923) Case report: Subtotaloesophagectomy by thoracoscopy and laparoscopy. Minimally Invasive Ther.ll2:183-1 85.
-202 -
Dallemagne B, Weerts JM, Jehaes C, Markiewicz S, and Lombard R. (1994)Laparoscopic highly selective vagotomy. Br. J. Surg. 81:554-556.
Desormeaux AJ. (1865) Transactions of the Societe de Chirurgie, Paris. Gazette des
hop.
Deziel DJ, Millikan KW, Economou SG, Doolas A, Ko S, and Airan MC. (1993)Complications of laparoscopic choleystectomy: A National survey of 4292 hospitalsand an analysis of 77604 cases. Am. J. Surg. 165:9-14.
Diebel LN, Wilson RF, Dulchavsky SA, and Saxe J. (1992) Effect of increased intra-abdominal pressure on hepatic arterial, portal venous, and hepatic microcirculatoryblood flow. J. Trauma. 33(2):279-283.
Diehl LF. (1991) Radiation and chemotherapy in the treatment of esophageal cancer.Gastroenterol. Clin. North Am. 207 65 -77 4.
Dion Y. (1993) Laparoscopic inguinal herniorrhaphy: An induvidualized approach.Surg. Laparosc. Endosc. 6:451-455.
Dion Y and Morin J. (1992) Laparoscopic inguinal herniorrhaphy. Can. J. Surg. 35:209-212.
Ditesheim JA, Richards W, and Sharp K. (1989) Fatal and disastrous complicationsfollowing percutaneous endoscopic gastrostomy. Am. Surg. 55:92-96.
Donahue PE, Yoshida J, Bombeck CT, and Nyhus LM. (1986) The simplifiedendoscopic Congo red test for completeness of vagotomy. Surg. Gynecol. Obstet.163:287-289.
Donahue PE, Yoshida J, Richter HM et al. (1987) Can the use of an endoscopic Congored test decrease the incidence of incomplete proximal gastric vagotomy?. Gastro.Endosc. 33:427-431.
Donaldson MC, Weinberg DS, Belkin M, Whittemore AD, and Mannick JA. (1990)Screening for hypercoagulable states in vascular surgical practice: A preliminary studyJ. Vasc. Surg. 11:825-831.
Dragstedt LR. (1945) Vagotomy for gastroduodenal ulcer. Ann. Surg. 122:973-989
Dubois F, Berthelot G, and Levard H. (1989) Cholecystectomie par celioscopie. Presse
Med. 18:980-982.
Dubois F, Bertelot G, and Levard H. (1991) Laparoscopic Cholecystectomy: Historicperspective and personal experience. Surg. Laparosc. Endosc. I (l):52-57 .
Dubois F. Laparoscopic vagotomy. 1992;(20) :25 45 -2262.
-203 -

Dubois F. (1994) Vagotomies - laparoscopic or thoracoscopic approach. End. Surg.2:100-104.
Duh QY and'Way LW. (1993a) Laparoscopic jejunostomy using T-Fasteners as
retractors and anchors. Arch. Surg. 128:105-108.
Duh QY and V/ay LV/. (1993b) Laparoscopic gastrostomy using T-fasteners as
retractors and anchors. Surg Endosc. 7:60-63.
Earlam R and Cunha-Melo JR. (1980) Oesophageal squamous cell carcinoma: A criticalreview. Br. J. Surg. 67:381-390.
Edelman DS and Unger SW. (1991) Laparoscopic gastrostomy. Surg. Gynecol. Obstet.173:401
Ellis P, Kleinsaser L, and Speer R. (1957) Changes in Coagulation Occurring in DogsDuring Hypothermia and Cardiac Surgery. Surgery. 4l 198-210.
Farmer DA and Smithwick RH. (1952) Hemigastrectomy combined with resection ofthe vagus nerves. N. Engl. J. Med. 247:1071-1022.
Fervers C. (1933) Die laparoskopie meit dem Cystoscope. Ein Beitrag zurVereinfachung der Technik und zur Endoscopischen Strandurchtrennung in derBauchole. Medizin Klinik. 29 :1042-1045.
Ferzli GS and Dysarz FA. (1994) Extraperitoneal endoscopic inguinal hernionhaphyperformed without carbon dioxide insufflation. J. Laparoendosc. Surg. 4(5):301-304.
Filipi CJ,Fitzgibbons RJ and Salemo GM. (1991) Historical review: Diagnosticlaparoscopy to laparoscopic cholecystectomy and beyond. In: Zucker KA, Bailey RWand Reddick EJ. (Eds.) Surgical Laparoscopy, pp. 3-19. St. Louis: Quality MedicalPuiblishing.
Filipi CJ, Fitzgibbons RJ, Jr., Salerno GM, and Hart RO. (1992) Laparoscopicherniorrhaphy. Surg. Clin. North Am. 7 2:I 109 -l 124.
Fitzgibbons RJ, Jr. (1994) Personal communication.
Fitzgibbons RJ, Salerno GM, Filipi CJ, Hunter WJ, and Watson P. (1994) Alaparoscopic intraperitoneal onlay mesh technique for the repair of an indirect inguinalhernia. Ann. Surg. 219:144-156.
Flanagan L and Bascom JU. (1981) Herniorrhaphies performed upon outpatients underlocal anaesthesia. Surg Gynecol. Obstet. 153:557-560.
Fletcher DR. (1993) Elective treatment of duodenal ulcer - Time for assessment andchange. Gastroenterol.Hepatol. 8 :43 7-A3 7. (Abstract)
-204-

Fourestier N, Gladu A, and Vulmiere J. (1952) Perfectionments a I'endoscopeicmedicale; realisation bronchoscopique. Presse i|l4ed. 60 :1292
Fowler DL and White SA. (1991) Laparoscopic resection of a submucosal gastriclipoma: A case report. J. Laparoendosc. Surg. 1:303-306.
