
Right Ventricular Injury in ST-Elevation Myocardial Infarction: Risk Stratification by Visualization...
31
1942-0080 American Heart Association. All rights reserved. Print ISSN: 1941-9651. Online ISSN: 2011 Copyright © Dallas, TX 72514 Circulation: Cardiovascular Imaging is published by the American Heart Association. 7272 Greenville Avenue, DOI: 10.1161/CIRCIMAGING.111.967810 published online November 11, 2011; Circ Cardiovasc Imaging Gutberlet Suzanne de Waha, Steffen Desch, Ingo Eitel, Meinhard Mende, Holger Thiele and Matthias Matthias Grothoff, Christian Elpert, Janine Hoffmann, Johannes Zachrau, Lukas Lehmkuhl, Resonance Visualization of Wall Motion, Edema and Delayed Enhancement Cardiac Magnetic Right Ventricular Injury in ST-Elevation Myocardial Infarction: Risk Stratification by World Wide Web at: The online version of this article, along with updated information and services, is located on the initial publication. Advance online articles must include the digital object identifier (DOIs) and date of publication priority; they are indexed by PubMed from initial publication. Citations to available prior to final publication). Advance online articles are citable and establish not yet appeared in the paper journal (edited, typeset versions may be posted when Advance online articles have been peer reviewed and accepted for publication but have http://www.lww.com/reprints Reprints: Information about reprints can be found online at [email protected] 351 West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax: 410-528-8550. E-mail: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer Health, http://circimaging.ahajournals.org/site/subscriptions/ Subscriptions: Information about subscribing to Circulation: Cardiovascular Imaging is online at by guest on February 21, 2013 circimaging.ahajournals.org Downloaded from
-
Upload
uniklinikum-leipzig -
Category
Documents
-
view
4 -
download
0
Transcript of Right Ventricular Injury in ST-Elevation Myocardial Infarction: Risk Stratification by Visualization...

1942-0080American Heart Association. All rights reserved. Print ISSN: 1941-9651. Online ISSN: 2011 Copyright ©
Dallas, TX 72514Circulation: Cardiovascular Imaging is published by the American Heart Association. 7272 Greenville Avenue,
DOI: 10.1161/CIRCIMAGING.111.967810 published online November 11, 2011;Circ Cardiovasc Imaging
GutberletSuzanne de Waha, Steffen Desch, Ingo Eitel, Meinhard Mende, Holger Thiele and Matthias Matthias Grothoff, Christian Elpert, Janine Hoffmann, Johannes Zachrau, Lukas Lehmkuhl,
ResonanceVisualization of Wall Motion, Edema and Delayed Enhancement Cardiac Magnetic
Right Ventricular Injury in ST-Elevation Myocardial Infarction: Risk Stratification by
World Wide Web at:
The online version of this article, along with updated information and services, is located on the
initial publication. Advance online articles must include the digital object identifier (DOIs) and date ofpublication priority; they are indexed by PubMed from initial publication. Citations to available prior to final publication). Advance online articles are citable and establishnot yet appeared in the paper journal (edited, typeset versions may be posted when Advance online articles have been peer reviewed and accepted for publication but have
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected] West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax: 410-528-8550. E-mail:Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer Health,
http://circimaging.ahajournals.org/site/subscriptions/Subscriptions: Information about subscribing to Circulation: Cardiovascular Imaging is online at
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Right Ventricular Injury in ST-Elevation Myocardial Infarction:
Risk Stratification by Visualization of Wall Motion, Edema and Delayed
Enhancement Cardiac Magnetic Resonance Grothoff et al: Right Ventricular Injury in CMR
Matthias Grothoff¹, MD; Christian Elpert¹, BSc; Janine Hoffmann¹, MD;
Johannes Zachrau², BSc; Lukas Lehmkuhl¹, MD; Suzanne de Waha², MD;
Steffen Desch², MD; Ingo Eitel², MD; Meinhard Mende³, PhD;
Holger Thiele²*, MD; Matthias Gutberlet¹*, MD
The first three authors contributed equally to this work
*H.T. and M.G. should be both considered as senior authors
¹Department of Radiology, University of Leipzig – Heart Center, Germany
²Department of Cardiology, University of Leipzig – Heart Center, Germany
³Clinical Trial Centre – University of Leipzig, Germany
Correspondence to: Matthias Grothoff, MD Department of Diagnostic and Interventional Radiology University of Leipzig, Heart Center Strümpellstr. 39 04289 Leipzig, Germany Tel.: +49-341-865-1702 Fax: +49-341-865-1803 E-mail: [email protected]
Journal Subject Codes: Acute myocardial infarction, CT and MRI, Catheter-based coronary
interventions: stents
GRadiology, University of Leipzig Heart Center, Germany
C
e
Radiology, University of Leipzig Heart Center, Germany
Cardiology, University of Leipzig – Heart Center, Germany
entre – University of Leipzig, Germany
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Abstract Background Patients with right ventricular injury (RVI) complicating ST-elevation
myocardial infarction (STEMI) suffer from impaired prognosis, but it is unclear which
patients are at risk of developing RVI. Cardiac magnetic resonance (CMR) can identify these
patients and might add important information on risk stratification, prognosis and treatment.
Aims were to determine the predictors and the prognostic significance of RVI assessed by
wall motion abnormalities, edema, myocardial-salvage-index (MSI) and delayed enhancement
(DE) in acute reperfused STEMI.
Methods and Results We studied 450 patients 1-4 days after primary angioplasty in
STEMI. T2-weighted and DE CMR was used for visualizing edema and scar to calculate
MSI. Cine-imaging was performed to assess wall motion abnormalities, which, in
combination with edema, were considered diagnostic for RVI. Patients with RVI were
compared to matched patients with isolated left ventricular (LV) infarction. The primary
endpoint was the occurrence of a major adverse cardiac event (MACE): a composite of death,
reinfarction and congestive heart failure after a median follow-up period of 20.9 months. RVI
was present in 69 patients and 41/69 showed myocardial necrosis. In a multivariable stepwise
forward logistic regression analysis a high RV myocardial mass (Odds-Ratio 2.06, 95%
Confidence-Interval 1.18-3.58, p=0.012) and a low TIMI-flow pre angioplasty (Odds-Ratio
0.50, 95% CI 0.32-0.76, p=0.011) were associated with RVI. Cox regression analysis
revealed RVI as the most statistically significant predictor of time to MACE (Hazard-Ratio
3.36, 95% CI 1.99-5.66, p<0.001).
Conclusions RVI detected by CMR is a strong and independent predictor of clinical
outcome after acute reperfused STEMI.
Clinical Trial Registration URL: http://www.clinicaltrials.gov. Unique identifier:
NCT01359306.
Key Words: acute myocardial infarction; cardiac magnetic resonance imaging; right ventricle
infarction; myocardial salvage; prognosis
on abnormalitittttieieieieieieies
VI. P PPPPPPatatatatatatatieieieieieieientntntntntntnts s s wiwiwiwiwiwiwi
tched patients with isolated left ventricular (LV) infarction.
occurrence of a major adverse cardiac event (MACE): a com o
c
9 tients and 41/69 showed ocardial necrosis. In a multivari
regression analysis a high RV myocardial mass (Odds-Rati
tched patients with isolated left ventricular (LV) infarction.
occurrence of a major adverse cardiac event (MACE): a compo
congestive heart failure after a median follow-up period of 20.9
9 patients and 41/69 showed myocardial necrosis. In a multivari
regression analysis a high RV myocardial mass (Odds-Rati
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Right ventricular injury (RVI) in ST-elevation myocardial infarction (STEMI) can cause
severe hemodynamic derangements and is associated with increased mortality and morbidity
(1). Owing to the right ventricular (RV) volume pump characteristics, RVI with
hemodynamic compromise requires a specific treatment (2). Hence, for optimizing
therapeutic strategies an early and accurate diagnosis is mandatory.
In necropsy studies RVI can be found in up to 50% of patients with inferior STEMI (3). In
clinical routine, however, RVI is diagnosed by echocardiography, electrocardiography and
clinical findings and detection rates show a wide range depending on the population and
diagnostic criteria used (2).
Cardiac magnetic resonance (CMR) emerged as a powerful tool in visualizing myocardial
injury after left ventricular (LV) STEMI. High signal intensity in T2-weighted imaging
visualizes myocardial edema representing myocardium at risk (4) and delayed enhancement
(DE) indicates myocardial necrosis (5). Comparing the extent of reversible to irreversible
injured myocardium allows for calculation of myocardial salvage or myocardial salvage index
(MSI), which to maximize is the goal of reperfusion because of its prognostic impact (6).
Recently, CMR has been also introduced for detection and visualization of RVI. Previous
studies demonstrated that early postinfarction RVI is common and is characterized by the
presence of myocardial edema, DE and functional abnormalities (7). However, to date, there
is no systematic evaluation of the clinical prognostic value of RVI assessed by CMR in a
large STEMI population.
The aim of this study was to investigate the predictors for RVI development and its prognostic
impact after reperfused STEMI. A secondary objective was to evaluate the utility and clinical
value of RV MSI assessment in a large STEMI cohort.
ooooooooooooool l l l l l l ininininininin v v vv v vvisisisisisisisuauauauauauaualililililililizizizizizizizinnnnnnn
sity ininininininin TTTTTTT2-2-2-2-2-2-2-weweweweweweweigiigii h
a
myocardial necrosis . Comparing the extent of reversible
um allows for calculation of m cardial salv e or m cardial
ardial edema representing myocardium at risk (4) and delayed
myocardial necrosis (5). Comparing the extent of reversible t
um allows for calculation of myocardial salvage or myocardial
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Methods
Patient population and study design
Primary angioplasty was performed in 524 consecutive patients with STEMI at our tertiary
care institution. Of these, 450 patients were referred to CMR 24-96 h after the index event.
Eligibility criteria were the onset of symptoms <12 h before angioplasty and ST-segment
elevation of >0.1 mV in 2 extremity leads or >0.2 mV in 2 precordial leads. Exclusion
criteria were usual CMR contraindications such as implanted defibrillators/pacemakers and
ferromagnetic intracranial metallic implants.
After physical examination and assessment of medical history the TIMI-risk score was
calculated for each patient (8). We conducted follow-up by a standardized telephone
questionnaire after a median follow-up period of 20.9 months (range 4.7 to 39.0 months). The
interviewers were blinded to the CMR results. Reported adverse events were verified by
hospital or out-patient documentation.
Some of the patients included in this prospective analysis have been included in randomised
trials published previously (6,9,10). The study was approved by the local ethics committee
and complies with the Declaration of Helsinki. All patients gave written informed consent.
Primary angioplasty, angiographic analysis and subsequent treatment
Intravenous application of 500 mg aspirin and 60 IU/kg bodyweight heparin was performed in
all patients prior to angioplasty. Clopidogrel with a 600 mg loading dose was given orally at
the earliest time point followed by daily administration of 75 mg for 12 months plus 100 mg
aspirin indefinitely. According to current guidelines glycoprotein IIb/IIIa inhibitors,
angiotensin-converting-enzyme-inhibitors, beta-blockers, and statins were administered (11).
Primary angioplasty was performed according to standard clinical practice. In case of a high
thrombus burden additional thrombectomy was conducted. Before and after angioplasty
coronary angiography was performed with the same projections. Post TIMI-flow was
bybybybybybyby a a aa a a a s sssssstatatatatatatandndndndndndndararararararardididididididizzzzzzz
angeeeeeee 4444444 7777777 tototototototo 33333339999999 00000
r
a
ents included in this os ctive anal is have been included n
e blinded to the CMR results. Reported adverse events wer
atient documentation.
ents included in this prospective analysis have been included in
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

