
Loss of astrocytic glutamate transporters in Wernicke encephalopathy

nature publishing group ORIGINAL CONTRIBUTIONS
LIV
ER
307
© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
INTRODUCTION Minimal hepatic encephalopathy (MHE) is a part of the spectrum
of overt hepatic encephalopathy (OHE). It has a characteristic
cognitive profi le that cannot be diagnosed clinically ( 1 – 4 ). It is
characterized by psychomotor slowing and cognitive defi cits in
visual – spatial perception, attention, concentration, and construc-
tional ability, which adversely aff ect daily activities such as driving
ability, social interaction, and communication ( 4,5 ). MHE has a
signifi cant impact on the health-related quality of life (HRQOL)
( 6,7 ). On follow-up, patients with MHE are more likely to develop
OHE, as compared with cirrhotics without MHE ( 8 – 10 ). MHE is
associated with poor prognosis and is probably an independent
predictor of survival ( 11 ).
Th ere is no gold standard for the diagnosis of MHE. Neuro-
psychometric (NP) and neurophysiological methods have
been used to diagnose MHE ( 1 – 3 ). Recently proposed tests
to diagnose MHE include critical fl icker frequency, inhibi-
tory control test, cognitive drug research test, and magnetic
resonance imaging with measurement of apparent diff usion
coeffi cient ( 3,12 ).
Rifaximin Improves Psychometric Performance and Health-Related Quality of Life in Patients With Minimal Hepatic Encephalopathy (The RIME Trial) Sandeep Singh Sidhu , MBBS, MD, DM 1 , Omesh Goyal , MBBS, MD, DM 1 , Bholeshwar Prashad Mishra , MBBS, PhD 2 , Ajit Sood , MBBS, MD, DM 1 , Rajoo Singh Chhina , MBBS, MD, DM 1 and Ravinder Kumar Soni , MBBS, MD 3
OBJECTIVES: Cirrhotics with minimal hepatic encephalopathy (MHE) have a poor health-related quality of life (HRQOL). Treatment of MHE is still evolving. The aim of this double-blind randomized pilot study was to assess the effi cacy of rifaximin in improving neuropsychometric (NP) test performance and HRQOL in patients with MHE.
METHODS: MHE was diagnosed if any two NP tests (number and fi gure connection tests, picture completion, digit symbol, and block design tests) were deranged beyond 2 s.d. of normal. HRQOL was assessed using the sickness impact profi le (SIP) questionnaire.
RESULTS: A total of 486 patients with cirrhosis were screened and 284 were found eligible. Out of these 115 (40.9 % ) had MHE, of which 21 refused consent and 94 were randomized to receive placebo ( n = 45) and rifaximin ( n = 49; 1200 mg / day) for 8 weeks. At the end of treatment, signifi cantly more number of patients in rifaximin group showed reversal of MHE (75.5 % (37 / 49) vs. 20 % (9 / 45) in placebo group; P < 0.0001). Rifaximin group also showed signifi cant reduction in mean number of abnor-mal NP tests (baseline, 2.35 (95 % confi dence interval (CI), 2.17 – 2.53); 2 weeks, 1.29 (95 % CI, 1.02 – 1.56), P = 0.002; 8 weeks, 0.81 (95 % CI, 0.61 – 1.02), P = 0.000), compared with placebo group (baseline, 2.31 (95 % CI, 2.03 – 2.59); 2 weeks, 2.03 (95 % CI, 1.74 – 2.31); 8 weeks, 1.97 (95 % CI, 1.69 – 2.25), P > 0.05). The mean total SIP score also improved signifi cantly in rifaximin group (base-line, 11.67 (95 % CI, 10.31 – 13.03); 8 weeks, 6.45 (95 % CI, 5.59 – 7.30); P = 0.000) compared with placebo group (baseline, 9.86 (95 % CI, 8.66 – 11.06); 8 weeks, 8.51 (95 % CI, 7.35 – 9.67); P = 0.82). Improvement in HRQOL correlated with improvement in NP tests. Rifaximin was well tolerated.
CONCLUSIONS: Rifaximin signifi cantly improves both cognitive functions and HRQOL in patients with MHE.
Am J Gastroenterol 2011; 106:307–316; doi: 10.1038/ajg.2010.455; published online 14 December 2010
1 Department of Gastroenterology, Dayanand Medical College and Hospital , Ludhiana, Punjab , India ; 2 Department of Psychiatry, Dayanand Medical College and Hospital , Ludhiana, Punjab , India ; 3 Department of Community Medicine, Dayanand Medical College and Hospital , Ludhiana, Punjab , India . Correspondence: Sandeep Singh Sidhu, MBBS, MD, DM , Department of Gastroenterology, Dayanand Medical College and Hospital , 118-R, Model Town, Ludhiana 141001 , Punjab , India . E-mail: [email protected] Received 31 March 2010; accepted 9 August 2010
see related editorial on page 317

308 LI
VE
R
The American Journal of GASTROENTEROLOGY VOLUME 106 | FEBRUARY 2011 www.amjgastro.com
Sidhu et al.
Treatment for OHE / MHE is mainly targeted toward the gut
because of ammoniagenic potential of the gut contents, which have
been hypothesized to cause OHE / MHE ( 3,4,13 ). Various treatment
modalities that have been shown to reverse MHE include lactulose /
lactitol, probiotics / synbiotics, L -carnitine, branched-chain amino
acids, and dietary manipulation ( 14 – 28 ). However, because of the
low tolerability in case of lactulose ( 3,29 ), lack of standardization
in case of probiotics, and lack of convincing evidence of effi cacy
for other treatments, better treatment options for MHE need to
be explored. Rifaximin is a non-absorbable, gut-specifi c antibiotic.
Compared with lactulose or neomycin, rifaximin has shown a gen-
eral trend toward better effi cacy and better tolerability in patients
with OHE ( 30,31 ). Till date, rifaximin has not been tried for the
treatment of MHE. Th is pilot study aimed to investigate the effi -
cacy of rifaximin therapy in improving NP test performance and
HRQOL in patients with MHE (RIME = Rifaximin In MHE).
METHODS Study design Th is study was designed as a prospective, randomized, double-
blind, placebo-controlled trial. It was conducted at the Gastroen-
terology outpatient department of a tertiary care hospital from
December 2008 to November 2009.
Protocol Patient population . All patients with liver cirrhosis without OHE
were screened for the presence of MHE. Cirrhosis was diag-
nosed on the basis of clinical, biochemical, and radiological or
liver histological data. Th e inclusion criteria were age 18 – 65 years
and MHE diagnosed by abnormalities in NP tests. All women of
childbearing potential were required to use at least two eff ective
contraceptive methods. Exclusion criteria were known allergy to
rifaximin / rifabutin / rifampin / rifapentine; current or recent ( < 6
weeks) use of alcohol; use of antibiotics within last 6 weeks; use
of lactulose / lactitol, probiotics, L -ornithine- L -aspartate, zinc,
metronidazole, neomycin, or rifaximin within last 6 weeks; use
of interferon or psychoactive drugs such as benzodiazepines,
psychotropic drugs, anti-epileptics within last 6 weeks; infec-
tion or gastrointestinal hemorrhage within last 6 weeks; acute
superimposed liver injury; advanced medical problems such as
congestive cardiac failure, advanced pulmonary disease, or renal
insuffi ciency or electrolyte imbalance; presence of hepatocellular
carcinoma; history of portosystemic shunt surgery or transjugular
intrahepatic portosystemic shunt; pregnancy and breastfeeding;
neurological or psychiatric problems that may infl uence quality
of life measurement; poor vision or motor defects that interfere
with the performance of psychometric tests; and current or past
history of OHE.
