
Secondary psychotic features in refugees diagnosed with post ...
Upload
independentCategory
view
0download
0
Resource utilization in a Canadian nationalstudy of people with schizophrenia andrelated psychotic disorders
Introduction
Apart from being extremely disabling for manyaffected individuals, their families and friends,schizophrenia and related psychotic disorders haveno cure and are very costly to treat. The total annualcost (direct health care and non-health care) oftreating schizophrenia in Canada is estimated at$1.12 billion (1996 $Can.) (US $730 million), withpsychiatric hospitalization accounting for a sub-stantial portion (21%) of this cost (1). Adjusting thecost, using the Consumer Price Index, the 2003 costwould be Can. $1.29 billion (US $840 million) (2).Furthermore, as the number of available in-patientbeds decreases, the costs of maintaining patients inthe community will increase. It is thus imperative todetermine which medications can reduce the risk ofhospitalization and out-patient resource use, andthus reduce the pharmacoeconomic burden oftreating these conditions.Among the first antipsychotic agents used to
treat schizophrenia were the so-called conventional
drugs, such as haloperidol and chlorpromazine.With the availability of more expensive atypical orsecond-generation antipsychotics, such as cloza-pine (CLZ), risperidone (RIS), olanzapine (OLZ)and quetiapine (QUE), studies have been conduc-ted to determine the economic costs and potentialclinical benefits of these atypical drugs comparedto the conventional agents (3–5). Atypical antipsy-chotic medications have been shown to decreasethe incidence and severity of adverse neurologicaleffects, decrease negative symptoms and diminishsymptoms in patients classified as treatmentrefractory (4, 6). Furthermore, due to theseimprovements in clinical parameters, the atypicaldrugs have been reported to result in lower overallcosts despite higher acquisition costs when com-pared to conventional drugs (7–9). The atypicaldrugs are now commonly used to treat patientswith schizophrenia and related disorders, high-lighting the urgent need to evaluate economic andrisk comparisons among these agents. Pharmaco-economic profiles to date tend to focus on com-
Kopala L, Smith G,Malla A,Williams R, Love L, Talling D, Balshaw R.Resource utilization in a Canadian national study of people withschizophrenia and related psychotic disorders.Acta Psychiatr Scand 2006: 113 (Suppl. 430): 29–39. ª 2006 BlackwellMunksgaard.
Objective: To determine how the use of the newer, so called atypicalantipsychotic medications, effects the pharmacoeconomic treatmentburden of schizophrenia and related conditions and to provide a clearcomparison of the costs and risks associated with these atypical drugs.Method: In this 2-year, open-label, prospective study, resourceutilization (RU) data were collected on 160 patients with theseconditions. A comparison between risks and costs was performed bycombining the generalized CNOMSS data on both economic factorsand risk assessments.Results: The main findings of the study were that the total adjusted1- and 2-year costs were lowest for quetiapine. Drug acquisition costswere lowest for risperidone for both the 1- and 2-year cohorts.Clozapine use was predictably associated with the highest overall andmedication costs at both 1 and 2 years.Conclusion: Treatment with risperidone or quetiapine was associatedwith the lowest overall costs when compared with olanzapine orclozapine.
L. Kopala1, G. Smith1, A. Malla2,R. Williams1, L. Love3, D. Talling3,R. Balshaw3
1Department of Psychiatry, University of BritishColumbia, Vancouver, BC, 2Department of Psychiatry,McGill University, Montreal, QC and 3SyreonCorporation, Vancouver, BC, Canada
Key words: schizophrenia; prognosis; cost analysis
Lili Kopala, Center for Complex Disorders, Departmentof Psychiatry, University of British Columbia, Vancouver,BC, Canada.E-mail: [email protected]
Acta Psychiatr Scand 2006: 113 (Suppl. 430): 29–39All rights reserved
Copyright ª Blackwell Munksgaard 2006
ACTA PSYCHIATRICASCANDINAVICA
29
parisons between RIS and OLZ, e.g. Edgell et al.(10) reported that RIS was more costly than OLZ,while other groups determined that RIS and OLZacquisition costs were similar (11, 12). Theseresults, as well as lack of studies which includeQUE or CLZ or risk assessments, underscore theneed for a more comprehensive pharmacoeconomicevaluation of the atypical drugs.The current study utilized data acquired as part
of the Canadian National Outcomes MeasurementStudy in Schizophrenia (CNOMSS). The latter wasa prospective, longitudinal, population-basedstudy involving 32 community and academic sitesacross Canada. CNOMSS enrolled 448 patientswith diagnoses of schizophrenia, schizophreniformdisorder, schizoaffective disorder or psychosis nototherwise specified. Of these, 276 were enrolledwhile on atypical monotherapy within 7 days ofrecruitment. Patients were eligible for inclusion inthe 1- or 2-year analysis cohorts if they werefollowed for at least 12 and 24 months and hadprovided at least 50% of the monthly resource useforms for the respective periods.Canadian National Outcomes Measurement
Study in Schizophrenia is the first study to providea direct pharmacoeconomic comparison of CLZ,RIS, OLZ and QUE via a detailed analysis ofin-patient andout-patient costs aswell as direct drugacquisition costs. Furthermore, CNOMSS alsoevaluated the rates of hospitalization and out-patient service use by patients treated with any oneof these drugs.
Aims of the study
The purpose of this study was to combine thegeneralized CNOMSS data on both economicfactors and risk assessments to provide a clearcomparison of the costs and risks associated withthese atypical drugs.
Material and methods
A description of the study appears in the firstarticle in this series (13). Of the 448 enrolled, 347patients were followed for 24 months. Of these,
160 were eligible for inclusion in the analysis, i.e.were using atypical antipsychotic monotherapywithin 7 days of recruitment, provided at least50% of the Resource Use Forms during theirfollow-up time, and provided data for all enroll-ment clinical and demographic predictor valuesused in the regression models (see Table 1).Analysis was based on an intent-to-treat meth-odology.A scientific advisory committee (see Acknowl-
edgements) selected sites based on known infor-mation about the respective sites’ case mix andresearch experience. The study was approved bythe Western Institutional Review Board (WIRB,Olympia, WA) and where applicable, by localInternal Review Boards.Demographic and clinical data were collected for
patients treated with antipsychotic medicationsunder conditions of routine clinical practice.Patients or their caregivers completed a monthly,resource use questionnaire which detailed thequantity of healthcare resources accessed by thepatient during the previous month. The outcomevariables included both monthly utilization ratesfor key cost drivers and estimated costs of careincluding in-patient, out-patient, medication andother costs. Utilization rates were calculated forhospitalization (days), emergency room (ER)(visits), community support worker (days), psychi-atric day care (days) and specialist visits.Medication costs included the costs of the novel
antipsychotics. In-patient costs included general in-patient care (In-patient), intensive care unit stay(ICU) and ER visits. Out-patient costs includedfamily doctor, specialist, counselor/psychologist,social worker, psychiatric nurse, occupational orrecreational therapist (OT/RT), community sup-port worker, suicide/crisis services, alcohol/drugrehab, group/family therapy, home care nursevisits, lab/diagnostic tests and psychiatric daycare. �Other� costs included education/skills pro-grams, emergency shelter visits, lawyer, police/legalinvolvement and probation officer. Indirect costsindicated days on which the patient could notcontinue their usual functions. Total monthly costsincluded the aggregated sum of these separate costs
Table 1. Patient disposition
Clozapine Olanzapine Quetiapine Risperidone Monotherapy total Other Overall
Number of subjects enrolled 61 92 21 102 276 172 448Number of subjects year 1 cohort 59 87 20 97 263 160 423Number of subjects in year 1 cohort with 50% RU submitted 54 79 18 80 231 101 332Number of subjects in year 2 cohort 51 70 16 80 217 130 347Number of subjects in year 2 cohort with 50% RU submitted 41 58 14 47 160 49 209
RU, resource utilization.
