Romanian Journal of - Military Medicine
84
• Efficacy and tolerability of antibiotic augmentation in schizophrenia spectrum disorders – A systematic literature review • Nonoperative management of high-grade splenic injury • Atherosclerosis in rheumatoid arthritis – The importance of imaging testing • Managing radial nerve injuries associated with humeral fracture • Intraoperative parathyroid hormone assay in patients with primary hyperparathyroidism • Metformin – Old treatment for diabetes, new treatment for psoriasis • Improving the outcomes for pregnancies in the context of kidney disease • Differential diagnosis in case of overdose of antiepileptic treatment – Case presentation • Cross-leg limb salvage solution: A case report regarding the management of a major defect in a patient with type IIIB open distal tibial fracture • Clinical and dermatoscopical aspects of pigmented basal cell carcinoma – Case series and literature review • Compliance of school doctors’ practice with medical legislation • In memoriam – General (Ret.) Academician Prof. Vasile Cândea MD, PhD www.revistamedicinamilitara.ro Founded 1897 • New Series Vol. CXXIII • No. 1/2020 • February REVISTA DE MEDICINĂ MILITARĂ Military Medicine Romanian Journal of Journal included in Web of Science, Emerging Sources Citation Index, Index Copernicus International, National Library of Medicine Catalog, Ulrich’s Periodicals Directory database, Directory of Open Access Journals, Directory of Research Journals Index, Eurasian Scientific Journal Index, Science Library Index and Open Academic Journals
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Romanian Journal of - Military Medicine

• Efficacy and tolerability of antibiotic augmentation in schizophrenia spectrum disorders – A systematic literature review
• Nonoperative management of high-grade splenic injury
• Atherosclerosis in rheumatoid arthritis – The importance of imaging testing
• Managing radial nerve injuries associated with humeral fracture
• Intraoperative parathyroid hormone assay in patients with primary hyperparathyroidism
• Metformin – Old treatment for diabetes, new treatment for psoriasis
• Improving the outcomes for pregnancies in the context of kidney disease
• Differential diagnosis in case of overdose of antiepileptic treatment – Case presentation
• Cross-leg limb salvage solution: A case report regarding the management of a major defect in a patient with type IIIB open distal tibial fracture
• Clinical and dermatoscopical aspects of pigmented basal cell carcinoma – Case series and literature review
• Compliance of school doctors’ practice with medical legislation
• In memoriam – General (Ret.) Academician Prof. Vasile Cândea MD, PhD
www.revistamedicinamilitara.ro
Founded 1897 • New Series
Vol. CXXIII • No. 1/2020 • February
REVISTA DE MEDICINĂ MILITARĂ
Military Medicine Romanian Journal of
Journal included in Web of Science, Emerging Sources Citation Index, Index Copernicus International, National Library of Medicine Catalog, Ulrich’s Periodicals Directory database, Directory of Open Access Journals, Directory of Research Journals Index, Eurasian Scientific Journal Index, Science Library Index and Open Academic Journals

Editorial Board of Romanian Journal of Military Medicine
Under the patronage Romanian Association of Military Physicians Carol Davila University of Medicine and Pharmacy, Bucharest, Romania
Honorary Editor Acad. Victor Voicu MD, PhD
Editors-in-Chief Florentina Ioniță Radu MD, PhD, MBA Dan Mischianu MD, PhD
Executive Editors Daniel O. Costache MD, PhD, MBA Victor L. Purcărea PhD, MBA
Associate Editor Mariana Jinga MD, PhD, MBA
Redactors Raluca S. Costache MD, PhD, MBA – Bucharest Mihail S. Tudosie MD, PhD – Bucharest
Editorial Assistants Ioana Bratu MD Cristina Solea
Technical Secretary Oana Ciobanu Ionuț M. Olteanu
Publisher Carol Davila University of Medicine and Pharmacy Publishing House
International Editorial Board
Natan Børnstein (Israel) Silviu Brill (Israel)
Cris S. Constantinescu (UK) Daniel Dănilă (USA)
Stergios Ganatsios (Greece)
Mihai Moldovan (Denmark) Ioan Opriș (USA)
Gerard Roul (France) Erwin Santo (Israel)
Adrian Săftoiu (Denmark)
Ioanel Sinescu (Romania) C. Ionescu Târgovişte (Romania)
Radu Ţuţuian (Switzerland) Shyam Varadarajulu (USA) Peter Vilmann (Denmark)
Scientific Publishing Committee
Adrian Barbilian (Bucharest) Anda Băicuş (Bucharest)
Cristian Băicuş (Bucharest) Andra R. Bălănescu (Bucharest)
Mircea Beuran (Bucharest) Ovidiu Bratu (Bucharest)
Daciana Brănișteanu (Iași) Dragoș Bumbăcea (Bucharest)
Marian Burcea (Bucharest) Mihai Ciocârlan (Bucharest) Cătălin Cârstoiu (Bucharest)
Sofia Colesca (Bucharest) Gabriel Constantinescu (Bucharest)
Silviu Constantinoiu (Bucharest)
Dan Corneci (Bucharest) Raluca S. Costache (Bucharest)
Dragoș Cuzino (Bucharest) Camelia Diaconu (Bucharest) Mircea Diculescu (Bucharest)
Lidia Dobrescu (Bucharest) Cosmin Dobrin (Bucharest)
Dumitru Constantin Dulcan (Bucharest) Silviu Dumitrescu (Bucharest)
Carmen G. Fierbințeanu (Bucharest) Cristian Gheorghe (Bucharest) Liana S. Gheorghe (Bucharest)
Viorel Jinga (Bucharest) Carmen Moldovan (Bucharest)
Ovidiu Nicodin (Bucharest) Tudor Nicolaie (Bucharest)
Ana Maria Oproiu (Bucharest) Carmen Orban (Bucharest)
Bogdan A. Popescu (Bucharest) Aurelian E. Ranetti (Bucharest)
Mugurel Rusu (Bucharest) Andrada Seicean (Cluj Napoca)
Carmen A. Sîrbu (Bucharest) Silviu Stanciu (Bucharest)
Ion Țintoiu (Bucharest) Sorin G. Țiplica (Bucharest) Daniel Vasile (Bucharest)
Dragoş Vinereanu (Bucharest)
REDACTION
B-dul Eroii sanitari, Nr.8, Sector 5, București, Tel/fax 021/318.07.59, tel. 021/318.08.62/Int. 199; Email [email protected] Romanian Journal of Military Medicine (RJMM) is included in Romanian College of Physicians Medical Publications Index.
www.revistamedicinamilitara.ro
Romanian Journal of Military Medicine, New Series, vol. CXXIII, No 1/2020, February ISSN-L 1222-5126; eISSN 2501-2312; pISSN 1222-5126

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
1
Founded 1897 • New Series Vol. CXXIII • No. 1/2020 • February
Contents
SYSTEMATIC REVIEW Octavian Vasiliu, Daniel Vasile, Victor Voicu
● Efficacy and tolerability of antibiotic augmentation in schizophrenia spectrum disorders – A systematic literature review 3
REVIEW ARTICLE Bogdan Socea, Cristiana Bogaciu, Alexandru C. Carâp, Vlad D. Băleanu, Dragoş V. Daviţoiu, Tiberiu Ş. Ţenea
Cojan, Ion Păun, Vlad D. Constantin ● Nonoperative management of high-grade splenic injury 21
Oana P. Ionescu, Silviu M. Stanciu, Mihai L. Ciobîcă ● Atherosclerosis in rheumatoid arthritis – The importance of imaging testing 26
ORIGINAL ARTICLES V. Cărbunaru, Alexandra Ciotei, Mihaela I. Zaharia
● Managing radial nerve injuries associated with humeral fracture 32 Cornelia Nițipir, Lucian Alecu, Iulian Slavu, Mădălina Mușat, Raluca Tulin, Bogdan Socea, Adrian Tulin
● Intraoperative parathyroid hormone assay in patients with primary hyperparathyroidism 37
Bogdan Șerban, Camelia C. Diaconu, Ana Maria A. Stănescu, Daniel O. Costache, Raluca S. Costache, Cătălin Cîrstoiu ● Metformin – Old treatment for diabetes, new treatment for psoriasis 42
Mona Zvâncă, Aida Petca, Oana Baltă, Mihaela Boț, Claudia Mehedințu, Nicoleta Măru, Răzvan Petca ● Improving the outcomes for pregnancies in the context of kidney disease 46
CLINICAL PRACTICE Mihail S. Tudosie, Genica Caragea, Ana D. Radu, Ilenuţa L. Dănescu
● Differential diagnosis in case of overdose of antiepileptic treatment – Case presentation 53 M. Turbatu, C. Condrea, A. Oproiu, A. Cursaru, A. Lupu
● Cross-leg limb salvage solution: A case report regarding the management of a major defect in a patient with type IIIB open distal tibial fracture 58
Anton M. Țilea, Viorel Trifu, Bogdan Dima, Mihai A. Badea, Raluca S. Costache, Daniel O. Costache, George S. Țiplica ● Clinical and dermatoscopical aspects of pigmented basal cell carcinoma – case series and literature review 62

2
VARIA Silviu Păun, Luiza M. Vasile, Sînziana Bîrsanu, Codruț A. Nanu
● Compliance of school doctors’ practice with medical legislation 69
*** ● In memoriam – General (Ret.) Academician Prof. Vasile Cândea MD, PhD 74
Guidelines for authors 77

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
3
Article received on October 4, 2019 and accepted for publishing on January 8, 2020. SYSTEMATIC REVIEW
Efficacy and tolerability of antibiotic augmentation in schizophrenia spectrum disorders – A systematic literature review
Octavian Vasiliu1, Daniel Vasile2, Victor A. Voicu2,3
Abstract: Background: A large number of augmentation agents have been tried in patients with schizophrenia spectrum disorders, because negative and cognitive symptoms are difficult-to-treat with current pharmacological agents, and because the high percentage of treatment-resistant cases requires new therapeutic solutions. Inflammation is one of the supposed pathophysiological mechanisms in schizophrenia; therefore, antibiotics have been explored as add-on agents. No systematic review or meta-analysis about the efficacy of antibiotics in psychotic disorders has yet been conducted. Objectives: To assess if the use of antibiotics as add-on to current antipsychotic treatment may improve core symptoms of schizophrenia spectrum disorders, global clinical status, overall functionality, and if this augmentation strategy is well tolerated. Methods: A systematic literature review was conducted, including papers published between 1980 and 2018, which have been found in the main electronic databases (PubMed/MEDLINE, CINAHL, NCBI, Embase, Thomson Reuters/Web of Science). The keyword search strategy was formulated using the following paradigm: „schizophrenia spectrum disorders”/ „schizophrenia”/ „schizo-affective disorder”/ „schizophreniform disorder”, AND „antibiotics”/ all the names of currently marketed antibiotics classes. This review was registered to PROSPERO database with the protocol number CRD42019119152. Results: Based on reviewing the selected trials regarding the efficacy of antibiotics over core symptoms of schizophrenia, only two agents were detected – minocycline and D-cycloserine. Minocycline as add-on to antipsychotic treatment was associated with mixed results, while regarding the efficacy of d-cycloserine either no significant difference, or superiority to placebo over negative and cognitive symptoms was reported. Minocycline had an overall effect over the clinical impression that was not distinguishable from placebo, although there was one trial supporting the efficacy of this antibiotic. The impact of minocycline over the global functioning when added to antipsychotic in patients with schizophrenia was mixed, with one positive and one negative trial (moderate to high quality designed trials). D-cycloserine had no significant impact over global clinical status or patients’ overall functionality. Conclusion: From all the data reviewed and hierarchized resulted that larger trials are needed in order to confirm the efficacy of antibiotics as add-on to antipsychotics over negative and cognitive symptoms of schizophrenia spectrum disorders.
Keywords: antibiotics, augmentation strategy, negative symptoms, cognitive symptoms, tolerability, schizophrenia spectrum disorders
BACKGROUND
Negative and cognitive symptoms are extremely challenging for clinicians who are treating patients with schizophrenia, and these clinical phenomena are important to approach because they are related to functional prognosis, real-world performance and quality of life. If currently marketed
antipsychotics can control positive, behavioral and sometimes affective symptoms of schizophrenia, when negative and cognitive symptoms are analysed
1 Department of Psychiatry, „Dr. Carol Davila” Central Military Emergency University Hospital, Bucharest, Romania 2 Department of Pharmacology, Toxicology and Clinical Psychopharmacology, „Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 3 Medical Sciences, Romanian Academy, Romania
Corresponding author Octavian Vasiliu MD [email protected]

4
longitudinally, the results are still disappointing [1]. The prevalence of treatment-resistant schizophrenia is estimated to be approximately 30% (range 10-45%) [2] and an important number of patients have „ultra-resistant” schizophrenia, defined as resistance to clozapine [3]. In all these cases, a significant number of psychotic symptoms persist, although several trials of antipsychotics have been conducted for enough time in adequate doses [3]. Treatment-resistant cases require additional therapeutic agents, and a large number of solutions have been formulated without reaching a consensus (except for clozapine, but as previously mentioned, there are cases resistant even to this second-line atypical antipsychotic).
A significant number of symptoms detected in treatment-resistant patients are based on cognitive deficits [4], and the N-methyl-D-aspartate (NMDA) receptor hypofunction hypothesis attempts explaining why antipsychotic treatment may attenuate the striatal dopaminergic dysfunction without having an influence over the prefrontal cortex in treatment-resistant cases [5]. Negative symptoms have been demonstrated to explain the highest part of variation in disease severity in treatment-resistant schizophrenia, and these symptoms mediated the effects of verbal fluency dysfunctions and high-level neurological soft signs on disease’s severity [6].
Many treatments from a large area of pharmacological, psychotherapeutical and other somatic approaches (e.g., deep brain stimulation) have been investigated for the management of negative and cognitive symptoms of schizophrenia, but there is no first-line therapy yet established for these cases. Atypical antipsychotics used at the lowest dose necessary to control positive symptoms, antidepressants as add-on agents, and cognitive-behavioral therapy have been suggested with limited efficacy in schizophrenia with prominent negative symptoms [7]. Many different pharmacological targets have been suggested for addressing cognitive symptoms in schizophrenia, from D1-agonists to glycine site agonists, and from type A gamma-amynobutyric acid (GABA-A) receptors agonists to alpha7-nicotinic receptors partial agonists, but without significant effects [8-10].
Antibiotics have been explored in clinical practice not only for their anti-microbial properties, but also for their neuroprotective and antiinflammatory effects. As schizophrenia has been associated with increased levels of circulating pro-inflammatory markers and microglial activation in both animal and human studies, researchers have become increasingly interested in the therapeutic potential of antibiotics [11]. Many β-lactams antibiotics have been associated with increased glutamate type 1 transporter
(GLT1) expression in animal models, which can lead to a prevention of toxic neuroexcitation by excessive glutamate transmission [12]. Macrolides may confer neuroprotection against ischemic damage following cerebral ischemia without cerebral blood flow impairments [13]. Doxycycline was proven to prevent amyloid-β toxicity both in vivo and in vitro in a Drosophila melanogaster model of Alzheimer disease [14]. Minocycline is a second generation, semi-synthetic tetracycline that has been associated with neuroprotective, anti-inflammatory and anti-apoptotic properties, which also can inhibit proteolysis, angiogenesis and tumour metastatis [15-17]. D-cycloserine is not only an antituberculosis agent, but also a glycine site partial agonist studied for its properties to enhance neuroplasticity in schizophrenia [18].
While many data on the effects of antibiotics over neuroplasticity are derived from animal models, information on the clinical impact of these pharmacological agents in patients diagnosed with schizophrenia spectrum disoders are contradictory [18-22].
The objectives of this systematic literature review are (1) the evaluation of antibiotics efficacy as add-ons in the management of the core symptoms of schizophrenia spectrum disorders, global clinical status, overall functionality, and (2) to verify if this augmentation strategy is well tolerated. These objectives are considered of clinical interest for psychiatrists, but they also may be useful for researchers oriented on finding new, non-dopaminergic-based treatments for psychotic disorders.
METHODS
This systematic review is based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Table 1) [23]. The protocol of this review was registered in the PROSPERO with the protocol number CRD42019119152 [24].
2.1. Outcomes
The primary outcome for this review was the efficacy of any antibiotic in decreasing symptoms severity in schizophrenia spectrum disorders. We considered the impact of these agents over positive, negative, cognitive, behavioral, and/or affective dimensions of psychosis, as determined by validated psychometric scales for this specific pathology.
The secondary outcomes were (a) tolerability of antibiotics, assessed by either subjective reports or validated instruments, (b) general functionality of patients, and (c) global clinical status, assessed by structured instruments.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
5
2.2. Search strategy
A keyword search strategy was formulated using the following paradigm: „schizophrenia spectrum disorders”/ „schizophrenia”/„schizo-affective disorder”/„schizophreni-form disorder”, AND „antibiotics”/all the names of currently marketed antibiotics classes. Electronic databases searched were Medline (PubMed), Embase, Cumulative Index to
Nursing and Allied Health Literature (CINAHL), National Center for Biotechnology Information (NCBI), and Thomson Reuters/Web of Science. Papers included in the references of the analyzed articles were also reviewed, and their results were included if the quality of research corresponded to the pre-defined inclusion and exclusion criteria. We selected clinical trials that were published in any language, between January 1980 and January 2019.
Table 1: PRISMA-P 2015 Checklist [25]
Section/topic # Checklist item Information reported
Line number(s) Yes No
ADMINISTRATIVE INFORMATION
Title
Identification 1a Identify the report as a protocol of a systematic review 92-94
Update 1b If the protocol is for an update of a previous systematic review, identify as such
Not applicable
Registration 2 If registered, provide the name of the registry (e.g., PROSPERO) and registration number in the Abstract
94
Authors
Contact 3a Provide name, institutional affiliation, and e-mail address of all protocol authors; provide physical mailing address of corresponding author
Title page
Contributions 3b Describe contributions of protocol authors and identify the guarantor of the review
138-150
Amendments 4 If the protocol represents an amendment of a previously completed or published protocol, identify as such and list changes; otherwise, state plan for documenting important protocol amendments
Not applicable
Support
Sources 5a Indicate sources of financial or other support for the review 146-148
Sponsor 5b Provide name for the review funder and/or sponsor Not applicable
Role of sponsor/funder 5c Describe roles of funder(s), sponsor(s), and/or institution(s), if any, in developing the protocol
Not applicable
INTRODUCTION
Rationale 6 Describe the rationale for the review in the context of what is already known
45-89
Objectives 7 Provide an explicit statement of the question(s) the review will address with reference to participants, interventions, comparators, and outcomes (PICO)
135-136, Table 1
METHODS
Eligibility criteria 8 Specify the study characteristics (e.g., PICO, study design, setting, time frame) and report characteristics (e.g., years considered, language, publication status) to be used as criteria for eligibility for the review
124-133, Table 1
Information sources 9 Describe all intended information sources (e.g., electronic databases, contact with study authors, trial registers, or other grey literature sources) with planned dates of coverage
124-133
Search strategy 10 Present draft of search strategy to be used for at least one electronic database, including planned limits, such that it could be repeated
104-111
STUDY RECORDS
Data management 11a Describe the mechanism(s) that will be used to manage records and data throughout the review
138-150

6
Selection process 11b State the process that will be used for selecting studies (e.g., two independent reviewers) through each phase of the review (i.e., screening, eligibility, and inclusion in meta-analysis)
138-150
Data collection process 11c Describe planned method of extracting data from reports (e.g., piloting forms, done independently, in duplicate), any processes for obtaining and confirming data from investigators
138-150
Data items 12 List and define all variables for which data will be sought (e.g., PICO items, funding sources), any pre-planned data assumptions and simplifications
138-150, Table 1
Outcomes and prioritization
13 List and define all outcomes for which data will be sought, including prioritization of main and additional outcomes, with rationale
96-102
Risk of bias in individual studies
14 Describe anticipated methods for assessing risk of bias of individual studies, including whether this will be done at the outcome or study level, or both; state how this information will be used in data synthesis
143-147
DATA
Synthesis 15a Describe criteria under which study data will be quantitatively synthesized
15b If data are appropriate for quantitative synthesis, describe planned summary measures, methods of handling data, and methods of combining data from studies, including any planned exploration of consistency (e.g., I 2, Kendall’s tau)
15c Describe any proposed additional analyses (e.g., sensitivity or subgroup analyses, meta-regression)
15d If quantitative synthesis is not appropriate, describe the type of summary planned
156-164
Meta-bias(es) 16 Specify any planned assessment of meta-bias(es) (e.g., publication bias across studies, selective reporting within studies)
Confidence in cumulative evidence
17 Describe how the strength of the body of evidence will be assessed (e.g., GRADE)
52-57
This checklist has been adapted for use with protocol submissions to Systematic Reviews from Table 3 in Moher D et al: Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews 2015 4:1
Figure 1: Results of the PRISMA-based search paradigm
2.3. Inclusion and exclusion criteria
Studies were eligible for inclusion if they were randomized/non-randomized, open label, single blind or double blind, with or without active comparator,
prospective/retrospective trials. These studies could be controlled with placebo, any other active drug, or usual care, and they must have specified diagnosis criteria for the explored clinical entity/entities. All patients included in these trials were over 18 years old at the initial visit, and no
30 studies included in qualitative synthesis
76 were excluded: - Different study design (n=54)
- Different outcomes (n=6) - Different primary diagnosis (n=3)
- Different intervention (n=13)
1,740 citations identified during the primary search, and 13 citations identified by other sources
1,102 were excluded 1,208 remained after de-duplication and were screened by
two reviewers
106 full-text articles remained and were assessed by eligibility by two reviewers

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
7
superior limit of age was established. Validated instruments for evaluation of the efficacy of the investigational product should be used at baseline and at least at end-point, e.g. Positive and Negative Syndrome Scale or Brief Psychiatric Rating Scale.
Only full-text articles were eligible for analysis, but if
abstracts with outcomes corresponding to those defined by us were found, authors of the respective works were contacted to provide full-text of their papers. No limitation about the duration of the follow-up was included as a criterion of trials selection. A more detailed presentation of the inclusion and exclusion criteria is emphasized in Table 2.
Table 2: Inclusion and exclusion criteria
Operational criteria Inclusion criteria Exclusion criteria
Population Minimum age of inclusion in the selected trial was specified as being 18, according to the study protocol. No superior age limit was specified. The main diagnosis was schizophrenia, schizo-affective disorder, schizophreniform disorder, or any combination of these entities. Diagnosis based on standardized criteria (DSM, ICD, or other compatible psychiatric classifications). Patients with resistant forms of schizophrenia were included (defined by resistance to at least 2 antipsychotic agents, each administered for a minimum duration and dosage, currently presenting symptoms of a minimum duration and severity determined by a standardized rating scale, and moderate or worse functional impairment) [15].
Patients with age under 18, except for cases where statistical procedures allowed for a separate evaluation of the adult vs. child population. The presence of severe somatic or psychiatric co-morbidities with significant impact over cognition, disposition, behavior, and overall functionality. The presence of infectious diseases, which require antibiotic therapy, as co-morbid or main diagnoses. Any co-morbidities which can create confusions in the domain of antibiotics efficacy over psychotic symptoms, either organic diseases (e.g., infections), or psychiatric (e.g., disorders induced or related to drugs or general medical conditions). Neurocognitive co-morbities were not allowed.
Intervention Antibiotics used as add-on to any antipsychotic agent, either typical or atypical. Antibiotics from any class that is currently marketed, with no limitations related to the dosing regimen, adverse events profile, or any pharmacokinetic/pharmacodynamic property. The effects of the intervention over targeted symptoms of schizophrenia spectrum disorders were quantified using at least one validated instrument.
Trials controlled by psychotherapy only. Studies controlled by non-pharmacologic and non-psychotherapy interventions, e.g., deep brain stimulation, electroconvulsive therapy, transcranian magnetic stimulation. Over-the-counter products or dietary supplements as add-on or active comparators. Investigational pharmacologic agents used in phase II or III clinical trials. Administration of more than one antibiotic at a time.
Environment Hospitals, day care, special care, permanent care, or intermediate care units. Both in-patient and out-patient regimen. A caregiver who is able to report on the patient’s evolution under treatment and therapeutic adherence was considered optional.
Correctional environments. Unspecified environment.
Primary and
secondary variables
Changes in psychotic symptoms (positive, negative, cognitive, behavioral, and/or dispositional) were evaluated by trained clinicians. Evaluation of the drugs tolerability, and patients overall functionality and global clinical status was also monitored. Studies were allowed to entered the analysis if they were focused on efficacy, tolerability, or both of these outcomes.
All trials using unspecified psychometric instruments, or only clinical observation were excluded.
Study design Intervention was studied in randomized/non-randomized, open label, single blind, or double blind, with or without active comparator/placebo, prospective/retrospective trials. No limitation about the duration of the treatment was established. Only peer-reviewed studies were included.
Studies with unspecified or insufficiently specified design. Lack of methodologic specifications regarding statistic processing of the primary/secondary variables related to the efficacy. Case reports, case series. Animal model studies. Systematic literature reviews, meta-analyses.
Language English, French, Spanish, Russian Any other language, except for those mentioned in the „inclusion criteria”

8
2.4. Data extraction and analysis
Screening was performed by two independent reviewers, and the resulted material was filtered using inclusion and exclusion criteria mentioned above. Data regarding the main outcomes, the secondary outcomes, and other relevant information about the studies were extracted into the table 3. Data extraction and quality assessment of the studies were done independently by two reviewers (OV and either VAV or DV), and if any disagreement between the two appeared and could not be resolved by consensus, the third reviewer has been consulted.
Consensus was obtained regarding the methodological quality for the included studies after each study was independently rated using the Cochrane Handbook for Systematic Reviews of Interventions - Assessing risk of bias in included studies [26]. Each study was rated as having low, moderate or high risk of bias, based on the (1) randomization procedure, (2) blinding and treatment allocation, (3) use of placebo or an active comparator, (4) methods used for evaluation of outcomes, and (5) dimension of the study group.
All included trials were reviewed critically by authors of the current article, with consideration to the bias risk. A meta-analysis could not be performed because of the heterogeneity of the methods used within the selected trials.
RESULTS
A number of 1753 citations returned after the primary search, and only 1208 remained after de-duplication. After filtering-out articles non-compatible with our predefined inclusion/exclusion criteria, and safter excluding papers for which full text could not be found or provided by authors, a number of 30 trials resulted (Figure1).
3.1. Methodological quality assessment
Among the 30 articles included in this review, a majority were of moderate quality (n=15), while the high and low quality were almost equally represented (7 and 8, respectively). Most of these trials were randomized, placebo-controlled (n=28), one open-label, and one trial had a bi-phasic design, with a single-blind, followed by a double-blind period of treatment. Only 4 trials had a sample size over 100, while 19 trials included below 50 subjects, which reduced the power of the analysis for the poor-populated trials.
Frequently encountered problems were lack of information about concealment of the randomization, and about the intent-to-treat (ITT) vs. per protocol analysis. The mean
percentage of agreement between the two reviewers for each trial was 90.7% (p<0.0001) for the validity criteria.
3.2. Evaluation of primary outcome: the efficacy of antibiotics in schizophrenia spectrum disorders
The only active interventions detected by our search were D-cycloserine (n=18 trials, most of them of moderate quality) and minocycline (n=10 trials, most of them of moderate and low quality).
The efficacy of minocycline as add-on to antipsychotic treatment was investigated in two large double-blind, placebo-controlled trials (n=200 and 207, respectively) and the results were negative [27, 28]. No improvement of negative (on medium and long term), cognitive and overall psychotic symptoms (on medium term) was detected by these two studies. A small trial (n=73 subjects) evaluated the impact of minocycline as add-on to clozapine over avolition and concluded that although higher plasma levels of clozapine were detected after minocycline initiation, there was no evidence that improvement in negative symptoms can be correlated with higher level of plasma antipsychotic [29].
Another small trial (n=52) concluded that minocycline did not improve significantly psychosis factor and overall BPRS (Brief Psychiatric Rating Scale) score, neither had it a significant impact over cognitive function, except for working memory [31]. The same trial reported a significant improvement in the BPRS anxiety/depression factor in the minocycline-treated patients [31].
Regarding the positive effects of minocycline, a small trial (n=24) detected significant improvements in patients treated with this drug over the positive and negative symptoms, compared to placebo, and a protective effect of this antibiotic over the gray matter loss in fronto-temporal areas involved in the pathophysiology of schizophrenia during 12-month of active treatment [32].
Another short-term trial (8 weeks, n=43 subjects) found that SANS (Scale for the Assessment of Negative Symptoms) total score decreased significantly compared to placebo, and the negative sub-scale of PANSS (Positive and Negative Syndrome Scale) also decreased, but not significantly compared to placebo [33].
A study that evaluated 92 patients with schizophrenia treated with risperidone who received minocycline as add-on for 16 weeks reported greater improvements on SANS total scores and PANSS negative subscale versus placebo [34]. This study observed no difference between groups in cognitive performances, except for the attentional domain [34].

Table 3: Qualitative analysis of the trials selected
Intervention Authors Objectives Design Population Outcomes Results Quality score
Minocycline Weiser M, Levi L, Burshtein S, et al. [27]
Efficacy of minocycline over positive, negative and cognitive symptoms of schizophrenia
16-week double-blind, placebo-controlled RCT; minocycline (200 mg/ day) /pramipexole /acetyl- salicilic acid/ placebo as add-on to antipsychotic treatment
N=200 patients with schizophrenia or schizo-affective disorder
Primary outcome measurements - PANSS total score at the end of the trial. Secondary outcomes- positive, negative and general psychopathology scored by PANSS; CGI-S, CGI-I; BACS; rates of drop-outs
No significant differences between minocycline and placebo for PANSS total score, PANSS subscales, CGI, and BACS were detected. No significant difference between groups in the frequency of adverse events.
High
Minocycline Deakin B, Suckling J, Barnes TRE, et al. [28]
Efficacy of minocycline over negative symptoms in schizophrenia with recent onset
12-month double-blind, placebo-controlled RCT; minocycline (200 mg/ day for 2 weeks, then 300 mg/day for the remainder of 12 months) vs. placebo plus continuing treatment
N=207 patients with schizophrenia spectrum disorders that begun in the last 5 years
Negative symptom subscale score of the PANSS; prefrontal grey matter volume, dorsolateral prefrontal cortex activation during working memory task, and plasma concentration of IL6
No effect of minocycline was observed over ratings of negative symptoms. Biomarker outcomes did not change over time, and were not affected by minocycline. No difference in the appearence of serious adverse events was detected between groups.
High
Minocycline Liu F, Xie L, Zhang B, et al. [30]
Effects of adjunctive minocycline over body metabolism in risperidone- treated patients with schizophrenia
16-week placebo-controlled, double-blind crossover RCT
N=63 patients diagnosed with schizophrenia,treated with stable dose of risperidone for ≥4 weeks
Body weight, BMI, waist circumference, fasting insulin, glucose and lipids serum levels
No difference between groups was detected (P’s>0.3)
Moderate
Minocycline Wehring HJ, Elsobky T, McEvoy JP, et al. [29]
Pharmacokinetic impact of minocycline over clozapine and correlation between modified levels of clozapine /norclozapine over negative symptoms in schizophrenia
10-week placebo-controlled RCT, minocycline vs. placebo as add-on to clozapine
N=73, DSM IV-TR- based diagnoses of schizophenia or schizo-affective disorder, currently treated with clozapine ≥200 mg/day and blood level of clozapine ≥350 ng/ml.
Serial plasma clozapine, norclozapine and total clozapine levels, SANS
Clozapine plasma levels are increased after the initiation of minocycline (21% increment to baseline) compared to placebo. However, smoking patterns were not analysed in relation to this plasmatic difference in concentration. Avolition improvement on SANS was not explained by changes in clozapine blood levels. There is no evidence that improvement in any symptom domain is due to higher clozapine levels.
Moderate
Minocycline Kelly DL, Sullivan KM, McEvoy JP, et al. [31]
Efficacy of minocycline as adjunctive treatment to clozapine in chronic psychoses
10-week double-blind, placebo-controlled RCT; 100 mg p.o BID minocycline vs. placebo.
N=52 patients with schizophrenia and schizo-affective disorder with persistent positive symptoms
Positive and cognitive symptoms were primary outcomes. Avolition, anxiety/depression, and negative symptoms were secondary outcomes.
BPRS- psychosis factor and BPRS- total score were not changed significantly during treatment. Still, a change in total BPRS score of more than or equal to 30% was observed more frequently in minocycline treated patients (p=0.044). Global cognitive function (MATRICS) did not differ between groups, but significant
Moderate

Intervention Authors Objectives Design Population Outcomes Results Quality score
improvement in working memory favored minocycline. SANS total score did not differ, but minocycline improved significantly working memory (p=0.023). Significant improvement in the BPRS anxiety/depression factor was observed with minocycline (p=0.028). The overall tolerability of minocycline was good.
Minocycline Chaves C, Marque CR, Maia-de- Oliveira JP, et al. [32]
Effects of minocycline on brain morphology and cerebral perfusion in patients with recent-onset schizophrenia
12-month double-blind, placebo-controlled RCT of minocycline as add-on treatment (200 mg/day minocycline vs. placebo)
N=24 outpatients with recent-onset schizophrenia
SPECT and MRI were performed after 12 months of treatment for detection of morphologic changes.
Minocycline may have protective effect against gray matter loss and modulate fronto-temporal areas involved in the pathophysiology of schizophrenia. Significant lower gray matter volumes were observed in the midposterior cingulate cortex and in the precentral gyrus in placebo group, in comparison with minocycline group. Positive and negative symptoms were significantly decreased versus placebo.
Moderate
Minocycline Ghanizadeh A, Dehbozorgi S, Omrani Sigaroodi M, Rezaei Z [33]
Effectiveness of add-on minocycline in schizophrenia
8-week placebo-controlled RCT; minocycline 200 mg/day + risperidone vs. placebo + risperidone.
N=43 patients diagnosed with DSM IV schizophrenia
Schizophrenia negative symptoms severity as primary outcome
SANS total score decreased significantly in the minocycline group at week 8, compared with placebo group. The decline of PANSS Negative score was more in the active treatment group than in the placebo group (not statistically signifi-cant). Tolerability of minocycline was good.
Moderate
Minocycline Liu F, Guo X, Wu R, et al. [34]
Efficacy and safety of minocycline for the treatment of negative symptoms and cognitive impairments in patients with schizophrenia
16-week double blind, placebo-controlled RCT; minocycline 200 mg/day vs. placebo.
N=92 with early stage schizophrenia treated with risperidone
The primary outcome was represented by negative symptoms of schizophrenia, evaluated by SANS scores. Secondary outcomes were scores of response rate on SANS, PANSS, CGI, cognitive tests
Patients receiving minocycline had greater improvements on SANS total scores and PANSS negative subscale scores vs. placebo. Rates of treatment response in the minocycline group were significantly higher than those in the placebo group after 16 weeks of treatment. Cognitive performances were not improved significantly by minocycline, except for the attentional domain.
High
Minocycline Khodaie- Ardakani MR, Mirshafiee O, Farokhnia M, et al. [35]
Efficacy and tolerability of minocycline add-on to risperidone in treatment of negative
8-week double-blind, placebo-controlled RCT; minocycline (titrated up to 200 mg/day) vs. placebo as add-on to
N=40 outpatients with chronic schizophrenia stabilized on risperidone for at least 8 weeks prior to baseline
Primary outcomes- negative symptoms evaluated by PANSS
Significant difference between groups on negative scale of PANSS favoured minocycline at the end of the trial (p<0.001). PANSS total score, positive score and general psychopathology score were also improved by minocycline compared to placebo.
Moderate