General clinical and laboratory assessment . All patients were
subjected to detailed history taking and physical examination.
Laboratory assessment including hemogram, liver and renal
function tests, prothrombin time index, fasting blood sugar, and
α -fetoprotein were carried out. Child – Pugh score for the stage
of cirrhosis was calculated. Etiology of cirrhosis was considered
to be alcohol, if the alcohol consumption per day was > 60 g for
males and > 30 g for females for > 5 years. Levels of HBsAg and
anti-HCV were estimated by ELISA for evaluating viral etiology .
Workup for autoimmune liver disease, Wilson ’ s disease, hemo-
chromatosis, and Budd – Chiari syndrome was carried out, where
indicated.
Neurological assessment . Complete neurological and mental state
examination, including detailed psychiatric evaluation to exclude
undiagnosed psychiatric illnesses, was carried out. Special empha-
sis was laid on the absence of disorientation, dysarthria, fl apping
tremors, increased tone, ataxia, and increased tendon refl exes.
Th e Mini Mental State Examination to exclude the presence of
any illness that could have aff ected neurological status was per-
formed, and only patients with a score > 25 were considered for
further analysis. Th e West Haven Criteria was used to diff erentiate
between grade 0 and grade 1 hepatic encephalopathy ( 1 ).
Diagnosis of MHE . Th e following NP tests were performed:
number Connection Test A (NCT-A), Figure Connection Test-A
(FCT-A), and three performance subtests of the Wechsler Adult
Intelligence Scale — Digit Symbol Test, Picture Completion Test
(PCT), and Block Design Test (BDT) ( 1,32,33 ). Th e diagnosis of
MHE was made if any two of the NP tests were impaired beyond
2 standard deviations (s.d.) of known control values. Th is diag-
nostic criterion conforms to the consensus statements of Ferenci
et al. ( 1 ). Th ese tests were performed over a period of 35 – 40 min.
Th e FCT is a universally applicable test for the assessment of
mental state that can be performed by illiterate people too ( 33 ).
Diff erent variations of NCT and FCT were used for serial evalu-
ation in order to avoid any learning eff ect. Th e NP test results
were expressed as Z -scores, indicating the diff erences (in s.d.)
between the observed and expected scores. A negative Z -score
indicated poor performance. A Z -score less than − 2 indicated
that the result is impaired beyond 2 s.d. of known control value.
A mean Z -score (mZS) was calculated for each patient in order
to avoid bias related to multiple comparisons. Changes in the
number of abnormal NP tests ( Δ abnormal NP) and the mZS
( Δ mZS) aft er 2 and 8 weeks of treatment served as measures of
psychometric change.
Assessment of HRQOL . HRQOL assessment was carried out
using the ‘ sickness impact profi le (SIP) ’ Questionnaire (John
Hopkins University, USA) ( 34 ). Th is questionnaire consists of
136 items grouped into 12 scales. Change in the total SIP score
aft er 8 weeks of treatment ( Δ SIP) served as a measure of change
in overall HRQOL. Patients were asked to read the questionnaire
and mark only those statements that described them at that point
of time and were related to their state of health. For those subjects
who were illiterate (22.3 % ) and those who did not understand
English well (15.9 % ), an exact Hindi language translation of the
questionnaire (provided by an expert) was read out aloud in the
order listed in the printed questionnaire, and their responses were
marked.

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
309
LIV
ER
Rifaximin Improves Minimal Hepatic Encephalopathy
Written informed consent was taken from each patient. Th e
study protocol was approved by the institutional ethics committee,
and it conformed to the ethical guidelines of the 1975 Declaration
of Helsinki. Th e trial has been registered with the ‘ Clinical Trial
Registry, India ’ (Reg. no- CTRI / 2009 / 091 / 000979) and the WHO
(UTN- U1111-1111-3609) .
Assignment All patients diagnosed to have MHE were randomized into two
groups (group A and B) using computer-generated randomiza-
tion.
Masking Sequentially numbered, sealed, opaque envelopes were used for
treatment allocation by a coordinator, who was not an investiga-
tor. Group A received placebo tablets (Lupin Limited, Mumbai,
India) and group B received rifaximin tablets (RCIFAX; Lupin
Limited) at a dose of 200 mg, two tablets three times a day, per
oral, for 8 weeks. Placebo tablets were similar in size, shape,
and color to the rifaximin tablets. Th e participant, investigator,
data-entry operator, and statistician were blinded regarding the
treatment drugs. Th e code was broken only aft er the study was
complete and analysis of the results was carried out. Criteria for
discontinuation of treatment were withdrawal of consent or side
eff ects thought to be related to possible drug toxicity, including
persistent nausea / vomiting, abdominal pain, or constipation.
Participant fl ow and follow-up Th e trial lasted for 8 weeks and involved three visits by both
the groups ( Figure 1 ). Th e fi rst visit consisted of (i) NP testing,
(ii) HRQOL assessment, (iii) laboratory assessment as mentioned
above, (iv) dietary consultation, and (v) distribution of drugs to
both the groups. Th e second visit at 2 weeks included all activi-
ties of the fi rst visit, except HRQOL assessment. Th e third visit
at 8 weeks included all activities of the fi rst visit. At the second
and third visits, assessment for compliance by checking empty
wrappers and for development of any new symptoms / treatment-
related complications was carried out.
Diet and concurrent therapy . Patients were allowed to take
normal protein diet ( ~ 1 g / kg of body weight, predominantly
vegetable / casein based) and to consume the same amount of
yogurt (if consuming previously). Salt restriction (2 g / day) was
advised to those patients who had ascites. Standard treatment for
cirrhosis including diuretics (spironolactone with / without furo-
semide) and β -blockers (propranolol) were given, if indicated.
Analysis Primary outcome measure was the reversal of MHE at 8 weeks.
Secondary outcome measures were reversal of MHE at 2 weeks
and improvement in HRQOL at 8 weeks. Primary end point was
the completion of 8 weeks of follow-up and secondary end points
were the development of OHE or development of treatment-
related side eff ects.
Sample size and power analysis Previous published studies on the treatment of MHE report an
average improvement of 62 % (50 – 80 % ) and 9 % (0 – 15 % ) in the
treatment and control groups, respectively ( 14 – 17,23,24 ). Assum-
ing that rifaximin would have a similar eff ect as lactulose and
Assessed for eligibility (n=486)
• Lost to follow-up (n=8)• Discontinued due to side effects (n=0)• Developed OHE (n=2)• Died (n=1)
Placebo for 8 weeks (n=45)Received allocated intervention (n=45)
• Lost to follow-up (n=5)• Discontinued due to side effects (n=0)• Developed OHE (n=1)• Died (n=0)
Rifaximin for 8 weeks (n=49)Received allocated intervention (n=49)
Analyzed (n=34)
Positive for MHE (n=115)
Excluded (n=205)
Patients enrolled (n=281)
Refused to participate (n=21)
Randomized (n=94)
Analyzed (n=43)
Figure 1 . Flow of participants into the study. MHE, minimal hepatic encephalopathy; OHE, overt hepatic encephalopathy.