categorized as: TIMI-flow III – reperfusion success; TIMI-flow 0-II –no reperfusion success.
Angiographic visual analysis was performed offline by two blinded observers.
ST-segment resolution and enzymatic infarct size analysis
Early ST-segment resolution was evaluated by measuring the sum of ST-segment elevation
before and approximately 90 minutes after angioplasty in a standard 12-lead ECG and
expressed as percentage. Data was also categorized as complete ( 70%), partial (<70-30%),
and no ST-segment resolution (<30%). The number of leads with ST-segment elevation was
obtained. Plasma creatine kinase and creatine kinase-myocardial band were assessed on
admission and subsequently for every 8 h for 2 days.
Cardiac magnetic resonance imaging
All CMR examinations were performed on a 1.5 Tesla scanner (Intera CV, Philips Medical
Systems, Best, The Netherlands). The scan protocol and technical parameters have been
described in detail previously (6). In brief, cine steady-state-free-precession sequences in
short-axis- and horizontal and vertical long-axis orientation were acquired for volumetric and
functional imaging. Visualization of myocardial edema was performed using a black-blood
T2-weighted short inversion time turbo-spin-echo sequence in short-axis orientation. DE
images, also covering both ventricles in short-axis orientation, were acquired for
quantification of necrosis and microvascular obstruction (MO) 10–15 minutes after
application of 0.15 mmol/kg/bodyweight gadobutrol (Gadovist, BayerSchering, Germany)
using a three-dimension T1-weighted inversion recovery turbo gradient echo sequence.
Inversion time for optimal nulling of RV and LV myocardium was individually optimized
within a range of 200–300 ms.
c
nations were performed on a 1.5 Tesla scanner Intera CV, Ph
The Netherlands The scan otocol and technical aramet
c resonance imaging
nations were performed on a 1.5 Tesla scanner (Intera CV, Ph
The Netherlands). The scan protocol and technical paramete
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