Intervention Authors Objectives Design Population Outcomes Results Quality score
symptoms in chronic schizophrenia
risperidone (maximum 6 mg/day)
No difference between groups regarding the severity of adverse effects was observed.
Minocycline Chaundhry IB, Hallak J, Husain N, et al. [36]
Efficacy of minocycline as add-on to treatment as usual over negative symptoms in early psychosis.
Placebo-controlled RCT, one year duration, minocycline (titrated up to 200 mg/day) vs. placebo.
N=144 patients with early psychosis
Primary outcomes- negative and positive symptoms evaluated by PANSS. Secondary outcomes- GAF, CGI, AIMS, neuropsychological outcome measures.
Minocycline improved negative symptoms (p<0.001) in the ITT population. No other outcomes were influenced significantly by minocycline. AIMS scores tend to improve more in the placebo group.
High
Minocycline Levkovitz Y, Mendlovich S, Riwkes S, et al. [37]
Efficacy of minocycline as add-on treatment for alleviating negative and cognitive symptoms in early-phase schizophrenia
Double-blind, placebo-controlled RCT, 6 months duration, minocycline 200 mg/day vs. placebo + atypical antipsychotic (200-600 mg/day chlorpromazine- equivalent doses).
N=54 early-phase schizophrenia patients (DSM IV) - age 18-35 years
Primary outcome- negative symptoms severity evaluated by SANS. Cognitive measures evaluated by CANTAB. Functional measures and clinical evaluations by GAF, SOFAS, MCAS, CGI.
A significant time effect for SANS total scores was detected in the minocycline group, negative symptoms improved since week 14. CGI improved better with minocycline, as did cognitive functioning, mainly executive functions (working memory, cognitive shifting, and cognitive planning). GAF and SOFAS showed a better improvement with minocycline. Also, minocycline had a favourable effect in preventing weight gain during treatment.
Moderate
Minocycline Miyaoka T, Yasukawa R, Yasuda H, et al. [38]
Efficacy and tolerability of minocycline as adjunct to antipsychotic medication in schizophrenia
Open-label, pilot study, minocycline 150 mg/day 4 weeks as adjunct to current antipsychotic medication
N=22 patients with schizophrenia
Psychotic symptoms severity determined by PANSS
All scales of PANSS improved during minocycline treatment. All patients tolerated the full dose during the study.
Low
D-cycloserine Takiguchi K, Uezato A, Itasaka M, et al. [39]
Effects of d-cycloserine over positive, negative and cognitive symptoms of schizophrenia. To investigate if white matter integrity influences response to d-cycloserine.
6-week placebo-controlled, double-blind, cross-over design RCT; d-cycloserine (50 mg) vs. placebo as add-on to their current antipsychotic treatment
N=41 patients, in- and out- patients with DSM IV diagnostic criteria for schizophrenia
PANSS and SANS scores, BACS, EQS- interpersonal, intrapersonal and situational domains; correlations between d-cycloserine treatment and MR-DTI white matter integrity.
No improvement of positive, negative, or cognitive symptoms of schizophrenia. The better treatment effect of d-cycloserine on BACS was observed when fractional anisotropy was higher in sagittal striatum, cingulum, fornix stria terminalis, genu of corpus callosum, and external capsule, and the better treatment effect on PANSS- general psychopathology score was observed when fractional anisotropy of the splenium of corpus callosum was higher. The better treatment effect on PANSS- general psychopathology score and SANS-IV was observed when fractional anisotropy was lower in the posterior thalamic radiation.
Moderate

Intervention Authors Objectives Design Population Outcomes Results Quality score
D-cycloserine Forsyth JK, Bachman P, Mathalon DH, et al. [40]
Exploration of NMDA-receptor signaling on working memory and experience- dependent plasticity
Double-blind, placebo-controlled, between-group design RCT, 100 mg d-cycloserine vs. placebo; subjects were tested at one day after d-cycloserine or placebo administration
N=45 patients diagnosed with schizophrenia
Neuroplasticity changes evaluated by cognitive tests and EEG with high-frequency visual stimulation
D-cycloserine did not affect plasticity (similar neural potentiation in both active and placebo group), similar information integration and weather prediction tasks performances. Still, patients who received active drug and who were actively involved in memory task had superior 2-back performace compared to placebo-receiving patients. NMDA-receptor-signaling was not translated into synaptic plasticity change in schizophrenia.
Moderate
D-cycloserine Cain CK, McCue M, Bello I, et al. [41]
Efficacy of d-cycloserine + cognitive remediation (CR) program in improving memory of patients with schizophrenia
8-week placebo-controlled RCT; 3-5 times per week CR program + once-weekly adjunctive treatment with 50 mg d-cycloserine or placebo administered before the first session within each week.
N=36 outpatients, stable medicated adults
Primary outcomes were performances on an auditory discrimination task, MATRICS battery composite scores, SANS total scores
Performance on the practiced auditory discrimination task significantly improved in the d-cycloserine group compared to placebo. Active treatment was associated with significantly greater negative symptom improvement for subjects symptomatic at baseline. Improvement on MATRICS was observed only in the placebo group.
Moderate
D-cycloserine Gottlieb JD, Cather C, Shanahan M, et al. [42]
Efficacy of d-cycloserine as add-on to CBT for the management of delusions in schizophrenia
Double-blind, cross-over, placebo controlled RCT, single oral dose of d-cycloserine 50 mg vs. placebo, one hour post-drug administration patients received 2 CBT sessions focused on challenging patients’ paranoid appraisals, with 7-day and 14-day re-evaluations
N=21 outpatients diagnosed with schizophrenia or schizo- affective disorder and moderately severe delusions
Delusional severity was assessed using SAPS; alternative explanations generated on the ABA; PSYRATS score
No significant effect of d-cycloserine on delusional distress or severity has been reported.
Moderate
D-cycloserine Goff DC, Cather C, Gottlieb JD, et al. [43]
Investigation of d-cycloserine over negative symptoms and cognition in schizophrenia
8-week double-blind, parallel-group RCT; add-on of d-cycloserine 50 mg or placebo administered once-weekly.
N=50 adult outpatients treated with any antipsychotic except clozapine
Primary outcomes were change from baseline to week 8 on SANS total score and on a composite cognitive score.
D-cycloserine significantly improved SANS total scores compared to placebo at week 8. Cognitive performance did not improve with d-cycloserine at week 8. Delayed thematic recall was significantly improved with the first dose of d-cycloserine vs. placebo, but not immediate thematic recall and item recall.
High

Intervention Authors Objectives Design Population Outcomes Results Quality score
D-cycloserine Buchanan RW, Javitt DC, Marder SR, et al. [44]
Efficacy of glycine or d-cycloserine in patients with schizophrenia with moderate to severe negative symptoms and cognitive impairments.
16-week double-blind, double-dummy, parallel-group RCT of adjunctive glycine, D-cycloserine, or placebo
N=157 inpatients and outpatients diagnosed with DSM-IV schizophrenia or schizo-affective disorder and retrospective and prospective criteria for moderate to severe negative symptoms without marked positive, depressive, or extra- pyramidal symptoms
The primary outcome- average rate of change of SANS total scores and change in the average cognitive domain z scores
No significant differences in change of the SANS total score between glycine and placebo, or d-cycloserine and placebo. No significant differences between glycine and placebo or d-cycloserine and placebo were recorded on the average cognition z score.
High
D-cycloserine Yurgelun- Todd DA, Coyle JT, Gruber SA, et al. [45]
Examination of patterns of cortical activation underlying d-cycloserine’s therapeutic efficacy in patients with schizophrenia
2-week single-blinded, placebo lead-in phase RCT; after placebo phase, patients received 50 mg/day d-cycloserine or placebo in a double-blind manner for 8 weeks.
N=12 out- and in-patients with DSM-IV criteria for schizophrenia on stable dose of antipsychotic for at least 4 months and presenting prominent negative symptoms
fMRI patterns of cortical activation; SANS for severity of negative symptoms
Patients receiving d-cycloserine had a significant increase in temporal lobe activation, associated with reduction in negative symptoms.
Low
D-cycloserine Goff DC, Herz L, Posever T, et al. [46]
Efficacy of d-cycloserine as augmenting agent for conventional antipsychotics in decreasing negative and cognitive symptoms of schizophrenia
Double-blind, parallel-blind RCT, 50 mg/day d-cycloserine or placebo for 6 months
N=55 patients with schizophrenia with prominent negative symptoms
Primary outcomes- negative symptoms and cognitive impairments evaluated by PANSS, SANS, cognitive battery
No difference between groups was detected on any primary outcome at 8 or 24 weeks (PANSS, SANS, cognitive tests).
High
D-cycloserine Duncan EJ, Szilagyi S, Schwartz MP, et al. [47]
Efficacy of d-cycloserine over negative and cognitive symptoms of schizophrenia
Double-blind, parallel-group RCT, 50 mg QD d-cycloserine or placebo for 4 weeks
N=22 male patients with schizophrenia displaying prominent negative symptoms stabilized on typical neuroleptics
Symptoms severity (SANS, BPRS, Abrams and Taylor rating scale). Cognition was assessed by the Sternberg Memory Test and the Continuous Performance Test.
No significant differences between the d-cycloserine and placebo group on any symptom rating
Low
D-cycloserine Evins AE, Amico E, Posever TA, et al. [48]
Effects of d-cycloserine when added to risperidone
Placebo-controlled RCT, 2 weeks of placebo and 4 doses of d-cycloserine
N=10 patients with schizophrenia treated with risperidone
Negative symptoms severity D-cycloserine (50 mg/day) significantly reduced negative symptoms.
Low

Intervention Authors Objectives Design Population Outcomes Results Quality score
on negative symptoms of schizophrenia
Ratings of depression, extrapyramidal side effects, and cognitive function were unchanged.
D-cycloserine Heresco- Levy U, Ermilov M, Shimoni J, et al. [49]
To investigate the clinical effects of d-cycloserine when added to conventional antipsychotics, olanzapine, or risperidone for treatment-resistant schizophrenia
Double-blind, placebo-controlled, crossover study, 2 random-order 6-week treatment arms (d-cycloserine, 50 mg/day vs. placebo), separated by 2-week adjuvant treatment washout.
N=24 patients diagnosed with treatment-resistant schizophrenia, and they were on stable doses of medication for at least 3 months before study entry
Psychotic symptoms evaluated by PANSS, depression severity evaluated by HAMD, and adverse events quantified by SAS and AIMS
Significant reduction in negative symptoms in patients treated with d-cycloserine. No difference between patients treated with conventional neuroleptics or atypical antipsychotics was observed.
Moderate
D-cycloserine Heresco- Levy U, Javitt DC, Ermilov M, et al. [50]
Efficacy of d-cycloserine over negative symptoms in schizophrenia
16-week, double-blind, placebo-controlled, adjuvant treatment RCT with 50 mg/day d-cycloserine
N=9 treatment- resistant chronic schizophrenia-diagnosed patients
Psychotic symptoms evaluated by PANSS, depression severity evaluated by HAMD, and adverse events quantified by SAS and SAS and AIMS
Symptoms changes between groups were not significant, except for a significant reduction in negative symptoms which was registered during treatment with d-cycloserine but not placebo. Greater reductions were registered in patients with lower baseline serum glycine levels. No side effects were registered.
Low
D-cycloserine van Berckel BN, Evenblij CN, van Loon BJ, et al. [51]
Effects of d-cycloserine as add-on to typical antipsychotics in reducing negative symptoms in schizophrenia
Double-blind, parallel group, placebo-controlled RCT; 50 mg d-cycloserine BID or placebo for 8 weeks.
N=26 patients with DSM-IV schizophrenia
PANSS, CGI, ESRS
D-cycloserine slightly worsened positive symptoms and general psychopathology compared to placebo. No significant change in negative symptoms was detected or extrapyramidal symptoms. Tolerability of d-cycloserine was good.
Moderate
D-cycloserine Goff DC, Henderson DC, Evins AE, Amico E [52]
Effects of d-cycloserine over negative symptoms in schizophrenia
6-week RCT, d-cycloserine 50 mg/day or placebo, crossover design separated by 1 week placebo washout for a total of 13 weeks
N=17 outpatients diagnosed with schizophenia (DSM-IV criteria) treated with clozapine
PANSS, SANS, GAF, HAMD, AIMS, SAS, BAS
D-cycloserine significantly worsened negative symptoms compared to placebo (increased SANS scores and negative subscale of PANSS)
Moderate
D-cycloserine Goff DC, Tsai G, Levitt J, et al. [53]
Efficacy of d-cycloserine over negative symptoms and cognitive function when added to conventional neuroleptics
8-week double-blind RCT, d-cycloserine 50 mg/day vs. placebo, added to their conventional neuroleptic
N=47 patients with schizophrenia meeting criteria for deficit syndrome
SANS total score The mean reduction in negative symptoms with d-cycloserine was significantly greater than with placebo (SANS scores). No differences were found in performance on any cognitive test between groups or in changes in any other clinical measure.
Moderate

Intervention Authors Objectives Design Population Outcomes Results Quality score
D-cycloserine Goff DC, Tsai G, Manoach DS, et al. [54]
Efficacy of d-cycloserine as add-on over negative symptoms in patients treated with clozapine
2-week placebo-controlled RCT; 5, 15, 20, 50 and 250 mg/day d-cycloserine
N=10 outpatients with schizophrenia receiving clozapine who presented criteria for primary deficit syndrome
SANS Significant dose effect of d-cycloserine on SANS scores, 50 mg/day produced a mean increase of 21% in SANS score. No improvement was detected on clozapine-treated patients with negative symptoms.
Low
D-cycloserine Rosse RB, Fay-McCarthy M, Kendrick K, et al. [55]
Efficacy of d-cycloserine as add-on to molindone in schizophrenia
4-week placebo-controlled, double-blind, parallel-group RCT, 10 or 30 mg/day d-cycloserine as adjuvant to molindone (150 mg QD)
N=13 patients diagnosed with schizophrenia
BPRS, SANS, CGI Neither dose of d-cycloserine had adjuvant therapeutic efficacy, although the tolerability of the d-cycloserine was good.
Low
D-cycloserine Goff DC, Tsai G, Manoach DS, Coyle JT [56]
Efficacy of d-cycloserine over negative symptoms of schizophrenia
2-week trials of placebo and four doses of d-cycloserine; 5, 15, 50, 250 mg/day d-cycloserine
N=9 outpatients with schizophrenia (DSM III R criteria) treated with stable doses of conventional antipsychotics for at least 4 months prior to inclusion
SANS, Negative symptoms subscale of BPRS, SAS, AIMS, GAF, Sternberg’s Item Recognition Paradigm
D-cycloserine at 50 mg/day produced significant reduction in negative symptoms and significantly improved reaction time (as a measure of executive dysfunction)
Low
RCT = randomized controlled trial; MR-DTI = Magnetic resonance - diffusion tensor imaging; PANSS = Positive and Negative Syndrome Scale; SANS = Scale for the Assessment of Negative Symptoms; EQS = Emotional Intelligence Scale; BMI = Body Mass Index; BPRS = Brief Psychiatric Rating Scale; ITT = Intent to treat analysis; GAF = Global Assessment of Functionality Scale; CBT = Cognitive Behavioral Therapy; SAPS = Scale for the Assessment of Positive Symptoms; ABA = Alternative Beliefs Assessment; PSYRATS = Psychotic Symptom Rating Scale; CANTAB = Cambridge Neuropsychological Test Automated Battery; SOFAS = Social and Occupational Functioning Assessment Scale; MCAS = Multinomah Community Ability Scale; HAMD = Hamilton Depression Rating Scale; SAS = Simpson-Angus Rating Scale; AIMS = Abnormal Involuntary Movement Scale; ESRS = Extrapyramidal Symptoms Rating Scale; BAS = Barnes Akathisia Scale; CGI-S = Clinical Global Impressions- Severity; CGI-I = Clinical Global Impressions- Improvements; BACS = Brief Assessment of Cognition in Schizophrenia

16
Another 8-week trial (n=40) confirmed significant differences between groups in favour of minocycline regarding the negative symptoms evaluated by PANSS, while positive and general psychopathology scores were non-significantly improved [35].
A large, long-term trial (n=144, 12 months) reported that minocycline improved negative symptoms in the ITT population (p<0.001) [36]. The efficacy of minocycline over negative symptoms was supported also by a study (n=54) which included early-phase schizophrenia patients, with difference between groups appearing at week 14 [37]. An open-label study confirmed a positive effect of minocycline over all scales of PANSS after 4 weeks [38].
D-cycloserine was associated with lack of efficacy over positive, negative and cognitive psychotic symptoms, in a small trial (n=41), but some interesting correlations were reported between MR-DTI (Magnetic resonance - diffusion tensor imaging) and score evolution of general and cognitive symptoms, i.e. fractional anisotropy in certain thalamic regions (where assymetric alterations in the white matter integrity were demonstrated) could be improved by this antibiotic and it may be a mediator of the therapeutic response [39].
No significant effects were observed in patients treated with d-cycloserine over neuroplasticity and cognitive performances, evaluated by cognitive tests and EEG with high-frequency visual stimulation, in a small trial (n=45) [40]. In a crossover design study, no significant effect of d-cycloserine on delusional distress or severity has been reported [42].
Data from a large trial (n=157) found no difference between d-cycloserine and placebo over the severity of cognitive and negative symptoms [44]. No significant differences were found between d-cycloserine and placebo in two trials, which included patients with prominent negative symptoms in the domains of negative and cognitive manifestations [46, 47]. D-cycloserine slightly worsened positive symptoms and general psychopathology compared to placebo, and it did not significantly change negative symptoms in an 8-week placebo-controlled trial (n=26) [51]. D-cycloserine significantly worsened negative symptoms compared to placebo in a 13-week trial (n=17) [52]. When added to clozapine, d-cycloserine worsened negative symptoms dose-proportionally in a small study (n=10) [54]. D-cycloserine added to molindone did not resulted in improvements of general psychopathology or negative symptoms (n=13) [55].
Regarding the positive results of d-cycloserine, this drug was significantly superior to placebo on reducing negative
symptoms compared to placebo (n=36, 8-week trial) [41]. D-cycloserine significantly improved SANS total scores after 8 weeks in small trial with outpatients, but no effect was observed over cognitive functions (n=50) [43]. A small trial (n=12) found that d-cycloserine increased significantly temporal lobe activation, a phenomenon correlated with negative symptoms [45].
Table 4: Efficacy of antibiotics over symptom severity in schizophrenia spectrum disorder
Treatment Clinical trials GRADE Recommendations
Minocycline [27-29,31-38] Positive symptoms: ? Negative symptoms: D+ Cognitive symptoms: D+ Behavioral symptoms: ? Affective symptoms: D Overall symptoms: D+
D-cycloserine [39-45,48,50-56] Positive symptoms: ? Negative symptoms: D+ (but not as add-on to clozapine)
Cognitive symptoms: ? Behavioral symptoms: ? Affective symptoms: ?
Overall symptoms:? GRADE recommendations for the level of evidence [57]: A=high quality= future research are very unlikely to change the validity of these recommendations; B= moderate quality= future research is likely to have an important impact on the appreciation of the recommendations; C=low quality= it is very likely that future research will have an important impact over the confidence in the estimate of effect and is likely to change the recommendations; D= very low quality= any estimate of the effect is very uncertain. Intermediate steps (+ or -) represent nuances of the recommedantions based on the quality of trials and tolerability of antidepressant agents, as resulted from these trials.
Another small trial (n=10) signaled reduced negative symptoms with d-cycloserine, but no effect of the same drug over cognitive function [48]. In a trial with treatment-resistant schizophrenia-diagnosed patients, adding d-cycloserine to current antipsychotic agent has lead to significant reduction in negative symptoms, without differences between patients treated with atypical or typical antipsychotics [49].
A small trial (n=9) reported significant improvements in negative symptoms versus placebo, especially in patients with lower baseline serum glycine levels [50]. A significant reduction in negative scores (evaluated by SANS) was observed in an 8-week double blind RCT (n=47), but no effect was detected over cognitive symptoms [53]. When added to conventional antipsychotics, D-cycloserine 50 mg/day produced significant reduction in negative symptoms and improved executive dysfunction in patients with schizophrenia (n=9) [56].

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
17
Table 5: Tolerability of antibiotics in patients diagnosed with schizophrenia spectrum disorders
Treatment Clinical trials GRADE Recommendations
Minocycline [27, 28, 31-38] Overall adverse events: B Extrapyramidal symptoms: B
Body weight, waist circumference, lipid and glucose
metabolism: B-
D-cycloserine [44, 48-52, 55, 56] Overall adverse events: B- Extrapyramidal symptoms: B-
Body weight, waist circumference, lipid and glucose
metabolism: ?
Table 6: Effect of antibiotics over global clinical status in patients
diagnosed with schizophrenia spectrum disorders
Treatment Clinical trials GRADE Recommendations
Minocycline [27, 34, 36, 37] D-
D-cycloserine [51, 52, 55, 56] D-
Table 7: Effect of antibiotics over global functionality in patients diagnosed with schizophrenia spectrum disorders
Treatment Clinical trials GRADE Recommendations
Minocycline [36, 37] D
D-cycloserine [51, 52, 55, 56] D-
3.3. Evaluation of antibiotics tolerability in the studied population
Tolerability of minocycline was evaluated in a number of nine trials of moderate quality, most of them being double blind, placebo-controlled, that included 825 patients, and had variable duration (between 4 weeks and 12 months). Most of these trials included small groups, but there were also 3 large-group (over 140 patients each) studies [27, 28, 36].
No significant differences in the rate of adverse events between minocycline- and placebo-treated patients were reported [27, 28, 31, 32, 35, 36, 38].
No difference between minocycline and placebo was detected in a study focused on tolerability in the domain of body weight, waist circumference, fasting insulin, glucose and lipid serum levels [30]. Minocycline had a favourable effect in preventing weight gain during treatment in a trial with early-phase schizophrenia patients (n=54) [37].
Tolerability of d-cycloserine was evaluated systematically in 6 trials, of low-to-moderate quality, that included 99 patients, with a duration between 2 and 16 weeks [44, 48-51, 55]. All these trials reported a good tolerability of d-
cycloserine, and the main adverse events monitored were extrapyramidal symptoms. However, none of the trials, which included scales for extrapyramidal symptoms, reported any significant changes during d-cycloserine administration [49-52, 56].
3.4. Evaluation of general functionality and global clinical status
Minocycline improved the global clinical impression in only one study (n=54) [37], while in other three studies (with a total of 436 subjects) it did not distinguished itself from placebo [27, 34, 36]. Trials included in this analysis were of high quality.
The global functioning was improved by minocycline more than by placebo in one trial (n=54) [37], but did not differ from placebo in another trial (n=144) [36]. The quality of these trials was high to moderate.
D-cycloserine had no significant impact over global clinical status or overall functionality, but data were derived from only 2 trials for each outcome, and they included low number of participants (39 and 26, respectively) and were of moderate to low quality [51, 52, 55, 56].
CONCLUSIONS
Based on reviewing the selected trials regarding the efficacy of antibiotics as add-on to antipsychotic treatment over core symptoms of schizophrenia, minocycline (n=10 trials, N=950 participants) was associated with mixed results regarding its efficacy, both positive [32-38] and negative [27-29, 31]. The large majority of these studies were of moderate and low quality, which further complicates the evaluation of their conclusions. Most of the data derived from these trials did not support a significant efficacy of minocycline over negative, cognitive, and overall psychotic symptoms, when it was added to various antipsychotic agents, clozapine included [27-29]. Other trials reported isolated efficacy of minocycline superior to placebo over anxiety/depression

18
factor of BPRS, working memory, or significant improvement in negative and/or positive symptoms [31-38]. Non-significant superior efficacy of minocycline over placebo was also reported over positive and general psychopathology [35]. A definite conclusion about the efficacy of minocycline can not be formulated based on these data, and the GRADE recommendation could not be over the D+ level regarding the positive, negative, and overall psychotic symptoms, as well as D level for affective symptoms of schizophrenia (table 4).
D-cycloserine was investigated in moderate quality trials (n=18, N=626 participants) focused on its efficacy over symptoms of schizophrenia, when used as add-on to antipsychotics. No significant difference between d-cycloserine and placebo was observed in trials focused on negative and cognitive symptoms of schizophrenia [39-56]. A trend to the worsening of positive symptoms by d-cycloserine was also reported, as well as a trend to aggravation of negative symptoms, especially when added to clozapine [51, 52, 54]. D-cycloserine was also proven superior to placebo over negative symptoms [41, 43, 45, 48-50, 53, 56] and cognitive function [56], without difference between atypical and typical antipsychotics as main treatment [49]. Based on these contradictory data, d-cycloserine could be rated as D+ recommendation for the treatment of negative symptoms of schizophrenia, when added to typical or atypical antipsychotics, but not to clozapine. Thorough monitorisation of patients undergoing d-cycloserine augmentation should be initiated because there is a risk of worsening positive symptoms or negative symptoms (the last case has been reported in clozapine-treated patients).
After reviewing the trials focused on tolerability of antibiotics in patients diagnosed with schizophrenia as add-on to antipsychotics (n=9, N=825 participants), the data collected was considered as being of moderate quality (table 5). Almost all of them reported no difference in the rate of adverse events between minocycline and placebo-treated patients, and two studies showed a favorable effect of this antibiotic over metabolic status of the patients undergoing antipsychotic treatment [27, 28, 30-32, 35-38]. These data support a level B- for the tolerability of minocycline as add-on to antipsychotic regarding the metabolic profile, body weight and waist circumference, and level B for the overall adverse events (extrapyramidal symptoms included).
Tolerability of d-cycloserine was also evaluated as good in
moderate to low quality trials (n=6 studies, N=99 participants), and the main adverse events were extrapyramidal symptoms [44, 48-51, 55]. These data support a level B- for the tolerability of d-cycloserine as add-on to antipsychotic regarding the overall adverse events (extrapyramidal symptoms included).
Minocycline had an effect over the clinical global impression that was not disguinshible from placebo [27, 34, 36], although there was one exception [37]. Data was derived from high quality studies (n=4, N=490 participants), and the recommendation for improving this outcome with minocycline as add-on is D- (table 6). The impact of minocycline over the global functioning when added to antipsychotic in patients with schizophrenia was mixed, with one positive and one negative trial (n=2, N=198 participants, moderate to high quality designed trials) [36, 37]. Based on these data a D level is formulated in this case.
D-cycloserine had no significant impact over global clinical status (n=2, N=39 participants) or overall functionality (n=2, N=26 participants) [51, 52, 55, 56]. These trials were of moderate to low quality and there was formulated a D- recommendation for each outcome based on the before-mentioned results (Tables 6 and 7).
From all the data reviewed and hierarchized it is evident that larger trials are needed in order to confirm the efficacy of minocycline and d-cycloserine over negative and cognitive symptoms of schizophrenia. The tolerability of these two antibiotics was good in almost all trials that were reviewed, which is encouraging in the perspective of designing new trials with these agents.
Limitations of this review are related to the heterogeneity of design in trials that were analysed, and the impossibility of contructing a meta-analysis. The use of different scales for monitoring the same cluster of symptoms made difficult the comparison of the results. In addition, most of the trials included in the current review were conduceted on small groups, which make the generalizability of data very difficult.
Disclaimer
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. No funding was received for this research.
All authors have contributed equally to the review.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
19
References:
1. Fusar-Poli P, Kempton MJ, Rosenheck RA. Efficacy and safety of second-generation long-acting injections in schizophrenia: a meta-analysis of randomized-controlled trials. Int Clin Psychopharmacol 2013;28(2):57-66.
2. Meltzer HY. Treatment-resistant schizophrenia- the role of clozapine. Curr Med Res Opin 1997;14(1):1-20.
3. Bartoli F, Crocamo C, Di Brita C, et al. Adjunctive second-generation antipsychotics for specific symptom domains of schizophrenia resistant to clozapine: A meta-analysis. Journal of Psychiatric Research 2019;108:24-33.
4. Iasevoli F, Avagliano C, Altavilla B, et al. Disease severity in treatment resistant schizophrenia patients is mainly affected by negative symptoms, which mediate the effects of cognitive dysfunctions and neurological soft signs. Front Psychiatry 2018;9:553.
5. Lowe P, Krivoy A, Porffy L, et al. When the drugs don’t work: treatment-resistant schizophrenia, serotonin and serendipity. Ther Adv Psychopharmacol 2018;8(1):63-70. doi: 10.1177/ 2045125317737003
6. Iasevoli F, Avagliano C, Altavilla B, et al. Disease severity in treatment resistant schizophrenia patients is mainly affected by negative symptoms, which mediate the effects of cognitive dysfunctions and neurological soft signs. Front Psychiatry 2018;9:553.
7. Remington G, Foussias G, Fervaha G, et al. Treating negative symptoms in schizophrenia: an update. Curr Ther Options Psychiatry 2016;3:133-150.
8. Goff DC, Hill M, Barch D. The treatment of cognitive impairment in schizophrenia. Pharmacol Biochem Behav 2011;99(2):245-253.
9. Tuominen HJ, Tiihonen J, Wahlbeck K. Glutamatergic drugs for schizophrenia. Cochrane Database Syst Rev 2006 Apr 19;(2):CD003730.
10. Arnsten AF, Girgis RR, Gray DL, Mailman RB. Novel dopamine therapeutics for cognitive deficits in schizophrenia. Biol Psychiatry 2017;81(1):67-77.
11. Müller N. Inflammation in schizophrenia: Pathogenetic aspects and therapeutic considerations. Schizophr Bull 2018;44(5):973-982
12. Rothstein JD, Patel S, Regan MR, et al. B-lactam antibiotics offer neuroprotection by increasing glutamate transporter expression. Nature 2005;433:73-77.
13. Inaba T, Katayama Y, Ueda M, Nito C. Neuroprotective effects of pretreatment with macrolide antibiotics on cerebral ischemia reprefusion injury. Neurol Res 2015;37(6):514-24. doi: 10.1179/ 1743132815Y.0000000005.
14. Costa R, Speretta E, Crowther DC, Cardoso I. Testing the therapeutic potential of doxycycline in a Drosophila melanogaster model of Alzheimer disease. J Biol Chem 2011;286(48):41647-41655. doi:10.1074/jbc.M111.274548
15. Kishimoto T, Horigome T, Takamiya A. Minocycline as a treatment for schizophrenia: is the discussion truly finished? Lancet Psychiatry 2018;5(11):856-857. doi: 10.1016/S2215-0366(18)30389-4.
16. Seki Y, Kato TA, Monji A, et al. Pretreatment of aripiprazole and minocycline, but not haloperidol, suppresses oligodendrocyte damage from interferon-γ-stimulated microglia in coc-culture model. Schizophr Res 2013;151:20-28.
17. Garrido-Messa N, Zarzuelo A, Galvez J. Minocycline: far beyond an antibiotic. Br J Pharmacol 2013;169(2):337-352.
18. Goff DC. D-cycloserine in schizophrenia: new strategies for
improving clinical outcomes by enhancing plasticity. Curr Neuropharmacol 2017;15(1):21-34.
19. Howes OD, McCutcheon R, Agid O, et al. Treatment-resistant schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) working group consensus guidelines on diagnosis and terminology. Am J Psychiatry 2017;174(3):216-229.
20. Vasiliu O. Maintenance pharmacologic therapies for opioid use disorders: beyond opioid agonists. Romanian Journal of Military Medicine 2019;CXXII(1):52-70.
21. Vasiliu O. Therapeutic management of schizophrenia and substance use disorders dual diagnosis- clinical vignettes. Romanian Journal of Military Medicine 2018;CXXI(2):26-34.
22. Ly D, DeLisi LE. Can antibiotics cause a psychosis? Schizophr Res 2017;189:204-207.
23. Moher D, Altman DG, Liberati A, Tezlaff J. PRISMA statement. Epidemiology 2011;22:128. doi: 10.1097/EDE.0b013e3181fe7825
24. Vasiliu O. Efficacy and tolerability of antibiotic augmentation in schizophrenia spectrum disorders- a systematic literature review. PROSPERO 2019 CRD42019119152 Available from: http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42019119152
25. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews 2015;4(1):1
26. Higgins JPT, Altman DG. Assessing risk of bias in included studies. In Higgins JPT, Green S, „Cochrane Handbook for Systematic reviews of Interventions: Cochrane Book Series”, 2008:187-241. doi:10.1002/9780470712184
27. Weiser M, Levi L, Burshtein S, et al. The effect of minocycline on symptoms in schizophrenia. Results from a randomized controlled trial. Schizophr Res pii: S0920-9964(18)30625-X. doi: 10.1016/j.schres.2018.10.023.
28. Deakin B, Suckling J, Barnes TRE, et al. The benefit of minocycline on negative symptoms of schizophrenia in patients with recent-onset psychosis (BeneMin): a randomised, double-blind, placebo-controlled trial. Lancet Psychiatry 2018;5(11):885-894. doi: 10.1016/S2215-0366(18)30345-6
29. Wehring HJ, Elsobky T, McEvoy JP, et al. Adjunctive minocycline in clozapine-treated patients with schizophrenia: analysing the effects of minocycline on clozapine plasma levels. Psychiatry Q 2018;89(1):73-80. doi: 10.1007/s11126-017-9515-x.
30. Liu F, Xie L, Zhang B, et al. No effect of adjunctive minocycline treatment on body metabolism in patients with schizophrenia. J Clin Psychopharmacol 2018;38(2):125-128. doi: 10.1097/ JCP.0000000000000841. 31. Kelly DL, Sullivan KM, McEvoy JP, et al. Adjunctive minocycline in clozapine-treated schizophrenia patients with persistent symptoms. J Clin Psychopharmacol 2015;35(4):374-81. doi: 10.1097 /JCP.0000000000000345.
32. Chaves C, Marque CR, Maia-de-Oliveira JP, et al. Effects of minocycline add-on treatment on brain morphometry and cerebral perfusion in recent-onset schizophrenia. Schizophr Res 2015;161(2-3):439-45. doi: 10.1016/j.schres.2014.11.031.
33. Ghanizadeh A, Dehbozorgi S, Omrani Sigaroodi M, Rezaei Z. Minocycline as add-on treatment decreases the negative symptoms of schizophrenia; a randomized placebo-controlled clinical trial. Recent Pat Inflamm Allergy Drug Discov 2014;8(3):211-5.
34. Liu F, Guo X, Wu R, et al. Minocycline supplementation for treatment of negative symptoms in early-phase schizophrenia:

20
double-blind, randomized, controlled trial. Schizophr Res 2014;153(1-3):169-76. doi: 10.1016/j.schres.2014.01.011.
35. Khodaie-Ardakani MR, Mirshafiee O, Farokhnia M, et al. Minocycline add-on to risperidone for treatment of negative symptoms in patients with stable schizophrenia: randomized double-blind placebo-controlled study. Psychiatry Res 2014;215(3):540-6. doi: 10.1016/j.psychres.2013.12.051.
36. Chaundhry IB, Hallak J, Husain N, et al. Minocycline benefits negative symptoms in early schizophrenia: a randomised double-blind placebo-controlled clinical trial in patients on standard treatment. J Psychopharmacol 2012;26(9):1185-93. doi: 10.1177/ 0269881112444941.
37. Levkovitz Y, Mendlovich S, Riwkes S, et al. A double-blind, randomized study of minocycline for the treatment of negative and cognitive symptoms in early-phase schizophrenia. J Clin Psychiatry 2010;71(2):138-49. doi: 10.4088/JCP.08m04666yel.
38. Miyaoka T, Yasukawa R, Yasuda H, et al. Minocycline as adjunctive therapy for schizophrenia: an open-label study. Clin Neuropharmacol 2008;31(5):287-92. doi: 10.1097/ WNF.0b013e3181593d45.
39. Takiguchi K, Uezato A, Itasaka M, et al. Association of schizophrenia onset age and white matter integrity with treatment effect of D-cycloserine: a randomized placebo-controlled double-blind cross-over study. BMC Psychiatry 2017;17(1):249. doi: 10.1186/s12888-017-1410-3.
40. Forsyth JK, Bachman P, Mathalon DH, et al. Effects of augmenting N-methyl-D-aspartate receptor signaling on working memory and experience-dependent plasticity in schizophrenia: an exploratory study using acute d-cycloserine. Schizophr Bull 2017;43(5):1123-33. doi: 10.1093/schbul/sbw193.
41. Cain CK, McCue M, Bello I, et al. d-Cycloserine augmentation of cognitive remediation in schizophrenia. Schizophr Res 2014;153(1-3):177-83.
42. Gottlieb JD, Cather C, Shanahan M, et al. D-cycloserine facilitation of cognitive behavioral therapy for delusions in schizophrenia. Schizophr Res 2011;131(1-3):69-74. doi: 10.1016/j.schres.2011.05.029.
43. Goff DC, Cather C, Gottlieb JD, et al. Once-weekly D-cycloserine effects on negative symptoms and cognition in schizophrenia: an exploratory study. Schizophr Res 2008;106(2-3):320-7. doi: 10.1016/j.schres.2008.08.012.
44. Buchanan RW, Javitt DC, Marder SR, et al. The Cognitive and Negative Symptoms in Schizophrenia Trial (CONSIST): the efficacy of glutamatergic agents for negative symptoms and cognitive impairments. Am J Psychiatry 2007;164(10):1593-602.
45. Yurgelun-Todd DA, Coyle JT, Gruber SA, et al. Functional magnetic resonance imaging studies of schizophrenic patients during word production: effects of D-cycloserine. Psychiatry Res 2005;138(1):23-31.
46. Goff DC, Herz L, Posever T, et al. A six-month, placebo-controlled trial of D-cycloserine co-administered with conventional antipsychotics in schizophrenia patients. Psychopharmacology (Berl) 2005;179(1):144-50.
47. Duncan EJ, Szilagyi S, Schwartz MP, et al. Effects of D-cycloserine on negative symptoms in schizophrenia. Schizophr Res 2004;71(2-3):239-48.
48. Evins AE, Amico E, Posever TA, et al. D-cycloserine added to risperidone in patients with primary negative symptoms of schizophrenia. Schizophr Res 2002;56(1-2):19-23.
49. Heresco-Levy U, Ermilov M, Shimoni J, et al. Placebo-controlled trial of D-cycloserine added to conventional neuroleptics, olanzapine, or risperidone in schizophrenia. Am J Psychiatry 2002;159(3):480-2.
50. Heresco-Levy U, Javitt DC, Ermilov M, et al. Double-blind, placebo-controlled, crossover trial of D-cycloserine adjuvant therapy for treatment-resistant schizophrenia. Int J Neuropsychopharmacol 1998;1(2):131-135.
51. van Berckel BN, Evenblij CN, van Loon BJ, et al. D-cycloserine increases positive symptoms in chronic schizophrenic patients when administered in addition to antipsychotics: a double-blind, parallel, placebo-controlled study. Neuropsychopharmacology 1999;21(2):203-10.
52. Goff DC, Henderson DC, Evins AE, Amico E. A placebo-controlled crossover trial of D-cycloserine added to clozapine in patients with schizophrenia. Biol Psychiatry 1999;45(4):512-4.
53. Goff DC, Tsai G, Levitt J, et al. A placebo-controlled trial of D-cycloserine added to conventional neuroleptics in patients with schizophrenia. Arch Gen Psychiatry 1999;56(1):21-7.
54. Goff DC, Tsai G, Manoach DS, et al. D-cycloserine added to clozapine for patients with schizophrenia. Am J Psychiatry 1996;153(12):1628-30.
55. Rosse RB, Fay-McCarthy M, Kendrick K, et al. D-cycloserine adjuvant therapy to molindone in the treatment of schizophrenia. Clin Neuropharmacol 1996;19(5):444-50.
56. Goff DC, Tsai G, Manoach DS, Coyle JT. Dose-finding trial of D-cycloserine added to neuroleptics for negative symptoms in schizophrenia. Am J Psychiatry 1995;152(8):1213-5.
57. GRADE Recommendations. Accessed on 02/07/2016 at www.gradeworkinggroup.org.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
21
Article received on May 20, 2019 and accepted for publishing on November 21, 2019. REVIEW ARTICLE
Nonoperative management of high-grade splenic injury. A review of the literature and case report
Bogdan Socea1, Cristiana Bogaciu2, Alexandru C. Carâp1, Vlad D. Băleanu2, Dragoş V. Daviţoiu1, Tiberiu Ş. Ţenea Cojan3, Ion Păun3, Vlad D. Constantin1
Abstract: Splenic injuries causedby traumatic events are common in the emergency departments, mostly because the spleen is frequently affected in trauma. The lesions of the spleen can be diagnosed using a contrast enhanced computed tomography and based on the results, the injury of the spleen is graded. The management of the patient can be operative or nonoperative. The choice of treatment is decided by the hemodynamic stability of the patient.
INTRODUCTION
Blunt abdominal trauma mostly due to sports activities is common in the emergency departments in Europe and 30% of the polytrauma patients have abdominal organs injuries [1]. The most frequently injured organ in blunt abdominal trauma is the spleen, which is involved in about 32% of abdominal injuries [2, 3].
The splenic injuries could be treated surgically or by a nonoperative management. In cases of hemodynamically stable patients, nonoperative management of the blunt splenic injuries is preferred and the recognition of the overwhelming post splenectomy infections also sustains the nonoperative management [2, 4].
The splenic injury in trauma is diagnosed based on computed tomography (CT) and it can also show other injuries associated with trauma [5]. The sensitivity of the CT examination in detecting splenic injuries has been reported to be as high as 95% [6].
On trauma patients should be performed FAST to find the evidence of intraabdominal hemorrhage. The patients with
positive FAST and unstable hemodynamically, with or without cardiovascular associated disorders [7-9], are rushed to the operating room and the stable ones are planned for contrast-enhanced computed tomography [10].
Based on the CT results, various grading systems were introduced to help physicians to take the best decision regarding the management of the patient [6].
The best known and used splenic and hepatic grading system is the one established by the American Associationfor the Surgery of Trauma (AAST) [11] (Figure 1).
Vascular injuries in splenic trauma with active bleeding could be detected on a contrast-enhanced helical CT scan as perisplenic material extravasation [6, 12].
The selection of the treatment, operative or nonoperative, is difficult, but there are some factors such as hemodynamic status, age, grade of splenic injury, quantity of the
1 "Sf. Pantelimon" Emergency Clinical Hospital, Department of General Surgery, "Carol Davila" University of Medicine and Pharmacy, Bucharest 2 "Sf. Pantelimon" Emergency Clinical Hospital, Department of General Surgery 3 University of Medicine and Pharmacy of Craiova, Department of Surgery, CFR Hospital of Craiova
Corresponding author Bogdan Socea MD [email protected]

22
hemoperitoneum and associated injuries useful to decide the optimal standard of care for the trauma patient [11].
The rate of success in the nonoperative management of splenic injuries is very high in many published series, between 80-94% in the cases of adult trauma patients[2, 11].
There is some evidence that older patients might have a worse prognosis with nonoperative management than younger patients, and several series have reported thatpatients older than 55 years are less likely to have a
successful nonoperativemanagement [11, 13, 14].
Other option of treatment in splenic lesions is the splenic artery embolization, which is classified as nonoperative treatment. Splenic artery embolization is used to reduce the incidence of reccurent bleeding, factor that would lead to hemodynamic instability [15-17]. Studies confirm a high rates of splenic salvage after the combined treatments such as splenic artery embolization and nonoperative management [3].
Table 1: The splenic organ in Jury Scaling System of the American Association for the Surgery of Trauma, 1994 revision
Grade* Injury description
I Hematoma Subcapsular, <10% surface area
Laceration Capsular tear, <1 cm parenchymal depth
II Hematoma Subcapsular, 10–50% surface area, <5 cm in diameter
Laceration 1–3 cm parenchymal depth that does not involve a trabecular vessel
III Hematoma Subcapsular, >50% surface area or expanding; ruptured subcapsular or parenchymal hematoma; intraparenchymal hematoma >5 cm or expanding
Laceration >3 cm parenchymal depth or involving trabecular vessels
IV Laceration Laceration involving segmental or hilar vessels producing major devascularization (>25% of spleen)
Laceration Completely shattered spleen
V Vascular Hilar vascular injury that devascularizes spleen *Advance one grade for multiple injuries up to grade III
The operative treatment is preferred in all cases of instable hemodynamically patients with/without dyselectrolytemia [18, 19]. There are two surgical options that the operator can take after examining the injury: splenectomy or spleen preserving surgery [20, 21].
There are some types of spleen preserving surgery including spleen packing, partial splenectomy or splenorrhaphy [11].
Spleen packing is used in selected cases with isolated splenic injuries and stable patients.
If the patient is unstable with a grade IV or V spleen injury splenectomy should be performed. Another surgical technique that can be performed is the partial splenectomy and this is possible because of the segmental nature of the splenic blood supply [20].
One of the most dangerous complications that could appear after a splenectomy performed in trauma is OPSI (overwhelming postsplenectomy infection). OPSI is an emergent condition which at first may develop as a mild infection and then rapidly progress to sepsis [22, 23] that has a 50-70% risk of mortality with or without treatment [24-28].
Vaccination against S. pneumoniae, N. meningitidis, and HIB are recommended in addition to a yearly influenza vaccine to avoid OPSI, but the administration of these vaccines is recommended after the postoperative day 14 to increase
the immune response in patients who have undergone splenectomy due to trauma [29-31].
MATERIAL AND METHOD
We highlight the key aspects of the nonoperative management of blunt trauma splenic injuries by doing a review of the literature.
We researched the PubMed and Cochrane datebases for studies involving nonoperative management of the splenic traumatic injuries. The studies we analyzed were published between 2017 and March 2019.
CASE REPORT
We present the case of a 25-year-old woman, who came into the emergency room after a motocycle accident. The clinical examination showed tenderness in the left upper quadrant and the right arm was painful, the patient was stable hemodynamically. An X-ray of the right arm showed fracture of the radius and cubitus that were immobilized in a cast [32].
Point of care abdominal ultrasound was performed and it suggested a splenic lesion – non-homogeneous echostructure and hypoechogenic areas (Figure 1), and free fluid in Morrison and Douglas pouches (Figure 2).

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
23
Figure 1: Ultrasound finding of splenic lesion
Figure 2: Hemoperitoneum: hypoechoic, nonhomogeneous paravesical image
Figure 3: Native CT image showing grade III splenic lesion (hypodense zone – densities between 34 and 41 Hounsfield Units –
from hilum to capsule)
Figure 4: Ultrasound finding of splenic lesion
Figure 5: Contrast-enhanced CT scan - spleen hilum involvement
Figure 6: Blood accumulation in Douglas' pouch

24
The blood tests revealed anemia (hemoglobin 9.30 g/dL) and leukocytosis (14.510/uL).
Contrast-enhanced CT scan of the abdomen and pelvis revealed a grade III splenic injury (5.6 cm hematoma and 2 cm laceration) (Figures 3, 5), fluid surrounding the liver, in the Morrison pouch, in the right and left paracolic gutters (Figure 6). No contrast extravasation at level of the spleen was detected, no other traumatic injuries (Figure 4).
Hypodense zones of splenic tissue should be differentiated from cystic lesions of spleen, even hydatid cyst that, in case of rupture, could mimic acute abdomen [33].
We decided to treat the patient conservatory, to monitor her clinically every 6 hours, the blood pressure and pulse were measured also every 6 hours and she was monitored ultrasonographic daily. There were no modifications during the admission into the hospital and the patient was discharged in the fifth day. She was informed about the signs of hemorrhage (abdominal pain, light-headedness, syncope, difficulty breathing and chest pain) and she was instructed to call immediately a surgical emergency center if any of these symptoms appear.
One week after the discharge the patient came to follow up, she was examined clinically, ultrasonographically and biologically and everything was normal.
At this moment, there is no information about the nonoperative management of the splenic trauma regarding how long should the patient be admitted, how long should it be between the discharge and the follow up, how frequently should the level of hemoglobin and hematocrit be measured and how frequent should the patient be examined ultrasonographically [34, 35].
CONCLUSION
Splenic injuries are common and the patients stable hemodynamically who have grade III splenic lesions due to trauma could be managed nonoperatively. There are no protocols about the nonoperative management of the splenic injuries and we think their existance could influence the morbidity and mortality of these patients. Prospective trials could be performed to establish a protocol of treatment and follow up.
References:
1. Fodor M, Primavesi F, Morell-Hofert D, Haselbacher M, Braunwarth E, Cardini B, Gassner E, Öfner D, Stättner S. Non-operative Management of Blunt Hepatic and Splenic Injuries-practical Aspects and Value of Radiological Scoring Systems. European Surgery. 2018;50(6):285-298.
2. Teuben MPJ, Spijkerman R, Blokhuis TJ, Pfeifer R, Teuber H, Pape HC, Leenen LPH. Safety of Selective Nonoperative Management for Blunt Splenic Trauma: The Impact of Concomitant Injuries. Patient Saf Surg. 2018;12:32.
3. Cinquantini F, Simonini E, Di Saverio S, Cecchelli C, Kwan SH, Ponti F, Coniglio C, Tugnoli G, Torricelli P. Non-surgical Management of Blunt Splenic Trauma: A Comparative Analysis of Non-operative Management and Splenic Artery Embolization-Experience from a European Trauma Center. Cardiovascular and Interventional Radiology. 2018;41(9):1324-1332.
4. Diaconu CC, Arsene D, Balaceanu A, Bartos D. A rare tumor revealed by abdominal trauma: case presentation. Romanian Journal of Morphology and Embryology 2014;55(3):973-976.
5. Diaconu C, Balaceanu A, Morosan E. Sepsis biomarkers: past, present and future. Farmacia 2015;63(6):811-815.
6. Wong Y-C, Wang L-J, Fang J-F, Chen C-J, Lin B-C, Chen R-J. Perisplenic Extravasation of Contrast Medium on Enhanced Helical Computed Tomography: A Reliable Indicator for Early Surgical Management in Blunt Splenic Injuries. Chang Gung Medical Journal. 2002;25(6):381-387.
7. Diaconu CC, Drăgoi CM, Bratu OG, Neagu TP, Pantea Stoian A, Cobelschi PC, Nicolae AC, Iancu MA, Hainăroșie R, Stănescu AMA,
Socea B. New approaches and perspectives for the pharmacological treatment of arterial hypertension. Farmacia. 2018; 66(3):408-415.
8. Manea M, Marcu D, Pantea Stoian A, Gaman MA, Gaman AM, Socea B, Neagu TP, Stanescu AMA, Bratu OG, Diaconu CC. Heart failure with preserved ejection fraction and atrial fibrillation. A review. Rev Chim (Bucharest). 2018;69(11):4180-4184.
9. Niculae A, Peride I, Marinescu-Paninopol A, Vrabie CD, Ginghină O, Jecan CR, Bratu OG. Renal artery bilateral arteriosclerosis cause of resistant hypertension in hemodialysed patients.Rom J Morphol Embryol. 2016;57(2):591-594.
10. Bagaria D, Kumar A, Ratan A, Amit G, Kumar A, Kumar S, Mishra B, Sagar S. Changing Aspects in the Management of Splenic Injury Patients: Experience of 129 Isolated Splenic Injury Patients at Level 1 Trauma Center from India. Journal of Emergencies, Trauma, and Shock. 2019;12(1):35-39.
11. Moore, Ernest Eugene, David V. Feliciano, and Kenneth L. Mattox. Trauma. 7th ed. New York: McGraw-Hill Education, 2017.
12. Karlo CA, Stolzmann P, Do RK, Alkadhi H. Computed tomography of the spleen: how to interpret the hypodense lesion. Insights Imaging. 2013;4(1):65–76.
13. Smith JS, Wengrovitz MA, DeLong BS. Prospective validation of criteria, including age, for safe, nonsurgical management of the ruptured spleen. J Trauma. 1992;33:363.
14. Bobic S, Socea B, Carâp A, Sandu VA, Popa F, Constantin VD. Non-operative management of the splenic trauma. Eur J Trauma Emerg Surg. 2017;43(Suppl 1): S147-8.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
25
15. Haan JM, Biffl W, Knudson MM, et al. Splenic embolization revisited: a multicenter review. J Trauma. 2004;56:542–7
16. Ekeh AP, Izu B, Ryan M, McCarthy MC. The impact of splenic artery embolization on the management of splenic trauma: an 8-year review. Am J Surg. 2009;197:337–41.
17. van der Vlies CH, Hoekstra J, Ponsen KJ, et al. Impact of splenic artery embolization on the success rate of nonoperative management for blunt splenic injury. CardiovascInterventRadiol. 2012;35:76–81.
18. Diaconu CC, Manea M, Iancu MA, Stănescu AMA, Socea B, Spînu DA, Marcu D, Bratu OG. Hyponatremia in patients with heart failure: a prognostic marker. Rev Chim (Bucharest). 2018;69(5): 1071-1074.
19. Diaconu CC, Stanescu AMA, Pantea Stoian A, Tincu RC, Cobilinschi C, Dragomirescu RIF, Socea B, Spinu DA, Marcu D, Socea LI, Bratu OG.Hyperkalemia and cardiovascular diseases: new molecules for the treatment. Rev Chim (Bucharest). 2018; 69(6):1367-1370.
20. Feliciano, D. V., C. G. Bitondo, K. L. Mattox, J. D. Rumisek, J. M. Burch, and G. L. Jordan. A Four-year Experience with Splenectomy versus Splenorrhaphy. Annals of Surgery. May 1985. Accessed May 1, 2019. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1250761/.
21. Socea B, Diaconu C, Bratu OG, Stoian AP, Constantin VD. Splenectomy in Immune Thrombocytopenia: When, Why and How? Revista Română de Paliaţie. 2019;12(1):16-19.
22. Spînu D, Bratu O, Popescu R, Marcu D, Rădulescu A, Mischianu D. Clostridium difficile-an emerging plague. Romanian Journal of Military Medicine. 2015;118(3):12-15.
23. Rădulescu A, Mădan V, Aungurenci A, Bratu O, Farcaș C, Dinu M, Mischianu D. Antibiotic resistant urinary tract infections in an urology ward. Romanian Journal of Military Medicine. 2015;118(3):20-22.
24. Morgan TL, Tomich EB. Overwhelming post-splenectomyinfec-tion (OPSI): a case report and review of the literature. J Emerg Med 2012;43:758–63.
25. Belli AK, Dönmez C, Özcan Ö, Dere Ö, Çaylak SD, Elibol FD, Yazkan C, Yılmaz N, Nazlı O. Adherence to Vaccination Recommendations after Traumatic Splenic Injury. UlusalTravmaAcilCerrahiDergisi. 2018;24:337-342.
26. Bisharat N, Omari H, Lavi I, Raz R. Risk of infection and death
among post-splenectomy patients. J Infect. 2001;43:182–6.
27. Thomsen RW, Schoonen WM, Farkas DK, Riis A, Jacobsen J, Fryzek JP, et al. Risk for hospital contact with infection in patients with splenectomy: a population-based cohort study. Ann Intern Med. 2009;151:546–55.
28. Kristinsson SY, Gridley G, Hoover RN, Check D, Landgren O. Long-term risks after splenectomy among 8,149 cancer-free American veterans: a cohort study with up to 27 years follow-up. Haematologica 2014;99:392–8.
29. Cohn AC, MacNeil JR, Clark TA, Ortega-Sanchez IR, Briere EZ, Meissner HC, et al; Centers for Disease Control and Prevention (CDC). Prevention and control of meningococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2013;62:1–28
30. Carlino C, Zaratti L, Lucciola G, Franco E. National Vaccine Prevention Plan (PNPV) 2012-2014 in the Italian Regions. IgSanitaPubbl. 2013;69:131–43.
31. Davies JM, Lewis MP, Wimperis J, Rafi I, Ladhani S, Bolton-Maggs PH; British Committee for Standards in Haematology. Review of guidelines for the prevention and treatment of infection in patients with an absent or dysfunctional spleen: prepared on behalf of the British Committee for Standards in Haematology by a working party of the Haemato-Oncology task force. Br J Haematol 2011;155:308–17.
32. Tiglis M, Neagu TP, Elfara M, Diaconu CC, Bratu OG, Vacaroiu IA, Grintescu IM. Nefopam and its role in modulating acute and chronic pain. Rev Chim (Bucharest). 2018;69(10):2877-2880.
33. Constantin VD, Popa F, Socea B, Carâp AC, Bǎlǎlǎu C, Motofei I, Banu P, Costea DI. Spontaneous rupture of a splenic hydatid cyst with anaphylaxis in a patient with multi-organ hydatid disease. Chirurgia. 2014;109(3): 393-5.
34. Laslo CL, Pantea Stoian A, Socea B, et al.New oral anticoagulants and their reversal agents. Journal of Mind and Medical Sciences.2018;5(2):195-201.
35. Țica OA, Țica O, Antal L, Hatos A, Popescu MI, Pantea Stoian A, Bratu OG, Găman MA, Pițuru SM, Diaconu CC. Modern oral anticoagulant treatment in patients with atrial fibrillation and heart failure: insights from the clinical practice.Farmacia.2018;66(6):972-976

26
Article received on May 20, 2019 and accepted for publishing on November 23, 2019. REVIEW ARTICLE
Atherosclerosis in rheumatoid arthritis – the importance of imaging tests
Oana P. Ionescu1, Silviu M. Stanciu1, Mihai L. Ciobîcă1
Abstract: As reported by literature, rheumatoid arthritis is a rheumatic disease with an increased risk of developing cardiovascular complications. Early detection of atherosclerosis by non-invasive techniques represent a current challenge of patient management. Current EULAR guidelines recommend careful monitoring of cardiovascular risk factors by stratification of patients and strict control of rheumatic disease activity to reduce it. The classic evaluation of intima-medium thickness (IMT) was completed by quantifying the degree of inflammation of the carotid plate using positron emission tomography or the degree of coronary calcifications by calculating Agatston score using Coronary Computer Tomography. These modern investigation techniques allow identification of several subclinical stages of atherosclerosis, the interest in their early detection resulting from the fact that, in this stage, through specific measures, the cardiovascular complications can be prevented.
Keywords: rheumatoid arthritis, atherosclerosis, cardiovascular risk, imaging tests
INTRODUCTION
Rheumatoid arthritis is a rheumatic disease with an increased risk of cardiovascular events due to advanced atherosclerosis [1]. The development of atheromatous plaque is based on chronic inflammation found in both rheumatoid arthritis and atherosclerosis[2]. Recent studies have shown a higher prevalence of plaque in patients with rheumatoid arthritis, which explains their negative predictive role[3,4]. The higher frequency of traditional risk factors in patients with rheumatoid arthritis (hypertension, type II diabetes, smoking, high cholesterol and obesity) is another factor contributing to the development of cardiovascular complications. Its impact is different from that of the population not suffering of this pathology [5,6]. Current EULAR guidelines recommend careful monitoring of cardiovascular risk factors by stratification of patients and strict control of rheumatic disease activity to reduce it [6]. The early detection of atherosclerotic changes by non-
invasive techniques is a current concern of patient management. Collaboration between rheumatologist and cardiologist and prospects of a new specialty - cardio-oncology will be encouraged in future in order to improve the prognosis of patients affected by rheumatoid arthritis and atherosclerosis.
NONINVASIVE IMAGING OF INTRACRANIAL VESSELS
Atherosclerotic plaque is the trigger for cardiovascular events, its vulnerability being due to plaque composition, inflammatory cell content, age, and not necessarily plaque size [7, 8]. In rheumatoid arthritis, advanced inflammation causes a particular phenotype of the plaque, thus presenting an increased risk of myocardial infarction or stroke [9, 10]. Transcranial Doppler examination is a method of measuring cerebral blood flow in the main intracranial arteries. This method uses 2 MHz ultrasound probes to dynamically detect intracranial arteries through thinner areas of the skull called
1 Carol Davila University Central Emergency Military Hospital, Bucharest, Romania
Corresponding author: Oana P. Ionescu MD [email protected]

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
27
acoustic windows [11, 12]. This study has proven inexpensive, reproducible and provides information on the prognosis of cardiovascular events [13, 14, 15, 16]. Measurement of average mean cerebral arterial flow rate, pulsatility index, and calculation of the relationship between these two indices revealed prognostic factors of recurrent cardiovascular events [17, 18] In patients with rheumatoid arthritis, there was an increase in the prevalence of distal occlusions of the middle cerebral artery and basilar artery detected by transcranial Doppler [11].
Another investigation commonly used in the clinic is the Doppler ultrasound of the carotid arteries. This is a good way to identify patients with rheumatoid arthritis at high cardiovascular risk who can benefit from active treatment.
Proper stratification of cardiovascular risk is a key element in the management of patients with rheumatoid arthritis. It is well known the EULAR's adaptation of cardiovascular risk assessment based on coronary risk assessment (SCORE) multiplied by 1.5 in patients with rheumatoid arthritis that meet two of the following three criteria: disease> 10 years, rheumatoid risk factor (RF) or anti-cyclic cytoplankin peptide (anti-CCP) antibody and presence of serious extra-articular manifestations [19]. However, the authors recommend performing a carotid ultrasound scan when SCORE (Figure 1)[20] does not report high cardiovascular risk, considering studies in which patients with rheumatoid arthritis were not considered at high risk for cardiovascular events by calculating SCORE risk, but who had significant cardiovascular events: myocardial infarction and stroke [21].
Figure 1: Cardiovascular risk estimation using SCORE
(Source: European Guidelines on CVD Prevention in Clinical Practice 2016 Eur J Prev Cardiol. 2016 Jul;23(11):NP1-NP96. doi: 10.1177/2047487316653709)
Carotid Doppler ultrasound evaluates intima-medium thickness (IMT) and highlights atherosclerotic plaques, making it an affordable, easy-to-use, reproducible, low cost study. A meta-analysis of 1384 patients with rheumatoid arthritis concluded that a carotid IMT increased from the control group population – 1147 patients (normal IMT <0.9 mm) [22]. Olah C. et al [11] also published in 2017 a study on the assessment of intracranial vessels in combination with carotid atherosclerosis and stroke in patients with rheumatoid arthritis in which more patients with rheumatic disease had at least a plaque in the right carotid artery, and its score was higher than that of the control group patients. Thus, we can say that carotid ultrasound remains an easy-to-use tool in practice, but different protocols for measuring the carotid plaque and operator-dependent, makes this investigation more and more replaced by carotid magnetic
resonance.
Carotid magnetic resonance has the advantage of capturing the entire circumference of the carotid wall, including the adventitia and the outer layer, as opposed to carotid ultrasound, which only visualizes the intima of the carotid artery. In the multiethnic study of atherosclerosis, conducted in six US research centers, 698 patients were included and examined by carotid ultrasound and MRI. The results of the study showed that MRI could be a better predictor of cardiovascular events than carotid ultrasound, as the combination of wall thickness measured by magnetic resonance was stronger than that of ultrasound-measured IMT [23]. In addition, the arterial history revealed by MRI seems to be a better predictor of cardiovascular complications in a study that showed an increase in inflammatory cytokine expression in aortic adventitia in

28
patients with rheumatoid arthritis who suffered from coronary artery bypasses compared to control patients [24, 25]. Another advantage of this method of non-invasive diagnosis is the strong correlation with the histological phenotype of atherosclerotic plaque, the dynamic contrast-enhanced MRI (DCE-MRI) allowing to evaluate the neovascularization of the atherosclerotic plaque, its vulnerability by the degree of inflammation and the degree of hemorrhage in plaque, and the effectiveness of therapeutic interventions [26, 27].
Another more modern technique capable of quantifying the degree of inflammation of the carotid plate is positron emission tomography. This exploration uses 18-F-fludeoxy-glucose, a glucose analogue, which has the ability to accumulate in inflamed atherosclerotic plaque, where exists a greater amount of marked pozitrons [28]. Thus, CT or magnetic resonance imaging is possible to map the affected area, the absorption of fludeoxoxiglucose being associated with the identification of lesions at high risk of embolization [29]. Another radioactive agent used in the detection of atherosclerosis is sodium fluoride (18-F-NaF), which is capable of binding to calcified unstable arterial zones. During the course of atherosclerotic disease, two types of vascular damage can occur: macrocalcification – conferring stability to plaque atheroma and microcalcification – associated with an increased risk of plaque vulnerability. Sodium fluoride PET-CT differentiates the two types of lesions presented above, the new technique being able to revolutionize the treatment of atherosclerosis, increasing the chances of preventing cardiovascular complications [30].
NONINVASIVE CARDIAC IMAGING
Advanced atherosclerosis in rheumatoid arthritis is also evident in the heart, manifesting itself in various forms: coronary ischemia - micro and macrovascular, inflammation or myocardial fibrosis (myocarditis) [31]. Rheumatoid arthritis should therefore be closely monitored using non-invasive techniques to identify patients at high risk of developing cardiovascular complications. A recent study performed by a Danish team, which included the entire population over 18 years old diagnosed with rheumatoid arthritis between 1978 and 2008, found an increased risk of heart failure in patients with rheumatoid arthritis, justifying the need for cardiovascular screening [32].
Coronary arteries can be assessed non-invasively by transthoracic or transesophageal ultrasound and magnetic resonance imaging computed tomography or computed tomography after endothelial-dependent vasodilation [33].
Transthoracic echocardiography is a classic method of
evaluating cardiac function that, by its characteristics, can detect patients with a high cardiovascular risk, such as those with rheumatoid arthritis. Recent studies have demonstrated subclinical impairment of right and left ventricular function in patients with rheumatoid arthritis versus control, as demonstrated by the comparison of early ventricular (E-wave) filling, late ventricular (A-wave) filling, and the E/A ratio of the two lots [34]. A modern clinical application of transthoracic echocardiography is transthoracic stress echography with dipiridamol, able to evaluate the left coronary reserve. This represents the ratio of maximal coronary flow during stress to basal rate, which is a very sensitive diagnostic marker (> 90%) for coronary heart disease [35, 36]. In the literature, it has been reported that a value of coronary reserve flow <2 is associated with the presence of coronary stenosis [37]. In the absence of evidence of epicardial coronary stenosis, an abnormal coronary flow reserve may indicate a pathology of coronary microcirculation in patients with reperfused myocardial infarction, hypertension, diabetes mellitus, hyper-cholesterolemia, X syndrome or hypertrophic cardiomyopathy. Recent studies have also demonstrated a negative prognostic value of coronary reserve flow in patients with or suspected of coronary artery disease [38].
Transesophageal cardiac ultrasound is an investigation that can successfully complete transthoracic cardiac ultrasound, which has the disadvantage of visualizing the posterior structures of the heart, or which has the disadvantage of a difficult window of exploration in obese patients or affected by lung disease. Transesophageal cardiac ultrasound was used in a case-control study conducted on a group of 30 patients diagnosed with rheumatoid arthritis, which concluded that there was a high frequency of regurgitation of the mitral and aortic valves and obvious signs of cardiomyopathy in most patients [39].
Computer tomography is another method of assessing atherosclerosis present in the patient diagnosed with rheumatoid arthritis by completing the classical techniques mentioned above. A recent study aimed at examining the impact of rheumatoid arthritis on the prevalence and severity of coronary artery disease, concluded that the presence of coronary calcifications is common in patients with serum-positive rheumatoid arthritis [40]. This result was based on measurements of calcium score, an indicator of the degree of coronary artery calcification, by means of computer tomography. Figure 2 presents intense calcifications in the coronary artery walls, more evident on the LAD 2 (60-70%). The examination is non-invasive, without the use of a contrast substance, guided by the ECG; it does not require a long examination time and shows