310 LI
VE
R
The American Journal of GASTROENTEROLOGY VOLUME 106 | FEBRUARY 2011 www.amjgastro.com
Sidhu et al.
probiotics, a sample size of at least 31 patients in each arm was
required, for a 5 % type 1 error, 90 % power, and a drop-out rate of
15 % ( 15 ). We aimed to enroll ~ 50 patients in each arm because
the exact follow-up rate in our population was not known. Dur-
ing the study period, we enrolled 45 patients in group A and 49
patients in group B; and at the end of study, 34 and 43 patients in
each group were analyzed, which was higher than the required
number, and gave a power of > 90 % .
Statistical analysis Data are presented as means with 95 % confi dence intervals (CI)
for quantitative variables and as proportions with 95 % CI for
qualitative variables. Th e changes in NP test results and SIP scores
within and between the groups were assessed by analysis of vari-
ance. Multiple logistic regression analysis was performed to assess
the impact of various factors on SIP score, and results expressed
as odds ratio (OR) with 95 % CI. Spearman ’ s rank correlation
co effi cient was performed to assess correlations between SIP and
NP tests. Fisher ’ s exact test was performed to assess improvement
in MHE on an intention-to-treat basis. A P -value of < 0.05 was
considered statistically signifi cant. Statistical analysis was carried
out with SPSS soft ware, version 11.5 (SPSS, Chicago, IL).
RESULTS Trial enrollment A total of 486 patients of cirrhosis presenting to the Gastro-
enterology OPD from December 2008 to November 2009 were
screened. Out of these, 281 (57.8 % ) patients met the eligibility cri-
teria, whereas 205 patients (42.2 % ) were excluded ( Figure 1 ). Th e
reasons for exclusion were history of OHE / presently being treated
with lactulose / L -ornithine- L -aspartate / rifaximin (136 patients),
recent infection or antibiotic use (28 patients), recent gastro-
intestinal bleeding (20 patients), history of recent alcohol intake
(15 patients), recent use of drugs aff ecting psycho motor perform-
ance (10 patients), unfi t to perform NP tests (9 patients), interferon
treatment (5 patients), hepatocellular carcinoma (4 patients), and
renal impairment (3 patients). A total of 25 patients were excluded
for more than one reason.
Of the 281 patients who were screened for MHE, 115 patients
(40.9 % ; 115 / 281) were detected to have MHE. In total, 21 MHE-
positive patients did not consent for the study / were not sure to come
for follow-up. Th us, 94 patients were randomized into two groups,
namely, placebo group ( n = 45) and rifaximin group ( n = 49).
Baseline characteristics Th e baseline clinical and demographic characteristics of patients with
and without MHE were similar, except that patients with MHE had
signifi cantly higher SIP scores ( Table 1 ). Age, Child–Turcotte– Pugh
(CTP) class, or alcohol etiology did not aff ect the prevalence of
MHE. Patients in rifaximin and placebo groups were comparable in
all the clinical characteristics ( Table 1 ) . Th e number of patients on
diuretics (placebo group 23 / 45 (51.1 % ) and rifaximin group 23 / 49
(46.9 % )), and β -blockers (placebo group 13 / 45 (28.9 % ) and rifax-
imin group 14 / 49 (28.6 % )) were similar in both the groups.
Clinical course In the placebo group, eight patients were lost to follow-up and two
developed OHE. One patient in the placebo group was admitted
because of massive gastrointestinal bleeding on day 24 of rand-
omization and died during hospital stay despite best endoscopic
and medical therapy. In the rifaximin group, fi ve patients were
lost to follow-up and one developed OHE. Th us, a total of 77
patients (placebo group = 34 and rifaximin group = 43) completed
the study ( Figure 1 ).
Outcomes
1. MHE reversal : Intention-to-treat analysis showed that the
percentage of patients showing reversal of MHE was sig-
nifi cantly higher in rifaximin group, both at 2 and 8 weeks
( Figure 2 ).
2. HRQOL improvement : Rifaximin led to a signifi cant reduc-
tion in 7 of the 12 scales of SIP score, total psychosocial and
physical sub-scores, and the total SIP score aft er 8 weeks of
treatment ( Table 2 ). Th e changes in SIP scores in placebo
group were not signifi cant.
End points
1. Development of OHE : One patient in rifaximin group and
two in placebo group developed OHE. Th is was statistically
nonsignifi cant ( P = 0.605).
2. Treatment-related side eff ects : Two patients in rifaximin group
reported epigastric discomfort and vomiting aft er 7 and 15
days of randomization. In the former, treatment was tem-
porarily stopped for 3 days because of persistent symptoms,
whereas symptoms of other patient improved aft er taking
antacids. Both these patients were subsequently lost to fol-
low-up. None of the patients in placebo group reported any
side eff ect ( P = 0.495).
NP performance Baseline . Tables 3 and 4 summarize the data about abnormal NP
test results in each group. Th e frequency of an abnormal result of
each NP test, the mean number of abnormal NP tests and the mZS
were similar in both the groups at baseline.
Aft er treatment . Intragroup comparisons ( Tables 3 and 4 ) — (i)
Semi-quantitative: Rifaximin group showed a signifi cant reduc-
tion in the percentage of patients having abnormal NCT, PCT and
BDT aft er 2 weeks and abnormal NCT, FCT, PCT and BDT aft er 8
weeks. In addition, there was a signifi cant reduction in the mean
number of abnormal NP tests aft er 2 and 8 weeks, compared with
baseline. However, there was a nonsignifi cant reduction in these
parameters in the placebo group. (ii) Quantitative : Rifaximin
group showed a signifi cant reduction in the mZS aft er 2 and 8
weeks, compared with baseline. However, the reduction in mZs in
placebo group was nonsignifi cant.

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
311
LIV
ER
Rifaximin Improves Minimal Hepatic Encephalopathy
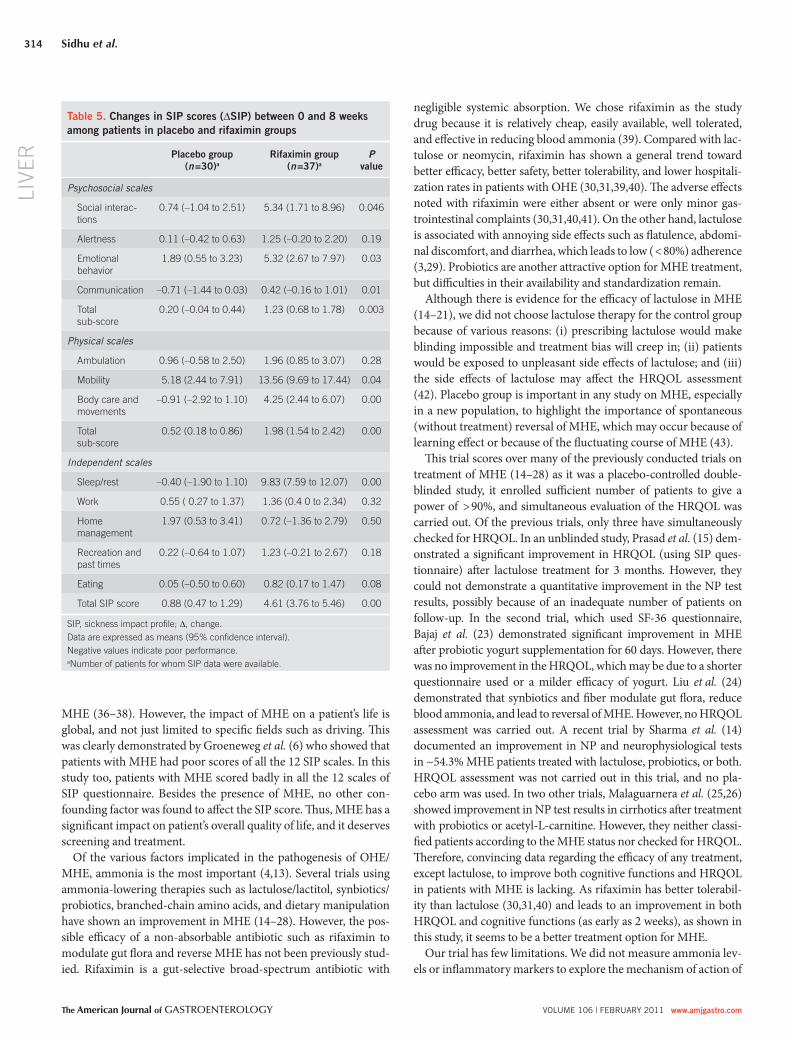
in placebo group were not signifi cant. When the Δ SIP between
both groups was compared, rifaximin group showed a signifi cant
improvement in six SIP scales, total psychosocial and physical
sub-scores, and the total SIP score ( Table 5 ).