Kopala et al.
30

areas. The cost per base unit came from aCanadian Cost Dictionary compiled for thisstudy. This cost dictionary accesses high-levelcost information from one Canadian province(British Columbia), and included the definition,data source(s) for information, the measurementand calculations used, the unit value derived fromthe calculations and any additional assumptionsused (see Appendix 1). All dollar values are repor-ted in 2002 $Can. and converted to $US using anaverage exchange rate (0.6515) for the period of thestudy: January 1, 2000 until December 31, 2002(14).All reported hospitalizations were confirmed
with the site investigator by Syreon Corporation.
Statistical methods
Frequency and estimated monthly costs of hospi-talization and emergency room visits were derivedfrom resource use questionnaires. For eachresource type, the number of units consumedeach month was multiplied by the cost per unitfrom the Canadian Cost Dictionary compiled forthis study. The resource costs were summed overthe month reported and aggregated over all reportssubmitted for the 12-month patient-year. Thepatient-year aggregate was divided by the numberof months reported to produce the patient’sestimated average monthly resource use cost. Atleast six of the 12 resource use reports in thatpatient-year had to be submitted for the patient’saverage monthly cost to be included in the overallestimated average monthly resource cost.Demographic and clinical variables at enroll-
ment were compared using ANOVA for continu-ous measures and chi-squared tests for categoricalmeasures. The unadjusted costs were obtained asthe average of the monthly costs per subject,without controlling for confounding factors, andwere compared both descriptively and using theGeneral Linear Model (GLM).A GLM model was used to produce adjusted
costs. The model controlled for both demographicand clinical variables and allowed for a comparisonof costs between the treatment groups as if thegroupswere identical with respect to the distributionof the baseline covariates. The demographic varia-bles included in the model were: age at registration,gender, income and marital status. The baselineclinical variables were: Brief Psychiatric RatingScale (BPRS), Social andOccupational FunctioningAssessment Scale (SOFAS), ClinicalGlobal Impres-sion of Illness-Improvement (CGI-I), ClinicalGlobal Impression of Severity of Illness (CGI-S)and positive symptoms, negative symptoms, cogni-
tive symptoms, diagnosis, hospitalizations in previ-ous 2 years, past substance abuse, duration of illnessprior to entry, and duration of continuous mono-therapy prior to enrollment.A Poisson regression model was used to com-
pare resource utilization for a small subset ofresource types: numbers of days hospitalized(including stays in ICU, visits to ER, communitysupport worker visits, psychiatric day care visitsand visitations to specialists, including psychia-trists). The Poisson model controlled for the sameset of baseline variables as in the linear regressionmodel. Poisson regression is a natural step beyondtraditional linear regression models for outcomemeasures that are essentially counts, addressingboth the skewness and heterogeneity of variancecommon in such data.
Results
Of a study cohort of 276 subjects on atypicalantipsychotics, 61 were treated with CLZ, 102 weretreated with RIS, 92 with OLZ and 21 with QUE.Table 2 summarizes the cohort baseline demo-graphics.
Unadjusted costs
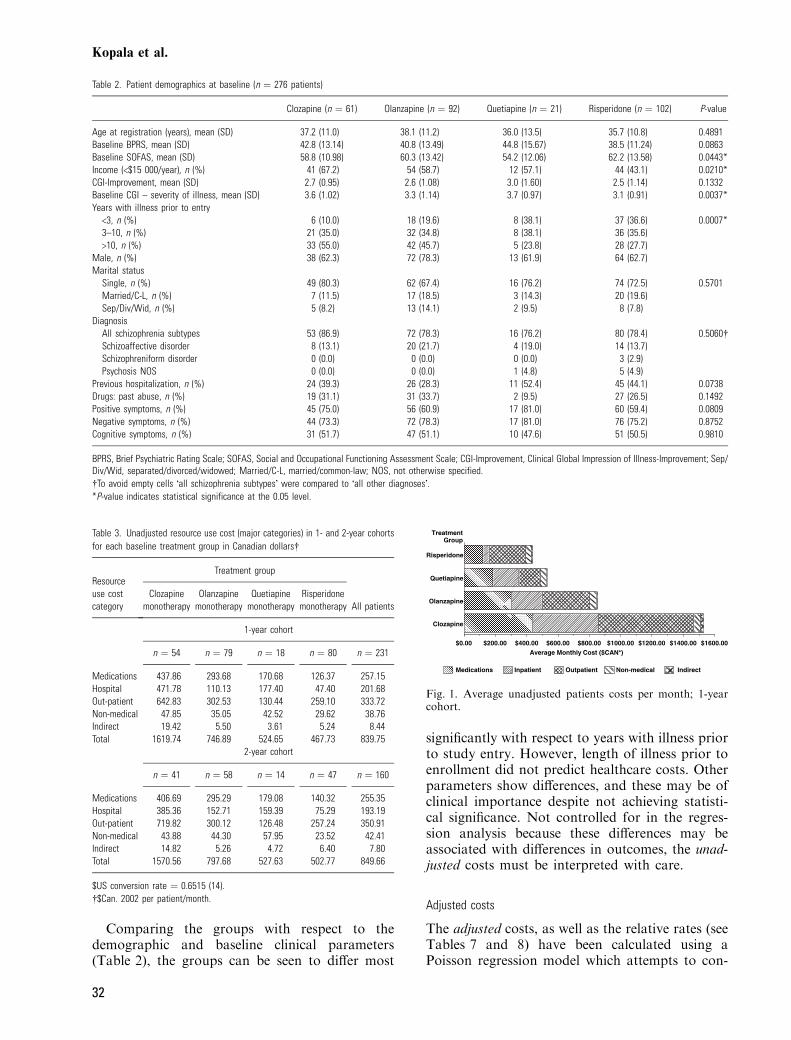
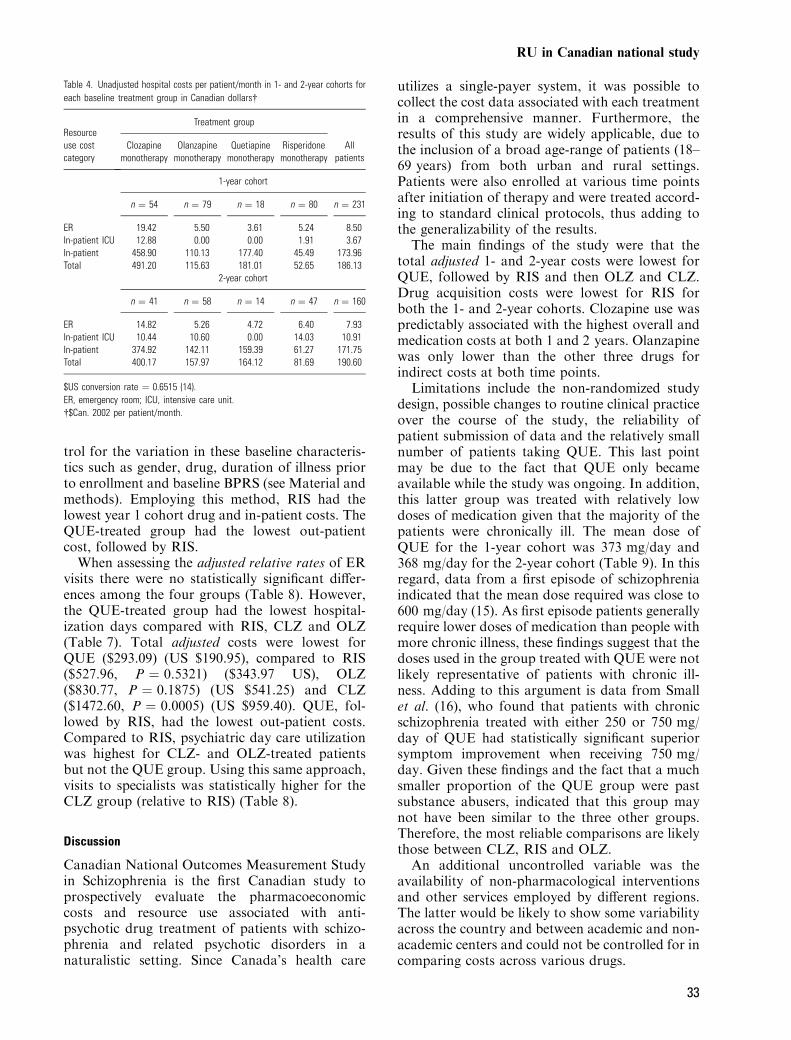
The monthly, unadjusted total cost analysis showedthat treatment with RIS resulted in the lowestoverall first year cost (Table 3) ($467.73) (US$304.73), followed by QUE ($524.65) (US$341.81), OLZ ($746.89) (US $486.60) and CLZ($1619.74) (US $1055.26) (Fig. 1). A breakdown ofthe unadjusted costs revealed that RIS had thelowest drug acquisition cost and in-patient cost ofall four atypicals. The QUE-treated group had thelowest out-patient cost, followed by RIS (Fig. 1and Table 3). The same pattern was evident forunadjusted 2-year costs (Fig. 2).A more detailed examination of unadjusted
in-patient costs can be found in Table 4. Thistable indicates that the low hospitalization costsassociated with RIS can be attributed to its low ER,in-patient intensive care unit (in-patient ICU) andin-patient costs. Table 5 addresses the breakdownof unadjusted out-patient service costs, and indica-ted that RIS had the lowest cost of family doctorand occupational therapy. OLZ had the lowestcosts for laboratory/diagnostic testing and special-ist visits while QUE was lowest for communitysupport worker, counselor, home care nurse andpsychiatric day care worker costs. In terms of totalunadjusted out-patient costs, QUE ($) was lowestfollowed by RIS. RIS had the lowest unadjustednon-medical costs at both 1 and 2 years (Table 6).
