Rethinking breast cancer risk and the environment: the case for the precautionary principle
7
Commentaries Rethinking Breast Cancer Risk and the Environment: The Case for the Precautionary Principle Devra Lee Davis,1'2 Deborah Axelrod,3 Lisa Bailey,4 Mitchell Gaynor,2 and Annie J. Sasco5 1World Resources Institute's Health, Environment, and Development Program, Washington, DC 20006 USA; 2Cornell Medical School, Strang Cancer Prevention Center, New York, NY 10021 USA; 3Beth Israel Medical Center, New York, NY 10003 USA; 4American Cancer Society, Oakland, CA 94612 USA; 5Unit of Epidemiology for Cancer Prevention, International Agency for Research on Cancer and Institut National de la Sante et la Recherche Medicale, Lyon, France The World Health Organization recently reported that breast cancer has become the most com- mon cancer in women throughout the world. Known risk factors account for less than half of all cases of breast cancer, and inherited germ line mutations occur in at most only 10% of all cases. Cumulative exposure to estradiol and other hormones link many of the established risk factors for breast cancer. This paper reviews epidemiologic and toxicologic evidence on breast cancer risks and presents a comprehensive construct of risk factors intended to focus on the identification of those factors that can be controlled or modified. We attempt to provide a framework for inter- preting the etiologic interplay of endogenous metabolic changes and environmental changes in the etiology of breast cancer. The construct we develop distinguishes between those risk factors that are directly causal, such as ionizing radiaton and inherited germ cell defects, those vulnerabdity factors that extend the time period during which the breast undergoes development, and those contributing factors that increase total hormonal stimulation of the breast. Some hormonally active compounds, such as those in soy and broccoli and other phytoesogen-containing foods, can be protective against breast cancer, while others, such as some environmental contaminants, appear to increae the risk of the disee by increasing levels of harmfud hormones. Efforts to explain patterns of breast cancer should distinguish between these different risk factors. Identification of vulnerability and contributing risk factors can foster the development of public policy to reduce the burden of this prevaent cancer. Prdent preautionary principles sugest that reducing exposure to avoidable or modifiable risk factors should receiver high priority from the public and private sectors. Key words. breast cancer, environment, hormones, prevention, risk fac- tors, theory. Environ Heal PenPect 106:523-529 (1998). [Online 17 August 1998] hatp.:lehpnetl.nihs. nih.gov/docs/1998/1 06p523-529daWabstrac html The World Health Organization recently reported that breast cancer has become the most common cancer in women through- out the world (1-3). The causes of this global pattern are not well understood. In those few countries where mammographic screening is routinely available, such as the United States and some provinces of Canada, increased ascertainment accounts for some of the recorded increase in inci- dence. In the United States recently, declines in breast cancer mortality have been reported for white and African- American women under 65 years of age (4). But changes in known risk factors, diagnostic procedures, or aging cannot account for domestic and worldwide pat- terns in breast cancer incidence and mor- tality. From 1973 to 1987, when routine population mammographic screening was not yet practiced, age-adjusted mortality increased in both developed and develop- ing countries (see Fig. 1 and 2). During this period, breast cancer mortality grew 20% or more in several central European countries and Japan, with rates of breast cancer being about four times lower in most Asian countries. Established Risk Factors for Breast Cancer Less than 10% of all breast cancer develops in women who have inherited germ cell mutations such as loss of tumor-suppressor genes including p53, BRCA1, BRCA2, or ATM (5,6). Established risk factors, which have been identified in less than half of all women with breast cancer (0, include inher- ited genetic defects, menarche before age 12, menopause after age 55, having either no pregnancy or late childbearing, no lactation, early or repeated exposures to radiation, pro- longed use of hormone replacement therapy, increased breast density, higher socioeco- nomic status, and postmenopausal obesity. Most of these risk factors can be linked with increased lifetime exposure to estrogen, other hormones, and higher exposures early in life (8-11). Most of these risk factors are not eas- ily modifiable (12). Breast development depends on the complex interplay of estro- gen, progesterone, and other growth factors. Therefore, the earlier in life that regular menses begins and the later that it ceases, the greater exposure to hormones that affect breast growth in a woman's life (13). Risk Factors In an effort to identify public policies that can be developed to reduce breast cancer, this paper distinguishes between risk factors that directly cause breast cancer, those that extend the time period of vulnerability of the breast by prolonging breast development and conse- quent susceptibility to damage, and those that contribute to altered levels of cancer- causing endogenous or xenohormones. What exactly do these demonstrated risk factors for breast cancer tell us? In fact, with the notable exceptions of ionizing radiation and inherited genetic damage, none of the established risk factors for breast cancer directly causes the Address correspondence to D.L. Davis, 1709 New York Avenue NW, Washington, DC 20006 USA. We thank J. Shaloff, A.O. Ip, M.J. Pongsiri, and K. Ahmed for assistance in the development of many drafts of this paper. Members of the Breast Cancer Prevention Collaborative Research Group provided important technical assistance, including H.L. Bradlow, L. Jones, M. Wolff, P. Madigan, L. Brinton, S. Zahm, and S. Sieber. This work was supported in part by grants from the following: Wallace Genetics, the Goldnman Fund, the Jennifer Altman Fund, the Breast Cancer Fund, the Starfire Fund, and program support from the American Cancer Society and the World Resources Institute. This paper is based on special lectures pre- sented to the Lemelson Center for Invention and Innovation of the Smithsonian Institution, National Museum of American History, and to the Jennifer Altman Fund. Received 15 May 1998; accepted 5 August 1998. Environmental Health Perspectives * Volume 106, Number 9, September 1998 The Precautionary Principle We must act on facts, and on the most accurate interpretation of them, using the best scientific information. That does not mean we must sit back until we have 100% evidence about every- thing. Where the state of the health of the people is at stake, the risks can be so high and the costs of corrective action so great, that prevention is better than cure. We must analyze the possible benefits and costs of action and inaction. Where there are significant risks of damage to the pub- lic health, we should be prepared to take action to diminish those risks even when the scientific knowledge is not conclusive, if the balance of likely costs and benefits justifies it. [Horton R The New New Public Health of Risk and Radical Engagement (editorial). Lancet352(9124):251 (1998).] 523
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Rethinking breast cancer risk and the environment: the case for the precautionary principle

Commentaries
Rethinking Breast Cancer Risk and the Environment: The Case for thePrecautionary PrincipleDevra Lee Davis,1'2 Deborah Axelrod,3 Lisa Bailey,4 Mitchell Gaynor,2 and Annie J. Sasco51World Resources Institute's Health, Environment, and Development Program, Washington, DC 20006 USA; 2Cornell Medical School,Strang Cancer Prevention Center, New York, NY 10021 USA; 3Beth Israel Medical Center, New York, NY 10003 USA; 4American CancerSociety, Oakland, CA 94612 USA; 5Unit of Epidemiology for Cancer Prevention, International Agency for Research on Cancer andInstitut National de la Sante et la Recherche Medicale, Lyon, France
The World Health Organization recently reported that breast cancer has become the most com-
mon cancer in women throughout the world. Known risk factors account for less than half of allcases of breast cancer, and inherited germ line mutations occur in at most only 10% of all cases.