Effect of confounding factors on SIP score Several possible confounding factors were selected for multivari-
ate analysis to evaluate their impact on total SIP score at baseline.
None of these factors were found to aff ect the total SIP score —
age ( < 50 years vs. > 50 years; OR 1.006; 95 % CI; 0.998 – 1.013),
sex (male vs. female; OR 0.999; 95 % CI, 0.991 – 1.008), education
(undergraduate vs. graduate or higher; OR 0.994; 95 % CI, 0.973 –
0.015), residence (rural vs. urban; OR 0.999; 95 % CI, 0.992 – 1.007),
duration of diagnosis of cirrhosis ( < 1 vs. > 1 year; OR 0.999; 95 %
CI, 0.992 – 1.007), CTP class (A vs. B / C; OR 0.999; 95 % CI, 0.992 –
1.007), etiology (alcohol vs. non-alcohol; OR 0.999; 95 % CI,
0.992 – 1.007), esophageal varices (presence vs. absence; OR 0.998;
Intergroup comparisons ( Table 4 ) — (i) Semi-quantitative: Th e
Δ abnormal NP was signifi cantly greater in the rifaximin group
than placebo group, both at 2 and 8 weeks. (ii) Quantitative: Com-
pared with placebo group, the Δ mZs was signifi cantly greater in
rifaximin group at 8 weeks. However, this change was nonsignifi -
cant at 2 weeks.
HRQOL assessment Baseline . Th e baseline mean scores of the SIP questionnaire of
patients in both the MHE groups are shown in Table 2 . Th e mean
scores of each scale and total SIP score were comparable in both
the groups at baseline. However, patients with MHE had signifi -
cantly higher SIP scores (all 12 scales and total score), as com-
pared with the patients without MHE ( Table 1 , Figure 3 ).
Aft er treatment . Rifaximin led to a signifi cant reduction in SIP
scores, as mentioned above ( Table 2 ). Th e changes in SIP scores
Table 1 . Clinical and demographic characteristics of patients
Characteristic MHE negative ( n =166) MHE positive
MHE total ( n =115) Placebo group ( n = 45)** Rifaximin group ( n = 49)**
Age (years)* 54.2 (52.5 – 55.9) 52.8 (51.0 – 54.6) 54.3 (51.6 – 57.1) 51.7 (49.0 – 54.3)
Male:female* 122:44 88:27 34:13 40:9
Rural:urban 108:48 72:53 26:19 34:19
Education
Illiterate 52 27 14 7
Undergraduate 104 81 30 38
Graduate 8 6 1 3
Post-graduate 2 1 0 1
CTP *
A 54 34 16 14
B 97 65 23 31
C 15 16 5 4
Duration of cirrhosis (years) 3.2 (2.6 – 3.8) 2.7 (2.1 – 3.3) 3.1 (2.2 – 3.9) 2.4 (1.7 – 3.2)
Etiology
Alcohol* 80 68 21 27
HBV 3 2 1 0
HCV 86 45 20 19
Other 11 a 8 b 4 5
Presence of varices 50 32 13 14
Presence of ascites 81 55 23 23
Total SIP score* 2.12 (1.96 – 2.28) c 10.71 (9.80 – 11.61) 9.86 (8.66 – 11.06) 11.67 (10.31 – 13.03)
CTP, Child – Turcotte – Pugh; HBV, hepatitis B virus; HCV, hepatitis C virus; MHE, minimal hepatic encephalopathy; SIP, sickness impact profi le questionnaire. Data are expressed as mean (95 % confi dence intervals) or numbers. * P value for comparison of age, sex, CTP score, and alcohol etiology between MHE-positive and -negative patients is non-signifi cant, while that of the SIP score is < 0.001. ** P value is non-signifi cant for all comparisons between the rifaximin and placebo groups. a Cryptogenic 6, non-alcoholic fatty liver disease 3, autoimmune 1, Budd – Chiari syndrome 1. b Cryptogenic 5, non-alcoholic fatty liver disease 3. c SIP data were available for 30 MHE-negative patients.

312 LI
VE
R
The American Journal of GASTROENTEROLOGY VOLUME 106 | FEBRUARY 2011 www.amjgastro.com
Sidhu et al.
95 % CI, 0.991 – 1.005), and ascites (presence vs. absence; OR 0.998;
95 % CI, 0.991 – 1.005). Only the presence of MHE signifi cantly
aff ected the total SIP score (OR 1.226; 95 % CI, 1.070 – 1.406).
Correlation of NP test performance with total SIP score Th e mean number of abnormal NP tests correlated signifi cantly
with total SIP score, both at baseline and at 8 weeks ( r = 0.319,
P = 0.003; and r = 0.325, P = 0.007, respectively). Th e mZs corre-
lated signifi cantly with total SIP score, both at baseline and at 8
weeks ( r = − 0.423, P = 0.000; and r = − 0.272, P = 0.026, respec-
tively). In addition, the Δ SIP correlated signifi cantly with Δ abnor-
mal NP and Δ mZs at 8 weeks ( r = 0.376, P = 0.002; and r = − 0.272,
P = 0.026, respectively).
DISCUSSION Th is pilot study demonstrates the benefi cial eff ect of rifaximin in
patients with cirrhosis who have MHE. Besides having a poor NP
test performance, patients with MHE also had higher SIP scores,
indicating the impact of MHE on their daily activities. Com-
pared with placebo group, rifaximin group showed a signifi cant
semi-quantitative cognitive improvement (reduction in mean
number of abnormal NP tests) as early as 2 weeks, and a signifi cant
80% Placebo group
Rifaximin group
18%
57%
75.5%
20%
70%
Per
cent
age
of p
atie
nts
show
ing
reve
rsal
of M
HE
60%
50%
40%
30%
20%
10%
0%
2 Weeks 8 Weeks
Duration of treatment
Figure 2 . Reversal of minimal hepatic encephalopathy (MHE) after 2 and 8 weeks of treatment in both the groups. The percentage of patients showing reversal of MHE was signifi cantly higher in the rifaximin group both at 2 weeks (57.1 % (28 / 49) vs. 17.8 % (8 / 45) in the placebo group; P < 0.0001) and at 8 weeks (75.5 % (37 / 49)) vs. 20 % (9 / 45) in the placebo group; P < 0.0001).