Gaff TD, Arbgast NR, and Phillips OC. (1959) Gas embolism: A comparitive study ofair and carbon-dioxide as embolic agents in the systemic vascular system. Am. J.
Obstet. Gynecol. 7 8:259-265.
Gazayerli MM. (1991) The Gazayerli emdoscopic retractor 1. Surg. Laparosc. Endosc.1:98-100
Geis'WP, Crafton'WB, Novak MJ, and Malago M. (1993) Laparoscopic herniorraphy:Results and technical aspects in 450 consecutive procedures. Surgery.ll4:765-774.
George JD. (1968) New clinical method for measuring the rate of gastric emptying: thedouble sample test meal. Gut.9:237-242.
Ger R. (1982) The management of certain abdominal herniae by intra-abdominalclosure of the neck of the sac: Preliminary Communication. Ann. R. Coll. Surg. Engl.64:342-344.
Ger R, Monroe K, Duvivier R, and Mishrick A. (1990) Management of indirect inguinalhernias by laparoscopic closure of the neck of the sac. Am. J. Surg. 159:370-373.
Ger R, Mishrick A, Hurwitz J, Romero C, and Oddsen R. (1993) Management of groinhernias by laparoscopy. V/orld J. Surg. 17:46-50.
Geraghty JG, Grace PA, Quereshi A, Bouchierhayes D, and Osborne DH. (1994)Simple new technique for laparoscopic inguinal hernia repair. Br. J. Surg. 81:93
Gertsch P, Baer HU, Kraft R, Maddern GJ, and Altermatt HJ. (1992) Malignant cellsare collected on circular staplers. Dis. Colon Rectum. 35:238-241.
Glassow F. (1986) The Shouldice Hospital technique. Int. Surg. 71:148-153.
Gleeson NC, Nicosia SV, and Mark JE. (1993) Abdominal wall metastases fromovarian cancer after laparoscopy. Am. J. Obstet. Gynecol. 169:522-523.
Gleysteen JJ, Burdeshaw JA, and Hallenbeck GA. (1976) Gastric emptying of liquidsafter different vagotomies and pyloroplasty. Surg Gynecol. Obstet. 142:41-48.
Go PMNYH. (1995) Prospective comparison studies on laparoscopic inguinal herniarepair. Surg. Endosc. 3 :7 19-720.
Goetze O. (1918) Rontgendiagnostik bei gasgefullter Bachohle eine neue Methode.Muenchner Med'Wochenschr. 65:127 5-1280.
-205 -
Goh P, Tekant Y, Kum CK, Isaac J, and Shang NS. (1992) Totally intra-abdominallaparoscopic Billroth II gastrectomy. Surg. Endosc. 6:160
Goldminc M, Maddem GJ, LePrise E, Meunier B, Campion JP, and Launois B. (1993)Oesophagectomy by a transhiatal approach or thoracotomy: a prospective randomisedtrial. Br. J. Surg. 80:367-370.
Goligher J.C. (1974) A technique for highly selective (parietal cell or proximal gastric)vagotomy for duodenal ulcer. Br. J. Surg. 6I:337-345.
Gossot D, Ghnassia MD, Debiolles H et al. (1992) Thoracoscopic dissection of theesophagus: an experimental study. Surg. Endosc. 6:59-61.
Gossot D, Fourquier P, and Celerier M. (1993) Thoracoscopic esophagectomy:Technique and initial Results. Ann. Thorac. Surg. 56:667-670.
Gottfried EB and Plumser AB. (1984) Endoscopic gastrojejunostomy: a technique toestablish small bowel feeding without laparotomy. Gastrointest. Endosc. 30:355-357
Greenberg AG. (1987) Revisiting the recurrent groin hernia. Am. J. Surg. 154:35-40
Griffrth CA and Harkins HN. (1957) Partial gastric vagotomy, an experimental study.Gastroenterology. 32:9 6 -102.
Grunow JE, al Hafidh A, and Tunell WP. (1989) Gastroesophageal reflux followingpercutaneous endoscopic gastrostomy in children. J. Pediatr. Surg.24:42-44.
Guillou PJ,Darzi A, and Monson JRT. (1993) Experience with laparoscopic colorectalsurgery for malignant disease. Surg. Oncol. 2(Suppl I):43-49.
Haggie JA. (1992) Laparoscopic tube gastrostomy. Ann. R. Coll. Surg. Engl.74:258-259.
Hales JRS. (1973) Radioactive microsphere measurement of cardiac output and regionaltissue blood flow in sheep. Pfluegers Arch. 344:ll9-I32.
Hales JRS. (1974) Radioactive microsphere techniques for studies of the circulation.Clin. Exp. Pharmacol. Physiol. (Suppl.). l:31-46.
Hales JRS. (1994) Practical considerations in the use of microspheres for evaluation ofcardiovascular and thermoregulatory interactions. Biomedical Thermology. In press.
Halkier BK, Ho CS, and Yee AC. (1989) Percutaneous feeding gastrostomy with theSeldinger technique: review of 252 patients. Radiology. 17l:359-362.
Hallenbeck GA, Gleysteen JJ, Aldrete JS, and Slaughter RL. (1976) Effect of twooperative techniques on clinical and gastric secretery results. Ann. Surg. 184:435-441
-206-
Halsted V/S. (1893) The Radical Cure of Inguinal Hernia in the Male. Johns. Hopkins.Hosp. Bull. 4:17-28.
Halsted WS. (1903) The cure of the more difficult as well as the simpler inguinalruptures. Johns. Hopkins. Hosp. Bull.208-214.
Halverson K and McVay CB. (1970) Inguinal and femoral hernioplasty: A 22-yearStudy of the authors'methods. Arch. Surg. 101:I27-135.
Hanafy M. (1993) Laparoscopic hernia repair: a review. Minimally Invasive Ther.2:229-236.