CMR image analysis was performed by fully blinded observers on an independent
workstation in the CMR core laboratory, which has proven low intra- and interobserver
variability as well as reproducibility for assessment of infarct size, MSI and MO (9).
Biventricular volumes and function were determined by manually tracing endocardial and
epicardial borders in end-systole and end-diastole. Biventricular myocardial masses were
calculated on cine images in end-diastole. In T2-weighted images and in the corresponding
DE images the area of high signal intensity was manually delineated in each short-axis slice.
For RV edema assessment, signal intensity of LV edema was taken as reference and slices
were compared to short-axis cine images as described previously (7). MO was included into
infarct size and additionally assessed in a separate fashion. Patients with non-diagnostic image
quality of the RV myocardium were excluded from further analysis. Right ventricular regional
wall motion abnormalities were assessed qualitatively and classified as dyskinesia, akinesia,
or hypokinesia.Wall motion impairment in combination with edema was considered as being
diagnostic for RVI.
The following parameters were calculated for both the RV and LV:
- end-diastolic, end-systolic, stroke-volume index and myocardial mass index (related to body
surface area)
- ejection fraction
- %area at risk=volume edema/ventricular mass
- %infarct size=volume infarct/ventricular mass
- %MO=volume MO/ventricular mass
- MSI=area at risk–infarct size/area at risk
For comparison every patient with RVI was matched without replacement to a patient with
isolated LV infarction with the same vessel (RCA, LAD or LCX), and, where possible, with
the same vessel segment (proximal, mid, distal). Furthermore age (±3 years) and sex were
matched. Isolated LV infarction was defined by CMR absence of RVI (Table 1).
nnnnnnntststststststs w wwwww wititititititith h h h h h h nononononononon-n-n-n-n-n-n-dididididididiagagagagagagag
ysis RiRiRiRiRiRiRighghghghghghghttttttt vvvvvvvenenenenenenentrtrtrtrtrtt ic
o e
Wall motion impairment in combination with edema was cons d
V
ormalities were assessed qualitatively and classified as dyskine
Wall motion impairment in combination with edema was consid
VI.
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Endpoints
The primary endpoint of this study was the occurrence of major adverse cardiac event
(MACE), a composite of death, reinfarction and new congestive heart failure. Secondary
endpoints were the individual components of the primary endpoint.
At index hospitalization reinfarction was diagnosed based on clinical symptoms, new ST-
segment changes and an increase in the creatine kinase-myocardial band levels as previously
described (12). During follow-up any new ischemic symptoms leading to hospital admission
in combination with troponin elevation were defined as recurrent infarction. Congestive heart
failure was diagnosed in case of rales and dyspnea (New York Heart Association class III-IV)
occurring >24 h after the index and requiring medical attention. In case of more than one
event, the first event was chosen for the combined clinical endpoint. When 2 events occurred
simultaneously, the most severe event was chosen (death>myocardial reinfarction>congestive
heart failure).
Statistical Analysis
Categorical variables are expressed as number and percentage. Normally distributed variables
are presented as mean ± SD, non-normally distributed variables are given as median [25%,
75% percentile]. Differences between groups were assessed by the student’s t-test for
continuous data with normal distribution and homogeneity of variance. The Wilcoxon rank-
sum test was used for continuous not normally distributed data or for continuous data without
homogeneity of variance. Differences between categorical variables were assessed either by
the Chi-Square or Fisher‘s exact test. Differences between related continuous variables were
tested using the paired t-test or the Wilcoxon signed-rank depending on their distribution.
Univariate and multivariable conditional binary logistic regression analyses were performed
to find factors associated with RVI. This method accounts for the matched-pair nature of the
HeHeHeHeHeHeHeararararararart tt t t tt AsAsAsAsAsAsAssososososososocicicicicicciatatatatatatatioioioioioioionnnnnnn
on IIIIIIInnnnnnn cacacacacacacasesesesesesese ooooooofffffff mm
v v
h o
vent was chosen for the combined clinical endpoint. When 2 ev
he most severe event was chosen (death>myocardial reinfarctio
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

sample. Categorical variables included Killip-class on admission, categorized TIMI-flow after
angioplasty and categorized ST-segment resolution. Continuous variables included pain-to-
balloon time, biventricular myocardial mass index, LV area at risk, LV infarct size, LV MSI,
peak creatine kinase, peak creatine kinase-myocardial band, number of leads with ST-segment
elevation, sum of ST-segment elevation, mean blood pressure,heart rate and TIMI-risk score
as quasi continuous. A stepwise forward regression procedure was performed to select
variables into multivariable models.
The Kaplan-Meier method was applied for the combined clinical endpoint and death;
differences were assessed by the log-rank test. To identify possible predictors of MACE
univariate Cox-regression analyses were performed using CMR parameters and traditional
prognostic factors. A multivariable stepwise forward Cox regression analysis took only three
of the significant variables into the model. Including matched-pairs as strata accounted for the
paired structure of the data. The tests were performed as two-sided at significance level
=0.05. For statistical analyses the SPSS software, version 16.0 (SPSS Inc., Chicago, Il,
USA) was used.
Results
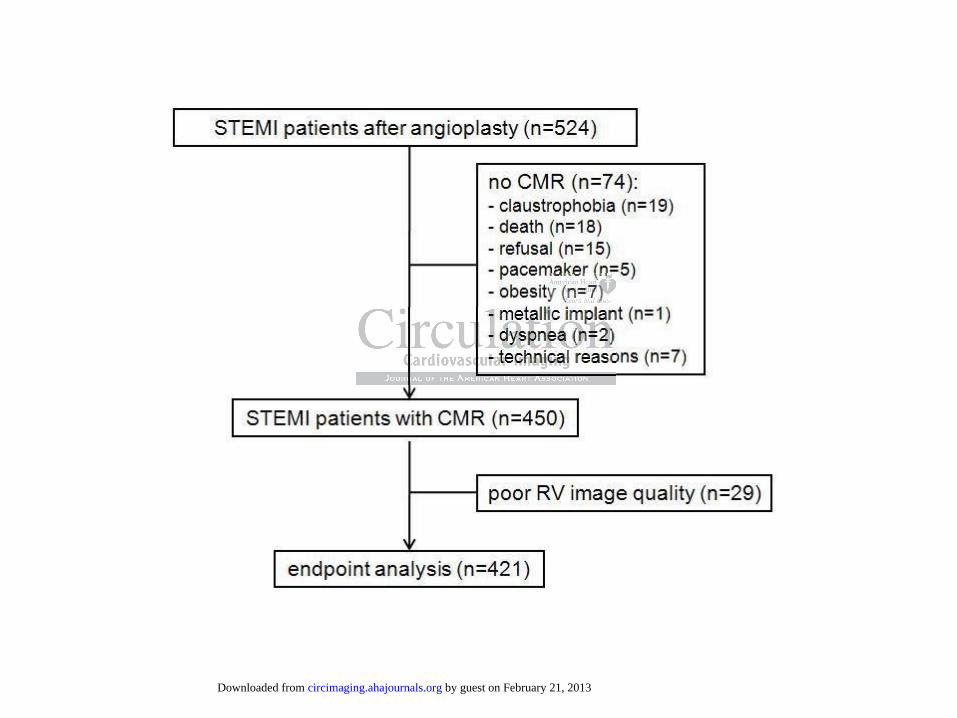
Of 524 STEMI patients undergoing primary angioplasty, 450 were referred to CMR 24-96 h
after reperfusion. Reasons for not undergoing CMR are listed in Figure 1. Image quality for
RV edema quantification was inappropriate in 29 (6.4%) patients; 7 patients were lost to
follow-up. In 414 patients clinical outcome data were available.
Right ventricular injury
RVI as defined by a combination of myocardial edema (Figure 2) and local wall motion
impairment occurred in 69 out of 421 patients (16.4%). Of these 69 patients, 54 (78%)
presented with hypokinesia and 15 (22%) with akinesia. None of the patients showed RV
MRMRMRMRRRR p p pp p p parararararararamamamamamamametetetetetetetererererererers ss s s ss anananananana
ssionnnnnnn anananananananalalalalalalalysysysysysysysisisisisisisis ttttto
o
i
i ,
variables into the model. Including matched-pairs as strata acco
of the data. The tests were performed as two-sided at signi
istical analyses the SPSS software, version 16.0 (SPSStt Inc.,
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