Table 2 . SIP scores of patients in each group at baseline and 8 weeks
SIP scales Placebo group Rifaximin group
Baseline ( n = 39) a 8 Weeks ( n = 30) a Baseline ( n = 42) a 8 Weeks ( n = 37) a
Psychosocial scales
Social interactions 12.25 (9.59 – 14.91) 10.37 (7.30 – 13.44) 15.37 (11.57 – 19.18) 9.82 (6.91 – 12.74) b
Alertness 2.08 (0.80 – 3.36) 2.12 (0.51 – 3.72) 3.31 (1.90 – 4.72) 2.08 (0.79 – 3.37)
Emotional behavior 11.21 (8.03 – 14.39) 10.3 (6.69 – 13.92) 15.7 (11.78 – 19.63) 9.32 (6.78 – 11.86) c
Communication 3.52 (1.96 – 5.08) 3.3 (1.76 – 4.83) 2.28 (1.08 – 3.48) 1.32 (0.40 – 2.24)
Total subscore 2.91 (2.34 – 3.45) 2.69 (2.12 – 3.28) 3.66 (2.95 – 4.37) 2.25 (1.73 – 2.78) d
Physical scales
Ambulation 4.79 (3.07 – 6.53) 2.76 (1.47 – 4.05) 4.93 (3.27 – 6.59) 2.18 (1.12 – 3.23) e
Mobility 22.54 (18.01 – 27.09) 17.35 (12.90 – 21.81) 28.49 (24.46 – 32.53) 16.01 (13.01 – 19.00) f
Body care and movements 8.32 (4.49 – 12.16) 7.52 (4.29 – 10.74) 11.29 (7.40 – 15.19) 5.46 (3.27 – 7.66) g
Total subscore 3.56 (2.81 – 4.32) 2.76 (2.10 – 3.42) 4.47 (3.86 – 5.08) 2.36 (1.89 – 2.84) h
Independent scales
Sleep / rest 13.29 (11.06 – 15.52) 14.16 (11.49 – 16.82) 15.86 (13.68 – 18.04) 5.66 (3.76 – 7.56) i
Work 4.16 (2.83 – 5.50) 4.06 (2.62 – 5.51) 4.3 (2.87 – 5.73) 2.67 (1.58 – 3.75)
Home management 9.85 (6.62 – 13.08) 6.71 (4.29 – 9.12) 6.55 (4.23 – 8.88) 4.78 (2.62 – 6.94)
Recreation and past times 3.69 (2.51 – 4.87) 3.4 (2.07 – 4.73) 4.26 (2.62 – 5.91) 2.42 (1.31 – 3.53)
Eating 2.88 (1.78 – 3.97) 3.02 (2.07 – 3.98) 4.42 (2.98 – 5.87) 2.79 (1.99 – 3.58) j
Total SIP score 9.86 (8.66 – 11.06) 8.51 (7.35 – 9.67) 11.67 (10.31 – 13.03) 6.45 (5.59 – 7.30) k
SIP, sickness impact profi le. Data are expressed as means (95 % confi dence interval). a Number of patients for whom SIP data were available.
Signifi cant improvement in the rifaximin group after 8 weeks in these scores: b P =0.025, c P =0.009, d P =0.007, e P =0.000, f P =0.013, g P =0.013, h P =0.050, i P =0.002, j P =0.00, k P =0.000.

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
313
LIV
ER
Rifaximin Improves Minimal Hepatic Encephalopathy
quantitative cognitive improvement (reduction in mean Z- score)
at 8 weeks. In addition, the rifaximin group showed a signifi cant
improvement in HRQOL (SIP scores), which strongly correlated
with the improvement in NP tests, thus confi rming that improve-
ment in HRQOL was linked to improvement in cognitive func-
tions. Rifaximin was well tolerated.
MHE is fairly common in patients with cirrhosis. Th e prevalence
of MHE in our patient population with cirrhosis who did not have
any past history of OHE was 40.9 % . Th e large variation in pre-
viously reported prevalence of MHE (22 – 84 % ) is because of dif-
ferent diagnostic criteria used and the patient population studied
( 1 – 3,35 ). We followed the most commonly used diagnostic criteria
laid down by Ferenci et al. ( 1 ). To avoid the infl uence of age, educa-
tion, and learning on NP test results, we adjusted Z -scores for age
and education, and used diff erent variations in NCT and FCT.
Th ere is compelling evidence in the literature to suggest that
MHE has a profound impact on patients ’ daily functioning and
well-being ( 6,7 ). About half of the patients with MHE may be unfi t
to work and may not have regular employment ( 6,7 ). Numerous
studies have demonstrated poor driving abilities in patients with
0
5
10
15
20
25
30
Mea
n S
IP s
core
Non-MHE
Group A
Group B
Social
inte
racti
ons
Alertn
ess
Emot
ional
beha
vior
Ambu
lation
Body c
are
and
mov
emen
ts
Sleep/
rest
Wor
k
Recre
ation
and
pas
t tim
es
Total
SIP sc
ore
Eating
Home
man
agem
ent
Mob
ility
Comm
unica
tion
Figure 3 . Sickness impact profi le (SIP) scores of patients with and without minimal hepatic encephalopathy (MHE) ( P < 0.001 for comparison of all scores between the non-MHE group and MHE group (rifaximin and placebo)).
Table 3 . Prevalence of abnormalities in individual NP tests in each group at baseline, 2 weeks, and 8 weeks
NP test Placebo group Rifaximin group
0 Week ( n =45) 2 Weeks ( n =37) 8 Weeks ( n =34) 0 Week ( n =49) 2 Weeks ( n =45) 8 Weeks ( n =43)
Abnormal NCT a 65.5 % (47.3 – 80.2 % ) 52.2 % (32.9 – 70.8 % ) 45.0 % (25.8 – 65.8 % ) 86.7 % (73.5 – 94.1 % ) b 43.9 % (29.9 – 58.9 % ) c 25.0 % (14.0 – 40.4 % ) d
Abnormal FCT a 80.0 % (63.8 – 90.3 % ) 78.6 % (60.1 – 90.1 % ) 80.0 % (60.4 – 91.6 % ) 89.6 % (73.4 – 95.9 % ) e 72.1 % (57.2 – 83.4 % ) 52.4 % (37.7 – 66.6 % ) f
Abnormal DST a 12.9 % (4.5 – 29.5 % ) 12.5 % (3.5 – 31.8 % ) 0.0 % (0.0 – 18.2 % ) 6.7 % (1.6 – 18.5 % ) 2.4 % (0.06 – 13.7 % ) 0.0 % (0.0 – 10.7 % )
Abnormal PCT 57.8 % (43.3 – 71.0 % ) 37.8 % (24.0 – 53.9 % ) 41.2 % (26.3 – 57.8 % ) 34.7 % (22.9 – 48.7 % ) g 6.7 % (1.6 – 18.5 % ) h 4.7 % (0.44 – 16.3 % ) i
Abnormal BDT 60.0 % (45.4 – 73.0 % ) 48.6 % (33.5 – 64.1 % ) 50.0 % (34.1 – 65.9 % ) 46.9 % (33.7 – 60.6 % ) j 8.9 % (2.9 – 21.3 % ) k 7.0 % (1.7 – 19.3 % ) l
BDT, block design test; DST, digit symbol test; FCT, fi gure connection test; NCT, number connection test; NP, neuropsychological; PCT, picture completion test. Data are expressed as percentages (95 % confi dence interval). a Illiterate patients (20, 18, and 11 patients did not perform NCT, DST, and FCT tests, respectively).