RU in Canadian national study
31
Comparing the groups with respect to thedemographic and baseline clinical parameters(Table 2), the groups can be seen to differ most
significantly with respect to years with illness priorto study entry. However, length of illness prior toenrollment did not predict healthcare costs. Otherparameters show differences, and these may be ofclinical importance despite not achieving statisti-cal significance. Not controlled for in the regres-sion analysis because these differences may beassociated with differences in outcomes, the unad-justed costs must be interpreted with care.
Adjusted costs
The adjusted costs, as well as the relative rates (seeTables 7 and 8) have been calculated using aPoisson regression model which attempts to con-
Table 3. Unadjusted resource use cost (major categories) in 1- and 2-year cohortsfor each baseline treatment group in Canadian dollars�
Resourceuse costcategory
Treatment group
All patientsClozapine
monotherapyOlanzapinemonotherapy
Quetiapinemonotherapy
Risperidonemonotherapy
1-year cohort
n ¼ 54 n ¼ 79 n ¼ 18 n ¼ 80 n ¼ 231
Medications 437.86 293.68 170.68 126.37 257.15Hospital 471.78 110.13 177.40 47.40 201.68Out-patient 642.83 302.53 130.44 259.10 333.72Non-medical 47.85 35.05 42.52 29.62 38.76Indirect 19.42 5.50 3.61 5.24 8.44Total 1619.74 746.89 524.65 467.73 839.75
2-year cohort
n ¼ 41 n ¼ 58 n ¼ 14 n ¼ 47 n ¼ 160
Medications 406.69 295.29 179.08 140.32 255.35Hospital 385.36 152.71 159.39 75.29 193.19Out-patient 719.82 300.12 126.48 257.24 350.91Non-medical 43.88 44.30 57.95 23.52 42.41Indirect 14.82 5.26 4.72 6.40 7.80Total 1570.56 797.68 527.63 502.77 849.66
$US conversion rate ¼ 0.6515 (14).�$Can. 2002 per patient/month.
Table 2. Patient demographics at baseline (n ¼ 276 patients)
Clozapine (n ¼ 61) Olanzapine (n ¼ 92) Quetiapine (n ¼ 21) Risperidone (n ¼ 102) P-value
Age at registration (years), mean (SD) 37.2 (11.0) 38.1 (11.2) 36.0 (13.5) 35.7 (10.8) 0.4891Baseline BPRS, mean (SD) 42.8 (13.14) 40.8 (13.49) 44.8 (15.67) 38.5 (11.24) 0.0863Baseline SOFAS, mean (SD) 58.8 (10.98) 60.3 (13.42) 54.2 (12.06) 62.2 (13.58) 0.0443*Income (<$15 000/year), n (%) 41 (67.2) 54 (58.7) 12 (57.1) 44 (43.1) 0.0210*CGI-Improvement, mean (SD) 2.7 (0.95) 2.6 (1.08) 3.0 (1.60) 2.5 (1.14) 0.1332Baseline CGI – severity of illness, mean (SD) 3.6 (1.02) 3.3 (1.14) 3.7 (0.97) 3.1 (0.91) 0.0037*Years with illness prior to entry<3, n (%) 6 (10.0) 18 (19.6) 8 (38.1) 37 (36.6) 0.0007*3–10, n (%) 21 (35.0) 32 (34.8) 8 (38.1) 36 (35.6)>10, n (%) 33 (55.0) 42 (45.7) 5 (23.8) 28 (27.7)
Male, n (%) 38 (62.3) 72 (78.3) 13 (61.9) 64 (62.7)Marital statusSingle, n (%) 49 (80.3) 62 (67.4) 16 (76.2) 74 (72.5) 0.5701Married/C-L, n (%) 7 (11.5) 17 (18.5) 3 (14.3) 20 (19.6)Sep/Div/Wid, n (%) 5 (8.2) 13 (14.1) 2 (9.5) 8 (7.8)
DiagnosisAll schizophrenia subtypes 53 (86.9) 72 (78.3) 16 (76.2) 80 (78.4) 0.5060�Schizoaffective disorder 8 (13.1) 20 (21.7) 4 (19.0) 14 (13.7)Schizophreniform disorder 0 (0.0) 0 (0.0) 0 (0.0) 3 (2.9)Psychosis NOS 0 (0.0) 0 (0.0) 1 (4.8) 5 (4.9)
Previous hospitalization, n (%) 24 (39.3) 26 (28.3) 11 (52.4) 45 (44.1) 0.0738Drugs: past abuse, n (%) 19 (31.1) 31 (33.7) 2 (9.5) 27 (26.5) 0.1492Positive symptoms, n (%) 45 (75.0) 56 (60.9) 17 (81.0) 60 (59.4) 0.0809Negative symptoms, n (%) 44 (73.3) 72 (78.3) 17 (81.0) 76 (75.2) 0.8752Cognitive symptoms, n (%) 31 (51.7) 47 (51.1) 10 (47.6) 51 (50.5) 0.9810
BPRS, Brief Psychiatric Rating Scale; SOFAS, Social and Occupational Functioning Assessment Scale; CGI-Improvement, Clinical Global Impression of Illness-Improvement; Sep/Div/Wid, separated/divorced/widowed; Married/C-L, married/common-law; NOS, not otherwise specified.�To avoid empty cells �all schizophrenia subtypes� were compared to �all other diagnoses�.*P-value indicates statistical significance at the 0.05 level.
Medications Inpatient Outpatient Non-medical Indirect
TreatmentGroup
Clozapine
Olanzapine
Quetiapine
Risperidone
Average Monthly Cost ($CAN*)$0.00 $200.00 $400.00 $600.00 $800.00 $1000.00 $1200.00 $1400.00 $1600.00
Fig. 1. Average unadjusted patients costs per month; 1-yearcohort.