edema without local wall motion abnormalities in the same region. In 41 of these patients
(59.4%) RV myocardial necrosis was detected in DE imaging. RV MO was present in only
one patient (Figure 3). Distribution of the culprit lesion is shown in Table 1. Patients with a
lesion in the left circumflex had a left dominant coronary circulation and a lateral to inferior
injury of the left ventricular myocardium, extending to the inferior wall of the right ventricle.
Baseline characteristics of the entire patient cohort, RVI patients and the matched control-
group are presented in Table 1. RVI patients had a significantly higher RV myocardial mass
index compared to the non-RVI group. These patients also presented with a significantly
longer pain-to-balloon time and a lower LV MSI. Within the RVI-group the number of
patients with 100% myocardial salvage (RV MSI=1) was high (28/69; 40.6%), resulting in
significantly higher mean RV MSI (0.80±0.2) as compared to the mean LV MSI (0.47±0.2;
p<0.01). Furthermore, patients with RVI showed a significantly lower ST-segment resolution
and a lower RV ejection fraction (Table 1).
Predictors of RVI
In a multivariable stepwise forward regression model adjusted for significant variables in
univariate regression analysis using RVI as the dependent variable a low TIMI-flow pre
angioplasty was a predictor of RVI (Table 2). Also RV myocardial mass index was related to
RVI. Pain-to-balloon time was associated with RVI in the univariate analysis but failed to
predict RVI in the multivariable model. The sum of ST-segment elevation and the number of
leads with ST-segment elevation were not related to RVI.
Prognostic impact of RVI
MACE occurred in 73/421 patients (17.3%). Most MACE with 22/69 (31.9%) occurred in
patients with RVI compared with 5/69 (7.3%) in the matched non-RVI group. There were 8
h h h h h h (2(2(2(2(2(2(28/8/8/8/8/8/8/69696969696969; ; ; ; ; 40404040404040.6.6.6.6.6.6.6%)%)%)%)%)%)%)
the mmmmmmmeaeaeaeaeaeaeannnnnnn LVLVLVLVLVLVLV MMMMM
m
e
more, patients with RVI showed a significantly lower ST-segm
ejection fraction (Table 1).
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

deaths, 6 non-fatal reinfarctions and 8 cases of new congestive heart failure in patients with
RVI as opposed to 3 deaths and 2 non-fatal reinfarctions in the matched non-RVI patients.
Within the RVI-group patients with MACE demonstrated with greater RV area at risk (23.2%
[15.3, 34.7] vs. 18.2% [10.0, 27.9]; p=0.047), a greater RV infarct size (8.7% [5.2, 11.7] vs.
0% [0, 3.9]; p<0.001) and a lower RV MSI (0.61 [0.57, 0.75] vs. 1.00 [0.81, 1.00]; p<0.001)
compared to RVI patients without MACE.
Kaplan-Meier estimates illustrated reduced periods of MACE-free survival and higher
mortality in patients with RVI compared to the matched non-RVI group (Figure 4 a & b).
These results were confirmed when the analysis was repeated with LV EF categorized for the
presence or absence of severe LV dysfunction (LV EF / >40%) used as stratum. Log-rank
tests pooled over these strata were both significant (MACE: p<0.001, mortality: p=0.036)
demonstrating the prognostic value of RVI independent of LV dysfunction. Within the RVI-
group patients with RV MSI=1 had a better prognosis than patients with MSI<1 (Figure 5 a &
b). Furthermore prognosis of patients with RV MSI=1was not different from patients with
isolated LV infarction (p=0.70).
Analyzing the entire patient group, RVI remained associated with MACE in the univariate
Cox-regression analysis but also other established markers of increased patient risk
demonstrated significant associations with MACE (Table 3). However, in a multivariable Cox
regression, RVI together with LV ejection fraction and TIMI-risk score remained the only
independent predictors for occurrence of MACE. In the subgroup of patients with RVI plus
matched non-RVI patients (n=138) RVI showed association with the combined endpoint in
univariate (HR 6.74, 95%CI [2.32-19.59]) and multivariable (HR 5.5, 95%CI [1.71-14.94])
Cox regression analysis.
%)%)%)%)%)%)%) u uuuuu usesesesesesesed d d d ddd asasasasasasas s s s s s sstrtrtrtrtrtrtratatatatatatatuuuuuuu
p<0000 000000000000001111111 mmmmmmmororororororortatatatatatt l
e
i
p nosis of atients with RV MSI=1was not different from
e prognostic value of RVI independent of LV dysfunction. Wi
ith RV MSI=1 had a better prognosis than patients with MSI<1
prognosis of patients with RV MSI=1was not different from
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Discussion
To the best of our knowledge this is the first CMR study to evaluate the prognostic impact of
RV area at risk as measured with edema sensitive T2-weighted images and infarct size by
using DE in a large group of reperfused STEMI patients. The results might be summarized as
follows: 1) RVI with DE is a strong independent prognostic marker of long-term prognosis
after STEMI; 2) Similar to isolated LV infarction, RV area at risk, infarct size, and MO can
also be calculated; 3) RVI is associated with a low LV MSI, an impaired ST-segment
resolution and a high RV mass index; 4) RVI defined by regional RV edema and wall motion
impairment or right-sided infarction can be found in approximately 17% of STEMI patients
after mechanical reperfusion.
Assessment of RV area at risk, infarct size and MO
The concept of myocardial salvage calculated by the area at risk in T2-weighted images and
the infarct size in DE images is increasingly used for the assessment of reperfusion therapy in
LV infarction (6,13). Whereas a few studies showed the applicability for DE of the RV (7,14)
only limited studies evaluated the RV area at risk (7).
Our study clearly demonstrates that RV area at risk, visualized by T2-weighted imaging, can
be quantified in the majority of patients with RVI. Consequently, RV-MSI can be calculated
with significantly higher MSI values compared to the LV (15). As shown by our data, a
substantial number of patients reaches major or even complete salvage of the RV area at risk.
Such a high incidence of aborted RV infarctions is in line with a recent publication (7) and
may be explained by the lower oxygen demand and the dual anatomic supply system of the
RV myocardium making it less vulnerable to ischemia. Our findings in part underline a
previous thesis assuming that acute right ischemic dysfunction represents viable myocardium
(16). Nevertheless, ischemic scarring also exists in the RV myocardium, probably too small to
cause sustained impairment of global RV function in the majority of cases. According to the
V
myocardial salvage calculated by the area at risk in T2-wei e
n DE ima s is increasin used for the assessment of r erfu i
V area at risk, infarct size and MO
myocardial salvage calculated by the area at risk in T2-weighte
n DE images is increasingly used for the assessment of reperfusi
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