Rifaximin group : P value signifi cant for the following comparisons: bc P = 0.0001, bd P < 0.0001, ef P = 0.0001, gh P = 0.0009, gi P = 0.0005, ik P = 0.0001, and jl P = 0.0001. Placebo group : P value is non-signifi cant for all comparisons between baseline and 2 weeks, and between baseline and 8 weeks for each NP test.
Table 4 . Prevalence and changes in quantitative and semi-quantitative abnormalities in NP tests in each group at baseline, 2 weeks, and 8 weeks
Placebo group Rifaximin group
0 Week ( n = 45) 2 Weeks ( n = 37) 8 Weeks ( n = 34) 0 Week ( n = 49) 2 Weeks ( n = 45) 8 Weeks ( n = 43)
Mean mZS − 2.61 ( − 2.89 to − 2.33) a
− 2.44 ( − 2.72 to − 2.16) c
− 2.26 ( − 2.55 to − 1.98) e
− 2.54 ( − 2.81 to − 2.27) b
− 1.83 ( − 2.18 to − 1.47) d
− 1.44 ( − 1.84 to − 1.03) f
Δ mZS 0.60 (0.32 to 0.89) g 0.46 (0.18 to 0.74) i 0.86 (0.58 to 1.14) h 1.13 (0.88 to 1.37) j
Mean no. of abnormal tests
2.31 (2.03 to 2.59) k 2.03 (1.74 to 2.31) m 1.97 (1.69 to 2.25) o 2.35 (2.17 to 2.53) l 1.29 (1.02 to 1.56) n 0.81 (0.61 to 1.02) p
Δ Abnormal NP tests
0.64 (0.36 to 0.93) q 0.32 (0.04 to 0.61) s 1.16 (0.91 to 1.41) r 1.56 (1.30 to 1.82) t
mZS, mean Z -score; NP, neuropsychological; Δ , change. Data are expressed as mean (95 % confi dence interval). Intra-group comparisons: Baseline vs. 2 weeks — ac P =0.393, bd P =0.002, km P =0.127, ln P =0.000; Baseline vs. 8 weeks — ae P =0.119, bf P =0.000, ko P =0.075, lp P =0.000; 2 weeks vs. 8 weeks — ce P =0.435, df P =0.146, mo P =0.935, np P =0.006. Inter-group comparisons: Baseline — ab P =0.725, kl P =0.766; change between baseline and 2 weeks — gh P =0.243, qr P =0.016; change between baseline and 8 weeks — ij P =0.000, st P =0.0001; change between 2 and 8 weeks — mZs, P =0.177, no. of abnormal NP tests, P =0.018.
314 LI
VE
R
The American Journal of GASTROENTEROLOGY VOLUME 106 | FEBRUARY 2011 www.amjgastro.com
Sidhu et al.
MHE ( 36 – 38 ). However, the impact of MHE on a patient ’ s life is
global, and not just limited to specifi c fi elds such as driving. Th is
was clearly demonstrated by Groeneweg et al. ( 6 ) who showed that
patients with MHE had poor scores of all the 12 SIP scales. In this
study too, patients with MHE scored badly in all the 12 scales of
SIP questionnaire. Besides the presence of MHE, no other con-
founding factor was found to aff ect the SIP score. Th us, MHE has a
signifi cant impact on patient ’ s overall quality of life, and it deserves
screening and treatment.
Of the various factors implicated in the pathogenesis of OHE /
MHE, ammonia is the most important ( 4,13 ). Several trials using
ammonia-lowering therapies such as lactulose / lactitol, synbiotics /
probiotics, branched-chain amino acids, and dietary manipulation
have shown an improvement in MHE ( 14 – 28 ). However, the pos-
sible effi cacy of a non-absorbable antibiotic such as rifaximin to
modulate gut fl ora and reverse MHE has not been previously stud-
ied. Rifaximin is a gut-selective broad-spectrum antibiotic with
negligible systemic absorption. We chose rifaximin as the study
drug because it is relatively cheap, easily available, well tolerated,
and eff ective in reducing blood ammonia ( 39 ). Compared with lac-
tulose or neomycin, rifaximin has shown a general trend toward
better effi cacy, better safety, better tolerability, and lower hospitali-
zation rates in patients with OHE ( 30,31,39,40 ). Th e adverse eff ects
noted with rifaximin were either absent or were only minor gas-
trointestinal complaints ( 30,31,40,41 ). On the other hand, lactulose
is associated with annoying side eff ects such as fl atulence, abdomi-
nal discomfort, and diarrhea, which leads to low ( < 80 % ) adherence
( 3,29 ). Probiotics are another attractive option for MHE treatment,
but diffi culties in their availability and standardization remain.
Although there is evidence for the effi cacy of lactulose in MHE
( 14 – 21 ), we did not choose lactulose therapy for the control group
because of various reasons: (i) prescribing lactulose would make
blinding impossible and treatment bias will creep in; (ii) patients
would be exposed to unpleasant side eff ects of lactulose; and (iii)
the side eff ects of lactulose may aff ect the HRQOL assessment
( 42 ). Placebo group is important in any study on MHE, especially
in a new population, to highlight the importance of spontaneous
(without treatment) reversal of MHE, which may occur because of
learning eff ect or because of the fl uctuating course of MHE ( 43 ).
Th is trial scores over many of the previously conducted trials on
treatment of MHE ( 14 – 28 ) as it was a placebo-controlled double-
blinded study, it enrolled suffi cient number of patients to give a
power of > 90 % , and simultaneous evaluation of the HRQOL was
carried out. Of the previous trials, only three have simultaneously
checked for HRQOL. In an unblinded study, Prasad et al. ( 15 ) dem-
onstrated a signifi cant improvement in HRQOL (using SIP ques-
tionnaire) aft er lactulose treatment for 3 months. However, they
could not demonstrate a quantitative improvement in the NP test
results, possibly because of an inadequate number of patients on
follow-up. In the second trial, which used SF-36 questionnaire,
Bajaj et al. ( 23 ) demonstrated signifi cant improvement in MHE
aft er probiotic yogurt supplementation for 60 days. However, there
was no improvement in the HRQOL, which may be due to a shorter
questionnaire used or a milder effi cacy of yogurt. Liu et al. ( 24 )
demonstrated that synbiotics and fi ber modulate gut fl ora, reduce
blood ammonia, and lead to reversal of MHE. However, no HRQOL
assessment was carried out. A recent trial by Sharma et al. ( 14 )
documented an improvement in NP and neurophysiological tests
in ~ 54.3 % MHE patients treated with lactulose, probiotics, or both.
HRQOL assessment was not carried out in this trial, and no pla-
cebo arm was used. In two other trials, Malaguarnera et al. ( 25,26 )
showed improvement in NP test results in cirrhotics aft er treatment
with probiotics or acetyl- L -carnitine. However, they neither classi-
fi ed patients according to the MHE status nor checked for HRQOL.
Th erefore, convincing data regarding the effi cacy of any treatment,
except lactulose, to improve both cognitive functions and HRQOL
in patients with MHE is lacking. As rifaximin has better tolerabil-
ity than lactulose ( 30,31,40 ) and leads to an improvement in both
HRQOL and cognitive functions (as early as 2 weeks), as shown in
this study, it seems to be a better treatment option for MHE.