Cumulative exposure to estradiol and other hormones link many of the established risk factorsfor breast cancer. This paper reviews epidemiologic and toxicologic evidence on breast cancer risksand presents a comprehensive construct of risk factors intended to focus on the identification ofthose factors that can be controlled or modified. We attempt to provide a framework for inter-preting the etiologic interplay ofendogenous metabolic changes and environmental changes in theetiology of breast cancer. The construct we develop distinguishes between those risk factors thatare directly causal, such as ionizing radiaton and inherited germ cell defects, those vulnerabdityfactors that extend the time period during which the breast undergoes development, and thosecontributing factors that increase total hormonal stimulation of the breast. Some hormonallyactive compounds, such as those in soy and broccoli and other phytoesogen-containing foods,
can be protective against breast cancer, while others, such as some environmental contaminants,
appear to increae the risk of the disee by increasing levels of harmfud hormones. Efforts to
explain patterns of breast cancer should distinguish between these different risk factors.Identification of vulnerability and contributing risk factors can foster the development of publicpolicy to reduce the burden of this prevaent cancer. Prdent preautionary principles sugest thatreducing exposure to avoidable or modifiable risk factors should receiver high priority from thepublic and private sectors. Key words. breast cancer, environment, hormones, prevention, risk fac-tors, theory. Environ Heal PenPect 106:523-529 (1998). [Online 17 August 1998]hatp.:lehpnetl.nihs.nih.gov/docs/1998/106p523-529daWabstrac html
The World Health Organization recentlyreported that breast cancer has become themost common cancer in women through-out the world (1-3). The causes of thisglobal pattern are not well understood. Inthose few countries where mammographicscreening is routinely available, such as theUnited States and some provinces of
Canada, increased ascertainment accounts
for some of the recorded increase in inci-dence. In the United States recently,declines in breast cancer mortality havebeen reported for white and African-American women under 65 years of age
(4). But changes in known risk factors,diagnostic procedures, or aging cannot
account for domestic and worldwide pat-terns in breast cancer incidence and mor-
tality. From 1973 to 1987, when routinepopulation mammographic screening was
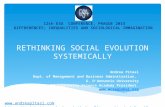
not yet practiced, age-adjusted mortalityincreased in both developed and develop-ing countries (see Fig. 1 and 2). Duringthis period, breast cancer mortality grew
20% or more in several central Europeancountries and Japan, with rates of breastcancer being about four times lower inmost Asian countries.
Established Risk Factors forBreast CancerLess than 10% of all breast cancer developsin women who have inherited germ cellmutations such as loss of tumor-suppressorgenes including p53, BRCA1, BRCA2, or
ATM (5,6). Established risk factors, whichhave been identified in less than half of all
women with breast cancer (0, include inher-ited genetic defects, menarche before age 12,menopause after age 55, having either no
pregnancy or late childbearing, no lactation,early or repeated exposures to radiation, pro-
longed use of hormone replacement therapy,increased breast density, higher socioeco-nomic status, and postmenopausal obesity.Most of these risk factors can be linked withincreased lifetime exposure to estrogen, otherhormones, and higher exposures early in life(8-11). Most of these risk factors are not eas-
ily modifiable (12). Breast developmentdepends on the complex interplay of estro-
gen, progesterone, and other growth factors.Therefore, the earlier in life that regularmenses begins and the later that it ceases, thegreater exposure to hormones that affectbreast growth in a woman's life (13).
Risk FactorsIn an effort to identify public policies thatcan be developed to reduce breast cancer, thispaper distinguishes between risk factors thatdirectly cause breast cancer, those that extendthe time period of vulnerability of the breastby prolonging breast development and conse-
quent susceptibility to damage, and thosethat contribute to altered levels of cancer-
causing endogenous or xenohormones. Whatexactly do these demonstrated risk factors forbreast cancer tell us? In fact, with the notableexceptions of ionizing radiation and inheritedgenetic damage, none of the established riskfactors for breast cancer directly causes the
Address correspondence to D.L. Davis, 1709 NewYork Avenue NW, Washington, DC 20006 USA.We thank J. Shaloff, A.O. Ip, M.J. Pongsiri, and K.Ahmed for assistance in the development of manydrafts of this paper. Members of the Breast CancerPrevention Collaborative Research Group providedimportant technical assistance, including H.L.Bradlow, L. Jones, M. Wolff, P. Madigan, L.Brinton, S. Zahm, and S. Sieber.This work was supported in part by grants from thefollowing: Wallace Genetics, the Goldnman Fund,the Jennifer Altman Fund, the Breast Cancer Fund,the Starfire Fund, and program support from theAmerican Cancer Society and the World ResourcesInstitute. This paper is based on special lectures pre-sented to the Lemelson Center for Invention andInnovation of the Smithsonian Institution, NationalMuseum of American History, and to the JenniferAltman Fund.Received 15 May 1998; accepted 5 August 1998.
Environmental Health Perspectives * Volume 106, Number 9, September 1998
The Precautionary Principle
We must act on facts, and on the most accurateinterpretation of them, using the best scientificinformation. That does not mean we must sitback until we have 100% evidence about every-thing. Where the state of the health of the peopleis at stake, the risks can be so high and the costsof corrective action so great, that prevention isbetter than cure. We must analyze the possiblebenefits and costs of action and inaction. Wherethere are significant risks of damage to the pub-lic health, we should be prepared to take actionto diminish those risks even when the scientificknowledge is not conclusive, if the balance oflikely costs and benefits justifies it.
[Horton R The New New Public Health ofRisk and Radical Engagement (editorial).
Lancet352(9124):251 (1998).]
523

Commentaries * Davis et al.
lapan
Norway
Netherlands
Italy
United Kingdom
France
Finland
United States
Canada
Percent
Figure 1. Percent change in breast cancer mortality in developeInternational Agency for Research on Cancer (3).