lower degree of RV scarring, right-sided MO is a very rare finding after acute reperfused
STEMI and was found in only one out of 421 patients. Further studies with large patient
cohorts might be necessary to assess the incidence and potentially the prognostic impact of
RV MO.
Predictors of RVI
RVI typically occurs with infarction of the LV inferior wall. In the present study population
the culprit lesion was located in most patients (84%) in the right coronary artery, mainly in the
proximal and mid segments. Additionally, we were able to identify a low TIMI-flow pre
angioplasty as a furtherparameter associated with RVI. Patients with RVI also demonstrated
with an increased RV myocardial mass index.
Only one patient in the RVI group suffered from severe pulmonary hypertension as a reason
of RV hypertrophy. Two more patients in this group demonstrated with mild pulmonary
hypertension and an RV myocardial mass within the upper normal range. An increased
oxygen demand in high RV mass might result in injury of the RV myocardium which would
confirm the results of non-imaging studies (17-19). These studies in part also report necropsy
data of chronic RV infarctions in which edema can be excluded. On the other hand there are
studies reporting an increase of LV myocardial mass caused by edema (20) and swelling of
the thin compacted layer of RV myocytes might also result in an increase of measured RV
myocardial mass. Actually we assessed RV myocardial mass after infarction and certainly
included a substantial amount of RV edema in the calculation of myocardial mass. Thus, it is
most likely that increased RV mass is the result rather than the cause of RVI.
s s s s s s wiwiwiwiwiwiwiththththththth R R RR R RRVIVIVIVIVIVIVI a a a a a a alslslslslslslso o ooo oo
in the RVI ou suffered from severe ulmona h ertens o
p l
d an RV m cardial mass within the r normal ran . A
in the RVI group suffered from severe pulmonary hypertensio
phy. Two more patients in this group demonstrated with mil
d an RV myocardial mass within the upper normal range. A
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Comparison with recent studies
Compared to other studies assessing RVI in STEMI, the percentage of RVI was lower in our
larger consecutive patient group with approximately 17%. Kumar et al. found RV DE in 57%
of patients with inferior infarction and a mean pain-to-balloon time of 8.8±5.4 h (21). This
difference might be explained by the shorter pain-to-balloon time in our patient group with a
median of only 211 minutes. Masci et al. also presented a higher percentage of RV edema
with 51% and RV DE with 31% (7), but again in this study, the pain-to balloon-time was
longer (252±134 minutes for RVI patients, 270±166 minutes for non-RVI patients) compared
with the current cohort. One discrepancy in the assessment of RV edema was the use of the
integrated body coil in the current approach, whereas Masci et al. used surface coils with a
correction algorithm to homogenize signal. However, it is unlikely that this accounts for the
significant difference in the occurrence of RV edema. Other parameters were comparable
between Masci et al. and the present study: In both the RCA was identified as the infarct
related artery in 43% and also the distribution of the affected RCA segments were similar.
In a recent study Francone et al. reported on the influence of time to reperfusion on
myocardial injury assessed by CMR after STEMI with primary angioplasty (22). The authors
found that the extend of myocardial edema did not change significantly as pain-to-balloon
time progressed. This is in contradiction to our results, which show an association of pain-to-
balloon time to the occurrence of RVI defined by edema. However, Francone et al. report on
LVs and our findings relate to RVs. Owing to the better collateralization of the RV the
oxygen supply of the myocardium might be initially sufficient for not developing edema.
Prognostic impact of RVI
Our study clearly demonstrates the prognostic impact of RVI in a large group of reperfused
STEMI patients when no complete myocardial salvage can be achieved. This is in line with
two recent studies, which found RV edema being a prognostic factor for RV function
ttt a a a aaaal.l.l.l.l.l. u u u u uu usesesesesesesed d d d d d d sususususususurfrfrfrfrfrfrfacacacacacacaceeeeeee
kelyyy ttttttthahahahahahahatttttt thththththththisisisisisisis aaaaaaacccccc
e
et al. and the present stu : In both the RCA was identified
4 r
ence in the occurrence of RV edema. Other parameters were
et al. and the present study: In both the RCA was identified
43% and also the distribution of the affected RCA segments wer
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

recovery at follow-up (7, 23). However, in one of these studies no clinical follow-up data was
reported (7) and the other study included only “soft” clinical endpoints such as recurrent
angina and repeated revascularization. A recent study demonstrated a strong predictive value
of RV infarction assessed by CMR (24). The authors also defined RV ejection fraction as an
important prognostic marker. However, this study did not measure RV edema and RV
myocardial salvage. Moreover, our study did not find such a strong relationship between RV
ejection fraction and clinical outcome. In contrast we could demonstrate that prognosis of
patients with RVI mainly depends on RV MSI rather than RV ejection fraction.
Analyzing the entire patient group RVI was independently related to “hard” outcome
parameters. In addition, RVI assessed by CMR was compared to established clinical,
angiographic and CMR parameters.
In clinical routine RVI is diagnosed by echocardiography and/or ECG, but both modalities
have their specific limitations. Wall motion impairment of the inferior RV wall is sometimes
difficult to visualize in echocardiography and may lead to false negative results. ECG changes
of RVI are transient, frequently vanishing 8-10 h after symptom onset (25). CMR is a
promising tool to fill this diagnostic gap and to identify patients with RVI. This might lead to
an early adequate therapy before developing severe hemodynamic compromise.
Limitations
Assessment of myocardial edema is discussed controversially (26). Quantification of RV
edema is even more challenging than in the LV. Using a black-blood T2-weighted short
inversion time turbo spin-echo sequence with a surface coil leads to inhomogeneities of the
myocardium which might result in misinterpretation of edema. Therefore we combined the
T2-weighted sequence with the body coil to achieve signal homogeneity in the biventricular
myocardium. Nevertheless, signal-to-noise ratio in this sequence is relatively low and the thin
compacted myocardial layer of the RV makes hyperintense areas less obvious. Additionally
papapapapaaparerererererered d d d d dd tototototototo e e e e e e eststststsss ababababababablililililililisssssss
ne RVI is dia osed b echocardio hy and/or ECG, but bo
ic limitations. Wall motion impairment of the inferior RV wall
ize in echocardio and m lead to false n ative results.
ne RVI is diagnosed by echocardiography and/or ECG, but bo
ic limitations. Wall motion impairment of the inferior RV wall
ize in echocardiography and may lead to false negative results.
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