Our trial has few limitations. We did not measure ammonia lev-
els or infl ammatory markers to explore the mechanism of action of
Table 5 . Changes in SIP scores (ΔSIP) between 0 and 8 weeks among patients in placebo and rifaximin groups
Placebo group
( n =30) a Rifaximin group
( n =37) a P
value
Psychosocial scales
Social interac-tions
0.74 ( – 1.04 to 2.51) 5.34 (1.71 to 8.96) 0.046
Alertness 0.11 ( – 0.42 to 0.63) 1.25 ( – 0.20 to 2.20) 0.19
Emotional behavior
1.89 (0.55 to 3.23) 5.32 (2.67 to 7.97) 0.03
Communication – 0.71 ( – 1.44 to 0.03) 0.42 ( – 0.16 to 1.01) 0.01
Total sub-score
0.20 ( – 0.04 to 0.44) 1.23 (0.68 to 1.78) 0.003
Physical scales
Ambulation 0.96 ( – 0.58 to 2.50) 1.96 (0.85 to 3.07) 0.28
Mobility 5.18 (2.44 to 7.91) 13.56 (9.69 to 17.44) 0.04
Body care and movements
– 0.91 ( – 2.92 to 1.10) 4.25 (2.44 to 6.07) 0.00
Total sub-score
0.52 (0.18 to 0.86) 1.98 (1.54 to 2.42) 0.00
Independent scales
Sleep / rest – 0.40 ( – 1.90 to 1.10) 9.83 (7.59 to 12.07) 0.00
Work 0.55 ( 0.27 to 1.37) 1.36 (0.4 0 to 2.34) 0.32
Home management
1.97 (0.53 to 3.41) 0.72 ( – 1.36 to 2.79) 0.50
Recreation and past times
0.22 ( – 0.64 to 1.07) 1.23 ( – 0.21 to 2.67) 0.18
Eating 0.05 ( – 0.50 to 0.60) 0.82 (0.17 to 1.47) 0.08
Total SIP score 0.88 (0.47 to 1.29) 4.61 (3.76 to 5.46) 0.00
SIP, sickness impact profi le; Δ , change. Data are expressed as means (95 % confi dence interval). Negative values indicate poor performance. a Number of patients for whom SIP data were available.

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
315
LIV
ER
Rifaximin Improves Minimal Hepatic Encephalopathy
REFERENCES 1 . Ferenci P , Lockwood A , Mullen K et al. Hepatic encephalopathy – defi ni-
tion, nomenclature, diagnosis, and quantifi cation: fi nal report of the work-ing party at the 11th World Congresses of Gastroenterology, Vienna, 1998 . Hepatology 2002 ; 35 : 716 – 21 .
2 . Ortiz M , Jacas C , Cordoba J . Minimal hepatic encephalopathy: diagnosis, clinical signifi cance and recommendations . J Hepatol 2005 ; 42 : S45 – 53 .
3 . Bajaj JS . Management options for minimal hepatic encephalopathy . Expert Rev Gastroenterol Hepatol 2008 ; 2 : 785 – 90 .
4 . Mullen K , Ferenci P , Bass NM et al. An algorithm for the management of hepatic encephalopathy . Sem Liver Dis 2007 ; 27 : 32 – 48 .
5 . Weissenborn K , Giewekemeyer K , Heidenreich S et al. Attention, memory, and cognitive function in hepatic encephalopathy . Metab Brain Dis 2005 ; 20 : 359 – 67 .
6 . Groeneweg M , Quero JC , De Bruijn I et al. Subclinical hepatic encepha-lopathy impairs daily functioning . Hepatology 1998 ; 28 : 45 – 9 .
7 . Schomerus H , Hamster W . Quality of life in cirrhotics with minimal hepatic encephalopathy . Metab Brain Dis 2001 ; 16 : 37 – 41 .
8 . Romero-G ó mez M , Boza F , Garc í a-Valdecasas MS et al. Subclinical hepatic encephalopathy predicts the development of overt hepatic encephalopathy . Am J Gastroenterol 2001 ; 96 : 2718 – 23 .
9 . Das A , Dhiman RK , Saraswat VA et al. Prevalence and natural history of subclinical hepatic encephalopathy in cirrhosis . J Gastroenterol Hepatol 2001 ; 16 : 531 – 5 .
10 . Saxena N , Bhatia M , Joshi YK et al. Electrophysiological and neuropsycho-logical tests for the diagnosis of subclinical hepatic encephalopathy and prediction of overt encephalopathy . Liver 2002 ; 22 : 190 – 7 .
11 . Amodio P , Del Piccolo F , Marchetti P et al. Clinical features and survival of cirrhotic patients with subclinical cognitive alterations detected by the number connection test and computerized psychometric tests . Hepatology 1999 ; 29 : 1662 – 7 .
12 . Sugimoto R , Iwasa M , Maeda M et al. Value of the apparent diff usion coeffi cient for quantifi cation of low-grade hepatic encephalopathy . Am J Gastroenterol 2008 ; 103 : 1413 – 20 .
13 . Lockwood AH , Yap EW , Wong WH . Cerebral ammonia metabolism in patients with severe liver disease and minimal hepatic encephalopathy . J Cereb Blood Flow Metab 1991 ; 11 : 337 – 41 .
14 . Sharma P , Sharma BC , Puri V et al. An open-label randomized control-led trial of lactulose and probiotics in the treatment of minimal hepatic encephalopathy . Eur J Gastroenterol Hepatol 2008 ; 20 : 506 – 11 .
15 . Prasad S , Dhiman RK , Duseja A et al. Lactulose improves cognitive func-tions and health related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy . Hepatology 2007 ; 45 : 549 – 59 .
16 . Dhiman RK , Sawhney MS , Chawla YK et al. Effi cacy of lactulose in cirrhotic patients with subclinical hepatic encephalopathy . Dig Dis Sci 2000 ; 45 : 1549 – 52 .
17 . Watanabe A , Sakai T , Sato S et al. Clinical effi cacy of lactulose in cirrhotic patients with and without subclinical hepatic encephalopathy . Hepatology 1997 ; 26 : 1410 – 4 .
18 . Horsmans Y , Solbreux PM , Daenens C et al. Lactulose improves psycho-metric testing in cirrhotic patients with subclinical encephalopathy . Ali-ment Pharmacol Th er 1997 ; 11 : 165 – 70 .
19 . Zeng Z , Li YY . Eff ects of lactulose treatment on the course of subclinical he-patic encephalopathy [in Chinese] . Zhonghua Yi Xue Za Zhi 2003 ; 83 : 1126 – 9 .
20 . McClain CJ , Potter TJ , Kromhout JP et al. Th e eff ect of lactulose on psy-chomotor performance tests in alcoholic cirrhotics without overt hepatic encephalopathy . J Clin Gastroenterol 1984 ; 6 : 325 – 8 .
21 . Morgan MY , Alonso M , Stanger LC . Lactitol and lactulose for the treat-ment of subclinical hepatic encephalopathy in cirrhotic patients . J Hepatol 1989 ; 8 : 208 – 17 .
22 . Salerno F , Moser P , Maggi A et al. Eff ects of long term administration of low dose lactitol in patients with cirrhosis but without overt encephalopa-thy . J Hepatol 1994 ; 21 : 1092 – 6 .
23 . Bajaj JS , Saeian K , Christensen KM et al. Probiotic yogurt for the treatment of minimal hepatic encephalopathy . Am J Gastroenterol 2008 ; 103 : 1707 – 15 .
24 . Liu Q , Duan ZP , Ha DK et al. Symbiotic modulation of gut fl ora: eff ect on minimal hepatic encephalopathy in patients with cirrhosis . Hepatology 2004 ; 39 : 1441 – 9 .