Kopala et al.
32
trol for the variation in these baseline characteris-tics such as gender, drug, duration of illness priorto enrollment and baseline BPRS (see Material andmethods). Employing this method, RIS had thelowest year 1 cohort drug and in-patient costs. TheQUE-treated group had the lowest out-patientcost, followed by RIS.When assessing the adjusted relative rates of ER
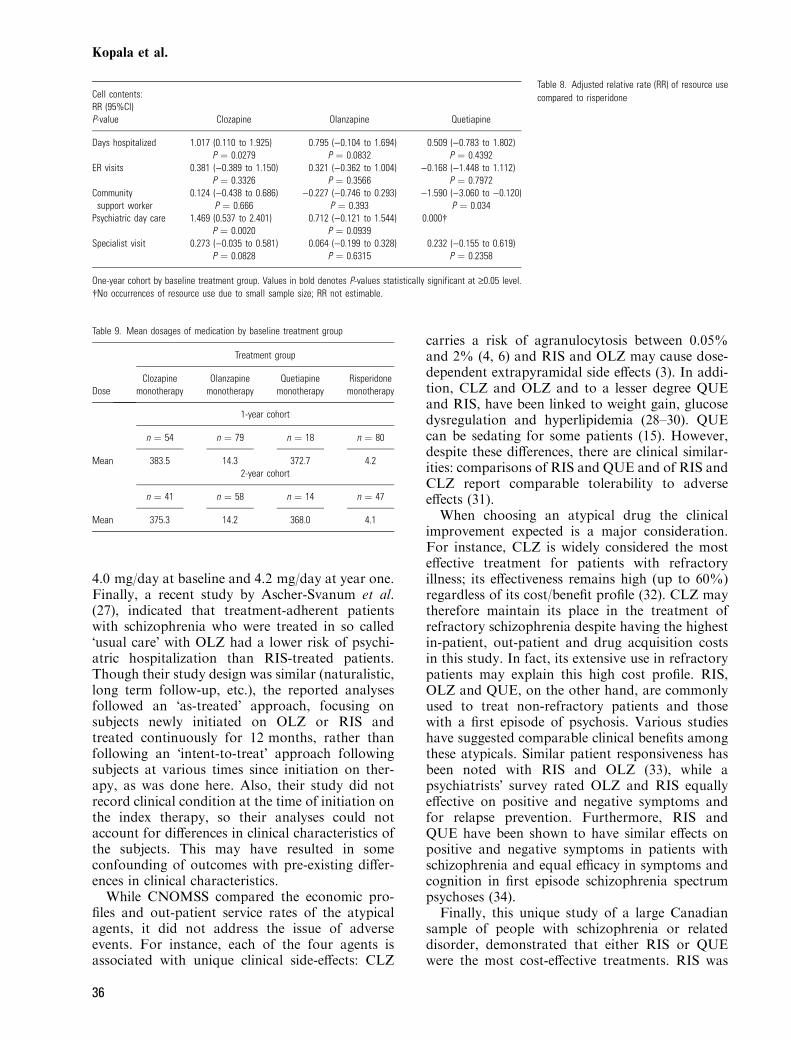
visits there were no statistically significant differ-ences among the four groups (Table 8). However,the QUE-treated group had the lowest hospital-ization days compared with RIS, CLZ and OLZ(Table 7). Total adjusted costs were lowest forQUE ($293.09) (US $190.95), compared to RIS($527.96, P ¼ 0.5321) ($343.97 US), OLZ($830.77, P ¼ 0.1875) (US $541.25) and CLZ($1472.60, P ¼ 0.0005) (US $959.40). QUE, fol-lowed by RIS, had the lowest out-patient costs.Compared to RIS, psychiatric day care utilizationwas highest for CLZ- and OLZ-treated patientsbut not the QUE group. Using this same approach,visits to specialists was statistically higher for theCLZ group (relative to RIS) (Table 8).
Discussion
Canadian National Outcomes Measurement Studyin Schizophrenia is the first Canadian study toprospectively evaluate the pharmacoeconomiccosts and resource use associated with anti-psychotic drug treatment of patients with schizo-phrenia and related psychotic disorders in anaturalistic setting. Since Canada’s health care
utilizes a single-payer system, it was possible tocollect the cost data associated with each treatmentin a comprehensive manner. Furthermore, theresults of this study are widely applicable, due tothe inclusion of a broad age-range of patients (18–69 years) from both urban and rural settings.Patients were also enrolled at various time pointsafter initiation of therapy and were treated accord-ing to standard clinical protocols, thus adding tothe generalizability of the results.The main findings of the study were that the
total adjusted 1- and 2-year costs were lowest forQUE, followed by RIS and then OLZ and CLZ.Drug acquisition costs were lowest for RIS forboth the 1- and 2-year cohorts. Clozapine use waspredictably associated with the highest overall andmedication costs at both 1 and 2 years. Olanzapinewas only lower than the other three drugs forindirect costs at both time points.Limitations include the non-randomized study
design, possible changes to routine clinical practiceover the course of the study, the reliability ofpatient submission of data and the relatively smallnumber of patients taking QUE. This last pointmay be due to the fact that QUE only becameavailable while the study was ongoing. In addition,this latter group was treated with relatively lowdoses of medication given that the majority of thepatients were chronically ill. The mean dose ofQUE for the 1-year cohort was 373 mg/day and368 mg/day for the 2-year cohort (Table 9). In thisregard, data from a first episode of schizophreniaindicated that the mean dose required was close to600 mg/day (15). As first episode patients generallyrequire lower doses of medication than people withmore chronic illness, these findings suggest that thedoses used in the group treated with QUE were notlikely representative of patients with chronic ill-ness. Adding to this argument is data from Smallet al. (16), who found that patients with chronicschizophrenia treated with either 250 or 750 mg/day of QUE had statistically significant superiorsymptom improvement when receiving 750 mg/day. Given these findings and the fact that a muchsmaller proportion of the QUE group were pastsubstance abusers, indicated that this group maynot have been similar to the three other groups.Therefore, the most reliable comparisons are likelythose between CLZ, RIS and OLZ.An additional uncontrolled variable was the
availability of non-pharmacological interventionsand other services employed by different regions.The latter would be likely to show some variabilityacross the country and between academic and non-academic centers and could not be controlled for incomparing costs across various drugs.
Table 4. Unadjusted hospital costs per patient/month in 1- and 2-year cohorts foreach baseline treatment group in Canadian dollars�
Resourceuse costcategory
Treatment group
Allpatients
Clozapinemonotherapy
Olanzapinemonotherapy
Quetiapinemonotherapy
Risperidonemonotherapy
1-year cohort
n ¼ 54 n ¼ 79 n ¼ 18 n ¼ 80 n ¼ 231
ER 19.42 5.50 3.61 5.24 8.50In-patient ICU 12.88 0.00 0.00 1.91 3.67In-patient 458.90 110.13 177.40 45.49 173.96Total 491.20 115.63 181.01 52.65 186.13
2-year cohort
n ¼ 41 n ¼ 58 n ¼ 14 n ¼ 47 n ¼ 160
ER 14.82 5.26 4.72 6.40 7.93In-patient ICU 10.44 10.60 0.00 14.03 10.91In-patient 374.92 142.11 159.39 61.27 171.75Total 400.17 157.97 164.12 81.69 190.60
$US conversion rate ¼ 0.6515 (14).ER, emergency room; ICU, intensive care unit.�$Can. 2002 per patient/month.