Mauritius
Costa Rice
Portugal
Poland
Hungary
Yugoslavia
Bulgaria
Czechoslovakia
1015 2025
Percent
Figure 2. Percent change in breast cancer mortalityInternational Agency for Research on Cancer (3).
disease (14). Radiation and inherited defectscan be said to cause breast cancer in that theyproduce alterations in cell growth, repair,and metabolism that are understood to bemechanistically linked with the developmentof breast cancer. According to accepted epi-demiological criteria, risk factors can beextracted from studies that consistentlyreveal an association between certain condi-tions that precede the development of breastcancer (15). Even where such criteria aremet, a fundamental question must beanswered: Is the association between theserisk factors and the disease due to somedirect mechanism or causal link? Outside ofpharmaceutical and other medical interven-tions such as diagnostic radiation, which arestudied under controlled conditions, fewhuman exposures can be directly linked withspecific health consequences.
A variety of studies indicate that thepotential for aberrant growth is dependent
,in developir
on two fithe extening radiadifferentitiming otently coradiationgreater rthan do (
levels of c
Thesbreast cimportar
which occur when breasts are undergoingrapid cell differentiation, cell growth, ordevelopment of the whole gland duringpuberty could also be especially importantcauses of breast cancer.
Vulnerability FactorsMore rapidly developing cells, such asthose of the prepubescent breast, are at aspecial state of vulnerability. Vulnerabilityfactors for breast cancer are those thatextend the time during which the breast isgrowing and the rate of this growth. Forinstance, early menses, no lactation, andlate menopause prolong the time periodduring which the developing breast ispotentially exposed to estradiol and delete-rious agents (see Fig. 3). Evidence for thisincreased vulnerability is provided by
,d countries, 1973-1987. Data from the observations of women born to motherswho had unusually high or low levels ofestrogen during pregnancy. Toxemia is tiedwith preeclampsia and lower levels of estro-gen. Women born to mothers who weretoxemic had an adjusted odds ratio (OR)of 0.41 for breast cancer compared to thosewho underwent normal pregnancy. In con-trast, women who experienced elevated lev-
M11_ els of hormones prenatally or neonatallywere found to have an OR of 3.96 (18).
Regarding the risk factor of lactation,the situation is complex. Lactation is apotentially modifiable factor that can beconsidered as both a vulnerability and acontributing risk. Premenopausal womenwho lactated have a reduced risk of breastcancer, with further significant reductionsof risk for women who lactate earlier or forlonger cumulative duration. Animal studies
ig countries, 1973-1987. Data from the have demonstrated that early reproductivelife breast tissue is positively influenced bylactation (19). Immediately before and
actors: the rate of cell growth and after the termination of pregnancy, thet of exposure (16). Even for ioniz- rapidly growing or lactating breast may alsotion, the same dose can produce be at risk from proliferative processes andial responses depending upon the agents. After lactation ends, the breastif exposure. Studies have consis- becomes more differentiated, reducing sus-infirmed that females exposed to ceptibility to such agents (20). However,i prior to puberty have a much postmenopausal women who have lactatedisk of developing breast cancer do not show reduced risk of breast cancerolder women subject to the same in comparison to women who have not lac-!xposure (Se. tated (19). This may reflect the fact thate findings about radiation and cumulative exposures to other cancer-caus-ancer highlight a profoundly ing xenohormones overwhelm any earlierlt component of risk factors for protective effects from lactation.
diseases with long latency: timing of expo-sure can be more important than dose.Radiation during the critical periods whenbreast cells are first forming prenatally orduring early adolescence induces propor-tionally more neoplastic transformation ofcells and is thereby more carcinogenic thanexposures that occur later in life (17). Thissuggests that other carcinogenic exposures
Contributing FactorsContributing factors can directly affect over-all exposure to circulating hormones and caninteract with vulnerability factors. Some hor-mones are potent stimulators of cell growth(21), and some hormonal metabolites canbind to DNA and trigger aberrant cellgrowth (22,23). Alcohol, lack of exercise,
Volume 106, Number 9, September 1998 * Environmental Health Perspectives524

Commentaries * Rethinking breast cancer risk and the environment
diets low in fiber and vitamin D, and expo- cells, making themsure to some pesticides, solvents, fuels, and quent exposures. W]pharmaceuticals increase the total amount of ulating agents, tibioavailable estradiol (20). Bioavailable estra- respond more quickdiol represents the fraction of estradiol that is growth renders tissuinot readily excreted when bound to sex hor- to carcinogens or]mone-binding globulin (SHBG) or albumin pounds. In a simila(24). This binding reduces the availability of exposures can expedestradiol to the cells. Thus, processes that breast growth anddecrease hormone binding increase circulat- More rapidly develcing levels of estradiol. Contributing factors to sustaining aberrarcan also alter metabolism of other growth- anisms can be swarregulating hormones that alter breast cell menses or obesity agrowth and metabolism and increase the cumulative exposurlikelihood of aberrant cell growth. lites as adipose cells
Alcohol is a prime example of a risk fac- gens. Thus, exposuitor that may increase the circulation of hor- can alter both the lmones, thereby rendering it a contributing hormonal stimulaticrisk factor. A large nurses' health study(25), later corroborated by a women's Role of Hormhealth study (26), determined that post- Clinical and animalmenopausal women who consumed alcohol lifetime exposure tomanifested a 40% increased risk of breast estradiol predictscancer with estrogen administration, while (31,32). Under onthose who did not consume alcohol or con- alter hormonal metasumed it at levels below the average daily of breast cancer wintake of 5 g showed no increased risk. and/or hormonal paWhen alcohol interacts with estrogen, the paths to breast can(bioavailable estradiol level rises sharply indicates that differeabove breast cancer-promoting levels for ol oxidation have Fwomen in general (27). Another explana- logical effects (seetion as to why regular consumption of humans is hydroxylalcohol increases breast cancer likelihood is irreversible and mbecause ethanol is directly estrogenic (28). ways- 16 a-hydro)When additional direct risk factors, such asinherited genetic mutations and p53 genes(29) are taken into account, the effects ofalcohol are magnified (30).