Hannon JK, Snow L, and Weinstein LS. (1993) Linear gastrectomy: An endoscopicstaple-assisted anterior highly selective vagotomy combined with posterior truncalvagotomy for treatment of peptic ulcer disease. Surg. Laparosc. Endosc. 2:254-257.
Hashikura Y, Kawasaki S, MunakataY, Hashimoto S, Hayashi K, and Makuuchi M.(1994) Effects of peritoneal insufflation on hepatic and renal blood flow. Surg. Endosc.8:759-761.
Hassan MA and Hobsley M. (1970) Positioning of subject and nasogastric tube during agastric secretion study. Br. Med. J. i:458-460.
Hasson HM. (1971) Modihed instrument and method for laparoscopy. Am. J. Obstet.Gynecol. 110:886-887.
Heij HA, Seldenrijk CA, and Vos A. (1991) Anterior gastropexy prevents gastrostomy-induced gastroesophageal reflux: an experimental study in piglets. J. Pediatr. Surg.26:557-559.
Heymann AD. (1977) The effect of incidental hypothermia on elderly surgical patientsJ. Gerontol . 32:146-148.
Heymann MA, Payne BD, Hoffman JIE, and Rudolph AM. (1977) Blood flowmeasurement with radionuclide-labeled particles. Prog. Cardiovasc. Dis.20:55-79
Hill GL and Barker MCJ. (1978) Anterior highly selective vagotomy with posteriortruncal vagotomy : a simple technique for denervating the parietal cell mass. Br. J. Surg.65:702-705.
Himpens JM. (1993) Laparoscopic inguinal hernioplasty. Repair with a conventional vsa new self-expandable mesh. Surg. Endosc. 7:315-318.
Ho HS, Gunther RA, and V/olfe BI|i4.. (1992) Intraperitoneal carbon dioxide insufflationand cardiopulmonary functions. Laparoscopic cholecystectomy in pigs. Arch. Surg.127:928-932.
-207 -
Hopkins HH. (1953) On the diffraction theory of optical images. Proc. Soc. Lond.A2Il:408
Hughes ES, McDermott FT, Polglase I, and Johnson WR. (1983) Tumor recurrence inthe abdominal wall scar after large bowel cancer surgery. Dis. Colon Rectum. 26:57I-572.
Hunt JN. (1974) A modif,rcation to the method of George for studying gastric emptyingGut. 17:812-813.
Hunter JG, Becker JM, Lee RG, Christian PE, and Dixon JA. (1989) Anterior lessercurvature laser seromyotomy with posterior truncal vagotomy: a potential treatment ofpeptic ulcer disease. Br. J. Surg. 76:949-952.
Imrie MM and Hall GM. (1991) Body temperature and anaesthesia. Br. J. Anaesth.64:346-354.
Ishizaki Y, Bandai Y, Shimomura K, Abe H, Ohtomo Y, and Idezuki Y. (1993a)Changes in splanchnic blood flow and cardiovascular effects following peritonealinsufflation of carbon dioxide. Surg. Endosc.T:420-423.
Ishizaki Y, Bandai Y, Shimomura K, Abe H, Ohtomo Y, and Idezuki Y. (1993b) Safeintraabdominal pressure of carbon dioxide pneumoperitoneum during laparoscoicsurgery. Surgery. 114:549-554.
Jacobaeus HC. (1910) Uber die Moglichkeit, die Zystoskopie bei Untersuschung serserHohlungen anzuwenden. Muenchner Med Wochenschr. 57 :2090-2092.
Jacobi C, Keller H'W, and Said S. (1994) Implantation metastasis of unsuspectedgallbladder carcinoma after laparoscopy. Br. J. Surg. 81(Suppl.):82(Abstract)
Jakeways MRS, Mitchell V, Hashim IA et al. (1994) Metabolic and inflammatoryresponses after open or laparoscopic cholecystectomy. Br. J. Surg. SI:127-I31.
Jamieson GG, Watson DI, Britten-Jones R, Mitchell PC, and Anvari M. (1994)Laparoscopic Nissen fundoplication. Ann. Sur g. 220(2):137 -l 45 .
Jarnagin WR, Duh QY, Mulvihill SJ, Ridge JA, Schrock TR, and Way LW. (1992) Theefficacy and limitations of percutaneous endoscopic gastrostomy. Arch. Surg.I27:261-264.
Johnston D and Wilkinson AR. (1969) Selective vagotomy with innervated antrumwithout drainage procedure for duodenal ulcer. Br. J. Surg. 56:626
Jorgensen JO, Gilles RB, Lalak NJ, and Hunt DR. (1994) Lower limb venoushemodynamics during laparoscopy: An animal study. Surg. Laparosc. Endosc.4:32-35
-208 -
Jorgenson JO, LalakNJ, North L, Hanel K, Hunt DR, and Morris DL. (1994) Venousstasis during laparoscopic cholecystectomy. Surg. Laparosc. Endosc.4:I28-I33.
Kashtan J, Green JF, Parsons EQ, and Holcroft JW. (1981) Hemodynamic effects ofincreased abdominal pressure. J. Surg. Res. 30:249-255.
Katkhouda N, Heimbucher J, and Mouiel J. (1994) Laparoscopic posterior vagotomyand anterior seromyotomy. End. Surg. 2:95-99.
Katkhouda N and Mouiel J. (1991) A new technique of surgical treatment of duodenalulcer without laparotomy by videocoelioscopy. Am. J. Surg. 161:36I-364.
Katkhouda N and Mouiel J. (1993) Laparoscopic treatment of inguinal hernias. End.Surg. l:193-197.
Kavic MS. (1995) Laparoscopic hernia repair. Three year experience. Surg. Endosc.9:12-15.
Kelling G. (1902) Uber Oesophagoskopie, Gastroskopie und Koelioscopie. MuenchnerMed Wochenschr. 49 :21-24.