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
29
minimal irradiation.
Figure 2: Intense calcifications present in the coronary artery walls, more evident on the LAD 2 (60-70%). Normal detachment of
coronary arteries.
The patient is lying down during the exam, and the calcium score is measured in deep inspiration. Coronary CT scan
provides information on cardiovascular risk by calculating Agatston score: a small risk is equivalent to a score below 100 Agatston units, an intermediate risk of 100 to 300 Agatston units, and an increased risk of more than 300 Agatston units (Figure 3). The presence of an elevated risk score (over 300 Agatson units) requires a myocardial scintigraphy and the presence of a score of over 600 Agatson Units to perform invasive coronarography.
Still in the field of noninvasive imaging techniques, cardiac nuclear magnetic resonance is increasingly used, which is the gold standard for the evaluation of myocardial viability.
This modern technique was used in a study comparing the structure and function of myocardial patients with rheumatoid arthritis compared to a control group included in the multi-ethnic Baltimore study on atherosclerosis, unaffected by rheumatic pathology.
Figure 3: Cardiac CT: Calcium Scoring 529.74 Agaston units (LAD 329 UA, LCX 70.62 UA, RCA 129.86 UA)
The findings showed that there was no statistically significant difference between the two volumes in the left ventricular and telediastolic volumes, but that the left ventricular ejection fraction and the cardiac output were lower in patients with rheumatic arthritis, indicating a progression of heart failure [41]. Cardiac Magnetic Resonance has also been applied to a group of rheumatoid arthritis patients with no history of cardiovascular disease (pulmonary hypertension, coronary artery disease, valvulopathy, atrial fibrillation or diabetes), and the results were detection of subendocardial infusion defects in correlation with disease activity, respectively with markers of inflammation – PCR and VSH [42]. These results confirm the major involvement of inflammation in worsening cardiovascular status in patients with rheumatoid arthritis.
NON-INVASIVE IMAGING OF PERIPHERAL CIRCULATION
Peripheral circulation can be investigated non-invasively by a variety of methods from the classical ankle-arm index, or measuring post-occlusive reactive hyperemia with a plethysmograph up to brachial artery mediated vasodilatation, measured ultrasonographically or by magnetic resonance. These tests are useful in assessing endothelial function and may have considerable potential in the future in assessing rheumatic patients.
CONCLUSIONS
In conclusion, we can state that the modern investigation techniques allow identification of several subclinical stages of atherosclerosis, the interest in their early detection

30
resulting from the observation that in this stage, through specific measures, the cardiovascular complications can be prevented. Systemic chronic inflammation in atherosclerosis and rheumatic diseases brings to the forefront the need for a multibiomarker approach in cardiovascular risk assessment. Biological markers correlated with imaging tests may be important prognostic elements capable of delaying the progression of atherosclerosis, providing the opportunity for early cardiovascular treatment. Until now, atherosclerosis imaging has been more centered on the anatomical aspect, with current trends focusing on a
more functional approach using multi-modal images. The ultimate goal would be to fuse between anatomical and functional data and to achieve a more faithful image of the atherosclerotic plaque. In the future, an exploration of molecular and cellular mechanisms of cardiovascular disease is expected through molecular imaging that is able to overcome various aspects of inflammation involved in atherosclerosis. Slowing or stopping the progression of the inflammation process will be the future target of patient management by improving their prognosis and decrease the rate of their cardiovascular complications.
References:1. Ruscitti P, Margiotta DPE, Macaluso F, et al, Subclinical atherosclerosis and history of cardiovascular events in Italian patients with rheumatoid arthritis: Results from a cross-sectional, multicenter GIRRCS (Gruppo Italiano di Ricerca in Reumatologia Clinica e Sperimentale) study. Medicine (Baltimore) 2017;96:e8180.
2. Libby P. Inflammation in atherosclerosis. Nature. 2002; 420:868-74.
3. Maradit-Kremers H., Crowson C.S., Nicola P.J. et al, Increased unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: a population-based cohort study. Arthritis Rheum 2005; 52(2), 402–11.
4. Sodergren A., Stegmayr B., Ohman M.L., Walberg-Jonsson S., Increased incidence of stroke and impaired prognosis after stroke among patients with seropositive rheumatoid arthritis. Clin Exp Rheumatol 2009; 27(4), 641–4.
5. Radner H, Lesperance T, Accortt NA, Solomon DH, Incidence and prevalence of cardiovascular risk factors among patients with rheumatoid arthritis, psoriasis, or psoriatic arthritis. Arthritis Care Res (Hoboken) 2017;69(10):1510–8.
6. Pujades-Rodriguez M., Duyx B., Thomas S.L. et al, Rheumatoid arthritis and incidence of twelve initial presentations of cardiovascular disease: a population record-linkage cohort study in England. PLoS One 2016;11(3):e0151245.
7. Rothwell PM, Gutnikov SA, Warlow CP, Reanalysis of the final results of the European Carotid Surgery Trial. Stroke 2003;34(2), 514–23.
8. Redgrave JN, Lovett JK, Gallagher PJ, Rothwell PM, Histological assessment of 526 symptomatic carotid plaques in relation to the nature and timing of ischemic symptoms: the Oxford plaque study. Circulation 2006, 113(19), 2320–8.
9. Sandoo A, Veldhuijzen van Zanten JJ, Metsios GS, Caroll D, Kitas GD, Vascular function and morphology in rheumatoid arthritis: a systematic review. Rheumatology (Oxford) 2011, 50, 2125–2139.
10. Giles, JT, Post WS, Blumenthal RS, et al., Longitudinal predictors of progression of carotid atherosclerosis in rheumatoid arthritis. Arthritis Rheum. 2011;63:3216–3225.
11. Olah C, Kardos Z, Sepsi M et al., Assessment of intracranial vessels in association with carotid atherosclerosis and brain vascular lesions in rheumatoid arthritis. Arthritis Research & Therapy (2017); 19:213.
12. DeWitt LD, Wechsler LR. Transcranial Doppler. Stroke 1988;19(7):915–921
13. Alexandrov AV, Sloan MA, Wong LK, et al., American Society of Neuroimaging Practice Guidelines Committee. Practice standards for transcranial Doppler ultrasound: part I—test performance. J Neuroimaging. 2007;17(1):11–18.
14. Babikian VL, Feldmann E, Wechsler LR et al., Transcranial Doppler ultrasonography: Year 2000 update. J Neuroimaging 2000;10:101–115.
15. Serrador JM, Picot PA, Rutt BK, Shoemaker JK, Bondar RL, MRI measures of middle cerebral artery diameter in conscious humans during simulated orthostasis. Stroke. 2000;31(7):1672–1678.
16. Vriens EM, Kraaier V, Musbach M, Wieneke GH, van Huffelen AC, Transcranial pulsed Doppler measurements of blood velocity in the middle cerebral artery: reference values at rest and during hyperventilation in healthy volunteers in relation to age and sex. Ultrasound Med. Biol. 1989;15(1):1–8.
17. Marinoni M, Ginanneschi A, Forleo P, Amaducci L, Technical limits in transcranial Doppler recording: inadequate acoustic windows. Ultrasound Med Biol. 1997;23(8):1275–7.
18. Wijnhoud AD, Koudstaal PJ, Dippel DW, The prognostic value of pulsatility index, flow velocity, and their ratio, measured with TCD ultrasound, in patients with a recent TIA or ischemic stroke. Acta Neurol Scand.2011;124(4):238–44.
19. Peters MJ, Symmons DP, McCarey D, et al., EULAR evidence-based recommendations for cardiovascular risk management in patients with rheumatoid arthritis and other forms of inflammatory arthritis. Ann Rheum Dis. 2010;69(2):325–331.
20. Piepoli MF, Hoes AW, Agewall S et al., 2016 European Guidelines on CVD Prevention in Clinical Practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur J Prev Cardiol. 2016 Jul;23(11):NP1-NP96.
21. Crowson CS, Gabriel SE. Towards improving cardiovascular risk management in patients with rheumatoid arthritis: the need for accurate risk assessment. Ann Rheum Dis 2011;70:719–21.
22. Van Sijl AM, Peters MJ, Knol DK, et al. Carotid intima media thickness in rheumatoid arthritis as compared to control subjects: a meta-analysis. Semin Arthritis Rheum 2011;40:389–397
23. Zavodni AE, Wasserman BA, McClelland RL et al., Carotid artery plaque morphology and composition in relation to incident cardiovascular events: the Multi-Ethnic Study of Atherosclerosis

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
31
(MESA). Radiology. 2014;271(2):381-389.
24. Skilton MR, Boussel L, Bonnet F, et al., Carotid intima-media and adventitial thickening: comparison of new and established ultrasound and magnetic resonance imaging techniques. Atherosclerosis. 2011;215(2):405–10.
25. Ahmed A, Hollan I, Curran SA et al., Brief report: Proatherogenic Cytokine Microenvironment in the aortic adventitia of patients with rheumatoid arthritis. Arthritis Rheumatol. 2016;68(6):1361–6.
26. Kerwin WS, Hooker A, Spilker M, et al., Quantitative magnetic resonance imaging analysis of neovasculature volume in carotid atherosclerotic plaque. Circulation. 2003;107(6), 851–6.
27. Kerwin WS, O’Brien KD, Ferquson MS, Polissar N, Hatsukami TS, Yuan C, Inflammation in carotid atherosclerotic plaque: a dynamic contrast-enhanced MR imaging study. Radiology. 2006;241(2), 459–68.
28. Rudd JHF, Warburton EA, Fryer TD, et al. Imaging Atherosclerotic plaque inflammation with [¹⁸F]-fluorodeoxyglucose positron emission tomography. Circulation. 2002; 105: 2708–2711.
29. Davies JR, Rudd JH, Fryer TD et al. Identification of culprit lesions after transient ischemic attack by combined 18F fluorodeoxyglucose positron-emission tomography and high-resolution magnetic resonance imaging. Stroke.2005;36(12), 2642–7.
30. Irkle A, Vesey AT, Lewis DY, et al. Identifying active vascular microcalcification by 18F-sodium fluoride positron emission tomography. Nat. Commun. 2015;6:7495.
31. Giles JT, Fernandes V, Lima JA, Bathon JM. Myocardial dysfunction in rheumatoid arthritis: epidemiology and pathogenesis. Arthritis Res Ther. 2005;7:195–207.
32. Khalid U, Egeberg A, Ahlehoff, O et al, Incident Heart Failure in Patients With Rheumatoid Arthritis: A Nationwide Cohort Study. Journal of American Heart Association, 2018;7. pii:e007227.
33. Atzeni F, Corda M, Gianturco L, Porcu M, Sarzi-Puttini P, Turiel M, Cardiovascular Imaging Techniques in Systemic Rheumatic Diseases. Frontiers in Medicine, 2018;5:26.
34. Rexhepaj N, Bajraktari G, Berisha I, et al, Left and right ventricular diastolic functions in patients with rheumatoid arthritis without clinically evident cardiovascular disease. Int J Clin Pract. 2006;60:683–688.
35. Caiati C, Zedda N, Montaldo C, Montisci R, Iliceto S, Contrast-enhanced transthoracic second harmonic echo Doppler with adenosine: a noninvasive, rapid and effective method for coronary flow reserve assessment. J Am Coll Cardiol. 1999;34:122–130.
36. Hozumi T, Yoshida K, Ogata Y, et al., Noninvasive assessment of significant left anterior descending coronary artery stenosis by coronary flow velocity reserve with transthoracic color Doppler echocardiography. Circulation. 1998;97:1557–1562.
37. Dimitrow PP, Transthoracic Doppler echocardiography – noninvasive diagnostic window for coronary flow reserve assessment. Cardiovasc Ultrasound. 2003; 1:4.
38. Rigo F, Gherardi S, Galderisi M, et al. The prognostic impact of coronary flow-reserve assessed by Doppler echocardiography in non-ischaemic dilated cardiomyopathy. Eur Heart J. 2006;27:1319–1323.
39. Guedes C, Bianchi-Fior P, Cormier B, Barthelemy B, Rat AC, Boissier MC. Cardiac manifestations of rheumatoid arthritis: a case-control transesophageal echocardiography study in 30 patients. Arthritis Rheum. 2001;45(2):129-35
40. Tinggaard AB, Thurah A, Andersen IT et al, Increased Prevalence and Severity of Coronary Artery Disease in Patients with Chest Pain and Seropositive Rheumatoid Arthritis: an analysis from a large-scale population cohort referred for cardiac computed tomography. Ann Rheum Dis, 2019; 78: 1124.
41. Giles JT, Malayeri AA, Fernandes V, et al. Left ventricular structure and function by cardiac magnetic resonance imaging in Rheumatoid Arthritis. Arthritis Rheum. 2010, 62:940–51.
42. Kobayashi Y, Giles JT, Hirano M, et al. Assessment of myocardial abnormalities in rheumatoid arthritis using a comprehensive cardiac magnetic resonance approach: a pilot study. Arthritis Res Ther. 2010.12:R171.

32
Article received on April 15, 2019 and accepted for publishing on August 23, 2019. ORIGINAL ARTICLES
Managing radial nerve injuries associated with humeral fracture
V. Cărbunaru, Alexandra Ciotei, Mihaela I. Zaharia
Abstract: : The overall prevalence of radial nerve injury after humeral shaft fractures is up to 18% representing the most common peripheral nerve injury associated with long bone fractures.Spiral or oblique fractures of the junction between the middle and distal third of the humeral shaft are at greater risk for radial nerve injury. Iatrogenic damage to the radial nerve may also occur during manipulations of closed reduction.
Material and methods: A prospective study between 2017-2019 following 5 patients (all male, with ages between 30 and 56 years old), who were treated at our clinic for complete radial nerve palsy after a high-energy fracture of the humerus Results: All the patients were followed-up for a mean of 6 months (range 4 - 15 months) post op. The first 3 cases showed the initial signs of recovery 4 weeks after the operation. In the last 2 cases, a palliative radial intervention was required. Conclusions: The consequences of the radial nerve palsy associated with humeral fractures is strongly related to trauma mechanism. In high-energy fractures, severe contusion or transection of the nerve must be expected. In this case, nerve recovery is unlikely and the patients should be informed of the poor prognosis and the need of tendon transfers.
Keywords: humeral fracture, compression, upper limb, radial nerve, callus
INTRODUCTION
Fractures of the humerus are often complicated with radial nerve palsy. The overall prevalence of radial nerve injury after humeral shaft fractures is up to 18% representing the most common peripheral nerve injury associated with long bone fractures.[1-5] This is caused by the relatively fixed position of the radial nerve and the direct contact with the periosteum of the humerus as the nerve courses through the middle and distal thirds of the upper arm and by the nerve’s diminished mobility where it pierces the lateral intermuscular septum. As such, at this level the bone ends can easily entrap, contuse, or even lacerate the radial nerve, varying from neurapraxias to complete neurotmesis.
Spiral or oblique fractures of the junction between the middle and distal third of the *humeral shaft are at greater risk for radial nerve injury.[6] Iatrogenic damage to the radial nerve may also occur during manipulations of closed reduction or at the time of surgical intervention, during
internal fixation with a intramedullary nailing or compression plate.[7, 8, 9]
Treatment is often expectant (non-operative), though surgery is also sometimes necessary by a variety of often imaginative procedures. Because radial nerve injuries are the least debilitating of the upper limb nerve injuries, results are usually satisfactory.[10]
PATIENTS AND METHODS
A prospective study between 2017-2019 following five patients (all male, with ages between 30 and 56 years old), who were treated at our institution for complete radial nerve palsy after a high-energy fracture of the humerus. In all cases, the fracture was stabilized and no other complications except the radial palsy. Baseline electrophysiological studies (i.e. nerve conduction velocity studies and electromyography) conducted before admittance showed a complete motor paralysis of the nerve

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
33
and all had an absent Tinel’s sign at each clinical examination.
Operative Procedure
Case 1: A 41-year-old male, with a 4 months old high-energy transverse diaphyseal fracture of the left humerus and faulty soft tissues following a car accident was treated with plating.
The same anterolateral approach used for plating was used during our surgical exploration where we found contusion of the radial nerve and perineurial adhesions of a small segment at the level of the humeral fracture (Figure 1).
Figure 1: Perineural adhesion of the radial nerve to the humerus
External neurolysis was practiced (Figure 2).
Figure 2: Neurolysis of the radial nerve
Case 2: A 38-year-old male, with 3 months old closed fracture of the right humeral shaft following a recreational arm wrestling match was treated with two non-staggered plates.
Upon surgical exploration via dorsal approach, a partially lacerated nerve draped over a loose compression plate.
Treatment associated the refixation of the plate and embedment of the nerve in the triceps muscle.
Case 3: A 40-year-old male, with a 3-month-old fracture of the humeral shaft following a car crush was treated with external fixator.
During surgical exploration, the distal pin of the external fixator was found to run through the brachioradial muscle into the body of the radial nerve destroying 15% of its circumference (Figures 3 and 4).
Figure 3: Distal pin winded up in the radial nerve
Figure 4: Radial nerve buried in the fracture callus
The pin was removed and reattached after releasing the nerve and embedding it in the triceps muscle.
Case 4: A 56-year-old male with a six-month-old fracture of the left humeral shaft was treated with internal fixation after crush in the conveyor belt.
Surgical exploration had a posterior approach through a lateral para-tricipital window revealing the nerve enveloped

34
in the fracture callus more than 8 cm with the impossibility of finding the proximal end (Figure 5).
Figure 5: Presenting the donor tendons. From left to right: palmaris longus, flexor superficialis middle finger and flexor ulnaris carpi
A follow-up tendon transfer procedure was carried out flexor ulnaris carpi to extensor ulnaris carpi, flexor superficialis of middle finger to extensor digitorum communis, palmaris longus to extensor pollici longus (Figures 6 and 7).
Figure 6: Tenoplasty of the extensor digitorum communis and extensor pollici longus by Pulvertaft technique
Figure 7: Active extension of the wrist, thumb and fingers 6 weeks post op
Case 5: A 30-year-old male, with a 12-month-old chainsaw trauma, which required open reduction and fixation of the humerus, anastomoses of the brachial artery with venous grafting and neurorrhaphy of median nerve and ulnar nerve, with the impossibility of finding the radial nerve ends, presented for second intervention in our clinic.
A palliative radial intervention practicing tendon transfer was used.
We transferred the pronator teres tendon to extensor carpi radialis tendon, flexor carpi radialis tendon to extensor digitorum communis and plamaris longus to extensor pollicis longus (Figures 8 and 9).
Figure 8: Presenting the donor tendons. From left to right: pronator teres, flexor radialis carpi and palmaris longus

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
35
Figure 9: Tenoplasty of the extensor carpi radialis (over the scissors tip), extensor digitorum communis (forceps) by Pulvertaft
technique
Postoperative follow-up examination included radiographic evaluation of the fracture, physical examination (i.e. Tinel’s sign), and monthly electrophysiological studies for motor and sensory nerve recovery.
RESULTS
All the patients were followed-up for a mean of 6 months (range 4-15 months) post op. The first three cases showed the initial signs of recovery 4 weeks after the operation. Full nerve recovery was achieved in a mean of 19 weeks (range 16-22 weeks) with a slight sensory discomfort in the third case. An advancing Tinel’s sign was a good predictor for nerve recovery.
In the last two cases where palliative radial intervention practicing tendon transfer was used, the imobilization was removed after approximately 4 weeks and a volar custom splint made by a hand therapist was applied with extension slings for the MP joint of the fingers. Active range-of-motion exercises of the fingers were begun at 3 to 4 weeks, and the wrist at 6 weeks.
Splinting as protection yielded excellent results and was done for 8 to 12 weeks postoperatively.
DISCUSSIONS
These cases highlights the necessity of a postreduction examination of the fracture. Nerve function should always be thoroughly assessed before and after reduction, with complete documentation in the medical record. To ensure accuracy, any patient who requires conscious sedation for reduction must return to full consciousness and alertness before obtaining the postreduction exam.
Radial nerve injury associated with a humeral shaft fracture
is a very important injury pattern among trauma patients with an incidence up to 18%. [3] These injuries can be either primary or secondary depending on the timing of the palsy presentation. Early surgical exploration of the nerve is generally indicated for those cases, in which there was an open fracture, fractures that cannot achieve an adequate closed reduction requiring open reduction, fractures associating a vascular injury or a severe soft tissue injury [11].
Patients who demonstrate a primary radial nerve palsy have a reported spontaneous recovery rate of over 70% [12]. In the management of nerve palsy, nerve conduction examination with electrophysiological studies could be obtained at three months post injury, as motor potential should be recovered by this point, and these nerve conduction data will enable the clinician to determine if the injury should require surgical intervention. Early exploration revealing a nerve injury that can be repaired can lead to a quicker return to function and better nerve recovery. Degeneration of the motor endplate and irreversible muscle atrophy occurs if sufficient reinnervation is not present within 12–18 months after injury. [13] Poor functional recovery has been demonstrated in experimental studies when nerve repair is delayed for 6 months due to decreased motor neuron regeneration capacity. [14, 15]
Tendon transfer remains an essential technique in irreparable or long-standing radial nerve palsies for hand function restoration. Because the first signs of nerve recovery can be quite delayed, patience is merited before considering tendon transfers. A waiting period of 12 months is usually sufficient to see any evidence of nerve regeneration. Following a radial nerve injury, the extrinsic extensor function of the hand and wrist is lost, resulting in an inability to extend the fingers and wrist. It affects grip strength and has a large influence on thumb usage. Tendon transfer surgery must restore wrist, thumb and finger function without inflicting other motor deficits on the hand. [15] It is important that the joints have achieved good passive mobility in order to achieve optimal function post-tendon transposition. The donor muscles are tested for strength before surgery, and must come from a region unaffected by the pathology. [16]
Modern medicine sheds light on biological therapies and nerve regeneration. Research is being conducted with pluripotent stem cells and nerve conduits with promising developments using human amniotic membranes loaded with human umbilical cord mesenchymal stem cells in radial nerve repair. [17]

36
References:
1. Pollock FH, Drake D, Bovill EG, Day L, Trafton PG. Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg 1981;63:239–43.
2. Amillo S, Barrios RH, Martinez-Peric R, Losada JI. Surgical treatment of the radial nerve lesions associated with fractures of the humerus. J Orthop Trauma 1993;7:211–5.
3. Ekholm R, Adami J, Tidermark J, et al. Fractures of the shaft of the humerus. An epidemiological study of 401 fractures. J Bone Joint Surg Br 2006;88(11): 1469–73.
4. Bostman O, Bakalim G, Vainionpaa S, Wilppula E, Patiala H, Rokkanen P. Radial palsy in shaft fracture of the humerus. Acta Orthop Scand 1986;57(4):316–319.
5. Duncan DM, Johnson KA, Monkman GR. Fracture of the humerus and radial nerve palsy. Minn Med 1974;57(8):659– 662.
6. Shao YC, Harwood P, Grotz MRW, Limb D, Giannoudis PV. Radial nerve palsy associated with fractures of the shaft of the humerus. A systematic review. J Bone Joint Surg Brit Vol 2005;87:1647–52
7. Farragos A, Schemitsch E, McKee M. Complications of intramedullary nailing for fractures of the humeral shaft: a review. J Orthop Trauma 1999;13:258–67.
8. Bell M, Beauchamp C, McMurty R. The results of plating humeral shaft fractures in patients with multiple injuries. J Bone Joint Surg Brit Vol 1985;67:293–6.
9. Dabezies EJ, Banta CJ 2nd, Murphy CP, D’Ambrosia RD. Plate fixation of the humeral shaft for acute fractures, with and without radial nerve injuries. J Orthop Trauma 1992;6: 10–13.
10. Holstein A, Lewis GM. Fractures of the humerus with radial nerve paralysis. J Bone Joint Surg 1963;45:1382–8.
11. Packer JW, Foster RR, Garcia A, Grantham SA. The humeral fracture with radial nerve palsy: is exploration warranted? Clin
Orthop Relat Res 1972;88:34–38.
12. Bumbasirevic´ M, Lesic´ A, Bumbasirevic´ V, Cobeljic´ G, Milosevic´ I, Atkinson HD. The management of humeral shaft fractures with associated radial nerve palsy: a review of 117 cases. Arch Orthop Trauma Surg 2010;130:519–22.
13. Lowe J, Sen S, Mackinnon S. Current approach to radial nerve paralysis. Plastic Reconstr Surg 2002;110:1099–112
14. Fu SY, Gordon T. Contributing factors to poor functional recovery after delayed nerve repair: prolonged denervation. J Neurosci 1995;15:3886–95.
15. Smith RJ. Tendon transfers to restore wrist and digit extensions. In: Tendon transfers of the hand and forearm. Boston: Little, Brown; 1987:35-56.
16. Kozin SH. Tendon transfers for radial and median nerve palsies. J Hand Ther 2005;18:208-215.
17. Li Z, Qin H, Feng Z, et al. Human umbilical cord mesenchymal stem cell-loaded amniotic membrane for the repair of radial nerve injury. Neural Regen Res 2013;8:3441-3448.
18. A. M. Oproiu, I. Lascar, C. Moldovan, O. Dontu, M. Pantazica, C. Mihaila, C. Florea, L. Dobrescu, I. Sebe, R. Scarlet, D. Dobrescu, T.Neagu, O. Ionescu, I. C. Stoica and A. Edu, Peripheral Nerve WIFI Interfaces and Electrodes for Mechatronic Prosthetic Hand, ROMJIST, Volume 21, Number 2, 2018, pp. 129–138
19. Oproiu, A.M., Lascar, I., Dontu, O., Florea, C., Scarlet, R., Sebe, I., Dobrescu, L., Moldovan, C., Niculae, C., Cergan, R., Besnea, D., Cismas, S., David, D., Muraru, D., Neagu, T., Pogarasteanu, M.E., Stoica, C., Edu, A., Ifrim, C.F., Topography of the Human Ulnar Nerve for Mounting a Neuro-Prosthesis with Sensory Feedback, Rev. Chim. (Bucharest), 69, no. 9, 2018, p. 2494- 249.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
37
Article received on July 23, 2019 and accepted for publishing on December 13, 2019. ORIGINAL ARTICLES
Intraoperative parathyroid hormone assay in patients with primary hyperparathyroidism
Cornelia Nitipir1, Lucian Alecu2, Iulian Slavu3, Madalina Musat4, Raluca Tulin2, Bogdan Socea5, Adrian Tulin2
Abstract: Introduction: Currently, parathyroidectomy represents the elective surgical treatment and the only one curative that relieves the patient of metabolic complications and improves the quality of life of the patient. Intraoperative confirmation of PTH is required to reflect the fact that the correct parathyroid gland has been extracted. Material and method: The study is retrospective. The period on which the data was gathered over a period of 2 years. The values of the PTH assay were obtained from blood drawn from the ipsilateral cephalic vein of the hyperproductive parathyroid gland: 1. at the moment of anesthesia induction; 2. at identification; 3. at 10 minutes after the extraction; 4. at 20 minutes after extraction. Results: We identified a number of 25 patients operated for primary hyperparathyroidism. Preoperative values of PTH were 380pg/mL with a maximum value of 821 pg/mL. PTH values decreased by 55% at 5 min, 68% at 10 minutes and 74% at 15 minutes. A marked reduction in PTH values occurred after the first 5 minutes while the interval between 10-15minutes associated a variation of only 8-10% decrease. Conclusion: Intraoperative PTH assay is a useful technique to predict the success of the intervention. The technique is standard although some issues have been raised and are still under discussion.
Keywords: PTH, hyperparathyroidism
INTRODUCTION
The first reported intraoperative dosage of the parathormone or PTH was reported in 1988 by Nassaum et al. [1] The level and the extension of the cervical dissection in patients with primary hyperparathyroidism is still under discussion. In the absence of any preoperative imagistic or laboratory investigations and using only the intraoperative exploration of the parathyroid glands Satava et al. confirmed a rate of succes up to 96% in identifying and extracting the correct parathyroid gland responsible of primary hyperparathyroidism [2].
However, this technique has its limitations which can lead to surgical failure if one encounters a case of multiglandular hyperplasia, multiple parathyroid adenomatous nodules or
hyperfunctional parathyroid ectopic tissue.
Primary hyperparathyroidism is an endocrinological disorder commonly found to be produced in 87% of cases by a single adenoma [3, 4]. Hyperparathyroidism associated with the presence of two hyperfunctional adenomas associates an incidence of up to 15% [3, 4].
Currently, parathyroidectomy represents the elective surgical treatment and the only one curative that relieves the patient of metabolic complications and increases the quality of life. To achieve this goal, a minimally invasive
1 Elias Emergency Clinical Hospital, Bucharest, Romania 2 General Surgery Clinic, Agrippa Ionescu Emergency Clinical Hospital, Bucharest, Romania 3 General Surgery Clinic, Emergency Clinical Hospital, Bucharest, Romania 4 C.I. Parhon Endocrinology Institute, Bucharest, Romania 5 St. Pantelimon Emergency Clinical Hospital, Bucharest, Romania
Corresponding author: Alecu Lucian [email protected]

38
surgical procedure, aimed at a single parathyroid gland that houses the hyperfunctional nodule, is now successfully used, thus replacing bilateral exploratory cervical dissections. This procedure was quickly adopted due to the effectiveness of paraclinical investigations in the field of scintigraphy that allow the exact identification of the parathyroid adenoma during the preoperative evaluation [5].
However, an intraoperative confirmation is required to reflect the fact that the correct parathyroid gland has been extracted. In this regard, the intraoperative PTH dosage is used which due to the reduced half-life of 2-5 minutes coupled with a 50% reduction of the circulating intraoperative values compared to the preoperative values confirms the correctness of the procedure or the opens up the possibility to a cervical exploration to identify other parathyroid glands or parathyroid ectopic tissue [6].
The current protocol involves 4 dosages of PTH: at the time of induction of anesthesia (which will be used as a threshold value) at the moment of identification, at 10 and 15 minutes after the gland has been extracted. Success rates when this technique is used can reach 94% [7].
However, literature has begun to bring into discussion the efficacy of PTH evaluation when multinodular hyperplasia is encountered and the cost-effectiveness of the technique [8].
The study represents a retrospective evaluation of the effectiveness of this technique incorrectly identifying the hyperfunctional parathyroid gland in patients operated in our clinic for primary hyperparathyroidism by a minimally invasive technique.
MATERIAL AND METHODS
The study is retrospective. The period on which the data was gathered over a period of 2 years (01.01.2017-01.01.2019). Data were obtained from the clinic of general surgery of the Clinical Emergency Hospital “Prof. Dr. Agrippa Ionescu,” Bucharest, Romania. The following variables were obtained: age, sex, preoperative values of PTH, intraoperative PTH values, postoperative complications, preoperative scintigraphy, surgery time, and length of hospital stay.
The patients were operated using the standard technique of minimally invasive parathyroidectomy.
PTH values were obtained from blood drawn from the ipsilateral cephalic vein of the hyperproductive parathyroid gland: 1. at the moment of anesthesia induction; 2. at identification; 3. at 10 minutes after the extraction; 4. at 20 minutes after extraction.
Laboratory PTH values were obtained using the Radioimmunoassay method.
Inclusion Criteria: Diagnosis of primary hyperparathyroidism and surgery for primary hyperparathyroidism.
Ethics: The retrospective analysis of the data has been approved by an Ethics Committee of the institution.
RESULTS
We identified 25 patients, which were operated for primary hyperparathyroidism with a minimally invasive technique on which intraoperative PTH hormone assay was done (Figure 1).
Figure 1: Right parathyroid adenoma operated with a minimally invasive technique – the incision had a length of 5 cm and was
focused on the parathyroid gland. The adenoma is clearly visible.
The average age at diagnosis was 54 years with a range of 32-68 years.
The study group was composed of 16 women and 9 men.
A number of 20 patients were diagnosed with singular parathyroid adenoma while multiple glandular adenomas were identified in five patients.
There were no mortalities reported in the studied group. There were no recurrent nerve lesions.
All of the patients were investigated before surgery with Tc 99m Scintigraphy to identify the location of the

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
39
hyperproductive parathyroid gland. Only three cases did not correctly associate the preoperative scintigraphy with intraoperative exploration.
The average hospital stay was 2.3 days while a number of 8 patients were discharged on day 1 after surgery.
All of the patients were operated under general anesthesia.
Average preoperative values of PTH were 380pg/mL with a maximum value of 821 pg/mL.
The mean value (SD) for LVEDV was 144.37 (69.2) ml by 2DE and 143.6 (67.2) ml by 3DE, p=0.8, Spearman’s coefficient 0.86. For LVESV the mean value (SD) was 106.26 (59.53) ml by 2DE, 103.24 (55.02) ml by 3DE, p=0.051, Spearman’s coefficient 0.85 (Figure 2).
Figure 2: Decrease of intraoperative PTH values after parathyroidectomy at 5 minutes, 10 minutes and 15 minutes
Average PTH values decreased by 55% at 5 min, 68% at 10 minutes and 74% at 15 minutes.
From the above graph, we can observe that a marked reduction in PTH values occurred after the first 5 minutes while the interval between 10-15 minutes associated a variation of only 8-10% decrease of PTH values.
There were no extended lateral cervical dissections done.
Two cases required local explorations by lifting and exploring the posterior region of the thyroid gland. In these cases, the PTH values decreased by 10% in one case at 20 minutes and the other they did not change.
DISCUSSIONS
The methods/techniques one uses to locate the parathyroid gland responsible for hyperparathyroidism has long been a topic of debate. Some surgeons advocate for preoperative investigations such as scintigraphy or cervical ultrasonography while others have fought for bilateral cervical exploration as a standard technique.
Today in order to identify the parathyroid gland, the scintigraphic examination is recognized as the gold standard, while other imaging solutions such as cervical ultrasound allow for a complete examination. Computer tomography and Magnetic Resonance Imaging are widely used to explore the suprarenal gland [9].
Ultrasound and scintigraphy are synergistic. When used together, they achieve a 95% sensitivity in identifying the hyperproductive parathyroid gland [10].
All of these investigations allow for a minimal-invasive targeted approach that translates into reduced hospitalization time, offer the possibility to use local anesthesia and ambulatory surgery, reduced operative time and low failure rates of only 1.5% [11, 12]. All of these advantages have led to a global reduction in costs [11, 12].
Surgical extraction of the parathyroid gland responsible for primary hyperparathyroidism produces a decrease in circulating PTH values thus confirming in real time the success of surgery or indicates towards a rapid change of tactics with the patient still on the operating table and under anesthesia. Failure of primary hyperparathyroidism surgery is largely related to correctly identify the parathyroid gland as it can be confused with lymphatic tissue or thyroid tissue [13].
Another cause of failure is multinodular hyper-parathyroidism, which, in the absence of advanced diagnostic techniques, will force the operator to do a cervical exploration – to identify at least four thyroid glands, extraction of the macroscopically affected glands and to wait for the extemporaneous investigation. This technique associates increased comorbidities and a significant increase in operative time. In literature, so-called false-negative results in intraoperative PTH assay were reported which were due to increased PTH values after extraction of the gland or a delay of up to 30 minutes until the values were reduced. These are mainly due to manipulation of the parathyroid tissue at dissection [14].
No such cases have been encountered in the studied group.