slow-flow artifacts in the intertrabecular recesses, which are adjacent to edema, can
complicate quantification of the latter.
Also visualization of DE in the thin RV myocardium is more difficult as compared with the
thicker compacted myocardial layer of the LV wall. We used the same inversion time for both
ventricles. Choosing a shorter inversion time for the RV does not improve image quality and
reproducibility and may result in dark rim artifacts (27).
Owing to these specific challenges, both acquisition and evaluation of CMR in RVI is time
consuming and requires expertise in this field. Therefore calculation of RV edema and RV
MSI might only be accomplished in CMR referral centers.
Conclusions
This large prospective study demonstrates that RVI, defined as edema, wall motion
impairment and DE as assessed by CMR, is a strong predictor for the occurrence of death,
reinfarction and congestive heart failure when no complete myocardial salvage can be
achieved. It should therefore be considered for further risk stratification and optimized clinical
treatment.
pective study demonstrates that RVI, defined as edema,
DE as assessed CMR, is a strong predictor for the occurre
l
pective study demonstrates that RVI, defined as edema,
DE as assessed by CMR, is a strong predictor for the occurre
congestive heart failure when no complete myocardial sal
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Disclosures
Matthias Grothoff: none; Christian Elpert: none; Janine Hoffmann: none; Johannes Zachrau:
none; Lukas Lehmkuhl: none; Suzanne de Waha: none; Steffen Desch: none; Ingo Eitel: none;
Meinhard Mende: none; Holger Thiele: none
Matthias Gutberlet: Research Grant:
Siemens Syngo Via <$10k
Core Lab for CRISP-AMI study (Counterpulsation to Reduce Infarct
Size Pre-PCI-Acute Myocardial Infarction) <$10k
Grip Study Bayer (Safety of Gadolinium in renally-impaired
Patients) <$10k
Other Research Support:
IMRICOR interventional MRI <$10k
Honoraria:
Talks for Siemens <$10k
Consultant/Advisory Board
Philips iCT Advisory Board no money
Other Research Support:
IMRICOR interventional MRI <$10k
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

References
1. Mehta SR, Eikelboom JW, Natarajan MK, Diaz R, Yi C, Gibbons RJ, Yusuf S. Impact
of right ventricular involvement on mortality and morbidity in patients with inferior
myocardial infarction. J Am Coll Cardiol. 2001; 37:37-43.
2. Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med. 1994; 330:1211-7.
3. Andersen HR, Falk E, Nielsen D. Right ventricular infarction: frequency, size and
topography in coronary heart disease: a prospective study comprising 107 consecutive
autopsies from a coronary care unit. J Am Coll Cardiol. 1987; 10:1223-32.
4. Aletras AH, Tilak GS, Natanzon A, Hsu LY, Gonzales FM, Hoyt RF Jr., Arai AE.
Retrospective determination of the area at risk for reperfused acute myocardial
infarction with T2-weighted cardiac magnetic resonance imaging: histopathological
and displacement encoding with stimulated echoes (DENSE) functional validations.
Circulation. 2006; 113:1865-70.
5. Kim HW, Farzaneh-Far A, Kim RJ. Cardiovascular magnetic resonance in patients
with myocardial infarction: current and emerging applications. J Am Coll Cardiol.
2009; 55:1-16.
6. Eitel I, Desch S, Fuernau G, Hildebrand L, Gutberlet M, Schuler G, Thiele H.
Prognostic significance and determinants of myocardial salvage assessed by
cardiovascular magnetic resonance in acute reperfused myocardial infarction. J Am
Coll Cardiol. 2010; 55:2470-9.
7. Masci PG, Francone M, Desmet W, Ganame J, Todiere G, Donato R, Siciliano V,
Carbone I, Mangia M, Strata E, Catalano C, Lombardi M, Agati L, Janssens S,
Bogaert J. Right Ventricular Ischemic Injury in Patients With Acute ST-Segment
Elevation Myocardial Infarction. Characterization With Cardiovascular Magnetic
Resonance. Circulation. 2010; 122:737-42
M,M,M,M,M,,, H Hoyoyoyoyoyoyoyt t RFRFRRRR J Jr.r.r.r.r.r.r., , , , , , , AAAAAAA
usedddddd aaaaaaacucucucucucucutetetetetetete mmmmmmmyoyoyoyoyoyoyocac
a
acement encoding with stimulated echoes (DENSE) functional v
o
with T2-weighted cardiac magnetic resonance imaging: histopa
acement encoding with stimulated echoes (DENSE) functional v
on. 2006; 113:1865-70.
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

8. Morrow DA, Antman EM, Charlesworth A, Cairns R, Murphy SA, de Lemos JA,
Giugliano RP, McCabe CH, Braunwald E. TIMI risk score for ST-elevation
myocardial infarction: A convenient, bedside, clinical score for risk assessment at
presentation: An intravenous nPA for treatment of infarcting myocardium early II trial
substudy. Circulation. 2000; 102:2031-7.
9. Desch S, Engelhardt H, Meissner J, Eitel I, Sareban M, Fuernau G, de Waha S,
Grothoff M, Gutberlet M, Schuler G, Thiele H. Reliability of myocardial salvage
assessment by cardiac magnetic resonance imaging in acute reperfused myocardial
infarction. Int J Cardiovasc Imaging. 2011 Jan 30. [Epub ahead of print].
10. Thiele H, Hildebrand L, Schirdewahn C, Eitel I, Adams V, Fuernau G, Erbs S, Linke
A, Diederich KW, Nowak M, Desch S, Gutberlet M, Schuler G. Impact of high-dose
N-acetylcysteine versus placebo on contrast-induced nephropathy and myocardial
reperfusion injury in unselected patients with ST-segment elevation myocardial
infarction undergoing primary percutaneous coronary intervention. The LIPSIA-N-
ACC (Prospective, Single-Blind, Placebo-Controlled, Randomized Leipzig Immediate
PercutaneouS Coronary Intervention Acute Myocardial Infarction N-ACC) Trial. J
Am Coll Cardiol. 2010; 55:2201-9.
11. Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, Falk V, Filippatos
G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG, Tubaro M, Verheugt F,
Weidinger F, Weis M, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K,
Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem
U, Silber S, Tendera M, Widimsky P, Zamorano JL, Silber S, Aguirre FV, Al-Attar N,
Alegria E, Andreotti F, Benzer W, Breithardt O, Danchin N, Di Mario C, Dudek D,
Gulba D, Halvorsen S, Kaufmann P, Kornowski R, Lip GY, Rutten F. Management of
acute myocardial infarction in patients presenting with persistent ST-segment
elevation: the Task Force on the Management of ST-Segment Elevation Acute
V,V,V,V,V,V,V, F F FF FF Fueueueueueueuernrnrnrnrnrnrnauauauauauauau G G G GGG G, , ,, ,, , ErErErErErErEr
hulerrrrrrr GGGGGGG IIIIImpmpmpmpmpmpmpacacacacacacacttttttt o
y y
o c
under in imar rcutaneous coronar intervention. The L
ysteine versus placebo on contrast-induced nephropathy and my
on injury in unselected patients with ST-segment elevation myoc
undergoing primary percutaneous coronary intervention. The L
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2008;
29:2909-45.
12. Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. J
Am Coll Cardiol. 2007; 50:2173-95.
13. Friedrich MG, Abdel-Aty H, Taylor A, Schulz-Menger J, Messroghli D, Dietz R. The
salvaged area at risk in reperfused acute myocardial infarction as visualized by
cardiovascular magnetic resonance. J Am Coll Cardiol. 2008; 51:1581-7.
14. Ibrahim T, Schwaiger M, Schomig A. Images in cardiovascular medicine. Assessment
of isolated right ventricular myocardial infarction by magnetic resonance imaging.
Circulation. 2006; 113:e78-e79.
15. Eitel I, Desch S, Sareban M, Fuernau G, Gutberlet M, Schuler G, Thiele H. Prognostic
significance and magnetic resonance imaging findings in aborted myocardial
infarction after primary angioplasty. Am Heart J. 2009; 158:806-13.
16. Goldstein JA. Pathophysiology and management of right heart ischemia. J Am Coll
Cardiol. 2002; 40:841-53.
17. Forman MB, Wilson BH, Sheller JR, Kopelmann HA, Vaughn WK, Virmani R,
Friesinger GC. Right ventricular hypertrophy is an important determinant of right
ventricular infarction complicating acute inferior left ventricular infarction. J Am Coll
Cardiol. 1987; 10:1180-7.
18. Isner JM, Roberts WC. Right ventricular infarction complicating left ventricular
infarction secondary to coronary heart disease. Frequency, location, associated
findings and significance from analysis of 236 necropsy patients with acute or healed
myocardial infarction. Am J Cardiol. 1978; 42:885-94.
19. Kopelman HA, Forman MB, Wilson BH, Kolodgie FD, Smith RF, Friesinger GC,
Virmani R. Right ventricular myocardial infarction in patients with chronic lung
chulererererererer GGGGGGG ThThThThThThThieieieieieieielelelelelelele H
nce and m netic resonance im in findin in aborted oc d
JA. Path siol and mana ment of ri t heart ischemia. J
nce and magnetic resonance imaging findings in aborted myocard
after primary angioplasty. Am Heart J. 2009; 158:806-13.
JA. Pathophysiology and management of right heart ischemia. J
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