RU in Canadian national study
33

With reference to other studies, Conley et al.,reported lower hospitalization rates with RIS thanwith CLZ (17). While Conley et al., found similar
rehospitalization rates for the two drugs up tomonth 10. They also found that the rehospitaliza-tion rates for RIS were higher than those for CLZbetween months 10 and 26. However, this studywas fundamentally different from CNOMSS withregards to the patient cohort examined. The studyby Conley et al., only followed patients who wereinitially hospitalized, while it is very possible thatCNOMSS patients were started on their respectivedrugs without initial hospitalization. Therefore, itcannot be excluded that RIS may have preventedthe initial hospitalization event. As well, in contrastto Conley et al., another study by Rabinowitzet al., displayed nearly equivalent rehospitalizationrates for both RIS and CLZ (18). It is alsointeresting to note that Kelly et al., found thatdischarge rates were higher for RIS patients than
Table 5. Unadjusted out-patient costs per patient/month in 1- and 2-year cohorts for each baselinetreatment group in Canadian dollars�
Resourceuse costcategory
Treatment group
Allpatients
Clozapinemonotherapy
Olanzapinemonotherapy
Quetiapinemonotherapy
Risperidonemonotherapy
1-year cohort
n ¼ 54 n ¼ 79 n ¼ 18 n ¼ 80 n ¼ 231
Family doctor 20.46 15.06 14.03 12.48 15.34Specialist 71.07 50.88 72.91 49.37 56.76Counselor/psychologist 25.65 14.59 7.17 11.74 15.59Social worker 17.57 7.38 2.06 6.68 9.09Psychiatric nurse 38.54 13.14 6.69 17.37 20.03OT/RT 41.76 35.36 14.69 15.38 28.27Community support worker 4.35 2.71 1.03 3.35 3.18Depot injection clinic 3.75 0.81 0.84 0.21 1.29Suicide/crisis services 0.15 0.16 0.35 0.32 0.23Alcohol/drug rehab 1.66 17.06 2.98 10.23 10.00Group/family therapy 5.58 1.85 0.29 7.02 4.40Home care nurse visits 1.21 4.62 0.50 0.24 1.98Lab/diagnostic tests 46.64 4.91 6.90 3.40 14.25Psychiatric day care 364.43 134.00 0.00 121.31 172.81Total 642.83 302.53 130.44 259.10 353.22
2-year cohort
n ¼ 41 n ¼ 58 n ¼ 14 n ¼ 47 n ¼ 160
Family doctor 21.74 15.58 12.37 12.43 15.72Specialist 73.57 48.85 67.61 49.42 56.53Counselor/psychologist 26.82 14.31 8.65 10.53 15.58Social worker 17.94 6.80 3.18 7.62 9.50Psychiatric nurse 37.11 14.73 7.08 17.31 20.44OT/RT 44.35 35.17 11.26 15.95 28.81Community support worker 4.28 2.77 1.03 3.12 3.12Depot injection clinic 4.04 0.50 2.51 0.50 1.52Suicide/crisis services 0.07 0.15 0.41 0.21 0.17Alcohol/drug rehab 0.83 19.83 5.20 9.23 10.38Group/family therapy 4.53 1.33 0.18 7.45 4.14Home care nurse visits 1.95 4.82 0.42 0.34 2.21Lab/diagnostic tests 46.76 5.76 6.57 4.31 15.25Psychiatric day care 435.85 129.52 0.00 118.82 189.75Total 719.82 300.12 126.48 257.24 373.11
$US conversion rate ¼ 0.6515 (14).OT/RT, occupational or recreational therapist.�$Can. 2002 per patient/month.
Medications Inpatient Outpatient Non-medical Indirect
TreatmentGroup
Clozapine
Olanzapine
Quetiapine
Risperidone
Average monthly cost ($CAN*)
$0.00 $200.00 $400.00 $600.00 $800.00 $1000.00 $1200.00 $1400.00 $1600.00
Fig. 2. Average unadjusted patients costs per month; 2-yearcohort.
Kopala et al.
34
for OLZ patients, indicating that the use of RISmay decrease hospitalization time (19). Malla et al.also found lower rates of and delayed rehospital-ization for first episode patients treated with RIScompared to typical antipsychotics (20).As well as hospitalization rates and costs,
CNOMSS also considered drug costs. RIS was
the least expensive, followed by QUE, then OLZand CLZ. RIS costs were less than half the cost ofOLZ [see Table 3 (unadjusted costs) and Table 7(adjusted costs)]. While no other studies directlycompared these four atypical drugs, studies com-paring RIS to either OLZ or CLZ predominantlysupport these findings. For instance, Lewis et al.,reported that the overall costs associated with RISwere lower than those associated with OLZ andCLZ (21). This latter study determined themonthly service costs for each drug and includedmodalities such as psychiatric admission, socialservices and occupational therapy in the economicevaluation. Monthly service costs for CLZ andOLZ were found to be US $1589 higher and US$1006 higher than for RIS respectively. In terms ofdrug acquisition cost, numerous studies demon-strated that the cost of RIS was lower than that ofCLZ or OLZ (19, 22–24). Interestingly, however,the drug cost of CLZ in Israel appears to be lowerthan that for RIS (25).Other authors have compared in-patient and
out-patient costs between RIS and OLZ patients(10). Although the differences in the total perpatient medical costs between these two drugs werenot statistically different, this study did find RIS tobe more costly than OLZ. A possible explanationcomes from the parent study conducted by Tranet al. (26), in which higher RIS dosages (mean RISdosage of 7.9 mg/day) than those seen in routineclinical practice were used. In the currentCNOMSS study, the mean dose of RIS was
Table 6. Unadjusted non-medical costs per patient/month in 1- and 2-year cohorts for each baselinetreatment group in Canadian dollars�
Resourceuse costcategory
Treatment group
Allpatients
Clozapinemonotherapy
Olanzapinemonotherapy
Quetiapinemonotherapy
Risperidonemonotherapy
1-year cohort
(n ¼ 54) (n ¼ 79) (n ¼ 18) (n ¼ 80) (n ¼ 231)
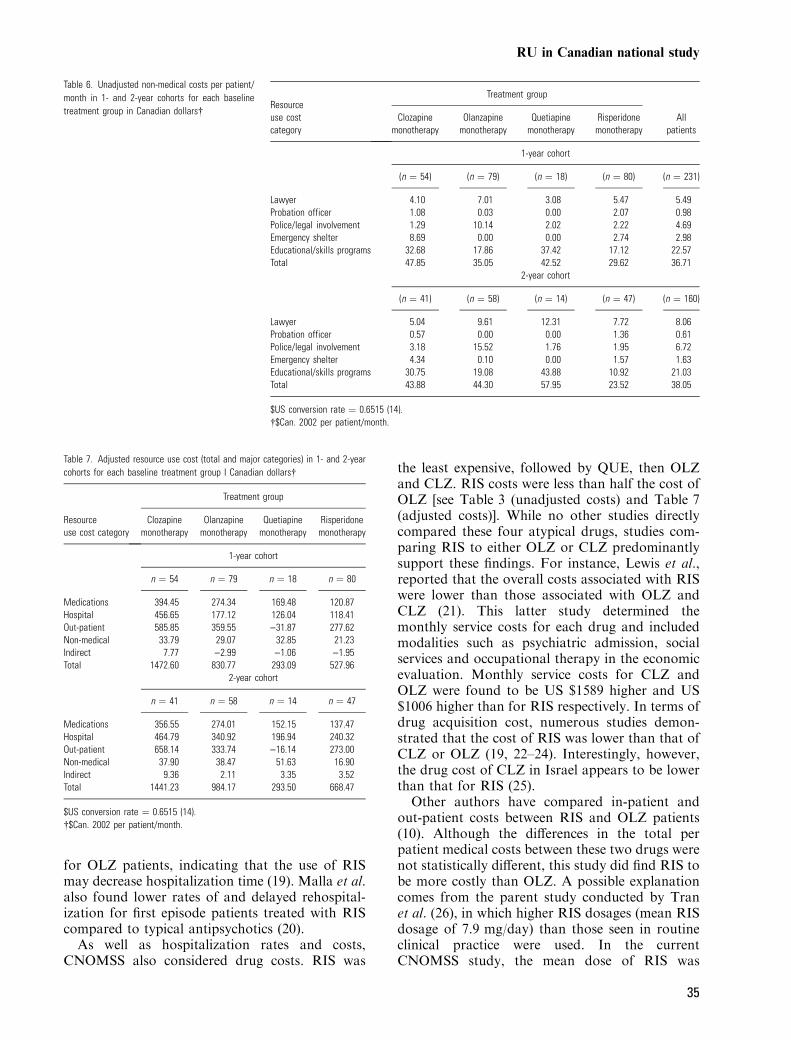
Lawyer 4.10 7.01 3.08 5.47 5.49Probation officer 1.08 0.03 0.00 2.07 0.98Police/legal involvement 1.29 10.14 2.02 2.22 4.69Emergency shelter 8.69 0.00 0.00 2.74 2.98Educational/skills programs 32.68 17.86 37.42 17.12 22.57Total 47.85 35.05 42.52 29.62 36.71
2-year cohort
(n ¼ 41) (n ¼ 58) (n ¼ 14) (n ¼ 47) (n ¼ 160)
Lawyer 5.04 9.61 12.31 7.72 8.06Probation officer 0.57 0.00 0.00 1.36 0.61Police/legal involvement 3.18 15.52 1.76 1.95 6.72Emergency shelter 4.34 0.10 0.00 1.57 1.63Educational/skills programs 30.75 19.08 43.88 10.92 21.03Total 43.88 44.30 57.95 23.52 38.05
$US conversion rate ¼ 0.6515 (14).�$Can. 2002 per patient/month.