Critical Windows of ExposureUnder this emerging paradigm, three distinctcritical windows need to be considered: pre-natal, prepubescent, and perimenopausal.Prenatal exposure to elevated levels of estradi-ol or other growth-regulating hormonesthroughout gestation may imprint breast
Risk fctors for breast cancer
* Radiaton, especially during puberty* Inherited mutations
* Lack of exercise / Early menses* Excess of alcohol Lae* Earmenopause*Deficiencies of vitamin D, *N opregnancy or lacteion
fiber, melatonin??* Harmful xenohormonesIsome plastics, fuels,pesticides)
* Increased insulin-likegrowth factor
Figure 3. Risk factors can be distinguished in terms of their ability to causebreast cancer directly, through genetic damage, or by altering hormonalmetabolism. Vulnerability factors prolong the duration of breast cell growth,while contributing factors can distort hormone levels.
more sensitive to subse-hen later exposed to stim-hese primed cells mayly. Thus, early breast celle subsequently vulnerablehormonally active com-ar manner, prepubescentite the process of aberrantattendant susceptibility.oping cells may be pronent growth, as repair mech-mped. Extended lifetimefter menopause increasesres to hormonal metabo-in fat tissue release estro-ires at these critical timesmagnitude and extent ofDn of the breast.
onal Metabolitesstudies indicate that totalunbound or bioavailable
s risk of breast cancere theory, exposures thatabolites can affect the riskrorking through geneticaths (33). As to hormonalicer, an array of evidencent by-products of estradi-profoundly different bio-Fig. 4) (34). Estrone inlated to form one or twoLutually exclusive path-xyestrone (16-OHEI) or
2-hydroxyestrone (2-OHE1) (35). The for-mer metabolite appears to bind covalently tothe estrogen receptor (ER), while the latterstimulates cell repair and inhibits cancer.Another estradiol metabolite, 4-hydroxye-strone (4-OHEI), also appears highly car-cinogenic, although its significance forhumans is not clear (22). Two distinct mech-anisms can influence the potential for aber-rant cell growth: materials can directly bindwith hormone receptors altering cell prolifer-ation, or they can modify breast cell prolifera-tion by affecting the intricate balancebetween key hormonal metabolites that influ-ence parenchymal growth factors in otherways. Some studies have found that exposinghuman breast cancer cells that are ER positiveto lipophilic organochlorine compoundsincreases 16-OHEI and suppresses 2-OHEI(36), as do known mammary carcinogenssuch as dimethylbenzanthracene.
Concerning genetic paths, xenohormonescan cause structural or functional damage toDNA (37). Functional damage can affectprocesses of cell growth, the ability of tumor-suppressor genes to restrain malignantgrowth, and the expression of telomerase toovercome cellular senescence. Such damageimpedes critical cell repair systems, hindersrecognition of aberrant cells, and allows theaccumulation of harmful mutations.Structural damage to DNA can occur fromgenotoxic agents and from free radical orredox cycling of harmful xenoestrogens that
Bifnctonal pathways to breast cancer
o/ \7
'7Figure 4. Bifunctional pathways to breast cancer. Abbreviations: E2, 17p-estra-diol; E1, estrone; OHE1, hydroxyestrone; ER, estrogen receptor. In the bifunc-tional pathway, the E2 metabolites affect cell proliferation and breast cancerdevelopment either directly via receptor-independent mechanisms involvingstructural/functional alterations in DNA, or indirectly via receptor-dependentmechanisms involving phenotypic growth regulation. Both mechanisms even-tually upregulate aberrant proliferation and development of breast cancer (37).
Environmental Health Perspectives * Volume 106, Number 9, September 1998 525

Commentaries * Davis et al.
produce reactive oxygen species. This redoxcycling yields high rates of radical-inducedDNA damage, including 8-hydroxyguanineand adenine adducts, apurinic sites, or loss ofring opening products (e.g., 2,6-diamino-4-hydroxy-5-formamidopyrimidine) (38,39).Women with breast cancer have been report-ed to have significandy higher rates of suchradical-induced damage than do womenwithout the disease (40).
Not all xenohormones disrupt normalendocrine functioning or damage DNA.Many are "good" xenoestrogens that bindstrongly with the ER and appear to have pro-tective effects. Several of these are found inplants, e.g., daidzein, genistein, isoflavonoids,as well as in fish oil (41-43). Some of themappear to serve as antioxidants. Certain goodxenoestrogens inhibit angiogenesis or proteaseor kinase activity. In this manner they canreduce the propensity of aberrant breast cellsto proliferate, increase DNA repair, or pro-duce other changes in the genetic or hormon-al microenvironments that alter malignantprogression (44).
Unexplained Patterns ofBreast CancerOur proposed conceptual framework canpartly account for the observed temporalchanges in some established risk factors forbreast cancer, such as the decline in age atmenarche over the last half-century. It ispossible that this decline could reflectchanges in both vulnerability and con-tributing factors. In part, increased totalcaloric intake in the diet has resulted in girlsaccumulating proportionally more body fat.Fat is a direct source of estrogens earlier inlife. Those who are heavier earlier in lifewill experience menses and their breasts willbegin developing at earlier ages. In addi-tion, the extensive use of growth hormones,including diethylstilbestrol and other estro-genic compounds, in domestic animalproducts and the bioaccumulation of suchxenohormones as organochlorine pesticidesmay also contribute to early menarche andelevate circulating levels ofhormones.
Factors may contribute to breast cancerby impairing the function of tumor-suppres-sor genes such as p53 expression or byimpeding the ability of proteins such as tyro-sine kinase and protein kinase C functions(45) to detoxify and excrete carcinogens. Anexpanding scientific literature indicates thatprostaglandin levels are higher in canceroustissue than in normal tissue (46). Cancer ofthe breast forms more prostaglandins thannormal breast tissue (47). Up regulation ofthe cyclooxygenases (Cox-1 and Cox-2) cat-alyzes the formation ofprostaglandins, whichin turn have multiple effects that favor car-cinogenesis. Contributing factors that inhibit
Cox activity reduce the risk of colon, breast,and lung cancer in animals and humans.Prostaglandins such as PGF 2 and PGE 2 areimportant factors during fetal development,ovulation, and luteinization. Contributingfactors can convert procarcinogens to car-cinogens via Cox-mediated metabolism ofarachidonic acid.
Because carcinogens such as benzopy-rene induce Cox-2, these may be importantfor the development of breast cancer aswell. Overexpression of Cox-2 inhibitsapoptosis and enhances invasiveness ofmalignant cells. Young women exposed toagents that exacerbate such overexpressionare likely to be at increased risk for cancer.Thus, it is logical to expect that those indi-viduals with inherited or environmentallyincreased levels of carcinogen-activatingenzymes such as Cox-2 will have enhancedcancer vulnerability (48), while those withlower levels will have reduced risk (49). Inaddition, decreased dietary intake of thenatural Cox-2 inhibitors such as soyisoflavones, curcumin, and retinoid is aprobable vulnerability factor for the devel-opment of breast cancer.
The framework we offer can alsoaccount for differences in rates of breastcancer in some areas. Lower rates of breastcancer have consistently been found inwomen living in Asian countries, althoughrates have increased recently (50).Pollution in this region is not known to beparticularly low; in fact levels are consider-ably elevated in China (51). But diets havetraditionally been rich in protective factorssuch as soy products, fish, and vegetablesand low in animal dairy products that canconcentrate some contaminants. Theseprotective factors may account for the rela-tively low rates of breast cancer and otherhormonally mediated diseases in Asianwomen (50).