40
In these situations, the extemporaneous examination of the resected parathyroid gland is of real use. Good communication with the anatomopathological and the laboratory physician is mandatory in order to establish the optimal therapeutic course.
Intraoperative PTH assay has seen its share of discussions. We used this technique with great success and it has proven to be effective in the majority of our surgical interventions. The reproaches are of economical nature, cost-effectiveness and the half-life of PTH, which seems to differ in cases of a single parathyroid adenoma and multiglandular parathyroid hyperplasia. Other issues raised are related to the technique: intraoperative time of PTH harvesting and the PTH value set as the baseline to which a reduction of more than 50% after extraction of the gland is considered effective [15].
Therefore, some authors recommend as the baseline the PTH values from the preoperative day while other surgeons use the PTH value as baseline obtained at anesthesia induction. On the studied group, we used as the baseline the PTH values obtained before induction although some authors consider this value to be 60% higher than the previous day dosing. Subsequent PTH assays after gland extraction showed a 30-40% drop in values and a reduction in of more than 50% at 15 minutes in the cases of correct parathyroid removal.
In cases of multinodular hyperparathyroidism, the extraction of the parathyroid gland can lead to so-called false-positive. In these cases, one can observe a more than 50% reduction in PTH values from baseline although there is incomplete removal of all the hyperproductive parathyroid tissue [16]. To avoid these situations when there is a suspicion of multiglandular hyperparathyroidism, it has been proposed that one should pursue a more than 70% reduction in PTH
values from the baseline [17]. A reduction of over 70% of intraoperative PTH values to 10 minutes is associated with healing with a sensitivity of 85% and specificity of 100% (18). When multiglandular hyperparathyroidism exists, preoperative investigations imaging investigations in particular scintigraphy allow for a complete evaluation.
As we observed in our studied group, of great importance is the place where the blood is obtained for the PTH assay. It should be obtained from the ipsilateral cephalic vein of the hyperproductive parathyroid gland. Contralateral blood harvesting delays the decrease in PTH values to more than 10 minutes due to the circulatory time of the hormone. Such contradictory values can raise false doubts as to the fairness of the procedure. In order to increase the sensitivity of the PTH assay, one can harvest blood the upper, middle or inferior thyroid veins [19].
Study limits:
However, the study has limits. It was difficult to appreciate the evolution of the disease until surgery. We could not follow-up, in the long run, the effectiveness of the surgical procedure.
In conclusion, although medical treatment in primary hyperparathyroidism has evolved in time, surgery has remained one of the pillars of treatment. Direct PTH evaluation is a useful real-time technique and can predict utility of the surgical procedure. The technique is standard although some issues have been raised and are still under discussion. As demonstrated in our study a reduction of more than 50% of PTH values when compared to baseline at anesthesia induction can predict the success of the intervention in agreement with the literature. Preoperative scintigraphy plays a key role if one decides to use this technique as it can decrease surgery time and hospital stay.
References:
1. Nussbaum, Thompson, Hutcheson, Gaz, Wang. Intraoperative measurement of parathyroid hormone in the surgical management of hyperparathyroidism. Surgery 1988; 104: 1121-1127.
2. Satava, Beahrs, Scholz. Success rate of cervical exploration in hypeparthyroidism. Arch. Surg. 1975; 110:625-628
3. Attie JN, Bock G, Auguste LJ. Multiple parathyroid adenomas: report of thirtythree cases. Surgery. 1990;108(6):1014-1020
4. Bartsch D, Nies C, Hasse C, Willuhn J, Rothmund M. Clinical and surgical aspects of double adenoma in patients with primary hyperparathyroidism. Br J Surg. 1995;82(7):926-929.
5. Mack LA, Pasieka JL. Asymptomatic primary hyper-parathyroidism: a surgical perspective. Surg Clin North Am. 2004;84(3):803-816.
6. Irvin GL III, Solorzano CC, Carneiro DM. Quick intraoperative
parathyroid hormone assay: surgical adjunct to allow limited parathyroidectomy, improve success rate, and predict outcome. World J Surg. 2004;28(12):1287-1292.
7. G. Prager, P. Riss, C. Bieglmayer, B. Niederle, The role of intraoperative quick PTH measurements in primary hyperparathyroidism, Ann. Ital. Chir. 74 (4) (2003) 395e399.
8. G.C. Karakousis, D. Han, R.R. Kelz, et al., Interpretation of intra-operative PTH changes in patients with multi-glandular primary hyperparathyroidism (pHPT), Surgery 142 (6) (2007) 845e850.
9. Bilezikian, J.P.Powell, D.Wells, S.A.Monchik, J.Mallette et al. Preoperative localization of abnormal parathyroid tissue. The American Journal of Medicine , Volume 55 , Issue 4 , 505 - 514
10. D. Hajiott, T. Jyngkaran, C. Panagamuwa, D. Mili, M.P. Stearns, Preoperative localization of parathyroid adenoma: ultrasonography, sestamibi scintigraphy or both? Clin. Otolaringol. 29 (2004) 549.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
41
11. Chen H, Sokoll LJ, Udelsman R. Outpatient minimally invasive parathyroidectomy: a combination of sestamibi – SPECT localization , cervical block anesthesia and intraoperative parahyroid hormone assay. Surgery 1999; 126; 1016-1021
12. Carty SE, Worsey MJ, Virji MA, Brown ML, Watson CG, Concise parathyroidectomy: the impact of preoperative SPECT Tc, sestamibi scanning and intraoperative quick parathormone assay. Surgery. 1997; 122:1107-1116.
13. J.A. Olson, G.S. Leight Jr., Surgical management of secondary hyperparathyroidism, Adv. Ren. Replace. Ther. 9 (2002) 209.
14. Kao PC, Van Heerden JA, Taylor RL. Intraoperative monitoring of parathyroid procedures by a 15-minute parathyroid hormone immunochemiluminometric assay. Mayo Clin Proc. 1994;69:532-537.
15. Irvin, Sfakianakis, Yeung, et al. Ambulatory parathyroidectomy for primary hyperparathyroidism. Arch Surg. 1996; 131: 1074 -1078
16. Gordon LL, Snyder WH, Wians F, Nwariaku F, Kim LT. The validity of quick intraoperative parathyroid hormone assay: an evaluation in seventy-two patients based on gross morphologic criteria. Surgery. 1999;126:1016-1021.
17. D.N. Singh, S.K. Gupta, G. Chand, et al. Intra-operative parathyroid hormone kinetics and influencing factor with high baseline PTH: a prospective study, Clin. Endocrinol. (Oxf) 78 (6) (2013) 935e941.
18. M.C. Gioviale, G. Gambino, C. Maione, et al. Use of monitoring intraoperative parathyroid hormone during parathyroidectomy in patients on waiting list for renal transplantation, Transpl. Proc. 39 (6) (2007) 1775e1778.
19. Saharay M, Farooquie A, Farrow S, Fahie-Wilson, Brown A. Intra-operative parathyroid hormone assay for simplified localization of parathyroid adenomas. J R Soc Med. 1996;89:261-264.

42
Article received on May 15, 2019 and accepted for publishing on September 3, 2019. ORIGINAL ARTICLES
Metformin – old treatment for diabetes, new treatment for psoriasis
Bogdan Serban¹˒², Camelia C. Diaconu¹˒³, Ana Maria A. Stanescu¹, Daniel O. Costache4, Raluca S. Costache1,4, Catalin Cirstoiu¹˒²
Abstract: Metformin was a revelation in the treatment of patients with type 2 diabetes, being widely used, with remarkable outcomes. Lately, research has greatly expanded the indications of metformin treatment, which can be used not only in diabetes but also in many other conditions. Although still debatable, several studies have shown the beneficial effects of metformin treatment in patients with psoriasis. This article is a review of the latest data of scientific literature about the effects of metformin administration in patients with diabetes and psoriasis, but also in nondiabetic patients with psoriasis.
Keywords: metformin, diabetes, psoriasis
INTRODUCTION
Psoriasis is a chronic inflammatory disorder characterized by hyperproliferation and inflammation of keratinocytes. Psoriasis is a complex disorder, both from the standpoint of the disease and from the many associated comorbidities. Obesity, diabetes, metabolic syndrome, arthritis and cardiovascular disease are the most common comorbidities in patients with psoriasis [1, 2, 25]. Pathophysiologically, patients with psoriasis present changes of the tumor necrosis factor alpha and interleukins [6, 8, 12, 17, 19 and 23], highlighting the pathophysiological link with the metabolic syndrome [3]. There is a two-way link between psoriasis and diabetes, patients with psoriasis are at risk of developing diabetes, while patients with diabetes are at risk of developing psoriasis [4, 5].
Numerous therapies are available for the treatment of
psoriasis, from topical to biological. Many of the current therapies for psoriasis are expensive and/or may cause toxicity; new and more accessible therapies with reduced adverse effects are needed.
Metformin, a herbal remedy, was first synthesized in 1922, and subsequently Jean Sterne highlighted the properties of the metformin as Glucophage compound (glucose eater) (6). Metformin is largely used in the treatment of diabetes, being accessible, easy to administer, with few side effects and with potential to decrease the body weight in obese patients. Since 2009, metformin has been recommended by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) in patients with type 2 diabetes as first-line oral therapy [7]. Many studies focused on the potential benefits of metformin administration in patients with diabetes and other conditions.
Although generally well tolerated, metformin has a number of contraindications to administration (Figure 1).
1 Carol Davila University of Medicine and Pharmacy, Bucharest, Romania 2 Emergency University Hospital Bucharest, Bucharest, Romania 3 Clinical Emergency Hospital of Bucharest, Bucharest, Romania 4 Carol Davila University Central Emergency Military Hospital, Bucharest, Romania
Corresponding author: Camelia C. Diaconu, Raluca S. Costache [email protected]; [email protected]

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
43
Figure 1: Contraindications to metformin administration
METFORMIN IN THE TREATMENT OF DIABETES
Metformin is widely used for the treatment of type 2 diabetes. It is a first-line treatment as monotherapy or can be used as a combination therapy when monotherapy is no longer effective; insulin (regardless of the number of insulin injections/day) can be combined with a sulphonylurea, incretin or flozin [8]. In addition to the potential of lowering high blood glucose, metformin has a favorable effect on body weight, a very important aspect in diabetic patients.
Metformin does not cause hypoglycemia, because it does not stimulate the insulin secretion by the beta cells of the pancreas, the effect of lowering the serum glucose is due to inhibition of hepatic glucose production and sensitization of peripheral tissue to the effect of insulin.
Kirpichnikov et al emphasized the ability of metformin to reduce hemoglobin A1c by 1.3% - 2%, and may have a higher degree of reduction in patients with higher blood glucose levels during pre-treatment [9]. Although lifestyle changes seem to be more effective in the prevention of type 2 diabetes in people at risk, metformin can reduce the progression of diabetes and can be administered from the age of 10 years [10].
Following the administration of metformin in diabetics, in addition to the glucose-lowering effects, an improvement not only in the cardiovascular morbidity and mortality has been noticed, but also in the general health [11]. From the cardiovascular point of view, in patients at risk, the benefit of metformin administration is observed by the reduction of the body stress consequently to lower glucose levels, reducing the risk of myocardial infarction or arrhythmias.
In addition to the administration of metformin in type 2
diabetes, recent studies focused on its administration in type 1 diabetes. Nadeau et al, following the administration of metformin in patients with type 1 diabetes, observed a decrease in insulin dose, an improvement in body mass index and a decrease in waist circumference, especially in women [12]. Libman et al, in their study, have found that HbA1c was not significantly decreased following metformin administration, although the decrease in insulin dose was noted, and the patients complained of gastrointestinal distress [13]. Other observations following metformin administration in type 1 diabetes were improved outcomes of heart failure (regardless of decreased hemoglobin A1c) and decreased androgen levels in women with type 1 diabetes and hyperandrogenism [14, 15].
The benefits of using metformin in pre-diabetes were highlighted by the study of Capitanio et al, who have noticed a reduced risk of type 2 diabetes (by 31%) and a reduction of the body weight by average 2 kg in those who used metformin [16]. People with prediabetes should reduce their body weight and increase their daily physical activity; in addition, metformin can be considered for the prevention of type 2 diabetes in people at risk.
METFORMIN IN THE TREATMENT OF PSORIASIS
Starting from the pathophysiological mechanisms of psoriasis, with hyperproliferation and abnormal differentiation of epidermal keratinocytes, the main method of treatment of psoriasis focuses on inhibiting the excessive proliferation of keratinocytes [17}. HaCaT are cell lines derived from keratinocytes in normal adult skin, and excessive proliferation of these keratinocytes results in psoriatic lesions, with HaCaT cells being used as an in vitro
Contraindications to metformin
administrationPregnancy
Ketoacidosis
Circulatory failure (NYHA III, IV),
myocardial infarction, shock
Kidney failure
Liver failure
Respiratory failure
Severe infection

44
model for the study of anti-psoriasis agents [18].
He et al investigated the effects of metformin on the proliferation of human immortalized keratinocytes. Metformin treatment regulated the level of p-AMPK and p-ERK1/2 in HaCaT cells and significantly inhibited the proliferation of HaCaT cells in vitro, by a mechanism associated with activation of the protein signaling pathway, mitogen-activated kinase [19].
Xuan et al have found differences in the quality of life of patients with psoriasis treated with metformin plus methotrexate, compared with patients treated with methotrexate alone. Combined metformin + methotrexate therapy contributes to a significant improvement in the quality of life of patients with psoriasis [20].
Because many psoriasis patients have also metabolic syndrome, Singh and Bhansali studied the effects of metformin (1000 mg/day) on the metabolic syndrome in psoriatic patients. These authors showed a marked improvement of the metabolic syndrome, following metformin administration, at 52.4%, compared with placebo (metformin versus placebo – OR (95% CI), 5.2 (1.3–20.7), P value 0.019) [21}. The proven efficacy of metformin on the metabolic syndrome is a potential axis for improving psoriasis. Because of metformin administration, 14.3% of patients compared with placebo (10%) had no changes or increases in IL-6 and TNF-α, followed by recurrence of psoriasis within the next 6 months [21].
Brauchli et al estimated a low risk of developing psoriasis (as a new diagnosis) using metformin compared to controls [OR = 0.77 (95% CI - 0.62-0.096)] [22].
Regarding the safety of metformin administration in patients with psoriasis and diabetes, it did not cause increased mortality, did not increase the severity of psoriasis or the rate of hospitalization for any other reason, metformin being safe to administer to patients with psoriasis [23].
Wu et al looked at the risk of developing psoriasis in patients with diabetes depending on the antidiabetic medication; they observed an increased risk of developing psoriasis in people with severe diabetes under insulin treatment, while the risk of developing psoriasis was not associated with metformin [5].
Starting from the cases of lichenoid rash and erythema multiforme that appeared following the administration of oral antihyperglycaemic drugs, we have found in the scientific literature only a case published in 2003 (possibly the first of this type reported), who suggests the occurrence of psoriatic rash following the administration of metformin, which eruption recovered after stopping the drug and reappeared with the reintroduction of the drug [24].
In addition to the proven beneficial effects of metformin on psoriasis, it seems that it has other applications in dermatology. Among the dermatological disorders studied from the point of view of metformin administration are acanthosis nigricans, acne, disorders of increased pigmentation, eruptive xanthomas, suppurative hidradenitis, hirsutism, skin cancer, squamous cell carcinoma, and melanoma.
CONCLUSION
The more extensive the metformin research areas, the more therapeutic applications appear. From the point of view of psoriasis, the use of metformin is safe and beneficial. Further studies are needed to determine the optimal dose of metformin recommended in patients with psoriasis, depending on the associated comorbidities.
Acknowledgement
All the authors have equal contribution.
References:
1. Gelfand JM, Yeung H. Metabolic syndrome in patients with psoriatic disease. J Rheumatol Suppl. 2012; 89:24–28.
2. Armstrong EJ, Harskamp CT, Armstrong AW. Psoriasis and major adverse cardiovascular events: A systematic review and meta-analysis of observational studies. J Am Heart Assoc. 2013; 2(2):e000062.
3. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, Costa F. Diagnosis and management of the metabolic syndrome. An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Executive summary. Cardiol Rev. 2005; 13(1):322–327.
4. Armstrong AW, Harskamp CT, Armstrong EJ. Psoriasis and the risk of diabetes mellitus: a systematic review and meta-analysis. JAMA Dermatol 2013; 149(1):84-91.
5. Wu CY, Shieh JJ, Shen JL, Liu YY, Chang YT, Chen YJ. Association between antidiabetic drugs and psoriasis risk in diabetic patients: results from a nationwide nested case-control study in Taiwan. J Am Acad Dermatol 2015; 72(1):123-130.
6. Pryor R, Cabreiro F. Repurposing metformin: an old drug with new tricks in its binding pockets. Biochem J. 2015; 471(3):307-322.
7. Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, Zinman B. Medical management of hyperglycemia in type

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
45
2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009; 32(1):193-203.
8. Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2012; 55(6):1577–1596.
9. Kirpichnikov D, McFarlane SI, Sowers JR. Metformin: an update. Ann Intern Med. 2002; 137(1):25-33.
10. Diabetes Prevention Program Research Group. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015; 3(11):866‐875.
11. Brufani C, Fintini D, Nobili V, Patera PI, Cappa M, Brufani M. Use of metformin in pediatric age. Pediatr Diabetes. 2011; 12(6):580-588.
12. Nadeau KJ, Chow K, Alam S, Lindquist K, Campbell S, McFann K, Klingensmith G, Walravens P. Effects of low dose metformin in adolescents with type I diabetes mellitus: a randomized, double-blinded placebo-controlled study. Pediatr Diabetes. 2015; 16(3):196-203.
13. Libman IM, Miller KM, DiMeglio LA, Bethin KE, Katz ML, Shah A, Simmons JH, Haller MJ, Raman S, Tamborlane WV, Coffey JK, Saenz AM, Beck RW, Nadeau KJ. Effect of metformin added to insulin on glycemic control among overweight/obese adolescents with type 1 diabetes: a randomized clinical trial. JAMA. 2015; 314(21):2241-2250.
14. Bacha F, Klinepeter Bartz S. Insulin resistance, role of metformin and other non-insulin therapies in pediatric type 1 diabetes. Pediatr Diabetes. 2016; 17(8):545-558.
15. Evans JM, Doney AS, AlZadjali MA, Ogston SA, Petrie JR, Morris AD, Struthers AD, Wong AK, Lang CC. Effect of Metformin on mortality in patients with heart failure and type 2 diabetes mellitus. Am J Cardiol. 2010; 106(7):1006-1010.
16. Capitanio S, Marini C, Sambuceti G, Morbelli S. Metformin and
cancer: Tech-nical and clinical implications for FDG-PET imaging. World J Radiol. 2015; 7(3):57–60.
17. Rahman M, Alam K, Ahmad MZ, Gupta G, Afzal M, Akhter S, Kazmi I, Jyoti, Ahmad FJ, Anwar F. Classical to current approach for treatment of psoriasis: a review. Endocr Metab Immune Disord Drug Targets. 2012; 12(3):287–302.
18. Stein M, Bernd A, Ramirez-Bosca A, Kippenberger S, Holzmann H. Measurement of anti-inflammatory effects of glucocorticoids on human keratinocytes in vitro. Comparison of normal human keratinocytes with the keratinocyte cell line HaCaT. Arzneimittelforschung. 1997; 47:1266–1270.
19. Li W, Ma W, Zhong H, Liu W, Sun Q. Metformin inhibits proliferation of human keratinocytes through a mechanism associated with activation of the MAPK signaling pathway. Exp Ther Med. 2014; 7(2):389–392.
20. Xuan THT, Thi VB, Ngoc AT, Van ED, Dang QT, Van TN, Minh PPT, Thi LP, Huu ND, Gandolfi M, Satolli F, Feliciani C, Tirant M, Vojvodic A, Lotti T. Quality of life in psoriasis vietnamese patients treated with metformin in combination with methotrexate. Open Access Maced J Med Sci. 2019;7(2):302–303.
21. Singh S, Bhansali A. Randomized placebo control study of insulin sensitizers (metformin and pioglitazone) in psoriasis patients with metabolic syndrome (topical treatment cohort). BMC Dermatol. 2016; 16(1):12.
22. Brauchli YB, Jick SS, Curtin F, Meier CR. Association between use of thiazolidinediones or other oral antidiabetics and psoriasis: A population based case-control study. J Am Acad Dermatol. 2008; 58(3):421–429.
23. Yu-Jih Su, Tien-Hsing Chen, Chung-Yuan Hsu, Wen-Tsen Chiu, Yu-Sheng Lin, Ching-Chi Chi. Safety of metformin in psoriasis patients with diabetes mellitus: a 17-year population-based real-world cohort study. The Journal of Clinical Endocrinology & Metabolism. 2019; 104(8):3279–3286.
24. Koca R, Altinyazar HC, Yenidünya S, Tekin NS. Psoriasiform drug eruption due to metformin hydrochloride: A case report. Dermatology Online Journal. 2019; 9(3):11.
25. Georgescu M, Poenaru M, Țoropoc I, Costache DO, Morariu SH, Richea L, Badea MA, Țiplica GS Lipid profile and comorbidities in patients with psoriasis vulgaris, Rom J Mil Med 2017; CXX(1): 34-42

46
Article received on April 9, 2019 and accepted for publishing on September 23, 2019. CLINICAL PRACTICE
Improving the outcomes for pregnancies in the context of kidney disease
Mona Zvâncă1,2, Aida Petca1,2, Oana Baltă2, Mihaela Boț1,2, Claudia Mehedințu1,3, Nicoleta Măru1, Răzvan Petca1,4
Abstract: Renal disease in pregnancy is a rare pathology, but it raises several problems in terms of normal pregnancy evolution. Among pregnant women with renal injury, the rate of complications such as spontaneous abortion, preeclampsia, hypertension, intrauterine growth restriction, premature birth, fetal and neonatal mortality are much higher. For a good understanding of the pathology and a correct management of pregnant women with renal disease, it is necessary to know the normal pregnancy changes and the differentiation of chronic kidney disease from the acute injuries occurring during pregnancy.
It is useful to ensure counseling prior to conception and to perform all prophylactic measures in order to prevent pregnancy complications and subsequent decline in renal function in all cases of pregnant women with chronic renal insufficiency. Treatment of acute renal failure in pregnancy involves therapy of the underlying condition that caused renal injury, prevention of irreversible kidney injury and pre-vention of maternal and fetal secondary complications. Monitoring carefully this cate-gory of pregnant women, although additional risks strike, often results in favorabl pregnancy evolution.
Keywords: pregnancy, chronic kidney disease, acute renal failure, complications, preeclampsia
INTRODUCTION
Chronic kidney disease (CKD) affects 3% of pregnant women and represents an isolated risk factor for the occurrence of complications such as preeclampsia, arterial hypertension, premature birth and intrauterine growth restriction [1]. Such complications are not the only challenges that women with kidney disorders face during pregnancy, adding the potential teratogenicity of medications and the risk for disease progression. The management of chronic kidney disease in the context of pregnancy has lately become increasingly relevant to the practicing obstetrician, women becoming pregnant at more advanced age. Challenges brought by the presence of an underlying disease in pregnancy, such as
autoimmune disease or diabetes mellitus, raise the necessity of interdisciplinary medical team to ensure satisfying maternal and fetal outcomes. The presence of acute kidney injury in pregnancy is generally declining worldwide, but still remains a significant health concern in developing countries, where pregnancy might be the first time to diagnose the kidney disease or the hypertension. Acute kidney injury affects a very small number of pregnant women and in this case the renal function decreases rapidly. The etiologies of acute kidney failure are diverse and require specific treatment [2-4]. It is critical to understand and evaluate normal physiologic changes in pregnancy in order to establish the proper diagnosis. The most common causes of chronic kidney disease are diabetes mellitus and hypertension [5]. Preconception counseling is required for women known with renal insufficiency, so patients would
1 ”Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 2 Elias Emergency Hospital, Bucharest, Romania 3 Malaxa Clinical Hospital, Bucharest, Romania 4 ”Prof. Dr. Th. Burghele” Clinical Hospital, Bucharest, Romania
Corresponding author: Aida Petca [email protected]

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
47
understand the potential risks of pregnancy and make various changes of the treatment for kidney disease, so the therapeutic agents won’t affect the pregnancy’s normal course [2, 5]. There are cases in which, through serum and urinalysis investigations carried out at the beginning of the pregnancy, patients are diagnosed for the first time with chronic kidney disease [5, 6].
PHYSIOLOGICAL CHANGES OF THE RENAL FUNCTION DURING PREGNANCY
The pregnancy changes in the renal and urinary tract are both anatomical and functional [2, 7]. Anatomically, the renal volume increases up to 30 %, attributed to the expansion of kidney vascular and interstitial volume, by approximately 1-1.5 cm, predominantly at the level of the collector system. A certain degree of ureteral and renal pelvis dilation occurs, mainly secondary to progesterone-induced relaxation of the muscular layers and due to mechanical compression on the ureters themselves [2, 8]. In almost 86% of pregnant women is a right-sided preponderance of hydronephrosis, attributed to the right ureter peculiar anatomy, crossing over the iliac and ovarian vessels at an angle before entering the pelvis, while the left ureter passes at less acute angle and travels in parallel with the ovarian vein [9]. As a result, these changes should not be interpreted as hydronephrosis during an ultrasound [2, 10].
From a functional point of view, during pregnancy, blood volume increases by up to 50%, systemic vascular resistance decreases, cardiac rate increases by up to 30%, blood pressure decreases in the first two trimesters, with a compensatory increase in heart rate, and returns to the values before the pregnancy in the third trimester. [5, 11, 12]. These cardiovascular changes lead to increased renal blood flow by up to 50%, increased filtration rate up to 30%, and serum creatinine levels decrease up to 20%.
PREGNANCY AND CHRONIC KIDNEY DISEASE
Chronic kidney disease is a pathophysiological process that ultimately results in end-stage renal disease through a progressive loss of nephron number and function that persist 3 or more months [5]. It affects up to 6% of women of childbearing age and is estimated to be associated in 3% of pregnancies. Although the etiology does not significantly influence the evolution of pregnancy, we underline the most common causes: diabetic nephropathy, chronic focal glomerulonephritis, systemic lupus erythematosus, scleroderma and nodulous periarteritis, chronic pyelonephritis, reflux nephropathy, polycystic kidney disease, chronic nephrolithiasis, post-nephrectomy status and congenital unique kidney [13-17] Women with chronic
kidney disease are frequently impaired to make the renal adaptations needed for a normal course of preg-nancy. These patients often show the inability to increase levels of renal hormones leading to reduced expansion of plasma volume, normochromic normocytic anaemia and vitamin D deficiency [16]. Advanced renal dysfunction with poorly controlled underlying primary renal disease, associating proteinuria, frequently causing hypertension, are all significant risks for adverse maternal, fetal and postpartum renal outcomes. These are the main reasons to plan the pregnancies, whenever is possible, thus achieving the best outcomes, allowing the opportunity to counsel the future parents in advance and to optimize these risks.
Chronic kidney disease in pregnancy is classified according to serum creatinine levels in three categories: • Mild-serum creatinine level < 1.5 mg/dl • Moderate – serum creatinine level 1.5-2.5 mg/dl • Severe – Serum creatinine level > 2.5 mg/dl [18].
Another important marker of renal function in pregnancy is proteinuria/24 h, also being a diagnostic factor for preeclampsia [18].
The pregnancies in patients with mild or moderate renal disease, normotensive, generally evolve favorably, although these patients’ prone higher risks for complications compared to pregnant women with normal renal function. Pregnant women with severe chronic kidney disease are more exposed to complications such as intrauterine growth restriction or premature birth, but these cases are extremely rare, the fertility rate at this stage of the disease being low [1]. Although of great importance, the kidney function is not the only predictive factor for the pregnancy outcome, changes in endothelial function and active systemic disease are more likely to be involved.
It is considered that the pregnancy accelerates more rapidly the renal dysfunction due to proteinuria and hypertension, but there are insufficient data in this matter [1], moreover, several small single centre studies suggested that the rate of progression of renal disease to end stage is unaffected by gestation, despite the known fact that many women experience a temporary decline in renal function during pregnancy, given the pathophysiological effects of hyperfiltration [19].
MATERNAL AND FETAL RISKS
Preeclampsia
The risk of developing preeclampsia for pregnant women with renal disease is significantly higher compared to the general population. In mild renal dysfunction, the risk is 20%,

48
and in the severe one increases up to 60-80%, compared to the 5% risk in the general population [5]. The main fetal risks generated by preeclampsia are the restriction of intrauterine growth and premature birth [14]. A reduction of the risk for preeclampsia by 25% was demonstrated by daily administration during pregnancy of 150 mg of aspirin [5, 20].
Renal function
The decline in renal function rarely occurs in women with mild disease, but the risk for moderate illness is 25% in terms of definitive loss of 25% of renal function [5].
Hypertension
Once placental development is fully achieved, by 16 weeks’ gestation, a 50% rise in plasma volume occurs, and in the vast majority of women blood pressure falls, due to the vasodilator response accompanied by an elevation of the cardiac output, arterial underfilling, subsequent ADH release and the stimulation of the renin-angiotensinogen system. Relaxin may also play a role in this chain of changes, because
it has been linked to ADH secretion and water drinking, while levels are increased during pregnancy. In the third trimester, blood pressure starts to rise, reaching almost the pre-pregnancy values.
Among patients with renal disease, preexisting pregnancy hypertension is common, but during pregnancy it becomes much harder to control, on the one hand, due to the adaptive changes in pregnancy in the second and third trimester [5,10] and on the other hand, by the inability to use therapeutic agents of election, as inhibitors of the conversion enzyme and receptor blockers for angiotensin [5].
To reduce maternal and fetal complications it is necessary to maintain blood pressure below 140/90 mmHg, but an important decrease below 120/70 mmHg was correlated with increased risk of fetal demise [21]. Therapeutic agents that can be used in pregnancy are Methyldopa, Labetalol, Nifedipine, and Hydralazine (Table 1) [1, 5, 10, 22-24].
Table 1: Drugs used in pregnancy for women with kidney diseases, diabetes or kidney transplant
Drug FDA Indication Fetal/neonatal effects Use in pregnancy Teratogenicity
ACE inhibitors/ARB D Hypertension Cardiovascular, central nervous system defects in first trimester,
FGR and neonatal anuria in second and third trimesters, fetal
renal tubular dysplasia, oligohydramnios, perinatal acute
renal failure, and other major congenital anomalies
Stop at conception Yes
Beta-blockers C Hypertension FGR in first trimester Atenolol may cause fetal bradycardia in
the first trimester
Labetolol often used first line Atenolol can be used safely
later in pregnancy
No
Ca channel antagonists – nifedipine, amlodipine
C Hypertension Nimodipine is prohibited Used second line with methyldopa or labetolol
No
Hydralazine C Hypertension
Used for more severe hypertension
Used in combination with methyldopa or beta-blockers
No
Methyl-Dopa B Hypertension Often used first line No
Biguanides – Metformin C Diabetes Administered from first trimester
No
Second generation oral sulfonylurea hypoglycemic agent – Glyburide
B Diabetes Neonatal hypoglycemia higher when compared to insulin
Administered from first trimester
Does not cross the placenta
No
Isophane (NHP) insulin C Diabetes Can cause fetal macrosomia, and due to increased oxygen
requirements is a risk factor for fetal death
First choice long-acting insulin The most natural agent for
hyperglicemia
No
Rapid-acting insulin analogues – Aspart, Lispro
C Diabetes May be preferable to start pre-pregnancy
No
Longer acting insulin anlogues: Detemir,Glargine
C Diabetes Few studies, but encouraging results
No

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
49
Prednisolone/IV methylprednisolone
C Kidney transplantation
Rare – except at large doses (cataract, adrenal insufficiency
and infection) Increased frequency of premature rupture of
membranes
maternal side effects: glucose intolerance, hypertesion,
weight gain, hirsutism, acne, cushingoid features, impaired wound healing, osteoporosis,
mood changes
Possible increase in oral
clefts and mental
retardation
Azathioprine – Imuran D Kidney transplantation
Maternal increased risk of infection and neoplasia.
Crosses the placenta as an inactive form. No congenital abnormalities
have been observed.
Calineurin Inhibitors C Kidney transplantation
Transient immune alterations in the neonate (Cyclosporine) Hyperkalaemia and renal impairment (Tacrolimus)
Increasingly used - they have decreased rejection episodes
and improved survival in transplant recipients.
No
Mycophenolate mofetil D Kidney transplantation
Increased risk of miscarriage and congenital abnormalities.
Congenital malformations of the external and middle ear, cleft lip and cleft palate, and other major
structural malformations involving the eye, hands and fingers, cardiac, bowel and
skeletal systems.
Should be discontinued before pregnancy
Yes
Sirolimus (Rapamune) C Kidney transplantation
Small-for-gestational-age infants and delayed bone ossification
Immunosuppressant that could be used during pregnancy
Has not been implicated in specific fetal
malformations. Further
investigations are required
Proteinuria
The gold standard to diagnose proteinuria of pregnant women is the 24-hour urine collection and quantification of urine proteins level. Even so, errors in timing and urine retention in the dilated systems make urine collections incomplete, because of the large volumes contained at one time in the upper urinary tract.
The increase of the excretory level of urinary proteins is associated with important risk for intrauterine growth restriction and increased risk for renal dysfunction. [18, 20, 21].
In patients developing nephrotic syndrome during pregnancy (proteinuria > 3g/day, albuminuria > 30 mg/L and edema) there is a high risk for thromboembolic accidents and maternal death, even if blood pressure is maintained at satisfactory levels. In this category of patients, anticoagulant prophylaxis with low molecular weight heparins is recommended, up to 6 weeks postpartum. [5, 25].
Preconception Counseling
As general rule, the conception should not be discouraged as long as possible risks are understood and careful monitoring
of the pregnancy is available. [1, 14, 20]. It is necessary to discontinue and substitute therapeutic agents with teratogenic potential (Table 1).
Patients with active vasculitis or lupus should be advised to wait for the episode to end prior to the conception. [5, 26].
RENAL TRANSPLANTATION AND PREGNANCY
Maternal status and fetal development in posttransplant renal patients is favorable, significantly better when compared to pregnant women with advanced renal disease requiring dialysis, especially if the following conditions are fulfilled [1, 8]:
• Renal function is stable
• Minimum one year after renal transplantation; latest recommendations ex-tend the waiting period at 2 years, thus reducing the risk for allograft failure
• Proteinuria maintained under 1g/day
• Controlled hypertension
• Minimal doses of immunosuppressants required (prednisone, tacrolimus, azathioprine, ciclosporin) (Table 1)