disease: possible role of right ventricular hypertrophy. J Am Coll Cardiol. 1985;
5:1302-7.
20. Schroeder AP, Houlind K, Pedersen EM, Nielsen TT, Egeblad H . Serial magnetic
resonance imaging of global and regional left ventricular remodeling during 1 year
after acute myocardial infarction. Cardiology. 2001; 96:106-14.
21. Kumar A, Abdel-Aty H, Kriedemann I, Schulz-Menger J, Gross CM, Dietz R,
Friedrich MG. Contrast-enhanced cardiovascular magnetic resonance imaging of right
ventricular infarction. J Am Coll Cardiol. 2006; 48:1969-76.
22. Francone M, Bucciarelli-Ducci C, Carbone I, Canali E, Scardala R, Calabrese FA,
Sardella G, Mancone M, Catalano C, Fedele F, Passariello R, Bogaert J, Agati L.
Impact of primary coronary angioplasty delay on myocardial salvage, infarct size, and
microvascular damage in patients with ST-segment elevation myocardial infarction:
insight from cardiovascular magnetic resonance. J Am Coll Cardiol. 2009; 54:2145-53
23. Jensen CJ, Jochims M, Hunold P, Sabin GV, Schlosser T, Bruder O. Right ventricular
involvement in acute left ventricular myocardial infarction: prognostic implications of
MRI findings. AJR Am J Roentgenol. 2010; 194:592-8.
24. Miszalski-Jamka T, Klimeczek P, Tomala M, Krupinski M, Zawadowski G, Noelting
J, Lada M, Sip K, Banys R, Mazur W, Kereiakes DJ, Zmudka K, Pasowicz M. Extent
of RV dysfunction and myocardial infarction assessed by CMR are independent
outcome predictors early after STEMI treated with primary angioplasty. JACC
Cardiovasc Imaging. 2010; 3:1237-46.
25. Braat SH, Brugada P, de Zwaan C, Coenegracht JM, Wellens HJ. Value of
electrocardiogram in diagnosing right ventricular involvement in patients with an
acute inferior wall myocardial infarction. Br Heart J. 1983; 49:368-72.
26. Friedrich M, Kim H, Kim R. T2-weighted imaging to assess post-infarct myocardium
at risk. JACC Cardiovasc Imaging. 2011; 4:1014-1021
lolooloooo R R R R R RR, , ,,,,, BoBoBoBoBoBoBogagagagagagagaererererererert ttt tt t J,J,J,J,J,J,J, A AA A A A A
rdiallll sasasasasasasalvlvlvlvlvlvlvagagagagagagageeeeeee iiiiiiinfnnnnnn a
cular dama in tients with ST-s ment elevation m cardial
om cardiovascular magnetic resonance. J Am Coll Cardiol. 2009
J h
cular damage in patients with ST-segment elevation myocardial
om cardiovascular magnetic resonance. J Am Coll Cardiol. 2009
J, Jochims M, Hunold P, Sabin GV, Schlosser T, Bruder O. Righ
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