Inconsistent ResultsRecent human studies have focused onassessing the impact of organochlorinecompounds and have not addressed thebroad array of other suspect xenohor-mones, many of which leave no biologicmarkers, such as benzo[a]pyrene, someplastics, and fuels. Nor have protective fac-tors such as genistein and other isoflavonesbeen widely studied. Organochlorines havebeen studied largely because these com-pounds are persistent and can be measuredyears after exposures have occurred. Studiesof these lipophilic compounds have pro-duced inconsistent results. Results of someof the early studies on organochlorineresidues tended to be positive, with higherlevels of polychlorinated biphenyls (PCBs)and dichlorodiphenyldichloroethylene
(DDE), either in the blood or in adiposetissue, found among women with breastcancer than in controls (52,53). In addi-tion, nested case-control prospective stud-ies in this field have tended to yield posi-tive results, especially those that havelooked at ER positive cases (54). Thus, asmall case-control study in Canada foundthat women with elevated levels of DDEhad 8.9 times the risk of ER positive dis-ease than did women with relatively lowerlevels of this metabolite (54). ER positivecases appear to be increasing overall inwomen over 60 years of age, according toone report from California (55). In somestudies, negative results were also describedfor the total cancer study population (56)or for specific subgroups of breast cancersubjects, such as Asian women (57).
Three recent case-control studies(56,58,59) of organochlorine residues havereported that when first diagnosed, womenwith breast cancer actually have lower levelsof these compounds in their bodies com-pared with cases that do not have these dis-eases. These studies could not examine therole of exposures during critical windowsearlier in life, but looked only at residuesremaining after the disease was expressed.In all of these studies, levels of these conta-minants measured after the disease hasbeen detected are severalfold lower thanthose reported three decades earlier, indi-cating the success of programs to reducethe use of these materials (1). Negativestudies should be considered separately interms of the regions involved and in termsof the compounds measured.
In two of these studies, which wereconducted outside the United States(56,59), the authors have indicated that amajority of the cases were stage II or IIIwhen sample collection was undertaken. Inthese circumstances, preclinical disease mayhave altered lipid metabolism, which couldaccount for the fact that these patientstended to have lower levels of someorganochlorine compounds. One of thestudies, which was conducted in Germany,the Netherlands, Northern Ireland,Switzerland, and Spain, found significantlyhigher means of DDE in controls than incases (59); the OR comparing the highestto the lowest tertiles of DDE indicated areduced risk for the most highly exposedsubjects. Results are less clear in the otherstudy (61), which was conducted inMexico, a country where DDT is still inuse. The arithmetic and geometric meansof DDE were somewhat higher amongcases than among controls; but this findingwas not statistically significant. However,reduced ORs were found when the highestand lowest tertiles were compared (56).
Volume 106, Number 9, September 1998 * Environmental Health Perspectives526

Commentaries * Rethinking breast cancer risk and the environment
In the United States, a recent nestedcase-control study of the Nurses' HealthStudy (58) examined 240 cases, 200 ofwhich involved invasive disease. Samplesobtained in the 2 years before diagnosisshowed relatively low levels ofDDE metabo-lites in this group, with levels being six timeslower than those found in U.S. women inthe 1970s (58). As with the recent foreignstudies, it is undear whether these lower lev-els in cases are a consequence of the diseasebecause blood was analyzed when the cancerprocess had been underway for periods of upto a decade or more. Also, data were not col-lected on the role of protective factors suchas natural Cox-2 inhibitors and protectivephytoestrogens, such as those found in soyand fish oil, nor was information obtainedon possible exposures earlier in life.Moreover, residues ofDDE measured in theplasma did not show the same estrogenicactivity as the parent mixtures. In fact, DDEacts primarily as an antiandrogen (60). Themost highly estrogenic contaminants cannotbe detected years after exposure.
A more recent report from this sameresearch group used a prospective designand confirmed that early exposures togrowth factors can be significant, especiallyfor premenopausal causes of breast cancer.This new study found that premenopausalcases of breast cancer with the highest levelsof insulin-like growth factor-1 as measured4 years or more before diagnosis had nearlya sevenfold greater risk of breast cancercompared to those without the disease (61).This finding indicates the importance oflooking at a broad array of potential protec-tive and disruptive factors, as well as thevalue of conducting longer term prospectivestudies that permit their identification.
Studies that consider current levels ofmetabolites of pesticides in cancer patientshave been described as analogous to "lookingunder the nearest lamppost for lost keysbecause that is where there is light" (60).Two critical questions must be raised: Whatwere exposures to xenohormones during crit-ical windows of development, including theprenatal and prepubescent periods, and whatwas the lifetime exposure to hormonallyactive parent compounds? Studies that lookat contemporaneous measures of lipophilicmetabolites of organochlorine compoundscannot resolve these questions. Moreover,measures of total PCBs cannot distinguishbetween active materials that are highlyestrogenic and those which are antiestro-genic, and analytic studies of exposure needto be standardized for lipid adjustment (62.
Need for Longer Term StudiesLimited epidemiological studies have beenconducted on the role of harmfuil or protective
xenohormonal factors throughout the lifecycle. No long-term comprehensive studieshave yet been conducted or planned onlarge populations involving prenatal risk fac-tors for breast cancer. In addition, biomark-ers or metabolites of many quickly metabo-lized suspected agents such as some compo-nents of plastics, fuels, and aromatic materi-als cannot be directly measured in womenlong after exposure has ceased. Studies thatlook at current levels of lipophilic residues incases of breast cancer compared to controlscannot resolve the issue of whether pastexposures play a role in the development ofthe disease. The process of cancer altersmetabolism in ways that are not well under-stood. Given the complex and competingroles of xenohormones, only long-termprospective studies that cover two genera-tions will be able to resolve the issue of therelative roles of prenatal, prepubescent, andsubsequent exposures to harmful and benefi-cial xenohormones. Especially as potentforms of materials are excreted, it will bevery important to obtain residues over thenatural lifetime. Thus, the relative role ofharmful or protective xenohormones andother factors such as Cox-2 inhibitors inaffecting breast cancer vulnerability and indirectly causing the disease is a matter thatcan only be resolved by studies that collecttissue for analyses through two generations.