50
• No prior or pending rejection of renal transplantation [5].
Thus, women with diagnosed advanced kidney disease are often encouraged to wait until after successful kidney transplantation to obtain a pregnancy. The reason for this recommendation is that fertility is improved after transplantation and the risks for pregnancy complications, such as preterm birth and hypertension, are much lower. Pregnancy is considered a sensitizing event, which can result in the formation of anti-HLA antibodies that may impend finding a future suitable donor.
The incidence of premature childbirth, intrauterine growth restriction and preeclampsia is higher compared to the general population and 30% of pregnancies will be affected by these complications.
Vaginal childbirth is not contraindicated in case of mothers with renal transplantation. When Caesarian section is preferred, the approach of the lower segment may be difficult due to the trajectory of the transplanted ureter. [1, 5].
DIABETIC NEPHROPATHY AND PREGNANCY
Lately, as women do tend to procreate later in life, diabetic nephropathy is probably becoming the most common CKD seen in pregnancy. Pregnancy in women with diabetes type 1 or type 2 is associated with a two- to four-time increased risk of pre-term delivery, preeclampsia and perinatal mortality compared with the general population [27]. Pregnancies in women with CKD associate poor placentation and fetal growth restriction, with an incidence of small for gestational age newborns of 31% [19]. It is rather unclear if growth restriction is based on poor placentation or on fetal hyperinsulinamia, but women with more severe renal impairment are exposed to a greater risk for pregnancies with poorly grown infants, despite maternal hyperglycaemia, thus antenatal documentation of fetal growth restriction has been linked with worse fetal outcomes than macrosomia.
The first clinical sign of kidney malfunction is microalbuminuria, and urinary albumin excretion of 30–300 mg/24 h, corresponding to a spot urine albumin/creatinine ratio of 30–300 μg/mg. The progression towards diabetic nephropathy is seen in all cases left untreated, when microalbuminuria becomes persistent proteinuria, associating hypertension and an unavoidably decline in GFR [28].
Diabetic nephropathy adversely affects the course of pregnancy by the following three mechanisms: development of severe hypertension superimposed on the deterioration
of kidney function in the mother, preterm delivery due to high maternal blood pressure and preeclampsia, and fetal intrauterine growth restriction and fetal distress caused by placental insufficiency.
The prepregnancy preparations in women with diabetic nephropathy or microalbuminuria would comprise intensive glycaemic control, low-dose aspirin, and intensive antihypertensive treatment. The treatment with ACE inhibitors followed by strict metabolic control for at least 6 months, usually results in low levels of albumin excretion and it has been found to be associated with a high rate of successful pregnancy outcome [27]. On the onset of pregnancy, early in the first trimester, ACE inhibitors are linked to increased risk of congenital malformations [29], as for the last part of the pregnancy, are associated with abnormal fetal renal development and neonatal renal failure [30] therefore treatment with ACE inhibitors or AngII antagonists should be stopped before conception. In the event of an unplanned pregnancy, women with diabetic nephropathy which necessitates continuous treatment with blockers of the RAS (renin angiotensin system), can benefit from a shift to other antihypertensive drugs successfully in early pregnancy. Severe congenital malformations have been linked to poor glycemic control before pregnancy, therefore the goal is strict glycemic control and HbA1c as close to normal as possible, at least <7% is recommended [31, 32].
In all women with high risk for pre-eclampsia, treatment with low-dose aspirin is proven to have some preventive effect, thus, at least theoretically, the same treatment could be of benefit in women with diabetic nephropathy [20] and is recommended in American and British guidelines.
The goal for CKD and diabetic pregnacy should be BP <135/85 mmHg and urinary albumin excretion <300 mg/24 h, obtained with antihypertensive treatment with pregnancy-friendly drugs, strict glycemic control (HbA1c <6.0%) and low-dose aspirin.
For many years, a pregnancy in women with diabetic nephropathy was related to a decline in maternal kidney function and important perinatal mortality, but recent improvements in pregnancy management substantially reduced those risks.
Cesarean delivery should be considered for every case where fetal weight is estimated for more than 4500 g. Vaginal birth at 39 weeks gestation is safe whenever blood glucose levels are well controlled and kidney function is normal. In those cases with vascular complications and poorly controlled blood glucose, delivery should be considered at 36 0/7 to 38 6/7 weeks or even earlier, depending on maternal and fetal

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
51
status [33].
ACUTE RENAL INSUFFICIENCY IN PREGNANCY
Acute renal insufficiency is defined as the sudden degradation of renal function, ranging from the slight decline in renal function to the necessity of renal function replacement therapy [3, 34].
In the first part of the pregnancy, infectious pathology and hypovolemia are the most common causes of renal injury, and in the second part of the pregnancy, the most frequent etiological factors are preeclampsia, placental abruption or severe anemia.
The best management of this pathology is possible using the classification of the acute renal insufficiency by the cause, as pre-renal, renal and post-renal. Pre-renal injury occurs predominantly secondary to hypovolemia, hemorrhage, congestive heart failure, sepsis. Renal insufficiency has as main etiologies acute tubular necrosis, renal cortical necrosis, thrombotic microangiopathy, preeclampsia, acute interstitial nephritis, and glomerulonephritis. Post-renal insufficiency occurs due to ureteropelvic block, but rarely causes bilateral renal injury [3, 5].
Clinically, pregnant women with acute renal insufficiency present oliguria, de-fined as a urine production < 0.5 ml/kg/h. [3, 35]. Another marker of renal injury is the increased level of serum creatinine, which is difficult to be appreciated due to its low level in normal pregnancy. Secondary to renal injury, as a compensatory mechanism for renal hypo-filtration, an increase in systemic blood pressure and intravascular volume appears and changes of urinary
electrolytic values due to the action of the system renin-angiotensin-aldosterone [36-38].
Treatment of acute kidney failure involves treating the underlying condition that caused renal injury and focuses on the restoration of urine production, avoiding secondary injury and increasing renal infusion. The effects of this pathology on the fetus are diverse, specific to each etiology, and may require delivery, as in the case of preeclamsia or placental abruption. [39, 40].
CONCLUSIONS
Although the risk of complications in pregnancy in patients with chronic kidney disease is higher than in the general population, in most cases, with the correct management of pregnancy and kidney disease, the pregnancy has a favorable evolution. There are insufficient data to certify the pregnancy as a potential factor in the decline of the renal function.
Intensive pre-pregnancy antihypertensive treatment in patients with diabetic nephropathy and good glycaemic control results in preservation of kidney function and favorable maternal and fetal outcomes.
Acute renal insufficiency, occurring during pregnancy, may benefit from specific etiological treatment, but may also require emergency delivery.
Close obstetric surveillance and screening for kidney function is important to improve pregnancy outcomes in these high-risk pregnancies.
References:
1. Webster P, Lightstone L, McKay DB, Josephson MA. Pregnancy in chronic kidney disease and kidney transplantation. Kidney Int. 2017;91(5):1047-56.
2. Van Hook JW. Acute kidney injury during pregnancy. Clin Obstet Gynecol. 2014;57(4):851-61.
3. Petca RC, Popescu RI, Boț M, Veduța A, Petca A. The role of ultrasound in diagnosis and management in renal colic during pregnancy. Proceedings of the 6th Congress of the Ultrasound Society in Obstetrics and Gynecology. Bucharest, Romania. 2018; 478-84.
4. Bumbu A, Nacer K, Bratu O, Berechet M, Bumbu G, Bumbu B. Ureteral lesions in gynecological pathology. Proceedings of the 14th National Congress of Urogynecology and the National Conference of the Romanian Association for the Study of Pain. Eforie, Romania. 2017; 82-89.
5. Hall M, Brunskill NJ. Renal disease in pregnancy. Obstet
Gynaecol Reprod Med 2010;20(5):131-7.
6. Petca A, Radu DC, Petca RC, Mehedintu C, Barac RI, Ionescu A, et al. Current trends of liquid chromatography tandem mass spectroscopy use in clinical gynecology. Rev Chim (Bucharest). 2019;70(6):2021-5.
7. Katz AI, Davison JM, Hayslett JP, Singson E, Lindheimer MD. Pregnancy in women with kidney disease. Kidney Int. 1980;18(2):192-206.
8. Spinu DA, Marcu RD, Socea B, Diaconu CC, Scarneciu I, Scarneciu C, et al. Ureteral JJ stent – which one is better? Rev Chim (Bucharest). 2018;69(8):2061-3.
9. Bumbu GA, Berechet MC, Nacer K, Bumbu G, Maghiar OA, Bratu OG, et al. Clinical, surgical and morphological assessment of the pyeloureteral syndrome. Rom J Morphol Embryol. 2018;59(4):1173-7.
10. Krane NK, Hamrahian M. Pregnancy: kidney diseases and

52
hypertension. Am J Kidney Dis. 2007;49(2):336-45.
11. Cheung KL, Lafayette RA. Renal physiology of pregnancy. Adv Chronic Kidney Dis. 2013;20(3):209-14.
12. Veduta A, Petca R, Petca A. The impact of the fear of pain on the decision regarding invasive prenatal diagnosis. Proceedings of the 14th National Congress of Urogynecology and the National Conference of the Romainian Association for the Study of Pain. Eforie, Romania. 2017: 199 – 202.
13. Davison JM, Lindheimer MD, editors. Pregnancy and chronic kidney disease. Semin Nephrol; 2011: Elsevier.
14. Petca A, Vladareanu S, Zvanca M, Bot M, Vladareanu R. Timing for the delivery of the growth-restricted fetus: a resolvable issue. Proceedings of the 49th annual scientific meeting of the European Society for Clinical Investigation. Cluj Napoca, Romania. 2015: 273-277.
15. Mehedintu C, Antonovici M, Brinduse L, Bratila E, Stanculescu R, Berceanu C, et al. The influence of progesterone on immunohystochemical markers in endometriosis. Rev Chim (Bucharest). 2018;69(3):581-4.
16. Timofte D, Ochiuz L, Ursaru M, Ciuntu B, Ionescu L, Calu V, et al. Biochemical Modifications Related to Calcium Deficiencies in Obesity and After Laparoscopic Sleeve Gastrectomy. Rev Chim (Bucharest). 2017;68(10):2341-5.
17. Spinu D, Bratu O, Popescu R, Marcu D, Radulescu A, Mischianu D. Clostridium difficile – an emerging plague. Rom J Mil Med. 2015;118(3):12-15.
18. Vellanki K. Pregnancy in chronic kidney disease. Adv Chronic Kidney Dis. 2013;20(3):223-8.
19. Bramham K, Rajasingham D. Pregnancy in diabetes and kidney disease. J Ren Care. 2012;38:78-89.
20. Zvanca ME, Bot M, Radu D, Radu N, Petca A. Impact of early supplementation with low-dose aspirin on functional first trimester parameters in low-risk pregnancies. J Matern Fetal Neonatal Med. 2019;32(4):604-609.
21. Piccoli GB, Attini R, Vasario E, Conijn A, Biolcati M, D'Amico F, et al. Pregnancy and chronic kidney disease: a challenge in all CKD stages. Clin J Am Soc Neph-rol. 2010;5(5):844-55.
22. Langer O, Conway DL, Berkus MD, Xenakis EM-J, Gonzales O. A comparison of glyburide and insulin in women with gestational diabetes mellitus. N Engl J Med. 2000;343(16):1134-8.
23. Maru N, Rusu MC, Sandulescu M. Variant anatomy of nasal turbinates: supreme, superior and middle conchae bullosae, paradoxical superior and inferior turbi-nates, and middle accessory turbinate. Rom J Morphol Embryol. 2015;56(3):1223-6.
24. Chhabria S. Aicardi's syndrome: are corticosteroids teratogens? Arch Neurol. 1981;38(1):70-.
25. Palma-Reis I, Vais A, Nelson-Piercy C, Banerjee A. Renal disease and hypertension in pregnancy. Clinical Medicine. 2013;13(1):57-62.
26. Dogaroiu C, Avramoiu M. Correlation between chronological
age and the stage of union of the distal femur and proximal tibia epiphyses in a Romanian sample population. Rom J Leg Med. 2015;23:171-6.
27. Mathiesen ER, Ringholm L, Feldt-Rasmussen B, Clausen P, Damm P. Obstetric nephrology: pregnancy in women with diabetic nephropathy—the role of antihypertensive treatment. Clin J Am Soc Nephrol. 2012;7(12):2081-8.
28. Parving H-H, Smidt UM, Hommel E, Mathiesen ER, Rossing P, Nielsen F, et al. Effective antihypertensive treatment postpones renal insufficiency in diabetic nephropathy. Am J Kidney Dis.1993;22(1):188-95.
29. Cooper WO, Hernandez-Diaz S, Arbogast PG, Dudley JA, Dyer S, Gideon PS, et al. Major congenital malformations after first-trimester exposure to ACE inhibitors. New England Journal of Medicine. 2006;354(23):2443-51.
30. Tabacova S, Little R, Tsong Y, Vega A, Kimmel CA. Adverse pregnancy outcomes associated with maternal enalapril antihypertensive treatment. Pharmacoepidemiology and drug safety. 2003;12(8):633-46.
31. Boulot P, Chabbert-Buffet N, d’Ercole C, Floriot M, Fontaine P, Fournier A, et al. Diabetes and Pregnancy Group, France. French multicentric survey of outcome of pregnancy in women with pregestational diabetes Diabetes Care. 2003;26:2990-3.
32. Evers IM, de Valk HW, Visser GH. Risk of complications of pregnancy in women with type 1 diabetes: nationwide prospective study in the Netherlands. Bmj. 2004;328(7445):915.
33. ACOG Practice Bulletin No. 201: Pregestational Diabetes Mellitus. Obstet Gy-necol. 2018;132(6):e228-e248.
34. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure–definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Critical care. 2004;8(4):R204.
35. Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Critical care. 2007;11(2):R31.
36. Nwoko R, Plecas D, Garovic VD. Acute kidney injury in the pregnant patient. Clin Nephrol. 2012;78(6):478-86.
37. Dogaroiu C, Capatina CO, Gherghe EV, Avramoiu M. The importance of the os-sification centre morphology in the left hand-wrist bones for age evaluation. Rom J Leg Med. 2014;22:105-8.
38. Lafayette R. AKI in pregnant patient: two lives at stake. Nephrology Times. 2010;3(5):9-10.
39. Needham E. Management of acute renal failure. Injury. 2005;1(7):524.
40. Radulescu A, Madan V, Aungurenci A, Bratu O, Farcas C, Dinu M, Mischianu D. Antibiotic resistant urinary tract infections in an urology ward. Rom J Mil Med. 2015;118(3):20-22.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
53
Article received on March 8, 2019 and accepted for publishing on October 13, 2019. CLINICAL PRACTICE
Differential diagnosis in case of overdose of antiepileptic treatment. Clinical case
Mihail S. Tudosie2, Genica Caragea1, Ana D. Radu4, Ilenuţa L. Dănescu3
Abstract: Acute drug-related acute intoxications or suicidal ideation following overdose with anticonvulsants may cause major morbidity, in many cases requiring intensive care and prolonged periods of hospitalization. The case of a 35-year-old patient known for a history of epilepsy with phenobarbital and carbamazepine treatment is brought to the Emergency Unit by transfer from another hospital in a comatose state with insufficient respiratory performance, bilateral active mydriasis. From the family members' claims, the patient discontinued treatment with phenobarbital two weeks ago. Following interdisciplinary examination, hospitalization in the Neurology Department with the diagnosis of epileptic status is decided. Due to the progressive aggravation of acute respiratory insufficiency, the ventilator support is constituted. Since the biological samples related to probability diagnosis and cerebral imaging were not conclusive, toxicological samples were collected. The GC/MS analytical toxicology screening in urine reveals the presence of carbamazepine and phenobarbital and their plasma levels (5.92 and 92.3 mg/l) as determined by the FPIA method indicate an overdose of phenobarbital therapy. The patient is taken over by the Department of Clinical Toxicology where specific intensive care measures are applied. Clinical evolution is favorable. The psychiatric examination highlights the depressive idea, suicidal ideas, and uselessness. The suicide attempt is confirmed. It also presents a review of the main information about acute poisoning with anticonvulsants, but also about the analytical laboratory methods that bring precious information in establishing the diagnosis of certainty.
Keywords: phenobarbital, carbamazepine, GC/MS, urine, acute poisoning
INTRODUCTION
Acute drug-related acute intoxications or suicidal ideation following overdose with anticonvulsants may cause major morbidity, in many cases requiring intensive care and prolonged periods of hospitalization. The evaluation and stabilization of the poisoned patient is similar to all cases presented at the Emergency Unit and aims at detecting vital risk disruptions and correcting them in the shortest possible time [1].
Phenobarbital (C12H12N2O3) is a drug of the barbiturates group used since 1912. It is generally administered to epileptic patients at doses of 60-200 mg/day, commonly in
combination with other anticonvulsants [2]. In the chronic administration of 200 mg / day in epileptic patients, the concentrations had average values of 29 mg/l and 16-48 mg/l [3]. Plasma concentrations of 10-30 mg/l are generally considered appropriate for patients receiving phenobarbital as an anticonvulsant and may require 14-21 days to reach the level of equilibrium.
The compound had a plasma half-life of about 4 days [4]. Toxic reactions to phenobarbital at chronic doses occur at plasma concentrations exceeding 40 mg/l. Patients develop
1 Military Medical Research Center, Bucuresti, Romania 2 University of Medicine and Pharmacy “Carol Davila”, Bucharest 3 ICU II Toxicology, Clinical Emergency Hospital, Bucharest 4 National Forensic Institute, Bucharest, Romania
Corresponding author: Genica Caragea [email protected]

54
coma with reflexes present at plasma concentrations of 65-117 mg/l and reflexes loss occurs at concentrations of 100-134 mg/l [5].
The mechanism of action of barbiturates and implicitly of phenobarbital is related to their affinity for the GABAA receptor, which is fixed in distinct sites with both benzodiazepines and GABA (the main CNS inhibitor neurotransmitter), potentiating its effect. Barbiturates also block a glutamate receptor - the major excitatory neurotransmitter in the CNS [6].
In acute intoxication with barbiturates, because of the depression of central respiratory control mechanisms, following a general depression and anxiety, death may occur in the absence of artificial ventilation and vital functions support measures. In short-duration barbiturates intoxication, the cardiopulmonary arrest may be the cause of premature death and late: circulatory insufficiency, cerebral edema, acute pulmonary edema. Central nervous effects are related to the severity of intoxication. Because there is no specific antidote, the goal of therapy remains to increase the elimination of toxic and support vital functions. In determining the establishment of measures to increase the elimination of anticonvulsants (hemodialysis, hemoperfusion, plasmapheresis), it is also important to measure the plasma levels of these substances in relation to the clinical condition of the patient.
Carbamazepine is a classic anticonvulsant, largely used, with an iminostilbene nucleus, similar to that of tricyclic antidepressants, with a prolonged digestive absorbtion time. Its mechanism of action is partially known, acting on the neuronal membrane towards stabilizing its hyperexcitability, inhibiting repetitive neuronal discharges and reducing excitatory synaptic transmission by blocking voltage-dependent sodium channels. The reduction is glutamate discharge and the stabilization of the neuronal membrane contribute only supplementary to the antiepiletic effect [7]. Its main metabolite is 10,11-carbamazepine epoxide, an essential metabolite which possesses the same toxic effects as the basic drug. In pharmacological doses, the distribution volume of carbamazepine is of 1.4 l/Kg, and the half-life is of 15 hours.
The absorbtion of carbamazepine occurs slowly, 65-85% of it binds to plasma proteins and it is quickly distributed to all tissues. The maximum serum levels are reached within 6 to 8 hours following ingestion and steady-state plasma concentrations, considered to be therapeutic levels of carbamazepine, considerably vary between individuals; for most patients, the therapeutic level of carbamazepine is between 4 and 12 ml//l and the concentration of the active
metabolite (10,11 epoxide-carbamazepine) is 30% of the plasma levels of carbamazepine [7]. In epilepsy, carbamazepine is administered in doses of 0.8 to 1.2 g / day, 2-3 times a day for an adult and 0.1-1 g / day (10-25 mg / kg / day) for children of ages from 1 to 15. Therapeutic doses can be optimized through therapeutic monitoring (TDM) due to a good correlation between plasma levels and the therapeutic effect [8]. As it is an enzymatic inducer, carbamazepine can induce its own metabolism, this phenomenon being responsible for the reduction of its half-life over repeated administrations.
In case of carbamazepine overdose, many of the observed effects can be tied to secondary mechanisms of its tricyclic structure. The symptomatology of an acute intoxication is characterized by coma, pyramidal signs, nausea/vomiting, hypotension, hypothermia, anticholinergic symptomatology (tachycardia, mydriasis, redness, urinary retention etc.) tremor, convulsions, respiratory depression, cyanosis, sinusal bradycardia or atrio-ventricular conduction disorders [9]. Plasma levvels of carbamazepine between 18-70 µg/ml have been measured in carbamazepine overdoses, while levels higher than 40 µg/ml have been associated with an increased risk of complications such as coma, convulsions, respiratory insufficiency, and cardiac conduction disorders [10].
CASE PRESENTATION
A.G, female gender, 35 years old, admitted for being comatose, with acute respiratory insufficiency and non-reactive bilateral mydriasis.
Personal medical history – known to have had previous comitial crises, treated with phenobarbital and carbamazepine
History – Comitial patient, brough from the Emergency Admission Unit in a coma, transferred from another hospital. From her family’s affirmations, the patient had stopped taking phenobarbital 2 weeks before.
Interdisciplinary consults performed in the Major Emergency Department:
- neurosurgical consult: coma GCS = 5 points, no neurological signs;
- internal diseases consult: PA = 100 mmHg, AV = 76 b/min, ECG sinusal rhythm with no pathological alterations.
CT scan: no heterodense lesions are present at brain level, ventricular system situated on median line.
The patient is taken over by the Neurology Department with a diagnosis of epilepsy.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
55
Objective examination upon admission: second degree coma; non-reactive; oro-tracheal tube, spontaneously breathes through the tube; TA = 120/70 mmHg, AV = 85 b/min; gastric statis = 200 ml; diuresis = 400 ml; positive bilateral Babinski bilateral; fixed mydriasis, pupil OD>OS, fixed eyeballs; no meningeal signs; spontaneously and discreetely mobilizes right superior limb. Due to the progressively aggraveted acute respiratory insufficiency, mechanical ventilation is applied (BIPAP, PEEP = 5 mbar, FiO2 = 40%, Pmax = 19 mbar);
In order to confirm the diagnosis, lumbar punction was performed and probes of cerebrospinal fluid were sent for biochemstry, bacteriology and cellularity.
A central subclavicular catheter was also applied.
The pulmonary radiography does not show evolving pleuro-pulmonary changes.
As the diagnosis could not be confirmed by the biological samples, toxicological samples were taken. The GC/MS examination of the urine shows the presence of carbamazepine and phenobarbital.
Biological table: biochemistry, hematology, coagulation within normal limits.
The patient is taken over by the Clinical Toxicology Department.
Intensive therapy measures: ventilation support; ensuring permeability of respiratory pathways – aspiration of tracheo-bronchial secretions through the IOT probe; naso-gastric drainage tube; hydro-electrolytic rebalancing; plasmatic and urinary alkalinization under paraclinical control (EAB).
Support therapy: monitoring of vital functions; ventilatory support; hemodynamic monitoring; diuresis monitoring; analytical control of urine.
Clinical evolution is favorable – the patient becomes conscious, reacts to stimuli; shows spontaneous breathing signs; is detubed and restarts spontaneously breathing. Physical recovery measures continue.
Psychiatric exam reveals depressive ideation, suicidal ideas and ideas of uselessness. A suicide attempt is confirmed.
She is tranferred to the specialized psychiatry clinic.
Analytical diagnosis of certainty in case of acute drug intoxication
One of the most used methods in identifying the substances incriminated in acute drug intoxications is gas chromatography - GC coupled with mass spectrometry - MS.
Thus, by gas chromatograph injection of a completely unknown matrix, if the working conditions are well chosen, at the exit of the GC they will be placed in turn at the detector's disposal. If the detector is of the MS type and the injection matrix contains organic substances whose molecular weight falls within the working range of the mass filter, it will determine the mass spectrum for each substrate. In our case, the urine sample collected from the patient is follows to the liquid-liquid analytical procedure and injected into the GC/MS system, with ion trape detection, electronic ionisation 70eV. Midazolam is used as an internal standard. The method chosen for the separation and qualitative identification of analytes by GC / MS is called medicamente.mth, with a 45-minute acquisition time. Upon completion of the acquisition program, read the total recorded chromatogram. Apply the background correction and then proceed to the identification of each chromatographic peak. It establishes the mass spectrum that corresponds to it and these spectra are automatically compared with the existing spectra in the laboratory database. The database includes specialized spectral libraries (Nist98, PMW, Wiley6).
The temperature program used was:
- temperature injector: 280 ° C,
- for column oven: Start at 1400C, 2 minute range, increase temperature by 5° C / min to 290° C, 13 minutes (total time 45 minutes).
Following these investigations, the result is established. In our case, we separated the chromatographic column and identified the following substances: Phenobarbital and carbamazepine at the retention times shown in Table 1, based on the mass spectrum obtained by EI.
Table 1: Data on identified compounds (molecular weight, retention times and characteristic spectral lines m/z)
Compound MW
(g/mol) Retention time (min)
CAS. No. Spectral
lines (m/z)
Phenobarbital 232 16.001 50-06-6 117, 204,
231
Carbamazepine 236 16,944 298-46-4 193, 236
Midazolam (SI) 326 26,951 59467-70-
8 310, 327
In case of acute drug intoxications, measuring plasma levels is important both to establish the seriousness of the intoxication and to monitor the efficiency of the medical treatment.
Therapeutic drug monitoring is performed based on the

56
principle of fluorescent light polarization on a Cobas Integra 400/800 system for serum samples taken from patients. It is a quantitative method which uses the the fluorescence of substances and is based on immunological properties (antigen- antibody) of the analyzed substances. The principle of this method is based on exciting the sample with a fixed
wavelength and measuring the quantity of light emitted by a substance called a luminophore, on another wavelength. The specific antigens, present in the tracer, bind to the antibodies present in the sample [11]. Thus, the quantity of light emitted by the sample will be inversely proportionate to the quantity of searched substance.
Figure 1: Phenobarbital mass spectrum (top) and full scan chromatogram obtained from SD urine extract
Chromatogram Plot
File: c:\saturnws\data\SD.sms Sample: SD Sample Notes: urina toxi Operator: Scan Range: 1 - 2699 Time Range: 0.00 - 44.97 min.
100 200 300 400 m/z
0%
25%
50%
75%
100%
51 89
115
144 161
204
233
259 392 444
Spect 1 16.001 min. Scan: 961 Chan: 1 Ion: 144 us RIC: 1281691 BP 204 (212326=100%) SD.SMS
12.5 15.0 17.5 20.0 22.5 25.0 minutes
0
1
2
3
MCounts RIC all SD SMS
Midazolam [SI]
Carbamazepina
Fenobarbital
2 751 901 1051 1201 1351 1501
Scans
Figure 2: Calibration curve (in 6 points) for carbamazepine on the Cobas Integra 400+ System
In this case, determinations of the plasma levels of carbamazepine and phenobarbital in the samples were performed using the FPIA method, which implies determinations on a calibration curve in 6 points. The quality
control is performed for three known concentrations.
The plasma concentration of carbamazepine on the first and second day of hospitalization was 5.92 and 2.90 mg/L, respectively. Because this value falls within the therapeutic limit, no measurements have been made during hospitalization. In contrast, the plasma level of phenorbarbital was increased and its variation in the first 7 days of hospitalization is shown in Figure 3.
CONCLUSIONS
Antiepileptic treatment based on selective anticonvulsant medication (carbamazepine and phenobarbital) follows the avoidance and treatment of epilepsy seizures, and at therapeutic doses these crises stop. Unfortunately, cases of overdose of treatment may occur either accidentally or for a
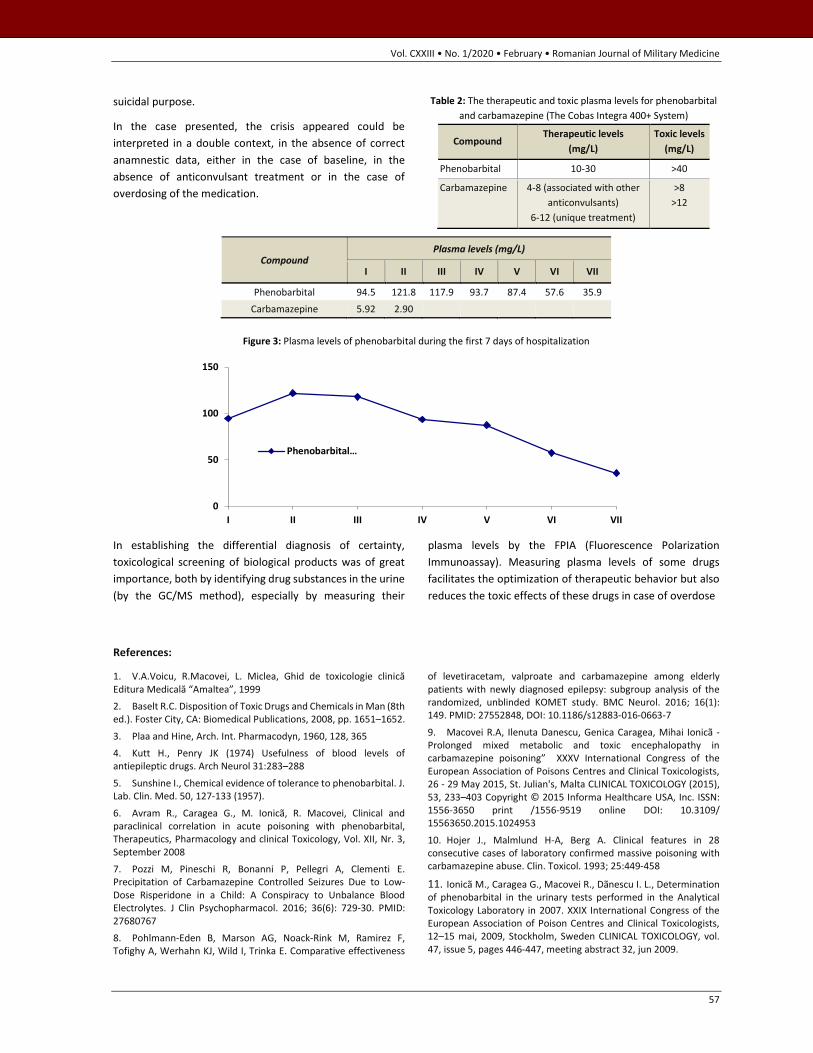
Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
57
suicidal purpose.
In the case presented, the crisis appeared could be interpreted in a double context, in the absence of correct anamnestic data, either in the case of baseline, in the absence of anticonvulsant treatment or in the case of overdosing of the medication.
Table 2: The therapeutic and toxic plasma levels for phenobarbital and carbamazepine (The Cobas Integra 400+ System)
Compound Therapeutic levels
(mg/L) Toxic levels
(mg/L)
Phenobarbital 10-30 >40
Carbamazepine 4-8 (associated with other anticonvulsants)
6-12 (unique treatment)
>8 >12
Compound Plasma levels (mg/L)
I II III IV V VI VII
Phenobarbital 94.5 121.8 117.9 93.7 87.4 57.6 35.9 Carbamazepine 5.92 2.90
Figure 3: Plasma levels of phenobarbital during the first 7 days of hospitalization
In establishing the differential diagnosis of certainty, toxicological screening of biological products was of great importance, both by identifying drug substances in the urine (by the GC/MS method), especially by measuring their
plasma levels by the FPIA (Fluorescence Polarization Immunoassay). Measuring plasma levels of some drugs facilitates the optimization of therapeutic behavior but also reduces the toxic effects of these drugs in case of overdose
References:
1. V.A.Voicu, R.Macovei, L. Miclea, Ghid de toxicologie clinică Editura Medicală “Amaltea”, 1999
2. Baselt R.C. Disposition of Toxic Drugs and Chemicals in Man (8th ed.). Foster City, CA: Biomedical Publications, 2008, pp. 1651–1652.
3. Plaa and Hine, Arch. Int. Pharmacodyn, 1960, 128, 365
4. Kutt H., Penry JK (1974) Usefulness of blood levels of antiepileptic drugs. Arch Neurol 31:283–288
5. Sunshine I., Chemical evidence of tolerance to phenobarbital. J. Lab. Clin. Med. 50, 127-133 (1957).
6. Avram R., Caragea G., M. Ionicã, R. Macovei, Clinical and paraclinical correlation in acute poisoning with phenobarbital, Therapeutics, Pharmacology and clinical Toxicology, Vol. XII, Nr. 3, September 2008
7. Pozzi M, Pineschi R, Bonanni P, Pellegri A, Clementi E. Precipitation of Carbamazepine Controlled Seizures Due to Low-Dose Risperidone in a Child: A Conspiracy to Unbalance Blood Electrolytes. J Clin Psychopharmacol. 2016; 36(6): 729-30. PMID: 27680767
8. Pohlmann-Eden B, Marson AG, Noack-Rink M, Ramirez F, Tofighy A, Werhahn KJ, Wild I, Trinka E. Comparative effectiveness
of levetiracetam, valproate and carbamazepine among elderly patients with newly diagnosed epilepsy: subgroup analysis of the randomized, unblinded KOMET study. BMC Neurol. 2016; 16(1): 149. PMID: 27552848, DOI: 10.1186/s12883-016-0663-7
9. Macovei R.A, Ilenuta Danescu, Genica Caragea, Mihai Ionicã - Prolonged mixed metabolic and toxic encephalopathy in carbamazepine poisoning” XXXV International Congress of the European Association of Poisons Centres and Clinical Toxicologists, 26 - 29 May 2015, St. Julian's, Malta CLINICAL TOXICOLOGY (2015), 53, 233–403 Copyright © 2015 Informa Healthcare USA, Inc. ISSN: 1556-3650 print /1556-9519 online DOI: 10.3109/ 15563650.2015.1024953
10. Hojer J., Malmlund H-A, Berg A. Clinical features in 28 consecutive cases of laboratory confirmed massive poisoning with carbamazepine abuse. Clin. Toxicol. 1993; 25:449-458
11. Ionicã M., Caragea G., Macovei R., Dãnescu I. L., Determination of phenobarbital in the urinary tests performed in the Analytical Toxicology Laboratory in 2007. XXIX International Congress of the European Association of Poison Centres and Clinical Toxicologists, 12–15 mai, 2009, Stockholm, Sweden CLINICAL TOXICOLOGY, vol. 47, issue 5, pages 446-447, meeting abstract 32, jun 2009.
0
50
100
150
I II III IV V VI VII
Phenobarbital…

58
Article received on April 4, 2019 and accepted for publishing on October 23, 2019. CLINICAL PRACTICE
Cross-leg limb salvage solution: A case report regarding the management of a major defect in a patient with type IIIB open distal tibial fracture
M. Turbatu, C. Condrea, A. Oproiu, A. Cursaru, A. Lupu
Abstract: Tissue coverage of lower limb defects after tibial fractures remain one of the hardest areas for a surgeon to deal with. The definitive management of Gustillo type IIIB fractures depends on a series of factors, which have a high impact in the multidisciplinary management of this severe trauma.
Although free flaps have been used succesfully in the last two decades, there remains some cases where easier plasties using the contralateral limb tissue reserved could be indicated. We describe our experience with a cross-leg flap in a severe-smoking patient for the reconstruction of a difficult leg defect.
Keywords: Cross-leg plasty, Type IIIB fractures, External fixators
INTRODUCTION
The tibia is reported to be the most commonly fractured long bone in the human body. Gustilo-Anderson IIIB injuries are a major trauma requiring aggressive excision, adequate fixation, and good coverage of tissue defects. They are open tibial fractures more difficult to manage than other I, II, and III A forms.
Stable skeletal fixation with immediate soft tissue cover has been the key to the optimal results in treating open tibial fractures, in particular, type IIIB fractures. The prognosis of these fractures depends on the degree of contamination of the wound, the devitalization of the soft tissue and area of the defect.
Pedicled cross-extremity flaps for calves wound coverage have been replaced by free tissue transfer in the last two decades. However, there are certain difficult situations where the free flap cannot be employed and alternative
methods are needed.
We describe our experience with a cross-leg gastrocnemius flap in a heavy-smoker patient with little tissue reserve necessary for the coverage of a defect in the middle to lower third anterior calf.
CASE PRESENTATION
We present the case of 58 years old patient who was admitted in the Orthopedics and Traumatology Clinic of the Emergency University Hospital of Bucharest with an injury after a direct trauma by axe and had pain in the calf, functional impotence of the inferior member and an open wound of about 10 cm on the inner side in the 1/3 middle anterior calf.
Following wound debridement (including post-debridement measurement) and skeletal fixation, the anterior defect was assessed [1].
The following days the patient underwent antibiotherapy and careful daily wound dressing until a proper defect coverage plan was decided.
University Emergency Hospital Bucharest, Plastic surgery and Orthopaedics, Bucharest, Romania

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
59
Free flaps are usually the first choice for soft tissue coverage in the distal leg. There continue to be, however, some clinical situations in which local fasciocutaneous and myocutaneous flaps are often not available [2].
Occasionally, a free flap may also have failed because of technical errors or damaged vasculature. In these situations, a cross-leg flap is the best choice.
In the end we decided to perform a pedicled cross-leg gasctrocnemius flap, with the utilization of an external fixator to keep both legs immobilized after the surgery.