Kern FH, Morana NJ, Sears JJ, and Hickey PR. (1992) Coagulation defects in neonatesduring cardiopulmonary bypass. Ann. Thorac. Surg. 54:541-546.
Kieturakis MJ, Nguyen DT, Vargas H, Fogarty TJ and Klein SR. (1994) Balloondissection facilitated laparoscopic extraperitoneal hernioplasty. Am. J Surg. 168:603-608.
Kipfmuller K, Naruhn M, Melzer A, Kessler S, and Buess G. (1989) Endoscopicmicrosurgical dissection of the esophagus. Results in an animal model. Surg. Endosc.3:63-69.
Kipfmuller K, Duda D, Kessler S, Melzer A, and Buess G. (1990) Endoscopicmicrosurgical dissection of the esophagus: a contribution to the reduction of pulmonarycomplications following esophageal resection? A comparative animal experiment studyLangenbecks Arch. Chir. 375: I 1-l 8.
Kitano S, Tomikawa M, and Iso Y. (1992) A safe and simple method to maintain a clearfield of vision during laparoscopic cholecystectomy. Surg. Endosc. 6:197-198.
Klemm B and Salm R. (1995) Vacuum-supported endoscopic access. End. Surg. 3:58-62.
Ifuight MT, Dawson R, and Melrose DG. (1977) Fibrinol¡ic response to surgery.Labile and stable patterns and their relevance to post-operative deep venous thrombosis.Lancet. 2:370-373.
-209 -
Kum CK and Goh P. (1992) Laparoscopic posterior truncal vagotomy and anteriorhighly selective vagotomy--a case report. Singapore. Med. J. 33:302-303.
Kum CK and Goh PMY. (1993) Laparoscopic vagotomy: A new toll in themanagement of peptic ulcer disease fletter]. Br. J. Surg.79:977
Kvietys PR, Shepherd AP, and Granger DN. (1998) Laser-doppler, H2 clearance, andmicrosphere estimates of mucosal blood flow. Am. J. Physiol. 249:G221-G227.
Lassen MR, Borris LC, Christiansen HM et al. (1991) Clinical trials with low molecularweight heparins in the prevention of postoperative thromboembolic complications: a
meta-analysis. Semin. Thromb. Hemost. 17 :284-290.
Laszlo A, Sprung J, Polic S, Kampine JP, and Bosnjak ZJ. (1990) Effects ofhypothermia and potassium variations on maximum diastolic potential. Anesthesiology.73:3A
Lauroy J, Champault G, Risk N, and Boutelier P. (1994) Metastatic recurrence at thecannula site: should digestive carcinomas still be managed by laparoscopy? Br. J. Surg.81(Suppl.):31.
Lavigne ME, Wiley ZD,Martin P. et al. (1979) Gastric, pancreatic and biliary secretionand the rate of gastric emptying after parietal cell vagotomy. Am. J. Surg. I 3 8 :6 44-65L
Leahy PF, Pennino RP, Hinshaw JR, O'Connor TP, andLanzafame RI. (1990)Minimally invasive esophagogastrectomy: an approach to esophagogastrectomythrough the left thorax. J. Laparoendosc. Surg. l:59-62.
Lichenstein IL, Shulman AG, Amid PK, and Montllor MM. (1989) The Tension-FreeHernioplasty. Am. J. Surg. 157:188-193.
Lichtenstein IL and Shore JM. (1976) Exploding the myths of hernia repair. Am. JSurg. 132:307
Lloyd DM, Vipond M, Robertson GSM, Hanning C, and Veitch PS. (1994)Thoracoscopic oesophago-gastrectomy - A new technique for intra-thoracic stapling.End. Surg.2:26-31.
Lointier P, Bail JP, Bourlier P, Person H, and Senecail B. (1993a) Thoracoscopicdissection of the esophagus in human cadavers. J. Laparoendosc. Surg. 3:177-186.
Lointier P, Leroux S, Ferrier C, and Dapoigny M. (1993b) A technique of laparoscopicgastrectomy and billroth ii gastrojejunpstomy. J. Laparoendosc. Surg. 3:353-363.
Ludbrook J. (1994) Repeated measurements and multiple comparisons in cardiovascularresearch. Cardiovasc. Res. 28:303 -3 I | .
-2to -

Lukaszcyryk JJ and PreletzzuJ. (1992) Laparoscopic resection of benign stromal tumorof the stomach. J. Laparoendosc. Surg. 2:331-335.
Lundquist PB and Sewdenborg J. (1981) Postoperative hypercoagulability, detectionand measurement using a modified recalcification time system, effects of low doseheparin and types of surgery. Thromb. Haemost. 46:16
MacFayden BV, Arregui M, Corbitt J, and et al. (1993) Complications of laparoscopichernionhaphy. Surg. Endosc. 7: I 55-1 58.
Maddern GJ, Rudkin G, Bessell JR, Devitt P, and Ponte L. (1994) A comparison oflaparoscopic and open inguinal hernia repair as a day surgical procedure. Surg. Endosc.8:1404-1408.
Manncke K, Raestrup H, Kanehira E, weiss u, and Buess G. Q99a$ ThoracoscopicOesophagectomy with Intrathoracal Stapled Anastomosis. End. Surg. 2:37 -41.
Manncke K, Raestrup H, 'Walter D, Buess G, and Becker HD. (1994b) Technique ofEndoscopic Mediastinal Dissection of the Oesophagus. End. Surg. 2:10-15.
Mannell A and Becker PJ. (1991) Evaluation of the results of oesophagectomy foroesophageal cancer. Br. J. Surg.78:36-40.
Mansberger JA and Kavouklis JH. (1990) combined endoscopic and surgicalgastrostomy when percutaneous endoscopic gastrostomy is contraindicated. Am. Surg56:138-140.