Significant and unexplained elevatedrates of breast cancer have been found acrossthe United States, in places as diverse asCape Cod, Massachusetts, and centralIllinois. A recent report from San Francisco,California, like an earlier one from LongIsland, New York, found that differences inthe prevalence of so-called risk factors couldtheoretically account for all of the differencesin the rate of breast cancer in that area (63).This study employed no individual mea-sures, but modeled risk factors obtained inprevious surveys of populations at risk ofovarian cancer compared to the populationof San Francisco. In contrast, a nationalstudy of breast cancer mortality found thatknown risk factors accounted for only abouthalf of the overall regional excess (64).Historically breast cancer incidence is aboutfour- to sevenfold higher in the United Statesthan in Asia. The risk of breast cancerincreases when women migrate from thosecountries to the West. Those Asian-American women whose grandparents wereborn in America have 60% greater risk ofbreast cancer than those whose grandparentswere born in Asia. Immigrants living in theWest for a decade or longer have a risk ofbreast cancer 80% higher than more recentimmigrants (50). The notion that there issomething protective about being Asian isalso borne out by a study that found no
increased risk from elevated organochlorinesin Asian-American women, but a two- tothreefold risk in white and African-American women (57.
Basic Research IssuesWe need to ask a number of basic researchquestions based on this proposed rethinkingof risk factors. Why do girls who are tallerand heavier at earlier ages have a greater rateof breast cancer? Could growth hormones inchickens, eggs, and dairy and meat productsbe involved in addition to greater amounts ofcalories overall? Why do women who lactatehave a reduced risk of premenopausal breastcancer? Could lactation rid the body ofpotentially harmful, cancer-causing lipophilicagents in the mostly fatty breast tissue? Forpostmenopausal women, could cumulativebuildup of harmful xenoestrogens effectivelyvoid the added protection lactation providesfor premenopausal women? Why do womenwho regularly consume alcohol have an excessrisk of breast cancer? Why does alcohol con-tribute so dramatically to circulations of hor-mones in the blood? Why do women whoexercise regularly have less breast cancer?Could their bodies contain lower levels ofhormones, proportionally less fat, and lesscontaminants in fat that damage the breasts?Does a diet high in beneficial xenohormones,such as genistein and omega-3-fatty acids,protect against breast cancer in Asian women?Would supplements or diets high in thesefoods prevent breast cancer? Does exposure toelectromagnetic fields lower melatonin,which is a natural suppressor of breast cancercell growth (65)? Do combustion by-prod-ucts from fossil fuels (66) or from uncon-trolled incineration of medical waste play anyrole in the increased rates of breast cancer inthe urban environment (67)?
Public Policy QuestionsIt has been sardonically noted that one outof every four breast cancer cases amongwhite women could be prevented if allwhite women had children before age 20,underwent menarche after age 14, had par-ents with no genetic or cultural predisposi-tions to the disease, and had no benignbreast conditions detected by a biopsy (12).In fact, most well-established risk factors forbreast cancer cannot be changed in the pre-sent generation. Many of the risk factorsinvolve exposures and circumstances thatarise early in life; others entail matters overwhich women have little or no control asadults, such as the onset of menopause.Current proposed interventions to reducebreast cancer mainly focus on changingindividual behaviors, including such self-imposed restrictions as lifelong administra-tion of pharmaceutical agents or radical
Environmental Health Perspectives * Volume 106, Number 9, September 1998 527

Commentaries * Davis et al.
changes in diet, exercise regime, or repro-ductive behavior. However, some of thecauses of breast cancer and related diseasescan only be controlled by social and politi-cal action aimed at reducing the produc-tion, use, transport, and disposal of agentsthat directly or indirectly affect breast can-cer risks.
The identification of contributing andvulnerability risk factors will provide a keymissing component for fostering the promo-tion of policies that require public policyinterventions. The public and private sectorscould, for example, devise policies to pre-vent, restrict, or reduce exposures to agentsin the household, workplace, and generalenvironment that extend the duration andonset of breast growth or alter the hormonalenvironment. For these policies to succeed,experimental screening tests to identifyxenohormones and other disruptive agentsmerit high priority. Once such test systemsare in place, procurement policies as well aspolicies regarding workplace safety, educa-tion, and training and international tradecan be modified to encourage the use ofmaterials found to be less likely to alter hor-monal metabolism and extend cell growth.
Where there are significant risks of damage tothe public health, we should be prepared to takeaction to diminish those risks even when the sci-entific knowledge is not conclusive, if the bal-ance of likely costs and benefits justifies it [fromHorton (68].
The remaining central question for publicpolicy is what risk factors give rise to 19 outof 20 cases of breast cancer. For more than30 years, studies have repeatedly confirmedunmodifiable risk factors. These account forless than half of all cases. Probing for whatavoidable causes lurk behind breast cancer inSan Francisco, Cape Cod, or anywhere elsewill be vital to solving the growing puzzlesurrounding the disease and reducing itsburden further.
For further information, see the WorldResources Institute Website (6S1l.
REFERENCES AND NOTES
1. WHO. The World Health Report 1997: ConqueringSuffering-Enriching Humanity. Geneva:WorldHealth Organization, 1997.
2. Parkin DM, Whelan SL, Ferlay J, Raymond L, Young J,eds. Cancer Incidence in Five Continents. Vol. VIl.IARC Scientific Publications No 143. Lyon:lnternationalAgency for Research on Cancer, 1997.
3. Coleman MP, Esteve J, Damiecki P, Arslan A, RenardH, eds. Trends in Cancer Incidence and Mortality.IARC Scientific Publications No 121. Lyon:lnternationalAgency for Research on Cancer, 1993.
4. Ries LAG, Hankey BF, Edwards BK, eds. CancerStatistics Review 1973-94. Bethesda, MD:NationalCancer Institute, 1997.
5. Kelsey JI, Bernstein L. Epidemiology and prevention ofbreast cancer. Annu Rev Public Health 17:47-67 11996).
6. McPherson K, Steel CM, Dixon JM. Breast cancer-
epidemiology, risk factors, and genetics. Br Med J309:1003-1006(1994).
7. Madigan MP, Ziegler RG, Benichou J, Byrne C,Hoover RN. Proportion of breast cancer cases in theUnited States explained by well-established risk fac-tors. J NatI Cancer Inst 87(22):1681-1685 (1995).
8. Kelsey JL, Gammon MD. Epidemiology of breast can-cer. Epidemiol Rev 12:228-240 (1990).
9. Cole P, MacMahon B. Oestrogen fractions duringearly reproductive life in the aetiology of breast can-cer. Lancet 1:604-606 (1969).
10. Toniolo PG. Endogenous estrogens and breast can-cer risk: the case for prospective cohort studies.Environ Health Perspect 105(3):587-592 (1997).
11. Dao TL. The role of ovarian steroid hormones in mam-mary carcinogenesis. In: Hormones and BreastCancer. Banbury Report No 8 (Pike MC, Siiteri PK,Welsch CW, eds). Cold Spring Harbor, NY:Cold SpringHarbor Laboratory Press, 1981;281-295.
12. Rockhill B, Weinberg CR, Newman B. Populationattributable fraction estimation for established breastcancer risk factors: considering the issues of highprevalence and unmodifiability. Am J Epidemiol147(9):826-833 (1998).