60
After proper preoperative markings, the flap was raised including the fascia. The inclusion of fascia in the flap makes the length-to-breadth ratio 3: 1 perfectly safe [3]. This allows much greater area of skin to be transferred with much more freedom of leg position. The donor site was covered using direct sutures and a split skin graft was also used to cover the donor muscle flap [4].
OUTCOME AND FOLLOW-UP
The release of the flap was performed at 21 days and the unaffected contralateral member was removed from fixation [5]. The patient continued treatment by monoplane external fixation for 8 weeks with progressive mobilization with the support of the unaffected limb. The patient evolution was satisfactory also making regular X-rays checks for the consolidation of the fracture.
At 4 months after the trauma, the ablation of the external fixation [6] was decided and the patient resumed progressive mobilization of both lower limbs. With the presence of the consolidated fracture, at 4 months
postoperatively the patient successfully achieved a score of 62 according to Clinical rating system for the ankle and hindfoot [7].
CONCLUSION
The cross-leg Filatov flap is still considered a safer and more reliable solution to free tissue transfer in certain situations of lower-limb trauma, especially open distal tibial fractures in which rotation flaps are not a viable solution.

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
61
References:
1. Codorean I., Cuzino D., Codorean I.B., G. Toma – Imagistica prin rezonanta magnetica in evaluarea leziunilor traumatice ale gleznei – Revista de medicina militara,2009, CXX
2. Teusdea C.B. , Dogaru S. – Accesul intravascular intraosos in conditii de urgenta – Revista de medicina militara, 2013, Nr. 1-2
3. P. Agarwal, Raza H.K.T. - Cross-leg flap: Its role in limb salvage – Indian journal of Orthopaedics, 2008, Oct-Dec. 439-443
4. Ramasamy P.R. – Management of Gustillo Anderson IIIB open tibial fractures by primary fascio-septo-cutaneous local flap and primary fixation: The fix and shift technique – Indian Journal of
Orthopaedics 2017, Jan-Feb. 55-68
5. Calhoun JH, Gogan WJ, Beraja V, Howard RJ, Oliphant JR. Dynamic axial fixation for immobilization of cross-leg flaps in chronic osteomyelitis. Ann Plast Surg. 1989;23:354–6.
6. Velazco A, Fleming LL, Nahai F. Soft-tissue reconstruction of the leg associated with the use of the Hoffmann external fixator. J Trauma. 1983;23:1052–7.
7. Benacquista T, Kasabian AK, Karp NS. The fate of lower extremities with failed free flaps. Plast Reconstr Surg. 1996;98:834–40

62
Article received on October 4, 2019 and accepted for publishing on January 23, 2020. CLINICAL PRACTICE
Clinical and dermatoscopical aspects of pigmented basal cell carcinoma – Case series and literature review
Anton M. Țilea1, Viorel Trifu1, Bogdan Dima2, Mihai A. Badea3, Raluca S. Costache1, Daniel O. Costache1, George S. Țiplica4
Abstract: The diagnosis of pigmented basal cell carcinoma can bring significant distress to patients and physicians alike. However, astute clinicians that can employ correctly the clinical and dermatoscopical clues can reach a correct preoperative diagnosis, and as such can avoid unnecessary worry for the patient, additional work-up, or overtreatment. We present a case series of pigmented basal cell carcinomas and a comparative case with pigmented cutaneous melanoma, together with a literature review, that will highlight these aspects of the management of pigmented tumours of the skin.
Keywords: dermoscopy, basal cell carcinoma
INTRODUCTION
Pigmented tumours of the skin bring significant distress to patients and to physicians alike. While pigmented basal cell carcinoma is not a benign tumour, its prognosis is highly favourable if it is diagnosed and treated early. The dermatologist is also in the position to tell the patient that even if the tumour to be excised is a malignant tumour, the treatment, i.e the excision of the tumour, will result in the complete healing of the lesion, with a low probability of local recurrence.
We present a case series of pigmented basal cell carcinomas and a review of the literature in an effort to show that this particular pigmented tumour of the skin can be easily identified by the experienced dermatologist with the aid of clinical and dermatoscopical clues.
REVIEW OF LITERATURE
Background
One of the oldest references [1] to pigmented basal cell carcinoma (pBCC) in PubMed involves a differential diagnosis with cutaneous melanoma. Indeed, the spectrum of pigmented cutaneous melanoma (PCM) can plague the management of a pigmented lesion of the skin leading to overtreatment, if a wide excision of the supposed PCM is intended, and/or to unnecessary worry of the patient and extended additional work-up, e.g. lymph-node ultra-sonography, lung radioscopy etc.
Goldenberg et al [15] describe the age-adjusted incidence of BCC in American population to be 226 per 100000 persons and the age-adjusted prevalence of BCC to be 342 per 100000 persons.
Maloney et al [13] and Betti et al [14] describe the histopathology epidemiology of pBCC to be of around 6.7% and 8.5% respectively of the total cases of BCC taken into consideration.
Altamura et al [17] found that actually the dermatoscopically
1 “Dr. Carol Davila” Emergency University Central Military Hospital, Bucharest, Romania 2 Elias Emergency University Hospital, Bucharest, Romania 3 Târgu-Mureș County Hospital, Targu-Mures, Romania 4 Colentina Clinical Hospital, Bucharest, Romania; “Carol Davila” University of Medicine and Pharmacy Bucharest

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
63
non-pigmented BCCs can be as low as 15.1%, and the rest of the BCCs have some degree of pigmentation, from low to heavy. They [17] have not used the diagnosis of pBCC according to the histopathology, but according to the dematoscopical features pigmentation, albeit all lesions were confirmed with histopathology to be BCC.
Both studies, of Maloney et al [13] and Betti et al [14] found that pBCC has a better prognosis with clear excision margins than the other types of BCC. A similar conclusion is reached also by Ito T et al [6] by saying that narrow-margins excision of 3mm may be enough to obtain clear margins for pBCC, as opposed to 4mm margins required for classic non-pigmented BCC.
Clinical aspect
The clinical aspect of BCC should not be disregarded as we consider that an astute clinician can observe significant clinical clues that can lead him to an appropriate preoperative diagnosis.
Bolognia et al [11] describe the clinical aspect of a nodular BCC as “shiny, pearly papule with a smooth surface and the presence of arborizing telangiectasias”. They [11] also describe a “thin rolled border” in superficial BCC.
Wu et al [12] describe the clinical aspect of BCC to have a “pearly or translucent quality” with telangiectasias, the lesions having a “periphery more raised than the middle” – a rolled border. In addition, they [12] say that “a shiny quality” can be observed when a superficial BCC is illuminated.
Huang et al [10] used translucency as a clinical indicator to learn computer aided systems to detect BCC and achieved a 93% accuracy.
Dermatoscopy
Dermatoscopy, if correctly employed, can be an invaluable tool in diagnosing BCC and especially pBCC.
A very thorough article on the dermatoscopy of pBCC is the one of Menzies et al [5]. They established that there are several highly specific dermatoscopical patterns, e.g. “maple leaflike areas” and “spoke wheel areas” that have a specificity of 100%, albeit a low sensitivity of 17% and respectively 10% [5, 16]. Other dermatoscopical criteria with high specificity were “large grey-blue ovoid nests”, “multiple grey-blue globules” and “arborizing (treelike) telangiectasia” [5 , 16].
Marghoob et al [7] also describe several specific dermatoscopy aspects for pBCC: large blue-grey ovoid nests, multiple blue-grey globules, leaf-like structures, spoke-
wheel-like structures, arborizing telangiectasias and ulceration.
Kittler et al [8] describe the dermatoscopic patterns of pBCC as “radial lines, dots, clods and structureless zones” and they say that a common pattern is blue clods of different shapes and sizes. In addition, other structures may appear, such as brown clods, grey, blue and brown dots, white structureless zones and radial lines. They [8] also describe patterns that are very strong indicators against BCC, e.g. non-radial lines (reticular, branched, curved and parallel), pseudopods and circles. Also, the description of the typical vessels found in BCC would be: “branched serpentine vessels that originate from thick stem” – usually found in nodular BCC, while in superficial BCC a polymorphous pattern of vessel can appear, e.g. thin, serpentine and coiled vessels. The pattern of dot vessels is a strong indicator against BCC [8], unless found within ulceration.
Cabo et al [9] considers the dermatoscopical pigmented structures, e.g. maple leaflike areas, spoke-wheel area, multiple blue-grey dots or small globules, blue-grey ovoid nests to be characteristic for pBCC, while “white shiny blotches and strands” are an additional criterion only seen with polarized dermatoscopy.
Felder et al [18] and Turkmen et al [19] describe a dermatoscopical blue-white variant of pBCC. This type of pBCC is included in the class of heavily pigmented BCC as described by Altamura et al [17]
Lallas et al [21] describe dermatoscopic features to differentiate between superficial BCC (e.g. maple-leaf like areas and short, fine telangiectasias) and nodular BCC (e.g. blue-grey ovoid nests, arborizing vessels, ulceration). Wozniak - Rito et al [20] agree with these findings.
Additional work-up
Usually additional work-up is not necessary for the diagnosis of pBCC. However, cytology i.e fine needle biopsy can be used [3] in certain cases that the clinical and dermoscopical aspects are not enough to establish a certain diagnosis. Usually this happens when the lesions are pure nodular, without a superficial part.
CASE SERIES
Case 1
A 59 years old female patient presented to our dermatology department for a 2/2 cm, ulcerated, pigmented lesion in the left axilla. The lesion had a history of about 8 years. The patient also had a personal history with another BCC lesion operated 10 years prior to this admission.

64
The clinical aspect of the lesion (Figure 1): - central ulceration with serohematic crust on the surface, - the non-ulcerated part of the lesion has a translucent greyish feature with superimposed dark-brown, blue, black punctate pigmentation - the periphery of the lesion has a pearly pigmented aspect - the lesion has a smooth-shiny surface that does not continue the adjacent normal skin architecture
Figure 1: The clinical aspect of Case 1 has a very specific pearly-pigmented aspect of the periphery of the lesion along with a
translucent quality
The dermatoscopical aspect of the lesion Figure 2: - brown and blue-black-grey ovoid nests - leaf-like areas (high specificity for pBCC) - fine telangiectasias - ulceration
Figure 2: The dermatoscopical aspect of Case 1 has leaf-like areas and brown and blue-black-grey ovoid nests
The lesion was excised with 4 mm margins and the histopathological examination established the diagnosis of pBCC, (Figure 3) with islands of basaloid cells with peripheral palisading, clefts between the islands and the stroma, and focal deposits of melanin within the basaloid islands.
Case 2
A 63 years old male patient presented to our dermatology department for a 1.5/2cm pigmented lesion on the posterior
thorax. The lesion had a history of about 1 year. The patient had no significant medical history.
Figure 3: The histopathology of Case 1 established the diagnosis of pigmented basal cell carcinoma
The clinical aspect of the lesion (Figure 4): - small central ulceration - translucent feature of almost the entire lesion with pigmentation – large pearly structures pigmented bluish-black - shiny smooth surface that does not continue the architecture of the adjacent normal skin
Figure 4: The clinical aspect of Case 2 has an overall pigmented pearly and translucent feature with shiny smooth surface
The dermatoscopical aspect of the lesion (Figure 5): - blue-grey ovoid nests and globules - arborizing telangiectasias - the polarized dermatoscopy image showed white lines and blotches
The lesion was excised with 4mm margins and the histopathological diagnosis confirmed it was a pBCC.
Case 3
An 82 years old female patient, with no significant medical history, presented to our dermatology department for a 0.7/0.7 cm pigmented lesion on the left thigh. The lesion had a history of about 6 months.
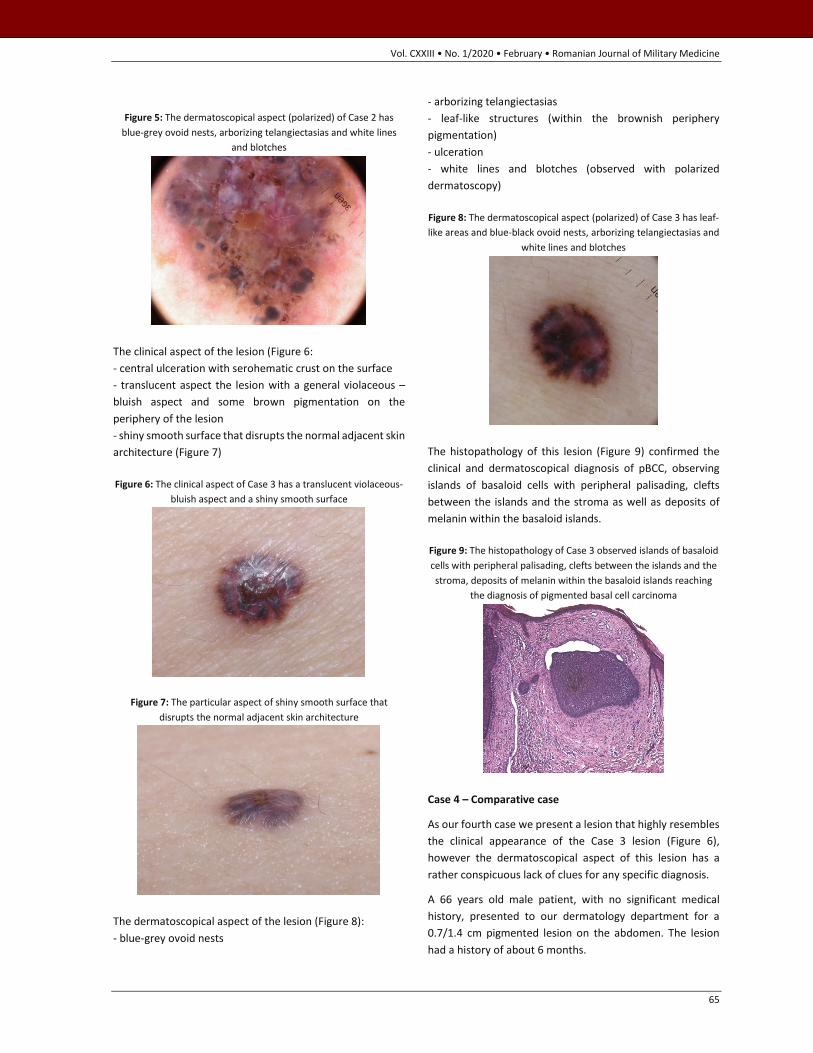
Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
65
Figure 5: The dermatoscopical aspect (polarized) of Case 2 has
blue-grey ovoid nests, arborizing telangiectasias and white lines and blotches
The clinical aspect of the lesion (Figure 6: - central ulceration with serohematic crust on the surface - translucent aspect the lesion with a general violaceous – bluish aspect and some brown pigmentation on the periphery of the lesion - shiny smooth surface that disrupts the normal adjacent skin architecture (Figure 7)
Figure 6: The clinical aspect of Case 3 has a translucent violaceous-bluish aspect and a shiny smooth surface
Figure 7: The particular aspect of shiny smooth surface that disrupts the normal adjacent skin architecture
The dermatoscopical aspect of the lesion (Figure 8): - blue-grey ovoid nests
- arborizing telangiectasias - leaf-like structures (within the brownish periphery pigmentation) - ulceration - white lines and blotches (observed with polarized dermatoscopy)
Figure 8: The dermatoscopical aspect (polarized) of Case 3 has leaf-like areas and blue-black ovoid nests, arborizing telangiectasias and
white lines and blotches
The histopathology of this lesion (Figure 9) confirmed the clinical and dermatoscopical diagnosis of pBCC, observing islands of basaloid cells with peripheral palisading, clefts between the islands and the stroma as well as deposits of melanin within the basaloid islands.
Figure 9: The histopathology of Case 3 observed islands of basaloid cells with peripheral palisading, clefts between the islands and the stroma, deposits of melanin within the basaloid islands reaching
the diagnosis of pigmented basal cell carcinoma
Case 4 – Comparative case
As our fourth case we present a lesion that highly resembles the clinical appearance of the Case 3 lesion (Figure 6), however the dermatoscopical aspect of this lesion has a rather conspicuous lack of clues for any specific diagnosis.
A 66 years old male patient, with no significant medical history, presented to our dermatology department for a 0.7/1.4 cm pigmented lesion on the abdomen. The lesion had a history of about 6 months.

66
The clinical aspect of the lesion (Figure 10): - ulceration with serohematic crust - pigmentation – pink – red – violaceous – black - textured surface – tends to keep the architecture of adjacent normal skin, even if somewhat disorganized (the surface is not smooth - shiny) - ovoid/rather rectangular shape
Figure 10: The clinical aspect of Case 4 observed rather similar type of pigmentation with Case 3, i.e. pink – red – violaceous – black, however with a textured surface (as opposed to Case 3, here the
surface is not shiny)
The dermatoscopical aspect of the lesion (Figure 11): - ulceration - pink – red – violaceous colour - white lines and blotches on the periphery of the lesion (polarized dermatoscopy) - lack of specific clues for pBCC (blue –grey ovoid nests, leaf-like structures, arborizing telangiectasias)
Figue 11: The dermatoscopical aspect of Case 4 has pink – red violaceous colour with lack of specific clues for pBCC
The histopathology of this lesion (Figure 12) reached the diagnosis of pigmented cutaneous melanoma (PCM), with a Breslow thickness of 0.8 mm.
As a discussion of Case 3 vs Case 4, Figure 13 presents a comparative view of both the clinical and dermatoscopical aspects of both lesions. On the clinical part, both lesions are ulcerated and have somewhat the same type of
pigmentation.
Figure 12: The histopathology of Case 4 established the diagnosis of pigmented cutaneous melanoma, Breslow thickness of 0.8 mm,
Clark IV
However the clinical clue of smooth – shiny surface that disrupts the normal adjacent skin architecture can be found in Case 3 and not in Case 4 where we find a textured surface of the lesion that tends to keep the normal adjacent skin architecture, even if somewhat disorganized. On the dermatoscopical part, both lesions present ulceration and similar type of pigmentation. However, while the Case 3 dermatoscopy image has conspicuous clues for pBCC, Case 4 dermatoscopy has a discomforting lack of clues for pBCC or for other pigmented lesion of the skin. Even though the polarized dermatoscopy clue of white lines and blotches are present in both Case 3 and Case 4, this comparative case shows that this particular clue cannot be used to differentiate between pBCC and PCM.
Figure 13: Comparative view of clinical and dermatoscopical aspects of Case 3 and Case 4
DISCUSSIONS
Regarding the epidemiology of pBCC we think that if the clinical and dermatoscopical aspect of pigmented structures within a BCC lesion are taken into consideration when

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
67
establishing the pBCC diagnosis, the percentage may be significantly higher than what the studies of Maloney et al [13] and Betti et al [14] are suggesting, 6.7% to 8.5% . This may be because even in clinically non-pigmented BCC, the dermoscopy may reveal some pigmentation [17, 22], e.g. leaf-like structures, blue-grey ovoid nests or globules, and these structures may not appear in a given histopathology slide. To prove our point, Altamura et al [17] found that some degree of dermatoscopical pigmentation could be found in almost 85% of the BCC lesions. Therefore, the quantitative feature of the pigmentation may have an important role to play in reaching a histopathological diagnosis of pBCC.
To our knowledge, the clinical clue of disruption of the adjacent normal skin architecture within the lesion of a superficial pBCC has not been clearly described so far. There are papers that describe the “shiny quality” [12] or “shiny… smooth surface” [11] in superficial BCC and we think it refers to the same clinical quality. We consider this clinical clue important because superficial spreading cutaneous melanoma tends to conserve adjacent normal skin architecture within the lesion, as opposed to pBCC.
The clinical clue of pigmentation, even though is the most worrisome in the differential diagnosis of pBCC with PCM, should be observed within the overall aspect of the lesion, e.g. pearly translucent feature, rolled border.
If the clinical aspect of a suspected pBCC lesion is not enough to reach a correct diagnosis, usually dermatoscopy comes with supplementary clues. Moreover, some clues are highly specific for pBCC, e.g. leaf-like structures and spoke-wheel like structures [5] [7] [9]. Other clues that are indicative for pBCC are blue-grey ovoid nests, globules and dots, arborizing telangiectasias [5] [7] [9] (brown clods, grey, blue and brown dots, branched serpentine vessels that originate from thick stem [8]).
Even though the clinical and dermoscopical aspects of the pBCC are usually enough to diagnose a pBCC, there are papers [2 -4] that do not use dermoscopy as an aid.
On the other hand, papers focusing on dermatoscopy tend to overlook the clinical aspect of the lesion. As such, Turkmen et al [19], even though they present the clinical
aspect of the lesions, the pictures are small and cannot be evaluated properly. In their article [19] the Case 3 and Case 6 seem to have a rolled border that may be a strong indicator for BCC, considering the fact that the dermatoscopical aspect, with blue-white veil cannot differentiate between pBCC and pigmented cutaneous melanoma (PCM).
While we consider the dermatoscopical aspect of pBCC of paramount importance, considering the highly specific clues that can simply establish the diagnosis of pBCC, we also consider the clinical clues very important, especially when the dermatoscopical clues are lacking, as we showed in our case series.
Considering the data regarding the clearing of margins in the pBCC management [6] [13] [14] we think that a careful evaluation, clinical and dermatoscopical, of a pigmented lesion can avoid unnecessary worry for the patient, additional work-up and overtreatment.
CONCLUSION
We consider that the clinical and dermatoscopical aspects, as well as the histopathological diagnosis should have a synergy within the management of pBCC.
Therefore, the clinical aspect of pearly border, translucency, and shiny surface – disruption of the adjacent normal skin architecture should be combined with the dermatoscopical aspect of “leaflike areas”, “spokewheel areas”, blue-grey ovoid nests and globules as well as arborizing telangiectasias and the diagnosis of pBCC can be reached in a swift manner. By doing so one can avoid unnecessary patient worry and additional work-up as well as one can adapt the treatment according to the diagnosis. Nevertheless, a biopsy should always confirm the clinical/dermatoscopical diagnosis.
Author Contributions: The individual contributions of the authors is as follow: conceptualization, A.M.T., M.A.B.; methodology, A.M.T., B.D.; validation, G.S.T, V.T; formal analysis, A.M.T.; writing—original draft preparation, A.M.T.; writing—review and editing, D.O.C., R.S.C.; supervision, G.S.T.
Conflicts of Interest: The authors declare no conflict of interest.
References:
1. Rogers JD. A case for diagnosis (pigmented basal cell epithelioma or melanoma?). Arch Derm Syphilol. 1946 Nov;54:589
2. K, Deepadarshan et al. “Pigmented Basal cell carcinoma: a clinical variant, report of two cases.” Journal of clinical and
diagnostic research: JCDR vol. 7,12 (2013): 3010-1. doi:10.7860/JCDR/ 2013/7568.3831
3. Jain M, Madan NK, Agarwal S, Singh S. Pigmented basal cell carcinoma: Cytological diagnosis and differential diagnoses. J Cytol. 2012;29(4):273–275. doi:10.4103/0970-9371.103952

68
4. Abudu B, Cohen P R (April 02, 2019) Pigmented Basal Cell Carcinoma Masquerading as a Melanoma. Cureus 11(4): e4369. doi:10.7759/cureus.4369
5. Menzies SW, Westerhoff K, Rabinovitz H, Kopf AW, McCarthy WH, Katz B. Surface Microscopy of Pigmented Basal Cell Carcinoma. Arch Dermatol. 2000;136(8):1012–1016.
6. Ito T, Inatomi Y, Nagae K, Nakano-Nakamura M, Nakahara T, Furue M, Uchi H. Narrow-margin excision is a safe, reliable treatment for well-defined, primary pigmented basal cell carcinoma: an analysis of 288 lesions in Japan. J Eur Acad Dermatol Venereol. 2015 Sep;29(9):1828-3
7. Marghoob A, Malvehy J and Braun R. (2012). Atlas of dermoscopy. London: Informa Healthcare.
8. Kittler, Harald, et al. Dermatoscopy: pattern analysis of pigmented and non-pigmented lesions. Vienna, Austria: Facultas, 2016. Print.
9. Cabo, Horacio, and Aimilios Lallas. Comprehensive atlas of dermatoscopy cases. Cham, Switzerland: Springer, 2018. Print.
10. H. Huang, P. Kharazmi, D. I. McLean, H. Lui, Z. J. Wang and T. K. Lee, "Automatic detection of translucency using a deep learning method from patches of clinical basal cell carcinoma images," 2018 Asia-Pacific Signal and Information Processing Association Annual Summit and Conference (APSIPA ASC), Honolulu, HI, USA, 2018, pp. 685-688.
11. Bolognia JL, Jorizzo JJ, Schaffer JV, Callen JP, Cerroni L, Heymann WR et al. Dermatology, 3rd edition. London: Elsevier, 2012.
12. Wu P, Stern R, Robinson J, Corona R Epidemiology, pathogenesis, and clinical features of basal cell carcinoma, Oct 2019 UpToDate. Retrieved 24 Nov 2019 from https://www.uptodate.com/contents/epidemiology-pathogenesis-and-clinical-features-of-basal-cell carcinoma
13. Maloney M, Jones D, Sexton F. Pigmented Basal Cell Carcinoma: Investiagtion of 70 cases J Am Acad Dermatol. 1992;27:74-78.
14. Betti R, Gualandri R, Cerri A, Inselvini E, Crosti C. Clinical Features and Histologic Patterns Analysis of Pigmented Basal Cell Carcinomas in an Italian Population. J Dermatol. 1997; 25:691-694
15. Goldenberg G, Karagiannis T, Palmer JB, Lotya J, O'Neill C, Kisa R, Herrera V, Siegel DM. Incidence and prevalence of basal cell carcinoma (BCC) and locally advanced BCC (LABCC) in a large commercially insured population in the United States: A retrospective cohort study. J Am Acad Dermatol. 2016 Nov;75(5):957-966.e2.
16. Menzies SW. Dermoscopy of pigmented basal cell carcinoma. Clin Dermatol. 2002 May-Jun;20(3):268-9. Review.
17. Altamura D, Menzies SW, Argenziano G, Zalaudek I, Soyer HP, Sera F, Avramidis M, DeAmbrosis K, Fargnoli MC, Peris K. Dermatoscopy of basal cell carcinoma: morphologic variability of global and local features and accuracy of diagnosis. J Am Acad Dermatol. 2010 Jan;62(1):67-75.
18. Felder S, Rabinovitz H, Oliviero M, Kopf A. Dermoscopic pattern of pigmented basal cell carcinoma, blue-white variant. Dermatol Surg 2006;32(4):569e70.
19. Türkmen M, Turk B, Karaarslan K I, Yaman B, Ozdemir F. (2018). Blue-white variant of pigmented basal cell carcinoma. Dermatologica Sinica. 36. 10.1016/j.dsi.2018.05.003.
20. Wozniak-Rito A, Zalaudek I, Rudnicka L. Dermoscopy of basal cell carcinoma. Clin Exp Dermatol. 2018 Apr;43(3):241-247. doi: 10.1111/ced.13387. Epub 2018 Jan 17. Review.
21. Lallas A, Tzellos T, Kyrgidis A, Apalla Z, Zalaudek I, Karatolias A, Ferrara G, Piana S, Longo C, Moscarella E, Stratigos A, Argenziano G. Accuracy of dermoscopic criteria for discriminating superficial from other subtypes of basal cell carcinoma. J Am Acad Dermatol. 2014 Feb;70(2):303-11.
22. Lallas A, Argenziano G, Kyrgidis A, Apalla Z, Moscarella E, Longo C, Ferrara G, Piana S, Benati E, Zendri E, Sotiriou E, Zalaudek I. Dermoscopy uncovers clinically undetectable pigmentation in basal cell carcinoma. Br J Dermatol. 2014 Jan;170(1):192-5

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
69
.
Article received on September 2, 2019 and accepted for publishing on November 28, 2019. VARIA
Compliance of school doctors’ practice with medical legislation
Silviu Paun1, Luiza M. Vasile2, Sinziana Birsanu3, Codrut A. Nanu1
Abstract: School doctors’ practice comprises specific aspects governed by legal rules. Knowledge and compliance with the applicable legislation are necessary in order to ensure respect of the patient’s rights, to avoid claims of medical malpractice and to assure medical act’s quality. The present study investigated compliance of school doctors’ practice with the applicable legal requirements.
All respondent doctors violate the applicable legal requirements. Future quantitative research is necessary to measure the amplitude of the identified vulnerabilities.
INTRODUCTION
School doctors’ assistance implies ensuring special conditions for children with chronic diseases, coordinating the optimal response during medical emergencies and managing school environment’s health and safety.
Sports competitions for students represent another special feature in this field, given the school doctor’s task of issuing a favourable notice for competition to students who participate in such competitions following a brief clinical examination, without always having the student’s personal background checks or the possibility to send the student to a specialist for control, without having an appropriate emergency kit and under improper conditions for a medical act which can all generate problems related to malpractice.
Specific aspects of their activity expose them in case of ignorance and non-compliance of the applicable legal regulations.
RESEARCH OBJECTIVE
The assumption under which our research was initiated was that school doctors from Bucharest are not fully aware and do not fully comply with the legislation in force.
The research objective was to collect information regarding the compliance of school doctors’ practice with the applicable legal requirements.
MATERIAL AND METHOD
The present research aimed to identity the existence of a phenomenon (the issue regarding compliance of school medical activities with the applicable legal provisions) and to establish the framework for possible future quantitative research addressed to the newly developed area of interest.
The target group included 25 general practitioners activating as school doctors in Bucharest. Sample was selected taking into account the qualitative objects of the research, in the sense that we aimed to identify possible specific tendencies among school doctors. The investigative techniques were represented by interviews, which led to structuring of a questionnaire comprising five closed questions destined to evaluate the risk of malpractice in the school doctors’
1 “Carol Davila” University of Medicine and Pharmacy, Department 14 - Orthopaedics and Anaesthesiology, Discipline of Medical Law Aspects and Malpractice, Bucharest, Romania 2 “Carol Davila” University of Medicine and Pharmacy, Faculty of Medicine, Bucharest, Romania 3 Bucharest Bar, Lawyer