Martinez JIA, Blanco CIT, Ballesteros ML et al. (1988) Estudio de las modificacionestromboelastograf,rcas inducidas por la heparinizacion prolifactica en cirugia general. CirEsp. 43(4):518-526.
Martinoli S. Lower oesophageal sphincter function. 1982;l(2):62-65
Mattheussen MD, Boutros A, Van Aken H, and Flameng W. (1990) Effect of theVolatile Anesthetics on the Hypothermic Myocardium. Anesthesiology. 73:A574
Matthews, H.R., Waterhouse, J.A.H., Powell, J., Robertson, J. and McConkey, C.C.(1987) In: Cancer of the oesophagus, pp. 59-91. London: Macmillan Press.
McAnena OJ, Rogers J, and Williams NS. (1994) Right Thoracoscopically AssistedOesophagectomy for Cancer. Br. J. Surg. 81:236-238.
McKernan JB. (1993) Laparoscopic extraperitoneal repair of inguiofemoral herniation.End. Surg. I:198-203.
McKernan JB and Laws HL. (1993) Laparoscopic repair of inguinal hernias using atotally extraperitoneal prosthetic approach. Surg. Endosc. 7 :26-28.
-2tt -
McKeman JB and Champion JK. (1995) Access techniques: Veress needle - initialblind trocar insertion versus open laparoscopy with Hasson trocar. End. Surg. 3:35-38.
Mclaughlin JG, Scheeres DE, Dean RJ, and Bonnell BW. (1995) The adversehemodynamic effects of laparoscopic cholecystectomy. Surg. Endosc. g:l2l-r24
McVay CB. (1989) Groin Hernioplasty: Cooper Ligament Repair. In: Nyhus, L.M.(Ed.) Hernia, pp. 119-136. Philadelphia: JP Lippincott.
McVay CB and Anson BJ. (1942) A fundamental error in current methods of inguinalherniorrhapy. Surg Gynecol. Obstet. 7 4:7 46-7 50.
Melzer A, Riek S, Roth K, and Buess G. (1995) Endoscopically controlled trocar andcannula insertion. End. Surg. 3:63-68.
Milkins RC, Lansdown MJR,'Wedgewood KR, Brough WA, and Royston CMS. (1993)Laparoscopic hernia repair: a prospective study of 409 cases. Minimally Invasive Ther.2:237-242.
Millard JA, Hill BB, cook PS, Fenoglio ME, and stahlgren LH. (1993) Intermittentsequential pneumatic compression in prevention of venous stasis associated withpneumoperitoneum during laparoscopic cholecystectomy. Arch. Surg. 128:9I4-9I9.
Millikan KW, Kosik ML, and Doolas A. (1994) A preospective comparison oftransabdominal preperitoneal laparoscopic hernia repair versus traditional open herniarepair in a University setting. Surg. Laparosc. Endosc. 4(4):247-253.
Mintz M. (1977) Risk and prophylaxis in laparoscopy. J. Reprod. Med. 18:269-272.
Mitchell PC and Jamieson G. (1994) Coeliac axis and mesenteric arterial thrombosisfollowing laparoscopic Nissen fundoplication. Aust. N. Z. J. Surg.64:728-730.
Monagle J, Bradfield S, and Nottle P. (1993) Carbon dioxide, temperature andlaparoscopic cholecystectomy. Aust. N. Z. J. Surg.63:186-189.
Morris DL, Harrison JD, Jorgensen Jo, Perkins AC, and Stanley J. (1993) Posteriortruncal vagotomy and stapling of the anterior stomach wall in 30 patients with duodenalulcer: Acid inhibition, gastric emptying and endoscopic dye spraying. Prospects forendoscopic vagotomy. Surg. Laparosc. Endosc. 3:375-380.
Morris RH. (1971) Influence of ambient temperature on patient temperature duringintraabdominal surgery. Ann. Surg. I 73 (2):230 -233 .
Morris RH and Kumar A. (1972) The effect of warming blankets on maintenance ofbody temperature of the anethetized, paralysed adult patient. Anesthesiology. 36:408-411.
-212-

Morris RH and Wilkey B. (1970) The effects of ambient temperature on patienttemperature during surgery not involving body cavities. Anesthesiology. 32:102-107.
Morrison JA. (1993) Laparoscopic inguinal herniorrhaphy. Can. J. Surg. 34(4):326-325
Mouiel J and Katkhouda N. Laparoscopic posterior truncal vagotomy and anteriorseromyotomy . I 9 92 ;(21) :263 -27 2.
Murphy C, Rosemurgy AS, Albrink MH, and Carey LC. (1992) A simple technique forlaparoscopic gastrostomy. Surg Gynecol. Obstet. 17 4:424-425 .
Nagai H, Inabo T, and Kamiya S. (1991) A new method of laparoscopiccholecystectomy: an abdominal wall lifting technique without pneumoperitoneumSurg. Laparosc. Endos c. I :126
Nathanson LK. (1995) Trocars and other access techniques. End. Surg. 3:33-34.
Neugebauer E, Troidl H, Spangenberger W, Dietrich A, Lefering R, and TheCholecystectomy Study Group. ( 1 99 1 ) Conventional versus laparoscopiccholecystectomy and the randomized controlled trial. Br. J. Surg. 78:150-154
Newman L, Eubanks S, Mason E, and Duncan TD. (1993) Is laparoscopicherniorrhaphy an effective alternative to open hernia repair? J. Laparoendosc. Surg3(2):t2I-128.
Norgrenj and Svensson JO. (1985) Anal implantation metastases with carcinoma of thesigmoid colon and rectum - a risk when performing anterior resection with the EEAstapler. Br. J. Surg.72:602
Nottle PD. (1991) Laparoscopic vagotomy for chronic duodenal ulcer. Med. J. Aust.155:648
Nyhus LM, Condon RE, and Harkins HN. (1960) Clinical experiences withpreperitoneal hernial repair for all types of hernia of the groin. Am. J. Surg. 100:234-244.