13. Pike MC, Krailo MD, Henderson BE, Cassagrande JT,Hoel DG. 'Hormonal risk factors, "breast tissue age'and the 'age-incidence of breast cancer." Nature303:767-770 (1983).
14. Rothman KJ, ed. Causal Inference. Chestnut Hill,MA:Epidemiology Resources Inc., 1988.
15. Hill B. Principles of Medical Statistics. NewYork:Oxford University Press, 1966.
16. Davis DL, Friedler G, Mattison D, Morris R. Male-medi-ated teratogenesis and other reproductive effects:biologic and epidemiologic findings and a plea forclinical research. Reprod Toxicol 6:289-292 (1992).
17. Committee on the Biological Effects of IonizingRadiation, Board on Radiation Effects Research.Health Effects of Exposure to Low Levels of IonizingRadiation: BEIR V. Washington, DC:National AcademyPress, 1989.
18. Ekbom A, Hsieh CC, Lipworth L, Adami HQ,Trichopoulos D. Intrauterine environment and breastcancer risk in women: a population-based study. JNatI Cancer Inst 89:71-76 (1997).
19. Newcomb PA, Storer BE, Longnecker MP, MittendorfR, Greenberg RE, Clapp RW, Burke KP, Willett WC,MacMahon B. Lactation and a reduced risk of pre-menopausal breast cancer. N EngI J Med 330(2):81-87(1994).
20. Kelsey JL, Bernstein L Epidemiology and prevention ofbreast cancer. Annu Rev Public Health 17:47-67 (1996).
21. Sonnenschein C, Soto AM, Fernandez MF, Olea N,Olea-Serrano MF, Ruiz-Lopez MD. Development of amarker of estrogenic exposure in human serum. ClinChem 41:1888-1895 (1995).
22. Liehr JG, Ricci MJ. 4-Hydroxylation of estrogens asmarker of human mammary tumors. Proc NatI AcadSci USA 93:3294-3296 (1996).
23. Telang NT, Katdare M, Bradlow HL, Osborne MP.Estradiol metabolism: an endocrine biomarker formodulation of human mammary carcinogenesis.Environ Health Perspect 105(suppl 3):559-564 (1997).
24. Mendel CM. The free hormone hypothesis: a physio-logically based mathematical model. Endocr Rev10(3):232-274 (1989).
25. Colditz GA, Stampfer MJ, Willett WC, Hennekens CH,Rosner B, Speizer FE. Prospective study of estrogenreplacement therapy and risk of breast cancer inpostmenopausal women. JAMA 264:2648-2653 (1990).
26. Gapstur SM, Potter JD, Sellers TA, Folsom AR.Increased risk of breast cancer with alcohol con-sumption in postemenopausal women. Am JEpidemiol 136:1221-1231 (1992).
27. Ginsburg EL, Mello NK, Mendelson JH, Barbieri RL,Teoh SK, Rothman M, Gao X, Sholar JW. Effects ofalcohol ingestion on estrogens in postmenopausalwomen. JAMA 276:1747-1751 (1996).
28. Reichman ME, Judd JT, Longcope C, Schatzkin A,Clevidence BA, Nair PP, Campbell WS, Taylor P.Effects of alcohol consumption on plasma and uri-nary hormone concentrations in premenopausalwomen. J Natl Cancer Inst 85:722-727 (1993).
29. Hartmann A, Blasyk H, Sartok S, Toushima K, TamuraY, Cunningham JM, McGovern RM, Schroeder JJ,Sonimer SS, Kovach SS. High frequency of p53 genemutations in primary breast cancers in Japanesewomen, a low-incidence population. Br J Cancer73:896-901 (1996).
30. Zumoff B. Does postmenopausal estrogen administra-tion increase the risk of breast cancer? Contributionsof animal, biochemical, and clinical investgative stud-ies to a resolution of the controversy. NewYork:Society for Experimental Biology and Medicine,1998;30-37.
31. Toniolo PG. Endogenous estrogens and breast can-cer risk: the case for prospective cohort studies.Environ Health Perspect 10(suppl 3):587-592 (1997).
32. Dorgan JF, Longcope C, Stephenson HE Jr, Falk RT,Miller R, Franz C, Kahle L, Campbell WS, Tangrea JA,Schatzkin A. Serum sex hormone levels are related tobreast cancer risk in postmenopausal women.Environ Health Perspect 105(suppl 3):583-585 (1997).
33. Davis DL Pongsiri MJ, Wolff M. Recent developmentson the avoidable causes of breast cancer. In:Preventive Strategies for Living in a Chemical World-A Symposium in Honor of Irving J. Selikoff (Bingham E,Rail DP, eds). Ann NY Acad Sci 837:513-523 (1997).
34. Davis DL, Axelrod D, Osborne MP, Telang NT.Environmental influences on breast cancer risk. SciMed 4:56-63(1997).
35. Bradlow HL, Hershcopf RJ, Martucci CP, Fishman J.Estradiol 16-hydroxylation in the mouse correlateswith mammary tumor incidence and presence ofmurine mammary tumor virus: a possible model forhormonal etiology of breast cancer in humans. ProcNatI Acad Sci USA 82:6295-6299 (1985).
36. Bradlow HL, Davis DL, Lin G, Sepkovic D, Tiwari R.Effects of pesticides on the ratio of 16o/2-hydroxy-estrone: a biologic marker of breast cancer risk.Environ Health Perspect 103(suppl 7):147-150 (1995).
37. Davis DL, Telang NT, Osborne MP, Bradlow HL.Medical hypothesis: bifunctional genetic-hormonalpathways to breast cancer. Environ Health Perspect105(suppl 3):571-576 (1997).
38. Malins DC, Holmes EH, Polissar NL, Gunselman SJ.The etiology of breast cancer: characteristic alter-ations in hydroxyl radical-induced DNA base lesionsduring oncogenesis with potential for evaluating inci-dence risk. Cancer 71:3036-3043(1993).
39. Arnold SF, Vonier PM, Collins BM, Klotz DM, GuilletteW Jr, Mclachlan JA. In vitro synergistic interactionof alligator and human estrogen receptors with com-binations of environmental chemicals. Environ HealthPerspect 105(suppl 3):615-618 (1997).
40. Tsutsui T, Barrett JC. Neoplastic transformation ofcultured mammalian cells by estrogens and estro-genlike chemicals. Environ Health Perspect 105(suppl 3):619-624 (1997).
41. Safe SH. Is there an association between exposureto environmental estrogens and breast cancer?Environ Health Perspect 105(suppl 3):675-678 (1997).