27. Grosse-Wortmann L, Macgowan CK, Vidarsson L, Yoo SJ. Late gadolinium
enhancement of the right ventricular myocardium: is it really different from the left ? J
Cardiovasc Magn Reson. 2008; 10:20.
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Table 1. Patient characteristics
Entire patient group n=421
RVI-group n=69
Non-RVI-group n=69
P-value
Age, years 66±12 65±13 65±11 0.81
Male sex, n (%) 321 (76) 55 (80) 55 (80)
Killip-class on admission, n (%) I II III IV
304 (72) 92 (22) 19 (5) 6 (1)
53 (77) 12 (17) 3 (5) 1 (1)
56 (82) 11 (16) 1 (1) 1 (1)
0.57
TIMI*- risk score 3 [2,4] 2 [1,3] 1 [0,2] 0.14
Pain-to-balloon time, min 211 [140,352] 240 [157,431] 179 [129,324] 0.04
RV† injury, n 69 69 0
TIMI*-flow after angioplasty, n 0-II III
53 368
9 60
10 59
0.81
ST-segment resolution, % 73 [49,95] 61 [37,91] 91 [66,100] 0.004
LV‡ ejection fraction, % 49±12 48±9 50±10 0.29
RV† ejection fraction, % 50±9 43±10 54±6 <0.001
LV‡ end diastolic volume index, ml/m² 77±17 78±18 73±14 0.10
RV† end diastolic volume index, ml/m² 77±19 79±19 75±20 0.27
LV‡ myocardial mass index, g/m² 66±15 65±15 60±14 0.045
RV† myocardial mass index, g/m² 25±5 23±4 0.002
Infarct size, % LV 21±12 17±14 0.10
Infarct size, % RV 5±6
LV‡ myocardial salvage index 0.57±0.25 0.47±0.2 0.59±0.26 0.006
RV† myocardial salvage index 0.80±02
Microvascular obstruction, % LV 1.47±4.46 1.12±1.80 0.79±1.26 0.19
Localization of culprit lesion, n LAD§ (proximal/mid/distal) RCA|| (proximal/mid/distal) LCX¶ (proximal/distal)
185 (74/104/7) 182 (89/51/42) 54 (46/8)
11 (5/5/1) 53 (23/21/9) 5 (5/0)
11 (4/6/1) 53 (26/15/12) 5 (5/0)
Cardiovascular risk factors, n (%) Diabetes mellitus Hypertension Smoking Hyperlipidemia Family history of coronary artery disease
111 (26) 292 (69) 175 (42) 142 (34) 128 (30)
15 (22) 46 (67) 33 (48) 21 (30) 17 (25)
14 (20) 46 (67) 27 (39) 24 (35) 20 (29)
0.83 1.00 0.30 0.59 0.56
Heart rate, beats per minute 80±17 77±17 78±14 0.58
Mean blood pressure, mmHg 95±17 93±16 94±14 0.67
Continuous data are presented as mean±SD or median (interquartile range). Categorical variables are given as frequency and percentage. *TIMI=Thrombolysis in myocardial infarction; †RV=right ventricular; ‡LV=left ventricular; §LAD=left anterior descending coronary artery; ||RCA=right coronary artery; ¶LCX=left circumflex coronary artery
59
91919191919191 [ [ [ [ [ [ [66666666666666,1,1,,,,, 00000000000000]]]]]]]
50505050505050±1±1±1±1±1±1±10000000
o
o
o
s
a
21±12 17±14
on, % 50±9 43±10 54±6
olume index, ml/m² 77±17 78±18 73±14
olume index, ml/m² 77±19 79±19 75±20
ss index, g/m² 66±15 65±15 60±14
ass index, g/m² 25±5 23±4
21±12 17±14
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Table 2. Univariate and multivariable stepwise forward logistic regression analysis for the
prediction of RVI
RVI group and matched group, n=138
Parameter Univariate Multivariable
p-value OR* [CI†] p-value OR* [CI†]
TIMI‡-risk score 0.14 1.17 [0.95;1.44]
Pain-to-balloon time (per 10 minutes)
0.03 1.03 [1.00;1.05]
RV§-myocardial mass index (per 5 g/m²)
0.004 1.94 [1.24;3.05] 0.01 2.06 [1.18;3.58]
LV||-myocardial mass index (per 5 g/m²)
0.05 1.12 [1.00;1.27]
LV||% infarct size (per 5%)
0.10 1.12 [0.98;1.29]
LV||% area at risk (per 5%)
0.96 1.00 [0.91;1.10]
LV|| myocardial salvage index
0.01 0.16 [0.04;0.65]
Killip-class on admission 0.49 1.21 [0.70;2.10]
Peak CK¶ (μmol/ls) 0.049 1.02 [1.00;1.03]
Peak CK¶-MB# (μmol/ls) 0.07 1.20 [0.99;1.45]
TIMI‡-flow pre angioplasty 0.001 0.50 [0.34;0.74] 0.001 0.49 [0.32;0.76]
TIMI‡-flow post angioplasty 0.63 0.98 [0.78;1.19]
Incomplete ST-segment resolution (<70%)
0.02 1.37 [1.17;2.62] 0.06 1.58 [1.22;2.46]
Sum ST-segment elevation (mV) 0.64 1.12 [0.70;1.78]
Leads with ST-segment elevation (number)
0.75 0.96 [0.75;1.23]
Mean blood pressure (per 10 mmHg)
0.66 0.95 [0.76;1.19]
Heart rate (per 10 beats per minute)
0.58 0.94 [0.76;1.16]
*OR=odds ratio, †CI=confidence interval; ‡TIMI=Thrombolysis in myocardial infarction; §RV=right ventricular; ||LV=left ventricular; ¶CK=creatine kinase; #MB=myocardial band
s
0.96 1.00 [0.91;1.10]
0.01 0.16 [0.04;0.65]
ssion 0.49 1.21 [0.70;2.10]
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Table 3. Predictors of MACE in the univariate and stepwise forward multivariable Cox regression analysis of the entire patient group, n=421
Univariate Multivariable Parameter
p Hazard ratio [CI*] p Hazard ratio [CI*]
<0.001
0.02
2.66 [1.61-4.11]
0.97 [0.94 -0.99]
<0.001
3.36 [1.99-5.66]
RV† injury
RV† ejection fraction
LV‡ ejection fraction
LV‡-MSI
<0.001
<0.001
0.93 [0.94-0.97]
0.12 [0.04-0.36]
0.004
0.96 [0.93-0.99]
<0.001 1.04 [1.02-1.05] LV‡% infarct size
TIMI§-flow after angioplasty 0-II 0.002 2.41 [1.38-4.21]
Microvascular obstruction (%LV‡) 0.001 1.04 [1.02-1.07]
<0.001 1.25 [1.13-1.38] 0.01 1.20 [1.04-1.34] TIMI§-risk score
ST-segment resolution (%) 0.03 0.99 [0.99-1.00]
*CI=confidence interval; †RV= right ventricular; ‡LV= left ventricular;
§TIMI=Thrombolysis in myocardial infarction
0000000 01010101010101
%) 0.03 0.99 [0.99-1.00]
i
o
%) 0.03 0.99 [0.99-1.00]
interval; †RV= right ventricular; ‡LV= left ventricular;
lysis in myocardial infarction
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

Figure Legends
Figure 1. Study flow chart. STEMI=ST-elevation myocardial infarction; CMR=cardiac
magnetic resonance; RV=right ventricle
Figure 2. Coronary angiography and CMR of a patient with isolated RV infarction (a)
demonstrating a high degree stenosis of the right coronary artery, (b)
successfully treated by angioplasty with a TIMI-flow III after treatment. (c)
There is a large area at risk (brown contour) of the inferior and free RV wall,
(d) but no infarction zone in DE imaging resulting in a 100% myocardial
salvage.
Figure 3. Coronary angiography and CMR of a severe inferior infarction: (a) proximal
occlusion of the right coronary artery, (b) after angioplasty with post TIMI-
flow II. (c) Area at risk (brown contour) extends from the LV inferior wall to
the interventricular septum and the RV inferior and free wall. In d MO of the
the LV (cyan contour) and the area of infarction (magenta contour) is shown.
Figure 4a & b. Kaplan-Meier curves of all matched patients (n=138) (a) for the incidence of
MACE and (b) for the incidence of death in patients with (solid line; n=69) and
without (broken line; n=69) RVI.
Figure 5a & b. Kaplan-Meier curves of all RVI-patients (n=69) (a) for the incidence of
MACE and (b) for the incidence of death in patients with 100% RV
myocardial salvage (broken line RV MSI=1; n=28) and patients <100%
myocardial salvage (solid line RV MSI<1; n=41).
ululululuu titingngngngngngng i in n n n n n a a 101010100000%0%0%0%0%0%0%
oronary angiography and CMR of a severe inferior infarction
c t
o n
oronary angiography and CMR of a severe inferior infarction:
clusion of the right coronary artery, (b) after angioplasty wit
ow II. (c) Area at risk (brown contour) extends from the LV in
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from
by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from

by guest on February 21, 2013circimaging.ahajournals.orgDownloaded from




