Table 7. Adjusted resource use cost (total and major categories) in 1- and 2-yearcohorts for each baseline treatment group I Canadian dollars�
Resourceuse cost category
Treatment group
Clozapinemonotherapy
Olanzapinemonotherapy
Quetiapinemonotherapy
Risperidonemonotherapy
1-year cohort
n ¼ 54 n ¼ 79 n ¼ 18 n ¼ 80
Medications 394.45 274.34 169.48 120.87Hospital 456.65 177.12 126.04 118.41Out-patient 585.85 359.55 )31.87 277.62Non-medical 33.79 29.07 32.85 21.23Indirect 7.77 )2.99 )1.06 )1.95Total 1472.60 830.77 293.09 527.96
2-year cohort
n ¼ 41 n ¼ 58 n ¼ 14 n ¼ 47
Medications 356.55 274.01 152.15 137.47Hospital 464.79 340.92 196.94 240.32Out-patient 658.14 333.74 )16.14 273.00Non-medical 37.90 38.47 51.63 16.90Indirect 9.36 2.11 3.35 3.52Total 1441.23 984.17 293.50 668.47
$US conversion rate ¼ 0.6515 (14).�$Can. 2002 per patient/month.
RU in Canadian national study
35
4.0 mg/day at baseline and 4.2 mg/day at year one.Finally, a recent study by Ascher-Svanum et al.(27), indicated that treatment-adherent patientswith schizophrenia who were treated in so called�usual care� with OLZ had a lower risk of psychi-atric hospitalization than RIS-treated patients.Though their study design was similar (naturalistic,long term follow-up, etc.), the reported analysesfollowed an �as-treated� approach, focusing onsubjects newly initiated on OLZ or RIS andtreated continuously for 12 months, rather thanfollowing an �intent-to-treat� approach followingsubjects at various times since initiation on ther-apy, as was done here. Also, their study did notrecord clinical condition at the time of initiation onthe index therapy, so their analyses could notaccount for differences in clinical characteristics ofthe subjects. This may have resulted in someconfounding of outcomes with pre-existing differ-ences in clinical characteristics.While CNOMSS compared the economic pro-
files and out-patient service rates of the atypicalagents, it did not address the issue of adverseevents. For instance, each of the four agents isassociated with unique clinical side-effects: CLZ
carries a risk of agranulocytosis between 0.05%and 2% (4, 6) and RIS and OLZ may cause dose-dependent extrapyramidal side effects (3). In addi-tion, CLZ and OLZ and to a lesser degree QUEand RIS, have been linked to weight gain, glucosedysregulation and hyperlipidemia (28–30). QUEcan be sedating for some patients (15). However,despite these differences, there are clinical similar-ities: comparisons of RIS and QUE and of RIS andCLZ report comparable tolerability to adverseeffects (31).When choosing an atypical drug the clinical
improvement expected is a major consideration.For instance, CLZ is widely considered the mosteffective treatment for patients with refractoryillness; its effectiveness remains high (up to 60%)regardless of its cost/benefit profile (32). CLZ maytherefore maintain its place in the treatment ofrefractory schizophrenia despite having the highestin-patient, out-patient and drug acquisition costsin this study. In fact, its extensive use in refractorypatients may explain this high cost profile. RIS,OLZ and QUE, on the other hand, are commonlyused to treat non-refractory patients and thosewith a first episode of psychosis. Various studieshave suggested comparable clinical benefits amongthese atypicals. Similar patient responsiveness hasbeen noted with RIS and OLZ (33), while apsychiatrists� survey rated OLZ and RIS equallyeffective on positive and negative symptoms andfor relapse prevention. Furthermore, RIS andQUE have been shown to have similar effects onpositive and negative symptoms in patients withschizophrenia and equal efficacy in symptoms andcognition in first episode schizophrenia spectrumpsychoses (34).Finally, this unique study of a large Canadian
sample of people with schizophrenia or relateddisorder, demonstrated that either RIS or QUEwere the most cost-effective treatments. RIS was
Table 8. Adjusted relative rate (RR) of resource usecompared to risperidoneCell contents:
RR (95%CI)P-value Clozapine Olanzapine Quetiapine
Days hospitalized 1.017 (0.110 to 1.925)P ¼ 0.0279
0.795 ()0.104 to 1.694)P ¼ 0.0832
0.509 ()0.783 to 1.802)P ¼ 0.4392
ER visits 0.381 ()0.389 to 1.150)P ¼ 0.3326
0.321 ()0.362 to 1.004)P ¼ 0.3566
)0.168 ()1.448 to 1.112)P ¼ 0.7972
Communitysupport worker
0.124 ()0.438 to 0.686)P ¼ 0.666
)0.227 ()0.746 to 0.293)P ¼ 0.393
)1.590 ()3.060 to )0.120)P ¼ 0.034
Psychiatric day care 1.469 (0.537 to 2.401)P ¼ 0.0020
0.712 ()0.121 to 1.544)P ¼ 0.0939
0.000�
Specialist visit 0.273 ()0.035 to 0.581)P ¼ 0.0828
0.064 ()0.199 to 0.328)P ¼ 0.6315
0.232 ()0.155 to 0.619)P ¼ 0.2358
One-year cohort by baseline treatment group. Values in bold denotes P-values statistically significant at ‡0.05 level.�No occurrences of resource use due to small sample size; RR not estimable.
Table 9. Mean dosages of medication by baseline treatment group
Dose
Treatment group
Clozapinemonotherapy
Olanzapinemonotherapy
Quetiapinemonotherapy
Risperidonemonotherapy
1-year cohort
n ¼ 54 n ¼ 79 n ¼ 18 n ¼ 80
Mean 383.5 14.3 372.7 4.22-year cohort
n ¼ 41 n ¼ 58 n ¼ 14 n ¼ 47
Mean 375.3 14.2 368.0 4.1
Kopala et al.
36

associated with the lowest drug acquisition costsfor both the 1-year and 2-year cohorts whencompared to the three other drugs. Subsequentstudies, employing a larger, more representativesample of patients treated with more current,optimal doses of QUE are now required to addressoutstanding questions.