42. Zava DT, Blen M, Duwe G. Estrogenic activity of nat-ural and synthetic estrogens in human breast cancercells in culture. Environ Health Perspect 105(suppl3):637-645 (1997).
43. Blanco A, Habib A, levy-Toledano S, Maclouf J.Involvement of tyrosine kinase in the induction ofcyclooxygenase-2 in human endothelial cells. JBiochem 312:419-423 (1995).
44. Bennett A. The production of prostanoids in humancancers, and their implications for tumor progres-sion. Prog Lipid Res 25:539-542 (1986).
45. Bennett A, Charlier EM, McDonald AM, Simpson JS,Stamford IF, Zebro T. Prostaglandins and breast can-cer. Lancet 2(8039):624-626 (1977).
46. Levine L. Chemical carcinogens stimulate canine kid-ney (MDCK) cells to produce prostaglandins. Nature268:447-448(1977).
47. Harris RE, Namboodiri KK, Farrar WB. Nonsteroidalantiinflammatory drugs and breast cancer.Epidemiology 7:203-205(1996).
48. Schreinemachers DM, Everson RB. Aspirin use andlung, colon, and breast cancer. Epidemiology5:138-146({1994).
49. Kelley DJ, Sacks PG, Ramonetti JT, Schanta SP,
528 Volume 106, Number 9, September 1998 * Environmental Health Perspectives

Commentaries * Rethinking breast cancer risk and the environment
Dannenberg AJ. Curcumin inhibits prostaglandin syn-thesis and cyclooxygenase-2 expression in oral epithe-lial cells. Proc Am Assn Cancer Res 37:909 (1996).
50. Ziegler RG, Hoover RN, Pike MC, Hildesheim A,Nomura AM, West DW, Wu-Williams AH, Kolonel LN,Horn-Ross PL, Rosenthal JF, et al. Migration patternsand breast cancer risk in Asian-American women. JNatI Cancer Inst 85:1819-1827 (1993).
51. Falck F Jr, Ricci A Jr, Wolff MS, Goldbold J, DeckersP. Pesticides and polychlorinated biphenyl residuesin human breast lipids and their relation to breastcancer. Arch Environ Health 47:143-146 (1992).
52. Wu C, Gottlieb M, Davis DL. World Resources Report1998-99: Regional Profile: China's Health andEnvironment. Washington, DC:World ResourcesInstitute, 1998.
53. Wolff MS, Toniolo PG, Lee EW, Rivera M, Dubin N.Blood levels of organochlorine residues and risk ofbreast cancer. J NatI Cancer Inst 85:648-652 (1993).
54. Dewailly MS, Dodin S, Verrault R, Ayotte P, Sauve L,Brisson J. High organochlorine body burden inwomen with estrogen receptor-positive breast can-cer. J NatI Cancer Inst 86(3):232-234 (1994).
55. Glass R, Hoover RN. Rising incidence of breast can-cer relationship to stage and receptor status. J NatICancer Inst 82(8):693-696 (1990).
56. Lopez-Carillo L, Blair A, Lopez-Cervantes M, Cebrian
M, Rueda C, Reyes R, Mohar A, Bravo J.Dichlorodiphenyl trichloroethane serum levels andbreast cancer risk: a case-control study fromMexico. Cancer Res 57:3728-3732 (1997).
57. Krieger N, Wolff MS, Hiatt RA, Rivera M, Vogelman J,Orentreich N. Breast cancer and serum organochlo-rines: a prospective study among white, black, andAsian women. J Nati Cancer Inst 86:589-599 (1994).
58. Hunter DJ, Hankinson SE, Laden F, Colditz GA,Manson JAE, Willet WC, Speizer FE, Wolff MS.Plasma organochlorine levels and the risk of breastcancer. N EngI J Med 337:1253-1258 (1997).
59. van't Veer P, Lobbezoo IE, Martin-Moreno JM, GuallarE, Gomez-Aracena J, Kardinaal AFM, Kohimeier L,Martin BC, Strain JJ, Thamm M, et al. DDT (dico-phane) and postmenopausal breast cancer in Europe:case-control study. Br Med J 315:81-85 (1997).
60. vom Saal FS, Hansen LG. Organochlorine residues andbreast cancer [letter]. N EngI J Med 388(14):988 (1998).
61. Hankinson SE, Willett WC, Colditz GA, Hunter DJ,Michaud DS, Deroo B, Rosner B, Speizer FE, PollakM. Circulating concentrations of insulin-like growthfactor and risk of breast cancer. Lancet351:1393-1396 (1998).
62. Gammon MD, Terry MB, Teitelbaum SL, Britton JA,Levin B. Organochlorine residues and breast cancer[letter]. N EngI J Med 388(14):989 (1998).
63. Robbins AS, Brescianini S, Kelsey JL. Regional differ-ences in known risk factors and the higher incidenceof breast cancer in San Francisco. J Natl Cancer Inst89(13:960-965 (1997).
64. Sturgeon SR, Schairer C, Gail M, McAdams M,Brinton LA, Hoover RN. Geographic variation in mor-tality from breast cancer among white women in theUnited States. J NatI Cancer Inst 87:1846-1853 (1995).
65. Harland JD, Liburdy RP. Environmental magneticfields inhibit the antiproliferative action of tamoxifenand melatonin in a human breast cancer cell line.Bioelectomagnetics 18:555-562 (1997).
66. Wolff MS, Collman GW, Barrett JC, Huff J. Breastcancer and environmental risk factors: epidemiologi-cal and experimental findings. Annu Rev PharmacolToxicol 36:573-596 (1996).
67. Hettenbach T. "Greening Hospitals": An Analysis ofPollution Prevention in America's Top Hospitals,Washington, DC:The Environmental Working Group,1998.
68. Horton R. The new new public health of risk and radi-cal engagement [editorial]. Lancet352(9124):251 (1998).
69. World Resources Institute Home Page. Washington,DC:World Resources Institute, 1996. [Available:http:llwww.wri.org].
Attention Resea~rchersl--Publish fster and puls frt vwith Online Pbishig
The pace' of scientific research is increasing all the timne.EIHP: meets. the deadfrfse ulcton-
all re'search articles accepted for.publicati.on in EHP are publishedolnfist through..the En:.vironm.en'tal.Healt.h..Infor.maotion Service at.
Wi'th Online Publishing -yo'u can:publsh you reseachmonhs earier thnthe pint vesion ad.aedo or optto* preciselyestablish publication pr~~~~~~~~~~~~~~~~~~~iorttoa pcfi a
* stay infonned on the veryrlatest developments in environmental health science~~~~~~~~~~~~~~~~~~~~~~~~~~~~~7 7
Visitustodayl http://ohis.ni.bs.nih.gov.
Environmental Health Perspectives * Volume 106, Number 9, September l998 529