25 . Malaguarnera M , Greco F , Barone G et al. Bifi dobacterium longum with fructo-oligosaccharide (fos) treatment in minimal hepatic encephalopa-thy: a randomized, double-blind, placebo-controlled study . Dig Dis Sci 2008 ; 52 : 3259 – 65 .
26 . Malaguarnera M , Gargante MP , Cristaldi E et al. Acetyl-L-carnitine treat-ment in minimal hepatic encephalopathy . Dig Dis Sci 2008 ; 53 : 3018 – 25 .
rifaximin. However, we believe that there are two possible mecha-
nisms by which rifaximin could lead to an improvement in MHE.
First, by decreasing the ammonia-producing bacteria in the gut,
it could lead to a decrease in serum ammonia concentration, as
already shown in a previous study ( 39 ). Second, rifaximin could
be a key factor in decreasing bacterial translocation and infl am-
mation, thus improving MHE. Th is hypothesis needs to be studied
in future trials. A second limitation of our trial was that follow-up
of patients aft er stopping the treatment was not done. Future pro-
spective trials are required to study the impact of rifaximin treat-
ment on the natural history of MHE, that is, prevention of further
episodes of MHE or development of OHE. Now that the present
trial has shown rifaximin to be benefi cial in MHE, we also propose
a head-to-head trial of rifaximin vs. lactulose / probiotics to com-
pare their effi cacy with reverse MHE and improve HRQOL.
We conclude that MHE is common in patients with cirrhosis.
MHE leads to diminished HRQOL and has a global impact on
day-to-day activities. Th erefore, all patients with cirrhosis, irre-
spective of their job profi le, deserve screening and treatment for
MHE to improve their quality of life. Rifaximin is a safe and eff ec-
tive treatment for improving cognitive functions and HRQOL in
patients with MHE.
ACKNOWLEDGMENTS Th e sickness impact profi le questionnaire was provided by the MAPI
Research Trust, Information Resources Centre, Lyon, France.
CONFLICT OF INTEREST Guarantor of article: Sandeep Singh Sidhu, MBBS, MD, DM.
Specifi c author contributions: Data collection and conduct of the
study: Omesh Goyal and Bholeshwar Prasad Mishra; draft ing and
conceptualization of the study: Ajit Sood and Rajoo Singh Chhina;
statistical analysis and draft ing of the manuscript: Ravinder Kumar
Soni. All authors reviewed and approved the fi nal manuscript.
Financial support : Th is work was supported by the Department
of Gastroenterology, Dayanand Medical College and Hospital,
Ludhiana, Punjab, India. Study drugs (rifaximin and placebo) were
provided by LUPIN limited, Laxmi towers, Plot No. C-25, C Wing,
4th fl oor, Bandra Kurla Complex, Mumbai- 400051, India.
Potential competing interests: None.
Study Highlights
WHAT IS CURRENT KNOWLEDGE
3 Minimal hepatic encephalopathy (MHE) is common and leads to poor quality of life.
3 Treatment for minimal hepatic encephalopathy is evolving.
3 Lactulose although effective, has concerns of poor tolerability.
3 Role of non-absorbable antibiotics for treatment of MHE has never been studied.
WHAT IS NEW HERE
3 Rifaximin leads to signifi cant improvement in cognitive functions and reversal of MHE.
3 Rifaximin leads to signifi cant improvement in quality of life in patients with MHE.

316 LI
VE
R
The American Journal of GASTROENTEROLOGY VOLUME 106 | FEBRUARY 2011 www.amjgastro.com
Sidhu et al.
27 . de Bruijn KM , Blendis LM , Zilm DH et al. Eff ect of dietary protein manip-ulation in subclinical portal-systemic encephalopathy . Gut 1983 ; 24 : 53 – 60 .
28 . Egberts EH , Schomerus H , Hamster W et al. Branched chain amino acids in the treatment of latent portosystemic encephalopathy. A double blind placebo-controlled crossover study . Gastroenterology 1985 ; 88 : 887 – 95 .
29 . Qadri AM , Ogunwale BO , Mullen KD . Can we ignore minimal hepatic encephalopathy any longer? Hepatology 2007 ; 45 : 547 – 8 .
30 . Maclayton DO , Eaton-Maxwell A . Rifaximin for treatment of hepatic encephalopathy . Ann Pharmacother 2009 ; 43 : 77 – 84 .
31 . Jiang Q , Jiang XH , Zheng MH et al. Rifaximin vs. nonabsorbable disaccha-rides in the management of hepatic encephalopathy: a meta-analysis . Eur J Gastroenterol Hepatol 2008 ; 20 : 1064 – 70 .
32 . Ramalingaswamy P . Manual of Indian Adaptation of WAIS Performance Scale . Manasayan: Delhi , 1974 , 2 – 29 .
33 . Dhiman RK , Saraswat VA , Verma M et al. Figure connection test: a universal test for assessment of mental state . J Gastroenterol Hepatol 1995 ; 10 : 14 – 23 .
34 . Bergner M , Bobbitt RA , Cartner WB et al. Th e sickness impact profi le: development and fi nal revision of a health status measure . Med Care 1981 ; 19 : 787 – 805 .
35 . Hartmann IJ , Groeneweg M , Quero JC et al. Th e prognostic signifi cance of subclinical hepatic encephalopathy . Am J Gastroenterol 2000 ; 95 : 2029 – 34 .
36 . Wein C , Koch H , Popp B et al. Minimal hepatic encephalopathy impairs fi tness to drive . Hepatology 2004 ; 39 : 739 – 45 .
37 . Bajaj JS , Hafeezullah M , Hoff mann RG et al. Minimal hepatic encepha-lopathy: a vehicle for accidents and traffi c violations . Am J Gastroenterol 2007 ; 102 : 1903 – 9 .
38 . Bajaj JS , Hafeezullah M , Zadvornova Y et al. Th e eff ect of fatigue on driv-ing skills in patients with hepatic encephalopathy . Am J Gastroenterol 2009 ; 104 : 898 – 905 .
39 . Pedretti G , Calzetti C , Missale G et al. Rifaximin vs. neomycin on hyperammoniemia in chronic portal systemic encephalopathy of cirrhotics. A double-blind, randomized trial . Ital J Gastroenterol 1991 ; 23 : 175 – 8 .
40 . Leevy CB , Phillips JA . Hospitalizations during the use of rifaximin vs. lactulose for the treatment of hepatic encephalopathy . Dig Dis Sci 2007 ; 52 : 737 – 41 .
41 . Bass NM , Mullen KD , Sanyal A et al. Rifaximin treatment in hepatic en-cephalopathy . N Engl J Med 2010 ; 362 : 1071 – 81 .
42 . Kalaitzakis E , Bjornsson E . Lactulose treatment for hepatic encephalopathy, gastrointestinal symptoms, and health-related quality of life . Hepatology 2007 ; 46 : 949 – 50 .
43 . Tan HH , Lee GH , Th ia KT et al. Minimal hepatic encephalopathy runs a fl uctuating course: results from a three-year prospective cohort follow-up study . Singapore Med J 2009 ; 50 : 255 – 60 .
All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.
Copyright © 2022 FDOKUMEN







![Giosue Carducci - Rime nuove [ebook ITA]](https://static.fdokumen.com/doc/165x107/6345631cf474639c9b04d2fd/giosue-carducci-rime-nuove-ebook-ita.jpg)