Acknowledgements
This study was sponsored by Janssen-Ortho, Inc. and admin-istered by Syreon Corporation, Canada.The Scientific Advisory Committee:Dr Lili Kopala, Vancouver, BCDr Ashok Malla, Montreal, PQDr Geoff Smith, Vancouver, BCDr Richard Williams, Victoria, BCWe acknowledge the participation of the members of theCNOMSS group:Dr Jean-Michel Beau, Malartic; Dr Linda Beauclair, Montreal;Dr Pierre Chue, Edmonton; Dr Hubert Colohan, Claresholm;Dr Norman Costigan, Red Deer; Dr John Dougan, Acton;Dr Angelo Fallu, Sherbrooke; Dr Brian Hoffman, Toronto;Dr Sunny Johnson, Mississauga; Dr Jamie Karagianis,St Johns; Dr Lili Kopala, Halifax; Dr Ivan Kowalchuk,Winnipeg; Dr Alain Labelle, Ottawa; Dr Pierre Landry,Montreal; Dr Paul Latimer, Kelowna; Nadia Lesnikova,Vancouver; Dr Henry Leung, Sault Ste Marie; Dr WilsonLit, Guelph; Dr Ashok Malla, London; Dr Fiona McGregor,Vernon; Dr Alexander McIntyre, Penticton; Dr CharlesMesser, Regina; Dr Roumen Milev, Regina; Dr HeatherMilliken, Halifax; Dr Javad Moamai, Hull; Dr David Mulhall,Kentville; Dr Saibal Nandy, Medicine Hat; Dr KizhakeRamachandran, North Battleford; Dr Jeff Reiss, Winnipeg;Dr Satish Shrikhande, Saskatoon; Dr Jatindar Takhar,London; Dr Mark Triantifillou, Charlottetown; Dr NormanWhite, Powell River; Dr Richard Williams, Victoria.
Declaration of Interests
G. Smith, L. Kopala, R. Williams and A. Malla are consultantsfor Janssen-Ortho. Love and Balshaw are employees of SyreonCorporation, the contract research organization hired byJanssen-Ortho to collect, manage and analyze the data fromCNOMSS. Statistics were performed by D. Talling andR. Balshaw, Syreon Corporation.The protocol is available from Janssen-Ortho, Inc., bycontacting Doanh Luong ([email protected]).
References
1. Goeree R, O’Brien BJ, Goering P et al. The economicburden of schizophrenia in Canada. Can J Psychiatry1999;44:464–472.
2. Statistics-Canada. Consumer Price Index: historical sum-mary. http://www.40.statcan.ca/101/cst01/econ46.htm(accessed August 25, 2004). 2004.
3. Brown CS, Markowitz JS, Moore TR, Parker NG. Atypicalantipsychotics: part II: adverse effects, drug interactions,and costs. Ann Pharmacother 1999;33:210–217.
4. Worrel JA, Marken PA, Beckman SE, Ruehter VL. Atyp-ical antipsychotic agents: a critical review. Am J HealthSyst Pharm 2000;57:238–255.
5. Revicki DA. Cost effectiveness of the newer atypical anti-psychotics: a review of the pharmacoeconomic researchevidence. Curr Opin Investig Drugs 2001;2:110–117.
6. Campbell M, Young PI, Bateman DN, Smith JM, ThomasSH. The use of atypical antipsychotics in the managementof schizophrenia. Br J Clin Pharmacol 1999;47:13–22.
7. Galvin PM, Knezek LD, Rush AJ, Toprac MG, Johnson B.Clinical and economic impact of newer vs. older antipsy-chotic medications in a community mental health center.Clin Ther 1999;21:1105–1116.
8. Cohen LJ. Looking beyond the formulary budget in cost-benefit analysis. Am J Manag Care 1997;3(Suppl.): S11–S17.
9. Glazer WM, Ereshefsky L. A pharmacoeconomic model ofoutpatient antipsychotic therapy in �revolving door� schi-zophrenic patients. J Clin Psychiatry 1996;57:337–345.
10. Edgell ET, Andersen SW, Johnstone BM, Dulisse B, RevickiD, Breier A. Olanzapine vs. risperidone. A prospectivecomparison of clinical and economic outcomes in schizo-phrenia. Pharmacoeconomics 2000;18:567–579.
11. Almond SO, O’Donnell O. Cost analysis of the treatment ofschizophrenia in the UK. A simulation model comparingolanzapine, risperidone and haloperidol. Pharmacoeco-nomics 2000;17:383–389.
12. Bhana N, Foster RH, Olney R, Plosker GL. Olanzapine:an updated review of its use in the management of schi-zophrenia. Drugs 2001;61:111–161.
13. SmithG,MallaA,WilliamsR,KopalaL,LoveL,BalshawR.The Canadian National Outcomes Measurement Study inSchizophrenia: overview of the patient sample and meth-odology. Acta Psychiatr Scand 2006;113(Suppl. 430):2–9.
14. Canada, B.o. Rates and statistics – exchange rates.http://www.bankofcanada.ca/en/rates/exchange.html (ac-cessed October 17, 2005), 2005.
15. Kopala LC, Good KP, Milliken H et al. Treatment of a firstepisode of psychotic illness with quetiapine: an analysis of2 year outcomes. Schizophr Res 2006;81:29–39.
16. Small JG, Hirsch SR, Arvanitis LA, Miller BG, Link
CG. Quetiapine in patients with schizophrenia. A high-and low-dose double-blind comparison with placebo.Seroquel Study Group. Arch Gen Psychiatry1997;54:549–557.
17. Conley RR, Love RC, Kelly DL, Bartko JJ. Rehospitali-zation rates of patients recently discharged on a regimen ofrisperidone or clozapine. Am J Psychiatry 1999;156:863–868.
18. Rabinowitz J, Lichtenberg P, Kaplan Z, Mark M, Nahon D,Davidson M. Rehospitalization rates of chronically illschizophrenic patients discharged on a regimen of risperi-done, olanzapine, or conventional antipsychotics. Am JPsychiatry 2001;158:266–269.
19. Kelly DL, Nelson MW, Love RC, Yu Y, Conley RR.Comparison of discharge rates and drug costs for patientswith schizophrenia treated with risperidone or olanzapine.Psychiatr Serv 2001;52:676–678.
20. Malla AK, Norman R, Zirul S, Scholten D, Kotteda V. Acomparison of long-term outcome in first episode schizo-phrenia patients treated with risperidone or typical anti-psychotics. J Clin Psychiatry 2001;62:179–184.
21. Lewis M, McCrone P, Frangou S. Service use and costs oftreating schizophrenia with atypical antipsychotics. J ClinPsychiatry 2001;62:749–756.
22. Procyshyn RM, Zerjav S. Drug utilization patterns andoutcomes associated with in-hospital treatment with ris-peridone or olanzapine. Clin Ther 1998;20:1203–1217;discussion 1192–1203.
RU in Canadian national study
37

23. Rabinowitz J, Lichtenberg P, Kaplan Z. Comparison of cost,dosage and clinical preference for risperidone and olanza-pine. Schizophr Res 2000;46:91–96.
24. Zhao Z. A retrospective economic evaluation of olanzapinevs. risperidone in the treatment of schizophrenia. ManagCare Interface 2002;15:75–81.
25. Ginsberg G, Shani S, Lev B. Cost-benefit analysis of ris-peridone and clozapine in the treatment of schizophreniain Israel. Pharmacoeconomics 1998;13:231–241.
26. Tran PV, Hamilton SH, Kuntz AJ et al. Double-blindcomparison of olanzapine vs. risperidone in the treatmentof schizophrenia and other psychotic disorders. J ClinPsychopharmacol 1997;17:407–418.