Nyhus LM, Pollak R, Bombeck CT, and Donahue PE. (1988) The preperitonealapproach and prosthetic buttress repair for recurrent hernia: The evolution of atechnique. Ann. Surg. 208:7 33 -7 37 .
Nylamo EI. (1987) Relationship between gastric acid secretion and clinical outcomeafter parietal cell vagotomy. Acta Chir. Scand. 153:33-36.
Oostvogel HJM and van Vroonhoven TJMV. (1988) Anterior lesser curveseromyotomy with posterior truncal vagotomy versus proximal gastric vagotomy. Br. JSurg. 75: I2l-124.
-2t3 -
Orringer MB. (1984) Transhiatal esophagectomy without thoracotomy for carcinoma ofthe thoracic esophagus. Ann. Surg. 200:282-288.
Oninger MB and Sloan H. (1978) Esophagectomy without thoracotomy. J. ThorCardiovasc. Surg. 7 63 -654:643 -654.
Oshinsky GS and Smith AD. (1992) Laparoscopic needles and trocars: an overview ofdesigns and complications. J. Laparoendosc. Surg. 2:lI7-125.
Ott DE. (1991a) Laparoscopic hypothermia. J. Laparoendosc. Surg. l:127-131
Ott DE. (1991b) Correction of laparoscopic insufflation hypothermia. J. LaparoendoscSurg.1:183-186.
Paget GV/. (1994) Laparoscopic inguinal hernionhaphy.Med. J. Aust. 161:249-253.
Panton ONM and Panton RJ. (1994) Laparoscopic hernia repair. Am. J. Surg. 167:535-537
Paul A, Troidl H, Peters S, and Stuttmann R. (1994) Fatal intestinal ischaemiafollowing laparoscopic cholecystectomy. Br. J. Surg . 8I:1207
Payne JH, Grininger LM, IzawaMT, Podoll EF, Lindahl PJ, and Balfour J. (1994)Laparoscopic or open herniorrhaphy. Arch. Surg. 129:973-981.
Peden CJ and Prysroberts C. (1993) Capnothorax - Implications for the Anaesthetist.Anaesthesi a. 48 :664-666.
Peracchia A, Ancona E, Ruol A, Bardini R, Segalin A, and Bonavina L. (I992a) Use ofmini-invasive procedures in esophageal surgery. Chirurgie. 1 1 8 :305-309.
Perissat J, Collet DR, and Belliard R. (1989) Gallstones, laparoscopic treatment,intracorporeal lithotripsy followed by cholecystostomy or cholecystectomy: A personaltechnique. Endoscopy . 2I :37 3 -37 4.
Peto. (1972) Rank tests of maximal power against Lehmann type altematives.Biomedika. 59:472-47 4.
Phillips EH, Arregui M, Carroll BJ et al. (1995) Incidence of complications followinglaparoscopic hernioplasty. Surg. Endosc. 9 :l 6-21 .
Pietrafitta JJ, Schultz LS, Graber JN, and Hickok DF. (1991) Laser laparoscopicvagotomy and pyloromyotomy. Gastrointest. Endosc. 37 :338-3 43 .
Polglase AL and McMurrick PJ. (1994) Laparoscopic or open repair of inguinalhernias? Med. J. Aust. 161:238-239.
-214-

Ponsky JL and Gauderer MW. (1989) Percutaneous endoscopic gastrostomy:indications, limitations, techniques, and results. V/orld J. Surg. 13:165-170.
Popp LV/. (1993) Hemioscopic stuffing of direct inguinal hemia in female patientsusing resorbable mesh. Surg. Endosc. T:22-25.
Ralphs DNL, Brain AJL, Grundy DJ, and Hobsley M. (1980) How accurately can directand indirect inguinal hernias be distinguished? Br. Med. J. 280:1039-1040.
Ramos JM, Gupta S, Anthone GJ, Ortega AE, Simons AJ, and Beart RW Jr. (1994)Laparoscopy and colon cancer. Is the port site at risk? A preliminary report. 129:897-899.
Rand Corporation. (1983) Conceptualisation and measurement of physiologic health foradults. 1983;3-120.
Ravitch, M.M. (1969) Repair of hernia, Chicago: Year Book Medical.
Read RC. (1989) Preperitoneal herniorrhaphy: A historical review. V/orld J. Surg.13:532-540.
Reddick EJ and Olsen DO. (1990) Outpatient laparoscopic laser cholecystectomy. Am.J. Surg. 160:485-489.
Roe CF. (197I) Effect of bowel exposure on body temperature during surgicaloperations. Am. J Surg. 122:13-15.
Rosenfeld BA, Beattie C, Christopherson R et al. (1993) The effects of differentanesthetic regimens on fibrinolysis and the development of postoperative arterialthrombosis. Anesthesiology. 7 9(3):43 5-443.
Rossi M. (1994) Flexistap@BC: A new flexible circular stapler for endoscopic surgery.End. Surg.2:69-70.
Rowbotham BJ, Whitaker AN, Harrison J, Murtaugh P, Reasbeck P, and Bowie EJW.(1992) Measurement of crosslinked fibrin derivatives in patients undergoing abdominalsurgery. Blood Coag. Fibrin. 3:25-31.
Ruddock JC. (1934) Peritoneoscopy. 'Western J Surg. 42:392
Rudolph AM and Heymann MA. (1967) The circulation of the fetus in utero. Circ. Res2I:163-184.
Rudolph AM and Heymann MA. Measurement of flow in perfused organs, usingmicrosphere technique s. 197 I ;I 12-127 .
Russell TR, Brotman M, and Noris F. (1984) Percutaneous gastrostomy. A new andcost-effective technique. Am. J. Surg. 148:132-137.
-215 -

Rutledge RH. (1988) Cooper's ligament repair: A25-year experiences with a singletechnique for all groin hernias in adults. Surgery. 103:l-10.