70
activity. Developed models because of previous research in the field of knowledge and compliance with medical legislation by doctors were used when preparing the questionnaire.
The questionnaires were then circulated and filled in anonymously during a workshop organized by the Administration of Hospitals and Medical Services Bucharest (Administrația Spitalelor și Serviciilor Medicale București - ASSMB) and which took place in Bucharest, on 8.12.2017.
Participants were asked to answer the questions based on their daily practice and not on theoretical knowledge or personal opinions regarding the respective matters.
Moreover, respondents were informed that their answers would be used exclusively for scientific purposes, for performing an objective valuation of the malpractice risk resulting from non-compliance with the legal framework applicable to school doctors’ practice.
Definition of the valuation criteria for answers to the questionnaire’s inquiries
Thus, the interviews aimed to investigate if medical practice of respondent doctors respects the applicable legislation.
The doctors’ answers were marked as “correct” if they indicated the fact that the practice of the respondent doctor respects the legal requirements involved by the question or “wrong” when the answer demonstrated non-compliance of the law by the respondent doctor during his daily medical activity.
In addition, the alternative answers selected by respondent doctors were analysed in detail with the purpose of identifying some models of practice and their justifications. Programme IBMSPSS Statistic, version 20 was used for processing the obtained data.
RESULTS AND DISCUSSION
General results
None of the respondent doctors chose the “correct” answer to all the questions. Therefore, we can consider that, in their current activity, respondent doctors do not fully respect the legal framework applicable to school doctors.
Specific results
Based on received answers we identified some domains of medical practice in which specific legal requirements are not fully respected: informed consent, confidentiality of medical data, patients’ access to personal medical information, filming/photographing of patients and limiting the doctor’s activity to one’s own medical specialty.
Question no. 1
“How do you proceed when a patient requires health care for an associated disorder beyond the scope of competence of your specialty?”
Proposed alternatives to answer: a) I do not provide health care, regardless the patient’s status. b) I provide health care after consulting a specialized doctor in the field of the respective disorder. c) I provide health care in emergencies.
The correct answer (to be chosen between the proposed alternatives) is: c)
The general representation of answers to Question no. 1 is included in Table 1 and Chart 1.
Chart 1: Representation of answers to Question no. 1, according to valuation: correct/wrong.
Table 1: Answers to Question no. 1
Frequency Percent Valid percent
Cumulative percent
Valid
a 1 4.00 4.00 4.00
b 4 16.00 16.00 20.00
b, c 5 24.00 24.00 44.00
c 14 56.00 56.00 100.00
Total 25 100.00 100.00
It may be noticed that 44% of answers were wrong. In order to identify the respondent doctors’ attitude concerning limiting the medical practice to its own specialty we performed a detailed analysis of the received answers to each question, the results being included in Table 1 and Chart 1.
The correct action for the situation described by this question from the questionnaire is prescribed by legal texts: the medical practitioners are civilly liable for the damages caused during the exercise of their profession and when they exceed the limits of their competence. In case of some associated disorders’, each of these conditions will have to
56
44
correct wrong

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
71
be supervised/diagnosed/treated by a doctor specialized in the respective area of expertise/competence. Therefore, the legislation includes an interdiction for doctors to perform medical acts that are not covered by their specialty.
There is an exception to this rule in case of emergencies when there is an imminent danger/irreversible deterioration of patient’s health state and when a medical practitioner with the necessary competence is not available. [3]
It may be noticed that 24% from respondents included the correct alternative c), but they also added alternative b) (which is wrong), while 16% from respondents mentioned only alternative b) as being correct.
The attitude of respondent doctors is to provide health care beyond their specialty in every situation after they ask a medical practitioner having the necessary area of expertise. These attitudes do not comply with the abovementioned legal requirements.
In situation when all 3 conditions are cumulatively met (urgency, imminent danger for patient’s life/irreversible deterioration of patient’s health state, lack of specialized medical practitioners) medical activities beyond one’s area of expertise can be performed without the need to consult another medical practitioner.
Question no. 2
“Can information regarding the treatment prescribed to a patient be communicated to third parties?”
Proposed answers: a) Yes, to non-governmental organizations which support the patients. b) Yes, to patient’s family members. c) No.
The correct answer (to be chosen from the proposed alternatives) is: c).
According to the law, the doctor cannot disclose to any other person than the patient data regarding its health state. Information concerning patient’s status, results of medical investigations, diagnosis, prognosis, treatment and personal data are confidential, even after the patient’s death.
General representation of answers to Question no. 2 is included in Table 2 and Chart 2.
Wrong answers were generated by the doctors’ attitude to communicate medical data to patient’s family members. It may be supposed that doctors chose this answer given the fact that patients’ majority (with the exception of students) are minors.
Chart 2: Representation of answers to Question no. 2, according to valuation: correct/wrong
Table 2: Answers to Question no. 2
Frequency Percent Valid percent
Cumulative percent
Valid
b 12 48.00 48.00 48.00
c 13 52.00 52.00 52.00
Total 25 100.00 100.00
However, the question did not refer to minor patients. Even if we referred to minor patients, not every family member is a legal representative (there are various circumstances prescribed by law in which parents, relatives, other people can be legal representatives for a minor patient). Therefore, not even under this scenario, the alternative b) would have been correct. This represents more a vulnerability of respondent doctors’ practice with respect to compliance of medical practice with the abovementioned legal requirements.
Question no. 3
"The informed consent of the patient may be obtained:"
Proposed answers were the following: a) From the patient attaining the age of 18. b) From a minor patient under some circumstances. c) From one of the minor patient’s parents.
Correct answer to this question: a), b), c).
According to law, the statutory age for giving an informed consent is 18.
Minor patients may give their consent in absence of parents or legal representative, in medical situations related to the diagnosis and/or treatment of sexual and reproductive problems, when specifically requested by a minor patient who is over 16 years old.
The important amount of wrong answers (96%) requires an in-depth analysis of answers to this question.
52
48
correct wrong

72
Chart 3: Representation of answers to Question no. 3, according to valuation correct/wrong
Table 3: Answers to Question no. 3
Frequency Percent Valid percent
Cumulative percent
Valid
1 4.00 4.00 4.00
a 3 12.00 12.00 16.00
a, b, c 1 4.00 4.00 20.00
a, c 20 80.00 80.00 100.00
Total 25 100.00 100.00
80% from respondent doctors only selected two of the three correct answers. Therefore, the legal prescription, which allows obtaining an informed consent from minor patients, which are at least 16 years old for sexual and reproductive problems, is not known and respected. Surprisingly, 12% of respondents did not identify the answers as being applicable to medical practice given the fact that these people consider that it is mandatory to obtain the informed consent from both parents of a minor patient.
Question no. 4
“Should medical data concerning undertaken investigations, established diagnosis and recommended treatment be made available to the patient?"
The proposed alternatives to answer: a) It is not necessary; when discharging the patient from hospital, the treatment scheme and the necessity to come back for control should be explained to the patient. b) Yes, always, in a complete manner. c) Information related to diagnosis and established treatment should be made available to the patient”
The correct answer (to be chosen from the proposed alternatives) is b).
According to law no. 46/2003, the patient has unlimited access to all personal medical information and the doctor has to make it available to the patient and, in writing, if the patient requests it.
Almost half of respondent school doctors (44%) do not ensure unlimited access to personal medical information for patients/legal representatives.
Chart 4: Representation of answers to Question no. 4, according to valuation correct/wrong
Table 4: Answers to Question no. 4
Frequency Percent Valid percent
Cumulative percent
Valid
1 4.00 4.00 4.00
b 15 60.00 60.00 64.00
b, c 3 12.00 12.00 76.00
c 6 24.00 24.00 100.00
Total 25 100.00 100.00
The analysis of chosen answers demonstrates that 24% from doctors consider that only information regarding diagnosis and treatment must be made available to the patient/legal representative.
This attitude may also be caused by an excess of legislation, which generates confusion. Thus, law no. 46/2003 was amended in 2016, the following article being added: “Article 12: the patient or the person expressly designated by the patient, according to articles 9 and 10, has the right to receive, when discharged from hospital, a written summary of investigations, diagnosis, treatment, medical care provided during hospitalisation and, upon request and once, a copy of high performance investigations’ records.”.
It may be generated the impression that information mentioned in this article could be accessed only by patients, but this interpretation would contradict article 9 of the norms for application with respect to Law no. 46/2003 regarding patient’s rights which prescribes the following: “the hospital units must ensure unlimited access to personal medical data for patients ”.
We believe that medical practice should take into account the most restrictive (unlimited access) legal requirement and this represents a correct attitude for a school doctor,
4
96
correct wrong
56
44
correct wrong

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
73
Question no. 5
"May the medical personnel film the patient in the medical unit?"
The proposed answers were the following> a) After obtaining the patient’s written consent. b) By protecting the patient’s identity. c) For teaching and research purposes exclusively.
The correct answer (to be chosen from the proposed alternatives) is b).
The patient cannot be photographed or filmed in a medical unit without his consent, with the exception of the situation when the images are necessary for diagnosis and treatment and for avoiding the suspicion of medical malpractice.
Therefore, the medical personnel may film/photograph without the patient’s or the legal representative’s consent if the confidentiality of data which is obtained throughout this means is protected.
Chart 5: Representation of answers to Question no. 5, according to valuation correct/wrong
Table 5: Answers to Question no. 5
Frequency Percent Valid percent
Cumulative percent
Valid
1 4.00 4.00 4.00
a 11 44.00 44.00 48.00
a, b 2 8.00 8.00 56.00
a, b, c 6 24.00 24.00 80.00
a, c 1 4.00 4.00 84.00
b 2 8.00 8.00 92.00
b, c 1 4.00 4.00 96.00
c 1 4.00 4.00 100.00
Total 25 100.00 100.00
Most of wrong answers are generated by respondent doctors’ conviction that they need patient’s consent for filming/photographing him/her. It may be noticed that there are many alternatives of answers selected for this question that suggests the ignorance of the specific legal framework.
CONCLUSIONS
School doctors’ practice does not respect entirely the applicable legal framework.
The consequences are that civil liability may be incurred against doctors and the protections of malpractice assurance ceases. Moreover, respecting patients’ rights represents an element to measure medical act’s quality, as defined by the National Authority of Quality Management in Health (Autoritatea Naţională de Management al Calităţii în Sănătate – ANMCS) throughout specific accreditation standards for medical units. Extensive further studies are necessary in order to determine this phenomenon’s amplitude and configuring some education projects destined to cover the identified educational need is necessary.
References:
1. Daniela Rajka, Asigurarea urgențelor în cabinetul medical școlar, Revista de Medicină Şcolară şi Universitară, Vol IV, Nr. 2, aprilie 2017
2. Nanu. A, Georgescu. D,Voic. V,Ioan. B, Place and relevance of legal provisions in the context of medical practice in Romania, Revista Romana de Bioetica, Volume: 9, Issue: 4, Pages: 90-101
3. Parliament of Romania, Law no. 95/2006 on health-care reform, republished, Official Journal of Romania, 1st part, no. 652/2015, available in Romanian, art 653
4. Parliament of Romania, Law no. 46/2003 on patient rights, republished, Official Journal of Romania, 1st part, no. 51/2003, available in Romanian, art 6,10,21
5. Parliament of Romania, Law no. 95/2006 on health-care reform, republished, Official Journal of Romania, 1st part, no. 652/2015,
available in Romanian, art 661
6. Parliament of Romania, Law no. 46/2003 on patient rights, republished, Official Journal of Romania, 1st part, no. 51/2003, available in Romanian, art 24
7. Parliament of Romania, Law no. 46/2003 on patient rights, republished, Official Journal of Romania, 1st part, no. 51/2003, available in Romanian, art 20
8. Pituru, S; Vladareanu, S; Paun, S; Nanu, A, Malpractice and professional liability of medical personnel, FARMACIA, Volume: 63 Issue: 2 Pages: 318-324
9. https://anmcs.gov.ro/web/proces-elaborare-standarde-ambulatoriu/
8
92
correct wrong

74
VARIA
In memoriam – General (Ret.) Academician Prof. Vasile Cândea MD, PhD
A FLAME WENT OUT, A LIFE DEDICATED TO SCIENCE
On the morning of January 14, 2020, people working is the "Dr. Carol Davila” University Central Emergency Military Hospital (SUUMC) found out, with great regret and pain, about the passing away of one of Romania's greatest scientific personalities, a great physician, a visionary who put his whole life, intelligence and work power in the service of people and for the promotion of science, General (in retirement) Academician Professor Vasile CÂNDEA Ph.D., one of the parents of contemporary Romanian medicine, President of the Romanian Academy of Scientists and founder of the Army Emergency Clinical Center of Cardiovascular Diseases.
For us, it was a privilege to be contemporary with a scientist, a scholar, a Man like Vasile Cândea, with the Professor, the General, the Doctor, the Surgeon, the President, the Founder Vasile CÂNDEA, a Man who discovered the vocation of his existence in saving lives, working, studying, researching, in order to help and cure people.
Unfortunately, there are and were few such personalities, who managed to mix, at a higher level, professional, creative, scientific, managerial, relational and psycho-moral qualities, as Professor Cândea did. With a broad scientific and cultural horizon, with a comprehensive and profound understanding of man and his problems as a biological and social being, he made his voice heard in a constructive and creative sense as a great authority, not only in his professional activity - medicine, respectively, cardiology and cardio-vascular surgery, but also in the management positions of high responsibility that he exercised, without interruption, for more than four decades (1976-2017), in different national and international forums and institutions.
There would be much to say and even more to write about the strong impact of the personality of General Academician Prof. Vasile Cândea on society and especially on the destiny
of Romanian medicine, but for editorial economy reasons, we will mention only a few historical landmarks.
Doctor Vasile Cândea, as he used to characterize himself and liked to be called, making proof of diplomacy and elegance, humbleness and love towards those suffering and especially of the beauty, fairness and respect inscribed in the DNA of the Romanian village of Bărăgan spirit as it was described by the great author Marin Sorescu, in the novel “Moromeţii”, and additional to these, having an intact reputation, managed to cope both with the communist desert and with the difficult period of transition to democracy.
Professor Cândea started his activity in 1957 as a general practitioner and from April 1959 until October 1995 he worked in the Ministry of National Defense. At first he was a unit military physician from 1959-1962 (Timisoara, Constanta, Bucharest - Border Guard Command). Then he passed the clinical secondary exam - General Surgery 1962-1964 - Central Military Hospital of Bucharest, with the 3-month internship, Bucharest Emergency Clinic, Fundeni Urology Clinic in Bucharest, the Thoracic Surgery Clinic, then primary physician general surgery 1964-1972 - Surgery I Department from the Central Military Hospital, primary

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
75
physician cardiovascular surgery (second specialty) - 1976, doctor in medical sciences in 1975 - confirmed in 1976, Head of Cardiovascular Surgery Department in the Central Military Hospital - 1976-1990, Manager of the Army Cardiovascular Diseases Center - May 1990-1995, Manager of the Institute of Cardiovascular Diseases “Prof. Dr. C.C. Iliescu ", Fundeni Bucharest, December 1995-2002, November 1996 - December 2000, Deputy in the Romanian Parliament, founding member, University Professor and Vice-Rector at" Titu Maiorescu" University of Bucharest, 1990-2003, Honorary Professor at" Ovidius "University Constanta , Faculty of Medicine and Pharmacy, April 2000, Consultant Professor, 2003-2008, "Titu Maiorescu" University in Bucharest, Consultant Professor, 2005-2008, Carol Davila University of Medicine and Pharmacy Bucharest.
Specializing in France, Austria, Israel, USA, he became the father of military cardiac surgery in Romania, he received the academic recognition of several scientific and academic, national and international forums out of which we mention: Academy of Scientists in Romania (President of Honor); Academy of Medical Sciences (Head of the Surgical Specialties Section); Romanian Society of Cardiovascular Surgery (ex-president, founding member); Balkan Medical Union (President of the Romanian National Section, 1992-1993, international secretary general - 1993 - until 2020); Mediterranean Medical Antanta (International Secretary General from 1993-2020); National Academy of Ecological Sciences of the Republic of Moldova (1999); Russian Academy of Natural Sciences (since 2007); Balkan Society of Angiology and Vascular Surgery (vice president; founding member); Romanian Phlebology Society (founding member); Romanian Society of Vascular Surgery and Angiology (founding member); European Society of Cardiovascular Surgery; International Society of Cardiovascular Surgery "Michael E. Debakey" (since 1976, New York); International Society of Angiology; Society of Military Doctors and Pharmacists.
Throughout his prodigious career, Academician Vasile Cândea received the Award of the Romanian Academy “Dr. Gh. Marinescu ”, 1975, the distinction“ The Man of the Year 2000 ”, offered by the American Biographical Institute, the National Order the Romanian Star – Knight degree, December 2002, the distinction of the Honorary Committee of the Diplomats of the Superior School of War in Brazil and of the Embassy of Brazil, September 7, 2009, Order "Military Merit", classes 3, 2, 1 and multiple diplomas of excellence, distinctions, medals and plaques, offered by scientific research institutes, universities, official state institutions (Ministry of Defense, Ministry of Internal Affairs, Ministry of Health, Bucharest City Hall etc.)
In 2007, he has been awarded the title of "Citizen of honor" of the village where he was born - Viişoara in Teleorman county. In 2011 he received the title of Citizen of honor of the city of Mioveni – Argeş County.
His contribution and involvement in the academic world earned him the title of Doctor "Honoris Causa" of several universities, such as: University of Medicine and Pharmacy Timisoara; "Nicolae Testemitanu" State University of Medicine and Pharmacy of the Republic of Moldova; Ovidius University Constanta; Faculty of Medicine and Pharmacy; University of Oradea / Faculty of Medicine; "BIOTERRA" University; University of Medicine and Pharmacy Cluj Napoca; "Valahia" University Târgovişte; "Andrei Şaguna" University; National Defense University; "Apollonia" University, Iasi.
In the field of medicine, its name is linked to remarkable original contributions, with both national and international resonance, in the study and clinical-surgical treatment of cardiovascular diseases, lung, liver, pancreas and of the immune system.
Academician Professor Vasile CÂNDEA Ph.D. was a man with an exceptional moral standing and intellectual background, a true friend and a caring man who impressed many personalities and became the savior of thousands of lives. With each life saved he increased the nobility of the soul, he came closer to God, he became closer to his fellow human beings and, paradoxically, he became more humble and modest although, his personality is impressive and almost impossible to be described in a few words. He dedicated himself to others and gathered people around him, in the name of a common ideal: to dedicate his life to the rescue of other people lives. He set up and led research groups and surgical teams in difficult interventions which took hours, under the pressure of time. It happened more than often for him to be called in the middle of the night from home, because only him, the doctor Vasile CANDEA, was the guarantee and the hope that life will continue for the patient. He saved so many lives. So many people are still alive because the Good God has given this man, the grace and power to sacrifice himself for his fellow human beings.
More than two decades ago, Academician Professo Vasile CÂNDEA Ph.D. was a visionary of military medicine and not only of the latter, when he implemented, for the first time worldwide, an integrative solution for the problem of cardiovascular diseases, based on the idea of solving it in the format of a multidisciplinary team: clinical cardiology, interventional cardiology and cardiovascular surgery, since he was a promoter of teamwork.
Professor Cândea was the model and benchmark that we,

76
those who had the chance to work and complete our career beside his impressive personality, as well as the new generations that come, still need.
We, all those who have had the privilege to be touched, even tangentially, by the light of the personality of the General Academician Professor Dr. Vasile CÂNDEA, cannot and do not want to tell him "Goodbye", because the spirit and values he has promoted throughout his career, will continue to be a natural and motivating presence in our medico-military and scientific world, as they have been up to present, and his name will continue to protect our destinies, being written on the frontispiece of the Cardiovascular Diseases Center of the Central Military Emergency University Hospital "Dr. Carol Davila"(SUUMC), all the necessary steps have already been taken for that.
In a world riddled with the avalanche of information for which there is no time for verification and validation, in which forms without essence are promoted, we, those left behind, promise you doctor that we will not get lost along the difficult way to performance, that we will stay united to defend and to preserve your professional values and standards, so that the legacy you leave us, will be handed to future generations, with pious gratitude while remembering you.
We have the honor to greet you, General Academician Professor Vasile CÂNDEA! May our tears and grief illuminate your path to angels, where you belong!
Condolences to the bereaved family! God rest his soul!

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
77
ADMINISTRATIVE ISSUES
Guidelines for authors
Thank you for your interest in Romanian Journal of Military Medicine. Please read the complete Author Guidelines carefully prior to submission, including the section on copyright. To ensure fast peer review and publication, manuscripts that do not adhere to the following instructions will be returned to the corresponding author for technical revision before undergoing peer review. Note that submission implies that the content has not been published or submitted for publication elsewhere except as a brief abstract in the proceedings of a scientific meeting or symposium. Once you have prepared your submission in accordance with the Guidelines, manuscripts should be submitted online at [email protected]. We look forward to your submission.
EDITORIAL AND CONTENT CONSIDERATIONS Aims and Scope Romanian Journal of Military Medicine (RJMM) is the official journal of the Romanian Association of Military Physicians and Pharmacists. The Journal publishes peer-reviewed original papers, reviews, meta-analyses and systematic reviews, and editorials concerned with clinical practice and research in the fields of medicine. Papers cover the medical, surgical, radiological, pathological, biochemical, physiological, ethical and historical aspects of the subject areas. Clinical trials are afforded expedited publication if deemed suitable. RJMM also deals with the basic sciences and experimental work, particularly that with a clear relevance to disease mechanisms and new therapies. Case reports and letters to the Editor will not be considered for publication. Editorial Review and Acceptance The acceptance criteria for all papers and reviews are based on the quality and originality of the research and its clinical and scientific significance to our readership. All manuscripts are peer reviewed under the direction of an Editor. The Editor reserves the right to refuse any material for review that does not conform to the submission guidelines detailed throughout this document, including ethical issues, completion of an Exclusive License Form and stipulations as to length.
ETHICAL CONSIDERATIONS Principles for Publication of Research Involving Human Subjects Manuscripts must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the Declaration of Helsinki (as revised in Brazil 2013), available at http://www.wma.net/en/30publications/10policies/b3/index.html. It should also state clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under the study should be
omitted. Photographs need to be cropped sufficiently to prevent human subjects being recognized (or an eye bar should be used). Registration of Clinical Trials We strongly recommend, as a condition of consideration for publication, registration in a public trials registry. Trials register at or before the onset of patient enrolment. This policy applies to any clinical trial. We define a clinical trial as any research project that prospectively assigns human subjects to intervention or comparison groups to study the cause-and-effect relationship between a medical intervention and a health outcome. Studies designed for other purposes, such as to study pharmacokinetics or major toxicity (e.g., phase 1 trials) are exempt. We do not advocate one particular registry, but registration with a registry that meets the following minimum criteria: (1) Accessible to the public at no charge; (2) Searchable by standard, electronic (Internet-based) methods; (3) Open to all prospective registrants free of charge or at minimal cost; (4) Validates registered information; (5) Identifies trials with a unique number; and (6) includes information on the investigator(s), research question or hypothesis, methodology, intervention and comparisons, eligibility criteria, primary and secondary outcomes measured, date of registration, anticipated or actual start date, anticipated or actual date of last follow-up, target number of subjects, status (anticipated, ongoing or closed) and funding source(s). Plagiarism Detection The journal employs a plagiarism detection system. By submitting your manuscript to this journal you accept that your manuscript may be screened for plagiarism against previously published works. Committee on Publication Ethics The journal subscribes to the principles of the Committee on Publication Ethics (COPE).
MANUSCRIPT CATEGORIES AND SPECIFICATIONS All articles, with the exception of Editorials, must contain an abstract of no more than 250 words. Abstracts for original articles should be formatted into subheadings, as detailed below. Titles must not be longer than 120 characters (including spaces). Editorials These are invited by the Editor-in-Chief or their delegated editor, and should be a brief review of the subject concerned, with reference to and commentary about one or more articles published in the same issue of RJMM. Editorials are generally 1200–1500 words, may contain one table or figure and cite up to 15 references, including the source article [this should be cited as Military Med. Today (year); (vol): [this issue]. Review Articles RJMM welcomes reviews of important topics across the scientific basis of medicine, and advances in clinical practice. Most published

78
reviews are in response to editorial invitation, including thematically related “mini-series” of reviews. Authors considering submitting a review for RJMM are advised to canvas their possible review with the Editor-in-Chief or a colleague editor; this avoids early rejection if the subject matter is not deemed a high priority for the Journal at the time of submission. Reviews are limited to 3500–5000 words, with an abstract of up to 250 words and up to 75 references and 3–7 figures or tables. Meta-Analyses or Systematic Reviews RJMM particularly welcomes submission of Meta-Analyses and Systematic Reviews, which underpin evidence-based medicine. Guidelines for preparation of Meta-Analysis and Systematic Reviews are similar to other reviews, and articles are subject to the usual peer review process. Meta-Analyses and Systematic Reviews have a word limit of 3500–5000 words, with an abstract of up to 250 words and up to 75 references and 3–7 figures or tables. Original Articles (including clinical trials) RJMM welcomes original articles concerned with clinical practice and research in the fields of medicine. Papers can cover the medical, surgical, radiological, pathological, biochemical, physiological, ethical and/or historical aspects of the subject areas. Clinical trials are afforded expedited publication if deemed suitable. RJMM also deals with the basic sciences and experimental work, particularly that with a clear relevance to disease mechanisms and new therapies. Original articles are limited to 3000 words, with an abstract of up to 250 words and up to 50 references and 3–7 figures and tables. Education and Imaging The Editors welcome contributions to the Education and Imaging section. The purpose is to present imaging for the evaluation of unusual features of common conditions or diagnosis of unusual cases. Contributions will be reviewed by the Education and Imaging Coordinating Editors. The format of the Images pages involves two parts, each of which will occupy up to one journal page. In part 1, a case will be described briefly, including a summary of the presentation, clinical features and key laboratory results. One to two key images will then be presented. It is helpful to the reader if the author responds to questions that follow from the images of the case, such as ‘What is your diagnosis? What are the features indicated on the CT scan? What is the differential diagnosis?’ Part 2 will briefly describe the imaging features, particularly those that lead to diagnosis or which are critical for management. Differential diagnosis should be mentioned. It will be useful to include either further images or pathological details that validate the imaging diagnosis. Occasionally, presentation of analogous cases or related images from a similar case might be appropriate. Please include between one and three references to definitive studies and appropriate reviews of the subject. The format of the Images page involves a brief background to and description of the disorder of interest together with two figures of high quality. Colored photographs are encouraged. The submission may take the form of a case report or may illustrate particular features from more than one patient.
MANUSCRIPT PREPARATION Style Manuscripts should follow the style of the Vancouver agreement detailed in the International Committee of Medical Journal Editors’ revised ‘Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publication’, as presented at http://www.ICMJE.org/. Spelling. The journal uses US spelling and authors should therefore follow the latest edition of the Merriam-Webster’s Collegiate Dictionary. Units. All measurements must be given in SI units as outlined in the latest edition of Units, Symbols and Abbreviations: A Guide for
Biological and Medical Editors and Authors (Royal Society of Medicine Press, London). Abbreviations should be used sparingly and only where they ease the reader’s task by reducing repetition of long technical terms. Initially use the word in full, followed by the abbreviation in parentheses. Thereafter use the abbreviation. Trade names should not be used. Drugs should be referred to by their generic names, rather than brand names. Parts of the Manuscript The manuscript should be submitted in separate files: title page; main text file; figures. Title page The title page should contain (i) a short informative title that contains the major key words. The title should not contain abbreviations; (ii) the full names of the authors (if possible, not more than 5 authors per title); (iii) the author's institutional affiliations at which the work was carried out; (iv) the full postal and email address, plus telephone number, of the author to whom correspondence about the manuscript should be sent; (v) disclosure statement; and (vi) acknowledgements. The present address of any author, if different from that where the work was carried out, should be supplied in a footnote. Disclosure statement The source of financial grants and other funding should be acknowledged, including a frank declaration of the authors’ industrial links and affiliations. In the case of clinical trials or any article describing use of a commercial device, therapeutic substance or food must state whether there are any potential conflicts of interest for each of the authors: failure to make such a statement may jeopardize the article being sent out for peer-review. Acknowledgments The contribution of colleagues or institutions should also be acknowledged. Thanks to anonymous reviewers are not allowed. Main text As papers are double-blind peer reviewed the main text file should not include any information that might identify the authors. The main text of the manuscript should be presented in the following order: (i) abstract and key words, (ii) text, (iii) references, (iv) tables (each table complete with title and footnotes), (vii) figure legends. Figures and supporting information should be submitted as separate files. Footnotes to the text are not allowed and any such material should be incorporated into the text as parenthetical matter. Abstract and keywords Original articles must have a structured abstract that states in 250 words or less the purpose, basic procedures, main findings and principal conclusions of the study. Divide the abstract with the headings: Background and Aim, Methods, Results, Conclusions. The abstracts of reviews need not be structured. The abstract should not contain abbreviations or references. Three to five keywords should be supplied below the abstract and should be taken from those recommended by the US National Library of Medicine’s Medical Subject Headings (MeSH) browser—(http://www.nlm.nih.gov/ mesh/meshhome.html). Text Authors should use subheadings to divide the sections of their ma-nuscript: Introduction, Methods, Results, Discussion Acknowledg-ments and References. References The Vancouver system of referencing should be used. In the text, references should be cited using superscript Arabic numerals in the order in which they appear. If cited only in tables or figure legends, number them according to the first identification of the table or figure in the text. In the reference list, the references should be numbered and listed in order of appearance in the text. Cite the names of all authors when there are six or less; when seven or more list the first three followed by et al. Names of journals should be

Vol. CXXIII • No. 1/2020 • February • Romanian Journal of Military Medicine
79
abbreviated in the style used in MEDLINE. Reference to unpublished data and personal communications should appear in the text only. References should be listed in the following form: Number references in the order cited as Arabic numerals in parentheses on the line. Only literature that is published or in press (with the name of the publication known) may be numbered and listed; abstracts and letters to the editor may be cited, but they must be less than 3 years old and identified as such. Refer to only in the text, in parentheses, other material (manuscripts submitted, unpublished data, personal communications, and the like) as in the following example: (Chercheur X, unpublished data). If the owner of the unpublished data or personal communication is not an author of the manuscript under review, a signed statement is required verifying the accuracy of the attributed information and agreement to its publication. Use Index Medicus as the style guide for references and other journal abbreviations. List all authors up to six, using six and "et al." when the number is greater than six. Tables Tables should be self-contained and complement, but not duplicate, information contained in the text. Number tables consecutively in the text in Arabic numerals. Type tables on a separate page with the legend above. Legends should be concise but comprehensive – the table, legend and footnotes must be understandable without reference to the text. Vertical lines should not be used to separate columns. Column headings should be brief, with units of measurement in parentheses; all abbreviations must be defined in footnotes. Footnote symbols: †, ‡, §, ¶ should be used (in that order) and *, **, *** should be reserved for P-values. Statistical measures such as SD or SEM should be identified in the headings. Figure legends Type figure legends on a separate page. Legends should be concise but comprehensive – the figure and its legend must be understandable without reference to the text. Include definitions of any symbols used and define/explain all abbreviations and units of measurement Indicate the stains used in histopathology. Identify statistical measures of variation, such as standard deviation and standard error of the mean. Figures All illustrations (line drawings and photographs) are classified as figures. Figures should be numbered using Arabic numerals, and cited in consecutive order in the text. Each figure should be supplied as a separate file, with the figure number incorporated in the file name. Preparation of Electronic Figures for Publication: Although low quality images are adequate for review purposes, publication requires high quality images to prevent the final product being blurred or fuzzy.
SUBMISSION REQUIREMENTS Manuscripts should be submitted online at [email protected] A cover letter containing an authorship statement should be included. The cover letter should include a statement covering each of the following areas: 1. Confirmation that all authors have contributed to and agreed on the content of the manuscript, and the respective roles of each author. 2. Confirmation that the manuscript has not been published previously, in any language, in whole or in part, and is not currently under consideration elsewhere. 3. A statement outlining how ethical clearance has been obtained for the research, particularly in relation to studies involving human subjects, and animal experimentation. The institutional ethics committees approving this research must comply with acceptable international standards (such as the Declaration of Helsinki) and this must be stated.
4. For research involving pharmacological agents, devices or medical technology, a clear Conflict of Interest statement in relation to any funding from or pecuniary interests in companies that could be perceived as a potential conflict of interest in the outcome of the research. 5. For clinical trials, that these have been registered in a publically accessible database. If the above items are not included in the cover letter, manuscripts cannot be sent for review. Please also note that the cover letter does not require a detailed or lengthy description of the content or structure of the manuscript itself. Two Word-files need to be included upon submission: A title page file and a main text file that includes all parts of the text in the sequence indicated in the section 'Parts of the manuscript', including tables and figure legends but excluding figures which should be supplied separately. The main text file should be prepared using Microsoft Word, doubled-spaced. The top, bottom and side margins should be 30 mm. All pages should be numbered consecutively in the top right-hand corner, beginning with the first page of the main text file. Each figure should be supplied as a separate file, with the figure number incorporated in the file name. For submission, low-resolution figures saved as .jpg or .bmp files should be uploaded, for ease of transmission during the review process. Upon acceptance of the article, high-resolution figures (at least 300 d.p.i.) saved as .eps or .tif files will be required.
PUBLICATION PROCESS AFTER ACCEPTANCE Accepted papers will be passed to production team for publication. The author identified as the formal corresponding author for the paper will receive an email, being asked to complete an electronic license agreement on behalf of all authors on the paper. Accepted Articles The accepted ‘in press’ manuscripts are published online very soon after acceptance, prior to copy-editing or typesetting. Accepted Articles are published online a few days after final acceptance, appear in PDF format only, are given a Digital Object Identifier (DOI), which allows them to be cited and tracked. After print publication, the DOI remains valid and can continue to be used to cite and access the article. Given that copyright licensing is a condition of publication, a completed copyright form is required before a manuscript can be processed as an Accepted Article. Proofs Once the paper has been typeset, the corresponding author will receive an e-mail alert containing instructions on how to provide proof corrections to the article. It is therefore essential that a working e-mail address is provided for the corresponding author. Proofs should be corrected carefully; the responsibility for detecting errors lies with the author. The proof should be checked, and approval to publish the article should be emailed to the Publisher by the date indicated; otherwise, it may be signed off on by the Editor or held over to the next issue. Offprint A PDF reprint of the article will be supplied free of charge to the corresponding author. Additional printed offprint may be ordered for a fee.
COPYRIGHT, LICENSING AND ONLINE OPEN Details are on the Copyright Agreement Form that must be completed and signed when the Article is accepted.

80


New Series, Vol. CXXIII, No 1/2020, February ISSN-L 1222-5126; eISSN 2501-2312; pISSN 1222-5126