27. Ascher-Svanum H, Zhu B, Faries D, Ernst FR. A compar-ison of olanzapine and risperidone on the risk of psychi-atric hospitalization in the naturalistic treatment ofpatients with schizophrenia. Ann Gen Hosp Psychiatry2004;3:11.
28. Conley RR, Meltzer HY. Adverse events related to ola-nzapine. J Clin Psychiatry 2000;61(Suppl. 8):26–29; dis-cussion 30.
29. Meyer J. Cardiovascular illness and hyperlipidemia in pa-tients with schizophrenia. In: Meyer JM, Nasrallah H, eds.Medical illness and schizophrenia. Washington D.C.APPI, 2003:58–89.
30. Jin H, Meyer JM, Jeste DV. Phenomenology of and riskfactors for new-onset diabetes mellitus and diabeticketoacidosis associated with atypical antipsychotics: ananalysis of 45 published cases. Ann Clin Psychiatry2002;14:59–64.
31. Azorin JM, Spiegel R, Remington G et al. A double-blindcomparative study of clozapine and risperidone in themanagement of severe chronic schizophrenia. Am J Psy-chiatry 2001;158:1305–1313.
32. Sharif ZA, Raza A, Ratakonda SS. Comparative efficacy ofrisperidone and clozapine in the treatment of patients withrefractory schizophrenia or schizoaffective disorder: a ret-rospective analysis. J Clin Psychiatry 2000;61:498–504.
33. Gilbody SM, Bagnall AM, Duggan L, Tuunainen A. Ris-peridone vs. other atypical antipsychotic medication forschizophrenia. Cochrane Database Syst Rev 32000;CD002306.
34. Mullen J, Jibson MD, Sweitzer D. A comparison of therelative safety, efficacy, and tolerability of quetiapine andrisperidone in outpatients with schizophrenia and otherpsychotic disorders: the quetiapine experience with safetyand tolerability (QUEST) study. Clin Ther 2001;23:1839–1854.
Appendix 1
Summary of the preparation and update of the cost dictionary for the Canadian National Outcomes Study in Schizophrenia (CNOMSS)
The cost dictionary employed in the economic analysis performed for the CNOMSS study was derived to provide analytical researchpersonnel with clear, concise, detailed information on the cost assumptions for each of the economic resource elements collected.This cost dictionary accesses high-level cost information from one Canadian province (British Columbia). Originally created in 1999,the document was reviewed and updated again in 2003. Costs were obtained through several known, documented sources, including:
• The BC Medical Association Guide to Fees, 15 Dec 2002,
• Medical Services Plan of British Columbia (MSP) 2002 Guide to Fees,
• Health Sciences Association of BC,
• Union of Psychiatric Nurses, Physiotherapy Association of British Columbia,
• Occupational Therapy Society of British Columbia,
• Homelessness – Causes & Effects: The Costs of Homelessness in BC,
• Ministry of Social Development and Economic Security, 2001.
Detailed information for each element included the definition, data source(s) for information, the measurement and calculationsused, the unit value derived from the calculations and any additional assumptions used.Costs in the current dictionary are based on Canadian currency (2002). Historical costs have been updated by applying the annualincrease in the Canadian Consumer Price Index (CPI). The year and average inflation increase are documented below.
Year % annual increase
1989 5.01990 4.81991 5.61992 1.51993 1.81994 2.01995 2.21996 1.61997 1.61998 0.91999 1.72000 2.72001 2.62002 2.2
Kopala et al.
38
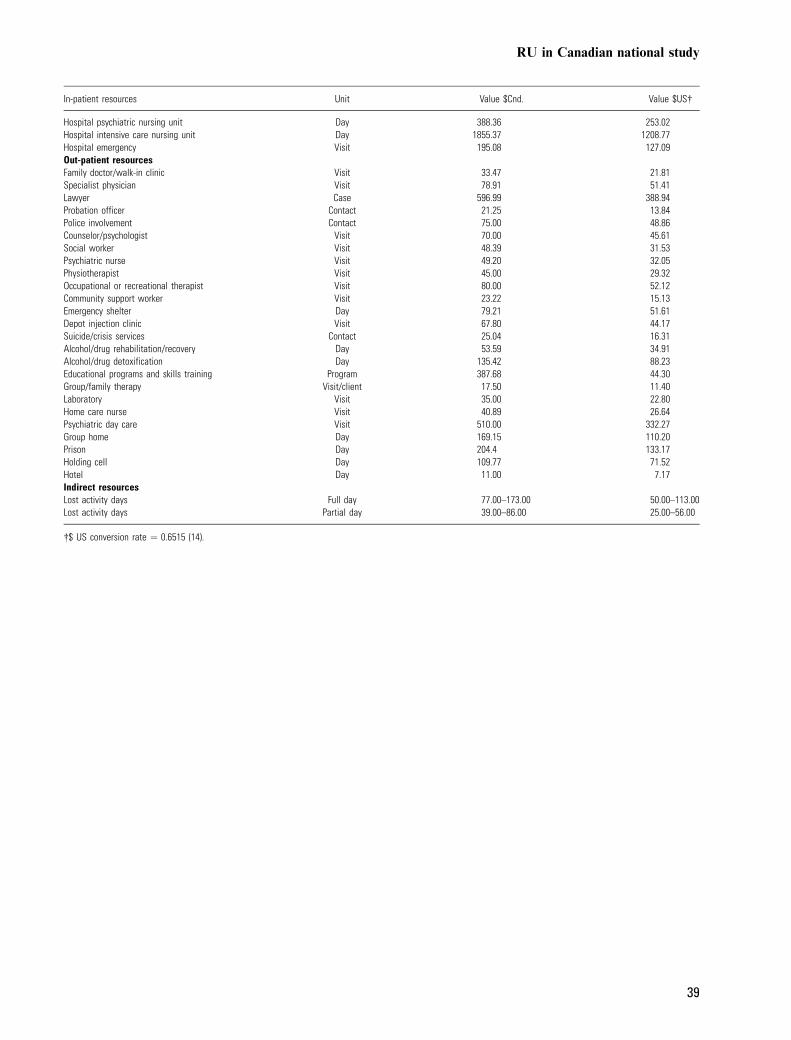
In-patient resources Unit Value $Cnd. Value $US�
Hospital psychiatric nursing unit Day 388.36 253.02Hospital intensive care nursing unit Day 1855.37 1208.77Hospital emergency Visit 195.08 127.09Out-patient resourcesFamily doctor/walk-in clinic Visit 33.47 21.81Specialist physician Visit 78.91 51.41Lawyer Case 596.99 388.94Probation officer Contact 21.25 13.84Police involvement Contact 75.00 48.86Counselor/psychologist Visit 70.00 45.61Social worker Visit 48.39 31.53Psychiatric nurse Visit 49.20 32.05Physiotherapist Visit 45.00 29.32Occupational or recreational therapist Visit 80.00 52.12Community support worker Visit 23.22 15.13Emergency shelter Day 79.21 51.61Depot injection clinic Visit 67.80 44.17Suicide/crisis services Contact 25.04 16.31Alcohol/drug rehabilitation/recovery Day 53.59 34.91Alcohol/drug detoxification Day 135.42 88.23Educational programs and skills training Program 387.68 44.30Group/family therapy Visit/client 17.50 11.40Laboratory Visit 35.00 22.80Home care nurse Visit 40.89 26.64Psychiatric day care Visit 510.00 332.27Group home Day 169.15 110.20Prison Day 204.4 133.17Holding cell Day 109.77 71.52Hotel Day 11.00 7.17Indirect resourcesLost activity days Full day 77.00–173.00 50.00–113.00Lost activity days Partial day 39.00–86.00 25.00–56.00
�$ US conversion rate ¼ 0.6515 (14).
RU in Canadian national study
39
Copyright © 2022 FDOKUMEN




