Safran DB and Orlando R. (1994) Physiological effects of pneumoperitoneum. Am. JSurg. 167:281-286.
Salerna GM, Fitzgibbons RJ, and Filipi CJ. Laparoscopic inguinal hemia repairl99l;l:281-293.
Sali A, Wong P, Read A, McQuillan T, and Conboy D. (1993) Percutaneous endoscopicgastrostomy: the heidelberg repatriation hospital experience. Aust. N. Z. J. Surg.63:545-550.
Schaller G, Kuenkel M, and Manegold BC. (1995) The optical "Veress needle" - initialpuncture with a minioptic. End. Surg. 3:55-57.
Schaub RD, Lynch PR, and Stewart GJ. (1978) The response of canine veins to threetypes of abdominal sugery: a scanning and transmission electron microscope study.Surgery. 83:4lI-424.
Schauer PR and Schwesinger'WH. (1995) Hemodynamic effects of laparoscopy. Surg.Endosc. 9:ll9-120.
Schedl PH. (1966) Use of polyethylene glycol and phenol red as unabsorbed indicatorsfor intestinal absorption studies in man. Gut. 7:159
Schneider TA, Wittgen CM, Andrus CH, and Kaminski DL. (1992) Comparison ofminimally imvasive methods of parietal cell vagotomy in a porcine model. Surgery.l12:649-654.
Schneider TA and Andrus CH. (1992) The endoscopic Congo red test during proximalgastric vagotomy: an essential procedure. Surg. Endosc. 6:16-17.
Schulman AG, Amid PK, and LichtensteinlL. (1992) The safety of mesh repair forprimary inguinal hernias: Results of 3019 operations from five diverse surgical sources.Am. Surg. 58:255-7.
Schulman AG, Amid PK, and Lichenstein IL. (1994) Patch or plug for groin hernia.Am. J. Surg. 167:331-336.
Schultz L, Graber J, Pietrafitta JJ, and Hickok D. (1990) Laser laparoscopicherniorrhaphy: a clinical trial. Preliminary results. J. Laparoendosc. Surg.l:41-45
Schurr MO and Buess G. (1993) V/ittmoser's technique of thoracoscopicsympathectomy and vagotomy. End. Surg. l:266-270.
-216-
Scott TR, Zucker KA, and Bailey RW. (1992) Laparoscopic cholecystectomy: a reviewof 12,397 patients. Surg. Laparosc. Endosc.2:I9l-198.
Seid AS, Deutsch H, and Jacobson A. (1992) Laparoscopic hernionhaphy. Surg.Laparosc. Endosc. 2:59-60.
Seitzinger MR and Dudgeon LS. (1993) Decreasing the degree of hypothermia duringprolonged laparoscopic procedures. J. Reprod. Med. 38:511-513.
Semm K. (1983) Endoscopic appendicectomy. Endoscopy. 15:59-64.
Sessler DI, Hynson J, McGuire J, Moayeri A, and Heier T. (1992) Thermoregulatoryvasoconstriction during isofluorane anaesthesia minimally decreases heat loss.Anesthesiology . 7 6:67 0-67 5 .
Sessler DI. (1993) Perianesthetic thermoregulation and heat balance in humans. FASEB1.7:638-644.
Shallman RW. (1991) Laparoscopic percutaneous gastrostomy. Gastrointest. Endosc.37:493-494.
Shanks CA, Ronai AK, and Schafer MF. (1988) The effects of airway heat conservationand skin surface insulation on thermal balance during spinal surgery. Anesthesiology.69:956-958.
Shapiro S, Gordon L, Dayhkovsky L, Grundfest W, and Chandra M. (1991)Development of laparoscopic anterior seromyotomy and right posterior truncalvagotomy for ulcer prophylaxis. J. Laparoendosc. Surg. 1 :277-286.
Shearburn EW and Myers RN. (1969) Shouldice repair for inguinal hernia. Surgery.66:450-459.
Sheflreld CW, Sessler DI, and Hunt TK. (1994) Mild hypothermia during isofluoraneanesthesia decreases resistance to e.coli dermal infection in guinea pigs. Anesth. Analg.38(3):201-205.
Siewert JR, Holscher AH, and Horvart OP. (1986) TransmediastinaleOesophagektomie. Langenbecks. Arch. Chir. 367 :203-213.
Sigman HH, Fried GM, Garzon J, Hinchey EJ, V/exler MJ, Meakins JL, and Barkun JS.(1993) Risks of blind versus open approach to celiotomy for laparoscopic surgery. Surg.Laparosc. Endosc. 3 :296-299
Skandalakis LJ, Gray S'W, and Skandalakis JE. (1986) The history and surgicalanatomy of the vagus nerve. Surg Gynecol. Obstet. 162:75-85.
Slotman GJ, Jed EH, and Burchard KW. (1985) Adverse Effects of hypothermia inpostoperative patients. Am. J. Surg. 149:495-501.
-217 -
Smith RS, Fry WR, Tsoi EKM et al. (1993) Gasless laparoscopy and conventionalinstruments. Arch. Surg. 128 :1102-1107.
Snyders D. (1993) Laparoscopic pyloroplasty for duodenal ulcer fletter]. Br. J. Surg.80:127
Stevens WC, Cromwell TH, Halsey MJ, Eger EI, Shakespeare TF, and Bahlman SH.(197I) The cardiovascular effects of a new inhalational anesthetic, Forane, in humanvolunteers at constant aretrial carbon dioxide tension. Anesthesiology. 35:8-16.
Stewart JR, Hoff SJ, and Johnson DH. (1993) Improved survival with neoadjuvanttherapy and resection for adenocarcinoma of the esophagus. Ann. Surg. 218:571-578
Stiegmann GV, Goff JS, Silas D, Pearlman N, Sun J, and Norton L. (1990) Endoscopicversus operative gastrostomy: final results of a prospective randomized trial.Gastrointest. Endosc. 3 6:I -5.
Stoker D, Spiegelhalter DJ, Singh R, and Wellwood JM. (1994) Laparoscopic versusopen inguinal hernia repair: Randomised prospective trial. Lancet. 343:1243-1245.
Stoppa RE and'Warlaumont CR. (1993) The Preperitoneal Approach and ProstheticRepair of Groin Hernia. In: Nyhus LM. (Ed.) Hernia, pp.199-225. Philadelphia: JPLippincott.
Sugarbaker PH and Wilson RE. (1976) Using celioscopy to determine stages ofintraabdominal malignant neopasms. Arch. Surg. I Il:41.
Taylor TV. (1982) Lesser curve seromyotomy. In: Baron JH, Alexander-Williams J,
Allgower M, Muller C, and Spencer J. (Eds.) Vagotomy in Modern Surgical Practice,pp. 132-137. London: Butterworths.
Taylor TV. (1982b) Anterior lesser curve seromyotomy and posterior truncal vagotomyin the treatment of chronic duodenal ulcer. Lancet. 2(8303):846-843.
Taylor TV. (1985) Mortality and morbidity after anterior lesser curve seromyotomywith posterior truncal vagotomy for duodenal ulcer. Br. J. Surg .72:950-95I.
Taylor TV, Lythgoe JP, McFarland JB, Gilmore IT, Thomas PE, and Ferguson GH.(1990) Anterior lesser curve seromyotomy and posterior truncal vagotomy versustruncal vagotomy and pyloroplasty in the treatment of chronic duodenal ulcer. Br. J
Surg. 77:1007-1009.
Temple JG and McFarland J. (197 5) Gastro-oesophageal reflux complicating highlyselective vagotomy. Br. Med. J.2:168-169.
Tollofsrud S, Gunderson Y, and Anderson R. (1984) Perioperative hypothermia. ActaAnaesthesiol. Scand. 28:5 1 1-5 I 5.
-2r8-
Toy FK and Smoot RT. (1992) Laparoscopic hernioplasty update. J. LaparoendoscSurg. 2(5):197 -205.
Veress J. (1938) Ein neues Instrument zur Ausfuhrung von Brustoder Bauchpunktionenund Pneumothoraxbehandlung. Deut Med'Wachenschr. 64 : I 480- 1 48 1 .
Voeller GR, Pridgen WL, and Mangiante EC. (1991) Laparoscopic posterior truncalvagotomy and anterior seromyotomy: a porcine model. J. Laparoendosc. Surg. 1:375-8,379 dis.
Voeller GR, Mangiante EC, and Britt LG. (1993) Preliminary evaluation oflaparoscopic herniorrhaphy. Surg. Laparosc. Endosc. 3 : 1 00- 1 05.
Vogt DM, Curet MJ, Pitcher DE, Martin DT, and Zucker KA. (1995) Preliminaryresults of a preospective randomised trial of laparoscopic onlay versus conventionalinguinal herniorrhaphy. Am. J. Surg. 169:84-90.
Voyles CR. (1992) Education and engineering solutions for potential problems withlaparoscopic monopolar electrosurgery. Am. J Surg. I 64:57 -62.
Voyles CR, Haick AJ, and Koury AM. (1992) Trocar cannulas in laparoscopic surgery.Surgical Rounds. I 5 :7 99 -804.
Wagner HN, Rhodes BA, Sasaki Y, and Ryan JP. (1969) Studies of the circulation withradioactive microspheres. Invest. Radiol. 4:37 4-386.
Walenga JM, Hoppensteadt D, Fareed J, and Pifarre R. (1992) Hemostaticabnormalities in total artificial heart patients as detected by specific blood markersAnn. Thorac. Surg. 53:844-850.
Wallasvaara MP. (1992) Ventilation and body temperatures during laparoscopic vsopen cholecystectomy. Anesth. Analg. 74:5340
Warfiz GE. (1989) The Canadian Repair: Personal observations. World J. Surg. 13:516-s2r.
Vy'arshaw AL, Tepper JE, Shipley WH. (1986) Laparoscopy in the staging and planningof therapy for pancreatic cancer. Am. J. Surg. 151 :76.
Wexner SD and Cohen SM. (1995) Port site metastases after laparoscopic colorectalsurgery for cure of malignancy. Br. J. Surg. 82:295-298.
Wheeler KH. (1993) Laparoscopic inguinal hemiorraphy with Mesh: An 18-monthexperience. J. Laparoendosc. Surg. 3 (4) : 3 45-3 5 0.
Wheler KH. (1993) Laparoscopic inguinal herniorrhaphy with mesh: An l8-monthexperience. J. Laparoendosc. Surg. 3 :345-350.
-2t9 -
Wilbur BG and Kelly KA. (1973) Effect of proximal gastric, and truncal vagotomy oncanine gastric electric activity, motility and emptying. Ann. Surg. 178:295-303.
V/illiams MD and Mun PC. (1993) Laparoscopic insufflation of the abdomen depressescardiopulmonary function. Surg. Endo sc. 7 :12-I 6.
Wilson YG, Allen PE, Skidmore R, and Baker AR. (1994) Influence of compressionstocking on lower limb venous haemodynamics during laparoscopic cholecystectomy.Br. J. Surg. 8l:841-844.
Winchester DJ, Dawes LG, Modelski DD et al. (1993) Laparoscopic inguinal herniarepair - a preliminary experience. Arch. Surg. 128:781-786.
\ù/ong J. (1987) Esophageal resection for cancer : The rationale of current practice. Am.J. Surg. 153:18-24.
Wong J, Cheung H, Lui R, Fan YW, Smith A, and Sui KF. (1987) Esophagogastricanastomosis performed with a stapler: The occurence of leakage and stricture. Surgery101:408-414.
V/oodward ER. (1987) The History of Vagotomy. Am. J. Surg. 153:9-17
-220 -